THE ROLE OF THE LABORATORY - Home | Curry International ...
25
TB CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE March 27-30, 2017 Curry International Tuberculosis Center, UCSF 300 Frank H. Ogawa Plaza, Suite 520 Oakland, CA; Office (510) 238-5100 THE ROLE OF THE LABORATORY LEARNING OBJECTIVES Upon completion of this session, participants will be able to: 1. Describe three laboratory methods used in the diagnosis and control of TB resulting in a better understanding of laboratory results and improved communication between the clinician, the laboratory, and the patient INDEX OF MATERIALS PAGES 1. The Role of the Laboratory– slide outline Presented by: Mark Pandori, Ph.D., H.C.L.D. (A.B.B.) 1-22 SUPPLEMENTAL MATERIAL None
Transcript of THE ROLE OF THE LABORATORY - Home | Curry International ...

TB CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE March 27-30, 2017
Curry International Tuberculosis Center, UCSF 300 Frank H. Ogawa Plaza, Suite 520 Oakland, CA; Office (510) 238-5100
THE ROLE OF THE LABORATORY
LEARNING OBJECTIVES
Upon completion of this session, participants will be able to:
1. Describe three laboratory methods used in the diagnosis and control of TB resulting in a better understanding of laboratory results and improved communication between the clinician, the laboratory, and the patient
INDEX OF MATERIALS PAGES
1. The Role of the Laboratory– slide outline Presented by: Mark Pandori, Ph.D., H.C.L.D. (A.B.B.)
1-22
SUPPLEMENTAL MATERIAL
None
TB CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE March 27-30, 2017
Curry International Tuberculosis Center, UCSF 300 Frank H. Ogawa Plaza, Suite 520 Oakland, CA; Office (510) 238-5100
ADDITIONAL REFERENCES
• CDC. Availability of an Assay for Detecting Mycobacterium tuberculosis, Including Rifampin- Resistant Strains, and Considerations for Its Use – United States, 2013. MMWR 2013;62 (No.41) October 18, 2013.
• CDC. Guide to the application of genotyping to tuberculosis prevention and control.
Page last updated September 1, 2012. www.cdc.gov/tb/programs/genotyping/manual.htm
• CDC. Report of an expert consultation on the uses of nucleic acid amplification tests for the diagnosis of tuberculosis. Page last updated September 1, 2012. www.cdc.gov/tb/publications/guidelines/amplification_tests/background.htm
• WHO. Drug-resistant tuberculosis. Frequently asked questions. January 2012. http://www.who.int/tb/challenges/mdr/tdrfaqs/en/# (Accessed November 10, 2014).
• CDC. Updated Guidelines for Using Interferon Gamma Release Assays to Detect
Mycobacterium tuberculosis Infection, United States. MMWR 2010; 59 (No.RR-5) See CDC factsheet Interferon-Gamma Release Assays (IGRAs). Page last updated September 1, 2012. http://www.cdc.gov/tb/publications/factsheets/testing/IGRA.htm
• Chang-Hong, S., Xiao-Wu, W., Hai, Z., et al. Immune responses and protective efficacy
of the gene vaccine expressing Ag85B and ESAT6 fusion protein from Mycobacterium tuberculosis. DNA Cell Biol. 2008 Apr;27(4):199-207.
• Honscha, G., Von Groll, A., Valenca, M., et al. The laboratory as a tool to qualify
tuberculosis diagnosis. Int. J. Tuberc Lung Dis. 2008;12(2):218-20.
• Perez-Martinez, I., Ponce-De-Leon, A., Bobadilla, M., et al. A novel identification scheme for genus Mycobacterium, M.tuberculosis complex, and seven mycobacteria species of human clinical impact. Eur. J. Clin. Microbiol. Infect. Dis. 2008;27(6):451-459.
• Barman, P., Gadre, D., A study of phage based diagnostic technique for tuberculosis. Indian J. Tuberc. Jan. 2007; 54(1):36-40.
• Haldar, S., Chakravorty, S., Bhalla, M., De Majumdar, S., Tyagi, JS. Simplified detetion of Mycobacterium tuberculosis in sputum using smear microscopy and PCR with molecular beacons. J. Med. Microbiol. 2007;56(Pt.10):1356-62.
• Nahid, P., Pai, M., Hopewell, P. Advances in the diagnosis and treatment of tuberculosis. Proc. Am. Thorac. Soc. 2006; 3:103-110.
TB CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE March 27-30, 2017
Curry International Tuberculosis Center, UCSF 300 Frank H. Ogawa Plaza, Suite 520 Oakland, CA; Office (510) 238-5100
• Somoskovi, A., Dormandy, J., Mitsani, D., Rivenburg, J., Salfinger, M. Use of smearpositive
samples to assess the PCR-based genotype MTBDR assay for rapid, direct detection of the Mycobacterium tubercuslosis complex as well as its resistance to isoniazid and rifampin. J. Clin. Microbiol. 2006;44(12):4459-4463.
• Lin, G., Probert, W., Lo, M., Desmond, E. Rapid detection of isoniazid and rifampin
resistance mutations in Mycobacterium tuberculosis complex from cultures or smearpositive sputa by use of molecular beacons. J. Cli. Microbiol. 2004;42(5):4204-4208.
• Barnes, P., Cave, D. Molecular epidemiology of tuberculosis. NEJM. 2003;349(12): 1149-1155. Review article.
• Dowdy, D.W., Maters, A., Parrish, N., Beyer, C., Dorman, S.E. Cost-effectiveness
analysis of the gen-probe amplified mycobacterium tuberculosis direct test as used routinely on smear-positive respiratory specimens. J. Clin. Microbiol. 2003;41(3):948-53.
• Drobniewski, F.A., Caws, M., Gibson, A., Young, D. Modern laboratory diagnosis of
tuberculosis. Lancet Infect. Dis. 2003;3(3):141-47.
• Van Der Zanden, A.G., Te Kopppele-Vije, E.M., Vijaya Bhanu, N., et al. Use of DNA extracts from Ziehl-Neelsen-stained slides for molecular detection of rifampin resistance and spoligotyping of Mycobacterium tuberculosis. J. Clin. Microbiol. 2003;41(3):1101-08.
• Gillespie, S. Minireview. Evolution of drug resistance in Mycobacterium tuberculosis:
clinical and molecular perspective. Antimicrob. Agents Chemother. 2002;46(2):267-274.
• Mostowy, S., Behr, M.A., Comparative genomics in the flight against tuberculosis: diagnostics, epidemiology and BCG vaccination. Am. J. Pharmacogenomics. 2002;2(3):189-196.
• Somoskovi, A., Mester, J., Hale, Y.M., Parsons, L.M., Salfinger, M. Laboratory diagnosis of nontuberculous mycobacteria. Clin. Chest Med. 2002;23(3):585-597.
• Breese, P.E., Burman, W.J., Hildred, M., et al. The effect of changes in laboratory
practices on the rate of false-positive cultures for Mycobacterium tuberculosis. Arch Pathol. Lab Med. 2001;125(9):1213-1216.
• Somoskovi, A., Parsons, L.M., Salfinger, M. The molecular basis of resistance to
isoniazid, rifampin, and pyrazinamide in Mycobacterium tuberculosis. Respir. Res. 2001;2(3):164-168.
• Hale, Y.M., Desmond, E.P., Jost, K.C., Jr., Salfinger, M. Access to newer laboratory procedures: a call for action. Int. J. Tuberc Lung Dis. 2000;4(12 suppl 2):S171-175.
Role of the Laboratory1
TB Case Management and Contact Investigation IntensiveMarch 27-30, 2017Curry International Tuberculosis Center
LABORATORY
METHODS:
Mycobacterium
tuberculosis
Mark W. PandoriAlameda County Public Health Laboratory
Oakland, CA 510‐268‐2700
Presentation Goals
Discuss specimen collection
Microscopy & Culture (growth): “traditional” identification Including susceptibility testing
Nucleic Acid based detection (aka “molecular” testing
Slides:
ACPHL, M.W.P.
Dr. Ed Desmond, CDPHL
The United States Agency for International Development (USAID) TB Response (TBCARE 1)
Role of the Laboratory2
TB Case Management and Contact Investigation IntensiveMarch 27-30, 2017Curry International Tuberculosis Center
Specimen collection and transport
• Specimens (sputum, bronchial washings, urine, etc.) should be collected in a laboratory-approved sterile, leak-proof, non-breakable container
• Containers must be labeled with patient’s name and date collected
• Collect specimens prior to initiation of therapy
Specimen collection and transport (2)
Sputum is the most common specimen• Collect 5-10 mls of an early morning
specimen, prior to eating
• Usually 3 specimens on 3 different days are recommended for diagnosis
Specimen collection and transport (3)
Contaminated specimens can be minimized by:
• Instructing the patient to rinse mouth with preferably sterile water before collecting the specimen
• Returning the specimen to the lab as soon as feasible after collection
Role of the Laboratory3
TB Case Management and Contact Investigation IntensiveMarch 27-30, 2017Curry International Tuberculosis Center
Specimen collection and transport (4)
o Indicate type of specimen on laboratory requisition form
o Keep all specimens refrigerated and transport as soon as possible to the lab
How many specimens to collect?
The greater the number of specimens, the higher the probability of a positive
Law of diminishing returns: 4 specimens doesn’t give many more positives than 3, so 3 is usual guideline
Processing pulmonary specimens Digestion and decontamination
Pulmonary specimens are exposed to a mucolytic agent to dissolve mucin and to liquefy the specimen
N-acetyl-L-cysteine (NALC) is the most common mucolytic agent used
Role of the Laboratory4
TB Case Management and Contact Investigation IntensiveMarch 27-30, 2017Curry International Tuberculosis Center
Processing pulmonary specimens (2)o Digestion and decontamination
• Specimens are also treated with a liquid decontaminant, generally sodium hydroxide, a strong alkali which is more toxic to oral flora than AFB
• Material is concentrated by centrifugation
MTB are “Acid Fast Bacilli” (AFB)
Once they are stained (with any of a variety of stains)
-they resist de-colorization by acid-alcohol treatment
-they have waxy, tough outer membranes and walls
Staining concentrated smear Fluorescent stains
• Fluorochrome stained smears require a fluorescent microscope
• Auramine-rhodamine is an example of such a stain where the AFB appear yellow against a black background

Role of the Laboratory5
TB Case Management and Contact Investigation IntensiveMarch 27-30, 2017Curry International Tuberculosis Center
Carbol fuchsin-based stains• Utilize a regular light microscope• Must be read at a higher magnification• Two types: Ziehl-Neelsen and Kinyoun. (ZN is
more sensitive)• Smear is then decolorized with acid-(HCI)
alcohol and counter-stained with methylene blue
Staining concentrated smear (2)
From CDC Lab Manual

Role of the Laboratory6
TB Case Management and Contact Investigation IntensiveMarch 27-30, 2017Curry International Tuberculosis Center
REPORTING AFB SMEAR RESULTS*
Number of AFB found: Report:
0 Negative
1-2 / 300 fields
1-9 / 100 fields 1+
1-9 / 10 fields 2+
1-9 / field 3+
>9 / field 4+
*CDC System (WHO system goes up to 3+ only)
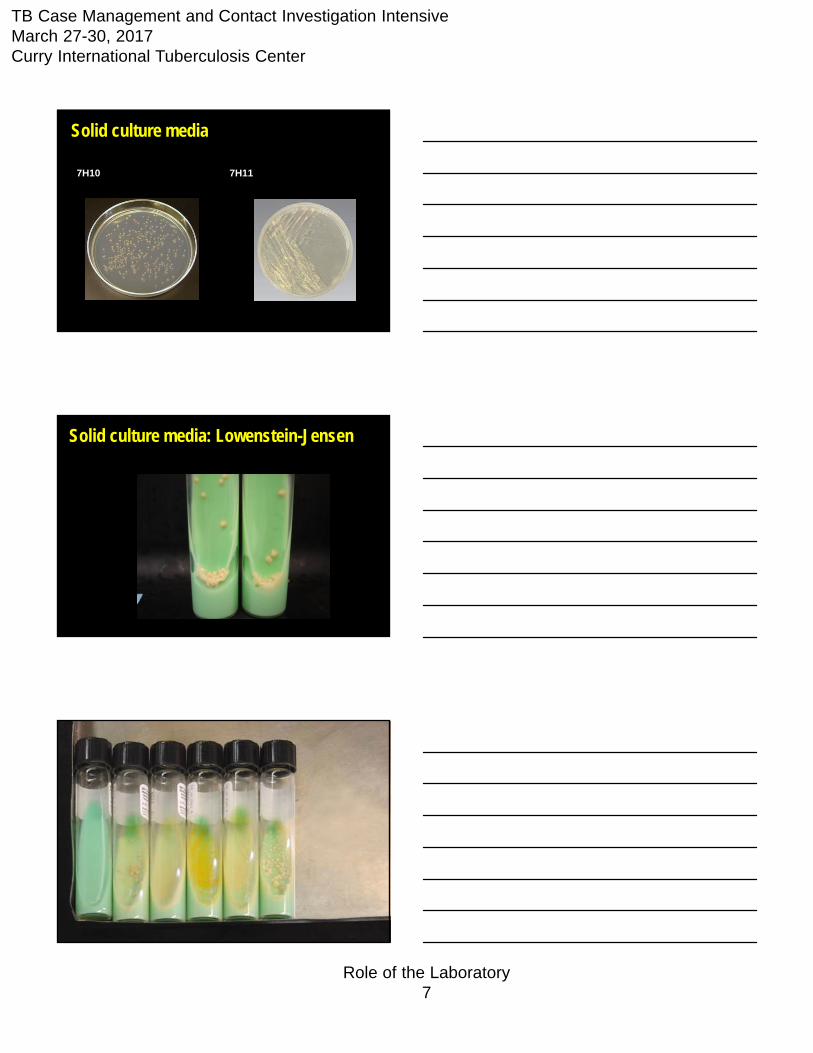
Growth media for culture: 2 kinds of mediaSolid media
Two types most commonly used are:
• Lowenstein-Jensen (egg-based)
• Middlebrook 7H10 or 7H11
Liquid Media
Essentially one: 7H9
The “MGIT” broth
It is: Liquid 7h10 minus the Vit. B6 and malachite green
Growth media for culture:Advantages of solid media:
Organisms (colonies) can be seen on the surface of the medium; morphology is visible
If there is mixed growth or contamination, picking individual colonies can allow you to obtain a pure culture
Role of the Laboratory7
TB Case Management and Contact Investigation IntensiveMarch 27-30, 2017Curry International Tuberculosis Center
Solid culture media
7H10 7H11
Solid culture media: Lowenstein-Jensen

Role of the Laboratory8
TB Case Management and Contact Investigation IntensiveMarch 27-30, 2017Curry International Tuberculosis Center
Liquid media• Liquid or broth medium has the advantage of
allowing detection of AFB more quickly• Drug susceptibility testing using growth in
liquid media leads to more rapid reporting of results
• Examples of liquid media are Trek and MGIT systems
Inoculating growth media for culture
MGIT Incubator

Role of the Laboratory9
TB Case Management and Contact Investigation IntensiveMarch 27-30, 2017Curry International Tuberculosis Center
Accuracy problems in the TB lab False positive results, due to:
o Cross-contamination during specimen processing
o Specimen mix-up or mislabeling
Inadequate primary culture media (some labs use only solid media)
Identification of acid-fast bacilli (AFB)
Growth characteristics (preliminary ID) Preliminary indication of M. tb can be made from
physical parameters (in addition to microscopic observation)• Rate of growth; temperature• Colonial morphology• Pigmentation
Rate of growth
Rapid-grower: isolated in less than a week not TB
Slow-grower: usually 3 weeks, up to 6 weeks could be TB

Role of the Laboratory10
TB Case Management and Contact Investigation IntensiveMarch 27-30, 2017Curry International Tuberculosis Center
Growth temperature
Incubation: 36 ± 1 °C
M. tuberculosis does not grow at lower or higher temperatures.
Pigment production
Non-chromogen TB
Chromogens non-TB
Colonial Morphology
Smooth Rough
Role of the Laboratory11
TB Case Management and Contact Investigation IntensiveMarch 27-30, 2017Curry International Tuberculosis Center
Biochemical tests There is a battery of 8-12 biochemical tests used
to differentiate within the mycobacterium genus Nitrate reduction and niacin accumulation are
definitive for M. tb
Identification of acid-fast bacilli (AFB)
Biochemical tests
Niacin production Nitrate reduction Catalase negative at 68 °C
Always use pure cultures, otherwise they will yield false results.
Test should be performed in the BSC – aerosols are produced.
Nucleic acid probe tests (non-amplified)
Requires a pure colony of organism DNA probe tests are species-specific Require less time than biochemical tests for
identification Commercial probes are available for M. tb
complex, MAC, M. kansasii and M. gordonae
Identification of acid-fast bacilli (AFB)

Role of the Laboratory12
TB Case Management and Contact Investigation IntensiveMarch 27-30, 2017Curry International Tuberculosis Center
High performance liquid chromatography (HPLC)
• HPLC uses a chromatography method to identify mycobacteria based on their mycolic acid profiles (cell wall composition)
• Instrument is expensive/usually reserved for larger laboratories
MALDI-TOF aka “Mass Spec.” (matrix assisted laser desorption ionization-time of flight) is now being validated
Like HPLC, expensive instrument, but quicker
Identification of acid-fast bacilli (AFB) (2)
Susceptibility testing of M. tuberculosisWhen to test: All primary M. tb isolates from patients should
be tested isolates from relapse or re-treatment cases when drug resistance is suspected
Susceptibility testing of M. tuberculosis (2)Methods for susceptibility testing
• Agar proportion method compares growth on agar media with and without one of the four primary drugs
• Broth based (MGIT, Trek)–Requires inoculation of the strain in broth with each
of the (5) primary drugs, plus control vial–Growth of the strain in a vial with a drug indicates
resistance to that drug

Role of the Laboratory13
TB Case Management and Contact Investigation IntensiveMarch 27-30, 2017Curry International Tuberculosis Center
MGIT System (Becton Dickinson)
Nucleic Acid Amplification Tests
AKA “Molecular” Tests

Role of the Laboratory14
TB Case Management and Contact Investigation IntensiveMarch 27-30, 2017Curry International Tuberculosis Center
Molecular Tests-- Allow for direct detection of MTB in a clinical
specimen
-- No culture required; they amplify DNA/RNA
-- Highly specific
-- Very fast
CDC guidelines recommend as standard of practice
Will allow quicker diagnosis in some smear neg patients
Only if patients are true TB suspects
Only for untreated patients
test smear negatives when clinical suspicion of TB is moderate or high
Molecular Tests (2)
More recommendations to use Molecular/ NAAT Pascopella (2004) J. Clin. Microbiol 42:4209
For smear neg patients, health care providers often/typically don’t start Rx until culture is +
Results in a delay in initiation of Rx, typically ~3 weeks
NAA would detect many of these patients, earlier initiation of Rx
MMWR guidelines: Jan. 16, 2009 58(1):7-10
Role of the Laboratory15
TB Case Management and Contact Investigation IntensiveMarch 27-30, 2017Curry International Tuberculosis Center
2 FDA Approved NAA Tests• Cepheid GeneXpert and Gen-Probe MTD test– the
only FDA-approved options
– MTD is labor intensive and time consuming
– MTD may be the most sensitive method
– GeneXpert easy to do; provides drug susceptibility data
Homebrew / RUO Tests• All are PCR -based
• Homebrew: rather inexpensive
• Performance can be excellent (See Halse & Musser JCM 2010, NYS lab)
But:
• They can require much more initial set-up / quality control
NAAT methods: challenges• Culture still rules: higher sensitivity
-higher specimen volume is tested by culture than by NAAT (MTD & GeneXpert may be exceptions)
-TB is a bit tougher than other organisms
-sputum often doesn’t contain many MTB organisms(compared to viral specimens (herpes, flu etc..) for example)
Role of the Laboratory16
TB Case Management and Contact Investigation IntensiveMarch 27-30, 2017Curry International Tuberculosis Center
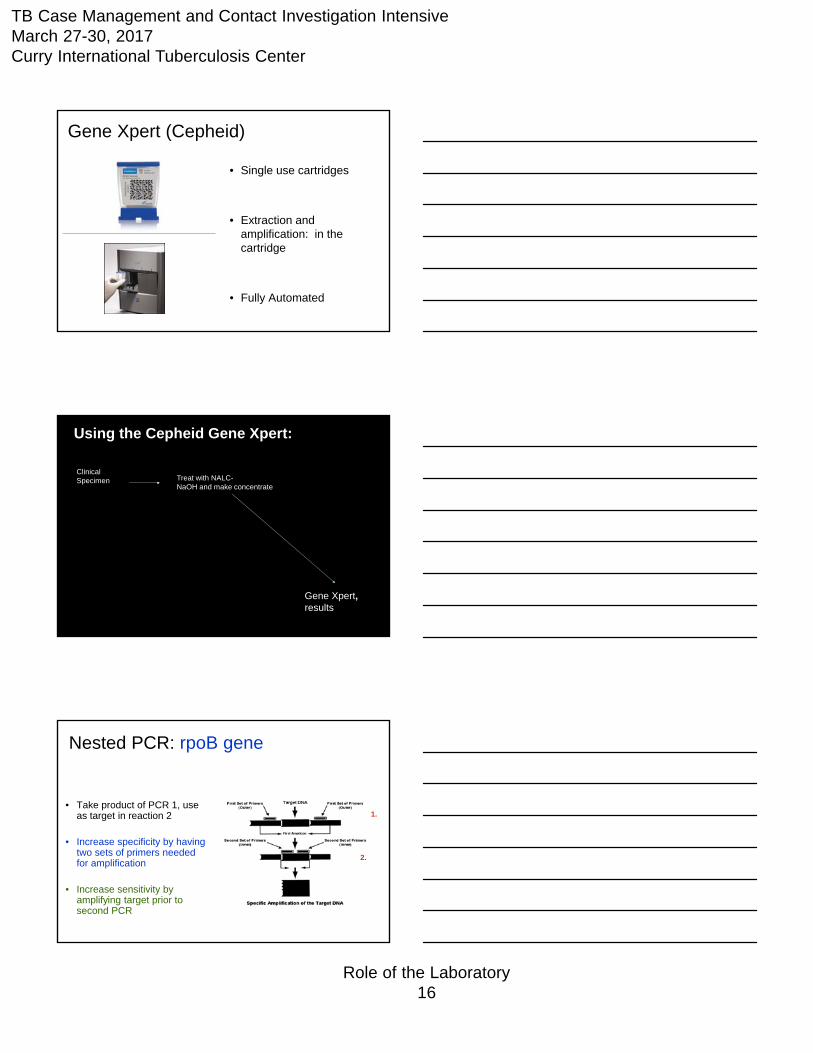
Gene Xpert (Cepheid)
• Single use cartridges
• Extraction and amplification: in the cartridge
• Fully Automated
Clinical Specimen
Gene Xpert,results
Using the Cepheid Gene Xpert:
Treat with NALC-NaOH and make concentrate
Nested PCR: rpoB gene
• Take product of PCR 1, use as target in reaction 2
• Increase specificity by having two sets of primers needed for amplification
• Increase sensitivity by amplifying target prior to second PCR
1.
2.

Role of the Laboratory17
TB Case Management and Contact Investigation IntensiveMarch 27-30, 2017Curry International Tuberculosis Center
Target DNA sequence: rpoB gene
• The target of rifampin: RNA polymerase subunit B
• PCR amplifies a small region relevant for rifampin resistance; uses 5 probes to assess for mutations
probes
Cepheid MTB: positive result
• five probes
-assay has anInternal PCRControl (for inhibitionassessment)
Test gives semi-quantitative results: “high”, “medium”, “low”, “very low” and “negative”
Cepheid MTB: negative result
Role of the Laboratory18
TB Case Management and Contact Investigation IntensiveMarch 27-30, 2017Curry International Tuberculosis Center
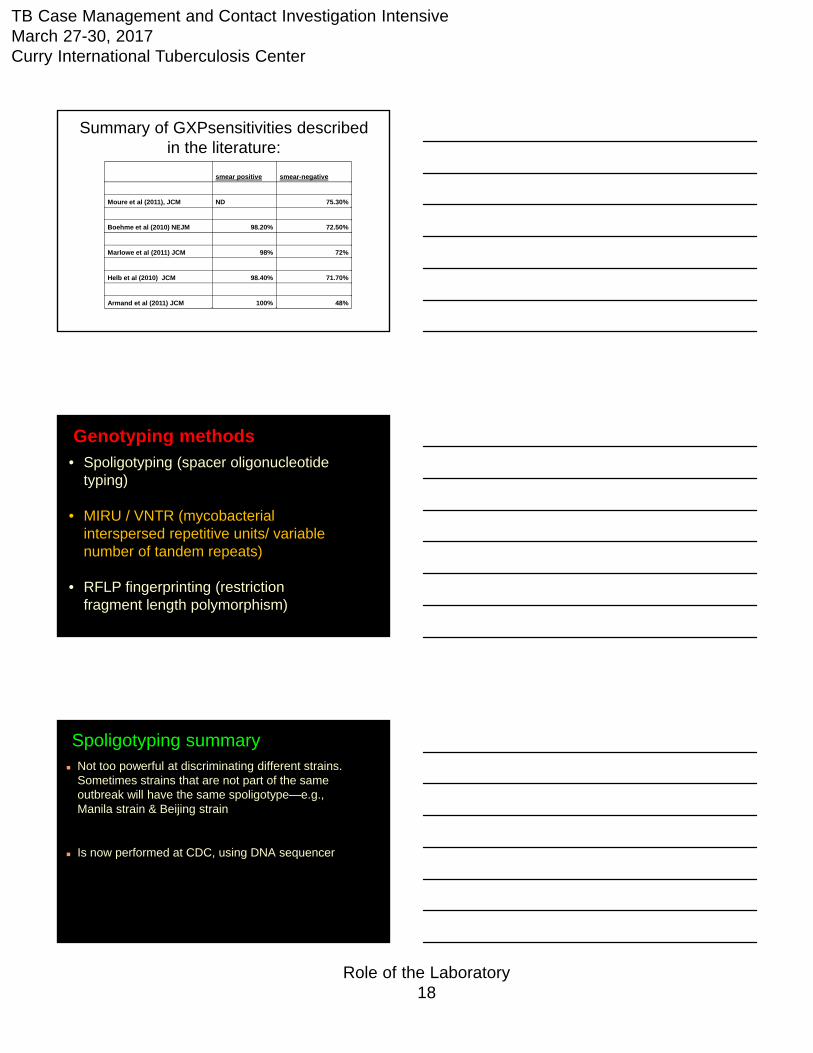
Summary of GXPsensitivities described in the literature:
smear positive smear-negative
Moure et al (2011), JCM ND 75.30%
Boehme et al (2010) NEJM 98.20% 72.50%
Marlowe et al (2011) JCM 98% 72%
Helb et al (2010) JCM 98.40% 71.70%
Armand et al (2011) JCM 100% 48%
• Spoligotyping (spacer oligonucleotidetyping)
• MIRU / VNTR (mycobacterialinterspersed repetitive units/ variable number of tandem repeats)
• RFLP fingerprinting (restriction fragment length polymorphism)
Genotyping methods
Spoligotyping summary Not too powerful at discriminating different strains.
Sometimes strains that are not part of the same outbreak will have the same spoligotype—e.g., Manila strain & Beijing strain
Is now performed at CDC, using DNA sequencer
Role of the Laboratory19
TB Case Management and Contact Investigation IntensiveMarch 27-30, 2017Curry International Tuberculosis Center
MIRU summary A PCR-based method, like spoligotyping
Like spoligotyping, the result is a number (24 digits)
Uses a DNA sequencer instrument to analyze the PCR products
Like spoligotyping, MIRU sometimes doesn’t discriminate between unrelated strains
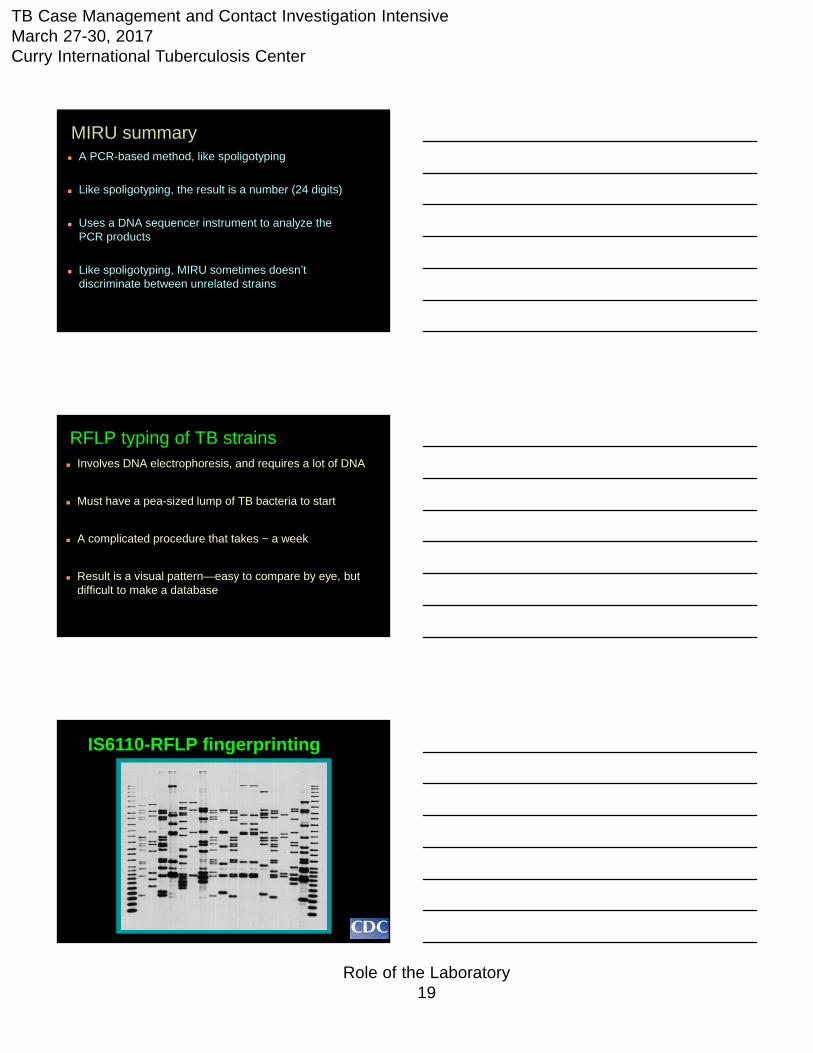
RFLP typing of TB strains Involves DNA electrophoresis, and requires a lot of DNA
Must have a pea-sized lump of TB bacteria to start
A complicated procedure that takes ~ a week
Result is a visual pattern—easy to compare by eye, but difficult to make a database
IS6110-RFLP fingerprinting
Role of the Laboratory20
TB Case Management and Contact Investigation IntensiveMarch 27-30, 2017Curry International Tuberculosis Center
Genotyping: Uses
1. Cross contamination studies
2. Outbreak investigation
3. TB Control needs, such as identifying settings where transmission occurs
Molecular Detection of Drug Resistance:
PCRDNA Sequencing
Principles of Molecular Detection of Drug Resistance methods
PCR
• Fast
• Uses “probes” to look for pre-characterized mutations; GeneXpert can only assess Rif susceptibility
• Can be integrated directly into testing
• Can be “fooled” by silent mutations
Sequencing
• More time than PCR
• “Reads” entire DNA code
• Detects any and all mutations
• Cannot be “fooled”
Either can guide treatment until cultureDST is completed

Role of the Laboratory21
TB Case Management and Contact Investigation IntensiveMarch 27-30, 2017Curry International Tuberculosis Center
Suggestion for requesting molecular detection of drug resistance: Acid-fast smear-positive specimen
Some of the specimen sediment is available for sending to reference lab (Public Health Lab or CDC)
Drug resistance is suspected, or
A susceptible population has been exposed, or
The culture is mixed or non-viable, so regular drug suscept. testing can’t be done
CDC also has Molecular Detection of Drug Resistance (MDDR) program: tests for mutations associated with resistance to additional drugs—ethambutol, pyrazinamide
Notice: Next Generation Sequencing
The ability to generate massive amounts of DNA sequence data very quickly
Can be used to “Deep Sequence” which means to sequence everything within a given specimen
Can be used to perform “Whole Genome Sequencing”
Platforms becoming affordable: ~$100 per sample
Can multiplex samples
Available now at our Laboratory
New York State PH Lab uses this for all Drug susceptibility testing
Whole Genome Sequencing:
Perhaps achievable ~24 hours
Performed on an isolate(and possibly a specimen)
You get:
Role of the Laboratory22
TB Case Management and Contact Investigation IntensiveMarch 27-30, 2017Curry International Tuberculosis Center
Perhaps achievable ~24 hours
Performed on an isolate(and possibly a specimen)
You get:
E V E R Y T H I N G
Whole Genome Sequencing:
Perhaps achievable ~24 hours
Performed on an isolate(and possibly a specimen)
You get:
E V E R Y T H I N G
That means:
-species
-genotyping; strain
-virulence factors
-Drug Susceptibility
Whole Genome Sequencing:
Thank you