The Potential Impact of Health Care Reform on California: Consumer Affordability
10
www.healthpolicy.ucla.edu The Potential Impact of Health Care Reform on California: Consumer Affordability Dylan H. Roby, Ph.D. Assistant Professor of Health Services, UCLA School of Public Health Research Scientist, UCLA Center for Health Policy Research This project is supported by
-
Upload
shoshana-klein -
Category
Documents
-
view
24 -
download
1
description
Dylan H. Roby, Ph.D. Assistant Professor of Health Services, UCLA School of Public Health Research Scientist, UCLA Center for Health Policy Research This project is supported by. The Potential Impact of Health Care Reform on California: Consumer Affordability. - PowerPoint PPT Presentation
Transcript of The Potential Impact of Health Care Reform on California: Consumer Affordability

www.healthpolicy.ucla.edu
The Potential Impact of Health Care Reform on California:
Consumer Affordability
Dylan H. Roby, Ph.D.
Assistant Professor of Health Services, UCLA School of Public HealthResearch Scientist, UCLA Center for Health Policy Research
This project is supported by

Patient Protection and Affordable Care Act (HR 3590)“The Senate Bill”
Subsidies in the Health Insurance Exchange (100%-400% of FPL)
Premium Credits
• Available if you are:
• 1) not offered Employer-Based coverage;
• 2) offered Employer-Based coverage with a low actuarial value (less than 60%) or would spend 9.8% of income on the employer-based premiums.
Cost Sharing Credits
• Based on increasing actuarial value of purchased policies
Out-of-Pocket Spending Maximums (based on income)
• For example, 100-200% of FPL ($1,983 single / $3,967 family)

Affordable Health Care for America Act (HR 3962)“The House Bill”
Subsidies in the Health Insurance Exchange (133%-400% of FPL)
Premium Credits
• Available if you are:
• 1) not offered Employer-Based coverage;
• 2) previously a CHIP enrollee (>150% of FPL)
Cost Sharing Credits
• Based on increasing actuarial value of purchased policies
Out-of-Pocket Spending Maximums (based on income)
• For example, 100-200% of FPL ($500 single / $1,000 family)
• Maximum amount of $5,000/$10,000 over 350% of FPL

Comparison of Individual Market Premium Spending: National vs. Western U.S.
Source: Analysis of Medical Expenditure Panel Survey

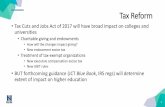
Premium Subsidy Thresholds versus Current Spending in the Individual Market
Source: Analysis of Medical Expenditure Panel Survey

Who Would Benefit from the Premium Subsidies?
Based on the median, it does not look like higher-income families would benefit from the subsidies.
However, the distribution of spending throughout the population tells us otherwise:
In the Senate bill, an individual or family can opt-out due to financial constraints if premiums are greater than 8% of their income.
In the House bill, the opt-out threshold is 12% of income
Potential Financial Opt-Out Rate for incomes over 400% of FPL: Senate (14%) and House (5%)
201 to 250%
251 to 300%
301 to 350%
351 to 400%
SenatePremium 61.7% 34.2% 10.9% 29.5%Out-of-Pocket Max 32.3% 7.0% 13.1% 8.4%HousePremium 57.4% 24.4% 10.9% 22.4%Out-of-Pocket Max 39.0% 7.0% 10.1% 3.7%

Concerns with the Affordability Provisions
There are currently 706,000 uninsured individuals in California with incomes over 400% of FPL
If 5% opted out due to the House provisions – 35,000 uninsured
If 14% opted out due to the Senate provisions – 99,000 uninsured
About 7% of employer-based households (300-400% of FPL) pay over 9.8% in their share of premiums
These estimates are based on 2007 data in 2009 dollars, given the increases we are seeing in the uninsured and insurance premiums, we could be underestimating the necessity for affordability protections for higher income groups
In combination, premium subsidies, cost sharing, and out-of-pocket limits may protect many from high health care costs.
However, many families will still face significant costs that they cannot afford:
UC Berkeley Labor Center Spending Calculator:
http://laborcenter.berkeley.edu/healthpolicy/index.shtml#calculator

The Future State of California (under health care reform)
Expansion of Medi-Cal Coverage
Close to 2 million Californians could be added to Medi-Cal
Under the House bill, CHIP kids would be added as well unless they opt into the Exchange
Although affordability is protected for this group, the ability for Medi-Cal beneficiaries to access primary care providers is not yet clear
The House bill calls for Medi-Cal fees to equal Medicare rates
Under the Senate bill, additional FMAP may not be enough to increase fee schedule and guarantee access
Existing Medi-Cal HMOs may be able to fill needs using their existing networks of private physicians
Community Health Center investment in both bills
Children in third grade will find the words “Actuarial Value” and “Silver Plan” on their vocabulary quizzes

The Future State of California, Continued
Potential for Basic Health Plan development (Senate Bill)
California will be especially skilled at delivering this type of care due to Health Care Coverage Initiatives and existing local plans
If state chooses this model for 133-200% of FPL group, those individuals would not be eligible for subsidies in the Exchange
State flexibility
In 2007 reform effort, there was exploration of using subsidies up to 600% of FPL – is that necessary in CA?
Will California be able to use CMS waivers and waivers to the national plan to expand coverage and fill in the gaps?
What will happen to Share of Cost beneficiaries?
Could states opt for more generous protections that might need less monitoring (SCHIP approach)?

Closing Thoughts
If the Senate bill is passed by the House, the affordability protections are solid, but could improve
Californians will be more likely to hit the financial opt-out thresholds than people in other states
Three times as many Californians would qualify in the Senate bill when compared to the House bill – Opportunity for Reconciliation
Although this reform was not designed specifically for California, it would certainly help many low-income Californians (<133% of FPL)
It would provide better transparency and regulation in the health insurance market, that could enable consumers
Risk of starting from scratch on these complex issues
These premium and cost-sharing subsidies and OOP maximums were designed fairly well, and starting from scratch and keeping it simple is a risk