Implementing the Next Accreditation System for Urology Programs ...

Accreditation Council for Graduate Medical Education
The Next Accreditation System
Association of Pediatric Program Directors
October 3-5, 2012
Mary W. Lieh-Lai, MD, FAAP, FCCP
Senior Vice President for Medical Accreditation
© 2012 Accreditation Council for Graduate Medical Education (ACGME)

© 2012 Accreditation Council for Graduate Medical Education (ACGME)
Disclosure
Professor of Pediatrics (Voluntary), Wayne
State University School of Medicine
Pediatric Intensivist
A recovering PD and DIO
Full-time salaried by ACGME
No conflicts of interest to report

© 2012 Accreditation Council for Graduate Medical Education (ACGME)

© 2012 Accreditation Council for Graduate Medical Education (ACGME)

© 2012 Accreditation Council for Graduate Medical Education (ACGME)

© 2012 Accreditation Council for Graduate Medical Education (ACGME)
Organizational Structure of the ACGME
Executive Committee Transitional Year
Review Committee
Specialty Review Committees
Monitoring Committee
Requirements Committee
(Ad Hoc) Appeals Committees
Institutional Review Committee
Council of Review
Committee Chairs
Accreditation
Council (BOD)
Awards Committee
Journal Oversight
Bylaws
Governance
Finance Committee
DA
S
Field Staff Services
Data Services
Policies and Procedures
Senior VPs

© 2012 Accreditation Council for Graduate Medical Education (ACGME)
The New Senior Vice Presidents at the ACGME
Department of Accreditation Services
Dr. Louis Ling: SVP for Hospital Based Accreditation: Radiology, Emergency Medicine, Anesthesiology, Medical Genetics, Pathology
Dr. John Potts: SVP for Surgery Accreditation
Dr. Kevin Weiss: SVP for Safety and Quality Improvement – CLER and IRC
Dr. Mary Lieh-Lai: SVP for Medical Accreditation: Internal Medicine, Pediatrics, Family Medicine, PM&R, Allergy and Immunology, Neurology, Psychiatry

© 2012 Accreditation Council for Graduate Medical Education (ACGME)
The 2005 ACGME Strategic Plan1:
Emergence of “The New Accreditation Model”
“November 2005 retreat, ACGME Executive Committee
endorsed 4 strategic priorities designed to enable
emergence of the new accreditation model:
Foster innovation and improvement in the learning environment
Increase the accreditation emphasis on educational outcomes
Increase efficiency and reduce burden in accreditation
Improve communication and collaboration with key internal and
external stakeholders
1 ACGME 2005 Strategic Plan. (Emphasis Added, TJN)

© 2012 Accreditation Council for Graduate Medical Education (ACGME)
NAS
“By changing nothing, nothing changes
Tony Robbins

© 2012 Accreditation Council for Graduate Medical Education (ACGME)
What is good about the current system?
1981: 2 major stresses
Variability in the quality of resident education
Emerging formalization of subspecialty education
Solution:
Emphasis on program structure
↑ quantity/quality of formal teaching
Fostered balance between service & education
Promoted resident evaluation & feedback
Required support for trainees

© 2012 Accreditation Council for Graduate Medical Education (ACGME)
What is good about the current system?
Certifying exam results improved
Residents are prepared to deal with
increasing volume and complexity of
information
Contribution to clinical advances and
innovation
Role of PD established as an educational
career path
Improved formal teaching & assessment

© 2012 Accreditation Council for Graduate Medical Education (ACGME)
What is not so good with the current system?
Program requirements prescriptive, with
loss of innovation
↑ administrative burden: PDs manage
programs rather than mentor residents
(burn-out)
Educational standards lag behind delivery
system changes
The program information form (PIF)

© 2012 Accreditation Council for Graduate Medical Education (ACGME)
What is not so good with the current system?
Episodic biopsy
4- or 5-year cycle
“PIFmanship”
Year 1 of a 5-year cycle
“Why do today what you can put off until tomorrow?”

© 2012 Accreditation Council for Graduate Medical Education (ACGME)
What is not so good with the current system?
6 months before a scheduled site visit

1 Nasca, T.J., Philibert, I., Brigham, T.P., Flynn, T.C.
The Next GME Accreditation System: Rationale and Benefits.
New England Journal of Medicine. Published Electronically, February 22, 2012. In Print, March 15, 2012.
DOI:10.1056/nejmsr1200117 www.nejm.org .
NEJM. 2012.366;11:1051-1056.
© 2012 Accreditation Council for Graduate Medical Education (ACGME)

© 2012 Accreditation Council for Graduate Medical Education (ACGME)
The Next Accreditation System
“All great changes are preceded by chaos”
Deepak Chopra

© 2012 Accreditation Council for Graduate Medical Education (ACGME)
NAS
CLER
CCC
EPAs
Milestones

© 2012 Accreditation Council for Graduate Medical Education (ACGME)
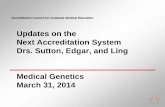
The Building Blocks of
The Next Accreditation System
CLER Visits
Continuous RRC Oversight and
Accreditation
Sponsor Oversight
Institutional
Review
prn Site Visits
(Program or Institution)
Self
Study

© 2012 Accreditation Council for Graduate Medical Education (ACGME)
Aims of NAS
Enhance the ability of the peer-
review system to prepare
physicians for practice in the 21st
century
To accelerate the movement of
the ACGME toward accreditation
on the basis of educational
outcomes
Reduce the burden associated
with the current structure and
process-based approach

© 2012 Accreditation Council for Graduate Medical Education (ACGME)
NAS
Instead of biopsies, annual data collection
Trends in key performance measurements
Milestones, Residents, fellows and faculty survey
Scholarly activity template
Operative & case log data
Board pass rates
Scheduled accreditation visits every 10 years with
focused site visits if annual data trends suggest
problems
PIF replaced by self-study
High-quality programs will be freed to innovate – detailed
process standards

© 2012 Accreditation Council for Graduate Medical Education (ACGME)
NAS
Building the case for milestones………

© 2012 Accreditation Council for Graduate Medical Education (ACGME)
Competencies/Milestones
Mid-late this past decade
Competency evaluation stalls at individual programmatic
definitions
MedPac, IOM, and others question
the process of accreditation
preparation of graduates for the “future” health care delivery
system
House of Representatives codifies “New Physician
Competencies”
MedPac recommends modulation of IME payments
based on competency outcomes
Macy issues 2 reports (2011)
IOM 2012-2013

Why Milestones and Clinical Competency Committees?
J graduated with honors from a prestigious medical school and the faculty and PD
were ecstatic that he matched into their residency program. During orientation, the
chief residents complain that J asked for multiple “golden” weekends off to attend
weddings, birthdays, etc. In the first 6 months of his internship year, he shows up
several hours late for his ED shift. He did not show up for call a couple of times.
The nurses complain that he is almost impossible to get a hold of and his
supervising third year residents complain that he frequently disappears. His write-
ups and presentations are generally acceptable. His ITE score is 2 SD below the
national mean. Faculty members who supervise his rotations have called the PD
to let her know that J’s fund of knowledge is poor, and he is often “flippant” and
appears disinterested. It is now May, and the PD and the education committee
members decide that J needs some form of warning to improve his performance,
without which, he will be placed on probation and remediation. In order to gather
“evidence” for this action, his evaluations are reviewed.
© 2012 Accreditation Council for Graduate Medical Education (ACGME)

© 2012 Accreditation Council for Graduate Medical Education (ACGME)

© 2012 Accreditation Council for Graduate Medical Education (ACGME)

© 2012 Accreditation Council for Graduate Medical Education (ACGME)

© 2012 Accreditation Council for Graduate Medical Education (ACGME)
J
Review of 4 other evaluation forms show “scores” in the
good to excellent section; a few evaluations are missing
Comments are few:
Needs to read more
Needs to be more organized
In a division that performs resident evaluations as a
group, a junior faculty member verbally complains that
he wanted to give J a poor evaluation but was over-ruled
by the other more senior members of the division
Supervising residents listed J’s deficiencies in their
evaluations
Nurses had negative comments about J in their
evaluations

© 2012 Accreditation Council for Graduate Medical Education (ACGME)
J
When the PD attempts to solicit impressions of J from
faculty members, a couple ask to see his picture. Some
state they only worked with him briefly and cannot provide
an opinion. Some do not remember working with him at all.
With the lack of documentation, the PD is unable to
implement her plan of action at this time.
Had there been a CCC in place looking at milestones,
would things have been different………..

© 2012 Accreditation Council for Graduate Medical Education (ACGME)
Milestones
Observable developmental steps moving from Novice to
Expert/Master
“Intuitively” known by experienced medical educators in
each specialty
Organized under the rubric of the six domains of clinical
competency
Trajectory of progress: neophyte → independent practice
Articulate shared understanding of expectations
Set aspirational goals of excellence
Framework & language for discussions across the continuum

© 2012 Accreditation Council for Graduate Medical Education (ACGME)
Pediatricians Understand Milestones

The Continuum of Clinical Professional Development
Authority and Decision Making versus Supervision
Authority and Decision Making Low High
Superv
isio
n
Low
High Physical Diagnosis
Internship
Residency
Fellowship
Sub-Internship
Attending
Clerkship
“Graded or Progressive
Responsibility”
© 2012 Accreditation Council for Graduate Medical Education (ACGME)

© 2012 Accreditation Council for Graduate Medical Education (ACGME)
6 Competencies - Continuum of Clinical Medical Education Dreyfus (modified) Conceptual Model1
• Medical Knowledge
• Patient Care and Procedural
Skills 2
• Interpersonal and
Communication Skills
• Professionalism
• Practice Based Learning and
Improvement
• Systems Based Practice
1 as presented by Leach, D., modified by Nasca, T.J.
American Board of Internal Medicine Summer Retreat, August, 1999. 2 Patient Care Competency modified 9/2010 by ACGME and ABMS
• Novice
• Advanced Beginner
• Competent
• Proficient
• Expert
• Master
• Undergraduate
• Graduate
• Continuing

The Goal of the Continuum of Clinical Professional Development
Master
Expert
Proficient
Competent
Advanced
Beginner
Novice Undergraduate Graduate Medical Clinical
Medical Education Education Practice
© 2012 Accreditation Council for Graduate Medical Education (ACGME)

© 2012 Accreditation Council for Graduate Medical Education (ACGME)
ACGME Goal for Milestones - Permits fruition of the
promise of “Outcomes Based Accreditation”
Specialty specific normative data and common
expectations for progress of individual residents
Less prescriptive ACGME program requirements,
lengthened program site visit cycles, less frequent
standards revision
Promote curricular innovation
Enhance curricular and rotation design flexibility
Development of specialty specific evaluation tools and
techniques

© 2012 Accreditation Council for Graduate Medical Education (ACGME)
ACGME Goal for Milestones - Permits fruition of the
promise of “Outcomes Based Accreditation”
Tracks what is important - Outcomes
Begins using existing tools and observations of the
faculty
Clinical Competency Committee triangulates progress of
each resident
Essential component of a valid and reliable clinical evaluation
system
ABMS Board has the opportunity to track the identified individual
ACGME Review Committee tracks unidentified individuals’
trajectories

The “Envelope of Expectations”
Professionalism:
Accepts responsibility and follows through on tasks
Medical PGY 1 PGY 2 PGY 3 PGY 4 PGY 5 MOC
School Expert
Proficient
Competent
Advanced
Beginner
Novice
Resident completes many assigned
tasks on time but needs extensive
guidance on local practice and/or
policy for patient care.
Resident routinely completes most
assigned tasks in a timely manner in
accordance with local practice and/or
policy, but still requires guidance in
unfamiliar circumstances.
Resident frequently prioritizes multiple
competing demands and completes the
vast majority of his/her responsibilities in
a timely manner. Self identifies
circumstances and actively seeks
guidance in unfamiliar circumstances.
Resident always prioritizes and willingly
works on multiple competing complex
and routine cases in a timely manner by
directly providing patient care or by
overseeing it. In difficult circumstances
appropriately seeks guidance. Is
regularly sought out by peers and
subordinates to provide them guidance.
Resident effectively manages
multiple competing tasks, and
effortlessly manages complex
circumstances. Is clearly identified
by peers and subordinates as
source of guidance and support in
difficult or unfamiliar circumstances.
© 2012 Accreditation Council for
Graduate Medical Education (ACGME)

Professionalism
Unprofessional
Resident seeks out opportunities
to demonstrate compassion and
empathy in the care of all patients;
and demonstrates respect and is
sensitive to the needs and
concerns of all patients, family
members, and members of the
health care team.
Resident demonstrates
compassion and empathy in care
of some patients, but lacks the
skills to apply them in more
complex clinical situations or
settings. Occasionally requires
guidance in how to show respect
for patients, family members, or
other members of the health care
team.
Resident frequently fails to
recognize or actively avoids
opportunities for compassion
or empathy. On occasion
demonstrates lack of
respect, or overt disrespect
for patients, family members,
or other members of the
health care team
© 2012 Accreditation Council for Graduate Medical Education (ACGME)

© 2012 Accreditation Council for Graduate Medical Education (ACGME)
Competence
RM Epstein: “the habitual and judicious use of communication,
knowledge, technical skills, clinical reasoning, emotions, values
and reflection in daily practice for the benefit of the individuals
and communities being served
6 domains:
Medical knowledge
Patient care
Professionalism
Communication and interpersonal skills
Practice-based learning and improvement
Systems-based practice
Epstein RM: Assessment in Medical Education. N Engl J Med, 2007; 356:387-96. Departments of
Family Medicine, Psychiatry, and Oncology and the Rochester Center to Improve Communication in
Health Care, University of Rochester School of Medicine and Dentistry

© 2012 Accreditation Council for Graduate Medical Education (ACGME)
Competence: RM Epstein
Not an achievement, but a habit of lifelong
learning
Assessment of competence should provide
insight into actual performance and capacity to
adapt to change, find and generate new
knowledge and improve overall performance
Contextual: relationship between abilities,
setting and particular situation
Developmental

© 2012 Accreditation Council for Graduate Medical Education (ACGME)
Competence: Olle ten Cate and Fedde Scheele
Competency is a personal quality, not an action
Oxford Dictionary: the ability to do something
successfully
Competencies and activities
Separate but relevant
Not one or the other but both
“we can only fully trust someone to carry out a critical
activity once they have attained all the competencies
that are needed to adequately complete this activity”
Viewpoint: Competency-Based Postgraduate Training: Can we Bridge the Gap
between Theory and Clinical Practice. Academic Medicine, 2007; 82:542-547

© 2012 Accreditation Council for Graduate Medical Education (ACGME)
Miller’s Pyramid of Clinical Competence1 1Miller, GE. Assessment of Clinical Skills/Competence/Performance.
Academic Medicine (Supplement) 1990. 65. (S63-S67)
Knows MCQ, Oral Examinations
Knows How MCQ, Oral Examinations, Standardized
Patients
Shows How
(Shows Can Do)
Clinical Observation, Simulation,
Standardized Patients, Mini CEX
Does
Clinical Observations, Mini CEX,
Multi-Source Feedback, Teamwork Evaluation,
Operative (Procedural) Skill Evaluation
van der Vleuten, CPM, Schuwirth, LWT. Assessing professional competence:
from Methods to Programmes. Medical Education 2005; 39: 309–317

© 2012 Accreditation Council for Graduate Medical Education (ACGME)
Miller’s Model of Clinical Competence
Knows
Shows How
(Shows Can Do)
Knows How
Does
Miller, GE. Assessment of Clinical
Skills/Competence/Performance.
Academic Medicine (Supplement)
1990. 65. (S63-S67)
van der Vleuten, CPM, Schuwirth,
LWT, Scheele, F, Driessen, EW,
Hodges, B.
The assessment of professional
competence: building blocks for
theory development.
Best Practice & Research Clinical
Obstetrics and Gynaecology 24
(2010) 703–719
“Habitual Practice”
Evaluation
Tools
Psychometrically
Validated
“Objective”
Measurement
Tools

The “GME Envelope of Expectations”
AKA - Milestones
Aspirational
Goal
Graduating Resident
Intermediate Level Resident
Finishing PGY 1
Entering PGY 1
Expert
Proficient
Competent
Advanced
Beginner
Novice
PGY 1 PGY 2 PGY 3 PGY 4 PGY 5 MOC
© 2012 Accreditation Council for
Graduate Medical Education (ACGME)

© 2012 Accreditation Council for Graduate Medical Education (ACGME)
Clinical Competency Committee
“A year from now you will wish you had
started today”
Karen Lamb

© 2012 Accreditation Council for Graduate Medical Education (ACGME)
Clinical Competency Committee
May already be in place under a different name
A clinical version of the Scholarship Oversight
Committee
Start thinking about this and decide on composition,
procedure, data elements
What should be reviewed:
Continue to look at current methods of evaluations: OSCE,
simulation, 360-degree evaluations
Milestones, EPAs, narratives
Issues:
Time constraints
Large residency programs
Small fellowship programs

© 2012 Accreditation Council for Graduate Medical Education (ACGME)
Clinical Competency Committees
Learn your specialty milestones
Decide how to measure milestones
Narratives
EPAs
Teach the faculty the definitions
Teach the faculty the tools
FACULTY DEVELOPMENT IS KEY

© 2012 Accreditation Council for Graduate Medical Education (ACGME)
The difference between a beginning
teacher and an experienced one is
that the beginning teacher asks, "How
am I doing?" and the experienced
teacher asks, How are the children
(residents/fellows) doing?”
― Esm

© 2012 Accreditation Council for Graduate Medical Education (ACGME)
The Clinical Competency Committee
A group of faculty members trained in looking at
milestones using narratives or EPA’s
The same set of eyes looking at other evaluations:
End of rotation
Nurses
Patients and families
Peers
Others: OSCE, simulation, MCQ
The same process is applied uniformly

© 2012 Accreditation Council for Graduate Medical Education (ACGME)
The Clinical Competency Committee
Avoids common problematic issues:
“I don’t like to give negative evaluations”
“I spent little time working with this resident”
“Herd” mentality: positive or negative
Grade inflation
Vague statements:
“I just didn’t like this resident, but I can’t put my
finger on it”
Hearsay: I’ve heard she is lazy

© 2012 Accreditation Council for Graduate Medical Education (ACGME)
Move from Numbers to Narratives1
Numerical systems produce range restriction
(ABIM, others)
Narratives:
easily discerned by faculty
shown to produce data without range restriction
(Hodges and others) 1 Most recent reference:
Regehr, Glen, Ginsburg, S., Herold, J., Hatala, R., Eva, K., Oulanova, O.
Using “Standardized Narratives” to Explore New Ways to Represent
Faculty Opinions of Resident Performance.
Academic Medicine. 2012. 87(4); 419-427.

© 2012 Accreditation Council for Graduate Medical Education (ACGME)
Regehr G et al
19 faculty members interviewed
57 actual resident descriptions → 16 narrative
profiles created: represented range of resident
competence
14 clinicians grouped profiles to reflect various
levels of performance
Strong consistency in rankings
More consistency in decisions regarding
excellent, competent and problematic compared
to a numeric scale

© 2012 Accreditation Council for Graduate Medical Education (ACGME)
Entrustable Professional Activities
“Professional activities that together constitute
the mass of critical elements that operationally
define a profession”…….ten Cate
Units of work awarded at the moment when
supervisors confirm that the trainee is ready to
assume responsibility for such activities
Can happen at any time

© 2012 Accreditation Council for Graduate Medical Education (ACGME)
Conditions of EPAs
Part of essential professional work in a given context
Must require adequate knowledge, skill and attitude
Must lead to recognized output of professional labor
Should be confined to qualified personnel
Should be independently executable
Should be executable within a time frame
Should be observable and measurable in its process and
outcome (well done or not well done)
Should reflect one or more competencies

© 2012 Accreditation Council for Graduate Medical Education (ACGME)
EPA’s
Real life patient care episodes
Usually composed of elements of most if not all
“competencies”
Benchmark of performance is the ability to be entrusted
to perform care with “indirect supervision with direct
supervision available”
Progression: achievement of EPA’s of increasing
difficulty, risk, or sophistication
Proficiency: achievement of the most sophisticated
EPA’s required of the resident

Long Island Pilot Experience
• Six pediatrics milestones
• Two pediatrics programs
• Ward and PICU rotations/July 2012
• Replaced current questions on global
assessment form with milestones
Susan Guralnick, MD
Associate Dean/DIO Winthrop University Hospital
© 2012 Accreditation Council for Graduate Medical Education (ACGME)

Winthrop Evaluation form for ICS
© 2012 Accreditation Council for Graduate Medical Education (ACGME)

© 2012 Accreditation Council for Graduate Medical Education (ACGME)

Winthrop Faculty Training
After one hour, PICU and ward faculty reported:
They could “visualize” where a resident is at
They agreed with the interpretations
(low inter-rater variability)
They could use evaluations as effective feedback tool
They could define what to work on
Favorable response to milestones
© 2012 Accreditation Council for Graduate Medical Education (ACGME)

© 2012 Accreditation Council for Graduate Medical Education (ACGME)
Narratives and Milestones
Study in Internal Medicine Program
Time: 20 minutes to 6 hours for 6 residents
Ratings were very close
Residents preferred feedback using milestones
Better idea of their level of competency
Concrete descriptions provided them with the
knowledge of where they needed to improve – made
expectations clear

Expert
Proficient
Competent
Advanced
Beginner
Novice
Increase the Accreditation Emphasis on Educational Outcomes
© 2012 Accreditation Council for Graduate Medical Education (ACGME)

© 2012 Accreditation Council for Graduate Medical Education (ACGME)
The “Next Accreditation System”
in a Nutshell
Continuous Accreditation Model – annually updated
Based on annual data submitted, other data requested, and
program trends
Scheduled Site Visits replaced by 10 year Self Study Visit with
focused site visits as needed
Standards revised every 10 years
Standards Organized by
Structure
Resources
Core Processes
Detailed Processes
Outcomes

The Conceptual Change
From…
The Current Accreditation System
Rules
Corresponding Questions
“Correct or Incorrect”
Answer
Citations and
Accreditation Decision
Rules
Corresponding Questions
“Correct or Incorrect”
Answer
Citation and
Accreditation Decision
© 2012 Accreditation Council for Graduate Medical Education (ACGME)

The Conceptual Change
To…
“Continuous”
Observations
Assure that the Program Number of Potential
Fixes the Problem Problems Promote
Innovation
Diagnose
the Problem
(If there is one)
The “Next Accreditation System”
© 2012 Accreditation Council for Graduate Medical Education (ACGME)

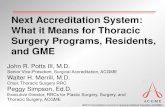
Conceptual Model of Standards Implementation
Across the Continuum of Programs in a Specialty
STANDARDS
Core and
Detailed:
Structure
Resources
Process
Outcomes
Initial
Accreditation
New
Programs
Core and Detailed:
Structure
Resources
Process
Outcomes
Withhold Accreditation
Withdrawal of Accreditation
2-4% 10-15% 75%-80%
2.8%
Accreditation
with Warning
New Programs,
Accredited Programs
with Major Concerns
Probationary
Accreditation
Core and Detailed:
Structure
Resources
Process
Outcomes
Maintenance of
Accreditation
Accredited Programs without
Major Concerns
Maintenance of
Accreditation with
Commendation
Core:
Structure
Resources
Process
Outcomes
© 2012 Accreditation Council for Graduate Medical Education (ACGME)

© 2012 Accreditation Council for Graduate Medical Education (ACGME)
Trended Performance Indicators
Annual ADS Update
Program Attrition – Changes in PD/Core Faculty/Residents
Program Characteristics – Structure and Resources
Scholarly Activity
Board Pass Rate – Rolling Rates
Resident Survey – Common and Specialty Elements
Clinical Experience – Case Logs or other
Faculty Survey – Core Faculty
Semi-Annual Resident Evaluation and Feedback
Milestones
Annual Sponsor Site Visit (CLER)

© 2012 Accreditation Council for Graduate Medical Education (ACGME)
Annual Data Collected and Reviewed
(Focus on Existing Information)
1. Annual ADS Update - Streamlined
1. Program Attrition
2. Program Characteristics – Structure and Resources
3. Scholarly Activity
2. Board Pass Rate – Rolling multi-year rates
3. Clinical Experience
4. Resident Survey
5. Faculty Survey – Core Faculty
6. Semi-Annual Resident Evaluation and Feedback
1. Milestones
2. Clinical Competency Committees
7. Sponsor Site Visit (CLER) TBD-total picture

© 2012 Accreditation Council for Graduate Medical Education (ACGME)
1. Annual Update Streamlined
33 questions removed
14 questions simplified
Almost no essay questions
Self-reported board pass rate removed
13 specialties now get directly, working with other
boards
Faculty CVs removed (except for PD)
11 MCQ or Y/N questions added

© 2012 Accreditation Council for Graduate Medical Education (ACGME)
Preparing for Annual Update
Identify Core Faculty and refine your list
Devote >15 hours/week
Track scholarly activity
Involved in resident evaluation
Members of clinical competency committee

© 2012 Accreditation Council for Graduate Medical Education (ACGME)
ADS Update Turnover
Examples of turnover – one or more of the
following leave the program:
Residents
Core faculty
Program director
Chair
CEO
*Turnover can sometimes be a good thing

© 2012 Accreditation Council for Graduate Medical Education (ACGME)
Current Mechanism to Collect Scholarly Activity
CVs currently reviewed only at time of SV
Textual data cannot be analyzed
No way to assess overall scholarly activity
Performance indicator cannot be created – no
trends available
RCs not be able to read all CVs every year
25% of ACGME database is filled with CVs
35% of Support calls involve faculty and questions
regarding CVs – most frequent call/complaint – about
19 calls per day
Programs do not keep CVs current – huge burden

© 2012 Accreditation Council for Graduate Medical Education (ACGME)
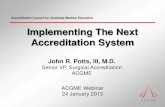
Scholarly Activity in NAS
Annual summary for faculty and
residents/fellows:
Publications (PubMed IDs and textbooks)
Number of presentations (conferences/grand rounds)
Grant activity (funding, PI)
Teaching responsibilities

© 2012 Accreditation Council for Graduate Medical Education (ACGME)
Example of Scholarly Activity Summary for Faculty

© 2012 Accreditation Council for Graduate Medical Education (ACGME)
2. Board certification
Nationally agreed upon outcome of training
RRCs working with ABMS boards
Subs will self-report
Pass rate only, not individual scores
Multi-year rolling rates for small programs

© 2012 Accreditation Council for Graduate Medical Education (ACGME)
3. Clinical Experience
Case Logs
Review the number and mix of cases
How do you know what your residents are doing?
Correct incomplete data entry
Need all (not just minimum) numbers
Multi-site programs
Tracking incomplete reporting
For those who do not use case logs, resident
survey questions may be added

© 2012 Accreditation Council for Graduate Medical Education (ACGME)
4. Resident survey
Emphasis on themes
De-emphasize individual questions
High level
Minimize single resident impact
Only significant deviation from compliance are
indicators
Trend data
Domains: Duty hours, Faculty, Educational
Content, Evaluations, Resources, Patient
safety, Teamwork

© 2012 Accreditation Council for Graduate Medical Education (ACGME)
5. Faculty Survey
Core faculty (presumed to be more
knowledgeable about program)
Similar domains as resident survey
Faculty supervision, Educational Content, Resources,
Patient safety, Teamwork
Similar timing as resident survey
Planned start in winter 2013 for Phase 1
specialties (2012-2013 data)

© 2012 Accreditation Council for Graduate Medical Education (ACGME)
Faculty Survey
Hours spent teaching and supervising
Questions
About program director
Faculty development
Scholarly activity
Fatigue
Patient safety

© 2012 Accreditation Council for Graduate Medical Education (ACGME)
6. ACGME Goal for Milestones
Specialty specific normative data and common
expectations for progress of individual residents
Less prescriptive ACGME program requirements,
lengthened program site visit cycles, less frequent
standards revision
Promote curricular innovation
Enhance curricular and rotation design flexibility
Development of specialty specific evaluation tools and
techniques
Opportunity for communication and improvement across
the continuum of medical education

© 2012 Accreditation Council for Graduate Medical Education (ACGME)
6. Milestones: Specialty Driven
• Drafts completed by 2012
• Phase 1 to start using milestones by July 2013
First milestones (Core) report December 2013
• Phase 2 to start using milestones by July 2014
First milestones report December 2014
• Clinical Competency Committees
• Formed for Phase 1 by January 2013
• Formed for Phase 2 by January 2014

© 2012 Accreditation Council for Graduate Medical Education (ACGME)
Challenges/Opportunities
Culture Change and Faculty Development
Program Directors, Designated Institutional Officials
Faculty
Review Committee Members
“Retooling” of ACGME Infrastructure and Personnel
Improving quality of faculty observations/documentation
The “Community of Educators” in each specialty has
come together and agree on:
core elements of the competencies (Milestones)
levels of performance
core methods of assessment

© 2012 Accreditation Council for Graduate Medical Education (ACGME)
Phase I and Phase II Programs
How was the decision made to include programs
in Phase I or Phase II?
Phase I, aka Early Adaptors, Early 7:
Internal Medicine
Pediatrics
Urology
Orthopedic Surgery
Emergency Medicine
Diagnostic Radiology
Neurologic Surgery

© 2012 Accreditation Council for Graduate Medical Education (ACGME)
“If you talk about it, it’s a dream.
If you envision it, it’s possible,
but if you schedule it – it is real.
Anthony Robbins

Key Dates for Phase I specialties under NAS ACGME News and Reviews, J Grad Med Educ, 2012; 4(3): 399
Month & Year ACGME Activities Program and Institutional
Activities
Spring 2012 CPR & PR for Phase I
specialties categorized into
core, detail & outcomes
SV for Phase I programs with
cycle length 3,4,5y moved to
NAS
7/1/12-6/30/13 Phase I programs provide data
including the annual ADS
update, resident survey, faculty
survey, case log data, and data
on scholarly activities
July & Aug 2012 Alpha testing of CLER process
September 2012 Beta testing of CLER visits
December 2012 Milestones are published for all
core specialties
© 2012 Accreditation Council for Graduate Medical Education (ACGME)

Key Dates for Phase I specialties under NAS ACGME News and Reviews, J Grad Med Educ, 2012; 4(3): 399
Month & Year ACGME Activities Program and Institutional
Activities
March 2013 Final SVs in current accreditation
system are completed for Phase I
programs newly accredited or with a
short cycle length
June 2013 Phase I programs form CCC
and faculty members prepare to
assess milestones
July 2013 Phase I Specialties and subspecialties begin operating under NAS
7/1/13-6/30/14 Phase I subspecialty milestone
development begins
Phase I milestones
assessments begin for core
programs
Fall 2013 RRC in Phase I specialties review
annual data from Academic year
2012-2013 (without milestone data)
December 2013 Core Programs submit the first
set of Phase I milestones
assessments to ACGME
© 2012 Accreditation Council for Graduate Medical Education (ACGME)

Key Dates for Phase I specialties under NAS ACGME News and Reviews, J Grad Med Educ, 2012; 4(3): 399
Month & Year ACGME Activities Program and Institutional
Activities
June 2014 Programs submit the second set
of Phase I milestones
assessment to ACGME
Fall 2014 RRCs in Phase I specialties
review annual data from AY
2013-2014
First self-study SVs for Phase I
programs with a 2014 self-study
date
© 2012 Accreditation Council for Graduate Medical Education (ACGME)

Subspecialties under NAS
Month & Year ACGME Activities Program and Institutional
Activities
July 2013 – June
2014
Subspecialty programs develop
milestones
July 2015???? Milestones assessments begin
for subspecialty programs?
© 2012 Accreditation Council for Graduate Medical Education (ACGME)
Note: Subspecialties might not need full year to develop
Milestones – will focus on medical knowledge and patient care

Key Dates for Phase II specialties under NAS
Timelines will lag at least 1 year behind
the Phase I specialties
Changes may be made based on
knowledge gained from Phase I efforts
(learning as we go)
Currently creating schedule for Phase
II RRC members to attend conferences
to orient them to NAS. RC members
and EDs from Phase I will help in this
effort
© 2012 Accreditation Council for Graduate Medical Education (ACGME)

Self Study & Program Improvement
ACGME self study visits begin July 2014
Internal reviews
No longer required as of July 2013
Still may be helpful for some programs
Schedule, reviewers and format flexible
Don’t do it for accreditation
Tool for program improvement
ILP on steroids
© 2012 Accreditation Council for Graduate Medical Education (ACGME)

Self Study & Program Improvement
NOT A PIF
Tool for improvement
Regular goal setting
Longer term: 3-5 years
Includes self-reflection/self-study
Consider SWOT (strengths/weaknesses/
opportunities and threats)/stakeholders
Consider program outcome trends
Don’t have to wait until ACGME
announces visit
© 2012 Accreditation Council for Graduate Medical Education (ACGME)

Self-Assessment: Common Benefits
Identifies successes and opportunities for
improvement
Jump-starts a new change initiative or steps up an
existing improvement effort
Energizes the workforce and stakeholders
Focuses the program/organization on common goals
relevant to the program
Measures progress against goals
Assesses performance against benchmarks
(within or outside the industry)
Aligns resources with strategic objectives
© 2012 Accreditation Council for Graduate Medical Education (ACGME)

Suggested “to-do” list (not all-inclusive):
Define and select core faculty
Optimize annual update and board scores
Learn about milestones
Create clinical competency committees
Faculty development re: milestones
Integrate GME and quality/safety
Develop a self-study and strategic plan
© 2012 Accreditation Council for Graduate Medical Education (ACGME)

© 2012 Accreditation Council for Graduate Medical Education (ACGME)
Webinars – coming to a computer near you
CLER
NAS Update
Milestones/CCC/Evaluations
Self-Study
Will be recorded and made accessible
Dedicated email address for questions
Blogs?

Accreditation Council for Graduate Medical Education
Thank You!
© 2012 Accreditation Council for Graduate Medical Education (ACGME)