THE OPTIC NERVE WORK-UP PTERYGIUM: CURRENT ...
20
Volumen VI No.1 Febrero 2007 III I Asociacion Pan-Americana de Oftalmologla Pan-American Association of Ophthalmology Associacao Pan-Americana de Oftalmologia Fundacion Pan-Americana de Oftalmologia Pan-American Ophthalmological Foundation Fundacao Pan-Americana de Oftalmologia THE OPTIC NERVE WORK-UP Alfredo A. Sadun, MD, PhD. - Rogerio F. Farsoni. MD. PTERYGIUM: CURRENT CONCEPTS AND TREATMENT MODALITIES Sathish Srinivasan FRCSEd. FRCOphth. - Allan R. Siomovic. MD, FRCSe. llNFLUYE LA ALTURA DEL MONITOR EN LOS FENOMENOS ASTENOPICOS? Eduardo Arenas MD. - Elena Oudovitchenko MD.
Transcript of THE OPTIC NERVE WORK-UP PTERYGIUM: CURRENT ...

Volumen VI No.1 Febrero 2007 I I I I
Asociacion Pan-Americana de Oftalmologla Pan-American Association of Ophthalmology Associacao Pan-Americana de Oftalmologia Fundacion Pan-Americana de Oftalmologia Pan-American Ophthalmological Foundation Fundacao Pan-Americana de Oftalmologia
PAN~
THE OPTIC NERVE WORK-UP Alfredo A. Sadun, MD, PhD. - Rogerio F. Farsoni. MD.
PTERYGIUM: CURRENT CONCEPTS AND TREATMENT MODALITIES Sathish Srinivasan FRCSEd. FRCOphth. - Allan R. Siomovic. MD, FRCSe.
llNFLUYE LA ALTURA DEL MONITOR EN LOS FENOMENOS ASTENOPICOS? Eduardo Arenas MD. - Elena Oudovitchenko MD.


VISION PAN-AMERICA
Mark J. Mannis, MD University of California, Davis
Sacramento, California Editor-in-Chief
Cristian Luco, MD Teresa J. Bradshaw Santiago, Chile Arlington, Texas Associate Editor Managing Editor
EDITORIAL BOARD
Eduardo Alfonso, MD David E. Pelayes, MD Miami, Florida U.S.A. Buenos Aires, Argentina
Eduardo Arenas, MD Alfredo Sad un, MD Bogota, Colombia Los Angeles, California U.S.A.
J. Fernando Arevalo, MD Jose Benitez del Castillo Sanchez, MD Caracas, Venezuela Madrid, Spain
Jose A. Roca Fernandes, MD Allan Slomovic, MD Lima, Peru Toronto, Ontario, Canada
Denise de Freitas, MD Luciene Barbosa de Sousa, MD Sao Paulo, Brazil Sao Paulo, Brazil
Marian Macsai, MD Lihteh Wu, MD Chicago, Illinois U.S.A. San Jose, Costa Rica
OFFICERS
Enrique Graue Wiechers, MD Mexico City, Mexico
President, Pan-American Association of Ophthalmology
Rubens Belfort, MD Sao Paulo, Brazil
Chairman of the Board, Pan-American Ophthalmological Foundation
PRODUCTION STAFF
Juan Pablo Cuervo Graphic Design
Eliana Barbosa Director of Production and Distribution
PAOF INDUSTRY SPONSORS
Advanced Medical Optics Inc. Carl Zeiss Meditec Inc. Alcon Inc. Merck & Co. Inc. Allergan Inc. Novartis Inc. Bausch & Lomb Inc. Santen Inc.
Prepress Creative Latin Media. Printed in Printer Colombiana - Colombia
This it is a product of
.:."~. .:_: Creative Latin Media Slrill~Y • Commllnicilll.on • Mil.h1:lnll
WIJ©O~PAN·AMERICA 3

Dear Colleagues in Ophthalmology:
Education is one of the primary missions of the Pan-American Association of Ophthalmology (PAAO) One of our committees, chaired by
Juan Verdaguer MD, is especially dedicated to this. Ophthamic education, in fact, is one of the global strategies of the International Council of Ophthalmology. This strategy seeks to standardize op~lthalmic training in the world and it promises the best possible conditions.
The PAAO, for its part, has assumed this global challenge. In fact, it was in Latin America that tile first educational model took place called "Teaching the Teachers". This strategy's objective, designed as a first step, is to standardize the manner and the most practical methods to teach ophthalmology. These courses have also helped to define the competencies of the specialists and they have been integrated in the different university curricula of our specialty.
The first course took place in Mexico City two years ago; the second course, using the same model, took place in Cairo, Egypt; and the third took place in Lima, Peru, last year. In July, in conjunction with the Argentine Congress of Opllthalmology, the next course in this series will take place.
These courses have been sponsored in large part by the pharmaceutical industry. This support was provided without conflict of interest and without publicity. Other support came from the International Council of Ophthalmology and its Foundation, and the PAAO and our Foundation.
If any of you are interested in attending the upcoming courses, please send an email to the PAAO. We will put you in touch with the organizers. This is also a good opportunity to invite you to attend the XXVII PanAmerican Congress of Ophthalmology which is scheduled to take place May 30 through June 3, 2007, in Cancun, Mexico.
See you there!
Estimables compafieros oftalmologos:
U na de las acciones qiJe en esta gesti6n ha empeliado la Asociaci6n Panamericana de Oflalmologfa (APAO) es 10 relacionado a la edu
caci6n. Uno de nuestros Comites, acargo del Profesor Juan Verdaguer, se dedica especialmente aello. La educaci6n oftalmol6gica es, de hecho, una de las estrategias globales del International Council of Ophthalmology.
La estrategia persigue que la formaci6n de oftalm610gos en el mundo tenga una orientaci6n similar y se otorgue en las mejores condiciones posibles.
La APAO, por su parte se ha sumado a esta estrategia global. De hecho, fue en nuestro continente donde se IIev6 acabo el primer modelo educativo encaminado a "enseflar a quienes enseflan". Esta estrategia, diseliada como un primer paso, tiene como objeto el estandarizar la forma y los metodos mas practicos para enseliar oftalmologfa De estos cursos se ha desprendido tambien la persecuci6n de competencias generales comunes a los especialistas yque deben, de alguna forma ser integrados a los diferentes currfculos universitarios de nuestra especialidad.
EI primer curso se IIev6 acabo en la ciudad de Mexico hace ya dos alios; el segundo, con el mismo modelo, se efectu6 en el continente africano en la ciudad del Cairo; el tercero en la ciudad de Lima, Peru, y pr6ximamente en el mes de julio y en conjunci6n con el Congreso Argentino de Oftalmologfa, se Ilevara cabo el siguiente de elios.
Los cursos Ilan sido patrocinados por la industria farmaceutica que en forma desinteresada y sin publicidad ha aportado buena parte de los recursos financieros necesarios; por ellnternacional Council of Ophthalmology ysu fundaci6n; ypor la Asociaci6n Panamericana de Oftalmologfa ynuestra Fundaci6n Panamericana.
Si alguien de ustedes esta interesado en asistir, por favor comunfquese con nosotros a la direcci6n electr6nica de la APAO y 10 pondremos en contacto con los organizadores
Es esta tambien una buena oporlunidad para insistirles, una vez mas, en su asistencia al Congreso Panamericano de Oftalmologfa acelebrarse en la Ciudad de Cancun del 30 de mayo al 3 de Junio. No dejen de inscribirse.
iLes esperamos!
4: WO@O@I!iJPAN·AMERICA

New Directions for the Pan-American Ophthalmological Foundation
The Pan-American Ophthalmological Foundation (PAOF) has invested US$ 1 million during the pasl decade in education and training in ophthalmology in Latin America, focusing an investing in exchange programs, teaching, human resources, and is now preparing two simultaneous initiatives in 2007, grant awards and research
Research Grants We have US$100.000 a ailable for the current year to be awarded in 10
selected research grants All the information is available at the PAAO website. Our priority is for those research projects already in development, and preferably those involving different institutions with international partnerships, where the relatively small grant offered by the Pan-American Foundation of Ophthalmology (US$1 0000) could be used 10 supply occasional necessities. In 2007, three will be two submission dates May 15 and September 15. We hope to announce the first grants in Cancun in June. During the past few years, we had very few investigators who demonstrated interest. As such, we are encouraging those who are engaged in research in ophthalmology to complete the forms and submit their proposals by ihe deadlines. We are certain that with the appropriate use of those resources. 'e can go forward and make progress
Initiation of Assistance Activities The Pan-American Foundation of Ophthalmology is announcing a new
program called Buy Vision in latin America ("Compre Visao na America Latina") in 2007. Aspecilic program for retinopathy of prematurity was selected considering the cos -benefit ratio in that area. This disease can cause permanent blindness, and an untrea ed child with this disease can live for 70 years in absolute blindness. The cost of evaluating 10 children and treating one is about US$ 70000 in Latin America. The Pan-American Foundation has created this program through hich resources will be forwarded to ophthalmologists treating those children in Latin America. During the second half of 2007, we Will be registering centers for treatment of retinopathy of prematurity in Latin America in order to keep the program active and efficient. We are looking to ophthalmologists, indus ry and the community for donations to the program "Buy Vision in Latin America".
At the Pan-American meeting in Cancun, we Will sponsor the Pan-American dinner. It will be asocial and benefit activity. Representatives of the ophthalmic industry have agreed to match the funds raised by ophthalmologists for "Buy Vision in Latin America Program" In this way, industry Will donate money to the program based on the number of couples who attend to the dinner. It will be a great party with presentations and important activities. We will also have an auction at which ophthalmologists will be able to help blind children in Latin America, and at the same time have fun and bring home gifts and souvenirs back home.
We are counting on you to apply for the research grants and, in addition, to donate to benefit vision in Latin America. Also, we are looking forward to having you taking advantage of the best of the Pan-American Association: an ophthalmologic environment of education and training between friends and colleagues for life.
Novas Dire~6es da Funda~ao Pan-Americana de Ottalmologia
A FundaGao Panamericana de Oftalmologia, ap6s investir US$1 milhao nos ultimos 10 anos em EducaGao eTreinamento em Oftalmologia na America
Latina, prestigiando e investindo em Programas de intercambio, ensino e formaGao de recursos humanos prepara-se agora para desencadear duas novas etapas simultaneas de atividades em 2007.
Concessao de Grants e Pesquisa Temos US$100 mil d61ares para investir em 2007 em pesquisa selecio
nando 10 grants de pesquisa Todas as informaGoes estao na Web e sao facilmente disponiveis. A prioridade e para Pesquisas ja em andamento e de preferencia multi institucionais com parcerias internacionais e onde 0
investimento relativamente pequeno concedido pela FundaGao Panamericana de Oftalmologia (US$1 0mil) possaser utilizado parasuprir eventuais necessidades. Em 2007 teremos duas datas para envio das propostas que sao respectivamente o 15 de mayo e 0 15 de setembro. Esperamos divulgar as primeiras Grants ja no Congresso de Cancun em junho. Nos ultimos anos tivemos um numero muito pequeno de investigadores interessados. Assim, estamos estimulando a todos que estejam realizando atividades de pesquisa em oftalmologia que preencham os formularios de instruGoes eenviem as propostas dentro do prazo pre determinado. Temos certeza que com a utilizaGao adequada desses recursos podermos continuar nesse fluxo emesmo aumentar.
Presta~ao de Atividade Assitencial AFundaGao Panamericana de Oftalmologia esta tambem lanGando em 2007
o Programa Compre Visao na America Latina (Buy Vision in Latin America). Foi selecionado 0 Programa especifico para Retinopatia da Prematuridade pois trata-se de uma das areas onde 0 CLiStO beneficio eadequado. Retinopatia da Prematuridade, (todos nos oftalmologistas sabemos) pode levar acegueira permanente. Uma crianGa nao tratada com Retinopatia da Prematuridade pode licar 70 anos de cegueira completa, absoluta epermanente. 0 custo na America Latina do exame de 10 crianGas e0 tratamento de uma, porcentagem por crianGas de risco etratamento de uma (como normalmente de observa) e de cerca de US$700. A FundaGao Panamericana entao esta lanGando esta campanha onde todos os recursos serao encaminhados aoftalmologistas que estejam tratando essas crianGas na America Latina. No segundo semestre de 2007 estaremos registrando a lista de Centros de tratamentos de Retinopatia da Prematuridade na America Latina para podermos manter este Programa ativo, eficiente e ulilizando de maneira maxima os recursos utllizados. Estamos solicitando paralelamente a todos os oftalmologistas, a industria e toda comunidade interessada a possibllidade de doaGoes especificas para 0 Programa Compre Visao na America Latina da FundaGao Panamericana de Oftalmologia.
No Congresso Panamericano de Cancun teremos a grande cena Panamericana. Sera uma grande atividade social mas tambem de cunllO filantropico. Os melhores representantes da industria oftalmologica presentes na America Latina ja concordaram em doar para 0 Programa Compre Vi sao na America Latina a mesma quantia arrecada atraves de Oftalmologistas par 0 jantar Assim, a indlJstria doara ao programa dolares para cada casal que comparecer a este jantar. Sera uma grande festa, com SllOW e atividades importantes inclusive provavelmente um grande lei lao onde nos oftalmologistas teremos oportunidade de ajudar crianGas cegas na America Latina eao mesmo tempo nos divertir etrazer para casa objetos e lembranGas importantes do mundo atual
Continuamos contando com todos para se inscrever para receber verbas para Pesquisa e doar em beneficio da vi sao na America Latina e tambem, porque nao, usufruirmos do melhor que aAssociaGao Panamericana tem: um ambiente oftalmologico de educaGao etreinamento entre amigos eparceiros por toda avida.
WO~D@[I!]PAN·AMERICA : 5

I~REVIEW
The Optic Nerve Work-up Rogerio F. Farsoni. MD
Thornton Proressor or Ophthalmology Alfredo A. Sadun, MD, PhD
International Fellow in Neuro-Ophthalmology Doheny Eye Institute Doheny Eye Institute Keck-USC School or Medicine Keck-USC School or Medicine Los Angeles, CA. Los Angeles, CA.
Dne olthe most common workups in neuro- I the optic canal is about 9mm in length II I
ophthalmology entails the likelihood I Another 16mm usually brings the intracranial I I Ithat the cause of visual loss is from an optic optic nerve to the optic chiasm, All alongI I
neuropathy, A systematic and sophisticated I this route (except for the intraorbital portion) I
approach leads to the timely diagnosis, often II the nerve is covered in the same three layers
II
without the need for costly and unnecessary I of the meninges as is the rest of the brain, I I I
testing As ageneral overview, the diagnostic I The outermost dura is rather firm and tough I I I
workup in patients with optic Ileuropathies I The more delicate arachnoid has tendrils I I Irequires consideration of six items, and multiple channels under which runs theI I I cerebral spinal fluid (CSF), all continuous I
1) Basic anatomy and physiology of the optic I I I with the brain, With increased intracranial I nerve, I I pressure, the pressure is transmitted alongI I2) The most useful distinctions of macula vs, I Ithe CSF to the optic disc where engorgementoptic nerve disease, I I I of the axons and vasculature manifest as I3) Particularly useful items in the history that I I papilledema (ref, Hayreh), The same increasepoint to the optic nerve, I in pressure also causes a bulging out of the4) Particularly useful signs in the physical exa- I
optic nerve sheathmination of patients with an optic neuropathy, The retrobulbar nerve is about 7-8mm5) Special tests to detect, and characterize
longer than the actual distance from tile eye tooptic neuropathies, the optic canal; hence there is redundancy that6) The most common two optic neuropathies. allows for eye movement and for proptosis, up to a length of about 9mm.1) Basic anatomy and physiology Each fiber of the optic nerve consists
of the optic nerve. I of a retinal ganglion cell axon and a myelinI sheath. Saltatory conduction of a nerve im-The optic nerve, of course, relays all II pulse occurs at the interruptions of the Iinformation from the eye to the brain. It may I II myelin (Nodes of Ranvier) (ref, Encyclopedia Ibe injured in a variety of ways including di-I Neurosci). Diseases of demyelination may I
seases of the eye and diseases of the brain I I I lead to decreased conduction, delays of(ref Sadun-book Hoyt). Each optic nerve is I
I
I conduction and irreversible damage to the I
composed of about 1.2 million fibers that I
I Iaxons,collect Irom the retinal ganglion cell axolls I I
and progress, through the lamina cribrosa I I I 2) The most useful distinctions of I I Ito exit the eye posteriorly (ref Sadun-book I macula vs. optic nerve disease. I
I Glaser). The fibers run for adistance of about I
I I50mm before 53% decussate in the optic I The differentiation ot optic neuropathies I
I Ichiasm. Although the fibers continue past from maculopathies may be difficult sinceI I to terminate in various visual nuclei in the I that many optic nerve diseases can resemble I
I Ibrain, the clinical manifestations of an optic I macular disease. This represents a challenge I
neuropathy are distinct and constitute their II to the ophthalmologist to distinguish between I
I
own entity (ref Sadun-book Hoyt). I the two on clinical grounds. I
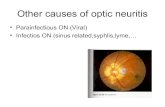
As figure 1demonstrates, the bulbar optic I
The clinician should be able to make II Inerve is only Imm and consists of unmyeli- an early and accurate differential diagnosis I Inated libel'S. As it exits the eye, its diameter avoiding unnecessary complementary exams
increases to approximately 3,5mm and thell it and therapeutic modalities that are expensive II Icontinues to increase in caliber posteriorly and and, sometimes, harmful to the patient. Com- I I I
(ref. Sadun, Taban Neuro-ophthalmology) and specifics ophthalmologic tests can be I
In its retrobulbar course the optic nerve runs realized to make this differentiation. I
has a diameter of almost 5mm intracranially plete neuro-ophthalmological evaluation
I I between the 6 muscles in a cone of fat for a I Patients with optic nerve lesions often I
I I length of about 25mm. The passage through I complain of visual loss as darkness, clouding, I
6: \'!I'[@~PAN-AMERICA
~
..
desaturation of colors or as gelleralized dimness across portions of the visual field, whereas macular lesion usually express as blurriness and metamorphopsia and the palient may experience photophobia, glair or that object appears too bright.
The most useful clinical tests to differentiate optic neuropathies from maculopathies are color vision, brightness sense and afferent papillary defects that, in general, are out of proportion to loss of visual acuity in optic nerve diseases, Other special tests as visual field, contrast sensitive, photostress test, eletrophysiologic test and optical coherence tomography (OCT) can be very useful to help the clinician to distinguish optic nerve disorders from maculopathies1,2,3.4.
3) Particularly useful items in the history that point to the optic nerve.
In the history is particularly important to elicit from the patient the time course of visual loss and associated symptoms, Sudden onset with visual loss that occurs over several hours to several days that then stabilizes and remains stable is more characteristic of ischemic optic nerve disorder3 Optic neuritis is characterized by loss of vision evolving over days to weeks followed by spontaneous recovery that begins to improve within 3 weeks. Pain, particularly with eye movements that can precede the visual loss occurs in 92% of patientss.6 Atemporary loss of vision with exercises or increase in body temperature (Uhthoff's symptoms) can occur in the chronic or in the setting of a previous episode of optic neuritis? Slowly progressive visual loss over months or years is, typically, of compressive causesB
4) Particularly useful signs in the physical examination of patients with an optic neuropathy.
The visual acuity by itself is not the most useful sign to make the differentiation of optical neuropathy from maculopathy. The issue is to compare the extent of loss of vision with color vision, brightness sense and relative afferent papillary defect (APDl4

Febrero 2007
In optic nerve disease the deficit of dyscromatopsia may be proportionately greater than the degree of Snellen visual acuity loss and usually produce red-green deficits. In contrast. maculopathy commonly causes symmetric losses in color discrimination and visual acuity
Impairment of brightness sense, which can be estimated subjectively when the patient is asked which eye sees a light as brighter, is a consistent finding among patients with optic neuropathies and ca be more sensitive than otller tests in establishing the presence
9of disease3. In subgroups of patients who are strongly suspect of having an APD but in whom papillary testing is not possible, brightness comparison testing can reliably predict presence or absence of an ADp10 Patients with maculopathies usually show slightly reduced or increased brightness
3senseArelative afferen pupillary defect (RAP D)
is an indicator of an as mmetric lesion of the anterior visual path lay and can be detected througll swinging flashlight test, probably the most useful diagnostic test in neuroophthalmology. Only e ensive retinal or macular disease may sho l aRAPD, such that the diagnosis is obviou .
Fundus examina ion can reveal both the macula and the op i nerve changes explaining the patient's decreased isual acuity.
Optic atrophy is he main sign of damage to the retinal ganglion cells and is visualized first about one month after acute injury of the nerve. Sometimes. the dropout of the peripapillary nerve fiber layer may precede visible optic atrophy.
Optic neuropathies may produce sectoral disc edema with flame hemorrhages (anterior ischemic optic neuropathy), peripapillary telangiectasia that do not leak fluorescein (Leber hereditary optic neuropathy), sectoral optic atrophy, buttertly optic atrophy (Lesions damaging the body of the chiasm). Macular hole, epiretinal membrane, retinal pigment epithelial irregularities and exudates also can be observed.
Confrontation testing has ahigh sensitivity for detecting altitudinal visual loss, centrall cecocentral scotoma and homonymous hemianopsia11
.
5) Special tests to detect, and characterize optic neuropathies.
Pelli-Robson charts are the more sensitive in detecting loss of peak contrast sensitive in the setting of normal visual acuity
and give more reproducible results than Regan and the Vistech charts. Patients with optic neuropathies may show deficiencies in the middle-to-high spatial frequencies whereas patients with maculopathies usually have deficiencies only in the highest spatial frequencies.
Photostress test is a simple clinical test that can help to differentiate visual loss caused by amaculopathy Irom optic neuropathy. This test is based on the principle that visual pigments bleach when exposed to an intense light source, resulting in a transient state of sensitiVity loss and reduced central visual acuity. With the patient wearing their best correction the visual acuity is determined monocularly After, the patient is asked to cover one eye while the other eye is subject directly into a strong light held 2-3 cm from the affected eye for 10 seconds, then the patient is directed to read backwards the line of letters just above their best line of acuity. Patients with a macular disease usually have recovery times lasting 90-180 seconds or more. If the cause for tile reduce visual acuity is the optic nerve, the normal recovery time (45-60 seconds) is maintained1213.
Conduction delay in one optic nerve following an episode of optic neuritis may lead to an impairment of binocular depth perception specially with moving objects. Because of the disparity in neuronal transmission, apendulum tllat swings in one plane
may appear to trace an elliptical pathway (Pulfrich phenomenon)3J
Amsler grid testing is useful and sensitive as a screeni ng test of the central 10° of visual field. The patient may describe any central area of distortion (metamorphopsia), a strong indicator of macular disease. Tangent screen is an effective method to asses the central 20° of visual field and when performed at 2m may identify a small central scotoma much easier and allow evaluation of non organic visual field loss3
Electrophysiological tests may be used when the physician is confronted with apatient who has unexplained loss of vision and an apparently normal fundus examination.
Visual evoked potentials (VEP) may be used as ameasure of afferent pathway integrity and represents sensory activity that begins at the retina and ends at the occipital cortex. The VEP can be used to document optic nerve function and to differentiate among retinal, optic nerve, and cortex diseases3.
Optical Coherence Tomography (OCT) may be used to measure structures such as retinal thickness or retinal nerve fiber layer (RNFL) thickness and can be very useful to neuro-ophthalmologist to differentiate maculopathies from optic neuropathies. OCT may sllow reductions in RNFL thickness in patients with previous attack of optic neuritis and multiple sclerosis (MS) supporting validity for this test as a secondary clinical outcome measure for MS trials14 .
Figure 1. Sagittal section through a normal orbit showing the intraocular and intraorbital divisions of the optic nerve.
W1J~O@lmPAN·AMERICA : 7

REVIEW
6) The most common two optic neuropathies.
The most common optic neuropathies are optic neuritis (ON) in yOUllg adults and nonarteritic anterior ischemic optic neuropathy (NAION) in older persons3
ON entails inflammation of the optic nerve, and is referred to as papillitis when the optic disc is swollen and as retrobulbar optic neuritis when it appears normal IS The annual incidence of acute optic neuritis is estimated to be about 5 per 100,000. ON is most often seen in patients 15-35 years and women are affected twice as often as men. ON is the first expression of disease in 50% of patients with MS, and 80% will develop some degree of visual impairment during the course of their diseaseH
Patients with optic neuritis experience loss of vision in one eye deteriorating over several hours to weeks, followed by spontaneous recovery usually within six to eight weeks. The severity of visual loss varies from mild visual field defect to no light perceptionS,15 Pain in or around the eye may, aggravated by eye movement, is noted in over to 92% of the cases, anlj this precedes or occurs concurrently with visual loss6.
Losses of color vision and contrast sensitivity occur in almost all patients with optic neuritis out of proportion to tile level of visual acuity A relative afferent pupillary defect commonly is found. A reduced sensation of brightness sense also can be present in the affected eye and occasionally may be more prominent than the decreased vision lo
The typical visual field defect in optic neuritis is a central or paracentral scotoma, but almost any type of field loss is possible Retinal nerve fiber layer (RNFL) thinning and macular volume loss can be detected by Optical Coherence Tomograplly (OCT) following optic neuritis; OCT measurements reflect the intact axonal population within the RNFL15 OCT may be also a structural biomarker for generalized axonal loss ill MS as reductions in RNFL thickness have been documented in MS patients without a history of acute optic neuritis '4 .
Wilen the clinical course is typical, neither serologic nor CSF studies are necessary. Clinical features that suggest nontypical optic neuritis include the presence of retinal hemorrhages, a markedly swollen nerve, retinal exudates, the absence of pain, progressive visual loss alter two weeks and absence of visual recovery within 60 days6, In the setting of atypical optic neuritis some
8; WO@O@[}:1PAN·AMERICA
: studies should be performed such as serum I VDRL and RPR, serum angiotensin-convertin : enzyme levels (to screen for sarcoidosis), : ESR, ANA, anti-DNA antibody testing to I assess for lupus and other vasculitic diseases : and chest radiography16 : An MRI scan is the most valuable pre-I dictor for the development of subsequent MS : and is recommended in every case of optic : neuritis, In the Optic Neuritis Treatment Trial I (ONTI), the live year risk for MS was 16% : with a normal brain MRI scan, 37% with one : or two typical MRI white matter lesions and I 51 %with three or more lesions. At ten years, : the increased risk of MS was 22% with normal : MRI scan and 56% with one or more lesions. : Other features that might increase the risk of I MS include younger age, female sex, and : Caucasian raceS,16.
: The ONTI demonstrated that at two year I follow-up the use of intravenous methyl: prednisolone (IVMP) 1g for three days, follo: wed by oral prednisone 1mg/kg/day, slightly I decreased the risk for development of recu: rrence, but the beneficial effect was not main: tained after three years, Oral prednisolle alone, I at the dose used, not only sllowed no benefit : but was associated with an increased risk of : recurrence of optic neuritisS,16. I Immunomodulalion therapy with interfe: ron beta-1A (Avonex), interferon beta-1 B : (Betaseron) and the synthetic copolymir gla-I tiramir acetate (Copaxone) is of proven benefit i for reducing morbidity in the relapsing-remi
tting form of MS in patients with typical MRI white matter lesionss
The nonarteritic form of anterior ischemic : optic neuropathy (AION) accounts for 95% of I AION cases and is the most common acute : optic neuropathy in patients over 50 years 01 : age, with an annual incidence in the United I States of 3,25 per 100.000 population, No I I gender predisposition exists, but the disease : occurs with significantly higher frequency in I the white population than in black or HispanicII individuals'6,1B : NAION usually manifests as acute painI less monocular visual loss, Presenting visualI I acuity is worse than 20/64 in about 50% of : patients and may subsequently improve I slightly (30% - 40% of patients) or remainI I unchanged (in 45% of cases). Rarely, NAION : is in progressive form with decrements of I vision over 2-3 weeks prior to eventualI I stabilization16,19 : In AI ON color vision loss may be mild : compared to visual loss, A RAPD is almost I present with monocular optic neuropathy, As : in other optic neuropathies the brightness
: 1
: : I
: : I
: : I
: : I
: : : I
:
: I
: : I
J
: i
: sense will be much reduced in the affected : eye9 The optic disc edema in NAION can I be diffuse or sectorial, When the swelling is
focal, it often corresponds to the visual field defect20
The optic nerve usually becomes atrophic within 8weeks and persistence of edema after this period supports an alternative diagnosis, Focal telangiectasia of the edematous disc surface vasculature and focal narrowed arterioles in the peripapillary region can also be noticed 16.
The most consistently identified vasculopathic risk factor is diabetes mellitus, which also is associated with the development of I~AION at a younger age Systemic hypertension, hypercholesterolemia and smoking have also been described as risk factors for I~AION1B Optic disc drusen has also been related with NAION at younger age 21. There are several case reports suggesting a link between erectile dysfunction medications (phosphodiesterase - PDE) and NAION. It has been theorized that PDE inhibitors may act as risk factors precipitating NAION as increase nitric oxide levels can provoke hypotension19,
Neither carotid occlusive disease nor prothrombic disorders have been shown to be significant risk factors for NAION, Hyperhomocysteinemia, sleep apnea and nocturnal hypotension have been proposed as risk factors but are currently unproven16

The structure of the optic disc with small or absent cup is though to predispose to higher tissue pressure secondary to obstruction to axoplasmic flow. Subclinical ischemia in the crowded laminar region results in additional swelling with compression and obstruction of the microcirculation in the abnormally rigid cribiform plate, aggra alin~ hese factors22
Medical and su gical reatments have been proposed for patients 'ith NAION, how
ever, such therapies have not been show to give significant benefit.
A careful history, with emphasis on the character and tempo of visual loss and an examination that includes the triad of optic nerve tests and funduscopy usually leads to the correct diagnosis of an optic neuropathy
Febrero 2007
I. Sadun AA. Di-tin~i:,hing between clinical impairments clue to optic nerve or mat:ular disease. Metab Pediatr Syst Ophthalmol1990; 13 (2-4): 79-84. 2. Bianchi !\[ar.wlli '. '.Iartinelli V. Optit: Neuritis: differential diagnosis. Neuro Sci. 2001; 22: S52-S54. 3. Sadun AA. DiJT..n-ntialion of optical nerve from retinal macular disease. In: Yanoff M, Duker IS. Ophthalmology, 2nd eel. London, Mosby; 1999: 11: 3.1-:... 4. Saciun AJ\. Topi. 'II .Jingnosis of acquired optic nerve disoTClers. In: Walsh & Hoyt:1 Clinical Neuro-ophthalmology, 6th ed. Philadelphia. Lippincott \,'illiam- ,mt! \\'jjkens; 2005: vol 1 chapter 4: 197-236. 5. Amold :\c. PI'" I'li\e: Eyolving management of optic neuritis and multiple sclerosis. Am J Ophthalmol. 2005; 139: 1101-1108 6. Frohman E\1 1'1 ..1. The nemo-ophtha] I1lOlogy of multiple sclerosis. Lancet Neural. 2005; 4: 111-21. 7. Glaser JS. Tr••pi,·a diagnosis: prcchiasmal visual patll\vays In: Glaser IS. Neuro-ophthalmology,3rd ed. Philadelphia. Lippincott Williams and ~ ilK"Il-: 1999: 147. 8. Sarkes NJ. I tit'nene sheath meningioma: diagnostic features and therapeutic alternatives. Eye 1987; 1: 597-602. 9. Sadun AX L ",·11::. Brightness-sense and optic nerve disease. Arch Ophthalmol. 1985; 103: :39-43. 10. Brownilli! lJJ. BULlle\ IG Reliability of brightness comparison testing in predicting afferent pupillary defects. Arch Ophthalmol. 1988; 106: 3-ll-:~n
11. Johnson L I. Bal"h FG. The accuracy of confrontation visual field test in comparison with automated perimetry. .J Natl Med Assoc. 1991 Oct:83 Ifl\: /;)- . 12. Glaser J:3 et 31. The photostress recovery test in the clinical assessment of visual function. Am.l Ophthalmol. 1977 Fcb;8:3(2):255-60. 13. Zabriskip " .l,. h:mlon RH. The pupil photostress lest. Ophthalmology. 1994 Iltl1; 101 (6): 1122-30_ 14·. Fisher JB f'. al. Helation of visual function to retinal nerve fiber layer thickness in Dlultiple sclerosis. OphlJwlrnology. 2006 Feb;113(2):3:"-!-3::'. 15. Trip SA el·1. ptie nerve atrophy and retinal nerve fibre layer thinning following optic neuritis: Evidence that axonal loss is a substrate of '.1R1-,lelected atrophy. Neuroimage. 2006 May 15;:31(1):286-93. 16. Kline LB d aI. _-\ll1eriCall Academy of Ophthalmology Basic and Clinical Science Course - Neuro-ophlhalmology, 2005-2006 ed. San Francisco: 122-::'.=;.2005. 17. WiJejto '.Lel ilL The cl inical fealures, MRJ findiugs, and outcome of optic neuritis in children, NeLtrology. 2006 JuI25;67(2):258-62. 18. Amold _.l,c. Pathogenesis of nonarteritic anterior ischemic optic neuropathy. J Neuroophthalmol. 2003 .Iun;23(2):157-63. 19. McGwiu Jr G el aL \on-arteritic anterior ischemic optie neuropathv and the treatment of erectile dysfunction. British Journal of Ophthalm%g\. 2006:90:154-157. 20. Hayreh ::;::: ('1 aL \'isuallield abnormalities in nonarteritic ischemic oplic neuropathy. Arch Oplztlzalmol. 2005; 123: 1554-1562. 21. Pun'in Y pt a1. .-\ nterior isehemic {}plic neuropathy in eyes with optic disc dTUsen. Arch Ophthalmol. 2004;122:48-53. 22. Arnold _\C Ischemic Optic Neuropathy. In: Wedsh & Hoyt's Clinical iVellro-ophthalowlogy, 61h ed. Philadelphia. Lippincott Williams and Wilkens: 2005: \'011 dillpter 7: 362.
PAAO FUTURE MEETINGS
14 November 2007
Lo Mejor de la Academia en Espanol 7:30 am - 5:30 pm; LaSalle Ballroom, Intercontinental Hotel New Orleans, Lousiana
7 - 8 March 2008
XV Pan-American Regional Course Conrad Punta del Este Resort & Casino; Punta del Este, Uruguay http://www.apaoregiona/2008.org
WO@O@[l!]PAN·AMERICA : 9

REVIEW
Pter gium: Current Concepts and Treatment Modalities Sathish Srinivasan FRCSEd, FRCOphth 51. Paul's Eye Unit 8Z Link Royal Liverpool University Hospital Prescot Street Liverpool L7 8XP England. United Kingdom E-mail: [email protected]
I. Introduction. The term Pterygium is derived is from the
Greek Pterygion meaning "wing". Clinically it appears as a fleshy wing shaped growth in the interpalpebral area. It typically occurs nasally, occasionally nasally and temporally, and rarely only on the temporal side. Pterygium is more frequent in areas with more ultraviolet radiation (UV), I in hot, dry, windy, dusty, and smoky environments. 2, 3
II. Clinical features. Pterygi um appears as afleshy fi brovascu lar
growth involving the interpalpebral area. Typically it is triangular in shape and consists of a cap head and body (Figure 1). The cap is situated at the leading edge of the pterygium and is composed of a gray subepithelial corneal opacity. Hence it is also referred to as the gray zone. With chronicity abnormal pooling of tears in the region of the cap leads to the deposition of hemosiderin from the tears leading to the formation of a corneal epithelial iron line (Stocker's line)4 The head of the pterygium is an elevated which mass that is firmly adhered to the underlying episcleral tissues. The body of the pterygium is a fleshy fibrovascular mass that is demarcated from the normal surrounding conjunctiva by folds. Pterygia are more frequently located nasally than temporallyS They either progress towards the visual axis with marked vascular engorgement or become quiescent remaining stationary over time. In advanced cases, the pterygium encroaches onto visual axis and may cause visual loss either from the loss ot corneal transparency within the visual axis or due to irregular corneal astigmatism. This phenomenon ot irregular astigmatism results from the abnormal pooling ot tears in advance of the apex of the pterygium 6 Mechanical torces may also playa role leading to tractional corneal flattening? Apseudopterygium should be distinguished from true pterygium, as it
Allan R. Siomovic, MD, FRCSC Associate Professor or Ophthalmology University of Toronto Toronlo. Ontario Canada
represents an inflammatory adherence of the conjunctiva to the cornea in response to mechanical or chemical or thermal injury. Many corneal inflammatory disorders may also predispose to fibrovascular ingrowth that may resemble pterygia. Although similar in histology, a pinguecula is distinguisl1able from a pterygium by virtue of its conjunctival location away from the limbus, and the lack of wing shaped radial vascular orientation towards the corneal apex.
III. Prevalence The prevalence rate of pterygium varies I
according to the population surveyed. Over-all : the prevalence rate varies from 0.7% to 31 % : around the worldS. 8. 9 There is a worldwide I
distribution of pterygia but they are more : common in warm and dry climates. 1 The I
I
common factor appears to be latitude, with I I
pterygia occufring mostly within the peri I
equatorial "pterygium belt", latitudes of II
37 degrees north and south of the equator. II
Several studies have shown that the preva I
lence of pterygia increases with age 2. 3. 10 II
Tile commonest age of onset appears to be I I
in the 20s and 30s 2, II The prevalence rate I
of pterygium increases with age, although a II
decline in prevalence rates have been reported II
inpatients over 60 to 70 years. 5.8 I I I
IV. Risk factors II I
The most important risk factors are en II
vironmental in nature; namely, solar and ul I
traviolet radiation, and chronic irritation from II
air-borne particulate matter. I
I
a. Ultraviolet radiation The major environmental risk factor for the development of pterygium is exposure to UV lighl. '2 A high prevalence of pterygia occurs in the equatorial (pterygium belt) bounded by
I
latitudes 37° north and 37° south. Mackenzie et al confirmed that those who live at latitudes
less than 30° during the first five years of life have a 40-fold increased risk of pterygium developmenl. '3 The use of protective eyewear and sun visors may mitigate some of these risk factors. 14
b. Genetic factors Several case reports have described clusters of family members with pterygium, and a hospital-based case control study showed family history to be signiricant, suggesting a possible autosomal dominant pattern. 15 16
c. Other factors Proponents of the "chronic keratitis" theory have cited chronic irritation or inflammation occurring at the limbus or at the peripheral cornea as arisk factorH This chronic inflammation is implicated as an important cause ot limbal stem cell deficiency, which is discussed later. 18 Wong has also suggested the presence of a "pterygium angiogenesis factor", and consequently the use of antiangiogenic pharmacotherapy has been reported to be atherapeutic option.19 Dust, low humidity and microtrauma from particulate matter, dry eyes and the human papilloma virus have also been implicated.2023
V. Pathogenesis The pathophysiology of pterygium has
intrigued surgeons for many years. There
10 : W!J@O@IJi]PAN·AMERICA

Indications for the treatment of Pterygium
Indications Grading
I.Visual loss due to proximity to visual axis 10/10
2.Threat to the visual axis 10/10
3.Visualloss secondary to astigmatism 8/10
4. Ocular motility restriction 8/1 0
5.Atypical appearance (possible dysplasia) 8/10
6. Documented growth by ophthalmologist 6/10
7. Reported growth by the patient 4/10
8. Ocular surface symptoms (irritation/ discomfort) 4/10
9. Cosmetic concerns
Tabla 1
seems to be this ongoing debate on why ptergia occur and how best to manage them. Within the last two decades several peaces of the puzzle seem to have fallen in place. Important in the pathogenesis of pterygia is the histological evidence hat the limbal, corneal and conjunctival epithelial cells have adjacent and joined basemen membranes that allows possible migration of any of their basal cells onto each others basement membrane 24, 25
Normally, the paren al stem cells in the limbal epithelium next to the conjunctival cells maintain a constant posterior border and do not migrate across the bo:der onto conjunctival basement membrane. Pterygia originate from amigration of an entire segment of vimentinexpressing altered limbal epithelial basal stem cells onto cornea! basement membrane, followed by conjunctival epithelial cells 26,27
Dushku and Reid demonstrated over expression of p53 tumor-suppression gene without apoptosis in these limbal epithelial cells of pterygia.2: They found that UV-B induced p53 mutations are one of the early events in the development of pterygium, and this damages the apoptosis mechanism in the limbal stem cells. Thereafter, mutations in other genes are progressively acquired that allow the development of pterygia. Based on their findings of p53 over expression and overproduction of transforming growth factor (TGF)-~ by the UV-B damaged limbal basal
4/1 0
cells Dushku et al 28 proposed atheory of two possible pathways in the pathogenesis of pterygia 1. Damaged p53-dependent apoptosis pathway. 2. p53-retinoblastoma-TGF ~ pathway. P53- dependent pathway: UV light causes an early mutation in the p53 tumor suppressor genes which are located in the parental limbal basal cells. Because of this mutation in the p53 programmed cell death mechanism, mutation occurs in other genes which lead to this cascade of events that leads to the development of pterygia from p53-expressing cells in the limbal epithelium. Damage to the p53 genes also triggers the overproduction of pterygium cells via the P53-retinoblastoma-TGF ~ Pathway.
Angiogenesis theory Although UV radiation induced mutation in the cellular level seems to trigger off the growth of pterygium several fibroangiogenic factors seems to contribute to the growth and increased vascularity that is clinically seem in a pterygium Tile details of these and their clinical relevance are discussed the newer treatment options later.
VI. Management a. Medical management Before planning on surgical management a careful history and slit lamp examination
is mandatory to rule out the diagnosis of pseudopterygium, conjunctival intraepitheIial neoplasia, squamous cell carcinoma and a corneal macro pannus. Recommendations for the prevention of pterygium formation should include avoidance of exposure to UV radiation. Mackenzie et al has showed that there is adoubling risk of pterygium formation associated with never wearing ahat outdoors between the ages of 20 and 29 years and nine fold increased risk of pterygium formation if sun glasses were never work ill the decade before the pterygium developed. 13Hence in areas where UV exposure is high, the use of UV-absorbing sunglasses and hats are advisable. Ocular surface cliscomfort secondary to pterygium can be managed with the use of topical lubricants or mild topical antihistamine/vasoconstrictor. Secondary dellen formation can be managed with frequent topicallubrication.
b. Surgical management Surgery is the definite treatment for pterygium management. There are afew broadly accepted reasons for the surgical removal of pterygium. Few would argue that apterygium with a documented growth that extends towards the visual axis should be removed. There would also be little disagreement that pterygium that affects the extraocular motility should be removed. Apart from these two definitive indications the reasons for surgically removing a pterygium has been an area of great debate among ophthalmologist. There have been very few published reports on the indications for pterygium removal. Recently, Hirst29 published ascoring system based on a 10 point grading scale, which is summarised in table 1. The fact that numerous different surgical techniques have been described underscores the POillt that no single approach in universally successfu 1
30 The major outcome measures of pterygium removal relate to recurrence (which can be conjunctival or comeal), visual and cosmetic appearance. The most common endpoint determined in scientific literature is the recurrence of pterygium, which is defined as the growth of fibrovascular tissue across the limbus in to clear cornea. Anduze31 proposed a grading system for recurrence from grade 1to 4where grade 1 is normal postoperative appearance and grade 4 is a growth of fibrovascular tissue into clear cornea. Although several techniques are available evidence-based literature has shown us that certain treatment techniques offer clear-cut advantages over others in terms of decreasing the pterygium
\\70@D@OOPAN·AMERICA : 11

REVIEW
recurrence rates. This has been reviewed by Hirst in an extensive evidence-based review on the surgical treatment of pterygium 29 We herein review both the current methods and recent advances in the surgical treatment of pterygium.
Bare Scleral Closure This technique involves removal of pterygium from the cornea combined with excision of some bulbar conjunctiva nasally, and allowing the defect to real naturally Bare scleral excision is probably the most common surgical technique used when adjunctive therapy such as intra operative alld post operative mitomycin (MMC) is used. The major benefit of this procedure is the simplicity of the technique This technique was the most preferred method of removing a pterygium in the 60's and 70's and long term follow-up studies have shown that it is by far the least satisfactory surgical method with respect to recurrence rates which can range from 24% to as high as 89%32.33
Conjunctival Flaps The high recurrence rate following bare sclera technique lead to the development of various other surgical strategies using the premise that closure of healtilY conjunctival tissue following pterygium excision would prevent recurrence. The three basic variations on this strategy include simple conjunctival closure, sliding conjunctival flaps and conjunctival autografts. The simple conjunctival closure involves removal of the pterygium with minimal conjunctival excision and closure of the residual conjunctiva with absorbable/non absorbable sutures. Apart from two studies there is paucity of evidence to support this method of removal where the recurrence rates range from 45-69%.34,35
Conjunctival Autograft Conjunctival autograft transplantation was first described by Kenyon et al in 198536
In this technique, following excision of the pterygium a free conjunctival autograft harvested from the superotemporal bulbar conjunctiva is used to resurface the bare scleral area, This technique has gained in popularity and has become the standard treatment option, Kenyon36 in his original description of the technique reported a recurrence rate of 5.3% after 57 procedures (16 primary and 41 recurrent pterygia) with amean follow-up of 24 montlls. Over the last 15 years there have been several prospective
12 : W!J§O@lmPAN·AMERICA
/retrospective studies looking at the recurrence rates of both primary and recurrent pterygia treated with conjunctival autografts, The recurrence rate with this tecllnique varies from 2%37 to 39%.38 Compared with other techniques, the overall, the recurrence rate with this technique is low. Pooled data Irom eight different studies using conjunctival autograft showed an overall recurrence rate of 7.9% (21 recurrences among 265 cases),39 Complications from conjunctival autografting are infrequent and are not sight threatening, Minor post operative complications include conjunctival graft edema, corneoscleral dellen and epithelial inclusion cysts. Less common complications include induced astigmatism; graft hematomas, tenon's granuloma and graft retraction / necrosis,
Conjunctival Limbal Autograft (CLAG) The evolution of conjunctival transplant surgery for pterygium has mirrored the changing bel ief regarding the etiopathogenesis of pterygium During the last decade two types of conjunctival autograft have been harvested: conjunctival grafts that purely consist of bulbar conjunctiva (without any limbal tissue) and conjunctival limbal autografts (CLAG) The harvesting technique of CLAG is similar to conjunctival autograft harvesting, except that the limbal edge of the donor graft is extended to include limbal epithelium, either by superficial keratectomy, or by superficial lamellar dissection, This side of the graft is then placed at tile limbal edge of the recipient scleral bed so as to match and reconstruct the limbus with stem cell-containing epithelium. Although the early reports on conjunctival transplantation for pterygium have been on the use of conjunctival autografts, more recent publications have reported on the use of CLAG for both primary and recurrent pterygium. These techniques have been based on the premise that the CLAG help to repopulate the limbal stem cells which have been damaged by UV light 40, 41, 42 In our experience we retrospectively followed 65 eyes that underwent CLAG for primary pterygium with the use of fibrin glue; at a mean follow-up of 11 months there were no cases of pterygium recurrence that required repeat surgery Fayez 42 data shows that both CLAG and traditional conjunctival autografts were effective in cases of advanced primary pterygia, whereas in recurrent pterygium CLAG appears to be more effective in preventing recurrence. Certainly well- defined prospective randomized studies are required to determine whether inclusion of limbal
tissue in the autograft affects the rate of recurrence in both primary and recurrent pterygia,
Amniotic Membrane Transplantation (AMT) The use of preserved human amniotic membrane as an alternative basement membrane substrate has been reported for use in ocular surface transplantation procedures such as limbal allograft transplantation pterygium surgery 43-44 The use of amniotic membrane transplantation (AMT) has been shown to reduce pterygium recurrence Amniotic membrane is effective in reducing scarring and fibrosis in ocular surface surgery. Most recently, it has also been shown to suppress TGF-~ signalling in conjunctival and pterygium fibroblasts 45,46 Although less efficient than conjunctival autogratting in preventing recurrence (14,8% versus 4,8% in a comparative study),34 the procedure often results in an excellent cosmetic result It has certain advantages over conventional autografting in that the superior conjunctiva is not utilized and the procedure is relatively simple to perform, Tile main draw-backs are the cost and accessibility of AMI
c. Adjunctive Therapies The four main agents used as adjuncts either during pterygium removal or postoperatively include beta irradiation and thiotepa (both used postoperatively) and MMC (used both intra and post operatively).
Beta Irradiation Ionizing radiation inhibits the mitosis of rapidly dividing cells and therefore actively proliferating tissues are most susceptible Beta irradiation with Strontium-90 has been used at doses [rom 1000-7000 cGy. Although beta-irradiation has been used for over half a century, reported studies on both efficacy and safety are generally lacking in numbers, and follow-up time, and few prospective randomized trials exis!.4u8
The adverse events relating to betairradiation surgery are believed to be doserelated, and include serious complications such as cataract formation, iris atroplly, scleral necrosis and melting, and calcific scleral plaque formation 33-34 Ocular surface complications reported include conjunctivitis, conjunctival cicatrisation, keratitis, photophobia and ptosis. In view of the potential serious complications and the existence of
I effective alternate therapeutic strategies, we do not recommend the adjunctive use of beta-i rradiation.

Febrero 2007
........_--------------------------------
Baxter /
Tisseel® Kit VH 1.0 m Two·Componenl Fibrin ~alanl (Human), Vapor Heated Colle de fibrine it deu~ composanls (humaillll), Iraltee ala vapeur
Figure 2: The commercially a"ailable fibrin glue (Tisseel).
Mitomycin C(MMC) Mitomycin-C (MMC) is an antibiotic-anticancer agent lhat inhibits DNA, RNA and protein synthesis and has a longterm effect on cell proliferation MMC has been used as an adjunct to glaucoma and pterygium surgery, where it induces prolonged localized inhibition of Tenon's fibroblasts. This reduces trabeculectomy bleb scarring and pterygium recurrence. Topical 0.02% MMC has been used after pterygium surgery twice daily for 5 days. The side effects of topical MMC may be associated with significant and potential sightthreatening complications. These include iritis, limbal avascularity, corneal melting, scleral melting or calcific plaque formation, corneal decompensation, scleral or corneal perforations, secondary glaucoma and cataract. 49-52
Figure 3: The Duploject injector systcm, which simultaneously delivers both the prolein and the setting solution.
Fibrin Glue Fibrin-based adhesives, by contrast, have a lower tensile strength and slower polymerization, but, being biologic and biodegradable, they may be used under a superficial covering layer (eg, conjunctiva, amniotic membrane) and induce minimal inflammation, Recently the use of fibrin glue for attaching the conjunctival autograft during pterygium surgery has gained in popularity 59, 60
There are several commercially avai lable fibrin glue products The most commonly available in North America is from Baxter. Tisseel® (Tisseel 1.0 ml VH, Baxter Corporation) is a commercially available two component fibrin sealant which mimics the natural librin and acts as tissue glue with sealing, hemostatic and gluing properties (Figure 2), The glue has two components 1. Sealant Protein A freeze dried powder composed of human fibrinogen, fibrinonectin, plasminogen and Factor XIII reconstituted in a bovine aprotinin solution, 2. Sealant Setting: A solution composed of human thrombin reconstituted in a calcium chloride solution, When both these solutions interact, through the action of thrombin, the fibrinopeptides are broken down to fibrin monomers These monomers aggregate by cross linking, leading to the formation of fibrin clot. There are several ways in which the glue can be applied. The most common and our preferred technique is to use the Duploject injector system (Figure 3) which simultaneously delivers both the protein and setting solution. The glue is applied to the bare sclera following which; the cOlljunctival graft is laid on its surface
WO@O@If!JPAN·AMERICA : 13
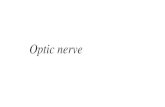
Figure 4: Intraoperative phorograph demonstrating the application of fibrin glue to the scleral bed.
In an attempt to reduce the toxicity and complications associated with topical MMC use, several studies now advocate a single intraoperative application of MMC, as is used in glaucoma filtration surg eryS3-56
Recurrence rates reported with intraoperative MMC application range from 3% to 43%, and are generally comparable to topical MMC. Complications have also been reported with the use of intraoperative MMC. These include early punctate epithelial keratitis, chemosis and delayed conjunctival wound healing and conjunctival granulomas There has also been one case of corneal melting after intrao
perative MMC application reported. 57, 58
We currently use intraoperative MMC for recurrenl pterygia only at a concelltration of 0.02 mgjml MMC on asaturated weck cell for 2 minutes. The bare scleral site is then closed with aconjunctival autograft.
d. Newer Treatment Modalities
Tissue Adhesives The types of tissue adllesives used in ophthal-mology can be broadly divided in to synthetic adhesives (eg, cyanoacrylate derivatives) and biologic adhesives (eg, fibrin-based adhesives). Cyanoacrylate derivatives are compounds with very high tensile strength that rapidly polymerize on contact with basic substances such as water or blood to form astrong bond.

REVIEW
Figure 6: Well secured conjunctival autograft following the application of fibrin glue.
Figure 5: Intraoperative photograph demonstrating the application of fibrin glue to the scleral bed.
(Figure 4-5). Alternatively the conjunctival graft (with the right orientation) can be laid on the scleral bed and Ouploject injector system can be used to deliver the fibrin glue underneath the graft, In our experience we find that this technique minimises the wastage of glue as glue applied to the bare sclera seems to often run down to the inferior fornix,
Koranyi et al 59 in a randomized prospective clinical study demonstrated that using glue instead of sutures when attaching the conjunctival transplant in pterygium surgery causes significantly less postoperative pain and shortens surgery time significantly Recently the same gro up61 in a large retrospective study showed that using afibrin tissue adhesive instead of sutures when attaching the conjunctival transplant in primary pterygium surgery results in a significantly lower recurrence rate. We recently reported on our cohort of 65 eyes of 62 patients who underwent CLAG for primary pterygium surgery with fibrin glue, At a mean follow up of 9,5 months (range 9-14 months) there were no cases of recurrence that required repeat surgery62 (Figure 6) Although the recent literature on the use of fibrin glue during primary pterygium surgery is promising further prospective studies are required to analyse their long term out come in both primary and recurrent pterygium surgeries
Anti-Angiogenesis Therapy Recently Aspiotis63 and his co-authors in a laboratory study demonstrated higher expre-ssion of angiogenesis-related factors (higher count of microvessels, increased vascular endothelial growth factor [VEGF], decreased expression of thrombospondin 1 [TSP-1]) Gebhardt et al64 also demonstrated higher expression of VEGF in pterygia when compared with normal conjunctiva but with similar levels of expression in the limbus and pterygia, These results suggest that VEGF has some role to play in the development of pterygium and further clinical studies are required to see whether the currently available anti VEGF drugs are of benefit in the medical management of pterygium.
14 : WU~[]@{Ii]PAN·AMERICA

~--------------------------
Febrero 2007
I. Saw SM, Tan D. Pten'gium: pre\'alenee,
demography and risk l"c1ors. Ophthalmic Epidemiology 1999: 6.2 2. Moran DJ, Hollows Fe. Plervgium and ultraviolct radialion:.a positi\'e correlation. Br J Ophthalinol 1984; 68:343-346
3. Hill JC, Maske R. Pathooene"i" of pterygium. Eye 1989;3:218-226 4. Barraquer-Somers £. Chan Cc. GreeJl WR. Corneal
epitheli~1 iron depositi"n. Ophtualmology 1983;90:729 5. YoungsoJl RM. Ptengium i11 hraeL Am] Ophth'almol 1972:~-!:95-!
6. Oldenburg J13. Conj,mcti\'al ptel)'gia: mechanism of corneal topographic chaJlg"•. Cornea 1990;200:9 7 ..Cridley M], PerlmaJl [\[:.-\ form of variable asligmati'slll induced b~' PseudopterygiuJII. Ophlhulm.ic Surg 1986;17:794 8. Sivasubramanial1 P. Pte''\'gium in Ceylon. Br] Ophthalmol 1971:.5.5:.55.
9.. Norn MS. Prevaleuce l,f pinguecula in Greenland and in .Copenhagen. and iL..; rdation to pterygium,and
spheroid degeneration..-\cta OphthalmoI1979;57:96) 10. Coroneo M. Pten'gium as an early indicator of ultraviolet in~olati"n: a 11\1'0thcsis. Br J OphtbaJllJol 1993; 77:734-739 II. Hinit Hli. DistributioJl. risk factors, and
epidemiology "f pter:giuJII. In: Taylor HR, editor. Pterygium. Tbe "etherlands: Kugler Publications ,2000:15-28 12. Cameron M. UtIa- ... iolet radiatiou. Pterygium th.roughout the l'iorld 1965: 41-54. '
13, Mackeu"ie tD et a!. Ri,k analysis in the,.iIevelopmeJlt oj pten·~>ia. Ophthalmology 1992;99:1056. 14; Coroneo M. _-\lbedo roncentration in the anterior
··eye: a phenomenon that lo('ales some solar diseases. Opbthalmic Surgen' ]990: 20:60·66 15, Zhang J-D. An invcstigalion of aetiology ~nd
heredity of pte,,'gium. Report of 11 eases in a family. A<:ta Ophthalmologica 1987; 65:413-416
16. Hilgers, JHCh. Pten'gium: Its inciclence, beredity and etiology. Am J Ophthalmol 1960; 635-644' 17. Pinkerton OD. Hokama Y, Sbigeniura LA.
.Immunologic basis for the pathogeuesis of pterygium. Am J Ophthalmol 198-!: 98:225-228 18. Tseng SCG, Lee 5-8, Li D-Q. limbal stem cell deficiency in the pathogenesis of ptel)'gium. ·In: Taylor HR, editor.. Pterygium. The Netherlands: Kugler Public~tions, 2000:-!I-56 19. Wong Ww. A h\'pothesis on the pathogene";,is of ptel)'giums. Anll.OphthalmoI1978; 10:303-309 20. Goldberg L, David R. Pterygium and its relationship to tbe dr~' e\'e in the Bantu. ilr.]. Ophthalmol1976; 60:721-~31
'. 21. Biedner B, Biger Y. RoghkoIJ L. Pterygium and basie [eaT secretion. Aun.Ophthalmol 1979; Il:123,5' 22. Dimitry'!' The dust far tor in the production of pterygium. Am J Ophthalmol1937; 20:4'{)-45 2'3. Varinli S, Variuli I, E.rki,;i M, Dorau E Human
papil10mlivilUs iu pJerygilllu. Central Afr] Med 1994; 40:24-26
24. SchermeT A. Galvin S. Sunn IT. Differentiationrelated expressiou of maj"T 64k comeal keratin ill vivo and in (;'ulture suggests.limballoeulion of cor_neal epithelial stem cells. J Cell Bioi 1986;103:49-62. 25. Wei.ZG, Wu RL, Lavker RM, Sunn 'IT In vilro growth and differentiation of rabbit bulbar, fornix,
. and palpebral conjunctival epitbelia: implications on conjunctiyal epithelial transdifferelltiation and slem ':ells. Invest Ophthalmol Vis Sri 199;1;.34:1814-1828. 26. Dushkll N,Tyler N, Reid TW.
In'l.nlUn?his~ochemicaL evidenee that pterygia arise from altered limbal e.pithelial basal stem cells (abstract) Invest OphthaImol Vis Sci 1993;34:51013.
27. Dushku N. Reid TW.lm'"l1nohistoehellliral evidence t.hat.human pterygia OiigiIHlte (rom an invasion of vimentin-expressing altt';,red limbal epithelial basal cells. CUlT Eye Res 1994;13:473-481. 23. Dushku N, Hatcher SL. Albert DW, Reid TW, , p53 expression llnd relation to human papilloma,:irlls infectioil iH pingueculae. I-'lerygia and limbaltumors: Arch Ophthalmnl 1999;117:1593-1599. 29. Hirst LW, The treatment of Pterygium. SlIrv. Ophthalmo12003;4.s:140-180.
30. Ricb AM et at A simillified way to reI\)OYe pterygia. Ann OphthahnoI197It;6:739. :31. Anduze AL Ptel;-gium staging in the Caribbean. AnnOphthalmoI1998;30,92-9tt,
32 . .Jaros'PA, DeLe'lise· VP. Pingileeulae and pte.rygia. Surv OphthalmoI1988;33:11-49. 33. Sing G, Wilson MR, Fosler CS. Mitomycin eye drops as treatment for pterygium..Ophthalmology 1988;95:813-821. 34.• Prabhasawat P, Balion K, Burkett G,Tseng SC.
Comparison of conjunctival autografts, amniotic membrane' grafis;and primary dpsure fdI' pterygilln, excision. Ophthalmology 1997;104:974-985. 35. Riordan-Eva P, Kielhom I, Ficker LA et a!. COlljun6tj\'~Ll alltografti-ng in the surgical- trealment·of pte''ygiulll. E:ye 1993;7:634-63836. Kenyon KR, Wagoner MD, Hettinger ME. Conjunctival autograft transplantation for ad;'auced and recunelll pterygiulll. Ophthalmology 1985;92:1.461.
37. Tan DTH, Chee SP, Deat: KBG, Lim ASiVL Effect ofpte~·ygillIT1 morphology on pterygium "recurrence in a controlled tlial comparing conjunctival autograftiug with bare sclera excision. Arcb Ophthahnol 1997; 115:1235-1240. 38. Chen PP,A1'j'vasuRC, Kaza Y, L1Bree LD,· MeDollnell Pl- A raudomi"ed trial comparing .mitomycin C and cOl\junctival autogJ'aft alter excision of prima')''"pterygium. Am J Ophthalmol 1995;120:151-160 39. Allan 'DDS et al. Pterygium exc,i.ion with
'eonjul1cti,'al alltografting: cUI effective and safe
technique. 81' J Ophthal.moI1993;17:698 40, Mut!u FM, Sobaci G, Tatar T. A comparative study of recurrent pte')'giulll surgen': limbal conjunctival autograft transplantation VerSllS mitomycin C with conjunctival flap. Ophthalmology 1999;106:817-82141. Cris 0, Guell JL, Del Campo Z. l.imbalconj"netival autograft ll'ausplantation for the treatment of recurrent pte'}'giul1I, Ophthalmology 2000;107:270273. 42. Al.F'ayez l\1F. Lililbal verSllS conjunct;\'al
autograft transplantation for advanced aud recuri'ent ptel),giunl. OphthalmOlogy 2002;109:1752-1755. 4·3. Shimazaki.J, Shinozaki N, Tsubota K. Tr~ns'plpqtation of anmio'lic membrane and limbal autograft for patients with rerunent pterygium assoc,ia(edwith symblepharon. Br J Ophlhalmol 1998;82:235-240 44. Lee S, Tseng S. Anllliotic membrane transplantation for per$istent epithelial "delects with
. lliceration. Am J Ophihal.iuoI1997;123:303-312 4-5. Shirnazaki J, YangH-Y, Tsubota K. Anmiotic merribrane transplantatioil for ocula1' sUlfaee r.econstruction in patients with chemica] aBct th~rm~t
bllrns. Ophthalmology 1997;104.12:2068-2076 46. Tseng SCG, Prabhasawat P, Barton K, Gra)' T, MeHer D. Amniotic membrane transplantation with Or withoutlimbal allografts for coOrnea] surface reconstruc.tioll·;n patients with linIDal stem 'cell deficiency. Arch OphthaJmoI1998;J.l6:4..:n -441 '47. MacKenzie Fb, Hirst LI'i~ Kynaston-B,. Bain C. Recurrence rate and complirations after bt:ta ilTacliation for pterygi,a. Ophthalmol"gv 1991:
98,12:1776-1781
48. Moriarty AP, Crawford GJ, McAllister fL, Constable !.T. Severe corneo,scleral infeclion: a
complication ofbeta i~'adiation scleral necrosi~ following pterygium excision. Arch. Ophthalmoll993; 111:947-951 49. Hubinfeld RS, Pfister RR, SteinRM, Foster CS, M~;lin NF, Stbleru S, et al. .Seri;us complications
of topical mitomycin-c a1ter'pterygiull1's~lrgeI)" Ophthaln'lOlogy 1992; 99.1 1:1641-1654 50~ Dun~ J.P, Seamone CD,Osilcr HB,Nickel BL: Beallo A. De"elopmcnt of scleral ulceration' and calcification after ptel),giulll excision and mim,mycin therapy. Am] Ophthalmol ] 991;343-344 51. Lin C~P, Shih M-H, Tsai M-C.Clinical experiences of iljfeetious scleral ulceration: A complicationofpterygium operation. Br..I Ophthalmol 1997; 81:980"983 52. Frueht-Pel), J, Siganos CS, Ilsar 1'Il.InlrllOperative application of topical mitomycin C for<pterygiultl SurgCl}'. Opbthalmology 1996;103.4:674-677 53.C81:dillo JA,Ahes MR, Ambrosio U(Potelio MB, Jose NK. Single intraoperative application vcrsus postoperative mitomycin C eye drops in- pterygium surgelY Ophthalmology 1995;102.12:1949-1952 54.Yanyali AC, Talu 1-1, Alp BN, Kat'abas L, Ay GM,
Caglar Y. hll.raoperativc mitomycin C in the trealmenl ofpterygiull1. Cornea 2000;19:471-473 .
55. Frucht-Pel}' J. Siganos'CS, flsar M. Intraoperative application of topical milomyoin C for pterygium . surgcI)'. Ophthalmology 1996;103.4:674-677 56. Poterio MB, AI,,,,s MR, Cardillo JA, Jose NK. An
i'tnpro\'ed ·surgicallcchniqu(; fo~ pletygium."exclsion with intnwperatiye application of milomyc.in-C. Ophthalmic Surgery and Lasers 1998;29:685;687 :37. Doughert)' P.J, Hardten DR, Lindstrom HL. Corneoscleral mell after ptel;-gium surgery using a single intraoperative application ofmitomycin-C. Cornca J.996; 15:537-540 58: Helai M, Messiha N, A;nayem A, EI-'Maghraby A, Elsherif Z, Dabees M. Intraoperative mitomycin C versus postoperative mitomycin C.for the lreatmenl
of pler)'gium. Ophthalmic Surgcl)' and Las,;r8)996; 27:674-678 59. Koran)'i G, Seregard S, Kupp E D. Cut 'and paste:
a no "ntuI'e, smaiL i,ir.ision approarh to pte'ygiull1 ,urgeiy. Br.T Ophthalmo12004;88:911-914. 60. Uy HS, Reyes .JiI'1G, Flores JDG, et a!. Coniparisorr of fibrin Glue and sutures fi)l'attaching conjunctival autografts after pterygium excisidll.' " Ophthalmology 2005;112:667-{j71.
61. Koranyi G, Seregard S"Kopp. Ep. The cUI-andpaslemetbod. for pri mary ptel}'gium surgery: long-term follo\Nlp. AGta Ophthalmol Scand. 2005 Jun;83:2983bl. 62. Srinivasan S, DoUin M, Rootman DS, Sloll1o"ic
AR. Apl?lication of fibli11 glue to conj\lIlctivalautog1'aft dmi n{!; plimary ptel),gium surgery. Annuill meet ing of the Amel;can Society of Cataract and Refi'active Surg~ry, Mareh 2006, San Fr<nrcisco, USA. 63. Aspiotis M, Tsanou E, Gorezis S, loachim E, Skyrlas A, Sfefaniotou Malainou-Mitsi V. Angiogenesis in pteI;-gium: study of micl:ovessel density, vascular eudothelial gni;,th f~ctor ami
lhroll1bospondin-l. Eye ad"anre o';line publication, 23 June 2006; doi:! 0.1038/sj.eye,6702495. 64.Cebbardt M,Mentlcin R, Schaudig U, Pufe 1', 'et al. bifferential expression of vascldar endothelial grpwlh faclor implies 'the lin~bal origin of,ptClygia. Ophthalmology 2005;112:1023;1030.
WO~O@ImPAN·AMERICA 15

CLINICAL SCIENCES
Lin lu e I al ur I sni enomen e
, ico?
Eduardo Arenas MD Elena Oudovilchenko MD Bogota. Colombia
RESUMEN Se presenta un estudio prospectivo en el
que se analizan una serie de pacientes en los que se les sospech6 una cefalea oftalmica inducida por la mala posici6n de uso de los monitores de computador, de acuerdo a un protocolo en el que se recomienda que la altura del mismo este al menos 15 grados por debajo del eje visual. Todos los pacientes inclufdos usaban el computador tipo personal por un lapso mayor de 4 horas diarias, tenian cefalea yutilizaban el monitor por encima del eje visual. A todos se les descart6 cualquier otra causa oftalmol6gica 0 sistemica responsable de la cefalea. Se excluyeron aquellos pacientes usuarios de laptop. La mejoria de los sfntomas asten6picos fue del 70% tres semanas 0 mas despues de haber corregido la altura de uso del monitor. Se insiste en la importancia desde el punto de vista ocular, laboral yergol6gico yse explican las posibles causas fisiol6gicas responsables de este nuevo sfndrome del Monitor.
SUMMARY We present aprospective study analyzing
a series of patients with ophthalmic cephalgia, probably induced by an erroneous posi-tion of the screen more than five degrees above the level of the sight in VDT users. All patients included in the analysis used the VDT more than 4 hours every day, complained of cephalgia and asthenopia as one of their symptoms and were using the screen computer 15 degrees above eye level. Patients with other causes of cephalgia such as inappropriate refraction, general disorders and use of laptops were excluded. After several weeks and proper positioning of the screen, patients were questioned about their symptoms, and 70% reported a clear improvement. The pathophysiology of this finding called "screen VDT cephalgia" are discussed along with its importance and relevance in the workplace from and ophthalmologic and ergonomic standpoint.
INTROOUCCION. Hoy en dfa los computadores personales
11an tomado un puesto de gran importancia en todas las actividades del ser humano. No s610 dentro de la industria, sino tambiEm en la vida cotidiana, como reflejo de la expansi6n de los sistemas de comunicaci6n.
Dicho aumento ell el uso de los computad ores ha conducido a la aparici6n de riesgos para la salud antes no conocidos. Un porcentaje importante de estos son debidos a alteraciones que afectan la funci6n y desempeno visual. Donders en 1864 fue el primer autor quien resalt6 la importancia del trabajo visual cercano prolongado y su relaci6n con trastornos de acomodaci6n y binocularidad.
Con la popularizaci6n de los computadores de uso personal y en la oficina, un numero creeiente de publicaciones han senalado los factores de riesgo y las earaeteristicas epidemio16gicas de los trastornos visuales asociados al uso prolongado del computador. Actualmente se considera que la afecci6n visual de los trabajadores de computadores puede Ilegar hasta al 70% de los usuarios.
De acuerdo aun estudio previa hecho por nosotros en relaci6n ala cefalea oftal mica, las principales quejas visuales que se presentan son oj os cansados (85,7%), hiperemia conjuntival (571%), visi6n borrosa (48,6%), dlficultad para enfocar (40%), epifora (37,1%), sensaci6n de cuerpo extrano (28,6%), dolor ocular (371%), fotofobia (314%), cefalea (14,3%) (10)6. Con el fin de cornprobar en que proporci6n afecta el uso de los monito I
res en personas j6venes se diseM un estudio en el eual se hizo bastante enfasis en la altura I
de uso del mOllitor.
Se realiz6 un estudio plloto, prospectivo de los pacientes con cefalea 0 quejas visuales, con una agudeza visual mejor corregida 20/20 ambos ojosy usodiario del computador mayor de cuatro horas, seleccionados de la consulta de uno de los autores (EA) que asistieron a examen oftalmol6gico por primera vez desde febrero del 2001 hasta abril de 2002.
Todos los pacientes fueron interrogados
Figura 1: Altura apropiada 15 grados por debajo del eje visual.
Figura 2: Altura inapropiada enfoque de la pantalla por encima del eje visual.
en relaci6n a un listado de quejas (Tabla1), para determinar la presencia del sindrome por uso inadecuado de computadores segun la altura de uso de la pantalla del computador por encima de 15 grados del nivel de los oios Se excluyeron los pacientes en los cuales se diagnostic6 una patologfa organica ocular 0 defectos refractivos no corregfdos que explicaran la sintomatologia, as! como los usuarios de computadores portatiles porque en este caso la altura de la pantalla es siempre la posici6n normal de lectura fisiol6gica. Se tomaron los datos de la histaria clinica, se hizo examen oftalmol6gico completo incluyendo agudeza visual, sensibilidad al contraste, visi6n los colores, refracci6n, prueba Schirmer, biomicroscopia ocular, presi6n intraocular y fondo de ojo EI defecto refractivo rue clasificado en miopfa (menor de 5dioptrfas ymayor de 5dioptrias), hipermetropia (menor de 3 dioptrias y mayor de 3 dioptrias) y astigmatismo (mayor 0 menor de 3dioptrias).
Se evalu6 la altura del monitor a traves de una escala analoga visual. Figuras 1 y 2
A los pacientes con diagn6stico de asten6pia por uso prolongado de computador se les hizo la recomendaci6n de corregir la altura del monitor en el angulo 0 distancia explicada
16 : WU©O®Gt]PAN·AMERICA

..I
Sintomas visuales relacionados con el trabajo
en computador
I. Cansancio visual.
2.Ardor ocular.
3. Dolor ocular.
4. Enrojecimiento.
5. Sensacion de cuerpo
extrano ocular.
6. Lagrimeo.
7.Vision borrosa.
8. Cefalea.
9. Fotofobia.
10. Sequedad.
I I.Temblor palpebral.
Tabla 1
por nosotros. No se realiz6 ninguna otra intervenci6n (cambio de len es correctoras, terapia farmacol6gica t6pica 0 sistemica, etc)
Los datos analizados fueron edad, sexo, tiempo continuo de uso del computador durante el dia, refracci6n sintomas y signos visuales, altura previa del monitor.
La evaluaci6n y seguimiento de los sfntomas se realiz6 a 'raves de una escala porcentual de mejoria 0 empeoramieto.EI seguimiento de los sintomas de los pacientes se hizo alraves de una nueva consulta personal oatraves de una encuesta telef6nica.
Se incluyeron en el estudio 38 pacientes, quienes completaron los requisitos de ingreso, Seis de estos pacientes se excluyeron por no completarse el seguimiento (actual mente no viven en el pals) Los resultados que se presentan corresponden a 32 pacientes en quienes se complet6 la evaluaci6n.
Los pacientes ten fan 33.7arios en promedio (rango de 18 a 51 arios), 18 (56,2%) de ellos fueron mujeres, 14 (437%) hombres. AI evaluar el estado refractivo de los pacientes se encontr6 que 9 (28.1 %) de ellos eran emetropes En los pacientes quienes ten fan algun delecto refractivo 4 (17.4%) eran miopes menores de 50, 1 (4,3%) miope mayor de 50, 8 (347%) hipermetropes menor de 3D, 1 (43%) hipermetrope mayor de 3D y 9
Febrero 2007 ~
Caracterlsticas de los pacientes (n=32)
Caracterfstica Sexo (hombres/mujeres %)
Edad , promedio (anos) (rango)
Tiempo de uso de computador, horas (rango)
Defecto refractivo (%) Miopes
< -5.00 D > -5.00 D
Hipermetropes < 3.00 D > 3.00 D
Astigmatismo < -3.00 D > -3.00 D
Emetrope
Altura previa del monitor, grados (rango)
Media 43.7% / 56.2%
33.7 ( 18-51 )
8.2 h (4-12h)
23 (71.8%)
4 1
8 1
9 o 9 (28.1%)
9 grados (0-22)
Tabla 2
(39,1%) presentaban astigmatismo menor de 3D, (Tabla 1)
Se encontr6 que el tiempo promedio de uso del computador (ue de 8.2 horas al dfa (rango entre 4y12 horas) y la altura promedio del monitor 9grados por encima del horizonte visual (rango -5 a20 grados) Tabla 2
La mayoria de los pacientes presentaba mas de 3 quejas visuales y la distribuci6n de los sfntomas se presenta en la Tabla 3.
Las quejas mas frecuentes fueron cansancio visual, celalea, ardor y enrojecimiento
Los pacientes fueron seguidos entre 2 y 12 meses despues de su valoraci6n inicial. Se encontr6 que los pacientes habian disminuido la altura del monitor 10 grados en promedio desde la altura inicial (rango de -5 a 20 grados ), Veintiocho (87.5%) de los pacientes reportaron mejoria de sus sfntomas, dichos sintomas mejoraron en promedio 703% con respecto a sus molestias previas (rango de 10 a100%) Cuatro (12,5%) de los pacientes no referieron cambios, Ninguno de los pacientes present6 empeoramiento de los sfntomas Tabla 4,
La evidencia de los hallazgos clinicos de mejorfa en la sintomatologia previa, indica que evidentemente la mala posici6n de los ojos en relaci6n con la pantalla del monitor desencadena una serie de trastornos
en la fisiologia normal que ha desarrollado el hombre a traves de los mecarlismos de acomodaci6n convergencia en su evoluci6n para efectuar labores manuales y lectura
En 1993 Heuer identific6 la altura del monitor como un factor del riesgo para desarrollo de sintomatologfa visual. Nuestro trabajo muestra que 87.5% de los pacientes refieren algun grado de mejoria, la cual fue evaluada en forma subjetiva y referida como 70,3% de mejoria de sus sfntomas. Los sintomas visuales relacionados con trabajo en computador en nuestro estudio fueron similares a un estudio realizado en Mexico, aunque
Tabla 3
Proporci6n de sintomas en pacientes c1asificados de tener
el sind rome del Monitor
Cansancio visual 75
Cefalea 62,5
Enrojecimiento 62,5
Ardor Ocular 56,3
Fotofobia 34,4
Temblor palpebral 28,1
Lagrimeo 25
Sequedad 21,9
Dolor ocular 15,6
Sens.Cuerpo extrano 12,5
Wll@O@OOPAN·AMERICA : 17

CLINICAL SCIENCES
Cambios en los sintomas visuales despues de disminuir la altura del monitor
Resultados Total
Disminucion de altura del 10
monitor grados Rango 5 -20
Pacientes con mejoria, % 87.5
- % de mejoria 70.32
Pacientes sin cambio. % 12.5
Tabla 4
se encontr6 una mayor incidencia de cefalea y una menor frecuencia de visi6n borrosa, sensaci6n de cuerpo extrano y dolor ocular en los pacientes colombianos.
Pensamos que los sfntomas visuales relacionados can la altura por encima del horizonte visua I del monitor pueden ser debidos a varios mecanismos risiopatol6gicos La congesti6n ocular ocup6 el segundo lugar en frecuencia de sintomas probablemente deb ida a la alteraci6n en la lubricaci6n al tener una mayor superficie ocular expuesta y disminuci6n del parpadeo espontaneo como ha sido observado par Tsubota y Cois. Los sfntomas de dolor y cansancio se deben al transtorno en la sinquinesis acomodaci6n convergencia ymiosis que debe producirse can la lectura, completamente alterados en una posici6n inadecuada, como 10 anota Murube
Con base en estos datos se puede concluir que el trabajo can monitor aumenta la evaporaci6n de la pelfcula lacrimal par mayor superficie ocular expuesta y disminuci6n del parpadeo espontaneo. EI usa de un monilor localizado a nivel a sabre el horizonte visual implica cambios en la pelfcula lacrimal secundarios a los mecanismos mencionados y en relaci6n con dicha altura. En segundo lugar, la aparici6n de cansancio visual y cefalea pueden ser explicados par fatiga muscular ydolor reflejo frontal reflejo secundarios al esluerzo prolongado y t6nico de los musculos involucrados en la elevaci6n del globo ocular y el parpado superior. Yen tercer lugar para mantener la fusi6n de los objetos cercanos se requiere el mecanismo
18 : W1J©O®OOPAN·AMERICA
de Sinquinesis acomodaci6n-convergencia el cual s610 es posible mantenerse en el plano horizontal de la orbita (plano de aducci6n de los rectos medias). Si el objeto de fijaci6n pr6xima se encuentra arriba del horizonte visual en posici6n vertical de la cabeza, se requiere elevar el plano horizontal de la orbita hasta el plano del objeto de fijaci6n Esto se logra can la extensi6n del cuello mediado par el reflejo oculo-vestibular La fijaci6n prolongada en esta posici6n implica acci6n t6nica de los extensores del cuello, produciendo fatiga muscular y cefalea tensional secundaria.
Es posible que la asten6pia relacionada con el usa del compulador sea una causa frecuente de consulta al oftalm610go entre los pacientes j6venes y laboralmente activos. EI oftalm61ogo debe sospechar e interrogar al paciente acerca de la altura del monitor en todos los pacientes que consulten por sfntomas de asten6pia

Febrero 2007 EiJIIIIIII
Vision Pan-America es la publicacion olicial de la Asociacion Panamericana de Oltalmologia La publicacion esta particularmente interesada en recibir manuscritos que sean cortas revisiones de materias novedosas de interes pa a los oltalmologos miembros de la Asociacion. Ademas de las revisiones. la publicacion esta interesada en artfculos acerca de nuevas tecnicas quirurgicas, nuevas terapias medicas, ycasos de correlacion clfnico-patologica.
Informacion de Presentacion: Los manuscritos deben enviarse electronicamente al jefe de redaccion,
Mark J Mannis, ~ 0 a [email protected] puede enviarse via correo a:
Mark J. Mannis, MD, Department of Ophthalmology University of California, Davis 4860 YStreet, Suite 2400 Sacramento, CA 95817 U.SA
Si se envfa el trabajo por correo, este debe ir tanto impreso (a maquina, etc.) y en forma electr6nica (CD, etc.). Todas las presentaciones deben ser publicaciones originales que no se hayan publicado en otra parte. Las presentaciones pueden ser escritas en idioma espanol, ingles 0
portugues Todos los trabajos deben tener un resumen en ingles y en espanol
Los trabajos presentados no deben sobrepasar las 1500 palabras (seis paginas escritas adoble espacio) mas las referencias.
Las referencias deben ser incluidas como una lista en una pagina separada al final del manuscrito can referencias citadas codificadas al texto en el orden de aparicion
Formato de Presentacion: EI siguiente formato debe usarse para las referencias
Jones JS, Garcia TL. Perrero M. Retinopatfa Diabetica en Bolivia. Cornea, 1996; 26 (2) 341 - 343.
Smith OJ, Caldera MC, Chang N, Ferrer RJ Managing Trauma Ocular. Hofstra y Publicadores de Kennimore, Londres, 1989.
Se aceptan figuras de color y deben enviarse en PICT 0 formato JPG. EI formato de Powerpoint no es aceptable.
La pagina del titulo debe incluir 10 siguiente
(1) EI nombre completo de cada autor (es decir, nombre, apellido y la ·inicial media si usa,) y el grado academico mas alto;
(2) La ciudad, estado, y pars en que el trabajo se lIevo acabo; (3) EI nornbre y direcci6n del autor para recibir pedidos de separata; (4) Oeclaraci6n de los autores si existe 0 no interes financiero en un
producto citado 0 utilizado en el trabajo.
Vision Pan-America is the oflicial publication of the Pan-American Association of Ophthalmology. The publication is particularly interested in receiving manuscripts that are short state-of-the-art review papers that will be 01 interest to the practicing PAAO member ophthalmologist.
In addition to review articles, the publication is interested in articles on new surgical techniques, medical therapies, and case reports that emphasize clinicopathologic correlations.
Submission information: Manuscripts should be submitted electronically to the Editor-in
Chief, Mark J Mannis, MD at [email protected] can be sent via mail to:
Mark J. Mannis, MD, Department of Ophthalmology University of California, Davis 4860 YStreet, Suite 2400 Sacramento, CA 95817 U.SA
All submissions must be provided in electronic form as well as written manuscript lorm if mailed. All submissions must be original publications that have not been published elsewhere. Submissions can be in Spanish, English, Portuguese or French. All papers should be preceded by an abstract in either English or Spanish
Papers submitted should be no longer than 1500 words (six doublespaced type-written pages) piUS references.
References should be included as a list on aseparate page at the end of the manuscript with cited relerences keyed to the text in the order of appearance.
Submission Format: The following format should be used for referenced papers:
Jones JS, Garcia TL, Perrero M. Diabetic retinopathy in Bolivia. Cornea, 1996; 26 (2): 341- 341
Smith OJ, Caldera MC, Chang N, Ferrer RJ Managing Ocular Trauma. Hofstra and Kennimore Publishers, London, 1989.
Color ligures are encouraged and should be submitted in PICT or ,IPEG format. Powerpoint format is not acceptable.
The title page should ioclude the following
(1) each author's full name (i.e, first name, middle initial if used, and last name) and highest degree;
(2) city, state, and country in which work was carried out; (3) name and address of author to receive reprint requests; (4) statement about the authors' proprietary or financial interest in a
product or lack thereof.
W!J@O@OOPAN·AMERICA : 19

LUMfGAN~ (oimato~rost) ~.~J%
Preserva la vIsion alcanzando las menores presiones-objetivo en mas pacientes
Investigadores de diversos estudios, lAGIS, Shirakashi, Shields} han comprobado que alcanzar y mantener la PIO entre 14 y 15 mmHg reduce la progresion de perdida del campo visuap,2,3.
Lumigan® alcanza la PIO-objetivo de 14/15 mmHg en un mayor numero de pacientes:
LUMLGAN" vs. t' 1 14 ! LUMIGAN'vs dorzolamida/ LUMIGAN' vs. latanoprost 6
Imo () I . timo/o/ 5
Porcentaje de Pacientes que
alcanzaron la PID-Dbjetivo :s; 14 21% 9% 17% 2% 19% B%
Porcentaje de Pacientes que
alcanzaron la PID-Dbjetivo :s; 15 31% 16% 24% 9% 29% 14%
Mejor comodidad poso/6gica:
1 vez al dia.
No requiere refrigeracion.
Presentaci6n conteniendo 3 mI.
lumigarf bimatoprost 0,03%
SolUQ80 Ofl8lmlca Eslerll
UsoAdulto
~~~~~~~:r~~~~I~~ig61)crfr~~~~~~~~~~~~li~o:f6fdsaend~~\~~i·[~a:lcOo~i~~tx~~a~gd°cia:o~fo~t~~~~~~o ~a~:d~lci6~n~:n~ gre~i~g i~~a~~~~lgr~~;~aci:h~~U~~i~~~~eiocg~~~~;~:~a~fp~~e~~~J~d~ ~~n~:!Zg~~~i~na~~~a'~~m~~~:~;~e_filr.3i~a~i~~~~~r~J~fG~~;~bl~ig~~sYlLTe~·T~~ga~s~cb~~aOGUlaLContraindicaciones. LUMIGAN:& (blmatoprost) eSla conlralndicado en pacienles con h.ipersensibilldad al bimatoprosl 0 cualqUier olro componente de la fOrmula ~el prod ucla. Precauclones y Advertencias. AQlferlencias. Fueron relatados aumento Qf21ual del crescimienlo de las peslal'las en.el largo y espesura, y oscureclmiento de las pestaiias (en 22~J de los paClen1es despues 3 meses, y 36% despu~s 6 mEsas de U3lamJenloj, y, oscureCilnienlo de los parpados (en I a <3% de los paclen1es despues 3 meses y 3 a 10% ae los pacienles despues 6 meses de lIatamlenloj. Tambien lue relatado oscurecimiento del ins en 0,2% de los paclenles Iratados duranle 3 meses y en 1.t% de los pacienles lralados durante 6 meses. Algunas de esas alleraciones pueden ser permanenles. Pacienles Que deben -aaba el lratamienlo de apenas UIlO de los ojos, deben sel infOfmados a respeclo de esas feacciones. Precauciones WM1GANl3 (bimatoprost) na fue es~udiado ell llacientes can insuficiencia renal a he~lica y por 10 1anto debe ser uhlizado con cautela en lales pacienles.Las lelll::s de cantaclo deMn
~~r ~~if~d~~oa~1g~l~e e~~~~~~~a;i~~dgeul~~~~~~~; d~~~:~f~~~1 ~nP~n~~~~I~e~~e~g:~~a~:n~; ~~r~~fo~~~~ee~asl~tlr~~~~t::.~;be~~a s~~~~~~f~~~s~:.1~:N~ rbi:I~~ro~~ll~~~:e~~~r~~~u~~cT;n:6~~~°Ca~u:Ci~~J~~~~~e~f: ~~Sn~~~\;Sv~~1~~:~~~~so~e~~sma~~~n~~ ~i~d~~~a~~~~ ~T:c~~~~f~j~ti~~~lede c~~~~'O~~~~leS~~u~~,r(e~ii~~~~~r~o~~~a~~~O'~sd;;gl~;~a~ei~~1:~~!6~~~n6c~~a:es~Otm~an~S 3~ ~~ii~~~~f)~b:' ~~~a~~al ~~ra~a Iff~~i~nn~i~~~~:l~~~~~:~ ~~ ~0~1~t~~n~r~:~:6~~~i~~all;t~~~r,Ci~~~o~~~~~f~aesnti~~~~~~~~:r~ne~~~~Ee~~;~~nec~n~~~~~~;s No son conocidas incompalibilidades. Reacciones adversiJs, LUMIGANf (bimaloprost) es bien [alerado, pudlendo causar eventos adversos ocurares leves a moderados y no gralfes.EVljnlos adlfersos ocurriendo en 18-40% de las llacienles Que recibieron closes. urucas diarias, duranle 3 meses, en arden decrecienle de incidencia lueron: tliperenia conjuntival. crecimen!o de las peslaflas y prurito ocular,Eventos adlfersos ocurriendo en aproximadamente 3 a <.19% de los,pacienles, en orden decreclenle de incldencia, incluyeron: sequedad ocular ,ardor ocular. sensaclon de cuerpo estraM en el 910, dolor ocul?r y diSI\lrblOS de la vision Evenlos adversos ocumend~ en 1 a < 3~? .de los pacientes lueron: cefalea. e!itema de los llarllados, PI~mentacion de la pie I periocular, irritaclon ocular. secreclon ocular, aSlenopia. ~oniut1tlviHs alergica,
~a?rl~~eSla1 (1~~~[~a~~~'i~).~~~I~a~:ml~l~i ~~s r~~~~~e~~u~~Cr6~a~~~~n i6~~~;~~~.I~~:~i~I~~, I~;~~~~~~ a~e~~o~I~~I:ta~~m~~~~i~rb1e~~r~pr::~~~~If.~~:~lo{~e ~~~r~';ir6s ap~~i~~il~, d~~~P~~~~~li~~,.tb~~:~~ti~e~a~~~:n~a~n~~c~{i~t~~ie~t~~C~a~~~~l:c[&~I~~~O~e~ab~b~~~g;~~ durante 6 meses. ademas de los evenlos de mas arriba. lueron observados en aproxlmadamente 1 a <3% de los pacientes, erosion de la cornea. y empeofamiento de la aculdad visual. En menos de llJrio de los paclentes. blelarospasmo, depfcsi6n. retraCC!lin de los parpados.
~:~~~i~g~or~~~~a:c~;:r't~g~~a ~~;~~eunn~~aYd~rr~~~~~~sdru~O~e~~~:~id~d~~~S?: ~d~~~s~;~~f~~n~a~sl~e~~edn~~i~u~d:ndi~~i~~ili ~,C~i~j~:gnhi~~~~~~o~aS~~~~sl~e~~~~~~:~an n~C~rOef.tG~I~;:~(~~~fo~r~~~~:~:c~~·:g~r~[SI~~~og~~n~~mi:a~i~~~~~~a~~n uo~~~~;r~~~~:osa~'~a~~f~ :~~I\?~~Jrlr:t~cCI~ ~ ~~J~WI1iA~. iBU~No6olaco~m~~~1~TE'I~61~t~o~~31b1:1 ~G~OJI~ ~~~~I~~~~eAIDv'EdR~~~S1~a6i~~MI~nsm~J~~6n~ls~~~TM~~6n6~rD~~C'M tl~~CtE'mEp[~~2W~E~~~~N'~gJ~~~ri~ ~~6It~ AR~~~gMt~llN6ml~~~I~~1~f~~"t~ 1. The AGIS Investigators: The Advanced Glaucoma Inlervelion Study - The Relationship Between Control of Intraocular Pressure and Visual Field Deterioration. Am. J. Ophlhalmol, 130 (4): 429-40, 2000. 2. Shirakashi, M. et al: Intraocular Pressure·Dependel1t Progression of Visual Field loss ill Advanced Primary Opell-Angle Glaucoma: A 15·Year Follow-Up. Ophlhalmologica. 207: 1-5, 1993. 3. Mao, lK; Stewart, we; Shields, MB: Correlation Between Intraocular Pressure Conlrol and Progressive Glaucomatous Damage ill Pr1mary Open-Angle Glaucoma. Am. J. OphthaimOl, 111: 51-55, 1991. 4. Higginbotham. EJ et al. One-Year Comparison of Bimatoprost with Timolol in Patients with Glaucoma or Ocular Hyperlension. Presented at American Academy Ophthalmology, Nov 11-14, 2001. 5. Gandolfi, Set al. Three-Month Comparison 01 Bimatoprost and latanoprost in Patients wflh Glaucoma and Ocular Hypertension. Mv. Ther, 18 (3): 110-' 2t, 2001. 6. Co:eman, At el a1: A 3-Mon\h Comparison of Bimatoprosl with nmoloVOorzolamide in Patients WITh Glaucoma or Ocular Hypertension. Presellted at American Acedemy 01 Ophthalmol, New Orleans, la, 2001.