The Respiratory System History
25
description
The Respiratory System History. Dr. J.A. Coetser Department of Internal Medicine [email protected]. Presenting symptoms. Cough Sputum Haemoptysis Dyspnoea Wheeze Chest pain Fever Hoarseness Night sweats. SOCRATES. S ite O nset C haracter R adiation A lleviating factors - PowerPoint PPT Presentation
Transcript of The Respiratory System History

THE RESPIRATORY SYSTEM HISTORYDr. J.A. CoetserDepartment of Internal [email protected]
PRESENTING SYMPTOMS Cough Sputum Haemoptysis Dyspnoea Wheeze Chest pain Fever Hoarseness Night sweats

SOCRATES Site Onset Character Radiation Alleviating factors Timing Exacerbating factors Severity
COUGH Cough clears airways from secretions or
foreign bodies ONSET
Acute = e.g. bronchitis / pneumonia Chronic = e.g. asthma
CHARACTER Sound
Barking = croup Loud and brassy = compression of trachea Bovine (hollow) = recurrent laryngeal nerve palsy
Productive of sputum?

COUGH ALLEVIATING FACTORS
Asthma inhaler improves cough in asthma TIMING
Lying down = GERD or cardiac failure Coughing at work = occupational irritants Worse at night = asthma / cardiac failure Worse in morning = chronic bronchitis
EXACERBATING FACTORS Eating / drinking = incoordinate swallowing /
GERD / tracheo-oesophageal fistula SEVERITY
How does coughing influence daily functioning / work?
COUGH Associated symptoms with coughing:
Postnasal drip or sinus congestion = upper airway cough syndrome
Irritating dry cough = GERD / ACE-I / interstitial lung disease

SPUTUM Ask about type and amount Purulent (yellow or green) = pneumonia /
bronchiectasis Foul-smelling, dark-coloured = lung abscess Frothy pink = pulmonary oedema

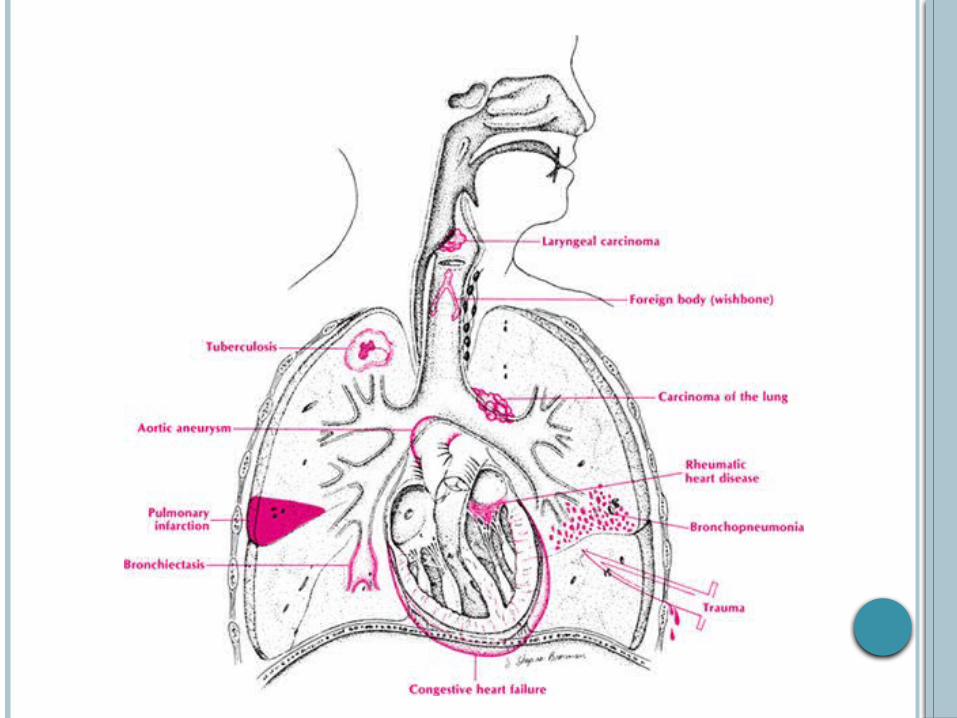
HAEMOPTYSIS Def: Coughing up of blood
Mild <20mL/24h Massive >250mL/24h
Must distinguish haemoptysis from: Haematemesis Nasopharyngeal bleeding
How much blood was produced? Spotting in sputum / cup / bucket?
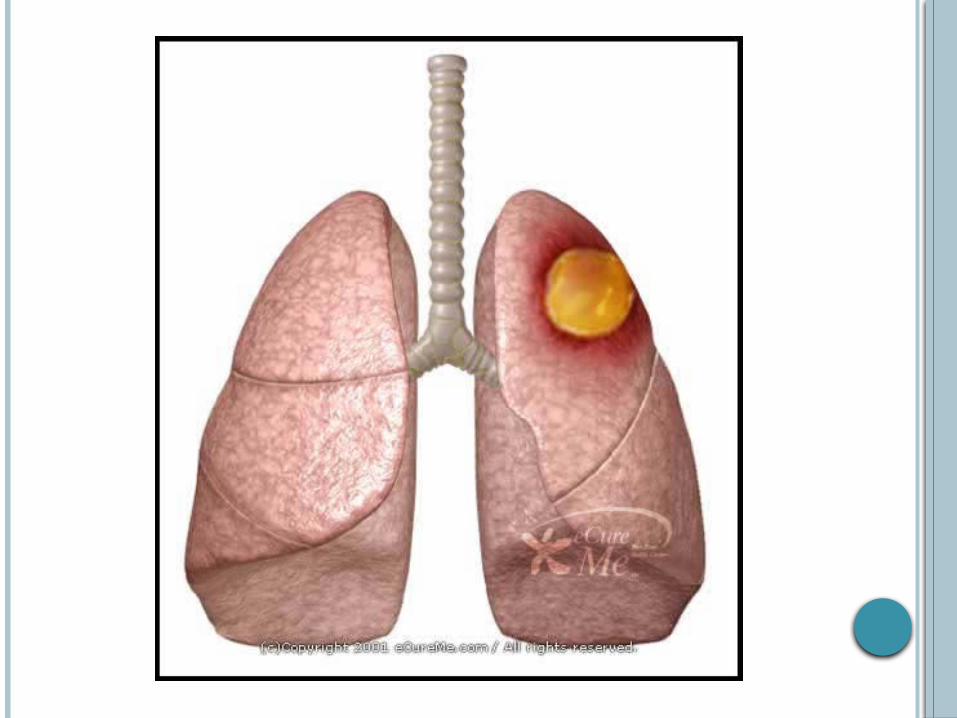
Most common causes: Carcinoma Tuberculosis Bronchiectasis

DYSPNOEA Def: an awareness of effort required to
breathe ONSET
Worsening slowly over weeks / months or years = interstitial lung disease
Rapid onset = acute infection / pulmonary embolism / pneumothorax
CLASSIFICATION Class I – disease present but no dyspnoea /
dyspnoea only with heavy exertion Class II – dyspnoea on moderate exertion Class III – dyspnoea on minimal exertion Class IV – dyspnoea at rest
WHEEZE Whistling noise coming from chest Usually maximal during expiration Causes
Asthma COPD Infections e.g. bronchiolitis Airway obstruction e.g. foreign body / tumor
Differentiate from stridor Loudest over trachea Occurs during inspiration


CHEST PAIN Pleura and airways have abundant pain fibre
innervation Sudden onset of pleuritic pain
Lobar pneumonia Pulmonary embolism and infarction Pneumothorax
OTHER PRESENTING SYMPTOMS Flu-like viral prodome preceding viral
pneumonia Fever at night
TB (also ask about night sweats) Pneumonia Lymphoma
Hoarseness (dysphonia) Laryngitis Vocal cord tumor Recurrent laryngeal nerve palsy
OTHER PRESENTING SYMPTOMS Sleep apnoea
Central = no respiratory effort for at least 10s Obstructive = respiratory effort present, but
airflow stops for at least 10s Typical presentation
Daytime somnolence Chronic fatigue Morning headaches Personality disturbances Loud snoring often present
Epworth sleepiness scale to quantify severity Hyperventilation
Often due to anxiety Development of alkalosis = parasthesiae, light-
headedness, chest pain
TREATMENT Chronic drugs taken by patient
Steroids (chronic lung disease, e.g. COPD, sarcoidosis)
Inhalers (COPD and asthma) Pulmonary side-effects of drugs
Oral contraceptives = pulmonary embolism Cytotoxic agents, e.g. MTX = interstitial lung
disease Beta-blockers = bronchospasm ACE-inhibitors = chronic dry coughing

PAST HISTORY Previous respiratory illness? Previous respiratory investigations?
Bronchoscopy Lung biopsy Spirometry

OCCUPATIONAL HISTORY Very, very important in the respiratory history Ask about the occupation
What patient does specifically at work Duration of exposure Use of protective devices Have other workers become ill?
Ask about exposure to Dusts in mines (e.g. asbestos, coal, silica) Industrial exposures (cotton, beryllium) Exposure to animals (psittacosis, Q-fever) Organic dusts, e.g. bird feathers, mould (allergic
alveolitis)
SOCIAL HISTORY Smoking history
Calculate the number of pack years How does the condition interfere with work,
daily activities and family life? Alcohol intake
Predisposes to pneumococcal and Klebsiella infections
IV drug users at risk for lung abscess

FAMILY HISTORY Family history of asthma, cystic fibrosis, lung
cancer or emphysema Family members infected by tuberculosis
THANK YOU!