The Rate of Hemorrhagic Transformation and Safety of ...
125
The Rate of Hemorrhagic Transformation and Safety of Antithrombotic Therapy in Pediatric Cardioembolic Arterial Ischemic Stroke by Elizabeth Pulcine A thesis submitted in conformity with the requirements for the degree of Master of Science Institute of Medical Science University of Toronto © Copyright by Elizabeth Pulcine 2019
Transcript of The Rate of Hemorrhagic Transformation and Safety of ...

The Rate of Hemorrhagic Transformation and Safety of
Antithrombotic Therapy in Pediatric Cardioembolic Arterial
Ischemic Stroke
by
Elizabeth Pulcine
A thesis submitted in conformity with the requirements
for the degree of Master of Science
Institute of Medical Science
University of Toronto
© Copyright by Elizabeth Pulcine 2019

Pulcine ii
The Rate of Hemorrhagic Transformation and Safety of
Antithrombotic Therapy in Pediatric Cardioembolic Arterial
Ischemic Stroke
Elizabeth Pulcine
Master of Science
Institute of Medical Sciences
University of Toronto
2019
Abstract
Antithrombotic therapy (ATT) is currently recommended for stroke prevention in pediatric
cardioembolic arterial ischemic stroke (CE-AIS). Rates of hemorrhagic transformation (HT) in
pediatric CE-AIS are unknown. This single-center retrospective study of CE-AIS in children
evaluated factors associated with HT to explore the relationship between ATT, HT and clinical
outcome. Eighty-two children met inclusion criteria [male 44 (54%); neonates 23 (28%); median
age 0.43 years (0.08 – 4.23)]. HT occurred in 20 of 82 children (24%), 5 (6%) of whom had
symptomatic intracranial hemorrhage. Four (5%) had major systemic hemorrhage. HT was not
associated with antiplatelet vs. anticoagulant use nor combination therapy. Children with
univentricular physiology were less likely to have HT [10% vs. 90%; p=0.03] and had higher
rates of recurrent stroke, prior to definitive cardiac repair, despite receiving ATT. However, the
risk-benefit ratio of ATT remains unknown in the context of each primary cardiac diagnosis and
warrants further study.

Pulcine iii
Acknowledgments
This thesis is the result of the collaborative support of many mentors, colleagues, family and
friends.

Pulcine iv
Statement of Contributions
Study Design: Gabrielle deVeber
Nomazulu Dlamini
Mahendranath Moharir
Leonardo Brandão
Michael Seed
Database Management: Allyssa Johnston
Alexandra Linds
Kathleen Mounce
Clinical Data Abstraction: Scherazad Musaphir
Sujatha Parthasarathy
Radiological Assessment: Manohar Shroff
Sunitha Palasamudram
Statistical Analysis: Mahmoud Slim
Funding Sources: This research was supported by the Thrombosis
Canada CanVECTOR Fellowship 2018-2019

Pulcine v
Table of Contents
Acknowledgments ................................................................................................................ iii
Statement of Contributions ................................................................................................... iv
Table of Contents .................................................................................................................. v
List of Abbreviations ............................................................................................................. ix
List of Tables ........................................................................................................................xii
List of Figures ...................................................................................................................... xiv
Chapter 1 .............................................................................................................................. 1
Background ................................................................................................................... 1
1.1 Arterial Ischemic Stroke in Neonates and Children ..............................................................1
1.1.1 Incidence ................................................................................................................................................ 1
1.1.2 Pathophysiology .................................................................................................................................... 2
1.1.3 Risk Factors ............................................................................................................................................ 2
1.2 Cardioembolic Arterial Ischemic Stroke in Children .............................................................3
1.2.1 Thrombosis Risk Factors in Children with Congenital Heart Disease..................................................... 3
1.2.2 Thrombosis Risk Factors in Adults with Congenital Heart Disease ........................................................ 5
1.2.3 Thrombosis Risk Factors in Children and Adults with Acquired Heart Disease ..................................... 6
1.3 Hemostasis in Children .......................................................................................................8
1.3.1 Differences in the Coagulation System of Children with Congenital Heart Disease ............................ 10
1.4 Acyanotic Congenital Heart Disease and Thrombosis Risk ................................................. 11
1.5 Cyanotic Congenital Heart Disease and Thrombosis Risk According to Different Stages of
Cardiovascular Surgery ................................................................................................................. 12
1.5.1 Norwood and Blalock-Taussig Shunt (Stage I Palliation) ..................................................................... 12
1.5.2 Bidirectional Cavopulmonary Anastomosis (Stage II Palliation) .......................................................... 13
1.5.3 Fontan (Stage III Palliation) .................................................................................................................. 14
1.5.4 Thromboprophylaxis Across All Stages of Cardiovascular Surgery ...................................................... 15

Pulcine vi
1.6 Cardiac Catheterization .................................................................................................... 16
1.7 Cardiopulmonary Bypass .................................................................................................. 17
1.8 Extracorporeal Membrane Oxygenation ........................................................................... 18
1.9 Ventricular Assist Devices ................................................................................................ 19
1.10 Prevention and Treatment of Arterial Ischemic Stroke in Children with Cardiac Disease ..... 20
1.10.1 Antiplatelet Therapy ....................................................................................................................... 21
1.10.2 Anticoagulant Therapy .................................................................................................................... 22
1.10.3 Tissue Plasminogen Activator ......................................................................................................... 24
1.10.4 Mechanical Thrombectomy ............................................................................................................ 24
1.11 Prior Data on Antithrombotic Safety and Risk of Hemorrhagic Transformation in Children
with Arterial Ischemic Stroke........................................................................................................ 25
1.12 Hemorrhagic Transformation in Adults with Arterial Ischemic Stroke ................................ 28
1.12.1 Pathophysiology of Hemorrhagic Transformation .......................................................................... 30
1.13 Summary of Key Points .................................................................................................... 31
Chapter 2 ............................................................................................................................ 32
Research Aims and Hypothesis ..................................................................................... 32
2.1 Rationale and Objectives .................................................................................................. 32
2.1.1 Primary Study Aim ............................................................................................................................... 33
2.1.2 Secondary Study Aim ........................................................................................................................... 33
2.2 Research Questions and Hypothesis ................................................................................. 33
2.2.1 What is the rate of HT amongst neonates and children with CE-AIS? ................................................. 33
2.2.2 What are the clinical factors associated with HT amongst neonates and children with CE-AIS? ........ 34
2.2.3 What are the radiological factors associated with HT amongst neonates and children with CE-AIS? 34
2.2.4 What is the rate of stroke recurrence in neonates and children with cardiac disease and CE-AIS? ... 34
2.2.5 Is asymptomatic and/or symptomatic HT associated with worse clinical outcome and death?......... 35
Chapter 3 ............................................................................................................................ 36
Methods ...................................................................................................................... 36

Pulcine vii
3.1 Study Population and Design ............................................................................................ 36
3.2 Ethics Approval ................................................................................................................ 36
3.3 Criteria for Study Participants .......................................................................................... 36
3.4 Data Collection ................................................................................................................ 37
3.5 Cardioembolic Arterial Ischemic Stroke Definition and Subtype ........................................ 37
3.6 Infarct Size Analysis ......................................................................................................... 38
3.7 Hemorrhagic Transformation Analysis .............................................................................. 39
3.8 Antithrombotic Therapy ................................................................................................... 40
3.9 Stroke Recurrence ............................................................................................................ 41
3.10 Neurological Outcome ..................................................................................................... 41
3.11 Statistical Analysis ........................................................................................................... 41
Chapter 4 ............................................................................................................................ 43
Results ......................................................................................................................... 43
4.1 Patient Characteristics ..................................................................................................... 43
4.1.1 Blood Pressure ..................................................................................................................................... 44
4.2 Cardiac Diagnosis and Interventional Procedures .............................................................. 44
4.2.1 Cardiac Diagnosis ................................................................................................................................. 44
4.2.2 Procedural Risk .................................................................................................................................... 46
4.3 Radiological Features ....................................................................................................... 51
4.3.1 Imaging Timing and Modalities............................................................................................................ 51
4.3.2 Stroke Characteristics .......................................................................................................................... 52
4.3.3 Modified Pediatric ASPECTS – Stroke Volume ..................................................................................... 53
4.4 Hemorrhagic Transformation and ECASS .......................................................................... 53
4.5 Antithrombotic Therapy ................................................................................................... 63
4.6 Arterial Ischemic Stroke Recurrence ................................................................................. 67

Pulcine viii
4.7 Outcome ......................................................................................................................... 67
Chapter 5 ............................................................................................................................ 71
Discussion .................................................................................................................... 71
5.1 General Discussion ........................................................................................................... 71
5.1.1 Patient Characteristics ......................................................................................................................... 72
5.1.2 Cardiac Diagnosis and Interventional Procedures ............................................................................... 73
5.1.3 Radiological Features ........................................................................................................................... 78
5.1.4 Hemorrhagic Transformation .............................................................................................................. 79
5.1.5 Antithrombotic Therapy ...................................................................................................................... 83
5.1.6 Arterial Ischemic Stroke Recurrence ................................................................................................... 85
5.1.7 Neurological Outcome ......................................................................................................................... 87
5.2 Study Strengths ............................................................................................................... 88
5.3 Study Limitations ............................................................................................................. 89
Conclusion ........................................................................................................................... 91
Future Directions ................................................................................................................. 92
References........................................................................................................................... 94
Appendix – The Hospital for Sick Children Arterial Ischemic Stroke Guidelines .................... 102

Pulcine ix
List of Abbreviations
ACT – Activated Clotting Time
ACT – Anticoagulant Therapy
AIS – Arterial Ischemic Stroke
AoV/MV – Aortic/Mitral Valve Abnormalities
APT – Antiplatelet Therapy
AS – Aortic Stenosis
ASA – Aspirin
ASD – Atrial Septal Defect
ATT – Antithrombotic Therapy
AVSD – Atrioventricular Septal Defect
BAS – Balloon Atrial Septostomy
BCPS – Bidirectional Cavopulmonary Shunt
BTS – Blalock–Taussig Shunt
CCHB – Congenital Complete Heart Block
ccTGA – Congenitally Corrected Transposition of the Great Arteries
CE – Cardioembolic
CE-AIS – Cardioembolic Arterial Ischemic Stroke
CHD – Congenital Heart Disease
CI – Confidence Interval
CNS – Central Nervous System
CoA – Coarctation of the Aorta/Aortic Arch Abnormalities
COX-1 – Cyclooxygenase-1
CPB – Cardiopulmonary Bypass
CT – Computed Tomography
DORV – Double Outlet Right Ventricle
DWI – Diffusion-Weighted Imaging
ECASS – European Cooperative Acute Stroke Study
ECMO – Extracorporeal Membrane Oxygenation

Pulcine x
HLHS – Hypoplastic Left Heart Syndrome
HR – Hazard Ratio
ICH – Intracranial Hemorrhage
IE – Infective Endocarditis
INR – International Normalized Ratio
IPSS – International Paediatric Stroke Study
IQR – Interquartile Range
IV – Intravenous
IVH – Intraventricular Hemorrhage
IVS – Intact Ventricular Septum
LPA – Left Pulmonary Artery
LMWH – Low Molecular Weight Heparin
MCA – Middle Cerebral Artery
MRI – Magnetic Resonance Imaging
MTHFR – Methylenetetrahydrofolate Reductase
NIHSS – National Institutes of Health Stroke Scale
NINDS – National Institute of Neurological Disorders and Strokes
OHT – Orthotopic Heart Transplant
OR – Odds Ratio
PA – Pulmonary Atresia
PA/IVS – Pulmonary Atresia with Intact Ventricular Septum
PFO – Patent Foramen Ovale
PO – By Mouth
PS – Pulmonary Stenosis
PT – Prothrombin Time
PTT – Partial Thromboplastin Time
RR – Relative Risk
SAH – Subarachnoid Hemorrhage
SC – Subcutaneous
SDH – Subdural Hemorrhage

Pulcine xi
SV – Single Ventricle
SVP – Single Ventricle Physiology
SWI – Susceptibility Weighted Imaging
TA – Tricuspid Atresia
TAPVC – Total Anomalous Pulmonary Venous Connection
TEG – Thromboelastography
TGA – Transposition of the Great Arteries
TIA – Transient Ischemic Attack
TIPS – Thrombolysis in Pediatric Stroke
TOF – Tetralogy of Fallot
tPA – Tissue Plasminogen Activator
UFH – Unfractionated Heparin
VAD – Ventricular Assist Device
VSD – Ventricular Septal Defect

Pulcine xii
List of Tables
Table 1. Incidence data for arterial ischemic stroke and stroke associated with cardiac disease in
neonates and children from different geographical regions.
Table 2. Summary of hemorrhagic transformation rates and associated risk-factors in two
pediatric cohort studies by Beslow et al 2011 and Schecter et al 2012.
Table 3. Baseline patient characteristics and primary cardiac diagnoses.
Table 4. Additional breakdown of the primary cardiac diagnoses.
Table 5. Additional cardiac, non-cardiac and procedural risk factors associated with
cardioembolic arterial ischemic stroke.
Table 6. Details of additional cardiac, non-cardiac and procedural risk factors associated with
cardioembolic arterial ischemic stroke.
Table 7. Radiological features of pediatric cardioembolic arterial ischemic stroke.
Table 8. Salient demographic, clinical, neuroimaging and follow-up details of cardioembolic
stroke patients with hemorrhagic transformation divided by the presence of hemorrhage on initial
or follow-up neuroimaging.
Table 9. Categories of antithrombotic treatment including commencement, escalation or no
change to ongoing therapy for secondary stroke prevention.
Table 10. Additional details of the type of antithrombotic treatment pre and post radiological
diagnosis of cardioembolic arterial ischemic stroke.
Table 11. Type of antithrombotic therapy at the time of stroke recurrence.
Table 12. Type of cardiac physiology at the time of stroke recurrence.

Pulcine xiii
Table 13. Comparison of hemorrhagic transformation rates from three retrospective studies in
children with arterial ischemic stroke including our own.

Pulcine xiv
List of Figures
Figure 1. Methods flow chart.
Figure 2. Rate of procedure-related stroke based on a 30-day vs. 72-hour definition.
Figure 3. Details of palliative cardiac surgery associated with procedural CE-AIS.
Figure 4. Details of definitive cardiac surgery associated with procedural CE-AIS.
Figure 5. Frequency of procedure-related stroke based on a 30-day definition over a 14-year
period (2003 – 2017).
Figure 6. ECASS classification of hemorrhagic transformation.
Figure 7. Representative CT scans showing types of hemorrhagic transformation.
Figure 8. Timing of hemorrhagic transformation from initial radiological stroke diagnosis
distributed by type of antithrombotic therapy at the time of hemorrhage.
Figure 9. Representative CT scan showing cortical laminar necrosis.
Figure 10. Representative CT scans showing other types of intracranial hemorrhage.
Figure 11. Details of the treatment decision for secondary stroke prevention and rates of
antithrombotic therapy-associated hemorrhage.
Figure 12. Indications for antithrombotic treatment at the time of cardioembolic arterial
ischemic stroke.
Figure 13. Neurological status at discharge.
Figure 14. Frequency distribution of neurological outcome compared to normal, mild and severe
ECASS grade.

Pulcine xv
Figure 15. Timing, cause of death and distribution of hemorrhagic transformation in deceased
patients.

Pulcine 1
Chapter 1
Background
1.1 Arterial Ischemic Stroke in Neonates and Children
1.1.1 Incidence
Arterial ischemic stroke (AIS) can happen at any age with the highest risk of stroke across the
pediatric lifespan occurring in the neonatal period (Bernson-Leung & Rivkin, 2016). When both
ischemic and hemorrhagic stroke subtypes are included in neonates and children, pediatric stroke
incidence rates range from 3 to 25 per 100 000 per year (Ferriero et al., 2019). The incidence of
ischemic stroke alone is estimated to be 1 in 2 500 to 1 in 4 000 live births in neonates (G. A.
deVeber et al., 2017; Ferriero et al., 2019) and 2 to 8 per 100 000 in children aged 28 days to 18
years (G. A. deVeber et al., 2017; Kirton & deVeber, 2015; Mallick et al., 2014). The incidence
is even higher in neonates and children with cardiac disease and is reported to be as high as 132
in 100 000 or 1 in 757 (Hoffman et al., 2011), which translates into a 17-fold increased risk
compared to that of the general pediatric population. Improved medical management and
surgical outcomes has decreased mortality but contributed to a greater lifetime exposure of
thromboembolic complications (Hoffman et al., 2011). Amongst different types of cardiac
diagnosis, those with cyanotic congenital heart disease, especially with right-to-left shunting and
single ventricle physiology appear to be at greatest risk of AIS with a stroke incidence rate of
1380 in 100 000 or 1 in 72 (Hoffman et al., 2011). Table 1 summarizes the overall incidence of
AIS and incidence of AIS associated with cardiac disorders in children from previous studies.
Study Cohort Overall Incidence
(Giroud et al., 1995) Childhood AIS (France) 13/100 000
(G. deVeber, 2000) Childhood AIS (Canada) 2.6/100 000
(Agrawal, Johnston, Wu,
Sidney, & Fullerton, 2009)
Childhood Hemorrhagic
Stroke and AIS (USA)
2.3 – 4.6/100 000
(Hoffman et al., 2011) All Cardiac AIS (USA) 132/100 000
(Hoffman et al., 2011) Single Ventricle AIS (USA) 1380/100 000

Pulcine 2
(G. A. deVeber et al., 2017) Childhood AIS (Canada) 1.72/100 000
(G. A. deVeber et al., 2017) Neonatal AIS (Canada) 10.2/100 000 live births
Table 1. Incidence data for arterial ischemic stroke and stroke associated with cardiac disease in
neonates and children from different geographical regions.
1.1.2 Pathophysiology
Arterial ischemic stroke occurs due to interruption of blood flow to the brain. This can occur in
one of two ways: (1) from an embolus which originates elsewhere in the body, such as the heart,
or a vein if there is a venous-to-arterial shunt; or (2) from thrombosis in situ, frequently in the
setting of arteriopathy or hypercoagulable state due to inflammation (Amlie-Lefond, 2018;
Bernson-Leung & Rivkin, 2016). In neonates and children with CE-AIS the presumed
mechanism is often embolic; however, in-situ arterial thrombosis may also play a role (Dowling
et al., 2013). This is because children with cardiac disease often have underlying chronic
conditions including anemia, polycythemia, hypoxemia, recurrent infections, procedural
interventions and mechanical circulatory support, predisposing them to acquired pro-
inflammatory or pro-thrombotic states.
1.1.3 Risk Factors
Much of adult AIS is caused by the interaction of traditional risk factors including
atherosclerosis, hypertension, dyslipidemia, obesity, diabetes mellitus and cigarette smoking
(Ferriero et al., 2019). Unlike the acquired cardiovascular risk factors in adults, pediatric
ischemic stroke etiologies consist of primarily congenital cardiac disorders, genetic or acquired
abnormalities of the cerebral arteries, known as arteriopathies, sickle cell disease, thrombophilia
and chronic systemic disease such as lupus (Andrade, Yau, & Moharir, 2015; Bernson-Leung &
Rivkin, 2016). About 50 – 80% of children with AIS have at least one of these risk factors
(Andrade et al., 2015; Mackay et al., 2011) and in the majority of cases multiple stroke risk
factors are identified. With current approaches to etiological investigations, only 9% of children
will have no risk factors identified (Mackay et al., 2011). Up to 50% of all childhood AIS is
associated with cerebral arteriopathies and up to 30% with cardiac disease (acquired and
congenital), both of which predict increased rates of recurrent stroke (Amlie-Lefond, 2018). For
this reason, antithrombotic therapy is typically recommended for stroke prevention. Stroke

Pulcine 3
recurrence despite antithrombotic therapy is known, including in CE-AIS (Rodan et al., 2012).
Therefore, a better understanding of the risks, benefits and potential additive and synergistic
effects of multiple risk factors on current antithrombotic therapy is required in pediatric CE-AIS.
1.2 Cardioembolic Arterial Ischemic Stroke in Children
Cardioembolic stroke accounts for 20-30% of all ischemic strokes in adults (O'Carroll & Barrett,
2017) and up to 30% of ischemic strokes in children (Sinclair et al., 2015). Cardioembolic stroke
can arise via different pathophysiological mechanisms, including formation of a mural thrombus
in a dyskinetic ventricle, clot formation or vegetation on an abnormal heart valve, arrhythmia
resulting in pooling of blood and non-laminar flow or paradoxical embolism of a venous
thrombus in right-to-left shunting due to congenital structural heart defects (Ferriero et al., 2019;
Giglia et al., 2013; Roach et al., 2008; Sinclair et al., 2015). In adults ischemic heart disease with
myocardial infarction is the most common predisposing cause for these mechanisms.
Dowling et al found that, compared to children with other stroke etiologies, children with cardiac
disease are younger at presentation and are more likely to have a cardioembolic stroke pattern on
imaging defined as multiple, bilateral and involving both the anterior and posterior circulation
(Dowling et al., 2013).
1.2.1 Thrombosis Risk Factors in Children with Congenital Heart Disease
The incidence of CHD is 4 to 10 cases per 1 000 live births in the United States (Go et al., 2014).
Similarly, about 1 in 100 children in Canada are born with CHD (Irvine, Luo, & Leon, 2015).
Congenital heart defects are structural problems which result from abnormal formation of the
heart or major blood vessels that arise from the heart. They range in severity from small
connections between two chambers of the heart, for example atrial septal defects, which may
spontaneously close over time, to complex malformations that require multiple corrective or
palliative surgeries, both of which are life-limiting (Go et al., 2014).
Children with CHD are at high risk of developing thrombosis and the risk can vary over the
lifespan (Sinclair et al., 2015). This increased propensity to thrombosis is perhaps best explained
by the interaction of three important variables historically described by Rudolph Virchow:
alterations in blood flow; alterations in blood composition; and endothelial injury (Giglia et al.,
2013; Sinclair et al., 2015). Alterations in blood flow can result from the presence of a

Pulcine 4
hypoplastic ventricle or a severely dilated atrium limiting the ability for inflow and outflow and
resulting in a non-laminar, turbulent circulation. Alterations in blood composition have long been
noted in children with CHD with a greater frequency of genetic and acquired thrombophilias
compared to healthy controls (Strater et al., 1999). Finally, endothelial injury can result from
presence of a central venous catheter, mechanical circulatory support, or sutures from cardiac
surgery which expose the blood to artificial thrombogenic material (Sinclair et al., 2015).
Perhaps the most important risk factor in developing thrombosis depends on the type of
structural cardiac defect. As early as 1961 unrepaired tetralogy of Fallot (TOF) was recognized
as one of the most important risk factors in patients with AIS due to the right-to-left intracardiac
shunting needed to sustain adequate cardiac output (Martelle & Linde, 1961). Although stroke
has been associated with most types of acquired and congenital cardiac disease, cyanotic and
single ventricle heart defects are at highest risk due to formation of intracardiac thrombi and
paradoxical embolism due to right-to left shunting (Bernson-Leung & Rivkin, 2016). In order to
to repair many types of single ventricle heart defects including hypoplastic left heart syndrome
(HLHS), tricuspid atresia (TA) and pulmonary atresia with intact ventricular septum (PA/IVS),
surgeons often perform a series of staged open-heart procedures over several years to allow the
heart to function as a one-sided pump with two chambers (Allen D. Everett, 2011). Cardiac
surgery itself poses a significant thromboembolic risk in addition to a risk of global hypoxic-
ischemic injury. During surgical repair, the use of cardiopulmonary bypass (CPB) is often
necessary. CPB temporarily exposes the patient’s blood to plastic tubing and other thrombogenic
materials in the artificial circulatory system (Silvey & Brandao, 2017). This results in activation
and aggregation of platelets and the fibrin-forming coagulation system with subsequent thrombus
formation within the tubing or circuitry of the machine. A retrospective study from our tertiary
care centre (The Hospital for Sick Children, Toronto, Ontario, Canada) examined 5 526 children
with congenital heart disease who underwent cardiac surgery from 1992 – 2001 and found that
the incidence of ischemic stroke (28 with arterial ischemic stroke and 2 with cerebral sinus
venous thrombosis) was 5.4 per 1 000 children from 1992 – 2001 (Domi et al., 2008). Risk
factors associated with procedural stroke included older age at the time of the surgery, longer
duration of CPB, reoperation and number of days hospitalized after the operation (Domi et al.,
2008). The authors hypothesized that children who require reoperation likely have more severe
underlying cardiac disease placing them at higher risk for procedure-related complications

Pulcine 5
(Domi et al., 2008). More recently, Asakai et al examined 76 children from Melbourne, Australia
with cardiac disease and radiologically-confirmed AIS and found that stroke occurred in 68%
(95% CI: 58% – 79%) of children following cardiac procedures (Asakai et al., 2015). This
translated into 4.6 strokes per 1 000 surgical procedures and 1.7 strokes per 1 000 cardiac
catheterizations from 1993 – 2010 (Asakai et al., 2015). The authors concluded that the
prevalence of procedural stroke was highest in patients with cyanotic CHD undergoing palliative
surgery, which is consistent with previously published literature (Asakai et al., 2015). It remains
unknown which individual patient characteristics further alter the risk of stroke in the procedural
period, for instance, congenital or acquired resistance to antithrombotic therapy. In infants and
young children, normal developmental changes in the hemostatic system may also contribute to
this risk and will be discussed in a later section.
Stroke recurrence in CHD is as high as 27% at 10 years and can occur even in children on
antithrombotic therapy (Rodan et al., 2012). Rodan et al showed that the recurrence risk was
highest in the period immediately following the sentinel stroke and decreased with time (Rodan
et al., 2012). Similarly, Asakai et al found a 17% rate of stroke recurrence amongst children with
cardiac disease at a median time of 21 days from the sentinel event (IQR 10.5 – 141 days) with a
smaller follow-up interval (Asakai et al., 2015). For this reason, antithrombotic therapy is
recommended by several consensus-based guidelines (Ferriero et al., 2019; Giglia et al., 2013;
Monagle et al., 2012; Roach et al., 2008) for secondary stroke prevention following CE-AIS.
However, the duration of ATT remains institution dependent and ranges from at least 3-months
post-stroke and thereafter for 2-5 years to sometimes even lifelong following CE-AIS at our
tertiary care center (The Hospital for Sick Children, Toronto, Ontario, Canada, unpublished
observations). Studies have shown that stroke recurrence can occur many years following
surgery, sometimes greater than 5 years after the most recent procedure (Fox, Sidney, &
Fullerton, 2015; Rodan et al., 2012), resulting in controversy in management and knowing when
it is safe to step-down, transition or stop antithrombotic therapy altogether.
1.2.2 Thrombosis Risk Factors in Adults with Congenital Heart Disease
Longer term studies of children surviving CHD show the increased risk for thromboembolism
persists into adulthood. Studies have shown that the stroke risk continues to be elevated in adult
CHD survivors many years after staged palliative cardiac repair with a prevalence of 0.05% per-

Pulcine 6
patient year (Hoffmann et al., 2010). Although this prevalence may appear low, when compared
to the general population of similar age this is 10 – 100 times higher (Hoffmann et al., 2010). In
addition to the risk factors commonly seen in neonates and children, including right-to-left
shunting, adult specific risk factors are unique and include atrial fibrillation, ventricular
dysfunction and arrhythmias, Fontan circulation complicated by protein-losing enteropathy,
pregnancy and the use of estrogen containing oral contraception (Giglia et al., 2013; Kirsh,
Walsh, & Triedman, 2002).
1.2.3 Thrombosis Risk Factors in Children and Adults with Acquired Heart Disease
Acquired heart disease leads to stroke in up to 20% of children (Bernson-Leung & Rivkin, 2016;
Roach et al., 2008). Acquired cardiac disease includes valvular heart disease, endocarditis,
cardiac tumours, cardiac arrhythmias and cardiomyopathy. Other rarer etiologies are beyond the
scope of this review. Valvular heart disease may arise from rheumatic, infective, prosthetic,
myxomatous and congenital disorders (Roach et al., 2008). Although rheumatic heart disease is
less common since the advent of antibiotics, the lifetime thromboembolic risk from untreated
rheumatic mitral stenosis is significantly elevated at 20% (Roach et al., 2008). Interestingly,
adults with uncomplicated mitral valve prolapse comprise 2 – 3 % of the general population and
do not have an increased risk of embolic stroke (Orencia et al., 1995). In the absence of
rheumatic heart disease, this finding appears to be also true in children (Roach et al., 2008). It is
well recognized that both adults and children with prosthetic heart valves in the systemic
circulation (aortic, mitral or both) are at an increased risk of both thromboembolic stroke and
endocarditis (Roach et al., 2008). Children with placement of mechanical heart valves require
long-term oral anticoagulation (Giglia et al., 2013). In children, valve replacement is performed
for the treatment of both acquired and congenital heart disease and replacement valves may be
tissue or mechanical in nature (Giglia et al., 2013). As a general rule, mechanical valves used for
systemic valve replacement require anticoagulation to prevent thromboembolic complications in
both children and adults (Giglia et al., 2013). One retrospective study of 48 children receiving a
bileaflet mechanical valve on the systemic side, while not on any anticoagulation, identified a
thromboembolic risk of 5.7 ± 2.1% per-patient year (Sade, Crawford, Fyfe, & Stroud, 1988).

Pulcine 7
Neurological complications occur at a frequency of 20 to 40% in patients with infective
endocarditis involving the left-side of the heart and stroke accounts for about half of those
complications (Roach et al., 2008). Pathophysiological mechanisms include septic emboli,
infective aneurysmal formation and vasculitis (Roach et al., 2008). For this reason it is generally
recommended to avoid anticoagulation in infective endocarditis because of the high risk of
hemorrhagic stroke from septic aneurysmal dilatation of major intracerebral arteries (Roach et
al., 2008).
Cardiac myxomas are the most common primary cardiac tumors in adults. On the other hand, in
children, rhabdomyomas are the most common primary cardiac tumours (Roach et al., 2008).
Although cardiac rhabdomyomas occur in two thirds of children with tuberous sclerosis and
occasionally as an isolated lesion, only a few of these children have developed a stroke (Butany
et al., 2005). As a result, these children do not typically receive prophylactic antithrombotic
therapy; however, the factors predicting increased stroke risk in this condition are not entirely
clear.
Although arrhythmias are not as prevalent in neonates and children compared to the general adult
population various types of arrhythmias have been described in children with stroke. Atrial
fibrillation has been reported to occur more frequently in children with hyperthyroidism,
rheumatic heart disease and post-palliative repair of univentricular congenital heart disease
(Giglia et al., 2013; Roach et al., 2008). Pediatric and adult CHD patients who have surgery
involving their atria are particularly at increased risk for intra-atrial reentrant tachycardia (Giglia
et al., 2013). Not surprisingly, for this reason, atrial fibrillation in young people is most often
associated with CHD (Radford & Izukawa, 1977). Kirsh et al demonstrated that 20% of children
with CHD that required cardioversion had atrial fibrillation (Kirsh et al., 2002). The presence of
a thrombus in the left atrial appendage is a well-established risk factor for embolic stroke (Giglia
et al., 2013). To date there are no published studies of anticoagulation therapy in pediatric
patients with atrial arrhythmias and adult literature is often used to guide their management.
Children with cardiomyopathy have an increased risk of thrombus formation and embolism. This
is primarily due to reduction in the ejection fraction, resulting in low cardiac output and/or focal
wall-motion abnormality leading to formation of a thrombus in a dyskinetic ventricle. Thrombi
are most commonly found in the left ventricle, near the apex of the free wall, but can also occur

Pulcine 8
in the atria and right ventricle or in other vascular structures (Gunthard et al., 1997). Thrombus
formation can occur despite the use of prophylactic antithrombotic therapy. McCrindle et al
reviewed 66 children with dilated or inflammatory cardiomyopathy and found 9 (15%) with
thromboembolism. Four children had an intracardiac thrombus at presentation, 4 children who
developed an intracardiac thrombus during a follow-up period of 15 days – 2.8 months, and one
child who died and was found to have an intracardiac thrombus at autopsy (McCrindle et al.,
2006). Despite this, only 1 patient had CE-AIS (McCrindle et al., 2006). Those children with
thrombus formation had lower ejection fractions (21% vs. 29 %; p<0.05) and were more likely to
be given systemic anticoagulation (McCrindle et al., 2006). Among the 9 children with
thrombosis, 6 were receiving no anticoagulation (e.g. had thrombosis at presentation) and three
were receiving anticoagulation at thrombosis (sub-therapeutic in two and therapeutic in one).
Thrombus formation was not related to age at presentation, initial ejection fraction, ventricular
dysfunction, use of anticoagulation at presentation nor the duration of follow-up possibly due to
small sample size (McCrindle et al., 2006). Adults with cardiomyopathy have been demonstrated
to have increased fibrinopeptide A and thrombin-antithrombin complexes, both of which are
markers of activation of the coagulation cascade (Yamamoto et al., 1995). In adults with heart
failure with left ventricular ejection fraction of less than 35% and absence of arrhythmia, two
studies, the Warfarin and Antiplatelet Therapy in Chronic Heart Failure (WATCH) trial (Massie
et al., 2009) and Warfarin vs. Aspirin in Reduced Cardiac Ejection Fraction (WARCEF) trial
(Homma et al., 2012) showed that anticoagulation with warfarin had a slight advantage over
aspirin in preventing CE-AIS but this was at a cost of increased risk of major hemorrhagic
complications. There are no age-specific evidence-based data to support the current best stroke
prevention strategies and treatment recommendations in children with cardiomyopathy and
congestive heart failure, regardless of the etiology. The 2013 American Heart Association
(AHA) scientific statement on prevention and treatment of thrombosis in pediatric congenital
heart disease recommends treatment with systemic anticoagulation for at least three months if a
child has evidence of an intracardiac thrombus (Giglia et al., 2013).
1.3 Hemostasis in Children
The hemostatic system consists of platelets and numerous coagulation system proteins. When
these become activated, they form a thrombus via aggregation, producing a fibrin-platelet plug
(Andrew et al., 1988; Andrew et al., 1987; Andrew et al., 1992). Thereafter, this fibrin-platelet

Pulcine 9
plug is degraded via fibrinolysis. These pathways are modulated at every step by proteins that
serve as inhibitors and activators of the entire process (Andrew et al., 1988; Andrew et al., 1987;
Andrew et al., 1992). This ensures a fine balance between clotting and bleeding and prevents
pathologic thrombosis or fibrinolysis (Andrew et al., 1988; Andrew et al., 1987; Andrew et al.,
1992).
The coagulation system in neonates and infants is physiologically distinct from adults and this
phenomenon is termed developmental hemostasis (Andrew et al., 1988; Andrew et al., 1987;
Andrew et al., 1992). For this reason, it is important to consider age-appropriate ranges, where
available, when interpreting test results. Neonates and children have decreased protein C, protein
S and antithrombin which are natural inhibitors of the coagulations system (Andrew et al., 1988;
Andrew et al., 1987; Andrew et al., 1992). Term newborns and infants typically have low levels
of antithrombin, which can range from 20 – 80% of adult levels, and approach adult values at
around 6 months of age (Andrew et al., 1988; Andrew et al., 1987; Andrew et al., 1992). Despite
the decreased level of antithrombin, a coagulation inhibitor, this does not typically result in
thrombosis, possibly due to a similar decrease in other pro-coagulation factors (Andrew et al.,
1988; Andrew et al., 1987; Andrew et al., 1992; Giglia et al., 2013). Neonates and children are
also reported to have decreased tissue plasminogen activator (tPA), plasminogen and increased
plasminogen activator inhibitor protein type 1, which are all involved in fibrinolysis (Ferriero et
al., 2019). These proteins approach adult levels at around 12 months and in some instances only
reach adult norms in adolescence (Andrew et al., 1988; Andrew et al., 1987; Andrew et al.,
1992). Children with acyanotic CHD appear to reach age-appropriate levels more rapidly than
children with cyanotic CHD (Giglia et al., 2013; Silvey & Brandao, 2017). Differences in
platelet function have also been reported in neonates and children (Michelson, 1998). In
neonates, studies have shown that platelets appear to be hyporeactive to a number of platelet-
activating agents although the exact pathophysiology for this is unclear (Michelson, 1998).
Neonates and children with CHD may also develop acquired von Willebrand disease known to
affect platelet aggregation and testing (Silvey & Brandao, 2017).
When there are inherited or acquired deficiencies in platelets or the aforementioned proteins,
excessive thrombosis or fibrinolysis can occur resulting in excessive clotting or bleeding.
However, the extent of their contribution to CE-AIS remains unstudied.

Pulcine 10
1.3.1 Differences in the Coagulation System of Children with Congenital Heart Disease
Hyperviscosity often occurs in cyanotic CHD due to a phenomenon called decompensated
erythrocytosis (Tempe & Virmani, 2002). This occurs due to a cascade of physiological
processes that become overactive in the presence of chronic tissue hypoxemia. In an attempt to
increase tissue oxygenation, the kidneys release erythropoietin, a hormone that stimulates the
bone marrow to increase the production of red blood cells (Tempe & Virmani, 2002). In the
presence of a significant right-to-left shunt, erythropoietin continues to attempt to increase
normal tissue oxygenation by increasing red cell mass and hemoglobin concentration thereby
increasing blood viscosity and paradoxically reducing oxygen delivery (Tempe & Virmani,
2002). Normal systemic oxygen saturation is not usually achieved until after the Fontan
procedure. Chronic hypoperfusion of the liver results in impaired metabolism of coagulation
proteins and low-grade inflammation (Manlhiot et al., 2012). This leads to decreased levels of
hepatically-manufactured proteins: protein C, protein S and antithrombin (Silvey & Brandao,
2017). As CHD patients undergo corrective surgical procedures, their coagulation profile
continues to be altered (Silvey & Brandao, 2017). A study by Odegard et al showed that patients
with single-ventricle physiology were more likely to have thrombophilic abnormalities compared
with age-matched healthy controls at all three stages of their palliative surgical repair (Odegard
et al., 2009). The study found that most coagulation proteins were significantly lower but that
factor VIII levels increased after the Fontan (stage III palliation) procedure in children that were
longitudinally followed from their first stage of repair (Odegard et al., 2009). Increased factor
VIII levels have been demonstrated to be associated with an increased risk of thrombosis (Giglia
et al., 2013). However, it is not known from this study if the coagulation profile of these children
continues to change over the year post-Fontan or if this correlates with the risk of thrombotic
events (Odegard et al., 2009). Not surprisingly, genetic and acquired thrombophilias have been
reported to occur at a greater frequency in children with cardiac disease and AIS compared with
age-matched healthy controls (Strater et al., 1999). The reason for this is thought to be
multifactorial including those discussed above as well as due to increased consumption,
decreased production and increased fibrinolysis of proteins involved in hemostasis (Silvey &
Brandao, 2017). However, this does not explain why genetic thrombophilias are more common
in children with cardiac disease, with the exception of those with syndromic disease such as
Down syndrome, chromosome 8 deletion or duplication (Giglia et al., 2013) with known

Pulcine 11
abnormalities in the function of Factor VII. Specific reported abnormalities include elevated
lipoprotein (a), protein C deficiency, presence of anticardiolipin antibodies and combined
prothrombotic disorders (Strater et al., 1999).
Children with cyanotic CHD are also known to be at an increased risk of bleeding due to a
variety of factors including polycythemia, hyperviscosity, thrombocytopenia and platelet
function abnormalities (Giglia et al., 2013). CHD patients have been shown to have abnormal
platelet numbers and function for several reasons including hypoxic inhibition of platelet
production, increased platelet destruction, decreased platelet aggregation and known genetic
disorders such as Noonan’s syndrome which may present with both platelet dysfunction and
cardiac disease (Silvey & Brandao, 2017). Platelet survival has also been demonstrated to be
decreased in children with CHD: below 80 hours compared to a normal survival time of 80 to
130 hours (Waldman et al., 1975).
1.4 Acyanotic Congenital Heart Disease and Thrombosis Risk
Acyanotic CHD includes atrial septal defect (ASD), ventricular septal defect (VSD),
atrioventricular septal defect (AVSD) and various aortic arch abnormalities including coarctation
of the aorta (CoA). Children with acyanotic CHD are less likely to undergo repeated cardiac
surgery with CPB, depending on the type of septal structural defect, as a number of them
spontaneously close (Silvey & Brandao, 2017). For this reason, they are less likely to have
thromboembolic complications. However, they are still at risk of paradoxical embolism due to
transient increases in right atrial pressure with right-to-left shunting, should a septal defect
remain open.
Patent foramen ovale (PFO) is a common anatomical variant found in 25% of the general
population and should be distinguished from a congenital heart defect (Kent et al., 2013). Much
like in adults who lack traditional atherosclerotic risk factors, it remains unclear whether isolated
PFO plays a role in childhood stroke particularly given that the timing of normal physiological
PFO closure is variable, remaining open in up to 35% of people between 1 and 29 years of age
(Ferriero et al., 2019; Roach et al., 2008). It is also unclear if a PFO with right-to-left shunt is
more prevalent in children with cryptogenic stroke and if the PFO should undergo interventional
closure in order to prevent stroke recurrence (Ferriero et al., 2019). One small study suggested
that PFO with right-to-left shunt is more prevalent in children with cryptogenic stroke than in

Pulcine 12
healthy controls (Benedik, Zaletel, Meglic, & Podnar, 2011). As in adults, interventional
treatment of PFO remains controversial in pediatric stroke and there maybe anecdotal risk with
the device itself including atrial fibrillation and risk of embolism during and after the procedure
(Giglia et al., 2013). Excluding PFO, it is well recognized that children with congenital structural
heart conditions are at an increased risk of stroke (Sinclair et al., 2015).
1.5 Cyanotic Congenital Heart Disease and Thrombosis Risk According to Different Stages of Cardiovascular Surgery
In order to repair many types of cyanotic CHD surgeons often perform a series of open-heart
procedures over several years. This is known as staged reconstructive heart surgery (Allen D.
Everett, 2011). The ultimate goal is to have the heart function like a one-sided pump with two
chambers (Allen D. Everett, 2011). Thromboembolic complications are well recognized in
patients undergoing cardiac surgery. One study by Manlhiot et al from the Hospital for Sick
Children and McMaster Children’s Hospital found several predictors for thrombotic
complications during surgery including age < 31 days, baseline oxygen saturation < 85%,
previous thrombosis, heart transplantation, use of deep hypothermic circulatory arrest, longer
cumulative time with central lines and the postoperative use of ECMO (Manlhiot et al., 2011).
Thrombotic complications at different stages of single ventricle palliation will be discussed
further below.
1.5.1 Norwood and Blalock-Taussig Shunt (Stage I Palliation)
The period in and around the time of stage I palliation is generally considered to be the highest
risk for thromboembolic complications (Giglia et al., 2013; Manlhiot et al., 2012; Silvey &
Brandao, 2017). In most cases of univentricular physiology, stage I palliation, will occur within
several days of birth (Allen D. Everett, 2011). Depending on the type of heart defect, different
surgical procedures may be used, including the Norwood procedure (Allen D. Everett, 2011).
The purpose of this operation is to ensure that blood-flow is controlled enough to prevent
damage to the heart and lungs and that enough blood is reaching the lungs to keep the child
adequately oxygenated until the second operation (Allen D. Everett, 2011). One aspect of
surgical palliation for many children with CHD is the placement of systemic-to-pulmonary artery
shunts, which often vary in their diameter, flow characteristics and composition (Giglia et al.,
2013). The Blalock–Taussig shunt (BTS) is a common surgical procedure in neonates with

Pulcine 13
single-ventricle physiology, where a shunt is created between the subclavian artery and the
ipsilateral pulmonary artery to increase pulmonary blood flow (Allen D. Everett, 2011). This
shunt creates a low-flow area that increases the risk of thrombosis and surgically removed shunts
have been found to be thrombosed at a rate of 1 – 17% (Manlhiot et al., 2012; Silvey & Brandao,
2017). Shunt thrombosis is a major cause of shunt failure and mortality in CHD patients. A 4%
risk of death resulting from shunt failure has been reported (Giglia et al., 2013). For this reason,
antithrombotic therapy is often required for BTS prophylaxis. The effectiveness of
anticoagulation therapy compared to antiplatelet therapy alone has not been studied in these
children.
1.5.2 Bidirectional Cavopulmonary Anastomosis (Stage II Palliation)
The bidirectional cavopulmonary anastomosis (BCPS), also called the Glenn or hemi-Fontan, is
the second staged palliative procedure, which usually occurs within six months of birth (Allen D.
Everett, 2011). During this surgery the superior vena cava, a large vein that carries deoxygenated
blood from the upper body into the heart, is disconnected from the heart and attached to the
pulmonary artery (Allen D. Everett, 2011). After this operation, deoxygenated blood from the
upper body goes to the lungs without passing through the heart (Allen D. Everett, 2011).
Although there are limited data, current experience suggests that the risk of thrombosis after
bidirectional cavopulmonary anastomosis is low (Giglia et al., 2013; Manlhiot et al., 2012). After
this surgery patients are at an increased risk of developing pleural effusions and chylothoraxes
(Giglia et al., 2013). This can result in a hypercoagulable state, especially if there is significant
drainage, due to loss of important proteins, including protein C, protein S and antithrombin. In
addition, loss of antithrombin can limit the effectiveness of heparin. Chronic drainage from a
pleural effusion can also result in dehydration and relative systemic hypotension (Giglia et al.,
2013). With elevated superior vena cava pressures, there is slower drainage of the cerebral
venous return which may result in a cerebral sinovenous thrombosis and venous stroke (Giglia et
al., 2013). The main concern regarding thrombosis at this palliative stage is the development of
pulmonary embolism, with a subsequent increase in pulmonary vascular resistance, making
patients unsuitable for further palliative surgeries (Manlhiot et al., 2012; Silvey & Brandao,
2017). The 2013 American Heart Association (AHA) scientific statement on prevention and
treatment of thrombosis in pediatric congenital heart disease recommends long-term prophylactic
therapy with antiplatelet agents after BCPS (Giglia et al., 2013).

Pulcine 14
1.5.3 Fontan (Stage III Palliation)
The Fontan procedure is the last surgery in the staged repair of univentricular hearts. It occurs at
approximately 2 to 3 years of age. During this surgery the inferior vena cava, a large vein that
carries deoxygenated blood from the lower body into the heart, is disconnected from the heart
and attached to the pulmonary artery (Allen D. Everett, 2011). After this operation all of the
deoxygenated blood from the body goes to the lungs without passing through the heart (Allen D.
Everett, 2011). The Fontan procedure was first performed in 1968. It has since undergone many
modifications, although the mechanism of the anastomosis of the inferior vena cava to the
pulmonary arteries remains unchanged (Gewillig & Brown, 2016). Patients undergoing the
Fontan procedure are also at an increased risk of developing thromboembolism. The incidence of
thrombosis after Fontan is reported to range from 17 – 33% in cross-sectional studies (Giglia et
al., 2013), while the prevalence of ischemic stroke following a Fontan procedure is estimated to
be between 1.4 –19% (Firdouse, Agarwal, Chan, & Mondal, 2014; Manlhiot et al., 2012).
However, this risk is not uniform and has been reported to vary over time. The highest risk is
reported within the perioperative period extending 3 to 12 months and then again at 5 to 10 years
after the procedure (Giglia et al., 2013). Previously identified post-Fontan thrombosis risk factors
include passive blood flow, chronic venous hypertension, and atrial arrhythmias (Giglia et al.,
2013; Silvey & Brandao, 2017; Sinclair et al., 2015). Liver congestion from chronic venous
hypertension may result in decreased vitamin K-dependent proteins C and S (Giglia et al., 2013).
As previously discussed, children post-Fontan have elevated factor VIII levels, which may
further increase thrombosis risk (Odegard et al., 2009). Adding to this risk maybe the type of
Fontan modification performed. Initially, the patient may have a fenestration placed within the
atria, called a fenestrated-Fontan, to provide a pop-off for venous blood to the left side, if right-
sided pressures are high (Allen D. Everett, 2011). This in turn could lead to the development of
paradoxical emboli if a thrombus travels to or originates within the right side of the heart (Allen
D. Everett, 2011; Giglia et al., 2013). It is still not clear, however, why the risk increases after 5
to 10 years. Several authors have postulated that at that time additional chronic risk factors come
into play that are more commonly seen in adult survivors of CHD: ventricular dysfunction, atrial
arrhythmia, prolonged immobilization, protein-losing enteropathy and chronic pleural effusions
(Giglia et al., 2013). Barker et al reviewed 402 children who underwent the Fontan procedure
between 1975 and 1998 for single-ventricle physiology and followed them for a median of 3.5

Pulcine 15
years postoperatively (Barker et al., 2005). The study found that risk of stroke was not related to
the type of Fontan nor the presence of fenestration (Barker et al., 2005). Not surprisingly, they
found a significantly lower rate of stroke in patients on antithrombotic treatment with aspirin or
warfarin compared to those not treated with antithrombotic therapy (2.4 per 1 000 patient-years
vs. 13.4 per 1 000 patient years; p=0.02) (Barker et al., 2005). In order to determine the most
effective antithrombotic therapy regimen, Monagle et al performed a multicenter randomized
trial comparing aspirin of 5 mg/kg/day to warfarin, with a target international normalized ratio
(INR) of 2-3, for prevention of thrombosis following Fontan (Monagle et al., 2011). Children
were screened at 3 months and 2 years with transthoracic and transesophageal echocardiograms
(Monagle et al., 2011). Interestingly, the risk for both asymptomatic and symptomatic
thrombosis was 19% at 2 years and was similar in both groups with no significant difference
between those on aspirin or warfarin (Monagle et al., 2011). Of the 111 patients studied 12
developed thrombosis in the aspirin group and 13 in the heparin/warfarin group with an increase
in minor bleeding rate in the latter (Monagle et al., 2011). Therefore, prophylaxis with either
aspirin or warfarin is warranted; however, clinical practice still varies both within and amongst
centers.
In the adult population with an open Fontan fenestration, no study to date has shown that a patent
fenestration in isolation is a risk factor for thrombosis or stroke (Giglia et al., 2013). Despite this,
long-term warfarin therapy is recommended for primary stroke prevention in adult patients with
Fontan circulation who have a documented intracardiac shunt due to additional acquired risk
factors which were discussed in section 1.2.1.
1.5.4 Thromboprophylaxis Across All Stages of Cardiovascular Surgery
Because of the high risk of developing thromboembolic complications during cardiac surgery
and cardiac procedures a number of studies have looked at the efficacy of thromboprophylaxis in
children with univentricular CHD (Manlhiot et al., 2012; Monagle et al., 2011). Antiplatelet and
anticoagulant agents have both been successfully used to reduce thromboembolic complications
(Manlhiot et al., 2012; Monagle et al., 2011). Manlhiot et al examined the association between
thromboprophylaxis and thrombosis risk across all three stages of palliative cardiac repair
(Manlhiot et al., 2012; Manlhiot et al., 2011). The study found that after stage I palliation [HR
0.5; p=0.05] and after stage II palliation [HR 0.2; p=0.04] enoxaparin compared to no

Pulcine 16
antithrombotic therapy was associated with a reduced risk of thromboembolic complications
(Manlhiot et al., 2012). After stage III palliation, both warfarin [HR 0.27; p=0.05] and aspirin
[HR 0.18; p=0.02] were associated with a reduced rate of thromboembolic complications
compared to no antithrombotic therapy (Manlhiot et al., 2012). In terms of bleeding risk, two
patients on enoxaparin and one patient on warfarin experienced major bleeding complications
without any associated morbidity or mortality: two with subdural hematomas and one with an
intrathoracic bleed (Manlhiot et al., 2012). Because thrombotic complications were associated
with increased mortality after stage I palliation [HR 5.5; p<0.001] and stage II palliation [HR
12.5; p<0.001] the authors concluded that the risk-benefit ratio was in favour of
thromboprophylaxis in children with CHD undergoing palliative repair but the best type of
antithrombotic therapy is not known (Manlhiot et al., 2012). Interestingly, while the study found
that thromboprophylaxis across all stages of palliative cardiac repair had an overall reduction in
thrombosis risk, it did not have the same reduction on thromboembolic complications directly
associated with cardiovascular surgery (Manlhiot et al., 2012). This procedure-related
thrombosis risk represents a significant proportion of overall thrombosis risk in children with
CHD (Manlhiot et al., 2012). Perhaps, multifactorial strategies are needed to specifically target
this high-risk period such as use of peripheral venous lines instead of central venous lines and
thrombophilia screening prior to surgery with thromboprophylaxis for those at highest risk.
1.6 Cardiac Catheterization
Diagnostic and interventional cardiac catheterization is performed in children with acquired and
congenital heart disease for both diagnostic and therapeutic purposes (Allen D. Everett, 2011;
Silvey & Brandao, 2017). Known complications of these procedures include in situ thrombosis
and distal embolus (Giglia et al., 2013; Silvey & Brandao, 2017). The prevalence of AIS in
children due to cardiac catheterization is estimated to be 0.28 – 1.3% (Liu, Wong, & Leung,
2001; Weissman, Aram, Levinsohn, & Ben-Shachar, 1985). When undergoing cardiac
catheterization, the femoral artery or vein is accessed for catheter insertion immediately prior to
a bolus of unfractionated heparin (UFH) for prophylaxis (Allen D. Everett, 2011; Giglia et al.,
2013). The typical anticoagulation protocol for diagnostic or interventional cardiac
catheterization includes a loading dose of 100 U/kg (up to 5000 U maximum) and an additional
50 to 100 U/kg of heparin bolus to keep the activated clotting time (ACT) > 200 seconds (Giglia

Pulcine 17
et al., 2013). ACT is a quantitative assay for monitoring heparin anticoagulation during various
medical and surgical procedures (Giglia et al., 2013).
One common interventional catheterization procedure is called a balloon atrial septostomy
(BAS), where a balloon catheter is used to create or enlarge a patent foramen ovale or atrial
septal defect between the two upper chambers of the heart in order to increase oxygen saturation
(Allen D. Everett, 2011). In essence, this procedure is used to temporarily rescue the physiology
of transposition of the great arteries (TGA), a life-threatening cyanotic CHD seen in infants,
while awaiting definitive corrective surgery: the arterial switch operation (ASO). In one study,
Block et al found that BAS was significantly associated with preoperative AIS in infants with
TGA (RR=4; 95% CI:1.5-9.3; p=0.0015) (Block et al., 2010). However, other studies have not
found the same association (Petit et al., 2009). In practice the use of prophylactic anticoagulation
during BAS currently varies both within and among centers and is not evidence-based.
1.7 Cardiopulmonary Bypass
Cardiopulmonary bypass (CPB) is defined as “the process of diverting venous blood from a
patient’s heart and lungs to a gas exchange system for the addition of oxygen, removal of carbon
dioxide and subsequent reinfusion to the patient’s arterial system” (Allen D. Everett, 2011).
Thereby CPB maintains the circulation of blood and oxygen to all organs while facilitating
surgery on the open heart and its great vessels. Patients who undergo CPB are temporarily
exposed to an artificial vascular surface which can result in platelet activation and downstream
effects that transiently alter hemostasis (Giglia et al., 2013; Silvey & Brandao, 2017). CPB in
children results in platelet activation and an initial drop in the platelet count that subsequently
recovers post-surgery (Giglia et al., 2013). Patients younger than 1 year of age are more likely to
develop thrombocytopenia while undergoing CPB (Silvey & Brandao, 2017). At the same time,
thrombi can originate in the bypass circuit due to tissue factor activation from contact with an
artificial surface, which leads to increased thrombin generation and thereby fibrin clot formation.
Thrombi can travel and enter the cerebral circulation directly, bypassing the pulmonary
circulation, embolizing in distal vessels (Sinclair et al., 2015).
Optimal anticoagulation during CPB will prevent clot formation within the CPB circuit and
minimize consumption of coagulation factors while minimizing excessive intraoperative
bleeding (Giglia et al., 2013). Heparin is the most common anticoagulant used for CPB. A

Pulcine 18
loading dose of 300 to 400 U/kg is given IV and is also used to prime the pump and circuit. The
optimal target ACT that will prevent clot formation within the CPB circuit is not precisely
known, but clot formation is unlikely to occur with an ACT > 300 seconds (Giglia et al., 2013).
Commonly, a target of ACT > 480 seconds is used in neonates and children (Giglia et al., 2013).
Typically, ACT is determined 2 to 5 minutes after administration of heparin. Factors known to
prolong ACT include hypothermia, hemodilution and decreased platelet function (Giglia et al.,
2013). All these factors may be present during CPB making this a time both of increased risk of
hemorrhage and thrombosis.
1.8 Extracorporeal Membrane Oxygenation
Extracorporeal membrane oxygenation (ECMO) is a closed CPB circuit designed to provide
cardiorespiratory support for a short period of time; generally up to 14 days (Giglia et al., 2013).
ECMO is used frequently for cardiac support in neonates and children with acquired and
congenital heart disease. Indications include intractable low cardiac output, cardiac arrest or as a
bridge to heart transplant (Giglia et al., 2013). Two types of ECMO are generally available:
venovenous and venoarterial. In venovenous ECMO blood is withdrawn from the venous system
and returned to the venous system to exchange oxygen and carbon dioxide (Allen D. Everett,
2011; Giglia et al., 2013). It is primarily indicated for patients with isolated respiratory failure
with preserved cardiac function (Allen D. Everett, 2011; Giglia et al., 2013). In venoarterial
ECMO deoxygenated venous blood is removed, exchanging oxygen and carbon dioxide, and
pumped back into the patient’s arterial circulation in order to provide cardiopulmonary support
(Giglia et al., 2013). Like CPB, ECMO exposes the blood to foreign material resulting in
thrombus formation and requires use of anticoagulation in order to prevent clot formation (Giglia
et al., 2013). Despite anticoagulation, thromboembolic complications are not infrequent on
ECMO. The prevalence of ischemic stroke in children treated with ECMO is reported to be 7 –
11%, while the incidence rate on ECMO is reported to be 1 – 2 events per 100 days of support
(Almond et al., 2011; Cengiz, Seidel, Rycus, Brogan, & Roberts, 2005). The typical
anticoagulation protocol for ECMO includes a loading dose of 100 U/kg heparin before
cannulation and a continuous infusion of heparin to maintain ACT between 180 and 220 seconds
(Giglia et al., 2013). Other suggested targets for anticoagulation on ECMO include, prolongation
of the partial thromboplastin time (PTT) to 1.5 to 2.5 times the control value and anti-factor Xa
level of 0.3 to 0.7 IU/mL (Giglia et al., 2013). In general a lower level of anticoagulation is

Pulcine 19
necessary compared with patients undergoing surgery using CPB although a recent study
suggested that higher heparin doses in patients on ECMO results in improved survival despite the
potential increased risk of bleeding complications (Giglia et al., 2013).
When ECMO is used to support the circulation of patients after cardiac surgery, it is commonly
referred to as post-cardiotomy ECMO (Giglia et al., 2013). Post-cardiotomy ECMO has been
reported at a rate of 2 – 5% of all postoperative patients in large tertiary care centers (Giglia et
al., 2013). Indications include failure to wean from CPB or due to low cardiac output or cardiac
arrest post-operatively (Giglia et al., 2013). This subpopulation of patients are at a particularly
increased risk of bleeding as they cannot be weaned from CPB and their heparin cannot be
reversed (Giglia et al., 2013).
1.9 Ventricular Assist Devices
Ventricular assist devices (VADs) are primarily designed to support patients with terminal heart
failure who are refractory to medical therapy while they await heart transplanation (Almond et
al., 2011). Pediatric VADs, specifically the Berlin Heart EXCOR VAD, is superior to ECMO for
bridging to heart transplant and has emerged as the new standard of care with device approval
granted in 2011 by the U.S. Food and Drug Administration (FDA) (Almond et al., 2011). For the
same reasons that CPB and ECMO increase the risk of thromboembolic complications, use of
VAD also increases risk of thrombosis by exposing blood to an artificial vascular surface, but for
a more prolonged period of time, thereby increasing the overall cumulative prevalence of these
complications (Giglia et al., 2013). Children with a Berlin Heart EXCOR VAD have a combined
hemorrhagic and ischemic stroke prevalence of 28 – 34%, with a reported incidence rate of 0.5
events per 100 days of support (Fraser et al., 2012). When compared to ECMO, the prevalence
rate appears significantly higher while the incidence rate somewhat lower. This may be
explained by the shorter exposure period for ECMO as the typical duration of support is less than
14 days compared to VAD duration which often exceeds 30 days (Sinclair et al., 2015). In
contrast, VADs typically used in adults such as the HeartMate II appear to have a significantly
lower risk of stroke in adolescents, approximately 6 – 12% based on small pediatric studies
(Cabrera et al., 2013). The reasons for this are not entirely known but may be a reflection of the
differing underlying cardiac diseases or a shorter duration of use related to a greater availability
of organ donation in older children and adults. In any case, multiple concurrent anticoagulant and

Pulcine 20
antiplatelet agents are required with VADs to prevent thrombosis given the typical prolonged
duration of use while awaiting heart transplant.
1.10 Prevention and Treatment of Arterial Ischemic Stroke in Children with Cardiac Disease
As children with cardiac disease are at an increased risk of thrombosis and ischemic stroke,
physicians have used antithrombotic therapy to treat and prevent thromboembolic complications,
all of which are used off-label (Giglia et al., 2013). Antithrombotic therapy can be divided into
three main groups: antiplatelet, anticoagulant and fibrinolytic agents. Five international
consensus-based guidelines exist that address the use of antiplatelet, anticoagulant and
fibrinolytic therapy in children with ischemic stroke: The American Heart Association/American
Stroke Association (Ferriero et al., 2019; Roach et al., 2008); The American College of Chest
Physicians (Monagle et al., 2012); The American Heart Association Scientific Statement on
Prevention and Treatment of Thrombosis in Pediatric Congenital Heart Disease (Giglia et al.,
2013); The Royal College of Paediatrics and Child Health and Stroke Association, (Kmietowicz,
2017); and The Australian Clinical Consensus Guidelines (Medley et al., 2019). In general, the
available guidelines recommend anticoagulation for secondary stroke prevention if there is
confirmed dissection or cardioembolic source with the duration of treatment largely dependent
on the underlying condition and individual risk factors. If the above etiologies are ruled out, the
recurrence risk is deemed to be lower and antiplatelet therapy with aspirin or clopidogrel is then
reasonable for secondary stroke prevention. In neonates, in the absence of congenital heart
disease, the risk of recurrence is deemed to be negligible and as a result no further antithrombotic
therapy is recommended. Institutional practices for anticoagulation for children with cardiac
disease are highly variable in the absence of evidence demonstrating safety and clinical efficacy,
but anticoagulation appears to be generally well tolerated (Ferriero et al., 2019). No clinical trials
have evaluated whether antiplatelet or anticoagulant or combination of therapies is best. Primary
prevention has been difficult because of small patient numbers and heterogeneity of cardiac
disease with coexistence of multiple risk factors. For secondary stroke prevention, the
antiplatelet therapy most commonly used in children with AIS is aspirin and anticoagulants most
often used are LMWH and warfarin (Ferriero et al., 2019). However, it remains unclear in which
situation and for which type of cardiac disease antiplatelet or anticoagulant medications are the
best for initial and long-term secondary stroke prevention. A recent study by Leijser et al found

Pulcine 21
significantly more post-operative brain injury in neonates with single ventricle physiology (SVP)
receiving preoperative anticoagulation for secondary stroke prevention when compared to those
neonates who were not. Most of this injury was attributed to ischemic stroke and occurred
despite frequent use of anticoagulation prophylaxis preoperatively (Leijser et al., 2019).
Moreover, they found that there was no apparent protective effect from prophylactic
antithrombotic therapy on post-operative ischemic stroke in children with TGA and SVP (Leijser
et al., 2019). Those neonates receiving ASA and anticoagulation had an increased incidence of
subdural hemorrhage compared to those only receiving anticoagulation (Leijser et al., 2019).
These findings are important because a high proportion of CE-AIS occur in the periprocedural
period and reoperation is an independent stroke risk factor (Domi et al., 2008). Intuitively,
antithrombotic therapy is thought to help lessen this risk. Although, thromboprophylaxis has an
overall effect on reducing the thrombosis risk in children with CHD undergoing staged cardiac
repair, it may not have an effect on thrombosis associated with the surgical procedure itself as
suggested by one author (Manlhiot et al., 2012). These findings add further controversy to the
optimal medical management in this cohort of patients and highlights the fact that the best
thromboembolic prevention strategy and timing for children with CHD are still largely unknown.
1.10.1 Antiplatelet Therapy
Aspirin inhibits platelet cyclooxygenase-1 (COX-1) and prevents thromboxane B2 production
(Michelson & Bhatt, 2017). In most children with CE-AIS continued maintenance therapy
consists of aspirin dosed at 3 – 5 mg/kg/day. Low-dose aspirin has been used for the prevention
of long-term thrombotic complications for many decades given the perceived low risk-to-benefit
ratio (Giglia et al., 2013). Bleeding risk with aspirin is thought to be lower than with
anticoagulants like heparin and warfarin. The duration of aspirin therapy depends on the
underlying conditions and ongoing risk of recurrent stroke. For example, aspirin may be
considered for primary prophylaxis either in children following the Fontan procedure (Monagle
et al., 2011) or it can be used in children after a device is placed in the cardiac septum via
catheterization in order to close an intracardiac connection (Giglia et al., 2013). Following
definitive cardiac repair or heart-transplant most children with perioperative CE-AIS are treated
with aspirin for two years to cover the time window when the vast majority of recurrent strokes
occur (Ferriero et al., 2019).

Pulcine 22
Another antiplatelet agent, clopidogrel, is increasing being used. Clopidogrel irreversibly blocks
the adenosine diphosphate receptor on platelet cell membranes thereby inhibiting platelet
aggregation by blocking activation of the glycoprotein IIb/IIIa pathway (Giglia et al., 2013).
However, clopidogrel was recently shown to have clinical equipoise when compared to placebo
or conventional therapy with aspirin in reducing mortality and shunt-related thrombosis in
cyanotic CHD patients palliated with systemic-to-pulmonary artery shunts (Wessel et al., 2013).
Despite the fact that it does not appear to have superior clinical efficacy, clopidogrel is often
used in selected circumstance when there is apparent aspirin failure or intolerance to aspirin
(Giglia et al., 2013).
1.10.1.1 Aspirin Resistance
Aspirin resistance is well studied in the adult literature (Michelson et al., 2005) where it has been
reported to have a mean laboratory prevalence of 25% in the general population (Hovens et al.,
2007). It can be broadly defined as persistent platelet activation and aggregation despite aspirin
therapy (Snoep et al., 2007). Therefore, not all patients benefit from aspirin to the same extent
and aspirin may be inadequate for ongoing prevention of recurrent thrombotic events in some
patients. Aspirin resistance and its clinical consequences have not been well studied in children
until more recently. Mir et al examined the incidence of aspirin responsiveness in 20 infants with
single-ventricle physiology after palliative heart surgery (Mir et al., 2015). They found an 80%
incidence of aspirin resistance immediately after single-ventricle shunt palliation by measuring
thromboelastogram (TEG) (Mir et al., 2015). The thromboelastogram uses activated whole blood
to measure hemostasis and fibrinolysis (Giglia et al., 2013). In their study, age, weight,
hemoglobin level, and platelet count were not associated with aspirin resistant status (Mir et al.,
2015). Similarly to adult data, another study found that aspirin resistance is associated with
increased risk of thrombosis in pediatric patients undergoing cardiac surgery (Emani et al.,
2014). Aspirin resistance is not routinely measured in clinical practice in pediatric patients with
cardiac disease making it difficult to know dosing efficacy and rates of true aspirin failure versus
resistance.
1.10.2 Anticoagulant Therapy
Warfarin functions as an anticoagulant by decreasing the plasma concentration of vitamin-K
dependent factors: II, VII, IX and X (Giglia et al., 2013). Warfarin is commonly dosed at 0.2

Pulcine 23
mg/kg daily and the dose is titrated to a pre-specified INR level. It has a narrow therapeutic
index which necessitates frequent monitoring of the INR. Warfarin therapy is not routinely
recommended in children < 1 year of age because of physiologically decreased plasma levels of
vitamin K-dependent factors, variable vitamin K levels based on variable nutritional intake as a
child goes through the various developmental stages and requirement for more frequent INR
monitoring (Giglia et al., 2013).
Heparin achieves anticoagulation by amplifying the activity of antithrombin (Giglia et al., 2013).
Heparin binds to a lysine residue on antithrombin thereby increasing the thrombin inhibition of
circulating antithrombin by more than a thousand times (Giglia et al., 2013). Heparin has the
advantage in that it can be rapidly reversed with protamine, which makes it ideal to use in
situations such as bridging therapy prior to procedures and in high-risk situations where systemic
or intracranial hemorrhage is a consideration. LMWH is a short-chain heparin that does not
influence the PTT. The anti-factor Xa level is the only measure of the effect of LMWH therapy.
LMWH has advantages over UFH in that it can be used on an outpatient basis with infrequent
testing of anti-factor Xa levels (Giglia et al., 2013). However, it requires once- or twice-daily
subcutaneous injections.
1.10.2.1 Heparin Resistance
Similar to aspirin resistance, the presence of heparin resistance can lead to inadequate prevention
of thrombosis. There is no agreed upon definition of heparin resistance. Some authors have
defined it as the need for substantially higher than normal heparin dosing to achieve a
satisfactory safe level on anticoagulation or inability to achieve safe levels of anticoagulation
(Giglia et al., 2013). When applied to children receiving CPB it is defined as the “inability to
achieve ACT > 300 seconds after administration of > 6000 U/kg of heparin” (Giglia et al., 2013).
Heparin resistance can occur for a number of reasons the most common of which is antithrombin
deficiency, but other factors such as, preoperative heparin treatment, severe thrombocytosis,
sepsis and hypereosinophlic syndrome have also been reported (Giglia et al., 2013; Hage,
Louzada, & Kiaii, 2019). A recent Canadian practice parameter highlighted sepsis-induced
heparin resistance during ECMO in adults (Hage et al., 2019). In sepsis, activated neutrophils
release various heparin-binding proteins, leading to decreased effectiveness of heparin and
thrombosis prevention (Hage et al., 2019). Antithrombin deficiency can be inherited or acquired.

Pulcine 24
Regardless of the etiology, in children experiencing heparin resistance it is recommended to give
antithrombin concentrate and fresh frozen plasma in order to increase the effectiveness of
heparin therapy (Giglia et al., 2013).
1.10.3 Tissue Plasminogen Activator
Tissue plasminogen activator (tPA) converts plasminogen into plasmin, while plasmin degrades
fibrin which is needed to cross-link platelets in order to form a clot (Giglia et al., 2013). In
adults, intravenous (IV) tPA significantly improves clinical outcome when given within 4.5
hours of AIS onset, despite a 6.4% risk of intracranial hemorrhage (Emberson et al., 2014). In
the absence of contraindications, it is the standard of care in acute AIS across all stroke
etiologies in adults. Observational studies report the use of IV tPA in pediatric patients but safety
and efficacy have not been established in pediatric arterial ischemic stroke (Bernson-Leung &
Rivkin, 2016). One retrospective case series of 80 children looked at the safety and outcomes of
IV tPA in systemic arterial and venous thrombi and found efficacy in clot resolution with a low
margin of safety (Gupta et al., 2001). The only prospective treatment trial of IV tPA to date in
children, the Thrombolysis in Pediatric Stroke (TIPS) trial, was closed due to lack of enrollment.
However, it allowed for the establishment of pediatric stroke treatment centers. A recent abstract
presented at the International Stroke Conference (ISC) reported that children are not at an
increased risk of symptomatic intracranial hemorrhage following IV tPA for acute stroke (Amlie-
Lefond C, 2019). This study used a Poisson model to fit retrospective data, from a prospectively
enrolled cohort of patients, collected from the TIPS stroke centres and compare it to know adult
rates of hemorrhagic transformation in acute AIS (Amlie-Lefond C, 2019). Recently, Bigi et al
reported on 16 children from a Swiss Registry who underwent acute thrombolytic stroke therapy
(Bigi et al., 2018). Amongst 16 patients, complications of recanalization therapy with IV tPA
occurred in 2 (12.5%): one with asymptomatic hemorrhagic transformation (HT) of the AIS and
one with mucosal bleeding (Bigi et al., 2018). In terms of applicability, intravenous thrombolysis
is not feasible in many pediatric CE-AIS as this cohort of children is usually already receiving
prophylactic or therapeutic antithrombotic therapy, which is a contraindication to IV tPA use.
1.10.4 Mechanical Thrombectomy
In adults, mechanical thrombectomy with stent retrievers is now recommended as the standard of
care in AIS caused by a proximal large vessel occlusion in the anterior circulation (Casaubon et

Pulcine 25
al., 2015; Goyal et al., 2016). In comparison, mechanical thrombectomy is rarely used in children
with a recently reported rate of 10% from a Swiss cohort (Bigi et al., 2018). This is primarily due
to delay to diagnosis and uncertainty regarding clinically efficacy and safety, chief among them
being fatal bleeding complications. Currently it is not known whether thrombectomy has the
same, increased or decreased rate of hemorrhagic complications in children as compared to that
of adults (Bigi et al., 2018). Bigi et al reported on 16 children from a Swiss Registry who
underwent acute thrombolytic stroke therapy (Bigi et al., 2018). Six of those children underwent
thrombectomy alone while 5 received intravenous or intraarterial tPA in addition to
thrombectomy (Bigi et al., 2018). No child had symptomatic intracranial hemorrhage and only
one who received IV tPA, but not thrombectomy, had asymptomatic hemorrhage as mentioned in
the previous section (Bigi et al., 2018). No complications occurred during endovascular
procedures and rates of hemorrhagic transformation and mortality did not differ between the two
groups (Bigi et al., 2018). As mentioned previously, the majority of children with CE-AIS are
already receiving antithrombotic therapy at the time of their stroke, a contraindication to IV
thrombolysis, making mechanical thrombectomy an attractive alternative option. However, more
prospective safety and efficacy data are needed in children before this can be considered as a
standard of care in certain pre-selected groups.
1.11 Prior Data on Antithrombotic Safety and Risk of Hemorrhagic Transformation in Children with Arterial Ischemic Stroke
One of the main concerns regarding the use of antithrombotic therapy for prophylaxis and
therapeutic purposes is the risk of bleeding complications, the most feared amongst them being
intracerebral hemorrhage. No randomized-controlled trials have looked at the safety of
antithrombotic therapy for secondary stroke prevention in children regardless of the stroke
etiology. However, a few retrospective and prospective follow-up studies have been performed.
One of the first studies to look systematically at antithrombotic therapy in pediatric ischemic
stroke was a retrospective multicenter, non-randomized trial of 135 children comparing aspirin 2
– 5 mg/kg/day versus low-dose LMWH 1 – 1.5 mg/kg/day for secondary stroke prevention
(Strater et al., 2001). The study aimed to compare children selected clinically for the two
different treatments on the risk of stroke recurrence (Strater et al., 2001) during the median
observational period of 36 months, no patient in the aspirin or LMWH group showed drug-
associated side effects, including systemic and intracranial hemorrhage (Strater et al., 2001). The

Pulcine 26
study concluded that there was equipoise between the two treatments arms with respect to stroke
recurrence. However, a major limitation of the study was that the therapies were not
administered in a randomized fashion leading to selection bias (Strater et al., 2001). A follow-up
study by Bernard et al examined 37 children in two centers with AIS and non-moyamoya
arteriopathy who received prophylactic (once-daily LMWH 57%) or therapeutic (UFH infusion,
twice-daily LMWH or once-daily warfarin 43%) anticoagulation for at least 4 weeks (Bernard et
al., 2009). They found no major bleeding episodes and no intracranial hemorrhage over a period
of 1329 patient-months amongst the 37 children (Bernard et al., 2009). A major limitation of this
study was lack of standardized follow-up neuroimaging to look for evidence of asymptomatic
intracranial hemorrhage. Similarly, to the previous study, anticoagulation-therapy was not
randomized but individualized at the treating physician’s discretion.
The first published study in North America to analyze the clinical and radiological predictors of
hemorrhagic transformation (HT) in children with AIS, irrespective of etiology, was performed
by Beslow et al (Beslow et al., 2011). The study retrospectively reviewed 63 children and found
that 30% (19/63) had HT within 30 days of stroke (Beslow et al., 2011) with only 3% (2/19)
being symptomatic. Most hemorrhages were petechial 84% (16/19) (Beslow et al., 2011). There
was no significant difference in the development of HT amongst those children treated with
antiplatelet therapy alone as compared to those treated with systemic anticoagulation (35% vs.
21%; p=0.26) (Beslow et al., 2011). The development of HT was significantly associated with an
infarct volume greater than 5% of the supratentorial brain volume (RR 4.81; 95% CI: 1.54 –
15.08; p=0.0026) with a trend toward increased risk of HT in children with cardiac disease (RR
1.97; 95% CI: 0.96 – 0.45; p=0.12) and meningitis (RR 2.77; 95% CI: 1.37 – 5.59; p=0.08)
(Beslow et al., 2011). The study was again limited by selection bias in the allocation of
antithrombotic therapy and a lack of standardized follow-up imaging which may have
underestimated the risk of asymptomatic HT, as children with HT had more neuroimaging
(Beslow et al., 2011). The first published study in North America whose primary objective was
to evaluate the safety of protocol-based anticoagulant therapy in children with AIS, irrespective
of etiology, was conducted by Schechter et al. The study looked at a 14-year period of
prospectively enrolled cohort of children with AIS who were receiving anticoagulation therapy:
out of 215 children, 123 received anticoagulation therapy while 75 did not (Schechter et al.,
2012). The rate of HT was not significantly different between the two groups (11% vs. 16%)

Pulcine 27
(Schechter et al., 2012). No clinical or radiological predictors of anticoagulation-associated
hemorrhage were identified due to a small sample size (Schechter et al., 2012). The authors
concluded that anticoagulation is relatively safe in children with AIS with 4% risk of
symptomatic intracranial hemorrhage (Schechter et al., 2012). Table 2 summarizes the rate and
associated risk factors of hemorrhagic transformation in the two aforementioned studies by
Beslow et al and Schechter et el.
Beslow N=63 Schecter N=123
Rate of Hemorrhagic Transformation
Within 30 Days 30% (19/63) 11% (14/123)
Rate of Symptomatic Hemorrhagic
Transformation Within 30 Days 3% (2/63) 4% (5/123)
Hemorrhagic Transformation on
Antiplatelet (APT) Therapy Alone 35% (34/63 on APT) N/A
Hemorrhagic Transformation on
Anticoagulant (ACT) Therapy Alone 21% (24/63 on ACT) 11% (123/215 on ACT)
European Cooperative Acute Stroke Study Grade of Antithrombotic Therapy (ATT)-
Associated HT
HI1 14 7
HI2 2 3
PH1 2 0
PH2 1 1
Unknown 3
Clinical Predictors
Cardiac Disease (RR
1.97; 95% CI: 0.96 –
0.45; p=0.12)
Meningitis (RR 2.77;
95% CI: 1.37 – 5.59;
p=0.08)
None
Radiological Predictors
Infarct Volume > 5% of
Supratentorial Brain
Volume (RR 4.81; 95%
CI: 1.54 – 15.08;
p=0.0026)
None
Table 2. Summary of hemorrhagic transformation rates and associated risk-factors in two
pediatric cohort studies by Beslow et al 2011 and Schecter et al 2012.
Dowling et al examined a large cohort of children enrolled in the International Paediatric Stroke
Study (IPSS) with primarily cardiac disorders and AIS (n=204) and compared them to children
with other causes of stroke (n=463). The study found a higher rate of HT in those with CE-AIS
(15.2% vs. 6.6%; p=0.001) but the study did not control for the type of antithrombotic therapy

Pulcine 28
used or timing of the HT which may have contribute to the increased rate (Dowling et al., 2013).
More recently, Asakai et al conducted a retrospective single-center review of 76 children with
cardiac disease and AIS. The study found an incidence of HT amongst their cohort of 17% with
23% immediate deaths due to stroke with secondary hemorrhagic conversion although it was not
clear how much HT contributed to this (Asakai et al., 2015). The study did not comment further
on the type of HT seen, the proportion of children that were asymptomatic, nor the type of
antithrombotic therapy at the time of HT. As expected, a larger proportion (45%) of the cardiac
patients were receiving antithrombotic treatment before the sentinel CE-AIS which may have
contributed to the risk of HT (Asakai et al., 2015).
As illustrated, few studies to date have examined hemorrhagic transformation in pediatric CE-
AIS. Distinct stroke mechanisms and age-related differences in hemostasis limit extrapolation of
adult data to children (Bernson-Leung & Rivkin, 2016). When a child has a brain hemorrhage
while receiving anticoagulation the anticoagulant is typically held or reversed (Ferriero et al.,
2019). However, there are no clear guidelines on when it is safe to restart the anticoagulant
therapy. Often a multidisciplinary discussion weighing the risks versus benefits of withholding
versus restarting anticoagulation or alternatively moving to antiplatelet treatment is required.
Factors such as size of the bleed, clinical status of the child, indication for anticoagulation, high
risk of thrombosis due to concurrent CBP, ECMO, VAD or the presence of a mechanical heart
valve or pulmonary embolism may favor ongoing anticoagulation.
1.12 Hemorrhagic Transformation in Adults with Arterial Ischemic Stroke
Hemorrhagic transformation is a well-known and well-studied complication of AIS in adults,
which dictates approach to treatment and impacts clinical outcome (Hutchinson & Beslow,
2019). HT can occur spontaneously or as a complication from acute thrombolytic and
endovascular therapies or from antithrombotic therapies initiated for secondary stroke prevention
(Hutchinson & Beslow, 2019). Excluding treatment with tissue plasminogen activator and
mechanical thrombectomy, risk factors for HT in adults include higher stroke severity at
presentation (mean National Institutes of Health Stroke Scale (NIHSS) score of 9.9 with HT vs.
5.9 without HT; p=0.003) (Kablau et al., 2011); altered level of consciousness at presentation
(Hornig, Dorndorf, & Agnoli, 1986); cardioembolic mechanism of stroke (Lodder, Krijne-Kubat,

Pulcine 29
& Broekman, 1986); size of the infarct especially territorial infarction (88% with HT vs. 58.8%
without HT; p=0.007) (Kablau et al., 2011); mass effect on the initial CT scan (Hornig et al.,
1986); and contrast enhancement of the infarct on head CT (Hornig et al., 1986; Hutchinson &
Beslow, 2019).
A commonly used classification system was developed for the European Cooperative Acute
Stroke Study (ECASS), which divides hemorrhagic transformation into four subtypes (Beghi et
al., 1995; Fiorelli et al., 1999): “H0 – no hemorrhage detected; HI1 – scattered heterogenous
petechiae along the margins of the infarct; HI2 – more confluent petechia; PH1 – small
parenchymal hemorrhage with less than 30% of infarcted area with no to mild mass effect; PH2
– large parenchymal hemorrhage with greater than 30% infarcted area with significant mass
effect or hemorrhage remote from the stroke location” (Fiorelli et al., 1999). In adults, ECASS
grade HI1, HI2 and PH1 within the first 36 hours of stroke onset were not associated with a
higher risk of neurological morbidity or mortality when compared to patients without
hemorrhagic transformation (Beghi et al., 1995; Fiorelli et al., 1999). PH2, however, was
associated with a significantly increased risk of early and 3-month mortality as well as acute
neurological deterioration (Fiorelli et al., 1999).
Frequency of HT varies among studies and its risk factors have been usually studied in patients
with anterior ischemic stroke who receive thrombolytic therapy (Valentino et al., 2017).
Symptomatic intracranial hemorrhage occurs in 6.4% of adult patients treated with IV tPA within
4.5 hours of stroke onset (Emberson et al., 2014). Regardless of the initial hyperacute stroke
treatment, the timing of anticoagulation therapy after acute AIS remains controversial. In the
adult stroke population, current thinking is that intracerebral bleeding in patients taking
anticoagulants reflects spontaneous bleeding that is exacerbated by anticoagulation (Steiner,
Weitz, & Veltkamp, 2017). Therefore, anticoagulants in theory can sustain intracerebral
hematoma formation but do not necessarily cause it (Steiner et al., 2017). Hart et al hypothesized
that the use of oral anticoagulants simply unmasks intracerebral bleeding that would otherwise
remain asymptomatic when the right clinical risk factors are present including advancing age,
hypertension and cerebral amyloid angiopathy. None of these theories have been directly proven
but a risk stratification tool in adults who present with an acute ischemic stroke and have an
ongoing indication for anticoagulation has been developed and validated recently and will be
discussed further below (Marsh, Llinas, Hillis, & Gottesman, 2013; Marsh et al., 2016).

Pulcine 30
1.12.1 Pathophysiology of Hemorrhagic Transformation
Following acute stroke there is breakdown of the blood brain barrier resulting in friable
intracranial microvasculature which theoretically increases risk of intracerebral bleeding into the
area of ischemia (Marsh et al., 2013). Higher grades of hemorrhagic transformation can
significantly worsen outcome (Fiorelli et al., 1999). HT is usually seen in the first 4 days
following infarction but is rare in the first 6 hours (Di Muzio, 2019). Almost 50% of infarcts will
have some form of HT although the incidence varies (Di Muzio, 2019). HT can occur as a result
of two different processes: petechial hemorrhage also commonly referred to as “red softening”
by pathologists or secondary hematoma (Di Muzio, 2019). Petechial hemorrhage usually occurs
within a day of thrombolysis and are seen on neuroimaging as areas of small foci of bleeding
with no associated mass effect and are not thought to affect clinical outcome or management.
Secondary hematoma formation is rarer and occurs in about ~5% of cases and has negative
prognostic implications (Di Muzio, 2019). Secondary hematoma usually occurs within the first 4
days and are rare in the first 6 hours and most commonly occur within 24 hours of ischemia-
reperfusion (Di Muzio, 2019). Some difficulty can occur when the first neuroimaging is obtained
sometime after the symptom onset when hemorrhage is already present. The key to the diagnosis
is the surrounding infarcted brain tissue. In most cases one can see an established non-
hemorrhagic component which conforms to a vascular territory with involvement of the cortex
and subcortical white matter indicating cytotoxic as opposed to vasogenic edema (Di Muzio,
2019). It is possible for large hemorrhagic transformation to occur at the time of acute infarction
especially if a patient has coagulopathy or is pharmacologically anticoagulated (Hutchinson &
Beslow, 2019). It is thought to arise from early ischemic-reperfusion injury as reperfusion of the
damaged vessels is not able to withstand the arterial pressures and ruptures (Di Muzio, 2019).
For this reason, the rates of secondary hematoma formation are significantly higher with acute
reperfusion therapies such as intravenous tPA and mechanical thrombectomy. This makes acute
reperfusion therapy risky as in the process of trying to improve clinical outcome one could
inadvertently worsen it. Therefore, hemorrhagic transformation is used as a safety end point for
most arterial ischemic stroke acute treatment and secondary prevention trials in adults.
In adults, cardioembolic stroke is frequently reported as a risk factor for hemorrhagic
transformation (Lodder et al., 1986). This is thought to be due to ischemia-reperfusion injury
and a significant higher rate of brain herniation and death from embolism causing large vessel

Pulcine 31
occlusion (Lodder et al., 1986). The higher frequency of cardioembolism in those with HT
should be emphasized as a possible mechanistic pathway for the occurrence of HT (Park et al.,
2012). Spontaneous arterial recanalization, which occurs frequently in CE-AIS, can lead to
reperfusion hemorrhage because blood vessels and brain tissue are friable and sensitized
following acute ischemia (Park et al., 2012). No data exits to suggest how long this lasts or what
other factors may contribute. One recent study showed that age, infarct volume and renal
impairment were associated with increased risk for hemorrhagic transformation of acute AIS
(Marsh et al., 2013). The role of renal impairment in intracranial hemorrhage has received more
attention recently. One potential way that renal failure increases bleeding risk is through the
secondary dysfunction of platelets called “uremic platelets” (Marsh et al., 2013). Children with
AIS rarely suffer from chronic renal impairment and so are unlikely to carry the same uremic
platelet risk.
1.13 Summary of Key Points
Currently, anticoagulation is recommended for secondary stroke prevention in pediatric
cardioembolic arterial ischemic stroke where the risk of recurrence is high. No controlled or
prospective data on antithrombotic therapy in pediatric patients with ischemic stroke is available.
Neonates and children increasingly receive antithrombotic therapy based on adult studies.
However, stroke mechanisms and age-related differences in the coagulation system limit
extrapolation of adult safety and efficacy data to children. Risk factors for hemorrhagic
transformation in adults, such as hypertension, older age, and concomitant thrombolytic therapy,
are not represented in most pediatric stroke series. Furthermore, hemorrhagic complication rates
in pediatric cardioembolic arterial ischemic stroke are largely unknown and adult safety data are
of limited applicability. This results in controversy in clinical management and reflects the belief
that not all cardiac conditions have the same associated risk of stroke recurrence. In addition, it
reflects concerns regarding hemorrhagic complications, systemic and intracranial, which could
inadvertently worsen clinical outcome in the process of trying to improve it. Knowing the risk-
benefit ratio of ATT for each primary cardiac diagnosis with respect to primary and secondary
stroke prevention strategies would be clinically useful and provide better care for neonates and
children with cardiac disease and stroke.

Pulcine 32
Chapter 2
Research Aims and Hypothesis
2.1 Rationale and Objectives
Antithrombotic therapy (ATT) decreases the risk of thromboembolism and arterial ischemic
stroke. However, ATT can also increase the risk and exacerbate the degree of intracerebral
hemorrhage. A prior study (Rodan et al., 2012) suggested that one of the predictors of stroke
recurrence in children with congenital heart disease was a lack of effective antithrombotic
therapy despite consensus-based guidelines recommending its use. In this study, out of the 19
children with stroke recurrence, 7 (37%) were not taking any antiplatelet or anticoagulant
medications while 3 (16%) were taking an anticoagulant at subtherapeutic levels (Rodan et al.,
2012). Varying institutional practices reflects the belief that not all congenital or acquired cardiac
conditions have the same associated risk of stroke. Lack of adherence to guidelines reflects the
uncertainty regarding what type of cardiac anatomy, physiology and individual risk factors are
associated with an increased stroke risk and reflects concerns regarding hemorrhagic
transformation exacerbated by ATT. Determining the probability of hemorrhagic transformation
of acute CE-AIS is clinically useful as risk of hemorrhage often needs to be weighed against risk
of recurrent stroke in deciding on whether or not to initiate or escalate ATT in the acute clinical
setting.
Children with a cardioembolic source are more likely to receive antithrombotic therapy. As a
result, the majority will already be on prophylactic or therapeutic therapy at the time of stroke
ictus for a number of various reasons. When faced with a clinical decision to initiate
antithrombotic therapy for secondary stroke prevention, the need for anticoagulation versus the
risk of hemorrhage needs to be carefully weighed. Two questions that need to be considered are:
1) should new or additional antithrombotic therapies be given at the stroke ictus; and 2) what is
the optimal timing of initiation and duration of antithrombotic treatment after CE-AIS in order to
minimize the risk of intracerebral and systemic hemorrhage and to avoid risk of stroke
recurrence? In adults who present with an acute ischemic stroke and have an ongoing indication
for anticoagulation, a risk stratification tool has been developed and validated (Marsh et al.,
2013; Marsh et al., 2016). However, the underlying risk factors for HT differ between pediatric

Pulcine 33
and adult AIS. In adults, older age, hypertension, stroke volume, concomitant thrombolytic
therapy and renal impairment are predictors of HT (Marsh et al., 2013; Marsh et al., 2016;
Schechter et al., 2012). With the exception of stroke volume (Beslow et al., 2011), these risk
factors for HT are largely not represented in the pediatric CE-AIS population. As a result, the
objective of this study is to analyze the clinical and radiological factors associated with
hemorrhagic transformation in infants and children with cardioembolic arterial ischemic stroke
who either are or are not receiving antithrombotic therapy.
Based on clinical experience, we hope to show that antithrombotic therapy is safe in stroke
prevention in children with congenital and acquired heart disease. In addition, this study will
provide crucial safety data that will translate into better care for neonates and children with CE-
AIS and improved clinical and developmental outcomes. At an institutional level, enhanced
collaboration between cardiology and neurology will be strengthened and will advance
harmonized management strategies in children with CE-AIS. Internationally the results will
inform paediatric stroke treatment guidelines and future randomized trial design to determine
ATT safety and efficacy.
2.1.1 Primary Study Aim
1. Describe the rate of hemorrhagic transformation amongst neonates and children with
cardioembolic arterial ischemic stroke.
2. Evaluate the clinical and radiographic factors associated with hemorrhagic transformation
and stroke recurrence to assess the safety of ATT.
2.1.2 Secondary Study Aim
1. Compare clinical outcomes including neurological recovery, stroke recurrence, and death
in neonates and children with cardioembolic arterial ischemic stroke with and without
hemorrhagic transformation.
2.2 Research Questions and Hypothesis
2.2.1 What is the rate of HT amongst neonates and children with CE-AIS?
Based on clinical experience and previously published literature, we hypothesize that the rate of
HT amongst neonates and children with CE-AIS will be slightly higher than the current reported

Pulcine 34
rate in children with arterial ischemic stroke due to all etiologies 11 – 30% (Beslow et al., 2011;
Schechter et al., 2012). Beslow et al found a trend for increased risk of HT in children with
cardiac conditions (RR 1.97; 95% CI: 0.96 – 4.05; p=0.12), although more details about the type
of cardiac anatomy and type of antithrombotic therapy were not available (Beslow et al., 2011).
Children with cardiac disease are at high risk of developing thrombosis and they also have a
higher lifetime exposure to antithrombotic therapy for numerous prophylactic and therapeutic
indications as outlined in Chapter 1. We hypothesized for this reason they would have a higher
incidence of HT. When comparing neonates to older children we hypothesized that neonates
maybe at an even greater risk of HT due to developmental hemostasis. No prior studies have
reported rates of HT in neonates after AIS.
2.2.2 What are the clinical factors associated with HT amongst neonates and children with CE-AIS?
Based on clinical experience we hypothesize a priori that clinical factors associated with
hemorrhagic conversion will include cardiac malformations with uncorrected right-to-left shunts,
single ventricle physiology, atrial arrthymias, infective endocarditis, combination antithrombotic
therapy prior to onset of CE-AIS, tPA or acute endovascular treatment at the time of CE-AIS,
post-procedural CE-AIS, post-cardiotomy ECMO and history of reoperation.
2.2.3 What are the radiological factors associated with HT amongst neonates and children with CE-AIS?
Based on clinical experience and extrapolating from adult stroke literature, we hypothesize a
priori that radiological factors associated with hemorrhagic conversion will include large infarct
size as indirectly measured by the modified pediatric ASPECTS, anterior circulation
involvement, cortical and subcortical involvement which implies larger infarct volume and
presence of other types of intracranial hemorrhage prior to initiation of antithrombotic therapy
including subdural, subarachnoid and intraventricular hemorrhage.
2.2.4 What is the rate of stroke recurrence in neonates and children with cardiac disease and CE-AIS?
We hypothesize that stroke recurrence in those with HT will occur more frequently compared to
those without HT as children deemed to be at higher risk of stroke recurrence would be selected
for more intensive ATT. Overall, we hypothesize that the rate of stroke recurrence in this group

Pulcine 35
would be higher than for other known pediatric stroke etiologies and comparable to the
previously reported rate of 27% at 10 years at our center (Rodan et al., 2012)
2.2.5 Is asymptomatic and/or symptomatic HT associated with worse clinical outcome and death?
It is well recognized that blood products are toxic to the surrounding brain parenchyma both due
to mechanical compression and indirect ischemic injury (Park et al., 2012). In adults,
asymptomatic HT has been shown to adversely affect clinical outcome after acute ischemic
stroke despite lack of acute neurological deterioration (Park et al., 2012). We hypothesize that
both asymptomatic and symptomatic HT will result in worse clinical outcome when compared to
those with no HT, regardless of stroke volume. In addition, we hypothesize that there will be
increased rates of mortality in patients with higher grades of HT as measured by the European
Cooperative Acute Stroke Study, which divides hemorrhagic transformation into four subtypes
(Fiorelli et al., 1999).

Pulcine 36
Chapter 3
Methods
3.1 Study Population and Design
This is a single-center, retrospective study of a prospectively enrolled cohort of neonates (32
weeks to 28 days) and children (29 days to 18 years) with radiologically-confirmed
cardioembolic arterial ischemic stroke from January 2003 – December 2017: a 14-year cohort.
Cases were identified through the SickKids Children’s Stroke Program Database at the Hospital
for Sick Children, Toronto, Ontario, Canada.
3.2 Ethics Approval
Research ethics board approval (#1000059405) was obtained from the Hospital for Sick
Children, Toronto, Ontario, Canada.
3.3 Criteria for Study Participants
Study participants were included if they met all of the following criteria: 1) radiologically-
confirmed cardioembolic arterial ischemic stroke confirming to an established vascular territory
from January 2003 – December 2017; 2) neonates to less than 18 years of age at the time of
diagnosis; and 3) have a primary diagnosis of congenital or acquired heart disease. Although not
required for inclusion, the majority of the study participants were receiving antithrombotic
therapy within 30 days of the stroke: anticoagulants and/or antiplatelet drugs with the primary
indication of secondary stroke prevention. Other indications for antithrombotic therapy included
systemic vein thrombosis, cardiac prophylaxis, extracorporeal membrane oxygenation,
ventricular assist device, cardiac catheterization or cardiopulmonary bypass. Study participants
were excluded if they met any of the following criteria: 1) primary hemorrhagic stroke; 2)
primary cardiac anatomy consistent with an isolated patent foramen ovale (PFO); 3) cerebral
sinovenous thrombosis or vascular malformation; 4) prematurity < 37 weeks at the time of
diagnosis of arterial ischemic stroke; 5) primary stroke etiology due to intracranial vasculopathy
including radiologically-confirmed moyamoya, CNS vasculitis, dissection, or transient cerebral
arteriopathy; 6) primary watershed infarction or hypoxic ischemic encephalopathy; 7)
unavailable imaging studies; and 9) unavailable medical records. A radiologic definition of

Pulcine 37
stroke was used because of difficulty in identifying acute neurological evens in neonates and
children who were receiving postsurgical sedation, pharmacological paralysis and/or anesthesia,
masking symptoms associated with stroke.
3.4 Data Collection
Data were abstracted from hospital records. Data were stored and managed in a REDCap
database at the Hospital for Sick Children (Harris et al., 2009). Patient demographics, cardiac
risk factors, procedural and post-procedural risk factors, antithrombotic therapy, stroke
recurrence and outcome were abstracted from medical records. Normal ranges for blood pressure
based on sex and height were used to classify the first available blood pressure at the time of
stroke ictus into percentiles, where clinically available. Radiological features examined included
type of neuroimaging, stroke location, number of visible infarcts, vascular involvement, stroke
volume using the modified pediatric ASPECTS (Beslow et al., 2012) and hemorrhagic
transformation subtype according to the European Cooperative Acute Stroke Study (Fiorelli et
al., 1999). Details of hemorrhagic transformation including time to hemorrhage, presentation and
clinical symptomatology, need for decompressive craniectomy and hemorrhagic change over
time were collected. Presence of cortical laminar necrosis, scattered foci of susceptibility in
keeping with cerebral microhemorrhages, presence of systemic hemorrhage, hematological
parameters and therapeutic drug monitoring at the time of hemorrhage, presence of coagulopathy
and other types of intracranial hemorrhage including epidural, subdural, subarachnoid and
intraventricular were also collected from medical records and radiological review.
3.5 Cardioembolic Arterial Ischemic Stroke Definition and Subtype
Cardioembolic arterial ischemic stroke (CE-AIS) was defined as confirmed cardiac source of
cerebral embolism, such as structural heart disease with abnormal cardiac function, arrhythmia or
endocarditis. In addition, CE-AIS was defined as having a cardiac procedure within 30 days of
stroke and involvement of medium or large-sized cerebral arteries or multifocal parenchymal
involvement. Radiologically, a discrete and abrupt blockage of an artery consistent with a
thrombus, without any surrounding irregularity or stenosis suggestive of arteriopathy was
defined as consistent with CE-AIS.

Pulcine 38
Cardiac anatomy and physiology were categorized first based on the initial structural heart
abnormality: cyanotic, acyanotic, cardiomyopathy, infective endocarditis, valvular dysfunction
or primary arrhythmia; and subsequently on biventricular vs. univentricular physiology.
Procedure-related cardioembolic arterial ischemic stroke was defined as CE-AIS that occurred
within 30 days of cardiac surgery or catheterization. When both cardiac surgery and cardiac
catheterization occurred in close proximity, without intervening neuroimaging, this was defined
as multiprocedural CE-AIS. All other CE-AIS was defined as non-procedural. A sub-analysis
was performed on those with procedure-related arterial ischemic stroke within 72 hours of the
cardiac procedure.
Further subgrouping of patients with procedure-related stroke was performed based on cardiac
anatomy and associated surgical management at the time of stroke: 1) cyanotic CHD post-
palliative surgery (residual right-to-left shunting); 2) cyanotic CHD post-definitive surgery (no
residual right-to-left shunting); and 3) acyanotic CHD post-surgery. Reoperation was defined as
previous cardiac surgery not within the same cardioembolic stroke admission.
3.6 Infarct Size Analysis
In dating ischemic stroke, tables from previously published methods (Allen, Hasso, Handwerker,
& Farid, 2012) were used as a reference with particular attention to diffusion-weighted imaging
when MRI was available. Infarct size was estimated using the modified pediatric ASPECTS
scoring system described by Lauren Beslow (Beslow et al., 2012). Modified pediatric ASPECTS
on acute MRI estimates arterial ischemic stroke volume as a percent of supratentorial brain
volume for perinatal and childhood infarction with excellent interrater reliability (Beslow et al.,
2012). However, the modified pediatric ASPECTS overestimated stroke volume in multifocal
ischemic stroke (Beslow et al., 2012). In addition, it does not account for infratentorial stroke
volume (cerebellar or brainstem) and has not been validated on CT in children. With the
exception of CT neuroimaging, these limitations to the modified pediatric ASPECTS precluded
its use in the aforementioned circumstances and those scores were omitted from the final analysis
of infract size.

Pulcine 39
3.7 Hemorrhagic Transformation Analysis
Based on institutional guidelines, CT or MRI scans were performed on average 3 to 5 days post
antithrombotic therapy initiation or escalation and with any clinical suspicion of neurological
deterioration. Additional follow-up imaging was individualized. Hemorrhagic transformation
was defined as any imaging evidence of intracerebral hemorrhage in the area of ischemic
infarction within the first 30 days from radiologic CE-AIS diagnosis. Other types of intracranial
hemorrhage including subdural, subarachnoid, and intraventricular were excluded from this
definition and were captured separately, with the exception of one case where all three were
present post ATT initiation and led to the patient’s death. Hemorrhagic transformation was
classified by the method used in the European Cooperative Acute Stroke Study (Fiorelli et al.,
1999) which include the following definitions: H0 – no hemorrhage; HI1 – punctate petechial
hemorrhage without space-occupying effect; HI2 – confluent petechial hemorrhage; PH1 – small
parenchymal hemorrhage less than 30% of the infarcted area with mild mass effect; PH2 – large
parenchymal hemorrhage with greater than 30% of the infarcted area with significant mass effect
or hemorrhagic transformation remote from the stroke location. In cases of more than 1 area of
hemorrhagic transformation on CT or MRI examination, the highest ECASS category was
assumed. Presence of hemorrhagic transformation was primarily determined by visual
inspection: hemorrhage was identified on non-contrast head CT as areas of hyperdensity and on
MRI as areas of hypointensity on T2-gradient ECHO (GRE) and/or MR susceptibility-weighted
imaging (SWI) sequences. All CT and MRI images were reviewed by a neuroradiologist
(Sunitha Palasamudram) who was blinded to the clinical characteristics and progression towards
hemorrhagic transformation. A second neuroradiologist (Manohar Shroff) adjudicated any
challenging cases including instances where the previous two reviewers disagreed on the
presence of hemorrhagic transformation, ECASS classification or presence of cortical laminar
necrosis. In order to distinguish between cortical laminar necrosis and ECASS HI1, where
possible, SWI was used to review the area of interest and if no susceptibility or blooming was
seen on SWI then cortical laminar necrosis was confirmed. In other instances, where SWI was
not available, presence of cortical laminar necrosis vs. HI1 was made at the discretion of the
neuroradiologist (SP and MS). Change in ECASS scores over time were documented.
Neonates and children with hemorrhagic conversion were considered to be symptomatic if they
had new or worsening neurological deficits, headache, and/or seizures. Patients that were sedated

Pulcine 40
and/or receiving neuromuscular blockade at the time of the radiologically confirmed
hemorrhagic transformation, where clinical examination was limited, were categorized as
unknown.
Presence of other types of intracranial hemorrhage were abstracted from visual inspection of CT
or MRI images and/or medical records. Other type of intracranial hemorrhage included: epidural,
subdural, subarachnoid, and intraventricular hemorrhage.
3.8 Antithrombotic Therapy
Treatment for secondary stroke prevention was based on institutional guidelines (see Appendix).
Antithrombotic therapy was individualized at the discretion of the caring team in consultation
with the inpatient thrombosis and stroke services. Treatment was categorized as follows: 1)
anticoagulant therapy (ACT) – receiving unfractionated heparin, low molecular weight heparin
or warfarin; 2) antiplatelet therapy (APT) – receiving aspirin or clopidogrel or dipyridamole or ;
3) antiplatelet and anticoagulant (APT + ACT) – receiving any combination of anticoagulant and
antiplatelet therapy simultaneously; and 4) neither – receiving no anticoagulant nor antiplatelet
therapy. Antithrombotic therapy was subsequently categorized into monotherapy or combination
therapy. Combination therapy was further subdivided into sequential (one after the other) and/or
concurrent (at the same time or simultaneous) with unfractionated heparin, low-molecular-
weight heparin, warfarin, aspirin, clopidogrel and/or dipyridamole. Dosing for secondary stroke
prevention based on institutional guidelines and published reference guidelines (Monagle et al.,
2012) was as follows: UFH commenced without a bolus, with an initial maintenance dose ≤ 1
year of age: 28 units/kg/hr IV or > 1 year of age: 20 units/kg/hr IV and titrated to anti-factor Xa
level of 0.35 – 0.7 IU/mL; LMWH initial maintenance dose ≤ 2 months of age: 1.5 mg/kg/dose
SC every twelve hours or > 2 months of age: 1 mg/kg/dose SC every twelve hours and titrated to
anti-factor Xa level of 0.5 – 1.0 IU/mL; warfarin initial maintenance dose of 0.2 mg/kg/day PO
titrated to international normalized ratio of 2. 0 – 3.0; ASA maintenance dose of 3 – 5 mg/kg/day
PO; clopidogrel maintenance dose of 1 mg/kg/day PO; dipyridamole maintenance dose of 1.7
mg/kg/dose PO three times a day and used exclusively in patients with a ventricular assist
device. Antithrombotic therapy dose (loading and/or maintenance) and duration (start and stop
dates) were collected where available. Dose was calculated based on the patient’s weight at the
time of the sentinel CE-AIS. The maximum dose of LMWH used was 4.8 mg/kg/dose and the

Pulcine 41
maximum dose of warfarin used was 0.61mg/kg/day. Two children also received thrombolysis
with intravenous tissue plasminogen activator (tPA) with individualized dosing based on weight
and indication. Laboratory parameters at the time of CE-AIS diagnosis and at the time of HT
were collected, where available, including complete blood count, coagulation parameters, and
anticoagulant therapeutic drug monitoring.
3.9 Stroke Recurrence
Stroke recurrence was defined as recurrent AIS or transient ischemic attack (TIA) occurring > 24
hours after sentinel CE-AIS. Recurrent symptomatic stroke was defined as acute neurological
deficit or seizure with acute infarction noted on CT or MRI. TIA was defined as an acute
neurological deficit lasting < 24 hours duration not attributed to seizure, migraine or other cause
and with no infarction noted on imaging. Silent infarct was defined as infarction noted on CT or
MRI with no clinical symptoms or signs.
3.10 Neurological Outcome
Patients were followed in serial stroke clinic visits. Clinical outcomes were determined at the
latest follow-up by a pediatric stroke neurologist using the validated pediatric stroke outcome
measure (PSOM) (Kitchen et al., 2012). Five PSOM subscores are graded using the following
definitions: 0 – no deficit; 0.5 – mild deficit that does not interfere with function; 1 – moderate
deficit that interferes with function; and 2 – severe deficit with loss of function (Kitchen et al.,
2012). The total PSOM score spans from 0 (no deficit) – 10 (severe) (Kitchen et al., 2012).
Maximal score (10) was imputed for children who died due to any cause. A new validated
PSOM classification scoring system was used to determine clinical outcome (Slim M, 2018).
Outcome was further dichotomized into good if the PSOM was normal or mild and poor
outcome if the PSOM outcome was moderate, severe or the patient was deceased for any reason.
Clinical outcomes were compared in children with and without hemorrhagic transformation.
3.11 Statistical Analysis
An exploratory analysis of the relationship between antithrombotic therapy and hemorrhagic
transformation was performed. Data were summarized using descriptive statistics. Continuous
variables were summarized as means (standard deviations) or medians (interquartile ranges) and
categorical variables summarized as frequencies (percentage). Clinical and radiological

Pulcine 42
characteristics of neonates and children with and without hemorrhagic transformation were
compared using Chi-square or Fisher’s exact test for categorical variables and Wilcoxon Mann-
Whitney test for nonparametric continuous variables. As a measure of association between HT
and other independent variables we calculated an odds ratio (OR) or relative risk (RR), where
appropriate, with 95% confidence intervals (CI) by means of logistic regression analysis. Given
the small sample size, multivariable logistic regression analysis was performed only for outcome
and infarct size, where the relationship between 1) hemorrhagic transformation and 2) infarct
volume were used to determine the impact on clinical outcome measured by the PSOM. A two-
tailed p-value of < 0.05 was considered to be significant and 0.06 – 0.10 considered as a trend.
Data analysis was performed by using SAS 9.4 software (SAS Institute Inc., Cary, NC, USA).

Pulcine 43
Chapter 4
Results
4.1 Patient Characteristics
Two hundred and twelve children were identified based on the initial screening criteria with 119
excluded for reasons outlined in Figure 1. A further 11 patients were excluded from the final
analysis due to hemorrhagic transformation on their initial neuroimaging, the exact timing of
which could not be determined due to the retrospective nature of the study.
Figure 1. Methods flow chart.
Eighty-two children met inclusion criteria [male 44 (54%); mean age 3.0 ± 4.8 years]. Median
age at stroke ictus was 0.43 years [IQR 0.08 – 4.23] with 23 (28%) of the cohort less than 28
days of life at the time of radiologically-confirmed CE-AIS. None of the subjects were less than
37 weeks’ gestation at the time of stroke. The median weight was 5.24 kilograms [IQR 3.72 –
15.9]. Demographic data and primary cardiac diagnosis are listed in Table 3. There was no
difference in sex, age, weight or proportion of neonates between those with and without HT.
Total
(n=82) HT (n=20)
No HT
(n=62)
P-
value†
Mean Age (years ±±±± SD) 3.02 ± 4.80 3.03 ± 5.18 3.01 ± 4.72 0.67
212 Patients were screened based on the initial inclusion criteria
SickKids Children’s Stroke Program Registry
January 2003 – December 2017
119 Were excluded → met at least one exclusion criterion:
72 Isolated patent foramen ovale (PFO)
21 Imaging studies unavailable
7 Cerebral venous sinus thrombosis (CSVT)
7 Intracranial vasculopathy
3 Vein of Galen malformations (VOGMs)
3 Acute myeloid leukemia (AML)
2 Watershed infarction/hypoxic ischemic encephalopathy (HIE)
2 Prematurity <32 weeks
2 Trauma
93 Were eligible
Cyanotic Heart
Disease 49 (60%)
Cardiomyopathy/
Myocarditis 14 (17%)
Acyanotic Heart
Disease 13 (16%)
Infective Endocarditis
3 (4%)
Primary Arrhythmia
2 (2%)
Rheumatic Heart
Disease 1 (1%)
11 Were excluded → due to early hemorrhagic transformation on
their initial neuroimaging
82 Final analysis

Pulcine 44
Median Age (years [IQR]) 0.43 [0.08 –
4.23]
0.44 [0.05 –
3.66]
0.40 [0.08 –
4.22] 0.67
Male Gender (%) 44 (54%) 13 (30%) 31 (70%) 0.24
Neonates (< 28 days of life), n (%) 23 (28%) 6 (26%) 17 (74%) 0.82
Primary Cardiac Diagnosis
Cyanotic Heart Disease 49 (60%) 12 (24%) 37 (76%) 0.04
Acyanotic Heart Disease 13 (16%) 1 (8%) 12 (92%) 0.69
Cardiomyopathy/Myocarditis 14 (17%) 4 (29%) 10 (71%) 0.74
Other 6 (7%) 3 (50%) 3 (50%) 1.00
Univentricular Physiology, n (%) 30 (37%) 3 (10%) 27 (90%) 0.03
Procedure-Related Stroke Within 30
Days 50 (61%) 10 (20%) 40 (80%) 0.25
Table 3. Baseline patient characteristics and primary cardiac diagnoses.
†Chi-square or Fisher’s exact test for categorical variables and Wilcoxon Mann-Whitney test for nonparametric
continuous variables
4.1.1 Blood Pressure
Systolic and diastolic blood pressure data were available in 29 (35%) children at the time of
stroke presentation and a large proportion 53 (65%) were missing values. Given that a significant
number of CE-AIS were procedure-related (61%) the exact time of onset was not always clear
due to prolonged postsurgical sedation and pharmacological paralysis. Furthermore, there was a
large proportion of missing height measurements (40%) which are needed to convert isolated
blood pressure values to blood pressure norms and percentiles in neonates and children. For all
these reasons, blood pressure determination could not be performed accurately and was omitted
from the final analysis.
4.2 Cardiac Diagnosis and Interventional Procedures
4.2.1 Cardiac Diagnosis
Primary cardiac diagnosis included 49 (60%) children with cyanotic heart disease, 13 (16%) with
acyanotic heart disease, 14 (17%) with cardiomyopathy/myocarditis, 3 (4%) with infective
endocarditis, 2 (2%) with primary arrhythmia and 1 (1%) with rheumatic heart disease.
Additional breakdown including the details of the type of cardiac structural defect are listed in
Table 4. Other type of cyanotic heart disease included right atrial isomerism with unbalanced
atrioventricular septal defect (AVSD) and total anomalous pulmonary venous connection
(TAPVC) to the right superior vena cava. Other types of acyanotic heart disease included left

Pulcine 45
intramural coronary artery and left ventricular failure related to thrombus in the aortic root and
coronary artery. There was a trend towards the presence of primary arrhythmia in those with HT
[p=0.06] (Table 4).
Primary Cardiac Diagnosis Total (n=82) HT (n=20) No HT (n=62) P-value†
Cyanotic Heart Disease 49 (60%) 12 (24%) 37 (76%) 0.04
HLHS, SV 16 (33%) 1 (6%) 15 (94%)
TOF, PA/VSD, DORV 13 (27%) 4 (31%) 9 (69%)
TA 5 (10%) 0 5 (100%)
PA/IVS, critical PS 5 (10%) 2 (40%) 3 (60%)
TGA 8 (16%) 4 (50%) 4 (50%)
ccTGA 1 (2%) 1 (100%) 0
Other 1 (2%) 0 1 (100%)
Acyanotic Heart Disease 13 (16%) 1 (8%) 12 (92%) 0.69
ASD 2 (15%) 0 2 (100%)
VSD 1 (8%) 0 1 (100%)
CoA 3 (23%) 1 (33%) 2 (67%)
AoV/MV 4 (31%) 0 4 (100%)
AVSD 1 (8%) 0 1 (100%)
Other 2 (15%) 0 2 (100%)
Cardiomyopathy/Myocarditis 14 (17%) 4 (29%) 10 (71%) 0.74
Infective Endocarditis 3 (4%) 1 (33%) 2 (67%) 1.00
Rheumatic Heart Disease 1 (1%) 0 1 (100%) 1.00
Primary Arrhythmia 2 (2%) 2 (100%) 0 0.06
Table 4. Additional breakdown of the primary cardiac diagnoses.
ASD=atrial septal defect; AoV/MV=aortic/mitral valve abnormalities; AVSD=atrioventricular septal defect;
ccTGA=congenitally corrected transposition of the great arteries; CoA=coarctation of the aorta; DORV=double
outlet right ventricle; HLHS=hypoplastic left heart syndrome; PA=pulmonary atresia; PA/IVS=pulmonary atresia
with intact ventricular septum; PS=pulmonary stenosis; SV=single ventricle; TA=tricuspid atresia;
TGA=transposition of the great arteries; ToF=tetralogy of Fallot; VSD=ventricular septal defect
†Chi-square or Fisher’s exact test for categorical variables
Children with cyanotic heart disease accounted for more than half of all the cases of
radiologically confirmed CE-AIS 60% (49/82); among those 23% (19/49) had biventricular
physiology and 61% (30/49) had univentricular physiology. Across all types of primary cardiac
diagnosis, those children with biventricular physiology were significantly more likely to have
hemorrhagic transformation [OR 3.27 95% CI: 1.04 – 10.24; p=0.03]. In addition, there was a
significant difference in the type of cyanotic heart disease between the two groups with
hypoplastic left heart syndrome (HLHS) and tricuspid atresia (TA), both of which comprise

Pulcine 46
single-ventricle physiology, more commonly represented in the group without hemorrhagic
transformation (Table 4).
4.2.2 Procedural Risk
Sixty-one percent of children had procedure-related CE-AIS. The number of children with
additional cardiac and non-cardiac stroke risk factors, procedure-related stroke and procedural-
complications are listed in Table 5. Additional breakdown and details of the type of risk factors,
procedures and complications are listed in Table 6. None of these factors were significantly
different between the two groups with the exception of cardiac catheterization which occurred
more frequently in those with HT [67% vs. 33%; p=0.07] but did not reach statistical
significance (Table 5).
Total
(n=82) HT (n=20)
No HT
(n=62)
P-
value†
Additional Cardiac Risk Factors 38 (46%) 8 (21%) 30 (79%) 0.51
Additional Non-Cardiac Risk Factors 30 (37%) 10 (33%) 20 (67%) 0.15
Procedure-Related Stroke Within 30
Days 50 (61%) 10 (20%) 40 (80%) 0.25
Cardiovascular Surgery 23 (46%) 3 (13%) 20 (87%) 0.31
Cyanotic CHD Post-Palliative 15 (30%) 2 (13%) 13 (87%) 0.70
Cyanotic CHD Post-Definitive 4 (8%) 1 (25%) 3 (75%) 1.00
Acyanotic CHD Post-Surgery 8 (16%) 0 8 (100%) 0.18
Catheterization 21 (42%) 7 (33%) 14 (67%) 0.07
Multiprocedural 6 (12%) 0 6 (100%) 0.33
Post-Procedural Complications 18 (36%) 2 (11%) 16 (89%) 0.25
Postcardiotomy ECMO 4 (8%) 0 4 (100%) 0.57
Reoperation 24 (29%) 4 (17%) 20 (83%) 0.40
Table 5. Additional cardiac, non-cardiac and procedural risk factors associated with
cardioembolic arterial ischemic stroke.
CHD=congenital heart disease; ECMO=extracorporeal membrane oxygenation
†Chi-square or Fisher’s exact test for categorical variables
Total
(n=82)
HT
(n=20)
No HT
(n=66)
P-
value†
Additional Cardiac Risk Factors 38 (46%) 8 (21%) 30 (79%)
0.51
Previous CBP 27 (33%) 6 (22%) 21 (78%)
Acquired Arrhythmia 11 (13%) 3 (27%) 8 (73%)
Previous ECMO 6 (7%) 1 (17%) 5 (83%)
Infective Endocarditis 2 (2%) 0 2 (100%)
Mechanical Valve 1 (1%) 1 (100%) 0

Pulcine 47
Additional Non-Cardiac Risk Factors 30 (37%) 10 (33%) 20 (67%)
0.15
Systemic Infection/Meningitis 21 (26%) 6 (29%) 15 (71%)
Cardiogenic/Hypovolemic Shock 16 (20%) 6 (38%) 10 (62%)
Prothrombotic State 4 (5%) 0 4 (100%)
Hypoxia-Asphyxia 3 (4%) 0 3 (100%)
Systemic Vasculopathy 1 (1%) 1 (100%) 0
Procedure-Related Stroke Within 30
Days 50 (61%) 10 (20%) 40 (80%)
0.25 Cardiac Surgery 23 (46%) 3 (13%) 20 (87%)
Catheterization 21 (42%) 7 (33%) 14(67%)
Balloon Atrial Septostomy 9 (43%) 4 (44%) 5 (56%)
Multiprocedural 6 (12%) 0 6 (100%)
Post-Procedural Complications 18 (36%) 2 (11%) 16 (89%)
0.25
Vasopressor/Inotropic Support 6 (12%) 1 (17%) 5 (83%)
Mechanical Circulatory Support 5 (10%) 1 (20%) 4 (80%)
Dysrhythmias 4 (8%) 0 4 (100%)
Systemic Infection 2 (4%) 0 2 (100%)
Intraoperative Complication 2 (4%) 0 2 (100%)
Cardiac Arrest 2 (4%) 0 2 (100%)
Post-Operative Bleeding 2 (4%) 0 2 (100%)
Table 6. Details of additional cardiac, non-cardiac and procedural risk factors associated with
cardioembolic arterial ischemic stroke.
ECMO=extracorporeal membrane oxygenation
†Chi-square or Fisher’s exact test for categorical variables
Additional cardiac risk factors, which were not mutually exclusive, occurred in 38 (46%)
children and did not differ between the two groups [8 (21%) vs. 30 (79%); p=0.51]. They
included 27 (33%) children with previous history of cardiopulmonary bypass, 11 (13%) with
acquired arrhythmia managed through medication and/or pacemaker, 6 (7%) with previous
history of extracorporeal circulatory support, 2 (2%) with previous history of infective
endocarditis and 1 (1%) with prior mechanical valve insertion (Table 6).
Additional non-cardiac stroke risk factors, which were not mutually exclusive, occurred in 30
(37%) children and did not differ between the two groups [10 (33%) vs. 20 (67%); p=0.15]. They
included 21 (26%) children with systemic infection/meningitis/encephalitis, 16 (20%) with
cardiogenic/hypovolemic/or septic shock, 4 (5%) with prothrombotic states, 3 (4%) with anoxia-
asphyxia and 1 (1%) with systemic vasculopathy in the form of Takayasu’s arteritis which was
diagnosed after the initial CE-AIS presentation. This sole patient with systemic vasculopathy did
not have any intracranial vasculopathy and presented with an intracardiac thrombus which
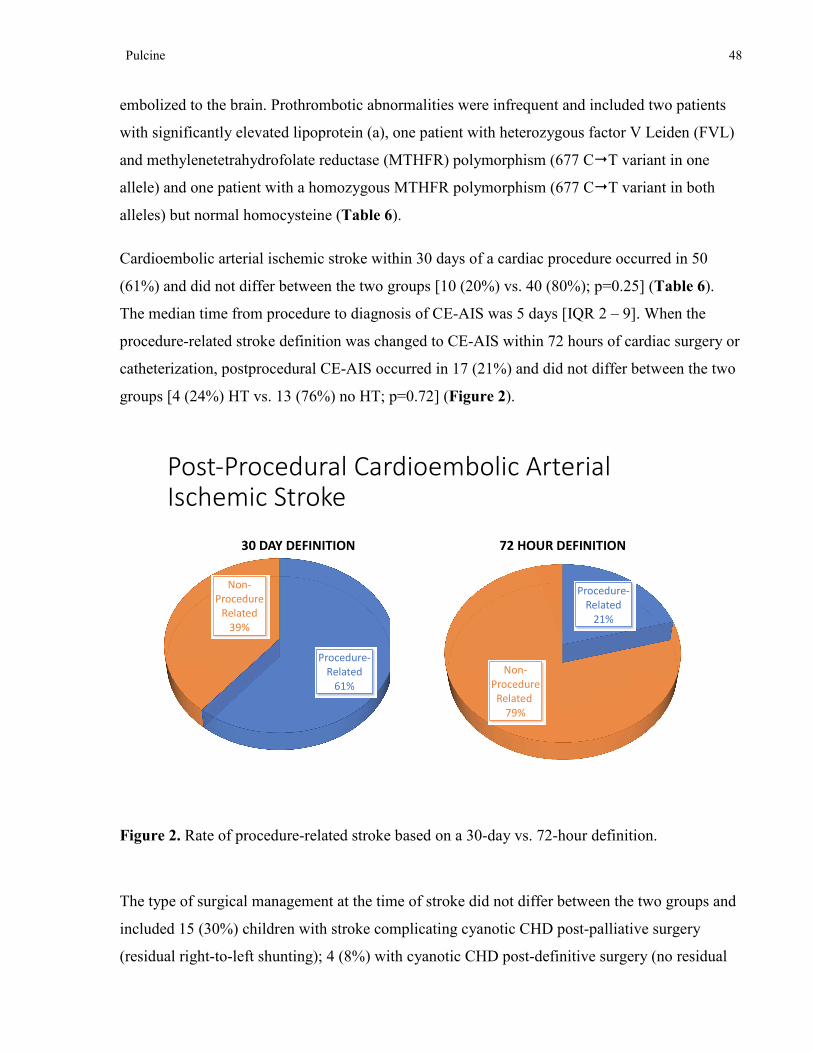
Pulcine 48
embolized to the brain. Prothrombotic abnormalities were infrequent and included two patients
with significantly elevated lipoprotein (a), one patient with heterozygous factor V Leiden (FVL)
and methylenetetrahydrofolate reductase (MTHFR) polymorphism (677 C�T variant in one
allele) and one patient with a homozygous MTHFR polymorphism (677 C�T variant in both
alleles) but normal homocysteine (Table 6).
Cardioembolic arterial ischemic stroke within 30 days of a cardiac procedure occurred in 50
(61%) and did not differ between the two groups [10 (20%) vs. 40 (80%); p=0.25] (Table 6).
The median time from procedure to diagnosis of CE-AIS was 5 days [IQR 2 – 9]. When the
procedure-related stroke definition was changed to CE-AIS within 72 hours of cardiac surgery or
catheterization, postprocedural CE-AIS occurred in 17 (21%) and did not differ between the two
groups [4 (24%) HT vs. 13 (76%) no HT; p=0.72] (Figure 2).
Figure 2. Rate of procedure-related stroke based on a 30-day vs. 72-hour definition.
The type of surgical management at the time of stroke did not differ between the two groups and
included 15 (30%) children with stroke complicating cyanotic CHD post-palliative surgery
(residual right-to-left shunting); 4 (8%) with cyanotic CHD post-definitive surgery (no residual
Post-Procedural Cardioembolic Arterial Ischemic Stroke
Procedure-
Related
61%
Non-
Procedure
Related
39%
30 DAY DEFINITION
Procedure-
Related
21%
Non-
Procedure
Related
79%
72 HOUR DEFINITION
Post-Procedural Cardioembolic Arterial Ischemic Stroke
Procedure-
Related
61%
Non-
Procedure
Related
39%
30 DAY DEFINITION
Procedure-
Related
21%
Non-
Procedure
Related
79%
72 HOUR DEFINITION

Pulcine 49
right-to-left shunting); and 8 (16%) acyanotic CHD post-surgery. The types of palliative and
definitive cardiac repairs performed at the time of the perioperative CE-AIS are illustrated in
Figures 3 and 4. At the time of cardiac surgery, most patients required cardiopulmonary bypass
22 (96%). Rate of reoperation, or number of previous cardiac surgeries, was not significantly
different between those with and without HT [4 (17%) vs. 20 (83%); p=0.40] (Table 5).
Figure 3. Details of palliative cardiac surgery associated with procedural CE-AIS.
Type of Palliative Cardiac Surgery
Bidirectional
Cavopulmonary Shunt
19%
Norwood
31%
Systemic-to-Pulmonary
Artery Shunts
25%
Fontan
19%
Other
6%

Pulcine 50
Figure 4. Details of definitive cardiac surgery associated with procedural CE-AIS.
In order to account for possible changes in surgical practice over a 14-year period (2003 – 2017)
a histogram was constructed to look at the frequency of procedure-related stroke by year as
illustrated in Figure 5. While the average number of procedure-related CE-AIS per year was 3.3
± 1.7 [1 – 7] there was an apparent higher rate in 2004 [6] and in 2016 [7] with no specific trend
observed over the course of the 14-year period.
Type of Definitive Cardiac Repair
Right Ventricular
Outflow Tract
Reconstruction
22%
Ventricular Septal
Defect Closure
17%
Valvular Repair
5%Atrial Septal Defect Closure
11%
Atrioventricular
Septal Defect Repair
5%
Arterial Switch
Operation
5%
Aortic Arch Repair
6%
Orthotopic Heart
Transplant
6%
Ventricular Assist
Device Implantation
6%
Other
17%

Pulcine 51
Figure 5. Frequency of procedure-related stroke based on a 30-day definition over a 14-year
period (2003 – 2017).
Post-procedural systemic and cardiac complications occurred in 18 (36%) children, which were
not mutually exclusive, and did not differ between the two groups [2 (11%) vs. 16 (89%);
p=0.25]. They included 6 (12%) with vasopressor and inotropic support, 5 (10%) with
mechanical circulatory support, 4 (8%) with dysrhythmias, 2 (4%) with systemic
infection/sepsis, 2 (4%) with intraoperative complication/injury, 2 (4%) with cardiac arrest and 2
(4%) with post-operative systemic bleeding (Table 6).
4.3 Radiological Features
4.3.1 Imaging Timing and Modalities
Timing and modality of imaging varied widely in this cohort due to variations in patient
presentation, clinical severity and availability of imaging. Initial neuroimaging that was used to
diagnose CE-AIS included CT in 49 (60%) and MRI in 33 (40%). The median number of follow-
up images within 30 days of stroke was two after the initial scan [IQR 1 – 2]. Eight patients did
not have follow-up imaging within 30 days of CE-AIS but went on to have subsequent
neuroimaging outside of this time window.

Pulcine 52
4.3.2 Stroke Characteristics
The salient radiological features of CE-AIS are listed in Table 7. At the time of diagnosis, 41
(50%) had a single visible infarct, 32 (39%) had evidence of multiple concurrent infarcts and 9
(11%) had multiple infarcts of different ages (recurrent infarcts). CE-AIS laterality was
distributed as follows: 50 (61%) unilateral [right-sided 26 (52%); left-sided 24 (48%)], 16 (20%)
bilateral and 16 (20%) multifocal. Anterior circulation stroke occurred in 57 (70%), posterior
circulation stroke occurred in 5 (6%), and 20 (24%) had both anterior and posterior circulation
involvement. Infarcts involving both the cortical and subcortical regions (white matter or basal
ganglia) were seen in the majority of stroke patients 68 (83%) while pure subcortical
involvement was seen in 14 (17%) (Table 7).
Total (n=82) HT (n=20) No HT (n=62) P-
value†
CE-AIS Number of Visible Infarcts
Single 41 (50%) 11 (27%) 30 (73%) 0.71
Multiple –
Concurrent
(Same Age)
32 (39%) 8 (25%) 24 (75%)
Multiple –
Different Ages 9 (11%) 1 (11%) 8 (89%)
CE-AIS Laterality
Unilateral 50 (61%) 12 (24%) 38 (76%)
1.00 Bilateral 16 (20%) 4 (25%) 12 (75%)
Multifocal 16 (20%) 4 (25%) 12 (75%)
Anterior Circulation 57 (70%) 14 (25%) 43 (75%) 0.96
Posterior Circulation 5 (6%) 0 5 (100%) 0.33
Anterior + Posterior
Circulation 20 (24%) 6 (30%) 14 (70%) 0.50
Cortical + Subcortical
Involvement 68 (83%) 19 (28%) 49 (72%) 0.17
Subcortical
Involvement Only 14 (17%) 1 (7%) 13 (93%) 0.17
Modified Pediatric
ASPECTS (mean ±±±±
SD [range])
4.3 ± 2.8 [1 – 13] 6.1 ± 3.3 [2 – 13] 3.5 ± 2.3 [1 – 9] 0.006
ECASS Hemorrhagic
Transformation
Subtype (% of all CE-
AIS)
20 (24%)
HI1 (% of HT) 9 (45%)
HI2 (% of HT) 6 (30%)
PH1 (% of HT) 4 (20%)
PH2 (% of HT) 1 (5%)

Pulcine 53
Symptomatic HT (%
of HT) 5 (25%)
HT Change Over
Time (% of HT) 3 (15%)
Median Time to HT
(days [IQR]) 4.0 [3.0 – 7.5]
Other Types of Intracranial Hemorrhage
Subdural 20 (24%) 5 (25%) 15 (75%) 1.00
Subarachnoid 2 (2%) 2 (100%) 0 0.06
Intraventricular 3 (4%) 2 (67%) 1 (33%) 0.15
Systemic Hemorrhage 4 (5%) 2 (50%) 2 (50%) 0.25
Cortical Laminar
Necrosis 11 (13%) 1 (9%) 10 (91%) 0.28
SWI+
Microhemorrhages 14 (17%) 2 (14%) 12 (86%) 0.50
Table 7. Radiological features of pediatric cardioembolic arterial ischemic stroke.
ASPECTS=Alberta Stroke Program Early CT Score; CE-AIS=cardioembolic arterial ischemic stroke;
ECASS=European Cooperative Acute Stroke Study; HT=hemorrhagic transformation; SWI=susceptibility weighted
imaging
†Chi-square or Fisher’s exact test for categorical variables and Wilcoxon Mann-Whitney test for nonparametric
continuous variables
4.3.3 Modified Pediatric ASPECTS – Stroke Volume
The modified pediatric ASPECTS was calculated at the time of radiologic CE-AIS diagnosis
using available DWI MRI or non-contrast CT. Five children had infratentorial involvement (i.e.
brainstem/cerebellum) while 21 had multifocal involvement; therefore, the modified pediatric
ASPECTS could not be accurately calculated in these 26 cases and they were excluded from the
final analysis of stroke volume [4 excluded from HT group and 22 excluded from non-HT
group]. The mean modified pediatric ASPECTS score in children was 4.3 ± 2.8 [1 – 13]. The
mean modified pediatric ASPECTS score in children with and without HT was significantly
different [6.1 ± 3.3 vs. 3.5 ± 2.3; p=0.006] (Table 7).
4.4 Hemorrhagic Transformation and ECASS
Table 8 summarizes the salient clinical and radiological data on the 31 children with HT divided
into two groups: those that had HT on day 0 at the time of diagnosis (n=11) and those that had
HT on their follow-up neuroimaging after antithrombotic therapy was initiated (n=20). We could
not ascertain the exact timing of HT in relation to antithrombotic therapy due to the

Pulcine 54
observational nature of this study. As a result, these 11 cases were excluded from the final
analysis.
As illustrated in Table 7 and Figure 6, of the remaining 82 children HT occurred in 20 (24%), 5
(6%) of whom were symptomatic. Hemorrhage classification was as follows: HI1 in 9 (45%),
HI2 in 6 (30%), PH1 in 4 (20%) and PH2 in 1 (5%). Representative CT scans showing the type
of hemorrhagic transformation is shown in Figure 7.
Figure 6. ECASS classification of hemorrhagic transformation.
ECASS=European Cooperative Acute Stroke Study
Hemorrhagic Transformation 24% (20/82)
HI1
45%
HI2
30%
PH1
20%
PH2
5%
ECASS HEMORRHAGIC CLASSIFICATION
Symptomatic HT in 5 (6%) within 15 days of stroke
Median time to HT 4 days [IQR 3 – 7.5]

Pulcine 55
Figure 7. Representative CT scans showing types of hemorrhagic transformation.
The median time to HT was 4 days [IQR 3 – 7.5]. Figure 8 shows the timing of HT from
radiological CE-AIS diagnosis distributed by the type of antithrombotic therapy. There appears
to be a peak of HT at 48 – 72 hours (Figure 8). No HT occurred while on antiplatelet therapy
alone or on no antithrombotic therapy.
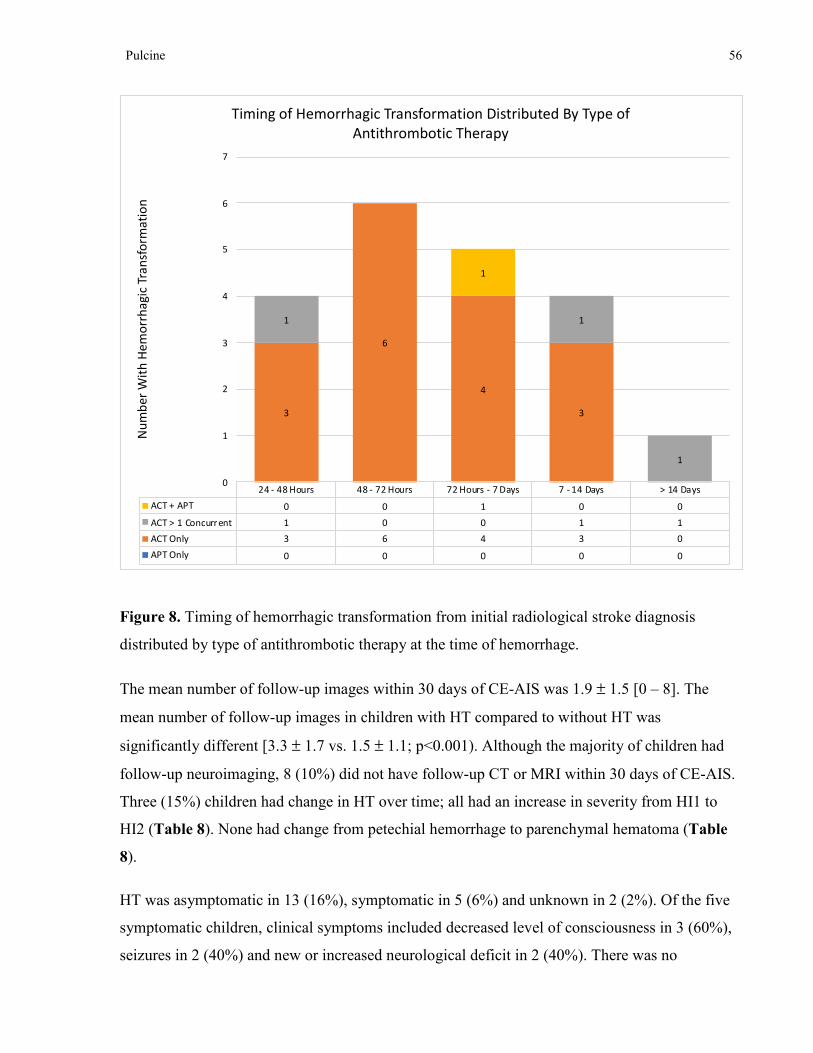
Pulcine 56
Figure 8. Timing of hemorrhagic transformation from initial radiological stroke diagnosis
distributed by type of antithrombotic therapy at the time of hemorrhage.
The mean number of follow-up images within 30 days of CE-AIS was 1.9 ± 1.5 [0 – 8]. The
mean number of follow-up images in children with HT compared to without HT was
significantly different [3.3 ± 1.7 vs. 1.5 ± 1.1; p<0.001). Although the majority of children had
follow-up neuroimaging, 8 (10%) did not have follow-up CT or MRI within 30 days of CE-AIS.
Three (15%) children had change in HT over time; all had an increase in severity from HI1 to
HI2 (Table 8). None had change from petechial hemorrhage to parenchymal hematoma (Table
8).
HT was asymptomatic in 13 (16%), symptomatic in 5 (6%) and unknown in 2 (2%). Of the five
symptomatic children, clinical symptoms included decreased level of consciousness in 3 (60%),
seizures in 2 (40%) and new or increased neurological deficit in 2 (40%). There was no
24 - 48 Hours 48 - 72 Hours 72 Hours - 7 Days 7 - 14 Days > 14 Days
ACT + APT 0 0 1 0 0
ACT > 1 Concurrent 1 0 0 1 1
ACT Only 3 6 4 3 0
APT Only 0 0 0 0 0
3
6
4
3
1 1
1
1
0
1
2
3
4
5
6
7
Nu
mb
er
Wit
h H
em
orr
ha
gic
Tra
nsf
orm
ati
on
Timing of Hemorrhagic Transformation Distributed By Type of
Antithrombotic Therapy

Pulcine 57
relationship between ECASS grade and symptomatic status: 1 symptomatic PH2, 1 symptomatic
PH1, 1 symptomatic HI2 and 2 symptomatic HI1. Due to the small sample size no significant
factors associated with symptomatic HT were found.
The single patient with PH2 on initial presentation had a diagnosis of hypoplastic left heart
syndrome (HLHS) status post pulmonary artery banding. He underwent cardiac catheterization to
implant a new stent and was put on prophylactic LMWH prior to discharge. He presented to the
ER 25 days later with decreased level of consciousness and focal seizure and urgent CT revealed
a CE-AIS and HT with ECASS grade PH2 for which he was taken urgently for a decompressive
craniectomy. He had no other identifiable risk factors for HT and his LMWH level was within
the therapeutic window at the time (Table 8). The single patient with PH2 on follow-up
neuroimaging, 6 days post CE-AIS, was a term newborn with pulmonary atresia with intact
ventricular septum (PA/IVS) whose clinical course was complicated by necrotizing enterocolitis
(NEC). He had a prior BTS which showed subsequent narrowing and required inotropic support
and vasopressors to achieve adequate oxygen saturation. He presented with a seizure and was
found to have a right parietal infarct. Six days later he developed decreased level of
consciousness and further seizures and a repeat CT showed bilateral subdural, subarachnoid and
intraventricular hemorrhage which lead to his subsequent death. Interestingly, he did not have
HT of his right parietal infarct, but was classified as PH2 given the ECASS classification system
also defines PH2 as hemorrhage remote from the stroke location (Fiorelli et al., 1999).
Analysis of factors associated with HT included greater stroke volume [modified ASPECTS 6.1
± 3.3 vs. 3.5 ± 2.3; p=0.006] (Table 7) and a trend for combination ATT [32% vs. 68%; p=0.06]
(Table 11), which is often administered in a step-wise fashion at our institution, with initial IV
heparin, when the risk of hemorrhage is deemed to be relatively high so that it can be quickly
reversed. Presence of univentricular physiology appeared to be protective from hemorrhagic
transformation although we did not control for volume of infarct [10% vs. 90%; p=0.03] (Table
3).
At the time of radiological CE-AIS diagnosis, 11 (13%) children had additional cortical laminar
necrosis on neuroimaging (Figure 9) while 14 (17%) had scattered foci of susceptibility on MRI
in keeping with cerebral microhemorrhages, as a result of prior cardiac surgery with
cardiopulmonary bypass (Table 7). There was no difference between the two groups. Two (2%)

Pulcine 58
children required decompressive craniectomy within 2 days [IQR 0 – 2] of stroke ictus.
Indications for decompression in both included large infarct size resulting in malignant MCA
syndrome (Table 8). Both had evidence of HT [HI1 and PH1] prior to decompression (Table 8).
Other types of intracranial hemorrhage seen are illustrated in Figure 10 and included: 20 (24%)
subdural, 2 (2%) subarachnoid and 3 (4%) intraventricular. There was a trend toward
subarachnoid and intraventricular hemorrhage in the HT group as the one patient with PH2,
described above, presented with all three on day six post CE-AIS (Table 6).
Figure 9. Representative CT scan showing cortical laminar necrosis.

Pulcine 59
Figure 10. Representative CT scans showing other types of intracranial hemorrhage.
Only 4 (5%) children had major systemic hemorrhage which included two with pulmonary
hemorrhage, one with hematochezia and one with a large 11 x 7 cm hematoma compressing the
right ventricle and displacing the heart to the left, felt most likely to be post-insertion of the
Berlin heart cannula (Table 7). There was no difference in the rate of systemic hemorrhage
between the two groups.

Pulcine 60
Case
Age
and
Sex
Cardiac
Diagnosis Procedural CE-AIS
Pre-
Existing
ICH
Total
Modified
Pediatric
ASPECTS
ECASS
Grade
Change
Over
Time
Clinical
Symptoms
Time
to HT
(days)
Treatment at
Time of HT (anti-
Xa level IU/mL)
Risk Factors for
HT
Clinical
Outcome
PSOM
Hemorrhagic Transformation on Follow-Up Neuroimaging Day > 0
1 14
M CoA
Yes – interventional
catheterization No MRI – 8 HI2 No Symptomatic
2
UFH bolus
481U/kg � UFH
20U/kg/hr (0.21)
Decompressive
craniectomy post
HT
1 – Mild
2 0.0
M
Primary
arrhythmia No No MRI – 13 HI2 No Asymptomatic 3
UFH 28U/kg/hr
(0.26) Infarct size
4 –
Severe
3 0.0
M TGA Yes – BAS
Yes -
SDH MRI – 6* HII HI2� Asymptomatic 2
UFH 28U/kg/hr
(0.48) None
0 –
Normal
4 0.2
M PA/IVS
Yes – interventional
catheterization No MRI – 4* HI2 No Asymptomatic 2
UFH 30U/kg/hr
(0.34) None
4.5 –
Moderate
5 0.0
M TGA No No MRI – 4* HI1 HI2� Asymptomatic 3
UFH 28U/kg/hr
(0.21)
AIS recurrence at
time HT
0 –
Normal
6 2.9
F
ccTGA /
acquired
arrhythmia
No No CT – 4 HI1 No Symptomatic 15
UFH 20U/kg/hr �
LMWH
1.5mg/kg/dose
(0.98) +
Warfarin
0.2mg/kg/day
INR 1.7
ACT transition
Received FFP due
to HT
Deceased
– long-
term F/U
7 15.6
M Cardiomyopathy No No MRI – 8 HI1 No Symptomatic 1
Warfarin
0.09mg/kg/day
INR 3.6 � UFH
20U/kg/hr
(0.22)
Infarct size
ACT transition
Deceased
– CE-AIS
8 0.4
F DORV
Yes – diagnostic
catheterization^ No MRI – 3 HI2 No Asymptomatic 3
UFH 28U/kg/hr
(0.1) � LMWH
1.1mg/kg/dose
(0.53)
ACT transition 1 – Mild
9 0.5
F DORV Yes – cardiac surgery^
Yes –
SDH CT – 7*† HI1 No Asymptomatic 11
UFH 28U/kg/hr �
LMWH
1mg/kg/dose
(0.75)
Infarct size
Thrombocytopenia
INR 2.2
0 –
Normal
10 0.0
M TGA Yes – BAS^
Yes –
SDH MRI – 4 HI2 No Asymptomatic 9
UFH 29U/kg/hr �
LMWH
1.8mg/kg/dose
(0.71)
None 1 – Mild
11 1.3
F Cardiomyopathy No No CT – 5 HI1 HI2� Asymptomatic 7
Warfarin
0.3mg/kg/day INR
2 �
UFH 39U/kg/hr
(0.67) + ASA
2.3mg/kg/day +
Clopidogrel
0.6mg/kg/day +
VAD
Combination
therapy
AIS recurrence at
time HT
3 –
Moderate

Pulcine 61
Dipyridamole
4mg/kg/day
12 13.8
F Cardiomyopathy No No CT – 10 PH1 No Unknown 5
UFH 18U/kg/hr
(0.29)
Infarct size
Decompressive
craniectomy
Takayasu arteritis
Systemic
hemorrhage
Thrombocytopenia
AIS recurrence at
time HT
Deceased
– other
causes
13 0.4
M DORV No No MRI – 8 HI1 No Asymptomatic 5
UFH 28U/kg/hr
(0.65) � LMWH
1mg/kg/dose
(0.45)
Infarct size
ACT transition
9 –
Severe
14 0.0
M TGA
Yes – BAS
complicated by
ECMO
Yes –
SAH /
IVH
MRI – 5 PH1 No Asymptomatic 3
UFH 20U/kg/hr
stopped 3 days
prior to HT
ECMO 2 – Mild
15 4.4
F
IE / mechanical
valve No No MRI – 8 PH1 No Asymptomatic 12
UFH 33U/kg/hr
(0.70) + Warfarin
0.2mg/kg/day �
LMWH
1.4mg/kg/dose
(0.84)
Infarct size
Septic emboli
ACT transition
3 –
Moderate
16 0.0
M
Primary
arrhythmia No No MRI – 6 HI2 No Asymptomatic 3
UFH 37U/kg/hr
(0.38) ECMO 1 – Mild
17 0.2
M Complex SV No No CT – 2 HI1 No Asymptomatic 3
UFH 37U/kg/hr
(0.42) None
Deceased
– cardiac
causes
18 5.6
F
Myocarditis /
acquired
arrhythmia
Yes – BAS^ No CT – 2 HI1 No Unknown 6 UFH 20U/kg/hr
(0.5)
Thrombocytopenia
INR 1.5
Systemic
Hemorrhage
ECMO
VAD
AIS recurrence at
time HT
2.5 –
Mild
19 1 M DORV Yes – cardiac surgery^ Yes –
SDH MRI – 10 PH1 No Symptomatic 11
UFH 28U/kg/hr �
LMWH
1mg/kg/dose
Infarct size 2.5 –
Moderate
20 0.1
M PA/IVS Yes – cardiac surgery^ No CT – 2 PH2 No Symptomatic 6
LMWH
1.5mg/kg/dose
NEC/sepsis
BTS failure
Deceased
– ICH
Hemorrhagic Transformation on Initial Neuroimaging Day = 0
1 10.9
F IE No No MRI – 4* HI2 No Unknown 0 None
Septic emboli
Thrombocytopenia
4 –
Moderate

Pulcine 62
ACT=antithrombotic therapy; AVSD=atrioventricular septal defect; BAS=balloon atrial septostomy; BTS=Blalock-Taussig shunt; ccTGA=congenitally corrected transposition of
the great arteries; CE-AIS=cardioembolic arterial ischemic stroke; CoA=coarctation of the aorta; DORV=double outlet right ventricle; ECMO=extracorporeal membrane
oxygenation; ICH=intracranial hemorrhage; IE=infective endocarditis; IVH=intraventricular hemorrhage; LPA=left pulmonary artery; LMWH=low molecular weight heparin;
NEC=necrotizing enterocolitis; PSOM=Pediatric Stroke Outcome Measure; SAH= subarachnoid hemorrhage; SDH=subdural hemorrhage; SV=single ventricle; TA=tricuspid
atresia; TGA=transposition of the great arteries; ToF=tetralogy of Fallot; UFH=unfractionated heparin; VAD=ventricular assist device;
*Multifocal ASPECTS
†Infratentorial ASPECTS
^Periprocedural > 72 hours
Table 8. Salient demographic, clinical, neuroimaging and follow-up details of cardioembolic stroke patients with hemorrhagic transformation
divided by the presence of hemorrhage on initial or follow-up neuroimaging.
2 1.7
M
Ebstein’s
anomaly
Yes – cardiac surgery
complicated by
infection/dysthymia^
No CT – 1† HI2 No Asymptomatic 0 UFH 22U/kg/hr
(0.19) None
0 –
Normal
3 0.1
M ToF No No MRI – 4* PH1 No Unknown 0 None
Premature 33 6/7
Thrombocytopenia
Deceased
– other
causes
4 0.2
M HLHS
Yes – interventional
catheterization^ No CT – 7 PH2 PH1� Symptomatic 0
LMWH
1.5mg/kg/dose
(0.16)
Decompressive
craniectomy due to
HT
1 –
Normal
5 0.2
F
DORV /
congenital heart
block
Yes – diagnostic
catheterization No CT – 1 HI1 No Asymptomatic 0 None None
1.5 –
Mild
6 0.4
M DORV Yes – cardiac surgery^ No CT – 1 HI2 No Asymptomatic 0
UFH 28U/kg/hr �
LMWH
1.6mg/kg/dose
(0.51)
None 3 –
Moderate
7 2.6
M TA No No MRI – 0† HI2 No Asymptomatic 0 None None
0 –
Normal
8 4.3
M ToF
Yes – interventional
catheterization
complicated by LPA
dissection and
aneurysm
No CT – 12 PH1 No Unknown 0 UFH 20U/kg/hr
(0.58)
Infarct size
Decompressive
craniectomy post
HT
8 –
Severe
9 6.1
M IE No No MRI – 2 HI1 HI2� Unknown 0 None
Septic emboli
Loeys-Dietz
syndrome
1 – Mild
10 2.4
F AVSD Yes – cardiac surgery No CT – 4 HI2 No Symptomatic 0 None
ECMO
Systemic
hemorrhage
Noonan syndrome
0 –
Normal
11 0.5
M
DORV /
acquired
arrhythmia
Yes – cardiac surgery No CT – 2 HI2 No Unknown 0 UFH 28U/kg/hr
(0.67) None
1.5 –
Normal

Pulcine 63
4.5 Antithrombotic Therapy
The details of antithrombotic therapy, timing and type of therapy are outlined in Figure 11. Of
the 93 children who met the initial inclusion criteria, 11 (12%) had HT on their initial
neuroimaging and were defined as having early HT (Figure 11). Of these, six (7%) were not
receiving any prior antithrombotic therapy and therefore were defined as having early
spontaneous HT. The other five were receiving antithrombotic therapy at the time of CE-AIS
diagnosis. We could not ascertain the exact timing of HT in relation to ATT due to the
observational nature of this study. As a result, these 11 cases were excluded from the final
analysis. The remaining eighty-two patients were left with a treatment decision whether or not to
initiate or further optimize ATT for secondary stroke prevention. Nearly all 78 (95%) were
treated with ATT as shown in Figure 11. Out of the 4 patients that did not receive ATT, none
had late spontaneous HT. These 4 patients were treated conservatively because of concerns about
malignant transformation of their infarct in 2 and infective endocarditis in 2. No HT occurred
while on antiplatelet therapy alone or after IV tPA administration.
Figure 11. Details of the treatment decision for secondary stroke prevention and rates of
antithrombotic therapy-associated hemorrhage.
93 CE-AIS Patients
56% Male
26% Neonates
Median Age 0.44 years
EARLY HT
11/93 (12%) HT on Initial CT/MRI
82 CE-AIS Patients
54% Male
28% Neonates
Median Age 0.43 years
78/82 (95%)
Treated with ATT
Within First 30 days CE-AIS
4/82 (5%)
Not Treated with ATT
Within First 30 days CE-AIS
LATE SPONTANEOUS HT
0% had bleed on no ATT
0/5 (0%)
Bleed while on APT
Rx APT 5/78 (6%)
19/64 (30%)
Bleed while on ACT
Rx ACT 64/78 (82%)
1/9 (11%)
Bleed while on APT + ACT
Rx APT + ACT 9/78 (12%)
0/2 (0%)
Bleed after IV tPA
Rx IV tPA 2/82 (2%)
5/11 (46%)
ATT Pre CE-AIS → 5/5 ACT
EARLY SPONTANEOUS HT
6/93 (7%)
No ATT Pre CE-AIS
HT POST ATT INITIATION
20/82 (24%)
TREATMENT DECISION

Pulcine 64
Seventy-eight (95%) patients received antithrombotic therapy within 30 days of CE-AIS, which
was initiated at a mean of 1.5 ± 5.7 days [0 – 4]. Of these, 63 (77%) commenced treatment or
their antithrombotic regimen was escalated, while 15 (18%) had no change in antithrombotic
treatment as illustrated in Table 9. Indications for antithrombotic treatment at the time of
radiological CE-AIS diagnosis are outlined in Figure 12. These are not mutually exclusive, and
the number of patients indicate all the possible consideration for ATT at the time of stroke
diagnosis, including secondary stroke prevention. Out of the 20 patients with HT 6 (30%) were
subtherapeutic on ATT at the time of HT, 13 (65%) were therapeutic and 1 (5%) was
supratherapeutic.
Total (n=82) HT (n=20) No HT (n=62) P-value†
Remained on No Treatment
Following Stroke Ictus 4 (5%) 0 4 (100%) 0.57
No Change in
Antithrombotic Treatment 15 (18%) 3 (20%) 12 (80%) 0.75
Commenced Treatment or
Antithrombotic Regimen
Was Escalated
63 (77%) 17 (27%) 46 (73%) 0.54
Table 9. Categories of antithrombotic treatment including commencement, escalation or no
change to ongoing therapy for secondary stroke prevention.
†Chi-square or Fisher’s exact test for categorical variables

Pulcine 65
Figure 12. Indications for antithrombotic treatment at the time of cardioembolic arterial
ischemic stroke.
Among children receiving antithrombotic therapy following CE-AIS diagnosis, 12 (15%) were
on monotherapy, 50 (64%) were on sequential therapy (one ATT after another as is often
encountered in standard practice) and 16 (21%) were on concurrent combination therapy. There
was no difference in the use of concurrent combination therapy between those with and without
HT [4 (25%) vs. 12 (75%); p=1.00]. Amongst children receiving antithrombotic therapy, the
majority were treated with anticoagulant therapy (ACT) 64 (82%) and only 5 (6%) were
receiving antiplatelet therapy (APT) alone. Nine (12%) were on combination therapy with ACT
and APT. Despite this, HT was not associated with monotherapy vs. combination therapy nor
antiplatelet vs. anticoagulant therapy. There was a trend for sequential combination ATT [16
(32%) vs. 34 (68%); p=0.06]; sequential combination ATT is often administered in a step-wise
fashion at our institution, with initial IV heparin, when the risk of hemorrhage is deemed to be
relatively high so that it can be quickly reversed.
Two children received thrombolysis with IA or IV tPA and did not have any subsequent
intracerebral hemorrhage: one child presented with a hyperacute stroke with proximal artery
occlusion and received intra-arterial tPA 9 mg in total before diagnosis of endocarditis was

Pulcine 66
made; the other child received IV tPA for left aortic thrombus occluding the left main coronary
artery, discovered shortly after birth, resulting in left ventricular infarction and subsequent CE-
AIS due to thromboembolism. No child received endovascular mechanical clot retrieval during
the study interval.
Total (n=82) HT (n=20)
No HT
(n=62)
P-
value†
Type of ATT Pre CE-AIS
ATT Pre CE-AIS 39 (48%) 7 (18%) 32 (82%) 0.20
APT 7 (18%) 0 7 (100%) 0.45
ACT 26 (67%) 6 (23%) 20 (77%)
ACT + APT 5 (13%) 1 (20%) 4 (80%)
Fibrinolytic IV tPA 1 (3%) 0 1 (100%)
Monotherapy 33 (85%) 6 (18%) 27 (82%) 1.00
Combination Therapy –
Concurrent 6 (15%) 1 (17%) 5 (83%) 1.00
Type of ATT Post CE-AIS
ATT Post CE-AIS 78 (95%) 20 (26%) 58 (74%) 1.00
APT 5 (6%) 0 5 (100%) 1.00
ACT 64 (82%) 19 (30%) 45 (70%) 0.10
ACT + APT 9 (12%) 1 (11%) 8 (89%) 0.44
Fibrinolytic IV tPA 1 (1%) 0 1 (100%) 1.00
Monotherapy 12 (15%) 2 (17%) 10 (83%) 0.13
Combination Therapy –
Sequential 50 (64%) 16 (32%) 34 (68%) 0.06
Combination Therapy –
Concurrent 16 (21%) 4 (25%) 12 (75%) 1.00
Mean Time from CE-AIS to
Initiation of ATT (mean ±±±± SD
days [range])
1.5 ± 5.7 [0 – 41] 0.5 ± 0.9 [0 –
3]
1.9 ± 6.5 [0 –
41] 0.76
Median Time from CE-AIS
to Initiation of ATT (days
[IQR])
0 [0 – 1] 0 [0 – 0.5] 0 [0 – 1] 0.76
Table 10. Additional details of the type of antithrombotic treatment pre- and post-radiological
diagnosis of cardioembolic arterial ischemic stroke.
APT=antiplatelet; ATT=antithrombotic therapy; ACT=anticoagulant; CE-AIS=cardioembolic arterial ischemic
stroke; tPA=tissue plasminogen activator;
†Chi-square or Fisher’s exact test for categorical variables and Wilcoxon Mann-Whitney test for nonparametric
continuous variables

Pulcine 67
4.6 Arterial Ischemic Stroke Recurrence
Stroke recurrence occurred in 11 (13%) children including 6 (55%) with silent infarcts
discovered on follow-up neuroimaging, 4 (36%) with symptomatic stroke and 1 (9%) with a
transient ischemic attack. Median time to recurrence was 32 days [IQR 5.5 – 93]. There was no
difference in the frequency of stroke recurrence between the two groups [3 (15%) HT vs. 8
(13%) no HT; p=1.00]. One child had a procedure-related recurrence (9%). Ten (91%) children
were receiving some type of antithrombotic therapy at the time of recurrence, as illustrated in
Table 11, but therapeutic drug monitoring was not available to indicate if there was adequate
compliance or if the antithrombotic therapy was within therapeutic range.
Recurred No ATT 1 (9%)
Recurred on APT 0
Recurred on ACT 8 (73%)
Recurred on ACT + APT 2 (18%)
Table 11. Type of antithrombotic therapy at the time of stroke recurrence.
Recurrence by cardiac physiology is illustrated in Table 12. Stroke recurrence was highest in
those with cyanotic CHD pre-surgery, cyanotic CHD post-palliative surgery with residual right-
to-left-shunt and in those with cardiomyopathy.
Recurrence Cyanotic CHD Pre-Surgery 3 (27%)
Recurrence Cyanotic CHD Post-Palliative 3 (27%)
Recurrence Cyanotic CHD Post-Definitive 0
Recurrence Acyanotic CHD Post-Surgery 1 (9%)
Cardiomyopathy 4 (36%)
Table 12. Type of cardiac physiology at the time of stroke recurrence.
4.7 Outcome
As illustrated in Figure 13, neurological status at discharge included 41 (50%) children with a
neurological deficit, 22 (27%) with normal neurological exam, 12 (15%) with unknown clinical
status due to missing documentation, 4 (5%) deceased due to cardiac causes, 2 (2%) deceased
due to cardioembolic arterial ischemic stroke, and 1 (1%) deceased due to intracranial
hemorrhage.

Pulcine 68
Figure 13. Neurological status at discharge.
Follow-up information was available in 98% children and was missing in 2 (2%) without HT.
Mean time to follow-up was 4.1 ± 3.5 years [0.0 – 12.9]. PSOM scores were dichotomized into
good and poor outcome as previously described. Good outcome, which was defined as a normal
to mild PSOM using the new classification system (Slim M, 2018), occurred in 53 (66%) and
poor outcome occurred in 27 (34%). Mean time to PSOM with and without HT was not
significantly different [3.3 ± 2.9 vs. 4.3 ± 3.6 years; p=0.35]. In univariate analysis
HT was significantly associated with a poor outcome [OR 3.36; 95% CI 1.18 – 9.61; p=0.02]. In
multivariate logistic regression analysis, HT showed a trend towards poor outcome regardless of
infarct volume [adjusted OR 3.63; 95% CI 0.96 – 13.81; p=0.06].
PSOM scores did not correlate with increasing ECASS grades of HT (Spearman correlation
coefficient 0.66). However, when ECASS severity was categorized into normal (no HT), mild
(HI1 and HI2) and severe (PH1 and PH2) and compared to the dichotomized PSOM scores, the
proportion of patients with a favorable outcome decreased as the ECASS severity increased
(Figure 14).

Pulcine 69
Figure 14. Frequency distribution of neurological outcome compared to normal, mild and severe
ECASS grade.
Death occurred in 12 (15%) of the cohort. Seven (58%) died in the same hospital admission
during which CE-AIS occurred (defined as at discharge) with causality and HT distribution
illustrated in Figure 15. Of the seven that died with HT, two had HI1, 1 had PH1 and 1 had PH2
(Figure 15). Death during long-term follow-up occurred in a further 5 (42%) patients: 4 due to
cardiac causes and 1 due to cerebral edema and subsequent herniation (Figure 15). One of the
patients with PH2 died secondary to their intracranial hemorrhage. None of the other children
died as a result of HT.

Pulcine 70
Figure 15. Timing, cause of death and distribution of hemorrhagic transformation in deceased
patients.
Deceased
15% (12/80)
Discharge
58% (7/12)
Due to CE-AIS
29% (2/7)
HI1
Due to Cardiac Causes
57% (4/7)
HI1 / PH1
Due to ICH
14% (1/7)
PH2
Long-Term Follow-Up
42% (5/12)
Due to Cardiac Causes
80% (4/5)
HI1
Due to Cerebral Edema/ Herniation
20% (1/5)

Pulcine 71
Chapter 5
Discussion
5.1 General Discussion
The aim of this study was to determine the rate and factors associated with HT in children with
CE-AIS and perform an exploratory analysis of the relationship between antithrombotic therapy,
hemorrhagic transformation and clinical outcome. HT is used as a safety end point for most
arterial ischemic stroke treatment and secondary prevention trials in adults. In this study harm
due to HT was defined as death or increasing severity of PSOM. The main findings of our single-
center study of consecutive pediatric CE-AIS patients treated with antithrombotic therapy were:
(1) HT occurs at a rate of 24% in neonates and children with CE-AIS treated with ATT; 6% of
whom are symptomatic; (2) HT rate in ATT-treated patients is higher than the early spontaneous
HT rate [24% vs. 7%]; (3) HT did not occur more frequently in patient who received APT vs.
ACT vs. combination therapy with APT and ACT, although none of the patients on APT therapy
alone had HT; (4) HT was usually petechial, within the infarct, and consistent with a mild
ECASS grade of HI1 or HI2 in 75% of the cohort; (5) malignant HT was rare and usually
associated with additional risk factors for hemorrhage (e.g. infarct size, sepsis, shunt failure,
ECMO); (6) factors associated with HT included larger stroke volume [modified ASPECTS 6.1
± 3.3 vs. 3.5 ± 2.3; p=0.006] while univentricular physiology appeared to be protective [10% vs.
90%; p=0.03]; (7) rates of systemic hemorrhage were low 5% despite a large proportion of
children being critically ill and receiving ACT 9% for secondary stroke prevention (8) stroke
recurrence was lower, 13% at an average of 4 years, than the previously reported rate of 27% at
10 years (Rodan et al., 2012) possibly indicating the effectiveness of ATT in secondary stroke
prevention; (9) mortality did not differ between the two groups with and without HT; (10) long-
term follow-up demonstrated a trend towards worse neurological outcome in those with both
asymptomatic and symptomatic HT even when we controlled for infarct volume [adjusted OR
3.63; 95% CI 0.96 – 13.81; p=0.06]. In interpreting our findings, it is important to keep in mind
that ATT was not administered in a randomized fashion thereby leading to selection bias. Overall
our results are on the lower range of the reported rate of clinically significant major bleeding
(including intra and extracranial) in critically ill children receiving therapeutic unfractionated
heparin, which is estimated to be 24% (Kuhle et al., 2007), with a lower rate of stroke recurrence

Pulcine 72
than previously reported at our center (Rodan et al., 2012). However, the risk-benefit ratio
remains unknown in the context of the subgroup of each primary cardiac diagnosis.
5.1.1 Patient Characteristics
Previous studies have found that childhood CE-AIS involves younger children, when compared
to other stroke etiologies, with a median age of 6 months to 3 years (Asakai et al., 2015; Dowling
et al., 2013). Similarly, our cohort had a median age at stroke ictus of 0.43 years (IQR 0.08 –
4.23). The relationship with age in our study and in others (Asakai et al., 2015; Dowling et al.,
2013) is likely dependent on the timing of surgical intervention. It is estimated that by the age of
5 years approximately 80% of patients will require at least one surgical intervention to achieve
either complete or palliative cardiac repair (Silvey & Brandao, 2017). Therefore, children with
cardioembolic stroke tend to be younger compared to children with other stroke etiologies. When
looking at clinical factors associated with HT there was no difference in sex, age, weight or the
number of neonates between those with and without HT. Despite our hypothesis that neonates
maybe more at risk of major systemic and intracranial hemorrhage due to developmental
hemostasis we did not observe this in our cohort. In other words, our results show that neonates
are not at higher risk of hemorrhagic transformation compared to children with cardiac disease.
Blood pressure measurements were available in 35% of children at the time of stroke
presentation with a large proportion 65% of missing values. Given that approximately two-thirds
of CE-AIS were procedure-related, the exact time of onset was not always clear due to prolonged
postsurgical sedation and pharmacological paralysis in our cohort of critically ill children. For
this reason, blood pressure analysis could not be performed accurately. Factors that are
associated with increased risk of symptomatic hemorrhage in adults following IV thrombolysis
include hypertension in the first 24 hours (Khatri, Wechsler, & Broderick, 2007). However,
Beslow et al showed that in children blood pressure on admission was not associated with risk of
hemorrhagic transformation (Beslow et al., 2011). This can be explained by the fact that the
majority of children with AIS do not receive thrombolytic therapy and are more likely to receive
antithrombotic therapy instead. As a result, acute hypertension, which is needed to maintain
cerebral perfusion pressure, may not be as detrimental because of the different mechanism of
action of thrombolytic versus antiplatelet and anticoagulant therapies.

Pulcine 73
5.1.2 Cardiac Diagnosis and Interventional Procedures
Primary cardiac diagnosis included 60% children with cyanotic heart disease, 16% with
acyanotic heart disease, 17% with cardiomyopathy/myocarditis, 4% with infective endocarditis,
2% with primary arrhythmia and 1% with rheumatic heart disease. This distribution of cardiac
lesions is similar to that described by Asakai et al from a single tertiary-care center at the Royal
Children’s Hospital Melbourne: 55% cyanotic congenital heart disease, 29% acyanotic
congenital heart disease, 8% cardiomyopathy/myocarditis, 4% infective endocarditis and 4%
primary arrhythmia (Asakai et al., 2015; Dowling et al., 2013). A challenge when studying
congenital and acquired heart disease is the variability and complexity of the anatomy and
physiology as illustrated in the details of cardiac lesions in Table 4. Intuitively, those with more
complex cardiac lesions, especially univentricular physiology, or severe heart failure, who
undergo multiple surgical procedures were hypothesized to be at highest risk due to repeated
exposure to intensive anticoagulation as a result of cardiopulmonary bypass or the presence of
ventricular assistive devices. Due to our relatively small sample size we stratified the different
primary cardiac lesions further into univentricular or biventricular in order to investigate the risk
of hemorrhagic stroke by different lesion group. Not surprisingly, children with cyanotic
congenital heart disease accounted for more than half of all the cases of radiologically confirmed
CE-AIS with 23% having biventricular physiology and 61% having univentricular physiology.
The most interesting findings was that across all types of primary cardiac diagnosis, those
children with biventricular physiology were significantly more likely to present with
hemorrhagic transformation [OR 3.27 95% CI: 1.04 – 10.24; p=0.03] (Giang et al., 2018). This
can be explained by the fact that in our cohort there was a significant difference in the type of
cyanotic heart disease between those with and without HT. Hypoplastic left heart syndrome and
tricuspid atresia, both of which comprise single-ventricle physiology, were more commonly
represented in the group without hemorrhagic transformation as illustrated in Table 4. This is in
contrast to our initial hypothesis and a long-term study of hemorrhagic stroke in young patients
with congenital heart disease from Sweden where the highest relative risk of intracranial
hemorrhage among CHD patients when compared to controls were amongst those with severe
non-conotruncal defects, which included single ventricle defects, hypoplastic left heart syndrome
and endocardial cushion defects [IRR 16.5 95% CI 5.63 – 51.2] (Giang et al., 2018). In addition,
patients with coarctation of the aorta had the highest relative risk of subarachnoid hemorrhage,

Pulcine 74
perhaps related to systemic hypertension (Giang et al., 2018). The reason for this is not entirely
clear and is difficult to deduce from the present data. Perhaps, this may be attributed to both the
differences in grouping various complex cardiac lesions, exclusion of children with known
intracranial vascular pathology from our cohort and the varying definitions of intracranial
hemorrhage that were used in our study. Our study looked specifically at rates of hemorrhagic
transformation (HT), compared to the study from Giang et al, which looked at rates of
intracranial hemorrhage (ICH). In our study, hemorrhagic transformation was defined as any
evidence of intracerebral hemorrhage in the area of ischemic infarction within the first 30 days
from radiologic CE-AIS diagnosis. Other types of intracranial hemorrhage including subdural,
subarachnoid, and intraventricular were excluded from this definition and were captured
separately. On the other hand, Giang et al defined ICH using international classification of
disease (ICD) -8, -9 and -10 codes for intracranial hemorrhage. In our cohort, 24% had subdural,
2% had subarachnoid and 4% had intraventricular hemorrhage, which did not differ in frequency
between those with and without HT. Those with pre-existing subdural hemorrhage at the time of
CE-AIS diagnosis were all either neonates or younger than 1 year of age which may represent
subdural hemorrhage related to the birth process, reported in 26% of births. Intracranial
hemorrhage is encountered more frequently in newborns due to skull bone molding and normal
developmental differences in hemostasis as well as in those with CHD due to pre-existing
deficits in cerebral development resulting immature brain structure (Limperopoulos et al., 2001;
Miller et al., 2007). There was an uneven distribution of subarachnoid and intraventricular
hemorrhage in the HT group as the one patient with parenchymal hematoma type 2, presented
with all three on day six post CE-AIS. We did not find a trend between CoA and subarachnoid
hemorrhage in our cohort; but there were only two patients with subarachnoid hemorrhage, and
we excluded those with intracranial vascular malformations from our study.
Primary arrhythmia in those with HT appeared more frequently although not significantly as
illustrated in Table 4. This is not surprising as atrial fibrillation in adults carries a high risk of
thromboembolism requiring anticoagulation for stroke prevention. Various types of arrhythmias
have been described in children with stroke although arrhythmia is not as prevalent in neonates
and children compared to the general adult population. Atrial fibrillation has been reported to
occur more frequently in children with hyperthyroidism, rheumatic heart disease and post-
palliative repair of univentricular congenital heart disease (Giglia et al., 2013; Roach et al.,

Pulcine 75
2008). Pediatric and adult CHD patients who have surgery involving their atria are particularly at
increased risk for intra-atrial reentrant tachycardia (Giglia et al., 2013). Kirsh et al demonstrated
that 20% of children with CHD that required cardioversion had atrial fibrillation (Kirsh et al.,
2002). Atrial arrhythmias in all age groups are more frequently treated with anticoagulation,
although our numbers are too small to show this. When thrombi embolize into the
cerebrovascular circulation, spontaneous recanalization occurs, as they break off and travel more
distally in the arterial tree. This in turn can lead to reperfusion-hemorrhage because blood vessels
and brain tissue may be damaged when there is acute cerebral ischemia and is further exacerbate
by the presence of anticoagulation.
Additional cardiac risk factors, including previous ECMO, CBP, mechanical valve, secondary
arrthymias requiring medication or pacemaker and infective endocarditis, occurred in 46%
children and did not differ between those with and without hemorrhagic transformation [21% vs.
79%; p=0.51]. This may be explained by the heterogeneity of risk factors and complexity of the
interactions in a relatively small sample size. Nevertheless, it was important to consider these
factors. Post-cardiotomy ECMO which has been reported at a rate of 2 – 5% of all postoperative
patients in large tertiary care centers (Giglia et al., 2013) and is known to increase the risk of
bleeding as it is initiated often when a patient cannot be weaned off CPB and their heparin
cannot be reversed (Giglia et al., 2013). We did not find a difference between the rate of post-
cardiotomy ECMO in those with and without HT [0% vs. 100%; p=0.57] as illustrated in Table
5. Similarly, previous history of ECMO, CPB, secondary arrhythmias requiring the use of
medication or a pacemaker and mechanical valve, which are all surrogate markers of previous
intensive anticoagulation, were not different amongst the two groups.
Additional non-cardiac stroke risk factors, including systemic infection,
cardiogenic/hypovolemic shock, prothrombotic abnormalities, HIE and systemic vasculopathy,
occurred in 37% children and did not differ between those with and without hemorrhagic
transformation [33% vs. 67%; p=0.15]. We excluded those with intracranial vascular
malformations from our study. This sole patient with systemic vasculopathy did not have any
intracranial vasculopathy and presented with an intracardiac thrombus which embolized to the
brain. Unlike the findings of Rodan et al (Rodan et al., 2012) who looked specifically at risk
factors for stroke recurrence, the presence of a mechanical valve and prothrombotic
abnormalities were infrequent in our cohort and included two patients with significantly elevated

Pulcine 76
lipoprotein (a), one patient with heterozygous factor V Leiden (FVL) and
methylenetetrahydrofolate reductase (MTHFR) polymorphism (677 C�T variant in one allele)
and one patient with a homozygous MTHFR polymorphism (677 C�T variant in both alleles)
but normal homocysteine. This may be due to the fact that we only looked at persistent
thrombophilia abnormalities in this cohort of children as opposed to acute abnormalities at the
time of CE-AIS which normalized on follow-up testing.
Almost two-thirds, 61%, of AIS occurred in association with surgical procedures or
catheterization. Children who require multiple operations likely have more severe underlying
cardiac disease and undergo repeated exposure to procedure-related complications. Therefore,
reoperation is a surrogate marker for the severity of the underlying CHD. The period in and
around the time of stage I palliation, also known as the Norwood procedure is generally
considered to be the highest risk for thromboembolic complications (Giglia et al., 2013;
Manlhiot et al., 2012; Silvey & Brandao, 2017). Although there is limited data, current
experience suggest that the risk of thrombosis after bidirectional cavopulmonary anastomosis is
low (Giglia et al., 2013; Manlhiot et al., 2012). The risk following a Fontan, the final staged
palliative procedure, is reported to vary from 17 – 33% in cross-sectional studies (Giglia et al.,
2013) but is not uniform and appears to occur in the perioperative period and peak again 5- 10
years later (Giglia et al., 2013). This is reflected in our study as illustrated in Figure 3, post-
Norwood CE-AIS occurred in 31%, who underwent palliative cardiac surgery, with systemic-to-
pulmonary shunts in 25%, commonly constructed during a Norwood procedure, followed by
19% in Glenn and another 19% in Fontan shortly after surgery. In contrast, there was no pattern
detected in those who underwent complete cardiac repair as illustrated in Figure 4.
Cardiac catheterization alone was associated with HT. Cardiac catheterization occurred more
frequently in those with HT [33% vs. 67%; p=0.07] but did not reach statistical significance as
illustrated in Table 5. When the type of cardiac catheterization was further broken down into
diagnostic, interventional or more specifically balloon atrial septostomy, there was a trend
towards undergoing BAS in those with HT [44% vs. 56%; p=0.07] (Table 6). Children post-CPB
were not an increased risk of HT. One possible explanation for this maybe that children on CPB
have careful reversal of their anticoagulation versus those after cardiac catherization may not.
Known complications of cardiac catheterization procedures include in situ thrombosis and distal
embolus (Giglia et al., 2013; Silvey & Brandao, 2017). The prevalence of AIS in children due to

Pulcine 77
cardiac catheterization is infrequent and estimated to be 0.28 – 1.3% (Liu et al., 2001; Weissman
et al., 1985). When undergoing cardiac catheterization, the femoral artery or vein is accessed for
catheter insertion immediately prior to a bolus of unfractionated heparin (UFH) for prophylaxis
(Allen D. Everett, 2011; Giglia et al., 2013). The typical anticoagulation protocol for diagnostic
or interventional cardiac catheterization includes a loading dose of 100 U/kg (up to 5000 U
maximum) and an additional 50 to 100 U/kg of heparin bolus to keep the activated clotting time
(ACT) > 200 seconds (Giglia et al., 2013). One common interventional catheterization procedure
is called a balloon atrial septostomy (BAS), where a balloon catheter is used to create or enlarge
a patent foramen ovale or atrial septal defect between the two upper chambers of the heart in
order to increase oxygen saturation (Allen D. Everett, 2011). In essence, this procedure is used to
temporarily rescue the physiology of transposition of the great arteries (TGA), a life-threatening
cyanotic CHD seen in infants, while awaiting a definitive corrective surgery: the arterial switch
operation (ASO). In practice the use of prophylactic anticoagulation during BAS, including our
own, varies both within and among centers and is not evidence-based. The reason for our
findings is not entirely clear and is difficult to deduce from the present data given that we do not
routine give prophylactic ACT for BAS procedure at our center. Catheter-related strokes tend to
be embolic and could have several postulated origins. These include dislodging small thrombi
into the cerebral circulation or the formation of a thrombus in situ on the catheter tip during the
procedure, disrupting the endothelium and release a cascade of coagulation factors. In our cohort,
post-procedural complications which could further contribute to peri-procedure iatrogenic stoke
did not differ between those with and without HT [11% vs. 89%; p=0.25].
In order to account for possible changes in surgical practice over a 14-year period (2003 – 2017)
a histogram was constructed to look at the frequency of procedure-related stroke by year as
illustrated in Figure 5. While the average number of procedure-related CE-AIS per year was 3.3
± 1.7 [1 – 7] there appeared to be a higher rate in 2004 [6] and 2016 [7] with no specific trend
observed over the course of the 14-year period. We hypothesized that with advances in surgical
and cardiac catheter procedures there would be less instances of CE-AIS over the 14-year time
frame. We used the 30-day definition of procedure-related cardioembolic arterial ischemic stroke
due to difficulty in making the diagnosis in a post-operative medically fragile patient who may
not have the same focal findings as an older child or adult. In addition, there is difficulty in
obtaining definitive neuroimaging with MRI in order to make the diagnosis. When the

Pulcine 78
procedure-related stroke definition was changed to CE-AIS within 72 hours of cardiac surgery or
catheterization, postprocedural CE-AIS occurred in 17 (21%) and did not differ between the two
groups [4 (24%) HT vs. 13 (76%) no HT; p=0.72].
5.1.3 Radiological Features
Timing and modality of imaging varied widely in this cohort due to variations in patient
presentation, clinical severity and availability of imaging. The median number of follow-up
images within 30 days of stroke was 2 [IQR 1 – 2]. Eight patients did not have follow-up
imaging within 30 days of CE-AIS but went on to have subsequent neuroimaging outside of this
time window. They were still included in our analysis to ensure an adequate sample size and
because the timing of repeat neuroimaging in the CE-AIS population is challenging given
requirements for cardiac anesthesia, temporary pacing wires and mechanical support devices and
overall medical fragility.
The most frequent location of AIS was the anterior circulation 70% with both anterior and
posterior circulation 24% also commonly seen. Fifty percent had AIS in multiple territories
which supports the notion that there may be an underlying cardioembolic mechanism. The
International Pediatric Stroke Registry has also shown that infarcts in children with cardiac
disease are frequently bilateral and involving both the anterior and posterior circulation, when
compared to children with other stroke etiologies (Dowling et al., 2013). Similarly, Asakai et al
reported that more than 30% of CE-AIS in their cohort occurred in multiple territories and
predominantly in the anterior circulation (Asakai et al., 2015; Schechter et al., 2012).
The majority of AIS involved both cortical and subcortical regions 83%. Cortical and subcortical
involvement was more commonly seen in those with HT [28% vs. 72%; p=0.17] while
subcortical involvement only was more commonly seen in those without HT [7% vs. 93%;
p=0.17]. This can be explained by the fact that purely subcortical lesions are smaller in volume
and thus tend to have less risk of hemorrhagic conversion. Not surprisingly, greater stroke
volume was a significant predictor of HT [modified ASPECTS 6.1 ± 3.3 vs. 3.5 ± 2.3; p=0.006]
which has also been reported in other pediatric HT series (Beslow et al., 2011). A modified
pediatric ASPECTS of 5 maximized the sensitivity for differentiating large from small infarcts
(Beslow et al., 2012). A modified pediatric ASPECTS of >5 predicts a large infarct with
sensitivity of 80% and specificity of 87% (Beslow et al., 2012). In our cohort, mean ASPECTS

Pulcine 79
of 6.1 correlates with HT and indirectly with a larger infarct volume as was previously validated
by Beslow et al. In a subsequent study, Beslow et al showed that the development of HT was
significantly associated with an infarct volume greater than 5% of the supratentorial brain
volume [RR 4.81; 95% CI: 1.54 – 15.08; p=0.0026] with a trend toward increased risk of HT in
children with cardiac disease [RR 1.97; 95% CI: 0.96 – 0.45; p=0.12] (Beslow et al., 2011). This
is in agreement with our findings.
5.1.4 Hemorrhagic Transformation
Our study shows that the overall HT risk within 30 days of CE-AIS in neonates and children is
24%, and of symptomatic HT is 6%. ECASS hemorrhagic classification was as follows: HI1 in 9
(45%), HI2 in 6 (30%), PH1 in 4 (20%) and PH2 in 1 (5%). The single patient with PH2 on
follow-up neuroimaging, 6 days post CE-AIS, was a term newborn with pulmonary atresia with
intact ventricular septum (PA/IVS) whose clinical course was complicated by necrotizing
enterocolitis (NEC). He had a prior BTS which showed subsequent narrowing and required
inotropic support and vasopressors to achieve adequate oxygen saturation. He presented with a
seizure and was found to have a right parietal infarct. Six days later he developed decreased level
of consciousness and further seizures and a repeat CT showed bilateral subdural, subarachnoid
and intraventricular hemorrhage which lead to his subsequent death. Interestingly, he did not
have HT of his right parietal infarct but was classified as PH2 given the ECASS classification
system also defines PH2 as significant hemorrhage remote from the stroke location.
The mean number of follow-up images within 30 days of CE-AIS was 1.9 ± 1.5 [0 – 8]. The
mean number of follow-up images in children with HT compared to without HT was
significantly different [3.3 ± 1.7 vs. 1.5 ± 1.1; p<0.001]. Not surprisingly, those with HT,
specifically symptomatic HT, were more frequently re-imaged. Although the majority of
children had follow-up neuroimaging, 8 (10%) did not have follow-up CT or MRI within 30 days
of CE-AIS. Three (15%) children had change in HT over time; all had an increase in severity
from HI1 to HI2 as illustrated in Table 8. None had change from petechial hemorrhage to
parenchymal hematoma. HT was asymptomatic in 13 (16%), symptomatic in 5 (6%) and
unknown in 2 (2%).
Interestingly, there was no relationship between ECASS grade and symptomatic status with all
grades being symptomatic: 1 symptomatic PH2, 1 symptomatic PH1, 1 symptomatic HI2 and 2

Pulcine 80
symptomatic HI1. Two patients with HT were sedated and had no clinical examination at the
time of their HT and so were labelled as unknown. Asymptomatic HT occurs with a frequency of
3 – 37% in placebo groups and 5 – 43% in acute treatment groups in various IV thrombolysis
trials in adults (Khatri et al., 2007). However, given the low rate of hemorrhage and higher
potential for improved outcomes with thrombolytic therapy these factors do not preclude the
patient from receiving treatment (Khatri et al., 2007). Our rate of asymptomatic early
spontaneous HT was 7% in those that had HT on their initial neuroimaging but were not
receiving any prior antithrombotic therapy as illustrated in Figure 11. This may be an
underestimate of the spontaneous HT rate since HT evolves over days following the onset of
ischemic infarct, and the initial early imaging study may have preceded HT in some children.
The median time to HT was 4 days [IQR 3 – 7.5]. Since our study was retrospective and
observation the exact timing of HT is not precisely known. Figure 8 shows the timing of HT
from radiological CE-AIS diagnosis distributed by the type of antithrombotic therapy. Excluding
those with HT on their initial neuroimaging, there appears to be a peak of HT at 48 – 72 hours
which reflect adult literature. Following acute stroke there is breakdown of the blood brain
barrier resulting in friable intracranial vasculature which increases risk of intracerebral bleeding
into the area of ischemia (Marsh et al., 2013). HT is usually seen in the first 4 days following
infarction but is rare in the first 6 hours (Di Muzio, 2019). Almost 50% of infarcts will have
some form of HT although the incidence varies (Di Muzio, 2019). HT can occur as a result of
two different processes: petechial hemorrhagic or secondary hematoma (Di Muzio, 2019).
Petechial hemorrhage usually occurs within a day of thrombolysis and are seen on neuroimaging
as areas of small foci of bleeding with no associated mass effect and are not thought to affect
clinical outcome or management. Secondary hematoma formation is rarer and occurs in about
~5% of cases and has negative prognostic implications (Di Muzio, 2019; Fiorelli et al., 1999).
Secondary hematoma usually occurs within the first 4 days and are rare in the first 6 hours and
most commonly occur within 24 hours of ischemia-reperfusion (Di Muzio, 2019). It is possible
for large hemorrhagic transformation to occur at the time of acute infarction especially is a
patient who has coagulopathy or is pharmacologically anticoagulated (Hutchinson & Beslow,
2019). It is thought to arise from early ischemic-reperfusion injury as reperfusion of the damaged
vessels is not able to withstand the arterial pressures and ruptures (Di Muzio, 2019).

Pulcine 81
The first study to analyze the clinical and radiological predictors of HT in children with AIS,
irrespective of etiology, was performed by Beslow et al (Beslow et al., 2011). The study
retrospectively reviewed 63 children and found that 30% had HT within 30 days of stroke
(Beslow et al., 2011) with only 3% being symptomatic. Most hemorrhages were petechial 84%
(Beslow et al., 2011). There was no significant difference in the development of HT amongst
those children treated with antiplatelet therapy alone as compared to those treated with systemic
anticoagulation (35% vs. 21%; p=0.26) (Beslow et al., 2011). The development of HT was
significantly associated with an infarct volume greater than 5% of the supratentorial brain
volume (RR 4.81; 95% CI: 1.54 – 15.08; p=0.0026) with a trend toward increased risk of HT in
children with cardiac disease [RR 1.97; 95% CI: 0.96 – 0.45; p=0.12] and meningitis [RR 2.77;
95% CI: 1.37 – 5.59; p=0.08] (Beslow et al., 2011). The first study whose primary objective was
to evaluate the safety of protocol-based anticoagulant therapy in children with AIS, irrespective
of etiology, was conducted by Schechter et al. The study looked at a 14-year period of
prospectively enrolled cohort of children with AIS who were receiving anticoagulation therapy:
out of 215 children, 123 received anticoagulation therapy while 75 did not (Schechter et al.,
2012). The rate of HT was not significantly different between the two groups [11% vs. 16%]
(Schechter et al., 2012). No clinical or radiological predictors of anticoagulation-associated
hemorrhage were identified due to a small sample size (Schechter et al., 2012). The authors
concluded that anticoagulation is relatively safe in children with AIS with 4% risk of
symptomatic intracranial hemorrhage (Schechter et al., 2012).
Our rate of hemorrhagic transformation within 30 days of stroke is 24% which is comparable to
that of Beslow et al who reported a rate of 30% and double the rate of 11% reported by
Schechter et al (Table 13). This is the first cohort comprising of children with congenital and
acquired CHD at a tertiary care center. Our finding parallels the rate of clinically significant
major bleeding (including intra and extracranial) in critically ill children receiving therapeutic
unfractionated heparin, which is reported to be 24% (Kuhle et al., 2007). This rate reflects our
cohort well as the majority of our patients are medically fragile and require intensive care and
cardiac critical care monitoring. Our rate of symptomatic hemorrhage is double 6% compared to
that of 3% reported by Beslow et al and 4% reported by Schechter et al, which again can be
explained by the medical complexity and fragility of our patient population. Only 5% children
had systemic hemorrhage which included two with pulmonary hemorrhage, one with

Pulcine 82
hematochezia and one with a large 11 x 7 cm hematoma compressing the right ventricle and
displacing the heart to the left, felt most likely to be post-insertion of the Berlin heart cannula
(Table 7). There was no difference in the rate of systemic hemorrhage between the two groups.
This rate is lower than what is reported in adult literature on anticoagulation therapy and implies
that, from a systemic point of view, the current ATT being used to treat CE-AIS is safe in
children who are critically ill.
Beslow N=63 Schecter N=123 Pulcine N=82
Rate of Hemorrhagic
Transformation Within 30 Days 30% (19/63) 11% (14/123) 24% (20/82)
Rate of Symptomatic Hemorrhagic
Transformation Within 30 Days 3% (2/63) 4% (5/123) 6% (5/82)
Hemorrhagic Transformation on
Antiplatelet (APT) Therapy Alone
35% (34/63 on
APT) N/A
0% (5/82 on
APT)
Hemorrhagic Transformation on
Anticoagulant (ACT) Therapy
21% (24/63 on
ACT)
11% (123/215 on
ACT)
24% (20/82
on ACT)
European Cooperative Acute Stroke Study Grade of Antithrombotic Therapy-Associated
Hemorrhagic Transformation
HI1 14 7 9
HI2 2 3 6
PH1 2 0 4
PH2 1 1 1
Unknown 3
Table 13. Comparison of hemorrhagic transformation rates from three retrospective studies in
children with arterial ischemic stroke including our own.
Analysis of factors associated with HT included greater stroke volume [modified ASPECTS 6.1
± 3.3 vs. 3.5 ± 2.3; p=0.006] (Table 7) and a trend for combination ATT [32% vs. 68%; p=0.06]
(Table 11), which is often administered in a step-wise fashion at our institution, with initial IV
heparin, when the risk of hemorrhage is deemed to be relatively high so that it can be quickly
reversed. Presence of univentricular physiology appeared to be protective from hemorrhagic
transformation although we did not control for volume of infarct [10% vs. 90%; p=0.03] (Table
3). Due to the small sample size no significant predictors of symptomatic HT were found.

Pulcine 83
5.1.5 Antithrombotic Therapy
Seventy-eight (95%) patients received antithrombotic therapy within 30 days of CE-AIS, which
was initiated at a mean of 1.5 ± 5.7 days [0 – 4]. Of these, 63 (77%) commenced treatment or
their antithrombotic regimen was escalated, while 15 (18%) had no change in antithrombotic
treatment as illustrated in Table 9. In interpreting our findings, it is important to keep in mind
that ATT was not administered in a randomized fashion contributing to selection bias. Children
with abnormal cardiac anatomy and a potential cardioembolic source are more likely to receive
ongoing antithrombotic therapy. Many will already be on prophylactic or therapeutic therapy at
the time of stroke ictus for a number of reasons and therefore may not have their antithrombotic
therapy escalated based on clinical risk versus benefit. Indications for antithrombotic treatment
included cardiac prophylaxis, systemic vein thrombosis, ECMO, CPB, VAD and secondary
stroke prevention, as outlined in Figure 12. Out of the 4 patients that did not receive ATT, none
had late spontaneous HT. These 4 patients were treated conservatively because of concerns about
malignant transformation of their infarct in 2 and infective endocarditis in 2.
Amongst children receiving antithrombotic therapy, the majority were treated with anticoagulant
therapy 82%, only 6% were receiving antiplatelet therapy alone and 12% were on combination
therapy. This reflects the current treatment guidelines that recommend anticoagulation over
aspirin initially if a cardioembolic source is present. Systemic anticoagulation was not
significantly associated with HT in this study consistent with data from previous studies (Beslow
et al., 2011; Schechter et al., 2012). In addition, no patient on antiplatelet therapy alone had HT
in our cohort.
We looked at the ATT dose intensity and the type of ATT at the time of hemorrhage. For
unfractionated heparin, the therapeutic range was defined as an Xa level of 0.35 – 0.7 IU/mL; for
low molecular weight heparin, the therapeutic range was defined as an Xa level of 0.5 – 1.0
IU/mL; and for warfarin, the therapeutic range was defined as an INR of 2.0 – 3.0. Values below
and above this were defined as sub- and supratherapeutic. Out of the 20 patients with HT 6
(30%) were subtherapeutic on ATT at the time of HT, 13 (65%) were therapeutic and 1 (5%) was
supratherapeutic. This implies that there are multiple interacting risk factors that lead to HT
some possibly unrelated to the anticoagulation treatment as the majority of the patients were not
supratherapeutic on their ATT at the time of hemorrhage.

Pulcine 84
Among children receiving antithrombotic therapy following CE-AIS diagnosis, 20 (26%) were
on monotherapy, 50 (64%) were on sequential combination therapy and 16 (21%) were on
concurrent combination therapy. There was no difference in the use of concurrent combination
therapy between the two groups [25% vs. 75%; p=1.00]. There was a trend for sequential
combination ATT [32% vs. 68%; p=0.06], which is often administered in a stepwise fashion at
our institution, with initial IV heparin, when the risk of hemorrhage is deemed to be relatively
high so that it can be quickly reversed.
In order to control for coagulopathy, as a risk for HT, we looked at available hematological
parameters including platelet count, INR, PTT, fibrinogen and d-dimer. Given the retrospective
nature of this study, a large proportion of patients had missing laboratory values including
fibrinogen, prothrombin time, and d-dimer, precluding the use of a number of validated tools
such as the International Society of Thrombosis and Hemostasis Disseminated Intravascular
Coagulation score (ISTH-DIC) (Levi, Toh, Thachil, & Watson, 2009). This score relies on
platelet count, increase in fibrin markers, prothrombin time prolongation and fibrinogen level
(Levi et al., 2009) and is only appropriate for patients with an underlying medical condition that
can be associated with DIC. None of our patients had DIC. As a result, we compared the
hematological parameters that were available in most patients: platelet count, INR and PTT. In
comparing the absolute mean values between those with and without HT we found no statistical
difference. In addition, we looked at the 20 patients with HT and compared their platelet, INR
and PTT counts at the time of radiological CE-AIS diagnosis and time of radiological HT and
found no significant differences. Other values could not be compared due to the large proportion
of missing lab values. The missing lab values also lead to a likely under-estimation of
prothrombotic abnormalities in our patients.
Two children received thrombolysis with IA or IV tPA and did not have any subsequent
intracerebral hemorrhage: one child presented with a hyperactue stroke with proximal artery
occlusion and received intra-arterial tPA 9 mg in total before diagnosis of endocarditis was
made; the other child received IV tPA for left aortic thrombus occluding the left main coronary
artery, discovered shortly after birth, resulting in left ventricular infarction and subsequent CE-
AIS due to thromboembolism. No child received endovascular mechanical clot retrieval. The
numbers wherein are too small to draw conclusions.

Pulcine 85
Undoubtedly, one of the main concerns reflected in the varying institutional practices for
thromboprophylaxis for CE-AIS is the risk of systemic and intracranial bleeding complications.
Studies have reported an overall incidence of major bleeding of 24% in critically ill children
receiving therapeutic unfractionated heparin (Kuhle et al., 2007), less than 5% in children on
enoxaparin (Manlhiot et al., 2010) and less than 0.5% per year for children on warfarin (Streif et
al., 1999). Overall our results parallel the reported rate of clinically significant major bleeding,
including intra- and extracranial. Given the previously reported high rate of stroke recurrence in
children with CHD, 27% over the course of 10 years (Rodan et al., 2012), the benefit in this
population appears to outweigh the risk. However, the risk-benefit ratio of ATT remains
unknown in the context of each primary cardiac diagnosis and warrants further study.
5.1.6 Arterial Ischemic Stroke Recurrence
Stroke recurrence occurred in 13% at a median time of 32 days (IQR 5.5 – 93) from the index
stroke. This finding is consistent with previous reports that the risk of stroke recurrence in
children with congenital and acquired heart disease is significant: between 17% at a median time
of 21 days (Asakai et al., 2015) and 27% over the course of 10 years (Rodan et al., 2012).
However, the rate of stroke recurrence in our cohort was lower than previously reported despite
an adequate follow-up interval of 4.1 ± 3.5 years. In addition, the majority of children were
receiving ACT or a combination of ACT and APT at the time of recurrence as illustrated in
Table 10. This implies that ATT is effective in preventing stroke recurrence as exemplified by
the lower rate but also illustrates that further optimization of ATT is necessary as the majority of
children with stroke recurrence 91% were already on ATT. Unfortunately, therapeutic drug
monitoring was not available, given a large proportion of silent infarcts, to indicate if the
treatment dose was in the target range at the time of stroke recurrence. Likely patients perceived
to have the highest risk of recurrent stroke were selected by clinicians at our institution for more
intense ATT in some cases despite risks. This introduces the bias that would be avoided in a
randomized controlled trial. Rodan et al showed that the hazard ratio of stroke recurrence was
highest in the period following the initial AIS and that this risk decreased over time (Rodan et
al., 2012). On the other hand, Fox et al showed that recurrence risk remained elevated beyond the
immediate postoperative period, with almost half the cases occurring > 5 years after the most
recent procedure (Fox et al., 2015). Our cohort appears to corroborate the findings of Rodan et al
with an average time to recurrence of 70.6 days and a range of 3 – 241 days. None of the 82

Pulcine 86
children followed for more than 241 days were found to have recurrence with a mean follow-up
time of 4.1 ± 3.5 years. However, since most recurrent infarcts were silent (55%) and routine
follow-up neuroimaging in the months and years following index CE-AIS is not usually
performed, we likely underestimate the overall recurrence risk. Furthermore, factors that were
previously found by Rodan et al to be associated with an increased risk of stroke recurrence –
presence of mechanical valve, prothrombotic state, or systemic infection at the time of sentinel
stroke – were not found in our cohort. However, our main study aim was not to look at predictors
of stroke recurrence and as such these may have been inadvertently missed. Although
cardiopulmonary bypass, cardiac surgery and catheterization procedures represent important risk
factors for recurrent thromboembolism only 1 child had both procedure-related sentinel stroke
and procedure-related recurrence in our cohort.
When we looked at recurrence by type of cardiac physiology those with cyanotic CHD pre-
cardiac repair, post-palliative surgery with residual right-to-left shunting and those with
cardiomyopathy (Table 12) were the ones at highest risk. Only one child with acyanotic CHD
that was fully repaired had recurrence. Perhaps most interesting, no children with cyanotic CHD
that underwent definitive repair, for example those with TGA post arterial switch, had
recurrence. Mechanistically this is intuitive: those with cardiomyopathy have impaired left
ventricular ejection fraction and in adults heart failure has been shown to have an important
thromboembolic risk (Homma et al., 2012). Those with residual right-to-left shunting also have
ongoing thromboembolic risk. However, once the right-to-left shunt is closed the
thromboembolic risk is no longer present. Although our numbers are small, these findings can
have major clinical implications: in the absence of abnormal left ventricular function, residual
right-to-left shunting, and other individual stroke risk factors, ATT therapy may no longer be
required for secondary stroke prevention. This is again supported by published literature that
amongst different type of cardiac diagnosis, children with univentricular congenital heart
disease, with right-to-left shunting, appear to be at greatest risk of AIS, with a stroke incidence
rate of 1380 in 100 000 (Hoffman et al., 2011). Perhaps the single ventricle patients are
hypercoagulable, and this may protect them from HT; however, the ATT they receive is not
enough to downgrade their stroke recurrence risk. Whether this is a matter of low anticoagulant
power, lack of additional antiplatelet effect, or a third factor not addressed by any of those
agents, remains to be elucidated in a future multicenter trial.

Pulcine 87
5.1.7 Neurological Outcome
The impact of childhood stroke lasts well into adulthood and contributes to significant morbidity.
Neurological sequelae including cerebral palsy, epilepsy and higher cognitive deficits, in
surviving children post stroke have been quoted to be as high as 50 – 80% and mortality has been
quoted to be as high as 20 – 40% and even higher, one third, for primary hemorrhagic stroke
(Roach et al., 2008). Unlike in adults, developmental factors in the growing and maturing brain
contribute to the overall recovery and outcome from stroke in neonates and children. This means
that the outcomes of individual strokes in children cannot simply be determined by location of
injury but must be evaluated with a developmental lens in mind. In addition, there is added
complexity in that children with CHD have been found to have pre-existing deficits in cerebral
development such as high proportion of white matter lesions, lower brain volume and more
immature brain structure (Limperopoulos et al., 2001; Miller et al., 2007).
Follow-up information was available in 80 (98%) children with a mean time to follow-up of 4.1
± 3.5 years [0.0 – 12.9]. PSOM scores were dichotomized into good and poor outcome as
previously described. In our study, 34% had poor neurological outcome, which may be explained
by both a high proportion of children with a cardioembolic pattern of multifocal lesions 50%
[39% concurrent and 11% of differing ages], bilateral lesions in 20% and relatively higher rates
of recurrent AIS 13%. Additional brain injury beyond that attributable to the CE-AIS and due to
the cardiac disorder or surgical procedures likely contributes to poor outcome in our population.
Furthermore, an important finding in our multivariate logistic regression was a trend toward poor
outcome with HT independent of stroke volume [adjusted OR 3.63; 95% CI 0.96 – 13.81;
p=0.06]. Mean time to PSOM with and without HT was not significantly different [3.3 ± 2.9 vs.
4.3 ± 3.6 years; p=0.35] indicating that the tendency for poor outcome in the hemorrhagic
transformation group was not due to differing timing of follow-up assessments. We also looked
at the relationship between increasing grades of ECASS severity and neurological outcome.
When ECASS severity was categorized into normal (no HT), mild (HI1 and HI2 75%) and
severe (PH1 and PH2 25%) and compared to the dichotomized PSOM scores of good versus
poor, the proportion of patients with a favorable outcome decreased as the ECASS severity
increased as illustrated in Figure 14. These findings are concordant with each other and
supported in the literature. It is well recognized that blood products are toxic to the surrounding
brain parenchyma both due to mechanical compression and indirect ischemic injury (Park et al.,

Pulcine 88
2012). In adults, asymptomatic HT has been shown to adversely affect clinical outcome after
acute ischemic stroke despite lack of acute neurological deterioration (Park et al., 2012). Even in
the absence of hemorrhagic conversion of an ischemic brain injury, MRI demonstrating
hemosiderin staining indicative of previous brain hemorrhage has been associated with poorer
developmental outcomes in children with repaired congenital heart disease when compared to
controls without hemosiderin (Soul et al., 2009). These findings suggest that asymptomatic
hemorrhage, whether in the form of hemosiderin scattered through the brain parenchyma due to
cardiopulmonary bypass or hemorrhagic conversion of an ischemic stroke, is not entirely
innocuous, particularly in the growing and maturing brain. Such findings on imaging may be a
marker for more diffuse brain injury in this population.
Death occurred in 12 children (15%), 7 of whom died in the same hospital admission during
which CE-AIS was diagnosed and a further 5 during long-term follow-up as illustrated in Figure
15. The majority of deaths 67% were attributed to cardiac causes. One child with symptomatic
PH2 on day 6 post anticoagulant therapy with heparin followed by LMWH died secondary to
their intracranial hemorrhage. None of the remaining children died as a result of HT and only
one child who could did not undergo a decompressive craniectomy died as a result of their CE-
AIS due to cerebral herniation. The mortality rates appear to be similar to those reported by other
retrospective studies of AIS in children with cardiac and non-cardiac etiologies (Asakai et al.,
2015; Schechter et al., 2012).
5.2 Study Strengths
One of the main strengths of the study is that it is the largest single-center longitudinal cohort of
children with CE-AIS receiving ATT according to institutional guidelines and standardized
clinical practice, allowing for detailed comparative analysis. In addition, we included patients
who had follow-up neuroimaging with CT and/or MRI after anticoagulation therapy was
initiated. Obtaining neuroimaging in children with cardiac disease is challenging given
requirements for cardiac anesthesia, temporary pacing wires and mechanical support devices and
overall medical fragility combined with the high medical acuity of these patients. Based on
institutional guidelines, CT or MRI scans were routinely performed on average 3 to 5 days post
antithrombotic therapy initiation and with any clinical suspicion of hemorrhagic transformation.
This ensured that all cases of hemorrhagic transformation, asymptomatic and symptomatic, were

Pulcine 89
identified uniformly without bias towards imaging only those patients that were symptomatic. In
addition, all CT and MRI images were re-evaluated by a neuroradiologist who was blinded to the
clinical characteristics and progression towards hemorrhagic transformation. This ensured that
all cases of hemorrhagic transformation were accurately identified without prior selection bias
from the pediatric neurologist and ECASS scoring was consistent across raters. This systematic
blinded review of all available imaging minimized bias in detection of HT.
5.3 Study Limitations
The major limitation is the retrospective nature of this study. As a single-center study the sample
size that was not large enough to perform a well-powered multivariate logistic regression
analysis to detect difference between those with and without HT. The need for a larger patient
sample in CE-AIS is underlined by the highly heterogeneous population in which many patients
have unique circumstances and rare comorbidities that cannot be accounted for in a limited
sample. This study thus had limited power to detect associations or to adjust for potential
confounders. Also, as the primary study cohort was from a tertiary care center generalization of
the results to the broader pediatric cardiac population may be limited. Due to the retrospective
nature of the study, timing and modality of imaging varied widely and was dictated by variations
in patient’s presentation and imaging availability. A large proportion of cardioembolic arterial
ischemic stroke patient had initial and follow-up CT due to severity of their illness which
precluded the use of MRI. The relatively poor sensitivity of CT to detect subtle areas of ischemia
or punctate hemorrhage limited our ability to accurately quantify infarct size using the modified
pediatric ASPECTS. In addition, the heterogeneity in the time interval from stroke onset to the
acquisition of and frequency of follow-up imaging may have resulted in some asymptomatic
hemorrhagic transformation cases being missed. Those with large infarcts or with hemorrhagic
transformation had more frequent follow-up neuroimaging.
There was difficulty in differentiating cortical laminar necrosis from hemorrhagic infarction type
1 (HI1). Most areas of cortical laminar necrosis in pediatric patients showed no hemorrhage on
SWI (Niwa, Aida, Shishikura, Fujita, & Inoue, 2008) but most follow-up imaging was limited to
only CT scans. As a result, some cases of cortical laminar necrosis may have been overcalled as
HI1. A further limitation was the inability to evaluate stroke volume in 26 (32%) of our subjects.
The modified pediatric ASPECTS, which was used as a surrogate marker of stroke volume, is

Pulcine 90
subject to several limitations. The modified pediatric ASPECTS overestimates lesions volume in
multifocal stroke, it does not account for infratentorial stoke (i.e. cerebellar and brainstem) and it
if validated on DWI MRI but not on acute CT unlike the adult ASPECTS (Beslow et al., 2012).
A large proportion of cardioembolic stroke patients have CT due to severity of their illness and
several contraindications for MRI (i.e. cardiac pacemaker, pacing wires, ECMO, VAD etc.)
Another limitation in our ability to delineate factors associated with HT was lack of an objective
measurement of the initial clinical stroke severity by means of a stroke severity scale in our
study. Since stroke volume and clinical stroke severity are known risk factors for hemorrhagic
transformation in adults these limitations hamper our study.
Measure of hemostasis were gathered from retrospective chart abstraction; there were likely
numerous instances where heparin contamination of a central line blood sample used for testing
artificially prolonged the PTT. In addition, an overwhelming proportion of standardized
hematological parameters were missing, especially in the earlier years of the cohort. As a result,
we were not able to assess or control for varying degrees of coagulopathy.
Most importantly, our study is a nonrandomized comparison and so is subject to selection bias
with exclusion of patients with severe hemorrhagic transformation from receiving antithrombotic
therapy and inclusion of more mildly affected patients to receive antithrombotic therapy. It is
conceivable that the perceived risk of complications, based on patient characteristics and
comorbidities influences the choice of whether to use antiplatelet or anticoagulant therapy and
this might have affected the assessment of association between hemorrhagic transformation and
type of antithrombotic therapy used. Those with prior recurrence or multiple strokes may have
been treated with antithrombotic therapy despite hemorrhagic risks due to a perceived higher rate
of inherent recurrence leading to a treatment selection bias.
Finally, available data was limited to what was reported in the medical records, which may not
have been complete and the patients’ outpatient compliance with antithrombotic therapy at the
time of recurrence could not be readily assessed from the available records.

Pulcine 91
Conclusion
Overall our results parallel the reported rate of 24% of clinically significant major bleeding,
intra- and extracranially, in critically ill children receiving therapeutic unfractionated heparin and
antithrombotic therapy for secondary stroke prevention (Beslow et al., 2011; Kuhle et al., 2007;
Schechter et al., 2012). The 5% rate of clinically significant systemic hemorrhage is not elevated
compared to that of adult studies where systemic anticoagulation is felt to come at a higher cost
of bleeding complications. In addition, our results suggest a lower rate of stroke recurrence than
the previously reported 27% at 10 years (Rodan et al., 2012). Given the negative impact of
thromboembolic complications on survival in children with univentricular CHD (Manlhiot et al.,
2012), and the relatively low risk of significant bleeding complications leading to mortality seen
in our study, it is reasonable to conclude that ATT appears to be relatively safe in children with
CE-AIS for secondary stroke prevention. However, ATT warrants further optimization to
prevent stroke recurrence, particularly in those with univentricular physiology and impaired left
ventricular function. While only 6% were symptomatic, long-term follow-up showed a trend
towards worse neurological outcome in those with both asymptomatic and symptomatic HT even
when we controlled for infarct volume, which implies that blood products are not entirely
innocuous. Further multi-center prospective studies are needed to study antithrombotic therapy
as research in this area has been hampered by heterogeneity in the patient population.

Pulcine 92
Future Directions
There remains a need for large multicenter trials of antithrombotic therapy in pediatric patients
with cardiac disease to improve clinical and developmental outcomes. Ideally, future endeavors
would focus on creating a hemorrhagic risk calculator for risk stratification of children with
cardioembolic arterial ischemic stroke to predict any hemorrhagic transformation within 30 days
of sentinel stroke regardless of the type of antithrombotic therapy used. This would require a
prospective cohort. Further refinement of patient selection criteria for more or less intensive ATT
strategies is another need. In the past, cardioembolic stroke in children has been treated as a
single entity despite known differences in etiological risk with uniform recommendations for
secondary stroke prevention strategies. This had an advantage in that is allowed for a detailed
comparative analysis which was carried out in this study. However, it is time to further refine
consensus-based treatment guidelines in cardioembolic arterial ischemic stroke in children based
on the underlying primary cardiac diagnosis. Retrospective analyses like ours is vital as they
stimulate us to reflect and critically review our own management practices from time to time in
areas as rare, but potentially with the greatest potential for refinement, as stroke prevention in
congenital and acquired CHD. To this end, this study urges and challenges us to collaborate in
such rare conditions such as childhood CE-AIS, towards the design of prospective clinical trials.
The major requirement of such a randomized clinical trial is 1) establishment of definitive ACT
dosing, intensity and safety data and 2) standardized long-term radiological and clinical outcome
data. Practical recommendations would include standardizing measurements of blood pressure,
coagulation parameters, modality and timing of follow-up neuroimaging as well as ATT
thromboprophylaxis based on the underlying primary cardiac diagnosis.
Issue of coagulopathy stratification can be overcome with a prospective trial or we may defer to
the literature on brain trauma, which uses degree of coagulopathy to predict brain bleeding. In
brief, this can be quantified by using the ratios of PTT or PT (severe: > 1.5, moderate: between
1.2-1.5, normal: < 1.2) and platelet count (severe: < 50; moderate: 50-100; mild: 100-150). A
final score would then yield a yes vs. no, with severe to anyone with yes in the severe category.
Of course, PT would need to be gathered on all patients and the clinical significance of this score
would need to be validated in a prospective cohort.

Pulcine 93
Another possibility is the development of a new classification system for pediatric-specific
hemorrhagic transformation of varying severity with possible varied impact on neurological
outcome after cardioembolic arterial ischemic stroke. The ECASS system while convenient, is
outdated for the pediatric patient population and for the MRI neuroimaging that is required in
pediatric stoke. In addition, voxel-based lesion symptom mapping would allow us to look at the
location most prone to HT. Quantitative volumetric analysis using software such as ITK-SNAP
or FreeSurfer and creating lesion maps would be helpful in further delineating stroke location
and volume as a risk factor for HT.

Pulcine 94
References
Agrawal, N., Johnston, S. C., Wu, Y. W., Sidney, S., & Fullerton, H. J. (2009). Imaging data
reveal a higher pediatric stroke incidence than prior US estimates. Stroke, 40(11), 3415-
3421. doi:10.1161/STROKEAHA.109.564633
Allen D. Everett, D. Scott Lim. (2011). Illustrated Field Guide to Congenital Heart Disease and
Repair (Jasper Burns Ed. 3rd ed.). Charlottesville, VA: Scientific Software Solutions,
Inc.
Allen, L. M., Hasso, A. N., Handwerker, J., & Farid, H. (2012). Sequence-specific MR imaging
findings that are useful in dating ischemic stroke. Radiographics, 32(5), 1285-1297;
discussion 1297-1289. doi:10.1148/rg.325115760
Almond, C. S., Singh, T. P., Gauvreau, K., Piercey, G. E., Fynn-Thompson, F., Rycus, P. T., . . .
Thiagarajan, R. R. (2011). Extracorporeal membrane oxygenation for bridge to heart
transplantation among children in the United States: analysis of data from the Organ
Procurement and Transplant Network and Extracorporeal Life Support Organization
Registry. Circulation, 123(25), 2975-2984.
doi:10.1161/CIRCULATIONAHA.110.991505
Amlie-Lefond C, Ichord R, Abraham M, Barry D, Bernard T, Dowling M, Felling R, Kirton A,
Kurz J, Lee S, McMillan H, Rivkin M, Torres M, Cooper A, on behalf of TIPSTERS
Investigators. (2019). Children Are Not at Increased Risk of Symptomatic Intracranial
Hemorrhage Following Intravenous Tissue Plasminogen Activator for Acute Stroke.
International Stroke Conference.
Amlie-Lefond, C. (2018). Evaluation and Acute Management of Ischemic Stroke in Infants and
Children. Continuum (Minneap Minn), 24(1, Child Neurology), 150-170.
doi:10.1212/CON.0000000000000559
Andrade, A., Yau, I., & Moharir, M. (2015). Current concepts in pediatric stroke. Indian J
Pediatr, 82(2), 179-188. doi:10.1007/s12098-014-1604-3
Andrew, M., Paes, B., Milner, R., Johnston, M., Mitchell, L., Tollefsen, D. M., . . . Powers, P.
(1988). Development of the human coagulation system in the healthy premature infant.
Blood, 72(5), 1651-1657.
Andrew, M., Paes, B., Milner, R., Johnston, M., Mitchell, L., Tollefsen, D. M., & Powers, P.
(1987). Development of the human coagulation system in the full-term infant. Blood,
70(1), 165-172.
Andrew, M., Vegh, P., Johnston, M., Bowker, J., Ofosu, F., & Mitchell, L. (1992). Maturation of
the hemostatic system during childhood. Blood, 80(8), 1998-2005.
Asakai, H., Cardamone, M., Hutchinson, D., Stojanovski, B., Galati, J. C., Cheung, M. M., &
Mackay, M. T. (2015). Arterial ischemic stroke in children with cardiac disease.
Neurology, 85(23), 2053-2059. doi:10.1212/WNL.0000000000002036
Barker, P. C., Nowak, C., King, K., Mosca, R. S., Bove, E. L., & Goldberg, C. S. (2005). Risk
factors for cerebrovascular events following fontan palliation in patients with a functional
single ventricle. Am J Cardiol, 96(4), 587-591. doi:10.1016/j.amjcard.2005.04.025
Beghi, E., Boglium, G., Cosso, P., Fiorelli, G., Lorini, C., Mandelli, M., & Bellini, A. (1995).
Stroke and alcohol intake in a hospital population. A case-control study. Stroke, 26(9),
1691-1696.
Benedik, M. P., Zaletel, M., Meglic, N. P., & Podnar, T. (2011). A right-to-left shunt in children
with arterial ischaemic stroke. Arch Dis Child, 96(5), 461-467.
doi:10.1136/adc.2010.203992

Pulcine 95
Bernard, T. J., Goldenberg, N. A., Tripputi, M., Manco-Johnson, M. J., Niederstadt, T., &
Nowak-Gottl, U. (2009). Anticoagulation in childhood-onset arterial ischemic stroke with
non-moyamoya arteriopathy: findings from the Colorado and German (COAG)
collaboration. Stroke, 40(8), 2869-2871. doi:10.1161/STROKEAHA.109.550699
Bernson-Leung, M. E., & Rivkin, M. J. (2016). Stroke in Neonates and Children. Pediatr Rev,
37(11), 463-477. doi:10.1542/pir.2016-0002
Beslow, L. A., Smith, S. E., Vossough, A., Licht, D. J., Kasner, S. E., Favilla, C. G., . . . Ichord,
R. N. (2011). Hemorrhagic transformation of childhood arterial ischemic stroke. Stroke,
42(4), 941-946. doi:10.1161/STROKEAHA.110.604199
Beslow, L. A., Vossough, A., Dahmoush, H. M., Kessler, S. K., Stainman, R., Favilla, C. G., . . .
Smith, S. E. (2012). Modified Pediatric ASPECTS Correlates with Infarct Volume in
Childhood Arterial Ischemic Stroke. Front Neurol, 3, 122. doi:10.3389/fneur.2012.00122
Bigi, S., Dulcey, A., Gralla, J., Bernasconi, C., Melliger, A., Datta, A. N., . . . Steinlin, M.
(2018). Feasibility, safety, and outcome of recanalization treatment in childhood stroke.
Ann Neurol, 83(6), 1125-1132. doi:10.1002/ana.25242
Block, A. J., McQuillen, P. S., Chau, V., Glass, H., Poskitt, K. J., Barkovich, A. J., . . . Miller, S.
P. (2010). Clinically silent preoperative brain injuries do not worsen with surgery in
neonates with congenital heart disease. J Thorac Cardiovasc Surg, 140(3), 550-557.
doi:10.1016/j.jtcvs.2010.03.035
Butany, J., Nair, V., Naseemuddin, A., Nair, G. M., Catton, C., & Yau, T. (2005). Cardiac
tumours: diagnosis and management. Lancet Oncol, 6(4), 219-228. doi:10.1016/S1470-
2045(05)70093-0
Cabrera, A. G., Sundareswaran, K. S., Samayoa, A. X., Jeewa, A., McKenzie, E. D., Rossano, J.
W., . . . Morales, D. L. (2013). Outcomes of pediatric patients supported by the
HeartMate II left ventricular assist device in the United States. J Heart Lung Transplant,
32(11), 1107-1113. doi:10.1016/j.healun.2013.07.012
Casaubon, L. K., Boulanger, J. M., Blacquiere, D., Boucher, S., Brown, K., Goddard, T., . . .
Stroke Foundation of Canada Canadian Stroke Best Practices Advisory, Committee.
(2015). Canadian Stroke Best Practice Recommendations: Hyperacute Stroke Care
Guidelines, Update 2015. Int J Stroke, 10(6), 924-940. doi:10.1111/ijs.12551
Cengiz, P., Seidel, K., Rycus, P. T., Brogan, T. V., & Roberts, J. S. (2005). Central nervous
system complications during pediatric extracorporeal life support: incidence and risk
factors. Crit Care Med, 33(12), 2817-2824.
deVeber, G. (2000). Canadian paediatric ischemic stroke registry: analysis of children with
arterial ischemic stroke. Ann Neurol. Ann Neurol, 48, 526.
deVeber, G. A., Kirton, A., Booth, F. A., Yager, J. Y., Wirrell, E. C., Wood, E., . . . Bjornson, B.
H. (2017). Epidemiology and Outcomes of Arterial Ischemic Stroke in Children: The
Canadian Pediatric Ischemic Stroke Registry. Pediatr Neurol, 69, 58-70.
doi:10.1016/j.pediatrneurol.2017.01.016
Di Muzio, Bruno; Gaillard, Frank. (2019). Hemorrhagic transformation of ischemic infarct.
Domi, T., Edgell, D. S., McCrindle, B. W., Williams, W. G., Chan, A. K., MacGregor, D. L., . . .
deVeber, G. A. (2008). Frequency, predictors, and neurologic outcomes of vaso-
occlusive strokes associated with cardiac surgery in children. Pediatrics, 122(6), 1292-
1298. doi:10.1542/peds.2007-1459
Dowling, M. M., Hynan, L. S., Lo, W., Licht, D. J., McClure, C., Yager, J. Y., . . . International
Paediatric Stroke Study, Group. (2013). International Paediatric Stroke Study: stroke

Pulcine 96
associated with cardiac disorders. Int J Stroke, 8 Suppl A100, 39-44. doi:10.1111/j.1747-
4949.2012.00925.x
Emani, S., Trainor, B., Zurakowski, D., Baird, C. W., Fynn-Thompson, F. E., Pigula, F. A., &
Emani, S. M. (2014). Aspirin unresponsiveness predicts thrombosis in high-risk pediatric
patients after cardiac surgery. J Thorac Cardiovasc Surg, 148(3), 810-814; discussion
814-816. doi:10.1016/j.jtcvs.2014.06.016
Emberson, J., Lees, K. R., Lyden, P., Blackwell, L., Albers, G., Bluhmki, E., . . . Stroke
Thrombolysis Trialists' Collaborative, Group. (2014). Effect of treatment delay, age, and
stroke severity on the effects of intravenous thrombolysis with alteplase for acute
ischaemic stroke: a meta-analysis of individual patient data from randomised trials.
Lancet, 384(9958), 1929-1935. doi:10.1016/S0140-6736(14)60584-5
Ferriero, D. M., Fullerton, H. J., Bernard, T. J., Billinghurst, L., Daniels, S. R., DeBaun, M. R., .
. . Stroke, Nursing. (2019). Management of Stroke in Neonates and Children: A Scientific
Statement From the American Heart Association/American Stroke Association. Stroke,
50(3), e51-e96. doi:10.1161/STR.0000000000000183
Fiorelli, M., Bastianello, S., von Kummer, R., del Zoppo, G. J., Larrue, V., Lesaffre, E., . . .
Bozzao, L. (1999). Hemorrhagic transformation within 36 hours of a cerebral infarct:
relationships with early clinical deterioration and 3-month outcome in the European
Cooperative Acute Stroke Study I (ECASS I) cohort. Stroke, 30(11), 2280-2284.
Firdouse, M., Agarwal, A., Chan, A. K., & Mondal, T. (2014). Thrombosis and thromboembolic
complications in fontan patients: a literature review. Clin Appl Thromb Hemost, 20(5),
484-492. doi:10.1177/1076029613520464
Fox, C. K., Sidney, S., & Fullerton, H. J. (2015). Community-based case-control study of
childhood stroke risk associated with congenital heart disease. Stroke, 46(2), 336-340.
doi:10.1161/STROKEAHA.114.007218
Fraser, C. D., Jr., Jaquiss, R. D., Rosenthal, D. N., Humpl, T., Canter, C. E., Blackstone, E. H., . .
. Berlin Heart Study, Investigators. (2012). Prospective trial of a pediatric ventricular
assist device. N Engl J Med, 367(6), 532-541. doi:10.1056/NEJMoa1014164
Gewillig, M., & Brown, S. C. (2016). The Fontan circulation after 45 years: update in
physiology. Heart, 102(14), 1081-1086. doi:10.1136/heartjnl-2015-307467
Giang, K. W., Mandalenakis, Z., Dellborg, M., Lappas, G., Eriksson, P., Hansson, P. O., &
Rosengren, A. (2018). Long-Term Risk of Hemorrhagic Stroke in Young Patients With
Congenital Heart Disease. Stroke, 49(5), 1155-1162.
doi:10.1161/STROKEAHA.117.020032
Giglia, T. M., Massicotte, M. P., Tweddell, J. S., Barst, R. J., Bauman, M., Erickson, C. C., . . .
Stroke, Council. (2013). Prevention and treatment of thrombosis in pediatric and
congenital heart disease: a scientific statement from the American Heart Association.
Circulation, 128(24), 2622-2703. doi:10.1161/01.cir.0000436140.77832.7a
Giroud, M., Lemesle, M., Gouyon, J. B., Nivelon, J. L., Milan, C., & Dumas, R. (1995).
Cerebrovascular disease in children under 16 years of age in the city of Dijon, France: a
study of incidence and clinical features from 1985 to 1993. J Clin Epidemiol, 48(11),
1343-1348. doi:10.1016/0895-4356(95)00039-9
Go, A. S., Mozaffarian, D., Roger, V. L., Benjamin, E. J., Berry, J. D., Blaha, M. J., . . . Stroke
Statistics, Subcommittee. (2014). Heart disease and stroke statistics--2014 update: a
report from the American Heart Association. Circulation, 129(3), e28-e292.
doi:10.1161/01.cir.0000441139.02102.80
Pulcine 97
Goyal, M., Menon, B. K., van Zwam, W. H., Dippel, D. W., Mitchell, P. J., Demchuk, A. M., . . .
collaborators, Hermes. (2016). Endovascular thrombectomy after large-vessel ischaemic
stroke: a meta-analysis of individual patient data from five randomised trials. Lancet,
387(10029), 1723-1731. doi:10.1016/S0140-6736(16)00163-X
Gunthard, J., Stocker, F., Bolz, D., Jaggi, E., Ghisla, R., Oberhansli, I., & Wyler, F. (1997).
Dilated cardiomyopathy and thrombo-embolism. Eur J Pediatr, 156(1), 3-6.
doi:10.1007/s004310050541
Gupta, A. A., Leaker, M., Andrew, M., Massicotte, P., Liu, L., Benson, L. N., & McCrindle, B.
W. (2001). Safety and outcomes of thrombolysis with tissue plasminogen activator for
treatment of intravascular thrombosis in children. J Pediatr, 139(5), 682-688.
doi:10.1067/mpd.2001.118428
Hage, A., Louzada, M., & Kiaii, B. (2019). Sepsis-induced heparin resistance during
extracorporeal membrane oxygenation. CMAJ, 191(10), E283-E285.
doi:10.1503/cmaj.181061
Harris, P. A., Taylor, R., Thielke, R., Payne, J., Gonzalez, N., & Conde, J. G. (2009). Research
electronic data capture (REDCap)--a metadata-driven methodology and workflow
process for providing translational research informatics support. J Biomed Inform, 42(2),
377-381. doi:10.1016/j.jbi.2008.08.010
Hoffman, J. L., Mack, G. K., Minich, L. L., Benedict, S. L., Heywood, M., Stoddard, G. J., &
Saarel, E. V. (2011). Failure to impact prevalence of arterial ischemic stroke in pediatric
cardiac patients over three decades. Congenit Heart Dis, 6(3), 211-218.
doi:10.1111/j.1747-0803.2011.00510.x
Hoffmann, A., Chockalingam, P., Balint, O. H., Dadashev, A., Dimopoulos, K., Engel, R., . . .
Oechslin, E. (2010). Cerebrovascular accidents in adult patients with congenital heart
disease. Heart, 96(15), 1223-1226. doi:10.1136/hrt.2010.196147
Homma, S., Thompson, J. L., Pullicino, P. M., Levin, B., Freudenberger, R. S., Teerlink, J. R., . .
. Investigators, Warcef. (2012). Warfarin and aspirin in patients with heart failure and
sinus rhythm. N Engl J Med, 366(20), 1859-1869. doi:10.1056/NEJMoa1202299
Hornig, C. R., Dorndorf, W., & Agnoli, A. L. (1986). Hemorrhagic cerebral infarction--a
prospective study. Stroke, 17(2), 179-185.
Hovens, M. M., Snoep, J. D., Eikenboom, J. C., van der Bom, J. G., Mertens, B. J., & Huisman,
M. V. (2007). Prevalence of persistent platelet reactivity despite use of aspirin: a
systematic review. Am Heart J, 153(2), 175-181. doi:10.1016/j.ahj.2006.10.040
Hutchinson, M. L., & Beslow, L. A. (2019). Hemorrhagic Transformation of Arterial Ischemic
and Venous Stroke in Children. Pediatr Neurol, 95, 26-33.
doi:10.1016/j.pediatrneurol.2019.01.023
Irvine, B., Luo, W., & Leon, J. A. (2015). Congenital anomalies in Canada 2013: a perinatal
health surveillance report by the Public Health Agency of Canada's Canadian Perinatal
Surveillance System. Health Promot Chronic Dis Prev Can, 35(1), 21-22.
Kablau, M., Kreisel, S. H., Sauer, T., Binder, J., Szabo, K., Hennerici, M. G., & Kern, R. (2011).
Predictors and early outcome of hemorrhagic transformation after acute ischemic stroke.
Cerebrovasc Dis, 32(4), 334-341. doi:10.1159/000331702
Kent, D. M., Ruthazer, R., Weimar, C., Mas, J. L., Serena, J., Homma, S., . . . Thaler, D. E.
(2013). An index to identify stroke-related vs incidental patent foramen ovale in
cryptogenic stroke. Neurology, 81(7), 619-625. doi:10.1212/WNL.0b013e3182a08d59

Pulcine 98
Khatri, P., Wechsler, L. R., & Broderick, J. P. (2007). Intracranial hemorrhage associated with
revascularization therapies. Stroke, 38(2), 431-440.
doi:10.1161/01.STR.0000254524.23708.c9
Kirsh, J. A., Walsh, E. P., & Triedman, J. K. (2002). Prevalence of and risk factors for atrial
fibrillation and intra-atrial reentrant tachycardia among patients with congenital heart
disease. Am J Cardiol, 90(3), 338-340.
Kirton, A., & deVeber, G. (2015). Paediatric stroke: pressing issues and promising directions.
Lancet Neurol, 14(1), 92-102. doi:10.1016/S1474-4422(14)70227-3
Kitchen, L., Westmacott, R., Friefeld, S., MacGregor, D., Curtis, R., Allen, A., . . . deVeber, G.
(2012). The pediatric stroke outcome measure: a validation and reliability study. Stroke,
43(6), 1602-1608. doi:10.1161/STROKEAHA.111.639583
Kmietowicz, Z. (2017). Guidelines aim to help identify and treat stroke in children. BMJ, 357,
j2521. doi:10.1136/bmj.j2521
Kuhle, S., Eulmesekian, P., Kavanagh, B., Massicotte, P., Vegh, P., & Mitchell, L. G. (2007). A
clinically significant incidence of bleeding in critically ill children receiving therapeutic
doses of unfractionated heparin: a prospective cohort study. Haematologica, 92(2), 244-
247. doi:10.3324/haematol.10616
Leijser, L. M., Chau, V., Seed, M., Poskitt, K. J., Synnes, A., Blaser, S., . . . Miller, S. P. (2019).
Anticoagulation therapy and the risk of perioperative brain injury in neonates with
congenital heart disease. J Thorac Cardiovasc Surg. doi:10.1016/j.jtcvs.2019.02.029
Levi, M., Toh, C. H., Thachil, J., & Watson, H. G. (2009). Guidelines for the diagnosis and
management of disseminated intravascular coagulation. British Committee for Standards
in Haematology. Br J Haematol, 145(1), 24-33. doi:10.1111/j.1365-2141.2009.07600.x
Limperopoulos, C., Majnemer, A., Shevell, M. I., Rosenblatt, B., Rohlicek, C., Tchervenkov, C.,
& Darwish, H. Z. (2001). Functional limitations in young children with congenital heart
defects after cardiac surgery. Pediatrics, 108(6), 1325-1331.
doi:10.1542/peds.108.6.1325
Liu, X. Y., Wong, V., & Leung, M. (2001). Neurologic complications due to catheterization.
Pediatr Neurol, 24(4), 270-275.
Lodder, J., Krijne-Kubat, B., & Broekman, J. (1986). Cerebral hemorrhagic infarction at
autopsy: cardiac embolic cause and the relationship to the cause of death. Stroke, 17(4),
626-629.
Mackay, M. T., Wiznitzer, M., Benedict, S. L., Lee, K. J., Deveber, G. A., Ganesan, V., &
International Pediatric Stroke Study, Group. (2011). Arterial ischemic stroke risk factors:
the International Pediatric Stroke Study. Ann Neurol, 69(1), 130-140.
doi:10.1002/ana.22224
Mallick, A. A., Ganesan, V., Kirkham, F. J., Fallon, P., Hedderly, T., McShane, T., . . .
O'Callaghan, F. J. (2014). Childhood arterial ischaemic stroke incidence, presenting
features, and risk factors: a prospective population-based study. Lancet Neurol, 13(1), 35-
43. doi:10.1016/S1474-4422(13)70290-4
Manlhiot, C., Brandao, L. R., Kwok, J., Kegel, S., Menjak, I. B., Carew, C. L., . . . McCrindle, B.
W. (2012). Thrombotic complications and thromboprophylaxis across all three stages of
single ventricle heart palliation. J Pediatr, 161(3), 513-519 e513.
doi:10.1016/j.jpeds.2012.03.004
Manlhiot, C., Brandao, L. R., Somji, Z., Chesney, A. L., MacDonald, C., Gurofsky, R. C., . . .
McCrindle, B. W. (2010). Long-term anticoagulation in Kawasaki disease: Initial use of

Pulcine 99
low molecular weight heparin is a viable option for patients with severe coronary artery
abnormalities. Pediatr Cardiol, 31(6), 834-842. doi:10.1007/s00246-010-9715-8
Manlhiot, C., Menjak, I. B., Brandao, L. R., Gruenwald, C. E., Schwartz, S. M., Sivarajan, V. B.,
. . . McCrindle, B. W. (2011). Risk, clinical features, and outcomes of thrombosis
associated with pediatric cardiac surgery. Circulation, 124(14), 1511-1519.
doi:10.1161/CIRCULATIONAHA.110.006304
Marsh, E. B., Llinas, R. H., Hillis, A. E., & Gottesman, R. F. (2013). Hemorrhagic
transformation in patients with acute ischaemic stroke and an indication for
anticoagulation. Eur J Neurol, 20(6), 962-967. doi:10.1111/ene.12126
Marsh, E. B., Llinas, R. H., Schneider, A. L., Hillis, A. E., Lawrence, E., Dziedzic, P., &
Gottesman, R. F. (2016). Predicting Hemorrhagic Transformation of Acute Ischemic
Stroke: Prospective Validation of the HeRS Score. Medicine (Baltimore), 95(2), e2430.
doi:10.1097/MD.0000000000002430
Martelle, R. R., & Linde, L. M. (1961). Cerebrovascular accidents with tetralogy of Fallot. Am J
Dis Child, 101, 206-209.
Massie, B. M., Collins, J. F., Ammon, S. E., Armstrong, P. W., Cleland, J. G., Ezekowitz, M., . .
. Investigators, Watch Trial. (2009). Randomized trial of warfarin, aspirin, and
clopidogrel in patients with chronic heart failure: the Warfarin and Antiplatelet Therapy
in Chronic Heart Failure (WATCH) trial. Circulation, 119(12), 1616-1624.
doi:10.1161/CIRCULATIONAHA.108.801753
McCrindle, B. W., Karamlou, T., Wong, H., Gangam, N., Trivedi, K. R., Lee, K. J., & Benson,
L. N. (2006). Presentation, management and outcomes of thrombosis for children with
cardiomyopathy. Can J Cardiol, 22(8), 685-690.
Medley, T. L., Miteff, C., Andrews, I., Ware, T., Cheung, M., Monagle, P., . . . Mackay, M. T.
(2019). Australian Clinical Consensus Guideline: The diagnosis and acute management
of childhood stroke. Int J Stroke, 14(1), 94-106. doi:10.1177/1747493018799958
Michelson, A. D. (1998). Platelet function in the newborn. Semin Thromb Hemost, 24(6), 507-
512. doi:10.1055/s-2007-996049
Michelson, A. D., & Bhatt, D. L. (2017). How I use laboratory monitoring of antiplatelet
therapy. Blood, 130(6), 713-721. doi:10.1182/blood-2017-03-742338
Michelson, A. D., Cattaneo, M., Eikelboom, J. W., Gurbel, P., Kottke-Marchant, K., Kunicki, T.
J., . . . Working Group on Aspirin, Resistance. (2005). Aspirin resistance: position paper
of the Working Group on Aspirin Resistance. J Thromb Haemost, 3(6), 1309-1311.
doi:10.1111/j.1538-7836.2005.01351.x
Miller, S. P., McQuillen, P. S., Hamrick, S., Xu, D., Glidden, D. V., Charlton, N., . . . Vigneron,
D. B. (2007). Abnormal brain development in newborns with congenital heart disease. N
Engl J Med, 357(19), 1928-1938. doi:10.1056/NEJMoa067393
Mir, A., Frank, S., Journeycake, J., Wolovitis, J., Guleserian, K., Heistein, L., & Lemler, M.
(2015). Aspirin Resistance in Single-Ventricle Physiology: Aspirin Prophylaxis Is Not
Adequate to Inhibit Platelets in the Immediate Postoperative Period. Ann Thorac Surg,
99(6), 2158-2164. doi:10.1016/j.athoracsur.2015.02.026
Monagle, P., Chan, A. K. C., Goldenberg, N. A., Ichord, R. N., Journeycake, J. M., Nowak-
Gottl, U., & Vesely, S. K. (2012). Antithrombotic therapy in neonates and children:
Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of
Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest, 141(2 Suppl),
e737S-e801S. doi:10.1378/chest.11-2308

Pulcine 100
Monagle, P., Cochrane, A., Roberts, R., Manlhiot, C., Weintraub, R., Szechtman, B., . . . Fontan
Anticoagulation Study, Group. (2011). A multicenter, randomized trial comparing
heparin/warfarin and acetylsalicylic acid as primary thromboprophylaxis for 2 years after
the Fontan procedure in children. J Am Coll Cardiol, 58(6), 645-651.
doi:10.1016/j.jacc.2011.01.061
Niwa, T., Aida, N., Shishikura, A., Fujita, K., & Inoue, T. (2008). Susceptibility-weighted
imaging findings of cortical laminar necrosis in pediatric patients. AJNR Am J
Neuroradiol, 29(9), 1795-1798. doi:10.3174/ajnr.A1184
O'Carroll, C. B., & Barrett, K. M. (2017). Cardioembolic Stroke. Continuum (Minneap Minn),
23(1, Cerebrovascular Disease), 111-132. doi:10.1212/CON.0000000000000419
Odegard, K. C., Zurakowski, D., DiNardo, J. A., Castro, R. A., McGowan, F. X., Jr., Neufeld, E.
J., & Laussen, P. C. (2009). Prospective longitudinal study of coagulation profiles in
children with hypoplastic left heart syndrome from stage I through Fontan completion. J
Thorac Cardiovasc Surg, 137(4), 934-941. doi:10.1016/j.jtcvs.2008.09.031
Orencia, A. J., Petty, G. W., Khandheria, B. K., Annegers, J. F., Ballard, D. J., Sicks, J. D., . . .
Whisnant, J. P. (1995). Risk of stroke with mitral valve prolapse in population-based
cohort study. Stroke, 26(1), 7-13.
Park, J. H., Ko, Y., Kim, W. J., Jang, M. S., Yang, M. H., Han, M. K., . . . Gorelick, P. B. (2012).
Is asymptomatic hemorrhagic transformation really innocuous? Neurology, 78(6), 421-
426. doi:10.1212/WNL.0b013e318245d22c
Petit, C. J., Rome, J. J., Wernovsky, G., Mason, S. E., Shera, D. M., Nicolson, S. C., . . . Licht,
D. J. (2009). Preoperative brain injury in transposition of the great arteries is associated
with oxygenation and time to surgery, not balloon atrial septostomy. Circulation, 119(5),
709-716. doi:10.1161/CIRCULATIONAHA.107.760819
Radford, D. J., & Izukawa, T. (1977). Atrial fibrillation in children. Pediatrics, 59(2), 250-256.
Roach, E. S., Golomb, M. R., Adams, R., Biller, J., Daniels, S., Deveber, G., . . . Council on
Cardiovascular Disease in the, Young. (2008). Management of stroke in infants and
children: a scientific statement from a Special Writing Group of the American Heart
Association Stroke Council and the Council on Cardiovascular Disease in the Young.
Stroke, 39(9), 2644-2691. doi:10.1161/STROKEAHA.108.189696
Rodan, L., McCrindle, B. W., Manlhiot, C., MacGregor, D. L., Askalan, R., Moharir, M., &
deVeber, G. (2012). Stroke recurrence in children with congenital heart disease. Ann
Neurol, 72(1), 103-111. doi:10.1002/ana.23574
Sade, R. M., Crawford, F. A., Jr., Fyfe, D. A., & Stroud, M. R. (1988). Valve prostheses in
children: a reassessment of anticoagulation. J Thorac Cardiovasc Surg, 95(4), 553-561.
Schechter, T., Kirton, A., Laughlin, S., Pontigon, A. M., Finkelstein, Y., MacGregor, D., . . .
Brandao, L. R. (2012). Safety of anticoagulants in children with arterial ischemic stroke.
Blood, 119(4), 949-956. doi:10.1182/blood-2011-06-361535
Silvey, M., & Brandao, L. R. (2017). Risk Factors, Prophylaxis, and Treatment of Venous
Thromboembolism in Congenital Heart Disease Patients. Front Pediatr, 5, 146.
doi:10.3389/fped.2017.00146
Sinclair, A. J., Fox, C. K., Ichord, R. N., Almond, C. S., Bernard, T. J., Beslow, L. A., . . .
Jordan, L. C. (2015). Stroke in children with cardiac disease: report from the
International Pediatric Stroke Study Group Symposium. Pediatr Neurol, 52(1), 5-15.
doi:10.1016/j.pediatrneurol.2014.09.016

Pulcine 101
Slim M, Dlamini N, Fox C, Friefeld S, Westmacott R, Moharir M. MacGregor D, deVeber G.
(2018). Outcome severity assessment with the pediatric stroke outcome measure
(PSOM): validation of a novel classification system. Annals of Neurology, 84(22), S406.
Snoep, J. D., Hovens, M. M., Eikenboom, J. C., van der Bom, J. G., Jukema, J. W., & Huisman,
M. V. (2007). Clopidogrel nonresponsiveness in patients undergoing percutaneous
coronary intervention with stenting: a systematic review and meta-analysis. Am Heart J,
154(2), 221-231. doi:10.1016/j.ahj.2007.04.014
Soul, J. S., Robertson, R. L., Wypij, D., Bellinger, D. C., Visconti, K. J., du Plessis, A. J., . . .
Newburger, J. W. (2009). Subtle hemorrhagic brain injury is associated with
neurodevelopmental impairment in infants with repaired congenital heart disease. J
Thorac Cardiovasc Surg, 138(2), 374-381. doi:10.1016/j.jtcvs.2009.02.027
Steiner, T., Weitz, J. I., & Veltkamp, R. (2017). Anticoagulant-Associated Intracranial
Hemorrhage in the Era of Reversal Agents. Stroke, 48(5), 1432-1437.
doi:10.1161/STROKEAHA.116.013343
Strater, R., Kurnik, K., Heller, C., Schobess, R., Luigs, P., & Nowak-Gottl, U. (2001). Aspirin
versus low-dose low-molecular-weight heparin: antithrombotic therapy in pediatric
ischemic stroke patients: a prospective follow-up study. Stroke, 32(11), 2554-2558.
Strater, R., Vielhaber, H., Kassenbohmer, R., von Kries, R., Gobel, U., & Nowak-Gottl, U.
(1999). Genetic risk factors of thrombophilia in ischaemic childhood stroke of cardiac
origin. A prospective ESPED survey. Eur J Pediatr, 158 Suppl 3, S122-125.
Streif, W., Andrew, M., Marzinotto, V., Massicotte, P., Chan, A. K., Julian, J. A., & Mitchell, L.
(1999). Analysis of warfarin therapy in pediatric patients: A prospective cohort study of
319 patients. Blood, 94(9), 3007-3014.
Tempe, D. K., & Virmani, S. (2002). Coagulation abnormalities in patients with cyanotic
congenital heart disease. J Cardiothorac Vasc Anesth, 16(6), 752-765.
doi:10.1053/jcan.2002.128436
Valentino, F., Gentile, L., Terruso, V., Mastrilli, S., Aridon, P., Ragonese, P., . . . D'Amelio, M.
(2017). Frequency and determinants for hemorrhagic transformation of posterior cerebral
stroke : Posterior ischemic stroke and hemorrhagic transformation. BMC Res Notes,
10(1), 592. doi:10.1186/s13104-017-2889-x
Waldman, J. D., Czapek, E. E., Paul, M. H., Schwartz, A. D., Levin, D. L., & Schindler, S.
(1975). Shortened platelet survival in cyanotic heart disease. J Pediatr, 87(1), 77-79.
doi:10.1016/s0022-3476(75)80073-4
Weissman, B. M., Aram, D. M., Levinsohn, M. W., & Ben-Shachar, G. (1985). Neurologic
sequelae of cardiac catheterization. Cathet Cardiovasc Diagn, 11(6), 577-583.
Wessel, D. L., Berger, F., Li, J. S., Dahnert, I., Rakhit, A., Fontecave, S., . . . Investigators,
Clarinet. (2013). Clopidogrel in infants with systemic-to-pulmonary-artery shunts. N Engl
J Med, 368(25), 2377-2384. doi:10.1056/NEJMoa1114588
Yamamoto, K., Ikeda, U., Furuhashi, K., Irokawa, M., Nakayama, T., & Shimada, K. (1995).
The coagulation system is activated in idiopathic cardiomyopathy. J Am Coll Cardiol,
25(7), 1634-1640. doi:10.1016/0735-1097(95)00049-a

Pulcine 102
Appendix – The Hospital for Sick Children Arterial Ischemic Stroke Guidelines
Stroke Guidelines: Approach to Arterial Ischemic Stroke
The Hospital for Sick Children Electronic Formulary
The following is a summary of the recommended medical management for children with acute
arterial ischemic stroke. Modifications for individual clinical circumstances may be necessary. In
any child with potential stroke, ask the following stroke screening questions:
Stroke Specific
1. Is there a persistent focal neurological deficit?
a. unilateral weakness or sensory change
b. vision loss or double vision
c. speech difficulty
d. vertigo or trouble walking
2. Did the problem begin suddenly?
tPA Specific:
3. Is the child 4 years or older?
4. Was the onset of symptoms < 6 hours ago? When was the child last seen normal?
If yes to questions 1 and 2, high likelihood of acute arterial ischemic stroke (AIS) AND if yes to
questions 3 and 4, may be a tPA candidate. Page Neurology on-call immediately and refer to
Hyperacute Arterial Ischemic Stroke Pathway, available at
http://my.sickkids.ca/care/neurology/guidelines/Stroke-Guidelines/
ACUTE NEUROPROTECTIVE CARE
To minimize extent of neuronal damage, normalize body temperature, maintain normal blood
glucose and blood pressure, and aggressively control seizures.
o Fever: Treat core temperature (PO/PR) > 37.5 °C with an antipyretic
(acetaminophen), consider cooling in select cases in PICU.
o Blood Glucose: Monitor blood glucose (lab or bedside) at minimum q 6 hours for
24 hours following acute stroke, then q 12 hours for an additional 24 hours (target 5-
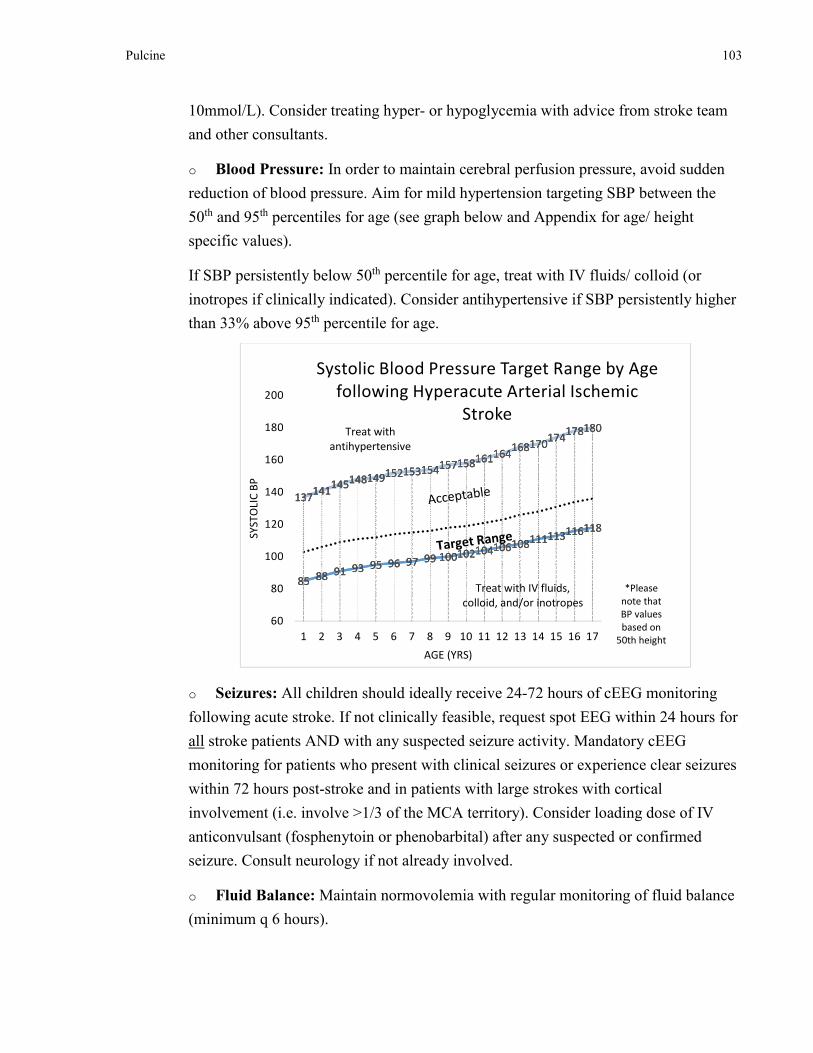
Pulcine 103
10mmol/L). Consider treating hyper- or hypoglycemia with advice from stroke team
and other consultants.
o Blood Pressure: In order to maintain cerebral perfusion pressure, avoid sudden
reduction of blood pressure. Aim for mild hypertension targeting SBP between the
50th and 95th percentiles for age (see graph below and Appendix for age/ height
specific values).
If SBP persistently below 50th percentile for age, treat with IV fluids/ colloid (or
inotropes if clinically indicated). Consider antihypertensive if SBP persistently higher
than 33% above 95th percentile for age.
o Seizures: All children should ideally receive 24-72 hours of cEEG monitoring
following acute stroke. If not clinically feasible, request spot EEG within 24 hours for
all stroke patients AND with any suspected seizure activity. Mandatory cEEG
monitoring for patients who present with clinical seizures or experience clear seizures
within 72 hours post-stroke and in patients with large strokes with cortical
involvement (i.e. involve >1/3 of the MCA territory). Consider loading dose of IV
anticonvulsant (fosphenytoin or phenobarbital) after any suspected or confirmed
seizure. Consult neurology if not already involved.
o Fluid Balance: Maintain normovolemia with regular monitoring of fluid balance
(minimum q 6 hours).
85 88 91 93 95 96 97 99 100102104106108111113116118
137141
145148149152153154157158161164168170
174178180
85 88 91 93 95 96 97 99 100102104106108111113116118
137141
145148149152153154157158161164168170
174178180
60
80
100
120
140
160
180
200
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17
SY
ST
OLI
C B
P
AGE (YRS)
Systolic Blood Pressure Target Range by Age
following Hyperacute Arterial Ischemic
StrokeTreat with
antihypertensive
Treat with IV fluids,
colloid, and/or inotropes
*Please
note that
BP values
based on
50th height

Pulcine 104
o Head of Bed Flat: Keep head of the bed flat for 72 hours following acute stroke
if tolerated by the patient and there are no signs of raised intracranial pressure.
Otherwise, keep head of the bed at 30 degrees.
ACUTE AND PREVENTATIVE ANTITHROMBOTIC MEDICATIONS
A. GENERAL GUIDELINES
o Acute Thrombolysis: If patient 4 years of age or older, neurological deficit
began < 6 hours from arrival to SickKids, and deficit is persisting, either intra-
venous (within 0-4.5 hrs) or intra-arterial (4.5-6 hrs) tPA could be feasible based
on joint decision by the Stroke Team, Thrombosis, Neuroradiology, PICU, IGT,
and MRP. See section on Alteplase below and refer to Hyperacute Arterial
Ischemic Stroke Pathway, available at
http://my.sickkids.ca/care/neurology/guidelines/Stroke-Guidelines/
o Anticoagulant Therapy (ACT): Contact Thrombosis for dosing and monitoring.
Refer to detailed protocols for unfractionated heparin (UFH), low molecular
weight heparin (LMWH), and warfarin for required baseline bloodwork (i.e.
CBC, INR, aPTT, INR, Fibrinogen, D-Dimer) and laboratory monitoring
guidelines.
• Neonates with AIS: No anticoagulant treatment is usually required due to
negligible risk of recurrent stroke. Exceptions: congenital heart disease,
concurrent systemic thrombosis, confirmed recurrent AIS, radiologically
proven occlusion of intracranial and/or neck arteries with intact brain
distal to the occlusion, proven prothrombotic disorder.
• Older infants and children (>1 mo age) with new/acute AIS: General
practice is to anticoagulate initially for 5-7days, unless there are
contraindications.
• Monitoring during ACT: For all children with arterial stroke who are
initiated on anticoagulation, an MRI (or CT scan without contrast as
second choice) should be obtained on day 4 (3-5) of therapy to assess for
sub-clinical intracranial hemorrhage and to rule out further accumulation
of infarcts despite treatment. In infants under one year of age, serial head
circumference and hemoglobin level (daily at minimum) are suggested to
screen for asymptomatic intracranial hemorrhage in addition to day 4
MRI.

Pulcine 105
o Secondary preventative therapy:
• Neonates rarely require secondary prevention therapy. Exception:
neonates with BOTH a prothrombotic risk factor and echo showing
persistent intracardiac defect with potential right to left shunt (i.e.
persistent PFO) may be treated with ASA for prevention.
• Since older infants and children have approximately 20% risk of stroke
recurrence (50% if no antithrombotic treatment, 66% if there is an
arteriopathy), long-term secondary preventative therapy is needed (i.e.
minimum duration of 2 years, typically indefinite). This usually consists of
ASA. Clopidogrel is an alternative for single agent therapy if there is ASA
intolerance or treatment failure with ASA. Circumstances may dictate
prolonged anticoagulation (i.e. several months to several years) with
LMWH or warfarin, such as with severe prothrombotic disorders, cardiac
disease, or dissection, (see: "AIS Flow Chart").
B. SPECIFIC ANTITHROMBOTIC MEDICATIONS
Thrombolytics
o Alteplase (tPA): Only used in carefully defined specific stroke situations within
4.5 hours of documented stroke onset (for intravenous route) or 6 hours (for intra-
arterial route) in children >4 years with a persistent, severe neurological deficit
and no contra-indications. Due to major potential risks, this medication should
only be given for hyperacute arterial ischemic stroke after consultation with
Stroke Team, Thrombosis, and Neurology.
Intravenous (IV) dosing:
Age < 12 years: 0.75 mg/kg (10% as bolus dose over 5 minutes, 90% as
infusion over 1 hour)
Maximum dose: 75 mg
Age > 12 years: 0.9 mg/kg (10% as bolus dose over 5 minutes, 90% as
infusion over 1 hour)
Maximum dose: 90 mg
Refer to Hyperacute Arterial Ischemic Stroke Pathway, available at
http://my.sickkids.ca/care/neurology/guidelines/Stroke-Guidelines/.

Pulcine 106
Anticoagulants
o Unfractionated (standard) Heparin: No loading dose, otherwise follow
guidelines
o Low Molecular Weight Heparin: Follow guidelines for treatment dosing
o Warfarin: Follow guidelines
Antiplatelets
o ASA: 3-5 mg/kg/day (taken daily or 3 times/week). Round dose to nearest
quarter-tablet (20 mg). Maximum dose: 325 mg/day.
Reye’s syndrome is not reported at this dose. Annual influenza immunization is
recommended in all children.
For Lumbar Puncture, Dental Extraction, or other invasive procedures, temporary
cessation (i.e. 5-7 days) of therapy prior to procedure may be required. Consult
Stroke Team and Thrombosis to assess risk for recurrent stroke while off ASA for
individual child. Bridging to heparin for the duration off ASA may be required.
Consider reducing ASA dose to 1-3 mg/kg/day or switching to an alternative
agent if there are adverse side effects on ASA.
o Clopidogrel (Plavix®): 1 mg/kg/day PO daily. Maximum dose: 75 mg/day
Clopidogrel is an alternative for single agent therapy if there is ASA intolerance
or treatment failure. Note that combination therapy with multiple anti-platelet
agents (i.e. ASA and Clopidogrel) is relatively contraindicated given recent
evidence of increased bleeding risk in children and adults with stroke.
APPROACH TO STROKE VARIANTS
The following is a brief summary of additional treatment approaches for several types of acute
AIS:

Pulcine 107
Type of
Cerebral
Arterial
Infarct
Additional Comments
With
Congenital
Heart Disease
(CHD)
ACT depends on the circumstance underlying cardiac anatomy and case
discussion among Cardiology, Thrombosis, and Stroke.
Given recurrence risk is14% in newborns and children with CHD (including
some with full cardiac correction), indefinite treatment with an anticoagulant
or antiplatelet agent is usually advisable.
With CNS
Vasculitis
Immunosuppressive medications may be indicated in addition to
antithrombotic treatment. Stroke Team and Rheumatology to guide decision-
making.
With
Moyamoya
Disease/
Syndrome
Refer to Moyamoya guidelines available at:
http://my.sickkids.ca/care/neurology/guidelines/Stroke-Guidelines/
Antiplatelet therapy is usually recommended over anticoagulation therapy.
Surgical revascularization is frequently required (consult vascular
neurosurgery).
Specialized neuro-imaging (usually annual MRI/MRA + Cerebrovascular
Reactivity study) and neuropsychological assessment via Stroke Team.
With
Prothrombotic
Disorders
Assess for persistence of abnormal clotting factors or circulating
anticoagulant at 3-6 months, and/or investigate family members. Thrombosis
Service to advise.

Pulcine 108
Type of
Cerebral
Arterial
Infarct
Additional Comments
Transient
Ischemic Attack
(TIA)
Definition: A transient episode of neurological dysfunction caused by focal
brain, spinal cord, or retinal ischemia without acute infarction. In suspected or
confirmed initial TIA, ASA therapy may be recommended until investigations
completed, provided there are no intracranial or systemic contraindications for
ASA and intracranial bleeding has been ruled out.
With Sickle
Cell Disease
(SCD)
Stroke is one of the major complications of SCD. Review of initial
neuroimaging should include careful screening of MRA for vasculopathies
(i.e. aneurysms, Moyamoya) that could affect treatment decisions.
Acute management of ischemic stroke resulting from SCD should include
optimal hydration, correction of hypoxemia, and correction of systemic
hypotension.
For acute ischemic stroke resulting from SCD, exchange transfusion to reduce
sickle hemoglobin to <30% total hemoglobin should be considered in
consultation with haematology team.
Refer to Sickle Cell guidelines
Although there is no evidence to support its efficacy, prescribing ASA at a
dose of 3-5 mg/kg (max dose 81 mg) in the absence of contraindications may
be reasonable to consider for a patient with SCD who accumulates white
matter infarcts on optimal SCD management or if there are reasons preventing
optimal SCD management.

Pulcine 109
EXTERNAL GUIDELINES FOR REFERENCE
The Canadian Best Practice Guidelines for Stroke Care 2010 now include paediatric guidelines
and are available online at http://www.strokebestpractices.ca/
The American Heart Association guidelines for the management of infants and children with
stroke (2012) can be found at http://stroke.ahajournals.org/content/39/9/2644.full.pdf
The Chest Guideline for Antithrombotic Therapy and the prevention of thrombosis (2012) are
available online at
http://journal.publications.chestnet.org/issue.aspx?journalid=99&issueid=23443

Pulcine 110