The Pathophysiology of Fragile X SyndromeANRV321-GG08-06 ARI 25 July 2007 17:29 The Pathophysiology...
23
The Pathophysiology of Fragile X Syndrome Olga Penagarikano, 1 Jennifer G. Mulle, 1 and Stephen T. Warren 1,2,3 1 Department of Human Genetics, 2 Department of Biochemistry and 3 Department of Pediatrics, Emory University School of Medicine, Atlanta, Georgia 30322; email: [email protected], [email protected], [email protected] Annu. Rev. Genomics Hum. Genet. 2007. 8:109–29 First published online as a Review in Advance on May 3, 2007. The Annual Review of Genomics and Human Genetics is online at genom.annualreviews.org This article’s doi: 10.1146/annurev.genom.8.080706.092249 Copyright c 2007 by Annual Reviews. All rights reserved 1527-8204/07/0922-0109$20.00 Key Words mental retardation, trinucleotide repeat expansion, FMR1, FMRP, synaptic plasticity, autism Abs tr ac t Fragile X syndrome is the most common form of inherited mental retardation. The disorder is mainly caused by the expansion of the trinucleotide sequence CGG located in the 5 UTR of the FMR1 gene on the X chromosome. The abnormal expansion of this triplet leads to hypermethylation and consequent silencing of the FMR1 gene. Thus, the absence of the encoded protein (FMRP) is the basis for the phenotype. FMRP is a selective RNA-binding protein that associates with polyribosomes and acts as a negative regulator of translation. FMRP appears to play an important role in synaptic plasticity by regulating the synthesis of proteins encoded by certain mRNAs localized in the dendrite. An advancing understanding of the pathophysiology of this disorder has led to promising strategies for pharmacologic interventions. 109 Annu. Rev. Genom. Human Genet. 2007.8:109-129. Downloaded from arjournals.annualreviews.org by EMORY UNIVERSITY on 08/31/09. For personal use only.
Transcript of The Pathophysiology of Fragile X SyndromeANRV321-GG08-06 ARI 25 July 2007 17:29 The Pathophysiology...

ANRV321-GG08-06 ARI 25 July 2007 17:29
The Pathophysiologyof Fragile X SyndromeOlga Penagarikano,1 Jennifer G. Mulle,1and Stephen T. Warren1,2,3
1Department of Human Genetics, 2Department of Biochemistry and 3Department ofPediatrics, Emory University School of Medicine, Atlanta, Georgia 30322;email: [email protected], [email protected],[email protected]
Annu. Rev. Genomics Hum. Genet. 2007. 8:109–29
First published online as a Review in Advance onMay 3, 2007.
The Annual Review of Genomics and Human Geneticsis online at genom.annualreviews.org
This article’s doi:10.1146/annurev.genom.8.080706.092249
Copyright c 2007 by Annual Reviews.All rights reserved
1527-8204/07/0922-0109$20.00
K ey Wo r ds
mental retardation, trinucleotide repeat expansion, FMR1, FMRP,synaptic plasticity, autism
A bst ract
Fragile X syndrome is the most common form of inherited mentalretardation. The disorder is mainly caused by the expansion of thetrinucleotide sequence CGG located in the 5 UTR of the FMR1gene on the X chromosome. The abnormal expansion of this tripletleads to hypermethylation and consequent silencing of the FMR1gene. Thus, the absence of the encoded protein (FMRP) is the basisfor the phenotype. FMRP is a selective RNA-binding protein thatassociates with polyribosomes and acts as a negative regulator oftranslation. FMRP appears to play an important role in synapticplasticity by regulating the synthesis of proteins encoded by certainmRNAs localized in the dendrite. An advancing understanding ofthe pathophysiology of this disorder has led to promising strategiesfor pharmacologic interventions.
109
Ann
u. R
ev. G
enom
. Hum
an G
enet
. 200
7.8:
109-
129.
Dow
nloa
ded
from
arjo
urna
ls.an
nual
revi
ews.o
rgby
EM
ORY
UN
IVER
SITY
on
08/3
1/09
. For
per
sona
l use
onl
y.

ANRV321-GG08-06 ARI 25 July 2007 17:29
F X : fragile X
F ragile si t es:chromosomalregions that appearas nonrandomchromatindiscontinuities atmetaphase duringcell division
F X S: fragile Xsyndrome
I N T R O D U C T I O N
In 1911, Thomas H. Morgan first pointedout sex-linked inheritance of genetic traits inDrosophila melanogaster when he noted that thephenotype “white-eyed” affected only males.Morgan suggested that there could be a re-cessive genetic trait affecting only males if thegene responsible for it was located on the Xchromosome, in the region not common withthe Y chromosome. Twenty-five years afterMorgan described sex-linked inheritance inflies, human studies were noting a higher in-cidence of mental retardation in males com-pared with females (90), and the first pedigreesshowing mental retardation associated to theX chromosome were published (79). How-ever, the idea of human intelligence being af-fected by X-linked genes was not fully ap-preciated until 1974, when Lehrke publishedthat 25–50% of mental retardation may beattributed to X-chromosome mutations (73).Although this estimation was later discoveredto be too high, his work established the con-cept of X-linked mental retardation (XLMR).Today, approximately 2% of the general popu-lation has an intelligence quotient (IQ) belowwhat is considered normal (IQ < 70) and 15–
F igu r e 1
The “marker X” chromosome. Metaphase chromosomes showing thepeculiar constriction at the end of the long arm of chromosome X that ischaracteristic in fragile X (FX) individuals.
20% of this is believed to be due to XLMR,with 202 conditions described, of which, todate, 45 have the responsible gene cloned (22).Although each of these X-linked MR loci con-tributes a relatively small percentage of hu-man XLMR, one locus, that responsible forfragile X syndrome, contributes the largestfraction.
F R A G I L E X SY N D R O M E
One of the first large families where mental re-tardation was transmitted in an X-linked fash-ion was described by Martin & Bell in 1943(79). In 1969, Lubs detected an unusual sec-ondary constriction at the end of the longarm of the X chromosome in four mentallyretarded males and three obligate carrier fe-males in a single family (76) (F igu r e 1). How-ever, this observation remained a mystery formore than a decade until Sutherland showedthat specific culture conditions are needed forthe cytogenetic expression of the “marker X,”enabling the recognition of additional fam-ilies (105). Fragile sites are named with theterm FRA, designating fragility, followed bythe chromosome where they are located and aletter indicating the order in which they werefound (14). Thus, the fragile site associatedto the fragile X chromosome, now localizedspecifically to band Xq27.3 (53), was namedFRAXA, as it was the first fragile site describedon chromosome X. Richards & Sutherland(93) later analyzed the original pedigree de-scribed by Martin and Bell and showed thatthe affected males did indeed have fragileX syndrome. Consequently, the descriptorsMartin-Bell syndrome or marker X syndromehave now been largely superseded by the des-ignation fragile X syndrome (FXS).
F R A G I L E X P H E N O T Y P E
Initially, the fragile or marker X chromo-some was not clearly associated with any otherphenotype but mental retardation. However,once the laboratory conditions necessary forthe reproducible expression of the cytogenetic
110 Penagarikano · M ulle · Warren
Ann
u. R
ev. G
enom
. Hum
an G
enet
. 200
7.8:
109-
129.
Dow
nloa
ded
from
arjo
urna
ls.an
nual
revi
ews.o
rgby
EM
ORY
UN
IVER
SITY
on
08/3
1/09
. For
per
sona
l use
onl
y.

ANRV321-GG08-06 ARI 25 July 2007 17:29
fragile site were established, a number ofaffected families were detected and the asso-ciated phenotype emerged.
Mental retardation is the most prominentphenotype, with IQ values typically between20 and 70 (41). The cognitive dysfunctionparticularly affects short-term memory forcomplex information, visuospatial skills, andspeech. A delay in speech is common and of-ten the first symptom that brings the child tomedical attention. Some patients show hyper-activity, hypersensitivity to sensorial stimuli,and attention deficit, and between 15–50% ofaffected individuals show some autistic behav-ior such as poor visual contact, tactile defen-siveness, and repetitive behaviors (26).
Individuals affected by FXS show a sub-tle, yet characteristic, facial morphologyof macrocephaly, with a long narrow faceand prominent forehead, jaw, and ears (23)(F igu r e 2). Macroorchidism, or enlarged tes-ticles, are commonly seen in postpubescentmale patients. Other physical features suchas the presence of a high arched palate, hy-potonia (51), flat feet, increased joint laxity,and mitral valve prolapse (74) have also beenreported. These findings are collectively be-lieved to be due to a poorly understood con-nective tissue abnormality that has receivedlittle research attention (58).
Several investigators have also reporteda neuroendocrine dysfunction in FXS. Al-though poorly understood at the molecularlevel, an unusual overgrowth pattern has beenattributed to this and includes an increasedbirth weight, macrocephaly, and increasedstature, particularly in childhood. Some in-dividuals affected by FXS have also been di-agnosed as Sotos (115) or Prader-Willi syn-dromes (32) due to their striking physicalsimilarity. Endocrine studies of these patientshave reported hypothalamus dysfunction (55).
U N U S U A L I N H E R I T A N C EPA T T E R N
As soon as families showing the FX chro-mosome were identified, it became apparent
F igu r e 2
The fragile X phenotype. Note the characteristicfacial features of the syndrome: long, narrow face,prominent forehead, jaw, and ears.
M acr oo rch idism:testicular volume>30 ml, which isprincipallydeveloped during thepostpubertal period
N T M : normaltransmitting male
that the inheritance pattern was not consis-tent with a recessive X-linked condition, aspreviously thought. The main conflicting datawere the existence of nonaffected male carri-ers and affected female carriers (84). Shermanet al. (99, 100) conducted extensive pedigreeanalyses and reported that 20% of males car-rying the mutated gene were not affected.These individuals were termed normal trans-mitting males (NTMs). In addition, 30% ofcarrier females showed some form of mental
www.annualreviews.org • Fragile X Syndrome 111
Ann
u. R
ev. G
enom
. Hum
an G
enet
. 200
7.8:
109-
129.
Dow
nloa
ded
from
arjo
urna
ls.an
nual
revi
ews.o
rgby
EM
ORY
UN
IVER
SITY
on
08/3
1/09
. For
per
sona
l use
onl
y.

ANRV321-GG08-06 ARI 25 July 2007 17:29
F M R 1: fragile Xmental retardation 1
M icr osat ell i t e:repetitive DNAsequence consistingof 1–4 base repeatunits
D ynam ic m u tat io n:A repetitive DNAsequence whoseincreasing length,beyond a certainthreshold, confers anincreasinginter-generationalinstability
impairment. They also noticed that the riskof inheriting the syndrome depended on theposition of an individual within the pedigree:The mothers of NTM showed three timesless risk of having affected sons than theirdaughters. This phenomenon is known as theSherman paradox and was not resolved until1991, when the gene responsible for the syn-drome was identified and, at the same time,a new mutational mechanism revealing theparticular inheritance model: trinucleotiderepeat expansion.
A N E W C O N C E P T O FM U T A T I O N
According to Mendel’s work in 1860, theinheritance of genetic traits is determinedby units of discrete nature, later namedgenes, which are transmitted intact and in-dependently to the next generation. Almost100 years later Benzer showed that genescould suffer mutations, but, once produced,these mutations would be transmitted in-tact to the next generation. This conceptis still valid for most genes; however, since1991, when the gene responsible for FXS wascloned, it has been revealed that specific repet-itive sequences in some genes are unstable andcan mutate serially upon transmission.
T h e F ragile X M u tat io n
The existence of the Xq27.3 cytogenetic frag-ile site associated with the syndrome wasa target for subsequent molecular studies.Pedigree analysis localized both the causal lo-cus and the fragile site to a 22-cM region onthe X chromosome (88), and further studiesrevealed a number of linked markers that re-duced the interval to 1–2 Mb and strength-ened the localization of the disease locus tothe fragile site (57, 95, 106, 107). Warren et al.(117) described somatic cell hybrids carryingthe human fragile X chromosome with ro-dent chromosome translocations at the FXsite. Heitz et al. (54) identified a yeast ar-tificial chromosome (YAC) containing two
markers known to flank the fragile site hy-brid break points and showed that this YACcontains a CpG island aberrantly methylatedin fragile X patients. Furthermore, these ab-normally methylated fragments were unstablein affected individuals and increased in sizewhen transmitted through a pedigree (88).In 1991, Verkerk et al. (114) used these so-matic cell hybrids and identified a gene, ex-pressed in the brain, that showed a tandemrepeat of the CGG trinucleotide in its 5 re-gion, which was expanded in affected individ-uals and was coincident with the fragile site.The gene was named Fragile X Mental Retar-dation 1 (FMR1), assuming that it was the firstof a number of yet-identified genes associatedwith the FX site. We now appreciate that theFMR1 gene resides in a gene desert, and thissingle gene is responsible for the syndrome.
Microsatellite sequences, such as the oneresponsible for FXS, are very frequent in thehuman genome, being present every 2 kband representing approximately 90 Mb of thehuman genome (62). Most of them show rel-atively high levels of polymorphism, but areusually stable upon transmission. The vari-ability in the repeat length represents a slightinstability in the sequence that usually appearsas an expansion or contraction of one or tworepeats (12). These small changes in repeatlength usually remain in the “normal” range;therefore, most microsatellites are not associ-ated with any disease. However, trinucleotiderepeats can show a much greater instability.In particular, when the transmitting allele isbeyond a certain threshold size, it generates anew lengthened allele when transmitted thatis often a large expansion that leads to geneticdisorders. This new and unexpected multistepmutational mechanism is called dynamic mu-tation (94). FXS, along with Kennedy disease[spinal-bulbar muscular atrophy (SBMA)],was the first to be identified among the disor-ders associated with trinucleotide repeat ex-pansion. To date, at least 16 disorders areknown to be caused by trinucleotide re-peat expansion (28). The trinucleotide repeatexpansion can lie within the coding region
112 Penagarikano · M ulle · Warren
Ann
u. R
ev. G
enom
. Hum
an G
enet
. 200
7.8:
109-
129.
Dow
nloa
ded
from
arjo
urna
ls.an
nual
revi
ews.o
rgby
EM
ORY
UN
IVER
SITY
on
08/3
1/09
. For
per
sona
l use
onl
y.

ANRV321-GG08-06 ARI 25 July 2007 17:29
of the gene, as in Kennedy disease or otherpolyglutamine diseases, where the expandedCAG triplet, which codes for glutamine, isincluded in the encoded protein and the newmutant protein gains a novel deleterious func-tion. Alternatively, the triplet expansion canbe located in a noncoding region, as in FXS,and, depending on the triplet and on the lo-cation (within an intron or within a nontrans-lated region of an exon), the pathogenic mech-anism is different, usually leading to a dimin-ished expression or even silencing of the gene.
T r i n ucleo tide R epeat E xpansio n
Since the molecular basis of this new mu-tational mechanism was described, specialefforts have been made to explain thephenomenon of expansion. The proposedmodels include unequal exchange of geneticmaterial during meiosis or mitosis due toan incorrect pairing of the chromatids alongthe repetitive sequence and gene conversion.Although these mechanisms could be thecause of some of the expansions observed intrinucleotide repeats, the initial event leadingto the instability of a normal allele thoughtto be slipped-strand mispairing during DNAreplication (70). Richards & Sutherland(93) suggested that the slippage would occurspecifically in the Okazaki fragments. Okazakifragments formed by long or uninterruptedrepetitive sequences will not be anchored byunique sequences at their ends, showing a riskof suffering slippage. If slippage occurs, DNArepairing enzymes could add nucleotides tothe template strand to make it complemen-tary to the newly formed strand, generatingan expansion. In support of this, the absenceof a functional flap endonuclease 1 (FEN-1),which is necessary for correct processing ofOkazaki fragments, has dramatic effects onrepeat instability. Indeed, FEN-1 activity isdiminished when the flap length is longerthan 11 repeats (72). If the flap is not correctlyprocessed, it will lead to an expansion of therepeat. Initially, a gradual accumulation ofone or a few repeats per generation would
O kazak i frag m e n t:short fragment ofDNA created on thelagging strand duringDNA replication dueto the intrinsic 5 –3
polarity of DNApolymerase
F lap e n do n uclease1 ( F E N -1): removes5 flaps from Okazakifragments. Flapscontaining repeatscould acquiredifferent DNAconformations thatenable them toescape FEN-1cleavage
occur; massive expansions could take placeby some continuous slippage due to a blockin the replication process generated by alter-native structures formed by the trinucleotiderepeat sequences (89). Because slipped-strandmispairing during DNA replication is themost accepted mechanism of trinucleotiderepeat expansion, it is natural to think thatthe mismatch repair system (MRS) wouldplay an important role. However, to date noclear data exist regarding its role in tripletrepeat instability.
T H E FMR1 G E N E
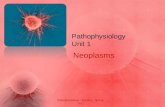
The FMR1 gene is 38 kb in length and con-tains 17 exons (F igu r e 3). The 4.4-kb full-length mRNA codes for a protein with amaximum length of 632 amino acids and amolecular mass of 80 kDa, although differ-ent transcripts can be produced by alternativesplicing (7). The translation start is located69 base pairs (bp) downstream the repetitiveregion and the repeat lays in the 5 untrans-lated region (UTR) within the first exon of thegene (7). In addition, the gene shows a CpG is-land located 250 bp upstream from the repeat(38). The repeat length is polymorphic andranges from 6–54 CGG in normal individuals(44). Female carriers and NTMs show an ex-pansion between 55 and 200 repeats, termedpremutation. When the expansion is morethan 200 repeats, it is termed full mutation.As a result of the expansion, the repeat, theupstream CpG island, and the surroundingsequence become hypermethylated and thegene silenced. Thus, the absence of the en-coded protein is the basis for the phenotype(91). Silencing the expanded FMR1 allele is aunique example of a local epigenetic changedriven by variation in the gene sequence.
Methylation of the FMR1 gene acts bothdirectly, by inhibiting the binding of tran-scription factors, and indirectly, by induc-ing chromatin condensation, which, in turn,prevents the transcription machinery frombinding. The transcriptionally inactive statusof the FMR1 gene shows four occupied
www.annualreviews.org • Fragile X Syndrome 113
Ann
u. R
ev. G
enom
. Hum
an G
enet
. 200
7.8:
109-
129.
Dow
nloa
ded
from
arjo
urna
ls.an
nual
revi
ews.o
rgby
EM
ORY
UN
IVER
SITY
on
08/3
1/09
. For
per
sona
l use
onl
y.

ANRV321-GG08-06 ARI 25 July 2007 17:29
1E-box-CREGC boxesGC richpalindrome
–129 –94 –66 – 44
Transcription start
+1 +130
ATGIntrons Exons Splicing
2 3 4 5
NLS
6 7 8 9 10 11 1213 14 15 16 17
TAA
Normal: 6-44 (CGG)n
Intermediate: 45-54 Premutation: 55-200 Full mutation: >200
KH1 KH2 NES RGG
F igu r e 3
Schematic representation of the fragile X mental retardation 1 (FMR1) gene. The FMR1 gene shows 17exons that undergo alternative splicing. The CGG repeat is located within the untranslated region of thefirst exon. Expansion over 200 repeats leads to methylation of the promoter and transcriptional silencing.The location of the principal domains of the normally encoded protein is also indicated.
transcription factor-binding sites in its pro-moter, including a palindrome, two GC-like boxes, and an overlapping E-box-cAMPresponse element (CRE) site. Studies onthe proteins that bind to these sites haveidentified the factors upstream stimulatoryfactor 1 (USF1) and USF2, nuclear respira-tory factor 1 (NRF1) and NRF2, specificityprotein 1 (Sp1) and cAMP response elementbinding protein (CREB) as the most activelyinvolved in FMR1 transcriptional activity (69,103). In addition, the 5 region of the FMR1gene is normally associated with histone pro-teins H3 and H4 acetylated in their lysineresidues, but this acetylation is reduced inFX cells (25). Changes in histone methyla-tion have also been described, with histone3 showing methylated lysine 4 and unmethy-lated lysine 9 in normal cells but the op-posite methylation pattern in FX cells (24).Attempts to pharmacologically reactivate thegene have shown a synergistic effect usingboth DNA methylation and histone deacety-lation inhibitors (20); however, the connec-tion between histone modifications and DNAmethylation remains unclear. It was recentlyshown that the transcriptionally active versusinactive state of the FMR1 gene display differ-ent broader chromatin conformations. Chro-matin segments located throughout a 50-kbdomain around the promoter interact less fre-
quently when FMR1 is expressed comparedwith when the gene is repressed. Therefore,the expression-correlated change in confor-mation affects a significantly larger domainthan the one marked by histone modifications(46). However, the cause-and-effect relation-ship among promoter activation, local histonemodifications, and broader changes in chro-matin remains to be determined.
All data suggest that the transcriptional re-pression of the FMR1 gene occurs when boththe CpG island and the CGG repeat becomehypermethylated. It is assumed that methyla-tion and consequent inactivation of the geneoccur after fertilization during embryogene-sis and that the protein is expressed duringthe first stages of embryonic development (75,119). However, this early expression does notseem to play an important biological role as in-dividuals affected as consequence of deletionsin the FMR1 gene, and therefore not express-ing the protein at any point during their devel-opment, do not show any phenotypic differ-ences from individuals affected owing to genemethylation (45, 120).
F acto rs I n fl u e nci ng C G G R epeatE xpansio n
With FXS, as in every dynamic mutation,there is a multistep process of expansion that
114 Penagarikano · M ulle · Warren
Ann
u. R
ev. G
enom
. Hum
an G
enet
. 200
7.8:
109-
129.
Dow
nloa
ded
from
arjo
urna
ls.an
nual
revi
ews.o
rgby
EM
ORY
UN
IVER
SITY
on
08/3
1/09
. For
per
sona
l use
onl
y.

ANRV321-GG08-06 ARI 25 July 2007 17:29
takes place over many generations. Normalrepeats (6–54 CGG) are usually transmit-ted stably, but sometimes increase (or de-crease) by a few repeats, creating a poolof at-risk alleles that can eventually becomepremutations. Premutations (55–200 CGG)tend to expand when maternally transmitted,as male spermatogenesis is unable to main-tain full-mutation alleles (78). The proba-bility of expansion depends on the repeatlength. Alleles larger than 90–100 CGG re-peats show an almost 100% risk of expan-sion to full mutation (>200 CGG) in thenext generation (86). Smaller alleles, althoughunstable, usually do not expand to a fullmutation in one generation. To date, thesmallest allele that has suffered that kind ofchange has 59 repeats (87). In addition, se-quencing analysis of normal FMR1 alleles re-vealed that the CGG repeat is not pure, butpresents an AGG interruption every 9–10 re-peat units, and the most common allele is(CGG)9 − 10AGG(CGG)9AGG(CGG)9 (71).However, in FX families the premutated al-leles usually have one or no interruptions.Loss or lack of one of these interruptionsis an important determinant for repeat in-stability (37). The 59 repeat allele that ex-panded to a full mutation in one generationhad no interruptions, supporting their impor-tant role. The fact that most of the premu-tation alleles bigger than 90 repeats expandto full mutation in one generation, and as-suming that the maximum number of AGGinterruptions that they show is probably 2,and that they are located every 9–10 CGG,suggests that approximately 70 pure repeatsare needed for the allele to be fully expanded.Because the most likely mechanism of expan-sion is slipped-strand mispairing during DNAreplication in the Okazaki fragments, whichrange among 25–300 nucleotides, and 70 re-peats make 210 nucleotides, there is a highprobability that this fragment is not anchoredby unique flanking sequences, which supportsthe idea of strand slippage.
Analysis of polymorphic markers withinand near the FMR1 gene shows that certain
L i n kagediseq u ilib r i u m:nonrandomassociation of allelesat two or morelinked loci
haplotypes are preferably associated with theFX mutation. This observation is denoted aslinkage disequilibrium and suggests the ex-istence of a pool of founder chromosomesthat lead to the FX chromosomes (71). Thus,apparently nonrelated individuals could havecommon ancestors, and the origin of the mu-tation could be the same. Different mutationalroutes that correspond to the different haplo-types observed in FX individuals may exist.They typically involve the generation of alle-les with longer tracts of pure CGG repeats ei-ther by loss of AGG interruptions or by grad-ual increase in the repeat length.
It is still not clear when the repeat ex-pansion occurs. First, the observation that af-fected individuals are mosaics, showing bothpremutation and full-mutation alleles or full-mutation alleles of different sizes, togetherwith the fact that affected males show onlypremutations in their sperm (42) led to theassumption of a postzygotic model, where thezygote harbors a premutation and the expan-sion occurs mitotically during early embrio-genesis. It was later pointed out that there wasno correlation between the repeat length andthe degree of mosaicism and that no mech-anism that distinguishes a maternal trans-mission, suffering expansion, from a pater-nal transmission, not suffering expansion, wasknown. Therefore, the mosaicism observed inpatients would likely be due to the contractionof somatic alleles rather than to the differ-ent expansion of maternal premutated allelesduring gametogenesis, and expansion wouldprobably be prezygotic (83). The prezygoticmodel of expansion is supported by the obser-vation of full-mutation alleles in oocytes andin fetal spermatogonia, but only premutationsin testes at a later stage, suggesting that theexpansion must occur before germinal differ-entiation (78).
Animal models will be essential to deter-mine the timing and the mechanism of boththe expansion and the methylation and inac-tivation seen in humans. However, althoughsome expansions were recently reported in amouse containing a human (CGG)98 repeat
www.annualreviews.org • Fragile X Syndrome 115
Ann
u. R
ev. G
enom
. Hum
an G
enet
. 200
7.8:
109-
129.
Dow
nloa
ded
from
arjo
urna
ls.an
nual
revi
ews.o
rgby
EM
ORY
UN
IVER
SITY
on
08/3
1/09
. For
per
sona
l use
onl
y.

ANRV321-GG08-06 ARI 25 July 2007 17:29
P O F : prematureovarian failure
F X T A S: fragile Xtremor ataxiasyndrome
(15) (even occasionally reaching the full-mutation range), to date there are no reportsof massive expansions occurring in the mouseat the same frequencies as are observed in hu-man pedigrees. In addition, mice with longrepeats ( 230 CGG) show an absence of ab-normal methylation, indicating that the FXfull mutation has not yet been mimicked inmice.
F ragile X Syn d r o m e W it h o u t C G GE xpansio n
Because the cause of the phenotype associatedwith FXS is the lack of the protein encoded bythe FMR1 gene, it is reasonable to think thatother mutations apart from the CGG expan-sion could lead to the disease. Actually, morethan 15 deletions affecting part of or the en-tire gene, and ranging from 1.6 kb to 13 Mb,have been described (45, 52, 56, 63, 81, 109,120). Besides deletions, point mutations thatlead to the phenotype due to the productionof a nonfunctional protein have also been de-scribed (31, 77). It is important to considerthat most diagnostic testing for FXS is lim-ited to the examination of the CGG repeatand largely ignores conventional mutations.However, because the full mutation leads toa functional null allele, it is likely that thereare many nonsense and missense mutationsof FMR1 that are being missed.
F R A G I L E X P R E M U T A T I O N
For many years, male and female premutationcarriers were considered asymptomatic. Thisview was gradually challenged by reports ofdifferent premutation-associated clinical phe-notypes over the past decade. The preva-lence of premutation alleles >54 repeats inthe general population is estimated at 1/259females and 1/813 males (96). As early as 1986,Fryns (43) noted an increased rate of twinningamong female premutation carriers, suggest-ing the possibility of ovarian dysfunction. Afew years later, Cronister et al. (27) noticedthat women carrying the FX mutation who
were cognitively normal had a higher preva-lence of premature ovarian failure. The meanage of menopause in the general population is51. It is assumed that it occurs as a result ofthe reduction of the initial oocyte pool belowa determined level. Premature ovarian fail-ure (POF) is defined as menopause before 40years of age. Both genetic and environmen-tal causes are known (97), but 60% of thecases have no obvious cause. When premuta-tion carriers could be distinguished from mu-tation carriers, it was shown that only the for-mer showed this higher prevalence (16–24%),whereas the latter showed the same risk asnoncarrier relatives and the general popula-tion ( 1%) (3). In addition, an increased levelof follicle-stimulating hormone (FSH), whichis as an indicator of ovarian aging, was foundin premutation carriers (104). Because only aproportion of women who carry the premuta-tion have ovarian dysfunction, it is importantto identify the risk factors that lead to clini-cal variability. The most obvious factors arethose related to the FMR1 gene. In a recentreport, Sullivan et al. (104) found a significantinfluence of repeat size on the risk for ovarianfailure, with increasing prevalence of POF anddecreasing age at menopause correlating withan increasing repeat size up to 100 repeats.
More recently, an emerging group of pre-mutation carriers showing neurological prob-lems was identified. Hagerman et al. (50) iden-tified five male patients with clinical featuresof intention tremor and cerebellar ataxia at50–60 years of age. The disorder was des-ignated as fragile X tremor ataxia syndrome(FXTAS). Prior to onset, these patients hadnormal cognitive ability. It was later shownthat this phenotype is not exclusive to males,as earlier suggested, but that females canalso be affected, although they show a lateronset, likely due to the degree of inacti-vation of the affected X chromosome (49).These patients show a general reduction inbrain size together with cerebellar damage,severe loss of Purkinje cells, spongiosis ofthe white matter, and axon dystrophy. Inaddition, eosinophilic intranuclear inclusions,
116 Penagarikano · M ulle · Warren
Ann
u. R
ev. G
enom
. Hum
an G
enet
. 200
7.8:
109-
129.
Dow
nloa
ded
from
arjo
urna
ls.an
nual
revi
ews.o
rgby
EM
ORY
UN
IVER
SITY
on
08/3
1/09
. For
per
sona
l use
onl
y.

ANRV321-GG08-06 ARI 25 July 2007 17:29
mainly formed by RNA and proteins, in neu-rons and astrocytes throughout the brainwere found in postmortem samples obtainedfrom symptomatic male premutation carri-ers (47). These types of granules have alsobeen found in other neurodegenerative dis-eases caused by trinuclotide repeat expansion,such as polyglutamine diseases and myotonicdystrophy.
The existence of phenotypes associated ex-clusively with the FX premutation suggeststhat a molecular cause other than the reduc-tion in FMRP levels must exist. mRNA levelsincreased up to tenfold in premutation carri-ers, despite the reduction of FMRP expres-sion (110). Transcriptional activity seems toincrease in response to a decreased translationrate (40). A dominant RNA gain-of-functionmechanism has been proposed as the molec-ular mechanism underlying FXTAS. The ele-vated number of FMR1 transcripts present inpremutation carriers might result in seques-tration of cellular proteins and formation ofinclusions. A mouse model for FXTAS thatdisplays similar neuronal intranuclear inclu-sions was recently generated (112). Furtherresearch on the development and composi-tion of the inclusions will help scientists tobetter understand the mechanism of RNA-mediated neurodegeneration. Ovarian dys-function could also result from a toxic effecton the follicles of an increased amount ofFMR1 RNA, leading to increased follicularatresia rates rather than a reduction of the ini-tial oocyte pool size. Future studies on ovariantissue from premutation carriers will be nec-essary to investigate this hypothesis.
F ragile X M e n tal R e tar dat io n P r o t ei n
Understanding the pathogenesis of FXS in-volves studying its cause and, thus, the func-tion of the molecule absent in affected in-dividuals: FMRP. The protein encoded bythe FMR1 gene is expressed widely, partic-ularly in the brain and testes (33), whichis consistent with the primary characteris-tics of the syndrome, mental retardation, and
F M R P: fragile Xmental retardationprotein
macroorchidism. As a result of alternativesplicing, the FMR1 gene can generate at least12 different proteins between 67–80 kDa (33,101). Their expression does not seem to be tis-sue specific, as different tissues show the sameexpression pattern (113). Alternative splicingaffects exons 12, 14, 15, and 17. In general,the most common isoforms lack exon 12, andisoforms lacking exon 14 show the lowest ex-pression (102). FMRP is predominantly local-ized in the cytoplasm; however, it was shownthat isoforms lacking exon 14 were localizedto the nucleus, consistent with the identifi-cation of a nuclear exportation signal (NES)encoded by this exon. FMRP also contains anuclear localization signal (NLS) in exons 1–5, indicating that FMRP shuttles between thenucleus and cytoplasm. This has been corrob-orated by electron microscopy (39).
FMRP shows sequence motifs character-istic of RNA-binding proteins. It has twoheterogeneus nuclear ribonucleoprotein KHomology (KH) domains in exons 8 and 10,an Arginine-Glycine-Glycine (RGG) box inexon 15 (7), and an RNA-binding domain inthe amino-terminal region of the protein (2).In vitro it binds to approximately 4% of themRNAs in fetal human brain, including itsown message (7). FMRP has also been shownto associate with polyribosomes in an RNA-dependent manner via messenger ribonucle-oprotein particles (mRNP) of about 660 kDa,which contain several other proteins includ-ing its two autosomal homologs fragile X re-lated protein 1 (FXR1P) and FXR2P encodedby autosomal genes localized to the chromo-somal regions 3q28 and 17p13.1, respectively(123). FXR1P and FXR2P show a 86% and70% level of similarity with FMRP, respec-tively, and show the same principal functionaldomains as FMRP: NLS and NES, the KHdomains, the RGG box, and a homodimer-ization domain. They are mainly localizedto the cytoplasm associated with polysomesas part of the same protein complex. Theyalso shuttle between the nucleus and cyto-plasm, and FXR2P shows a nucleolar local-ization signal (NoS) and shuttles between the
www.annualreviews.org • Fragile X Syndrome 117
Ann
u. R
ev. G
enom
. Hum
an G
enet
. 200
7.8:
109-
129.
Dow
nloa
ded
from
arjo
urna
ls.an
nual
revi
ews.o
rgby
EM
ORY
UN
IVER
SITY
on
08/3
1/09
. For
per
sona
l use
onl
y.

ANRV321-GG08-06 ARI 25 July 2007 17:29
Synaptic plast ici ty:ability of the synapseto change in strengthor change intransmembranepotential
cytoplasm and the nucleolus (108). In addi-tion to FMRP homologs, other proteins thatinteract with FMRP or that are present in thesame complex have been identified. However,it has not been determined whether all com-plexes are the same or if there are differencesin the associated proteins. If they were dif-ferent, each complex could be affected by theabsence of FMRP in a different way. Theseproteins include nuclear FMRP interactingprotein (NUFIP), cytoplasmic FMRP inter-acting protein 1 (CYFIP1) and CYFIP2, an82-kD FMRP interacting protein (82-FIP),nucleolin, and Y-Box factor 1/p50 (YB1/p50)(10, 11, 17, 18, 98).
Posttranslational modifications of FMRPhave also been reported. FMRP was recentlyshown to be normally methylated in the RGGbox, mainly in arginine 544, and this methyla-tion seems to regulate its protein-protein andprotein-RNA interactions (35). FMRP alsoshows a cluster of phosphorylated residues onthe N-terminal side. The primary site of phos-phorylation is at serine 499 and it triggersphosphorylation of nearby residues when theresidue is phosphorylated. This phosphoryla-tion does not affect the rate of degradationof FMRP or the species of RNA with whichFMRP is associated; rather, it has been ob-served that the phosphorylated form of FMRPis associated with apparently stalled polyribo-somes whereas the unphosphorylated form isassociated with actively translating polyribo-somes, suggesting that phosphorylation couldregulate FMRP function (19).
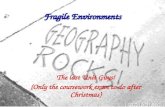
Identification of FMRP mRNA ligands invivo will lead to essential information aboutthe functional roles of FMRP. Several workshave focused on the search for mRNAs boundto the protein (16, 20, 29, 82). These exper-iments led to the identification of mRNAsthat encode for proteins with an importantrole for neuronal function, synaptic plastic-ity, and neuronal maturation. Efforts are be-ing made to elucidate the way that FMRPregulates its target mRNAs. On one hand,FMRP could recognize its targets directly.Darnell et al. (29) showed that the RGG box
binds to an RNA loop structure named Gquartet, where four guanines are stabilizedby Hoogsteen-type hydrogen bonds in a pla-nar conformation. Most of the mRNA targetsidentified for FMRP in the above-mentionedstudies contain a potential G-quartet struc-ture (F igu r e 4). Chen et al. (20) identified an-other set of RNA ligands containing U-richsequences with 5–23 bases of repeating Upentamers. In addition, the KH2 domain hasbeen shown to bind a complex RNA tertiarystructure named loop-loop pseudoknot or“kissing complex” (30). The authors showedthat RNAs with this structure can competeoff the association of FMRP with polyribo-somes, suggesting that this structure couldbe crucial for FMRP translational regulation.On the other hand, an indirect or more com-plex interaction between FMRP and its tar-get mRNAs could occur. Recent data haveshown the association of FMRP with themicroRNA pathway, which suggests a newway that FMRP could modulate translation.MicroRNAs are short (21 nucleotides) non-coding regulatory RNAs that modulate geneexpression by blocking translation of partiallyhomolog mRNAs. MicroRNAs are processedfrom longer RNAs by an RNAse III enzymenamed Dicer and are loaded into an RNA-induced silencing complex (RISC) proteincomplex, which mediates the interaction be-tween microRNAs and their mRNA targets.FMRP associates with both microRNAs andproteins from the RISC complex as well aswith Dicer activity, suggesting that it couldalso be involved in processing microRNAprecursors (66). The “kissing complex” mayrepresent the interaction between an mRNAand a microRNA or other noncoding RNA.FMRP was reported to bind to the smallnonmessenger cytoplasmic RNA BC1, whichsimultaneously associates to mRNA targetsknown to be regulated by FMRP (122). BC1has been suggested to mediate the forma-tion of a translational inhibition complexby association to a polyA-binding proteinand eIF4A (116). However, BC1 is foundin lighter polysome fractions than FMRP,
118 Penagarikano · M ulle · Warren
Ann
u. R
ev. G
enom
. Hum
an G
enet
. 200
7.8:
109-
129.
Dow
nloa
ded
from
arjo
urna
ls.an
nual
revi
ews.o
rgby
EM
ORY
UN
IVER
SITY
on
08/3
1/09
. For
per
sona
l use
onl
y.

ANRV321-GG08-06 ARI 25 July 2007 17:29
b
c
a
UU
U
AGUC
A
GUGGCGUCGG5'
3'
UUGCGCA
A G G G UA
A U G UU
G G C G G A
A
A AA
AAA
U UU
A G
GG
GGGCU
U C C U AGC
AG
U A C AU
C U G C G
UAAA
AA
A A
U CG
G
G G C
GU
U
ACCCC
C G G
UU
U G G U CC C A G
G
G
G
G
GCU
UUU
3'
31
33
34
42
40
38
37
43
46
47
48
51
G G
AGU
G GG G
G G
5'
F igu r e 4
RNA structuresrecognized by fragileX mental retardationprotein (FMRP).(a) G quartet, (b) Upentamer, (c) kissingcomplex.
making their direct interaction unlikely (68).Recent data support the interaction of FMRPwith the RISC complex in regulating synap-tic protein synthesis. FMRP interacts withthe calcium-calmodulin-dependent kinase II(CaMKII) mRNA, from which dendritic lo-cal protein synthesis is required for memoryformation (48). Translation of this mRNA isinhibited by RISC and relieved by neuronalstimulation, associating the miRNA pathwaywith the control of local protein synthesis inneurons (8).
N E U R O N A L - M O L E C U L A RC O N N E C T I O N
FMRP expression is widely seen during mouseembryogenesis. During development, the ex-pression level diminishes in some tissues,leading to a more specific expression pat-tern (9). In humans, embryonic studies haveshown FMRP expression in the central ner-vous system of a 9-week-old fetus whereasin a 25-week-old fetus FMRP expressionwas restricted to neurons (1). Autopsies per-formed in individuals affected with FXS have
www.annualreviews.org • Fragile X Syndrome 119
Ann
u. R
ev. G
enom
. Hum
an G
enet
. 200
7.8:
109-
129.
Dow
nloa
ded
from
arjo
urna
ls.an
nual
revi
ews.o
rgby
EM
ORY
UN
IVER
SITY
on
08/3
1/09
. For
per
sona
l use
onl
y.

ANRV321-GG08-06 ARI 25 July 2007 17:29
D e n d r i t ic spi n e:small membranousextrusion thatprotrudes from adendrite (branchedprojections of aneuron) and formsone half of a synapse
Synapse: specializedjunction throughwhich cells of thenervous systemsignal to one anotherfrom axons todendrites
L T P: long-termpotentiation
L T D : long-termdepression
made the associated brain abnormalities ap-parent. They show more immature (longerand thinner) dendritic spines, where mostof the synapses occur, and a higher densityof them, suggesting a possible misregulationin their development and elimination (65).An abnormal development of dendritic spinesin FMR1 knockout mice has also been re-ported (85). During development, synapsesare often produced in numbers that exceedthose that will ultimately survive. Maturationand pruning are therefore important to es-tablish the final synaptic pattern. Abnormal-ities in the dendritic spines have also beenassociated with nonsyndromic mental retar-dation as well as with Down, Rett, Coffin-Lowry, and Rubinstein-Taybi syndromes (34).One of the neurological problems in FXSlikely associated with this spine morphol-ogy is the presence of epileptic seizures be-cause the characteristic spine morphologycould cause a greater neuronal excitation (64).Specific proteins and biochemical pathwayshave been associated with spine morpho-genesis; many of these pathways ultimatelylead to actin rearrangement in the spine cy-toskeleton. The local synthesis of FMRP canpotentially influence other proteins or sig-naling cascades involved in morphogenesissuch as Rac1, MAP1B, CaMKII, calbindin,alpha-glucocorticoid receptor, and cadherins(48). Thus, FXS is considered a synapticdisease.
FMRP is an RNA-binding protein asso-ciated with polyribosomes, suggesting thatit has a role in modulating protein synthe-sis in neurons, where it is largely expressed.In neurons, protein synthesis in both cellbodies and dendritic spines is important forsynaptic plasticity, and certain mRNAs aretranslated in response to a specific synap-tic activation. Synaptic plasticity is essen-tial for memory and learning processes andinvolves long-term potentiation (LTP) andlong-term depression (LTD), which are as-sociated with synapse creation and elimi-nation in addition to synaptic transmission.Depending on the brain region, synaptic plas-
ticity is expressed pre- and/or postsynapti-cally. At the postsynaptic level, LTD canbe triggered by the activation of postsynap-tic N-methyl-D-aspartate (NMDA) recep-tors or group I metabotropic glutamate re-ceptors (mGluRs). Both types of LTD donot occlude each other, but result in a de-crease of surface expression of alpha-amino-3-hydroxy-5-methylisoxazole-4-propionic acid(AMPA) receptors (61). The activation ofgroup I mGluRs (mGluR1 and mGluR5) wasreported to stimulate the synthesis of FMRPin synapses (118) and in neuronal lysate (59).Fmr1 knockout mice (36) showed enhancedmGluR-LTD in the hippocampal Schaffercollateral synapses of the CA1 area (60) andin the cerebellar parallel fiber to Purkinje cellsynapses (67). NMDAR-LTD in Fmr1 knock-out mice remained the same as that in thewild-type control, indicating that the pheno-type was specific to the mGluR-dependentform of synaptic plasticity. In addition, pro-tein synthesis dependent on mGluR activationwas enhanced in the absence of FMRP (60).These data led to the hypothesis that FMRPnormally represses further protein synthesis(13). It was recently shown that the rapidincrease in FMRP synthesis associated withthe stimulation that can cause mGluR-LTDis transient and followed by a rapid decreasein FMRP back to baseline levels, suggestingthat FMRP is dynamically regulated duringmGluR-LTD, with rapid synthesis followedby rapid degradation in hippocampal slicesand homogenate. The authors also showedthat the ubiquitin-proteasome degradationpathway played a role in FMRP regulationafter mGluR stimulation because FMRP waspolyubiquitinated in the same temporal win-dow where its levels begin to decline (59).Therefore, it is reasonable to propose thatthe rapid degradation of FMRP might be re-quired to permit its target mRNAs to be trans-lated and consolidate mGluR-LTD. In ad-dition to local protein synthesis at synapses,FMRP appears to be involved in the mRNAtransport to the synaptic locations. Stimu-lation of mGluRs increases the transport of
120 Penagarikano · M ulle · Warren
Ann
u. R
ev. G
enom
. Hum
an G
enet
. 200
7.8:
109-
129.
Dow
nloa
ded
from
arjo
urna
ls.an
nual
revi
ews.o
rgby
EM
ORY
UN
IVER
SITY
on
08/3
1/09
. For
per
sona
l use
onl
y.

ANRV321-GG08-06 ARI 25 July 2007 17:29
FMRP-containing granules to the dendrites(5, 6). Together, these data suggest a dual rolefor FMRP: delivery and release of mRNAs foractivity-dependent translation.
T R E A T M E N T
Useful guidelines for health supervision ofFX children were published by the AmericanAcademy of Pediatrics (4) and include advicefor both physical and behavioral componentsof the syndrome. The therapy currently usedin FX individuals is designed specifically foreach patient and is focused on his/her specificbehavior symptoms. Unfortunately, there isnot yet a treatment to compensate for the ab-sence of FMRP. Attempts have been made toreactivate the silenced FMR1 gene and there-fore restore the production of the protein (21,92); however, reactivation processes are toogeneral and genes other than FMR1 may bereactivated. In addition, toxicity of such ap-proaches is very high. Regardless, reactivationof a full mutation would still produce a tran-script with a long repeat that renders the mes-sage inefficiently translated. The possibilityof gene therapy is currently not possible dueto difficulties in the delivery of the normalgene into neurons and its restoration of thephenotype.
More recently, the understanding of thefunction of FMRP and the consequence ofits absence has led to potential therapeu-tic approaches. Because FMRP is a transla-tional suppressor and mGluR 5 activation ofthe excitatory pathway stimulates local pro-tein synthesis, the absence of FMRP leadsto the apparent overstimulation of translationby mGluR5 signaling (13). This imbalance,which has fundamental consequences with re-gard to synaptic plasticity, may be counteredby mGluR5 antagonists (F igu r e 5). One suchantagonist is MPEP. Remarkably, MPEP wasrecently shown to be highly efficient in res-cuing phenotypes associated with FMRP lossin animal models for FXS. In the Drosophilamodel, McBride et al. (80) showed that MPEPcan rescue memory deficits in courtship be-
mGluR1/5
FMRP
mRNAtranslation
mGluR1/5
FMRP
mRNAtranslation
Fragile Xsyndrome
Normal
Drugtargets?Translation stimulation
Translation suppression
F igu r e 5
Role of fragile X mental retardation protein (FMRP) in modulatingsynaptic plasticity. The activation of group I metabotropic receptors(mGluR) stimulates translation of specific mRNAs at synapses. FMRPnormally acts as a translational repressor regulating such expression;however, in the absence of FMRP, overexpression of such messages isfound.
havior and mushroom body defects observedin mutant flies. Similarly, Yan et al. (121)showed that FMR1 knockout mice treatedwith MPEP exhibit a reduction in the sensi-tivity to audiogenic seizures and respond bet-ter to the open field test, with a reduced ten-dency to mainly be in the center of the field.Using zebrafish as a model for the study ofhuman FXS, Tucker et al. (111) recently re-ported that MPEP was able to rescue the ax-onal branching defect observed in these ani-mals. These data indicate that the interactionbetween mGluR signaling and FMR1 func-tion is responsible for some of the symptomsassociated with FXS. Thus, drugs targetingmGLuR5 or downstream signaling may be oftherapeutic potential in FXS. It is anticipatedthat clinical trials will begin within the nexttwo years. FXS is instructive regarding geneticdisease in general. Once given the “toe hold”of the identification of the responsible gene,basic scientific investigation into the nor-mal and abnormal function of encoded pro-teins can lead to sufficient molecular under-standing to suggest traditional pharmacologicinterventions for even the most seeminglyintractable disorders.
www.annualreviews.org • Fragile X Syndrome 121
Ann
u. R
ev. G
enom
. Hum
an G
enet
. 200
7.8:
109-
129.
Dow
nloa
ded
from
arjo
urna
ls.an
nual
revi
ews.o
rgby
EM
ORY
UN
IVER
SITY
on
08/3
1/09
. For
per
sona
l use
onl
y.

ANRV321-GG08-06 ARI 25 July 2007 17:29
S U M M A R Y P O I N T S
1. FXS is the most common form of inherited mental retardation, has striking behavioraloverlap with autism, and may be considered the best-understood form of autism.
2. FXS is caused by the functional absence of FMRP encoded by the FMR1 X-linkedgene, usually due to silencing of the gene caused by expansion of the trinucleotiderepeat CGG located in its 5 UTR.
3. FMRP is a selective RNA-binding protein associated with polyribosomes and ex-pressed in neurons including the dendritic spine, where it has been shown to regulatetranslation of mRNAs important for synaptic plasticity and neuronal maturation.
4. How FMRP plays its role in translational regulation is still unclear and involves directinteraction with mRNAs as well as interaction with the microRNA pathway.
F U T U R E ISS U E S T O B E R E S O L V E D
1. Animal models for both expansion of the CGG repeat and silencing of the FMR1gene will be essential to determine the timing and mechanism of repeat expansionand subsequent epigenetic changes in FMR1.
2. The molecular details of how FMRP regulates mRNA translation need to be eluci-dated as does the regulation of FMRP itself.
3. A better understanding is needed of the role of FMRP in local protein synthesis inthe dendrite, its normal role in synaptic plasticity, and the neuronal consequence ofits absence.
4. Pharmacological approaches have been identified that may compensate for the loss ofFMRP, and therapeutic approaches now need to be developed to improve the qualityof life of patients with fragile X syndrome.
D IS C L O S U R E S T A T E M E N T
SW serves as Chair of the Scientific Advisory Committee for Seaside Therapeutics, Inc.
LITERATURE CITED1. Abitbol M, Menini C, Delezoide AL, Rhyner T, Vekemans M, Mallet J. 1993. Nucleus
basalis magnocellularis and hippocampus are the major sites of FMR-1 expression in thehuman fetal brain. Nat. Genet. 4(2):147–55
2. Adinolfi S, Ramos A, Martin SR, Dal Piaz F, Pucci P, et al. 2003. The N-terminus of theFragile X mental retardation protein contains a novel domain involved in dimerizationand RNA binding. Biochemistry 42(35):10437–44
3. Allingham-Hawkins DJ, Babul-Hirji R, Chitayat D, Holden JJ, Yang KT, et al. 1999.Fragile X premutation is a significant risk factor for premature ovarian failure: theInternational Collaborative POF in Fragile X study—preliminary data. Am. J. Med. Genet.83(4):322–25
122 Penagarikano · M ulle · Warren
Ann
u. R
ev. G
enom
. Hum
an G
enet
. 200
7.8:
109-
129.
Dow
nloa
ded
from
arjo
urna
ls.an
nual
revi
ews.o
rgby
EM
ORY
UN
IVER
SITY
on
08/3
1/09
. For
per
sona
l use
onl
y.

ANRV321-GG08-06 ARI 25 July 2007 17:29
4. American Academy of Pediatrics Committee on Genetics. 1996. Health supervision forchildren with Fragile X syndrome Pediatrics. 98(3 Pt 1):467–72
5. Antar LN, Dictenberg JB, Plociniak M, Afroz R, Bassell GJ. 2005. Localization of FMRPassociated mRNA granules and requirement of microtubules for activity-dependent traf-ficking in hippocampal neurons. Genes Brain Behav. 4:350–59
6. Antar LN, Afroz R, Dictenberg JB, Carroll RC, Bassell GJ. 2004. Metabotropic glutamatereceptor activation regulates Fragile X mental retardation protein and FMR1 mRNAlocalization differentially in dendrites and at synapses. J. Neurosci. 24(11):2648–55
7. K ey r epo r tsh o wi ng t h eR N A - bi n di ngp r ope r ties ofF M R P an d givi ngt h e fi rst i nsigh ti n to i ts m olecu larfu nct io n .
7. Ash ley C T J, W il k i nso n K D , R ei n es D , W ar r e n S T . 1993. F M R 1 p r ot ei n: co nse rvedR N P fam ily do mai ns an d select ive R N A bi n di ng. Science 262(5133):563–66
8. Ashraf SI, McLoon AL, Sclarsic SM, Kunes S. 2006. Synaptic protein synthesis associatedwith memory is regulated by the RISC pathway in Drosophila. Cell 124:191–205
9. Bakker CE, de Diego Otero Y, Bontekoe C, Raghoe P, Luteijn T, et al. 2000. Immunocy-tochemical and biochemical characterization of FMRP, FXR1P, and FXR2P in the mouse.Exp. Cell. Res. 258(1):162–70
10. Bardoni B, Castets M, Huot ME, Schenck A, Adinolfi S, et al. 2003. 82-FIP, a novel FMRP(fragile X mental retardation protein) interacting protein, shows a cell cycle-dependentintracellular localization. Hum. Mol. Genet. 12(14):1689–98
11. Bardoni B, Schenck A, Mandel JL. 1999. A novel RNA-binding nuclear protein that inter-acts with the fragile X mental retardation (FMR1) protein. Hum. Mol. Genet. 8(13):2557–66
12. Barker GC. 2002. Microsatellite DNA: a tool for population genetic analysis. Trans. R.Soc. Trop. Med. Hyg. 96(Suppl. 1):21–24
13. A n ove rvie w oft h e r ole of F M R Pi n synapticplast ici ty w h e r e t h eau t h o rs p r ese n t at h eo ry t hat canacco u n t fo r dive rsen e u r ological an dpsych iat r ic aspectsof F X S.
13. B ear M F , H u be r K M , W ar r e n S T . 2004. T h e m G l u t h eo ry of F ragile X m e n talr e tar dat io n . Trends Neurosci. 27(7):370–77
14. Berger R, Bloomfield CD, Sutherland GR. 1985. Report of the committee on chromo-some rearrangements in neoplasia and on fragile sites. Cytogenet. Cell. Genet. 40(1–4):490–535
15. Brouwer JR, Mientjes EJ, Bakker CE, Niewenhuizen IM, Severijnen LA, et al. 2006.Elevated Fmr1 mRNA levels and reduced protein expression in a mouse model with anunmethylated Fragile X full mutation. Exp. Cell Res. 313(2):244–53
16. T h e fi rstide n ti ficat io n ofcan didat e m R N Asr egu lat ed by F M R Pi n m o use b rai n .
16. B r ow n V , Ji n P , C e man S, D ar n ell J C , O ’ D o n ell W T , e t al. 2001. M icr oar rayide n ti ficat io n of F M R P -associat ed b rai n m R N As an d al t e r ed m R N A t ranslat io nalp r o fi les i n F ragile X syn d r o m e. Cell 107(4):477–87
17. Ceman S, Brown V, Warren ST. 1999. Isolation of an FMRP-associated messenger ri-bonucleoprotein particle and identification of nucleolin and the fragile X-related proteinsas components of the complex. Cell. Biol. 19:7925–32
18. Ceman S, Nelson R, Warren ST. 2000. Identification of mouse YB1/p50 as a componentof the FMRP-associated mRNP particle. Biochem. Biophys. Res. Commun. 279(3):904–8
19. Ceman S, O’Donnell WT, Reed M, Patton S, Pohl J, Warren ST. 2003. Phosphorylationinfluences the translation state of FMRP associated polyribosomes. Hum. Mol. Genet.12:3295–305
20. Chen L, Yun SW, Seto J, Liu W, Toth M. 2003. The Fragile X mental retardationprotein binds and regulates a novel class of mRNAs containing U rich target sequences.Neuroscience 120(4):1005–17
21. Chiurazzi P, Pomponi MG, Pietrobono R, Bakker CE, Neri G, et al. 1999. Synergisticeffect of histone hyperacetylation and DNA demethylation in the reactivation of theFMR1 gene. Hum. Mol. Genet. 8(12):2317–23
www.annualreviews.org • Fragile X Syndrome 123
Ann
u. R
ev. G
enom
. Hum
an G
enet
. 200
7.8:
109-
129.
Dow
nloa
ded
from
arjo
urna
ls.an
nual
revi
ews.o
rgby
EM
ORY
UN
IVER
SITY
on
08/3
1/09
. For
per
sona
l use
onl
y.

ANRV321-GG08-06 ARI 25 July 2007 17:29
22. Chiurazzi P, Tabolacci E, Neri G. 2004. X-linked mental retardation (XLMR): fromclinical conditions to cloned genes. Crit. Rev. Clin. Lab. Sci. 41(2):117–58
23. Chudley AE, Hagerman RJ. 1987. Fragile X syndrome. J. Pediatr. 110(6):821–3124. Coffee B, Zhang F, Ceman S, Warren ST, Reines D. 2002. Histone modifications depict
an aberrantly heterochromatinized FMR1 gene in Fragile X syndrome. Am. J. Hum.Genet. 71(4):923–32
25. Coffee B, Zhang F, Warren ST, Reines D. 1999. Acetylated histones are associated withFMR1 in normal but not fragile X-syndrome cells. Nat. Genet. 22(1):98–101
26. Cornish K, Sudhalter V, Turk J. 2004. Attention and language in fragile X. Ment. Ret.Dev. Dis. 10:11–16
27. Cronister A, Schreiner R, Wittenberger M, Amiri K, Harris K, et al. 1991. Heterozygousfragile X female: historical, physical, cognitive, and cytogenetic features. Am. J. Med.Genet. 38(2–3):269–74
28. T h e lat estr evie w o n t h egr ow i ng n u m be r ofdiseases k n o w n tobe caused byt r i n ucleo tider epeat expansio nssi nce t h e discove ryof t h e causat ivem u tat io n of F X S.
28. C u m m i ngs C J, Z ogh bi H Y . 2000. T r i n ucleot ide r epeats: m echan isms an d pat h o -p hysiology. Annu. Rev. Genomics Hum. Genet. 1:281–328
29. Darnell JC, Jensen KB, Jin P, Brown V, Warren ST, et al. 2001. Fragile X mental retarda-tion protein targets G quartet mRNAs important for neuronal function. Cell 107(4):489–99
30. Darnell JC, Fraser CE, Mostovetsky O, Stefani G, Jones TA, et al. 2005. Kissing complexRNAs mediate interaction between the Fragile X mental retardation protein KH2 domainand brain polyribosomes. Genes Dev. 19:903–18
31. de Boulle K, Verkerk AJMH, Reyniers E, Vits L, Hendrickx J, et al. 1993. A point mutationin the FMR-1 gene associated with the Fragile X mental retardation. Nat. Genet. 3:31–35
32. de Vries BB, Fryns JP, Butler MG, Canziani F, Wesby-van Swaay E, et al. 1993. Clinicaland molecular studies in fragile X patients with a Prader-Willi-like phenotype. J. Med.Genet. 30(9):761–66
33. Devys D, Lutz Y, Rouyer N, Bellocq JP, Mandel JL. 1993. The FMR-1 protein iscytoplasmic, most abundant in neurons and appears normal in carriers of a Fragile Xpremutation. Nat. Genet. 4:335–40
34. Dierssen M, Ramakers GJ. 2006. Dendritic pathology in mental retardation: from molec-ular genetics to neurobiology. Genes Brain Behav. 5(Suppl. 2):48–60
35. Dolzhanskaya N, Merz G, Aletta JM, Denman RB. 2006. Methylation regulates the intra-cellular protein-protein and protein-RNA interactions of FMRP. J. Cell Sci. 119:1933–46
36. Dutch-Belgian Fragile X Consortium. 1994. Fmr1 knockout mice: a model to studyfragile X mental retardation. Cell 78:23–33
37. Eichler EE, Holden JJ, Popovich BW, Reiss AL, Snow K, et al. 1994. Length of uninter-rupted CGG repeats determines instability in the FMR 1 gene. Nat. Genet. 8(1):88–94
38. Eichler EE, Richards S, Gibbs RA, Nelson DL. 1993. Fine structure of the human FMR1gene. Hum. Mol. Genet. 2(8):1147–53
39. P laces F M R P i nt h e postsynap ticco m par t m e n ti m plicat i ng it i nlocal p r ot ei nsyn t h esis.
39. F e ng Y , G u t e k u nst C , E be r har t D E , Yi H , W ar r e n S T , e t al. 1997. F ragile X m e n talr e tar dat io n p r o t ei n: n ucleocyt oplasm ic sh u t t li ng an d associat io n wit h so mat ode n -d r it ic r iboso m es. J. Neurosci. 17(5):1539–47
40. Feng Y, Zhang F, Lokey LK, Chastain JL, Lakkis L, et al. 1995. Translational suppressionby trinucleotide repeat expansion at FMR1. Science 268(5211):731–34
41. Fisch GS, Simensen RJ, Schroer RJ. 2002. Longitudinal changes in cognitive and adaptivebehavior scores in children and adolescents with the Fragile X mutation or autism. J.Autism Dev. Disord. 32(2):107–14
124 Penagarikano · M ulle · Warren
Ann
u. R
ev. G
enom
. Hum
an G
enet
. 200
7.8:
109-
129.
Dow
nloa
ded
from
arjo
urna
ls.an
nual
revi
ews.o
rgby
EM
ORY
UN
IVER
SITY
on
08/3
1/09
. For
per
sona
l use
onl
y.

ANRV321-GG08-06 ARI 25 July 2007 17:29
42. Fisch GS, Snow K, Thibodeau SN, Chalifaux M, Holden JJ, et al. 1995. The Fragile Xpremutation in carriers and its effect on mutation size in offspring. Am. J. Hum. Genet.56(5):1147–55
43. Fryns JP. 1984. The fragile X syndrome. A study of 83 families. Clin. Genet. 26(6):497–52844. Fu Y, Kuhl DPA, Pizzuti A, Pieretti M, Sutcliffe JS, et al. 1991. Variation of the CGG
repeat at the Fragile X site results in genetic instability: resolution of the Sherman paradox.Cell 67:1047–58
45. Gedeon AK, Baker E, Robinson H, Partington MW, Gross B, et al. 1992. Fragile Xsyndrome without CCG amplification has an FMR1 deletion. Nat. Genet. 1(5):341–44
46. Gheldof N, Tabuchi TM, Dekker J. 2006. The active FMR1 promoter is associatedwith a large domain of altered chromatin conformation with embedded local histonemodifications. Proc. Natl. Acad. Sci. USA 103(33):12463–68
47. Greco CM, Hagerman RJ, Tassone F, Chudley AE, Del Bigio MR, et al. 2002. Neu-ronal intranuclear inclusions in a new cerebellar tremor/ataxia syndrome among fragileX carriers. Brain 125(Pt. 8):1760–71
48. Grossman AW, Aldridge GM, Weiler IJ, Greenough WT. 2006. Local protein synthesisand spine morphogenesis: Fragile X syndrome and beyond . J. Neurosci. 26(27):7151–55
49. Hagerman PJ, Greco CM, Hagerman RJ. 2003. A cerebellar tremor/ataxia syndromeamong fragile X premutation carriers. Cytogenet. Genome Res. 100(1–4):206–12
50. Hagerman RJ, Hull CE, Safanda JF, Carpenter I, Staley LW, et al. 1994. High functioningFragile X males: demonstration of an unmethylated fully expanded FMR-1 mutationassociated with protein expression. Am. J. Med. Genet. 51(4):298–308
51. Hagerman RJ, McBogg P, Hagerman PJ. 1983. The Fragile X syndrome: history, diag-nosis, and treatment. J. Dev. Behav. Pediatr. 4(2):122–30
52. Hammond LS, Macias MM, Tarleton JC, Pai GS. 1997. Fragile X syndrome and deletionsin FMR1: new case and review of the literature. Am. J. Med. Genet. 72:430–34
53. Harrison CJ, Jack EM, Allen TD, Harris R. 1983. The fragile X: a scanning electronmicroscope study. J. Med. Genet. 20(4):280–85
54. Heitz D, Rousseau F, Devis D, Saccone S, Abderrahim H, et al. 1991. Isolation of se-quences that span the fragile X and identification of a fragile X related CpG island. Science251:1236–39
55. Hessl D, Rivera SM, Reiss AL. 2004. The neuroanatomy and neuroendocrinology ofFragile X syndrome. Ment. Ret. Dev. Dis. 10:17–24
56. Hirst M, Grewal P, Flannery A, Slatter R, Maher E, et al. 1995. Two new cases of FMR1deletion associated with mental impairment. Am. J. Hum. Genet. 56(1):67–74
57. Hirst MC, Rack K, Nakahori Y, Roche A, Bell MV, et al. 1991. A YAC contig across thefragile X site defines the region of fragility. Nucleic Acids Res. 19(12):3283–88
58. Hjalgrim H, Fisher Hansen B, Brondum-Nielsen K, Nolting D, Kjaer I. 2000. Aspectsof skeletal development in Fragile X syndrome fetuses. Am. J. Med. Genet. 95(2):123–29
59. Hou L, Antion MD, Hu D, Spencer CM, Paylor R, Klann E. 2006. Dynamic translationaland proteasomal regulation of fragile X mental retardation protein controls mGluR-dependent long-term depression. Neuron 51(4):441–54
60. Huber KM, Gallagher SM, Warren ST, Bear MF. 2002. Altered synaptic plasticity in amouse model of Fragile X mental retardation. Proc. Nat. Acad. Sci. USA 99(11):7746–50
61. Huber KM, Kayser MS, Bear MF. 2000. Role for rapid dendritic protein synthesis inhippocampal mGluR-dependent long-term depression. Science 288(5469):1254–57
62. IHGSC (International Human Genome Sequencing Consortium). 2001. Initial sequenc-ing analysis of the human genome. Nature 409:860–921
www.annualreviews.org • Fragile X Syndrome 125
Ann
u. R
ev. G
enom
. Hum
an G
enet
. 200
7.8:
109-
129.
Dow
nloa
ded
from
arjo
urna
ls.an
nual
revi
ews.o
rgby
EM
ORY
UN
IVER
SITY
on
08/3
1/09
. For
per
sona
l use
onl
y.

ANRV321-GG08-06 ARI 25 July 2007 17:29
63. Imbert G, Feng Y, Nelson DL, Warren ST, Mandel JL. 1998. FMR1 and mutations inFragile X syndrome: molecular biology, biochemistry, and genetics. In Genetic Instabilitiesand Hereditary Neurological Diseases, ed. RD Wells, ST Warren, 3:27–53. San Diego:Academic
64. Incorpora G, Sorge G, Sorge A, Pavone L. 2002. Epilepsy in Fragile X syndrome. Brain.Dev. 24(8):766–69
65. Irwin SA, Patel B, Idupulapati M, Harris JB, Crisostomo RA, et al. 2001. Abnormaldendritic spine characteristics in the temporal and visual cortices of patients with fragile-Xsyndrome: a quantitative examination. Am. J. Med. Genet. 98(2):161–67
66. F i rst r epo r tsh o w i ng t h e i n vivoi n t e ract io nbe t w ee nmam mal ian F M R Pan d bo t hm icr o R N As an dt h e co m po n e n ts oft h e m icr o R N Apat h way.
66. Ji n P , Z ar n escu D C , C e man S, N akam ot o M , M ow r ey J, e t al. 2004. B ioch e m icalan d ge n e t ic i n t e ract io n be t w ee n t h e F ragile X m e n tal r e tar dat io n p r ot ei n an d t h em icr o R N A pat h way. Nat. Neurosci. 7(2):113–17
67. Koekkoek SK, Yamaguchi K, Milojkovic BA, Dortland BR, Ruigrok TJ, et al. 2005.Deletion of FMR1 in Purkinje cells enhances parallel fiber LTD, enlarges spines, andattenuates cerebellar eyelid conditioning in Fragile X syndrome. Neuron 47(3):339–52
68. Krichevsky AM, Kosik KS. 2001. Neuronal RNA granules: a link between RNA local-ization and stimulation-dependent translation. Neuron 32(4):683–96
69. Kumari D, Gabrielian A, Wheeler D, Usdin K. 2005. The roles of Sp1, Sp3, USF1/USF2and NRF-1 in the regulation and three-dimensional structure of the Fragile X mentalretardation gene promoter. Biochem. J. 386(Pt. 2):297–303
70. Kunkel TA. 1993. Nucleotide repeats. Slippery DNA and diseases. Nature 365(6443):207–8
71. Kunst CB, Warren ST. 1994. Cryptic and polar variation of the Fragile X repeat couldresult in predisposing normal alleles. Cell 17:853–61
72. Lee S, Park MS. 2002. Human FEN-1 can process the 5 -flap DNA of CTG/CAG tripletrepeat derived from human genetic diseases by length and sequence dependent manner.Exp. Mol. Med. 34(4):313–17
73. Lehrke RG. 1974. X-linked mental retardation and verbal disability. Birth Defects Orig.Artic. Ser. 10(1):1–100
74. Loehr JP, Synhorst DP, Wolfe RR, Hagerman RJ. 1986. Aortic root dilatation and mitralvalve prolapse in the Fragile X syndrome. Am. J. Med. Genet. 23(1–2):189–94
75. Losekoot M, Hoogendoorn E, Olmer R, Jansen CC, Oosterwijk JC, et al. 1997. Prenataldiagnosis of the Fragile X syndrome: loss of mutation owing to a double recombinant orgene conversion event at the FMR1 locus. J. Med. Genet. 34(11):924–26
76. Lubs HA. 1969. A marker X chromosome. Am. J. Hum. Genet. 21(3):231–4477. Lugenbeel KA, Peier AM, Carson NL, Chudley AE, Nelson DL. 1995. Intragenic loss of
function mutations demonstrate the primary role of FMR1 in Fragile X syndrome. Nat.Genet. 10(4):483–85
78. Malter H, Iber JC, Willemsen R, Graaff E, Tarleton JC, et al. 1997. Characterization ofthe full Fragile X syndrome mutation in fetal gametes. Nat. Genet. 15:165–69
79. Martin J, Bell J. 1943. A pedigree of mental defect showing sex linkage. Arch. Neurol.Psychiat. 6:154–57
80. McBride SM, Choi CH, Wang Y, Liebelt D, Braunstein E, et al. 2005. Pharmacolog-ical rescue of synaptic plasticity, courtship behaviour and mushroom body defects in aDrosophila model for fragile X syndrome. Neuron 45(5):753–64
81. Meijer H, de Graaff E, Merckx DM, Jongbloed RJ, de Die-Smulders CE, et al. 1994.A deletion of 1.6 kb proximal to the CGG repeat of the FMR1 gene causes the clinicalphenotype of the Fragile X Syndrome. Hum. Mol. Genet. 3(4):615–20
126 Penagarikano · M ulle · Warren
Ann
u. R
ev. G
enom
. Hum
an G
enet
. 200
7.8:
109-
129.
Dow
nloa
ded
from
arjo
urna
ls.an
nual
revi
ews.o
rgby
EM
ORY
UN
IVER
SITY
on
08/3
1/09
. For
per
sona
l use
onl
y.

ANRV321-GG08-06 ARI 25 July 2007 17:29
82. Miyashiro KY, Beckel-Mitchener A, Purk TP, Becker KG, Barret T, et al. 2003. RNAcargoes associating with FMRP reveal deficits in cellular functioning in FMR1 null mice.Neuron 37(3):417–31
83. Moutou C, Vincent MC, Biancalana V, Mandel JL. 1997. Transition from premutationto full mutation in Fragile X syndrome is likely to be prezygotic. Hum. Mol. Genet.6(7):971–79
84. Nielsen KB, Tommerup N, Poulsen H, Mikkelsen M. 1981. X-linked mental retardationwith fragile X. A pedigree showing transmission by apparently unaffected males andpartial expression in female carriers. Hum. Genet. 59(1):23–25
85. Nimchinsky EA, Oberlander AM, Svoboda K. 2001. Abnormal development of dendriticspines in FMR1 knock-out mice. J. Neurosci. 21(14):5139–46
86. C ollabo rat ivest u dy of 13labo rato r ies i n 8co u n t r ies wasestablish ed toexam i n e fo u r issu esco nce r n i ng F M R 1C G G - r epeati nstabili ty.
86. N oli n S, B r o w n W T , G licksman A , H o uck G E , G argan o A D , e t al. 2003. E xpansio nof t h e F ragile X C G G r epeat i n fe males w it h p r e m u tat io n o r i n t e r m ediat e al leles.Am. J. Hum. Genet. 72:454–64
87. Nolin SL, Lewis FA, Ye LL, Houck GE, Glicksman AE, et al. 1996. Familial transmissionof the FMR1 CGG repeat. Am. J. Med. Genet. 59:1252–61
88. Oberle I, Rousseau F, Heitz D, Kretz C, Devys D, et al. 1991. Instability of a 550 base pairDNA segment and abnormal methylation in fragile X syndrome. Science 252:1097–102
89. Pearson CE, Edamura KN, Cleary JD. 2005. Repeat instability: mechanisms of dynamicmutations. Nat. Rev. Genet. 6(10):729–42
90. Penrose LS. 1938. A clinical and genetic study of 1,280 cases of mental defect. In SpecialReport Series, Medical Research Council 299. London: Her Majesty’s Stationary Office
91. Pieretti M, Zhang F, Fu YH, Warren ST, Oostra BA, et al. 1991. Absence of expressionof the FMR1 gene in Fragile X syndrome. Cell 66:817–22
92. Pietrobono R, Pomponi MG, Tabolacci E, Oostra BA, Chiurazzi P, et al. 2002. Quanti-tative analysis of DNA demethylation and transcriptional reactivation of the FMR1 genein Fragile X cells treated with 5-azadeoxycytidine. Nucl. Acids Res. 30(14):3278–85
93. Richards RI, Sutherland GR. 1994. Simple repeat DNA is not replicated simply. Nat.Genet. 6(2):114–16
94. Richards RI, Sutherland GR. 1997. Dynamic mutation: possible mechanisms and signif-icance in human disease. Trends Biochem. Sci. 22(11):432–36
95. Rousseau F, Heitz D, Biancalana V, Blumenfeld S, Kretz C, et al. 1991. Direct diagnosisby DNA analysis of the Fragile X syndrome of mental retardation. N. Engl. J. Med.325(24):1673–81
96. Rousseau F, Rouillard P, Morel ML, Khandjian EW, Morgan K. 1995. Prevalence ofcarriers of premutation size alleles of the FMR1 gene and implications for the populationgenetics of the fragile X syndrome. Am. J. Hum. Genet. 57:1006–18
97. Santoro N. 2003. Mechanisms of premature ovarian failure. Ann. Endocrinol. (Paris)64(2):87–92
98. Schenck A, Bardoni B, Moro A, Bagni C, Mandel JL. 2001. A highly conserved proteinfamily interacting with the fragile X mental retardation protein (FMRP) and displayingselective interactions with FMRP-related proteins FXR1P and FXR2P. Proc. Natl. Acad.Sci. USA 98(15):8844–49
99. Sherman SL, Jacobs PA, Morton NE, Froster-Iskenius U, Howard-Peebles PN, et al.1985. Further segregation analysis of the Fragile X syndrome with special reference totransmitting males. Hum. Genet. 69(4):289–99
100. Sherman SL, Morton NE, Jacobs PA, Turner G. 1984. The marker (X) syndrome: acytogenetic and genetic analysis. Ann. Hum. Genet. 48(Pt. 1):21–37
www.annualreviews.org • Fragile X Syndrome 127
Ann
u. R
ev. G
enom
. Hum
an G
enet
. 200
7.8:
109-
129.
Dow
nloa
ded
from
arjo
urna
ls.an
nual
revi
ews.o
rgby
EM
ORY
UN
IVER
SITY
on
08/3
1/09
. For
per
sona
l use
onl
y.

ANRV321-GG08-06 ARI 25 July 2007 17:29
101. Siomi H, Siomi MC, Nussbaum RL, Dreyfuss G. 1993. The protein product of the fragileX gene, FMR1, has characteristics of an RNA-binding protein. Cell 74(2):291–98
102. Sittler A, Devys D, Weber C, Mandel JL. 1996. Alternative splicing of exon 14 determinesnuclear or cytoplasmic localisation of FMR1 protein isoforms. Hum. Mol. Genet. 5(1):95–102
103. Smith KT, Nicholls RD, Reines D. 2006. The gene encoding the fragile X RNA-bindingprotein is controlled by nuclear respiratory factor 2 and the CREB family of transcriptionfactors. Nucl. Acids Res. 34(4):1205–15
104. Sullivan AK, Marcus M, Epstein MP, Allen EG, Anido AE, et al. 2005. Association ofFMR1 repeat size with ovarian dysfunction. Hum. Reprod. 20(2):402–12
105. Sutherland GR. 1977. Fragile sites on human chromosomes: demonstration of theirdependence on the type of tissue culture medium. Science 197(4300):265–66
106. Suthers GK, Callen DF, Hyland VJ, Kozman HM, Baker E, et al. 1989. A new DNAmarker tightly linked to the fragile X locus (FRAXA). Science 246(4935):1298–300
107. Suthers GK, Hyland VJ, Callen DF, Oberle I, Rocchi M, et al. 1990. Physical mappingof new DNA probes near the fragile X mutation (FRAXA) by using a panel of cell lines.Am. J. Hum. Genet. 47(2):187–95
108. Tamanini F, Kirkpatrick LL, Schonkeren J, van Unen L, Bontekoe C, et al. 2000. Thefragile X-related proteins FXR1P and FXR2P contain a functional nucleolar-targetingsignal equivalent to the HIV-1 regulatory proteins. Hum. Mol. Genet. 9(10):1487–93
109. Tarleton J, Richie R, Schwartz C, Rao K, Aylsworth AS, et al. 1993. An extensive de novodeletion removing FMR1 in a patient with mental retardation and the Fragile X syndromephenotype. Hum. Mol. Genet. 2(11):1973–74
110. Tassone F, Hagerman RJ, Taylor AK, Mills JB, Harris SW, et al. 2000. Clinical involve-ment and protein expression in individuals with FMR1 premutation. Am. J. Med. Genet.91(2):144–52
111. Tucker B, Richards RI, Lardelli M. 2006. Contribution of mGluR and Fmr1 functionalpathways to neurite morphogenesis, craniofacial development and fragile X syndrome.Hum. Mol. Genet. 15(23):3446–58
112. Van Dam D, Errijgers V, Kooy RF, Willemsen R, Mientjes E, et al. 2005. Cognitive de-cline, neuromotor and behavioural disturbances in a mouse model for fragile-X-associatedtremor/ataxia syndrome (FXTAS). Behav. Brain Res. 162(2):233–39
113. Verkerk AJ, de Graaff E, De Boulle K, Eichler EE, Konecki DS, et al. 1993. Alternativesplicing in the fragile X gene FMR1. Hum. Mol. Genet. 2:399–404
114. R epo r ts t h eide n ti ficat io n of t h ege n e r espo nsiblefo r F X S.
114. Ve r k e r k AJ M H , P ie r e t t i M , Su tcl iffe JS, F u Y H , K u h l D PA , e t al. 1991. I de n t i fi -cat io n of a ge n e ( F M R -1) co n tai n i ng a C G G r epeat coi ncide n t wit h a b r eak poi n tcl ust e r r egio n exh ibit i ng le ngt h var iat io n i n F ragile X syn d r o m e. Cell 65:905–14
115. Verloes A, Sacre JP, Geubelle F. 1987. Sotos syndrome and fragile X chromosomes. Lancet2(8554):329
116. Wang H, Iacoangeli A, Popp S, Muslimov IA, Imataka H, et al. 2002. Dendritic BC1RNA: functional role in regulation of translation initiation. J. Neurosci. 22(23):10232–41
117. Warren ST, Zhang F, Licameli GR, Peters GF. 1987. The fragile X site in somatic cellhybrids: an approach for molecular cloning of fragile sites. Science 237(4813):420–23
118. F i rst evide nceof t h e pot e n tialr ole of F M R P i nm od u lat i ngsynap tic plast ici ty.
118. Weile r IJ, I r wi n S A , K li n tsova A Y , Spe nce r C M , B raz elt o n A D , e t al. 1997. F ragileX m e n tal r e tar dat io n p r ot ei n is t ranslat ed n ear synapses i n r espo nse to n e u r o -t ransm i t t e r act ivat io n . Proc. Natl. Acad. Sci. USA 94(10):5395–400
119. Willemsen R, Oosterwijk JC, Los FJ, Galjaard H, Oostra BA. 1996. Prenatal diagnosisof Fragile X syndrome. Lancet 348(9032):967–68
128 Penagarikano · M ulle · Warren
Ann
u. R
ev. G
enom
. Hum
an G
enet
. 200
7.8:
109-
129.
Dow
nloa
ded
from
arjo
urna
ls.an
nual
revi
ews.o
rgby
EM
ORY
UN
IVER
SITY
on
08/3
1/09
. For
per
sona
l use
onl
y.

ANRV321-GG08-06 ARI 25 July 2007 17:29
120. Wohrle D, Kotzot D, Hirst MC, Manca A, Korn B, et al. 1992. A microdeletion of lessthan 250 kb, including the proximal part of the FMR-I gene and the fragile-X site, in amale with the clinical phenotype of fragile-X syndrome. Am. J. Hum. Genet. (51)2:299–306
121. Yan QJ, Rammal M, Tranfaglia M, Bauchwitz RP. 2005. Suppression of two major FragileX syndrome mouse model phenotypes by the mGluR5 antagonist MPEP. Neuropharma-cology 49(7):1053–66
122. Zalfa F, Giorgi M, Primerano B, Moro A, Di Penta A, et al. 2003. The Fragile X syndromeprotein FMRP associates with BC1 RNA and regulates the translation of specific mRNAsat synapses. Cell 112(3):317–27
123. Zhang Y, O’Connor JP, Siomi MC, Srinivasan S, Dutra A, et al. 1995. The Fragile Xmental retardation syndrome protein interacts with novel homologs Fragile X R1 andFragile X R2. EMBO J. 14(21):5358–66
RELATED RESOURCESBilen J, Bonini NM. 2005. Drosophila as a model for human neurodegenerative disease. Annu.
Rev. Genet. 39:153–71Cao X, Yeo G, Muotri AR, Kuwabara T, Gauge FH. 2006. Noncoding RNAs in the mammalian
central nervous system. Annu. Rev. Neurosci. 29:77–103Matnya A, Kusher SA, Silva A. 2002. Genetic approaches to molecular and cellular cognition:
a focus on LTP and learning and memory. Annu. Rev. Genet. 36:687–720Nimchinsky EA, Sabatini BL, Svoboda K. 2002. Structure and function of dendritic spines.
Annu. Rev. Physiol. 64:313–53Steward O, Schuman EM. 2001. Protein synthesis at synaptic sites on dendrites. Annu. Rev.
Neurosci. 24:299–325
www.annualreviews.org • Fragile X Syndrome 129
Ann
u. R
ev. G
enom
. Hum
an G
enet
. 200
7.8:
109-
129.
Dow
nloa
ded
from
arjo
urna
ls.an
nual
revi
ews.o
rgby
EM
ORY
UN
IVER
SITY
on
08/3
1/09
. For
per
sona
l use
onl
y.

A R321- F M A R I 25 July 2007 19:20
A n n ual R evie w ofG e n o m ics an dH u man G e n e tics
Volume 8, 2007C ontents
H uman E volution and Its Relevance for G enetic E pidemiologyLuigi Luca Cavalli-Sfor za ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! 1
G ene D uplication: A D rive for Phenotypic D iversity and C ause ofH uman D iseaseBernard Conrad and Stylianos E . Antonarakis ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! 17
D N A Strand Break Repair and H uman G enetic D iseasePeter J. M cK innon and Keith W. Caldecott ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! 37
T he G enetic L exicon of D yslexiaSilvia Paracchini, T homas Scerri, and Anthony P. Monaco ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! 57
Applications of R N A Interference in M ammalian SystemsScott E . M artin and N atasha J. Caplen ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! 81
T he Pathophysiology of F ragile X SyndromeO lga Penagarikano, Jennifer G . M ulle, and Stephen T. Warren ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! !109
M apping, F ine M apping, and M olecular D issection of Q uantitativeTrait L oci in D omestic A nimalsM ichel G eorges ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! !131
H ost G enetics of M ycobacterial D iseases in M ice and M en:F orward G enetic Studies of B C G -osis and TuberculosisA . Fortin, L . Abel, J.L . Casanova, and P. G ros ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! !163
C omputation and A nalysis of G enomic M ulti-Sequence A lignmentsM athieu Blanchette ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! !193
microR N As in Vertebrate Physiology and H uman D iseaseTsung- Cheng Chang and Joshua T. M endell ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! !215
Repetitive Sequences in C omplex G enomes: Structure and E volutionJer zy Jurka, V ladimir V. Kapitonov, O leksiy Kohany, and M ichael V. Jurka ! ! ! ! ! ! ! !241
C ongenital D isorders of G lycosylation: A Rapidly E xpanding D isease F amilyJaak Jaeken and G ert M atthijs ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! !261
v
Ann
u. R
ev. G
enom
. Hum
an G
enet
. 200
7.8:
109-
129.
Dow
nloa
ded
from
arjo
urna
ls.an
nual
revi
ews.o
rgby
EM
ORY
UN
IVER
SITY
on
08/3
1/09
. For
per
sona
l use
onl
y.

A R321- F M A R I 25 July 2007 19:20
A nnotating N oncoding R N A G enesSam G riffiths-Jones ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! !279
U sing G enomics to Study H ow C hromatin Influences G ene E xpressionD ouglas R. H iggs, D ouglas Vernimmen, Jim H ughes, and Richard G ibbons ! ! ! ! ! ! ! ! !299
M ultistage Sampling for G enetic StudiesRobert C . E lston, D anyu L in, and G ang Zheng ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! !327
T he U neasy E thical and L egal U nderpinnings of L arge-ScaleG enomic BiobanksH enry T. G reely ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! !343
I n dexes
C umulative Index of C ontributing Authors, Volumes 1–8 ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! !365
C umulative Index of C hapter T itles, Volumes 1–8 ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! !368
E r rata
A n online log of corrections to Annual Review of G enomics and H uman G eneticschapters may be found at http:/ /genom.annualreviews.org/
vi Contents
Ann
u. R
ev. G
enom
. Hum
an G
enet
. 200
7.8:
109-
129.
Dow
nloa
ded
from
arjo
urna
ls.an
nual
revi
ews.o
rgby
EM
ORY
UN
IVER
SITY
on
08/3
1/09
. For
per
sona
l use
onl
y.