![Modified Weibull Distribution: Ordinary Differential Equations · 2018-12-07 · inverse survival function, probability density function, Weibull. the ones proposed by [30] and [31].](https://static.fdocuments.in/doc/165x107/5f3b522a2826065a115d0c58/modified-weibull-distribution-ordinary-differential-2018-12-07-inverse-survival.jpg)
THE PERFORMANCE OF INVERSE PROBABILITY OF TREATMENT ...
26
THE PERFORMANCE OF INVERSE PROBABILITY OF TREATMENT WEIGHTING AND PROPENSITY SCORE MATCHING FOR ESTIMATING MARGINAL HAZARD RATIOS By Jonatan Nåtman Department of Statistics Uppsala University Supervisor: Harry Khamis 2019
Transcript of THE PERFORMANCE OF INVERSE PROBABILITY OF TREATMENT ...
THE PERFORMANCE OF INVERSEPROBABILITY OF TREATMENT
WEIGHTING AND PROPENSITY SCOREMATCHING FOR ESTIMATINGMARGINAL HAZARD RATIOS
By Jonatan Nåtman
Department of Statistics
Uppsala University
Supervisor: Harry Khamis
2019

ABSTRACT
Propensity score methods are increasingly being used to reduce the effect of measured con-
founders in observational research. In medicine, censored time-to-event data is common. Using
Monte Carlo simulations, this thesis evaluates the performance of nearest neighbour matching
(NNM) and inverse probability of treatment weighting (IPTW) in combination with Cox pro-
portional hazards models for estimating marginal hazard ratios. Focus is on the performance
for different sample sizes and censoring rates, aspects which have not been fully investigated in
this context before. The results show that, in the absence of censoring, both methods can reduce
bias substantially. IPTW consistently had better performance in terms of bias and MSE com-
pared to NNM. For the smallest examined sample size with 60 subjects, the use of IPTW led to
estimates with bias below 15 %. Since the data were generated using a conditional parametri-
sation, the estimation of univariate models violates the proportional hazards assumption. As a
result, censoring the data led to an increase in bias.
Keywords: Monte Carlo simulations, propensity score, survival analysis, Cox model, censor-
ing rate, sample size

Contents
1 Introduction 1
2 Background 2
2.1 Causal Inference and the Potential Outcome Framework . . . . . . . . . . . . 2
2.2 Propensity Score Methods . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
2.2.1 Matching on the Propensity Score . . . . . . . . . . . . . . . . . . . . 4
2.2.2 Inverse Probability of Treatment Weighting . . . . . . . . . . . . . . . 5
2.3 Survival Analysis and the Cox Proportional Hazards model . . . . . . . . . . . 5
2.4 Previous Research . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
3 Methodology 7
3.1 Data Generating Processes . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
3.1.1 Scenario A . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
3.1.2 Scenario B . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
3.1.3 Scenario C . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
3.1.4 Censoring Times . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
3.1.5 Conditional Treatment Effect . . . . . . . . . . . . . . . . . . . . . . . 9
3.2 Simulation Design . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
3.3 Estimation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
4 Results 12
5 Discussion 19
2

1 Introduction
Randomised control trials (RCTs) are generally seen as the gold standard in medical research.
If treatment assignment is random, the treatment status should not be confounded with either
measured or unmeasured baseline characteristics. In some situations randomised controlled
studies cannot be conducted for ethical reasons. Research based on observational data also has
several advantages compared to randomised studies. The study subjects have not undergone
a strict selection procedure and might be more representative of the reality. The increasing
amount of register data also makes it possible to conduct medical studies at a lower cost, partic-
ularly when studying rare events or if long follow-up times are needed. The main disadvantage
of observational studies where the treatment assignment has not been randomised is the risk of
confounders that can make causal inference difficult.
Propensity score methods are increasingly being used to minimise the effects of confound-
ing when using observational data to estimate the effect of different treatments or exposures.
Censored time-to-event data are common in medical research. The effect of a treatment on
survival is often described with both a relative and an absolute measure in the biomedical lit-
erature, where hazard ratios and survival curves are the most commonly used measures. In
recent years, the performance of different propensity score methods to estimate hazard ratios
and survival curves have been examined in several simulation studies. These studies have fo-
cused on relatively large samples of 1000 or 10 000 subjects. Propensity score methods are
typically used in register based research where large amounts of data are available. However,
these methods are also often used for substantially smaller samples, for example when studying
patient groups with rare diseases. Also, the effect of censoring have not been fully investigated
in previous studies.
The aim of this thesis is to examine the performance of the most commonly used propen-
sity score methods in combination with Cox proportional hazards model to estimate marginal
hazard ratios. The main research question is "What is the behaviour of bias and MSE of 1:1
greedy nearest neighbour matching, with and without calipers, and inverse probability of treat-
ment weighting, when estimating marginal hazard ratios? We will focus on the performance
for different sample sizes and different censoring rates. When estimating the propensity scores,
four different models will be considered: i) a model including only the true confounder(s), ii)
a model including all variables related to outcome, iii) a model including all variables related
to treatment selection, and iiii) a model including all variables related to either outcome or
1

treatment selection. As a second question we will examine which of these models results in
estimates of marginal hazard ratios with the lowest bias and MSE.
The outline of the thesis is as follows. Section 2 provides an introduction to the theoretical
framework of this thesis. First, the potential outcome framework is presented followed by a
description of the propensity score methods. In the second part of section 2, the Cox propor-
tional hazards model is presented. Finally, a brief review of the previous research on propensity
score methods to estimate marginal hazard ratios is given. Section 3 describes the design of the
simulation study, followed by a presentation of the results in section 4. In the final part, section
5, the results are summarised and discussed.
2 Background
2.1 Causal Inference and the Potential Outcome Framework
The Rubin causal model and the concept of potential outcomes was introduced by Rubin1. Let
Zi denotes the treatment status of a subject ( Zi = 0 if the subject was assigned to the control
group and Zi = 1 if the subject received the treatment). This framework then assumes that
each subject has two potential outcomes. The first potential outcome, Yi(0), is the outcome
that would have been observed if the subject did not receive the treatment. The second, Yi(1),
is the outcome that would have been observed if the subject received the treatment. For each
subject, the individual treatment effect could then be defined as the difference between the two
potential outcomes: π1 = Yi(0)− Yi(1). However, only one of the potential outcomes can be
observed.
The average treatment effect (ATE) is the average effect of moving an entire population
from untreated to treated, expressed as E[Yi(0) − Yi(1)]. A different measure of the effect is
the treatment effect for the treated (ATT), E[Yi(0)−Yi(1)|Z = 1]. This measure describes the
average treatment effect in the population that was ultimately treated. In a randomised study,
the two measures will be equal. In an observational study however, there is no reason to expect
the ATE and ATT to be equal and which of the two measures is of greater interest depends on
the study question.
With time-to-event data, the average treatment effect would be the mean difference in sur-
vival times that results from the treatment. However, medical researchers are often more in-
terested in measures such as the difference in the probability of observing an event within a
2

specified follow-time or in the relative effect described by hazard ratios. In this thesis, which
focuses on estimating hazard ratios, we will use Austin’s2 modified definitions of ATE and
ATT. In the following sections, ATE will refer to the hazard ratio that would have been ob-
tained by regressing the hazard function on a treatment indicator in a dataset consisting of both
potential outcomes of all subjects. Similarly, ATT will be used to refer to the same analysis but
restricted to the population of subjects that actually received the treatment.
2.2 Propensity Score Methods
The propensity score is the probability of treatment assignment conditional on observed base-
line characteristics, ei = Pr(Zi = 1|Xi). Rosenbaum and Rubin3 showed that adjustment for
the propensity score is sufficient to remove bias due to measured confounders. In an obser-
vational study the propensity score is generally unknown and needs to be estimated. Several
methods can be used but the most common is estimation using logistic regression.
There is a discussion on how to select the propensity score model. The advice by Rubin
and Thomas4 is to include all variables that are related to the outcome, regardless of whether
they are related to exposure. Variables that are related only to exposure should not be included.
This is also the conclusion from two simulation studies5,6. This strategy for variable selection
might seem counter-intuitive but has been motivated by the notion that even if a variable is
theoretically unrelated to the exposure, there is a possibility that it is related to the exposure
by chance in the dataset. If that is the case, the variable will be a confounder in that particular
dataset. On the other hand, including a variable that is strongly related to treatment selection
but unrelated to the outcome will induce variability to the propensity score model that does not
correct for confounding5 .
When the propensity score has been estimated, there are four broad methods to adjust for it:
matching on the propensity score, stratification on the propensity score, covariate adjustment
using the propensity score and inverse probability of treatment weighting (IPTW)3,7. All of
these methods have been applied to survival data and have recently been evaluated in simula-
tion studies. It has been showed that matching and IPTW estimate marginal effects whereas
stratification and covariate adjustment estimate conditional effect8,9. Therefore, this thesis will
focus on propensity score matching and IPTW.
3

2.2.1 Matching on the Propensity Score
Matching on the propensity score means that a matched set is formed of treated and untreated
subjects that have similar values of the propensity score. There are several ways to implement
propensity score matching and Austin2 gives a good overview of different algorithms. The
most common implementation is to form pairs of treated and control subjects, which is called
one-to-one (1:1) matching. Another approach is one-to-many (1:M), where one treated subject
is matched to two or more control subjects. Full matching is another method that makes use
of all individuals in the data by forming matched sets of one treated subject and one or more
controls. Full matching can estimate both ATE and ATT whereas 1:1 matching always targets
ATT2. We will focus only on 1:1 matching, which is the most commonly used method for
propensity score matching.
A matching algorithm also needs to be chosen. The two most common are optimal match-
ing and greedy nearest neighbour matching (NNM)2. The first aims to minimise the average
difference in propensity score within the matched pairs. The latter, on the other hand, finds one
treated subject and then selects the untreated subject with closest propensity score as control.
The greedy matching algorithm chooses the order in which the treated subjects are matched
either randomly, sequentially from lowest to highest propensity or from highest to lowest, or
by the order of how close the best match is.
It is also common to put restrictions on the quality of the matches. This is called nearest
neighbour matching with calipers. Caliper matching is similar to NNM but if there is no un-
treated subject with a propensity score within a specified distance from the selected treated sub-
ject, the treated subject will not be included in the matched sample and the analysis. Austin10
recommends using a caliper of 0.2 standard deviations of the logit of the propensity score. The
choice of using calipers or not represents a trade off between two sources of bias. If no re-
strictions are put on the quality of the matches, or if the calipers are wide, the distribution of
propensity scores between the treated group and the control group might still differ substan-
tially after matching. If calipers are used, some treated subjects might get excluded from the
analysis and thus changing the target population.
Austin11 compared several different 1:1 matching algorithms in a simulation study where
differences in means were estimated. It was found that optimal matching had no advantage
over greedy NNM in achieving balance in the baseline covariates. NNM with calipers resulted
in estimates with less bias but slightly higher variability than NNM without restriction. For
4
greedy NNM, the order in which the treated subjects were selected did not have any particular
effect on estimation. Also, matching with replacement did not have better performance than
matching without replacement. Based on this, they recommend using NNM with calipers and
random order.
Two different methods for matching will be evaluated in this study: 1:1 greedy nearest
neighbour matching, with and without calipers.
2.2.2 Inverse Probability of Treatment Weighting
Inverse probability of treatment weighting (IPTW) uses the propensity score to compute weights.
These weights are used to construct a synthetic sample where the distribution of measured co-
variates is independent of treatment assignment. The weights can be chosen so they represent
different target populations, either to target the ATE or the ATT. We will focus on the ATT
weights since this is the measure that the 1:1 matching targets. Let Zi be the treatment indi-
cator and ei be the estimated propensity score for the ith subject . The ATT weights are then
given by
wi = Zi +ei(1− Zi)(1− ei)
. (1)
Thus, all treated subjects are given a weight of 1 and the subjects in the control group are
given a weight of ei/(1− ei).
2.3 Survival Analysis and the Cox Proportional Hazards model
Survival analysis, also called time-to-event analysis, is a collection of statistical procedures for
analysing data where the variable of interest is the time until an event occurs. The event of
interest can be for example death or relapse from remission. A common feature of these data is
that observations are censored. Censoring is a type of missing data problem that can occur due
to several reasons. In medicine, a frequent type is right censoring which means that all that is
known is that subject is still alive at a given time. Right censoring can for example occur when
the study is terminated before all subjects have experienced the event or if a subject leaves the
study before having experienced the event. Then we will only know that the subject was still
alive when it was censored but not the time when the event was experienced.
When analysing the effect of a treatment, usually both an absolute and a relative measure
of the effect is of interest. The techniques that are most commonly used to deal with censored
5

time-to-event data is the Kaplan-Meier estimator, which estimates the survival function, and
Cox proportional hazards (PH) model, which is used to model the effect of covariates on the
hazard rate. The hazard function is defined
h(t) = lim∆t→0
P[t ≤ T < t+ ∆t|T ≥ t]
∆t(2)
which is the probability that a subject will not survive for an additional time ∆t given that
it has survived until time t.
In the Cox PH model12, the effect of a one unit increase in a covariate has a multiplicative
effect on the hazard rate
h(t;X) = h0(t)eθZ+Xβ (3)
where h(t;X) is the hazard function at time t, h0(t) is the baseline hazard, θ is the treatment
effect, Z the treatment indicator, X is a vector of covariates and β is a vector of parameters.
The Cox PH model is semi-parametric since the functional form of the baseline hazard does
not need to be specified.
In the Cox model, θ is the treatment effect conditional on the covariates X. A measure of
an effect is said to be collapsible if the marginal and the conditional effect coincide in absence
of confounding13. That is true for linear models but not for hazard ratios or odds ratios in
general14. Regardless of whether X is related to Z, controlling for X will infer different
estimands. While conditional effects denote an average effect at the individual level, marginal
effects denote an effect at the population level. Thus, the marginal effect is the hazard ratio
of two identical populations, except that in one population all subjects received treatment and
in the other everyone was untreated. In that sense, adjusting for covariates at the design stage
by propensity score methods and controlling for the covariates in the regression analysis will
estimate different effects.
A key assumption of the Cox PH model is the proportional hazard assumption, meaning
that the effect of a covariate is constant over time. Chastang et al.15 showed that omission of
a covariate in a Cox PH model can cause bias, even if the covariate is completely balanced
between the treatment and the control groups. This results from the hazards in the two groups
no longer being proportional if a prognostic variable is omitted from the model. Even when the
PH assumption is violated, the estimate from a Cox model can still be useful. It can be seen as
6
a geometric average of the treatment effect over the support of the data. However, this estimate
will be a function of the distribution of censoring times16.
2.4 Previous Research
Gayat et al.8 evaluate the performance of stratification on the propensity score, covariate ad-
justment using the propensity score and propensity score matching. They concludled that the
methods, except matching, estimated conditional effects rather than marginal effects. How-
ever, matching on the propensity score gave unbiased estimates of the marginal hazard ratio.
The methods were evaluated with sample sizes of 1000 subjects and a censoring rate of 40 %.
They also investigated the effect of an unmeasured confounder. The unmeasured confounder
led to substantially biased estimates but replacing the unmeasured confounder with a highly
correlated variable could remove most of the bias.
Austin9 compares the performance of IPTW and propensity score matching for estimat-
ing marginal hazard ratios in a simulation study of several scenarios of different hazard ratios
and prevalences of exposure. It was found that both methods yield approximately unbiased
estimates of the effect in the treated population. IPTW had lower mean squared errors and
the difference between the methods increased when the prevalence of exposure was low. The
methods were evaluated in samples of 10 000 subjects and the data were not censored.
Pirracchio et al.6 examined the performance of IPTW and propensity score matching for
estimation of odds ratios in case of small samples. They found that both methods could yield
estimates with less than 10 % bias for sample sizes from 1000 down 40 subjects. IPTW had
better performance of bias and MSE except when the sample size was 40. For the smallest
sample size, matching yielded estimates with slightly lower bias.
3 Methodology
A Monte Carlo simulation study was performed to evaluate the behaviour of bias and MSE
when using propensity score methods to estimate marginal hazard ratios. To examine the per-
formance of the methods under different conditions, we used three slightly modified data gen-
erating processes to represent different situations. These simulated situations will be referred
to as Scenario A, B and C. In each scenario, samples of different sizes were generated. Also,
censoring times were simulated from different distributions. In each simulated data set, the
7

propensity score methods were applied separately and marginal Cox PH models were fitted.
The estimates were compared to the true treatment effect. Here follows a detailed description
of the simulation design and the estimation methods.
3.1 Data Generating Processes
3.1.1 Scenario A
Three baseline covariates, X1, X2 and X3, were simulated from independent standard normal
distributions. Of these, the first two affected treatment selection whereas the last two affected
the outcome. Thus, X2 is the only true confounder.
Each subject’s probability of being assigned to treatment was simulated using a logistic model
logit(pi) = log(α0) + log(α1)x1i + log(α2)x2i (4)
where α1 = α2 = 2 and α0 was chosen so that 30% of the subjects were treated. The treat-
ment status for each subject was then generated from a Bernoulli distribution with individual
parameter pi.
The event times were generated following the technique described by Bender et al.17. First,
a linear predictor was defined
LPi = θZi + log(β2)x2i + log(β3)x3i (5)
.
where β2 and β3 also were set to 2. These parameters were chosen so that the variables
should have a substantial impact on treatment selection and/or outcome.
The time-to-event, T, was simulated by inverting the cumulative hazard function of a
Weibull distribution,
Ti =
(−log(ui)
λexp(LPi)
)1/η
(6)
where ui ∼ U(0, 1). The scale parameter λ and the shape parameter η were set to 2 and
0.00002 respectively, as have been done in other studies9,18.
8

3.1.2 Scenario B
In Scenario B, a second confounder was added. Four variablesX1, ..., X4, were simulated from
independent standard normal distributions. Now, X1, ..., X3 affected treatment selection and
X2, ..., X4 affected the outcome. Thus, X2 and X3 are confounders.
The probability of assignment was simulated as in Scenario A, but adding the third variable
to the data generating process
logit(pi) = log(α0) + log(α1)x1i + log(α2)x2i + log(α3)x3i (7)
.
Also in this scenario, α0 was chosen so that 30% of the subjects received treatment. Event
times were generated as in Scenario A, with the variable X4 added to the linear predictor
LPi = θZi + log(β2)x2i + log(β3)x3i + log(β4)x4i (8)
.
Again, the parameters α1, ..., α3 and β2, ..., β4 were set to 2.
3.1.3 Scenario C
Scenario C is also a slightly modified version of Scenario A. However, α0 was changed so that
10% of the subjects received treatment. In all other aspects, the data generating processes were
the same as in Scenario A with three simulated variables of which one was a true confounder.
3.1.4 Censoring Times
To simulate censoring times Ci, two different distributions were used. First, censoring was
simulated from the Weibull distribution. The shape parameter η was set to 0.00002 and the
scale parameter λ was changed to obtain the desired censoring rate. A uniform distribution was
also considered, where Ci ∼ unif(0, b), changing the parameter b to obtain different rates.
3.1.5 Conditional Treatment Effect
Since the survival times were generated from a conditional model, exp(θ) is the conditional
treatment effect. An iterative bisection method was used to determine the conditional effect
9

Table 1: Summary of simulation settings
Scenario Data generating process Number ofconfounders
Samplesizes
Prevalenceof treatment
A logit(pi) = α0 + log(2)x1i + log(2)x2i 1 60,...,1000 30 %LPi = θZi + log(2)x2i + log(2)x3i
B logit(pi) = α0 + log(2)x1i + log(2)x2i + log(2)x3i 2 60,...,1000 30 %LPi = θZi + log(2)x2i + log(2)x3i + log(2)x4i
C logit(pi) = α0 + log(2)x1i + log(2)x2i 1 180,...,3000 10 %LPi = θZi + log(2)x2i + log(2)x3i
that induced the desired marginal hazard ratio. This method is described in detail by Austin to
generate data with a specified marginal odds ratio and has also been applied to hazard ratios9,19.
Briefly, a data set of 1000 subjects was simulated. For each treated subject, the two potential
outcomes were generated as described above. However, the survival times were not censored
since it most often is the true uncensored effect that is of scientific interest. Survival times
were then regressed on the treatment indicator using Cox regression. Over 10 000 replications,
the mean of the parameter estimates was taken as the true marginal hazard ratio in the treated
population corresponding to the conditional effect θ. We then searched for the value of θ that
gave the desired marginal hazard ratio.
3.2 Simulation Design
The true marginal hazard ratio was chosen to be 1.5. This was obtained by setting the condi-
tional hazard ratio exp(θ) ≈ 1.859 in Scenario A, exp(θ) ≈ 1.983 in Scenario B and exp(θ) ≈
1.864 in Scenario C. Seven different censoring distributions were simulated: the situation of no
censoring and censoring rates of 20% , 40% and 50% from uniform and Weibull distributions,
respectively. In each combination of censoring distribution and Scenario A-C, samples of dif-
ferent sizes were generated. In Scenario A and B, the samples ranged from 1000 down to 60
subjects (n = 1000, 900, 800, 700, 600, 500, 400, 300, 200, 180 , 160, 140, 120, 100, 80, 60).
In order to get a reasonable number of observations in the treated group in Scenario C, we mul-
tiplied the total sample sizes by three (n ranging from 3000 down to 180). Thus, the expected
number of treated subject were the same as in the other two scenarios. A summary of the three
scenarios is presented in Table 1.
10

3.3 Estimation
Within each simulated data set, the propensity scores were estimated using logistic regression.
The propensity scores were estimated using four different models: a model including only the
true confounder(s) (M1), a model including the variables related to outcome only (M2), a model
including the variables related to treatment selection only (M3) and finally a model including
all variables related to either outcome or treatment (M4).
The three different propensity score methods were applied: i)1:1 greedy nearest neigh-
bour matching (NNM), ii) 1:1 greedy nearest neighbour matching within a caliper 0.2 st.d. of
the logit of the propensity score (Caliper matching) and iii) inverse probability of treatment
weighting (IPTW). In the matched samples, a univariate Cox PH model was used to regress
time-to-event on the treatment indicator. For IPTW, a Cox PH model was also used to regress
time-to-event on the treatment indicator, including the ATT weights as sample weights. For
comparison, also an unadjusted model in the original sample was estimated (crude model), as
well as a correctly specified conditional model (adjusted model). Since we suspect that the
marginal hazards might violate the PH assumption we will check the proportionality by also
estimating hazard ratios for different time intervals.
The methods were evaluated with relative bias and mean squared error (MSE) on the log-
hazard scale
Bias =1
5000
5000∑i=1
δ̂i − δδ
(9)
MSE =1
5000
5000∑i=1
(δ̂i − δ)2 (10)
where δ̂i is the estimated log-hazard ratio of the ith simulated dataset and δ is the true
marginal log-hazard ratio in the treated population. When evaluating the conditional model, δ
was defined as the true conditional effect.
All simulations were performed in R version 3.5.1. The function glm was used to fit logistic
regressions to estimate the propensity scores. The function Match in the package Matching was
used for matching on the propensity score. To estimate Cox proportional hazard models, coxph
in the survival package was used.
11
4 Results
For each propensity score method, four different logistic models were considered when es-
timating the propensity score: a model including only the true confounder(s) (M1), a model
including all variables related to the outcome (M2), a model including all variables related to
treatment selection (M3) and a model including all variables related to either treatment selec-
tion or outcome (M4). In terms of bias, the differences between the four models were small
for Caliper matching and IPTW. M1 and M2 had slightly lower bias than M3 and M4. The
differences between the models were larger for NNM, where M1 and M2 produced less biased
estimated than did M3 and M4. There were however no large differences between M1 and
M2. When comparing MSE, M2 was better than the other three models in all cases but a few
exceptions across all simulations. There were no clear patterns in the relative performance of
the four models across the three simulated scenarios, sample sizes or censoring distributions.
In the remainder of this thesis, we will focus on the results produced by the model including all
variables related to the outcome, M2.
Table 2 shows some descriptive statistics, averaged over the 5000 Monte Carlo replica-
tions, that describes the quality of the matching methods and the IPTW. Since censoring does
not have any impact on the estimation of the propensity scores, only the results for the data
simulated in the case of no censoring are presented. First, in Scenario A with n = 1000,
95.7 % of the the treated subjects were successfully matched to a control subject with similar
propensity score when calipers were applied. As the sample size decreases, so does the share
of matched subjects. Thus, there is a relatively low risk of bias due to incomplete matching
when n = 1000, but the risk increases as the sample size decreases. In Scenario B, where a
second confounder is added, a lower share of the subjects are matched compared to Scenario
A with only one confounder. In Scenario C, 10 % of the subjects received the treatment. The
relatively larger number of control subjects makes it easier to find a match within the specified
calipers. Compared to Scenario A, only a small number of treated subjects are excluded from
the analysis. In NNM, all treated subjects are included in the analysis. Without any restriction
on the quality of the matches, there are no guarantees that the distribution of the covariates
will be similar in the matched sample. The second panel in Table 2 shows the difference in
means between the treated group and the control group in the matched sample, averaged over
the Monte Carlo replications. The variable that is related to treatment only is not included in
the propensity score model and the imbalance between the groups remains after matching. The
12
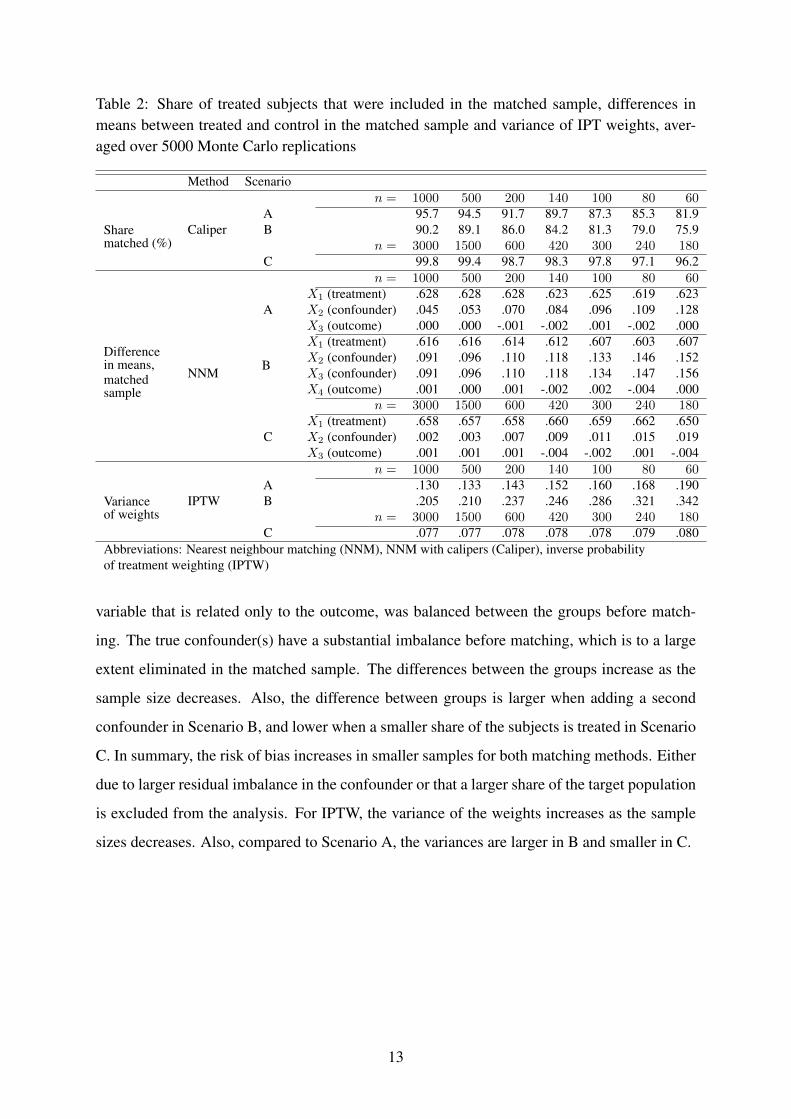
Table 2: Share of treated subjects that were included in the matched sample, differences inmeans between treated and control in the matched sample and variance of IPT weights, aver-aged over 5000 Monte Carlo replications
Method Scenarion = 1000 500 200 140 100 80 60
Sharematched (%)
CaliperA 95.7 94.5 91.7 89.7 87.3 85.3 81.9B 90.2 89.1 86.0 84.2 81.3 79.0 75.9
n = 3000 1500 600 420 300 240 180C 99.8 99.4 98.7 98.3 97.8 97.1 96.2
n = 1000 500 200 140 100 80 60
Differencein means,matchedsample
NNM
AX1 (treatment) .628 .628 .628 .623 .625 .619 .623X2 (confounder) .045 .053 .070 .084 .096 .109 .128X3 (outcome) .000 .000 -.001 -.002 .001 -.002 .000
B
X1 (treatment) .616 .616 .614 .612 .607 .603 .607X2 (confounder) .091 .096 .110 .118 .133 .146 .152X3 (confounder) .091 .096 .110 .118 .134 .147 .156X4 (outcome) .001 .000 .001 -.002 .002 -.004 .000
n = 3000 1500 600 420 300 240 180
CX1 (treatment) .658 .657 .658 .660 .659 .662 .650X2 (confounder) .002 .003 .007 .009 .011 .015 .019X3 (outcome) .001 .001 .001 -.004 -.002 .001 -.004
n = 1000 500 200 140 100 80 60
Varianceof weights
IPTWA .130 .133 .143 .152 .160 .168 .190B .205 .210 .237 .246 .286 .321 .342
n = 3000 1500 600 420 300 240 180C .077 .077 .078 .078 .078 .079 .080
Abbreviations: Nearest neighbour matching (NNM), NNM with calipers (Caliper), inverse probabilityof treatment weighting (IPTW)
variable that is related only to the outcome, was balanced between the groups before match-
ing. The true confounder(s) have a substantial imbalance before matching, which is to a large
extent eliminated in the matched sample. The differences between the groups increase as the
sample size decreases. Also, the difference between groups is larger when adding a second
confounder in Scenario B, and lower when a smaller share of the subjects is treated in Scenario
C. In summary, the risk of bias increases in smaller samples for both matching methods. Either
due to larger residual imbalance in the confounder or that a larger share of the target population
is excluded from the analysis. For IPTW, the variance of the weights increases as the sample
sizes decreases. Also, compared to Scenario A, the variances are larger in B and smaller in C.
13
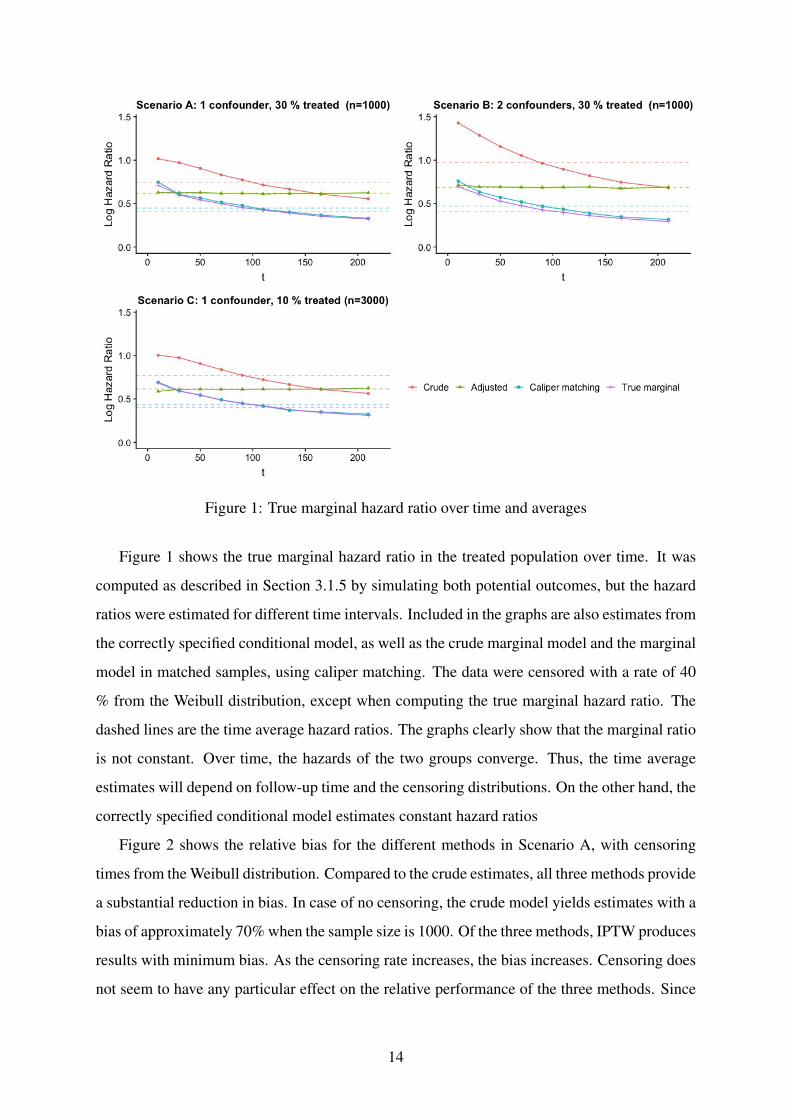
Figure 1: True marginal hazard ratio over time and averages
Figure 1 shows the true marginal hazard ratio in the treated population over time. It was
computed as described in Section 3.1.5 by simulating both potential outcomes, but the hazard
ratios were estimated for different time intervals. Included in the graphs are also estimates from
the correctly specified conditional model, as well as the crude marginal model and the marginal
model in matched samples, using caliper matching. The data were censored with a rate of 40
% from the Weibull distribution, except when computing the true marginal hazard ratio. The
dashed lines are the time average hazard ratios. The graphs clearly show that the marginal ratio
is not constant. Over time, the hazards of the two groups converge. Thus, the time average
estimates will depend on follow-up time and the censoring distributions. On the other hand, the
correctly specified conditional model estimates constant hazard ratios
Figure 2 shows the relative bias for the different methods in Scenario A, with censoring
times from the Weibull distribution. Compared to the crude estimates, all three methods provide
a substantial reduction in bias. In case of no censoring, the crude model yields estimates with a
bias of approximately 70% when the sample size is 1000. Of the three methods, IPTW produces
results with minimum bias. As the censoring rate increases, the bias increases. Censoring does
not seem to have any particular effect on the relative performance of the three methods. Since
14
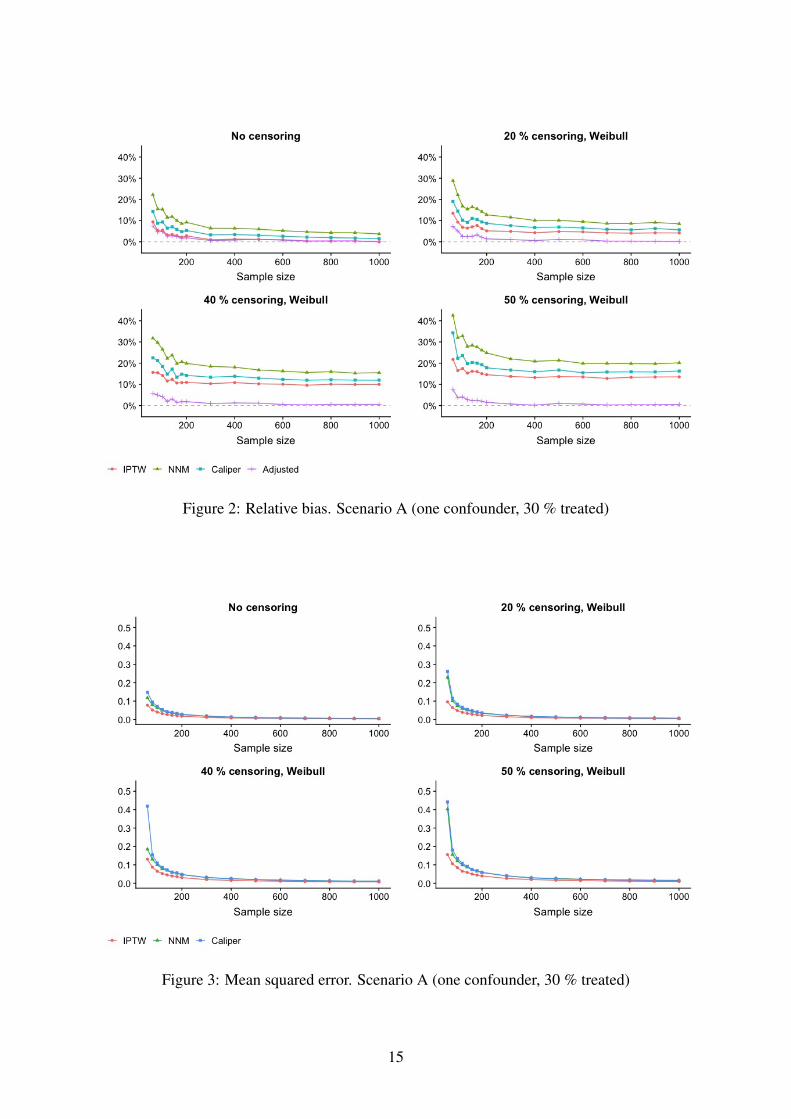
Figure 2: Relative bias. Scenario A (one confounder, 30 % treated)
Figure 3: Mean squared error. Scenario A (one confounder, 30 % treated)
15

the marginal hazards in the groups are nonproportional, the time average estimates are expected
to be a function of the censoring distribution. If subjects with longer survival times are more
likely to be censored, the hazard ratios at later time points will get a smaller weight in the
average hazard ratio. Since the hazards are convergent, this will result in overestimation of
the average hazard ratio. Similar shifts in the bias were obtained when censoring times were
simulated from a uniform distribution, however the shifts were slightly smaller. The bias of the
adjusted conditional model is not affected by the censoring distribution. Note however that this
model estimates and was compared to a different effect.
The mean squared errors for Scenario A are presented in Figure 3. Also in terms of MSE,
IPTW yields the best results. NNM and Caliper matching have similar MSE. As the sample
size gets smaller, the MSE of caliper matching increase sligtly more rapidly.
In Scenario B, where a second confounder is added, Figure 4 shows that bias increase for all
models. Also in this scenario, IPTW has the best performance for all sample sizes. Compared
to Scenario A, the use of calipers when constructing the matched sample seems to have a larger
effect on reducing the bias. Also in Scenario B, censoring of the data causes similar shifts in
the bias curves. The MSE, presented in Figure 5, shows that IPTW have the best performance
across all sample sizes. Caliper have lower MSE compared to NNM, except for the smallest
sample sizes.
Figure 6 shows the relative bias for Scenario C. Also in this scenario, IPTW has the lowest
bias. However, the differences between the three methods are small. When the sample size is
180, with 18 treated subjects on average, the bias of IPTW is 5.5 % in case of no censoring.
The MSE are presented in Figure 7. NNM and caliper matching have similar values for all
sample sizes. IPTW have the smallest MSE, approximately half of those for NNM and caliper
matching, and the difference gets larger for the smallest sample sizes. Thus, the variance of
the IPTW estimates seems to be less sensitive to sample size. The bias and MSE are almost
identical for NNM and caliper matching.
More comprehensive results are available on request: [email protected].
16

Figure 4: Relative bias. Scenario B (two confounders, 30 % treated)
Figure 5: Mean squared error. Scenario B (two confounders, 30 % treated)
17

Figure 6: Relative bias. Scenario C (one confounder, 10 % treated)
Figure 7: Mean squared error. Scenario C (one confounder, 10 % treated)
18

5 Discussion
In this thesis we have evaluated the performance of inverse probability of treatment weight-
ing (IPTW) and nearest neighbour matching (NNM), with and without calipers, to estimate
marginal hazard ratios (MHR) of a treatment effect in the treated population. The methods
were evaluated based on bias and MSE in a series of simulations.
First we examined different models to estimate the propensity score. It was confirmed
that for all three propensity score methods, the model that included all variables related to the
outcome, regardless of whether they were confounders, had the best performance. These results
are in agreement with other simulation studies5,6. All further comparisons of the propensity
score methods were based on this model.
The results show that the propensity score methods can adjust for measured confounders
and produce approximately unbiased estimates of MHRs in the absence of censoring. IPTW
had better performance across sample sizes and the different data-generating processes com-
pared to the matching methods, both in terms of bias and MSE. When there was one confounder,
IPTW produced estimates with bias of less than 10 % for sample sizes down to 60 subjects.
Adding a second confounder to the data-generating process resulted in slightly higher biases
for all methods. When a smaller proportion of the subjects received treatment, the differences
in bias and MSE between the methods decreased. Thus, a relatively large number of control
subjects was more important when using the matching methods. As the sample size decreased,
the bias increased for all methods. For the matching methods, it is possible that it is more
difficult to find a control subject with similar propensity score in a smaller sample. A possible
explanation for the increase in bias for IPTW could be the larger variability of the weights in
the smaller samples. Comparing the larger sample sizes, these results are in agreement with
Austin’s9 who simulated data without censoring and with sample sizes of 10 000 subjects.
When the data were censored, this introduced bias that increased with the censoring rate. It
has been showed by Chastang et al.15 that the PH assumption is violated, even if a completely
balanced covariate is omitted from the Cox PH model. When examining the proportionality of
the hazards, it was confirmed that conditional hazards were proportional whereas the marginal
hazards were convergent. This increase in bias is likely a result of the nonproportionality of the
hazards. When the hazards are nonproportional, the hazard ratios from the Cox PH regression
can be interpreted as a geometric average, weighted by the number of observations at each time
point. When the censoring rate was 50 %, the maximum increase in bias was about 15 percent-
19
age points. Gayat et al.8 simulated data with sample sizes of 1000 subjects and evaluated NNM.
With 40 % censoring rate they found, unlike this study, that it had approximately unbiased esti-
mates of the marginal hazard ratio. The differences between their results and the current study
could perhaps be due to that they took the censoring distribution into account when computing
the true marginal hazard ratio by simulating both potential outcomes and censoring the data.
Even if treatment assignment were completely randomised in a RCT, a marginal Cox model
would still yield estimates with similar bias, if the survival data came from the same conditional
model with the same distribution of censoring times. Three reviews of randomised clinical trials
recently published in oncology journals show that treatment effects are often evaluated using
marginal Cox models20–22. Also, the PH assumption was only justified or discussed in few of
the articles. As previous studies have noted, the propensity score methods estimates marginal
rather than conditional effects9. Although not specifying the correct conditional model violates
the assumptions of the Cox regression, propensity score methods can be a useful alternative to
estimate similar effects to those that are commonly reported in RCTs.
Aalen et al.23 discuss a problem of randomisation with the Cox model. Even if the treat-
ment assignment is randomised at the start of the study, this randomisation is lost by implicit
conditioning as soon has the first event occurs if the outcome model is not correctly specified.
Thus, the marginal hazards in these simulations might lack a clear causal interpretation.
There are certain limitations in this study. Since the models have been evaluated based on
simulations, it is difficult to know how generalisable the results are to other situations than the
specific settings in these simulations. For example, there could be different numbers of co-
variates or distributions of the covariates such as binary or correlated variables, different sizes
of treatment effects and other prevalences of treatment. Also, in reality it is unlikely that all
confounders are measured. However, these methods are difficult to evaluate analytically and
simulation studies are important in order to understand under which conditions the methods
work well. There are also several other matching algorithms, such as matching with replace-
ment, that perhaps could have given different results.
In summary, IPTW had consistently the lowest bias and MSE across the simulations. IPTW
and the matching methods had most similar performance when both sample size and the ratio
of the number of control to treated subjects were large. IPTW was less sensitive to sample size
and the number of control subjects.
20
References
1 Rubin D. Estimating causal effects of treatments in randomised and nonrandomised studies.
Journal of Educational Psychology. 1974 mar;66(6):688–701.
2 Austin PC. The use of propensity score methods with survival or time-to-event outcomes:
reporting measures of effect similar to those used in randomized experiments. Statistics
in Medicine. 2014 mar;33(7):1242–1258. Available from: https://www.ncbi.nlm.nih.gov/
pmc/articles/PMC4285179/.
3 Rosenbaum PR, Rubin DB. The central role of the propensity score in observational studies
for causal effects. Biometrika. 1983;70(1):41–55. Available from: https://academic.oup.
com/biomet/article/70/1/41/240879.
4 Rubin DB, Thomas N. Matching Using Estimated Propensity Scores: Relating Theory to
Practice. Biometrics. 1996 mar;52(1):249.
5 Brookhart MA, Schneeweiss S, Rothman KJ, Glynn RJ, Avorn J, Stürmer T. Vari-
able selection for propensity score models. American journal of epidemiology. 2006
jun;163(12):1149–56. Available from: https://www.ncbi.nlm.nih.gov/pubmed/16624967.
6 Pirracchio R, Resche-Rigon M, Chevret S. Evaluation of the Propensity score methods
for estimating marginal odds ratios in case of small sample size. BMC Medical Research
Methodology. 2012 dec;12(1):70. Available from: https://www.ncbi.nlm.nih.gov/pubmed/
22646911.
7 Rosenbaum PR. Model-Based Direct Adjustment. Journal of the American Statistical
Association. 1987 jun;82(398):387. Available from: https://www.jstor.org/stable/2289440.
8 Gayat E, Resche-Rigon M, Mary JY, Porcher R. Propensity score applied to survival data
analysis through proportional hazards models: a Monte Carlo study. Pharmaceutical Statis-
tics. 2012 may;11(3):222–229. Available from: http://doi.wiley.com/10.1002/pst.537.
9 Austin PC. The performance of different propensity score methods for estimating marginal
hazard ratios. Statistics in Medicine. 2013 jul;32(16):2837–2849. Available from: http:
//doi.wiley.com/10.1002/sim.5705.
21

10 Austin PC. Optimal caliper widths for propensity-score matching when estimating dif-
ferences in means and differences in proportions in observational studies. Pharmaceutical
Statistics. 2011 mar;10(2):150–161. Available from: http://doi.wiley.com/10.1002/pst.433.
11 Austin PC. A comparison of 12 algorithms for matching on the propen-
sity score. Statistics in medicine. 2014 mar;33(6):1057–69. Available from:
http://www.ncbi.nlm.nih.gov/pubmed/24123228http://www.pubmedcentral.nih.gov/
articlerender.fcgi?artid=PMC4285163.
12 Cox DR. On collapsibility and confounding bias in Cox and Aalen regression models.
Journal of the Royal Statistical Society. 1972;66(34):187–220.
13 Greenland S, Robins JM, Pearl J. Confounding and Collapsibility in Causal Inference;
1999. 1. Available from: https://projecteuclid.org/euclid.ss/1009211805.
14 Martinussen T VS. On collapsibility and confounding bias in Cox and Aalen regression
models. Lifetime data analysis. 2013 jun;66(9):279–96.
15 Chastang C, Byar D, Piantadosi S. A quantitative study of the bias in estimating the
treatment effect caused by omitting a balanced covariate in survival models. Statistics in
Medicine. 1988 dec;7(12):1243–1255. Available from: http://doi.wiley.com/10.1002/sim.
4780071205.
16 Boyd AP, Kittelson JM, Gillen DL. Estimation of treatment effect under non-
proportional hazards and conditionally independent censoring. Statistics in medicine. 2012
dec;31(28):3504–15. Available from: http://www.ncbi.nlm.nih.gov/pubmed/22763957http:
//www.pubmedcentral.nih.gov/articlerender.fcgi?artid=PMC3876422.
17 Bender R, Augustin T, Blettner M. Generating survival times to simulate Cox proportional
hazards models. Statistics in Medicine. 2005 jun;24(11):1713–1723. Available from: http:
//doi.wiley.com/10.1002/sim.2059.
18 Austin PC, Stuart EA. The performance of inverse probability of treatment weighting and
full matching on the propensity score in the presence of model misspecification when es-
timating the effect of treatment on survival outcomes. Statistical Methods in Medical Re-
search. 2017;26(4):1654–1670.
22

19 Austin PC, Stafford J. The Performance of Two Data-Generation Processes for Data with
Specified Marginal Treatment Odds Ratios. Communications in Statistics - Simulation and
Computation. 2008 may;37(6):1039–1051. Available from: http://www.tandfonline.com/
doi/abs/10.1080/03610910801942430.
20 Rulli E, Ghilotti F, Biagioli E, Porcu L, Marabese M, D’Incalci M, et al. Assess-
ment of proportional hazard assumption in aggregate data: a systematic review on sta-
tistical methodology in clinical trials using time-to-event endpoint. British Journal of
Cancer. 2018 dec;119(12):1456–1463. Available from: http://www.nature.com/articles/
s41416-018-0302-8.
21 Chai-Adisaksopha C, Iorio A, Hillis C, Lim W, Crowther M. A systematic review of using
and reporting survival analyses in acute lymphoblastic leukemia literature. BMC Hema-
tology. 2016 dec;16(1):17. Available from: http://bmchematol.biomedcentral.com/articles/
10.1186/s12878-016-0055-7.
22 Batson S, Greenall G, Hudson P. Review of the Reporting of Survival Anal-
yses within Randomised Controlled Trials and the Implications for Meta-Analysis.
PloS one. 2016;11(5):e0154870. Available from: http://www.ncbi.nlm.nih.gov/pubmed/
27149107http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=PMC4858202.
23 Aalen OO, Cook RJ, Røysland K. Does Cox analysis of a randomized survival study yield a
causal treatment effect? Lifetime Data Analysis. 2015 oct;21(4):579–593. Available from:
https://www.ncbi.nlm.nih.gov/pubmed/26100005.
23