The Planning Process - ontla.on.ca · Alice’s Adventures in Wonderland. ... because any or all of...
46
Information Management A System We Can Count On The Health Planner’s Toolkit Health System Intelligence Project – 2006 The Planning Process MODULE 1
Transcript of The Planning Process - ontla.on.ca · Alice’s Adventures in Wonderland. ... because any or all of...

Information Management
A System We Can Count On
The Health Planner’s ToolkitHealth System Intelligence Project – 2006
The Planning Process
MODULE
1

Introduction: Which Way To Go? . . . . . . . . . . . . . . . iii
This Module’s Purpose And Summary . . . . . . . . . . . iv
Section 1
What Is Health Planning? . . . . . . . . . . . . . . . . . . . . . . 1
1.1 Who Does Health Planning? . . . . . . . . . . . . . . . . . . 1
1.2 What Is Health Planning’s Main Deliverable? . . . . 1
1.3 What Are The Steps In A Health Planning Process? . . . . . . . . . . . . . . . . . . . . . . . . . . 2
1.4 Turning Plans Into Actions . . . . . . . . . . . . . . . . . . . 3
Section 2
What Are The Types Of Health Planning? . . . . . . . . 5
2.1 Health System Planning . . . . . . . . . . . . . . . . . . . . . 5
2.2 Health Services Planning . . . . . . . . . . . . . . . . . . . . 6
2.3 Health Goals Planning. . . . . . . . . . . . . . . . . . . . . . . 7
2.4 Population Health Planning . . . . . . . . . . . . . . . . . . 7
Section 3
What Are Critical Success Factors In
A Health Planning Process? . . . . . . . . . . . . . . . . . . . . 9
3.1 Defining The Right Question . . . . . . . . . . . . . . . . . 9
3.2 Choosing The Process Relevant to The Task . . . . 9
3.3 Engaging Stakeholders . . . . . . . . . . . . . . . . . . . . . 10
3.4 Establishing Effective Project Management . . . . 10
3.5 Planning Within An Ethical Framework . . . . . . . 10
3.6 Accessing and Applying Relevant Information . . 11
3.7 A Commitment to Monitoring and Evaluation . . 13
Section 4
What Is Strategic Planning Versus
Operational Planning? . . . . . . . . . . . . . . . . . . . . . . . . 15
4.1 Strategic Planning . . . . . . . . . . . . . . . . . . . . . . . . . 15
4.1.1 Strategic Planning Process Components . . . . . 16
4.2 Operational Planning. . . . . . . . . . . . . . . . . . . . . . . 17
Section 5
Other Useful Information . . . . . . . . . . . . . . . . . . . . . 19
5.1 Comprehensive Planning Process Versus Hurry Up and Go! . . . . . . . . . . . . . . . . . . . 19
5.2 Use of Advocacy Groups . . . . . . . . . . . . . . . . . . . 19
5.3 Planning Versus Action – Selling the Process . . . 19
Section 6
Summary: Keep The Goal in Sight . . . . . . . . . . . . . 21
Bibliography . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23
Appendix A
Public Health Goals For Canada . . . . . . . . . . . . . . . 24
Appendix B
Healthy People 2010 Toolkit . . . . . . . . . . . . . . . . . . 25
Appendix C
Health Impact Assessment . . . . . . . . . . . . . . . . . . . . 28
Appendix D
Needs Impact Based Planning Model . . . . . . . . . . . 30
Appendix E
The Oregon Experience . . . . . . . . . . . . . . . . . . . . . . . 31
Appendix F
The Balanced Scorecard . . . . . . . . . . . . . . . . . . . . . . 32
Appendix G
Strategic Planning Concepts and Tools . . . . . . . . . 33
Appendix H
Operational Planning Concepts and Tools . . . . . . 35
Appendix I
Evaluation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 38
Page i
Table of Contents

Health System Intelligence Project (HSIP)
The Health Planning Toolkit is produced by the HealthSystem Intelligence Project. HSIP consists of a team ofhealth system experts retained by the Ministry of Healthand Long-Term Care’s Health Results Team forInformation Management (HRT-IM) to provide the LocalHealth Integration Networks (LHINs) with:
• Sophisticated data analysis
• Interpretation of results
• Orientation of new staff to health system data analysisissues
• Training on new techniques and technologiespertaining to health system analysis and planning.
The Health Results Team for Information Managementcreated the Health System Intelligence Project tocomplement and augment the existing analytical andplanning capacity within the Ministry of Health andLong-Term Care. The project team is working in concertwith Ministry analysts to ensure that the LHINs areprovided with analytic supports they need for their localhealth system planning activities.
Report Authors
Sten Ardal
John Butler
Rick Edwards
Lynne Lawrie (Module 1 Lead Author)
Acknowledgements
Ann-Marie Marcolin, Manager, Community andCorporate Information, St. Joseph's Health Centre,Toronto
Page ii
About HSIP

Maria is a health planner. Her agency has decided thatit’s time to re-evaluate its role within the health system.
The organisation’s board and CEO support anexamination of the environment within which theorganisation operates and an assessment of its ownfuture within that environment. The outcome will be aplan for the organisation.
They have turned to Maria for advice. What kind ofplanning makes the most sense, given a tight time framefor looking into the future? Should the agency conductits planning within a broader framework? Does thisframework exist? If not, should the organisation delayits own planning until a broader plan is in place? Whatvalues will drive the planning? What should be the roleof its partner agencies and its funders in theorganisation’s planning? What should be the role of itsclients? What information is available as raw materialfor planning? What data doesn’t exist but needs to begenerated? How should the planning project bemanaged?
This module is meant to provide a starter kit for Mariaas she works with the CEO and the board to turn thegeneral idea of planning into a specific actionableplanning process.
Introduction Page iii
“Common sense is the knack of seeing things as
they are, and doing things as they ought to be
done.”
– Harriet Beecher Stowe
Introduction
Which Way To Go?

Health planning comprises a range of activities thatshare the goal of improving health outcomes, orimproving the efficiency of health services provision, orboth.
Health planning occurs within the pressuredenvironment of political direction, changing publicexpectation, new information and evidence aboutoutcomes, and on occasion, media headlines. A solidand well-designed health planning process will beresilient enough to accommodate these pressures and touse them as levers to go forward to dialogue andsolutions for improved health care provision and healthoutcomes in the population.
This module lays out the four types of health planning:
• health system planning
• health services planning
• health goals planning
• and population health planning.
It also describes characteristics and uses of strategicand operational planning as well as the differencesbetween them.
There are critical success factors for every planningactivity. How these weigh in will be different for eachprocess. A list of critical success factors such asdefining the question, planning within an ethicalframework and establishing effective projectmanagement are included in this module. Other factorssuch as engaging stakeholders and use of informationare dealt with here and in separate modules to provide agreater depth of information and advice.
This module’s ideas and recommendations are designedto provide insights into the health planning challenges,processes and outcomes, and to help those who lead orparticipate in health planning activities to select theappropriate framework for their work.
Page iv Introduction
This Module’s Purpose And Summary
What Is Planning?
A plan is defined as a map, as preparation, as an arrangement. Planning defines where one wants to go, how toget there and the timetable for the journey. Planning can also identify the journey’s milestones. Completeplanning sets out indicators for tracking progress and ways to measure if the trip was worth the investment.
Charting a course, navigating and keeping a travel log are all parts of a good planning process. Broad elementsof planning are therefore:
• identifying a vision and goals
• undertaking strategic planning
• and evaluation.
“If you don’t know where you are going, any road
will get you there.”
– Lewis Carroll,
Alice’s Adventures in Wonderland

Health planning is a process to produce health. It doesthis by creating an actionable link between needs andresources. Its nature and scope will depend upon:
• the time allowable
• the number of answerable questions to beaddressed within the process “answerable questions”comprise questions that are worth asking and forwhich there is evidence to allow them to beanswered (see Module 2, Assessing Need andModule 3, Evidence-Based Planning, for insightsinto approaches and tools used in answeringquestions)
• the resources available to support the process
• the broader political and social environment.
There are three broad elements in a planning process;identifying the vision and goals, undertaking thestrategic plan, and evaluation. Planning occurs withinfour potential constraints, creating a tension in manyplanning processes – a tension between what ought to
be done and what can be done.
1.1 Who Does Health Planning?
The health planning process occurs within the healthservice sector, usually initiated by government or bodiesdelegated by government to manage health resources inan area, such as a Regional Health Authority (seeModule 2, Assessing Need, for an exploration of the“social model” for health that underlies governmentinvolvement in planning). Local Health IntegrationNetworks (LHINs) in Ontario are designated to managelocal health planning efforts.
A health planning process may also be led by serviceproviders such as mental health agencies, hospitals,public health agencies and other service providers tohelp them define future roles or immediate servicegoals. Toronto teaching hospitals are a good example ofa group that has undertaken member planning on keydelivery areas such as neurosurgery and vascular surgery.
Professional associations (nurses’ or physicians’organizations for instance) may also establish planningprocesses to address areas of interest to them. Anexample is the Canadian Medical Forum’s work onphysician supply. As well consumers, through advocacygroups, forums or other processes, promote their needsto the government and thereby seek to increase orinfluence allocation of health resources.
This module is primarily focused on the first group citedabove – governmental and local health authoritymanagement group planning.
1.2 What Is Health Planning’s Main
Deliverable?
The outcome of an effective health planning processshould be an actionable link between needs andresources.
The health planning process itself can be a deliverable.A good planning process reflects necessary perspectivesand engages key stakeholders in the development ofstrategies. Through that process, some of the initialmarketing of the changes required will be accomplished.
Section 1: What is Health Planning? Page 1
Section 1
What Is Health Planning?
Figure 1: Constraints and Opportunities in Planning
CONSTRAINTS
T
IME
R
ES
OU
RC
ES
NUMBER OF ANSWERABLE QUESTIONS
IDENTIFY VISION
AND GOALS
U
ND
ER
TA
KE
S
TR
AT
EG
IC P
LA
NN
ING
EV
AL
UA
TE
THE
PLANNING
CYCLE
POLITICAL AND SOCIAL ENVIRONMENT
The health planning process itself can be adeliverable.

1.3 What Are The Steps In A Health
Planning Process?
At its core, health planning follows the same basic stepsthat any planning process follows. In health planningthese steps constitute a cycle that is normally repeated interms of planning for programs, systems, populations orhealth goals. Repetition of the cycle is usually necessarybecause any or all of the following conditions prevail:
• Definitions of what constitutes “health” will change,necessitating planning to take into account the effectof the new definition on society’s health goals.
• New techniques and technologies to create, restore orsupport health emerge continually, so planning mustbe cyclical to integrate these emerging innovationsinto the planning process.
• Unforeseen health conditions emerge (a rapidlyspreading infectious disease for example), requiring anew planning cycle to factor in these conditions.
Similarly, emerging social conditions (an increase inchild poverty for example) can have implications thatrequire a new planning cycle to deal with the healtheffects of the change.
• Changed economic conditions may necessitate a newcycle of planning. If a major economic downturnoccurs, for instance, a population’s health maydecline at the same time as governments constraintheir spending on health – making a new “lean times”planning cycle necessary.
• Evaluation of the results of a planning cycle will oftenshow weak spots in the initial planning, necessitatingnew cycles to correct for past oversights andmiscalculations.
Most planning cycles (health or non-health) compriseseven basic steps that can be shown graphically. Seefigure 2
Page 2 Section 1: What is Health Planning?
1. SURVEYING THE
ENVIRONMENT
(What is)
7. EVALUATION
(Did we get from what is
to what ought to be?)
6. IMPLEMENTATION
(Putting in place the best solutions)
5. BEST SOLUTION(S)
(Preferred ways to get to what
ought to be)
2. SETTING DIRECTIONS
(What ought to be)
3. PROBLEMS and CHALLENGES
(Differences between what is
and what ought to be)
4. RANGE OF SOLUTIONS
(Ways to get from what is,
to what ought to be)
Figure 2: The Planning Cycle

Step One – Surveying the Environment:
This often involves extensive information gathering todetermine the health or illness profiles and experiencesof the population of interest. It is meant to identify thecurrent state of the issue under consideration.
Step Two – Setting Directions:
This involves setting goals and objectives, and it alsoinvolves establishing the standards against whichcurrent health/illness profiles, or current organisationalor system performance, will be compared. This step ismeant to identify the desirable future state
(expressed as outcomes if possible) for the issue underconsideration.
Step Three – Problems and Challenges:
This involves identifying and quantifying the shortfalls(if any) between what is and what ought to be.
Step Four – Range of Solutions:
This involves identifying the range of solutions to eachidentified problem or challenge. This step should alsoinclude assessing each possible solution in terms of itsfeasibility, cost and effectiveness so alternate solutionscan be compared with each other.
This step often requires significant creativity, since nooff-the-shelf solutions may be available for someproblems and challenges.
Step Five – Best Solution(s):
This step involves a choice of the solution, or set ofsolutions, that should be implemented to address theproblems or challenges identified in step three. Thechoice may need to take into account fiscal, politicaland other limitations.
Step Six – Implementation:
This step involves implementation of the chosensolutions, and often begins with development of animplementation plan.
Step Seven – Evaluation:
This step involves evaluation of the results ofimplementation to determine whether the implementedsolutions are effective in achieving their goals. It also
involves evaluating the environment to see if it haschanged, thereby rendering the solutions less effective,more effective or irrelevant. This step may begin withdevelopment of an evaluation plan well beforeevaluation actually takes place. It may also involvedevelopment of ongoing monitoring methods to be usedto continuously identify and assess the intended andunintended consequences of implementation actions.
These steps are listed as if they were purely linear steps,but feedback loops must be created between and amongthem; the complexities of the real world mean that whatseems to make sense at one step may make less sensewhen seen from the perspective of a later step.
For instance, during step two (setting directions),planners may set a target for health improvement, onlyto find in step four (range of solutions) that none of thesolutions comes anywhere near achieving the targetwithout a change in provincial policy about how aservice can be provided. The planner may thereforeneed to set a lower target (i.e., a target achievablewithin current policy), while also recommending thatprovincial policy be changed and that the target bechanged if and when policy change takes place.
1.4 Turning Plans Into Actions
Some might argue that planners are only involved in thefirst five steps:
1. surveying the environment
2. setting directions
3. identifying problems and challenges
4. identifying the range of solutions to problems andchallenges
5. identifying the preferred solution(s).
Section 1: What is Health Planning? Page 3
Planning steps may seem linear, but feedback
loops must be created between and among the
steps so planning can deal with the real world’s
complexities.
However, planners have a stake in understanding andhelping to shape implementation and evaluation, andthey may be called upon to lend a hand in both theseactivities.
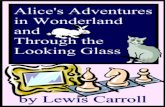
Organisational analyst Henry Mintzberg suggests thatplanning (particularly strategic planning) often failsbecause it is not allied with or embedded within thestrategic centre of an organisation (he argues thatplanning is about analysis, while strategy is aboutsynthesis).1
At the very least the planner should be aware thatwithin his/her organisation or system, planners areoften off to the side and that:
• decisions made on the basis of planning will be madenot by planners but by what Mintzberg calls thestrategic apex of the organisation or system
• the results of the planning will need to be embeddedwithin the operating core of the organisation or system.
Mintzberg’s schematic depicting organisational subunitscan be used to show the usual relationship betweenplanners and decision-makers in terms of makingplanning effective. This schematic is organisation-focused but a similar schematic could be created forsystem-level activity. See figure 3.
Page 4 Section 1: What is Health Planning?
Figure 3: The Plan-to-Action Path

Health planning includes several specific, oftenconnected, types of planning:
• health system planning. . . . . . . . . . . . . . . . . . . . . .
• health goals planning
• health services planning. . . . . . . . . . . . . . . . . . . . .
• population health planning.
The connections among the types of planning can beshown graphically (see figure 4).
Each planning type includes both strategic andoperational planning methods and approaches. Thedecision as to what planning methodology to followdepends upon the issue at hand. Data and informationare a key element to any type of planning, as arestakeholder input and consensus building (See Module2, Assessing Needs, and Module 3, Evidence-Based
Planning, for concepts related to information as rawmaterial for planning).
The following sections of this module describe the fourtypes of planning outlined above.
2.1 Health System Planning
In Canada, a recognised goal of government is to fundan efficient and well-organised health system. Thesystem itself is usually planned at the provincialgovernment level, and by provincial agents such asregional health boards. Health “system” implies:
• client access to a range of appropriate, andappropriately connected/integrated, services
• operational efficiency and a sustainable operation.
A well-organised and functioning system of healthservices is like the connectivity of the human bodysystem. Both require:
• command centres
• a supportive contextual infrastructure
• and a series of linked and inter-supporting activities.
An excellent example of how one area connects andmanages its population health goals with health servicesis the integration planning carried out by the Vancouver
Section 2: What Are The Types of Health Planning? Page 5
Section 2
What Are The Types Of Health Planning?
HEALTH SYSTEM
PLANNING
HEALTH SERVICES
PLANNING
POPULATION HEALTH PLANNING
Planning for a particular
health service
Planning for a system of
health services
Identifying desirable health
outcomes for the health
system and other systems
Planning for the
engagement of all
systems to promote health
HE
AL
TH
GO
AL
S
PL
AN
NIN
G
Figure 4: Connections Among Planning Types

Island Health authority (VIHA), show schematically inFigure 5.
There are two essential phases of health systemsplanning:
• the design and system development phase
• implementation of the system management andoperations components.
A health system cannot be achieved via a one-timeorganisation of providers. It is necessary to establishmechanisms for the ongoing running and adjustments ofthe system, just as the brain continues to regulate thefunctions of the body.
Health system or systems planning is the most complextype of health planning. It requires a clear andpolitically supported vision for the delivery model andthe support of service providers to make it happen.Health systems planning has the most potential forpayoff in improved health because it can include bothhealth services and population health within itsstrategic directions.
Alberta attempts to link these by including public healthwithin the regional health authority structure. Theprovince of Alberta Health and Wellness states that themandate of regional health authorities is to “promote
and protect the health of the population within the
region, and to work to prevent disease and injury.” 2
It further notes that the Province’s health authoritiesmust meet provincial public health targets.
2.2 Health Services Planning
Health services planning relates to a specific type ofservice or sector – mental health service delivery forexample. This type of planning can be undertaken bygovernment or devolved to providers. The Mental
Page 6 Section 2: What Are The Types of Health Planning?
Figure 5: Integration Planning, Vancouver Island Health Authority
Adapted from Vancouver Island Health Authority, Integration Plan 2007.
Health systems planning has the most potential
for payoff in improved health as it can include
both health services and population health
within its strategic directions.
Child and
Youth
Frail Elderly
Mentally Ill &
Addicted
Downtown/
Hard to Serve
Persons with
Disabilities
Chronically Ill
Aboriginal
People
Rural &
Remote
Mental Health
& Addictions
Primary
Health Care
Home &
Community CarePublic Health and Prevention
Acute & Rehab
Str
ate
gic
Co
mm
un
icati
on
s P
lan
Hu
man
Reso
urces
Pla
n
Ph
ysic
ian
Reso
urces P
lan
Info
rm
ati
on
Syste
ms P
lan
Bu
sin
ess
Develo
pm
en
t P
lan
Qu
ali
ty
Imp
ro
vem
en
t P
lan
Cap
ital
Pla
n
Q
U
A
L
I
T
Y
I
M
P
R
O
V
E
M
E
N
T

Health Implementation Task Forces convened acrossOntario in 2002/03 are a good example of taking aspecific sectoral approach to service planning. Itrepresented a combined planning effort on the part ofgovernment, providers and client advocacy groups. The Task Forces’ work was a strategic planningexercise that produced several options for systemdesign and implementation approaches.
At a different level (i.e. providers rather than funders)some providers such as community health centres andhospitals undertake health services planning related totheir particular piece of the delivery pie. In some casesthey do it with other organizations in the same field, butin many cases they do it within the context of their ownoverall budget and organisational priorities (that is,separate from a system-wide priority or role settingexercise). This planning may be an output of thestrategic directions of the organisation, but is usuallyconsidered as program or operational planning.
2.3 Health Goals Planning
Ontario’s health goals exercises in the seventies andeighties focused on several broad health goals and wereoften reflected in such initiatives as Healthy Communitiesand Healthy Cities initiatives. These had varying levels ofsuccess but were important in engaging municipalgovernment and provider groups, as well as citizens, indiscussion of the broader determinants of health.
Beginning in 2004 the federal government introduced aCanada-wide consultation process to identify healthgoals for the country, which presumably will beaddressed locally reflecting local needs andopportunities. These goals can be considered part ofany local health system planning exercise and will offera macro framework for health goals and how toestablish and report on them. Appendix A providesmore information on this process and its initial findings.
In the United States, healthy community activities haveevolved into a national umbrella focus on empoweringlocal areas to work on health goals and priorities. Anexcellent resource for health goals and priority settingand for health planning in general, can be found in the
Healthy People 2010 Tool Kit produced by the PublicHealth Foundation, Healthy People Initiative. SeeAppendix B for the initiative’s seven action areas andfor the short form of the health priorities checklistdeveloped by the initiative.
More recent groundbreaking work has been initiated inthe area of health impact assessment. A relatively newconcept in North America, it is gaining momentum as away to assess the relationship between plans for co-ordinating cities’ growth and economic strategies withopportunities to create health among citizens.
Health impact assessment is a promising butchallenging form of health planning because it requiresthe co-operation of people and institutions beyond theformal health system in determining what problemsneed to be addressed and how these problems can beaddressed, as well as implementing preferred solutions.
Appendix C provides an overview of methodology andpotential Ontario approaches in health impact assessment.
2.4 Population Health Planning
The World Health Organization’s definition of health isrelevant to all health planning, but particularlyunderlines the population health approach.
Ottawa Charter3 – In the wake of the Charter'sadoption, a new approach to improving and promotingpublic health was developed: Settings for Health. Thisapproach emphasises practical networks and projects tocreate healthy environments such as healthy schools,health-promoting hospitals, healthy workplaces andhealthy cities4. Settings for Health builds on thepremise that there is health development potential inpractically every organisation and community. Thismessage again relates to healthy communities initiativesand enlarges the circle of partners working to improvehealth status among the overall population of a givenarea. Tackling broader determinants of health andmoving away from the idea that health services alonecan produce the desired improvement in health of thepopulation is key to understanding health goals andpopulation health processes.
Section 2: What Are The Types of Health Planning? Page 7

The population health concept is commonly used as atool for public health (whose focus in Ontario hasshifted away from one-on-one care to more broadeducation and health surveillance activities) and forothers interested in health promotion activities.Population health starts from the premise ofunderstanding and then improving the health status of aparticular population or the population of a communityas a whole.
Strategic planning for population health usually focuseson macro issue identification and related strategydevelopment. The federal government uses healthstatus information to prioritise and target interventions(e.g. teenage smokers) and to develop strategies forbroad proactive public awareness (e.g. social marketingcampaigns about lifestyle).
Local public health units do operational planning toimplement specific programs such as increased TBscreening centres.
As noted above, the federal initiative around healthgoals will presumably impact decisions locally abouttarget population health improvement areas.
An evidence-based approach to population healthplanning can be found in the needs/impact basedplanning model. This model outlines a comprehensivemethod to plan based on the needs of the population.The approach comprises even steps and can be used atprovincial, regional/district and community servicelevels.5 Appendix D provides a diagram of this model.
Population health planning has its genetic roots ingroundbreaking work done in Canada in the 1970s thatresulted in the publication by the federal government ofthe report A New Perspective on the Health of
Canadians (1974), commonly known as the LalondeReport after Marc Lalonde, who was at that timeCanada’s Minister of National Health and Welfare. Thisreport first put forward the health field concept. Asthe report describes it:
“…the health field can be broken up into four broad
elements: human biology, environment, lifestyle and
health care organization. These four elements were
identified through an examination of the causes and
underlying factors of sickness and death in Canada,
and from an assessment of the parts the elements play
in affecting the level of health in Canada.”
The Lalonde Report is found at http://www.phac-aspc.gc.ca/ph-sp/phdd/pdf/perspective.pdf.
Page 8 Section 2: What Are The Types of Health Planning?
World Health OrganizationDefinition Of Health
Health is a state of complete physical,
mental and social well-being and not merely
the absence of disease or infirmity.
The above definition has not been amended since1948 but was expanded in the Ottawa Charter in1986.
The Ottawa Charter defined health promotion as“the process of enabling people to increase control
over and to improve their health.”
The Charter identified five priority action areas:
1. build healthy public policy
2. create supportive environments
3. strengthen community action
4. develop personal skills
5. reorient health services.

3.1 Defining the Right Question
The foremost critical success factor in a health planningprocess is to ensure that the question being addressed isthe “right” question. What is meant by the “right”question?
The planning question should:
• be specific to the actual advice required
• be posed in terms that are easy to understand (e.g.free of unnecessary adjectives and acronyms)
• be at the correct altitude, to ensure the issue isexpressed in the way that will elicit the maximumrelevant advice.
Consider the following scenario and three
potential questions for a health planning body:
• Question 1: What would be the impact of this moveon the three communities?
• Question 2: What are the health needs of persons inthe area currently being served by the three hospitals?
• Question 3: What would be the optimal configurationof hospital and community services to meet thecurrent and projected future needs?
In this case it is reasonably predictable that accesspatterns would change, and that people in at least twocommunities would fear loss of service and claim biasrelated to economic status. Thus the first question,
while important, will be stalled in the politics of thecommunities and the ethical considerations of anyperceived reduction of access to service change. Byproactively addressing the larger second question, theplanning process would provide a more usefulframework for looking at overall resource allocation inthat area from a population perspective. Based onanswers to the second question, the third question canthen be properly answered, leading to identification ofgaps and duplications, and helping to create serviceplans for both hospital and community services.
3.2 Choosing the Process Relevant to the
Task
The second critical success factor is to decide what typeof process is to be undertaken – usually a decisionbetween strategic and operational planning. The outcomedesired will define the planning focus – that is, whether itis a systems level task or service/program level task.
Regardless of which type of planning process is establish-ed, the discussions and strategies proposed must bebased on best available data, usually a combination ofhealth status, demographic and utilisation data used intandem with qualitative data obtained from activitiessuch as surveys and key informant interviews. Theseare then aligned with knowledge about best practices asidentified in evidenced-based literature or based onsuccessful local initiatives.
Section 3: What Are Critical Success Factors in a Health Planning Process? Page 9
Section 3
What Are Critical Success Factors In A Health Planning Process?
Hospital X operates two sites in two different
small communities. Along with hospital Y, who
operates a small hospital in a third community,
they have proposed to pool assets and build a
new site in the most economically advantaged of
the communities, where a large donation to the
foundation can be expected from a local
industry.
“Alice said very gently, ‘I should like to look all
round me first, if I might.’
‘You may look in front of you, and on both sides,
if you like,’ said the Sheep; ‘but you can’t look all
round you – unless you’ve got eyes at the back
of your head.’”
Lewis Carroll, Through the Looking-Glass
The desired outcome will define the planning focus.

3.3 Engaging Stakeholders
The third key success factor is to decide who needs tobe engaged in the planning and how the engagementwill occur. The stakeholders who participate in theplanning process are key to its success. Generally arange of perspectives should be at the table. Whenengaged in broad system planning at a strategic level,the goal will be to have experienced and recognisedleaders and thinkers from the health sector, challengedand augmented by representatives from areas such asconsumers, academia and the private sector.
There are several advantages to bringing together adiverse group:
• a broad range and depth of issues are explored
• the intended and unintended consequences of systemchange are considered
• the broader group will itself represent integrativethinking
• champions will emerge from a successful planningprocess.
Shorter term planning processes are often necessarywhen dollars become available toward the end of afiscal period or when new funding announcements aremade, requiring a quick plan for use of these resources.In these instances it is expeditious to have the issueexperts and current service providers (hospital clinicalleaders, physicians) help develop the response. Theplan will thus be driven primarily by provider realitiesand existing implementation opportunities.
3.4 Establishing Effective Project
Management
A fourth critical success factor for health planning iseffective project management. Process design andimplementation, a key aspect of project management,should stimulate useful discussion and debate amongkey participants, who will be persons with knowledgerelevant to the issue at hand. These persons may all bewithin the governmental or funder area (such as a tri-ministry committee), or may be multi-sectorstakeholders brought together as part of a local systems
process. In either case, dialogue may have to be coaxedout, or strictly managed to a tight time frame. Themethods used to facilitate and build consensus withinthe discussion process will make or break the dynamicsof the planning process.
Some of these tools are noted within Section 7 andwithin this module’s appendices. Module 5, Community
Engagement and Communication, provides morematerial on building consensus in the context ofcommunity engagement.
3.5 Planning Within an Ethical
Framework
An overlooked but important success factor in anyplanning project is transparent presentation of theproject’s ethics. Ethics in health planning is assumed,but not necessarily appropriately so. It is essential thatthe assumptions underlying decision-making processesbe clearly stated. And as Module 2 (Assessing Need)points out, choosing amongst values is inevitable whendetermining measurement tools.
Assuming the right people are at the table, the rightquestions and information are addressed and theoutputs are responsibly handled, the process willusually seem to have been done in an honest and ethicalmanner. Within this consideration, it will be easier topromote the ethics of a broad-based open inputplanning process than one that is done entirely behindthe closed doors of the funder. However, even in thelatter case, the results can be seen as sufficient as longas they are accompanied by explanation of data andevidence to support directions that have beendetermined.
Within the new LHINs in Ontario (given their statedcommitment to involve local areas in health priority-
Page 10 Section 3: What Are Critical Success Factors in a Health Planning Process?
“‘Tut, tut, child!’ said the Duchess. ‘Everything's
got a moral, if only you can find it.’”
– Lewis Carroll, Alice’s Adventures in
Wonderland

Section 3: What Are Critical Success Factors in a Health Planning Process? Page 11
setting and funding activities) challenges will likelyarise related to funding decisions. Therefore an ethicaland consistent decision-making approach will beimportant. Dealing with resource decisions in a tighthealth care funding environment implies that some maygain while others may appear to lose from planningoutcomes. The integrity of the process will be inquestion if the process is, or seems to be, poorlybalanced in terms of its participants or founded oninadequate information.
Perhaps the most broadly debated health priority settingexercise was undertaken in Oregon in the early 1990s.As two authors who examined the Oregon experienceput it, “The Oregon Plan has been widely heralded as
an innovation in health policy as the first public
insurance program to ration medical care explicitly,
systematically, and openly by denying coverage for
health care services.”6
In the Oregon initiative the state government undertooka consultative process to determine what the publicthought was most important to be covered by the state’sMedicaid budget. Advocates for groups such as peopleliving in poverty and people with HIV/AIDS challengedthe appropriateness of this process and what they sawas rationing of health services to the mostdisadvantaged. However, according to some studies theOregon experiment successfully engaged Oregonians inthinking about hard decisions and efficacy of healthcare interventions, and it resulted in higher fundinglevels for health services in the state rather than costsavings. Nonetheless the whole dispute has beencharacterised as advocates of transparency pittedagainst advocates for the most disadvantaged.
For more about the Oregon experience and itsrelevance for other jurisdictions, see Appendix E.
3.6 Accessing and Applying Relevant
Information
A taxonomy of human service planning informationwould include the following types of information.
“Hard data”:
These data include many kinds of information used inboth traditional and newer planning methodologies.Hard data include:
• Demographic data (what are the characteristics of apopulation?)
• Epidemiological and social indicator data (whatare the characteristics of social problems and healthdisorders within a population?)
• Inventory data (what are the numbers, types andcharacteristics of human service resources for apopulation – including the cost of these resourcesand the linkages among the resources?)
• Utilisation data (how does a population use thoseresources?)
• Outcome data (what changes in social and healthstatus do these resources produce for populations?)
Attitudinal and behavioural information:
This is information on the beliefs and attitudes ofconsumers and of providers concerning human servicesystems - it is the “sociology of well-being”. Forinstance, a consumer may believe that physicians arebetter helpers than other human service professionals,and may behave on the basis of this belief by seekingout a physician rather than another professional, evenin the face of hard outcome data suggesting thatanother professional (a nutritionist for example) mayyield a better outcome for that consumer.
Ignoring attitudinal and behavioural information mayproduce a plan that makes logical sense based on harddata, but which is impossible to implement because:
• it flies in the face of what people believe and how theyact
• or because it does not build in provisions for changingoutmoded attitudes and behaviours.
It is essential that the assumptions about
decision-making processes be clearly stated.

Expert opinion:
Both consumers and providers can be experts - aconsumer may well be the expert on what it is like to bea consumer – and the provider may be an expert onspecific approaches to improving social well-being andhealth.
Often these kinds of expertise are not easily codifiableas hard data, but they are still valuable sources ofinformation. If one were planning an improvement inrespiratory health, for instance, consumers might provideexpertise on the emotional burdens of chronic lungdisease. Similarly, a renowned environmental specialistmight have great expertise in helping disadvantagedpopulations experiencing high rates of asthma.
Political process information:
Human service issues are often political, in terms offormal electoral politics as well as the politics ofpowerful stakeholders, particularly in formal humanservice systems. Knowledge of formal positions taken
by political, bureaucratic or other social groupings maymake the difference between a plan that will beimplemented and a plan that will remain on a shelf.
In short, each of the information types can becharacterised as follows:
• Hard data – the facts of human services
• Attitudinal and behavioural information – thesociology of human services
• Expert opinion – the wisdom of human services
• Political process information – the politics of humanservices.
Using a Taxonomy:
Whether an information taxonomy uses the categoriesof information outlined above – or any other set ofcategories – it can prove useful in helping planners makeinformed decisions about what kind of information togather at each stage in the planning process.
Page 12 Section 3: What Are Critical Success Factors in a Health Planning Process?
Dem
ograp
hic
Ep
idem
iolo
ggic
al
Inven
tory
Uti
lisati
on
Ou
tco
me
Information
Type Hard Data by Type
1. What ought
to be?
2. What is?
3. Problems/ challenges
(#1 minus #2)
4. Range of solutions
5. Best
solution(s)
6. Implement
7. Evaluate
Attitudinal &
Behavioural
Information
Expert
Opinion
Political
Process
InformationPlanning
Stage 7
Figure 6: Relative Volumes of Information Matrix
Often a simple matrix can help a planner or planninggroup decide what kinds and relative volumes ofinformation should be gathered at each planning stage.See figure 6.
3.7 A Commitment to Monitoring and
Evaluation
Planning is often cyclical, in the sense that one cycle ofplanning leads into the next cycle, so that planning is acontinuous and iterative process that takes intoaccount:
• changed circumstances
• the effects of implementation of previous planning.
However, one cycle of planning cannot learn fromprevious cycles unless monitoring and evaluationprocesses are put in place to determine the effects ofprevious planning cycles.
Many planning processes make it part and parcel of theprocess to identify the monitoring and evaluationprocesses and tools that are needed and to exertinfluence to ensure these processes and tools aredeveloped and used.
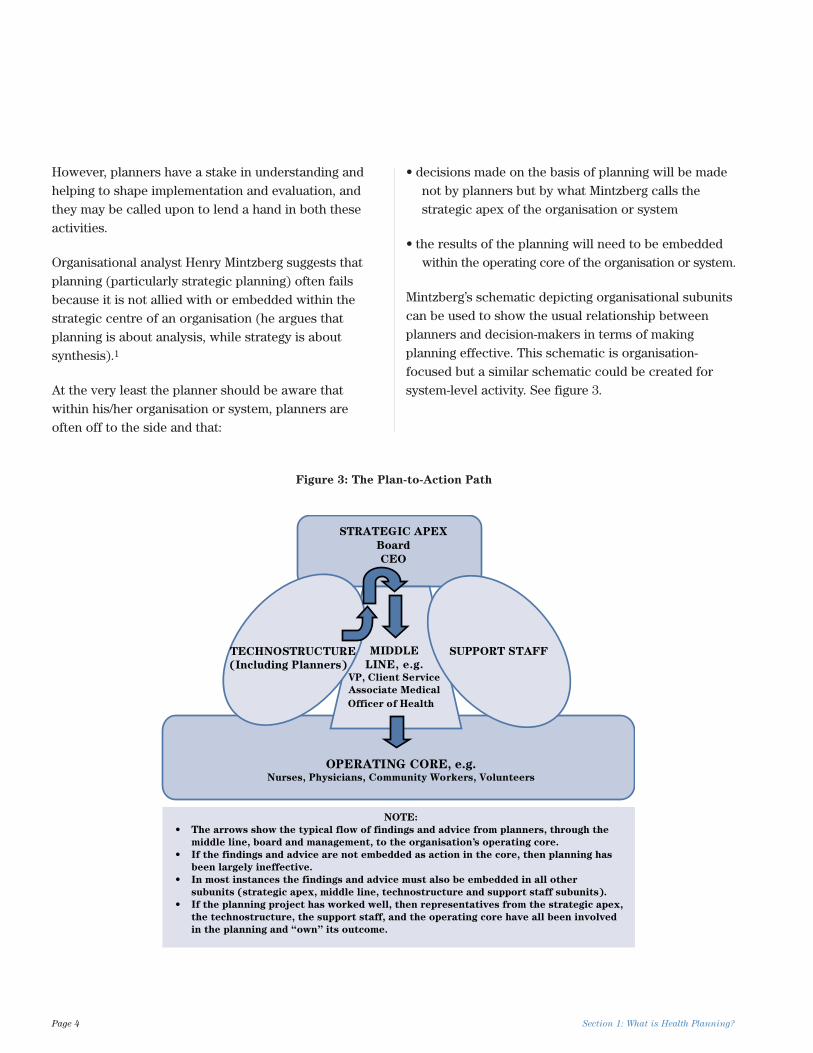
One interesting variation on the use of monitoring andevaluation is “trajectory planning”. This way of thinkingassumes that the implementation of any planning mayencounter turbulence – much like the headwinds ortailwinds that aircraft experience during their trajectoryfrom take-off point to landing point. See figure 7.
Trajectory planning uses monitoring tools to:
• identify turbulence
• determine whether that turbulence will aid or impedeachievement of the plan’s goals
• provide the basis for “mid-flight corrections” to helpensure that the plan achieves its goals.
Section 3: What Are Critical Success Factors in a Health Planning Process? Page 13
“‘I see nobody on the road,’ said Alice.
‘I only wish I had such eyes,’ the King remarked in a
fretful tone. ‘To be able to see Nobody! And at that
distance too! Why, it’s as much as I can do to see
real people, by this light.’”
– Lewis Carroll, Through the Looking-Glass
turbulence
(identified through monitoring tools)
end
adjustment points in trajectory
start
Figure 7: Trajectory Planning

Page 14 Section 3: What Are Critical Success Factors in a Health Planning Process?

4.1 Strategic Planning
A strategic planning process is used when there is abroad and open question to be answered, and manypaths are on the table - for example, identifying thedesired model for delivery of children’s mental healthservices in rural settings and determining how to moveto that model.
Usually a strategic planning process assumes a newlook at an issue, and an outcome that will take time toput in place but will exist for a period longer than onefunding cycle. Generally speaking it is assumed that astrategic plan will need to be revised or redone whenthe context in which the service exists changesmarkedly. A change in context could relate tochallenges to sustainability, opportunities to expand, ornewly identified best practices that should beincorporated into the plan. An example would be the
opportunity to design locally relevant multi-agencycentres for children’s mental health services within thecontext of the new LHIN areas.
A basic guideline for planning is that a vision should berenewed every three to five years and the strategicdirections emanating from that vision also re-evaluated,perhaps yearly. A strategic planning exercise will includestrategic goals and directions, and in some cases mayalso include specific implementation or operationalplanning components. For example in establishing anew local system of children’s mental health services,specific budgets, service expectations, timetables andhuman resource models may be designed by thestrategic planning group, for hand-off to providers.
The Vancouver Island Health Authority (VIHA) HealthServices Plan is an excellent resource document thatcan be found in its entirety on the VIHA web site atwww.viha.ca. The figure below illustrates VIHA’sstrategic planning approach, which calls for initialpriority action areas, then yearly establishment ofstrategic directions within an umbrella framework.
Section 4: What is Strategic Planning Versus Operational Planning? Page 15
Section 4
What Is Strategic Planning VersusOperational Planning?
… a vision should be renewed every three to five
years.
Figure 8: Vancouver Island Health Authority Strategic Plan Model
Adapted from Vancouver Island Health Authority, Integration 2005.8
Vision
Mission
Values
Goals & Strategies
Balanced Scorecard
Strategic Initiatives

The VIHA Five-Year Strategic Plan sets the overalldirection for future service delivery to 2010. It chartsthe move toward enhanced integration, responsivenessand innovation for all health services across the region.In particular it outlines:
• priority issues in the health authority
• critical challenges to population health and servicedelivery in the VIHA region
• goals and strategic themes that will guide servicedelivery
• strategic directions by sector and by geographic area.
The Plan advances strategic thinking to includeorganisational restructuring, new and innovative servicedelivery models, and future capacity forecasts. It isaligned with the strategic direction of the Ministry ofHealth, recognises the significant differences indemographics and health status throughout the healthauthority, and reflects clinical input and practicalexperience.9
4.1.1 Strategic Planning Process
Components
Within any strategic planning exercise the followingactivities will occur:
• a visioning exercise
• creating mission and goals
• establishing objectives
• establishing strategic directions
• developing a framework to establish and monitorsuccess – a balanced scorecard approach forinstance (see figure below)
• creating an implementation plan/timetable.
Although originally developed for the corporate sector,the balanced scorecard has become popular within thehealth sector as a tool for both planning and monitoring.The balanced scorecard suggests that an organization beviewed from four perspectives, and that data collectionand analysis be carried out relative to each of theseperspectives. See Figure 9. In some instances it has taken
Page 16 Section 4: What is Strategic Planning Versus Operational Planning?
MISSION
CUSTOMERS AND
STAKEHOLDERS
ORGANISATION CAPACITY(LEARNING & GROWTH)
INTERMEDIATE
BUSINESS PROCESS
FINANCIAL/BUDGET
VISION & STRATEGY
to achieve our vision,
how should we appear
to our funders?
• objectives
• measures
• targets
• initiatives
to achieve our vision,
how will we sustain our
ability to change and
improve?
• objectives
• measures
• targets
• initiatives
to achieve our vision,
how should we appear
to our clients and other
stakeholders?
to satisfy our client, funders and
other stakeholders, what business
should we excel at?
• objectives • targets
• measures • initiatives
• objectives
• measures
• targets
• initiatives
Figure 9: Public Sector Balanced Scorecard: The Four Perspectives
Adapted from H. Rohm, Balanced Scorecard Institute10

the place of a more formalised and longer-termevaluation exercise. For more on the application of abalanced scorecard see Appendix F.
Strategic planning processes should be supported by:
• use of data, both quantitative and qualitative
• consultation with stakeholders (related to all parts ofthe process, from visioning to data interpretation andcrafting recommendations)
• application of project management and facilitationtools, which may include activities such as SWOT(strengths, weaknesses, opportunities and threats)analysis, mind-mapping and strategic alignmentmodels
• monitoring and evaluation protocols.
Appendix G provides a sampling of these strategicplanning tools.
4.2 Operational Planning
An operational planning process starts from a point of aspecific objective, for example to increase the numberof clients served through a primary care clinic at aCommunity Health Centre, and focuses on the range ofopportunities within that delivery framework.
Operational planning will include:
• statement of purpose/deliverables/target to beachieved/success indicators
• use of available and relevant data and information
• stakeholder engagement (who needs to fund, deliverexpanded services?)
• selection of priority action approach (new programdesign)
• developing an implementation timetable and budget.
Operational planning processes may be supported byactivities or tools similar to those for strategic planningbut with a tighter question applied to these activities.Included in operational planning could be use of anactivity hierarchy model and a program logic model.
Evaluation goals – process or outcome, quantitative orqualitative – must be considered at the front end of anynew initiative.
Appendix H provides information on operationalplanning tools. Appendix I offers information onevaluation relevant to both strategic and operationalplanning.
Section 4: What is Strategic Planning Versus Operational Planning? Page 17
Evaluation goals – process or outcome, quantitative
or qualitative, must be considered at the front end
of any new initiative.

Page 18 Section 4: What is Strategic Planning Versus Operational Planning?

Planning is an art as well as a science. Keeping in mindthe science/art duality will keep planning processesbalanced and realistic. Project management courses arewidely available but health planning is not as wellunderstood. In reality the two disciplines must besuccessfully combined.
In both areas there is seldom a straight-ahead road withno bumps or diversions along the way. The challenge ofadaptability will always exist and meeting that challengeis critical to successful planning. The followingsubsections cite examples of adaptability issues.
5.1 Comprehensive Planning Process
Versus Hurry Up and Go!
In establishing a process to address a need oropportunity, there may not always be time for a pure,comprehensive and linear planning process. Decisionsmay have to be made to emphasise one or two elementsof the planning process and short circuit the rest.
For example if strategic directions are required in threemonths time, there may not be time for comprehensivecommunity engagement or broad discussions about bestpractices. An effective way to address the tight timelineissue is to establish parallel activity processes throughworking groups. The key to successfully using thisapproach is to have built-in relationships between theprimary strategic planning group and the workinggroups, best achieved by crossover membership toensure continuous information flow.
Other techniques may be employed such as substitutingkey informant meetings and presentations by experts inthe field in place of more comprehensive and time-consuming community and stakeholder consultations.
5.2 Use of Advocacy Groups
As noted earlier in this module, consumer and advocacygroups may have already identified their wish list in acertain area. Existing reports or background paperscreated by advocacy groups can be used to advanceplanning by bringing into the planning process consumeror provider views that have already been articulated(although these are not necessarily the only views to beconsidered). Acknowledging and incorporating thisconsensus into planning will strengthen the informationand best practice element, and reduce consultation time.
5.3 Planning Versus Action – Selling the
Process
A hospital CEO once described planning as a substitutefor action. While this comment was exaggerated foreffect, it expressed frustration felt by many within thehealth field about:
• the lack of overall health system direction
• the constantly changing landscape of funding andpriority setting.
Health planning will be most effective and most saleablewhen it flows from a clearly defined framework forhealth and health services at the senior level ofgovernment. Funding to follow strategic directions willmake it real for those required to make the changes atthe line level. Marketing change to large organizationsand smaller agencies alike requires a plan that speaks tothe challenges and opportunities each will face.
Section 5: Other Useful Information Page 19
Section 5
Other Useful Information
“If we are facing in the right direction, all we have
to do is keep on walking.”
Buddhist Proverb

Page 20 Section 5: Other Useful Information

A speech by Sir Winston Churchill in the early days ofthe Second World War contains one of the mostarticulate and memorable mission statements in modernhistory. The politics of appeasement had led Englandinto a new political stance and into war with Germany,and Churchill was compelled to frame the issue inunambiguous terms. In his address and rallying cry toBritish citizens Churchill had only one outcome in mind,and that was for his country to prevail. His speechstated clearly that all strategies would emanate fromthat singular goal.
Health planning in Ontario will not bear the harshnessof war, nor include the risk of loss of statehood.Nonetheless such examples help us to understand howpolitical developments lead to decisions, which lead toa mission, which is inevitably translated into a plan ofaction, which in turn affects citizens - sometimesprofoundly.
Reality dictates that political drivers both lead to, andare derived from, more deliberate policy development.Both are key aspects of health planning.
Section 6: Summary: Keep The Goal In Sight Page 21
Section 6
Summary: Keep The Goal In Sight
We shall defend our island whatever the cost may be.
We shall fight on the beaches
We shall fight on the landing grounds
We shall fight in the fields and in the streets
We shall fight in the hills
We shall never surrender.
Winston Churchill, June 4th 1940

1. Calgary Health Region. Building Canada’sHealthiest Community-Three Year Health Plan2005/06 – 2007/08. available from:http://www.calgaryhealthregion.ca/communications/healthplan.html
2. Canadian Centre for Advanced Research in Health.Provincial Overview Table. 2005.
3. Enhancing the evidence base for health impactassessment, Mindell et al. Journal of Epidemiologyand Community Health 2004; 58(7): 546-551 BMJPublishing Group Ltd. 2004.
4. Fiander M, Burns T. A Delphi Approach toDescribing Service Models of Community MentalHealth Practice.
5. James J.S. Oregon Health Rationing Plan: AIDSImpact Feared. AIDS Treatment News. 1991.
6. Library of Congress. Project Planning Check List.1997 Available from:http://memory.loc.gov/ammem/prjplan.html
7. McNamara Carter. Strategic Planning in non profitand for-profit organizations. Available from:http://www.managementhelp.org/plan_dec/str_plan
8. Saskatchewan Workers Compensation Board.Strategic and Operational Plan. 2002 – 2004.Available from:http://www.wcbsask.com/Forms_&_Publications/strategic-opplan2002-2004.pdf
9. SWOT analysis. Businessballs.com. available from:http://www.businessballs.com/freematerialsinword/free_SWOT_analysis_template.doc
10. World Health Organization. Healthy Cities andUrban Governance. 2005. Available from:http://www.euro.who.int/eprise/main/WHO/progs/hcp/Home
Page 22 Bibliography
Bibliography

1. Mintzberg H. The Rise and Fall of Strategic Planning:Reconceiving Roles for Planning, Plans, Planners.The Free Press, 1993.
2. Government of Alberta. Health and Wellness.Available from: www.health.gov.ab.ca/regions
3. The Ottawa Charter for Health Promotion, 1986,found athttp://www.who.int/hpr/NPH/docs/ottawa_charter_hp.pdf
4. World Health Organization. Available from:www.who.int/mediacentre/factsheets/fs171/en
5. Metropolitan Toronto District Health Council, AGuide to Needs/Impact-Based Planning, Final Reportof the Needs/Impact Based Planning Committee tothe Ministry of Health, Community Health Division,submitted April 1996
6. Oberlander J, Marmor T. Rationing medical care:rhetoric and reality in the Oregon Health Plan.Canadian Medical Association Journal, May, 2001
7. Loosely based on the stages in the planning cycledeveloped by Henrik L. Blum, Professor Emeritus ofHealth Planning at the University of California atBerkeley
8. Vancouver Island Health Authority. Strategic Plan to2010, 2005. Available from: http://www.viha.ca
9. Vancouver Island Health Authority. Strategic Plan to2010, 2005 Available from: http://www.viha.ca
10. Improve Public Sector Results with a BalancedScorecard: Nine Steps to Success, H Rohm,Balanced Scorecard Institute, 2002. Availablefrom:http://www.balancedscorecard.org/files/Improve_
References Page 23
References
‘In that case,’ said the Dodo solemnly, rising to its feet, ‘I move that the meeting adjourn, for
the immediate adoption of more energetic remedies.’
Lewis Carroll, Alice’s Adventures in Wonderland
At the First Ministers’ meeting in September 2004, thePrime Minister and the Premiers signed a ten-yearaction plan to pursue better health care for allCanadians. The plan included a commitment toestablish health goals to improve the health ofCanadians and to reduce pressure on the health system.Federal, provincial and territorial governments haveagreed to work together in this goal setting exercise.
The federal government initiated a cross-countryconsultation process to identify how health goals forCanada should be established. Roundtables were heldwith experts and citizens across the country. Theinformation from the roundtables will be synthesisedthrough a reference group appointed by the provincialand territorial health ministers.
The goals will build on public health goals that mayhave already been established in some jurisdictions, andwill be incorporated into a broad framework to helpalign public health efforts across the country.
Once released the public health goals will be publishedon the Public Health Goals web site atwww.healthycanadians.ca.
As part of this exercise the government has definedpublic health as different from health care services.They have stated that it encompasses every aspect of
people’s lives, from homes, to workplaces, tocommunities and schools. They have further statedthat, as the greatest share of health problems areattributable to broad social conditions, it is essential tointervene in these areas to promote health.
One strategy that has been announced is the integratedchronic disease prevention strategy. Scientific evidencedemonstrates that healthy eating and physical activity,and healthy weights protect against many chronicdiseases, including cancer, heart disease and stroke aswell as diabetes. This initiative is based on the findingthat major chronic diseases share common risk factors,thereby making an integrated approach the mosteffective and practical way to advance healthpromotion.
Page 24 Appendix A: Public Health Goals For Canada
Appendix A
Public Health Goals For Canada
“Public health is often described as the science and
art of promoting health, preventing disease,
prolonging life and improving quality of life through
the organized efforts of society.”
Learning from SARS,
Renewal of Public Health in Canada, 2003
Explanation and Overview of the Toolkit
Welcome to the Healthy People Toolkit! The Toolkitprovides guidance, technical tools, and resources tohelp states, territories, and tribes develop and promotesuccessful state-specific Healthy People 2010 plans1. Itcan also serve as a resource for communities and otherentities embarking on similar health planning endeavors.
This Toolkit is organized around seven major “actionareas,” which were derived from national and stateHealthy People initiatives2. With the assistance andguidance of the Office of Disease Prevention and HealthPromotion, U.S. Department of Health and HumanServices (HHS), the Public Health Foundation (PHF)reviewed both year 2000 and year 2010 initiatives andidentified these seven areas as common elements ofmost health planning and improvement efforts. Theseven action areas are:
• Building the Foundation: Leadership and Structure
• Identifying and Securing Resources
• Identifying and Engaging Community Partners
• Setting Health Priorities and Establishing Objectives
• Obtaining Baseline Measures, Setting Targets, andMeasuring Progress
• Managing and Sustaining the Process
• Communicating Health Goals and Objectives
Each action area includes:
• a brief explanation and rationale
• a checklist of major activities, which are taken fromthe comprehensive planning checklist tool in“Managing and Sustaining the Process”
• tips for success
• national and state examples to illustrate HealthyPeople processes in action
• recommended “hot picks” of resources for furtherinformation, designated by a star (icon)
• planning tools that can be easily adapted to state orlocal needs, designated by a tool (icon)
The suggested processes, tools, and resources in theseven action areas can help states build on pastsuccesses and round out their approaches to planningand developing year 2010 objectives. An effectiveplanning initiative should reflect the state’s uniqueneeds, resources, and buy-in from a broad constituency.
Attached as appendices are comprehensive listings ofresources; State, Territorial, and Tribal Action Contacts;and state and national Healthy People web sites3.
A web-based version of the Toolkit offers usersenhanced access, navigation, and search capabilitiesand is available at: http://www.health.gov/healthypeople/state/toolkit.
The web version contains direct links to state HealthyPeople web pages, up-to-date listings of state HealthyPeople action contacts, Healthy People 2010 leadagency content experts, and HHS Regional HealthAdministrators.
Because this Toolkit is in the public domain, weencourage you to copy the Toolkit to share with yourstate and local partners.
The Public Health Foundation would like to hear aboutyour year 2010 initiative, how you are using the Toolkit,and what additional resources or examples would behelpful to you. Please contact us at:
Public Health Foundation. . . . . . . . . . . . 202-898-5600 (T)
Healthy People Initiative. . . . . . . . . . . . . 202-898-5609 (F)
1220 L Street, NW, Suite 350 . . . . . . . . . . [email protected]
Washington, DC 20005
Appendix B: Healthy People 2010 Toolkit Page 25
Appendix B
Healthy People 2010 Toolkit
1 The term “state plan” will be used throughout the Toolkit to indicate “state-, territory-, or tribal-specific Healthy People 2010 plan.”
2 The hundreds of local health planning initiatives could fill a separate volume and were not reviewed for inclusion in the Toolkit. However, a small selection of local
resources is included for local Toolkit users.
3 The Public Health Foundation made every reasonable effort to confirm the accuracy of all web site addresses, resource listings, and contact information as of
February 2002. PHF apologizes for any inconvenience caused by inaccurate listings.

Action Checklist: Setting Health
Priorities and Establishing Objectives
(See page 113 of the U.S. Healthy People toolkit for acomplete planning and development checklist.)
❑ Evaluate input from community partners andexperts
❑ Collect and review previous health needs andassets assessments
❑ Conduct assessments of health needs and assets, ifnecessary
❑ Plan for transitions from year 2000 to year 2010health objectives
❑ Decide where changes from year 2000 are neededand what should be retained
❑ Define the scope of the state plan
❑ Set criteria for establishing potential priority orfocus areas
❑ Establish a process for final determination ofpriorities
❑ Identify and obtain information to evaluate areasaccording to criteria
❑ Select final priority or focus areas
❑ Determine types of objectives desired andestablish criteria for adopting them
❑ Outline standard information to include with allpriority areas and objectives
❑ Specify intervention points; identify potentialtopics and indicators for objectives
❑ Develop draft objectives
Tips
Perception is reality for many people
• Learn what the community and key partners see asimportant health issues (see action area,“Communicating Health Goals and Objectives,”within the tool kit for ideas on learning from targetaudiences)
• Review comments your state residents submitted onthe draft Healthy People 2010 focal areas andobjectives (see page 54 of the tool kit)
• Obtain qualitative data, where possible, to assess anddescribe community perceptions
• Build on perceptions to gain broader support forpriorities
Define the “rules of the game” up front – before
trying to establish priorities and objectives
• Make sure everyone understands and accepts theprocess for recommending and adopting finalpriorities
• Set a cut off date for proposing changes to the “rules”
• Determine what other plans and objectives should beexplicitly considered or incorporated into the stateplan (e.g., national Healthy People 2010 draftobjectives, state performance plans, existing tobaccoor HIV/AIDS plans)
• Determine how priority areas should be related to theagreed vision and scope of your plan
Page 26 Appendix B: Healthy People 2010 Toolkit

Be clear about your criteria for determining
priorities and establishing objectives
• Communicate important characteristics of objectives(e.g., feasibility, effectiveness, short-term/long-term,measurability) to work groups
• Make simple worksheets or checklists to helpplanning group members consistently considercriteria and see relevant information at a glance
• Strive for measurable objectives, but don’t neglectimportant health areas where measures need to bedeveloped and objectives may drive new data sources
You’re not starting from scratch – build on your
assets, not just your needs
• Align priorities, objectives and strategies with yourstate’s strengths, assets, and opportunities wherepossible
• Look to other sources for information such as leadingcauses of death, Basic Priority Rating or otherranking systems, surveillance systems, or outcomesfrom your state’s Healthy People 2000 plan
• Show respect for what has already been accomplishedto address priorities
Appendix B: Healthy People 2010 Toolkit Page 27

Health impact assessments look at the effect on healthof policies implemented outside the health care sector(see module 2, Assessing Need, for further discussionof health impact assessment).
Information in this appendix includes excerpts from thefollowing sources:
• Mindell et al. A Glossary for Health ImpactAssessment, Journal of Epidemiology andCommunity Health 2003; 57(9): 647-651, BMJPublishing Group Ltd. 2003
• Blau G and Mahoney M. The Positioning of HealthImpact Assessment in Local Government in Victoria,Health Impact Assessment Unit, Deakin University,Australia, October 2005.
Health impact assessment has its roots in environmentalimpact assessment. However, the scope of healthimpact assessment has broadened from this traditionalrisk/environmental/health protection model to publichealth/health promotion applications that can beapplied to all activities that may have an impact onhuman health.
It has long been recognised that health and itsdeterminants are strongly influenced by policies outsidethe health care sector, for example, transport,regeneration projects and housing. In recent yearsseveral countries have introduced health impactassessment to ensure that potential effects on health aretaken into account. It involves identifying disbenefitsand benefits to health, interpreting health risk andpotential health gain, and presenting this information toaid decision-making.
Health impact assessment is a multidisciplinary activitythat a consensus paper published by the WHO RegionalOffice for Europe describes as “a combination of
procedures, methods and tools by which a policy,
program or project may be judged as to its potential
effects on the health of a population, and the
distribution of those effects within the population”.
The Aim of Health Impact Assessment
All definitions of health impact assessment agree thatthe aim is to maximise the health gain (and minimisethe loss) that might result from a proposal, even whenthe proposal does not have health improvement as itsaim:
• Health impact assessment should be multidisciplinary,intersectoral and participatory, and should include afocus on health inequalities.
• Both quantitative and qualitative evidence should beused.
• The main values underlying the conduct of healthimpact assessment are:
• sustainability
• the promotion of health
• participation
• democracy
• equity
• equality (of all stakeholders in the process, but inparticular of the community affected)
• the ethical use of evidence.
Health Inequalities Impact Assessment
(HIIA)
This form of health impact assessment used in the UKaims at assessing impacts of a proposal on the healthand well-being of people in the community whoexperience health and other inequalities in relation toage, sex, ethnic background or socioeconomic status, toidentify whether there is a differential distribution ofimpacts.
The current consensus is that all health impactassessments should consider inequalities and/or thedistribution of potential health effects.
Page 28 Appendix C: Health Impact Assessment
Appendix C
Health Impact Assessment

Levels of Application
Health impact assessment can be applied to three mainlevels of proposal: a policy, a programme, or a project:
• A policy represents the way in which government oran organisation seeks to achieve the objectives it hasset. Health impact assessment at this level can bestrategic, enabling health concerns to beincorporated early on and a global view to be taken.In some cases (taxation for example) there is nolower level at which health impact assessment couldbe applied.
• A programme is a series of related activities that giveeffect to policy.
• A project is a component of a programme, and is adiscrete activity often undertaken at a specificlocation.
Health impact assessment at the programme and projectlevels allows health impacts to be assessed that arespecific to a particular locality or community. It is moretactical, with aims relating to proposal modification andimplementation.
Comparison of Policy Options
Ideally a health impact assessment will compare allpossible options that could be under consideration. Thisgives policy makers the most explicit information on thehealth consequences of their actions and increases thepossibility of integrated assessment.
Stages
Health impact assessment comprises six stages:
1. screening
2. scoping
3. appraisal or risk assessment
4. preparation of report and recommendations
5. submission of report and recommendations todecision makers
6. monitoring and evaluation.
Appendix C: Health Impact Assessment Page 29

Figure D1: Needs Impact Based Planning Model
Page 30 Appendix D: Needs Impact Based Planning Model
Appendix D
Needs Impact Based Planning Model
Source: Needs/Impact Based Planning Committee. A Guide to Needs/Impact Based Planning: Final Report to Ministry of Health. 1996.
Research
Research
Research
DETERMINE THE NEEDS
• Identify issues with greatest
impact on health using defined
Health Status scores
POTENTIAL
& CURRENT STRATEGIES
• Identify potentially feasible
interventions
• Estimate impact on the
identified issues
EVALUATE STRATEGIES
• Determine efficacy, effectiveness,
efficiency, availability and
appropriateness of the strategies
DETERMINE PRIORITIES
• Rank the identified health issues on
the basis of the evaluation
• set targets for implementation
• identify barriers to implementation
ACTION & ADVOCACY
• Implement
• Advocate for implementation
where appropriate
EVALUATE IMPACT
• Evaluate impact of the
chosen strategies

Since its inception in 1994 the Oregon Health Plan hasgarnered much attention. It has been heralded as aninnovation in medical care policy and rationing. At thesame time the process undertaken and the criticismsaround the process captured the attention of manyconcerned about equity of access to health care.
According to Oberlander et al the Oregon Health Planwas the first public insurance program to ration medicalcare explicitly, systematically and openly by denyingcoverage for health care services. Other jurisdictionswrestling with how to prioritise within competing healthdemands and increasing health care costs have lookedto this approach and its outcomes for possibleapproaches or lessons. At the same time considerableconcern has been expressed about the ethics of thisrationing process, especially as it could affect personswith non-mainstream health issues such as HIV/AIDS,tuberculosis and addictions.
While financial imperatives were behind the originalexperiment is has evolved into a more participatoryhealth care goal-setting exercise. Moreover, accordingto Oberlander et al it has not resulted in saving anyhealth care dollars.
Oberlander states that despite the Oregon Health Plan’sstatus as a celebrated US policy innovation, no US stateor other nation has emulated the Oregon model. In partthis is because what other jurisdictions presumed wasthe key to Oregon’s ability to expand coverage – the listand a formulaic system for rationing – turned out to beillusory. It is also the case that the furor over theOregon plan has dissuaded others from similar efforts.The political controversy that comes with the decisionto terminate coverage for medical services explicitlyand publicly is baggage that no other US state has beenwilling to take on.
The real innovations in Oregon have been the use ofpublic participation to build public support, and raisingrevenues for expanding coverage for the poor.
According to Oberlander the most important lesson forCanada is that explicit delisting of services is unlikely toproduce substantial savings. The political paradox ofrationing is that the more public the decisions are aboutpriority setting and rationing, the harder it is to rationservices to control costs.
Information for this appendix was taken from:
• Rationing medical care: rhetoric and reality in theOregon Health Plan, Oberlander et al, CanadianMedical Association Journal, May 29, 2001: 164 (11)
• http://www.oregon.gov/DHS/healthplan/index.shtml
• http://www.oregon.gov/DAS/OHPPR/HPC/docs/HVS2004Report.pdf
Appendix E: The Oregon Experience Page 31
Appendix E
The Oregon Experience
The balanced scorecard was developed in the early1990s by Robert S. Kaplan and David P. Norton of theHarvard Business School. This new approach to strategicmanagement was named the balanced scorecard toreflect the importance of measuring other factors tobalance traditional financial measurement. The balancedscorecard suggests that an organisation be viewed fromfour perspectives:
• learning and growth• business process• customer • financial
Under the balanced scorecard approach, metrics, dataand analysis should be developed and applied relative toeach of these four perspectives.
Howard Rohm, Principal and Director of the BalancedScorecard Institute, has adapted the balanced scorecardfor public sector (See Figure 9 on page 16) in awaywhich uses slightly different concepts from the privatesector approach (e.g. organisational capacity issubstituted for learning and growth).
The balanced scorecard is not just a measurementapproach. It is also an effective management tool toenable organisations to:
• clarify their vision and strategy • translate them into action.
It provides feedback around both the internal businessprocesses and the external outcomes in order tocontinuously improve strategic performance and results.
Kaplan and Norton describe the innovation of thebalanced scorecard as follows:
“The balanced scorecard retains traditional financial
measures. But financial measures tell the story of past
events, an adequate story for industrial age
companies for which investments in long term
capabilities and customer relationships were not
critical for success. Those financial measures are
inadequate, however, for guiding and evaluating the
journey that information age companies must take to
create future value through investment in customers,
suppliers, employees, processes, technology, and
innovation.”
Regardless of which terms are used, the balancedscorecard has been adopted by many health careorganizations for planning and monitoring purposes.
Information related to this appendix can be found at:
• www.balancedscorecard.org
• Rohm, H. Improve Public Sector Results with aBalanced Scorecard: Nine Steps to Success, found asa Shockwave file at: http://www.balancedscorecard.org/files/Improve_Public_Sector_Perf_w_BSC_0203.swf
Page 32 Appendix F: The Balanced Scorecard
Appendix F
The Balanced Scorecard

The development of a strategic plan for a whole healthsystem is a large and potentially daunting task.However, there are excellent examples of its use inseveral jurisdictions, including some in Canada. Earlierin this module the Vancouver Island Health Authoritystrategic plan was noted. Both the Strategic Plan to theYear 2010 and the earlier document entitled IntegrationPlan 2007 are useful resources. Information on theVancouver Island Health Authority and its planning is at:www.viha.ca.
As well, for strategic planning some organizations haveincorporated the balanced scorecard approach (seeAppendix F).
The best tools for strategic planning are often the onesthat the person leading the planning is most familiarwith and has used successfully in previous initiatives.However, there are commonly accepted tools that bringrigour and consistency to strategic planning. Some ofthese are described below.
SWOT Analysis:
This is an outline of strengths, weaknesses,opportunities of, and threats to, the organisation. It isusually done at the start of a strategic planning exercisein a group setting, to identify all factors in each area.The factors are usually organised in a table of fourquadrants so participants in the planning exercise canvisually (and easily) see the context for the planning.
• strengths include factors like staff capabilities,effective management processes, competitiveadvantage and unique programs or products.
• weaknesses include factors like gaps in staff skills,financial problems and inadequate informationsystems.
• opportunities include factors like global influences,new policy developments, partnerships and research.
• threats include factors like market demand, loss ofkey staff and political effects.
For more information on SWOT analysis seehttp://www.mindtools.com/pages/article/newTMC_05.htm
Affinity Diagrams:
An affinity diagram is a creative process used by agroup to gather and organise ideas. It can beparticularly powerful in a priority setting exercise.
The fundamentals of affinity exercises or diagrams isthat:
• a problem or question is stated
• participants write down their thoughts or answers
• all the ideas are posted and then grouped by likenessof ideas or themes
Usually this results in a clear visual demonstration ofareas of consensus on issues and responses.
For more information see:http://www.sytsma.com/tqmtools/affin.html
Mind-Mapping:
A new way of visioning and planning, mind-mapping hasmade its way into both the standard flip chart baseddiscussions, as well as computer based exercises.
It is a way of capturing ideas and organisinginformation. It relies on pictorial representations of theflow and synthesis of ideas.
For more information see:http://thinksmart.com/mission/workout/mindmapping_intro.html.
Appendix G: Strategic Planning Concepts and Tools Page 33
Appendix G
Strategic Planning Concepts and Tools

Mission Statement:
Key to any strategic planning exercise is thedevelopment of a vision and a clear mission statement.The mission statement may be more difficult because itmust express to all – employees, clients and otherstakeholders – what the organisation’s current purposeis. It should be expressed at a high level, yet be rich inportraying purpose, values and business.
The mission statement should:
• express an organisation’s purpose in a way thatinspires support and ongoing commitment
• motivate those who are connected to the organisation
• be articulated in a way that is convincing and easy tograsp
• use proactive verbs to describe what the organisationdoes
• be free of jargon
• be short enough so that anyone connected to theorganisation can easily repeat it.
For more information on mission statements see:http://www.businessplans.org/Mission.html.
Page 34 Appendix G: Strategic Planning Concepts and Tools

Program Logic Model:
This model creates a diagram of the program and allowsthe effects of a proposed change to be determined. It isvery helpful for program planning and implementationmonitoring. A logic model depicts action by describingwhat the program is and what it will do – the sequenceof events that links program investments to results. Themodel as adapted by the University of Missouri has sixcomponents:
• Situation: Problem or issue that the program is toaddress sits within a setting or situation from whichpriorities are set
• Inputs: resources, contributions and investments thatare made in response to the situation. Inputs lead to
• Outputs: activities, services, events, and productsthat reach people and users. Outputs lead to
• Outcomes: results or changes for individuals, groups,agencies, communities or systems
• Assumptions: beliefs we have about the program, thepeople, the environment and the way we think theprogram is going to work
• External factors: environment in which the programexists includes a variety of external factors thatinteract with and influence the program action.
More information is at:http://outreach.missouri.edu/fcrp/evaluation/plms.htmandhttp://www.charityvillage.com/cv/research/rstrat3.html.
Below is a sample logic model using the Government ofCanada’s logic model framework.
Appendix H: Operational Planning Concepts and Tools Page 35
Appendix H
Operational Planning Concepts and Tools
Figure H1: Logic Model: Networks of Centres of Excellence
Selection of networks Program management
Increased networking and
collaboration among
researchers
Increased partnerships
between networks and
industry/ government
Transfer and exploitation of findings and
other research knowledge by
industry and government
Increased productivity and
economic growth
Improved quality
of life for Canadians
High-quality, multi-disciplinary research training,
as well as attraction and retention
of experienced researchers
Leading-edge research findings
relevant to the needs of industry
and government and Canadaí s
socio-economic development
Agreements with
networksAdvice and direction
to networksReports on awards
monitoring, performance
reviews and evaluations
Funded networks
Monitoring & evaluationACTIVITIES
OUTPUTS
IMMEDIATE
OUTCOMES
INTERMEDIATE
OUTCOMES
FINAL OUTCOMES

Context Diagram:
Linked to SWOT analysis is the context diagram. Thisdiagram is best developed by a group of personsfamiliar with the organisation and vetted by the wholegroup engaged in the strategic planning process. Oftenthose outside an organisation or system will see thecontext in a broader way than those inside, and bothinternal and external perspectives should be captured.
A context diagram is a picture of the organisation orsystem and the other groups with which it sharesrelationships and information. It can show information
flow and how well the flow is working. It can thereforehighlight areas for improvement and identifyopportunities for solidifying alliances and partnerships.
It is common to see either a diagrammatic or writtenoutline of relationships for large multi-agencyadministrations such as Canada’s Department ofNational Defence (see http://www.vcds.forces.gc.ca/dgsp/pubs/dp_m/intro_e.asp)
A simple context diagram might look like this:
Page 36 Appendix H: Operational Planning Concepts and Tools
Figure H2: A Simplified Context Diagram
thickness of arrow = volume of client flow
ACUTE
TREATMENT
PROGRAM
PRIMARY
CARE
RESOURCES
OUT-OF-AREA
REHAB
PROGRAM
REHAB
PROGRAM
POST-REHAB
SUPPORT
PROGRAMS

Activity Hierarchy:
This tool is used to visually show the activities of anorganisation, sector or system. At each level within thehierarchy, activities should be broken down into moredetailed, discrete elements that are part of the largeractivity described in the level above.
Activity hierarchies are useful for planning because theyhelp create a clear picture of what a group does, or isaccountable for doing, as part of its mandate. They canalso show the impact of change in an organisation’sactivities or help in the development of new areas ofbusiness.
The core elements of an activity hierarchy diagram are:
• description of the organisation/sector/system
• the principal areas of activity
• the more elementary or sub activities that comprisethose primary functions.
A hierarchy diagram can be organised in flow-chartformat or in pyramidal form.
Appendix H: Operational Planning Concepts and Tools Page 37
Figure H3: Ways to Present an Activity Hierarchy
ACTIVITY GROUP
ACTIVITY TYPE ACTIVITY TYPE
ACTIVITY CLASS
ACTIVITY ACTIVITY ACTIVITY ACTIVITY ACTIVITY
ACTIVITY CLASS ACTIVITY CLASS
ACTIVITY
CATEGORY
ACTIVITY
CATEGORY
ACTIVITY
CATEGORY
ACTIVITY
GROUP
ACTIVITY TYPE
ACTIVITY
ACTIVITY CATEGORY
ACTIVITY CLASS

Evaluation is a key component of planning. However asa separate module (Module 7, Assessment and
Evaluation) will deal with this area, only basicinformation is included in this appendix.
A key for success with any planning effort is to agree atthe beginning on what will be tracked and evaluated.Process evaluation can be particularly useful whenpiloting new programs. Outcome evaluation is key inunderstanding if investments are yielding the expectedresults. Both can also identify unintendedconsequences.
Types of evaluation are not primarily distinguished bythe techniques involved (for example the differencebetween questionnaires and interviews) but by theirpurpose. In the article Dimensions of Evaluation
(Oxford Centre for Staff and Learning Development,Brookes University) David Jacques presents a numberof facets of evaluations as they relate to teaching andlearning. For example it describes quantitative vs.qualitative evaluation:
• Quantitative evaluation attempts to measure orobtain a quantitative fix on what is going on. Forexample it counts instances and uses numbers as itsbaseline for comparison.
• Qualitative evaluation attempts to describe what isgoing on through observations, interviews andstories.
Other excellent sources of information on evaluation are:
• Canadian Evaluation Society publications andworkshops: www.evaluationcanada.ca
• resources found at:http://www.managementhelp.org/evaluatn/evaluatn.htm
Page 38 Appendix I: Evaluation
Appendix I
Evaluation
Notes


© 2
006,
Que
en’s
Pri
nter
for
Ont
ario














![1) Alice’s Adventures in Wonderland · PDF file1) Alice’s Adventures in Wonderland ca. 1875 Lize’s avonturen in ’t Wonderland [Lize’s adventures in the Miracleland] Nijmegen:](https://static.fdocuments.in/doc/165x107/5a7b38447f8b9a2e6e8bba0e/1-alices-adventures-in-wonderland-alices-adventures-in-wonderland-ca-1875.jpg)