The Red Cell Histogram.pdf
9
CE Update 300 LABMEDICINE ■ Volume 42 Number 5 ■ May 2011 labmedicine.com To paraphrase an adage, 1 histogram graph is worth 1000 numbers. A large collection of data, displayed as a visual image, can convey information with far more impact than the numbers alone. In hematology, these data take on several forms, 1 of which is the RBC histogram. Visual scanning of the histogram gives a good initial sense of the range, size, shape, and other salient features of the red cell morphology. The RBC histogram, a graphic representation of particle size distribution, is now routinely available on automated cell analyzers as a standard part of automated complete blood count (CBC) analysis. This histogram in association with other CBC parameters, such as RBC distribution width (RDW) and mean corpuscular volume (MCV), has been found abnormal in various hematological conditions and may provide major clues in the diagnosis and management of sig- nificant red cell disorders. 1-4 In addition, it is frequently used, along with the peripheral blood film, as an aid in monitoring and interpreting abnormal morphological changes, particu- larly dimorphic red cells. Table 1 lists conditions associated with dimorphic red cell changes. Before reporting CBC results, a clear distinc- tion between dimorphic and dual populations must be clari- fied as they are sometimes interchangeable and confusing. In a dimorphic picture, the histogram may have 2 or more (multiple) red cell populations, whereas in dual populations the histogram has 2 distinct red cell populations (eg, hypo- chromic-microcytic and normochromic-normocytic red cells). These 2 distinct populations may be comprised of either a patient’s own red cells (post-iron treatment) or a mixture of patient and donor red cells (post-iron transfusion). Although this is an arbitrary categorization, the term dimorphic is less restrictive and therefore more widely used, as it can be applied to either the dual or the multiple red cell populations. Thus, the dimorphic blood picture will look like a dual popula- tion of microcytic and normocytic (Image 1A) or normocytic and macrocytic red cells, or an admixture of small, normal, and large cells of different sizes and forms (Image 1B). Some morphological features of dimorphism and the ensuing char- acteristic changes in their RBC histograms are discussed in this article. The Red Cell Histogram and The Dimorphic Red Cell Population Benie T. Constantino, SH, I; ART, MLT(CSMLS) (CML Healthcare Inc., Mississauga, Ontario, Canada) DOI: 10.1309/LMF1UY85HEKBMIWO Abstract The RBC histogram is an integral part of automated hematology analysis and is now routinely available on all automated cell counters. This histogram and other associated complete blood count (CBC) parameters have been found abnormal in various hematological conditions and may provide major clues in the diagnosis and management of significant red cell disorders. In addition, it is frequently used, along with the peripheral blood film, as an aid in monitoring and interpreting abnormal morphological changes, particularly dimorphic red cell populations. This article discusses some morphological features of dimorphism and the ensuing characteristic changes in their RBC histograms. Keywords: histogram, dimorphic red cells, red blood cell distribution width After reading this article, readers should be able to correlate a RBC histogram and red blood cell distribution width with microscopical findings. Hematology exam 51102 questions and corresponding answer form are located after this CE Update on page 309. Abbreviations CBC, complete blood count; RDW, red blood cell distribution width; MCV, mean corpuscular volume; MCHC, mean corpuscular hemo- globin concentration; IDA, iron deficiency anemia; RDW-CV, red blood cell distribution width coefficient of variation; thal, thalas- semia; SD, standard deviation; HPP, hereditary pyropoikilocytosis Corresponding Author Benie T. Constantino, SH, I; ART, MLT(CSMLS) [email protected] Submitted 4.30.10 | Revision Received 9.27.10 | Accepted 9.27.10 Table 1_Conditions Associated With Dimorphic Red Cells 5-12 Early iron developing microcytic population Folate/vitamin B12 developing macrocytic population Post-iron treatment of iron deficiency anemia Post-iron treatment of iron deficiency with megaloblastic anemia Post-iron treatment of megaloblastic anemia Post-iron treatment of megaloblastic anemia with iron deficiency Post-iron transfusion macrocytic anemia Post-iron transfusion microcytic anemia Iron deficiency anemia with either folate or vitamin B12 deficiency Sideroblastic anemia (myelodysplasia) Hemolytic anemia (reticulocytosis, spherocytosis, fragmentation, pyropoikilocytosis) Cold/warm auto agglutination Erythropoietin-induced erythropoiesis Delayed transfusion reaction Homozygous hemoglobinopathies (admixture of many RBC forms) Myelofibrosis (admixture of extramedullary hematopoiesis) Constitutional chromosomal translocation t(11;22)(p15.5;q11.21)
-
Upload
pieterinpretoria391 -
Category
Documents
-
view
109 -
download
6
description
The Red Cell Histogram
Transcript of The Red Cell Histogram.pdf

CE Update
300 LABMEDICINE ■ Volume 42 Number 5 ■ May 2011 labmedicine.com
To paraphrase an adage, 1 histogram graph is worth 1000 numbers. A large collection of data, displayed as a visual image, can convey information with far more impact than the numbers alone. In hematology, these data take on several forms, 1 of which is the RBC histogram. Visual scanning of the histogram gives a good initial sense of the range, size, shape, and other salient features of the red cell morphology.
The RBC histogram, a graphic representation of particle size distribution, is now routinely available on automated cell analyzers as a standard part of automated complete blood count (CBC) analysis. This histogram in association with other CBC parameters, such as RBC distribution width (RDW) and mean corpuscular volume (MCV), has been found abnormal in various hematological conditions and may provide major clues in the diagnosis and management of sig-nificant red cell disorders.1-4 In addition, it is frequently used, along with the peripheral blood film, as an aid in monitoring and interpreting abnormal morphological changes, particu-larly dimorphic red cells.
Table 1 lists conditions associated with dimorphic red cell changes. Before reporting CBC results, a clear distinc-tion between dimorphic and dual populations must be clari-fied as they are sometimes interchangeable and confusing. In a dimorphic picture, the histogram may have 2 or more
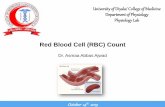
(multiple) red cell populations, whereas in dual populations the histogram has 2 distinct red cell populations (eg, hypo-chromic-microcytic and normochromic-normocytic red cells). These 2 distinct populations may be comprised of either a patient’s own red cells (post-iron treatment) or a mixture of patient and donor red cells (post-iron transfusion). Although this is an arbitrary categorization, the term dimorphic is less restrictive and therefore more widely used, as it can be applied to either the dual or the multiple red cell populations. Thus, the dimorphic blood picture will look like a dual popula-tion of microcytic and normocytic (Image 1A) or normocytic and macrocytic red cells, or an admixture of small, normal, and large cells of different sizes and forms (Image 1B). Some morphological features of dimorphism and the ensuing char-acteristic changes in their RBC histograms are discussed in this article.
The Red Cell Histogram and The Dimorphic Red Cell Population Benie T. Constantino, SH, I; ART, MLT(CSMLS) (CML Healthcare Inc., Mississauga, Ontario, Canada) DOI: 10.1309/LMF1UY85HEKBMIWO
Abstract The RBC histogram is an integral part of automated hematology analysis and is now routinely available on all automated cell counters. This histogram and other associated complete blood count (CBC) parameters have been found abnormal in various hematological
conditions and may provide major clues in the diagnosis and management of significant red cell disorders. In addition, it is frequently used, along with the peripheral blood film, as an aid in monitoring and interpreting abnormal morphological changes, particularly dimorphic red cell populations. This article discusses
some morphological features of dimorphism and the ensuing characteristic changes in their RBC histograms. Keywords: histogram, dimorphic red cells, red blood cell distribution width
After reading this article, readers should be able to correlate a RBC histogram and red blood cell distribution width with microscopical findings.
Hematology exam 51102 questions and corresponding answer form are located after this CE Update on page 309.
AbbreviationsCBC, complete blood count; RDW, red blood cell distribution width; MCV, mean corpuscular volume; MCHC, mean corpuscular hemo-globin concentration; IDA, iron deficiency anemia; RDW-CV, red blood cell distribution width coefficient of variation; thal, thalas-semia; SD, standard deviation; HPP, hereditary pyropoikilocytosis
Corresponding AuthorBenie T. Constantino, SH, I; ART, MLT(CSMLS) [email protected]
Submitted 4.30.10 | Revision Received 9.27.10 | Accepted 9.27.10
Table 1_Conditions Associated With Dimorphic Red Cells5-12
Early iron developing microcytic populationFolate/vitamin B12 developing macrocytic population Post-iron treatment of iron deficiency anemiaPost-iron treatment of iron deficiency with megaloblastic anemiaPost-iron treatment of megaloblastic anemiaPost-iron treatment of megaloblastic anemia with iron deficiency Post-iron transfusion macrocytic anemiaPost-iron transfusion microcytic anemiaIron deficiency anemia with either folate or vitamin B12 deficiencySideroblastic anemia (myelodysplasia)Hemolytic anemia (reticulocytosis, spherocytosis, fragmentation, pyropoikilocytosis) Cold/warm auto agglutinationErythropoietin-induced erythropoiesisDelayed transfusion reactionHomozygous hemoglobinopathies (admixture of many RBC forms)Myelofibrosis (admixture of extramedullary hematopoiesis)Constitutional chromosomal translocation t(11;22)(p15.5;q11.21)

CE Update
labmedicine.com May 2011 ■ Volume 42 Number 5 ■ LABMEDICINE 301
RBC Histogram: An Overview
The well-known Coulter principle of counting and sizing red cells provides the basis for generating the histogram. This method relies on the change in conductance as each cell passes through an aperture. The change in conductance results in an electrical pulse, the amplitude of which is proportional to the cell volume. The 256-channel pulse-height analyzer uses a number of thresholds to sort the cells into several size (volume) channels from which the histogram is formed. Each channel on the X-axis represents a specific size (volume) in femtoliter (24-360 fL), increasing from left to right. The Y-axis represents the number of cells per channel, with each cell being stored in the channel representing its size, so that after data accumula-tion is completed the relative number of cells (frequency) is provided. This data is further processed by the computer, and the RBC curve is smoothed by a moving average technique and displayed on a data management system.13 Figure 1A shows a typical normal RBC histogram. For a detailed explanation on the construction of histogram, please see reference 14.
Value of HistogramA histogram, as shown in Figure 1 and Figure 2, is a
graphic representation of a collection of data based on cell size and/or cell number depicting variations in the process. It is sometimes referred to as a frequency of distribution curve. Because graphics can show data in ways that are meaningful and quickly understood, the histogram is a very powerful tool in red cell morphological analysis. It enables one to visualize, analyze, and interpret empirical data that displays morpholog-ical changes graphically as points, peaks or valleys, or as a line of frequency curve. It allows the users to intuitively see the visual comparison of the center and spread of data and data containing 2 or more variables: dimorphic red cells, subpopu-lations, and skewed data, leading to quick and cost-effective decision making.
At times, a histogram can provide invaluable information that may not even be apparent in the automated numerical
data.5,15 For example, in megaloblastic anemia with developing iron deficiency, some of the hypochromic and microcytic red cells can be identified in the histogram but may not be reflected in the numerical data, and this may well be the first clue to a not uncommon occurrence. Likewise, iron deficiency may de-velop insidiously during the process of some other disease (eg, essential polycythemia), with normal cell counts and indices, except the RDW, which is elevated. The RBC histogram is also abnormal, showing a shoulder of microcytic red cells.16
Furthermore, a histogram can provide useful information for laboratorians in 1) monitoring the reliability of the re-sults generated by the analyzers; 2) investigating the potential cause(s) of the erroneous automated results; and 3) arriving at the presumptive diagnosis.7 For example, certain conditions like the presence of fragmented red cells or red cell agglutina-tion that could not have been identified earlier without blood film examination can now be presumably detected on the red cell histogram.3,16 Likewise, in patients with iron deficiency anemia (IDA) or megaloblastic anemia in treatment, a sequen-tial histogram can clearly show the progressive appearance of a new erythrocyte population well in advance of other numeri-cal parameters.3
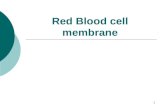
The presence of a right-sided shoulder usually corresponds to reticulocytosis (Figure 1J), and a trailer of erythrocyte popu-lations on the far right of the histogram correlates to red cell agglutination (Figure 1F). A leftward shift of the RBC histo-gram signifies microcytosis (Figure 1B and Figure 1C), and a rightward shift suggests macrocytosis (Figure 1D and Figure 1E). Bimodal red cell histograms (Figure 1F, Figure 1G, Figure 1K, Figure 1L and Figure 2B to Figure 2E) are usually associated with therapeutic transfusion and/or hematinic agent response to microcytic and macrocytic anemia, but they may also indicate other hematological disorders as shown in Table 1.
Although the size ranges for RBC histograms are between 24 fL and 360 fL, the instrument counts only those cells with volume sizes between 36 fL and 360 fL as red cells. Those cells counted in the 24 fL to 36 fL range are rejected and not included in the RBC count. They are enumerated and displayed in the histogram area between the 24 fL and 36 fL
Image 1_(A) Wright-stained peripheral blood film from post-iron treated patient showing dual population of hypochromic-microcytic (short arrow) and normochromic-normocytic red cells (long arrow). (B) Peripheral blood film from post-splenectomized patient with hereditary pyropoikilocytosis showing dimorphic picture of extreme variability of the RBCs such as red cell fragments (short arrow), microspherocytes (regular arrow), membrane budding (long arrow), elliptocytes, oval macrocytes, and polychromasia.
A B

CE Update
302 LABMEDICINE ■ Volume 42 Number 5 ■ May 2011 labmedicine.com
A B C
D E F
G H I
J K L
RBC Histograms
Figure 1_Red cell histograms in various hematological conditions. (Key hematological features of these conditions are summarized in Table 2.) Figure (A) Normal histogram, (B) Microcytosis, iron deficiency anemia, (C) Microcytosis, beta thal trait, (D) Macrocytosis with normal RDW, (E) Macrocytosis, megaloblastic anemia, (F) Cold agglutination, (G) Sideroblastic anemia, (H) Beta thalassemia major, (I) Pyropoikilocytosis, (J) Reticulocytosis, (K) Post-iron therapy, (L) Post-iron therapy.
Table 2_Key Hematological Features of Various Hematological Conditions in Figure 1
Hematological Parameters
Condition HGB (g/L) MCV (fL) MCHC (g/L) RDW-CV (%) RBC Histogram
1A Normal 146 89.6 330 14.4 Normal
1B Iron deficiency anemia 86 54.7 314 21.6 LS
1C Beta thalassemia 131 66.0 318 14.5 LS
1D Macrocytosis 131 102.8 351 14.3 RS
1E Megaloblastic anemia 65 127.8 324 35.7 DM RS SKL
1F Cold agglutinin 124 110.6 +++++ 17.5 DM BM
1G Sideroblastic anemia 92 90.9 320 39.2 DM BM LS SKR
1H Beta thal major 86 79.6 285 32.1 DM LS
1I Pyropoikilocytosis 99 60.2 358 41.5 DM LS SKR
1J Reticulocytosis 87 72.2 298 31.3 DP LS SKR
1K Post-iron therapy 132 81.1 317 14.8 DP BM
1L Post-iron therapy 112 85.8 330 35.0 DP BM Reference range 120-160 80-95 320-360 11.5-14.5
HGB, hemoglobin; MCV, mean corpuscular hemoglobin; RDW-CV, red cell distribution wiidth-coefficient of variation; DM, dimorphic; BM, bimodal; DP, dual population; LS, left-shift; RS, right-shift; SKR, skewed to the right; SKL, skewed to the left; MCHC (+++++) overrange.

CE Update
labmedicine.com May 2011 ■ Volume 42 Number 5 ■ LABMEDICINE 303
RBC HistogramsA B
C D
E F
G
Table 3_Key Hematological Features in Iron Deficiency Anemia After Treatment
Hematological Parameters
Condition HGB(PT) HGB(POT) MCV(PT) MCV(POT) RDW(PT) RDW(POT) SF(PT) RBC Histogram
2A Normal 144 84.7 13.9 Normal2B IDA 108 132 70.3 82.8 22.1 25.5 8 DP SKL2C IDA 80 107 69.2 81.1 18.0 29.2 7 DP BM 2D IDA 86 118 61.3 77.4 23.0 36.0 <5 DP BM 2E IDA 98 119 70.4 78.9 17.9 28.2 8 DP BM LS 2F IDA 95 106 65.6 70.2 19.5 28.8 <5 DP LS SKR2G IDA 81 91 62.9 68.6 19.5 25.9 <5 DM LS SKR
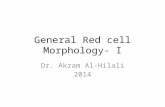
PT, pre-treatment; POT, post-iron treatment; IDA, iron deficiency anemia; DP, dual population; BM, bimodal; SKL, skewed to the left; SKR, skewed to the right; SL, left shift; SF, serum ferritin. SF normal range (female)=13-145 UG/L; SF (male)=27-220 UG/L.
Figure 2_Histograms of iron deficiency anemia after treatment (key hematological features are summarized in Table 3). Figures B to G are rep-resentative examples of dimorphic (dual) red cell population response to hematinic treatment of iron deficiency anemia in 6 patients.

CE Update
304 LABMEDICINE ■ Volume 42 Number 5 ■ May 2011 labmedicine.com
range, however, allowing the lower end of the histogram to be monitored. Normally, the space below 36 fL remains clear, but in certain conditions the histogram may begin above the baseline or show a high takeoff on the far left of the curve (Figure 1G to Figure 1I), which generally indicates the presence of small particles. These particles include red cell fragments, microspherocytes, nucleated RBCs, nonlyzed RBCs, elliptocy-tosis, macrothrombocytes, platelet clumps, bacteria, parasitic organisms, and other interfering substances such as cryoglobu-lin, cold agglutinin, and macroglobinemia.7,16-18
Analysis and Interpretations of Histograms in Figure 1 and Figure 2
The red cell histograms presented for illustration were randomly selected to represent various common hematological conditions and the different stages of post-iron IDA therapy. A histogram may be interpreted by looking at the shape of the data distribution. The distributional shape of the histogram can be classified as reflecting either single or dimorphic (mul-tiple) red cell populations. In a single population, the histo-gram may have a normal Gaussian or bell-shape curve, may be widened with or without left or right shift, may be skewed to the left or right, or may show some combination of all of these characteristics. In dimorphic populations, the histogram may be symmetric and/or bimodal, or bimodal but skewed to the left or right. The centeredness and width of the histogram also define the extent of RBC variability.
Potentially, a number of factors may affect the histogram of the aperture impedance cell distribution analysis. These include the coincident doublet of red cells, red cell agglutina-tion, inclusion of reticulocytes with mature red cells, altera-tion in red cell shape, and inclusion of leukocytes in certain diseases. These factors, in 1 way or another, influence the histogram’s appearances and accordingly will have a variable effect on any measurements made from the histogram.16 To reduce the effect of these problems, manufacturers design their instruments and reagent systems to specifically prevent and correct for interferences.13 They develop mathematical algorithms for particle counting and produce numeric data, graphic data, scatter plots, and interpretative comments that will assist or alert the users to potential incorrect results.19,20 In addition, to avoid interference in the calculations of RDW, the information below 20% of scale on the red cell histogram are excluded (Figure 3). These misleading data include cell coincidence, aperture artifacts, doublets and triplets, and agglutinates on the right side and platelet clumps, and mega-thrombocytes on the left side of the histogram.13,16
Before taking up complex histogram graphs, the beginner will find it helpful to examine the simple outline or overall pattern of a regular histogram as reflected in Figure 1A to Figure 1D. Familiarity with typical RBC histograms will make the task of evaluating other notable deviations easier. In view of this, to maximize the usefulness of the histogram, a dotted line depicting a reference normal curve (eg, symmetric nor-mal curve with MCV of 96 fL and RBC distribution width coefficient of variation [RDW-CV] of 15.0%) should be au-tomatically superimposed on every red cell histogram so any discernible deviation from that curve can be clearly delineated for contrast. Simply put, if the patient’s histogram strays from the reference normal range, it means that the histogram may be abnormal.
The following are important points to consider when reviewing/analyzing histograms.13
• positionofindividualpopulationscomparedtonormal/typical positions
• amountofseparationbetweenpopulationscomparedtonormal/typical separation
• relativeconcentrationofeachpopulationcomparedtonormal/typical concentrations
• presenceofunexpectedornon-typicalpopulations
Figure 1A to Figure 1D are typical examples of normal, microcytic, and macrocytic red cell histograms. They are symmetric, single-peaked, and “bell shaped” normal curves. The curve is considered symmetric if the 2 sides of the curve coincide when folded in half or are approximately mirror im-ages. When the distribution is not symmetric, it is referred to as skewed wherein 1 of the 2 sides (left or right) of the curve extends much further than the other. In a normal RBC histo-gram, the majority of each cell falls between 55 fL and 125 fL. The tail of the distribution consists of coincident doublets and anomalous pulses.16
In IDA and beta thalassemia (thal) trait, the red cell distribution curves are shifted to the left, and the percentage of microcytosis is increased. Although their histograms are similar, the degree of anisocytosis, as measured by the RDW, differentiates them. Iron deficiency anemia is characterized by elevated RDW, reflecting the heterogeneity in the acquired erythrocyte populations. In thal trait however, the RDW is usually within range due to the homogeneity of the inherited population of erythrocytes. Although this difference is useful to some extent in distinguishing them, cases involving severe anemia with homogenous microcytosis may give misleading results.3 Nonetheless, patients showing severe anemia with hemoglobin <90 g/L and with hypochromic-microcytic red cells are most likely (80%) iron deficient.21
Figure 3_Calculation of RDW. The RDW is calculated from the width of the histogram at 1 SD from the mean divided by MCV. The normal RDW-CV is 11.5% to 14.5%. The RDW-SD is the arithmetic width of the distribution curve measured at the 20% frequency curve. The normal RDW-SD is 39 to 47 fL.14

CE Update
labmedicine.com May 2011 ■ Volume 42 Number 5 ■ LABMEDICINE 305
Cautionary Note When Visually Observing and Interpreting RDW
Automated counters use 2 methods to measure the value of RDW. The first is referred to as RDW-CV (Figure 3). This reflects the ratio of 1 standard deviation (SD) to the MCV. Since it is a ratio, changes in either the SD or MCV will influence the results. Microcytosis will tend to elevate the RDW-CV simply by decreasing the denomina-tor (MCV) of the ratio. As a result, the RDW is probably a more sensitive parameter in microcytic than in macrocytic red cell disorders.11 Conversely, macrocytosis, by increasing the denominator, may offset the change in the SD and reduce the RDW-CV. Put simply, a population with a large MCV may appear wider on the histogram but may give a normal RDW-CV. Likewise, a population with a very small MCV may appear smaller but may give a large RDW-CV.2 The sec-ond method of calculating the RDW is called the RDW-SD, which is independent of MCV. It is a direct measurement of the width in fL at the 20% frequency level on the RBC curve (Figure 3).
The RDW-SD is a measure of the dispersion or scatter of values about the mean. The more spread apart the data, the higher the SD and vice versa. An RDW-CV is another mea-sure of the dispersion of data around the mean. It represents the ratio of 1 SD to the mean. Although both methods use SD to measure the degree of anisocytosis, they measure cell variation differently.
Consider Figure 1E - an abnormal histogram of megalo-blastic anemia with a RDW-CV of 35.7% and a RDW-SD of 172.8 fL. While both results are high, obviously the RDW-SD is relatively higher than the RDW-CV. This is probably because of the way dispersion is measured by the RDW-CV formula: 1 SD divided by MCV. The 1 SD imposed by the formula restricts its capability to measure variability to ± 1 SD.
As a result, other abnormal cells outside the ± 1 SD are excluded from the estimate hence the comparatively low RDW-CV results. In addition, the MCV (the denominator) is not a measure of disper-sion, but it can affect the RDW-CV result depend-ing on its average value. In this case, the high MCV value of 127.8 fL counterbalances the effect of high SD, hence the further reduction in the RDW-CV value. Thus, this method is not recommended for assessing highly abnormal histograms. However, it shows a better correlation as an indicator of aniso-cytosis when the MCV is in the low normal range and anisocytosis is difficult to detect, as seen in de-veloping iron deficiency. It is also a good method to monitor the effect of iron therapy and to differentiate IDA from thal trait.
On the other hand, because the RDW-SD is a direct measure across the RBC histogram, it is the better and more accurate measure of anisocytosis, especially in highly abnormal histograms. It seems to represent the genuine morphological and/or patho-logical status of the patients, as it encompasses the entire spectrum of MCV values. In other words, unlike in RDW-CV, those small and large abnor-mal cells in varying degrees of anisocytosis and/or poikilocytosis outside the ± 1 SD are included in the measurement, hence the relatively high RDW-SD re-sults. It appears, however, that the higher the RDWs,
the higher the degrees of anisocytosis and/or poikilocytosis. In view of the above, it seems logical that technologists
reading blood films should have ready access to both the RDW-CV and RDW-SD results for comparative review and better correlation of results.
MacrocytosisMacrocytosis with a MCV higher than 100 fL (and a normal
RDW) is found in 3% to 5% of adult patients, a significant proportion of whom may not have anemia22 (Figure 1D). Ac-cording to Gulati,23 macrocytic red cells of <25% with MCV of 95 fL to 110 fL are morphologically graded as (1+). Correlation between the grading level of macrocytosis (or other conditions) and the MCV should be verified microscopically.
Megaloblastic AnemiaPatients with macrocytic anemia due to vitamin B12/
folate deficiency may sometimes show a single widely distrib-uted peak of cells from very small cells and red cell fragments on the left to macrocytic cells approaching 250 fL on the right (Figure 1E). Note a large number of small cells, reflected as a high take-off on the left, are above the 20% frequency trim line. As a result, they are included in the determination of the MCV and the RDW, leading to their falsely reduced and greatly elevated values, respectively. In severe megaloblas-tic anemia, the white cell and platelet histograms as well as the counts and the morphology may give additional information.
Figure 1F to Figure 1L and Figure 2B to Figure 2G portray the many faces and mechanisms of dimorphism. While it is convenient to associate dimorphism with a single process, it must be emphasized that multiple interacting mechanisms are
Glossary
Anisocytosis: Variation in red cell size.
Anomalous pulses: This is an interference by electrical pulses/noises but at a very low level. These anomalous pulses and coincident doublets are reflected as a small tail to the right of a normal curve (Figure 1A and Figure 2A). In most normals, the frequency distribution of red cells does not exceed the range of 50 fL-200 fL. Despite the instrument’s refinement in aperture design, correction for coincidental passage of cells, and the use of sophisticated edit circuitry to exclude aberrant pulses, the presence of these interferences to some degree cannot be avoided.
Coincident doublets: Occasionally, 2 or more cells pass through an aperture at the same time and are counted as a single cell. The analyzer automatically corrects results for coincidence.
Dimorphic: According to the Webster New World College Dictionary, the word dimorphic means the occurrence of 2 types of individuals in the same species (2 different forms/sizes of cells in a sample). Note, however, that the term dimorphic is broadly defined in this article to signify 2 or more (multiple) red cell populations. This is because there are 2 technical meanings for the same word. When “dimorphic” is used, the context will determine the meaning.
Poikilocytosis: Variation in red cell shape.

CE Update
306 LABMEDICINE ■ Volume 42 Number 5 ■ May 2011 labmedicine.com
sometimes involved. The dimorphic population message is generated when there are 2 cell size populations or there are multiple peaks in the RBC histogram pattern.13,24
Cold AgglutinationBecause this is a time-, temperature-, and agglutinin titer-
dependent reaction, the frequency curves may vary in shapes (Figure 1F). A U-shape-like appearance of the curve would usually suggest the presence of 2 discrete populations, 1 on either side. However, in this case, the abnormal histogram is the result of a high titer cold agglutinin causing red cells to agglutinate and interfere with their sizing and enumeration. Some analyzers with an Interpretive Program of flags and messages may generate an RBC Agglutination flag.24 Dashes (- -) replace the data for RDW, and an asterisk (*) appears on most red cell associated parameters. This asterisk indicates that these results are unreliable and should be reviewed care-fully as per laboratory protocol.
On the other hand, despite the abnormal histogram, other instruments still measure and calculate the RDW, using only the major population of cells.13 The minor populations and the middle trough are excluded in order to avoid interference in RDW calculation. The high frequency entry on the left of the histogram could be due to the effect of the high titer antibody interfering in cell separation. Since the doublet or triplet red cells are counted as 1 cell and large clumps of cells are excluded from the count, the changes in RBC counts and volumes affect all the CBC parameters, except the hemoglobin.20 The varying degrees of agglutination in this condition result in a variety of various histogram curves with the varying amounts of trailer of red cells seen on the far right side of the graph.
Sideroblastic AnemiaThis is an example of a bimodal distribution with 2 sepa-
rated small, distinct high points (Figure 1G). To produce a single distribution, the 2 red cell populations must differ by less than 15% in volume.16,25 It appears that the particle size distribution is very wide, from a group of very small cells—reflected as a high take-off on the baseline of the curve, to a group of normal and macrocytic cells that are equally spread on the other side. The groups themselves represent different ranges of values so the entire sets of results are actually wide-spread. In other words, it is an admixture of small cells, nor-mal cells, and large cells in various proportions. The results of the red cell indices, however, are within normal range, and if one were to rely on indices alone, the important finding of mixed populations would be missed. This reinforces the importance of examining the blood cell histograms and blood film in tandem in order to detect the bimodal populations.2 When viewed microscopically, it is clear the red cell volume histogram accurately reflects the dimorphic appearances.
Beta Thalassemia Major (and Other Small Particles)
In this case, a high frequency of small cells (<50 fL) can be seen at the beginning of the histogram (Figure 1H). This may be due to the small particles seen in this disorder, such
as red cell fragments, nucleated RBCs, microspherocytes, and microcytic red cells, producing an erroneous mean cell vol-ume for the intact cell population. Although the curve appears unimodal, the instrument interpreted it as dimorphic, prob-ably due to the admixture of different cell populations. Any spurious cell population that is >1% as numerous as the red cells will influence the MCV, RDW, and histogram results.26 Thus, in all these examples, only by careful examination of the histogram, knowledge of the possible causes of the abnor-mal curves, and careful correlation with the peripheral blood morphology can a correct diagnosis be derived.
PyropoikilocytosisHereditary pyropoikilocytosis (HPP) is a congenital
hemolytic disorder characterized by moderate to severe hemo-lytic anemia27,28 (Figure 1I). Hereditary pyropoikilocytosis is also considered an aggravated form of hereditary elliptocy-tosis. It is a membrane defect as suggested by the increased susceptibility to fragmentation lyses at 46°C. The blood picture resembles those seen after severe burns. As in Figure 1H, the microspherocytes, nucleated RBCs, red cell frag-ments, membrane budding, and microelliptocytes observed in this condition may cause a moderate reduction in MCV and a high take-off of the histogram on the left. However, the RDW remains increased due to increased variability of red cell volumes, resulting in high SD. Recall the calculation for RDW-CV; SD is divided by MCV. Since the SD is dispro-portionately increased, compounded by the very low MCV, the RDW will be greatly elevated. The histogram obviously shows shift to the left as it begins near the modal value on the upper left of the graph and falls away on the right side, slightly skewing the curve to the right.
ReticulocytosisThe histogram is bimodal and is skewed to the right (Fig-
ure 1J). Usually, this may be the kind of picture seen in initial post-iron treatment IDA. Three to 8 days after effective iron therapy, a reticulocytosis (polychromasia) of this magnitude may occur, producing a secondary peak representing this new population of cells. Generally, reticulocytes are slightly larger than normal mature red cells.23 The reticulocyte count of this patient is 5.5%. According to some authors, a reticulocytosis in excess of 15% and/or a volume difference of 2 populations of less than 15% are required to affect histogram analysis.16,25 However, others have suggested it is possible to detect the ap-pearance of a new population of cells (eg, reticulocytes) even at just more than 5% of the total red cell population, by skewing the histogram.4 Thus, depending on the instrument algorithm, a cohort of cells even at 5% may be interpreted as another population, hence, the dimorphic instructive comment.
These 2 histograms (Figure 1K and Figure 1L) seem to be similar in appearance: both have 2 unevenly high peak points with middle trough or valley. What is surprising in these curves is the difference in the RDW results. Despite the bi-modal histogram, Figure 1K shows a normal RDW compared to Figure 1L, which has a higher RDW. The reason for the normal RDW is that only the major populations are included and measured for the MCV and RDW calculations, so the MCV and RDW are that of the main population only. The

CE Update
labmedicine.com May 2011 ■ Volume 42 Number 5 ■ LABMEDICINE 307
middle trough, which is below the 20% frequency truncation, and the minor populations, as represented by the low peak, are excluded from the MCV and RDW calculations. The inclusion of minor populations will also require the inclu-sion of the middle trough, and thus may spuriously elevate the RDW. On the other hand, because the valley in Figure 1L has surpassed the detection level, the minor and the major populations are included in the MCV and RDW calculations; hence, the higher RDW value. Microscopically, both show a dual population of hypochromic-microcytic and normochro-mic-normocytic red cells.
Figure 2A to Figure 2F are representative histograms of post-iron treatment IDA from 6 patients. The red cell histo-gram assists in confirming the diagnosis of IDA and in fol-lowing its treatment. Patients with microcytosis due to IDA usually have a unimodal frequency curve but with appropriate therapy, a second population of normocytic cells appears in the majority of cases. The readout on Figure 2G shows the initial result after 3 days of iron treatment. There is a small subpopulation of reticulocytes that merely contribute to the right skew of the graph.9 At this stage, the MCV starts to increase and the RDW further increases.16
After 2 to 4 weeks therapy, a distinct population of new emerging normocytic cells with some polychromasia is evi-dent on the graph and the blood film, though a secondary peak is just starting to shape up as seen in Figure 2F. Figure 2E shows 2 unequal distinct population peaks of microcytic and normocytic cells, meaning that >15% of the total cell population are normocytic cells and the remainder is micro-cytic cells. Five to 6 weeks later, Figure 2D shows 2 symmetric peaks representing an almost equal number of hypochromic microcytic and normochromic normocytic cells.4 Seven, and up to 15 weeks (105 days) forward, normocytic cells become the predominant cells, and the histogram starts to skew to the left as shown in Figure 2C and Figure 2B. After 17 weeks (120 days) of effective therapy, a population of mostly normochro-mic normocytic cells and a normal MCV and RDW ensue as seen in Figure 2A. Barring any complications or coexistence of vitamin B12/folate deficiency, it appears the histograms and/or MCV in different stages of post-iron treatment may vary; however, the pattern of red cell size changes from initial re-ticulocytosis to gradual normocytosis appear to be the same.
ConclusionIn assessing a histogram, the overall pattern is observed,
and the histogram is described by its shape, center, and spread. This pattern by itself as seen in the red cell distribu-tion curve is meaningless unless it is compared with a refer-ence normal curve and/or confirmed microscopically. Some distributions have simple shapes, such as symmetric and skewed, but others may be more challenging, especially when dimorphic (multiple) populations of red cells are present.
Given that dimorphic and dual populations are synony-mous and may cause confusion in the reporting of results, full recognition of dimorphic as more than just 2 cell populations has certain practical and clinical significance. Clinically, it is associated with many conditions as shown in Table 1. Practi-cally, since dimorphic is usually associated with abnormal red cell populations, morphological findings should be correlated with the graphical and numerical data for better interpretation of results.
Although direct inspection of the distribution curve offers a sensitive method for detecting small populations of microcytic or macrocytic red cells, the estimation of the num-ber of cells from the distribution curve should be avoided. Misleading results can occur because the frequency curve shows only the relative and not the actual number of cells in each size range.13 Even though the MCV can be easily located on any symmetric distribution curve, attempting to do so in a skewed, bimodal, or dimorphic population is discouraged because the MCV is an average value and does not reflect the heterogeneity or the presence of different cell populations.
When combined with the concept of the normal curve and the knowledge of particular CBC parameters, such as RDW and red cell indices, histograms become a practical working tool in the initial stage of morphological analysis. Observation of their outlines and the relations they suggest may be so evi-dent that the presence of fragments, hypochromic microcytic, macrocytic, or dimorphic red cells, as well as different combina-tions, can be presumed. In addition, the histogram provides a concise idea not only of the different sizes of cells but also of the distribution of cells from the center (MCV) and the spread (RDW), as these 2 CBC parameters are determined from the red cell histogram.13,29,30 Consequently, whatever instrument methods are used to obtain the red cell histogram, electrical impedance or optical flow cytometry, the relationship of the different sizes of cells can be readily delineated and contrasted, especially when a dotted line of reference normal is superim-posed on all automated abnormal red cell histogram results.
From reviewing the histograms, one can get a good idea of what to expect when actually evaluating the peripheral blood film. Unfortunately, most technologists have a limited under-standing in correlating the graphic displays with the morpholog-ical findings.31 This is probably because graphical representation of results, such as scatter plots or histograms, have been largely ignored in favor of the RDW, hemoglobin distribution width, and reticulocyte hemoglobin content that provide very useful information along with the red cell indices that have been tradi-tionally used.5,32,33 In fact, in some laboratories histograms are not being used when evaluating red cell morphology.
Moreover, there have been very few studies on the utility of red cell histograms in identifying common hematological disorders,3 with most studies favoring white cell histograms and their use in identifying and characterizing leukemic blast populations.34 Hopefully, the analysis and interpretations of histograms in this article provide good guidance in correlating histograms with microscopical findings.
The speed and reliability of the modern analyzers allow technologists time to evaluate abnormal blood films, consider diagnostic clues, and correlate clinical findings to histograms and other hematologic parameters with greater confidence and efficiency, all of which produce high returns in terms of patient health care. LM
1. Bessman JD, Gilmer PR Jr, Gardner FH. Improved classification of anemias by MCV and RDW. Am J Clin Pathol. 1983;80:322-326.
2. Williams LJ. Cell histograms: New trends in data interpretation and classification. J Med Technol. 1984;3:189-197.
3. Fossat C, David M, Harle JR, et al. New parameters in erythrocyte counting. Value of histograms. Arch Pathol Lab Med. 1987;111:1150-1154.
4. Lawrence A, Young M, Cooper A, et al. Red cell histograms in the diagnosis of diseases. In: Simpson E, ed. Hematology Beyond the Microscope. New York, NY: Technicon Instruments; 1984:155-164.

CE Update
308 LABMEDICINE ■ Volume 42 Number 5 ■ May 2011 labmedicine.com
5. Kakkar N, Makkar M. Red cell cytograms generated by an ADVIA 120 automated hematology analyzer: Characteristic patterns in common hematological conditions. LabMed. 2009;40:549-555.
6. Novak R. Q & A What is the significance of two distinct RBC populations aside from the obvious transfusion? In: Savage RA, ed. CAP Today. September 2005.
7. Gulati GL, Hyun BH. The automated CBC. A current perspective. Hematol Oncol Clin North Am. 1994;8:593-603.
8. Rees MI, Worwood M, Thompson PW, et al. Red cell dimorphism in a young man with a constitutional chromosomal translocation t(11;22)(p15.5;q11.21). Br J Haematol. 1994;87:386-395.
9. Bessman D. Erythropoiesis during recovery from iron deficiency: Normocytes and macrocytes. Blood. 1977;50:987-993.
10. Bessman JD. Erythropoiesis during recovery from macrocytic anemia: macrocytes, normocytes, and microcytes. Blood. 1977;50:995-1000.
11. Fishleder AJ, Hoffman GC. Automated hematology: Counts and indices. Lab Management. 1984;22:21-36.
12. Bessman JD, Banks D. Spurious macrocytosis, a common clue to erythrocyte cold agglutinins. Am J Clin Pathol. 1980;74:797-800.
13. Beckman Coulter LH 780 on line IB072841. Beckman Coulter Education Center, Miami Lakes, FL; 2007.
14. Munro BH. Statistical Methods for Health Care Research. 5th ed. New York, NY: Lippincott Williams and Wilkins; 2005,
15. Bate I, Bains BJ. Basic hematological techniques. In: Bates I, Bain BJ, Lewis SM, eds. Dacie and Lewis Practical Hematology. 9th ed. London: Churchill Livingstone; 2001:19-46.
16. Rowan RM. Blood Cell Volume Analysis—A New Screening Technology for the Hematologist. London: Albert Clark and Company; 1983:43-55.
17. Chaplin H, Glazer H, Hockett R, et al. Clinicopathologic conference: Abdominal pain, total intravascular hemolysis, and death in a 53-year-old woman. Am J Med. 1990;88:667-674.
18. Bessman JD. Red blood cell fragmentation. Improved detection and identification of causes. Am J Clin Pathol. 1988;90:268-273.
19. Steele BW, Wu NC, Whitcomb C. White blood cell and platelet counting performance by hematology analyzers: A critical evaluation. Lab Hematol. 2001;7:255-266.
20. Constantino BT, Cogionis B. High mean corpuscular hemoglobin concentration: Its causes and effects on automated CBC results. Can J Med Lab Sci. 2007;69:113-126.
21. Constantino BT. The evaluation and differentiation of hypochromic microcytic red blood cells of thalassemia trait and iron deficiency anemia. Can J Med Lab Sci. 1999;61:112-121.
22. Brigden ML. A systematic approach to macrocytosis: Sorting out the causes. Postgrad Med. 1995;97:171-184.
23. Gulati G. Blood Cell Morphology Grading Guide. Chicago, IL: ASCP Press; 2009:10-11.
24. Troubleshooting Guide Sysmex XE-Series Automated Hematology Systems Document number: MKT-40-1010. Sysmex America Inc.; 2004.
25. Bessman JD. Heterogeneity of red cell volume: Quantitation, clinical correlations, and possible mechanisms. Johns Hopkins Med J. 1980;146:226-230.
26. Park KI, Kim KY. Clinical evaluation of red cell volume distribution width (RDW). Yonsei Med J. 1987;28:282-290.
27. Ramos MC, Schafernak KT, Peterson LC. Hereditary pyropoikilocytosis: A rare but potentially severe form of congenital hemolytic anemia. J Pediatr Hematol Oncol. 2007;29:128-129.
28. Cochran DL, Burnside LK. Detecting and identifying hereditary pyropoikilocytosis. LabMed. 1999;30:26-29.
29. ADVIA 120 Hematology System “Technology and cytogram interpretation.” Bayer Diagnostics, Tarrytown, NY; 2005.
30. CELL DYN Sapphire TM System Operator Manual. Abbott Park, IL: Abbott Laboratories; 2005.
31. Sullivan E. Hematology analyzer: From workhorse to thoroughbred. LabMed. 2006;37:273-278.
32. Radtke H, Meyer T, Kalus U, et al. Rapid identification of iron deficiency in blood donors with red cell indexes provided by Advia 120. Transfusion. 2005;45:5-10.
33. Marković M, Majkić-Singh N, Subota V, et al. Reticulocyte hemoglobin content in the diagnosis of iron deficiency anemia. Clin Lab. 2004;50:431-436.
34. Krause JR, Costello RT, Krause J, et al. Use of the Technicon H-1 in the characterization of leukemias. Arch Pathol Lab Med. 1988;112:889-894.