
The Role of Endodontics in Interdisciplinary Dentistry · The Role of Endodontics in...
10
Opinions expressed by CE authors are their own and may not reflect those of Dentistry Today. Mention of specific product names does not infer endorsement by Dentistry Today. Information contained in CE articles and courses is not a substitute for sound clinical judgment and accepted standards of care. Participants are urged to contact their state dental boards for continuing education requirements. Continuing Education The Role of Endodontics in Interdisciplinary Dentistry: Are You Making the Right Decisions? Authored by John West, DDS, MSD Upon successful completion of this CE activity 2 CE credit hours will be awarded Volume 33 No. 4 Page 80
-
Upload
nguyenminh -
Category
Documents
-
view
264 -
download
12
Transcript of The Role of Endodontics in Interdisciplinary Dentistry · The Role of Endodontics in...
Opinions expressed by CE authors are their own and may not reflect those of Dentistry Today. Mention of
specific product names does not infer endorsement by Dentistry Today. Information contained in CE articles and
courses is not a substitute for sound clinical judgment and accepted standards of care. Participants are urged to
contact their state dental boards for continuing education requirements.
Continuing Education
The Role of Endodontics inInterdisciplinary Dentistry: Are You Making the Right Decisions?
Authored by John West, DDS, MSD
Upon successful completion of this CE activity 2 CE credit hours will be awarded
Volume 33 No. 4 Page 80
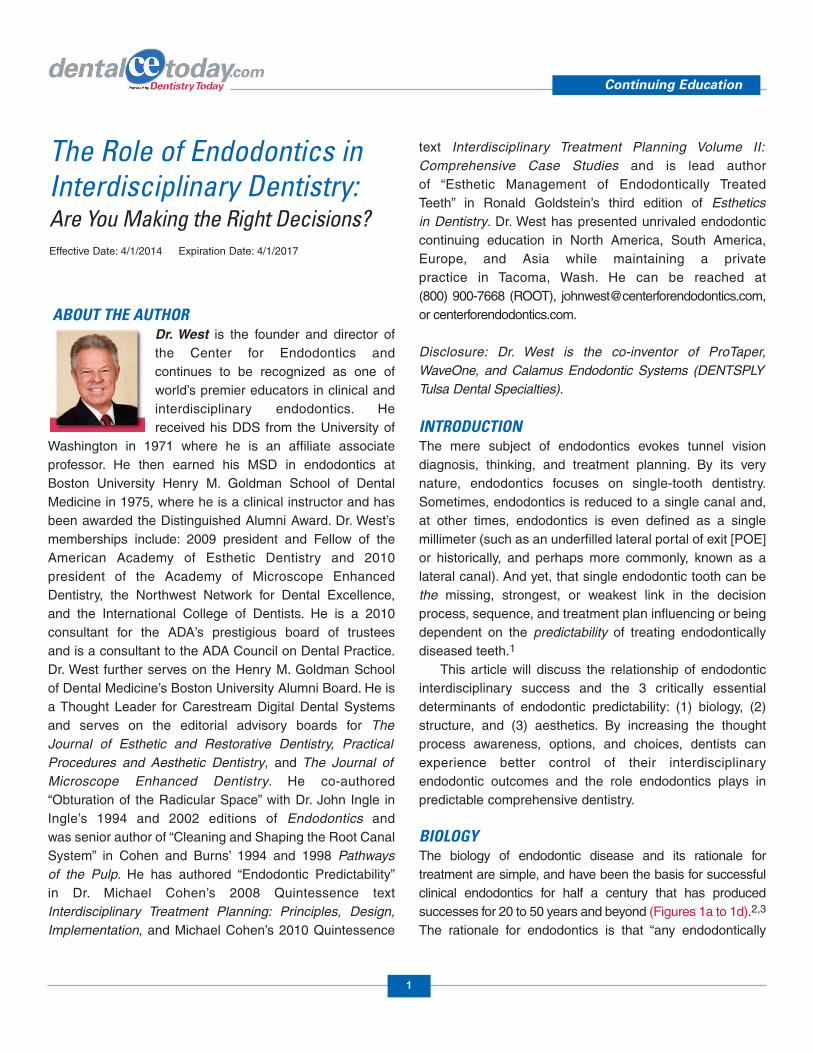
ABOUT THE AUTHORDr. West is the founder and director ofthe Center for Endodontics andcontinues to be recognized as one ofworld’s premier educators in clinical andinterdisciplinary endodontics. Hereceived his DDS from the University of
Washington in 1971 where he is an affiliate as sociateprofessor. He then earned his MSD in endodontics atBoston University Henry M. Gold man School of DentalMedicine in 1975, where he is a clinical instructor and hasbeen awarded the Distinguished Alumni Award. Dr. West’smemberships include: 2009 president and Fellow of theAmerican Academy of Esthetic Dentistry and 2010president of the Academy of Microscope EnhancedDentistry, the Northwest Network for Dental Excellence,and the International College of Dentists. He is a 2010consultant for the ADA’s prestigious board of trustees and is a consultant to the ADA Council on Dental Practice.Dr. West further serves on the Henry M. Goldman School of Dental Medicine’s Boston University Alumni Board. He isa Thought Leader for Carestream Digital Dental Systemsand serves on the editorial advisory boards for The Journal of Esthetic and Restorative Den tistry, PracticalProcedures and Aesthetic Den tistry, and The Journal of Microscope En hanced Dentistry. He co-authored“Obturation of the Radicular Space” with Dr. John Ingle inIngle’s 1994 and 2002 editions of Endodontics and was senior author of “Cleaning and Shaping the Root CanalSys tem” in Cohen and Burns’ 1994 and 1998 Pathways of the Pulp. He has authored “Endodontic Predictability” in Dr. Michael Cohen’s 2008 Quintessence text Inter disciplinary Treatment Planning: Principles, Design,Implementation, and Michael Cohen’s 2010 Quintessence
text Interdisciplinary Treatment Planning Volume II:Comprehensive Case Studies and is lead author of “Esthetic Management of Endodontically Treated Teeth” in Ronald Goldstein’s third edition of Esthetics in Dentistry. Dr. West has presented unrivaled endodonticcontinuing education in North America, South America,Europe, and Asia while maintaining a private practice in Tacoma, Wash. He can be reached at (800) 900-7668 (ROOT), [email protected],or centerforendodontics.com.
Disclosure: Dr. West is the co-inventor of ProTaper,WaveOne, and Calamus Endodontic Systems (DENTSPLYTulsa Dental Specialties).
INTRODUCTIONThe mere subject of endodontics evokes tunnel visiondiagnosis, thinking, and treatment planning. By its verynature, endodontics focuses on single-tooth dentistry.Sometimes, endodontics is reduced to a single canal and,at other times, en do dontics is even defined as a singlemillimeter (such as an underfilled lateral portal of exit [POE]or historically, and perhaps more commonly, known as alateral canal). And yet, that single endodontic tooth can bethe missing, strongest, or weakest link in the decisionprocess, sequence, and treatment plan influencing or beingdependent on the predictability of treating endodonticallydiseased teeth.1
This article will discuss the relationship of endodonticinterdisciplinary success and the 3 critically essentialdeterminants of endodontic predictability: (1) biology, (2)structure, and (3) aesthetics. By increasing the thoughtprocess awareness, options, and choices, dentists canexperience better control of their interdisciplinaryendodontic outcomes and the role endodontics plays inpredictable comprehensive dentistry.
BIOLOGYThe biology of endodontic disease and its rationale fortreatment are simple, and have been the basis for successfulclinical en dodontics for half a century that has producedsuccesses for 20 to 50 years and beyond (Figures 1a to 1d).2,3
The rationale for endodontics is that “any endodontically
Continuing Education
1
The Role of Endodontics inInterdisciplinary Dentistry: Are You Making the Right Decisions?Effective Date: 4/1/2014 Expiration Date: 4/1/2017

diseased tooth can be predictablytreated if the root canal systemcan be sealed either nonsurgicallyor surgically, and, if the perio -dontal condition is healthy or canbe made healthy.”4 Asendodontists, we are often askedthe question, “Do you think thistooth should be saved?” The rightquestion is, “Is this toothstructurally restorable?” From anendodontic perspective, ourquestion or your question as arestorative dentist performing endodontics should be, “Canwe produce the Endodontic Seal?”5 If the role ofendodontics is to prevent lesions of en do dontic origin(LEOs) where they do not exist and heal LEOs where theydo exist, then the 3-D treatment and ultimately elimination ofthe cause of endodontic disease (contents of the root canalsystem) is key. Of course, as I discuss later, the tooth mustalso be restorable and aesthetically valued.
Endodontics has become more precise with improvedtechnology that continues at a breakthrough pace:microscopes, Ni-Ti shaping, 3-D cleaning devices andsolutions of the root canal system, digital and 3-D imaging,microinstruments including ul trasonics and deliverysystems, and predictable 3-D obturation. But all the newesttechnology does not help the biologic outcome unless thedentist understands en dodontic principles and knowswhen, why, and how to use the latest tools. The clinicianremains the greatest determinant of all! The role ofendodontics in interdisciplinary dentistry still comes downto knowing what the biology wants, and what that comesdown to is doing predictable endodontics.
How can dentists do predictable endo dontics? Therecipe is simple. You only need the following 10 ingredients:
1. Design a successful access cavity with no restrictivedentinal triangles and yet full respect and protection of theferrule (see “Structure” below).
2. Find all canals. In order to do this time after time,magnification and illumination are essential. The best formof magnification and illumination is the operatingmicroscope. Period. In addition, digital imaging allows the
dentist to see small details by viewing a huge screen imageversus a dental periapical radiograph. Three-dimensionaldigital imaging can be a valuable road map for “finding” andtracing the root canal path. Knowl edge of the averagenumber of canals that are in each tooth can be helpful for thedentist who performs an occasional endodontic procedure.6
3. Follow all canals. The mastery of this skill is the singlemost significant skill in endodontics short of correct andproper diagnosis. Manual files must be curved and often inmultiple planes in order to successfully “follow” to theirtermini. Clinicians must be mindful of collagen or den tinmud—the fatal flaws of successful endodontic following.There are 3 other situations that prevent the successful skillof following to the canal radiographic terminus (somedistance from the physiologic terminus), and they are: (1)the curved file does not sufficiently mimic the canal 3-Dpath, (2) the tip of the chosen file is too wide apically, or (3)the shaft of the file is too wide coronally (coronal restrictivedentin). Knowledge, skill, and willingness are required tosolve each of these situations, or combination ofsituations.7
4. Shape the canals into the continuously taperingfunnel using ethylenediaminetetraacetic acid (EDTA) asirrigant. EDTA momentarily “softens” the radicular walls,making Ni-Ti shaping theoretically safer and, at the sametime, removes the smear layer as it is being created. Inother words, the desired shape preparation “connects thedots” between the minimal apical constriction and one thirdthe width of the tooth’s mesial-distal width as measured atthe cemento-enamel junction. This optimal shape provides
Continuing Education
2
The Role of Endodontics in Interdisciplinary Dentistry: Are You Making the Right Decisions?
Figures 1a to 1d. Biology:When endodontics is performed diligently with skill, knowledge, and willingnessfor patience and precision, long-term predictable results are not only possible but probable. (a) Pretreat-ment of endodontic failure. (b) Periapical radiograph at time of treatment. (c) The 32-year post-treatmentsuccess. (d) Shows healthy gingival and attachment apparatus while no sign of the original sinus tract.Tooth is fully functional.
a b c d

for sufficient obturation hydraulics while preserving preciousferrule not only in the mesial-distal dimension but also themore critical facial-lingual dimension. Shaping alsofacilitates 3-D cleaning.
5. Clean the root canal system by constant chamber andcanal flooding and exchanging with sodium hypo chlorite. Theuse of mechanical cleaning devices such as theEndoActivator (DENTSPLY Tulsa Dental Specialties) canimprove removal of detached pulp, necrotic debris, andbacteria through agitation.
6. Conefit. When is shaping finished? In these Ni-Titimes, magnified evidence of dentin in the file’s apical flutesvalidates that that file’s shape has been prepared. Thesuccessful conefit for vertical compaction of warm gutta-percha or size verifier for carrier-based obturation furtherconfirms that proper shaping is finished.
7. Remove smear layer prior to oburation pack. Agitatean EDTA product (such as QMix [DENTSPLY Tulsa DentalSpecialties]) in order to remove any remaining smear layer,capable of blocking portals of exit and then dry the canals.
8. Obturate the canals with preferred sealer with avertical compaction technique such as warm gutta-percha. (Iuse Kerr Pulp Canal Sealer [SybronEndo] because of itssealing longevity and radiopacity, plus it is bactericidal.)Carrier-based obturations (GuttaCore [DENTSPLY TulsaDental Specialties]) are preferred using root canal sealer(ThermaSeal [DENTSPLY Tulsa Dental Specialties]).
9. Back-pack 1.0 mm short of chamber entrance, etch,bond, and seal the canal orifice and chamber floor to thedepth of 2 mm (OptiBond [Kerr] and a flowable composite).
10. Restore coronal seal (access) with SonicFill (Kerr).
The acoustic wave produced with the SonicFill devicepredictably generates solid foundations. Check occlusion andtake final images. Schedule or proceed with onlay or crown.
Finally, if coronal leakage is present (see CarestreamLogicon technology), coronal caries must be removed,followed by the endodontics and new restorative. There fore,there are 2 parts of correcting a structural (leakage) of anendo dontically diseased tooth: en dododontic treatment orretreatment and structural retreatment. Even so, correctingboth the endodontics and the restorative remain financiallycompetitive with an implant while, at the same time, havingthe advantage of retaining and restoring natural tooth parts,if needed!
STRUCTUREEndodontic treatment can render a tooth unrestorable whenthe radicular preparation weakens the root or minimizes oreliminates the retentive ferrule. In endodontics, there is a fine
Continuing Education
3
The Role of Endodontics in Interdisciplinary Dentistry: Are You Making the Right Decisions?
Figure 2. Structure:Producing andprotecting sufficientrestorative toothsometimes requires creative thinking andtreatment planning.The endodontic,periodontal, andaesthetic determin-ants are revealed inthis single-linediagram. (Originalimage used withpermission from Dr. Frank Spear.)
Figures 3a to 3c. Aesthetics: Gingival discoloration for uncleaned root canal system chamber can degrade smile aesthetics. (a) Pretreat-ment clinical of discoloration along gingival contours. (b) Pretreatment image followed by image of “safe” bleach barrier that appears like abobsled outline from the facial. (c) Bleached and restoration placed with aesthetic result.
a cb
line between overshaping and undershaping. There is also afine line between the new buzzword “minimally invasive”endodontic canal preparations and a preparation that is sominimal that it cannot be properly cleaned or obturated in 3-D.In the 1950s, silver cone biologic underpreparationsprevented 3-D cleaning, shaping, and obturation; thereforepreventing long-term success, particularly when the coronalseal was given enough cyclic fatigue to structurally breakdown at the cavosurface margins producing coronalmicroleakage.
Ferrule must be present facially and lingually afterendodontic preparation that also ideally preserves the mesialand distal ferrule as well. In summary, the desired 4.0 mmfrom the height of bone to height of ferrule is the minimumrestorative determinant identified in the restorative literature.In ad dition, the outline form of the access preparation shouldnot be too small or too big...it should be just right!
There is also the importance of predictability regardingthe size of the access cavity, the largest POE of all! With theadvent of the microscope, most endodontists have beenable to reduce the size of their access by up to 50% whilestill maintaining the de sired straight-line access.8 Magnifi -cation and coaxial lighting allow the clinician to pinpointorifice locations without having to “search around” anddiscover orifices by “feeling” them. There is a balance here,however. For example, if you cannot predictably reach a21.0-mm rotary or reciprocation file into the MB of amaxillary second molar because of lack of oral access, thenyou may need to lean the mesial wall (more mesial thanotherwise ideal) in order to slip over the mesial cavosurfaceand slide into the MB without breaking a file. The angle of
access and incidence sometimes does not coincide wherepatient openings are limited.
Even more toward the “minimally invasive” extreme,there are some endodontists suggesting leaving the roof ofthe pulp chamber intact and “drilling” holes where,hopefully, the dentist can then slide files into the canals. Thefirst problem is that some canal entrances will not be seenand therefore missed due to aberrantly located canalsobscured by the chamber roof. Secondly, because of this“peep hole,” the dentist will not be in control of the delicateGlidepath management with subsequent rotary orreciprocation shaping and precision obturation. In addition,the now impossible-to-clean chamber and its pulp hornsremain as culs-de-sac for colonies of bacteria and pulptissue (dead or alive) that are inaccessible. Perhaps worse,anterior teeth would often become discolored and anaesthetic disaster requiring a crown. And finally, where isthe literature that supports the tooth is stronger withportions of the usual fragile roof in place? Sometimes, therole of endo dontics in interdisciplinary dentistry is todiscover and unravel steps that take dentistry backward intime.
Structure preservation is an es sential consideration inendodontic retreatments, since an endodontic preparationalready exists and may have already compromised orviolated the minimum 1.5 to 2.0 mm vertical height and 1.0mm ferrule thickness (Figure 2). In considering nonsurgicalretreatment, further coronal shaping, while intended toimprove funnel preparation, could compromise coronaltooth structure even further. Consequently, the lack ofstructure could make surgical retreatment a better,
Continuing Education
4
The Role of Endodontics in Interdisciplinary Dentistry: Are You Making the Right Decisions?
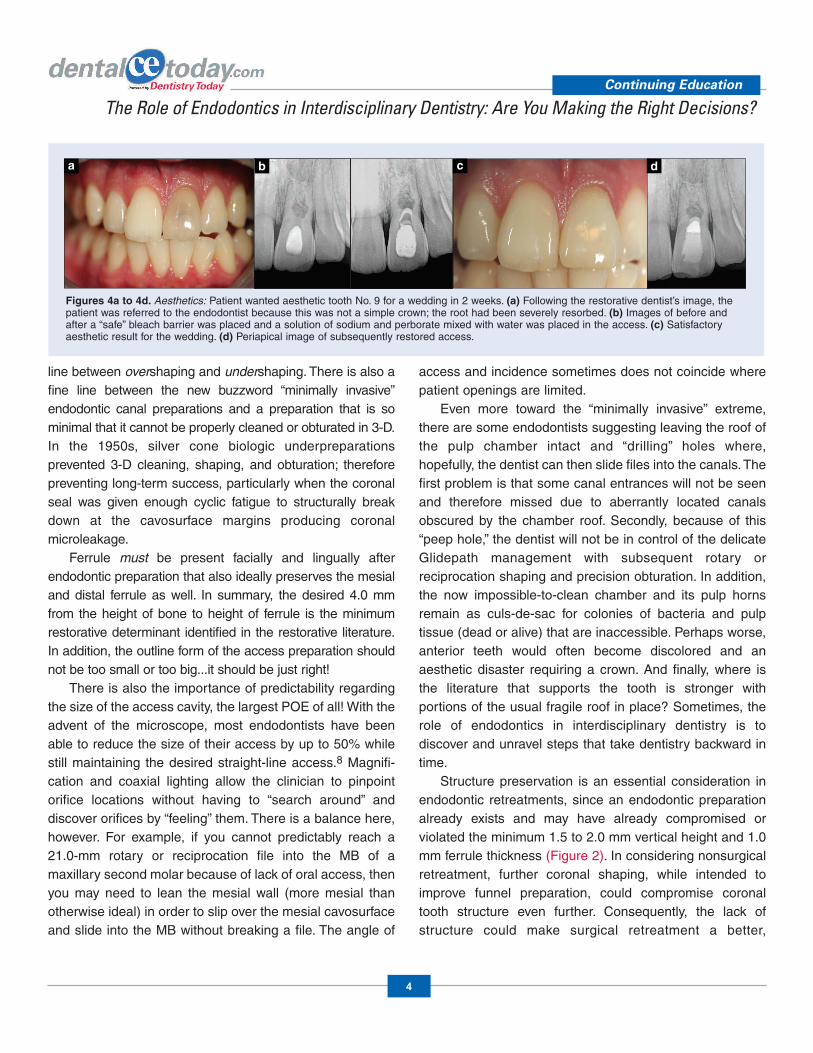
Figures 4a to 4d. Aesthetics: Patient wanted aesthetic tooth No. 9 for a wedding in 2 weeks. (a) Following the restorative dentist’s image, thepatient was referred to the endodontist because this was not a simple crown; the root had been severely resorbed. (b) Images of before andafter a “safe” bleach barrier was placed and a solution of sodium and perborate mixed with water was placed in the access. (c) Satisfactoryaesthetic result for the wedding. (d) Periapical image of subsequently restored access.
a cb d

a
“minimally invasive” patient option. And while a surgicaloption may protect tooth structure, the surgery couldcompromise the aesthetic outcome by resulting again in anattached gingival scar or a black triangle at the site of theinterproximal papilla.9 And so it goes, biology versusstructure versus aesthetics are collaborative treatmentplanning de terminants and considerations.
Another destructive structure condition that involves thepulp is the silent cracked tooth syndrome (CTS).Considerable misconception surrounds the diagnosis andtreatment plan for CTS. This patient will present with a tooththat hurts to bite on, and yet the pulp tests vital. Thesymptom of bite and pulpal pain typically do not occur in thesame tooth since pulp necrosis occurs in a coronal-apicaldirection. If the tooth has periapical symptoms, the pulpshould test nonvital, but the CTS tooth has, by definition, avital pulp. The Class I CTS does not affect the pulp. TheClass II CTS involves the pulp. How do you diagnose whichis which? The most accurate test is the “cotton wad” test (adamp portion torn off of a cotton roll) where the patient testshimself or herself. Once the patient personally duplicates
the culprit bite source, an orthodontic band is cemented tothe tooth. If the bite pain is eliminated and pulp remains vitaland asymptomatic, then restore with crown or cuspalcoverage. Excellent predictability can be expected if the bitepain is gone after ortho band placement but pulp symptomspersist if the dentist now performs endodontics and placesa crown or full coverage. If the ortho band solves the pulppain but not the bite pain, this tooth has a guarded long-term prognosis.
As a rule of thumb, steps for CTS include the following: 1. Place band and still painful to chew. If patient wants a
guarantee, then recommend removal and re placement.2. If no pain to chew, but pulp is symptomatic, then do endo
and restore.3. If band and no bite pain and no pulp pain and vital,
then restore with confidence.
AESTHETICSThe role of endodontics determinant in interdisciplinarydental aesthetics can be the weakest link.10 The color of theendodontic tooth may not match the aesthetic adjacent or
Continuing Education
5
The Role of Endodontics in Interdisciplinary Dentistry: Are You Making the Right Decisions?
a dcb
cb
e
d
Figures 5a to 5e. Aesthetics: Unraveling the dilemma of correcting aesthetics in the calcific metamorphosis tooth. (a) Pretreatment image afterunsuccessful external custom tray bleaching. Pretreatment image had remained the same for a decade. (b) Pulp was and still is vital. (c) A CBCT 3-Dimage reveals depth that pulp chamber begins in order to prevent pulp exposure. (d) Protective bleach barrier and “walking bleach” placed. (e) Approaching proper color with one more walking bleach and aesthetic access repair.
Figures 6a to 6d. Aesthetics: Patient presents with sinus tract due to underfilled root canal system. (a) Gutta-percha cone is tracing sinus tract. (b) Gingival levels noted dissimilar and referred for periodontal and orthodontic consultation. (c) Endodontic nonsurgical retreatment has beensuccessful for more than 16 years (right image). (d) Orthodontics immediately followed the initial endodontic success. Happy with her smile, thepatient’s improved self-esteem allowed her to risk going from a flight attendant to pilot. You never know what the role of an endodontically treated tooth can play in the interdisciplinary treatment plan.

contralateral tooth (Figures 3a to 4d). For example, if the pulphorns of an endodontically diseased tooth are not sufficientlycleaned, remaining necrotic pulp horns can be filled withdiscoloring tissue, bacteria, and blood bilirubins. Specialattention must also be made to improve the existing color of adiscolored tooth due to necrosis and gangrene using specialendodontic ultrasonics and ideally microscope qualitymagnification and light. While an off-color endodontic accessrepair may not noticeably affect the color, an off color canaffect a positive patient outcome when the access is far lessthan invisible. If the patient can see a discolored accessmaterial especially in a new crown, it appears like a mistake.
Another endodontic/aesthetic con tinuum is revealed indegeneration of calcific metamorphosis, which has longbeen a dilemma for the interdisciplinary team. When pulpsbecome calcified, it can make endodontics treacherouswhen finding the canal or when overpreparing the structuraldentin in order to find the canal. Pulps die and calcify in acrown-to-apex direction and therefore the canal can mostoften be located by penetrating deeper but often not withoutdestruction of the ferrule and remaining coronal toothstructure. In addition, light transmission is prevented incalcified crowns adding to an aesthetic dilemma. The teethappear dark. Where calcific metamorphosis teeth havenonvital pulps, endodontics must be attempted. Withknowledge, skill, and training, these patients can, however,experience successful treatment.
What if the pulp tests vital, and the patient wants to correctthe tooth (or teeth)? The treatment options are crown(s),veneer(s), endodontics and bleaching, external bleaching, orim plant(s). There is yet another treatment option, particularly inthe case of chamber calcific degeneration: a “walking bleach”procedure with no endo dontics can be noninvasive, safe, andaesthetically predictable and pleasing (Figures 5a to 5e). Theinterdisciplinary treatment of our pa tients’ smiles, by changingpreviously distracting endo dontically discolored teeth, cantruly change lives (Figures 6a to 6d).
A final area of the endodontic role in biologic, structural, andaesthetic dentistry is repair of the enododontic ac cess cavity.Access finishing re quires skill, care, attention, and time to do itright. For the clinician who simply wants to “get the treatmentover,” it is important to remember that optimal predictabilityrequires the same level of energy, attention to detail, and
patience at the end of a procedure as it did in the be ginning.Often, this is the difference that makes the difference.
CLOSING COMMENTSAre you still confused about the role of endodontics ininterdisciplinary den tistry? Most cases are obvious, butmore and more gray areas are facing dentists today in theirtreatment planning. A good question is to look in the mirrorand ask, “What would I do if it were me?” Therein lies theanswer for your patient as well.
Continuing Education
6
The Role of Endodontics in Interdisciplinary Dentistry: Are You Making the Right Decisions?
Table. Ten Action Steps to Increase YourEducation in The Role of Endodontics inInterdisciplinary Dentistry
1. Start your own interdisciplinary study club modeled after the Northwest Network for Dental Excellence. Send inquires via e-mail [email protected].
2. Attend Interdisciplinary Dental Education Academy.Visit the Web site at ideausa.net.
3. Join the Seattle Study Club. Send inquirers to [email protected].
4. Join Spear Education and Spear Digital SpearEducation. Visit speareducation.com.
5. Purchase the following book: Cohen M, ed.Interdisciplinary Treatment Planning: Principles,Design, Implementation. Chicago, IL: QuintessencePublishing Co; 2008.
6. Purchase the new Dr. Ron Goldstein book: GoldsteinRE, ed. Esthetics in Dentistry. 3rd ed. Shelton, CT:PMPH-USA; 2014: In press.
7. Visit endoruddle.com.
8. Visit endopro.net.
9. Subscribe to Endodontic Practice US. Visit the Website endopracticeus.com.
10. Subscribe to Journal of Esthetic and RestorativeDentistry. Visit the Web siteonlinelibrary.wiley.com/journal/10.1111/(ISSN)1708-8240.

REFERENCES1. West JD. Implants versus endodontics: “As the
pendulum swings.” Dent To day. 2014;33:10-12.2. Schilder H. Cleaning and shaping the root canal. Dent
Clin North Am. 1974;18:269-296.3. Schilder H. Vertical compaction of warm gutta-percha.
In: Gerstein H, ed. Techniques in Clinical En do dontics.Phila del phia, Pa: WB Saunders Co; 1982: 84-90.
4. West JD. Endodontic predictability: “What matters?”Dent Today. 2013;32:108-113.
5. West J. Endodontic up date 2006. J Esthet RestorDent. 2006;18:280-300.
6. West JD. Endodontic predictability—“Restore orremove: how do I choose?” In: Cohen M, ed.Interdisciplinary Treat ment Planning: Principles,Design, Implementation. Chicago, IL: Quin tessencePublishing Co; 2008: 123-164.
7. West J. Anatomy Matters. “Could it all simply be acoincidence?” Part 8. Endodontic Practice US.2013;6(5):52-55.
8. West JD. The role of the microscope in 21st centuryendodontics: Visions of a new frontier. Dent Today.2000;19:62-69.
9. Tarnow DP, Magner AW, Fletcher P. The effect of thedistance from the contact point to the crest of the boneon the presence or absence of the interproximal dentalpapilla. J Perio dontol. 1992;63:995-996.
10. West JD, Chivian N, Arens D, et al Estheticmanagement of endodontically treated teeth. In: Gold -stein RE, ed. Es thetics in Dentistry. 3rd ed. Shel ton,CT: PMPH-USA; 2014: In press.
Continuing Education
7
The Role of Endodontics in Interdisciplinary Dentistry: Are You Making the Right Decisions?

POST EXAMINATION INFORMATION
To receive continuing education credit for participation inthis educational activity you must complete the programpost examination and answer 6 out of 8 questions correctly.
Traditional Completion Option:You may fax or mail your answers with payment to DentistryToday (see Traditional Completion Information on followingpage). All information requested must be provided in orderto process the program for credit. Be sure to complete your“Payment,” “Personal Certification Information,” “Answers,”and “Evaluation” forms. Your exam will be graded within 72hours of receipt. Upon successful completion of the post-exam (answer 6 out of 8 questions correctly), a letter ofcompletion will be mailed to the address provided.
Online Completion Option:Use this page to review the questions and mark youranswers. Return to dentalcetoday.com and sign in. If youhave not previously purchased the program, select it fromthe “Online Courses” listing and complete the onlinepurchase process. Once purchased the program will beadded to your User History page where a Take Exam linkwill be provided directly across from the program title.Select the Take Exam link, complete all the programquestions and Submit your answers. An immediate gradereport will be provided. Upon receiving a passing grade,complete the online evaluation form. Upon submitting the form, your Letter of Completion will be providedimmediately for printing.
General Program Information:Online users may log in to dentalcetoday.com any time inthe future to access previously purchased programs andview or print letters of completion and results.
POST EXAMINATION QUESTIONS
1. The rationale for endodontics is that “anyendodontically diseased tooth can be predictablytreated if the root canal system can be sealed eithernonsurgically or surgically, and, if the periodontalcondition is healthy or can be made healthy.
a. True b. False
2. The 3-dimensional treatment and ultimatelyelimination of the cause of endodontic disease,contents of the root canal system, is key.
a. True b. False
3. Knowledge of average number of canals that are ineach tooth is interesting but not really helpful for thedentist that performs an occasional endodonticprocedure.
a. True b. False
4. The use of mechanical cleaning devices does notsignificantly improve removal of detached pulp,necrotic debris, and bacteria through agitation.
a. True b. False
5. The acoustic wave produced with the SonicFilldevice predictably generates solid foundations.
a. True b. False
6. With the advent of the microscope, mostendodontists have been able to reduce the size oftheir access by up to 90% while still maintaining thedesired straight-line access.
a. True b. False
7. Another destructive structure condition that involvesthe pulp is the silent cracked tooth syndrome (CTS).
a. True b. False
8. The most accurate test for CTS is the “cotton wad”test (a damp portion torn off of a cotton roll) wherethe patient tests himself or herself.
a. True b. False
Continuing Education
8
The Role of Endodontics in Interdisciplinary Dentistry: Are You Making the Right Decisions?
This CE activity was not developed in accordance withAGD PACE or ADA CERP standards.CEUs for this activity will not be accepted by the AGDfor MAGD/FAGD credit.

PROGRAM COMPLETION INFORMATION
If you wish to purchase and complete this activitytraditionally (mail or fax) rather than online, you mustprovide the information requested below. Please be sure toselect your answers carefully and complete the evaluationinformation. To receive credit you must answer 6 of the 8questions correctly.
Complete online at: dentalcetoday.com
TRADITIONAL COMPLETION INFORMATION:Mail or fax this completed form with payment to:
Dentistry TodayDepartment of Continuing Education100 Passaic AvenueFairfield, NJ 07004
Fax: 973-882-3622
PAYMENT & CREDIT INFORMATION:
Examination Fee: $40.00 Credit Hours: 2
Note: There is a $10 surcharge to process a check drawn on any bank other than a US bank. Should you have additionalquestions, please contact us at (973) 882-4700.
o I have enclosed a check or money order.
o I am using a credit card.
My Credit Card information is provided below.
o American Express o Visa o MC o Discover
Please provide the following (please print clearly):
Exact Name on Credit Card
Credit Card # Expiration Date
Signature
PROGRAM EVAUATION FORMPlease complete the following activity evaluation questions.
Rating Scale: Excellent = 5 and Poor = 0
Course objectives were achieved.
Content was useful and benefited your clinical practice.
Review questions were clear and relevant to the editorial.
Illustrations and photographs were clear and relevant.
Written presentation was informative and concise.
How much time did you spend reading the activity and completing the test?
What aspect of this course was most helpful and why?
What topics interest you for future Dentistry Today CE courses?
Continuing Education
The Role of Endodontics in Interdisciplinary Dentistry: Are You Making the Right Decisions?
ANSWER FORM: VOLUME 33 NO. 4 PAGE 80Please check the correct box for each question below.
1. o a. True o b. False 5. o a. True o b. False
2. o a. True o b. False 6. o a. True o b. False
3. o a. True o b. False 7. o a. True o b. False
4. o a. True o b. False 8. o a. True o b. False
PERSONAL CERTIFICATION INFORMATION:
Last Name (PLEASE PRINT CLEARLY OR TYPE)
First Name
Profession / Credentials License Number
Street Address
Suite or Apartment Number
City State Zip Code
Daytime Telephone Number With Area Code
Fax Number With Area Code
E-mail Address
/
9
This CE activity was not developed in accordance withAGD PACE or ADA CERP standards.CEUs for this activity will not be accepted by the AGDfor MAGD/FAGD credit.


















