
The Phenotypic Expression of Inflammatory Bowel Disease in Patients with Primary Sclerosing...
7
ORIGINAL ARTICLE The Phenotypic Expression of Inflammatory Bowel Disease in Patients with Primary Sclerosing Cholangitis Differs in the Distribution of Colitis David F. Schaeffer • Lay Lay Win • Sara Hafezi-Bakhtiari • Maria Cino • Gideon M. Hirschfield • Hala El-Zimaity Received: 23 November 2012 / Accepted: 18 April 2013 / Published online: 14 May 2013 Ó Springer Science+Business Media New York 2013 Abstract Background Inflammatory bowel disease (IBD) associ- ated with primary sclerosing cholangitis (PSC) is reported to be mild and prone to right-side predominance with rectal sparing. However, no dedicated studies evaluating patterns of presentation of liver disease with respect to IBD are available. Methods We performed a detailed histological examina- tion of the colonic biopsies in the context of PSC, identi- fying 97 patients [89 with ulcerative colitis and ten with Crohn’s disease (CD)] stratified into two groups, based on their initial disease presentation: hepatic/biliary (group 1— PSC-IBD; n = 56) versus colonic (group 2—IBD-PSC; n = 41). Results Inflammatory bowel disease that preceded PSC had a tendency to have a ‘‘pan-colitis’’ distribution; this group included all patients with CD. Inflammatory bowel disease diagnosis that followed PSC presentation was more likely to be right-sided, sparing the descending, sigmoid and rectal regions (p = 0.002). In both groups, colitis was mild with focal deep plasmacytosis and occasional mild cryptitis. Active cryptitis with crypt abscesses, surface erosion and ulceration were not identified in any of the patients. Conclusion Colitis associated with PSC shows mild dis- ease activity and the colitis pattern is associated with dis- ease presentation, i.e. colitis preceding PSC (IBD-PSC cohort) typically have a pancolitic distribution, while colitis following PSC (PSC-IBD cohort) demonstrates right-sided predominance. Awareness by pathologists and clinicians of these patterns of inflammatory bowel disease is important and of use in directing appropriate investiga- tions for patients. Keywords Ulcerative colitis Á Inflammatory bowel disease Á Primary sclerosing cholangitis Á Pancolitis Á PSC-IBD Á Colitis distribution Introduction The association of primary sclerosing cholangitis (PSC) with ulcerative colitis (UC) is long described [1]. An association with Crohn’s disease (CD) was also suggested early on, but was found to be less common than with UC [2]. More recent studies have proposed consideration of PSC-IBD as a third IBD phenotype, independent of UC and CD [2, 3]. This concept has been further strengthened by the discovery of distinctions in genetic associations for PSC and UC/CD [4]. A large PSC population-based study from the Netherlands recently also corroborated findings by demonstrating that the IBD phenotype was unique in a cohort of 579 PSC patients [5]. The prevalence rates of PSC-IBD vary considerably between different series, ranging from 80 % in northern D. F. Schaeffer Á S. Hafezi-Bakhtiari Á H. El-Zimaity (&) Department of Laboratory Medicine and Pathology, Toronto General Hospital, University of Toronto, 200 Elizabeth Street, Toronto, ON M5G 2C4, Canada e-mail: [email protected] L. L. Win Á M. Cino Liver Centre, Toronto Western Hospital, Toronto, ON, Canada M. Cino Á G. M. Hirschfield Division of Medicine, University of Toronto, Toronto, ON, Canada G. M. Hirschfield Centre for Liver Research, NIHR Biomedical Research Unit, University of Birmingham, Birmingham, UK 123 Dig Dis Sci (2013) 58:2608–2614 DOI 10.1007/s10620-013-2697-7
Transcript of The Phenotypic Expression of Inflammatory Bowel Disease in Patients with Primary Sclerosing...

ORIGINAL ARTICLE
The Phenotypic Expression of Inflammatory Bowel Diseasein Patients with Primary Sclerosing Cholangitis Differsin the Distribution of Colitis
David F. Schaeffer • Lay Lay Win •
Sara Hafezi-Bakhtiari • Maria Cino •
Gideon M. Hirschfield • Hala El-Zimaity
Received: 23 November 2012 / Accepted: 18 April 2013 / Published online: 14 May 2013
� Springer Science+Business Media New York 2013
Abstract
Background Inflammatory bowel disease (IBD) associ-
ated with primary sclerosing cholangitis (PSC) is reported
to be mild and prone to right-side predominance with rectal
sparing. However, no dedicated studies evaluating patterns
of presentation of liver disease with respect to IBD are
available.
Methods We performed a detailed histological examina-
tion of the colonic biopsies in the context of PSC, identi-
fying 97 patients [89 with ulcerative colitis and ten with
Crohn’s disease (CD)] stratified into two groups, based on
their initial disease presentation: hepatic/biliary (group 1—
PSC-IBD; n = 56) versus colonic (group 2—IBD-PSC;
n = 41).
Results Inflammatory bowel disease that preceded PSC
had a tendency to have a ‘‘pan-colitis’’ distribution; this
group included all patients with CD. Inflammatory bowel
disease diagnosis that followed PSC presentation was more
likely to be right-sided, sparing the descending, sigmoid
and rectal regions (p = 0.002). In both groups, colitis was
mild with focal deep plasmacytosis and occasional mild
cryptitis. Active cryptitis with crypt abscesses, surface
erosion and ulceration were not identified in any of the
patients.
Conclusion Colitis associated with PSC shows mild dis-
ease activity and the colitis pattern is associated with dis-
ease presentation, i.e. colitis preceding PSC (IBD-PSC
cohort) typically have a pancolitic distribution, while
colitis following PSC (PSC-IBD cohort) demonstrates
right-sided predominance. Awareness by pathologists and
clinicians of these patterns of inflammatory bowel disease
is important and of use in directing appropriate investiga-
tions for patients.
Keywords Ulcerative colitis � Inflammatory bowel
disease � Primary sclerosing cholangitis � Pancolitis �PSC-IBD � Colitis distribution
Introduction
The association of primary sclerosing cholangitis (PSC)
with ulcerative colitis (UC) is long described [1]. An
association with Crohn’s disease (CD) was also suggested
early on, but was found to be less common than with UC
[2]. More recent studies have proposed consideration of
PSC-IBD as a third IBD phenotype, independent of UC and
CD [2, 3]. This concept has been further strengthened by
the discovery of distinctions in genetic associations for
PSC and UC/CD [4]. A large PSC population-based study
from the Netherlands recently also corroborated findings by
demonstrating that the IBD phenotype was unique in a
cohort of 579 PSC patients [5].
The prevalence rates of PSC-IBD vary considerably
between different series, ranging from 80 % in northern
D. F. Schaeffer � S. Hafezi-Bakhtiari � H. El-Zimaity (&)
Department of Laboratory Medicine and Pathology, Toronto
General Hospital, University of Toronto, 200 Elizabeth Street,
Toronto, ON M5G 2C4, Canada
e-mail: [email protected]
L. L. Win � M. Cino
Liver Centre, Toronto Western Hospital, Toronto, ON, Canada
M. Cino � G. M. Hirschfield
Division of Medicine, University of Toronto, Toronto, ON,
Canada
G. M. Hirschfield
Centre for Liver Research, NIHR Biomedical Research Unit,
University of Birmingham, Birmingham, UK
123
Dig Dis Sci (2013) 58:2608–2614
DOI 10.1007/s10620-013-2697-7

Europe and North America [6] as compared to 50 % in
southern Europe [7] and 35 % in Asia [8, 9]. Treatment
guidelines for PSC, such as the American Association for
the Study of the Liver, stress the importance of screening
colonoscopy with histology, if IBD is not already known.
PSC may appear many years after proctocolectomy for
colitis, and the onset of IBD can be seen many years after
liver transplantation for PSC [10–12]. Clinically, backwash
ileitis, rectal sparing and low disease activity seem to
characterize IBD when associated with PSC [13]. The
subtleties of colitis in this context may not however always
be adequately appreciated by clinicians. We sought to
study, through detailed histopathologic review, the nature
of colitis in patients with PSC and to correlate patterns of
hepatic presentation with colonic disease activity and
extent.
Methods
Patient Selection
We identified patients with a diagnosis of PSC and IBD
from the clinical and pathology files of University Health
Network between the years 1995 and 2011. The diagnosis
of PSC required well-characterized clinical features, such
as radiological findings of beading, duct ectasia and/or
structuring of the intrahepatic or extrahepatic ducts. The
diagnosis of IBD required at least one colonoscopy with
segmental biopsies. In this study, as the use of immune-
modulatory agents to control rejection can confound
observations, we considered transplant an endpoint.
We reviewed patients’ medical records retrospectively
to determine primary disease presentation, as either hepa-
tic/biliary or colonic. We excluded patients if primary
disease presentation could not be elucidated with absolute
certainty. We collected demographic information, such as
age at IBD or PSC presentation, gender, duration of IBD,
interval between IBD and PSC or vice versa diagnosis and
history of liver transplant (see Table 1).
Histological Evaluation
All biopsies were fixed in formalin and prepared by routine
hematoxylin and eosin staining. As colitis associated with
primary sclerosing cholangitis is typically mild, we asses-
sed colonic inflammation as well as structural integrity on a
6-point grading system to help us identify small differences
(see Table 2). Assessment was made blinded to the pattern
of liver disease presentation. For the purpose of summa-
rizing disease activity a simplified grading scheme was
employed [negative (0), mild (1), moderate (2) and severe
(3)] to include overall changes in architectural distortion,
crypt destruction, erosion/ulceration, presence of plasma
cells and neutrophils. In short, scores 1 and 2 were com-
bined as mild (grade 1), scores of 3 graded as moderate
(grade 3) and scores 4 and 5 as severe (grade 3). We
considered the presence of neutrophilic inflammation evi-
dence of active disease. The presence of erosions or surface
ulceration was considered severe activity. Criteria for
chronicity included architectural distortion, basal plasma-
cytosis and Paneth cell metaplasia in the left colon. In the
left colon, deep plasmacytosis was defined as plasma cells
in the lower third of crypts (score of 2). Taking the pres-
ence of ‘‘normal’’ deep plasma cells within the cecum into
account, the scoring scale was adjusted accordingly and
only prominent lymphoplasmacytosis was considered to be
positive (score of 3 or higher) (Fig. 1; Table 2).
We separately evaluated biopsies from the terminal
ileum, caecum, ascending colon, transverse colon,
descending colon, sigmoid colon and rectum. For the
purpose of stratifying the extent of the colitis, biopsies
from the caecum and ascending colon were considered to
reflect the ‘‘right side’’. The ‘‘left side’’ was defined as
involving the transverse, descending and sigmoid colon.
An overall score was calculated per endoscopy by adding
all inflammatory scores, including acute and chronic, and
dividing by the number of specimens. The patient’s overall
inflammatory score represented the mean score of all sep-
arate endoscopies performed in this patient. Histologic
evaluation was blinded to clinical presentation, and specific
to this study.
Statistical Analysis
All scores were entered into a database and analyzed using
STATA 11 (StataCorp, College Station, TX). Fisher’s
exact test or, when appropriate the chi-square test, (both
2-tailed) were used for comparison of proportions. Statis-
tical significance of differences and relationships was
determined by p values of less than 0.05.
Ethics Approval
Ethics approval for the study was obtained from the
Research Ethics Board of the University Health Network.
Results
Patient Demographics and Clinical Features
This study included 97 patients with a diagnosis of PSC
and IBD. Of those, 56 developed colitis following the
diagnosis of primary sclerosing cholangitis (designated
PSC-IBD patient cohort). This group included 18 females
Dig Dis Sci (2013) 58:2608–2614 2609
123

(32 %) and 38 males (68 %), with an average age of
20 years at the time of PSC diagnosis (age range
11–47 years). Forty-four (79 %) patients underwent sur-
veillance colonoscopies given that there was a strong
relationship between PSC and IBD, but did not have any
GI-related symptoms. The remaining 12 (21 %) patients
presented with lower GI symptoms, such as watery or
bloody diarrhea with or without fever and abdominal pain,
prompting colonoscopic examination. The mean time
interval before the subsequent diagnosis of inflammatory
bowel disease was 1.9 years (range 0–16 years), with 51
patients (91 %) developing ulcerative colitis; only five
patients (9 %) developed Crohn’s disease. At the time of
analysis 26 patients (46 %) subsequently underwent liver
transplant for endstage PSC.
In comparison, 41 of the 97 patients developed colitis
prior to a diagnosis of primary sclerosing cholangitis
(designated the IBD-PSC group). This group had 11
females (27 %) and 30 males (73 %) with a mean age of 19
at colitis diagnosis (age range 1–59 years). Ulcerative
colitis was also more predominant in this group (36 [88 %]
had ulcerative colitis; only five patients [12 %] had Cro-
hn’s disease). The mean time interval between the initial
diagnosis of IBD and subsequent PSC was 6.1 years (range
0–29 years). In this group twenty-six patients (63 %)
underwent liver transplant.
We reviewed 1,153 endoscopic mucosal biopsies from
338 colonoscopies of the 97 patients. The number of col-
onoscopies was relatively similar between the PSC-IBD
and IBD-PSC group, as was the number of retrieved
endoscopic mucosal biopsies (see Table 1). Data on
colectomy specimen was not available for either group.
Pathological Features
Disease Activity
The study cohort showed a low overall grade of colitis. In
the PSC-IBD cohort 48 patients (86 %) displayed mild
colitis (combined grade 1) compared to 39 patients (95 %)
Table 1 Clinical features and
demographics of patient cohort
and subclassification for PSC-
IBD and IBD-PSC patients
PSC primary sclerosing
cholangitis, IBD inflammatory
bowel disease, UC ulcerative
colitis, CD Crohn’s disease, NA
not available
Characteristic Entire PSC-IBD cohort (n = 97)
Gender m:f [n (%)] 68:29 (70:30)
Age at disease onset (y; range) 19.8 (1–59)
Subtype of IBD [n (%)]
Ulcerative colitis 87 (90)
Crohn’s disease 10 (10)
Colonoscopies (n)
Total number 338
Endoscopies/patient [mean ± SD] 3.35 ± 3.25
Endoscopic mucosal biopsies (n)
Total number 1,153
Biopsies/patient (mean ± SD) 15 ± 11
Characteristic Primary liver diagnosis
[PSC-IBD; (n = 56)]
Primary colonic
diagnosis [IBD-PSC;
(n = 41)]
Gender m:f [n (%)] 38:18 (68:32) 30:11 (73:27)
Age at PSC onset (y; range) 20.3 (11–47) –
Age at IBD onset (y; range) – 19.3 (1–59)
Subtype of IBD (UC:CD) [n (%)] 51:5 (91:9) 36:5 (88:12)
Time interval between PSC and IBD
diagnosis (y) [mean (range)]
1.9 (0–16) 1.9 (0–16)
Time interval between IBD and PSC
diagnosis (y; range)
– –
Liver transplant [n (%)] 26 (46) 26 (63)
Colonoscopies (n)
Total number 186 152
Endoscopies/patient (mean ± SD) 3.9 ± 1.9 2.8 ± 4.6
Endoscopic mucosal biopsies (n)
Total number 629 524
Biopsies/patient (mean ± SD) 16 ± 12 13 ± 10
2610 Dig Dis Sci (2013) 58:2608–2614
123

in the IBD-PSC group. There was no statistically signifi-
cant difference between the groups. Importantly, none of
the study patients showed any severe activity within any
biopsy. The number of eosinophils present within the
lamina propria served as a surrogate marker for the amount
of inflammation present as demonstrated in Table 3.
Extent of Inflammatory Bowel Disease
A statistically significant higher number of IBD-PSC
patients (56 %) had a pancolitic distribution of disease than
localized to the right (20 %) or left side (24 %; p = 0.002).
This distribution was also significant (p = 0.018) when
Fig. 1 Prominent deep plasmacytosis in the lower third of crypts
(score of 3) in ascending colon [H&E 95]
Table 2 Grading scale used for histological assessment of inflam-
mation and structural damage
Grade Description
(1) Architectural change
Architectural distortion
0 Negative
1 10 % of crypts distorted
2 25 % of crypt distorted
3 50 % of crypts distorted
4 75 % of crypts distorted
5 100 % of crypts distorted
Crypt destruction
0 Negative
1 Probable—local excess
of neutrophils in part of
crypt
2 Probable—marked
attenuation
3 Unequivocal crypt
destruction \5 % of
specimen
4 Crypt destruction [5 but
\50 % of crypts
5 Crypt destruction [50 %
of crypts
Erosion or ulceration
0 No erosion The presence of erosions or
surface ulceration was
considered severe activity
1 Recovering
epithelium ? adjacent
inflammation
2 Probable erosion- focally
stripped
3 Unequivocal erosion
4 Granulation tissue or
ulcer \50 % of
specimen
5 Granulation tissue or
ulcer [50 % of
specimen
(2) Inflammatory cells
Plasma cells
0 Negative In the left colon, deep
plasmacytosis was defined as
plasma cells in the lower third
of crypts (score of 2). In the
caecum and ascending colon,
deep plasma cells had to be
more extensive to be
considered positive (score of 3
or higher)
1 Lower 1/3 loose
2 Lower 1/3 compact
3 Lower third and beyond
in \5 % of specimen
Table 2 continued
Grade Description
4 [5 % but \50 %
5 [ 50 %
Neutrophils (PMN)
0 Negative
1 PMNs in lamina propria
or surface epithelium
2 Cryptitis but no crypt
abscess
3 Cryptitis abscesses \5 %
of crypts
4 Cryptitis abscesses[5 but
\50 % of crypts
5 Cryptitis abscesses
[50 % of crypts
Paneth cell metaplasia
1 If present on left side
To summarize the overall disease activity, we converted the 6-point
scale to a 4-point colitis grade as follows: scores 1 and 2 = mild
(grade 1), scores 3 = moderate (grade 2) and scores 4 and 5 = severe
(grade 3)
Dig Dis Sci (2013) 58:2608–2614 2611
123
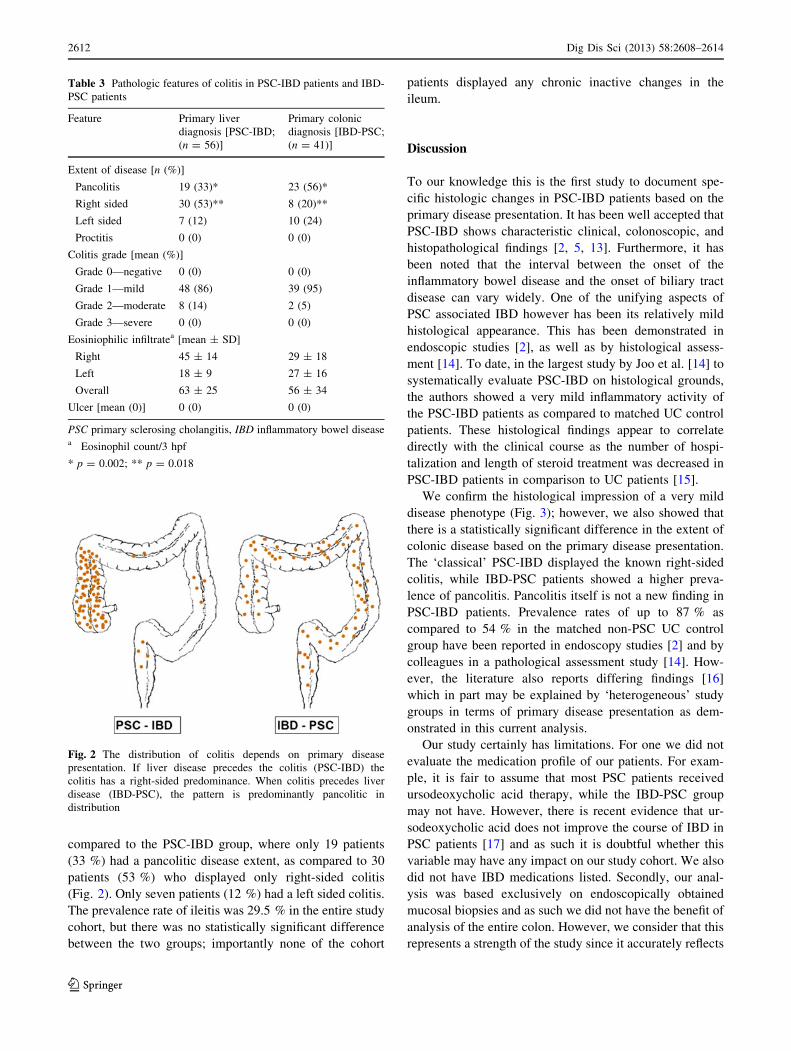
compared to the PSC-IBD group, where only 19 patients
(33 %) had a pancolitic disease extent, as compared to 30
patients (53 %) who displayed only right-sided colitis
(Fig. 2). Only seven patients (12 %) had a left sided colitis.
The prevalence rate of ileitis was 29.5 % in the entire study
cohort, but there was no statistically significant difference
between the two groups; importantly none of the cohort
patients displayed any chronic inactive changes in the
ileum.
Discussion
To our knowledge this is the first study to document spe-
cific histologic changes in PSC-IBD patients based on the
primary disease presentation. It has been well accepted that
PSC-IBD shows characteristic clinical, colonoscopic, and
histopathological findings [2, 5, 13]. Furthermore, it has
been noted that the interval between the onset of the
inflammatory bowel disease and the onset of biliary tract
disease can vary widely. One of the unifying aspects of
PSC associated IBD however has been its relatively mild
histological appearance. This has been demonstrated in
endoscopic studies [2], as well as by histological assess-
ment [14]. To date, in the largest study by Joo et al. [14] to
systematically evaluate PSC-IBD on histological grounds,
the authors showed a very mild inflammatory activity of
the PSC-IBD patients as compared to matched UC control
patients. These histological findings appear to correlate
directly with the clinical course as the number of hospi-
talization and length of steroid treatment was decreased in
PSC-IBD patients in comparison to UC patients [15].
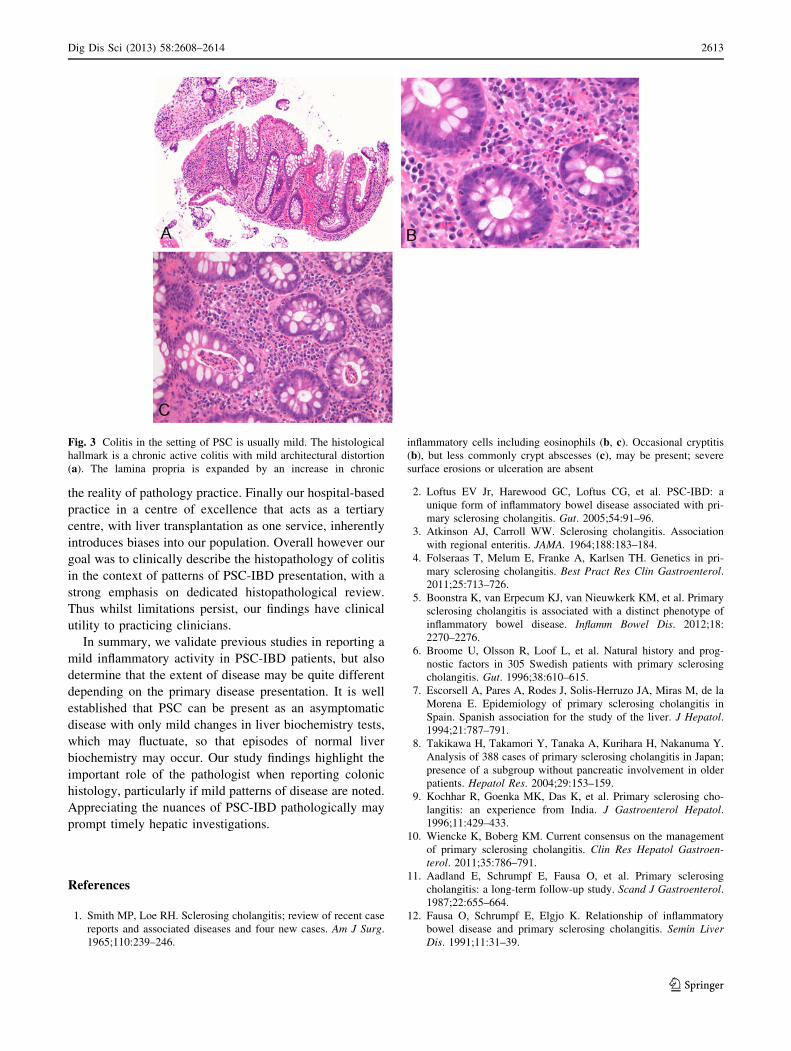
We confirm the histological impression of a very mild
disease phenotype (Fig. 3); however, we also showed that
there is a statistically significant difference in the extent of
colonic disease based on the primary disease presentation.
The ‘classical’ PSC-IBD displayed the known right-sided
colitis, while IBD-PSC patients showed a higher preva-
lence of pancolitis. Pancolitis itself is not a new finding in
PSC-IBD patients. Prevalence rates of up to 87 % as
compared to 54 % in the matched non-PSC UC control
group have been reported in endoscopy studies [2] and by
colleagues in a pathological assessment study [14]. How-
ever, the literature also reports differing findings [16]
which in part may be explained by ‘heterogeneous’ study
groups in terms of primary disease presentation as dem-
onstrated in this current analysis.
Our study certainly has limitations. For one we did not
evaluate the medication profile of our patients. For exam-
ple, it is fair to assume that most PSC patients received
ursodeoxycholic acid therapy, while the IBD-PSC group
may not have. However, there is recent evidence that ur-
sodeoxycholic acid does not improve the course of IBD in
PSC patients [17] and as such it is doubtful whether this
variable may have any impact on our study cohort. We also
did not have IBD medications listed. Secondly, our anal-
ysis was based exclusively on endoscopically obtained
mucosal biopsies and as such we did not have the benefit of
analysis of the entire colon. However, we consider that this
represents a strength of the study since it accurately reflects
Table 3 Pathologic features of colitis in PSC-IBD patients and IBD-
PSC patients
Feature Primary liver
diagnosis [PSC-IBD;
(n = 56)]
Primary colonic
diagnosis [IBD-PSC;
(n = 41)]
Extent of disease [n (%)]
Pancolitis 19 (33)* 23 (56)*
Right sided 30 (53)** 8 (20)**
Left sided 7 (12) 10 (24)
Proctitis 0 (0) 0 (0)
Colitis grade [mean (%)]
Grade 0—negative 0 (0) 0 (0)
Grade 1—mild 48 (86) 39 (95)
Grade 2—moderate 8 (14) 2 (5)
Grade 3—severe 0 (0) 0 (0)
Eosiniophilic infiltratea [mean ± SD]
Right 45 ± 14 29 ± 18
Left 18 ± 9 27 ± 16
Overall 63 ± 25 56 ± 34
Ulcer [mean (0)] 0 (0) 0 (0)
PSC primary sclerosing cholangitis, IBD inflammatory bowel diseasea Eosinophil count/3 hpf
* p = 0.002; ** p = 0.018
Fig. 2 The distribution of colitis depends on primary disease
presentation. If liver disease precedes the colitis (PSC-IBD) the
colitis has a right-sided predominance. When colitis precedes liver
disease (IBD-PSC), the pattern is predominantly pancolitic in
distribution
2612 Dig Dis Sci (2013) 58:2608–2614
123
the reality of pathology practice. Finally our hospital-based
practice in a centre of excellence that acts as a tertiary
centre, with liver transplantation as one service, inherently
introduces biases into our population. Overall however our
goal was to clinically describe the histopathology of colitis
in the context of patterns of PSC-IBD presentation, with a
strong emphasis on dedicated histopathological review.
Thus whilst limitations persist, our findings have clinical
utility to practicing clinicians.
In summary, we validate previous studies in reporting a
mild inflammatory activity in PSC-IBD patients, but also
determine that the extent of disease may be quite different
depending on the primary disease presentation. It is well
established that PSC can be present as an asymptomatic
disease with only mild changes in liver biochemistry tests,
which may fluctuate, so that episodes of normal liver
biochemistry may occur. Our study findings highlight the
important role of the pathologist when reporting colonic
histology, particularly if mild patterns of disease are noted.
Appreciating the nuances of PSC-IBD pathologically may
prompt timely hepatic investigations.
References
1. Smith MP, Loe RH. Sclerosing cholangitis; review of recent case
reports and associated diseases and four new cases. Am J Surg.
1965;110:239–246.
2. Loftus EV Jr, Harewood GC, Loftus CG, et al. PSC-IBD: a
unique form of inflammatory bowel disease associated with pri-
mary sclerosing cholangitis. Gut. 2005;54:91–96.
3. Atkinson AJ, Carroll WW. Sclerosing cholangitis. Association
with regional enteritis. JAMA. 1964;188:183–184.
4. Folseraas T, Melum E, Franke A, Karlsen TH. Genetics in pri-
mary sclerosing cholangitis. Best Pract Res Clin Gastroenterol.
2011;25:713–726.
5. Boonstra K, van Erpecum KJ, van Nieuwkerk KM, et al. Primary
sclerosing cholangitis is associated with a distinct phenotype of
inflammatory bowel disease. Inflamm Bowel Dis. 2012;18:
2270–2276.
6. Broome U, Olsson R, Loof L, et al. Natural history and prog-
nostic factors in 305 Swedish patients with primary sclerosing
cholangitis. Gut. 1996;38:610–615.
7. Escorsell A, Pares A, Rodes J, Solis-Herruzo JA, Miras M, de la
Morena E. Epidemiology of primary sclerosing cholangitis in
Spain. Spanish association for the study of the liver. J Hepatol.
1994;21:787–791.
8. Takikawa H, Takamori Y, Tanaka A, Kurihara H, Nakanuma Y.
Analysis of 388 cases of primary sclerosing cholangitis in Japan;
presence of a subgroup without pancreatic involvement in older
patients. Hepatol Res. 2004;29:153–159.
9. Kochhar R, Goenka MK, Das K, et al. Primary sclerosing cho-
langitis: an experience from India. J Gastroenterol Hepatol.
1996;11:429–433.
10. Wiencke K, Boberg KM. Current consensus on the management
of primary sclerosing cholangitis. Clin Res Hepatol Gastroen-
terol. 2011;35:786–791.
11. Aadland E, Schrumpf E, Fausa O, et al. Primary sclerosing
cholangitis: a long-term follow-up study. Scand J Gastroenterol.
1987;22:655–664.
12. Fausa O, Schrumpf E, Elgjo K. Relationship of inflammatory
bowel disease and primary sclerosing cholangitis. Semin Liver
Dis. 1991;11:31–39.
Fig. 3 Colitis in the setting of PSC is usually mild. The histological
hallmark is a chronic active colitis with mild architectural distortion
(a). The lamina propria is expanded by an increase in chronic
inflammatory cells including eosinophils (b, c). Occasional cryptitis
(b), but less commonly crypt abscesses (c), may be present; severe
surface erosions or ulceration are absent
Dig Dis Sci (2013) 58:2608–2614 2613
123

13. Sano H, Nakazawa T, Ando T, et al. Clinical characteristics of
inflammatory bowel disease associated with primary sclerosing
cholangitis. J Hepatobiliary Pancreat Sci. 2011;18:154–161.
14. Joo M, Abreu-e-Lima P, Farraye F, et al. Pathologic features of
ulcerative colitis in patients with primary sclerosing cholangitis: a
case-control study. Am J Surg Pathol. 2009;33:854–862.
15. Moayyeri A, Daryani NE, Bahrami H, Haghpanah B, Nayyer-
Habibi A, Sadatsafavi M. Clinical course of ulcerative colitis in
patients with and without primary sclerosing cholangitis. J Gas-
troenterol Hepatol. 2005;20:366–370.
16. Penna C, Dozois R, Tremaine W, et al. Pouchitis after ileal
pouch-anal anastomosis for ulcerative colitis occurs with
increased frequency in patients with associated primary scleros-
ing cholangitis. Gut. 1996;38:234–239.
17. Lindstrom L, Boberg KM, Wikman O, et al. High dose ursode-
oxycholic acid in primary sclerosing cholangitis does not prevent
colorectal neoplasia. Aliment Pharmacol Ther. 2012;35:451–457.
2614 Dig Dis Sci (2013) 58:2608–2614
123


















