THE REVISION HIP Porous metal augmentsof segmental defect percentages for each quad-rant is used to...
6
VOL. 95-B, No. 11, NOVEMBER 2013 103 THE REVISION HIP Porous metal augments BIG HOPES FOR BIG HOLES M. Abolghasemian, S. Tangsataporn, A. Sternheim, D. J. Backstein, O. A. Safir, A. E. Gross From Mount Sinai Hospital, University of Toronto, Toronto, Ontario, Canada M. Abolghasemian, MD, Assistant Professor of Orthopedic Surgery Iran University of Medical Sciences, Shafa hospital, Jaleh Street, Baharestan Square, Tehran, 1157637131, Iran. S. Tangsataporn, MD, Orthopedic surgeon, Research fellow A. Sternheim, MD, Clinical Fellow of Orthopedic Surgery D. J. Backstein, MD, FRCSC, Associate Professor of Orthopedic Surgery O. A. Safir, MD, FRCSC, Assistant Professor of Orthopedic Surgery A. E. Gross, MD, FRCSC, Professor of Orthopedic Surgery Division of Orthopaedics, Mount Sinai Hospital, University of Toronto, 600 University Avenue, Suite 476A, Toronto, Ontario, M5G 1X5, Canada. Correspondence should be sent to M. Abolghasemian; e-mail: [email protected] ©2013 The British Editorial Society of Bone & Joint Surgery doi:10.1302/0301-620X.95B. 32907 $2.00 Bone Joint J 2013;95-B, Supple A:103–8. Received 7 September 2013; Accepted after revision 8 September 2013 The conventional method for reconstructing acetabular bone loss at revision surgery includes using structural bone allograft. The disadvantages of this technique promoted the advent of metallic but biocompatible porous implants to fill bone defects enhancing initial and long-term stability of the acetabular component. This paper presents the indications, surgical technique and the outcome of using porous metal acetabular augments for reconstructing acetabular defects. Cite this article: Bone Joint J 2013;95-B, Supple A:103–8. Most acetabular revision operations are cur- rently performed using a hemispherical ace- tabular component. 1 However, when there is a significant amount of segmental and/or con- tained bone loss such that the initial stability or long-term fixation of the acetabular com- ponent cannot be achieved, augmentation is indicated. The conventional method of using either minor (< 50% of the acetabulum) or major (> 50% of the acetabulum) column structural allografts has disadvantages. The risk of disease transmission is low but possible 2 and in the longer term there may be immunological reactions by the host tissue and reabsorption of the graft material. 3 Porous materials facilitate bone ingrowth and augments made with these metals come in dif- ferent shapes and sizes. All offer the facility to fill variable defect types and to provide struc- tural support to the acetabular component (Fig. 1). The high porosity of the products is ideal for bone ingrowth, 4 the porous augment will be supported by the host bone after ingrowth occurs, and ultimately, the acetabu- lar implant will be supported both directly at its contact site to the host bone, and indirectly through the bony contact of the augment. This is the base of our concept of ‘effective host bone contact’, defined as the sum of the contact area of both porous implants (acetab- ular component and any augment) with the host bone. Since a certain amount of contact of the implant with host bone is considered essential for long term stability of the acetab- ular component, a porous augment will enhance this stability through increasing the contact area. It is to be noted that the aug- ment-bone contact area is often some distance from the acetabular component proper. This in effect extends the usable bone available to sustain acetabular stability Surgical technique After exposure of the acetabulum through the surgeon’s preferred approach, the old compo- nent, surrounding debris and fibrous tissue should be removed, careful not to compromise further the already defective bone stock. After exposing the acetabular floor, gentle reaming at the correct anatomical position should be performed to prepare the bony bed. The final classification of bone defect is best done at this stage. The authors use their own classification based on the percentage of acetabular bone that has been lost (Table I). 5 If the circumference of the actabular rim is intact, any bone loss will be considered con- tained. In the case of a segmental defect, the authors use the trial acetabulum to classify the defect. The bone defect is quantified based on the uncovered portion of a trial inserted into the cavity after completion of reaming. The trial is divided into four quadrants and the sum of segmental defect percentages for each quad- rant is used to compile the total defect. Once the classification has been made, the appropri- ate acetabular reconstruction can be deter- mined. Type I and II defects do not usually require the use of acetabular augments. In type I, conventional cemented or cementless com- ponents can be used. Type II defects are usually managed by morsellised bone grafting and nor- mal uncemented, or impaction grafting with cemented acetabular cups. If there is < 50% contact of the cup with viable host bone, the use of an ultra-porous acetabular component
Transcript of THE REVISION HIP Porous metal augmentsof segmental defect percentages for each quad-rant is used to...

VOL. 95-B, No. 11, NOVEMBER 2013 103
THE REVISION HIP
Porous metal augments BIG HOPES FOR BIG HOLES
M. Abolghasemian,S. Tangsataporn,A. Sternheim,D. J. Backstein,O. A. Safir,A. E. Gross
From Mount Sinai Hospital, University of Toronto, Toronto, Ontario, Canada
M. Abolghasemian, MD, Assistant Professor of Orthopedic SurgeryIran University of Medical Sciences, Shafa hospital, Jaleh Street, Baharestan Square, Tehran, 1157637131, Iran.
S. Tangsataporn, MD, Orthopedic surgeon, Research fellow A. Sternheim, MD, Clinical Fellow of Orthopedic Surgery D. J. Backstein, MD, FRCSC, Associate Professor of Orthopedic Surgery O. A. Safir, MD, FRCSC, Assistant Professor of Orthopedic Surgery A. E. Gross, MD, FRCSC, Professor of Orthopedic SurgeryDivision of Orthopaedics, Mount Sinai Hospital, University of Toronto, 600 University Avenue, Suite 476A, Toronto, Ontario, M5G 1X5, Canada.
Correspondence should be sent to M. Abolghasemian; e-mail: [email protected]
©2013 The British Editorial Society of Bone & Joint Surgerydoi:10.1302/0301-620X.95B. 32907 $2.00
Bone Joint J 2013;95-B, Supple A:103–8.Received 7 September 2013; Accepted after revision 8 September 2013
The conventional method for reconstructing acetabular bone loss at revision surgery includes using structural bone allograft. The disadvantages of this technique promoted the advent of metallic but biocompatible porous implants to fill bone defects enhancing initial and long-term stability of the acetabular component. This paper presents the indications, surgical technique and the outcome of using porous metal acetabular augments for reconstructing acetabular defects.
Cite this article: Bone Joint J 2013;95-B, Supple A:103–8.
Most acetabular revision operations are cur-rently performed using a hemispherical ace-tabular component.1 However, when there isa significant amount of segmental and/or con-tained bone loss such that the initial stabilityor long-term fixation of the acetabular com-ponent cannot be achieved, augmentation isindicated. The conventional method of usingeither minor (< 50% of the acetabulum) ormajor (> 50% of the acetabulum) columnstructural allografts has disadvantages. Therisk of disease transmission is low butpossible2 and in the longer term there may beimmunological reactions by the host tissueand reabsorption of the graft material.3
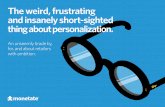
Porous materials facilitate bone ingrowth andaugments made with these metals come in dif-ferent shapes and sizes. All offer the facility tofill variable defect types and to provide struc-tural support to the acetabular component(Fig. 1). The high porosity of the products isideal for bone ingrowth,4 the porous augmentwill be supported by the host bone afteringrowth occurs, and ultimately, the acetabu-lar implant will be supported both directly atits contact site to the host bone, and indirectlythrough the bony contact of the augment.This is the base of our concept of ‘effectivehost bone contact’, defined as the sum of thecontact area of both porous implants (acetab-ular component and any augment) with thehost bone. Since a certain amount of contactof the implant with host bone is consideredessential for long term stability of the acetab-ular component, a porous augment willenhance this stability through increasing thecontact area. It is to be noted that the aug-ment-bone contact area is often some distance
from the acetabular component proper. Thisin effect extends the usable bone available tosustain acetabular stability
Surgical techniqueAfter exposure of the acetabulum through thesurgeon’s preferred approach, the old compo-nent, surrounding debris and fibrous tissueshould be removed, careful not to compromisefurther the already defective bone stock. Afterexposing the acetabular floor, gentle reamingat the correct anatomical position should beperformed to prepare the bony bed. The finalclassification of bone defect is best done at thisstage. The authors use their own classificationbased on the percentage of acetabular bonethat has been lost (Table I).5
If the circumference of the actabular rim isintact, any bone loss will be considered con-tained. In the case of a segmental defect, theauthors use the trial acetabulum to classify thedefect. The bone defect is quantified based onthe uncovered portion of a trial inserted intothe cavity after completion of reaming. Thetrial is divided into four quadrants and the sumof segmental defect percentages for each quad-rant is used to compile the total defect. Oncethe classification has been made, the appropri-ate acetabular reconstruction can be deter-mined. Type I and II defects do not usuallyrequire the use of acetabular augments. In typeI, conventional cemented or cementless com-ponents can be used. Type II defects are usuallymanaged by morsellised bone grafting and nor-mal uncemented, or impaction grafting withcemented acetabular cups. If there is < 50%contact of the cup with viable host bone, theuse of an ultra-porous acetabular component

104 M. ABOLGHASEMIAN, S. TANGSATAPORN, A. STERNHEIM, D. J. BACKSTEIN, O. A. SAFIR, A. E. GROSS
CCJR SUPPLEMENT TO THE BONE & JOINT JOURNAL
(i.e. trabecular metal (TM), Zimmer, Warsaw, Indiana) isrecommended to ensure sufficient initial stability andpotential for subsequent bone ingrowth.
Types III and IV defects are most frequently associatedwith the use of augments. Enhancing the stability of the cupwith structural support either with allograft bone oran augment is usually necessary when facing a defect of> 40%, or when the press-fit of a TM cup cannot beachieved.6 The potential for bony ingrowth by the hostbone is a requirement when planning to use an augment,otherwise non-biological alternatives such as conventionalmetal cages should be considered.7 Selection of the appro-priate augment is based on the size of the defect and thegeometry of the adjacent pelvic bone. Our experience has
been with trabecular metal (TM) augments and the rest ofthis text will refer to these products.
The augment can be placed in any position or orientationto improve the initial stability of the construct, but there aresome common situations. Firstly, a minor or major columndefect that is surrounded by an intact rim of acetabularbone within 30 mm of the outer perimeter of the trial ace-tabular cup, which is the maximum thickness of augmentsnormally available. One or two conventional augments canbe used in a ‘wedge’ configuration to fill a similarly shapeddefect (Fig. 2). The appropriate diameter of the augment ischosen based on the internal diameter of the segmentaldefect of the acetabulum, which is usually equal or smallerrelative to the trial cup diameter. Our preference is to fix the
Fig. 1c
Photographs of various augments, showing a) conventional augments in a range of thicknesses, b) anterior, posterior and straight column buttressaugments, c) restrictors and d) shim augments.
Fig. 1a Fig. 1b
Fig. 1d
Table I. Gross classification of acetabular bone loss
Type Defect
I No significant loss of bone stockII Contained loss of bone stock (cavitary)III Uncontained loss of bone stock involving < 50% of acetabulum (minor column defect)IV Uncontained loss of bone stock involving > 50% of acetabulum (major column defect)V Pelvic discontinuity with uncontained loss of bone stock

POROUS METAL AUGMENTS 105
VOL. 95-B, No. 11, NOVEMBER 2013
augment first, kept in place with the guide of the trial cup.As many screws as possible (at least two) should be insertedto fix the augment before inserting the TM cup.
Secondly, a severe contained medial defect is faced withan intact but thin peripheral rim which would not be suffi-ciently supportive for a cementless cup. A conventionalaugment could be inserted into the defect as a foundation inorder to provide medial support to the overlying acetabularshell (Fig. 3).
Thirdly, when a minor column defect is present with nobony rim available within 30 mm of the trial cup but with asupportive bony bed, a conventional augment can be used inthe opposite way of the ‘wedge’ configuration. The flat sur-face of the augment is placed medially against the ilium justabove the trial cup (Fig. 4), and secured to the bone withthree screws. This ‘flying buttress’ configuration is assumed
to be supportive to the cup as only a moderate amount ofshear force on the augment is expected with a minor columndefect. A thicker augment is preferable to obtain as broad acontact as possible with the underlying bone.
Finally, a major column defect is associated with lack ofbony rim within 30 mm of the trial cup. We feel that eventhe strongest conventional augment in ‘flying buttress’ con-figuration would not have enough host bone contact toresist the powerful shear forces exerted by the uncoveredelement of the acetabular component. Buttress augments inthis situation aim to maximise the bone contact area andstability of the construct as a whole. In case of a straightsuperior defect, a straight buttress (figure of seven) (Fig. 1)augment is desirable. When the defect is mainly in the ante-rior or posterior part of the trial acetabular component,an anterior or a posterior column buttress augment is
Fig. 2
Radiograph showing a minor column defect reconstructed with a TM cup and a TM augment in ‘wedge’ configuration.
Fig. 3a
A 53-year-old woman underwent an operation to revise a loose, protruded cup. a) The subsequentradiograph shows a small segmental defect associated with a large contained medial defect. Oneaugment in the ‘flying buttress’ configuration and one in the ‘foundation’ configuration were used toreinforce the TM cup. b) Post-operative radiograph after one year. Cup and augments are stable: thepatient is functioning very well.
Fig. 3b

106 M. ABOLGHASEMIAN, S. TANGSATAPORN, A. STERNHEIM, D. J. BACKSTEIN, O. A. SAFIR, A. E. GROSS
CCJR SUPPLEMENT TO THE BONE & JOINT JOURNAL
preferable (Fig. 1b). The corresponding part of the iliumshould be exposed in order to seat the augment. If a gappersists between the flat part of the augment and the ilium,a shim augment can be used (Fig. 5). The abutting surfacesof the shim and the buttress augment are then filled withbone cement. Any remaining contained defects should befilled with particulate bone graft.
The use of more than one augment in a single reconstruc-tion may be required,8 especially when a major columndefect is to be addressed using ‘wedge’ rather than ‘buttress’augments; they can be placed in wedge configuration, eitherside by side or at opposing poles of the acetabulum, basedon the location of the bone defect. The selected augmentfrequently is not a perfect match to the defect and someadjustments will be necessary. Minor mismatches could be
addressed by burring the bony bed to accommodate theaugment. Major discrepancies, however are usuallycorrected by removing the corresponding portion of theaugment using a rongeur. We routinely pack some morsell-ised bone graft into the windows of the augment to encour-age bone remodeling.
The augment will not provide full support for the cupand metal debris may be released through fretting if theyare not cemented. The ‘effective host bone contact’ conceptis valid only if there is a reasonable unity of the constructcomprised of the porous cup and the porous augment. Themechanical validity of this combined construct remains tobe verified, but as most of the forces between cup and aug-ment are compressive, the authors feel the cement is capa-ble of accommodating these forces. We have modified the
Fig. 4
Radiograph showing a minor column defect reconstructed with a TMaugment in ‘flying buttress’ configuration.
Fig. 5a
Radiograph showing a major column defect, which has been a) reconstructed by a TM cup in addition to b) a straight buttress and a shim augment.
Fig. 5b

POROUS METAL AUGMENTS 107
VOL. 95-B, No. 11, NOVEMBER 2013
original technique recommended by the manufacturer,including the application of bone cement to the interface ofcup and augment at the time of insertion of the TM cup. Asmall amount of cement is placed between the cup and theaugment while cementing the liner to the revision shell. Arevision TM shell is preferable when using an augment, asthe surgeon has some flexibility in positioning a revisioncup as minor mal-positions can be compensated for byadjusting the position of the liner within the shell. Extrascrew holes can also be drilled through the shell material tothe best available host bone. This type of porous tantalumrevision cup possesses a lower modulus of elasticity that isbiomechanically advantageous.4
The porous acetabular component is fixed with a mini-mum of three screws. It is beneficial to have some screwsinserted superiorly and postero-superiorly into the pelviccolumns, and an additional ischial screw to provide stabil-ity for the cup in as many planes as possible. If the best boneavailable to fix the screws is out of alignment with the man-ufacturer’s provided screw holes, new holes can be madewith a metal burr when using a revision TM shell. How-ever, in these circumstances, some metal debris will inevita-bly be released and, the long term consequence is as yetunknown. Occasionally it is possible to strengthen the con-struct further by aligning one screw hole of the cup with theaugment window so that a screw can go across both com-ponents into the host bone.
Porous augments have been used in combination withalternative acetabular components to ultra-porous cement-less shells. Recently, good results were reported for impac-tion grafting as well as application of combined cementedcups and porous augments.9 The authors have frequentlyused TM augments in association with cup-cage constructsand conventional cages, and the use of porous augmentscan also be justified in some primary hip replacements. Onecommon indication is when there is a significant segmentaldefect in acetabulum in an elderly patient, especially in theabsence of a usable femoral head for autograft.
Post-operatively, the patients are advised to restrictweight bearing for eight to 12 weeks based on the stabilityof fixation and the amount of bone loss (less for the wedgeconfiguration and more for other configurations). Patientsare followed regularly and radiographs are evaluatedregarding signs of cup or augment loosening, including theappearance of lucent lines around the implants, changes inposition of the components and progressive metal debrisshedding; a sign of friction between a loose cup and a stableaugment.6 Valid radiological criteria for augment looseningremains to be defined.
OutcomesThe use of porous augments in acetabular revision has beenrewarding in short and mid-term follow-up. In the fiveseries reported so far, 154 augments (147 conventional andseven buttress augments) were used in 149 hips.6,10-13 Weexcluded the reports on the mixed results of acetabular
reconstructions with and without augments.14 The mean fol-low up of these studies have ranged from 32 to 64.5 monthsand a total of seven aseptic failures were reported.Most recently, Abolghasemian et al6 reported on the first34 revisions performed with the use of TM cups and aug-ments in our institution. At a mean follow-up of64.5 months, there were three aseptic and one septic loos-enings. There were no aseptic failures in cases with minorcolumn defects treated by augments in either ‘wedge’ or‘flying buttress’ configuration, and only one of the 14 caseswith major column defects developed aseptic loosening.This is a better outcome compared with conventional meth-ods used to treat acetabular bone loss with the use of struc-tural bone allograft, where mid-term failure rates of around20% and 50% have been reported for minor and major col-umn allografting techniques respectively.15,16 The othertwo aseptic failures were in patients with pelvic discontinu-ity. No substantial distraction had been applied to the dis-continuity sites, and the authors concluded that using a TMcup and augment for treating pelvic discontinuity was notrecommended. However, studies from elsewhere showedpromising results regarding use of a TM cup with andwithout augment for pelvic discontinuity if applied with6 mm to 8 mm of distraction.17
Future perspectivesOur knowledge of augments and their proficiency in ace-tabular revision is limited by several factors. There is nolong term study yet available and what we have is mostlyon the use of conventional augments with no distinctionbeing made between the different configurations, and thereis very little data on results of restrictors and buttress aug-ments. Augment-cage and augment-cup-cage compositesalthough being used in some centres, have not been evalu-ated yet. Biomechanical studies will be of help to assess thestrength of cement in unifying the cup and augment, thepossibility of fatigue failure of augments under the com-pressive forces exerted by the adjacent cup, and the distinc-tive biomechanical features of different augment shapesand configurations.
Some concerns remain unresolved regarding the use ofporous augments. They do not restore bone stock and maycause even more bone loss if they have to be removed dur-ing revision surgery. The metal debris released at the time ofcreating new screw holes through the porous shells, orthose created by fretting between the augment and a loosecup might cause local and systemic adverse reactions. Con-sequently, we still tend to use bone allograft in youngpatients with high probability for another revision. How-ever, considering the versatility they offer to the surgeonand the favourable short- and mid-term outcomes reportedso far for TM augments, their use will become morefrequent in the immediate future until we know more abouttheir long-term performance.
No benefits in any form have been received or will be received from a commer-cial party related directly or indirectly to the subject of this article.

108 M. ABOLGHASEMIAN, S. TANGSATAPORN, A. STERNHEIM, D. J. BACKSTEIN, O. A. SAFIR, A. E. GROSS
CCJR SUPPLEMENT TO THE BONE & JOINT JOURNAL
This paper is based on a study which was presented at the 29th Annual Winter2012 Current Concepts in Joint Replacement® meeting held in Orlando, Florida,12th – 15th December.
References1. Park DK, Della Valle CJ, Quigley L, et al. Revision of the acetabular component
without cement. A concise follow-up, at twenty to twenty-four years, of a previousreport. J Bone Joint Surg [Am] 2009;91-A:350–355.
2. Ng VY. Risk of disease transmission with bone allograft. Orthopedics 2012;35:679–681.
3. Lee PT, Raz G, Safir OA, Backstein DJ, Gross AE. Long-term results for minor col-umn allografts in revision hip arthroplasty. Clin Orthop Relat Res 2010;468:3295–3303.
4. Bobyn JD, Stackpool GJ, Hacking SA, Tanzer M, Krygier JJ. Characteristics ofbone ingrowth and interface mechanics of a new porous tantalum biomaterial. J BoneJoint Surg [Br] 1999;81-B:907–914.
5. Saleh KJ, Holtzman J, Gafni ASaleh L, et al. Development, test reliability and val-idation of a classification for revision hip arthroplasty. J Orthop Res 2001;19:50–56.
6. Abolghasemian M, Tangsataporn S, Sternheim A, et al. Combined trabecularmetal acetabular shell and augment for acetabular revision with substantial boneloss: a mid-term review. Bone Joint J 2013;95-B:166–172.
7. Massin P, Duparc J. Total hip replacement in irradiated hips: a retrospective studyof 71 cases. J Bone Joint Surg [Br] 1995;77-B:847–852.
8. Sporer SM, Paprosky WG. Acetabular revision using a trabecular metal acetabularcomponent for severe acetabular bone loss associated with a pelvic discontinuity. JArthroplasty 2006;21(Suppl):87–90.
9. Borland WS, Bhattacharya R, Holland JP, Brewster NT. Use of porous trabec-ular metal augments with impaction bone grafting in management of acetabular boneloss. Acta Orthop 2012;83:347–352.
10. Nehme A, Lewallen DG, Hanssen AD. Modular porous metal augments for treat-ment of severe acetabular bone loss during revision hip arthroplasty. Clin OrthopRelat Res 2004;429:201–208.
11. Siegmeth A, Duncan CP, Masri BA, Kim WY, Garbuz DS. Modular tantalum aug-ments for acetabular defects in revision hip arthroplasty. Clin Orthop Relat Res2009;467:199–205.
12. Sporer SM, Paprosky WG. The use of a trabecular metal acetabular componentand trabecular metal augment for severe acetabular defects. J Arthroplasty2006;21(Suppl):83–86.
13. Del Gaizo DJ, Kancherla V, Sporer SM, Paprosky WG. Tantalum augments forPaprosky IIIA defects remain stable at midterm followup. Clin Orthop Relat Res2012;470:395–401.
14. Lingaraj K, Teo YH, Bergman N. The management of severe acetabular bonedefects in revision hip arthroplasty using modular porous metal components. J BoneJoint Surg [Br] 2009;91-B:1555–1560.
15. Woodgate IG, Saleh KJ, Jaroszynski G, et al. Minor column structural acetabularallografts in revision hip arthroplasty. Clin Orthop Relat Res 2000;371:75–85.
16. Kwong LM, Jasty M, Harris WH. High failure rate of bulk femoral head allograftsin total hip acetabular reconstructions at 10 years. J Arthroplasty 1993;8:341–346.
17. Sporer SM, Bottros JJ, Hulst JB, et al. Acetabular distraction: an alternative forsevere defects with chronic pelvic discontinuity? Clin Orthop Relat Res2012;470:3156–3163.