
The Pearls and Pitfalls of Diagnostic Allergy Testing (Ann Allergy Asthma Immunol 2008;101:580)...
66
The Pearls and Pitfalls of Diagnostic Allergy Testing (Ann Allergy Asthma Immunol 2008;101:580) Developed by the ACAAI/AAAAI Specific IgE Test Task Force (SETTaF) © 2010, AAAAI/ACAAI/JCAAI
Transcript of The Pearls and Pitfalls of Diagnostic Allergy Testing (Ann Allergy Asthma Immunol 2008;101:580)...

The Pearls and Pitfalls of Diagnostic Allergy Testing (Ann Allergy Asthma Immunol 2008;101:580)
Developed by the ACAAI/AAAAI Specific IgE Test Task Force (SETTaF)© 2010, AAAAI/ACAAI/JCAAI

3rd National Health and Nutrition Examination Survey Test Results:Test Results: Positive allergy skin tests very common Positive allergy skin tests very common
2
Arbes et al., J Allergy Clin Immunol 2005;116:377-83
10,508 subjects in general US population tested to 10 allergens from 1988 through 1994
54% positive to ≥ 1 allergen Mean = 3.5Median = 3.0

Common Allergic Diseases Seen in the Primary Care Office
• Atopic Dermatitis/Eczema
• Food Allergy
• Allergic Rhinitis
• Allergic Asthma

Clinical History of Allergic Disease
Collecting an optimal history for allergic disease involves determining the symptom complex, its relationship to allergen exposure and then a careful physical examination looking for the specific signs of allergy
Factors Potentially Influencing the Patient’s History
• Recognition of Symptoms: recall bias related missing data, lack of knowledge or ability to accurately describe symptoms
• Environment: rural, suburban, urban, pet ownership, smoking
• Allergen Exposure: Time between exposure and symptom recognition, exposure route (ingestion, inhalation, injection, adsorption)
• Demographics: age (adult vs child-parent), gender, social economic status, language, race, family history of atopy
• Prevalence of allergic disease in question in the population.
Why Test For Specific IgE? Isn’t the Clinical History Good Enough?
• History alone is insufficient to diagnose specific allergen sensitivity
• Allergy tests help direct and optimize management• If non-atopic: results will allow you to focus on other
etiologies
• If atopic: will provide guidance for appropriate treatment
• Inappropriate treatment recommendations may result if allergen sensitivity is based on history alone
• This may cause unnecessary environmental controls and patient costs or failure to implement appropriate environmental controls
6

Tests Performed in the Diagnostic Tests Performed in the Diagnostic Allergy LaboratorAllergy Laboratory
• Allergen-specific IgE (over 200 allergen extracts)
– Pollen (weeds, grasses, trees),
– Epidermals, dust mites, molds, cockroach
– Foods,
– Venoms,
– Drugs,
– Occupational allergens (e.g., natural rubber latex)
• Total Serum IgE (anti-IgE; ABPA)
• Multi-allergen screen for IgE antibody
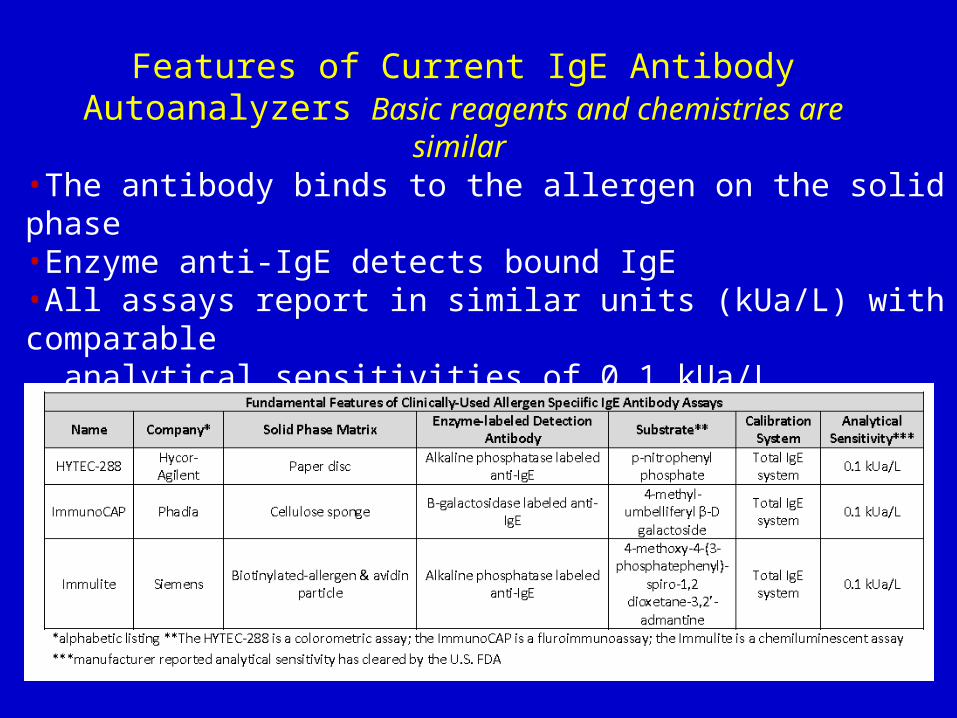
Features of Current IgE Antibody Autoanalyzers Basic reagents and chemistries are similar
•The antibody binds to the allergen on the solid phase •Enzyme anti-IgE detects bound IgE•All assays report in similar units (kUa/L) with comparable analytical sensitivities of 0.1 kUa/L•All assays primarily use allergens from extracts

Allergy Skin Testing• Skin testing remains the central test to confirm allergic
sensitivity when it can be performed 1
• Skin testing is fast (15-30 minutes), safe, sensitive and involves minimally invasive procedures which can be cost effective
• When performed correctly, skin testing is reproducible• Skin testing has demonstrated good correlation with
results of nasal challenge2 and bronchial challenges 3
• Results of skin test should always be used as an adjunct to the clinical history and physical examination when making the diagnosis of allergic disease
1. Oppenheimer et al, Ann Allergy 2006;S1:6-122. Bousquet et al, Clin Allergy 17:529-36, 19873. Cockcroft et al, Am Rev Respir Dis 135:264-7., 1987
Clinical Sensitivity & Specificity of Skin Tests
• Prick skin tests may be positive in individuals who are without respiratory symptoms:• 42% with a positive family history for asthma or rhinitis may
have + SPT and no disease• 29% of those with a negative family history for asthma or
rhinitis may have +SPT• Always use caution when interpreting skin tests; skin tests are a
confirmatory diagnostic tool reflecting sensitization and do not make the diagnosis of clinical allergy, which is based on:• Diagnosis of clinical allergy = history and confirmatory
allergy diagnostic tests.
Adinoff et al, J Allergy Clin Immunol 1990;86:766-74.

Utility of Food Allergy Testing
• Differentiate “allergy” from other adverse reactions
– ~3-5% affected by an immune response
– ~20% avoid food for perceived adverse reactions
– non-allergic adverse reactions include: intolerance (lactase deficiency), toxic effects (food poisoning), pharmacologic effects (caffeine)
• Confirm a food as a cause of a typical allergic reaction when food is a suspected trigger
– e.g., urticaria, angioedema, wheezing, anaphylaxis proximate to ingestion

Serological Evaluation for Sensitization to Food
Limitations
– Cost
– Does not assist in diagnosis on non-IgE mediated food hypersensitivity reactions
• Enterocolitis, enteropathy, proctocolitis
– Identifies sensitization but not intrinsically diagnostic of clinical reactivity (in most cases)
• Modest sensitivity/specificity lead to false positive and false negative
• Requires experienced clinician to optimally interpret data

Food-specific Ige Antibody Concentrations or Skin Test Size Correlate with Risk of Clinical Reactivity
Curve varies by:•Food•Disease•Age•Assay (brand)
Negative test is not zero risk
At certain high IgE values, the chance of a clinical reaction approaches certaintyOne study, one test brand, children age 5: Egg- 7 kIU/LMilk 15 kIU/L, Peanut 14 kIU/L
Sampson HA.. J Allergy Clin Immunol 2001;107:891-6.

Food specific IgE Predictive Values Vary by Age
• Results from 861 milk and 764 egg oral food challenges (Japanese children)
Komata . J Allergy Clin Immunol 2007;119:1272-4
Egg Milk

50% and 95% Predictive Value for Food Specific-IgE and SPT
Nowak-WÄ et al, Work Group report: Oral food challenge testing. J Allergy Clin Immunol 2009; 123:S365-S83.
Food specific-IgE measured with ImmunoCap™ and SPT with lancet (ref 17 & 21,) and bifurcated needle (ref 22)
Food Specific-IgE Test Limitations
• Cross-reactivity (among foods/with pollen) may result in clinically irrelevant positive tests
• Results do not predict severity
THEREFORE: – Avoid indiscriminate “panels” of
screening tests– Apply “prior probability” (reasoning from the
history) for test selection and interpretation

Example-Anaphylaxis
• 37 year old male with allergic rhinitis has anaphylaxis from an almond cookie purchased in a bakery.
• “Nut panel” results (kIU/L): cashew < 0.35, walnut-<0.35, pecan < 0.35, peanut-2.34, almond-3.7, hazelnut 35.3.
• Told to avoid peanut, hazelnut and almond
• Pitfalls – Additional history reveals prior tolerance of peanut and almonds
but mild past symptoms from cashew and pistachio
– Bakery uses cashew and pistachio in the almond cookies.
– Patient has birch pollen and grass pollen allergy so cross reactive proteins in these pollens with peanut, hazelnut and almond drive positive tests that, in this situation, were not relevant (but he admits mild itchy mouth with almond and peach)
– Repeat serum test shows pistachio IgE 1.2 kIU/L. Skin test by allergist is positive to cashew. PATIENT MUST AVOID CASHEW/PISTACHIO
• Lessons
– History is paramount
– Test has modest sensitivity and specificity
– Influence of cross-reactivity
– Care in tests using “panels”.

The Importance of “Prior Probability”
The test result to egg is moderately positive and in various studies indicates a 50% risk of reaction
• HISTORY #1: Patient eats egg and test was done to evaluate hyperactivity prior probability was zero, conclusion not allergic (no reason to test)
• HISTORY #2: Patient reacted to egg ingestion with hives and wheezing 3 weeks ago and 6 months ago prior probability was extremely high, test is now “diagnostic” Avoid egg
• HISTORY #3: Patient has recalcitrant atopic dermatitis prior probability and test moderate elimination diet/oral food challenge to secure a diagnosis

Additional Pearls for Food Testing
• Egg white is the major egg allergen (typically no need to test yolk, whole egg)
• Cow milk is a good test for cow milk allergy, no advantage to test milk proteins (alpha lactalbumin) or foods (cheese)
• There are no reliable tests for IgE antibody to additives/colors
• Clinical cross reactivity rates are often lower than test results would indicate (e.g., a peanut allergic individual often [>50%] tests positive to multiple legumes but reaction rates are ~5%)
• Persons with pollen allergies may test positive to numerous fruits/vegetables that may induce no or mild (oral) symptoms, but only rarely severe reactions

Which Clinical Conditions Should be Referred to an Allergy Specialist?
Insect sting anaphylaxis and bothersome large local reactions
Persistent asthmatics with exposure to a perennial allergen (NIH
expert panel (EPR-3) guidelines)
Atopic dermatitis: to identify food and/or inhalant allergen triggers
Food allergy: to determine causative allergen and plan avoidance
Allergic rhinitis: to identify triggers for effective environmental control
planning and monitoring
For consideration of allergen immunotherapy :
Incomplete control with medications and/or environmental control
measures.
Potential disease modifying
Preventive role of allergen immunotherapy

Conclusion
Selection of allergy diagnostic tests and
interpretation of specific IgE antibody results MUST
be directed, guided, and viewed within the context of the patient’s clinical history


Allergic Rhinitis: Current Approaches
David BK Golden, MD
Sinai Hospital Franklin Square Hospital Johns Hopkins University


A 27 year old man has progressively worse sneezing and itchy eyes occurring at work and now in the evenings too. In the past month he developed a dry cough disrupting work and sleep. Last week he became short of breath with exercise. He moved to this home last year and works in an modular office with 30 other people. He should now:
Eliminate the cat Skin test for inhalant allergens
Eliminate the carpets Begin a nasal steroid
Get a humidifier Begin antihistamine daily
Test for mold Begin immunotherapy
ALLERGIC RHINITIS CASE HISTORY

Prevalence of AR
• Up to 40 million Americans affected by AR1
• 6th most prevalent chronic illness1
• Prevalence estimates in adults: 10%-30%1
• Prevalence estimates in children: up to 40%1
– Most common chronic condition in children1
• Substantial increases in the prevalence of AR in developed countries in recent decades1-3
1. US Dept of Health and Human Services. Evid Rep Technol Assess. 2002 May;(54):1-198. AHRQ Pub No 02-E024.
2. Linneberg A et al. Allergy. 2000;55(8):767-772.3. Sibbald B et al. Br J Gen Pract. 1990;40(337):338-340.

Quality of Life Burden of AR• AR is associated with
– Fatigue and daytime sleepiness1,2
– Daily activity impairment3,4
– Reduced work productivity3-5
– Impaired cognitive functioning6,7
– Reduced learning abilities8
– Impaired sleep9
– Impaired disease-related quality of life2
1. Marshall PS et al. Psychosom Med. 2002;64(4):684-691.2. Stuck BA et al. J Allergy Clin Immunol. 2004;113(4):663-668.3. Bousquet J et al. J Allergy Clin Immunol. 2006;117(1):158-162.4. Tanner LA et al. Am J Manag Care. 1999;5(suppl 4):S235-S247.5. Blanc PD et al. J Clin Epidemiol. 2001;54(6):610-618.6. Wilken JA et al. Ann Allergy Asthma Immunol. 2002;89(4):372-380.7. Marshall PS et al. Ann Allergy Asthma Immunol. 2000;84(4):403-410.8. Vuurman EFPM et al. Ann Allergy. 1993;71(2):121-126.9. Léger D et al. Arch Intern Med. 2006;166(16):1744-1748.

In Chronic Rhinitis, Nonallergic Rhinitis Is a Major Causative Factor
Pure Nonallergic Rhinitis23%
Pure Allergic Rhinitis43%Mixture of
Both Allergic and Nonallergic Rhinitis 34%
National Rhinitis Classification Task Force Survey Results
57%*
Berger et al. J Managed Care Pharmacy. 2001;7(suppl):4-13.
* This percentage extrapolates to an estimated 39 million patients in the United States.
Results based on a survey of 975 patients entering allergists’ offices for chronic rhinitis. Patients were evaluated and classified into one of three groups: pure allergic, pure nonallergic, or mixed nonallergic and allergic.

Allergic Rhinitis: Comorbid Conditions
• Asthma• Sinusitis• Otitis media• Sleep disorders• Nasal Polyposis• Allergic conjunctivitis• Upper respiratory infection• Depression
AAAAI. The Allergy Report 2000. www.aaaai.orgSpector SL. J Allergy Clin Immunol 1997;99:S773-80

Association of Asthma and Rhinitis
Adapted from Guerra et al. J Allergy Clin Immunol. 2002;109:419-425.
Ad
just
ed O
dd
s R
atio
*
*Adjusted for years of follow-up, sex, age, atopic status, IgE tertiles, smoking status, and COPD.

Downloaded from: Middleton's Allergy Principles and Practice (on 11 November 2007 12:18 AM)
© 2007 Elsevier
Nasal Breathing Inhibits Bronchospasm in Exercise-induced Asthma

Allergic ResponseEarly-phase Reaction• Occurs within
minutes of allergen exposure
• Mast cell degranulation
• Inflammatory mediators (eg, histamine, tryptase, PDG2, leukotrienes)
Late-phase Reaction• Occurs within 2-4
hours and lasts up to 24 hours
• Leukocytes (eg, Th2 cells, eosinophils) gradually infiltrate tissue and activate
• Inflammatory mediators released
AAAAI. The Allergy Report 2000. www.aaaai.orgDykewicz et al. Ann Allergy Asthma Immunol 1998;81:478-518
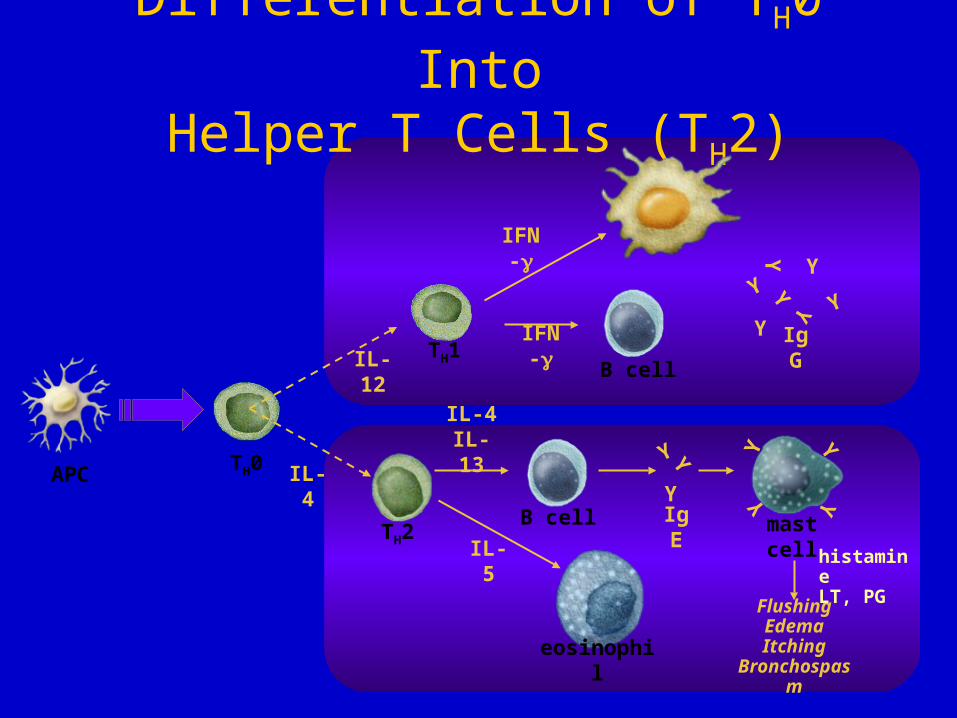
Differentiation of TH0 IntoHelper T Cells (TH2)
Y Y
Y
YY
Y
Y
IgG
YY
YIgE
YYY
Y
mast cell
FlushingEdemaItching
Bronchospasm
histamineLT, PG
APC
eosinophil
B cell
B cell
TH2
TH1
TH0
IL-12
IL-4
IFN-
IFN-
IL-5
IL-4IL-13

Management of Allergic Rhinitis
• Avoidance• Immunotherapy• Pharmacotherapy
– Intranasal corticosteroids– Nonsedating antihistamines– Leukotriene antagonists– Decongestants– Intranasal antihistamines


Inhibition of Wheal and Flare: Cetirizine HCl and Fexofenadine
Purohit A et al. Ann Allergy Asthma Immunol. 2001;86:387-392.
Randomized, double-blind, single-dose, crossover study
N = 26 healthy adults Duration of treatment effect was
defined as duration of wheal inhibition by > 70%.
Results Maximal wheal inhibition with
cetirizine achieved at 4 hours postdose
Cetirizine had a much longer duration of effect in inhibiting the wheal reaction19 hrs cetirizine8.5 hrs fexofenadine 120 mg9.3 hrs for fexofenadine180 mg
At 24 hours, only cetirizine inhibited > 60% of wheal response
In this study, low incidence of side effects for all drugs
0
20
40
60
80
100
0 0.5 1 2 4 6 8 10 12 24
Wh
eal A
rea
(mm
2)
Hours
Placebo
Fexofenadine 120 mg
Fexofenadine 180 mg
Cetirizine HCl 10 mg

Environmental Exposure Unit: Evaluating Effects of Medication on Subjects Exposed to an Allergen
Day JH et al. Ann Allergy Asthma Immunol. 1997;79:163-172.Day JH et al. Ann Allergy Asthma Immunol. 1997;79:163-172.
Feeder
Seating AreaSeating Area
T
V
T
V
3F
Enter/Exit
Directional-Type Fans
Box Fans
Rotorod Sampler
Directional-Type Fans
Box Fans
Rotorod Sampler
Actual EEU Unit
F2
F1
R3
R2
R1

Day JH et al. J Allergy Clin Immunol. 1998;101:638-645.Day JH et al. Ann Allergy. 2001;87:474-481.
Symptom Relief
Hours
60%
50%
40%
30%
20%
10%
0%
-10%
-20%0 0.5 21.51 2.5 3 3.5 4 4.5 5 23 23.5 24
Cetirizine10 mg q.d.(n = 67)
Loratadine10 mg q.d.(n = 67)Placebo(n = 68)
*
*
* ** * *
† † † † †
Double-blind, placebo-controlled, parallel-group, environmental exposure unit study
N = 202 patients Exposed to ragweed pollen
for one 7-h and one 6-h period over 2 days in EEU
Results Cetirizine demonstrated
2 times better mean overall symptom relief vs loratadine
Cetirizine demonstrated onset within 1 hour vs 3 hours for loratadine
Confirmed in a 2nd study In this study, no reports of
somnolence in patients
*P .05 vs loratadine and placebo.
†P < .05 vs placebo.
**
** * * * *
* *
** *
Please see full prescribing information.
Symptom Relief in the EEU with Cetirizine or Loratidine
Mea
n P
erce
nt Im
prov
emen
t fro
m B
asel
ine
in M
ajor
S
ympt
om C
ompl
ex S
ever
ity S
core
(%
)

Montelukast With and Without Loratidine: Daytime Nasal Symptom Scores
Meltzer et al. J Allergy Clin Immunol. 2000;105:917-922.
* P<0.001 vs placebo and P<0.05 vs either agent alone.
*
Lea
st-S
qu
are
Mea
n
Ch
ang
e F
rom
Bas
elin
e
MON 10 mg +
LOR 10 mg MON 10 mgPlacebo MON 20 mg LOR 10 mg

Montelukast With and Without Loratidine for Allergic Rhinitis
Daytime Nasal Symptom Score (0-3 point scale)
-0.7
-0.6
-0.5
-0.4
-0.3
-0.2
-0.1
0
Placebo
MNT
MNT+ LOR
LOR
* P0.003 vs placebo.MNT + LOR vs LOR = not significant.MNT + LOR vs MNT = not significant.
Mea
n C
han
ge
Fro
m B
asel
ine
(LS
Mea
n, 9
5% C
I)
Mean baseline score =2
* **
Nayak AS, et al. Ann Allergy Asthma Immunol. 2002;88;592-600.

Driving Performance Study Iowa Driving Simulator
Monitor driver and steering deviations
Monitor speed and view of participant
Monitor pedals and reaction times
Monitor driving simulation pod

Driving Performance Study Iowa Driving Simulator
*P<.05 vs placebo†P<.05 vs fexofenadine§ ~2.5 hours after fexofenadine, diphenhydramine, or placebo; ~1 hour after EtOH
Change From Baseline (Visual
Analog Scale 0-100)
Before Driving§ After 50-Minute Drive
* †
* †
†
Weiler et al. Ann Intern Med 2000;132:354-63
VAS Drowsiness

Intranasal Steroids• “. . . the most effective treatment of allergic
rhinoconjunctivitis.”1
—ARIA Workshop Report, 2001
• “Nasally inhaled corticosteroids are the most effective medication class for controlling symptoms of allergic rhinitis.”2
—Joint Task Force practice parameters, 1998
• “Intranasal corticosteroids are the first line of therapy when obstruction is a major component of the patient’s rhinitis.”3
—The Allergy Report
1. Bousquet et al. J Allergy Clin Immunol. 2001;108(5 suppl):S147-S334.2. Dykewicz & Fineman. Ann Allergy Asthma Immunol. 1998;81:463-468.3. American Academy of Allergy, Asthma and Immunology. The Allergy Report.
(http://www.theallergyreport.org)

TAA AQ: Rapid Onset of Action
Nasal Index (stuffiness, discharge, sneezing) Reduction Within 12-16 Hours*
*Based on treatment in the morning and symptom assessment at bedtime†P<.03 vs placebo
Settipane et al. Clin Ther 1995;17(2):252-63.
Mea
n C
han
ge
fro
m B
asel
ine
Baseline Day 1 Day 2 Day 3 Day 4Treatment Day
†
Placebo, n=111TAA AQ 220/110 g/d, n=109
TAA AQ 220/220 g/d, n=118
† †
† ††
† †

Key Secondary Endpoint—Mean Change From Baseline in AM Predose iTNSS Over 2-Week Treatment Period
24-Hour Control of Total Nasal Symptoms Associated With Ragweed SAR in Patients ≥12 Years
ImprovementImprovement
*
* Significant treatment difference vs placebo over entire treatment period: -1.38 (P<0.001).
Days
Mea
n C
ha
ng
e F
rom
Bas
eli
ne
in
AM
Pre
do
se i
TN
SS
ITT population (n=299).Endpoint = least square mean change over the entire 2-week treatment period.
Endpoint
Kaiser HB et al. J Allergy Clin Immunol. 2007. In press.

Response to Fluticasone Furoate Spray in Patients Response to Fluticasone Furoate Spray in Patients ≥12 Years With Perennial Allergic Rhinitis≥12 Years With Perennial Allergic Rhinitis
ImprovementImprovement
Mean Change From Baseline in Daily rTNSS Over 4-Week Treatment PeriodMean Change From Baseline in Daily rTNSS Over 4-Week Treatment Period
** Significant treatment difference vs placebo Significant treatment difference vs placebo over entire treatment period: -0.71 (over entire treatment period: -0.71 (PP=0.005).=0.005).
Mea
n C
ha
ng
e F
rom
Bas
eli
ne
in
Dai
ly r
TN
SS
Days
*
ITT population (n=302).Endpoint = least square mean change over the entire 4-week treatment period.
Data on file, GlaxoSmithKline.
Endpoint

Relief of Total Ocular Symptoms Associated With Ragweed SAR Over 24 Hours in Patients ≥12 Years
Other Secondary Endpoint—Mean Change From Baseline in AM Predose iTOSS* Over 2-Week Treatment Period
Mea
n C
ha
ng
e F
rom
Bas
eli
ne
in
AM
Pre
do
se i
TO
SS
Data on file, GlaxoSmithKline.
ITT population (n=299).* No multiplicity adjustments were made for this endpoint.† Treatment difference vs placebo over entire treatment period: -0.553 (P=0.007).
Endpoint = least square mean change over the entire 2-week treatment period.
ImprovementImprovement
†
DaysEndpoint

INSs: Risk of Cataracts• Retrospective, observational cohort study of 286,078
patients <70 years of age in the UK (1991-1996)
• Incidence of cataracts the same for users (BDP, FPANS, BUD) and nonusers of INSs: 1.0/1,000 person-years
• Incidence of cataracts for oral steroid users: 2.2/1,000 person-years
• Cataract risk did not increase with number of prior prescriptions for an intranasal corticosteroid
Derby & Maier. J Allergy Clin Immunol. 2000;105:912-916.

Allergic rhinitis causes the patient to have:
• Impaired sleep
• Impaired performance at work/school
• Frequent headaches and cough
• Increased frequency/severity/persistence of sinusitis
• Increased (6-fold) risk of asthma
AS THE NOSE GOES, SO GOES THE PATIENT
Allergic rhinitis can be prevented and controlled.



ELISA-sandwich Assay
Cox L, et al, Ann Allergy Asthma Immunol 2008; 101:580-92.
Allergy Skin Tests: General Rules
• The technician performing the skin tests and the clinician ordering and interpreting skin tests must understand the characteristics of the tests they are administering
• These include: • type of skin testing (intradermal vs percutaneous)
• device used (single vs multiple puncture)
• placement of tests (location and adjacent testing)
• the quality and potency of the extracts being used • potential confounder of medications that may
suppress skin test response.
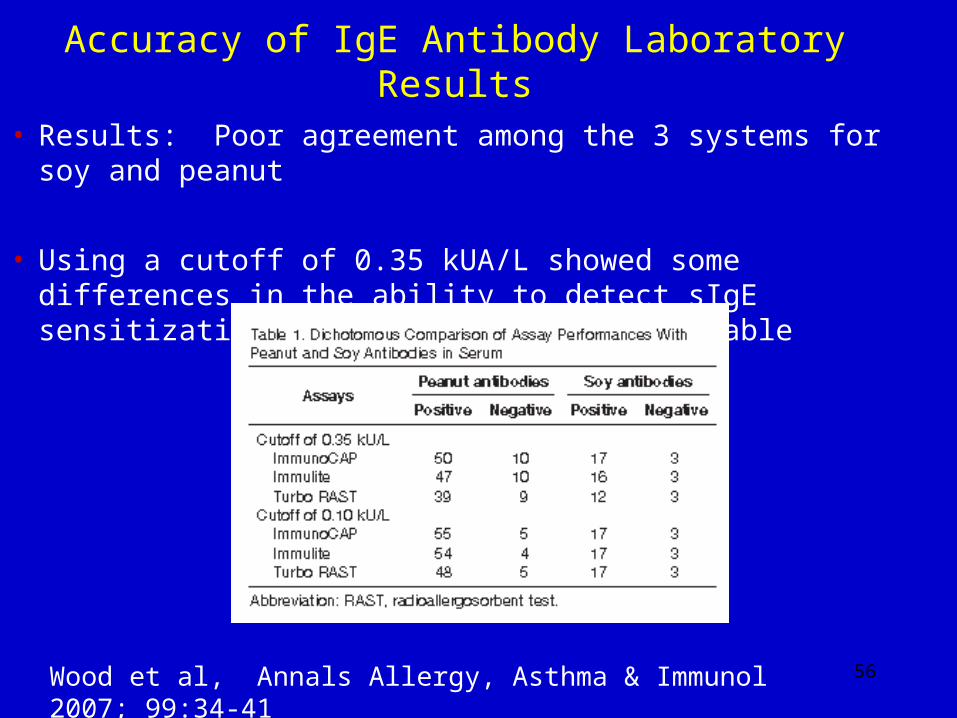
Accuracy of IgE Antibody Laboratory Results
• Results: Poor agreement among the 3 systems for soy and peanut
• Using a cutoff of 0.35 kUA/L showed some differences in the ability to detect sIgE sensitization with Turbo RAST most variable
56Wood et al, Annals Allergy, Asthma & Immunol 2007; 99:34-41




Classification• Emphasizes quality of life• Duration of symptoms
– Intermittent (primarily seasonal)• Symptoms occur <4 days/week OR duration <4 weeks
– Persistent (primarily perennial)• Symptoms >4 days/week AND >4 weeks
• 2 symptom-severity categories:– Moderate-Severe (1 of the following)
– Mild (none of the following)• Sleep disturbances
• Impairment of daily activities, leisure, and/or sport
• Impairment of school or work
• Troublesome symptoms Bousquet et al. J Allergy Clin Immunol 2001;108:S147-336

“One Airway”: Hypothesis• Inflammation is a key component of both allergic
rhinitis and asthma– Common triggers for both diseases– Similar mediators involved– Many individuals have both diseases– Upper airway symptoms may trigger lower airway
symptoms– Lower airway symptoms may trigger upper airway
symptoms• Treatment of the upper airway may improve lower
airway symptoms1-5 1. Foresi et al. J Allergy Clin Immunol. 1996;98:274-282.2. Watson et al. J Allergy Clin Immunol. 1993;91:97-101.3. Corren et al. J Allergy Clin Immunol. 1992;89:611-618.4. Aubier et al. Am Rev Respir Dis. 1992;146:122-126.5. Henriksen and Wenzel. Am Rev Respir Dis. 1984;130:1014-1018.

Omalizumab Blocks IgE Binding to Mast Cells
Mast cell
IgE molecule
FcRI receptor
Omalizumab Omalizumab

Relative Sedation with Antihistamines

0
1
2
3
4
5
6
7
8
9
10
Fluticasone Proprionate Significantly Reduced Time to Clinical Success In Acute Sinusitis
*P=0.01 vs placebo.
Dolor et al. JAMA. 2001;286:3097-3105.
Day
s to
Cli
nic
al S
ucc
ess
*
† All patients received xylometazoline HCl b.i.d. for 3 days and cefuroxime axetil b.i.d. for 10 days
6Days
6Days
9.5Days9.5
Days
FPANS†
Placebo†

0
10
20
30
40
50
60
70
80
90
100
Significantly Higher Rate of Clinical Success in Acute Sinusitis With Fluticasone Proprionate
*P=0.009 vs placebo.
Dolor et al. JAMA. 2001;286:3097-3105.
Cli
nic
al S
ucc
ess
(%)
*
† All patients received xylometazoline HCl b.i.d. for 3 days and cefuroxime axetil b.i.d. for 10 days
FPANS†
Placebo†
93.5%93.5%
73.5%73.5%

1. Allen. J Allergy Clin Immunol. 2000;106:S179-S190.2. Daley-Yates and Richards. J Allergy Clin Immunol. 2001;107:S313. Abstract 1023. 3. Daley-Yates and Richards. Presented at: AAAAI; New Orleans, Louisiana; March 16-21, 2001.
Bioavailability of INSsIntranasal Oral
Fluticasone propionate1 <1% <1%
Mometasone furoate1 <1% <1%
Budesonide1 34% 11%
Beclomethasone1 44% 41%
Triamcinolone acetonide2,3 46% 23%
Flunisolide1 49% 21%
The clinical relevance of these in vitro data are not known.


















