The Reproductive Health Implications of Depression: Postpartum Depression Association of...
52
The Reproductive Health Implications of Depression: Postpartum Depression Association of Reproductive Health Professionals www.arhp.org
-
Upload
ashley-evans -
Category
Documents
-
view
218 -
download
2
Transcript of The Reproductive Health Implications of Depression: Postpartum Depression Association of...

The Reproductive Health Implications of Depression: Postpartum Depression
Association of Reproductive Health Professionalswww.arhp.org
Expert Medical Advisory Committee
• Norma Jo Waxman, MD• Ellen Haller, MD• Ann Hutton, PhD, APRN • Kathy Besinque, PharmD

?Polling Question A

Learning Objectives
At the end of this session participants should be able to:• Recognize symptoms, risk factors and
presentations of depression in women, including pre-menstrual and post partum mood disorders.
• Screen women for depression throughout their reproductive years
• Prescribe medications for depression in women and know when to refer

Postpartum Depression (PPD)
A sad story…• 35 year old man, named, Moki, is a
Japanese immigrant, and member of suicide survivors grief support group
• His wife committed suicide two months prior to starting group
• She was four months postpartum with third child; two older children 5 and 8 years old

D. 80% of women who are pregnant and have symptoms of depression remain untreated.
?Question 1

Significance of Postpartum Depression
• During postpartum period up to 85% of women experience some type of mood disturbance, usually transient, “baby blues.”
• Depression in postpartum period not distinct from major depressive disorders in general
B. Symptom resolution within several days to 2 weeks following birth.
?Question 2

“Baby Blues”
• Occurs in 70-85% of women• Onset within the first few days (4-5 days)
after delivery• Resolves by 2 weeks• Symptoms include: mild depression,
irritability, tearfulness, fatigue, anxiety• May have increased risk of post-partum
major depression later on
Beck CT. Am J Nurs. 2006. Hirst KP, Moutier CY. Am Fam Physician. 2010. Pearlstein T, et al.Am J Obstet Gynecol. 2009.
A. Up to 15% of women are estimated to be affected by postpartum depression.
?Question 3

Postpartum Depression
• Similar symptoms but longer duration and more severe than “baby blues”
• Affects 7% to 15% of women
• 0.1% to 2% have postpartum psychosis
Beck CT. Am J Nurs. 2006. Hirst KP, Moutier CY. Am Fam Physician. 2010. Pearlstein T, et al.Am J Obstet Gynecol. 2009.

Postpartum Depression
• Most frequent in first 4 months following birth
• Significant impact on both mother and child
• Under diagnosed, universal screening needed
Beck CT. Am J Nurs. 2006. Hirst KP, Moutier CY. Am Fam Physician. 2010. Pearlstein T, et al.Am J Obstet Gynecol. 2009.

C. Older age at first birth is not a factor associated with increased risk of postpartum depression.
?Question 4

Risk Factors for Depression: Pregnancy and Postpartum
• History of prior depressive episodes, family history of depression
• History of childhood abuse, neglect• Single parent; low SES• Absence of emotional, social support• Unplanned pregnancy• Domestic conflict, violence, abuse

• Susceptibility to hormonal changes, PMS, PMDD
• Recent loss, death, stressful life events• Any infant health problems (ex: colic)
Risk Factors for Depression: Pregnancy and Postpartum

Postpartum Mood Disorders
Prevalence Onset Duration Treatment
Blues 50-80% 1-5 days <2 weeks Reassurance
Depression 10%-15% 2wk - 1 year 3-14 moMedication or psychotherapy
Psychosis 0.1-0.2%2 days to 1
monthVariable
Medication, hospitalization
?Polling Question B

Screening for Depression
• Inquire about mood history before delivery• Alert patient to note mood changes on
continuum• Severity guides treatment• Tools for screening

Two Question Screen for Depression
During the past month, have you been bothered by little interest or pleasure in doing things?
During the past months, have you often been feeling down, depressed, or hopeless?
Arroll B. BMJ 2003.
Validated screening tool with 97% sensitivity, 67% specificity

Edinburgh Postnatal Depression Scale
British Journal of Psychiatry 150:782-786

Edinburgh Postnatal Depression Scale
• A 10-item screening tool• Woman self-reports how she has been
feeling during the previous week for a number of affect states
• Maximum score is 30• Possible depression score: ≥ 10• Includes item to assess risk of suicide
Cox JL et al. Br J Psychiatry. 1987. Hirst KP, Moulter CY. Am Fam Physician. 2010.
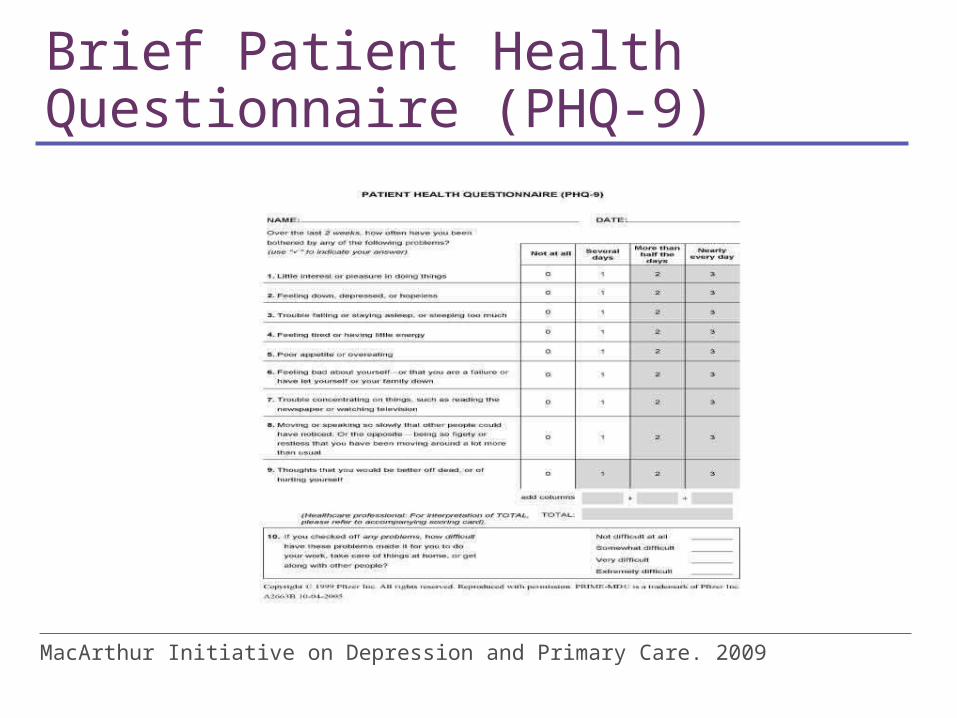
Brief Patient Health Questionnaire (PHQ-9)
MacArthur Initiative on Depression and Primary Care. 2009

PHQ-9
• 9 Questions based on DSM-IV criteria for major depression
• Scores between 10 and 27 = moderate to severe depression
• Used by CNMs to make referrals

Assessment of Suicide Risk
• Screen every patient suspected of depression
• Asking does not insult patient or initiate thought
• Ask direct questions: • "Have you had thoughts of hurting
yourself?" • "Do you sometimes wish your life was
over?"• "Have you had thoughts of ending your life?"
Hackley et al 2010. MacArthur Initiative on Depression and Primary Care. 2009

Assessment of Suicide Risk
• If yes, assess immediate risk:"Do you feel that way now?”"Do you have a plan?""Do you have the means to carry out your plan?”
• Contracting not to harm has not been shown to be a preventive strategy.
• Call 911 or the police, to have patient transported for evaluation (5150) if high risk
Hackley et al 2010. MacArthur Initiative on Depression and Primary Care. 2009

Common Symptoms of Postpartum Depression
Worry about the baby’s health, well-being and safety
Feelings of inadequacy or detachment from infant
Intrusive thoughts about harming the baby
Beck CT. Am J Nurs. 2006. Hirst KP, Moutier CY. Am Fam Physician. 2010. Pearlstein T, et al.Am J Obstet Gynecol. 2009.

Postpartum Depression with Atypical Features
• Common in young women with depression, Two of the following symptoms:• Hypersomnia• Either increased appetite or weight gain• Leaden paralysis• Interpersonal rejection sensitivity and
irritability

Comorbidities
• Anxiety Disorders• Eating Disorders• Substance related disorders• Personality Disorders:
▪ Avoidant▪ Borderline▪ Histrionic

C. Individual or group psychotherapy can effectively manage mild to moderate depression.
?Question 5

Postpartum Depression: Treatment
Beck CT. Am J Nurs. 2006. Dennis CL, Hodnett E. Cochrane Database Syst Rev. 2007.Hirst KP, Moutier CY. Am Fam Physician. 2010. Pearlstein T, et al. Am J Obstet Gynecol. 2009.
*Include the patient in decision-making
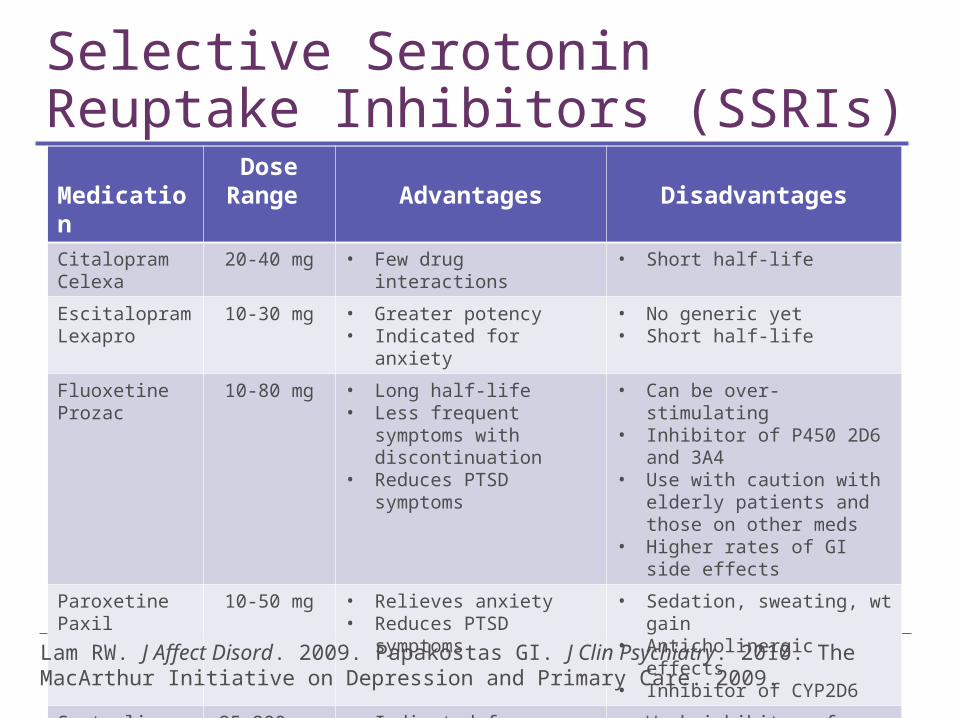
Selective Serotonin Reuptake Inhibitors (SSRIs)
MedicationDose
Range Advantages DisadvantagesCitalopramCelexa
20-40 mg • Few drug interactions • Short half-life
EscitalopramLexapro
10-30 mg • Greater potency• Indicated for anxiety
• No generic yet• Short half-life
FluoxetineProzac
10-80 mg • Long half-life• Less frequent symptoms
with discontinuation• Reduces PTSD symptoms
• Can be over-stimulating• Inhibitor of P450 2D6 and
3A4• Use with caution with elderly
patients and those on other meds
• Higher rates of GI side effects
ParoxetinePaxil
10-50 mg • Relieves anxiety• Reduces PTSD symptoms
• Sedation, sweating, wt gain• Anticholinergic effects• Inhibitor of CYP2D6
SertralineZoloft
25-200 mg • Indicated for anxiety disorders, PTSD
• Weak inhibitor of CYP2D6• Diarrhea
Lam RW. J Affect Disord. 2009. Papakostas GI. J Clin Psychiatry. 2010. The MacArthur Initiative on Depression and Primary Care. 2009.

Serotonin-Norepinephrine Reuptake Inhibitors (SNRIs)
MedicationDose
Range Advantages Disadvantages
Duloxetine Cymbalta
40-60 mg • Also indicated for GAD, diabetic neuropathy, fibromyalgia
• Nausea and vomiting• Sexual dysfunction
Venlafaxine Effexor and generic
75-375 mg
• Relieves anxiety disorders, neuropathic pain, and perimenopausal vasomotor symptoms
• Higher doses may increase risk of hypertension
• Drug interactions• Sexual dysfunction less common• Nausea and vomiting
DesvenlafaximePristiq
50-100 mg
• Relieves anxiety disorders, neuropathic pain, and vasomotor symptoms
• Can be started without titration at effective dose
• No generic
Lam RW. J Affect Disord. 2009. Papakostas GI. J Clin Psychiatry. 2010. The MacArthur Initiative on Depression and Primary Care. 2009.
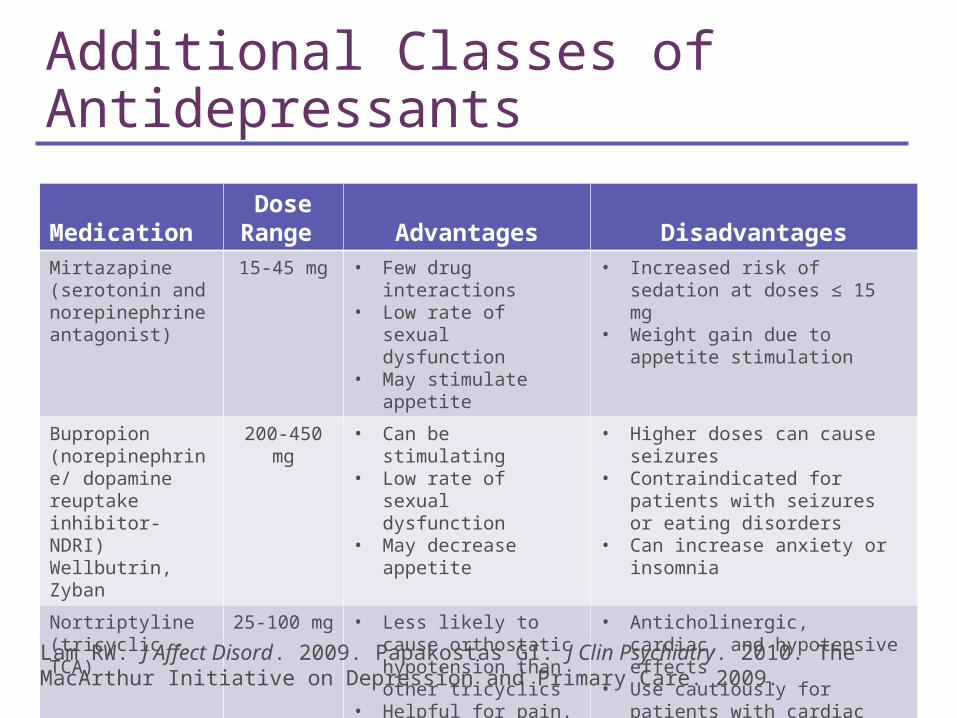
Additional Classes of Antidepressants
MedicationDose
Range Advantages DisadvantagesMirtazapine (serotonin and norepinephrine antagonist)
15-45 mg • Few drug interactions• Low rate of sexual
dysfunction• May stimulate appetite
• Increased risk of sedation at doses ≤ 15 mg
• Weight gain due to appetite stimulation
Bupropion (norepinephrine/ dopamine reuptake inhibitor- NDRI)Wellbutrin, Zyban
200-450 mg • Can be stimulating• Low rate of sexual
dysfunction • May decrease appetite
• Higher doses can cause seizures• Contraindicated for patients with
seizures or eating disorders• Can increase anxiety or insomnia
Nortriptyline (tricyclic - TCA)
25-100 mg • Less likely to cause orthostatic hypotension than other tricyclics
• Helpful for pain, migraine and insomnia
• Anticholinergic, cardiac, and hypotensive effects
• Use cautiously for patients with cardiac conduction disorder
Lam RW. J Affect Disord. 2009. Papakostas GI. J Clin Psychiatry. 2010. The MacArthur Initiative on Depression and Primary Care. 2009.

Safety Of Drugs: Lactation• All antidepressants found in breast milk
Limited data on newborn impact No findings of effect on growth or development
• Milk-to-plasma ratio of meds in breast milk varies, but usually < 0.1, decreasing concern about harm
• Sertraline, then Paroxetine, then Nortriptyline recommended for the least relative infant dose and the most studied
• Avoid Fluoxetine (Prozac) due to long half life- and increased accumulation in the infant
Lanza di Scalea. 2009.
Safety of SSRIs
• May delay developmental milestones• Cost-benefit of SSRIs during pregnancy and
postpartum• GlaxoSmithKline paid $2.5 million to settle
lawsuit relating to Paxil (paroxetine) that included birth defects.

SSRIs in Treatment • Use of standard dosages• Start with low dosage and check for response
▪ Ex: Zoloft (sertraline) 50 mg• Some women are rapid responders, others 2 to
4 weeks, but full remission may take several months, and dose may need to be increased
• May need additional meds for anxiety and sleep

SSRIs in Treatment
• Remain on SSRI 6 to 12 months to avoid relapse
• Monitoring and tracking with mood diary• Refer for evaluation to mental health provider
for complex cases, comorbid conditions, or failure to achieve remission

Complementary and Alternative Medicine Therapy for Depression• Commonly used and often not revealed• St. John’s Wort for mild-moderate depression
▪ Studies conflicting▪ Drug-drug interactions including hormonal
contraception, SSRIs and Coumadin▪ Most guidelines discourage use
• Exercise and mindfulness based stress reduction• Light therapy for seasonal affective disorder• No benefit in RCTs
▪ Accupuncture and Omega-3 fatty acids
Ravindran AV, et al. J Affect Disord. 2009. Cochrane Review, 2009. Freeman, M P et al. 2010. Complementary and alternative medicine in MDD: APA Task Force Report. J Clin Psy 2010.

Psychotherapy• Psychotherapy is important part of treatment for
women who have past history of depression, developmental abuse, marital conflict, lack of support, or comorbid mental health conditions
• Cognitive Behavior Therapy (CBT), Interpersonal Therapy (IPT) and Psychodynamic Therapy are all effective and may be cost-effective in improving long term outcomes

Joan
• 34 yo, 3 weeks postpartum• Moody, irritable, exhausted• Seems disconnected from her baby• Tearful and difficult to focus during the
visit• Having a hard time caring for the baby and gave up
nursing, feels very guilty • No local family support, partner works “all the time”• Prior history of depression• Emergency C-section

Joan
• Treatment:▪ Sertraline 50 mg increased to 100 mg▪ Individual psychotherapy▪ Encourage mothers club involvement
• Follow Up: ▪ Sertraline reduced irritability, stabilized mood▪ Therapy promoted insight ▪ Meeting other new moms gave her support and
outside of the house activities
D. All of the above care consequences of depression during pregnancy which can affect the infant.
?Question 6

Treat Prophylactically for Additional Pregnancies
• Increased likelihood of PPD after first episode of depression
• Case example: ▪ first pregnancy, possible “baby blues”; ▪ second pregnancy, psychotic depression,
hallucinated; ▪ third pregnancy covered with Zoloft prior to
delivery
Hormones and CNS
• Effect of estrogen and progesterone on affective states are probably not linear or dose-dependent
• Estrogen and progesterone modulate each others effects on CNS and that complicates understanding of their individual effects
Hormones and the Gender Difference
• Gender difference emerges at puberty• Some women more vulnerable, sensitive to
estrogen precipitous change from birth to 48 hours• Women more likely than men to become depressed
in response to stressful events• Sleep deprivation with motherhood may play a role• Need for further studies of treatment with
transdermal estradiol in treatment of PPD

Neuroimaging Studies of Women with PPD
• Dorsomedial prefrontal cortex less active in women with PPD than healthy new mothers
• DMPFC involved in voluntary and automatic control and reappraisal of emotional responses in social cognition (interpret emotional responses of others)
• Diminished HPA Axis drive DMPC connectivity with amygdala
Am J Psych, Sept. 2010
“SHAPED BY LIFE IN THE WOMB”
Comment on Perinatal Depression• Babies with mothers with untreated depression
(Perinatal) show neurobehavioral changes, born at earlier gestational age, and have elevated stress hormones
• Epigenetic changes and neurobiological models of emotion-behavior regulation are implicated; attention regulation capacities that call on brain stem and limbic system networks

Improved Outcome with Integrated Care
• Integrating primary care with mental health services has shown to improve overall medical care and reduces costs
• Collaborate with Certified Nurse Midwives and others who refer patients with depression and other mental health diagnoses
• Screen using the Patient Health Questionnaire (PHQ-9)

Provider Resources
• MacArthur Initiative on Depression in Primary Care▪ http://www.depression-primarycare.org/
• American Psychiatric Association▪ http://www.healthyminds.org/
• Cox, J.L., Holden, J.M., and Sagovsky, R. 1987. Detection of postnatal depression: Development of the 10-item Edinburgh Postnatal Depression Scale.

Provider and Patient Resources
• National Institute of Mental Health▪ http://
www.nimh.nih.gov/health/publications/women-and-depression-discovering-hope/index.shtml
• WomensHealth.gov• http://www.womenshealth.gov/faq/depression-
pregnancy.cfm• Mayo Clinic
• http://www.mayoclinic.com/health/depression/MH00035

Provider and Patient Resources
• Healthy Place▪ http://www.healthyplace.com/depression/women/
depression-in-women/menu-id-68/. • Massachusetts General Hospital Center for
Women’s Mental Health▪ http://www.womensmentalhealth.org/.