The National Ribat University College of Post...
62
The National Ribat University College of Post Graduate studies & Scientific Research Faculty of Nursing Sciences Assessment of nurses knowledge regarding the nursing care of the preeclamptic patients in Ribat UniversityHospital, Sahroon Hospital and Saad Aboalal Hospital in Khartoum State October to December 2014 A research thesis submitted in partial fulfillment for the requirement of the master degree in obstetrics and gynecological nursing By: Saria Mahgoub Balla Abdalla B.sc University of Gezira 2010 Prof.Um.Gumaa Mohammed Abdel Regal Hamid Nursing s and Midwifery educator
Transcript of The National Ribat University College of Post...

The National Ribat University
College of Post Graduate studies
& Scientific Research
Faculty of Nursing Sciences
Assessment of nurses knowledge regarding the nursing care of the
preeclamptic patients in Ribat UniversityHospital, Sahroon Hospital
and Saad Aboalal Hospital in Khartoum State
October to December 2014
A research thesis submitted in partial fulfillment for the
requirement of the master degree in obstetrics and gynecological
nursing
By:
Saria Mahgoub Balla Abdalla
B.sc University of Gezira 2010
Prof.Um.Gumaa Mohammed Abdel Regal Hamid
Nursing s and Midwifery educator



To my fathers sole
To my dear mother who always support s and encourages me to
achieve my goals
To my sisters and brothers
To all my family members.
To my teachers.
To my colleguses

First of all, thanks to God for His help,and mercy which enabled me to accomplish this study.
I would like to thank all the individuals who were so instrumental in helping me to accomplish this study.
My thanks to the faculty of nursing who gave me the chance to conduct this research.
I greatly indebted to my supervisor Prof. Um.Gumaa,who motivated and gave me confidence with her valuable instructions and
guidance. I also would like to express my greatest thanks to the nurses who
participanted in this study Special thanks with my special word of gratitude to my mother, who is
asking God to help me always.
Special thanks and gratitude To my dear batool sidig who consider
my second mother For her support and assistance through this
study .
Sincere deepest appreciation to my uncle Ahmed Ibrahim for her support and assistance
Lastly my gratitude and love for my family
LIST OF CONTENTS

Title Page
Dedication I
Acknowledgement II Table of contents III -IV
English abstracts V
Arabic abstract VI
List of figures VII
List of tables VIII
List of abbreviations IX
Chapter one
1.1Introduction 1 1.2Statement of the problem 1
1.3Justification 2 1.4Objectives 2
Chapter Two
2. Literature review and previous studies 3-19 Chapter Three
3. Methodology 20
3.1 Study Design 20
3.2 Study Area 20
3.3Study Period 20
3.4 study population 20
3.4.1 Inclusion criteria 20 3.4. 2 Exclusion criteria 20
3.5 sample size 20 3.6 Data collection tools 20
3.7Data collection methods 20 3.8Data analysis 20
3.9 Ethical consideration 20

Chapter Four
4.Results
21 -34
Chapter Five
5.1 Discussion 35-37 5.2Conclusion 38
5.3 Recommendations 39
5.4 References 40- 43
Appendix
Questionnaire
i.
ABSTRACT

Background:
and high blood pressureeclampsia is a disorder of pregnancy characterized by -Pre
.protein in the urineamounts of
Objective:-The study aims to assess BSC nurses knowledge regarding the
nursing care of the pre-eclamptic patients
Methodology :-
This is a descriptive cross-sectional based study, conducted in three Khartoum
State hospital during the period from October to December 2014. . It involved 50
nurses ,data collected by questionnaire, analyzed by Statistical Package for Social
Science (SPSS) and the study presented in tables and figures
Results: The results revealed that most participants (90%) have V good knowledge about
risk factor,
40(80%) have V good knowledge regarding care of sever preeclampsia and
33(6%) from them knew about effect of preeclampsia on fetus
Only 4(8%) of the nurses know about progresses from mild preeclampsia to sever
preeclampsia.
48% of participant had inadequate knowledge about definition of pre eclampsia.
Although the effect of preeclampsia on maternal increase maternal death
unfourtently (56%) of participant did not known the effect of pre eclampsia on
mother.
The study showed there is significant association between years of experience and
participants knowledge P value > 0.05
Conclusion
Generally the nurse have good knowledge of some aspects of the preeclampsia
and did not know other aspects
Recommendation: researcher recommend frequent refreshing courses regarding preeclampsia
Encourage them to update them self.
Conduct further studies related to this research.
البحث خصمل

خلفية البحث:
ير فر غر ا انر و يرو خرة ر يرض يارا ل نهلرم زرر فارت را -ياقبم االرتعاج:
انبل انبضت ف
-: اهداف الدراسه
االرتعاج()ياقبم ان ع انزضض فكانضس ةرخ ى يعضف انضغات هت تق
هج االبحث:من
الرر انطضمررو ارر ل ان زررض يرر يسزشررقات فرر رر ان را رر رر يقجعرر خضررت فرر رر
ت تى خو انباات ي ا ل ا زبا,يضغ 00و. شهت ان را 2012 زفضان ةسبض
اال اراي عضغرت انزرايح فر ى تى تلهم انباات عر مضرا انزلهرم ,اااا ن ض ان را
خ ال شكال.
نتيجة الدراسة :
لمرض تسمم الحملهبه المؤبالعوامل جيده جدا معرفه الديه عينه البحث أظهرت الدراسة أن 33لمدريض ماببدل اترتعدال الحداده و بالعنايده ( من المشاركات لديهن معرفه جيدة جددا 04%)04
%( لديهن معرفه بتاثير مرض تسمم الحمل على الجنين 66)
الى الحادة تسمم الحمل من البسيطة مرض اعراض %(فقط لديهن معرفه جيدة جدا عن 0)0
تسسم الحمل عن تعريفكافيه المشاركات لم يكن لديهن معرفه %( من00بينما )
%( مدن المشداركات فدى الدراسده لدم 66تاثير مرض تسمم الحمل يزيد من وفيات اتمهات لالسدف)
.يعرفن هذا التاثير
( P< 0.05ة بين المعرفه وسنوات الخبره )بيمتشير الدراسه الى وجود عالبه طرديه
: مستخلص البحث
نى نلان يا قبم االرتعاج يعضف فبعض اندال انزعهق فانضعا انال ان لثبع ان عيا
اندال ااض تعضف
التوصيات:
.يا قبم االرتعاج رعاز يض ر ات ت رل نهضغات فا طص انبا ث فعم ت
انلث عه ة را ات ااض ق اناه ف ا انبلث
تدا يض تسى انلمانضغات ا رة ي يعضفز تشدو
LIST OF FIGURES

Figure
NO
Title Page
NO
(1) percent distribution of study sample according to their age 21
(2) percent distribution of study sample according to their years of
experience
22
(3) distribution of study sample regarding of training course about
preeclampsia
23
LIST OF TABLES
Table NO Title Page NO

(1) knowledge of the study sample about Definition of pre- eclampsia 24
(2) knowledge of the study sample about causes of pre- eclampsia 24
(3) knowledge of the study sample about risk factors of pre-eclampsia 25
(4) knowledge of the study sample about the serious (subjective)signs of
severe preeclampsia.
25
(5) knowledge of the study sample about assessment of fetal wellbeing. 26
(6) knowledge of the study sample about bed rest for preeclamptic mother. 26
(7) knowledge of the study sample about weight measuring 27
(8) knowledge of the study sample about diet for preeclamptic mother 27
(9) knowledge of the study sample about mild to severe signs indicate progresses of preeclampsia
28
(10) knowledge of the study sample regarding care before administration of
Mgso4 28
(11) knowledge of the study sample about signs of Mgso4 toxicity.
29
(12) knowledge of the study sample about nursing care of sever
preeclampsia. 29
(13) knowledge of the study sample about indications for delivery of
preeclamptic mother.
30
(14) knowledge of the study sample about intrapartum care of preeclamptic
mother.
30
(15) knowledge of the study sample about signs of HELLP syndrome. 31
(16) knowledge of the study sample about effect of preeclampsia on mother. 31
(17) knowledge of the study sample about effect of preeclampsia on fetus. 32
knowledge of the study sample regarding preeclampsia in relation to
experience by years. 33-34
LIST OF ABBREVIATION ACOG American Congress of Obstetricians and Gynecologists
ARDS cute respiratory distress syndromeA

Bp Blood Pressure
BMI Body Mass Index
CBC Complete Blood Cells
C/S Cesarean Section
C T G Cardio ToCography
DIC Disseminated Intravascular Coagulopathy
DTRs Deep Tendon Reflexes
HELLP syndrome Hemolysis Elevate Liver Enzymes Low Platelets
I&O Intake and Output
IUGR Intra Uterine Growth Restriction
LOC Level of Consciousness
MgSo4 Magnesium Sulfate
PIGF actorlacental Growth Fp
PIH
Pregnancy Induced Hypertension
RBCs Red Blood Count SPSS Statistical Package for Social Sciences.
PPT Partial ThromboPlastin Time
PT Prothrombin Time
SEng Soluble Endoglin
SFlt Soluble Fms-like tyrosine kinase
VEGF actorascular Endothelial Growth FV
WHO World Health Organization

CHAPTER ONE
Introduction
1.1Introduction
Preeclampsia is a serious public health problem that affects the group of pregnant women
(1). the disease has severe obstetrics implications for decades has been located at the
international level as one of the three major causes of maternal death(2).
Approximately 800
women die from pregnancy or childbirth-related complications around the world every day
(3). Ninety-nine percent occur in developing countries.The complications that account for
80% of all maternal deaths are:-severe bleeding mostly bleeding after child birth,
infections usually after childbirth ,high blood pressure during pregnancy (preeclampsia
and eclampsia ) (4) .
Globally preeclampsia is a leading cause of maternal and infant illness and death.
By conservative estimates, these disorders are responsible for 76,000 maternal and
500,000 infant deaths each year (5).
Preeclampsia and related hypertensive disorders of
pregnancy impact 5-8% of all births in the United States. Incidence rates for preeclampsia
alone - in the United States, Canada and Western Europe, range from 2-5%.( 6,7)
In Latin
America, preeclampsia is the one cause of maternal death( 8)
. In the developing world,
severe forms of preeclampsia and eclampsia are more common, ranging from a low of 4%
of all deliveries to as high as 18% in parts of Africa( 6)
.
Maternal mortality in Sudan with pre-eclampsia/eclampsia accounting for 4.2% of
the obstetric complications and 18.1% of maternal deaths (9) .
In developing countries, a
woman is seven times as likely to develop preeclampsia than a woman in a developed
country. From 10-25% of these cases will result in maternal death (10)
.Preeclampsia should
be detected and appropriately managed before the onset of convulsions (eclampsia) and
other life-threatening complications (3).
1.2 Statement of the problem:
Pre-eclampsia affects approximately 2-8% of all pregnancies worldwide(11)
Ten
million women develop preeclampsia each year around the world. Worldwide about
76,000 pregnant women die each year from preeclampsia and related hypertensive
disorders. And, the number of babies who die from these disorders is thought to be on the
order of 500,000 per annum (1 2)
.Pre-eclampsia and eclampsia account for about 9% of

maternal deaths in Africa (13).
There is an extremely high maternal mortality in Sudan with
pre-eclampsia/eclampsia accounting for 4.2% of the obstetrics complications and 18.1% of
maternal deaths (9)
.
1-3 Justification:
Maternal mortality in Sudan with pre-eclampsia/eclampsia accounting for 4.2% of the
obstetric complications and 18.1% of maternal deaths (9)
.
In most instances, the nurse is the primary person involved in the care of the hospitalized.
The nurse is probably the first one to see the patient and will spend more time with them
than other health care provider.
The nurse has in a unique position to take care of preeclampsia patients and prevent
certain complication. This seems to indicate a need for current assessment of nurse’s
knowledge regarding preeclampsia patient
1-4 Objectives:
-4-1General objective:-
To assess nurses knowledge regarding the nursing care of the pre eclamptic patients.
1-4-2 Specific objectives:-
To assess nurses' knowledge regarding to rest of preeclampsia
To assess nurses' knowledge regarding to diet of preeclampsia .
To assess nurses' knowledge regarding to measuring blood pressure of
preeclampsia
To assess nurses' knowledge regarding to subjective sing of preeclampsia
To assess nurses' knowledge regarding to weight of preeclampsia
To assess nurses' knowledge regarding to monitoring of fetal condition of
preeclampsia
Assess the nurses' knowledge regarding the effected of preeclampsia on fetus
Assess the nurses' knowledge regarding the effected of preeclampsia on the
mother

CHAPTER TWO
Literature review
2.1 Definitions.
Preeclampsia: Is multisystem disorder of unknown etiology characterized by
development of hypertension to the extent of 140/90 mmHg or more with proteinuria
induced by pregnancy after the 20th week in previously normotensive and non protein
uric woman (14) .
2.2 Classification of preeclampsia
American Congress of Obstetricians and Gynecologists (ACOG) classified
Preeclampsia based on the severity using parameters such as blood pressure and systemic
involvement.
They categorized :- preeclampsia as mild to moderate and a severe group.
Mild to moderate preeclampsia :-include blood pressure of 140 to 159 mmHg systolic
and/or 90 to 109 mmHg diastolic.
Severe preeclampsia:- is said to set in if one or more of the following criteria are present;
i.e. BP is ≥160 mmHg systolic and/or ≥110 mmHg diastolic (on 2 occasions at least 6
hours apart, while the patient is on bed rest), proteinuria of ≥5 g/24 hours or ≥3+ (on 2
random urine samples, collected at least 4 hours apart), oliguria <500 mL/24 hours,
cerebral or visual disturbances, pulmonary oedema or cyanosis, epigastric or right upper
quadrant pain, impaired liver function, thrombocytopenia, fetal growth restriction(15)
2.3 Causes:-
There is no definitive cause of preeclampsia(16)
Many theories have attempted to explain why pre-eclampsia arises, and have linked
the syndrome to the presence of the following:
Endothelial cell injury
Immune rejection of the placenta
Compromised placental perfusion
Altered vascular reactivity

Imbalance between prostacyclin and thromboxane
Decreased intravascular volume
Increased central nervous system irritability
Disseminated intravascular coagulation
Uterine muscle stretch (ischemia)
Dietary factors, including vitamin deficiency
Genetic factors(17)
Environmental factors, e.g. air pollution(18)
Obesity ( 1 9)
Unfamiliar sperm theory (20)
Thyroid dysfunction: Subclinical hypothyroidism in early pregnancy, compared with
normal thyroid function, has been estimated to increase the risk of pre-eclampsia
with an odds ratio of 1.7 (2 1)
.
2.4 Pathological changes:-
Abnormalities in the maternal immune system and insufficiency of gestational immune
tolerance seem to play major roles in pre-eclampsia. One of the main differences found in
pre-eclampsia is a shift toward Th1 (T hellper cell) responses and the production of IFN-
(Inter Feron ). The origin of IFN-γ is not clearly identified and could be the natural killer
cells of the uterus, the placental dendritic cells modulating responses of T helper cells,
alterations in synthesis of or response to regulatory molecules, or changes in the function
of regulatory T cells in pregnancy . Aberrant immune responses promoting Preeclampsia
may also be due to an altered fetal all orecognition or to inflammatory triggers( 22).
It has
been documented that fetal cells such as fetal erythroblasts as well as cell-free fetal DNA
are increased in the maternal circulation in women who develop pre-eclampsia. These
findings have given rise to the hypothesis that pre-eclampsia is a disease process by which
a placental lesion such as hypoxia allows increased fetal material into maternal circulation
that leads to an immune response and endothelial damage ultimately resulting in pre-
eclampsia and eclampsia.
Some studies suggest that hypoxia resulting from inadequate perfusion upregulatess Flt-
1(Small Firms Impact Test), a VEGF(Vascular Endothelial Growth Factor) and
PlGF(Placental Growth Factor ) antagonist, leading to a damaged maternal endothelium

and restriction of placental growth( 2 3).
In addition, endoglin, a TGF-beta (Transforming
Growth Factor) antagonist, is elevated in pregnant women who develop pre-eclampsia (24)
Soluble endoglin is likely upregulated by the placenta in response to an upregulation of
cell-surface endoglin produced by the maternal immune system, although there is also the
potential that sEng is produced by the maternal endothelium. Levels of both sFlt-1 and
sEng increase as severity of the disease increases, with levels of sEng surpassing levels of
sFlt-1 in HELLP syndrome cases. Recent data indicate that Gadd 45a stress signaling
regulates elevated sFlt-1 expression in pre-eclampsia(25).
2.4.1 Worsening pathologic changes:-
HELLP syndrome development Characterized by
H- hemolysis of red blood cells(microangiopathic)
EL-Elevated liver enzymes (liver dysfunction)
LP-Low platelet count less than 100,000/mm) (thrombocytopenia)(26)
2.6 Risk factors:-
Known risk factors for preeclampsia include: -
Nulliparity (never given birth)
Diabetes mellitus
Renal disease
Chronic hypertension
Family history of preeclampsia
Advanced maternal age (>35 years)
Obesity
Anti phospholipid antibody syndrome
Multiple gestation (27)
2.7 Signs and symptoms:-
-woman develops: pregnant eclampsia is diagnosed when a-Pre
Blood pressure more than 140 mm Hg systolic or more than 90 mm Hg diastolic on two
separate readings taken at least four to six hours apart after 20 weeks gestation in an
individual with previously normal blood pressure.
Proteinuriahour urine sample or -mg) or more of protein in a 24 ams (300more than 0.3 gr
a SPOT urinary protein to creatinine ratio more than 0.3 or a urine dipstick reading of 1+

or greater (dipstick reading should only be used if other quantitative methods are not
available) (28)
.
2.7.1 Subjective signs
severe Headaches or pressure in the head (usually frontal)
Visual changes, such as blurred vision
Rapid onset edema of the face or abdomen or pitting edema in the feet or legs
after 12 hours of bed rest
Oliguria less than 500 ml/24 hours
Hyperreflexia
Nausea and vomiting (especially if new)
Epigastric pain(heart burn) or right upper quadrant pain (29)
2.7.2 HELLP Syndrome signs:-
HELLP syndrome is actually a laboratory diagnosis for a variant of sever pre-eclampsia .
The primary presentation is consistent with hepatic dysfunction evidenced by findings
from the patients liver function test. HELLP syndrome is characterized by rapidly
deteriorating liver function and thrombocytopenia. Liver capsule distention often produce
epigastric pain (30)
.
2.8 The nurses role in assessment and diagnosis:-
Early detection and appropriate management can minimize the severity of the
condition .
A comprehensive history taking at the womans first meeting with the midwife
will identify:-
Adverse social circumstances or poverty which could prevent the woman from
attending for regular antenatal care .
The mothers age and parity
First pregnancy or new partner with this pregnancy
A family history of hypertensive disorders
A past history of pre – eclampsia
2.8.1 Social history:-
(Marital status , cultural beliefs ,drug, tobacco ,and alcohol use )
Tobacco use may decrease risk of preeclampsia ,but increase risk of low birth weight
,placental abruption and over all maternal health. Advised to avoid alcohol, tobacco and
limit caffeine intake (29)
The presence of underlying medical disorders for example, renal disease, diabetes and
thromboembolic disorders .
On subsequent visits the midwife must take note of any further pregnancy
associated risk factors such as multiple pregnancy . The two essential features of
preeclampsia, hypertension and proteinuria, are assessed for at regular intervals
throughout pregnancy .
2.8.2 Blood pressure measurement:-
In order to detect incipient increases in blood pressure , the midwife should
take the mother s blood pressure early in pregnancy and compare this with all
subsequent readings , taking into account the normal pattern in pregnancy
It is important to consider several factors in assessing blood pressure. BP should not
be taken immediately after a woman has experienced anxiety ,pain , a period of
exercise or has smoked (31) .
. Use correct cuff size ,cuff should cover 80% of the upper arm or be 1.5 time
Length of the upper arm
Small cuff results in elevated readings
Large cuff result in falsely low readings.
BP measurement altered by position
BP is lowest( by 10 to 20 mm Hg) in lateral recumbent position
BP is highest when supine or standing ,and intermediate when sitting
Sitting position with arm at heart level using left or right arm.
The arm should be supported on a desk at level of the heart.
BP may vary by>10mm Hg with each arm ,record the higher reading .
Diastolic pressure should be record at:-
korotkoff phase V(disappearance of sound)
Not korotkoff phase IV (multing sound)
If the BP is elevated allow the woman to rest for 5 to 10 minutes then retake it.
Measurement with an automated devise should be checked with a manual device (29)

2.8.3 Urinalysis:-
Proteinuria is defined as the excretion of 300mg or more of protein every 24hours.
Check and record dipstick proteinuria:
daily if proteinuria is < 1+ on dipstick
twice if proteinuria is 1+ on dipstick
every specimen if proteinuria is 2+ on dipstick
notify the medical officer of increasing proteinuria(30)
2.8.4 Edema and excessive weight gain:-
These used to be included in the diagnostic criteria for preeclampsia but both are
variable findings and nowadays are usually considered only when a diagnosis of
preeclampsia has been made based on other criteria. Clinical edema may be mild
or severe in nature and the severity is related to the worsening of the preeclampsia
. Odema of the ankles in late pregnancy is a common occurrence . It is of a
dependant nature , usually disappears overnight and is not significant in the absence of
raised blood pressure and proteinuria. However , the sudden severe widespread
appearance of oedema is suggestive of preeclampsia or some underlying pathology
and further investigations are necessary. This oedema pits on pressure and may be
found in non dependent anatomical areas such as the face ,hands, lower abdomen,
vulvas and sacral areas . 2.9 Investigation:-
Complete urine examination: for protienuria, pus cell ,RBCs ,casts, specific gravity ,
culture and sensitivity .
Complete blood count (CBC)
Clotting studies (bleeding time , prothrombin time (PPT) partial thromboplastin time
(PPT) and fibrinogen).
liver enzyme (lactate dehydrogenase)
Kidney function test ( Serum uric acid >6mg % is abnormal during pregnancy)
Fetal condition (The fetus should be monitored by means of the cardiotocograph
fetal movement counts and regular sonar's for bio-physical profiles) (31).

2.9.1Laboratory tests affected by preeclampsia and HELLP syndrome
Pregnancy Preeclampsia
Hemoglobin 10-12g/dl Decrease in HELLP
Hematocrit 32%-40% Increase ,Decrease in
HELLP
Platelets 150,000-400,000/mm Decrease
Fibrinogen 300-600mg/dl Decrease
Fibrin split product Absent or minimal Increase
Prothrombin time 10-14sec Unchanged
PPT 20-31sec Unchanged
Bleeding time 1-3min(Duke) Unchanged
2-4min(Ivy) Decrease
2-8min(template) Increase
Hemolysis peripheral
smear
N/A A not applicable HELLP schistocytes or
burr cells present
Factors VII,VIII,IX,X Increase Increase
Factors XI,XIII Decrease Decrease

RENAL
Creatinine 0.4-1mg/dl Increase
blood urea and nitrogen 5-10g/dl Increase
Uric acid <6mg/dl Increase in HELLP
Creatinine clearance 130-180ml/min Decrease in HELLP
Uric acid clearance 10%Uric acid clearance
Hepatic
Alkaline phosphatase 60-480IU/ml Increase in HELLP
Albumin 2.8-3.7g/dl Decrease
Bilirubin Slight elevation from 0.2-
0.9mg/dl
Increase in HELLP
lactate dehydrogenase 90-200IUinternational units Increase in HELLP
2.10Care and management:-
The only known definitive treatment for preeclampsia is delivery of the fetus and Placenta.
The timing of delivery should balance the desire for optimal perinatal outcomes for the
fetus while reducing maternal risks. (32)
The severity of disease and the maturity of the
fetus are primary considerations (33)
These considerations are situation-specific and
management will vary with situation, location, and institution. Treatment can range from
induction of expectant management to expedited delivery of the fetus and placenta by
, in addition to pharmaceutical interventions. Important in Caesarian section or labor
management is the assessment of vulnerable maternal organ systems when possible,
management of severe hypertension, and prevention and treatment of eclamptic seizures(32)
.Separate interventions directed at the fetus may also be necessary.
Blood pressure:-
during pregnancy should hypertension The WHO recommends that women with severe
receive treatment with anti-hypertensive agents(34)
Severe hypertension is generally
considered systolic BP of at least 160 or diastolic BP of at least 110 (28) .
Evidence does not
support the use of one anti-hypertensive over another (32)
The choice of which agent to use

should be based on the prescribing clinician's experience with a particular agent, its cost, and
its availability. Diuretics are not recommended for prevention of preeclampsia and its
complications (34) .Labetolol, Hydralazine and Nifedipine are commonly used antihypertensive
agents for hypertension in pregnancy (7).ACE inhibitors and angiotensin receptor blockers are
contraindicated as they affect fetal development (19).
The goal of treatment of severe hypertension in pregnancy is to prevent cardiovascular,
kidney, and cerebrovascular complications (28)
Care of mild pre-eclampsia
Rest:- The woman should be in bed preferably in the left lateral position as much as
possible to lessen the effects of vena cava compression .rest in is to be continued until all
preeclamptic manifestations subside when proteinuria develops in addition to
hypertension ,the risks to the mother and fetus are considerable increased Admission to
the hospital is required at this stage to monitor and evaluate the maternal and fetal
condition.
Rest increases renal blood flow causing increases dieresis, increases uterine blood
flow causing placental perfusion and reduces blood pressure (14)
.
Activity level:-exercise amount and frequency (advised to engage in 30 minutes of
moderate exercise on most days.
Diet:-
Nutritious well balanced diet with food high in roughage 60 to 70g protein and 1200mg
calcium.
No sodium restriction limit excessively salty foods
Advised to drink six to eight 8ounce glasses of water per day .
Edema:-dependent edema (lowest or most dependent parts of the body) is common
during pregnancy .
Assessment of degree of edema
Minimal edema of lower extremities—1+
Marked edema of lower extremities—2+
Edema of lower extremities, face and hands—3+
Generalized edema including abdomen and sacrum—4+
pitting edema leaves a small indentation or pit after finger is applied to the area

Deep tendon reflexes (DTRs):-usually patellar reflex)classification
No response:0, sluggish ordiminised:1+,Active or normal:2+ ,Brisk:3+,and Brisk with
beats of clonus:4+ .
Assessment of clonus:-Briskly dorsiflex the foot while slightly flexion the knee ,Apply
continues pressure to sole of the foot ,involuntary oscillation are seen between flexion and
extension and record as number of beats(eg three beats clonus)
Weight gain:-
Daily weighing the patients at the same time (Average weight gain during pregnancy is
25to 35 pound , excessive weight gain is 2 pounds per day or 5 pounds per week (29)
Blood pressure:-
Blood pressure monitor daily every 4 to 6 hours (26)
.
Abdominal examination:-
Measure fundal height in centimeters from symphysis pubis to top of the funds between 20
to 32weeks, the fundal height should approximate the gestational age (29)
Is carried out
daily .Any discomfort or tenderness should be recorded and reported immediately to
the doctor as this may be a sign of placental abruption (31)
(uterine tenderness, hyper
systole, sustained abdominal pain,dark red vaginal bleeding, increase fundal height (29).
Urinalysis :- urine tested for albumin using first-voided specimen of the day ( 26)
.
Dipstick a clean catch urine specimen for presence of protein, mild preeclampsia
2+or3+,severe preeclampsia 3+or4+ , A 24-hour urine collection can measure the quantity
of protein mild preeclampsia proteinurea3to4g sever protein urea more than5g ,measure
intake and output oliguria is less than 30ml /hr or 120ml/4hr
Fetal assessment:-
To determine fetal health and well-being.This is done by the use of the following:-
Assess fetal heart rate with Doppler or electronic fetal monitors(normal baseline
rate110 to160bpm and note presence of acceleration and absent of decelerations)
Kick chart Fetal movement count
Non stress test (NST),Biophysical profile(BPP)
Serial ultrasound scans to check for fetal growth and amniotic fluid index(AFI)
Amniocentesis to assess pulmonary maturity (L/S ratio of 2:1) .
Care of severe preeclampsia:-

Pre-eclampsia is classified as severe when the diastolic blood pressure is >110mmHg on
two occasions at least twenty minutes
The following assessments should be carried out:-
The patient s blood pressure should be recorded at least hourly
The following symptoms and signs of imminent eclampsia should be reported
immediately :-
A blood pressure of 160/100 mmHg, despite treatment together with 3+ proteinuria
and severe or sudden increase in edema.
Oliguria
Severe headaches
Hyperreflexia ,irritability , restlessness, visual phenomena (spots before the eyes or
difficulty in focusing ) and a tendency to rub the nose
Pain over the liver
Pulmonary edema or cyanosis .
Test for proteinuria four timers per day .
Monitor fetal well-being by listening to the fetal heart 4 hourly and with CTG
at least 8 hourly.
Insert an indwelling urinary catheter and strictly record the out put4 hourly .
The same blood test as in mild pre-eclampsia.(31)
Pharmacologic therapy:-
Anticonvulsive therapy:-
Magnesium sulfate is the drug of choice in the prevention and treatment of seizures
Action:-decrease acetylcholine released by nerve impulse, therapy depresses CNS and
provides anticonvulsant effect
Acts peripherally as a vasodilator with transient decrease BP use with caution when renal
function is impaired contraindicated with myocardial damage heart block.
administered as secondary infusion (piggyback)by infusion pump 40g of magnesium
sulfate /1000ml intravenous (IV) fluid= 1g/25ml, Intramuscular (IM) route is not
recommended IM dose 5g, every 4hours using Z-track technique .
Potential side effects:-
Headache, flushing .diaphoresis, lethargy, nausea blurred vision

Antidote:-calcium gluconate 5to10mEqIV push over 1to 2 minutes (only as order)
Phenytoin can be used is magnesium sulfate is contraindicated
Antihypertensive therapy
Initiated when systolic blood pressure >160mmHg diastolic pressure>110mmHg
-Risk associated with blood pressure >160/110mmHg
Renal, hepatic , cardio cerebrovasular (left ventricular failure, cerebral Hemorrhage)
Most commonly used drugs are hydralazine and labetalol then nifedipine (procardia) Hydralazine
hydrochloride (apresoline):-
Reduces by relaxing smooth muscle result vasodilation reduces peripheral vascular
resistance increases cerebral and renal blood flow maybe contraindicated with cardiac
disease of side effects of tachycardia increase cardiac output and oxygen consumption
Dosage /Route:-for acute dosing 5-10mg IV push over 1-2min for a maximum of 30mg
Side effects:- tachycardia ,dizziness ,headache ,palpitations
Nursing intervention:-
Check BP every minute for 5 min, then every 5 min for 30 min
Goal to maintain diastolic BP between 90and 100mmHg.
Hypotension might decrease uteroplacental perfusion
Monitor fetal heart rate continuously
Assess intake and out put use with caution if tachycardia is present .
labetalol hydrochlorid (normodyne)
Alpha-and bête-blocker decreased peripheral resistance without significant change in
cardiac output or causing tachycardia contraindicated with asthma and congestive heart
failure.
Dosage /Route:-IV bolus doses initial dose 20mg if needed can give 40mg 10 min later
,then 80 mg10min after that to maximum of 300mg
Sideeffects:-orthostatic hypotension dizziness ,headache ,nausea/vomiting sweating
bronchospasm , dyspnea
Nursing intervention:-
Check BP every minute for 5 min, then every 5 min for 30 min
Less excessive hypotension tachycardia and rebound hypertension than hydralazine
Monitor for fetal bradycardia and neonatal respiratory depression

Nifedipinf (procardia)antihypertensive:-
Calcium channel blocker dilates arterioles and decreases systemic vascular resistance by
relaxing arterial smo0th muscle may potentiate CNS effects magnesium sulfate
Dosage /Route:10mg orally and repeat in 30min if need
Side effects:-headache, flushing
Nursing intervention:-
See hydralazine use caution if the woman is also receiving magnesium sulfate (29).
Note:- Antihypertensive medications not recommended
ACE inhibitors
First trimester use POSSIBLY associated with increased birth defects
Thiazide diuretics
Exacerbate IV fluid depletion in cases of superimposed preeclampsia (15).
Care of woman with preeclampsia receiving of magnesium sulfate:-
General guidelines:-frequency of vital signs and assessment as ordered and per situational
policy
Baseline assessment prior to starting infusion:-
Vital signs, oxygen saturation with pulse oximete , level of consciousness (LOC)
Deep tendon reflexes ,clonus, edema, proteinuria .
Signs of sever preeclampsia.
Assessment of fetal and uterine status
Insert a Foley catheter with urine meter for accurate measurement of output (because
magnesium sulfate is excreted by the kidneys ,toxicity can develop quickly with
impaired renal function
Discuss the rationale and side effects with the woman and her family initially she
may feel flushed, hot ,and sedated
Provide emotional support to help allay anxiety
Frequency of nursing assessments after infusion started
Every 15 minutes BP during loading dose (the nurse should stay at the bedside
during the bolus dose),every 30 minutes on maintenance dose
Every 30 minutes ; oxygen saturation
Every hour ; respiratory rate, pulse. LOC, DTRs ,intake and output (I&O)

Every 4hours temperature if membranes are intact ,every 2hours if rupture
Every 8 hours signs of worsening condition, degree of edema.
Continuous electronic fetal monitoring
Maintain fluid balance to reduce the risk of pulmonary edema.
Infuse Iv fluids only as ordered.
Total IV and oral fluids should not exceed 125ml/hr.
Evaluate laboratory studies and magnesium levels.
Monitor for signs of magnesium toxicity
Neonatal response to magnesium sulfate (magnesium crosses the placenta).The newborn
infant may have depressed respiratory and hyporeflexia .Pediatric term should attend the
birth in event of resuscitation (29)
Intrapartum care:-
Delivery is indicated in the preeclamtic patient for the following reasons:-
Deterioration of fetal well being or treatment in effective in improving the disease .
Uncontrolled blood pressure , thrombocytopenia or elevated liver enzymes with
epigastric pain and tenderness , HELLP syndrome , placental abruption , oliguria and
pulmonary edema( 29)
.Vaginal delivery is usually attempted and achieved after induction
with oxytocin .Continue assessment and implement precise care, hourly input and out put
is evaluated , monitor labor progress closely , continuous electronic fetal monitoring ,
support the patients and analgesia during labor is limited to small dose and is with held
during the 2 hours before delivery ( 26).
Management of labor
First stage:-
The midwife should remain with the mother throughout the course of labor .Blood
pressure tend to rise during labor and convulsions (intrapartum eclampsia ) my occur Its
essential to document blood pressure and urine out put
Fluid balance should be monitored carefully. The patient should be in the bed and sedative
(injection Pethidine ) should be given at intervals .Marked deviations should be noted and
medical assistance sought .The mother should be made as comfortable as possible by
providing general nursing care

Vital signs (Blood pressure and pulse are measured half hourly)
Measurement of the mean arterial pressure (MAP) is recommended because of the
hemodynamic change in eclampsia
Respiratory rate and level of consciousness must be assessed periodically
Examination of the optic fund can give an indication of cerebral edema. (Cerebral
irritability can be assessed by the degree of the hyperreflexia or the presence of the
clonus.
Fluid balance Intravenous fluids are administered using infusion pumps and the
recommended infusion rate is 85ml/h. Because of the reduced intravascular
compartment in preeclampsia, poorly controlled fluid balance can result in circulatory
overload, pulmonary edema, adult respiratory distress syndrome and ultimately death
A urinary catheter is inserted and urine output measured hourly .A quantity about
30ml /h reflects adequate perfusion .Urinalysis to detect the presence of protein,
ketones and glucose is done four hourly.
Pain relief Epidural analgesia my procure the best pain relief and reduce the blood
pressure .If cesarean section should be done epidural anesthesia is best.
Fetal condition: The fetal heart rate should be monitored continuously and deviation
from the normal must be reported and acted on.
Second stage
When the second stag commences, the obstetrician and pediatrician should be notified the
midwife will continue to care for the mother. Duration of the second stage is usually
shortened by the application of the forceps or ventouse .Depending on the blood pressure
reading ,the woman is sedated immediately following delivery of the baby with
intramuscular morphine to prevent postpartum eclampsia usually blood pressure drops
after delivery.
Third stage:-Ergometrine and synometrine should not be used as they can cause
peripheral vasoconstriction and increase blood pressure, In the presence of severe
hemorrhage, methergine intramuscularly or syntocinon in drip may be given .
Post partum care :-The maternal condition should be monitored at least every 4
hours for the next 48 hours the period during which convulsions usually occur .
Phenobarbitone Tab 6omg is repeated can produce effective sedation Hypotensive drugs

may be prescribed if the diastolic pressure is raised beyond 100mmHg the woman is kept
in the hospital until the blood pressure reaches a safe level and proteinuria disappears(14)
.
Critical care interventions of HELLP syndrome:-
Therapy for HELLP syndrome centers on improving the platelet count by transfusion of
fresh- frozen plasma or platelets and delivery as soon as feasible by vaginal or caesarean
birth (30).
2.11 Prevention:-
Preventative measures against preeclampsia have been heavily studied. Because the
pathogenesis of preeclampsia is not completely understood, prevention remains a complex
issue. Below are some of the currently accepted recommendations.
Diet:-
Protein or calorie supplementation have no effect on preeclampsia rates, and dietary
protein restriction does not appear to increase preeclampsia rates (35)
Further, there is no
(36) intake has an effect salt changingevidence that
such as vitamin C and E has no effect on antioxidants Supplementation with
preeclampsia nodoes supplementation with vitamin D Therefore, supplementation with
1gram per supplementation at least umCalci .37)(
vitamins C, E, and D is not recommended
day is recommended during pregnancy as it prevents preeclampsia where dietary calcium
status is associated with selenium Low.(38)
especially for those at high riskintake is low,
higher incidence of preeclampsia (39)
Aspirin:-
Taking aspirin is associated with a 1% to 5% reduction in preeclampsia and a 1% to 5%
reduction in premature births in women at high risk (40) (41)
.The WHO recommends low-
dose aspirin for the prevention of preeclampsia in women at high risk and recommend it be
United States Preventive Services Task The(34)
started before 20 weeks of pregnancy
h weekdose regimen for women at high risk beginning in the 12t-recommends a low Force
(42).
Physical activity
There is insufficient evidence to recommend either exercise ( 43)
or strict bed rest (44)
as
preventative measures of pre-eclampsia.
Smoking cessation
and a reduced risk of smoking risk pregnancies the association between cigarette-In low
preeclampsia has been consistent and reproducible across epidemiologic studies. High-risk
pregnancies (those with pregestational diabetes, chronic hypertension, history of
preeclampsia in a previous pregnancy, or multi fetal gestation) showed no significant
protective effect. The reason for this discrepancy is not definitively known; research
supports speculation that the underlying pathology increases the risk of preeclampsia to
such a degree that any measurable reduction of risk due to smoking is masked (45)
However, the damaging effects of smoking on overall health and pregnancy outcomes
outweighs the benefits in decreasing the incidence of preeclampsia (32) .
It is recommended
that smoking be stopped prior to, during and after pregnancy (46).
2.12 Complications:-
Complications of preeclampsia can affect both the mother and the fetus. Acutely
, HELLP syndrome , the development ofeclampsia preeclampsia can be complicated by
, acute kidney injury , liver damage and dysfunction,stroke hemorrhagic or ischemic
(27). (ARDS) stress syndromeacute respiratory di and
preterm ,Caesarian section Preeclampsia is also associated with increased frequency of
re can occur in . Furthermore, an elevation in blood pressuplacental abruption , anddelivery
some individuals in the first week postpartum attributable to volume expansion and fluid
mobilization.(12).
Fetal complications include fetal growth restriction and a potentially fetal
or prenatal death Long-term, an individual with preeclampsia is at increased risk for
recurrence of preeclampsia in subsequent pregnancies. There is also an increased risk for
cardiovascular complications, including hypertension and ischemic heart disease, and
kidney disease (47)
Eclampsiain a preeclamptic patient that may not convulsions is the development of new
be attributed to other cause. Eclampsia is a serious complication of preeclampsia and
results in high rates of perinatal and maternal morbidity and mortality (34)
Warning
symptoms for eclampsia in an individual with current preeclampsia may include
headaches, visual disturbances, and right upper quadrant or epigastric abdominal pain,
is used to ulfateMagnesium s . (32)
with headache being the most consistent symptom
prevent convulsions in cases of severe preeclampsia.
HELLP Syndrome:-

This condition may occur in 10-20% of patients with severe preeclampsia and eclampsia
is associated with increased maternal and fetal morbidity and mortality. In 50% of
instances, HELLP syndrome develops preterm, while 20% of cases develop in late
gestation and 30% during the post-partum
Previous studies:-
The study done in (2013) titled " Updating Nurses' knowledge about Preeclamptic
Patients' Care by Using a Poster in Minia Maternal and Child University Hospital, "
concluded that , years of experience is important factor of knowledge
Another study done `in (2012), titled " Evaluation of knowledge and management
practices of hypertension in pregnancy among health care workers in University of
Oslo Hospital , moshi urban, Tanzania, , University of Oslo Hospital " concluded that
definition of pre eclampsia , also this study comprises assessing fetal well being in
cases of preeclampsia and rest of preeclamptic mother (49)
The study done in (2010) titled "AN evaluation of the knowledge of the registered
midwives managing hypertensive disorders at primary health care level in eastern cape,
Stellenbosch University Hospital ,Eastern cape " concluded that definition of pre
eclampsia and diet of preeclampsia (50)
The study done in (2012) titled "management of preeclampsia/eclampsia in dares salaam
public health facilities concluded that the risk factors of preeclampsia (51)
The study done in (2013) titled " Operationalization of Nursing Assessment sheet for
administration of Magnesium Sulfate in Nehru Hospital ,India " concluded that care of
mgso4 before administration ( 52)
CHAPTER THREE
Methodology

3.1 Study Design:-
Design used for this study is descriptive cross_ sectional hospital based study
3.2 Study area:-
The study was conducted at Khartoum state hospitals in( Ribat university Hospital ,
Saad Abu alela Hospital and Sahroon Hospital )
3.3 Study Period:-
This study was carried out during the period from October to December 2014.
3.4 Study population:-
The population of the study included 50 BSC nurses
3.4 .1 Inclusion criteria:- `
All bachelors ( Bsc) nurse work in pre eclamptic word during period of study.
3.4 .2 Exclusion criteria:-
Nurse diploma and master Holder work in preeclamptic word
3.5 Sample size:-
Total coverage because the number of the population is limited.
3.6 Data collection tools:
An administered questionnaire It contain of 17 close-ended questions. which the questions
are read out by the researcher , to every one of the nurses to according her answers.
3.7 Data collection Technique:-
Individual interview.
3.8 Data analysis:-
The Data was entered and analyzed by computer using software program statistical
package for social sciences (SPSS) version 16 and the result presented in forms of tables
and figures.
3.9 Ethical considerations:-
The research conducted after approval taken from Ribat University faculty of nursing
sciences, from the Ministry of Health, hospitals authorities and from the nurses and
assured them that the data is used only for the purpose of the study.
CHAPTER FOUR

Results
Figure (4-1) percent distribution of study sample according to their age
17(34%) were in the age 21-25years,11(22%) werein the age 26-30, 15(30%) were
in the age 31-35, 7(14%) were in the age36 or more
17
11
15
7
0
2
4
6
8
10
12
14
16
18
21---25 26---30 31---35 36---40
no

Figure No (4-2) percent distribution of study sample according to their years of
experience
20(40%) have1- 5 years experience; 23 (46%) have 6 -10 years experience;
7 (14%) have 11 years experience and more.

Figure (3) distribution of study sample regarding receiving training course
about preeclampsia .
Shows that all study sample 50(100%) did not receivie training courses about
preeclampsia

Table NO (1): percent distribution knowledge of study sample about Definition
of pre- eclampsia
Definition of preeclampsia Frequency Percent
V. good 17 34%
Good 9 18%
Poor 24 48%
Total 50 100.0
Table (1) illustrates the knowledge of the study sample about definition of
preeclampsia it was found that 17(34) had V .good knowledge,9 (18%)had good ,
24(48%) poor knowledge
Table No (2) knowledge of study sample about causes of pre-eclampsia
Causes of preeclampsia Frequency Percent
V.good 19 38.0
Poor 31 62.0
Total 50 100.0
Table (2) illustrates the knowledge of the study sample about causes of preeclampsia
19( 38%) showed V good knowledge 31(62%)showed poor knowledge

Table No (3) knowledge of the study sample about risk factors for pre-eclampsia
Risk factors for pre-eclampsia Frequency Perce
nt
V. good 45 90%
Good 3 6%
Poor 2 4%
Total 50 100.0
Table (3) illustrates the knowledge of the study sample about risk factors for
preeclampsia was found that 45(90%) showed V.good knowelge3(6%) showed.good
knowelge 2(4%) poor knowledge.
Table (4) knowledge of study sample about serious (subjective) signs of
preclampsia
Serious signs of preclampsia Frequency Percent
V. good 29 58%
Good 1 2%
Poor 20 40%
Total 50 100.0
Table (4) illustrated the knowledge of the study sample about serious (subjective)
signs of severe preeclampsia it was found that 29(58%) V. good knowledge, 1(2%)
showed good knowledge ,3(6%) poor knowledge

Table (5) knowledge of study sample about assessmentof fetal wellbeing in
preeclamptic mother
Test of fetal well being in preeclamptic mother
Frequency Percent
V. good 6 12%
Good 19 38%
Poor 25 50%
Total 50 100.0
Table (5) illustrates the knowledge of the study sample about assessment of fetal well
being in preeclampsia 6(12%)showed V. good knowledge 19(3 8%)showed good
knowledge 25(50%) Poor knowledge
Table (6) knowledge of study sample about bed rest for preeclamptic mother
Bed rest for preeclamptic mother Frequency Percen
t
V good 17 34%
Good 10 20%
Poor 23 46%
Total 50 100.0
Table(6) illustrates the knowledge of the study sample about bed rest of
preeclampsia 17( 34%) showed V good knowledge 10( 20%) showed good knowledge ,
23 ( 46%)showed poor knowledge

Table (7) preeclamptic mother needs weight measuring every day
weight measuring Frequency Percent
V. good 21 42.0
Poor 29 58.0
Total 50 100.0
Table (7) illustrates the knowledge of the study sample about weight measuring of
preeclamptic mother 21(42%) showed V good knowledge 2 9(58%) showed poor
knowledge
Table (8) knowledge of the study sample about diet for preeclamptic mother
Diet for preeclamptic mother Frequency Percent
V. good 17 34%
Good 5 10%
Poor 28 56%
Total 50 100.0
Table (8) illustrates the knowledge of the study sample about diet of preeclampsia
17(34%) showed V.good knowledge5 (10%) showed good knowledge, 28(56%) showed
poor knowledge

Table (9) knowledge of the study sample about mild to severe signs indicate
progresses of preeclampsia
Progress from mild to severe preeclampsia Frequency Percent
V. good 4 8%
Good 10 20%
Poor 36 72%
Total 50 100.0
Table (9) illustrates the knowledge of the study sample about mild to severe signs indicate
progresses of preeclampsia 4(8%) showed V good knowledge 10(20%) showed good
knowledge, 36(7 2%) showed poor knowledge
Table (1o) knowledge of study sample regarding care before administration
Mgso4
Care before administration of Mgso4 Frequency Percent
V. good 45 90%
Good 0 0%
Poor 5 10%
Total 50 100.0
Table (10) illustrates the knowledge of the study sample before administration of Mgso4
45(90%) showed V. good knowledge 0(0%) showed good knowledge ,
5(10%) showed poor knowledge
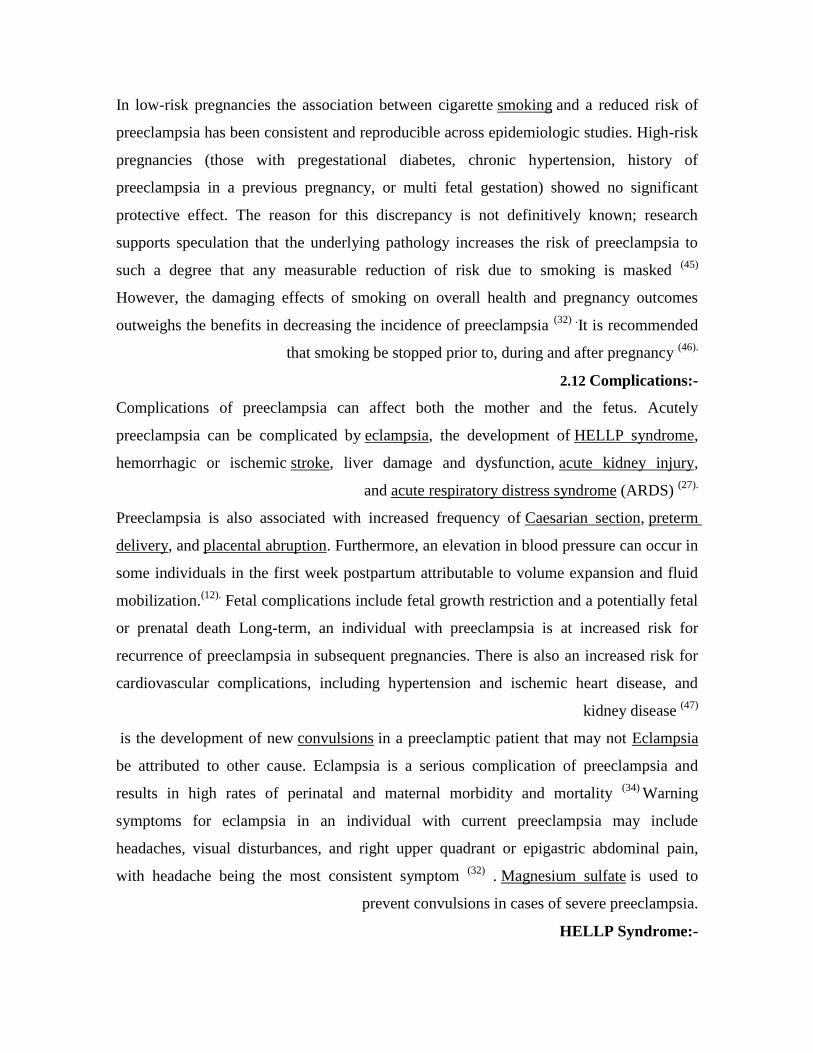
Table (11) knowledge of the study sample regarding the signs of Mgso4 toxicity
Signs of Mgso4 toxicity Frequency Percent
V. good 1 7 34%
Good 2 4%
Poor 31 62%
Total 50 100.0
Table (11) illustrates the knowledge of the study sample regarding the sings of Mgso4
toxicity 17 (34%) showed V good knowledge 2(4%) showed good knowledge ,31(
62%)showed poor knowledge
Table (12) percent distribution of the study sample knowledge about care of
sever preeclampsia
Care of severe preeclampsia
Frequency Percent
V. good 44 88%
Good 4 8%
Poor 2 4%
Total 50 100.0
Table (12) illustrates the knowledge of the study sample about care ofsevere
preeclampsia 44(88%) showed V good knowledge 4(8%) showed good knowledge 2(4%)
showed poor knowledge

Table (13) knowledge of the study sample about indications for delivery of
preeclamptic mother
Indication for delivery of preeclamptic mother Frequency Percent
V. good 7 14%
Good 14 2 8%
Poor 29 58%
Total 50 100.0
Table (13) illustrates the knowledge of the study sample about indication for delivery
of preeclamptic mother 7(14%) showed V. good knowledge 1 4(2 8%) showed good
knowledge 29(58%) showed poor knowledge
Table (14) knowledge of the study sample about intrapartum care of
preeclamptic mother
Intrapartum care of preeclampsia Frequency Percent
V .good 12 24%
Good 10 10%
Poor 28 56%
Total 50 100.0

Table (14) illustrates the knowledge of the study sample about intrapartum care of
preeclamptic mother 12( 24%) showed V good knowledge 10( 20%) showed good
knowledge , 28( 56%)showed poor knowledge
Table (15) knowledge of the study sample about signs of HELLP syndrome
Signs of HELLP syndrome
Frequency Percent
V. good 6 12 %
Good 1 2 24%
Poor 32 64%
Total 50 100.0
Table (15) illustrates the knowledge of the study sample about HELLP syndrome
signs 6 (12%) showed V. good knowledge 12(24%) showed good knowledge ,
32( 64%)showed poor knowledge
Table (16) knowledge of the study sample about the effect of preeclampsia on
mother
Effect of preeclampsia on mother Frequency Percen

t
V. good 10 20%
Good 12 24%
Poor 28 56%
Total 50 100.0
Table (16) illustrates the knowledge of the study sample about effect of preeclampsia
on maternal 10(20%) showed V. good knowledge ,12( 24%) showed good knowledge,
28(56%)showed poor knowledge
Table (17) knowledge of the study sample about effect of preeclampsia on the
fetus
Effect of preeclampsia on the fetus Frequency Percent
V. good 34 6
8%
Good 3 6%
Poor 13 26%
Total 50 100.0
Table (17) illustrates the knowledge of the study sample about effect of preeclampsia
on fetus 34 ( 68%) showed V good knowledge 3(6%) showed good knowledge ,
13(26%) showed poor knowledge

Table (18):- Crosstabs between knowledge of the study sample about
preeclampsia and years of experience
Years of experience total percent P value
1-5
years
6-10
years
11
years
Definition of preeclampsia V. good +good 3 12 11 26 52%
poor 15 9 0 24 48%
Total 50 100% .003
Causes of preeclampsia V. good +good 5 8 6 19 38%
poor 15 15 1 31 62%
Total 50 100% .0013
Risk factors V. good +good 8 18 22 48 96%
poor 2 0 0 2 4%
Total 50 100% .000
Subjective signs V. good +good 3 12 15 30 60%

poor 7 11 2 20 40%
Total 50 100% .003
Monitors fetal well being V. good +good 6 11 8 25 50%
poor 13 12 0 25 50%
Total 50 100% .003
Bed rest V. good +good 6 15 6 27 54%
poor 14 8 1 23 46%
Total 50 100% .004
Diet of preeclampsia V. good +good 5 10 7 22 44%
poor 15 13 0 28 56%
Total 50 100% .002
Weight measuring V. good +good 6 11 4 21 42%
poor 14 12 3 29 58%
Total 50 100% .015
Progress from mild to severe V .good +good 1 8 5 14 28%
poor 19 15 2 36 72%
Total 50 100% .001
Administration of MgSO4 V. good +good 4 16 20 40 90%
poor 5 5 0 10 20%
Total 50 100% .000
Signs of mgso4 toxicity V. good +good 5 8 6 19 38%
poor 15 15 1 31 62%
Total 50 100% 013.
Care of sever preeclampsia V. good +good 17 15 16 48 96%
poor 2 0 0 2 4%
Total 50 100% .002
Indication for delivery of
preeclamptic patient
V. good +good 5 10 16 21 42%
poor 15 13 1 29 58%
Total 50 100% .008
Intrapartum care V. good +good 3 12 7 22 44%

Table (18) shows the Correlation of knowledge and years of experience related to
nurses care of preeclampsia
P value was considered significant when P < 0.05
Mean of knowledge = 47.o5
CHAPTER FIVE
5.1 Discussions:
This descriptive cross-sectional hospital based study was conducted to assess knowledge
of BSC nurses regarding nursing care of preeclamptic patients in Ribat University
Hospital, Saad Abu Alela Hospitals and Sahroon Hospital at Khartoum state from
October to December 2014
Regarding receive of training course about preeclampsia the researcher showed that all
nurses 100% did not receive training courses .
Regarding years of experiences, it was found that 60% of the study sample had more than
5 years in the obstetrics and gynecology department showed that figure (3). This study
poor 17 11 0 28 56%
Total 50 100% .000
HELLP syndrome signs V. good +good 4 8 6 18 36%
poor 16 15 1 32 64% .
Total 50 100% .005
Effect on maternal V. good +good 3 12 7 22 44%
poor 17 11 0 28 56%
Total 50 100% .000
Effect on the fetus V .good +good 6 14 17 37 7 4%
poor 12 1 0 13 26%
Total 50 100% .001

found that experience is important source of knowledge This finding in line with Chiari
who find that nurses knowledge mostly depend on their experience (48).
This study showed that 24(48%) did not known the definition of pre eclampsia This
finding was consistent with study conducted in Tanzania which is showed that (44.1%) did
not known definition of preeclampsia (49)
At the same time it was inconsistent with study
in Eastern cape which is showed that (27.7%) of the participants had incorrect answer (50)
45 (90%) of study sample had very good knowledge about risk factors of preeclampsia and
3(6%) had good knowledge was showed that in table (3)
This finding was consistent with study conducted in Tanzania which showed that (86%)
knew the risk factors of preeclampsia (51).
Study revealed that half of study sample 25 (50%) had poor knowledge about assessing
fetal well being in cases of preeclampsia if we make comparison between this study and
anther one in Eastern cape( which showed that the majority of the participants (75.2%)
had correct answered about assessing fetal status( 49)
we find inconsistent with this study .
Although rest of preeclamptic patients is improve utroplacental blood flow and reduce BP
but result of this study showed that 23(46%) of the study sample did not know why to
encourage rest of preeclamptic patient table (6) The result in this study is inconsistent with
study in Eastern cape (which is showed that (84.1%), of the participants had correct
answer (49)
that means their big deficit knowledge regarding this variable .
In regard to measuring the weight of the preeclamptic patient 27(54%) of study sample
know about weight measuring of preeclamptic patient and 23(46%) of them did not known
table (8)
This study showed that 17(34%) of study sample knew about diet of preeclampsia
28(52%) showed poor knowledge (9) the result in this study inconsistent with study in
Eastern cape which is showed that (80.7%) of the participants had correct answer (50)

Only 4(8%) of the study sample knew about the signs of progresses from mild to severe
preeclampsia that means there is acute deficiency in knowledge in this variable
Knowledge about care of mgso4 before administration it will help to prevent
complications and leads to early detection of side effects, this study revealed that 45
(90%) of the study sample known about care of mgso4 before administration table (17)
this result accordance with Study conduct in India which showed that (96.3%) had
correct answer (52) .
This study showed that(88%) of study sample knew about care of severe preeclampsia
was show that in table(12) the researcher expect to see 100% correct answer
(56%) of study sample did not known the intrapartum care of preeclamptic mother and
24%kew the intrapartum care
HELLP Syndrome occur in 10-20% of patients with severe preeclampsia and increased
maternal and fetal morbidity and mortality The current study found that more than half
32(64%) of study sample did not know the signs of HELLP syndrome that means there is a
big deficit knowledge regarding in variable table(15).
Although the effect of preeclampsia in mother increase maternal mortality, unfortunately
most of the nurses 28(56%) not known about effect of preeclampsia on maternal table (16)
this bad result need to be taken account
Although the complication of preeclampsia increases prenatal death, more than half
(52%) did not known the effect of preeclampsia on the fetal table (17)
Preeclampsia still one of the major contributors to maternal and infant morbidity and
mortality unfortunately The results obtained in this study showed that inadequate
knowledge among the study sample Mean of knowledge = 47.o5
.

5.2 CONCLUSION:
Most of the study sample know about the following:
The risk factors of preeclampsia.
Subjective signs of preeclampsia
Care of Mgso4 before administration
Nursing care of severe preeclampsia .
Effected of preeclampsia on fetal .
Al most of the study sample did not know the following

Definition of preeclampsia
Causes of preeclampsia
Weight measuring of preeclampsia
Diet and rest of preeclampsia
Progresses from mild to severe of preeclampsia
Signs of mgso4 toxicity intrapartum care of preeclampsia
Effect of preeclampsia on mother
5.3RECOMMENDATIONS:
On the bases of the study results and conclusion, the researcher would like to
recommend the following:
Frequent refreshing courses regarding preeclampsia.

Encourage them to update them self.
Conduct further studies related to this research.
REFERENCES

1. Duley, L. The Global Impact of Pre-Eclampsia and Eclampsia. Seminars in Perinatology, 33, 30-
http://dx.doi.org/10.1053/j.semperi.2009.02.010(2009) 137.
2. Mikat, B., Gellhaus, A., Wagner, N., Birdir, C., Kimmig, R. and Köninger, A. Early Detection of Maternal Risk for Preeclampsia. ISRN Obstetrics and Gynecology, 2012, Article ID: 172808, 7
pages
3. World Health Organization Fact Sheet, May 2012
4. Cousens S, Blencowe H, Stanton C, Chou D, Ahmed S, Steinhardt L, Creanga AA, Tunçalp O, Balsara ZP, Gupta S, Say L, Lawn JE. National, regional, and worldwide estimates of stillbirth rates
in with trends since 1995: a systematic analysis. Lancet, 2011, Apr 16; 377(9774):1319-30. 5. Preeclampsia foundation, http://www.preeclampsia.org/ 2011.
)providers-http://www.preeclampsia.org/care(
6.Villar J, Say L, Gulmezoglu AM, Meraldi M, Lindheimer MD, Betran AP, Piaggio G; . In Pre-eclampsia, Critchly H, MacLean A, Poston L, Walker J, eds. London, RCOG Press, 2003, pp 189-207. 7. Ronsmans C, Graham WJ on behalf of the Lancet Maternal Survival Series steering group, “Maternal mortality; who, when, where and why.” The Lancet, Maternal Survival, September
2006.
8. Preeclampsia: A Decade of Perspective, Building a Global Call to Action. Preeclampsia Foundation, Melbourne, Florida, Nov 2010
9. Ali ,A .A. ,Okud, A., Khojali ,and Adam,I .High incidence of obstetric complications in Kassala hospital, eastern Sudan. (2012). J. Obstet. Gynaecol. 32, 148–149.
10. Maternal mortality in 2005: estimates developed by WHO, UNICEF, UNIFPA and the World Bank, Geneva, World Health Organization, 2007.
11.The women's: the royal women 'hospital ,magnesium sulphate protocol ,clinical
practice guidelines [online]. 2009 [cited on 2012 November 24]; Available from: http// www.thewomens.org.au/magnesium sulphate protocol CPG
12. Kuklina EV, et al. Hypertensive Disorders and Severe Obstetric Morbidity in the United States.
Obstet Gynecol 2009; 113:1299-306.
13.King Edward Memorial Hospital for Women- WA. Magnesium sulphate Infusion. Pharmacy and Medication Guidelines. 2008.
14. Jacob A. A Comprehensive text book of Midwifery &gynachological nursing ,3rd edition, new
delhi, Jaypee Brothers ,201 2:p.106-121 15. American Congress of Obstetricians and Gynecologists (ACOG) District II Hypertensive Crisis
Guidelines 2012 16. Steegers, Eric AP; von Dadelszen, Peter; Duvekot, Johannes J; Pijnenborg, Robert (August
2010). "Pre-eclampsia". The Lancet 376(9741): 631–644.
17. Courtney Reynolds, MD, William C. Mabie, MD, & Baha M. Sibai, MD. "Pre-eclampsia". Pregnancy - Hypertensive Disorders. Armenian Medical Network. Retrieved 2006-11-23.

18. Jun Wu, Cizao Ren, Ralph J. Delfino, Judith Chung, Michelle Wilhelm, & Beate Ritz . "Association Between Local Traffic-Generated Air Pollution and Pre-eclampsia and Preterm Delivery in the South Coast Air Basin of California". Environmental Health Perspectives. Retrieved
2009-07-05.
19. "Excess Weight Raises Pregnancy Risks". Medline Plus. 2010. Retrieved 2010-02-15.
20."The View from the Cuckhold". EPjournal. 2007. Retrieved 2011-07-20.
21.Van DenBoogaard, E.; Vissenberg, R.; Land, J. A.; Van Wely, M.; Van Der Post, J. A. M.; Goddijn, M.; Bisschop, P. H. "Significance of (sub)clinical thyroid dysfunction and thyroid autoimmunity before conception and in early pregnancy: A systematic review". Human Reproduction Update.
(2011). 17 (5): 60.
2 2.Laresgoiti-Servitje E, Gómez-López N, Olson DM (April 2010). "An immunological insight into the origins of pre-eclampsia". Hum Reprod Update 16 (5): 510–24.
http://humupd.oxfordjournals.org/cgi/content/abstract/16/5/510?etoc.
23. Maynard SE, Min JY, Merchan J, et al. (March 2003). "Excess placental soluble fms-like tyrosine kinase 1 (sFlt1) may contribute to endothelial dysfunction, hypertension, and proteinuria
in pre-eclampsia". The Journal of Clinical Investigation 111 (5): 649–58. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=151901
24. Venkatesha S, Toporsian M, Lam C, et al. (June 2006). "Soluble endoglin contributes to the
pathogenesis of pre-eclampsia". Nature Medicine 12 (6): 642–9.
25. Xiong Y, Liebermann DA, Tront JS, et al. "Gadd45a stress signaling regulates sFlt-1 expression in pre-eclampsia". Journal of Cellular Physiology(September 2009). 220 (3): 632–9.
26. Gilbert E S High risk pregnancy & delivery , Fourth edition ,U S A ,Mosby, 2007 :459_ 485.
27. Arulkumaran, N.; Lightstone, "Severe pre-eclampsia and hypertensive crises". Best Practice & Research Clinical Obstetrics & Gynaecology (December 2013). 27 (6): 877–
884. doi:10.1016/j.bpobgyn.2013.07.003
28. Pregnancy, developed by the Task Force on Hypertension ,Hypertension in pregnancy. in ISBN(2013). 978-1-934984-28-4
29. Susan Mattson, Core curriculum for maternal newborn nursing ,4th
edition,California,2011:P.433-443
30.Ward L S ,Hisley M S Maternal _ Child nursing care : First edition, United states of America , F. A. Davis company , 2009:357_365
31. Fraser D M, Cooper ,A and Notle A W Myles Textbook For Midwives African Edition
:2end edition ,U S A, Elsevier homepage,2010:373_387

32. Steegers, Eric AP; von Dadelszen, Peter; Duvekot, Johannes J; Pijnenborg, Robert "Pre-eclampsia". The Lancet (2010). 376(9741): 631–644. doi:10.1016/S0140-6736(10)60279-6
33. Obstetrics, Charles R.B. Beckmann ... [et al.] ; American College of; (ACOG), Gynecology Obstetrics and gynecology. (6th ed. ed.). Baltimore, MD: Lippincott Williams &
Wilkins. ISBN(2010). 0781788072
34. WHO recommendations for prevention and treatment of pre-eclampsia and eclampsia. 2011. ISBN 978-92-4-154833-5.
35. Kramer MS, Kakuma R Kramer, Michael S, ed. "Energy and protein intake in pregnancy". Cochrane Database of Systematic Reviews (4): R (2003). CD000032
36.Duley L, Henderson-Smart D, Meher S "Altered dietary salt for preventing pre-eclampsia, and its complications.". The Cochrane database of systematic reviews (4) (Oct 19, 2005). ":
CD005548.
37.Rumbold AR, Crowther CA, Haslam RR, Dekker GA, Robinson JS "Vitamins C and E and the risks of pre-eclampsia and perinatal complications". The New England Journal of Medicine(April
2006). 354 (17): 1796–806. 38. Hofmeyr, GJ; Lawrie, TA; Atallah, AN; Duley, L; Torloni, MR "Calcium supplementation during pregnancy for preventing hypertensive disorders and related problems.". The Cochrane database
of systematic reviews 6: (Jun 24, 2014). CD001059.
39. Rayman MP, Bode P, Redman CW "Low selenium status is associated with the occurrence of the pregnancy disease pre-eclampsia in women from the United Kingdom". American Journal of
Obstetrics and Gynecology (November 2003). 189 (5): 1343–9.
40. Henderson, JT; Whitlock, EP; O'Connor, E; Senger, CA; Thompson, JH; Rowland, MG . "Low-dose aspirin for prevention of morbidity and mortality from preeclampsia: a systematic evidence review for the U.S. Preventive Services Task Force.". Annals of internal medicine MG (May 20,
2014). 160 (10): 695–703. :
41. Duley L, Henderson-Smart DJ, Meher S, King JF "Antiplatelet agents for preventing pre-eclampsia and its complications". Cochrane Database Syst Rev (2) (2007).: CD004659. :
42. "Low-Dose Aspirin Use for the Prevention of Morbidity and Mortality From Preeclampsia". United States Preventive Services Task Force. Sep 2014. Retrieved 17 Sep 2014.
43. Meher S, Duley L Meher, Shireen, ed. "Exercise or other physical activity for preventing pre-eclampsia and its complications". Cochrane Database of Systematic Reviews (2) L (2006).:
CD005942. 44. Meher S, Duley L (2006). Meher, Shireen, ed. "Rest during pregnancy for preventing pre-eclampsia and its complications in women with normal blood pressure". Cochrane Database of
Systematic Reviews (2): CD005939.

45. Jeyabalan A, Powers RW, Durica AR, Harger GF, Roberts JM, Ness RB "Cigarette Smoke Exposure and Angiogenic Factors in Pregnancy and Preeclampsia". Am. J. Hypertens. August
2008).21 (8): 943–7. . 46. Whitworth, M; Dowswell, "Routine pre-pregnancy health promotion for improving
pregnancy outcomes.". The Cochrane database of systematic (Oct 7, 2009).
47. Mustafa, Reem; Ahmed, Sana; Gupta, Anu; Venuto, Rocco C. "A Comprehensive Review of Hypertension in Pregnancy". Journal of Pregnancy 2012: 1–1.
48. Ola M. I. Mousa, Hala Abd El-Fttah Ali, Ahmad Reda El Adawy. [ Updating Nurses' knowledge about Preeclamptic Patients' Care by Using a Poster in Minia Maternal and Child University
Hospital.J AmSci 2013;9(4):658-663]. (ISSN: 1545-1003). http://www.jofamericanscience.org.73
49. Elisabeth Berg Lohre & Sara ,Evaluation of knowledge and management practices of hypertension in pregnancy among health care workers in moshi urban, Tanzania,2012
50. Nompume Lelo lorraine Ngwekazi , AN evaluation of the knowledge of the registered midwives managing hypertensive disorders at primary health care level in the eastern cape
Copyright@ 2010 Stellenbosch University
51. Luzango E. Maembe (MD) ,management of preeclampsia/eclampsia in dares salaam public health facilities: availability of supplies and knowledge of healthcare workers November 2012
52. Baljit Kaur ,Operationalization of Nursing Assessment sheet for administration of Magnesium
Sulphate ,Nursing and Midwifery Research Journal, Vol-9, No.3, July 2013
The National Ribat University
Faculty of Nursing Science
Master of Science in Obstetrics and Gynecological Nursing

Questionnaire
Assessment of nurses knowledge regarding nursing care of pre-eclampsiSocio - demographic
data
1. Experiences
a.1-5 years
b .6-11 years
c .>11 years
2 .Training courses in care of preeclamptic patients
a.Training
b.No trainin
3. Definition of preeclampsia
a.hypertention develops after 20 weeks gestation characterize highBP by proteinureia
b.BP extend of 140/90mmHg or more with proteninuria induced by pregnancy after 20week
c. Is disorderof pregnancy characterized by high BP and large amounts protein in the urine
A B C
Very good Good Poor
3 2 1
-
4.Cause of preeclampsia unknown
Yes
NO
5. Risk factors for developing pre eclampsia:-
a.Nulliparity (never given birth)
b. Chronic hypertention
c. Age extremes above 35 years
A B C
Very good Good Poor
3 2 1
7. Serious (subjective) sign of sever Preeclampsia is:-

a.Nausea and vomiting.
b.double vision
C pitting edema
A B C
Very good Good Poor
3 2 1
8.The nurse monitors the fetal well being of preeclamptic mother by:-
a. fetal heart rate with Doppler or electronic fetal monitors
b. Measure fundal height in centimeters from symphysis pubis to top of the fundus
c. kick chart
A B C
Very good Good Poor
3 2 1
9. Why encourage bed rest of pre-eclamptic mother
a. To improve utero-placental blood flow
b. To encourage growth of the fetus
c .To reduce BP
A B C
Very good Good Poor
3 2 1
10.preeclampsia mother needs weight gain measuring every day
Yes
NO
11. The nurse should plan a diet for preeclamptic mother-
a.Low fat
b.sodium restriction
c. Rich protein
A B C
Very good Good Poor
3 2 1

12. When the patient progresses from mild Preeclampsia tosevere
a. BP160/110mmHg
b.Pulmonary edema or cyanosis
c.impaired liver function
13.Before administration of MgSO4 nurse has
a. explained purpose of administration to patient
b. filled the correct dose
c. monitored vital signs
A B C
Very good Good Poor
3 2 1
14.A nurse determines the a sign ofmagnesium sulfate toxicity a. respiration less than 14b\m
b .deep tendon reflex are absent
c .urinary out put less than 30 ml\ h )
A B C
Very good Good Poor
3 2 1
15. Nursing care of severe pre eclampsia:-
a .monitor fetal heart sound every4h
b.record urine out put every 4h
c.moniter of blood pressure every 4h
A B C
Very good Good Poor
3 2 1
1 6.Indication for delivery of preeclampticmother:-
a. signs of fetal distress
A B C
Very good Good Poor
3 2 1

b. un control BP
C. Abruption placenta
A B C
Very good Good Poor
3 2 1
17.Intrapartum nursing care ofpreeclamptic mother a.measured blood pressure half hourly( )
b. measured pulse half hourly
c.assessthe degree of the hyperreflexia
A B C
Very good Good Poor
3 2 1
18. HELLPsyndromesigns :-
A .nausea and vomiting
b. Right upper quadrant tenderness
c. bruising
A B C
Very good Good Poor
3 2 1
19.Effect of pre eclampsia on maternal :-
a. Insufficiency utroplacental
b.Renal failure
c. Abruption placenta
A B C
Very good Good Poor
3 2 1
20.Effect of pre eclampsia on fetues :-
a. IUGR (intra uterine growth restriction)
b. Perinatal death
c. Preterm delivery
A B C

Very good Good Poor
3 2 1