The Shoulder Joint. Scapulohumeral Rhythm Function: Maximize ROM Maintain glenoid fossa in optimal...
40
The Shoulder Joint
-
date post
21-Dec-2015 -
Category
Documents
-
view
234 -
download
2
Transcript of The Shoulder Joint. Scapulohumeral Rhythm Function: Maximize ROM Maintain glenoid fossa in optimal...

The Shoulder Joint

Scapulohumeral Rhythm
Function: Maximize ROM Maintain glenoid fossa in optimal
position Maintain optimal length-tension
relationship
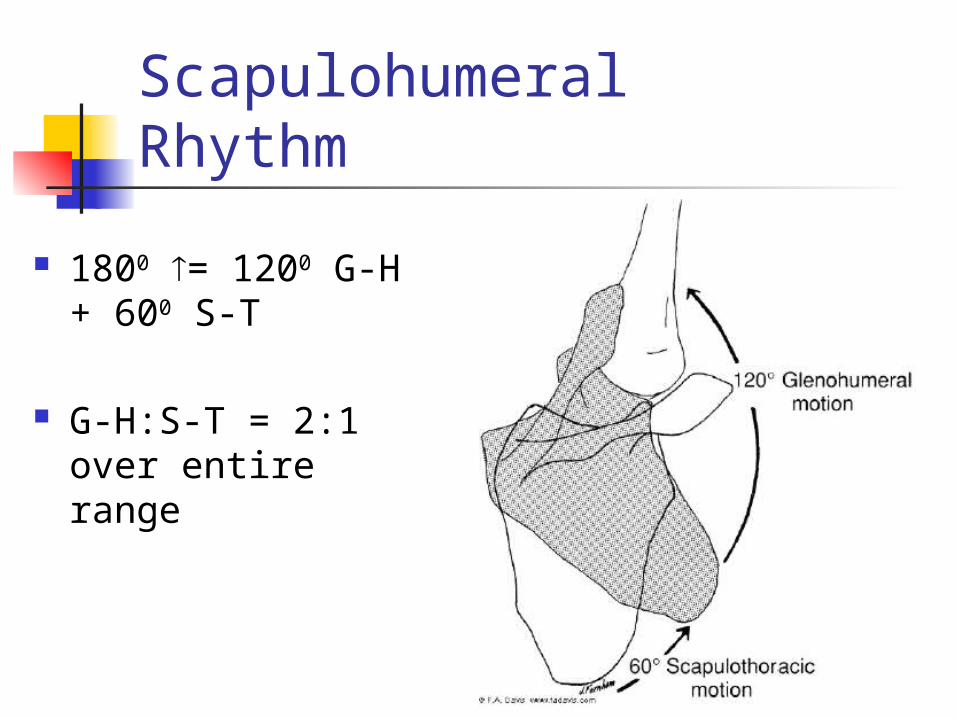
Scapulohumeral Rhythm
1800 = 1200 G-H + 600 S-T
G-H:S-T = 2:1 over entire range

Scapulohumeral RhythmPre-phase/Setting
Inconsistent amount of scapula movement Proximal STABILITY for distal mobility
G-H - 600 or 300 abduction
Total = 30-600 (all G-H motion)

Scapulohumeral RhythmPhase I / S-T Motion
Trapezius (upper & lower) & Serratus Anterior (upper & lower) contract
Coracoclavicular ligament tightens (locks AC joint)

Scapulohumeral RhythmPhase I / S-T Motion
Clavicle elevates ~ 300 thru SC joint
Costoclavicular ligament tightens
Tipping and 100 of winging

Scapulohumeral RhythmPhase I / S-T Motion
Total motion following Phase I:
300 of scapula rotation occurring at SC jt.
~ 300 of G-H movement

Scapulohumeral RhythmPhase I / S-T Motion
Total elevation = 30-600 (pre-phase G-H) 300 (S-T rotation)
+ 300 (G-H movement)90 – 1200 of total elevation
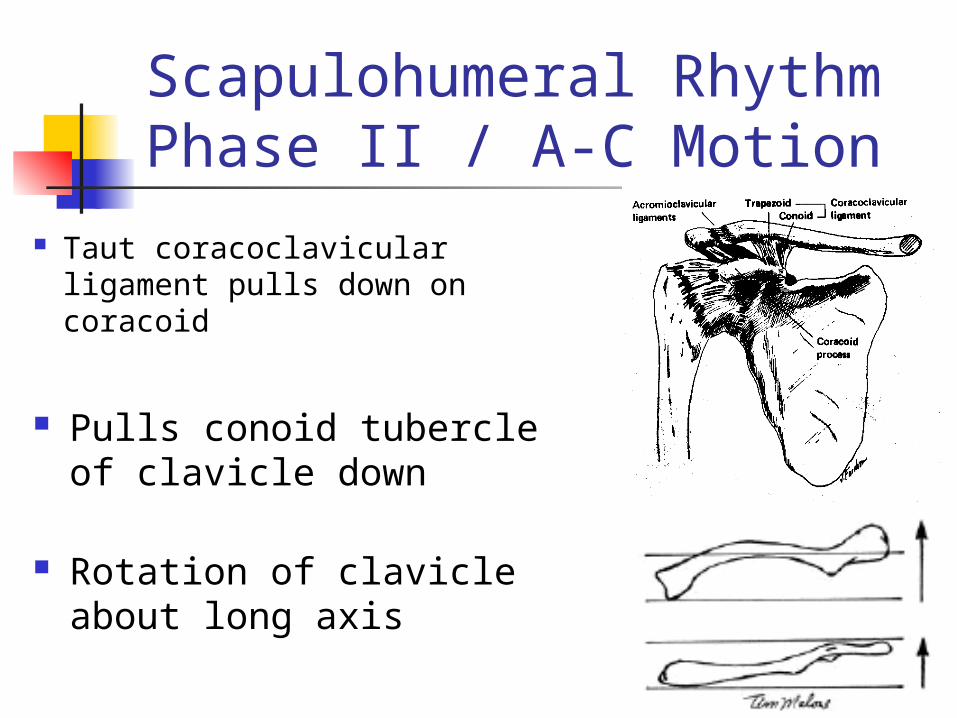
Scapulohumeral RhythmPhase II / A-C Motion
Taut coracoclavicular ligament pulls down on coracoid
Pulls conoid tubercle of clavicle down
Rotation of clavicle about long axis

Scapulohumeral RhythmPhase II / A-C Motion
Rotation of scapula about axis through A-C joint
200 tipping / 400 winging

Scapulohumeral RhythmPhase II / A-C Motion
Total elevation = 90 - 1200 (pre-phase + phase I) 300 (S-T rotation)
+ 30-600 (G-H movement) 1800
Scapulohumeral RhythmSummary
0 to 900 = 600 GH / 300 SH about SC joint
900 to 1800 = 600 GH / 300 SH about AC joint

Acromioclavicular Sprain
Plane-synovial joint
Intraarticular disk – degenerates w/ age
Separation
Acromioclavicular Sprain
Mechanisms: Direct force
Indirect force (less frequent)outstretched arm
Acromioclavicular Sprain
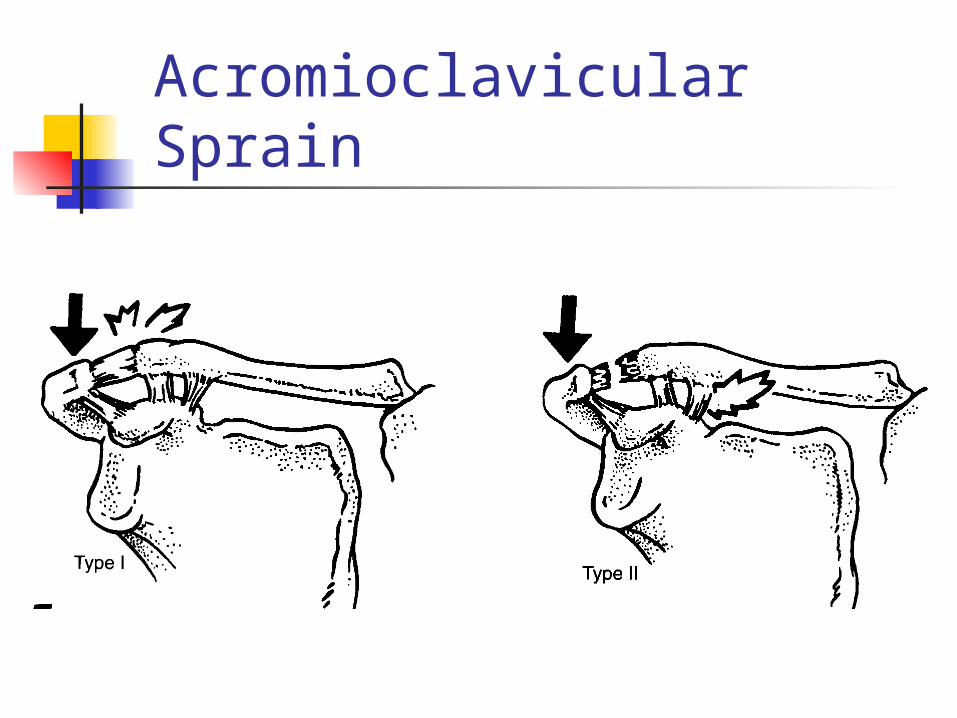
I: sprain of AC ligaments
II: tear of AC ligament / sprain of coracoclavicular
Acromioclavicular Sprain

Acromioclavicular Sprain
III: tear of AC and coracoclavicular ligaments
IV: torn ligaments / posterior displacement of clavicle

Acromioclavicular Sprain

Acromioclavicular Sprain
V: torn ligaments / inferior displacement of clavicle
VI: torn ligaments / clavicle driven into subacromial / subcoracoid position

Acromioclavicular Sprain

Glenohumeral Joint
Stability - intracapsular pressure (20-32 lbs.)
Concavity compression
Capsuloligamentous structures
Glenohumeral Joint
Stability Scapulohumeral balance ()
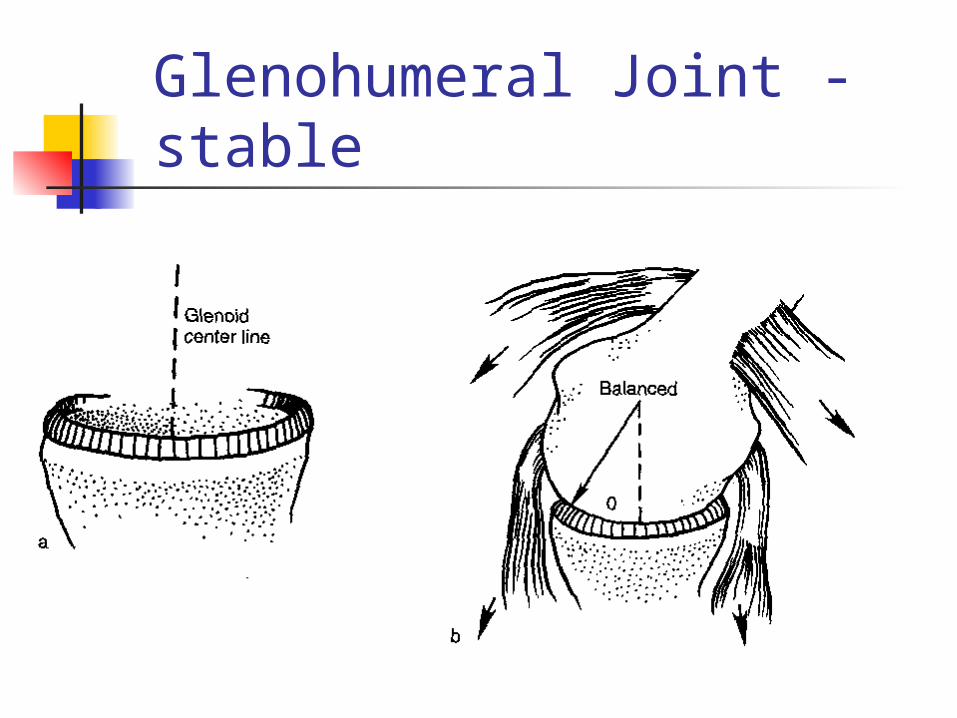
Glenohumeral Joint - stable

Glenohumeral Joint -unstable

Glenohumeral Joint
Dislocation > 90% anterior
Indirect
Direct

Glenohumeral Joint

Glenohumeral Joint
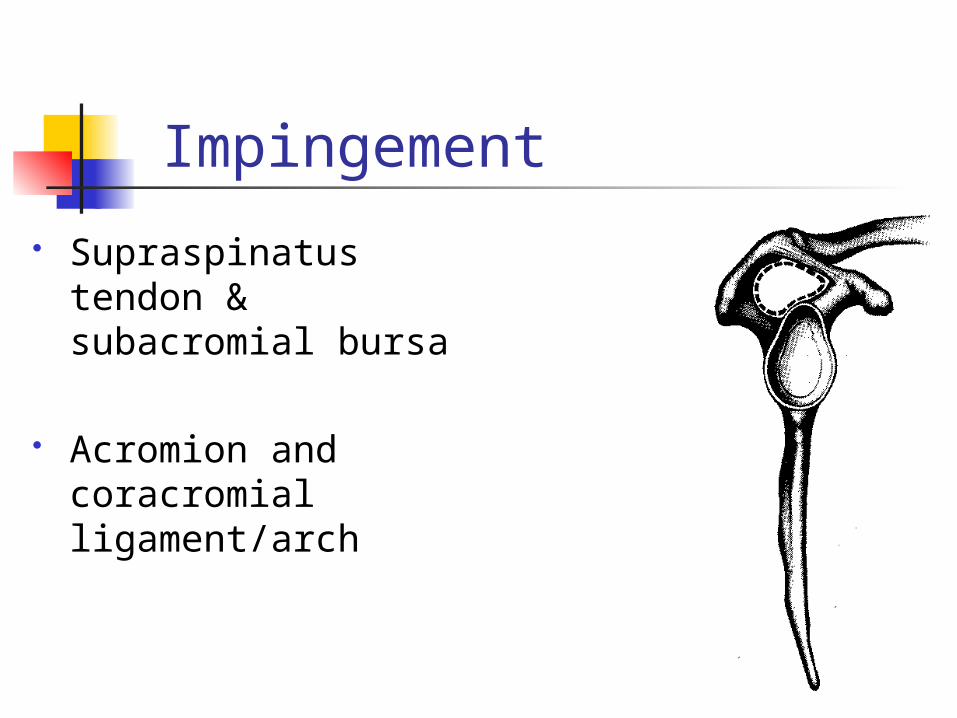
Impingement
Supraspinatus tendon & subacromial bursa
Acromion and coracromial ligament/arch
Impingement
Repetitive (< 35 y.o.)
Degenerative (> 35 y.o) spur formation capsular thinning tissue perfusion muscular atrophy
Repetitive Impingement
Repeated abduction stresses capsuloligamentous & musculotendinous
Tissue microtrauma tissue failure
GH instability subluxation

Impingement
Classification:I. Isolated impingement w/ no instabilityII. Overuse 20 overhead activities
instability w/ secondary impingementIII. II but w/ generalized (systemic)
ligamentous laxityIV. Traumatic – indirect or direct

Mechanisms of RTC Impingement
Extrinsic - forces outside RTC structural characteristics of
subacromial space
Intrinsic - inflammatory changes within the cuff

Extrinsic
Structural acromion shape
hooked > flat or curved
Spurs stress risers

Extrinsic
Structural Supraspinatu
s outlet
Intrinsic
Inherent due to compromised blood flow 20:
Impingement pressures Avascularity

Risk Factors
Awkward / static postures Heavy work Direct load bearing Repetitive UE movement Overhead movements

Populations
W/C athletes Pitchers Swimmers
RTC Rupture
Inflammation microtearing partial or full rupture
Compromised tissue integrity & muscle fatigue altered movement patterns

Kinematic Patterns w/ RTC Tears
I – stable fulcrum – supraspinatus & part of infra normal motion / near-normal strength
II – unstable fulcrum – supraspinatus & infra and TM disruption of force couples

Kinematic Patterns w/ RTC Tears
III – captured fulcrum – supraspinatus, post cuff, subscapularis centering of humeral head humeral elevation
IV – unstable fulcrum – supraspinatus & complete subscapularis disruption of force couples poor elevation