
The quest for the holy grail—lva ds as bridge to recovery
19
Myocardial Remodeling with Continuous-Flow LVADs Amrut V. Ambardekar, MD, FACC University of Colorado
-
Upload
drucsamal -
Category
Healthcare
-
view
150 -
download
1
Transcript of The quest for the holy grail—lva ds as bridge to recovery

Myocardial Remodeling with Continuous-Flow LVADs
Amrut V. Ambardekar, MD, FACC
University of Colorado

The Quest for the Holy Grail—LVADs as Bridge to Recovery “Choose Poorly”
LVAD Explant for Remodeling alone without Recovery
Patient develops recurrent HF
“Choose Wisely” LVAD Explant for
Remodeling and Recovery
Pt free of HF, without LVAD or transplant
“You must choose…” 22yo man s/p CF-LVAD 4 months ago for new HF, EF 10%, and shock. Now
has with LVEF 45%.

Review of the Journey Towards the Holy Grail
• What is LVAD related myocardial remodeling: organ level vs. cellular level?
• Does myocardial remodeling equate to recovery (i.e.. LVAD explant) in clinical
practice?
• What are the obstacles in the path towards the holy grail of full recovery?
– Incomplete cellular and molecular recovery
– Differences between pulsatile vs continuous unloading
– Possibilities of functional atrophy
• What further questions need answers to move us along
the correct pathway?

Theoretical Rationale for LVAD Induced
Remodeling
• Excess pressure/volume loading of the myocardium is an established stimulus for HF
– Examples: Valvular disease, Hypertension
• LVADs dramatically unload the LV and remove this stimulus
– Mechanical unloading results in normalization of abnormal filling pressures
• LVADs allow for complete restoration of cardiac output
– Improvement in end-organ perfusion decreases stimulus for neurohormonal activation
– Breaks the vicious cycle: ↓cardiac function↑compensatory neurohormones↓cardiac
function
– Hemodynamic stability to add neurohormonal antagonists

Remodeling at the Organ Level
Ambardekar et al. Circ HF. 2011; 4:425.
• Normalization of hemodynamics
after LVAD
• LV changes after LVAD
• Decreased chamber size
• Decreased hypertrophy and mass
• Improved ejection fraction
• This reversal of the seemingly
irreversible failing LV phenotype is
termed “Reverse Remodeling”

Remodeling at the Cellular Level
Ambardekar et al. Circ HF. 2011; 4:425.
• Pathological hypertrophy is a
hallmark feature of the failing
myocyte
• Numerous studies have suggested
that LVAD support helps myocytes
regress toward dimensions of
nonfailing myocytes
• Overt structural atrophy has not
been found

Early success in the Quest for the Holy Grail
• 15 patients with nonischemic cardiomyopathy treated with a combination of LVAD followed by conventional HF medical therapy (ACE, β-blocker, spironolactone, ARB) and then the selective β2 adrenergic receptor agonist clenbuterol.
• 11 had successful LVAD explant
• Survival free of HF was 100% at 1 year and 88.9% at 4 years
Birks et al. NEJM. 2006; 355: 1873-84.

Subsequent Crusades with Variable Results
Drakos et al. Circ. 2012; 126:230-241.

If you are not searching for grail, you won’t find it…
Sixth INTERMACS Report. JHLT. 2014; 33:555-564.

Summary of Clinical Recovery/LVAD Explant Data • Rates of LV recovery are highly variable
• LVAD alone likely not sufficient for recovery
• Adjunct therapies are needed, but unclear role of individual agents
• Role of atrophy and methods to combat atrophy not defined
• Differences between those who recover vs. those that don’t
• Younger age
• Shorter HF duration
• Is the lack of prior exposure to β-blockade the key to recovery?
• Systematic protocols to monitor and assess for recovery needed
• May partly explain low rates of recovery in INTERMACS Registry
• If you don’t look for something, you can’t find it…

Cellular & Molecular Mechanisms for Remodeling
• Bridge to transplant LVAD placement allows collection of discard tissue for cellular and
molecular analysis
• LV apical core removed for insertion of LVAD inflow cannula
• Entire heart removed at time of cardiac transplantation
• Paired comparisons from the same patient before/after LVAD allows for some control of
multiple variables that come from human samples
• Comparisons of different diseases (ischemic CM vs. familial)
• Medication differences may be a confounding variable
• Numerous studies have investigated mechanism of remodeling

Incomplete Recovery of Myocyte Contractility
Ambardekar et al. Circ HF. 2011; 4:425.
• In vitro assessments of contractility
have suggested that there is an
improvement in myocyte force with
LVAD support.
• Myocytes from LVAD supported
patients:
• Greater magnitude of shortening
• Faster time to peak contraction
• Faster time to shortening
• Improvements ≠ normalization
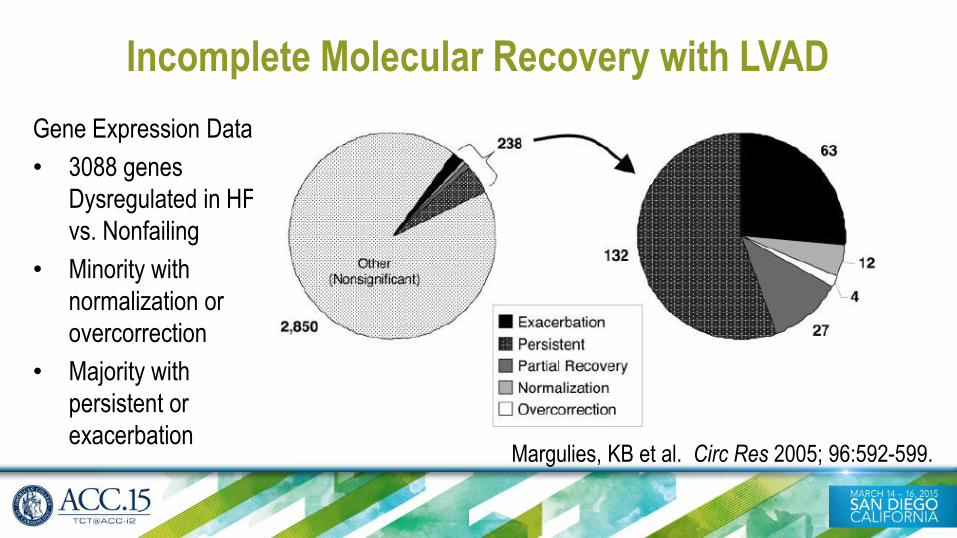
Incomplete Molecular Recovery with LVAD
Margulies, KB et al. Circ Res 2005; 96:592-599.
Gene Expression Data
• 3088 genes
Dysregulated in HF
vs. Nonfailing
• Minority with
normalization or
overcorrection
• Majority with
persistent or
exacerbation

Remodeling ≠ Recovery: Elastic vs. Plastic Deformation
Mann et al. JACC. 2012; 60:2465-72. Capable of Remodeling
(but Not Recovery)
Capable of Remodeling
and Recovery

Greater Unloading with Pulsatile vs. Continuous LVADs
• Retrospective analysis of 31 pulsatile vs. 30 continuous flow
LVADs from Columbia
• Higher EF, smaller LV dimensions, and lower LV pressure by
echocardiography in pulsatile flow LVAD group
• Lower serum BNP and extracellular matrix biomarkers in pulsatile
group
• Is pulsatile unloading need to foster recovery?
Kato et al. Circ HF. 2011;4:546.

Potential Negative Consequences of Mechanical Unloading:
(Pulsatile) LVAD Working Group Data
• One third of patients had an improvement in EF to >40% with LVAD support by 30 days
• Prolonged LVAD support to 120 days resulted in declining EF that approached values before LVAD support.
• LV Mass decreased by 30 days and stabilized thereafter
Maybaum Circ. 2007; 115: 2497-2505.
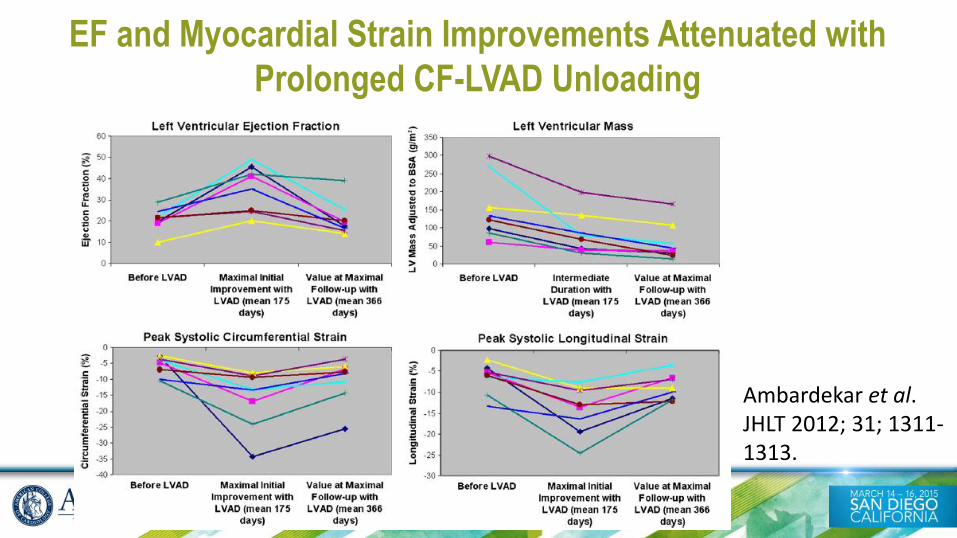
EF and Myocardial Strain Improvements Attenuated with
Prolonged CF-LVAD Unloading
Ambardekar et al. JHLT 2012; 31; 1311-1313.

Unanswered questions in the quest for the Holy Grail
• Dosage of Unloading?
– Type of unloading: pulsatile vs. continuous, full vs. partial
– Duration of unloading: daytime only vs 24/7, total duration, weaning
• Adjuvant therapy?
– Neurohormonal antagonists, anti-atrophy agents, cell or gene based therapies
• Optimal strategy for in vivo assessment of recovery?
– How long do you turn down an LVAD
• Prediction of who will have sustained recovery?
– Etiology of cardiomyopathy (ischemic vs. genetic vs. idiopathic), duration of HF
• Non-cardiac effects of LVADs which may impede recovery?

Conclusions • Heart failure has been conceptualized as an end-stage disease,
however many physiological parameters can improve and even normalize with LVAD therapy.
• LVAD implantation allows for both mechanical unloading as well as positively impacting systemic and biochemical responses that might ultimately recover LV contractile performance.
• Such changes can be observed clinically but also extend to the most basic aspects of genetic regulation and involve a complex, interconnected cascade of changes.
• BTT LVADs allow for unique access to tissue to better define the cellular and molecular mechanisms behind unloading and heart failure as a whole.
• Many crusades lay ahead, but the holy grail (LV Recovery) is worth pursuing…


















