The Renal Clearance of Amino Acids in...mine treatment), when the endogenous creatinine clear-ance...
11
The Renal Clearance of Amino Acids in Cystinuria J. C. Crawhall, … , C. J. Thompson, R. W. E. Watts J Clin Invest. 1967; 46(7):1162-1171. https://doi.org/10.1172/JCI105609. The renal clearance of cystine, lysine, ornithine, arginine, and glycine has been compared with the simultaneously determined glomerular filtration rate in nine cystinuric patients. Five were studied before and after stabilization on penicillamine therapy, two were studied only while taking penicillamine, and two were studied only in the absence of penicillamine administration. The renal clearances of cysteine-penicillamine and of penicillamine disulfide were also determined in the patients who were taking the drug. Amino acids were determined by quantitative ion exchange chromatography, and the reliability of the method has been evaluated in terms of its reproducibility and of the recovery of known amounts of amino acids added to plasma and to urine. The plasma levels of cystine and of the basic amino acids were less than normal in all the patients. Cysteine- penicillamine and penicillamine disulfide were cleared by the kidney at rates similar to that of cystine. Two of the patients had glycine clearances that were considerably above the normal value. The renal clearance of cystine exceeded the glomerular filtration rate in six of the nine patients. The results form a continuum from values approximately equal to the glomerular filtration rate to values about twice this amount. The renal clearances of cystine and of the basic amino acids vary independently of one another in the disease. The significance of these results […] Research Article Find the latest version: http://jci.me/105609/pdf Pdf
Transcript of The Renal Clearance of Amino Acids in...mine treatment), when the endogenous creatinine clear-ance...

The Renal Clearance of Amino Acids inCystinuria
J. C. Crawhall, … , C. J. Thompson, R. W. E. Watts
J Clin Invest. 1967;46(7):1162-1171. https://doi.org/10.1172/JCI105609.
The renal clearance of cystine, lysine, ornithine, arginine, and glycine has been comparedwith the simultaneously determined glomerular filtration rate in nine cystinuric patients. Fivewere studied before and after stabilization on penicillamine therapy, two were studied onlywhile taking penicillamine, and two were studied only in the absence of penicillamineadministration. The renal clearances of cysteine-penicillamine and of penicillaminedisulfide were also determined in the patients who were taking the drug.
Amino acids were determined by quantitative ion exchange chromatography, and thereliability of the method has been evaluated in terms of its reproducibility and of the recoveryof known amounts of amino acids added to plasma and to urine. The plasma levels ofcystine and of the basic amino acids were less than normal in all the patients. Cysteine-penicillamine and penicillamine disulfide were cleared by the kidney at rates similar to thatof cystine. Two of the patients had glycine clearances that were considerably above thenormal value. The renal clearance of cystine exceeded the glomerular filtration rate in six ofthe nine patients. The results form a continuum from values approximately equal to theglomerular filtration rate to values about twice this amount. The renal clearances of cystineand of the basic amino acids vary independently of one another in the disease.
The significance of these results […]
Research Article
Find the latest version:
http://jci.me/105609/pdf

Journal of Clinical InvestigationVol. 46, No. 7, 1967
The Renal Clearance of Amino Acids in Cystinuria *J. C. CRAWHALL,E. F. SCOWEN,C. J. THOMPSON,ANDR. W. E. WATTSt
(From the Medical Professorial Unit, [Dunn Laboratories], St. Bartholomew's Hospital,London, E.C.1., England)
Summary. The renal clearance of cystine, lysine, ornithine, arginine, andglycine has been compared with the simultaneously determined glomerularfiltration rate in nine cystinuric patients. Five were studied before and afterstabilization on penicillamine therapy, two were studied only while takingpenicillamine, and two were studied only in the absence of penicillamine ad-ministration. The renal clearances of cysteine-penicillamine and of penicil-lamine disulfide were also determined in the patients who were taking thedrug.
Amino acids were determined by quantitative ion exchange chromatog-raphy, and the reliability of the method has been evaluated in terms of itsreproducibility and of the recovery of known amounts of amino acids addedto plasma and to urine. The plasma levels of cystine and of the basic aminoacids were less than normal in all the patients. Cysteine-penicillamine andpenicillamine disulfide were cleared by the kidney at rates similar to that ofcystine. Two of the patients had glycine clearances that were considerablyabove the normal value. The renal clearance of cystine exceeded the glomeru-lar filtration rate in six of the nine patients. The results form a continuumfrom values approximately equal to the glomerular filtration rate to valuesabout twice this amount. The renal clearances of cystine and of the basicamino acids vary independently of one another in the disease.
The significance of these results is discussed in terms of the nature of therenal tubular transport defect that underlies the disorder.
Introduction
During our investigations of the action of D(-) -penicillamine 1 in the treatment of cystinuria (1, 2)we have measured plasma and urinary amino acidsbefore and during therapy with this drug. Dent,Senior, and Walshe (3) reported that the renalclearance of cystine was close to the glomerularfiltration rate (GFR) in the disease; this wasconfirmed in three out of four patients studied byArrow and Westall (4) and in three of the fourpatients studied by Frimpter and associates (5).Dent and Senior (6), Arrow and Westall (4), and
* Submitted for publication October 17, 1966; acceptedMarch 21, 1967.
t Address requests for reprints to Dr. R. W. E. Watts,Dunn Laboratories, St. Bartholomew's Hospital, London,E.C.1., England.
1 D(-)-penicillamine will be subsequently referred toas penicillamine.
Frimpter and co-workers (5) each have also re-ported single patients in whom the clearance ofcystine was significantly greater than the glomeru-lar filtration rate. Glycine excretion has also beenreported to be increased in cystinuria (5).
In this paper we present cystine, lysine, orni-thine, arginine, and glycine clearance data of ninepatients with cystinuria, in six of whom the renalclearance of cystine was greater than GFR. Theeffect of penicillamine therapy on the blood andurinary concentrations and on the renal clearancesof these amino acids and of cysteine-penicillamineand penicillamine disulfide is also reported. Someof these results have been the subject of a prelimi-nary communication (7).
MethodsDetermination of the renal clearances of the amino
acids and simultaneous measurement of GFR. The amino
1162

RENAL CLEARANCEOF AMINO ACIDS IN CYSTINURIA
TABLE I
Reproducibility of the amino acid determination*
Reproducibility (n comparisons)
Aqueous solution Urinet PlasmajAmino acid Mean SD n Mean SD n Mean SD n
Cystine 100.0 2.72 12 102.2 6.69 6 101.9 8.11 21Ornithine 100.4 2.56 12 98.6 3.69 6 104.3 8.58 21Lysine 99.6 1.79 12 102.0 6.80 6 100.5 6.94 21Arginine 101.3 1.81 12 101.7 6.09 6 99.9 7.66 21Glycine 104.1 6.50 11 101.4 4.16 6 102.6 6.66 21
* In the case of aqueous amino acid solutions, a volume (1.0 ml) of the standard amino acid solution, which contained0.1 pmole of each amino acid, was analyzed and the mean value obtained expressed as a percentage of this. In the case ofurine and plasma, each sample was analyzed twice, the value of 100% was arbitrarily assigned to the result of the firstdetermination, the result of the second analysis was expressed as a percentage of this, and the standard deviation of the(n) individual comparisons for each amino acid about the corresponding mean was calculated.
t Cystinuric.t Normal.
acid clearances and GFR were measured simultaneously,the renal clearance of inulin being used to measure GFRin all but one study (Patient 1, study before penicilla-mine treatment), when the endogenous creatinine clear-ance was employed. The patients were encouraged todrink water freely during the 9 hours before the test;they were otherwise fasting, and penicillamine was with-held for 12 hours before the investigation. The amountsof inulin infused and the timing of the blood and urinecollections were the following: 1) (Patients 1, 4, and 5).The loading infusion of inulin (4 g dissolved in 500 ml0.9% NaCl solution) was given over the course of 30minutes and followed by a maintenance infusion (2 g inu-lin per 500 ml 0.9%b NaCl solution) at a rate of 2 mlper minute for the rest of the study. Timed 30-minuteurine collection periods (without catheterization) werebegun 30 minutes after the start of the maintenance in-fusion. Blood samples were obtained immediately be-fore the study and at the midpoint of each clearanceperiod.
2) (Patients 2, 3, 6, 7, 8, and 9). The loading dose of
TABLE II
The recovery of amino acids added to urine and plasma*
Recovery
Urinet Plasmat
Glycine 99.5 (10.5)§ 96.3 (15.6)§Cystine 96.1 ( 4.1) 100.6 ( 9.8)Ornithine 107.0 ( 4.9) 98.7 (11.0)Lysine 99.5 (10.1) 111.7 (21.1)Arginine 99.3 ( 5.3) 100.3 (11.4)
* A known amount (0.1 Mmole) of each amino acid(1.0 ml) of the standard mixture of amino acids in 0.1N HCl was added to each specimen of urine and plas ma.An equal volume of 0.1 N HCI was added to the controlsamples.
t Cystinuric, 16 determinations.I Normal, 28 determinations.§ Standard deviation.
inulin (45 mg per kg body weight dissolved in 200 ml0.9%o NaCl) was infused over the course of approxi-mately 20 minutes and was followed by a maintenance in-fusion (25 mg inulin per minute per 100 ml approximateGFR, which had been previously determined on thebasis of the 24-hour endogenous creatinine clearance).The urine collection periods were timed to the end ofmicturition and were begun not less than 30 minutesafter the maintenance infusion was begun. Each urinecollection period lasted approximately 15 minutes. Bloodsamples were obtained at recorded times immediately be-fore the study, at the beginning of the first clearance pe-riod, in the middle of the second and third clearance pe-riods, and immediately after the third clearance period.The plasma inulin concentrations were plotted againsttime, and the concentration at the midpoint of eachclearance period was determined by interpolation. Weintroduced this modification of the clearance techniqueto improve the design of the procedure, not because thefirst method gave unsatisfactory clearance data.
Preparation of blood samples for analysis. Blood wasdrawn from an antecubital vein with a heparinized sy-ringe and immediately centrifuged at approximately 50 Cto separate the erythrocytes. Plasma (2.5 ml) was re-moved, a known amount of norleucine (0.1 /Amole, 0.1 mlsolution) was added as an internal standard, and theprotein was precipitated with salicylsulfonic acid (2.5ml). The precipitate was removed by centrifugation andwashed. The combined supernatants were evaporated todryness in a rotary evaporator at 400 C.
Analytical methods. Amino acids were determinedas described by Crawhall, Thompson, and Bradley (8)with a Technicon amino acid analyzer. The standardamino acid mixtures for calibrating the instrument werealso obtained from Technicon Co.2 Cysteine-penicillamineand penicillamine disulfide were prepared as describedpreviously (2). DL-Ornithine and DL-norleucine were
2Technicon Instruments Co., Ltd., Hanworth Lane,Chertsey, Surrey, England.
1163

CRAWHALL, SCOWEN,THOMPSON,ANDWATTS
00Um1-0 00ot) co U)O ooU)enr O0 0\m Cl4 " 0 to U)t-4 0 VU)oo e \o C140w ,0 -o +6o6 v6 o6 4 o6_ \_.6\6 r-\6 odt-\6 66o6 uio6ci %6t; \\1-4-4.4 1- -4 --ICl4 r- Cl4 1- -4 1- 1- - -4 - -
d4Cl Oc, r-. m0 U-) V' t0-I)V0 CO400
.Iq )-4 ClCl Clcl Cl1)In m uiu)) cll enen encq -.4 1-
00 M 0 00 U-
o 4U) U)U)
00 00 \VT- Cl400C%4 6 4 vzt-Cl Cl - - - Cl4
Cl4 CNC14 r-Cl6 4-
. .dI-4 toOr
C1
0 4~4 4--Clq
'I ClCl r
Cl4 00
U) 0%0% 4
*~4
in *+_N t
00 0%
-4---
0%0004--
- ClU') U)
Cli 4--LO en
W)
1.4 000
oo
C\00o6 .o
Cl 00U) U)
Cl4tt 00
o ClW.) ~4 14
00 U)C1
.4 00 rtVO -4 V-
to)r 00 -1r-I 6-.14
1it.Z C 0
V V
mm
U)
o-t m
U) 00
i o!
-0%_4 U)
-066
0 Cl00 %
66
U)0 -ON4 00t-
C; ..
--I -
Cl0 0
6f cli cN
t--0%%
.4l
- - Cl - Cl
NV .'40 0U) U-)ci 400 eU~4 -;t) Ul) Ul) V1 U) Ul)
-to -o\ rCoz-
-) Wu) CI C! It
6 o6 4 uo U)0\0 00%0~ 44-lt to-- 4
00r Cl
14 xl
Coo
~' 0t--000% -4-
en
00oV-
- C4 00
14 C4 -"
U)~U) Cli00 C4Cl4 Cl4 Cl
O 1
%0 0 00
00 \0 C,I" .
U) U) V
U) U66. i
d' U) VoU) C U
U)000
-ClU
0
..-
I_ I
-4--
Cli Cli
m I-
Cli Cli
- 4-
.. O
0 O
U) U)
C Cl
Cl 11
-- 0%
-00
- _
m t-
00
Cl4
1- Cl4
04--0%
004Dl4--t
U) V 00
00VV0 ON
%.0
Ul) 04--
Cl4 Cl Cl4
v-q Cl U
O
00-
Cls
0 Cl4 0-ON4.- 4--- 4- oCl U)cl "fi
o t)V U)o6%6
C Cl
-. -
Cl -
00
eq00
- -
000%*
-Cl
00
U) 4--00oo e- ve; c oo_o00 00 C4
O O~c
0C d4COO
* I.'. C1. t.OVU) coo
-- -t--
00 00\
O 0C
0l00Cl -
C .-.-004-- 4c
0 U)
U -
oo r
U) -
6soo
00 (Ds
o 5
.i Cl
-4 --4-0
- Cl U
0%o
0o
Cl4 'I 00U) 0% Vo
U) 4- 0%
U) U) Cl
U)q-0%
e#c66
U)4 -4
.- 6
to U)
~4 ~4
o oU)
0 0
U) Cl-+-00 It
Ue eU)
U)
-0
- Cl U)
0
0s
00rN
V 01-
~0E
-c
0 cl4- VVUV'in"-4 .4
c~i ci 6 %4e) o66 6
EC0C.)
0
d
Cd._
0)
04
r.
E
Cd
1164
14
*V.4
*4 1
4.4
*V4.4
-4
.* 0;
4)
o t
4.4
.44
_4.
1.t
0.4
0
0..
.. -0
U c
0
p4--
~.4)
=
. -
o440
0>.04
U -_- .
~oCl
ClCl
41-4
0 Ul)ZZ Cl*
0
N
1-
4-)
btJ4)
CQ
0
L.
0
0
04)0.
0
-C404)
"1
C'-
cd:
_
..a
cd4j)4
* ---* 4-

RENAL CLEARANCEOF AMINO ACIDS IN CYSTINURIA
'- en rawt- \C \0 \0t- 00 (1
. . * . * . . . ." *! .~_t C1 e- e4 --I _ e menot- 00 m
\-4 e- r;\ 6O'40eC~ -4 l
enX) 0%uie'me mc 0e 00n
o6w omo e5o m-ooi6 . . .~ .:: . .4 t. .6
'xICVo '4+4utLn CN-4 ,t
40- -_4 -s-- -
I-00 -00000 00 to 000ACi1;- l C-i e's!~
0% m1-4 - U)41).,J%0-4--el-
Ct Ns a,0 )O00o-4441) u) of ou0--- - - _q ci
t-Zo U)6M- CO- _ Min_l4 _4 C C4 C4 C1 C1 Cq C4 e C14 N
d4me 00r-%0 It 01%0 0X00
%0%0 0 -4 "tCi00 t-o 0O%4-0
--o Uote NU n
--_
---_ _ _ e e
_.eI 14- I 4-___ _ -4 V_4_1
u%%0to merge000% C)OoCo .14 r- 0oow 0 tpoQn"'iC' . SC'iC'i de4 ed
o0 U) 00 en d
00 m c-
0pro Odes~3t u0000
C500 C;Cs1 C;L _s 1-4 11. rag lo c
S~~~~~~~~~~L t-..oo~~m i~% -4 0%'-44- 00 r-r3.0% 1-l1)%0 00 4 O 4 .6 4 X- -4 -- -- _-4
-4C1 v- Cl M C, M .d C4 M
0U)
0o 0C
a- 00 CIA
obtained commercially.3 The reproducibility of thismethod was tested for aqueous amino acid solutions,urine, and plasma (Table I). The recoveries of knownamounts of the amino acids for which we report ana-lytical data are shown in Table II.
Creatinine and inulin were estimated by the methodsof Edwards and Whyte (9) and Schreiner (10), re-spectively.
Patients. The clinical states of the patients are sum-marized in the Appendix. They were hospitalized for theseinvestigations. Patients 2, 3, 6, 7, and 9 ate a repetitivediet for at least 6 days before the studies; Patients 1, 4,and 8 ate an unrestricted diet.
Results
The concentrations of glycine, cystine, lysine,ornithine, and arginine in plasma and urine of thenine patients during the clearance periods are pre-sented in Table III. Clearance measurementswere not made on Patients 3 and 7 before penicil-lamine therapy was begun or on Patients 8 and 9while they were on penicillamine treatment. Pa-tient 4 was studied twice before and twice whiletaking penicillamine. The fasting plasma cystineconcentrations agree with the values obtained inthis disease by previous investigators (4, 5, 11),and penicillamine treatment reduced it by morethan half in all cases. The concentrations of cys-teine-penicillamine sometimes exceeded the con-centrations of cystine, and the concentrations ofpenicillamine disulfide were considerably lowerthan those of the other disulfides. The precisionof the penicillamine disulfide analysis is, therefore,less than that of the other amino acids. The con-centrations of lysine and arginine in the- plasmaagree with the data of Frimpter (5, 12), beingrather lower than earlier reported values in nor-mal subjects (11, 12). The concentration of orni-thine is more variable among different patientsand within the normal range (2.95 to 10.6 jMmoleper 100 ml) (13) in some of the studies. Penicil-lamine administration did not alter the plasma con-centrations of the basic amino acids.
The amino acid clearances and the simultane-ously determined GFR are shown in Table IV.The ratio of cystine clearance (Ccystine) to GFRwas unaltered by penicillamine administration (Pa-tients 1, 2, 4, 5, and 6), and varies between aboutone and two. In six of the nine patients the cys-
3 Hopkin and Williams, Ltd., Chadwell Heath, Essex,England.
1165
00 "
cli e13
'In
X~of o60
r0-
a4-
VQ*z =
A
.
10. 5cd0
4).EId
ax
J.
cd0
4)E
4)
uy = v)
od-ie
UZ ..'I ...0
r
o - ui
" ci ciX'"' '1o:k
.-4)be rL. ._
a-
Q 44
0404
Cd S.°
U
.~4
*
04cio
Cd
Xo
N 0S1bn

CRAWHALL,SCOWEN,THOMPSON,ANDWATTS
O00 0 000
CI ) U) Cl C'-O C m
c o c) ClN
O0 'I O --I
C., m md 0
0 ; C6 C;6
cqO 00 00O'- ONOO~~sU: mS~s+
U) Oc No N r
00 0 400
O NO o O0Cs
U)0
-s U) lo
o
0
00~ ~ ~~
C-
00C1
U) Ul)0-4 -4-
00Cl) No U)
U-0 into00% r- t-_0
66
00%
08oO
_
0%00 +4+NOU) to
00 00
4u) e 4u)
C 65
00 00
U). .
0NO\0
O) mCl
O O
U)00
ClC
_
10 0O6 6
00 C1NO O0
U'- Cl4O O
o6 o:NO
0
00 et6
NO NO
(-)
000%4 --
0
00 C4 t'-oocl Cl_4 _ . -
oo Cm 00
Cl00 00
0%- -es
00 00 0
\0 rO O'
1166
0%00
.O O
.4 00
66;
66
Cl
00
00
90-\
00%
-(. C-0
00
W.
>b4
To
U
0
dd
¢~ e
CdU
~._
._
O
U
tC
._
10U8
U)td UW
0%C5
U'-
U-to
r-
VU)
0
0
C14 U)
_l
NO O
00 Ch
4)
4)J
= C
._
(U
U)
'0(n .
o>+
4)4)-= U
U..
0cn
'0
Wd
oC
4-)0.4)
t4)
cd4
48)
2 bOCd
7~-0
r. U
o0 E
'0-
CdCd W
>
(U 0'a._
'n Encd
'U
4)
(U >
C13
8 0
CXJ rL.
cro
Q

RENAL CLEARANCEOF AMINO ACIDS IN CYSTINURIA
1.3
1.1
1.01
0.91
0.8
p0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1.0 1.1 1.2 1.3 1.4 1.5CARGININE
G.F.R.
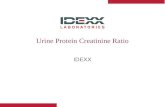
FIG. 1. RELATIONSHIP BETWEENTHE RATIOS Clyuine/GFR AND Carginlne/GFR. The regression line was cal-culated by the method of averages (the value enclosedin brackets was omitted from the calculation). The starindicates two identical values. C =clearance; GFR=glomerular filtration rate.
tine clearance is greater than the glomerularfiltration rate. In general, the clearance of cys-
teine-penicillamine tends to parallel the cystineclearance, but the clearances of the basic aminoacids do not necessarily parallel the clearances ofcystine. The present values for the ratio Carginine/GFRrange from 0.33 to 1.13 except for Patient 9,in whom this value was 0.051. The ranges of theratios Clysine/GFR and Cornithine/GFR are 0.44 to0.78 and 0.36 to 0.59, respectively. Patient 9 is ofspecial interest because her high cystine clearance(Ccystine/GFR = 1.47) is associated with smallerincreases in the basic amino acid clearances thanin the other patients, this being particularlymarked for arginine (Carginsne/GFR = 0.05, Clysine/GFR= 0.30, Cornithine/GFR = 0.14).
When the clearance ratios Cargiiine/GFR andCline/GFR are compared graphically (Figure 1),the results for Patient 9 lie on the line describingthe results for the other patients.
Discussion
Accuracy of the method of amino acid analysis.Ion exchange chromatography with automatedmethods of determining the amino acids in the col-umn effluent has been widely applied to the analy-sis of blood and urine. Its reliability for thedetermination of amino acids in aqueous solutions
and in protein hydrolyzates is well documented,but there have been few detailed investigations ofits validity when applied to biological fluids,which often present a more complicated analyticalproblem. Preliminary experiments confirmedthat the reproducibility of the present method(Table I) when applied to aqueous solutions wassatisfactory, the standard deviations of the indi-vidual values about their mean (expressed as100%o) being 2.72% or less for cystine and thebasic amino acids. Similar values are reported bySpackman, Stein, and Moore (14) and Dickin-son, Rosenblum, and Hamilton (13). We haveno explanation for the larger standard deviationthat we observed for glycine. The results obtainedwith urine and plasma showed a wider spread ofvalues about the corresponding means, lysine andornithine having the largest standard deviations inurine and plasma, respectively. This could havebeen due to small amounts of interfering sub-stances that behaved inconsistently on the ionexchange column. Average recoveries within 5%of the theoretical results were obtained for glycine,cystine, lysine, and arginine in urine and for gly-cine, cystine, ornithine, and arginine in plasma.The recovery of ornithine from urine and of. ly-sine from plasma was usually high, suggesting inthis case also that there was interference by an-other Ninhydrin-reacting compound, which wasnot being separated from the amino acid con-cerned; this was tryptophan in the case of plasmalysine. Urine contains no tryptophan, so that thiseffect is not observed when it is analyzed. Therange of values for the recovery data is wider forplasma than for urine, possibly due to the forma-tion of small and variable amounts of low molecu-lar weight substances during the deproteinizationprocedure, loss of free amino acids by absorptiononto the denatured protein precipitate, or both.Cystine is known to be absorbed onto plasma pro-teins before precipitation (13), but loss due tothis can be minimized by precipitating the plasmaproteins within 15 minutes of drawing the blood,as was done in the present studies. Salicylsulfonicacid is a convenient protein precipitant because itdoes not have to be removed before the protein-free supernatant is applied to the column of ionexchange resin. Dickinson and associates (13)concluded that it was at least as satisfactory as anyof the other methods that they studied; however,
[]
0 0
PATIE0*
O- PATIENT 9
1167

CRAWHALL, SCOWEN,THOMPSON,ANDWATTS
Gerritsen, Rehberg, and Waisman (15) thinkthat it leads to significant loss of some amino acidsas compared with ultrafiltration. The cystinedeterminations on both urine and plasma wereamong the most satisfactory from the point of viewof recovery and reproducibility (Tables I and II);the possible discrepancies that we have enumeratedwould not explain the relatively large differencesbetween, for example, cystine clearance and glo-merular filtration rate that we report.
Significance of Ccy8tjne/Cjwui,& greater than 1.While investigating the renal amino acid clear-ance of nine patients with cystinuria, we have en-countered six patients in whom the renal clear-ance of cystine was greater than the GFR. Onlyone of these was of a magnitude comparable to thepatient reported by Frimpter and associates (5),and the others appear to represent a continuousrange from clearances equal to the GFR to clear-ances twice the GFR. No attempt was made inthe present work to fractionate cysteine from cys-tine. However, the former amino acid cannot bedetected in urine, so that even if it is assumed thatall the plasma cysteine was oxidized to cystine dur-ing the preparation and analysis of the plasmasamples, the resulting error would reduce and notincrease the ratio Ccystine/GFR.
It has been suggested (4, 6) that the occurrenceof cystine clearances that are greater than theglomerular filtration rate in cystinuria could bedue to cystine being dissolved from calculi, andthat this would be particularly likely to occur dur-ing a diuresis. Further studies of cystinuric stone-forming patients have shown that a consistent in-crease in the cystine excretion occurred only in oneout of six patients during a diuresis of comparablemagnitude to that achieved in the present studies(16). The rates of urine flow and the urinarycystine concentrations vary during some of theclearance studies (e.g., study 2 on Patient 4, Ta-ble III) without a corresponding change in thecystine clearance or in the glomerular filtrationrate (Table IV), and this supports the view thatthe occurrence of Ccytine/GFR ratios greater thanunity cannot be explained by particularly highrates of urine flow during part of the investigation.In addition, we do not think that stone dissolutionexplains the cystine clearance values that exceededthe glomerular filtration rate in the present work
because some of the patients (1, 2, 6, 7, and 8) didnot have radiologically demonstrable calculi.
Frimpter and co-workers (5) have discussedthe significance of bidirectional flow of amino acidsacross the tubule cell as a possible mechanism toaccount for cystine clearances greater than GFRin cystinuria. Transport from the lumen of therenal tubule involves an influx pathway (IRT)from the renal tubule into the cell and an effluxpathway (Epo) from the cell into the peritubularcapillaries. Some reverse flow can also be envi-saged along the pathway (ERT) from the cell intothe lumen of the tubule and along an influx path-way (Ipc) from the peritubular capillaries intothe cell. In this system, the experimentally de-termined ratio Ccyttine/GFR depends upon the ac-tivities of IRT and ERT, and the occurrence of ra-tios greater than unity could be accounted for bya partial or complete defect that slows the rate oftransport along IRT without affecting ERT. Thisconcept of the disease is in accord with the invitro demonstration that kidney cortex slices fromcystinuric patients seem capable of actively trans-porting cystine (17), but it is not known if anyof the patients whose renal tissue was examinedin this way (17) had cystine clearance that wasgreater than GFR.
It has been shown that cystine does not existas such in the human renal cortex but is whollypresent in the reduced form (i.e., as cysteine)(18). Thus, it may be cysteine rather than cys-tine that is transported along the pathways Ep0and ERT. The appearance of more cystine in theurine than can be accounted for by cystine filteredat the glomerulus could be due to increased denovo synthesis of cystine in the renal tubular epi-thelium. Some support for this idea is providedby the observations of Frimpter (12) and ofRosenberg, Durant, and Holland (19), who foundthat the cystine concentrations in renal artery and-renal venous blood were the same. Frimpter (12)also reported that the concentration of cysteine inrenal venous blood was less than that in the bloodthat reached the kidney, producing a high ex-traction of this amino acid. This observation wasnot, however, confirmed by Rosenberg and as-sociates (19).
The renal clearances of cysteine-penicillamineand penicillamine disulfide are of the same order
1168

RENAL CLEARANCEOF AMINO ACIDS IN CYSTINURIA
of magnitude as the cystine clearance and do notdepend on the dose of penicillamine under the con-
ditions of these studies. This suggests that thecystinuric kidney may handle cystine and these"foreign" disulfides by the same, or similar, mecha-nisms and that some of these disulfides appear inthe urine not only by glomerular filtration, butalso by Ipc and ERT. It is also possible, by anal-ogy with cysteine (18), that penicillamine disulfideand cysteine-penicillamine may be reduced tothiols in the renal tubular cells.
Penicillamine administration lowered the plasmaand urinary cystine concentrations, but the cor-
responding values for the basic amino acids were
unaltered. The renal clearance values for thebasic amino acids were, like the cystine clearance,unaltered by penicillamine administration. Thus,there is no increased loss of basic amino acids, andthe over-all excretion of cystine plus the cysteinemoeity of cysteine-penicillamine is decreased bypenicillamine therapy (7).
Scriver, Efron, and Schafer (20) reported thatthe normal renal clearance of glycine was 4.7 (SD1.3) ml per minute per 1.73 M2. Some of thepresent group of patients had glycine clearancesthat were above this range, but only Patients 6and 8 had glycine clearances that approached thevalue (23 ml per minute per 1.73 m2) reported byFrimpter and co-workers (5) for their patientwith a cystine clearance greater than the glomeru-lar filtration rate.
Dissociation of the amino acid transport defectsin cystinuria. There are striking, differences inthe ratios Ccystine/GFR, Clysine/GFR, Cornithine/GFR, and Carginine/GFR from patient to patientand in the relative magnitudes of these ratioswithin a given patient. These differences were
not related to the administration of D-penicillamine.Thus, it appears that within a group of cystinuricpatients there exist variations in the degree of ex-
pressivity of the abnormal genetic mechanism,which does not affect the transport of the fouramino acids equally. Such variations of expres-
sivity with respect to a single structural gene di-recting the synthesis of a carrier for cystine andthe basic amino acids in the kidney would be ex-
pected to give rise to variations in the degree ofthe amino acid transport defect in which all fouramino acids would be affected to the same extent.
The present observation that the magnitude of thetransport defect varied among the different aminoacids as well as among different patients raisesthe possibility that the control of the formation ofthese mechanisms may depend upon the activity ofmore than one gene. This situation could prevaileither because the individual amino acids haveseparate carrier proteins or because there is amodifying effect from other genes that influencesthe activity of a single carrier protein in such away as to alter its affinity for the individualamino acids differentially.
Patient 9 is of particular interest because sheshows an extreme degree of dissociation of theamino acid transport defects; thus, although theratio Ccystine/GFR was 1.49, the clearances of thebasic amino acids were relatively lower thanthose observed for any of the other patients. Inparticular, the excretion of arginine was extremelylow relative to that of cystine. Another patientwith similar clearance data has recently been en-countered in this laboratory (21), and patientswith high cystine excretions but low arginine ex-cretions have been reported by Crawhall, Saun-ders, and Thompson (22) and by Harris, Mitt-woch, Robson, and Warren (23). When theclearance ratios Cargine/GFR and Cly8ine/GFRare compared graphically (Figure 1), the resultsfor Patient 9 lie on an extension of the line thatdescribes the results for the other patients. Thissuggests that the manifestations of the disease inthis patient represent an extreme degree of thesame genetic abnormality as exists in the otherpatients rather than a separate genetic variant.Extrapolation of the regression line for Carginine/GFRon Clysine/GFR cuts the latter axis at a finitevalue. These results indicate that at low rates ofbasic amino acid clearance the defect in lysinetransport is more marked than the defect in argi-nine transport, although at high rates of basicamino acid clearance the arginine clearance canbe greater than the lysine clearance (Figure 1).This is compatible with Harris and Robson's (24)generalization that when the reabsorptive capacityfor the four amino acids is partially limited, argi-nine is reabsorbed preferentially to cystine andlysine.
A few preliminary studies suggest that the pa-tients with Ccystine/GFR greater than unity may
1169

CRAWHALL,SCOWEN,THOMPSON,AND WATTS
or may not have parents with detectable abnor-malities of cystine and basic amino acid excretion.Similarly, the occurrence of high basic amino acidclearances does not appear to be correlated withthe types of genetic pattern previously describedby Harris and his colleagues (21, 23).
AppendixClinical data on the patients studied
Patient 1 is a twenty-three-year-old female with bi-lateral renal calculi for 4 years. Her urinary tract wasradiologically normal.
Patient 2 is a twenty-five-year-old female who hadright nephrectomy for recurrent calculi 15 years ago.Her left kidney and lower renal tract were radiologicallynormal.
Patient 3 is an eleven-year-old female who had rightnephrolithotomy and left renal colic 6 and 3 years ago,respectively. Her right kidney contained a small calcu-lus and had just detectable function on excretion pyelog-raphy.
Patient 4 is a twenty-one-year-old male with an 18-year history of bilateral renal colic who needed surgicaltreatment on several occasions. Calculi were present inhis left kidney.
Patient 5 is a thirty-year-old male with a 16-year his-tory of recurrent bilateral renal calculi who requiredsurgical treatment on several occasions. Bilateral cal-culi were present. Pretreatment renal clearance studieswere performed while he had thyrotoxicosis, which wastreated by subtotal thyroidectomy before D-penicillaminewas given.
Patient 6 is a nineteen-year-old male who had beenpassing stones and "gravel" for 5 years. His renal tractwas radiologically normal.
Patient 7 is a twenty-nine-year-old male. He had renalcolic and an impacted urethral calculus 5 years ago; hisleft kidney was not functioning then. He had repeatedright renal colic with an impacted calculus and uremiaon one occasion. No calculi were present at the time ofthe present studies.
Patient 8 is a twenty-two-year-old female (sister ofPatient 6). She had symptoms of renal calculi for 4years and bilateral nephrolithotomies. No calculi are nowpresent.
Patient 9 is a ten-year-old female who had bilateral re-nal calculi and an impacted left ureteric calculus. Thelatter was removed surgically 5 months before the presentstudies.
AcknowledgmentsWe acknowledge our indebtedness to the Board of
Governors of St. Bartholomew's Hospital for their gen-erous research grants. Wealso appreciate the help of P.Woodward, J. Gluck, D. I. Chapman, and P. Purkiss,as well as Sister J. Parke and the dieticians on our meta-bolic ward.
References1. Crawhall, J. C., E. F. Scowen, and R. W. E. Watts.
Effect of penicillamine on cystinuria. Brit. med.J. 1963, 1, 588.
2. Crawhall, J. C., E. F. Scowen, and R. W. E. Watts.Further observations on use of D-penicillamine incystinuria. Brit. med. J. 1964, 1, 1411.
3. Dent, C. E., B. Senior, and J. M. Walshe. Thepathogenesis of cystinuria. II. Polarographicstudies of the metabolism of sulphur-containingamino-acids. J. clin. Invest. 1954, 33, 1216.
4. Arrow, V. K., and R. G. Westall. Amino acidclearances in cystinuria. J. Physiol. (Lond.)1958, 142, 141.
5. Frimpter, G. W., M. Horwith, E. Furth, R. E. Fel-lows, and D. D. Thompson. Inulin and endoge-nous amino acid renal clearances in cystinuria:evidence for tubular secretion. J. clin. Invest.1962, 41, 281.
6. Dent, C. E., and B. Senior. Studies on the treat-ment of cystinuria. Brit. J. Urol. 1955, 27, 317.
7. Crawhall, J. C., and C. J. Thompson. Cystinuria:effect of D-penicillamine on plasma and urinarycystine concentrations. Science 1965, 147, 1459.
8. Crawhall, J. C., C. J. Thompson, and K. H. Bradley.Separation of cystine, penicillamine disulfide andcysteine-penicillamine mixed disulfide by auto-matic amino acid analysis. Analyt. Biochem. 1966,14, 405.
9. Edwards, K. D. G., and H. M. Whyte. The meas-urement of creatinine in plasma and urine. Aust.J. exp. Biol. med. Sci. 1958, 36, 383.
10. Schreiner, G. E. Determination of inulin by meansof resorcinol. Proc. Soc. exp. Biol. (N. Y.) 1950,74, 117.
11. Brigham, M. P., W. H. Stein, and S. Moore. Theconcentrations of cysteine and cystine in humanblood plasma. J. clin. Invest. 1960, 39, 1633.
12. Frimpter, G. W. Cystinuria: metabolism of the di-sulfide of cysteine and homocysteine. J. clin. In-vest 1963, 42, 1956.
13. Dickinson, J. C., H. Rosenblum, and P. B. Hamilton.Ion exchange chromatography of the free aminoacids in the plasma of the newborn infant. Pedi-atrics 1965, 36, 2.
14. Spackman, D. H., W. H. Stein, and S. Moore. Au-tomatic recording apparatus for use in the chro-matography of amino acids. Analyt. Chem. 1958,30, 1190.
15. Gerritsen, T., M. L. Rehberg, and H. A. Waisman.On the determination of free amino acids in se-rum. Analyt. Biochem. 1965, 11, 460.
16. Dent, C. E., M. Friedman, H. Green, and L. A. C.Watson. Treatment of cystinuria. Brit. med. J.1965, 1, 403.
17. Fox, M., S. Thier, L. E. Rosenberg, W. Kiser, and S.Segal. Evidence against a single renal transport
170

RENAL CLEARANCEOF AMINO ACIDS IN CYSTINURIA
defect in cystinuria. New Engl. J. Med. 1964, 270,556.
18. Crawhall, J. C., and S. Segal. The intracellular cys-
teine/cystine ratio in kidney cortex. Biochem. J.1966, 99, 19C.
19. Rosenberg, L. E., J. L. Durant, and J. M. Holland.Intestinal absorption and renal excretion of cys-
tine and cysteine in cystinuria. New Engl. J.Med. 1965, 273, 1239.
20. Scriver, C. R., M. L. Efron, and I. A. Schafer. Renaltubular transport of proline, hydroxyproline, and
glycine in health and in familial hyperprolinemia.J. dlin. Invest. 1964, 43, 374.
21. Crawhall, J. C., P. Purkiss, E. P. Saunders, andR. W. E. Watts. Unpublished data.
22. Crawhall, J. C., E. P. Saunders, and C. J. Thompson.Heterozygotes for cystinuria. Ann. hum. Genet.1966, 29, 257.
23. Harris, H., U. Mittwoch, E. B. Robson, and F. L.Warren. Phenotypes and genotypes in cystinuria.Ann hum. Genet. 1955, 20, 57.
24. Harris, H., and E. B. Robson. Cystinuria. Amer.J. Med. 1957, 22, 774.
1171