The role of cognitive biases and personality variables in subclinical delusional ideation
13
This article was downloaded by: [University of Waterloo] On: 25 October 2014, At: 06:48 Publisher: Routledge Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK Cognitive Neuropsychiatry Publication details, including instructions for authors and subscription information: http://www.tandfonline.com/loi/pcnp20 The role of cognitive biases and personality variables in subclinical delusional ideation Mahesh Menon a b c e , Lena Catherine Quilty d , John Anthony Zawadzki a b c , Todd Stephen Woodward e , Helen Moriah Sokolowski f , Heather Shirley Boon g & Albert Hung Choy Wong a b c a Schizophrenia Program and Research Imaging Centre , Centre for Addiction & Mental Health , Toronto , Canada b Department of Psychiatry , University of Toronto , Toronto , Canada c Institute of Medical Science , University of Toronto , Toronto , Canada d Clinical Research Department , Centre for Addiction & Mental Health , Toronto , Canada e Department of Psychiatry , University of British Columbia , Vancouver , Canada f Department of Psychology , University of Western Ontario , London , Canada g Leslie Dan Faculty of Pharmacy , University of Toronto , Toronto , Canada Published online: 04 Jul 2012. To cite this article: Mahesh Menon , Lena Catherine Quilty , John Anthony Zawadzki , Todd Stephen Woodward , Helen Moriah Sokolowski , Heather Shirley Boon & Albert Hung Choy Wong (2013) The role of cognitive biases and personality variables in subclinical delusional ideation, Cognitive Neuropsychiatry, 18:3, 208-218, DOI: 10.1080/13546805.2012.692873 To link to this article: http://dx.doi.org/10.1080/13546805.2012.692873 PLEASE SCROLL DOWN FOR ARTICLE Taylor & Francis makes every effort to ensure the accuracy of all the information (the “Content”) contained in the publications on our platform. However, Taylor & Francis, our agents, and our licensors make no representations or warranties whatsoever as to the accuracy, completeness, or suitability for any purpose of the Content. Any opinions
-
Upload
albert-hung-choy -
Category
Documents
-
view
213 -
download
1
Transcript of The role of cognitive biases and personality variables in subclinical delusional ideation

This article was downloaded by: [University of Waterloo]On: 25 October 2014, At: 06:48Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registeredoffice: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
Cognitive NeuropsychiatryPublication details, including instructions for authors andsubscription information:http://www.tandfonline.com/loi/pcnp20
The role of cognitive biases andpersonality variables in subclinicaldelusional ideationMahesh Menon a b c e , Lena Catherine Quilty d , John AnthonyZawadzki a b c , Todd Stephen Woodward e , Helen MoriahSokolowski f , Heather Shirley Boon g & Albert Hung Choy Wonga b ca Schizophrenia Program and Research Imaging Centre , Centrefor Addiction & Mental Health , Toronto , Canadab Department of Psychiatry , University of Toronto , Toronto ,Canadac Institute of Medical Science , University of Toronto , Toronto ,Canadad Clinical Research Department , Centre for Addiction & MentalHealth , Toronto , Canadae Department of Psychiatry , University of British Columbia ,Vancouver , Canadaf Department of Psychology , University of Western Ontario ,London , Canadag Leslie Dan Faculty of Pharmacy , University of Toronto ,Toronto , CanadaPublished online: 04 Jul 2012.
To cite this article: Mahesh Menon , Lena Catherine Quilty , John Anthony Zawadzki , ToddStephen Woodward , Helen Moriah Sokolowski , Heather Shirley Boon & Albert Hung Choy Wong(2013) The role of cognitive biases and personality variables in subclinical delusional ideation,Cognitive Neuropsychiatry, 18:3, 208-218, DOI: 10.1080/13546805.2012.692873
To link to this article: http://dx.doi.org/10.1080/13546805.2012.692873
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the“Content”) contained in the publications on our platform. However, Taylor & Francis,our agents, and our licensors make no representations or warranties whatsoever as tothe accuracy, completeness, or suitability for any purpose of the Content. Any opinions
and views expressed in this publication are the opinions and views of the authors,and are not the views of or endorsed by Taylor & Francis. The accuracy of the Contentshould not be relied upon and should be independently verified with primary sourcesof information. Taylor and Francis shall not be liable for any losses, actions, claims,proceedings, demands, costs, expenses, damages, and other liabilities whatsoeveror howsoever caused arising directly or indirectly in connection with, in relation to orarising out of the use of the Content.
This article may be used for research, teaching, and private study purposes. Anysubstantial or systematic reproduction, redistribution, reselling, loan, sub-licensing,systematic supply, or distribution in any form to anyone is expressly forbidden. Terms& Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions
Dow
nloa
ded
by [
Uni
vers
ity o
f W
ater
loo]
at 0
6:48
25
Oct
ober
201
4

The role of cognitive biases and personality variables in
subclinical delusional ideation
Mahesh Menon1,2,3,5, Lena Catherine Quilty4, John AnthonyZawadzki1,2,3, Todd Stephen Woodward5, Helen MoriahSokolowski6, Heather Shirley Boon7, and Albert Hung ChoyWong1,2,3
1Schizophrenia Program and Research Imaging Centre, Centre for
Addiction & Mental Health, Toronto, Canada2Department of Psychiatry, University of Toronto, Toronto, Canada3Institute of Medical Science, University of Toronto, Toronto, Canada4Clinical Research Department, Centre for Addiction & Mental
Health, Toronto, Canada5Department of Psychiatry, University of British Columbia,
Vancouver, Canada6Department of Psychology, University of Western Ontario, London,
Canada7Leslie Dan Faculty of Pharmacy, University of Toronto, Toronto,
Canada
Introduction. A number of cognitive biases, most notably a data gathering biascharacterised by ‘‘jumping to conclusions’’ (JTC), and the ‘‘bias against disconfir-matory evidence’’ (BADE), have been shown to be associated with delusions and
Correspondence should be addressed to Schizophrenia Program & PET Centre, Centre
for Addiction & Mental Health, 250 College St, Toronto, M5T 1R8, Canada.
E-mail: [email protected]
The authors would like to thank Sarah Mathewson, Dr Paul Fletcher and Wanna Mar for their
assistance with data collection on this study. The study was partially funded by a new staff startup
grant to MM from the Centre for Addiction & Mental Health, and a summer student fellowship
from the Leslie Dan Faculty of Pharmacy, University of Toronto. HMS was supported by an
Undergraduate Research Award from the Institute of Medical Sciences, University of Toronto.
AHCW is supported by a CIHR Clinician Scientist Fellowship and an NARSAD Independent
Investigator Award. All authors contributed to and approved the final manuscript. All authors
declare that they have no conflict of interest.
Cognitive Neuropsychiatry, 2013
Vol. 18, No. 3, 208�218, http://dx.doi.org/10.1080/13546805.2012.692873
# 2013 Taylor & Francis
Dow
nloa
ded
by [
Uni
vers
ity o
f W
ater
loo]
at 0
6:48
25
Oct
ober
201
4
subclinical delusional ideation. Certain personality variables, particularly ‘‘open-ness to experience’’, are thought to be associated with schizotypy.Methods. Using structural equation modelling, we examined the associationbetween two higher order subfactors (‘‘aspects’’) of ‘‘openness to experience’’(labelled ‘‘openness’’ and ‘‘intellect’’), these cognitive biases, and their relationshipto subclinical delusional ideation in 121 healthy, nonpsychiatric controls.Results. Our results suggest that cognitive biases (specifically the data gathering biasand BADE) and the ‘‘openness’’ aspect are independently associated withsubclinical delusional ideation, and the data gathering bias is weakly associatedwith ‘‘positive schizotypy’’. ‘‘Intellect’’ is negatively associated with delusionalideation and might play a potential protective role.Conclusions. Cognitive biases and personality are likely to be independent riskfactors for the development of delusions.
Keywords: Bias against disconfirmatory evidence; Cognitive biases; Delusions;
‘‘Jumping to conclusions’’; Openness; Personality; Subclinical delusional ideation.
INTRODUCTION
A growing body of evidence suggests that psychosis may exist as a
continuum, with illnesses like schizophrenia at one end (Kendler, Neale, &
Walsh, 1995), and schizotypal and paranoid personality disorder represent-
ing milder manifestations of the same aetiological processes (Meehl, 1962).
Consistent with this, epidemiological evidence indicates that subclinical
manifestations of psychotic symptoms such as delusions and hallucinations
occur with varying degrees of frequency and severity even within the
nonclinical, psychiatrically ‘‘healthy’’ population, and may be indicators of
schizotypy (Johns & van Os, 2001; van Os, Hanssen, Bijl, & Ravelli, 2000).
An examination of neurocognitive vulnerabilities and strengths within this
group may increase our understanding of the underlying cognitive processes
associated with more severe forms of psychosis, as well as of possible
protective factors that might prevent transition to frank psychosis in
vulnerable individuals.
Scales measuring schizotypy, such as the Schizotypal Personality Ques-
tionnaire (SPQ; Raine, 1991) consider schizotypy a multidimensional
construct, with the ‘‘odd beliefs/magical thinking’’ subscale most closely
resembling delusions, and the ‘‘unusual perceptions’’ most resembling
hallucinations. Newer instruments, such as the Peters Delusions Inventory
(PDI; Peters, Joseph, Day, & Garety, 2004) focus on subclinical forms of
common delusional subtypes. Both instruments have been used to examine
cognitive and personality variables in association with schizotypy and
subclinical delusional ideation.
Cognitive biases play an important role in the formation (Broome et al.,
2004) and maintenance of delusions (Menon, Mizrahi, & Kapur, 2008). Two
of the most consistently replicated cognitive biases are the data gathering
BIASES IN SUBCLINICAL DELUSIONS 209
Dow
nloa
ded
by [
Uni
vers
ity o
f W
ater
loo]
at 0
6:48
25
Oct
ober
201
4
bias, characterised by ‘‘jumping to conclusions’’ on probabilistic reasoning
tasks (see Garety & Freeman, 1999, for a review), and a bias against
disconfirmatory evidence (BADE; Woodward, Moritz, & Chen, 2006;
Woodward, Moritz, Cuttler, & Whitman, 2006; Woodward, Moritz, Menon,
& Klinge, 2008). Both cognitive biases are also associated with the presenceof subclinical delusional ideation (Warman & Martin, 2006a, 2006b;
Woodward, Buchy, Moritz, & Liotti, 2007), and the BADE bias is associated
with schizotypy (Buchy, Woodward, & Liotti, 2007).
Besides cognitive biases, personality likely presents a key variable
influencing the development of subclinical delusional ideation. Research
has examined the relationship between personality variables such as the ‘‘big
five’’ and psychosis vulnerability. Of the ‘‘big five’’ factors, ‘‘openness to
experience’’ has been found to be most closely associated with schizotypy(Johns & van Os, 2001), although this relationship has not been consistently
demonstrated (Miller & Tal, 2007). One possible reason is that ‘‘openness’’
appears to be a multidimensional construct consisting of two higher order
subfactors or ‘‘aspects’’ labelled ‘‘openness’’ and ‘‘intellect’’ (DeYoung,
Quilty, & Peterson, 2007). ‘‘Intellect’’ encompasses intellectual engagement
and perceived intellect, and is associated with general intelligence (g)
(DeYoung, Quilty, Peterson, & Gray, in press), whereas ‘‘openness’’
encompasses the domains of aesthetics, fantasy proneness, and willingnessto engage with novel stimuli or beliefs. We therefore hypothesise that only the
‘‘openness’’ aspect would be associated with schizotypy and, by extension,
with subclinical delusional ideation.
Personality variables, having a strong genetic component (Plomin, Owen,
& McGuffin, 1994; Tellegen et al., 1988), may influence or be related to
psychosis vulnerability. Although cognitive biases have been studied in
relation to psychosis vulnerability, the relationship between cognitive biases
and personality, as well as the nature of their relationship to psychosisvulnerability or subclinical delusions, has not been explored in detail.
Cognitive biases might independently influence psychosis vulnerability, or
mediate the relationship between personality and psychosis vulnerability. To
explore the effects of personality on cognitive biases and psychosis
vulnerability concurrently, we examined the impact of cognitive biases and
both aspects of ‘‘openness to experience’’ on subclinical delusional ideation
and schizotypy. Since these cognitive biases have been thought to be
specifically associated with delusions, we hypothesised associations betweenboth sets of variables (cognitive biases and ‘‘openness’’) and the PDI, and
with only the ‘‘odd beliefs/magical ideation’’ but not ‘‘unusual perceptions’’
subscales of the SPQ. To evaluate whether personality and cognitive biases
were also related to each other or showed any mediating relationships, these
two sets of variables were evaluated simultaneously using structural equation
modelling (SEM).
210 MENON ET AL.
Dow
nloa
ded
by [
Uni
vers
ity o
f W
ater
loo]
at 0
6:48
25
Oct
ober
201
4

METHODS
Participants
We recruited 121 healthy participants with no history of psychiatric illness
through advertisements posted within and outside the University of Torontocampus. All participants were fluent in English, with no history of
psychiatric illness, serious head injury, or substance abuse. Data from three
participants were removed because of incomplete responses, and another
because of a psychiatric history, leaving a final sample of 117 participants.
Measures
Subclinical delusional ideation was measured using the PDI (Peters et al.,
2004) and schizotypal traits using the SPQ (Raine, 1991). Personality was
assessed using the Big Five Aspects Scale (DeYoung et al., 2007), which
examines the five factor model and the two aspects of each factor. We were
particularly interested in the ‘‘intellect’’ and ‘‘openness’’ aspects of the
‘‘openness to experience’’ factor.
Probabilistic reasoning task. This widely used task (Garety, Hemsley, &
Wessely, 1991; Moritz & Woodward, 2005; Startup, Freeman, & Garety,
2008) was adapted from earlier studies by our group (Menon et al., 2008;
Menon, Pomarol-Clotet, McKenna, & McCarthy, 2006). In brief,
participants are shown a pair of jars with two types of different coloured
beads in an equal and opposite ratio. One jar has a ratio of 60 red beads and
40 black beads (the ‘‘mostly red’’ jar), and the other contains 40 red beads to60 black beads (the ‘‘mostly black’’ jar). The jars are hidden behind a screen
and beads are presented to participants one at a time in a pseudorandom
sequence and then returned to the jar. Beads are presented until participants
decide which jar the beads come from. The number of draws to decision is
the variable of interest.
BADE task. The BADE task (Woodward et al., 2007; Woodward,
Moritz, & Chen, 2006) is an interactive computer-based test of inferential
reasoning. Participants are presented with a social situation in the form ofthree statements (clues), presented one at a time (e.g., Jane is very thin; Jane
is hungry; Jane lives on the street), and three possible interpretations (e.g.,
Jane is a model; Jane is homeless; Jane is a librarian). After each statement
the participant is required to rate the plausibility of each of the given
interpretations independent of the other two, using a sliding scale of 0 to 10.
A number of the trials feature scenarios designed to lure the participant
BIASES IN SUBCLINICAL DELUSIONS 211
Dow
nloa
ded
by [
Uni
vers
ity o
f W
ater
loo]
at 0
6:48
25
Oct
ober
201
4

towards one of the interpretations (e.g., ‘‘Jane is a model’’ is a ‘‘lure’’); the
third statement (e.g., ‘‘Jane lives on the street’’) provides disconfirmatory
evidence to test participant willingness to accept the new evidence and
change previous interpretations. The computerised BADE task consisted of
35 scenarios (trials), 20 that tested for a bias against disconfirmatoryevidence (where there is a distinct lure), 10 trials where two options remain
equally likely, and five filler trials (where the explanation that appeared
initially likely remains that way). These trials serve to provide variation in the
pattern of responding.
For each of the BADE trials, we calculated the reduction in confidence
between the first and third trials for the ‘‘lure’’ interpretations, as a ratio of
the increased confidence for the ‘‘true’’ interpretations, a measure we refer to
as the BADE ratio. A higher value indicates greater continued confidence inthe lure interpretation, indicative of the bias against disconfirmatory
information being presented.
Analysis
Our variables of interest were the PDI total score (a composite of total scores
on the conviction, preoccupation, and distress items), and the scores on the
‘‘unusual perceptions’’, and ‘‘odd beliefs’’ subscales of the SPQ (consisting of
9 and 7 items respectively). To evaluate the impact of personality and
cognitive biases on schizotypal features, we conducted a series of six path
models. In each model, ‘‘openness’’ and ‘‘intellect’’ served as antecedent
variables (as personality traits likely precede the development of cognitivereasoning strategies); cognitive biases assessed by the BADE and probabil-
istic reasoning tasks served as mediators in separate models. PDI total, SPQ
odd beliefs, and SPQ unusual perceptions scale scores served as outcome
variables in separate models. Age and sex were included as covariates in all
models. Due to the presence of significant multivariate nonnormality
(Mardia’s coefficient of multivariate kurtosis�6.81), path analyses were
conducted in MPlus, utilising robust maximum likelihood method of
estimation (Muthen & Muthen, 1998). Goodness of fit of path models canbe assessed using x2; Confirmatory Fit Index (CFI), with values�.90
indicating acceptable fit; and Root Mean Square Error of Approximation
(RMSEA), with values�.1 indicative of poor fit,B.08 acceptable fit, and
B.05 close fit (Hu & Bentler, 1999).
RESULTS
The final sample consisted of 117 individuals (77 women and 40 men), with a
mean age of 30.7 (SD�12.6; range�18�62), and 16.4 years of total formal
212 MENON ET AL.
Dow
nloa
ded
by [
Uni
vers
ity o
f W
ater
loo]
at 0
6:48
25
Oct
ober
201
4

education (SD�3.4; range�10�25 years). On our measures of interest, our
participants showed mean scores of 14.8 (SD�12.3; range�0�60) on the
PDI, 1.7 (SD�1.9; range�0�7) on SPQ odd beliefs, and 1.8 (SD�1.8;
range�0�7) on SPQ unusual perceptions subscales. The mean ‘‘BADE
ratio’’ on the BADE task was �0.8 (SD�1.0; range��4.2 to 0.3), andmean number of draws to decision on the probabilistic reasoning task was 9
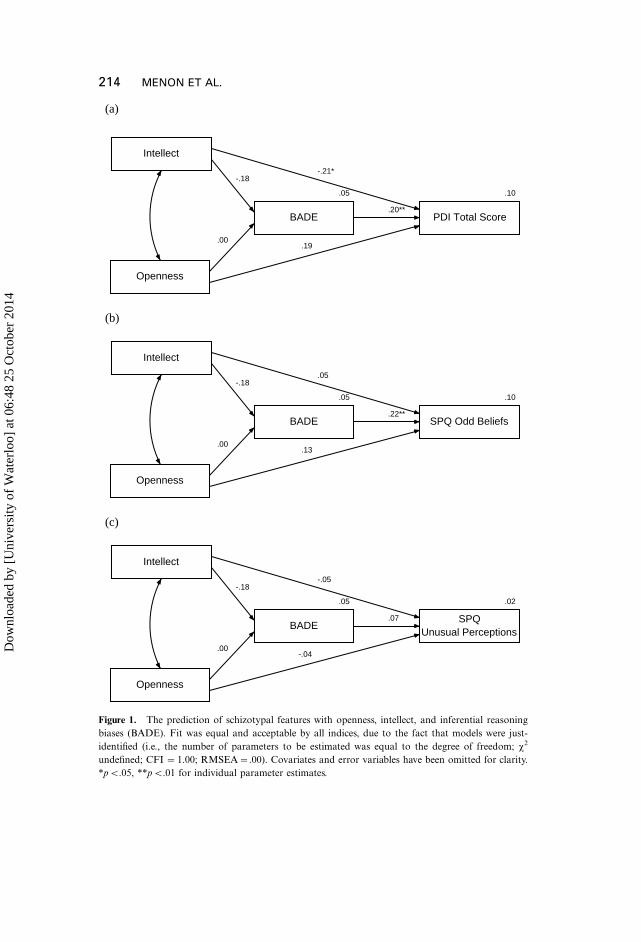
(SD�3.9; range�1�15). Path models are depicted in Figures 1 and 2. Age
and sex did not significantly predict cognitive biases or schizotypal features
(and are therefore omitted for clarity). The BADE bias (see Figure 1) was
specifically associated with subclinical delusional ideation (i.e., PDI total
and SPQ odd beliefs), but not subclinical hallucinations (i.e., SPQ unusual
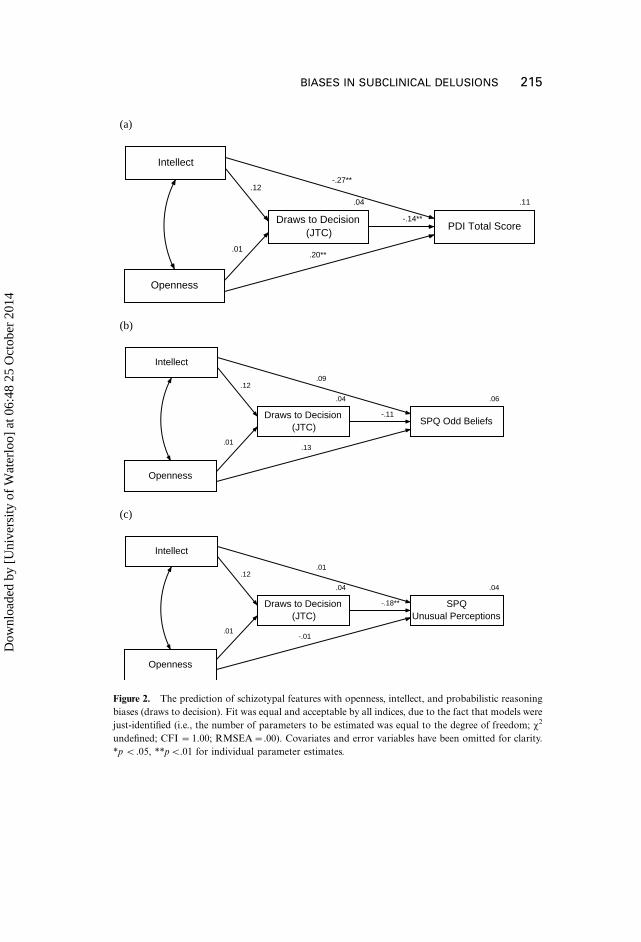
perceptions). On the probabilistic reasoning task, only 2/117 of our
participants showed the ‘‘jumping to conclusions’’ (JTC) response pattern,operationalised as two or fewer draws-to-decision (Garety et al., 2005;
Startup et al., 2008). As depicted in Figure 2, the number of draws to
decision was negatively associated with PDI total score and SPQ unusual
perceptions (but fell just short of significance with SPQ odd beliefs scale). In
both models, openness independently and positively predicted PDI total
score; whereas intellect negatively predicted PDI total score (at trend levels
of p�.058 in Model 1, and at pB.05 in Model 2). These personality
variables were not significantly predictive of either of the SPQ scale scores.The cognitive biases did not mediate the relationship between personality
and delusions (Kraemer, Stice, Kazdin, Offord, & Kupfer, 2001), and neither
openness or intellect were associated with the cognitive biases.
To evaluate empirical support for our causal ordering of variables, we also
repeated the analyses using cognitive biases as antecedent variables and
personality variables as mediators. The fit of an alternate model in which
cognitive reasoning measures are modelled as antecedent variables and
personality traits as mediator variables resulted in a significant decrease in fit(i.e., a decrease in CFI �.01, as per Cheung & Rensvold, 2002, and an
Akaike Information Criterion of greater value). These results suggest that
these results are robust and that an alternate ordering of variables cannot be
empirically justified.
DISCUSSION
Our results suggest that the BADE bias, characterised by a reduced
weighting of disconfirmatory information, is specifically associated with
subclinical delusional ideation, but not perceptual abnormalities indicative
of subclinical hallucinations. Although only two of the participants showed
the JTC response pattern, the number of draws to decision is negatively
correlated with both subclinical delusions and hallucinations. This has
BIASES IN SUBCLINICAL DELUSIONS 213
Dow
nloa
ded
by [
Uni
vers
ity o
f W
ater
loo]
at 0
6:48
25
Oct
ober
201
4
(a)
Intellect
Openness
.05
BADE
.10
PDI Total Score.20**
.19
-.21*
.00
-.18
(b)
Intellect
Openness
.05
BADE
.10
SPQ Odd Beliefs.22**
.13
.05
.00
-.18
(c)
Intellect
Openness
.05
BADE
.02
SPQUnusual Perceptions
.07
-.04
-.05
.00
-.18
Figure 1. The prediction of schizotypal features with openness, intellect, and inferential reasoning
biases (BADE). Fit was equal and acceptable by all indices, due to the fact that models were just-
identified (i.e., the number of parameters to be estimated was equal to the degree of freedom; x2
undefined; CFI �1.00; RMSEA�.00). Covariates and error variables have been omitted for clarity.
*pB.05, **pB.01 for individual parameter estimates.
214 MENON ET AL.
Dow
nloa
ded
by [
Uni
vers
ity o
f W
ater
loo]
at 0
6:48
25
Oct
ober
201
4
(a)
Intellect
Openness
.04
Draws to Decision(JTC)
.11
PDI Total Score-.14**
.20**
-.27**
.01
.12
(b)
Intellect
Openness
.04
Draws to Decision(JTC)
.06
SPQ Odd Beliefs-.11
.13
.09
.01
.12
(c)
Intellect
Openness
.04
Draws to Decision(JTC)
.04
SPQUnusual Perceptions
-.18**
-.01
.01
.01
.12
Figure 2. The prediction of schizotypal features with openness, intellect, and probabilistic reasoning
biases (draws to decision). Fit was equal and acceptable by all indices, due to the fact that models were
just-identified (i.e., the number of parameters to be estimated was equal to the degree of freedom; x2
undefined; CFI �1.00; RMSEA�.00). Covariates and error variables have been omitted for clarity.
*p B.05, **pB.01 for individual parameter estimates.
BIASES IN SUBCLINICAL DELUSIONS 215
Dow
nloa
ded
by [
Uni
vers
ity o
f W
ater
loo]
at 0
6:48
25
Oct
ober
201
4

parallels with patient data, which indicates that the ‘‘data gathering bias’’
might be associated with positive symptoms in general, rather than just
delusions (Menon et al., 2006).
An interesting and unanswered question has centred on how the genes for
psychosis vulnerability have persisted in the gene pool, and one possible
hypothesis is that, in their attenuated form, the psychosis vulnerability genes
and the associated personality constructs (schizotypal traits) may confer
some evolutionary advantage (such as ‘‘creativity’’). Openness has also been
shown to be associated with traits such as creativity, and has been speculated
to mediate the ‘‘schizotypy�creativity’’ link (Miller & Tal, 2007). Our current
results may shed light on this issue as they suggest that it is the ‘‘openness’’
aspect which is associated specifically with the subclinical delusions, with
‘‘intellect’’ showing a negative correlation, suggesting that it might be a
protective factor. It is possible that positive schizotypy (measured by the two
SPQ subscales we considered) is a more general construct, with weaker
associations with these aspects of personality. Alternatively, although the
PDI and the SPQ ‘‘odd beliefs’’ subscale putatively measure similar
underlying constructs, we found stronger associations with the PDI scores.
This indicates that the PDI might be a better indicator of subclinical
delusional ideation, or that the composite score created (which integrates
information on conviction, distress, and preoccupation) better captures the
range of underlying phenotypic features of these beliefs.
Importantly, the results indicate that cognitive biases and personality are
not related to each other, but, rather, are independently associated with
subclinical ideation, and therefore likely to be independent risk factors for
the development of delusions.
Manuscript received 2 December 2011
Revised manuscript received 13 March 2012
First published online 4 July 2012
REFERENCES
Broome, M., Johns, L., Woolley, J., Brett, C., Tabraham, P., Valmaggia, L., et al. (2004). The data-
gathering bias in the at-risk mental state (ARMS) for psychosis. Schizophrenia Research, 70,
100�101.
Buchy, L., Woodward, T. S., & Liotti, M. (2007). A cognitive bias against disconfirmatory evidence
(BADE) is associated with schizotypy. Schizophrenia Research, 90, 334�337.
Cheung, G. W., & Rensvold, R. B. (2002). Evaluating goodness-of-fit indexes for testing
measurement invariance. Structural Equation Modeling: A Multidisciplinary Journal, 9, 233�255.
DeYoung, C. G., Quilty, L. C., & Peterson, J. B. (2007). Between facets and domains: 10 aspects of
the big five. Journal of Personality and Social Psychology, 93, 880�896.
DeYoung, C..G., Quilty, L. C., Peterson, J. B., & Gray, J. R. (in press). Openness to experience,
intellect, and cognitive ability. Journal of Personality Assessment.
216 MENON ET AL.
Dow
nloa
ded
by [
Uni
vers
ity o
f W
ater
loo]
at 0
6:48
25
Oct
ober
201
4

Garety, P. A., & Freeman, D. (1999). Cognitive approaches to delusions: A critical review of
theories and evidence. British Journal of Clinical Psychology, 38, 113�154.
Garety, P. A., Freeman, D., Jolley, S., Dunn, G., Bebbington, P. E., Fowler, D. G., et al. (2005).
Reasoning, emotions, and delusional conviction in psychosis. Journal of Abnormal Psychology,
114, 373�384.
Garety, P. A., Hemsley, D. R., & Wessely, S. (1991). Reasoning in deluded schizophrenic and
paranoid patients*biases in performance on a probabilistic inference task. Journal of Nervous
and Mental Disease, 179, 194�201.
Hu, L. T., & Bentler, P. M. (1999). Cutoff criteria for fit indexes in covariance structure analysis:
Conventional criteria versus new alternatives. Structural Equation Modeling: A Multidisciplin-
ary Journal, 6, 1�55.
Johns, L. C., & van Os, J. (2001). The continuity of psychotic experiences in the general population.
Clinical Psychological Review, 21, 1125�1141.
Kendler, K., Neale, M., & Walsh, D. (1995). Evaluating the spectrum concept of schizophrenia in
the Roscommon Family Study. American Journal of Psychiatry, 152, 749�754.
Kraemer, H. C., Stice, E., Kazdin, A., Offord, D., & Kupfer, D. (2001). How do risk factors work
together? Mediators, moderators, and independent, overlapping, and proxy risk factors.
American Journal of Psychiatry, 158, 848�856.
Meehl, P. E. (1962). Schizotaxia, schizotypy, schizophrenia. The American Psychologist, 17, 827�838.
Menon, M., Mizrahi, R., & Kapur, S. (2008). ‘‘Jumping to conclusions’’ and delusions in
psychosis: Relationship and response to treatment. Schizophrenia Research, 98, 225�231.
Menon, M., Pomarol-Clotet, E., McKenna, P. J., & McCarthy, R. A. (2006). Probabilistic
reasoning in schizophrenia: A comparison of the performance of deluded and nondeluded
schizophrenic patients and exploration of possible cognitive underpinnings. Cognitive
Neuropsychiatry, 11, 521�536.
Miller, G. F., & Tal, I. R. (2007). Schizotypy versus openness and intelligence as predictors of
creativity. Schizophrenia Research, 93, 317�324.
Moritz, S., & Woodward, T. S. (2005). Jumping to conclusions in delusional and non-delusional
schizophrenic patients. British Journal of Clinical Psychology, 44, 193�207.
Muthen, L. K., & Muthen, B. O. (1998). Mplus user’s guide (4th ed). Los Angeles, CA: Muthen &
Muthen.
Peters, E., Joseph, S., Day, S., & Garety, P. (2004). Measuring delusional ideation: The 21-Item
Peters et al. Delusions Inventory (PDI). Schizophrenia Bulletin, 30, 1005�1022.
Plomin, R., Owen, M., & McGuffin, P. (1994). The genetic basis of complex human behaviors.
Science, 264, 1733�1739.
Raine, A. (1991). The SPQ: A scale for the assessment of schizotypal personality based on DSM-
III-R criteria. Schizophrenia Bulletin, 17, 556�564.
Startup, H., Freeman, D., & Garety, P. A. (2008). Jumping to conclusions and persecutory
delusions. European Psychiatry, 23, 457�459.
Tellegen, A., Lykken, D. T., Bouchard, T. J., Wilcox, K. J., Segal, N. L., & Rich, S. (1988).
Personality similarity in twins reared apart and together. Journal of Personality and Social
Psychology, 54, 1031�1039.
van Os, J., Hanssen, M., Bijl, R. V., & Ravelli, A. (2000). Strauss (1969) revisited: A psychosis
continuum in the general population? Schizophrenai Research, 45, 11�20.
Warman, D. M., & Martin, J. M. (2006a). Cognitive insight and delusion proneness: An
investigation using the Beck Cognitive Insight Scale. Schizophrenai Research, 84, 297�304.
Warman, D. M., & Martin, J. M. (2006b). Jumping to conclusions and delusion proneness: The
impact of emotionally salient stimuli. Journal of Nervous and Mental Disease, 194, 760�765.
doi:10.1097/01.nmd.0000239907.83668.aa
BIASES IN SUBCLINICAL DELUSIONS 217
Dow
nloa
ded
by [
Uni
vers
ity o
f W
ater
loo]
at 0
6:48
25
Oct
ober
201
4

Woodward, T. S., Buchy, L., Moritz, S., & Liotti, M. (2007). A bias against disconfirmatory
evidence is associated with delusion proneness in a nonclinical sample. Schizophrenia Bulletin,
33, 1023�1028.
Woodward, T. S., Moritz, S., & Chen, E. Y. H. (2006). The contribution of a cognitive bias against
disconfirmatory evidence (BADE) to delusions: A study in an Asian sample with first episode
schizophrenia spectrum disorders. Schizophrenai Research, 83, 297�298.
Woodward, T. S., Moritz, S., Cuttler, C., & Whitman, J. C. (2006). The contribution of a cognitive
bias against disconfirmatory evidence (BADE) to delusions in schizophrenia. Journal of
Clinical and Experimental Neuropsychology, 28, 605�617.
Woodward, T. S., Moritz, S., Menon, M., & Klinge, R. (2008). Belief inflexibility in schizophrenia.
Cognitive Neuropsychiatry, 13, 267�277.
218 MENON ET AL.
Dow
nloa
ded
by [
Uni
vers
ity o
f W
ater
loo]
at 0
6:48
25
Oct
ober
201
4