The Rise of State Medicine
24
Lecture 7 Cradle to Grave
description
The Rise of State Medicine. Lecture 7 Cradle to Grave. Lecture themes. Precursors of state medicine – charity and Poor Law Social medicine in the interwar period The birth of the NHS Was the NHS a radical new model of health care or were there important continuities with the past? - PowerPoint PPT Presentation
Transcript of The Rise of State Medicine

Lecture 7Cradle to Grave

Precursors of state medicine – charity and Poor Law
Social medicine in the interwar period
The birth of the NHS
Was the NHS a radical new model of health care or were there important continuities with the past?
Was the NHS born out of consensus or conflict? What is the relationship of the health care system
to wider political economy (John Pickstone’s model of productionist, communitarian and consumerist medicine)

Medical charity continued to play a vital role in health care up until setting up of NHS – especially voluntary hospitals
By early 20th century, more patients paid directly for care or paid for by insurance scheme, often run by a Friendly Society
Since 1870s voluntary hospitals under financial pressure – concerns about losing subscriptions
After introduction of NI increasingly took seriously ill patients referred by GP – more specialised
Still treated large number of poor as out-patients Hospitals anxious that treating patients who
could afford to pay
Precursors of state medicine: medical Precursors of state medicine: medical charitycharity

Poor Law of course was a form of state medicine, funded by local poor rates
Increasingly Poor Law provided better standard of care by late 19th/early 20th century, especially infirmary provision in major towns and cities
1929 Local Government Act abolished the Boards of Guardians – responsibilities transferred to local authorities and MOHs power increased as they assumed control over general hospitals
But Poor Law based on need/impoverishment not a ‘right’ to medical care
Precursors to state medicine: Poor LawPrecursors to state medicine: Poor Law

Edwin Chadwick: faith in central government and big engineering projects; poverty was linked to disease. Led to public health reform.
Early notion of state responsibility: role of the state to provide decent environmental conditions e.g. housing and factory. Role of MOHs.
Ideas of prevention: medicine and state working hand-in-hand to improve health through preventive approach/health education.
And of course vaccination, notification, infant welfare clinics, and so on.

1911- National Insurance Act◦ Access to GP services via a panel doctor◦ Hospital treatment not included◦ Three types of benefit: sickness, accident and disability,
pension◦ Financed by contributions from employer, employee & state
◦ Administered through ‘approved mutual societies’
◦ Benefits limited to the contributor (worker) - mainly men. Women and children were not covered
◦ The act was met with concern from medical practitioners who feared the impact on private practice

‘The Dawn of Hope’ The National Insurance Act of 1911

National Health Insurance introduced in 1911

Interwar periodInterwar period 1919 Ministry of Health created – took
responsibility for care of mothers and children and infant life protection, supervised local authority health services
The Dawson Report of 1920 put forward ambitious plan for integration of preventive and curative services - recommended a two tier system of GP and specialist health centres
1920s and 1930s local authorities ran large range of services – infant and maternal welfare clinics, VD clinics, TB clinics and sanatoria.
Responsible for environmental health, clean food and milk, refuse removal, clean air, river and water pollution

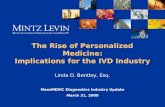
Finsbury Health Centre

Medical facilities available at a modern health centre Medical facilities available at a modern health centre contrasted with ill health in old-fashioned housing. contrasted with ill health in old-fashioned housing. Colour lithograph after A. Games, 1942. Colour lithograph after A. Games, 1942.

Strong perception that good health still a matter of individual and family responsibility. e.g. in safety campaigns emphasised that it was personal carelessness that caused accidents rather than dangerous conditions.
Faith in health education to train individuals and families. Fitness encouraged as was cleanliness.
But some argued (including number of MPs) that what needed to change – better working conditions, decent housing, improved nutrition, etc. But overall low incomes and socio-economic factors ignored.
Health educationHealth education

Women’s League of Health and Beauty Women’s League of Health and Beauty 1930s1930s

Socialist Medical Association – left wing doctors who called for a free national health service administered by local authorities.
1937: report by the Political and Economic Planning Group on British health services. Recommended a central role for GPs and a coordinated specialist system backing up primary care.
Emergency Medical Services. This was founded to deal civilian bombing casualties -hospital beds, casualty clearing facilities and specialist hospitals. Regional coordination directed by the Ministry of Health. Breakthrough in organisation and experience - critical in accelerating plans for a national health service.

Recommended a comprehensive social security system and health care service.
Health care should be available to all regardless of their ability to pay.
Proposed that doctors should be employed directly by the state.
More generally, the report recommended that the government should find ways of fighting the five ‘Giant Evils’ of ‘Want, Disease, Ignorance, Squalor and Idleness’.

Raised political temperature, setting out two guiding principles. Firstly, that a national health service should be comprehensive, with citizens receiving the advice, treatment and care they needed, combined with the best medical and other facilities available. Secondly, that the service should be free to the public at the point of use.
‘To ensure that everybody in the country- irrespective of means, age, sex and occupation - shall have equal opportunity to benefit from the most up to date medical and allied services available… to divorce the case of health from questions of personal means and other factors irrelevant to it; to provide the service free of charge… and to encourage a new attitude to Health - the easier obtaining of advice early on, the promotion of good health rather than only treatment of the bad.’

Labour Party election posters (1945)

Objected to the concept of a salaried service
Objected to Local Authority control
Fear that would threaten clinical freedom
Echoed control of Poor Law and Friendly Societies
Wanted an enhanced role for voluntary hospitals and consultants.

Members of the BMA
dressed as gladiators,
conceding the introduction of National
Health Service to Aneurin
Bevan, dressed as
Nero.

• Hospitals: Voluntary and local authority hospitals were nationalised – managed by regional boards
• Local authorities – health centres, clinics, health visiting, ambulances
• GP, dental and optician services – operated on an independent contractor basis; administered by Executive Councils.

NHS introductory leaflet
The NHS came into being on 5 July 1948.
Care was free at the point of delivery.
Free dental care, free spectacles, free consultations with a GP, referral to hospital and free treatment.


C20th : ‘great troika of progress - science, profession, state’
1900-1948 - Productionist focus on health of the industrial worker and the armed services – resulted in National Insurance.
1948-1970 - CommunitarianNHS - expansion of services, focus on social inclusionRise of the professional
1970-2000 - ConsumptionRenewed emphasis on market and lay management of health services. Medicine is serving consumers who demand more and more.

Turn of the 20th century: transformation in public and official expectation - notion of state intervention in health gained ground.
National Insurance Act 1911 marked a significant extension of medical and state involvement in the health of the nation.
The NHS greatly extended the reach of organised medicine and encouraged those who had previously been too poor or reticent to come forward for consultation/treatment.
Overall shift in perception of medicine as part of free market, governed by ability to pay to becoming a right for all citizens ‘from cradle to grave’.