THE NORTH AMERICAN SPINE SOCIETY SUMMER SPINE …globus Medical’s expandable technology has been...
52
THE NORTH AMERICAN SPINE SOCIETY SUMMER SPINE MEETING July 23-26, 2014 Omni Amelia Island Plantation Resort Amelia Island, FL FINAL PROGRAM AND PROCEEDINGS
Transcript of THE NORTH AMERICAN SPINE SOCIETY SUMMER SPINE …globus Medical’s expandable technology has been...

THE NORTH AMERICAN SPINE SOCIETY
SUMMER SPINE MEETING
July 23-26, 2014Omni Amelia Island Plantation ResortAmelia Island, FL
FINAL PROGRAMAND PROCEEDINGS

bringing fusion to new heights
RISE® TLIF CALIBER®
Life moves us is a registered trademark of globus Medical, inc.
For More information Contact globus Medical at www.globusmedical.com/tLiF
866.456.2871
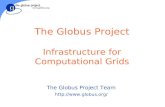
Minimal impactionContracted insertion height eases
insertion into the disc space
Controlled Disc height Restoration Continuous expansion and distraction force
designed to restore disc height
optimized FitWhen expanded in the disc space, the implant
optimizes endplate-to-endplate fit
globus Medical’s expandable technology has been designed with the following features and benefits which allow for restoration of sagittal balance and optimal fit.
Visit us at booth #10

DEAR COLLEAGUES,
Welcome to the North American Spine Society’s 2nd Annual Summer Spine Meeting, featuring a dynamic educational program that addresses some of the most pressing issues in spine care today. We hope you will find the informal and relaxed setting of the meeting the perfect forum to participate in open discussions and debates about the latest in spine care.
This year’s Summer Spine Meeting features symposia addressing cervical and thoracolumbar deformity, biologics, lumbar surgery complications and management, intraoperative pearls from the experts, and the evolution of healthcare. Technique workshops cover minimally invasive surgery and deformity correction. Open discussions address a wide range of topics including perioperative care of the deformity correction surgical patient and identifying the pain generator. Exhibiting companies demonstrate the latest spine care products and services.
We hope you take time this week to relax and enjoy the many amenities and recreational activities at the Omni Plantation Resort, as well as Amelia Island’s numerous sights and attractions, including world class dining, shopping, art and nightlife.
The NASS Summer Spine Meeting is a very different kind of meeting, designed for you to participate and collaborate with colleagues and the field’s leading experts to gain the skills needed for your patients and to help shape the future of spine care. Thank you for joining us in Amelia Island, and may your meeting experience this week be both rewarding and productive.
ACKNOWLEDGEMENTS
Summer Spine Meeting Program CommitteeJeffrey C. Wang, MD, Overall Chairman Michael L. Reed, DPT, OCS, Meeting ChairmanThomas E. Mroz, MD, Meeting Co-chairmanRoger Härtl, MDRaj D. Rao, MDJoshua D. Rittenberg, MDAlan Villavicencio, MD
Summer Spine Meeting Scientific Program ReviewersNASS thanks the following volunteers who spent numerous hours reviewing abstracts. Roger Härtl, MDEric O. Klineberg, MDThomas E. Mroz, MDMichael L. Reed, DPT, OCSJoshua D. Rittenberg, MDAlok D. Sharan, MDMatthew Smuck, MDJeffrey C. Wang, MD
TABLE OF CONTENTSMeeting Information . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4Resort Information . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6Meeting-at-a-Glance . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8Wednesday, July 23/Thursday, July 24 . . . . . . . . . . . . . . .10 Friday, July 25. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14Saturday, July 26 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18Electronic Posters . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21ePoster Proceedings . . . . . . . . . . . . . . . . . . . . . . . . . . . . .25Author Index/Subject Index . . . . . . . . . . . . . . . . . . . . . . . 41Disclosure Index . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .42Technical Exhibition . . . . . . . . . . . . . . . . . . . . . . . . . . . . 46NASS Membership . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 48
WELCOME TO THE NASS SUMMER SPINE MEETING
Jeffrey C. Wang, MDOverall Chairman
Michael L. Reed, DPT, OCSMeeting Chairman
Thomas E. Mroz, MDMeeting Co-chairman
AMELIA ISLAND, FL / JULY 23-26SUMMER SPINE

LEARNING OBJECTIVESUpon completion of this conference, participants will gain strategies to:• Promote discussion of new scientific developments and
best practices within spine care organizations;• Demonstrate the application of current techniques,
procedures and research;• Practice evidence- and value-based medicine relative
to spine care;• Exchange ideas with experts and peers from around the
globe to strengthen professional relationships.
ABOUT NASSThe North American Spine Society (NASS) is a multidisciplinary organization with over 8,000 members in North America and abroad. The membership consists of orthopedic surgeons, neurosurgeons, physiatrists and other specialists involved in spine care.
The leading multidisciplinary organization in the field of spinal disorders, NASS’ mission is to foster the delivery of quality spine care.
SESSION RECORDINGS ON DEMAND Visit https://www.spine.org/SummerOnDemand to purchase the conference session recordings and get 24/7 access to scientific presentations. This recording includes scientific abstract ePosters and symposia. These web-based, fully synchronized audio, video and slide presentations are available anywhere you can access the internet.
CONTINUING MEDICAL EDUCATION (CME) CREDITThis activity has been planned and implemented in accordance with the Essentials and Standards of the Accreditation Council for Continuing Medical Education (ACCME). The North American Spine Society is accredited by the ACCME to provide continuing medical education for physicians and takes responsibility for the content, quality and scientific integrity of this CME activity.
The North American Spine Society designates this live activity for a maximum of 17.75 AMA PRA Category 1 Credits™. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
The American Medical Association has determined that physicians not licensed in the U.S. to participate in this CME activity are eligible for AMA PRA Category 1 Credits™.
The American Academy of Physician Assistants (AAPA) accepts Category 1 credit from AOACCME, prescribed credit from the American Academy of Family Physicians (AAFP) and AMA PRA Category 1 CME Credit™ for the Physician’s Recognition Award from organizations, such as NASS, accredited by the ACCME.
Each state has different requirements for nurses, physical therapists and other medical providers; contact your credit granting organization for their requirements.
CME CERTIFICATESVisit www.spine.org/myaccount to claim education credit and print your CME certificate. For questions, contact [email protected].
SPEAKER INFORMATION CENTERSymposia, technique workshop and breakout session presenters can upload their presentations by visiting the Speaker Information Center located in the Magnolia Foyer, in the Registration Area.
Mac users must convert presentations to PowerPoint. Speakers are not permitted to use their own laptops for their presentations. NO exceptions will be made.
Speaker Information Center hours:Wednesday, July 23 2:00–6:00 p.m.Thursday, July 24 6:30 a.m.–1:00 p.m. Friday, July 25 6:30 a.m.–1:00 p.m. Saturday, July 26 6:30 a.m.–1:00 p.m.
MEETINGINFORMATION
N A S S S U M M E R S P I N E M E E T I N G
Don’t miss your opportunity to save $100 by using promo code 1QA2G.
Valid until 11/30/14
4

CORPORATE SUPPORT ACKNOWLEDGEMENTNASS thanks the following companies for their generous support of the Minimally Invasive Spine Surgery and Deformity Correction technique workshops.
Biomet SpineDePuy Synthes SpineGlobus MedicalImplanet
MEETING INFORMATION
5
WINE AND CHEESE OPENING RECEPTIONThe Wine and Cheese Opening Reception marks the official start of the 2014 Summer Spine Meeting on Wednesday, July 23, from 7:00–8:30 p.m. at Walker’s Landing at the Omni Amelia Island. Shuttles are available to take meeting attendees and their families to the reception. This is an opportunity to see familiar faces and meet new colleagues.
LANDMARKS 1 Hotel Lobby
16 Real Estate
20 Plantation Chapel
MEETING SPACE 8 Azalea Room
9 Hibiscus Room
11 Live Oak Room
13 Oceanview Room & Terrace
RESTAURANTS 2 Seaglass
6 Oceanside
14 Sunrise Café
19 Falcon’s Nest
23 Natural Slice
24 Marché Burette
25 PLAE
RECREATION & ACTIVITIES 3 Camp Amelia
4 Pools
5 Beach Shoppe
7 Towel Hut
10 Gamers
12 Hotel Fitness Center
15 Nature Center
17 Heron’s Cove Adventure Golf
18 Canopy Park
21 Amelia’s Wheels
22 The Spa & Salon
MAP ICONS INDICATE: Roadways
Pedestrian Walkway
Parking Lots
Elevator
Ocean/Intracoastal
Beach Access
Fishing Area
Orange trams loop every 15 minutes to Hotel, Falcon’s Nest, Spa, Shops & Conference Center
Additional blue trams available upon requests to golf, tennis & villas
ATLANTIC OCEAN
VILLAS>SandcastlesII
SandcastlesI
< VILLAS
Main Entrance
Conference
Center
Garage
Breezeway
Sunrise Wing
OceansideWing
1ST COAST HWY
1ST COAST HWY
A1A
A1A
Beach Wood Rd
Boxwood Ln
Beach Walker Rd
Beach Walker R
d
Dunes Row
Sea Marsh Rd
Marsh
Haw
k R
d
SHOPS
SecurityGate
AuryIsland
Playground
MagnoliaGarden
23 Har-Tru®Tennis Courts
LandmarkOakWillow
Conservancy
MAINENTRANCE
SHOPSENTRANCE27
23
19
1516
1 2
6
43
5
714
17
182021
2225
22
23
24
25
24
26
13
1011
12
9 8
904-261-6161 weeklyresortguide.com
RESORT MAP

GOLF Oak Marsh Golf Course Designed by Pete Dye, this 6,500-yard course will challenge even the most avid golfers. Meandering through native marshlands and Amelia Island’s signature live oaks, each hole presents some unique challenges, whether it’s one of 14 water hazards or numerous bulk-headed greens. A perfect blend of beauty and challenge, Oak Marsh can easily be considered Amelia Island’s toughest par 72 layout. Open daily 7:00 a.m.–7:00 p.m. Ocean Links Golf Course Renowned golf architects, Pete Dye and Bobby Weed collaborated to design this truly picturesque course. With five holes running directly parallel to the Atlantic shoreline, Ocean Links not only offers breathtaking views, but challenging play as well. Featuring narrow fairways and perpetually shifting coastal winds, the course demands stern concentration and pinpoint accuracy. At par 70, this 6,200-yard course also features ten holes that wander through coastal lagoons and marsh wetlands. Open daily 7:00 a.m.–7:00 p.m.
Long Point Golf Course The Amelia Island Club member course offers exclusive access to the Omni Amelia Island Plantation guests. Rolling through lush marshland and along the dunes of the ocean, the Tom Fazio layout stretches across 6,775 yards. Undulating fairways and large elevated greens present distinctive views and challenges on this par 72 layout. Golfers will encounter native marshlands and water on 12 holes, as well as Tiff Eagle putting surfaces that are known for their fast playing conditions. Open daily 7:00 a.m.–7:00 p.m.
Rental ClubsThe resort offers TaylorMade R1 and Rocketballz Stage 2 rentals at Oak Marsh and Ocean Links for $65 and $40 respectively. Rental clubs are free after 2:00 p.m.
TENNIS
Cliff Drysdale Tennis The Omni Amelia Island Plantation is a world-renowned tennis resort hosting the greatest players of all-time beneath its canopied live oaks. The Racquet Park offers guests 23 Har-Tru® clay courts in a distinctive setting, ranked as the No. 2 tennis resort on Florida’s East Coast by Tennis Magazine. The Cliff Drysdale Tennis program offers the “Ultimate Tennis Experience” in one of the world’s truly amazing locations to play tennis. Our programs operate year round and cater to the full spectrum of tennis players, for individuals, couples, families, and team groups, our comprehensive adult and junior options have everyone’s game covered.
SPA
Miles From Stress, Footsteps From The Sea An alluring hideaway tucked beneath the grand Florida oaks, guests are instantly transformed into a state of relaxation upon entering the full-service luxury spa inspired by nature. Offering floor-to-ceiling windows, the spa lounge overlooks the private gardens and glassy lake surrounding the nature-inspired spa. The spa offers an array of pampering treatments from Swedish Massages and Aromatherapy Massages to Pampered Soles Pedicures, Soft Palms Manicures and a full service hair salon.
RESORTINFORMATION
N A S S S U M M E R S P I N E M E E T I N G
6

DINING
Falcon’s Nest An aviation-themed pub offering a full bar, unique appetizers and a build-your-own-burger menu. Marché Burette Gourmet food market and deli offering a full breakfast, lunch and dinner, specialty sandwiches and salads, along with homemade gelato, ice cream, and specialty desserts. Marsh View Bar & Grill Enjoy breakfast, lunch, or libations indoors or on the outdoor terrace while overlooking spectacular golf courses and marsh views. Natural Slice Pizza & Surf Shop A surf-inspired pizza joint serving fresh ingredients on our signature saltwater crust. Oceanside Offering views of the Atlantic Ocean and overlooking a multi-tiered pool area, Oceanside is flip-flop friendly during the day and serves a specialty dinner menu in the evening. Rum + Tequila Experience Partake in the Rum + Tequila Experience, our newest poolside bar. From Blancos to Reposados to Anejos and Platinum varieties, the resort has more than 100 different types of rum and tequila to choose from, in addition to five signature margaritas and delicious cocktails. Seaglass Located directly off the lobby overlooking the Atlantic, Seaglass offers hand-crafted cocktails and a selection of small plate specialties. Gather indoors or on the terrace around multiple fire and water features. Sunrise Café Sunrise Café offers stunning views of the Atlantic and Ocean Links Golf Course, and features the “Art of Breakfast” and a southern inspired dinner menu indoors or al fresco on the terrace. Verandah Throughout the years, Verandah has established itself as one of Amelia Island’s finest restaurants. Enjoy fresh, traditional seafood along with an extensive yet approachable wine list. Delivering the flavors of the local Atlantic Ocean and neighboring farmers directly to your plate, our chefs’ dedication to the finest local ingredients guarantees that what’s fresh is what’s for dinner.
RESORT INFORMATION Marché Burette
Oceanside
Rum + Tequila Experience
Falcon’s Nest
77

THURSDAY, JULY 24
6:30–7:15 a.m. BreakfastMagnolia Ballroom D-G
6:30 a.m.–12:00 p.m.
Technical ExhibitionePoster KiosksMagnolia Ballroom D-G
6:30 a.m.–1:00 p.m.
RegistrationSpeaker Information CenterMagnolia Foyer
7:15–7:30 a.m. Opening RemarksMagnolia Ballroom A-C
7:30–9:00 a.m. Symposium: Thoracolumbar Deformity and ManagementMagnolia Ballroom A-C
9:00–10:00 a.m. Symposium: Cervical Deformity and ManagementMagnolia Ballroom A-C
10:00–10:30 a.m. BreakTechnical Exhibition Magnolia Ballroom D-G
10:30–11:30 a.m. Symposium: Occipital Cervical Junction Surgery Magnolia Ballroom A-C
11:30 a.m.–12:00 p.m.
BreakTechnical Exhibition Magnolia Ballroom D-G
12:00–1:00 p.m. Symposium: Cervical Surgery Complications and ManagementMagnolia Ballroom A-C
1:00–2:00 p.m. Lunch on Own
2:00–4:00 p.m. Breakout Session: Perioperative Care of the Deformity Correction Surgical Patient: MultidisciplinaryCumberland Ballroom C
2:00–6:00 p.m. Technique Workshop: Deformity Correction Requires additional registration feeCumberland Ballroom A
WEDNESDAY, JULY 23
2:00–6:00 p.m. Registration Speaker Information CenterMagnolia Foyer
7:00–8:30 p.m. Opening Wine and Cheese ReceptionWalker’s Landing, Omni Amelia Island
MEETING-AT-A-GLANCE
N A S S S U M M E R S P I N E M E E T I N G
8
Meeting takes place in the conference center.
DISCLAIMERThe material presented at the Summer Spine Meeting is made available by the North American Spine Society for educational purposes only. The material is not intended to represent the only, nor necessarily the best, method or procedure appropriate for the medical situations discussed; rather, it is intended to present an approach, view, statement or opinion of the faculty which may be helpful to others who face similar situations. NASS disclaims any and all liability for injury or other damages to any individual attending the meeting and for all claims which may arise out of the use of the techniques demonstrated therein by such individuals, whether these claims shall be asserted by physicians or any other person.
On occasion, changes in the program content or faculty may occur after the preliminary brochure has been distributed. This Final Program contains confirmed program content, faculty and presenters. Any further changes from the published Final Program are announced at the beginning of the session.

FRIDAY, JULY 25
6:30-7:25 a.m. Breakfast Magnolia Ballroom D-G
6:30 a.m.–12:00 p.m.
Technical Exhibition ePoster Kiosks Magnolia Ballroom D-G
6:30 a.m.–1:00 p.m.
RegistrationSpeaker Information CenterMagnolia Foyer
7:25–7:30 a.m. Opening RemarksMagnolia Ballroom A-C
7:30–9:00 a.m. Symposium: Lumbar Surgery Complications and ManagementMagnolia Ballroom A-C
9:00–10:00 a.m. Symposium: Evolution of HealthcareMagnolia Ballroom A-C
10:00–10:30 a.m. BreakTechnical Exhibition Magnolia Ballroom D-G
10:30–11:30 a.m. Symposium: Utility of Diagnostic and Therapeutic InjectionsMagnolia Ballroom A-C
11:30 a.m.–12:00 p.m.
BreakTechnical Exhibition Magnolia Ballroom D-G
12:00–1:00 p.m. Symposium: Minimally Invasive Spine SurgeryMagnolia Ballroom A-C
1:00–2:00 p.m. Lunch on Own
2:00–4:00 p.m. Breakout: Identifying the Pain Generator and Pain Management Strategies Cumberland Ballroom C
2:00–6:00 p.m. Technique Workshop: Minimally Invasive Spine Surgery Requires additional registration feeCumberland Ballroom A
SATURDAY, JULY 26
6:30–7:25 a.m. Breakfast Magnolia Ballroom D-G
6:30–10:00 a.m. Technical Exhibition ePoster Kiosks Magnolia Ballroom D-G
6:30 a.m.–1:00 p.m.
RegistrationSpeaker Information CenterMagnolia Foyer
7:25–7:30 a.m. Opening RemarksMagnolia Ballroom A-C
7:30–8:30 a.m. Symposium: Trauma ControversiesMagnolia Ballroom A-C
8:30–9:30 a.m. Symposium: My Worst Case Ever: Lessons LearnedMagnolia Ballroom A-C
9:30–10:00 a.m. BreakTechnical ExhibitionMagnolia Ballroom D-G
10:00 a.m. Technical Exhibition Closed
10:00–11:30 a.m. Symposium: Biologics in Spine Care: Present Options and Future PossibilitiesMagnolia Ballroom A-C
11:30–11:45 a.m. BreakMagnolia Foyer
11:45 a.m.–1:00 p.m.
Symposium: Intraoperative Pearls from the Experts: ExperiencedTricks of the Trade Magnolia Ballroom A-C
1:00 p.m. Meeting Adjourns
MEETING-AT-A-GLANCE
9

WEDNESDAY, JULY 23
2:00–6:00 p.m.
Registration Speaker Information Center OpenMagnolia Foyer
7:00–8:30 p.m.
Opening Wine and Cheese ReceptionWalker’s Landing, Omni Amelia Island
THURSDAY, JULY 24
6:30–7:15 a.m.
BreakfastMagnolia Ballroom D-G
6:30 a.m.–12:00 p.m.
Technical ExhibitionePoster KiosksMagnolia Ballroom D-G
6:30 a.m.–1:00 p.m.
RegistrationSpeaker Information CenterMagnolia Foyer
7:15–7:30 a.m.
Opening RemarksMagnolia Ballroom A-C
7:15–7:20 a.m.Michael L. Reed, DPT, OCS 7:20–7:25 a.m.William C. Watters III, MD 7:25–7:30 a.m.Thomas E. Mroz, MD
7:30–9:00 a.m.
Symposium: Thoracolumbar Deformity and ManagementMagnolia Ballroom A-C
Moderator: R. Douglas Orr, MD, FRCSC
This symposium focuses on strategies for managing thoracolumbar deformity. It begins with an understanding of how pelvic parameters guide treatment and strategies for addressing sagittal plane deformity. Proximal junctional kyphosis is a common complication of lumbar surgery and this session addresses the prevention and treatment of this condition. Lastly, the role of lateral interbody fusions in deformity surgery is explored.
Agenda
7:30–7:45 a.m.Assessing Sagittal Alignment and Decision MakingR. Douglas Orr, MD, FRCSC
7:45–8:00 a.m.Proximal Junctional KyphosisJohn G. DeVine, MD 8:00–8:15 a.m.Direct Lateral Approaches to Thoracolumbar Deformity: The Good, the Bad and the UglyTBD
8:15–9:00 a.m.Case Presentations Faculty Panel
FDA Device/Drug Status:R. Douglas Orr, MD, FRCSC: Lumbar and thoracic pedicle screws and
interbody cages—Approved. John G. DeVine, MD: Lumbar Total Disc Arthroplasty Devices—
Approved.TBD: Not available at time of printing.
WEDNESDAY, JULY 23 /THURSDAY, JULY 24
N A S S S U M M E R S P I N E M E E T I N G
10
Meeting takes place in the conference center.

9:00–10:00 a.m.
Symposium: Cervical Deformity and ManagementMagnolia Ballroom A-C
Moderator: Alpesh A. Patel, MD, FACS Our understanding and management of cervical deformity is changing rapidly. This symposium reviews the current evidence on cervical deformity, assesses critical clinical and radiographic parameters of cervical deformity, and provides guidance on incorporating this into clinical practice.
Agenda
9:00–9:05 a.m.Introduction and Case PresentationAlpesh A. Patel, MD, FACS
9:05–9:15 a.m.Clinical and Radiographic Assessment of Cervical DeformityAjit A. Krishnaney, MD 9:15–9:35 a.m.Deformity Correction Options: Rationale and OptionsTimothy Moore, MD
9:35–10:00 a.m.CasesAlpesh A. Patel, MD, FACS and Faculty Panel
FDA Device/Drug Status:Alpesh A. Patel, MD, FACS: Posterior cervical instrumentation—Not
Approved. Ajit A. Krishnaney, MD: This presentation does not discuss or include
any applicable devices or drugs. Timothy Moore, MD: Posterior cervical lateral mass screws—Not
Approved.
10:00–10:30 a.m.
Break/Technical Exhibition Magnolia Ballroom D-G
10:30–11:30 a.m.
Symposium: Occipital Cervical Junction SurgeryMagnolia Ballroom A-C
Moderator: Alan Villavicencio, MD
This session consists of a series of interactive presentations describing the anatomy, etiology, diagnosis and surgical treatment of craniocervical ( junction) abnormalities. The latest advancements and surgical treatment considerations are discussed and presented didactically and with case examples. Participants should be able to discuss typical issues and recommendations specific to disorders involving the craniocervical junction and describe surgical treatments that are available for the management of patients with such problems.
Agenda
10:30–10:45 a.m.Occipital Anatomy and Fixation: Pearls and PitfallsAjit A. Krishnaney, MD
10:45–11:00 a.m.C1-2 Fusion: Indications and Technique OptionsSaad B. Chaudhary, MD, MBA
11:00–11:15 a.m.Basilar Invagination: Pre-op Considerations and TechniquesDaniel J. Hoh, MD
11:15–11:30 a.m.Case ResolutionAlan Villavicencio, MD
FDA Device/Drug Status:Alan Villavicencio, MD: This presentation does not discuss or include
any applicable devices or drugs.Ajit A. Krishnaney, MD: This presentation does not discuss or include
any applicable devices or drugs. Saad B. Chaudhary, MD, MBA: Cervical 1 lateral mass fixation and
Cervical 2 pedicle fixation/laminar fixation—Approval pending for Class II for Cervical sessions.
Daniel J. Hoh, MD: This presentation does not discuss or include any applicable devices or drugs.
11:30 a.m.–12:00 p.m.
BreakTechnical Exhibition Magnolia Ballroom D-G
THURSDAY, JULY 24
11

12:00–1:00 p.m.
Symposium: Cervical Surgery Complications and ManagementMagnolia Ballroom A-C
Moderator: Ajit A. Krishnaney, MD
Although complications in cervical spine surgery are rare, when they do occur they can have devastating consequences. Cervical complication avoidance, recognition and management strategies are discussed.
Agenda
12:00–12:15 p.m.Vertebral Artery Injuries: Risks, Treatment and Work-upAlpesh A. Patel, MD, FACS
12:15–12:25 p.m.Ventral DurotomiesWarren Yu, MD
12:25–12:40 p.m.Failed Cervical Arthroplasty Saad B. Chaudhary, MD, MBA
12:40–1:00 p.m.Case DiscussionFaculty Panel
FDA Device/Drug Status:Alpesh Patel, MD, FACS: Posterior cervical instrumentation—Not
Approved. Warren Yu, MD: Not available at time of printing. Saad B. Chaudhary, MD, MBA: Cervical 1 lateral mass fixation and
Cervical 2 pedicle fixation/laminar fixation—Approval pending for Class II for Cervical sessions.
1:00–2:00 p.m.
Lunch on Own
2:00–4:00 p.m.
Breakout Session: Perioperative Care of the Deformity Correction Surgical Patient: MultidisciplinaryCumberland Ballroom C
Moderator: Michael L. Reed, DPT, OCS Securing optimal surgical outcomes in the management of patients with deformity-related spinal disorders demands a complex array of multidisciplinary interactions and efforts. Systematically developing a process that includes multidisciplinary support and clearly defining anticipated success could dramatically improve efficiencies, enrich results, drive down costs, and improve satisfaction for everyone. This breakout session is designed to benefit all spine-related disciplines and professionals. Attendees are introduced to a number of interdisciplinary considerations relative to optimizing spine deformity correction outcomes.
Agenda
2:00–2:05 p.m.Introduction Michael L. Reed, DPT, OCS
2:05–2:20 p.m.Psychosocial ConsiderationsDaniel J. Mazanec, MD
2:20–2:35 p.m.Considerations Related to Imaging DataJohn McIntyre, MD
2:35–2:50 p.m.Medical Management and Comorbidity ConsiderationsChristopher Reudink, PA-C
2:50–3:00 p.m.Preoperative Education and Conditioning Michael L. Reed, DPT, OCS
3:00–3:10 p.m.Interventional Pain ManagementE. Kano Mayer, MD
3:10–3:20 p.m.PharmacologyDaniel J. Mazanec, MD
3:20–3:35 p.m.Post-Surgical Rehabilitation Michael L. Reed, DPT, OCS
3:35–3:45 p.m.Biometric Data and ApplicationsMichael L. Reed, DPT, OCSE. Kano Mayer, MD
THURSDAY, JULY 24
12

3:45–4:00 p.m.DiscussionFaculty Panel FDA Device/Drug Status:Michael L. Reed, DPT, OCS: This presentation does not discuss or
include any applicable devices or drugs.Daniel J. Mazanec, MD: Gabapentin, Pregabalin, Ricyclic
antidepressants, Venlafaxine—Investigational. John McIntyre, MD: This presentation does not discuss or include any
applicable devices or drugs. Christopher Reudink, PA-C: Not available at time of printing. E. Kano Mayer, MD: Not available at time of printing.
2:00–6:00 p.m.
Technique Workshop: Deformity CorrectionCumberland Ballroom A
Course Chairman: R. Douglas Orr, MD, FRCSC
This workshop focuses on didactic discussions including: sagittal and coronal balance, clinical applications of pelvic parameters, osteotomy techniques, illiolumbar fixation techniques and anatomy techniques utilizing thoracic pedicle screws. Through expert lectures, moderated case discussions and hands-on practice on sawbones, spinal surgeons will gain practical knowledge and technical skills to improve the care they provide to their spinal deformity patients.
Agenda
2:00 p.m. Welcome and Introduction R. Douglas Orr, MD, FRCSC 2:05–2:20 Sagittal and Coronal BalanceR. Douglas Orr, MD, FRCSC 2:20–2:35 Pelvic Parameters: Clinical ApplicationsTBD 2:35–2:50 Iliolumbar Fixation TechniquesYu-Po Lee, MD
2:50–3:00 Thoracic Pedicle Screws: Anatomy and TechniquesSaad B. Chaudhary, MD, MBA
THURSDAY, JULY 24
Requires additional registration fee
3:00–3:15 Break
3:15–3:30 Smith-Petersen/Ponte Osteotomies: Technique and CasesNorman B. Chutkan, MD
3:30–3:45 Pedicle Subtraction Osteotomy (PSO): Technique and CasesNorman B. Chutkan, MD
3:45–4:00 Vertebral Column Resection (VCR): Technique and CasesTBD
4:00–6:00 Hands-on Sawbones Lab 6:00 p.m. Course Adjourns
13

FRIDAY, JULY 25
6:30–7:25 a.m.
Breakfast Magnolia Ballroom D-G
6:30 a.m.–12:00 p.m.
Technical Exhibition Open
ePoster Kiosks Magnolia Ballroom D-G
6:30 a.m.–1:00 p.m.
RegistrationSpeaker Information CenterMagnolia Foyer
7:25–7:30 a.m.
Opening RemarksMagnolia Ballroom A-CThomas E. Mroz, MD
7:30–9:00 a.m.
Symposium: Lumbar Surgery Complications and ManagementMagnolia Ballroom A-C
Moderator: William C. Watters III, MD This symposium discusses complications and management strategies for lumbar surgery procedures. Through case discussions and didactic lectures, the expert faculty illustrate the most common complications and how to manage them most effectively.
Agenda
7:30–7:45 a.m.Vascular Injuries with Anterior Surgery Stephen Tolhurst, MD
7:45–8:00 a.m.Failed Disc Arthroplasty Stephen Tolhurst, MD
8:00-8:15 a.m.Durotomies and Pseudomeningoceles Alan Villavicencio, MD
8:15–8:30 a.m.Cage Migration David T. Anderson, MD
8:30–9:00 a.m.Cases Faculty Panel
FDA Device/Drug Status:Stephen Tolhurst, MD: Not available at time of printing. Alan Villavicencio, MD: This presentation does not discuss or include
any applicable devices or drugs. David T. Anderson, MD: TLIF interbody cage device, lateral interbody
cage device, ALIF interbody cage device—Approved.
9:00-10:00 a.m.
Symposium: Evolution of HealthcareMagnolia Ballroom A-C
Moderator: Matthew J. McGirt, MD The unsustainable cost of healthcare and the Patient Protection and Affordable Care Act have introduced a number of value-based reform initiatives into healthcare. As spine care is among the most prevalent and expensive in healthcare, spine care providers are facing increasing demands to 1) prove the value of their services through quality data reporting, 2) adopt standardized, lean, best-evidence care pathways, and 3) participate in risk-sharing, bundled or capitated payment models. This session provides an overview of these topics and offers detailed examples of how spine care providers are adopting value-based care strategies.
Agenda
9:00–9:10 a.m.Evolution of Cost Containment in Spine Care: Risk Sharing Through Capitated, Bundled and Value-based PaymentMatthew J. McGirt, MD
9:10–9:25 a.m.Accurately Measuring Value in Surgical Spine Care: Application of the N2QOD Registry Anthony Asher, MD
FRIDAY, JULY 25
N A S S S U M M E R S P I N E M E E T I N G
14
Meeting takes place in the conference center.

9:25–9:40 a.m.Care Delivery, Reengineering and Risk Sharing Through Bundled Payment Paradigms: The Geisinger Health System Provencare® Lumbar Spine Program Jonathan Slotkin, MD
9:40–9:55 a.m.Use of a Standardized, Evidence-based Clinical Care Pathway to Reduce Utilization and Improve Efficiency in Low Back Care: The Saskatchewan Low-Back Pathway Adam S. Wu, MD 9:55–10:00 a.m.DiscussionFaculty Panel
FDA Device/Drug Status:Matthew J. McGirt, MD: This presentation does not discuss or include
any applicable devices or drugs.Anthony Asher, MD: This presentation does not discuss or include any
applicable devices or drugs. Jonathan Slotkin, MD: This presentation does not discuss or include
any applicable devices or drugs.Adam S. Wu, MD: Not available at time of printing.
10:00-10:30 a.m.
Break/Technical Exhibition Magnolia Ballroom D-G
10:30-11:30 a.m.
Symposium: Utility of Diagnostic and Therapeutic InjectionsMagnolia Ballroom A-C
Moderator: Matthew Smuck, MD
Cervical and lumbar foraminal injections are performed with diagnostic and therapeutic intentions. Due to safety concerns, the techniques have evolved in recent years. This symposium discusses the clinical utility of foraminal injections for both diagnostic and therapeutic purposes, reviews methods to maximize safety, and outlines predictors of therapeutic success.
Agenda
10:30–10:40 a.m.Cervical Transforaminal Epidural Steroid Injections: Utility and SafetyE. Kano Mayer, MD
10:40–10:50 a.m.Lumbar Transforaminal Epidural Steroid Injections: Therapeutic Utility and SafetyE. Kano Mayer, MD
10:50–11:05 a.m.Transforaminal Epidural Steroid Injection: Predictors of SuccessMatthew Smuck, MD
11:05–11:20 a.m.Cervical and Lumbar Selective Nerve Root Blocks: Diagnostic UtilityConor O’Neill, MD
11:10–11:30 a.m.Case PresentationsFaculty Panel
FDA Device/Drug Status:E. Kano Mayer, MD: Not available at time of printing. Matthew Smuck, MD: Local anesthetics—Approved; Corticosteroids—
Not Approved. Conor O’Neill, MD: Not available at time of printing.
11:30 a.m.–12:00 p.m.
BreakTechnical Exhibition Magnolia Ballroom D-G
12:00–1:00 p.m.
Symposium: Minimally Invasive Spine SurgeryMagnolia Ballroom A-C
Moderator: Michael P. Steinmetz, MD This session reviews basic and advanced techniques of minimally invasive surgery as currently applied to the cervical and lumbar spines. The microsurgical anatomy as well as surgical pearls are discussed for minimally invasive approaches for cervical and lumbar decompression, pedicle screw instrumentation, and interbody fusion.
Agenda
12:00–12:15 p.m.MIS Cervical ComplicationsMichael Y. Wang, MD, FACS
12:15–12:30 p.m.MIS Lumbar ComplicationsMichael P. Steinmetz, MD
FRIDAY, JULY 25
15

12:30–12:45 p.m.Pearls and Pitfalls of MIS DeformityPaul Park, MD
12:45–12:50 p.m.Debate: L4/5 Stenosis with Grade I SpondylolisthesisOpen TLIFMichael P. Steinmetz, MD 12:50–12:55 p.m.MIS TLIFMichael Y. Wang, MD, FACS FDA Device/Drug Status:Michael Y. Wang, MD, FACS: This presentation does not discuss or
include any applicable devices or drugs. Michael P. Steinmetz, MD: Lumbar pedicle screws, lumbar interbody
cages—Approved.Paul Park, MD: This presentation does not discuss or include any
applicable devices or drugs.
1:00–2:00 p.m.
Lunch on Own
2:00-4:00 p.m.
Breakout: Identifying the Pain Generator and Pain Management StrategiesCumberland Ballroom C
Moderator: Matthew Smuck, MD
Specialized spine care has increasingly focused on identifying and treating the pain generator. While many of the associated diagnostic tools and interventional techniques are now better defined, many have questioned the utility of this approach. This session highlights areas of controversy that stem from the pursuit of the pain generator, with opportunity for audience participation.
Agenda
2:00–2:20 p.m. Identifying Axial Pain on Physical ExaminationE. Kano Mayer, MD
2:20–2:40 p.m. Identifying Axial Pain on ImagingMatthew Smuck, MD
2:40–3:00 p.m. Invasive Pursuit of the Pain GeneratorConor O’Neill, MD
3:00–3:15 p.m. Panel and Audience DiscussionFaculty Panel
3:15–3:30 p.m. Medial Branch Blocks: ProE. Kano Mayer, MD
3:30–3:45 p.m. Medial Branch Blocks: ConConor O’Neill, MD
3:45–4:00 p.m. Panel and Audience DiscussionFaculty Panel
FDA Device/Drug Status:E. Kano Mayer, MD: Not available at time of printing. Matthew Smuck, MD: Local anesthetics—Approved; Corticosteroids—
Not Approved. Conor O’Neill, MD: Not available at time of printing.
2:00-6:00 p.m.
Technique Workshop: Minimally Invasive Spine Surgery Cumberland Ballroom A
Course Chairman: Michael Y. Wang, MD, FACS
This workshop provides an overview of new and less invasive techniques for the operative treatment of spinal disorders. Experts in minimally invasive surgery (MIS) discuss the pros and cons of MIS approaches, establishing the skills essential in selecting appropriate patients and pathologies for MIS surgery. Practical sessions allow the participant to apply some of the latest spinal techniques including spinal navigation. Participants have an opportunity to discuss difficult cases with the faculty during the panel discussion.
Agenda
2:00 p.m. Welcome and Introduction Michael Y. Wang, MD, FACS 2:05–2:20 p.m. MIS Decompression Procedures in the Lumbar Spine: Rationale and Current TechniquesSheeraz Qureshi, MD 2:20–2:35 p.m. Lateral Transpsoas ApproachDean Chou, MD 2:35–2:50 p.m. Spinal Endoscopic ProceduresFarhan Siddiqi, MD
FRIDAY, JULY 25
Requires additional registration fee
16

2:50–3:00 p.m. Spinal 3D Navigation in MIS SurgeryDaniel J. Hoh, MD
3:00–3:15 p.m. Break
3:15–3:30 p.m. Cervical MIS: Foraminotomies and LaminectomiesThomas E. Mroz, MD
3:30–3:45 p.m. MIS TLIF: Evolution and EvidenceDaniel J. Hoh, MD
3:45–4:00 p.m. Update on Evidence for MIS Treatment of Spinal DeformityPaul Park, MD
4:15–4:30 p.m. MIS: Cost, Outcomes, and ComplicationsMichael P. Steinmetz, MD
4:30–5:00 p.m. Challenging MIS CasesMichael Y. Wang, MD, FACS
5:00–6:00 p.m. Hands-on Practice on Sawbones Lab 6:00 p.m. Course Adjourns
FRIDAY, JULY 25
17

SATURDAY, JULY 26
6:30–7:25 a.m.
Breakfast Magnolia Ballroom D-G
6:30–10:00 a.m.
Technical Exhibition ePoster Kiosks Magnolia Ballroom D-G
6:30 a.m.–1:00 p.m.
RegistrationSpeaker Information CenterMagnolia Foyer 7:25-7:30 a.m.
Opening RemarksMagnolia Ballroom A-CMichael L. Reed, DPT, OCS
7:30–8:30 a.m.
Symposium: Trauma ControversiesMagnolia Ballroom A-C
Moderator: Timothy Moore, MD
This symposium focuses on two cases that are very controversial in terms of treatment. The first case is geriatric odontoid fractures and the second case is thoracolumbar burst fractures. There is no consensus on optimal treatment of these injuries and the supporting details of nonoperative and operative treatments are discussed.
Agenda
Debate 1: Geriatric Odontoid Fracture
7:30–7:40 a.m.Operate Sheeraz Qureshi, MD
7:40–7:50 a.m.Don’t OperateAdam S. Wu, MD 7:50–8:00 a.m. Case ResolutionFaculty Panel
Debate 2: Thoracolumbar Burst Fracture: Neurologically Intact
8:00–8:10 a.m.Operate Farhan Siddiqi, MD
8:10–8:20 a.m. Don’t Operate Warren Yu, MD
8:20–8:30 a.m. Case ResolutionFaculty Panel FDA Device/Drug Status:Sheeraz Qureshi, MD: This presentation does not discuss or include any
applicable devices or drugs.Adam S. Wu, MD: Not available at time of printing. John McIntyre, MD: This presentation does not discuss or include any
applicable devices or drugs. Farhan Siddiqi, MD: Globus RISE—Approved.Warren Yu, MD: This presentation does not discuss or include any
applicable devices or drugs.
8:30–9:30 a.m.
Symposium: My Worst Case Ever: Lessons LearnedMagnolia Ballroom A-C
Moderator: William C. Watters, III, MD
Every surgeon has challenging cases and even a worst case or two, but learning from the challenge is paramount. This interactive session features four surgeons sharing their worst case, why it was their worst case and the outcomes. Through discussion and audience participation, the faculty impart pearls and tips.
Agenda
8:30–8:45 a.m.Transthoracic Discectomy Complicated by CSF Leak and Cranial Subdural HematomaAlan Villavicencio, MD
8:45–9:00 a.m.T11-12 Fracture Dislocation Above an L4 Burst FractureTimothy Moore, MD
SATURDAY, JULY 26
N A S S S U M M E R S P I N E M E E T I N G
18
Meeting takes place in the conference center.

9:00–9:15 a.m. Minimally Invasive TLIFJohn Shin, MD
9:15–9:30 a.m.Minimally Invasive Lateral Thoracic Spine Corpectomy for Osteomyelitis with Contralateral Segmental Artery Injury Deb Bhowmick, MD FDA Device/Drug Status:Alan Villavicencio, MD: This presentation does not discuss or include
any applicable devices or drugs. Timothy Moore, MD: This presentation does not discuss or include any
applicable devices or drugs. John Shin, MD: This presentation does not discuss or include any
applicable devices or drugs. Deb Bhowmick, MD: This presentation does not discuss or include any
applicable devices or drugs.
9:30–10:00 a.m.
BreakTechnical ExhibitionMagnolia Ballroom D-G
10:00 a.m.
Technical Exhibition Closed
10:00–11:30 a.m.
Symposium: Biologics in Spine Care: Present Options and Future PossibilitiesMagnolia Ballroom A-C
Moderator: Thomas E. Mroz, MD This symposium addresses a multitude of biologic options available to spine surgeons. These include an overview of the state of the art in biologics, demineralized bone matrices, platelet-rich plasma, allograft cells, and the many facets of bone morphogenetic protein-2. At the end of the session, participants will have the tools to assess the biologics options that exist for spine fusion, the indications for their use, and evidence for their use.
Agenda
10:00–10:05 a.m.Introduction Thomas E. Mroz, MD 10:05–10:20 a.m. Demineralized Bone Matrix: Options and Evidence Alpesh A. Patel, MD, FACS
10:20–10:35 a.m.Allograft Cells in Spine Surgery Michael P. Steinmetz, MD
10:35–10:50 a.m.Platelet Rich Plasma in Spine Surgery Clinton J. Devin, MD
10:50–11:10 a.m.BMP-2: Indications, Evidence, Complications John G. DeVine, MD
11:10–11:20 a.m.BMP-2: Legal Risks Thomas E. Mroz, MD
11:20–11:30 a.m.Cases: BMP Complications Faculty Panel
FDA Device/Drug Status:Alpesh A. Patel, MD, FACS: This presentation does not discuss or
include any applicable devices or drugs. Michael P. Steinmetz, MD: Not available at time of printing. Clinton Devin, MD: Not available at time of printing. John G. DeVine, MD: This presentation does not discuss or include any
applicable devices or drugs.Thomas E. Mroz, MD: BMP-2—Not Approved.
11:30-11:45 a.m.
Break
11:45 a.m.–1:00 p.m.
Symposium: Intraoperative Pearls from the Experts: Experienced Tricks of the Trade Magnolia Ballroom A-C
Moderator: Warren Yu, MD
Intraoperative challenges face all spine surgeons during basic and complex procedures. Learn pearls and pitfalls from experienced surgeons on MIS surgery, deformity surgery, extracavitary approaches, and metastatic spine surgery.
Agenda
11:45–11:55 a.m.C1-2 Fusion: Bleeding and Dealing with the C2 RootMatthew J. McGirt, MD
11:55 a.m.–12:05 p.m.Deformity Correction in the Face of Significant Blood Loss/Instability R. Douglas Orr, MD, FRCSC
SATURDAY, JULY 26
19

12:05–12:25 p.m.Costotransversectomy and Extracavitary Approach: Pearls and PitfallsDeb Bhowmick, MD
12:25–12:45 p.m.Surgery for Vascular Metastatic Lesions: Pearls and PitfallsJohn Shin, MD
12:45–1:00 p.m.DiscussionFaculty Panel
FDA Device/Drug Status:Matthew J. McGirt, MD: This presentation does not discuss or include
any applicable devices or drugs.R. Douglas Orr, MD, FRCSC: Not available at time of printing. Deb Bhowmick, MD: This presentation does not discuss or include any
applicable devices or drugs.John Shin, MD: This presentation does not discuss or include any
applicable devices or drugs.
1:00 p.m.
Meeting Adjourns
SATURDAY, JULY 26
20

ELECTRONICPOSTERS
N A S S S U M M E R S P I N E M E E T I N G
Located in Magnolia Ballroom D-G
ePoster Kiosk hours:Thursday, July 24 6:30 a.m.–12:00 p.m. Friday, July 25 6:30 a.m–12:00 p.m. Saturday, July 26 6:30–10:00 a.m.
P1. A Novel Measurement of Postoperative Axial Plane Rotation in Adolescent Idiopathic Scoliosis Using Plain Radiographs
Benjamin T. Bjerke-Kroll, MD, MS1; Grant D. Shifflett1; Sravisht Iyer2; Zoe Cheung1; Peter D. Fabricant, MD1; Han Jo Kim, MD1
1Hospital for Special Surgery, New York, NY, US; 2Cambridge, MA, US
FDA DEVICE/DRUG STATUS: This abstract does not discuss or include any applicable devices or drugs.
P2. Assessment of Vertebral Curves Using the Manual Post-It® Technique
Benjamin T. Bjerke-Kroll, MD, MS; Brian P. Gladnick; Joseph Schreiber, MD; Grant D. Shifflett; Matthew E. Cunningham, MD, PhD
Hospital for Special Surgery, New York, NY, US
FDA DEVICE/DRUG STATUS: This abstract does not discuss or include any applicable devices or drugs.
P3. Hypertrophy and Fibrosis of the Ligamentum Flavum in Lumbar Spinal Stenosis is Associated with Increased Expression of LPA and LPAR1
Kai Zhang
Shanghai Jiao Tong University School of Medicine, Shang Hai, China
FDA DEVICE/DRUG STATUS: This abstract does not discuss or include any applicable devices or drugs.
P4. Kyphoplasty Using Temperature Gradient Injection Technique for the Treatment of Osteoporotic Vertebral Compression Fractures
Tao Liu, MD, PhD
The First Affiliated Hospital of Soochow University, Suzhou, China
FDA DEVICE/DRUG STATUS: This abstract does not discuss or include any applicable devices or drugs.
P5. The Diagnostic Value of MRI, CT, PET, Bone Scintigraphy (BS) and BS with SPECT (SPECT) in Detecting Vertebral Metastases
Tao Liu, MD, PhD
The First Affiliated Hospital of Soochow University, Suzhou, China
FDA DEVICE/DRUG STATUS: This abstract does not discuss or include any applicable devices or drugs.
P6. Vertebral Column Manipulation: A New Corrective Technique for Idiopathic Scoliosis for Three-Dimensional (3D) Correction: A Retrospective Study Based on the Two-Years Follow-Up
Pawel Grabala, MD; Robert Budkiewicz, MD, PhD; Dariusz Kossakowski, MD, PhD
Regional Specialist Children’s Hospital, Department of Pediatric Orthopaedic and Trauma Surgery, Olsztyn, Poland
FDA DEVICE/DRUG STATUS: This abstract does not discuss or include any applicable devices or drugs.
P7. Extreme Lateral Lumbar Interbody Fusion Using Osteocel Plus: 20-Month Outcome
Karthik Madhavan, MD1; Steven Vanni, DO, DC2
1Miami, FL, US; 2Lois Pope Life Center, Miami, FL, US
FDA DEVICE/DRUG STATUS: This abstract does not discuss or include any applicable devices or drugs.
P8. Minimally Invasive Spine Surgery: Its Effect on Patient Outcomes in the Treatment of Degenerative Disc Disease: A Comparison to the Classic Open Approach
Donald Kucharzyk, DO1; Dushan Budimir, BS2
1Pediatric & Spine Institute, Crown Point, IN, US; 2Downers Grove, IL, US
FDA DEVICE/DRUG STATUS: This abstract does not discuss or include any applicable devices or drugs.
P9. How Anal Are We About “Anal Tone” in Patients with Suspected Cauda Equina Syndrome
Ravi Badge, FRCS, MSc, MBBS
Wigan, UK
FDA DEVICE/DRUG STATUS: This abstract does not discuss or include any applicable devices or drugs.
21

P10. Analysis of Internet Information on the Controversial X-Stop Device
Joshua T. Anderson, BS1, 2; Thomas B. Sullivan, BSE1, 2; Uri M. Ahn, MD3; Nicholas U. Ahn, MD2
1Case Western Reserve University School of Medicine, Cleveland, OH, US; 2University Hospitals Case Medical Center, Department of Orthopedic Surgery, Cleveland, OH, US; 3New Hampshire NeuroSpine Institute, Bedford, NH, US
FDA DEVICE/DRUG STATUS: This abstract does not discuss or include any applicable devices or drugs.
P11. Analysis of Internet Information on a Controversial Procedure: Vertebroplasty
Joshua T. Anderson, BS1, 2; Thomas B. Sullivan, BSE1, 2; Uri M. Ahn, MD3; Nicholas U. Ahn, MD2
1Case Western Reserve University School of Medicine, Cleveland, OH, US; 2University Hospitals Case Medical Center, Department of Orthopedic Surgery, Cleveland, OH, US; 3New Hampshire NeuroSpine Institute, Bedford, NH, US
FDA DEVICE/DRUG STATUS: This abstract does not discuss or include any applicable devices or drugs.
P12. Analysis of Internet Information on a Controversial Procedure: Kyphoplasty
Joshua T. Anderson, BS1, 2; Thomas B. Sullivan, BSE1, 2; Uri M. Ahn, MD3; Nicholas U. Ahn, MD2
1Case Western Reserve University School of Medicine, Cleveland, OH, US; 2University Hospitals Case Medical Center, Department of Orthopedic Surgery, Cleveland, OH, US; 3New Hampshire NeuroSpine Institute, Bedford, NH, US
FDA DEVICE/DRUG STATUS: This abstract does not discuss or include any applicable devices or drugs.
P13. Severe Thoracic Stenosis is Associated with Advanced Degenerative Changes of the Ankle Joint: A Study of 720 Cadaveric Specimens
Joshua T. Anderson, BS1, 2; Alex V. Boiwka, MS1, 2; Uri M. Ahn, MD3; Nicholas U. Ahn, MD2
1Case Western Reserve University School of Medicine, Cleveland, OH, US; 2University Hospitals Case Medical Center, Department of Orthopedic Surgery, Cleveland, OH, US; 3New Hampshire NeuroSpine Institute, Bedford, NH, US
FDA DEVICE/DRUG STATUS: This abstract does not discuss or include any applicable devices or drugs.
P14. Lumbar Stenosis is Associated with Ankle Osteoarthritis and Increased Hindfoot Degeneration: A Post-Mortem Study of 720 Specimens
Joshua T. Anderson, BS1, 2; Alex V. Boiwka, MS1, 2; Uri M. Ahn, MD3; Nicholas U. Ahn, MD2
1Case Western Reserve University School of Medicine, Cleveland, OH, US; 2University Hospitals Case Medical Center, Department of Orthopedic Surgery, Cleveland, OH, US; 3New Hampshire NeuroSpine Institute, Bedford, NH, US
FDA DEVICE/DRUG STATUS: This abstract does not discuss or include any applicable devices or drugs.
P15. Pedicle-Lengthening Osteotomy: An In Vitro Study to Determine its Cutting Sites
Zong Ping Luo, PhD, MS1; Zhigang Zhang, MD2; Xin Mei3; Huilin Yang, MD, PhD3
1Soochow University Orthopaedic Institute, Suzhou, China; 2Suzhou, China; 3The First Affiliated Hospital of Soochow University, Suzhou, China
FDA DEVICE/DRUG STATUS: This abstract does not discuss or include any applicable devices or drugs.
P16. Reason for Lawsuit in Spinal Cord Injury Affects Final Outcome
Robert Quigley, MD1; Brent Forrest, MD2; Wayne K. Cheng, MD3
1Colton, CA, US; 2Loma Linda, CA, US; 3Loma Linda University, Loma Linda, CA, US
FDA DEVICE/DRUG STATUS: This abstract does not discuss or include any applicable devices or drugs.
P17. Utility of Preoperative MRI Co-Registered with Intraoperative CT Scan for the Resection of Complex Tumors of the Spine
Kenneth P. D’Andrea, DO1; Daniel K. Fahim, MD2
1Oakland University, William Beaumont School of Medicine, Royal Oak, MI, US; 2Baylor College of Medicine, Houston, TX, US
FDA DEVICE/DRUG STATUS: This abstract does not discuss or include any applicable devices or drugs.
P18. Lateral Transpsoas Access to the Lumbar Spine for Revision Surgery
Luiz H. Pimenta, MD, PhD; Rodrigo A. Amaral, MD; Luis Marchi, MS; Thiago P. Coutinho, MD; Thabata Bueno; Leonardo Oliveira, MD; Rubens Jensen, MD
Instituto de Patologia da Coluna, São Paulo, Brazil
FDA DEVICE/DRUG STATUS: This abstract does not discuss or include any applicable devices or drugs.
ePOSTERS
22

P19. Analysis of Local Sagittal Parameters in a Stand-Alone ALIF for L5S1 DDD: Minimum Two-Year Follow-Up
Luiz H. Pimenta, MD, PhD; Rodrigo A. Amaral, MD; Luis Marchi, MS; Leonardo Oliveira, MD; Thabata Bueno; Thiago P. Coutinho, MD; Rubens Jensen, MD
Instituto de Patologia da Coluna, São Paulo, Brazil
FDA DEVICE/DRUG STATUS: This abstract does not discuss or include any applicable devices or drugs.
P20. Clinical and Radiological Consequences of Interbody Cage Subsidence
Luiz H. Pimenta, MD, PhD; Luis Marchi, MS; Rodrigo A. Amaral, MD; Thiago P. Coutinho, MD; Leonardo Oliveira, MD
Instituto de Patologia da Coluna, São Paulo, Brazil
FDA DEVICE/DRUG STATUS: This abstract does not discuss or include any applicable devices or drugs.
P21. Complications in Lateral Transpsoas Access in the Lumbar Spine
Luiz H. Pimenta, MD, PhD; Rodrigo A. Amaral, MD; Luis Marchi, MS; Leonardo Oliveira, MD; Thabata Bueno; Thiago P. Coutinho, MD; Rubens Jensen, MD
Instituto de Patologia da Coluna, São Paulo, Brazil
FDA DEVICE/DRUG STATUS: This abstract does not discuss or include any applicable devices or drugs.
P22. Evaluation of the Calcium Phosphate Cement as Bone Graft for Lumbar Interbody Fusion
Luiz H. Pimenta, MD, PhD; Rodrigo A. Amaral, MD; Luis Marchi, MS; Leonardo Oliveira, MD; Thabata Bueno; Thiago P. Coutinho, MD; Rubens Jensen, MD
Instituto de Patologia da Coluna, São Paulo, Brazil
FDA DEVICE/DRUG STATUS: This abstract does not discuss or include any applicable devices or drugs.
P23. L5S1 Low-Grade Spondylolisthesis Treated by ALIF: Local Lordosis Correction
Luiz H. Pimenta, MD, PhD; Rodrigo A. Amaral, MD; Thiago P. Coutinho, MD; Luis Marchi, MS; Leonardo Oliveira, MD; Thabata Bueno; Rubens Jensen, MD
Instituto de Patologia da Coluna, São Paulo, Brazil
FDA DEVICE/DRUG STATUS: This abstract does not discuss or include any applicable devices or drugs.
P24. MIS Lumbar Fusion in an Ambulatory Surgery Center (ASC): Safety, Treatment Outcomes and Comparison with Inpatient Lumbar Fusion
William D. Smith, MD
Western Regional Center for Brain & Spine Surgery, Las Vegas, NV, US
FDA DEVICE/DRUG STATUS: This abstract does not discuss or include any applicable devices or drugs.
P25. Complications with rhBMP-2 in Lateral Approach Spine Surgery
William D. Smith, MD1; Luiz H. Pimenta, MD, PhD2; Juan S. Uribe, MD3
1Western Regional Center for Brain & Spine Surgery, Las Vegas, NV, US; 2Instituto de Patologia da Coluna, São Paulo, Brazil; 3University of South Florida, Tampa, FL, US
FDA DEVICE/DRUG STATUS: This abstract does not discuss or include any applicable devices or drugs.
P26. Neurologic Complications in Extreme Lateral Interbody Fusion (XLIF): A Comparative Analysis of Levels L2-3, L3-4 and L4-5
William D. Smith, MD
Western Regional Center for Brain & Spine Surgery, Las Vegas, NV, US
FDA DEVICE/DRUG STATUS: This abstract does not discuss or include any applicable devices or drugs.
P27. Acute and Hyperacute Corpectomy for Traumatic Burst Fractures Using a Mini-Open Lateral Approach
William D. Smith, MD
Western Regional Center for Brain & Spine Surgery, Las Vegas, NV, US
FDA DEVICE/DRUG STATUS: This abstract does not discuss or include any applicable devices or drugs.
P28. A Prospective Study of Reliability of a Novel Classification System for Thoracolumbar Injuries in Children and Adolescent
Xie En, MD1; Ding-Jun Hao, MD2
1Hong Hui Hospital, Xi’an Jiaotong University College of Medicine, Xi’an, Shan Xi, China; 2Xi’an Honghui Hospital, Xi’an, Shaanxi, China
FDA DEVICE/DRUG STATUS: This abstract does not discuss or include any applicable devices or drugs.
ePOSTERS
23

P29. A Study on the Surgical Techniques to Treat Thoracic Spine Lesions with a Sneak Resection Approach for the Anterior Sternal Upper Part: A New Surgical Technique
Xie En, MD1; Ding-Jun Hao, MD2
1Hong Hui Hospital, Xi’an Jiaotong University College of Medicine, Xi’an, Shan Xi, China; 2Xi’an Honghui Hospital, Xi’an, Shaanxi, China
FDA DEVICE/DRUG STATUS: This abstract does not discuss or include any applicable devices or drugs.
P30. Study of Lumbar Multifidus Muscles in Patients with Chronic Low Back Pain and in Asymptomatic Human: A Blinded Randomized Controlled Trial (RCT)
Lijun Zhou, MD1; Ding-Jun Hao, MD1; Xie En, MD2
1Hong Hui Hospital, Xi’an Jiaotong University College of Medicine, Xi’an, Shan Xi, China; 2Xi’an Honghui Hospital, Xi’an, Shaanxi, China
FDA DEVICE/DRUG STATUS: This abstract does not discuss or include any applicable devices or drugs.
ePOSTERS
24

P1. A Novel Measurement of Postoperative Axial Plane Rotation in Adolescent Idiopathic Scoliosis Using Plain Radiographs
Benjamin T. Bjerke-Kroll, MD, MS1; Grant D. Shifflett1; Sravisht Iyer2; Zoe Cheung1; Peter D. Fabricant, MD1; Han Jo Kim, MD1
1Hospital for Special Surgery, New York, NY, US; 2Cambridge, MA, US
BACKGROUND CONTEXT: Many methods of measuring axial rotation by radiographs have been described. However, all depend on an intact and visible spinous process, pedicle, and/or lateral borders of the spinal canal, rely on pre-defined vertebral shape parameters, or require oblique radiographs. Three-dimensional imaging provides rotation measurements, but is costlier and/or exposes the patient to additional radiation.PURPOSE: To create a simple and reproducible methodology of axial rotation measurements using routine radiographs.STUDY DESIGN/SETTING: Level 2: development of diagnostic criteria on consecutive patients with a universally applied gold standard performed at an academic institution.PATIENT SAMPLE: 3,552 instrumented spinal levels in 308 consecutive patients age 10-18 from July 2007 to July 2013 at our institution who underwent spinal fusion for adolescent idiopathic scoliosis (AIS) were reviewed. Nine of these patients underwent CT scans of the spine within 60 days of posteroanterior (PA) and lateral radiographs. 93 screw tips were visible and distinguishable on both radiographs and CT scan.OUTCOME MEASURES: Axial rotation measured by CT and novel radiographic technique.METHODS: Posterior to anterior length of the screw was measured on the lateral radiograph; medial to lateral length of the screw was measured on the PA radiograph, both parallel to the floor. Rod width was then measured on both radiographs at the nearest available level for reference. A correction factor δ was calculated to account for magnification differences. δ = LRod, Lateral/ LRod, PAHorizontal lengths of the screw visible on PA (corrected for rod width) and lateral images were then related using the trigonometric relationship described below to calculate axial rotation. Axial rotation was recorded as the medial angle formed by the screw body and horizontal. θ = tan-1[LLateral/ (δ x LPA)]Axial rotation was measured on CT scan by a line drawn through the screw body and a line parallel to the floor.RESULTS: Nine patients met criteria for analysis. 95 total spinal levels were visible on all radiographs and CT scans (190 pedicles visualized), or 2.7% (95/3,552). There were 93 visible pedicle screws at these levels, 38 non-visible screws, 12 hooks, 8 wires, and no instrumentation at 36 pedicles; 2 screws were offset from the rod, and 2 pedicle screws had disengaged inner set screws. A pedicle screw at the apical vertebra was present and measureable by this technique in 90.3% (272/308) of patients reviewed. The difference in axial rotation measured on CT and radiographs was 3.3° +/- 1.9°. 81.7% (76/93) of all pedicle screws measured on
radiographs were within 5° of the measured value on CT scan. Intrarater reliability for the three raters was excellent (ICC = 0.879, Range: 0.777-0.995). Interrater reliability was also excellent (ICC = 0.900). Intra- and inter-rater reliability were calculated using the intraclass correlation coefficient (ICC 2,1) with absolute agreement.CONCLUSIONS: This novel technique accurately measures axial rotation of pedicle screws in the post-operative spine, is validated by CT scan, and has good/excellent inter- and intra-observer reliability. Unlike previous methods, it does not require additional imaging or make assumptions about screw length or rod width. This method may provide an additional resource for future studies to estimate the maintenance of post-operative derotation. Future methodology may automate this process to create a computerized algorithm for the calculation of axial rotation.FDA DEVICE/DRUG STATUS: This abstract does not discuss or include any applicable devices or drugs.
P2. Assessment of Vertebral Curves Using the Manual Post-It® Technique
Benjamin T. Bjerke-Kroll, MD, MS; Brian P. Gladnick; Joseph Schreiber, MD; Grant D. Shifflett; Matthew E. Cunningham, MD, PhD
Hospital for Special Surgery, New York, NY, US
BACKGROUND CONTEXT: Modern picture archiving and communication systems (PACS) typically include software for evaluating measurements of distances and angles. However, in the outpatient spine setting, patients may present with radiographs stored on a physical disc, which may not include software for measuring vertebral curves. To our knowledge, there is no study that describes an accurate manual assessment of vertebral curves on digital radiographs when there is no available analytic software.PURPOSE: To report a manual technique for the evaluation of vertebral curves on digital spine radiographs, and to assess the agreement of this technique with that of digital software for measuring vertebral curves.STUDY DESIGN/SETTING: Retrospective radiographic review and reporting of a new technique.PATIENT SAMPLE: 24 consecutive patients were selected from a prospectively maintained spinal deformity database.METHODS: We reviewed anteroposterior (AP) and lateral spine radiographs of 24 spinal deformity patients from a prospective database. Two independent observers measured Cobb angles for: 1) the major coronal curve; 2) the thoracic kyphosis (T2-T12); and 3) the lumbar lordosis (T12-S1). Measurements were made: 1) digitally using our institution’s PACS; and 2) via manual technique, which involves placement of an adhesive Post-It® note directly on the computer screen, transcribing the angle onto the Post-It® note with a pencil, and measuring the angle with a handheld goniometer. Intraclass correlation coefficients (ICCs) were calculated to determine the agreement between the two methods. Intraclass correlation coefficients (ICC) were calculated to examine the agreement between the digital PACS and manual Post-It® techniques for each independent observer. ICCs were also used to calculate interobserver reliability for the digital PACS and manual Post-It® techniques between the two observers. In all cases, ICCs were calculated using a two-way mixed model with absolute agreement.RESULTS: Agreement between the manual Post-It® technique and digital PACS technique was graded as excellent for both observers.
ePOSTERPROCEEDINGS
N A S S S U M M E R S P I N E M E E T I N G
25

For the first observer, ICCs between the manual Post-It® and PACS techniques were 0.995 (major coronal curve), 0.977 (thoracic kyphosis), and 0.979 (lumbar lordosis). For the second observer, ICCs between the manual Post-It® and PACS techniques were 0.995 (major coronal curve), 0.992 (thoracic kyphosis), and 0.989 (lumbar lordosis). Interobserver reliability was similarly found to be excellent between observers. Using the PACS technique, ICCs between the two observers were 0.995 (major coronal curve), 0.987 (thoracic kyphosis), and 0.961 (lumbar lordosis). Using the manual Post-It® technique, ICCs between the two observers were 0.992 (major coronal curve), 0.983 (thoracic kyphosis), and 0.979 (lumbar lordosis).CONCLUSIONS: The Post-It® technique for measuring Cobb angles demonstrated excellent agreement with the PACS system in our series of spinal deformity patients. Curves on digital radiographs can be accurately measured using a convenient manual technique.FDA DEVICE/DRUG STATUS: This abstract does not discuss or include any applicable devices or drugs.
P3. Hypertrophy and Fibrosis of the Ligamentum Flavum in Lumbar Spinal Stenosis is Associated with Increased Expression of LPA and LPAR1
Kai Zhang
Shanghai Jiao Tong University School of Medicine, Shang Hai, China
BACKGROUND CONTEXT: Ligamentum flavum (LF) hypertrophy and fibrosis are important causes of Lumbar spinal stenosis (LSS). Lysophosphatidic acid (LPA) is involved in the fibrotic process in multiple organ systems.Therefore, we hypothesized that LPA and its receptors might also play a role in degeneration of the LF in LSS patients.PURPOSE: The purpose of this study was to determine the level of expression of LPA in the LF from LSS patients and to analyze the relationship among LPA, LPA receptor 1(LPAR1) and LF hypertrophy.STUDY DESIGN/SETTING: Histological, immunohistochemical, and ELISA analysis of the human ligamentum flavum (LF)PATIENT SAMPLE: Forty-one LF samples were enrolled in this study.OUTCOME MEASURES: The thickness of the LF was measured by MRI. Histologic analysis using hematoxylin and eosin (H&E) and Masson’s trichrome stain. The content of LPA and CTGF in LF samples was analyzed using ELISA. The expression of LPAR1 was determined by immunohistochemistry.METHODS: Forty-one LF samples were enrolled in this study. The thickness of the LF was measured by MRI. Histologic analysis using hematoxylin and eosin (H&E) and Masson’s trichrome stain was performed for each LF to evaluate the architecture of the extracellular matrix (ECM). The content of LPA and CTGF in LF samples was analyzed using ELISA. The expression of LPAR1 was determined by immunohistochemistry.RESULTS: Degeneration of the LF was characterized by an increase in disorganized elastic fibers and fibrotic transformation by extracellular collagen deposition. The thickness of the LF and the
concentration of LPA and CTGF in the hypertrophic LF group were significantly higher than the control group. Furthermore, the LPA and CTGF concentrations had a positive correlation with the LF thickness (r=0.91, P<0.001 and r=0.943, P<0.001, respectively). Based on immunohistochemical analysis, the expression of LPAR1 was increased in the hypertrophy group.CONCLUSIONS: The increased expression of LPA and LPAR1 is associated with the fibrosis and hypertrophy of the LF in patients with LSS. Further study on the mechanism underlying LF fibrosis may lead to new therapies for LF hypertrophy and fibrosis.FDA DEVICE/DRUG STATUS: This abstract does not discuss or include any applicable devices or drugs.
P4. Kyphoplasty Using Temperature Gradient Injection Technique for the Treatment of Osteoporotic Vertebral Compression Fractures
Tao Liu, MD, PhD
The First Affiliated Hospital of Soochow University, Suzhou, China
BACKGROUND CONTEXT: Kyphoplasty is an effective procedure for patients with acute vertebral fractures. But, until now, there are some complications. The most common complication is cement leakage. From 2003, we developed an injection technique called ‘Temperature gradient injection technology’ which can significantly decrease the cement leakage rate.PURPOSE: To prospectively compare kyphoplasty using ‘Temperature Gradient Injection Technique’ (‘Temperature Gradient Injection group’) with kyphoplasty using traditional injection technique (‘Traditional injection group’) for the treatment of osteoporotic vertebral compression fractures.STUDY DESIGN/SETTING: Prospective cohort study.PATIENT SAMPLE: 129 patients (160 vertebral fractures) in the ‘Temperature Gradient Injection group’ and 105 patients (128 vertebral fractures) in the ‘Traditional injection group’.OUTCOME MEASURES: Outcomes were measured pre- and postoperatively using VAS, ODI, the anterior vertebral height, the kyphosis angle, the occurrence of new vertebral fractures and cement leakage.METHODS: The study population included 129 patients (160 vertebral fractures) in the ‘Temperature Gradient Injection group’ and 105 patients (128 vertebral fractures) in the ‘Traditional injection group’. The mean follow-up period was 25.3 months and 24.7 months respectively. The baseline characteristics including sex, age, number of prevalent fractures, etc were comparable for both groups. Outcomes were measured pre- and postoperatively using VAS, ODI, the anterior vertebral height, the kyphosis angle, the occurrence of new vertebral fractures and cement leakage.RESULTS: In the ‘Temperature Gradient Injection group’, VAS improved from 7.8±1.3 preoperatively to 2.1±1.9 at last follow-up (P <.05). Preoperatively, the ODI was 77.3±5.9, which improved to 39.7±9.7 (P <.05). The anterior vertebral height improved from (61.5±5.7)% preoperatively to (84.6±2.9)% at last follow-up (P <.05). The kyphosis angle improved from 17.90±7.80 to 0.50±7.50 at last follow-up (P < .05). In ‘Traditional injection group’, VAS improved from 7.5±1.6to 2.3±2.5 at last follow-up (P <.001). Preoperatively, the ODI was 75.3±7.2, which improved to 38.7±10.9 (P <.05). The anterior vertebral height improved from (63.9±6.5)% preoperatively to (83.1±6.2)% at last follow-up (P <.05). The kyphosis angle improved from 18.30±8.50 to 8.70±6.50 (P < .05). There was no significant difference in VAS, ODI, the anterior vertebral height and the kyphosis angle between the two
ePOSTER PROCEEDINGS
26

groups both preoperatively and postoperatively (P >0.05). There was no significant difference in the occurrence of new fractures of vertebral bodies of the ‘Temperature Gradient Injection group’ (7.8%) versus the ‘Traditional injection group’ (7.6%). There were only 3 patients having cement leakage (2.3%) in ‘Temperature Gradient Injection group’, which was significantly less than ‘Traditional injection group’ (8 patients, 7.6%) (P <.05).CONCLUSIONS: Both kyphoplasty using ‘Temperature Gradient Injection Technique’ and kyphoplasty using traditional injection technique are effective at improving pain, functional disability, vertebral height and kyphosis angle; however, kyphoplasty using ‘Temperature Gradient Injection Technique’ has significantly less cement leakage.FDA DEVICE/DRUG STATUS: This abstract does not discuss or include any applicable devices or drugs.
P5. The Diagnostic Value of MRI, CT, PET, Bone Scintigraphy (BS) and BS with SPECT (SPECT) in Detecting Vertebral Metastases
Tao Liu, MD, PhD
The First Affiliated Hospital of Soochow University, Suzhou, China
BACKGROUND CONTEXT: The vertebral column is the region of the skeleton most frequently affected by metastatic disease. Autopsy series have demonstrated that vertebral metastases are found in as many as 30% of patients with malignancies.10% of all spinal metastases have no known primary tumor at the time of presentation. Vertebral metastases can cause severe pain, paralysis, and impairment of activities of daily living. Therefore, early diagnosis and treatment before the development of permanent neurologic and functional deficits is essential for a favorable prognosis. Imaging modalities are powerful tools in assessing malignant vertebral involvements. The widely used modalities for diagnosis of vertebral metastases included MRI, CT, PET, BS (Bone Scintigraphy) and SPECT (BS with Single photon emission computed tomography for focal lesions). Extensive research on the diagnostic value of these modalities has been done, but no consensus has been reached as to the optimal imaging modality for detection of vertebral metastases yet, for a wide variation in patient populations, imaging techniques, study designs and results exists. These factors make it difficult for workers in this field to know the relative diagnostic value of these imaging modalities.PURPOSE: To perform a meta-analysis to compare the diagnostic value of MRI, CT, PET, Bone Scintigraphy (BS) and BS with SPECT (SPECT) in detecting vertebral metastases.STUDY DESIGN/SETTING: A meta-analysisPATIENT SAMPLE: 1934 patientsOUTCOME MEASURES: Sensitivity, specificity, Diagnostic Odds Ratio (DOR) and Summary Receiver Operating Characteristic (SROC) curves.METHODS: MEDLINE, EMBASE, Scopus and some other databases were searched for relevant original articles published from January 1995 to January 2013. Inclusion Criteria was as follows: MRI, CT, PET, SPECT or BS was performed to detect vertebral metastases; Sufficient data were presented to construct a 2 x 2 contingency table; Histopathologic analysis and/or close clinical and imaging
follow-up and/or radiographic confirmation by multiple imaging modalities were used as the reference standard. Two reviewers independently extracted data. Software called “META-DiSc” was used to obtain pooled estimates of sensitivity, specificity, Diagnostic Odds Ratio (DOR) and Summary Receiver Operating Characteristic (SROC) curves.RESULTS: 20 articles consisting of 31 studies fulfilled all inclusion criteria. On per-patient basis, only MRI, SPECT and BS had enough data for analysis. The pooled sensitivity estimates for MRI, SPECT and BS were 91.9%, 93.1% and 79.2% respectively. For sensitivity, MRI= SPECT> BS. (”=”indicated no significant difference, P> .05 ;”>”indicated significantly higher, P< .05). The pooled specificity estimates for MRI, SPECT and BS were 93.1%, 93.4% and 93.5% respectively. For specificity, MRI= SPECT= BS. The pooled DOR estimates for MRI, SPECT and BS were 92.5, 143.2 and 40.2 respectively. For DOR, MRI= SPECT> BS. SROC curve for SPECT and MRI showed better diagnostic accuracy than BS. On per-lesion basis, the pooled sensitivity estimates for MRI, CT, PET, SPECT and BS were 87.3%, 66.7%, 94.1%, 90.1% and 81.1% respectively. For sensitivity, PET> SPECT= MRI> BS> CT. The pooled specificity estimates for MRI, CT, PET, SPECT and BS were 96.4%, 95.5%, 78.9%, 87.8%, and 59.3% respectively. For specificity, MRI= CT> SPECT > PET> BS. The pooled DOR estimates for MRI, CT, PET, SPECT and BS were 208.3, 24.9, 33.0, 71.7 and 3.0 respectively. For DOR, MRI> SPECT> PET= CT> BS. SROC curve for each modality showed MRI had the best diagnostic accuracy and CT had the lowest diagnostic accuracy.CONCLUSIONS: For diagnosis of vertebral metastases, MRI and SPECT were comparable and both better than BS on per-patient basis. On per-lesion basis, MRI was found to be the best modality.FDA DEVICE/DRUG STATUS: This abstract does not discuss or include any applicable devices or drugs.
P6. Vertebral Column Manipulation: A New Corrective Technique for Idiopathic Scoliosis for Three-Dimensional (3D) Correction: A Retrospective Study Based on the Two-Years Follow-Up
Pawel Grabala, MD; Robert Budkiewicz, MD, PhD; Dariusz Kossakowski, MD, PhD
Regional Specialist Children’s Hospital, Department of Pediatric Orthopaedic and Trauma Surgery, Olsztyn, Poland
BACKGROUND CONTEXT: All spinal deformities occur according to the three planes of the body. Idiopathic scoliosis is described as a lateral curvature of the spine with rotation in the absence of any congenital spinal abnormalities or associated musculoskeletal condition. The diagnosis and treatment of idiopathic scoliosis has experienced revolutionary advances since the first Harrington method. New techniques are being continuously developed in the surgical treatment of idiopathic scoliosis. There are interactions among the deformities in each plane, which determine both the progress of scoliosis and the outcomes of surgery.PURPOSE: The objective of this work was to evaluate a new corrective technique for three-dimensional (3D) correction of spinal deformities called vertebral column manipulation (VCM), and to demonstrate the efficacy assessment via illustrative cases.STUDY DESIGN/SETTING: Report of a new technique. A retrospective study carried out in a regional specialized center in Poland.PATIENT SAMPLE: Twenty eight female patients (mean age: 19years) with average follow-up of 2 years.
ePOSTER PROCEEDINGS
27

OUTCOME MEASURES: Indications for surgery, duration of symptoms prior to surgery. Details of operation were collected, including level of operation, blood loss, operative time, intraoperative complications, length of hospital stay, the duration of follow-up, postoperative complications (e.g., myelopathy and radiculopathy), and revision surgery. Patients characteristics included patient age at the time of surgery, body mass index (BMI), chronic conditions, smoking history and current smoking status at the time of the operation, medication use (antidepressants, anxiolytics, narcotics, stimulants) and date of surgery. Radiographic parameters measured before and after surgery were: curve magnitude including the Cobb angle, thoracic kyphosis, T1-S1 length, apical vertebral translation (AVT), apical vertebral height, and at follow-up. Scoliosis Research Society (SRS)-22 scores were measured during the final follow-up.METHODS: Twenty eight patients with Lenke type 1, 3 and 5 enrolled in this retrospective clinical study were divided into three groups (A, B, C). All cases had minimum 2-year follow-up. Five illustrative cases corrected by 3D synchronous derotation (VCM) were presented. Operative technique was a standard posterior incision exposure, and segmental screws placement was performed with the patient lying prone. Fixation and fusion levels were in accordance with Lenke standards, whereas the CD Legacy system (Medtronic) was used in this study. The basic principle and procedure for 3D derotation by VCM were previously described by Chang and Lenke. Two Vertebral Column Manipulation (VCM) devices were installed on the apical region of both curves which were synchronously derotated and following convex correction at both curves, the concave rods were secured in situ.RESULTS: The mean preoperative coronal Cobb angles of the thoracic curve was 56 degrees (range: 25-70), after the surgery they were corrected to 38 degrees (26-45). The mean preoperative major curve Cobb angle was 59 degrees (45-82), while after surgery it reached 26 degrees (13-44). Surgery was successful for most of the patients. Of all cases, approximately 25% complications were reported (prolonged postoperative wound healing, pleural effusion of unknown etiology, and one case of a serious neurological disorder which resolved spontaneously). The pedicle screws of the apical vertebra were successfully placed in all cases. CONCLUSIONS: The corrective technique for three-dimensional (3D) correction of spinal deformities called vertebral column manipulation (VCM) is effective and promising as the method assures very good results, low complication rate as well as some loss of correction in the two-year observation period. All patients operated on using this technique are reporting better quality of life for both physical and mental status. Our study suggests that VCM is an efficacious technique for potential use in the correction of idiopathic scoliosis in all three planes.FDA DEVICE/DRUG STATUS: This abstract does not discuss or include any applicable devices or drugs.
P7. Extreme Lateral Lumbar Interbody Fusion Using Osteocel Plus: 20-Month Outcome
Karthik Madhavan, MD1; Steven Vanni, DO, DC2
1Miami, FL, US; 2Lois Pope Life Center, Miami, FL, US
BACKGROUND CONTEXT: Iliac crest bone graft (ICBG) is considered the gold standard for its osteoconductive, osteoinductive and osteogenic properties. However donor site morbidity has directed the researchers towards alternative. Mesenchymal stem cells (MSCs) have gained lot of attention for their ability to differentiate to osteogenic lineage. Osteocel Plus (OC+) is an allograft cellular bone matrix containing mesenchymal stem cells (MSCs) and osteoprogenitor cells combined with DBM and cancellous bone. We present our series with use of osteocel plus in pure extreme lateral lumbar interbody fusion (XLIF/DLIF/LLIF). STUDY DESIGN/SETTING: We conducted a retrospective review of charts and images to evaluate for bony fusion in patients who underwent elective lateral LIF with use of osteocel plus. Bony fusion was evaluated from 3 month follow up through formation of trabecular bone and confirmed with the radiology reading. RESULTS: Our retrospective chart review yielded 19 patients who underwent extreme lateral LIF with use of Osteocel plus packed in and around PEEK cage on 28 levels. Three patients were stand-alone cages with no additional instrumentation. About 4.65 cc of Osteocel was used at each level. The age ranged between 36 to 83 years and male to female ratio was 1:2. Average follow up was 20 months (3-30 moths). Average blood loss was 25cc (10-110cc). Three month follow up X-rays revealed trabecular bone noted by radiologist and the senior author (SV). Solid bony fusion was noted in 100% of the patients by end of first year. No complications like signs of pseudoarthrosis, screw/pedicle fracture were noted. CONCLUSIONS: Although our data is small, Osteocel plus is a good alternative to ICBG as it brings about robust fusion has been noted in patients of all ages and both sexes. It avoids additional surgery for graft retrieval, reduces bleeding and operative time especially in medically challenged elderly population. This can also be used in stand-alone procedure in patients without gross instability. FDA DEVICE/DRUG STATUS: This abstract does not discuss or include any applicable devices or drugs.
P8. Minimally Invasive Spine Surgery: Its Effect on Patient Outcomes in the Treatment of Degenerative Disc Disease: A Comparison to the Classic Open Approach
Donald Kucharzyk, DO1; Dushan Budimir, BS2
1Pediatric & Spine Institute, Crown Point, IN, US; 2Downers Grove, IL, US
BACKGROUND CONTEXT: Minimally invasive spine surgery for instrumented lumbar fusion for degenerative spondylolisthesis is an attractive option with obvious advantages to the surgeon and the patient. but questions have arisen as to its effect on patient outcomes and return to work status. For it to be accepted, it should offer similar if not better outcomes compared to the classic open approach as well as offer shorter hospitalization, less blood loss, less muscle damage, and a quicker return to work. The impetus for an MIS minimally disruptive approach centers on the need to minimize paraspinal muscle damage as seen in the open
ePOSTER PROCEEDINGS
28

approach. The classic open approach leads to increased blood loss, more postoperative pain due to muscle stripping and more so direct muscle damage, and this affects overall function of the muscle postoperatively. This has been supported in the works of Kim, Stevens and Gejo.PURPOSE: To compare the results of a classic open approach to that of a Minimally invasive, Minimally disruptive approach in the treatment of degenerative lumbar spondylolisthesis STUDY DESIGN/SETTING: A non-randomized prospective study comparing open versus MIS was performed in single level L4-5 or L5-S1 fusions.PATIENT SAMPLE: 200 patients were divided into two groups of 100 patients each.OUTCOME MEASURES: ODI, SF36, BPSMETHODS: All patients were evaluated for blood loss, OR time, hospitalization, narcotic use, X-ray use, fusion rates, and return to work status.RESULTS: Open: OR time110min, bloodloss300ml, hospitalization3.3days, narcotic use51hrs, X-ray use65 seconds, fusion rate92.8%; MIS OR time90min, blood loss75ml, hospitalization1.5days, narcotic use12hrs, xray use80seconds, fusion rate94.5%.ODI open 52.5pre 28.4post MIS 54.1pre 12.2post; SF36 open 27.6pre 39.7post MIS 27.1pre49.6post; BPS open 16.4pre 8.1post MIS 17.1pre 2.0post; Return to work open/MIS 15/30% one, 45/70%three, 75/90%six, 80/95%twelve months based on job descriptions and FCE.CONCLUSIONS: MIS offered advantages in the properly selected patient revealing shorter hospitalization, less blood loss, less narcotic use, quicker entry into PT and functional rehab which lead to a sooner return to work. MIS showed improvements in all outcome measurement tools when compared to the open group and this is attributed to the muscle sparring minimally disruptive approach that MIS affords the surgeon. It did result in a slightly longer X-ray time utilization and but most importantly it resulted in similar fusion rates to that of the open approachFDA DEVICE/DRUG STATUS: This abstract does not discuss or include any applicable devices or drugs.
P9. How Anal Are We About “Anal Tone” in Patients with Suspected Cauda Equina Syndrome
Ravi Badge, FRCS, MSc, MBBS
Wigan, UK
BACKGROUND CONTEXT: Clinical diagnosis of “Cauda Equina Syndrome” (CES) can be challenging and a delay in prompt diagnosis and decompression results can result in poor outcomes. Hence, it is crucial to identify patients in early stages of CES. Assessment of anal tone with digital rectal examination (DRE) currently forms an essential part of the clinical examination, as well as vital medico-legal documentation, in suspected CES. However its accuracy and relevance is still debatable.PURPOSE: The aim of the study is to establish the value of assessment of anal tone in patients with suspected CES.METHODS: Our prospectively maintained electronic neurosurgical referrals database, MRI scans and operation notes were studied. Fifty-nine patients who underwent urgent surgical decompression
for CES secondary to disc herniation were identified over a period of two years. All patients included had radiological confirmation of CES on MRI scan. The main presenting symptoms and examination findings were recorded. RESULTS: There were 29 male and 30 female patients in this group with an average age of 43.6 years and average BMI of 37.2 kg/m2 (range: 18.2-49.7). 95% of patients presented with radicular pain, 42% with urinary symptoms, 17% with paraesthesia, 8% with foot drop and 1.6% with bowel dysfunction. Absent ankle reflexes (51%) and altered perianal sensation (30%) were the most consistent examination findings. DRE revealed 69% of patients had anal tone present, reduced in 26% and absent in 5%. CONCLUSIONS: In this study of radiologically (MRI) and surgically confirmed CES, radicular pain and urinary symptoms were the most consistent presenting symptoms. Absent ankle reflexes and altered perianal sensation were the most consistent clinical examination findings. 66% of these CES patients had normal anal tone documented. DRE can be an unpleasant and invasive examination. These results question the usefulness of DRE in helping the practitioner diagnose CES. FDA DEVICE/DRUG STATUS: This abstract does not discuss or include any applicable devices or drugs.
P10. Analysis of Internet Information on the Controversial X-Stop Device
Joshua T. Anderson, BS1, 2; Thomas B. Sullivan, BSE1, 2; Uri M. Ahn, MD3; Nicholas U. Ahn, MD2
1Case Western Reserve University School of Medicine, Cleveland, OH, US; 2University Hospitals Case Medical Center, Department of Orthopedic Surgery, Cleveland, OH, US; 3New Hampshire NeuroSpine Institute, Bedford, NH, US
BACKGROUND CONTEXT: The X-Stop is the first FDA-approved interspinous spacer for the treatment of intermittent neurogenic claudication secondary to lumbar spinal stenosis. Early studies reported good to excellent outcomes with low complication rates. Later studies published unacceptably high complication rates, reoperation rates, and costs. Frequently, patients use the internet to aid in medical decision-making. It has been shown that internet information actively influences patient choices. Multiple studies display the internet’s ineffectiveness in presenting high quality information on surgical procedures and devices to the public. This study is the first to examine internet information on the controversial X-Stop.PURPOSE: Our purpose was to determine how accurately and comprehensively publically accessible information over the internet reflects what exists in primary literature on the X-Stop and how patient decision-making could foreseeably be affected.METHODS: Search engines Google, Yahoo!, and Bing and search terms X-Stop, interspinous distraction device, and interspinous spacer decompression were used to identify 105 sites providing information on X-Stop. Sites were categorized by authorship then analyzed for the provision of appropriate patient inclusion and exclusion criteria, surgical and non-surgical treatment alternatives, purported benefits, common complications, peer-reviewed literature citations, and descriptions/diagrams of the procedure.RESULTS: 43% of websites were authored by private medical groups, 4% by academic medical groups, 16% by insurance companies, 9% by biomedical industry, 10% by news sources, and 19% by websites not fitting into those categories. 80% of the sites
ePOSTER PROCEEDINGS
29

contained descriptions and/or diagrams of the X-Stop procedure. 31% of webpages cited peer-reviewed literature. 56% of all sites provided at least one appropriate patient inclusion criterion (in addition to lumbar spinal stenosis). Only 20% of news and 40% of private medical group sites did the same. 33% of sites reported at least one patient exclusion criteria. Private medical group and news sites had the lowest reporting rates (13% and 10%) in this category. 91% of sites reported at least one purported benefit of X-Stop. One or more complications were reported in 23% of sites. One of the most commonly seen complications with all interspinous spacers, spinous process fractures, was discussed in 19% of sites. Specific non-surgical treatment alternatives were discussed in no higher than 28% of sites. 33% of sites mentioned the existence of conservative therapy without including specifics. 51% of sites included laminectomy and 22% fusion as surgical treatment options.CONCLUSIONS: We convincingly demonstrate the internet’s ineffectiveness in providing critically important information necessary for patient education on the X-Stop. Publically accessible information was of poor quality, often incomplete, and potentially misleading. The high reporting rates of benefits (91%) contrasted with the abysmally low reporting rates of complications (23%) raises the concern that this information lends itself more toward patient recruitment than to education. Medical professionals need to know that internet information is often used by patients and that it influences their decisions. Therefore, it is imperative that clinicians are informative about the procedure while emphasizing the limitations of internet information, which has proven itself an exceedingly inept substitute for direct patient-physician interaction.FDA DEVICE/DRUG STATUS: This abstract does not discuss or include any applicable devices or drugs.
P11. Analysis of Internet Information on a Controversial Procedure: Vertebroplasty
Joshua T. Anderson, BS1, 2; Thomas B. Sullivan, BSE1, 2; Uri M. Ahn, MD3; Nicholas U. Ahn, MD2
1Case Western Reserve University School of Medicine, Cleveland, OH, US; 2University Hospitals Case Medical Center, Department of Orthopedic Surgery, Cleveland, OH, US; 3New Hampshire NeuroSpine Institute, Bedford, NH, US
BACKGROUND CONTEXT: Vertebroplasty is a minimally invasive cement augmentation procedure used to treat osteoporotic vertebral compression fractures refractory to conservative therapy that gained widespread popularity after many studies evidenced its success. Two studies in 2009 indicated that vertebroplasty was not associated with a statistically significant difference in clinical outcomes. Moreover, the internet has become an increasingly common tool utilized by patients to help with medical decision-making. Studies have demonstrated the internet’s lack of quality medical information and how this information does indeed affect patient choices. No such study has been performed on the controversial vertebroplasty procedure. Disagreement regarding the efficacy of vertebroplasty makes it critical that patients receive accurate and well-balanced information.
PURPOSE: Our purpose was to evaluate the quality and comprehensiveness of information on vertebroplasty available to the general public through the internet.METHODS: Search engines Google, Yahoo!, and Bing with the search term vertebroplasty were used to identify 105 websites offering information on vertebroplasty. Sites were then evaluated for authorship and content.RESULTS: 16% of sites were sponsored by an academic institution, 62% by a private medical group, 8% by biomedical device companies, and 14% were otherwise sponsored. Appropriate indications were referenced in 74% of all sites while only 45% discussed a contraindication to the procedure. 82% of academic and 62% of industry sites represent the range of reporting rates of at least one appropriate indication, while 49% of private and 35% of academic sites represent the range reporting at least one contraindication. Benefits were expressed by 100% of all sites; at least one potential complication was outlined in only 53%. Industry sites reported the overall lowest mean number of complications per site (0). At least one alternative treatment was mentioned by 51% of all sites. 27% of sites referenced peer reviewed literature, 41% offered experiential or non-cited data based on American populations, and 7% offered analogous data from international populations. 99% of sites provided step-by-step descriptions of the procedure while 44% of sites also included images.CONCLUSIONS: Our analysis reveals a striking insufficiency of high quality, publically accessible internet information necessary for proper patient education on vertebroplasty. The imbalance between the number of sites reporting indications for (74%) and benefits of (100%) vertebroplasty and the number of sites providing contraindications (45%), complications (53%), and alternative therapies (51%) raises the concern that information made available to the public lends itself more toward patient recruitment than to education. This is particularly true in the case of industry sites which had the second lowest percentage of sites reporting contraindications (38%), the fewest mean number of risks (0), the fewest mean number of treatment alternatives (0.9), and the highest mean number of benefits (4.1). Such information is clearly not an acceptable substitute for the physician-patient dynamic. Medical professionals should be familiar with studies showing that patients frequently base their medical decisions off of internet information. The discussion of a patient’s understanding of a procedure with a physician remains as critical as ever. Patients should be counseled on the limitations of internet information.FDA DEVICE/DRUG STATUS: This abstract does not discuss or include any applicable devices or drugs.
ePOSTER PROCEEDINGS
30

P12. Analysis of Internet Information on a Controversial Procedure: Kyphoplasty
Joshua T. Anderson, BS1, 2; Thomas B. Sullivan, BSE1, 2; Uri M. Ahn, MD3; Nicholas U. Ahn, MD2
1Case Western Reserve University School of Medicine, Cleveland, OH, US; 2University Hospitals Case Medical Center, Department of Orthopedic Surgery, Cleveland, OH, US; 3New Hampshire NeuroSpine Institute, Bedford, NH, US
BACKGROUND CONTEXT: Vertebral compression fractures are a common cause of morbidity and mortality in patients with osteoporosis and other diseases of the skeletal system. Vertebroplasty and kyphoplasty are minimally invasive cement augmentation procedures for the treatment of VCFs that have generated a great deal of enthusiasm in the spine community. A pair of 2009 studies reporting no statistically significant difference in clinical outcomes using vertebroplasty has thrown these treatments into controversy. Frequently, patients turn to internet sources to educate themselves prior to making medical decisions. It has been demonstrated that internet information actively influences patient decision-making. Prior studies have shown an inadequacy of quality internet information regarding specific devices and surgical treatments. No such study has been performed on kyphoplasty.PURPOSE: This study aimed to characterize publically accessible internet information on kyphoplasty in order to assess its potential impacts on patient education and decision making. Relative incongruence of physician opinion on kyphoplasty and increasing patient reliance on internet information makes it imperative that this information is accurate.METHODS: Three popular search engines, Google, Yahoo!, and Bing were utilized to identify the top 105 sites (35 per engine) providing information on kyphoplasty. Sites were grouped by sponsorship and evaluated for the provision of appropriate indications, contraindications, potential benefits, potential complications, references to primary literature, and procedural descriptions/diagrams.RESULTS: 21% of sites were sponsored by an academic institution, 61% by a private medical group, 5% by industry firms, and 13% by other organizations. At least one appropriate indication for kyphoplasty was provided in 63% of sites. Only 39% of sites discussed at least one contraindication. No sponsorship subset had more than 50% of sites reporting a contraindication. All sites evaluated offered at least one benefit to treatment with kyphoplasty at a mean of 3.7 benefits discussed per site. In contrast, only 55% of sites discussed at least one complication of treatment with kyphoplasty at a mean of 2.9 complications described per site. 51% of sites mentioned an alternative treatment. Peer reviewed literature was referenced by 23% of sites. Descriptions of the kyphoplasty procedure were included in 93% of sites, and 50% of sites supported descriptions with illustrations or videos.CONCLUSIONS: We demonstrate a staggering inadequacy of quality information publically available over the internet in relation to kyphoplasty. This information was largely incomplete and potentially biased toward the recruitment of patients rather than toward their education. The paucity of well-balanced information
provided by universities and university affiliated hospitals is particularly surprising. While it is possible that sites might be designed under the assumption that a patient will inevitably have to discuss the procedure with a physician, physicians should be familiar with literature demonstrating that patients commonly base decisions off of information garnered on the internet, frequently without discussing it with their doctor. Therefore, it is imperative that physicians provide their patients with complete and accurate information while also emphasizing the stark limitations of publically accessible information over the internet.FDA DEVICE/DRUG STATUS: This abstract does not discuss or include any applicable devices or drugs.
P13. Severe Thoracic Stenosis is Associated with Advanced Degenerative Changes of the Ankle Joint: A Study of 720 Cadaveric Specimens
Joshua T. Anderson, BS1, 2; Alex V. Boiwka, MS1, 2; Uri M. Ahn, MD3; Nicholas U. Ahn, MD2
1Case Western Reserve University School of Medicine, Cleveland, OH, US; 2University Hospitals Case Medical Center, Department of Orthopedic Surgery, Cleveland, OH, US; 3New Hampshire NeuroSpine Institute, Bedford, NH, US
BACKGROUND CONTEXT: Neural compression in the thoracic spine can lead to myelopathy with ataxia and altered gait and subsequent deficits in the lower extremities. As with other conditions causing ataxia, this alteration in gait may ultimately lead to deterioration of lower extremity joints. No studies have investigated the relationship between ankle degeneration and the presence of thoracic stenosis.PURPOSE: Our purpose was to examine the relationship between ankle degeneration and the presence of thoracic spinal stenosis. Since stenosis in the thoracic region can lead to myelopathy, ataxia, and altered gait, and gait changes can lead to ankle deterioration, it makes logical sense that thoracic spinal stenosis could very well lead to ankle degeneration. STUDY DESIGN/SETTING: For this study, we utilized the Hamann-Todd Human Osteological Collection at the Cleveland Museum of Natural History in Cleveland, Ohio.PATIENT SAMPLE: 720 cadaveric subjectsOUTCOME MEASURES: The presence of advanced degenerative changes of the ankle joint as quantified by using the Kellgren-Lawrence classification system.METHODS: 720 adult cadaveric specimens between age 20 and 70 were selected from a collection of skeletal human specimens. All specimens had bony elements which were intact such that appropriate measurements could be made; in addition, all ankle and thoracic elements were present and available for study. In each subject, canal area was calculated at each thoracic level using a previously validated formula. In addition, ankle arthritis was quantified using the Kellgren-Lawrence classification system, as determined by presence and size of osteophytes along the articular surfaces. Linear regression analyses, correcting for confounding factors such as age, sex, race, and height were performed to identify the association between canal area throughout the thoracic spine and presence and severity of hindfoot arthritis.RESULTS: Subjects with severe stenosis were identified as those with a thoracic segment with area less than 2 SD below the mean as noted in a previously published study. A significant negative association was found between presence of severe thoracic
ePOSTER PROCEEDINGS
31

stenosis and ankle arthritis (p=0.04).CONCLUSIONS: The presence of severe thoracic stenosis and decreased canal area is associated with degeneration of the ankle joint. This may be secondary to gait changes which occur in these subjects from the ongoing cord compression.FDA DEVICE/DRUG STATUS: This abstract does not discuss or include any applicable devices or drugs.
P14. Lumbar Stenosis is Associated with Ankle Osteoarthritis and Increased Hindfoot Degeneration: A Post-Mortem Study of 720 Specimens
Joshua T. Anderson, BS1, 2; Alex V. Boiwka, MS1, 2; Uri M. Ahn, MD3; Nicholas U. Ahn, MD2
1Case Western Reserve University School of Medicine, Cleveland, OH, US; 2University Hospitals Case Medical Center, Department of Orthopedic Surgery, Cleveland, OH, US; 3New Hampshire NeuroSpine Institute, Bedford, NH, US
BACKGROUND CONTEXT: Neural compression in the lumbar spine, such as is seen in lumbar stenosis can lead to what is essentially a peripheral neuropathy, as the compression is distal to the conus. This is associated with motor and sensory changes and radicular pain in the lower extremities. This in turn can lead to gait changes. As with other peripheral neuropathies affecting the lower extremities, this alteration in gait may ultimately lead to deterioration of the ankle and hindfoot joints. No studies have investigated the relationships between ankle degeneration, hindfoot degeneration, and the presence of lumbar stenosis. PURPOSE: Our objective was to examine the relationship between ankle degeneration, hindfoot degeneration, and the presence of lumbar stenosis. Since stenosis in the lumbar region can lead to gait changes, and gait changes can lead to ankle/hindfoot deterioration, it makes logical sense that spinal stenosis could very well lead to ankle and hindfoot degeneration. STUDY DESIGN/SETTING: For this study, we utilized the Hamann-Todd Human Osteological Collection at the Cleveland Museum of Natural History in Cleveland, Ohio.PATIENT SAMPLE: 720 cadaveric subjectsOUTCOME MEASURES: The presence of ankle osteoarthritis and/or hindfoot degeneration as quantified using the Kellgren-Lawrence classification systemMETHODS: 720 adult cadaveric specimens age 20-70 were selected from a collection of skeletal human specimens. All specimens had intact bony elements such that ankle, foot, and lumbar elements were present and available for study. In each subject, canal area was calculated at each lumbar level using a previously validated formula. In addition, ankle arthritis was quantified using the Kellgren-Lawrence classification system, as determined by presence and size of osteophytes along the articular surfaces. Hindfoot arthritis (i.e., arthritis across the talonavicular [TN], subtalar [ST], and calcaneocuboid joints [CC]) was quantified using the same classification system, as determined by presence and size of osteophytes along the articular surfaces. Linear regression analyses, correcting for confounding factors of age, sex, race, and height were performed to identify the association between canal area throughout the
lumbar spine and presence and severity of ankle arthritis and hindfoot degeneration.RESULTS: A significant negative association was found between total canal area and severity of ankle arthritis (p = 0.02) as well as severity of hindfoot arthritis of the TN and CC joints (p=0.01). Stenosis in the more distal segments (L4-S1) was more strongly associated with severity of ankle arthritis and hindfoot degeneration than was stenosis at the upper lumbar segments, with higher correlation coefficients. However, both were associated with presence and severity of ankle arthritis and hindfoot degeneration (p<0.05). Subjects with severe stenosis, i.e. canal area less than 2 SD below the mean, had markedly increased degeneration across the ankle and hindfoot joints, even at young ages (ages less than 40).CONCLUSIONS: The presence of lumbar stenosis and decreased canal area is associated with degeneration across the ankle and hindfoot joints. The association was most strongly identified at the lower lumbar levels. This correlates physiologically, as the lower lumbar levels innervate the distal aspects of the lower extremities. Stenosis at these levels can lead to radiculopathy and subsequent gait changes, thus applying new and different forces on the joints of the ankle and hindfoot, leading to increased degeneration across those joints.FDA DEVICE/DRUG STATUS: This abstract does not discuss or include any applicable devices or drugs.
P15. Pedicle-Lengthening Osteotomy: An In Vitro Study to Determine its Cutting Sites
Zong Ping Luo, PhD, MS1; Zhigang Zhang, MD2; Xin Mei3; Huilin Yang, MD, PhD3
1Soochow University Orthopaedic Institute, Suzhou, China; 2Suzhou, China; 3The First Affiliated Hospital of Soochow University, Suzhou, China
PURPOSE: Pedicle-lengthening osteotomy is a new minimally invasive technique for surgical treatment of lumbar spinal stenosis. With the assistance of fluoroscopy, the technique involves making a pedicle passage, pedicle osteotomy from inside the pedicle passage, and lengthening using an implant bilaterally which results in the enlargement of the spinal canal and neural foramen. By largely preserving the normal anatomical structures, the procedure reduces major bleeding, complications, perineural scarring and postoperative instability. The critical component of the procedure is the determination and accuracy of the osteotomy site. The purpose of this study was to test if a fluoroscopic positioning method could be used to guide the osteotomy and to define the cutting site. METHODS: The test was performed on cadaveric vertebra (L3, L4 and L5, n=6). Under lateral C-arm fluoroscopy, a guide pin was driven through the pedicle into the vertebral body. Pedicle osteotomies were then performed bilaterally using a manual bone saw cutting the pedicles from inside the pedicle passages. The one-line sign technique was used to determine the posterior vertebral body line, 2 mm posteriorly to which the targeting transaction site was chosen. With the fluoroscopic guidance and tactile feedback, the surgeon manually operated and controlled the saw until the pedicles were cut circumferentially one at a time. After the pedicles were transected, the pedicle-lengthening implants were screwed into the pedicle passages. The implants lengthened a total of 3 mm, leading to an increase in the area of the spinal canal. 3D CT reconstruction was used to evaluate the
ePOSTER PROCEEDINGS
32

cutting site and to calculate the enlargement of the spinal canal. RESULTS: The manual saw consistently cut the pedicles at the desired sites with 2.3±0.5 mm from the posterior vertebral body line, which was only 0.3 mm from the targeted cutting site. Comparing to the theoretical simulation of CT reconstruction, the difference was insignificant. The spinal canal was also increased in the average of the across sectional area.CONCLUSIONS: The study tested systematically a fluoroscopic guiding method in vitro to be used in the new minimally invasive pedicle-lengthening osteotomy for lumbar spinal stenosis. The average cutting site was 0.3 mm from the targeted site, suggesting the possible clinical application of this technique although further verifications are necessary in vivo.FDA DEVICE/DRUG STATUS: This abstract does not discuss or include any applicable devices or drugs.
P16. Reason for Lawsuit in Spinal Cord Injury Affects Final Outcome
Robert Quigley, MD1; Brent Forrest, MD2; Wayne K. Cheng, MD3
1Colton, CA, US; 2Loma Linda, CA, US; 3Loma Linda University, Loma Linda, CA, US
BACKGROUND CONTEXT: Spinal cord injury has a significant worldwide health and social impact. Over 70% of patients that sue physicians were seriously affected by incidents that gave rise to litigation with long-term effects on work, social life, and family relationships. Spinal cord injury can, no doubt, have a significant impact on the patient’s life in these ways. Evaluating malpractice cases could provide valuable information for the physician who has been sued by a patient with spinal cord injury.PURPOSE: The purpose of this study is to evaluate whether the reason a physician is sued has an effect on the likelihood of losing a lawsuit.STUDY DESIGN/SETTING: We conducted a retrospective cohort study.PATIENT SAMPLE: We queried a large, national medicolegal research database (VerdictSearch) for cases involving spinal cord injury from the years 2000-2010.OUTCOME MEASURES: Patient demographic information including age, sex, occupation type, and level of injury was collected. The exposures of interest were the reasons that the physician was sued. The reason for the suit was categorized as either for an error in diagnosis or an error in treatment. The outcomes were either a defense verdict (win) or a plaintiff verdict/settlement (loss). We used Chi-Square test to analyze the proportions of cases in each group with a significance level of <0.05 and then calculated relative risk.METHODS: The database query returned 86 cases which were individually reviewed by 2 separate reviewers. Each case situation was evaluated independently and the reason for the lawsuit was characterized as either an error in diagnosis or an error in treatment. There was 100% agreement between the 2 reviewers. Nine cases were excluded because not enough demographic information was available and 4 cases were excluded for irrelevance. This left 73 cases that were included in the study. After analyzing each case, we had 25 cases in the error in treatment
group and 48 cases in the error in diagnosis group.RESULTS: There were no significant difference in demographic information between the two groups.For physicians who had been sued for an error in treatment, 11 of 25 cases (44%) lost the lawsuit. For physicians who had been sued for an error in diagnosis, 38 of 48 cases (79%) lost the lawsuit. This difference was significant (p=0.002). After calculating the relative risk, physicians sued for an error in diagnosis are 1.80 times more likely to lose a lawsuit than physicians sued for an error in treatment. The 95% confidence interval is 1.13 to 2.87.CONCLUSIONS: Physicians are sued by patients who sustain spinal cord injury. Our study shows that there is a relationship between being sued for an error in treatment and a defense verdict. Physicians should be very careful not to miss a diagnosis of spinal cord injury and yet not be afraid to treat patients which spinal cord injury for fear of litigation. FDA DEVICE/DRUG STATUS: This abstract does not discuss or include any applicable devices or drugs.
P17. Utility of Preoperative MRI Co-Registered with Intraoperative CT Scan for the Resection of Complex Tumors of the Spine
Kenneth P. D’Andrea, DO1; Daniel K. Fahim, MD2
1Oakland University, William Beaumont School of Medicine, Royal Oak, MI, US; 2Baylor College of Medicine, Houston, TX, US
BACKGROUND CONTEXT: Complete surgical resection is known to provide the best prognosis when treating complex tumors of the spine. The anatomy of the cervical spine and the extensive involvement often present by the time these lesions are discovered can make total resection challenging. A novel technique combining preoperative and intraoperative imaging for optimal intraoperative navigation can serve as an additional tool to facilitate complete and safe tumor resection.PURPOSE: To describe the utility of preoperative stealth MRI merged with intraoperative CT as a novel tool in the resection of complex tumors of the spine.STUDY DESIGN/SETTING: Case SeriesPATIENT SAMPLE: Four patients with complex cervical spinal tumors in which preoperative MRI merged with intraoperative CT was used for navigation to safely and completely resect the tumor and accurately achieve stabilization of the spine. These patients presented to our institution between July of 2011 and June of 2013.OUTCOME MEASURES: Preservation or restoration of neurological function, decompression of neural elements, accurate placement of instrumentation, extent of tumor resection, and pain relief.METHODS: Preoperative stealth MRI was co-registered with intraoperative CT for accurate, real-time, intraoperative navigation for complete resection of complex tumors of the cervical spine. The utility of this new technique is discussed.RESULTS: Stealth MRI co-registered merged with intraoperative CT allows for accurate visualization of tumor boundaries, osseous anatomy, and surrounding soft tissue structures. Total resection of extensive spinal tumors involving the anterior and posterior elements can be effectively achieved utilizing this technique.CONCLUSIONS: Preoperative stealth MRI with intraoperative CT can serve as a useful intraoperative imaging modality for facilitating complete resection of complex spine tumors.FDA DEVICE/DRUG STATUS: This abstract does not discuss or include any applicable devices or drugs.
ePOSTER PROCEEDINGS
33

P18. Lateral Transpsoas Access to the Lumbar Spine for Revision Surgery
Luiz H. Pimenta, MD, PhD; Rodrigo A. Amaral, MD; Luis Marchi, MS; Thiago P. Coutinho, MD; Thabata Bueno; Leonardo Oliveira, MD; Rubens Jensen, MD
Instituto de Patologia da Coluna, São Paulo, Brazil
BACKGROUND CONTEXT: Revision in spine surgery has been traditionally associated with significant morbidity and complications (vessel injury, blood loss, muscle damaging, adherence and neural risk). A revision using lateral transpsoas approachoffers the advantages associated with less invasive surgery, direct access to the interbody space; while avoiding vascular, abdominal, and retroperitoneal structures which would be placed at risk in a scarred surgical field.PURPOSE: Describe and discuss revision surgery for the anterior column through a lateral transpsoas approach (LLIF).STUDY DESIGN/SETTING: Retrospective study in a single center experience. PATIENT SAMPLE: Revision of Failed TDR – 19 patients that presented with failed artificial lumbar disc prosteses within 10 Charité cases, 2 Maverick, 1 Phisio-L, 1 Triumph and 5 Lateral Disc. Revision of Interbody Fusion Cage – 3 cases (1 TLIF, 2 LLIF); Revision of Nucleous Replacement – 23 cases; and Addition of XLIF after Prior Posterior Fixation – 9 cases.OUTCOME MEASURES: Decision making, technical details, intraoperative routes, and complications.METHODS: The cases required revision surgery by LLIF approach. The minimally invasive disruptive lateral transpsoas approachac acess has been used for disc removal and level fusion using cages in standalone construction, with supplemental lateral plates or pedicle screws. RESULTS: No major surgical complication occurred, 1 case of iliac vein tear-repaired and one case of partial ureter rupture. Mean surgical time was 139 minutes. Outcome assessment (VAS and ODI) showed important clinical improvement. Contralateral or ipsilateral access was used depending on the type of failure, correction need, or previous surgeries. Operative technique and tips and tricks for removal included of prosthesis with keel, core removal, or even displacement for revision instrumentation with special osteotomes/broaches to cut channels around previous implants, spiral extractor or special hooks. The surgeries were undertaken within the first few weeks of the primary surgery or after a few months have passed due to risk of excessive bleeding.CONCLUSIONS: Retrieval surgery in failed lumbar surgery is a demanding procedure, often technically difficult, and carries an incidence of morbidity. The LLIF can be a safe and effective strategy for minimally disruptive revision surgery at the L2-L3, L3-L4 and L4-L5 levels.FDA DEVICE/DRUG STATUS: This abstract does not discuss or include any applicable devices or drugs.
P19. Analysis of Local Sagittal Parameters in a Stand-Alone ALIF for L5S1 DDD: Minimum Two-Year Follow-Up
Luiz H. Pimenta, MD, PhD; Rodrigo A. Amaral, MD; Luis Marchi, MS; Leonardo Oliveira, MD; Thabata Bueno; Thiago P. Coutinho, MD; Rubens Jensen, MD
Instituto de Patologia da Coluna, São Paulo, Brazil
BACKGROUND CONTEXT: Sagittal decompensation following long adult lumbar spinal instrumentation and fusion to S1 occurs in high rates, when surgical procedures for degenerative disc disease usually don’t aim to restore local lordosis parameters. Postoperative improvement in L5 incidence and slip angle has been correlated with better outcomes. PURPOSE: The purpose of this paper is to analyze the contribution of a standalone L5S1 interbody procedure toward the treatment of degenerative disc disease and study resultant local sagittal parameters. STUDY DESIGN/SETTING: A prospective, non-randomized, single center study with up to three-year follow-up with a minimum follow-up of 24 months.PATIENT SAMPLE: 28 patients, mean age 50.1 y/o (31-82, range), mean BMI 26.1.OUTCOME MEASURES: Self-assessment questionnaires such as Visual Analogue Scale and Oswestry disability index were applied in all follow up visits. Radiological measurements such as focal lordosis at L4-L5 and L5-S1, and sacral slope were prospective collected. Intraoperative data was also recorded. METHODS: Radiological parameters were measured on lateral lumbar radiographs in standing position: L1S1 and L4L5 lordosis, and sacral slope (SS). Through a mini-ALIF procedure, L5S1 stand-alone interbody fusion was done with a lordotic cage with three looking screws. RESULTS: No intraoperative complications occurred. Two cases (7.1%) evolved with abdominal seroma in the incision. Average surgical duration was 120 minutes and average blood loss, 130cc. Two patients evolved with retroperitoneal hematoma and underwent drainage. Mean preop VAS back score changed from 71 to 34mm at 12-month evaluation (p<0.002). Mean preop ODI score changed from 45.3 to 29mm at 12-month evaluation (p<0.01). Focal lordosis at L5-S1 improved from average 18.6° to 26.8° (p<0.001), focal lordosis at L4-L5 decreased from 24.7° to 20.7° (p<0.001). Mean SS improved from average 30.3° at pre-op to 35.3° at last follow-up (p<0.001), indirectly showing PT decrease, once SS and PT are complimentary measurements. CONCLUSIONS: Clinical symptoms were successfully treated using stand-alone anterior interbody fusion without posterior decompression and supplementation. Stand-alone mini-ALIF provides a biomechanically stable solution with minimal complications and morbidity. Local sagittal parameters were significantly improved to a more harmonic distal lumbar spine, fact that has been increasing recognized on back pain and adjacent segment degeneration.FDA DEVICE/DRUG STATUS: This abstract does not discuss or include any applicable devices or drugs.
ePOSTER PROCEEDINGS
34

P20. Clinical and Radiological Consequences of Interbody Cage Subsidence
Luiz H. Pimenta, MD, PhD; Luis Marchi, MS; Rodrigo A. Amaral, MD; Thiago P. Coutinho, MD; Leonardo Oliveira, MD
Instituto de Patologia da Coluna, São Paulo, Brazil
BACKGROUND CONTEXT: Cage subsidence is a phenomenon found in standalone constructions, but its radiological characteristics and clinical correlation are yet unknown.PURPOSE: The main goal of this work is to describe a new grading system for cage subsidence, describing when and how it occurs, also analyzing its clinical consequences.STUDY DESIGN/SETTING: Retrospective analysis of a prospective clinical study.PATIENT SAMPLE: Seventy-four patients (57.2 ± 14.8 y/o; BMI 24.9 ± 2.5).OUTCOME MEASURES: Clinical outcomes were assessed by ODI and VAS up to 24 months.METHODS: Standing lateral radiographs were performed preoperatively, postoperatively at 1 and 6 weeks, 3 and 12 months. Standalone short-segment lateral lumbar interbody fusion was investigated. Subsidence was graded as grade 0; 25-49%– grade I; 50-74%– grade II; 75-100%– grade III. RESULTS: Subsidence was early detected at 6-week and didn’t significantly progressed. Major subsidence defined as 50% or more of cage settling (grade II or III) occurred in 22% of all patients based on 12-month radiographs (22 of 98 total levels). Moreover, subsidence was seen to occur predominantly (68% of the cases) in the inferior endplate of the assessed intervertebral disc. High-grade subsidence was correlated with transient axial back pain at 6-week follow-up point. In grade 0 and I cases disc height gain was observed in postoperative radiological assessments, in contrast to grade II and III cases. Lordosis gain was better achieved with lo-grade subsidence. Risk factors for high-grade subsidence were advanced age and female gender. CONCLUSIONS: Cage subsidence has the potential to results in loss of disc height, stenosis, sagittal malignment, and adjacent segment disturbances. Subsidence must be carefully evaluated at early follow-up. FDA DEVICE/DRUG STATUS: This abstract does not discuss or include any applicable devices or drugs.
P21. Complications in Lateral Transpsoas Access in the Lumbar Spine
Luiz H. Pimenta, MD, PhD; Rodrigo A. Amaral, MD; Luis Marchi, MS; Leonardo Oliveira, MD; Thabata Bueno; Thiago P. Coutinho, MD; Rubens Jensen, MD
Instituto de Patologia da Coluna, São Paulo, Brazil
BACKGROUND CONTEXT: XLIF gains popularity among spine surgeons as a less invasive alternative to open and endoscopic anterior lumbar interbody fusion. This approach avoids great vessel mobilization, minimizes the risk for visceral and vascular complications, avoids direct posterior muscle disruption, and, in males, retrograde ejaculation. It provides broad discectomy and placement of a wide cage with increased biomechanical support. PURPOSE: Although its benefits, the approach has shown some complications, which are not well covered by the existing literature, and so, remain not well known and may be a barrier to a safe and consented surgery indication.STUDY DESIGN/SETTING: Literature update and retrospective review of patients from a single center study. PATIENT SAMPLE: This work was developed as a literature update and has also some unique and non reported examples from a single center with more than 1000 cases.METHODS: Literature review and retrospective analysis of more than 1000 cases from a single center study.RESULTS: The complications are as follows, from most common to very rare occurrences: Transient psoas-related symptoms (10-40%); Transient plexus-related symptoms (10-40%); Subsidence (10-20%); Psoas hematoma (5%); Partial cage migration (2%); Vertebral body fracture (2%); Incisional Hernia/abdominal wall paresis (2%); Infection (2%); Urologic / bowel / vascular /neural injury (1%); Pulmonar Embolism (<1%); Death (<1%).CONCLUSIONS: The procedure must be done following the surgical steps, using proper material and neuromonitoring. Although it has been shown that the access route is relatively safe, transpsoas approach has some potential adverse effects and complications that are not totally well understood yet and deserve detailed reporting and study. FDA DEVICE/DRUG STATUS: This abstract does not discuss or include any applicable devices or drugs.
ePOSTER PROCEEDINGS
35

P22. Evaluation of the Calcium Phosphate Cement as Bone Graft for Lumbar Interbody Fusion
Luiz H. Pimenta, MD, PhD; Rodrigo A. Amaral, MD; Luis Marchi, MS; Leonardo Oliveira, MD; Thabata Bueno; Thiago P. Coutinho, MD; Rubens Jensen, MD
Instituto de Patologia da Coluna, São Paulo, Brazil
BACKGROUND CONTEXT: Autograft has traditionally been the “gold standard” for fusion, but generates significant morbidity and limitations. The use of recombinant bone growth factors have beneficial results compared to the autograft, but its price is still a limiting factor.PURPOSE: The aim of this study is to evaluate the clinical and radiological results of a bone graft option made from calcium phosphate cement in lumbar interbody fusion.STUDY DESIGN/SETTING: Prospective, non-randomized single center study.PATIENT SAMPLE: 68 patients (59.4±11.2 y/o; 105 levels) with lumbar interbody disc disease.OUTCOME MEASURES: The clinical evaluations included a physical examination for the lower limb motor and sensory function and self-assessment questionnaires using ODI and VAS for axial pain and legs at preoperative and postoperative visits.METHODS: Subjects were submitted to discectomy and interbody fusion by retroperitoneal lateral approach packed with molded calcium phosphate cement. Clinical and radiological (RX/CT/ MRI) data were analyzed in the pre-operative and postoperative visits with minimum of 12 months (max 36 months).RESULTS: The mean duration of surgery was 112.4 minutes (average 70 minutes per level) with <50ml of blood loss. Clinical improvement was observed in VAS going to an average of 55 to 31 in the last visit (about 45% of improvement); and ODI, 54 to 26 (about 52% of improvement). The radiological observation showed some graft reabsorption in 73% of levels in the 12 months evaluation. There were no pseudoarthrosis cases but only incomplete bone growth. There was less loss of bone graft in impaction after semi hardened cement, producing less loss of material when compared to other granular formulations. Increased metabolic reactions - bone remodeling evidenced by a T2 hyperintensity in MRI images - were observed in 20% of the cases.CONCLUSIONS: This kind of grafting preparation is safe and efficient to achieve surgical objectives and can be considered for intersomatic arthrodesis. FDA DEVICE/DRUG STATUS: This abstract does not discuss or include any applicable devices or drugs.
P23. L5S1 Low-Grade Spondylolisthesis Treated by ALIF: Local Lordosis Correction
Luiz H. Pimenta, MD, PhD; Rodrigo A. Amaral, MD; Thiago P. Coutinho, MD; Luis Marchi, MS; Leonardo Oliveira, MD; Thabata Bueno; Rubens Jensen, MD
Instituto de Patologia da Coluna, São Paulo, Brazil
BACKGROUND CONTEXT: Spondylolisthesis may cause local instability, facet distraction, and central/foraminal stenosis, and at L5-S1 the pathology can be worsened by the share force. Good clinical outcomes are related with restoration of correct values for the pelvic position-dependent parameters. Additionally, as the lordosis increases at the levels above the spondylolisthesis, this fact subsequently increase posterior stress on facet joints.PURPOSE: The purpose of this paper is to study radiological and clinical results of a mini-ALIF option for the treatment of L5S1 low-grade spondylolisthesis.STUDY DESIGN/SETTING: Prospective cohort study.PATIENT SAMPLE: Analysis of 21 subjects (mean age 46 years; 11 females) that underwent mini-ALIF for the treatment of spondylolisthesis.OUTCOME MEASURES: Radiological spinopelvic parameters were measured at preop and final follow-up point, and functional evaluation was made using the ODI, VAS and EQ-5D.METHODS: L5S1 low-grade spondylolisthesis was treated through a standalone mini-ALIF procedure. Enrolled patients consisted of ones with spondylolisthesis and minimum follow-up of 12 months after surgery.RESULTS: Mean surgical time was 111 minutes. Mean preop VAS back score changed from 69 to 38mm at 12-month evaluation (p<0.004); mean preop ODI score changed from 46 to 24 mm at 12-month evaluation (p<0.009); mean preop EQ-5D score changed from 0.48 to 0.73 at 12-month evaluation (p<0.004). Preoperative x-rays evidenced that the studied patient group had preop 23% of mean slippage, and the procedure was seen to achieve a 53% correction. Pelvic parameters were also significantly improved with the interbody fusion procedure, sacral slope from preop 41° to 45º (p<0.001), L5-S1 lordosis increased from 23° to 31° (p<0.001), L4-L5 lordosis decreased from 28° to 25° (p=0.03) and L5 takeoff had a modest but significant change from -19° to -16° (p=0.027).CONCLUSIONS: L5S1 low-grade spondylolisthesis was treated using minimally invasive anterior interbody fusion. Good clinical results were achieved, and concomitantly it was observed restoration of values for the pelvic position-dependent parameters, correction that may be benefit in preserving the adjacent segments (L4L5 and sacro-iliac joints).FDA DEVICE/DRUG STATUS: This abstract does not discuss or include any applicable devices or drugs.
ePOSTER PROCEEDINGS
36

P24. MIS Lumbar Fusion in an Ambulatory Surgery Center (ASC): Safety, Treatment Outcomes and Comparison with Inpatient Lumbar Fusion
William D. Smith, MD
Western Regional Center for Brain & Spine Surgery, Las Vegas, NV, US
BACKGROUND CONTEXT: ASCs are regularly utilized for procedures with low risk profiles, short ORT, and minimal needs for extended postoperative observation. Recent advancements in minimally disruptive approaches for lumbar interbody fusion have shown, with minimal approach morbidity, that early postoperative discharge is safe and reproducible in select patients.PURPOSE: The object of this work was to examine early safety and treatment outcomes following a mini-open lateral transpsoas approach for lumbar fusion performed at an ASC.STUDY DESIGN/SETTING: Retrospective review of single cohort from a single institution.PATIENT SAMPLE: 54 consecutive patients were treated at an ASC with extreme lateral interbody fusion (XLIF). Mean age was 50.6 years, 31% were female, BMI was 28.3, 41% were smoked, and 39% had previous surgery. 80 total levels were treated from L1-S1, with L1-5 treated with XLIF and L5-S1 treated with AxiaLIF (7 cases, 9%) or MIS TLIF (9 cases, 11%). One-, two- and three-level procedures were performed in 57%, 37%, and 6% of cases, respectively. The most common fixation method was anterolateral plating (37%).OUTCOME MEASURES: Treatment (ORT, EBL, & LOS), complication, hospitalization, or ER visits data. Patients also completed a post-discharge survey to assess general condition and pain.METHODS: Retrospective chart review.RESULTS: Mean ORT, EBL, and LOS were 86 mins (range 28–150), 71cc (range 20–400), and 5:46 (range 2:35–20:15). No intraoperative complications were observed. Two (3.7%) hospitalizations occurred: One transfer for urinary retention, which resolved in-hospital, A second was discharged admitted for uncontrolled pain following a three-level fusion. Two (3.7%) ER visits occurred, one for testicular pain, and the other for a fever on post-op day 2 which resolved without infection. Side effects of the approach included hip flexor weakness in three (5.6%) patients, anterior thigh discomfort in 10 (18.5%) patients. No perioperative reoperations occurred. 91% of patients completed the postoperative questionnaire an average of 4 days postoperative. Describing their current condition, 92% rated themselves as excellent (14.3%) or good (77.6%) and fair or poor in 8% (6.1% fair, 2% poor) of patients. Pain was none or slight in 67% of cases (8.3% none, 58.3% slight) while 25% reported moderate and 6.3% severe pain. Between one-level and two- and three-level cases, elevated ER visits and hospitalizations were observed in the two- and three-level (3.2% vs. 4.3%; 0% vs. 8.7%, respectively). Excellent or Good general postoperative condition were similar (93% vs. 91%), and pain was less for one-level patients compared to two- and three-level cases (None/Slight: 73% vs. 59%). A concurrent series of 61 one-level XLIFs and 48 one-level ALIFs performed inpatient showed postoperative rehospitalizations in 2.7% and 6.8% of cases, compared to 0% for the ASC one-level XLIFs.
CONCLUSIONS: Highly selected patients (by health and indication) can safely be treated in ASCs with XLIF or other MIS approaches without increased hospitalizations or ER visits compared to those treated as inpatients. One-level procedures appear to be slightly more favorable than two- or three-level cases in an ASC. With ASCs receiving 65% to 70% of inpatient coding, due to ASC modifiers, this has the potential to both substantially decrease payer costs in highly select patients and procedures, while providing patients with a safe surgery and ability to spend the early postoperative period recovering at home.FDA DEVICE/DRUG STATUS: This abstract does not discuss or include any applicable devices or drugs.
P25. Complications with rhBMP-2 in Lateral Approach Spine Surgery
William D. Smith, MD1; Luiz H. Pimenta, MD, PhD2; Juan S. Uribe, MD3
1Western Regional Center for Brain & Spine Surgery, Las Vegas, NV, US; 2Instituto de Patologia da Coluna, São Paulo, Brazil; 3University of South Florida, Tampa, FL, US
BACKGROUND CONTEXT: Recently, risks associated with the use of rhBMP-2 have been more closely examined in spine fusion. The risks have largely been attributed to an early inflammatory reaction (resorptive phase) which has led, in some studies, to increased rates of subsidence, osteolysis, and injury to neural structures.PURPOSE: This work examines cases of profound rhBMP-2-related complications in anterior lumbar interbody fusion performed using a lateral approach.STUDY DESIGN/SETTING: Multi-center retrospective case series.PATIENT SAMPLE: Six patients with BMP-related complications from 540 extreme lateral interbody fusion (XLIF) patients.OUTCOME MEASURES: Case descriptions and outcome.METHODS: Retrospective review.RESULTS: Out of 540 patients treated with XLIF and BMP from 2004 through 2011, six (6)(1.1%) cases of severe complication specific to the lateral approach following fusion with rhBMP-2 were identified. Cases with subsidence or other radiographic findings which could have caused the complications were excluded. Cases: Patient 1: L4-5 XLIF using BMP. Postoperative lower extremity motor evaluation was without deficit. By six weeks postoperative the patient developed right side quadriceps weakening. By three months post-operative, the patient was wheelchair bound with no right quadriceps function (1/5 strength), confirmed by EMG. By 5 years postoperative, the complete deficit remains. Resulting diagnosis: Right femoral nerve injury caused by chemical neuritis during rhBMP-2 inflammatory phase. Patient 2: L2-5 XLIF with lateral plating and BMP. Six-month postoperative CT showed extensive ectopic bone formation through the psoas muscle and L4-5, the patient had severe right leg pain. The patient required revision surgery for removal of the lateral plate and lateral screws with exploration of the psoas for removal of ectopic bone (Figures 1). Patient 3: L2-5 XLIF with rhBMP-2. Postoperative motor evaluation showed full strength. By 2-weeks postoperative, the patient developed profound left quadriceps weakness (2/5) with MRI showing psoas inflammation without hematoma or fluid collection. Quad weakness resolved by 3 months postoperative following aquatic and physical therapy. Patient 4. 52yo male treated for L4-5 grade I spondylolisthesis with XLIF, lateral plate, and interspinous plate. Follow-up CT showed significantly ectopic
ePOSTER PROCEEDINGS
37

bone within the iliopsoas muscle contralateral to the approach side. There were no symptoms associated with the bone growth and no revision was performed. Patient 5. 56yo male treated with an L4-5 XLIF. Immediate postoperative evaluation showed no motor or sensory deficits. On postoperative day 7, an anterior femoral cutaneous branch deficit was observed, which improved 6 months postoperatively. Patient 6. 44yo female treated with L4-5 XLIF following a failed nucleus replacement. No supplemental instrumentation was used. At 6 months postoperative, patient developed severe (10/10) right left pain (contralateral to approach) and back pain. CT showed ectopic bone growth into the neural foramen, which required a foraminotomy to address at 12 months postoperative.CONCLUSIONS: These cases of rhBMP-2 complications are consistent with recent literature, especially in similar reports of emerging radicular symptoms within several weeks of surgery in PLIF and TLIF performed with rhBMP-2. The mechanism for extra-discal damage, in this case, is assumed to be by migration of rhBMP-2, in an overly-active inflammatory phase, to the surrounding soft tissue – in these cases to the adjacent psoas, lumbar plexus, and neural foramen.FDA DEVICE/DRUG STATUS: This abstract does not discuss or include any applicable devices or drugs.
P26. Neurologic Complications in Extreme Lateral Interbody Fusion (XLIF): A Comparative Analysis of Levels L2-3, L3-4 and L4-5
William D. Smith, MD
Western Regional Center for Brain & Spine Surgery, Las Vegas, NV, US
BACKGROUND CONTEXT: Studies of relevant neural anatomy to the lateral approach have suggested that motor nerves of the lumbar plexus are often at risk of injury, especially at L4-5. Reported complication rates of neural injury with the extreme lateral interbody fusion (XLIF) approach, however, are low (0.7%-2.9%) due to the adherence to advanced neuromonitoring systems integrated with the procedure.PURPOSE: The objective of this study was to examine neural (sensory and motor) deficit rates following XLIF.STUDY DESIGN/SETTING: Retrospective review of a single site series.PATIENT SAMPLE: A total of 252 patients were treated for single-level cases of L2-3, L3-4, or L4-5 lumbar disease treated with XLIF from 2004 through 2008.OUTCOME MEASURES: Patient characteristic, treatment, and complication and resolution data.METHODS: Demographic, treatment, and complication data were collected retrospectively in single-level cases of L2-3, L3-4, or L4-5 lumbar disease treated with XLIF at a single institution. Average age was 58.5 years and 56.7% were female. L2-3 was treated in 31 cases (12.3%), with L3-4 treated in 64 (25.4%) and L4-5 in 157 (62.3%) cases. Pedicle screws were used in 70.2%, anterolateral plating in 7.9%, and no supplemental fixation was used in 21.8% of cases.RESULTS: In total, 25 (9.9%) patients experienced postoperative anterior thigh/groin sensory changes (numbness, tingling), 30
(11.9%) patients experienced anterior thigh/groin pain, and 2 (0.8%) patients exhibited new lower extremity motor deficits (foot drop) following XLIF. Thigh/groin sensory changes resolved completely in 76% of patients, improved in 20%, and were unchanged in 4% of cases by 12 weeks postoperative. Anterior thigh/groin pain completely resolved in 83.3%, improved in 13.3%, and no change occurred in 3.3% of cases by 12 weeks postoperative. Both postoperative motor deficits resolved, one at 12 weeks, the other at 12 months. When analyzed by level, 62.3% (118) of cases were treated at L4-5 and these patients experienced only 56% (14) of the thigh sensory events, 53% of the thigh pain events, and 100% (2) of the postoperative motor deficits. Of the 64 (25.4%) L3-4 patients, 9 patients experienced thigh sensory changes (36% of total thigh sensory change patients) and 9 patients experienced postoperative thigh pain (30% of total thigh pain patients), without any motor deficits observed. Finally, of those 31 (12.3%) patients treated at L2-3, they included 8% (2) of the thigh sensory change patients and 17% (5) of the thigh pain patients without any motor deficits.CONCLUSIONS: Thigh/groin sensory changes were relatively well distributed between L2-3, L3-4, and L4-5. Despite the majority of cases occurring at L4-5, a relatively low motor injury rate was observed (0.8%) even with more posterior docking for interbody spacer placement. Sensory and painful thigh/groin symptoms, however, are likely caused by irritation of the genitofemoral nerve, which runs on the anterior half of the lateral disc space from L2-5. In the case where a more anterior docking approach is used to avoid the lumbar plexus, this theoretically increases the likelihood of injury to the genitofemoral nerve which cannot be monitoring using electromyography.FDA DEVICE/DRUG STATUS: This abstract does not discuss or include any applicable devices or drugs.
P27. Acute and Hyperacute Corpectomy for Traumatic Burst Fractures Using a Mini-Open Lateral Approach
William D. Smith, MD
Western Regional Center for Brain & Spine Surgery, Las Vegas, NV, US
BACKGROUND CONTEXT: Historically, treatment of spinal burst fractures within 24, sometimes 72, hours from injury has been considered an “acute” treatment timeframe, and a rare occurrence when using conventional surgical approaches. Factors affecting time to treatment include patient polytrauma triage as well as multiple surgical specialty and hospital resource coordination, which regularly delay early treatment. With the advent of the mini-open lateral approach for thoracolumbar corpectomy, where anterior column access can be performed in both a minimally disruptive fashion but also without the need for an approach or general surgeon (as in thoracotomies), resource coordination required to treat these complex cases is theoretically minimized. PURPOSE: The purpose of this study was to examine the feasibility of acute (<24 hours) and hyper-acute (<8 hours) treatment of thoracolumbar burst fractures.STUDY DESIGN/SETTING: Retrospective chart review at a level I trauma center.PATIENT SAMPLE: 9 consecutive trauma patients treated within at an average of 7 hours from injury with MIS lateral corpectomy.OUTCOME MEASURES: ASIA, treatment variables.METHODS: Chart review was performed at a Level I trauma center on patients admitted and treated within 24 hours with a mini-open
ePOSTER PROCEEDINGS
38

lateral corpectomy for traumatic spinal pathology. Of 12 patients who met these criteria, 9 (75%) had evaluable preoperative, perioperative, and postoperative data and were included in the study. Patients were mostly male (78%), had a mean age of 31 years, and had a mean BMI of 24. 33 of patients used tobacco, 33% used illicit drugs, and significant medical comorbidities were present in only one patient. Five patients were treated with a wide-footprint expandable Titanium (Ti) vertebral body replacement (VBR) device, while four were treated with a cylindrical-endplate expandable Ti VBR device. Three patients received posterior transpedicular screw and rod fixation, while all but one patient received anterolateral fixation. Biologic materials included autograft (local bone) in all cases, supplemented with BMA in five cases, BMP in three, and a ceramic graft extender in one case. Real-time, intraoperative neuromonitoring was used in all cases.RESULTS: Burst fractures occurred at T8, T12, L1 (3), L2, and L3 (3). Patients presented with ASIA scores of A (3), C (3), and D (3), including 3 complete lower extremity paraplegias. Average time from injury to admission to the hospital was 1.8 hours (110 minutes), with an average time from the ER to OR of 4.7 hours, for a 6.6 hour average time from injury to start of surgery. Five of nine patients were treated within three hours from hospital admission, while three were treated within 8 hours of hospital admission. Only one was treated at longer than 8 hours from hospital admission (15 hours). From time of injury to start of surgery, three patients were treated within 4 hours, four within 8 hours, and two within 15.5 hours. OR time averaged 119 minutes, for an average total time from injury to end of surgery of 8.5 hours. Blood loss averaged 900 mL, without intraoperative complication. One postoperative complication occurred, a localized pleural effusion which was treated with a chest tube and resolved without sequelae. One patient developed an asymptomatic inferior vertebral body compression fracture following VBR (cylindrical endplate) cage subsidence. Length of hospital stay averaged 6.1 days, though when excluding two outliers who had extended hospitalizations (9 and 17 days) due to treatment for other injury-related trauma, the average hospital say was 4.1 days. Average postoperative follow up was 8.5 months, though one patient was lost to follow up. At last follow up, six of the eight (75%) patients experienced at least one ASIA grade improvement, with four patients achieving full (ASIA E) resolution, and three patients achieving near complete (D) resolution. Two patients showed no neurologic improvement, with one persistent complete lower extremity paraplegia and one with an ASIA D score at last follow up.CONCLUSIONS: These results suggest that modern minimally invasive approaches, using direct visualization, allow immediate decompression through hyper-acute (<8 hours) treatment of spinal trauma in eligible patients. Additionally, low perioperative and postoperative morbidity allow for hastened postoperative recovery and treatment for polytrauma.FDA DEVICE/DRUG STATUS: This abstract does not discuss or include any applicable devices or drugs.
P28. A Prospective Study of Reliability of a Novel Classification System for Thoracolumbar Injuries in Children and Adolescent
Xie En, MD1; Ding-Jun Hao, MD2
1Hong Hui Hospital, Xi’an Jiaotong University College of Medicine, Xi’an, Shan Xi, China; 2Xi’an Honghui Hospital, Xi’an, Shaanxi, China
BACKGROUND CONTEXT: The CATLIS is a recently introduced classification system for thoracolumbar spinal column injures in immature population designed to simplify injury classification and facilitate treatment decision making. Before being widely adopted, the reliability of the CATLIS must be studied.PURPOSE: To determine the reliability of the CATLIS system.STUDY DESIGN/SETTING: Prospective study of 2 spine surgeons rating 277 clinical cases of thoracolumbar spinal injuries using the Thoracolumbar Injury Score in children and adolescent (CATLIS) and then re-rating the cases in a different order 2 year later.METHODS: A total of 277 cases of thoracolumbar spinal trauma were distributed on imaging data to 2 attending spine surgeons, including clinical/radiographic data, details of the CATLIS, and a scoring sheet in which cases would be scored using the system. Since 2000, clinical data, surgical methods, efficacy and mechanism of 277 children and adolescents with thoracolumbar spine injury treated in Honghui hospital of Xi’an Jiaotong University School of Medicine. l were analyzed and compared. I a-c 137 cases, II a 60 cases, II b 37 cases, II c 43 cases. Treatment is in accordance with easy typing method of Honghui hospital of Xi’an Jiaotong University School of Medicine. The principles and systematic methods of analysis of such damage was emphasized. Clinical, physiological and psychological effects were observed. Intraobserver and interobserver reliability was calculated for CATLIS components, total score, and surgeon’s treatment decision using the Cohen unweighted kappa coefficients and Spearman rank-order correlation.RESULTS: According to easy typing method of Honghui hospital of Xi’an Jiaotong University School of Medicine. In 277 patients, clinical, imaging, and psychology had achieved good results.Interrater reliability assessed by generalized kappa coefficients was 0.40 +/- 0.03 for injury mechanism, 0.93 +/- 0.03 for neurologic status, 0.31 +/- 0.01 for ACTLIS total, and 0.61 +/- 0.01 for treatment recommendation. Respective results using the Spearman correlation were 0.33 +/- 0.034, 0.93 +/- 0.02, 0.49 +/- 0.02, 0.63 +/- 0.013, and 0.53 +/- 0.03. Surgeons agreed with the ACTLIS recommendation 97.74% of the time. Intrarater kappa coefficients were 0.59 +/- 0.03 for injury mechanism, 0.943 +/- 0.01 for neurologic status, 0.47 +/- 0.01 for ACTLIS total, and 0.64 +/- 0.03 for treatment recommendation. Respective results using the Spearman correlation were 0.730 +/- 0.03, 0.97 +/- 0.01, 0.32 +/- 0.035, 0.79 +/- 0.03, and 0.63 +/- 0.03.CONCLUSIONS: Simple type of CATLIS is easy to grasp. It applies to children and adolescents treatment of thoracic and lumbar spine injury to good effect. The ACTLIS has good reliability and compares favorably to other contemporary thoracolumbar fracture classification systems in children and adolescent.FDA DEVICE/DRUG STATUS: This abstract does not discuss or include any applicable devices or drugs.
ePOSTER PROCEEDINGS
39

P29. A Study on the Surgical Techniques to Treat Thoracic Spine Lesions with a Sneak Resection Approach for the Anterior Sternal Upper Part: A New Surgical Technique
Xie En, MD1; Ding-Jun Hao, MD2
1Hong Hui Hospital, Xi’an Jiaotong University College of Medicine, Xi’an, Shan Xi, China; 2Xi’an Honghui Hospital, Xi’an, Shaanxi, China
BACKGROUND CONTEXT: Surgical pathology in the region of the upper thoracic spine (T1-4) is uncommon compared with other regions of the spine. Often times posterior and posterolateral approaches can be used, but They have a huge flaw: Cancer and tuberculosis are not fully exposed, pathogens and tumor were drawn into the rear by latrogenic manipulation.PURPOSE: To investigate the surgical approach and clinical outcomes of a sneak resection approach for the anterior sternal upper part during thoracic spine surgery.STUDY DESIGN/SETTING: Retrospective comparative cohort study.METHODS: The upper thoracic lesions were treated with a sneak resection approach at the anterior sternal upper part. 57 patients were treated between July 2005 and September 2010, including 28 males and 29 females who were aged between 27 and 77 years, with an average age of 57.7 years. We analyze the upper thoracic sagittal CT before surgery. We analyze the scope of this approach can be exposed. Sternum upper bone part is cut. The upper sternum bone part of the half-moon was removed. After surgery into the chest, the brachiocephalic vein was tracted to both sides. The tracheoesophageal was tracted to the inside and cut prevertebral fascia to expose the upper thoracic spine. Tuberculosis and benign tumors were treated with curettage excision of the lesion, they were using autologous iliac bone graft; Malignant tumors were treated with wide excision to remove the tumor. They vertebral reconstruction using bone cement.RESULTS: 57 patients were successful. The present method can be revealed T3 vertebral following. It can be a good exposure of the upper thoracic lesions, and the results were satisfactory. All patients were followed up for an average of 22.7 months. There was no bone fusion and fixation failure. The grafts were bony fusion. Physiological curvature of the cervical and thoracic recovery. Without internal fixation failure, spinal stability. 57 cases of postoperative neurological symptoms were restored.CONCLUSIONS: This improved upper thoracic vertebral approach effectively reveals the range of T2-T4, allows the integrity of the sternoclavicular joint and preserves sternum. Revealed the full, safe and effective, and easy to operate, with few complications. It is the ideal approach for handling another upper thoracic lesion.FDA DEVICE/DRUG STATUS: This abstract does not discuss or include any applicable devices or drugs.
P30. Study of Lumbar Multifidus Muscles in Patients with Chronic Low Back Pain and in Asymptomatic Human: A Blinded Randomized Controlled Trial (RCT)
Lijun Zhou, MD1; Ding-Jun Hao, MD1; Xie En, MD2
1Hong Hui Hospital, Xi’an Jiaotong University College of Medicine, Xi’an, Shan Xi, China; 2Xi’an Honghui Hospital, Xi’an, Shaanxi, China
BACKGROUND CONTEXT: Several studies have described the histological and morphological changes to the PVM in patients with chronic low back pain and lumbar radiculopathy. However, there is little knowledge about the PVM changes in patients with A blinded randomized controlled trial.PURPOSE: To evaluate the paravertebral muscle (PVM) degeneration in patients with asymptomatic human , using 3.0T magnetic resonance imaging.STUDY DESIGN/SETTING: A prospective observational study. A blinded randomized controlled trial.METHODS: 297 patients with low back pain(LBP group) and 300 control patients without low back pain(Healthy volunteers, HV group) were examined. The purpose of the double-blind was to avoid any bias generating from the researchers and participants who know the adopted treatment. The method we use is : Patients were randomly assigned to be taken to different treatments (conservative treatment and surgery). Another doctor of the clinic (who doesn’t know the patient’s treatment) is a researcher for the evaluation and follow-up. Doctors confirm that patients could not see the different treatment from the wound. Because researchers and patients were masked, this study is a double blind clinical study. The cross-sectional area (CSA) and percentage of fat infiltration area (%FIA) of the bilateral multifidus and longissimus muscles at the L1-S1 levels were measured using T2-weighted axial magnetic resonance imaging and computer software. A multifidus muscle biopsy and histological evaluation were performed in some patients.RESULTS: In the LBP group, the CSA of the multifidus muscle was significantly smaller and the %FIA of both muscles was significantly higher on the concave side than on the convex side at all levels (P < 0.0001 for each). These differences were also found in the longissimus muscles at the L3-L4, L4-L5 and L5-S1 levels (P < 0.05 for each). Histologically, the multifidus muscle exhibited reductions in the muscle fiber size and number of nuclei on the concave side. In the LSS group, the total CSA and %FIA did not differ significantly between the left and right sides. However, in patients with unilateral radiculopathy, the CSA of the multifidus muscle was significantly smaller (P < 0.05) and the %FIA of both muscles was significantly higher (P < 0.05) on the symptomatic side, especially at 1 level below.CONCLUSIONS: This observational study with 3.0T magnetic resonance imaging and histology showed that muscle degeneration was more common on the concave side in patients with LBP. Radiculopathy and spinal deformity may contribute to the PVM degeneration.FDA DEVICE/DRUG STATUS: This abstract does not discuss or include any applicable devices or drugs.
ePOSTER PROCEEDINGS
40

AUTHOR INDEXAhn, Nicholas U.: P10, P11, P12, P13, P14Ahn, Uri M.: P10, P11, P12, P13, P14Amaral, Rodrigo A.: P18, P19, P20, P21, P22, P23Anderson, Joshua T.: P10, P11, P12, P13, P14Badge, Ravi: P9Bjerke-Kroll, Benjamin T.: P1, P2Boiwka, Alex V.: P13, P14Budimir, Dushan: P8Budkiewicz, Robert: P6Bueno, Thabata: P18, P19, P21, P22, P23Cheng, Wayne K.: P16Cheung, Zoe: P1Coutinho, Thiago P.: P18, P19, P20, P21, P22, P23Cunningham, Matthew E.: P2D’Andrea, Kenneth P.: P17En, Xie: P28, P29, P30Fabricant, Peter D.: P1Fahim, Daniel K.: P17Forrest, Brent: P16Gladnick, Brian P.: P2Grabala, Pawel: P6Hao, Ding-Jun: P28, P29, P30Iyer, Sravisht: P1Jensen, Rubens: P18, P19, P21, P22, P23Kim, Han Jo: P1Kossakowski, Dariusz: P6Kucharzyk, Donald: P8Liu, Tao: P4, P5Luo, Zong Ping: P15Madhavan, Karthik: P7Marchi, Luis: P18, P19, P20, P21, P22, P23Mei, Xin: P15Oliveira, Leonardo: P18, P19, P20, P21, P22, P23Pimenta, Luiz H.: P18, P19, P20, P21, P22, P23, P25Quigley, Robert: P16Schreiber, Joseph: P2Shifflett, Grant D.: P1, P2Smith, William D.: P24, P25, P26, P27Sullivan, Thomas B.: P10, P11, P12Uribe, Juan S.: P25Vanni, Steven: P7Yang, Huilin: P15Zhang, Kai: P3Zhang, Zhigang: P15Zhou, Lijun: P30
SUBJECT INDEXAccuracy: P9Acute: P27Adolescent Idiopathic Scoliosis: P1, P2Ambulatory: P24Anal tone: P9Ankle degeneration: P13Ankle osteoarthritis: P14Anterior lumbar interbody fusion (ALIF): P19Arthritis: P13Arthrodesis: P22Arthroplasty: P18Axial rotation: P1Bone graft: P22Bone scintigraphy: P5Calcium phosphate: P22Cauda equina: P9Cement augmentation: P11, P12Cervical spine: P17Children/teenagers: P28Cobb angle: P2Comparison open approach: P8Complication: P21, P26Deformity: P2Ectopic: P25Fibrosis: P3Hindfoot degeneration: P14Idiopathic scoliosis: P6Imaging: P1Intraoperative imaging: P17Intraoperative navigation: P17Invasive: P15Kyphoplasty: P4, P12Lateral: P26Lateral approach: P20, P21Lawsuit: P16Ligamentum flavum: P3Lumbar plexus: P21Lumbar spinal stenosis: P10, P14, P15Lysophosphatidic acid: P3Mesenchymal stem cell: P7Minimally invasive: P8, P10, P11, P12, P27Osteocel plus: P7Osteoporotic vertebral compression fracture (OVCF): P4Outpatient: P24Patient outcomes: P8Pedicle lengthening: P15PET: P5Revision: P18rhBMP-2: P25Sagittal parameters: P19, P23Spinal cord injury: P16, P28Spondylolisthesis: P23Standalone: P19, P20, P23Subsidence: P20Temperature gradient injection: P4Thoracic spinal stenosis: P13Thoracolumbar spine injury: P28Three-dimensional correction: P6Vertebral column manipulation: P6Vertebral metastases: P5Vertebroplasty: P11XLIF: P7, P18, P24, P25, P26, P27X-Stop: P10
AUTHOR INDEX /SUBJECT INDEX
N A S S S U M M E R S P I N E M E E T I N G
41

NASS FINANCIAL CONFLICT OF INTEREST DISCLOSURE POLICYNASS recognizes that professional relationships with industry are essential for development of new spine technologies and medical advancement. According to the NASS Ethics Committee, which authored the disclosure policy, “the goal is to create an environment of scientific validity, in which learners can accurately judge whether the information they receive is objective and unbiased, and to be sure that our members are current and forthright in their dealings with one another and with their colleagues and patients. “ The establishment of uniform disclosure requirements frees individuals from having to decide which relationships might influence his or her decision-making and which are irrelevant; transparent disclosure allows the audience to participate in the interpretation of the significance. All authors and faculty speaking at the Summer Spine Meeting have been required to provide complete disclosure of all conflicts of interest.
COMMERCIAL SUPPORT DISCLOSURE As a sponsor accredited by the ACCME, the North American Spine Society must ensure balance, independence, objectivity and scientific rigor in all its sponsored activities.
All individuals participating in a sponsored activity are expected to disclose to the activity audience any significant financial interest or other relationship (1) with the manufacturer(s) of any commercial product(s) and/or provider(s) of commercial services discussed in an educational presentation and (2) with any commercial supporters of the activity. Significant financial interest or other relationships may include: grants or research support, employee, consultant, major stockholder, member of the speaker’s bureau, etc. Disclosure information will be made available visually on a PowerPoint® slide before each presentation, in the Final Program and orally by the moderator.
PROGRAM COMMITTEE STATEMENT ON RESOLUTION OF CONFLICT OF INTEREST IN PRESENTATIONSThe intent of this disclosure is to ensure that all conflicts of interest, if any, have been identified and have been resolved prior to the speaker’s presentation. By doing so, the North American Spine Society has determined that the speaker’s or author’s interests or relationships have not influenced the presentation with regard to exposition or conclusion; nor does the Society view the existence of these interests or commitments as necessarily implying bias or decreasing the value of the presentation.
FDA DISCLOSUREIf a device or drug requiring FDA approval is identified as an important component of a presentation, the author must indicate the FDA status of those devices or drugs as Approved, Investigational or Not Approved for distribution within the United States. The Final Program includes all FDA status information. Certain medical devices and drugs identified at the 2nd Annual Summer Spine Meeting may have FDA clearance for use for specific purposes only, or in restricted research settings. The FDA has stated it is the responsibility of the physician to determine the FDA status of each drug or device he or she wishes to use in clinical practice and to use these products in compliance with applicable law.
PARTICIPANT AND PLANNER DISCLOSURE INDEX (Current as of 3/27/2014)
Range KeyLevel A: $100 to $1000Level B: $1,001 to $10,000Level C: $10,001 to $25,000Level D: $25,001 to $50,000Level E: $50,001 to $100,000Level F: $100,001 to $500,000Level G: $500,001 to $1MLevel H: $1,000,001 to $2.5MLevel I: Greater than $2.5M
Ahn, Nicholas U.: Research Support (Staff and/or Materials): Stryker (C); Grants: Stryker (None); Other: Legal firms, Workman’s compensation (Amount not disclosed).
Ahn, Uri M.: Royalties: Alphatec Spine (B, Paid directly to institution/employer); Other: Spine 360 (Amount not disclosed, Paid directly to institution/employer); Relationships Outside the One Year Requirement: Spine 360 (Expires 2015, Royalties, E).
Amaral, Rodrigo A.: Speaking and/or teaching arrangements: NuVasive (Amount not disclosed); Trips/travel: NuVasive (Amount not disclosed).
Asher, Anthony: Board of Directors: NeuroPoint Alliance (Travel expenses); Other Office: American Association of Neurological Surgeons (Travel expenses).
DISCLOSUREINDEX
N A S S S U M M E R S P I N E M E E T I N G
42

Bono, Christopher M.: Royalties: Wolters Kluwer (B); Consulting: Harvard Clinical Research Institute (None), United Health Care (B); Board of Directors: North American Spine Society (Second Vice President); Other Office: Intrinsic Therapeutics (B), JAAOS (B, Deputy Editor), The Spine Journal (Deputy Editor).
Chaudhary, Saad B.: Speaking and/or Teaching Arrangements: Medtronic (B); Scientific Advisory Board: U & I Corporation (A).
Cheng, Joseph S.: Board of Directors: North American Spine Society (Professional, Economic and Regulatory Chair); Other Office: AANS/CNS (Recording Secretary AANS/CNS Council of State Neurosurgical Societies; Past-Chair AANS/CNS Joint Spine Section).
Cheng, Wayne K.: Consulting: Musculoskeletal Transplant Foundation (B, Paid directly to institution/employer), DePuy Spine (B, Paid directly to institution/employer), Olympus Bioteoch (None, Paid directly to institution/employer).
Chou, Dean: Consulting: DePuy (C), Medtronic (B), Globus (B), Orthofix (B); Trips/Travel: AO North America (B).
Chutkan, Norman B.: Royalties: Globus Medical (E); Speaking and/or Teaching Arrangements: AO North America (Travel expenses); Scientific Advisory Board: Orthopedics Journal (None).
Cunningham, Matthew E.: Speaking and/or teaching arrangements: DePuy Johnson & Johnson (Amount not disclosed).
Dagenais, Simon: Royalties: Elsevier (A); Stock Ownership: Pacira Pharmaceuticals (<1%); Private Investments: Palladian Health (2%); Consulting: University of South Florida (C), Intrinsic Therapeutics (A), NCMIC Foundation (B), Dr. Louis Sportelli (B), Pacira Pharmaceuticals (D), New York University (C), Palladian Health (E), Foundation for Chiropractic Progress (B), Gerson Lehrman Group (A); Speaking and/or Teaching Arrangements: NCMIC Foundation (B), Chiropractic and Osteopathic College of Australasia (A); Trips/Travel: Canadian Chiropractic Research Foundation (A), North American Spine Society (B); Scientific Advisory Board: Societe Franco-Europenne de Chiropraxie (None), Palladian Health (C); Other Office: North American Spine Society (Annual Meeting Program Co-chair), Pacira Pharmaceutical (Salary); Grants: NCMIC Foundation (D).
Daubs, Michael D.: Royalties: Synthes Spine (F); Consulting: DePuy-Synthes Spine (B); Speaking and/or Teaching Arrangements: AOSpine North America (B); Board of Directors: AOSpine North America (B); Other Office: North American Spine Society (Annual Meeting Program Committee); Fellowship Support: AOSpine North America (D, Paid directly to institution/employer).
Devin, Clinton J.: Speaking and/or Teaching Arrangements: DePuy (Amount not disclosed, Paid directly to institution/employer); Research Support - Staff and/or Materials: Stryker (E, Paid directly to institution/employer); Relationships Outside the One-Year Requirement: DePuy/Stryker (Dissolved 8/2011, Research Support: Staff and/or Materials, D).
Dohring, Edward J.: Royalties: Board of Directors: North American Spine Society (CME Committee Chair).
Finkenberg, John G.: Royalties: Biomet Spine (E); Speaking and/or teaching arrangements: Biomet (Travel expenses); Board of Directors: North American Spine Society (Advocacy Committee Chair), Satori World Medical (Medical Advisor).
Ghogawala, Zoher: Board of Directors: American Association of Neurological Surgeons – NeuroPoint Alliance (None), Congress of Neurological Surgeons (Executive Committee), Collaborative Spine Research Foundation (None), North American Spine Society (Clinical Research Development Chair); Research Support (Staff/Materials): Stuart Foundation (F, Paid directly to institution/employer); Grants: NIH (None), PCORI (H, Paid directly to institution/employer).
Harris, Mitchel B.: Consulting: HCRI (Amount not disclosed), Medtronic (Medical Monitor for Open Tibia Fracture Study, Paid directly to institution/employer); Board of Directors: North American Spine Society (Governance Committee Chair).
Kauffman, Christopher P.: Stock Ownership: NOC2 (0.02%); Consulting: Hospital Corporation of America (HCA) - TriStar Spine Physician Advisory Panel (None); Speaking and/or teaching arrangements: North American Spine Society (Travel expenses); Board of Directors: North American Spine Society (Health Policy Council Director).
Kim, Han Jo: Royalties: World Scientific Publishers (None); Speaking and/or teaching arrangements: K2M (A); Scientific Advisory Board: Spine Innovation Advisory Board, Medtronic (B).
Kucharzyk, Donald: Royalties: Precision Spine (B); Consulting: NuVasive (D), Spinal USA (D); Speaking and/or teaching arrangements: NuVasive (B); Trips/travel: Precision Spine (Amount not disclosed); Research Support (Investigator Salary): NuVasive (B).
Lee, Yu-Po: Consulting: DePuy (C), Stryker (B); Fellowship Support: Synthes (E, Paid directly to institution/employer).
McGirt, Matthew J.: Consulting: Codman (Amount not disclosed); Research Support - Staff and/or Materials: Stryker Spine (E, Paid directly to institution/employer), DePuy (E, Paid directly to institution/employer).
Mick, Charles A.: Board of Directors: North American Spine Society (Past President, D).
Mitchell, William: Private Investments: South Jersey Cyberknife (<1%); Speaking and/or teaching arrangements: North American Spine Society (B); Trips/Travel: North American Spine Society (C); Board of Directors: North American Spine Society (Section Development Chair).
Mroz, Thomas E.: Stock Ownership: Pearl Diver (<1%); Consulting: CeramTec (None, Paid directly to institution/employer); Speaking and/or teaching arrangements: AOSpine (B); Board of Directors: AOSpine North America (None), North American Spine Society (Education Council Director); Fellowship Support: AOSpine (E, Paid directly to institution/employer).
Muehlbauer, Eric J.: Board of Directors: North American Spine Society (Executive Director); Other Office: World Spine Care (Advisor).
O’Brien Jr., David R.: Speaking and/or teaching arrangements: North American Spine Society (B); Trips/Travel: ISIS (B), AAPMR (Travel expenses); Board of Directors: North American Spine Society (Education Publishing Chair); Other Office: ISIS (Socioeconomic Council Vice-Chair), AAPMR (Program Planning Committee).
O’Neill, Conor: Stock Ownership: Relievant (17%), Nocimed (70%); Private Investments: Nocimed (<1%); Consulting: SpineView (B), ISTO (D), Alleeva (B); Scientific Advisory Board: Relievant (Stock options).
DISCLOSURE INDEX
43

Park, Paul: Royalties: Globus Medical (A); Consulting: Globus Medical (B), Medtronic (B); Speaking and/or Teaching Arrangements: Globus Medical (C), DePuy Synthes (B); Scientific Advisory Board: Neuralstem (A); Grants: NIH (B, Paid directly to institution/employer), Blue Cross Blue Shield of Michigan Foundation (E, Paid directly to institution/employer).
Pimenta, Luiz H.: Royalties: NuVasive (G); Consulting: NuVasive (Amount not disclosed), Zyga Tech (Amount not disclosed), MDT/Biotec (Amount not disclosed); Board of Directors: ISASS (None); Scientific Advisory Board: LASAS (Scientific Reviewer).
Prather, Heidi: Board of Directors: North American Spine Society (First Vice President); Other Office: American Academy of Physical Medicine and Rehabilitation (B, Paid directly to institution/employer).
Rao, Raj D.: Board of Directors: North American Spine Society (Travel expenses), Lumbar Spine Research Society (None); Other Office: American Academy of Orthopaedic Surgeons (Chairman, Diversity Advisory Board), Medicare Evidence Development and Coverage Advisory Commission (Voting Member of US Centers for Medicare and Medicaid Services MEDCAC); Grants: United States Department of Defense – Navy (G, Paid directly to institution/employer), United States Department of Defense – Army Medical Research Acquisition (F, Paid directly to institution/employer), National Highway Traffic Safety Administration (F, Paid directly to institution/employer), U.S. Department of Education, National Institute on Disability and Rehabilitation Research (G, Paid directly to institution/employer); Other: The Spine Journal (None), Editorial Board of JBJS Reviews (None).
Reitman, Charles A.: Trips/Travel: North American Spine Society (Travel expenses), AAOS Evidence Based Committee (Travel expenses); Board of Directors: North American Spine Society (Evidence Compilation and Analysis Chair, Annual Meeting Program Co-Chair); Scientific Advisory Board: Clinical Orthopedics and Related Research (B, Deputy Editor, Paid directly to institution/employer).
Resnick, Daniel K: Consulting: Asterias (B); Board of Directors: North American Spine Society (Research Council Director); CNS (President-Elect); Scientific Advisory Board: Asterias (Consulting disclosed).
Rothman, David J.: Board of Directors: North American Spine Society (Ethicist); Relationships Outside the One Year Requirement: State of Texas/Sheller (Expert witness, Dissolved 3/2012, E).
Schofferman, Jerome: Board of Directors: North American Spine Society (Committee on Ethics and Professionalism Chair).
Siddiqi, Farhan N.: Royalties: Globus (A); Consulting: Globus (B); Speaking and/or Teaching Arrangements: Wolf (B); Grants: Wolf (B).
Smith, William D.: Royalties: NuVasive (D); Stock Ownership: NuVasive (<1%); Consulting: NuVasive (C), Spineology (Amount not disclosed), Ceiling Technologies (Amount not disclosed), Baxano (Amount not disclosed), SpineGuard (Amount not disclosed), SI-Bone (Amount not disclosed); Speaking and/or teaching arrangements: NuVasive (Amount not disclosed), SI-Bone (Amount not disclosed); Trips/travel: NuVasive (B); Research Support (Investigator Salary): NuVasive (C, Paid directly to institution/employer); Research Support (Staff and/or Materials): NuVasive (B, Paid directly to institution/employer).
Smuck, Matthew: Consulting: ArthroCare (B), EMKinetics (A); Other Office: The Spine Journal (Deputy Editor), North American Spine Society (Annual Meeting Program Committee); Research Support - Investigator Salary: Cytonics Corporation (C, Paid directly to institution/employer); Research Support - Staff and/or Materials: Cytonics Corporation (D, Paid directly to institution/employer); Grants: International Spine Interventions Society (C, Dissolved 12/2012, Paid directly to institution/employer).
Sowa, Gwendolyn A.: Royalties: UpToDate (A); Board of Directors: Association of Academic Physiatrists (Board of Trustees); Other Office: Association of Academic Physiatrists (Research Committee), North American Spine Society (Annual Meeting Program Committee); Research Support - Investigator Salary: NIH, NIDRR, UPMC RI (E, Paid directly to institution/employer); Research Support - Staff and/or Materials: NIH/NIDRR, UPMC RI (F, Paid directly to institution/employer).
Truumees, Eeric: Royalties: Stryker Spine (C); Stock Ownership: Doctor’s Research Group (<1%); Private Investments: IP Evolutions (33%); Board of Directors: North American Spine Society (Administration and Development Council Director); Other Office: AAOS Communications Cabinet (Incoming Editor-in-Chief of AAOS Now, AAOS Communications Cabinet); Research Support (Investigator Salary): Relievant (B, Paid directly to institution/employer); Research Support (Staff/Materials): Globus (B, Paid directly to institution/employer); Other: Stryker Biotech (Unknown, Paid directly to institution/employer).
Uribe, Juan S.: Consulting: NuVasive (F); Speaking and/or teaching arrangements: Orthofix (F); Research Support (Investigator Salary): NuVasive (D, Paid directly to institution/employer); Research Support (Staff and/or Materials): NuVasive (C, Paid directly to institution/employer); Grants: NuVasive (B, Paid directly to institution/employer); Fellowship Support: NuVasive (D, Paid directly to institution/employer).
Vanni, Steven: Royalties: NuVasive (E); Consulting: Globus (B); Speaking and/or teaching arrangements: DePuy (B).
Villavicencio, Alan T.: Device or Biologic Distributorship (Physician-Owned Distributorship): Leading Edge Spinal Implants (A); Stock Ownership: Lanx (2%, Founder); Board of Directors: Justin Parker Neurological Institute (None); Other Office: Boulder Neurosurgical Associates (Managing Partner); Research Support - Investigator Salary: ProFibrix (F, Paid directly to institution/employer), Medtronic (F, Paid directly to institution/employer).
Wang, Jeffrey C.: Royalties: Stryker (B), Osprey (C), Aesculap (B), Biomet (F), Amedica (D), SeaSpine (D), Synthes (C), Alphatec (E); Stock Ownership: Fziomed (<1%), Alphatec (<1%); Private Investments: Promethean Spine (<1%), Paradigm Spine (<1%), Benvenue (<1%), Nexgen (<1%), Pioneer (<1%), Amedica (<1%), VertiFlex (<1%), ElectroCore (<1%), Surgitech (<1%), AxioMed (<1%), VG Innovations (<1%), CoreSpine (<1%), Expanding Orthopaedics (<1%), Syndicom (<1%), Osprey (<1%), Amedica (<1%), Bone Biologics (<1%), Curative Biosciences (<1%), Pearl Diver (<1%); Board of Directors: North American Spine Society (Treasurer), Cervical Spine Research Society (Travel expenses), AOSpine/AO Foundation (E), Collaborative Spine Research Foundation (Travel expenses); Fellowship Support: AO Foundation (E, Paid directly to institution/employer).
DISCLOSURE INDEX
44

DISCLOSURE INDEX
Wang, Michael Y.: Royalties: DePuy Spine (G); Consulting: DePuy Spine (E), Aesculap (B); Speaking and/or Teaching Arrangements: DePuy Spine (D); Scientific Advisory Board: ISD (None); Grants: Department of Defense (A, Paid directly to institution/employer).
Watters, William C.: Royalties: Stryker Corporation (B); Stock Ownership: Intrinsic Therapeutics (<1%); Board of Directors: North American Spine Society (President, E), World Spine Care (None), American College of Spine Surgeons (None); Scientific Advisory Board: Intrinsic Therapeutics (None, Dissolved 2014), Palladian Health (B, Clinical Advisory and Policy Board); Other: The Spine Journal (Deputy Editor), Spine Arthroplasty Journal (Assistant Editor), Spine (Reviewer), Kirby Glenn Surgical Center (1/22nd minority interest ownership).
Wetzel, F. Todd: Stock Ownership: Relievant Medical (1%); Board of Directors: McKenzie Institute International (B), North American Spine Society (Secretary).
Yu, Warren D.: Royalties: Spineart (D); Stock Ownership: Spineart (<0.01%); Consulting: Integra Spine (B), Interventional Spine (C); Speaking and/or Teaching Arrangements: Globus (B); Scientific Advisory Board: SpineFrontier (None).
The following participants have nothing to disclose: Anderson, David T. Anderson, Joshua T.Badge, RaviBhowmick, DebBjerke-Kroll, Benjamin T.Boiwka, Alex V.Budimir, DushanBudkiewicz, RobertBueno, ThabataCheung, ZoeCoutinho, Thiago P.D’Andrea, Kenneth P.DeVine, John G. En, XieFabricant, Peter D.Fahim, Daniel K.Forrest, BrentGladnick, Brian P.Grabala, PawelHao, Ding-JunHoh, Daniel J.Iyer, SravishtJensen, RubensKossakowski, DariuszKrishnaney, Ajit A. Liu, TaoLuo, Zong PingMadhavan, KarthikMarchi, LuisMayer, E. Kano A. Mazanec, Daniel J. McIntyre, John J. Mei, XinMoore, Timothy A. Oliveira, LeonardoOrr, R. DouglasPatel, Alpesh A.Quigley, RobertQureshi, Sheeraz A.Reed, Michael L.Reudink, R. ChristopherRittenberg, Joshua D.Schreiber, JosephShifflett, Grant D.Shin, John H.Slotkin, JonathanSteinmetz, Michael P.Sullivan, Thomas B.Tolhurst, StephenWu, Adam S.Yang, HuilinZhang, KaiZhang, ZhigangZhou, Lijun
45

Advanced Biologicswww.advancedbiologics.com
Advanced Biologics’ (ABC) focus is to develop innovative and clinically relevant biologic solutions across a wide degree of medical specialties. Our company is fully dedicated to improving patients’ lives and the health care provider’s experience with our products. ABC’s award-winning OsteoAMP® allogeneic-derived growth factor has shown to provide a true alternative to rhBMP-2 with clinical results showcasing faster, safer and denser bone growth.
Biomet Spinewww.biomet.com/spine
Applying today’s most advanced engineering and manufacturing technologies, we’ve developed our product line to offer surgeons a comprehensive approach for a wide variety of surgical applications for the spine. Visit our exhibit to see how our products can help surgeons change lives for the better, one patient at a time.
DePuy Synthes Spinewww.depuysynthes.com
DePuy Synthes Spine has one of the largest and most diverse portfolios of products and services in spine and is a global leader in traditional and minimally invasive treatment. We offer procedural solutions for the spectrum of spinal disorders including deformity, spinal stenosis, trauma and degenerative disc disease. DePuy Synthes Spine is part of DePuy Synthes Companies of Johnson & Johnson, the largest provider of orthopaedic and neurological solutions in the world. Visit www.depuysynthes.com
Eminent Spinewww.eminentspine.com
Eminent Spine is a highly innovative, just in time, engineering, manufacturing and distribution company. Eminent Spine is a privately held company that was founded in June of 2008 by Dr. Steve Courtney and Dave Freehill. Dr. Courtney and Mr. Freehill began Eminent Spine with the idea of combining a spine surgeon’s expertise with an engineer’s experience to design, engineer, manufacture and distribute highly innovative specialty tools, implants, and implements specifically for spinal surgery.
Globus Medicalwww.globusmedical.com
Globus Medical, Inc. is a leading musculoskeletal implant company based in Audubon, PA. The company was founded in 2003 by an experienced team of professionals with a shared vision to create products that enable surgeons to promote healing in patients with musculoskeletal disorders. Additional information can be accessed at www.globusmedical.com
K2M Inc.www.k2m.com
K2M Group Holdings, Inc. is a global medical device company focused on designing, developing and commercializing innovative complex spine and minimally invasive spine technologies and techniques used by spine surgeons to treat some of the most difficult and challenging spinal pathologies. K2M has leveraged these core competencies to bring to market an increasing number of products for patients suffering from degenerative spinal conditions. These technologies and techniques, in combination with a robust product pipeline, enables the company to favorably compete in the global spinal surgery market.
Life Instrument Corp.www.lifeinstruments.com
Life Instrument Corporation is dedicated to serving neurosurgeons and orthopedic surgeons with the highest quality surgical instruments. Over the years spine surgery has advanced with new procedures and approaches to the spine. Life Instrument Corporation is committed to meet the needs of spine surgeons for these new surgical techniques.
TECHNICALEXHIBITION
N A S S S U M M E R S P I N E M E E T I N G
46

TECHNICAL EXHIBITION
Mazor Roboticswww.mazorrobotics.com
Mazor Robotics is a leading innovator in spine and brain surgery—inspiring the art of surgery with mechanical guidance systems and complementary products that provide a safer surgical environment for patients, surgeons, and OR staff. Renaissance is powered by clinically validated technology and has been used in over 7,500 cases at leading medical institutions worldwide. Via Renaissance’s intuitive interface, the surgeon plans the operation in a virtual 3D environment creating a surgical blueprint. Renaissance easily integrates into the OR workflow, providing the highest level of accuracy and may lower the amount of fluoroscopy used for deformity, minimally-invasive, and revision spine procedures.
Medicreawww.medicrea.com
MEDICREA is a fully-dedicated spinal implant company focused on introducing reliable and innovative technologies to the global marketplace. With over 19 years of experience, MEDICREA provides a full range a full range of patented products that are conceived, developed and manufactured to advance patient outcomes and support the work of medical professional.
Orthofix, Inc.www.orthofix.com
Orthofix is a diversified, global medical device company focused on developing and delivering innovative repair and regenerative solutions to the spine and orthopedic markets. Our products are designed to address the lifelong bone-and-joint health needs of patients of all ages, helping them achieve a more active and mobile lifestyle.
Pacira Pharmaceuticalswww.pacira.com
Pacira Pharmaceuticals, Inc. is a specialty pharmaceutical company focused on the development of products that meet the needs of acute care practitioners and their patients. Its lead product, EXPAREL® (bupivacaine liposome injectable suspension), was launched in 2012. EXPAREL utilizes the Pacira proprietary delivery technology DepoFoam®. For more information, visit http://www.pacira.com.
SI-BONE, Inc.www.si-bone.com
SI-BONE, Inc. is the leading sacroiliac (SI) joint medical device company dedicated to the development of tools for diagnosing and treating patients with low back issues related to SI joint disorders. The company is manufacturing and marketing a minimally invasive surgical (MIS) technique for the treatment of SI joint pathology.
SpineGuard, Inc.www.spineguard.com
Hear and feel what you cannot see! PediGuard® is the first wireless device that can detect possible vertebral cortex perforations during pedicle preparation by accurately analyzing the electrical conductivity of the surrounding tissues in real-time. PediGuard has assisted both orthopedic spine surgeons and neurosurgeons in over 30,000 surgeries worldwide.
47

MEMBERSHIP
In the late 1970s, spine care pioneers made the observation that a scientific society including all members of the spine community regardless of specialty or locale was essential to the advancement of care, and in 1984, this vision was realized through the creation of the North American Spine Society (NASS).
Today, these same ideas inspire a new generation of members as NASS becomes the premier multidisciplinary medical organization representing the field of spine care. With more than 8,000 members worldwide, NASS provides our members with many professional opportunities, events and initiatives designed to advance their careers, support the field, and define the future of spine care.
NASS members receive access to critical benefits of membership in the areas of education, research, health policy, reimbursement, practice management, networking, career development and philanthropy. Visit the Registration Desk in the lobby for more information about membership, to renew your membership for 2014, or to apply to become a member. You can also learn more or apply online at www.spine.org.
CATEGORIES OF MEMBERSHIP
Active members are Board-certified MDs and DOs, PhDs, or international equivalents (as determined by the Board of Directors) who devote at least 50% of their professional activities to spine.
Annual Dues: $625.00 Includes print and online subscriptions to The Spine Journal (TSJ) and SpineLine
Associate members are Board-eligible MDs and DOs, PhD candidates, or individuals who have completed a substantially equivalent program (as determined by the Board of Directors) who devote at least 50% of their professional activities to spine.
Annual Dues: $625.00 Includes print and online subscriptions to TSJ and SpineLine
Affiliate members are physicians who devote less than 50% of their professional activities to spine, nurse practitioners, registered nurses, physician assistants, chiropractors, physical therapists, researchers, practice managers, coders, technical professionals or other health care professionals with an interest in spine.
Annual Dues: $325.00 Includes print and online subscriptions to TSJ and SpineLine
International members are health care professionals not residing in the United States with an interest in spine.
Annual Dues: $275.00 Includes print and online subscription to TSJ and online subscription to SpineLine
In-training members are physicians, medical students, graduate students or other individuals of the medical profession, basic sciences or allied services who are enrolled in a full-time, accredited training program or postdoctoral fellowship related to spine care. Individuals who have been awarded a terminal degree and are returning for additional education unrelated to spine care are not eligible for this membership category.
Annual Dues: Complimentary Includes print and online subscription to TSJ and online subscription to SpineLine
Honorary membership is bestowed by the Board of Directors to recognized leaders in the field of spine care.
Annual Dues: Complimentary Includes print and online subscriptions to TSJ and SpineLine
Emeritus members are individuals who have been Active members for at least fifteen years and have retired from the practice of medicine.
Annual Dues: Complimentary Includes online subscriptions to TSJ and SpineLine. Discounted print subscriptions to TSJ and SpineLine are available.
NASSMEMBERSHIP
N A S S S U M M E R S P I N E M E E T I N G
48

Full Name (including degrees):
Date of Birth (mm/dd/yy): Gender: q Male q Female
Preferred Mailing Address: q Professional q Home
Professional Address (as it should be listed in the membership directory)
Company Name:
Address:
City: State/Province: Postal Code: Country:
Phone: Fax: Email:
Office Manager Name (to contact regarding membership information):
Office Manager Email: Office Manager Phone:
Home AddressAddress:
City: State/Province: Postal Code: Country:
Mobile Phone: Email:
Professional InformationSpecialty:
MDs and DOs (or international equivalent): Are you board certified? q Yes q No Name of Board providing your certification (required if applying for Active or Associate membership):
Percentage of professional activities dedicated to spine: q Less than 50% q 50% or Greater
Percentage of professional activities spent in: % Academic % Clinical % Research
Primary Employer: q Hospital q Private Practice q Academic Institution q Other:
Has your license to practice ever been revoked or otherwise suspended? q No q Yes (if yes, please attach explanation)
Application RequirementsCurriculum Vitae/RésuméPlease submit a copy of your most recent curriculum vitae (CV) or résumé with this application. Your membership will remain inactive until a copy of this document is received.
Please provide your primary reason for applying for membership.q Recommendation from colleague (optional, provide colleague name: )q Career development, CME, or to receive updates on spine care issuesq To take advantage of membership discounts on educational offeringsq To access journals and publicationsq To network with colleaguesq To support and contribute to the fieldq Other:
APPLICATION FOR MEMBERSHIP
Follow us:
North American Spine Society7075 Veterans Blvd. | Burr Ridge, IL 60527 | Phone: 630-230-3600 | Fax: 630-230-3700
www.spine.org | [email protected]
The NASS Professional Compliance Panel (PCP) exists to ensure member compliance with the NASS ethics policies as well as any other rules or regulations incumbent upon a healthcare professional. By applying, you acknowledge that you are required to comply with such policies, rules and regulations, and further agree to promptly comply with all requests to provide documentation concerning PCP investigations, when it is within your legal ability to do so.

THE FAIRMONT ORCHID
The Fairmont Orchid, Hawaii is a 32-acre oceanfront luxury resort located on the Kohala Coast Hawaii with a white sand lagoon and aquamarine waters, Hawaiian spas, golf, tennis, and six restaurants.
SUBMIT AN ABSTRACT
Go to sms.spine.org to submit an abstract for Spine Across the Sea. The electronic abstract submission begins on September 9, 2014. The deadline to submit is December 17, 2014.
Spine Across the Sea 2015Join colleagues from around the world at
July 26-30, 2015The Fairmont OrchidKohala Coast, Hawaii, USA
The North American Spine Society and Japanese Society for Spine Surgery and Related Research come together to share current concepts, discuss issues and exchange ideas about spine care.
www.spine.org

• Rapid pain relief by 6 weeks• Sustained pain relief out to
6, 12, 24 and 40 months• Clinically significant pain relief
at all follow-up time points (≥2 point drop from baseline)
The iFuse Implant System is intended for sacroiliac joint fusion for conditions including sacroiliac joint disruptions and degenerative sacroiliitis. As with all surgical procedures and permanent implants, there are risks and considerations associated with surgery and use of the iFuse Implant. Please review the iFuse Instructions For Use for a complete discussion of contraindications, warnings, precautions, and risks.
Key: * Paid consultant of SI-BONE, Inc.; † Conducts clinical research for SI-BONE, Inc.; § Ownership interest in SI-BONE, Inc.
SI-BONE and iFuse Implant System are registered trademarks of SI-BONE, Inc. © 2014 SI-BONE, Inc. All rights reserved. 8827.061814
UniqUe DesignTriangular implants designed specifically to stabilize and fuse the heavily loaded SI joint.
strength of experience
More than 12,000 procedures have been performed with the iFuse Implant System® – the method of choice for SI joint fusion.
clinical resUlts
Published papers report clinical safety and effectiveness outcomes.
References1. Rudolf L*§†. Sacroiliac Joint Arthrodesis-MIS Technique with Titanium Implants: Report of the
First 50 Patients and Outcomes. Open Orthop J. 2012;6:495-502.
2. Sachs D*†, et al. Minimally Invasive Sacroiliac Joint Fusion: One-Year Outcomes in 40 Patients. Adv Orthop. 2013;2013:536128.
3. Cummings J Jr*†, et al. Minimally invasive sacroiliac joint fusion: one-year outcomes in 18 patients. Ann Surg Innov Res. 2013;7:12.
4. Gaetani P†, et al. Percutaneous arthrodesis of sacro-iliac joint: a pilot study. J Neurosurg Sci. 2013;57:297–301.
5. Graham Smith A*, et al. Open versus minimally invasive sacroiliac joint fusion: a multi-center comparison of perioperative measures and clinical outcomes. Ann Surg Innov Res 2013;7:14.
6. Schroeder JE, et al. Early Results of Sacro–Iliac Joint Fixation Following Long Fusion to the Sacrum in Adult Spine Deformity. HSS J. 2013;10:30–5.
7. Duhon B*†, et al. Safety and 6-month effectiveness of minimally invasive sacroiliac joint fusion: a prospective study. Med Devices (Auckl) 2013;6:219–29.
Rapid and Sustained Pain Relief*– VAS Pain
*All patients were treated for SI joint disruptions or degenerative sacroiliitis.
www.si-bone.com

invasiveminimally
FOCUS
The only public spine company
focused on MIS solutions for fusion
and decompression. Baxano Surgical
offers surgeons a suite of proprietary
products focused on the lumbar spine.
www.BaxanoSurgical.com | 866-256-1206
45
-615
7 R
ev A
8/1
2/1
3
Min
imally
Invasi
ve
Deco
mp
ress
ion
Syst
em
Min
imally
Invasi
ve
Rap
id F
acete
cto
my
Late
ral A
ccess
& In
terb
od
y
Fu
sio
n S
yst
em
Pre
sacra
l A
ccess
&
Inte
rbo
dy F
usi
on
Syst
em
For more information on training opportunities,
email: s [email protected]
MAXIMUM