The Most Common Foot and Ankle Conditions Every Primary ...
57
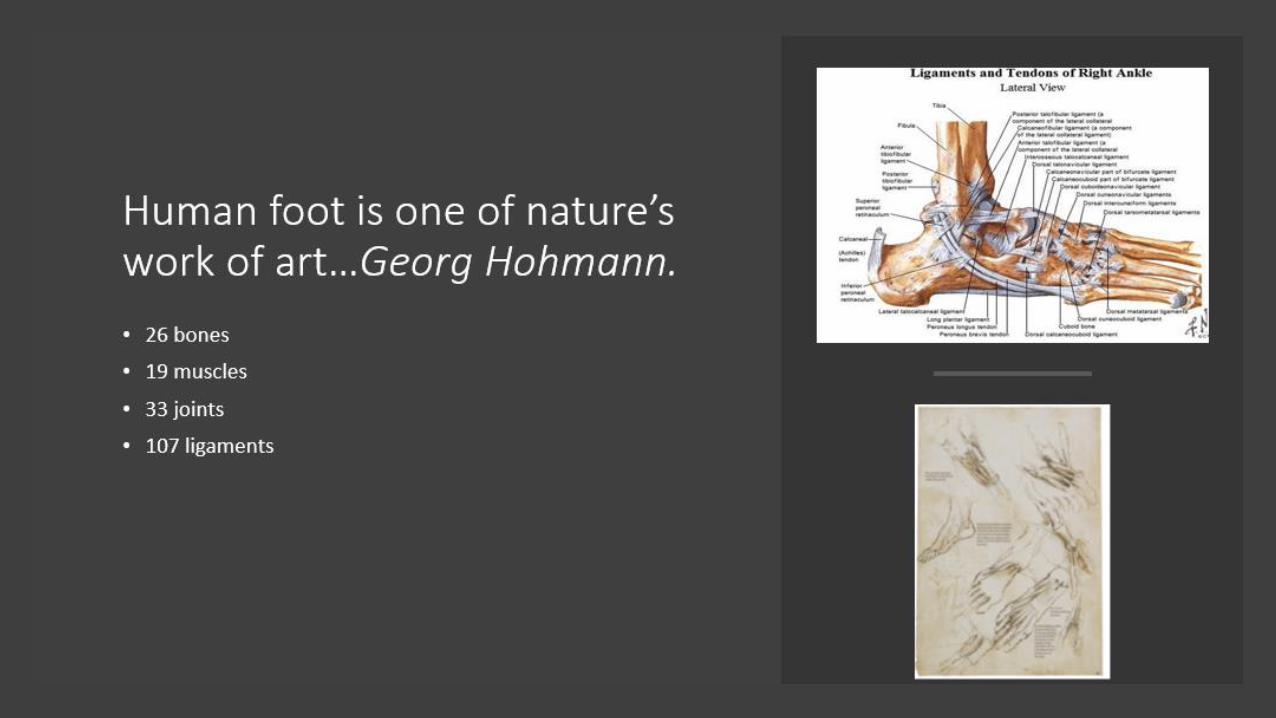
The Most Common Foot and Ankle Conditions Every Primary Care Physician May Encounter Alan Y. Yan, MD FAAOS Assistant Professor in Orthopedic Surgery University of Pittsburgh Medical Center
Transcript of The Most Common Foot and Ankle Conditions Every Primary ...

The Most Common Foot and Ankle Conditions Every Primary Care Physician May Encounter
Alan Y. Yan, MD FAAOS
Assistant Professor in Orthopedic Surgery
University of Pittsburgh Medical Center

Disclosure:
No Conflicts with the Current Topics.
How Popular are they? • Population study: 18-63% report pain,
aching or stiffness in feet.
• More with bunions, corns, calluses, nail issues
Garrow AP , Silman AJ , MacfarlaneGJ . The Cheshire Foot Pain and Disability Survey: a population survey assessing prevalence and associations, Pain , 2004
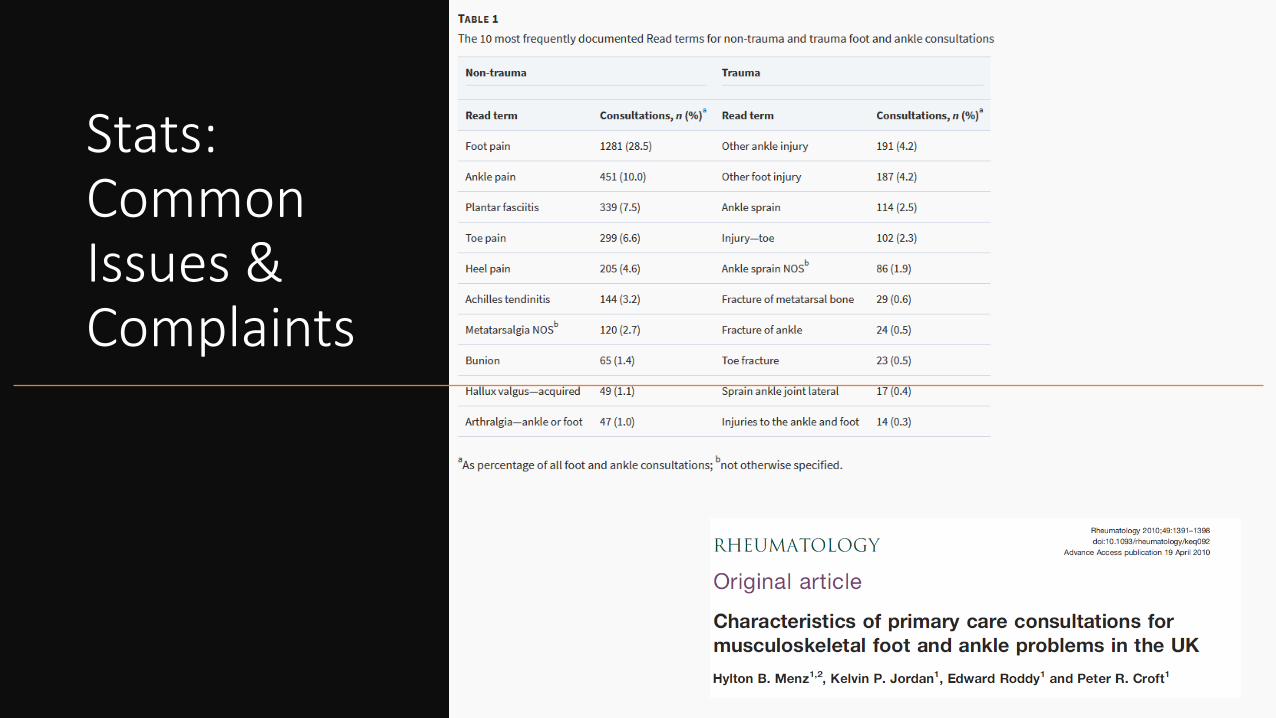
Stats: CommonIssues & Complaints
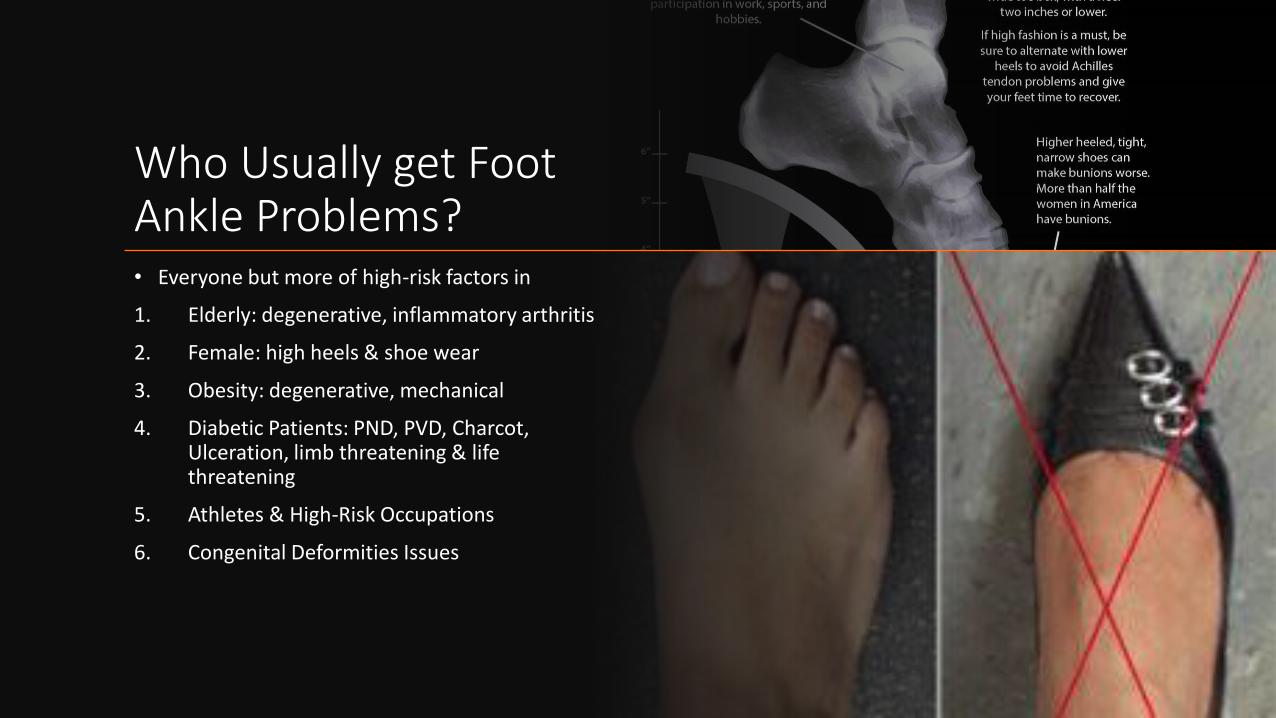
Who Usually get Foot Ankle Problems?• Everyone but more of high-risk factors in
1. Elderly: degenerative, inflammatory arthritis
2. Female: high heels & shoe wear
3. Obesity: degenerative, mechanical
4. Diabetic Patients: PND, PVD, Charcot, Ulceration, limb threatening & life threatening
5. Athletes & High-Risk Occupations
6. Congenital Deformities Issues

Who involved in the Care?
• Primary Care Physicians
• Orthopedic Surgeons
• Sports Meds
• Rheumatologist
• Podiatrists
• Wound Nurse
• Physical Therapist
• Orthotists
• Social Workers
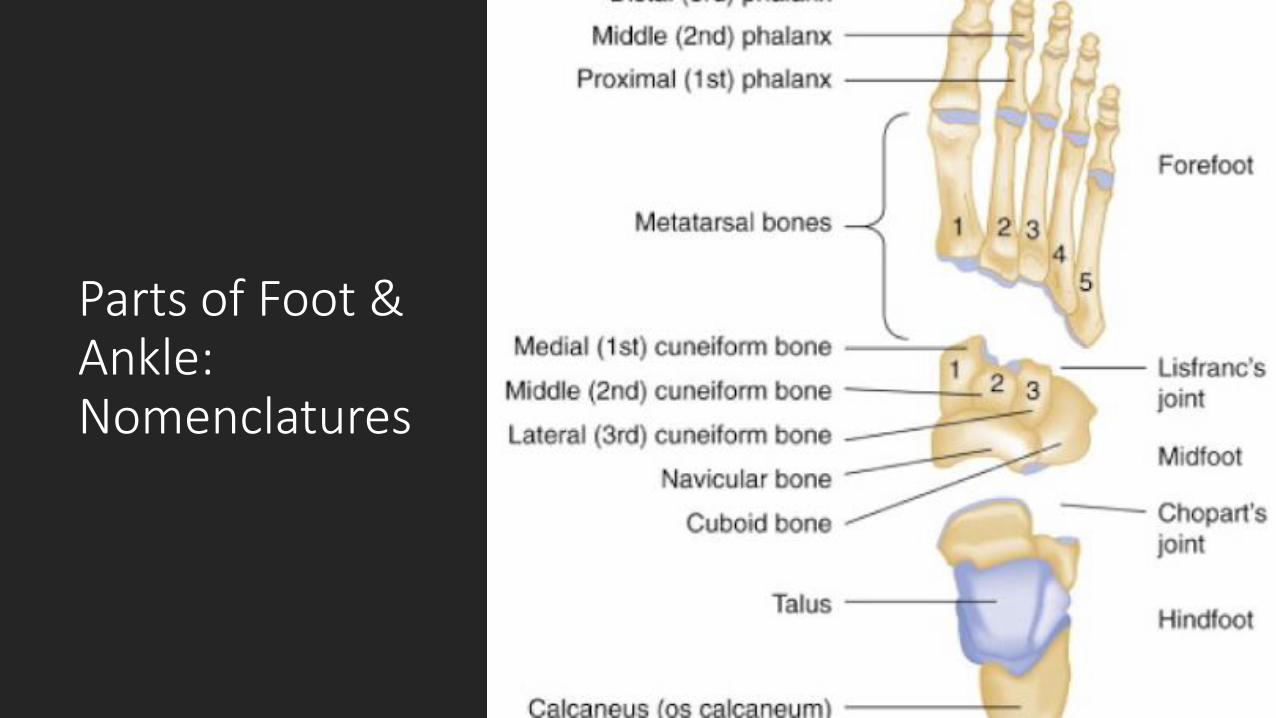
Parts of Foot & Ankle: Nomenclatures

•
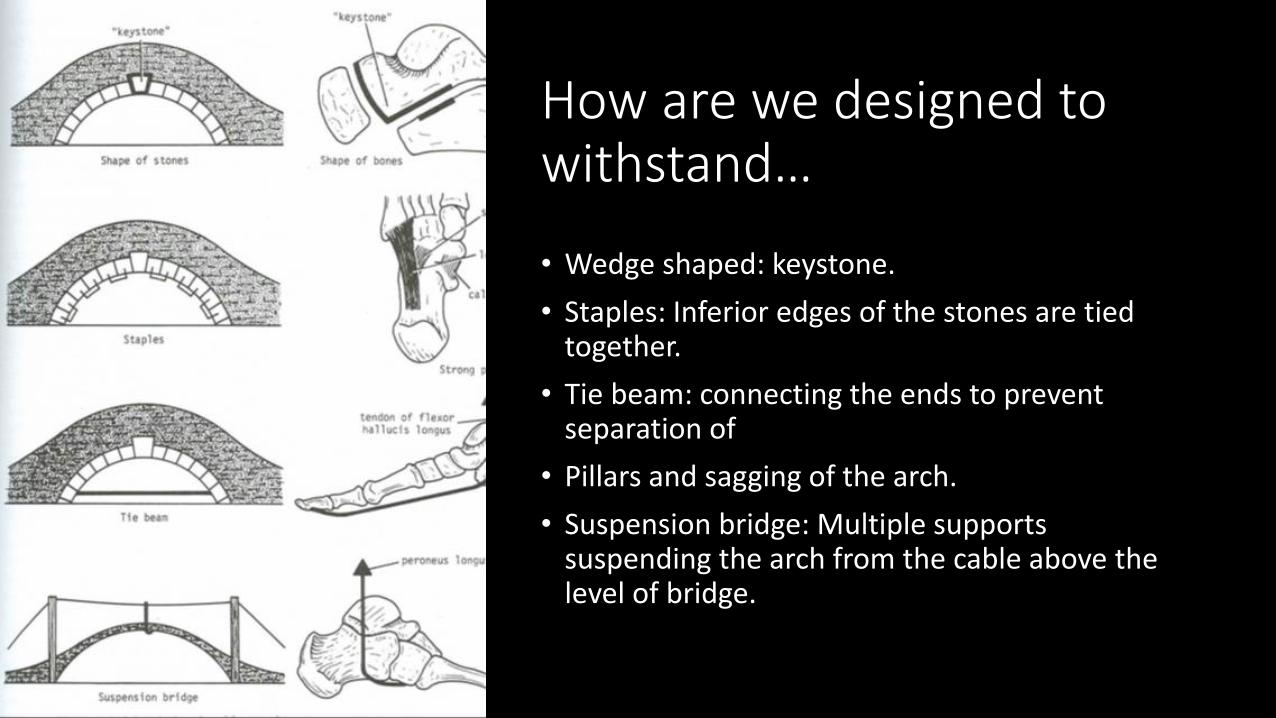
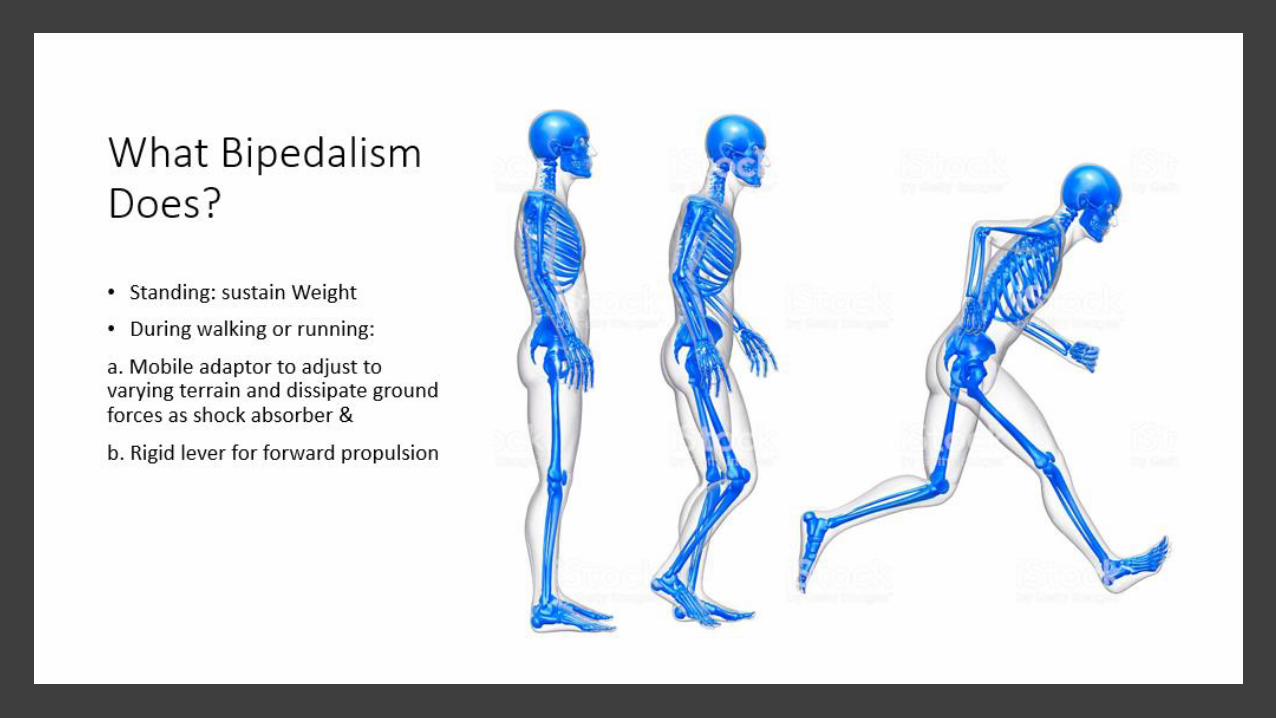
How are we designed to withstand…
• Wedge shaped: keystone.
• Staples: Inferior edges of the stones are tied together.
• Tie beam: connecting the ends to prevent separation of
• Pillars and sagging of the arch.
• Suspension bridge: Multiple supports suspending the arch from the cable above the level of bridge.

Painless Plantigrade Foot & Ankle:

Ankle Sprain: More Complicated than It Sounds
• Most Common Foot Ankle Injures You will Guarantee to See in your Clinic & commonly misdiagnosed: 23,000 each day in the U.S.
• Roll in vs Roll out
• Mechanism: from walking down the street to high level sports injury
• Symptoms: from some pain and swelling, to grapefruit sized swelling and not able to walk
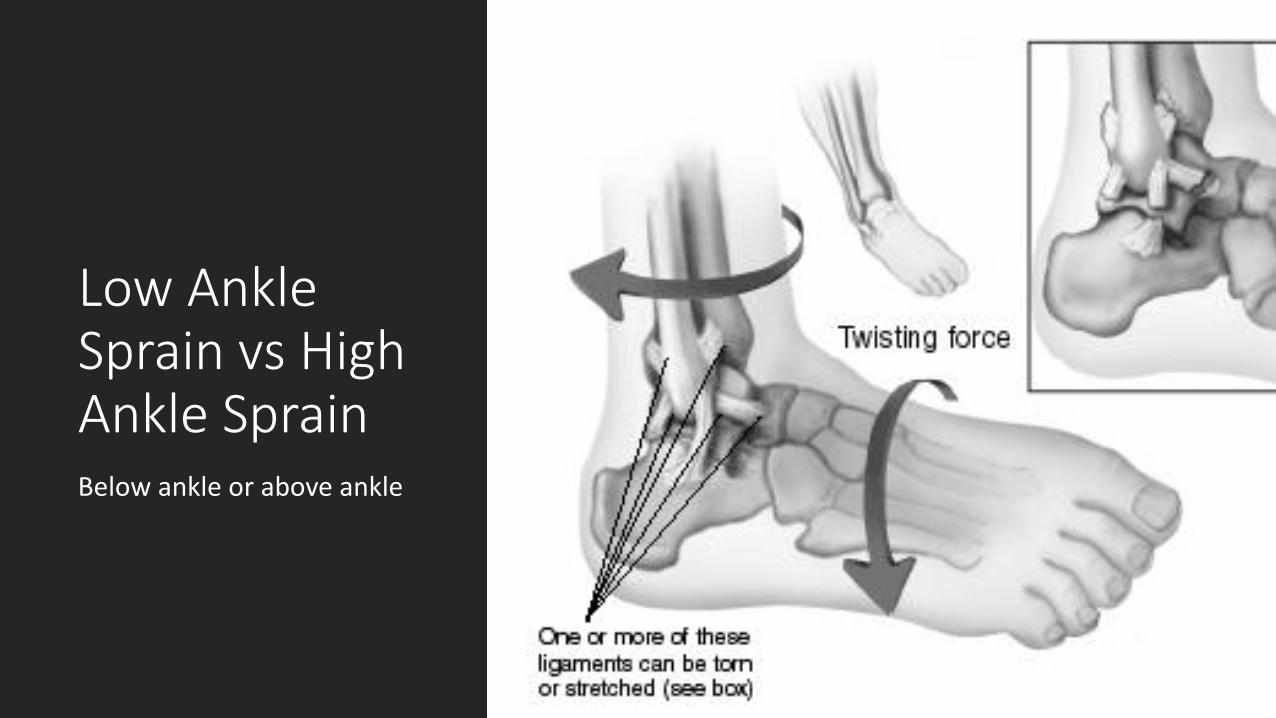
Low Ankle Sprain vs High Ankle SprainBelow ankle or above ankle
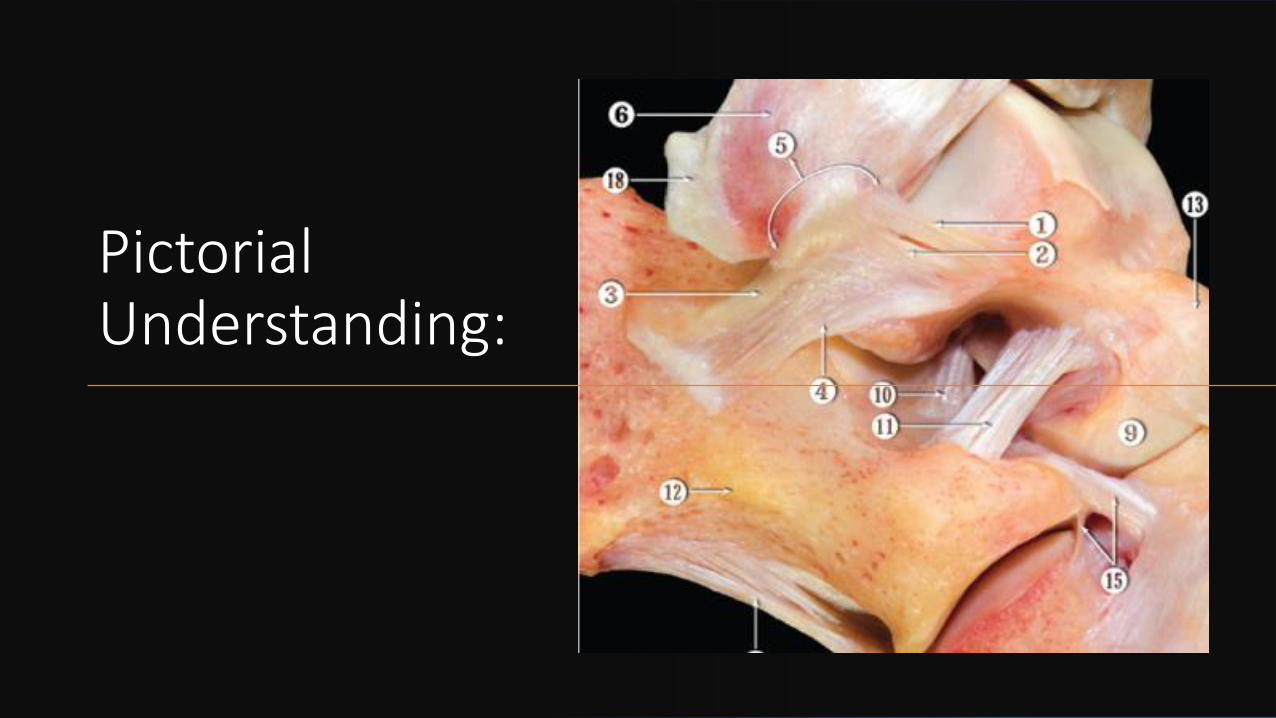
Pictorial Understanding:
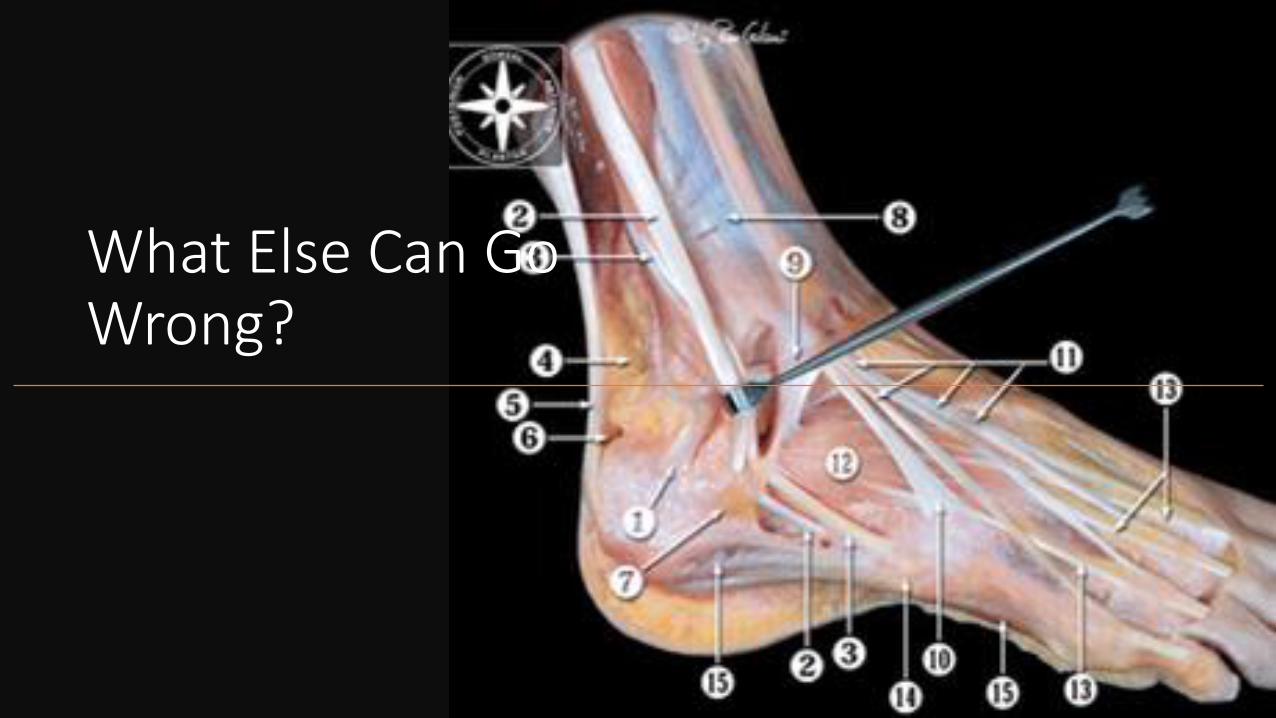
What Else Can Go Wrong?

And More?

And ?Cartilage Injuries: OLT or OCD lesions
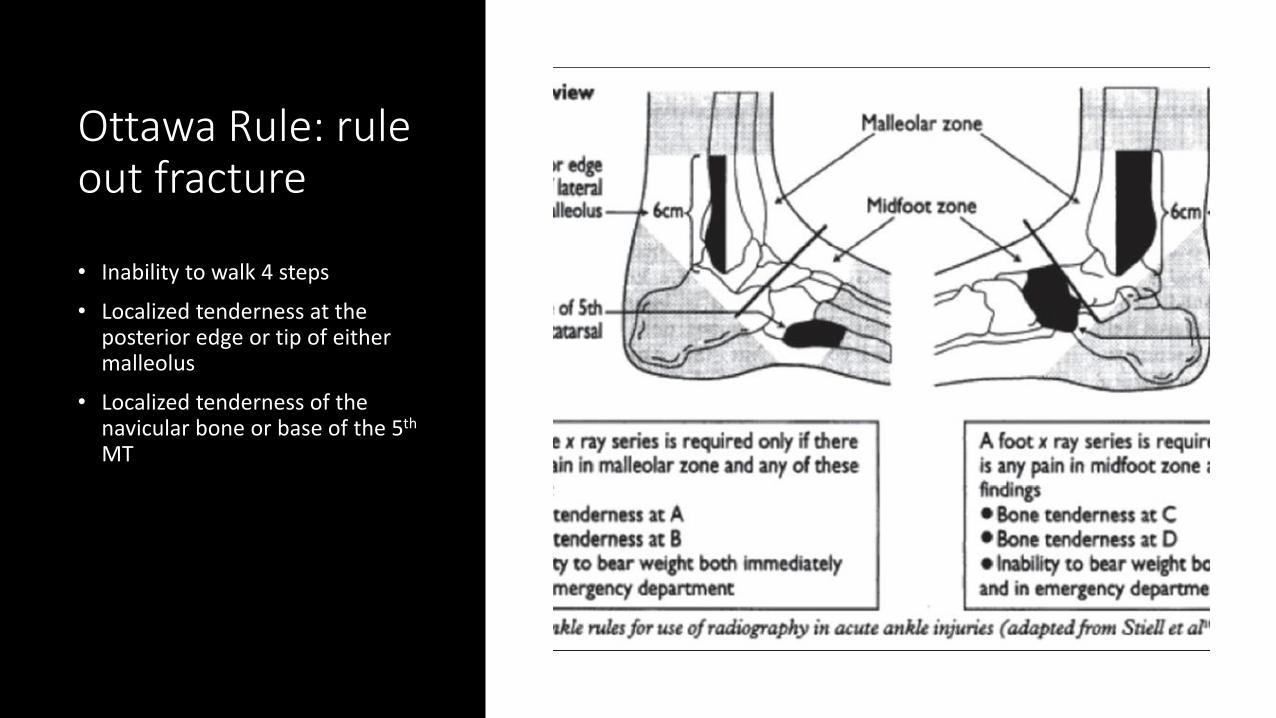
Ottawa Rule: rule out fracture
• Inability to walk 4 steps
• Localized tenderness at the posterior edge or tip of either malleolus
• Localized tenderness of the navicular bone or base of the 5th
MT
R.I.C.E.
• Acute Ankle Sprain: mostly NO need for surgery
• Rest, Ice, Compression, Elevation
• Brace or Boot with Crutches
• MRI needed if not better in 6 to 8 weeks
• Recurrent with chronic instability
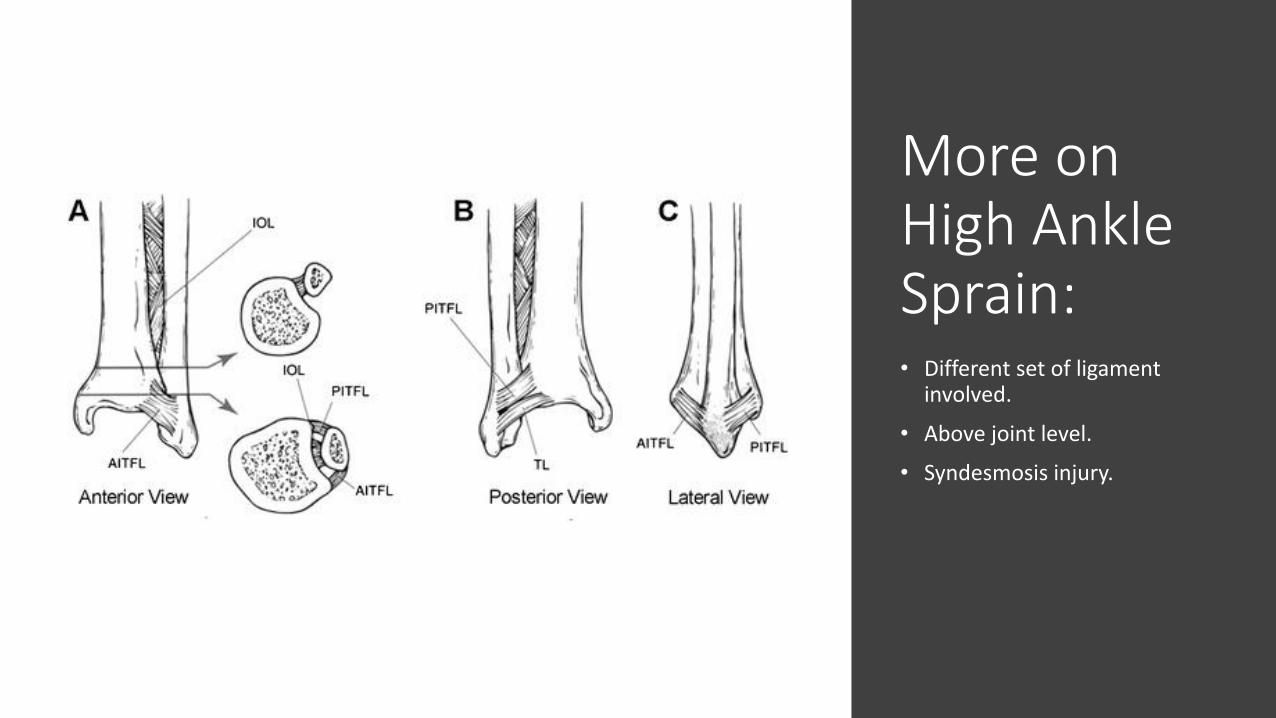
More on High Ankle Sprain: • Different set of ligament
involved.
• Above joint level.
• Syndesmosis injury.
Pitfalls: may NOT look as bad
• May have less swelling and bruising
• Does not LOOK THAT BAD: however took twice as long to heal
• Syndesmosis squeeze test
• May need surgery
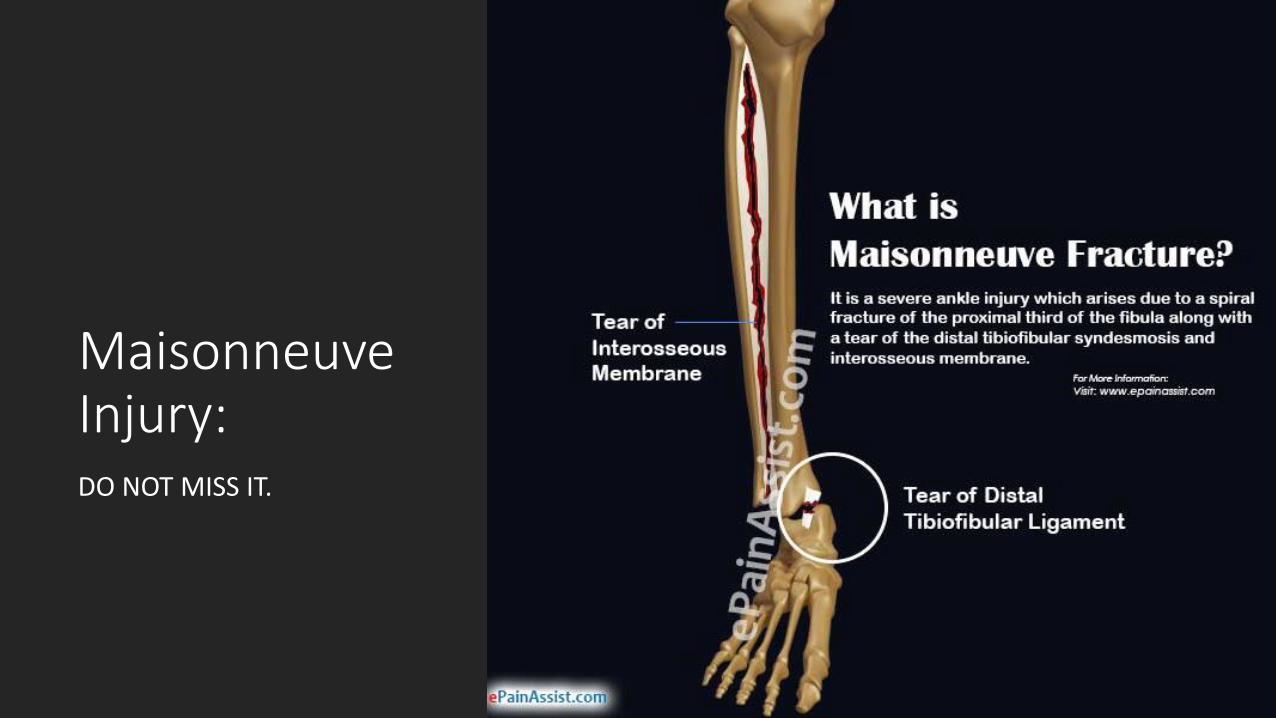
Maisonneuve Injury: DO NOT MISS IT.

Acute Ankle Injury or Achilles rupture?
MUST consider and exam if an acute ankle injury

Weekend Warrior’s Typical Story: Patient believe they just sprain the ankle.
Midfoot Sprain or Lisfranc injury:
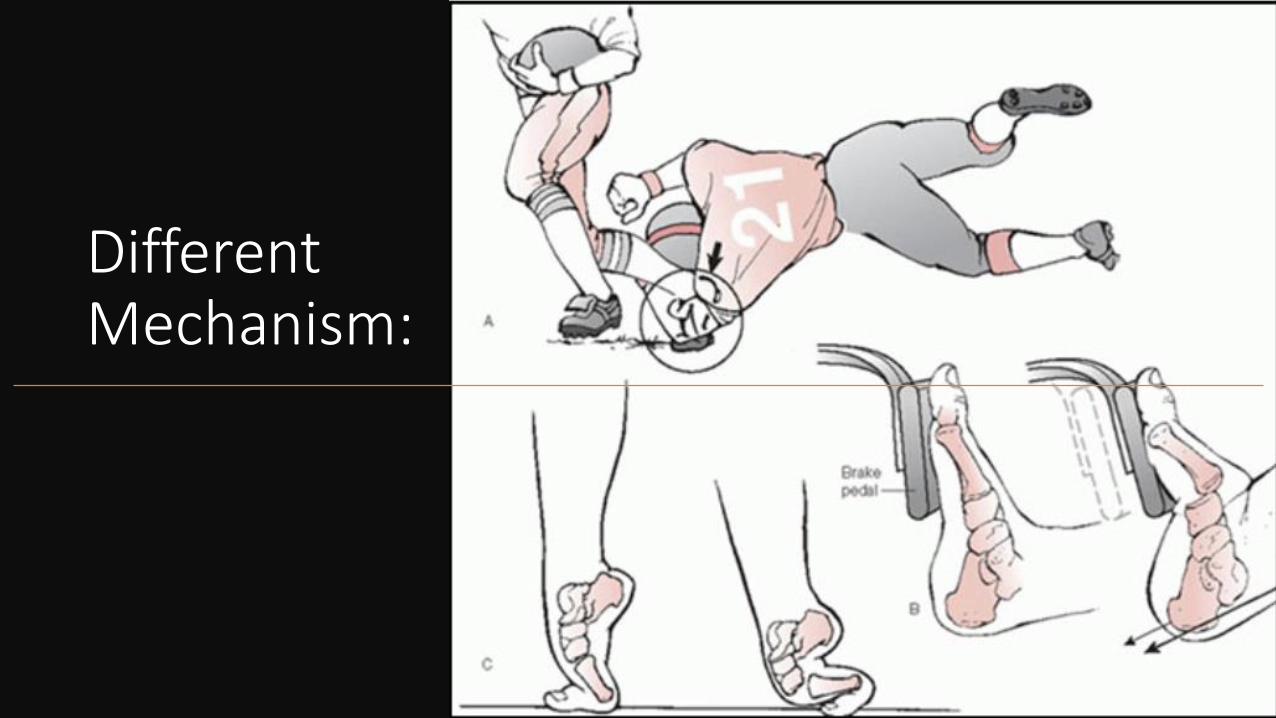
Different Mechanism:

Recognize this!!!

Heel Pain: Plantar Fasciitis
• Most common cause of heel pain without injury history
• 1 million visits to medical doctors per year
• 60% goes to primary care
• More of degenerative changes in fascia than an inflammatory process
• More accurate term should be: plantar fasciosis

Clinical Dx:
• Multifactorial: age, obesity, limited ankle dorsiflexion, prolonged WB, inappropriate shoe wear, rapid increase activity level.
• Overload at insertion at calc, micro tear, perifasicial edema, increased heel pad thickness.
• Medial heel pain with the first few steps in the morning or after a period of inactivity.

Good News & Bad News:
• Usually self limited and resolve in 80% in one year regardless of therapy
• Injection???
• Surgery???
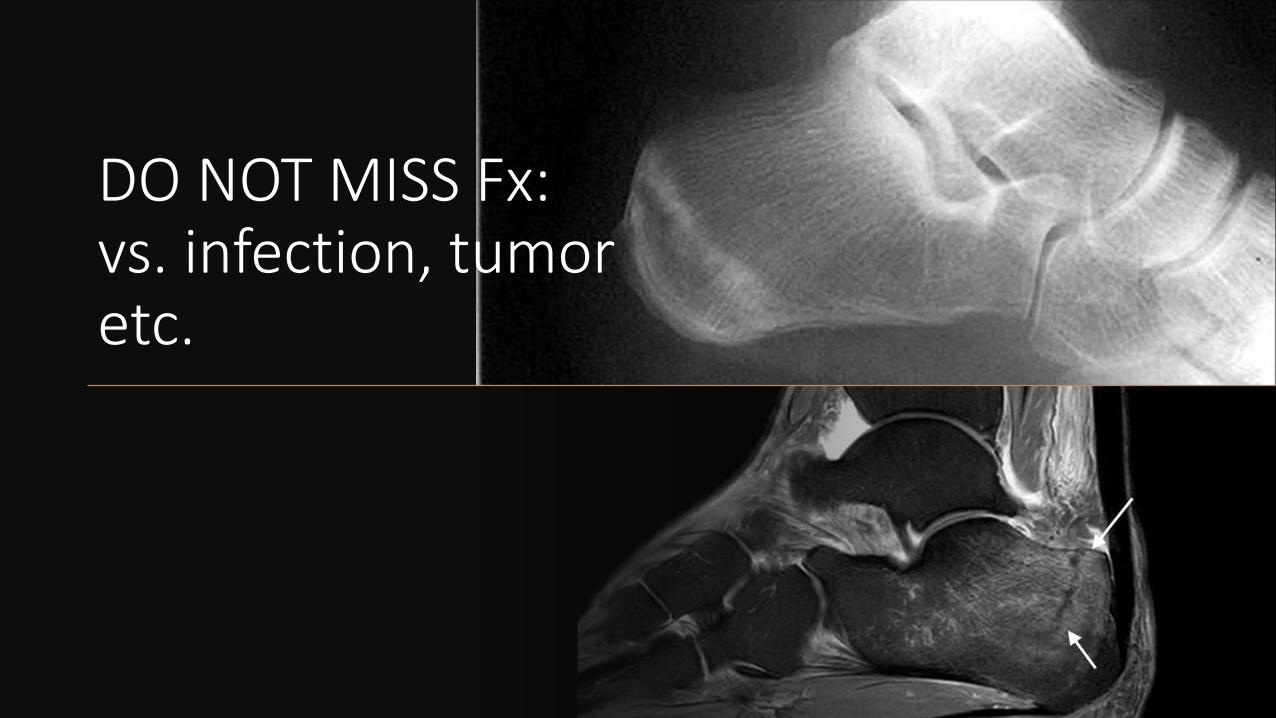
DO NOT MISS Fx:vs. infection, tumor etc.

Bunion: not just an ugly foot
• Hallux Valgus Deformity: pronation, valgus deviation
• Bursitis medially: pain in tight fitting shoes
• Imbalance of all supporting structures
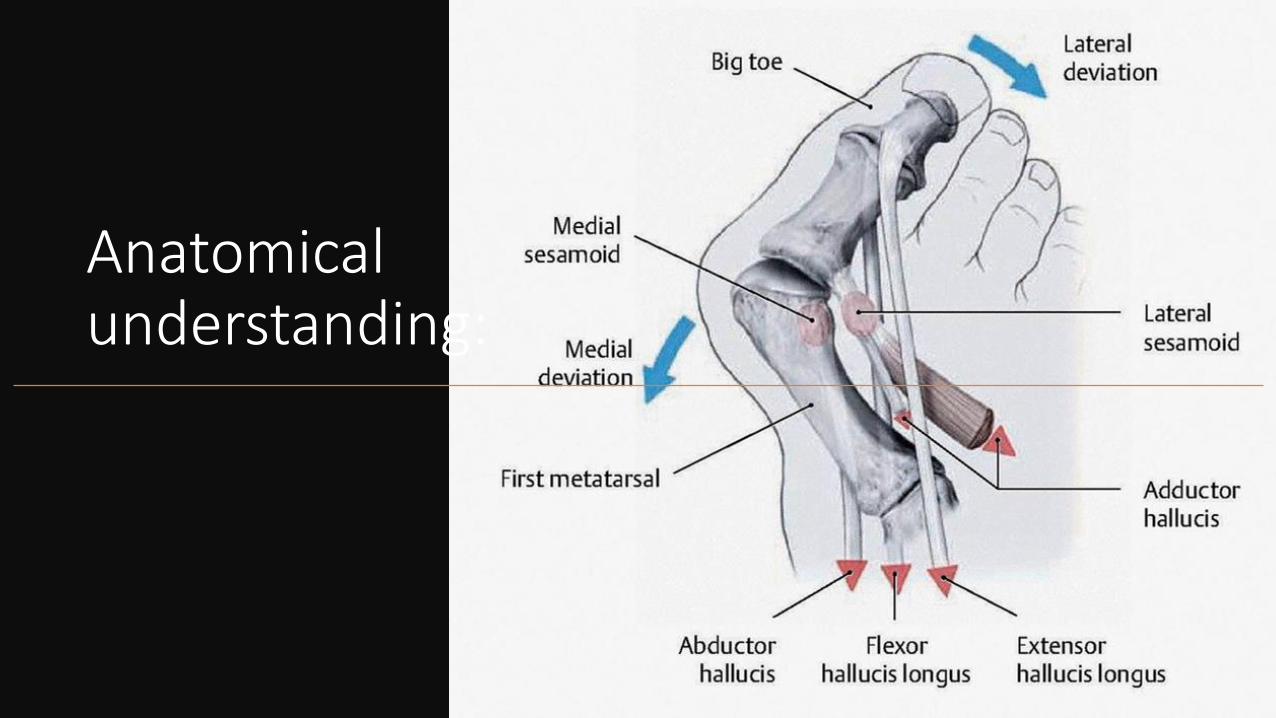
Anatomical understanding:

It is a surgical issue: fancy braces DOES NOT WORK

Bunionette: Taylor’s bunion

Other pain in the joints: Hallux Rigidus, inflammation or infection

Arthrocentesis:

Metatarsalgia & Morton's Neuroma: walking on Pebbles• Entrapment of one of the common digital N.
• Women to men: 8 to 1
• High heel narrow toe box
• Rule out stress fx
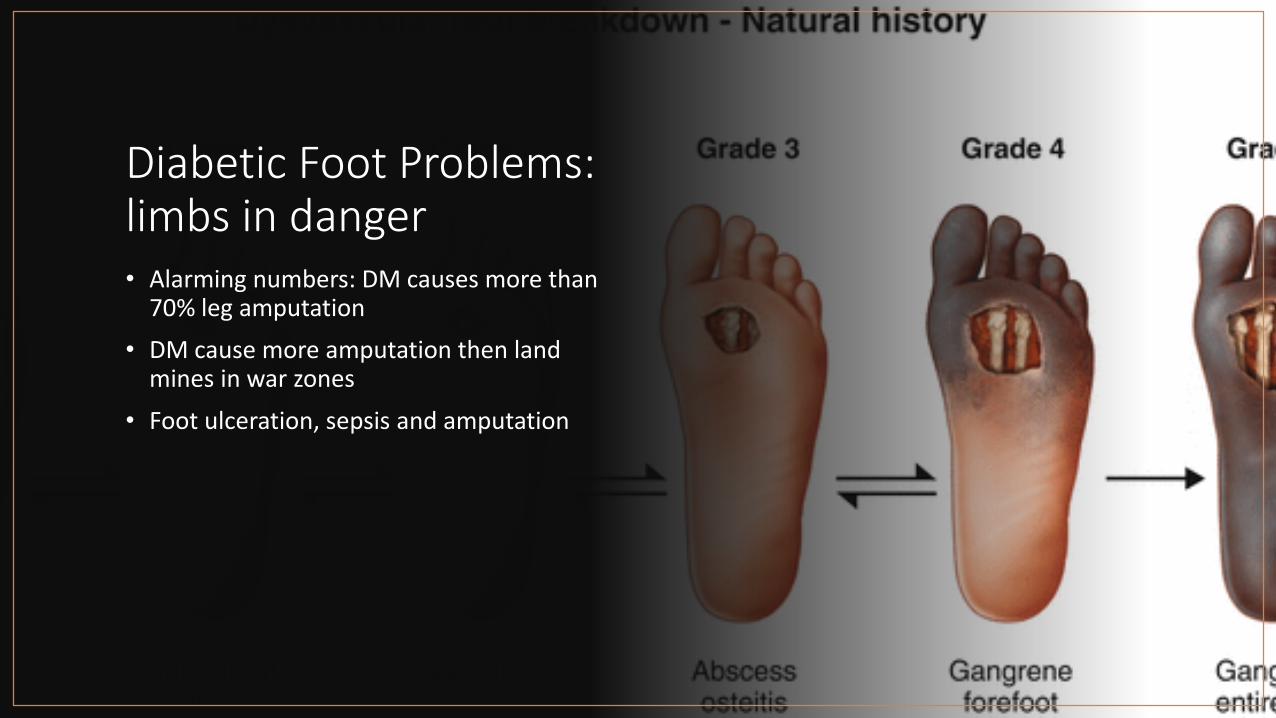
Diabetic Foot Problems: limbs in danger• Alarming numbers: DM causes more than
70% leg amputation
• DM cause more amputation then land mines in war zones
• Foot ulceration, sepsis and amputation

Scope of Problem:
• Long stretching hospitalization
• Mounting high expenses
• End result of amputation
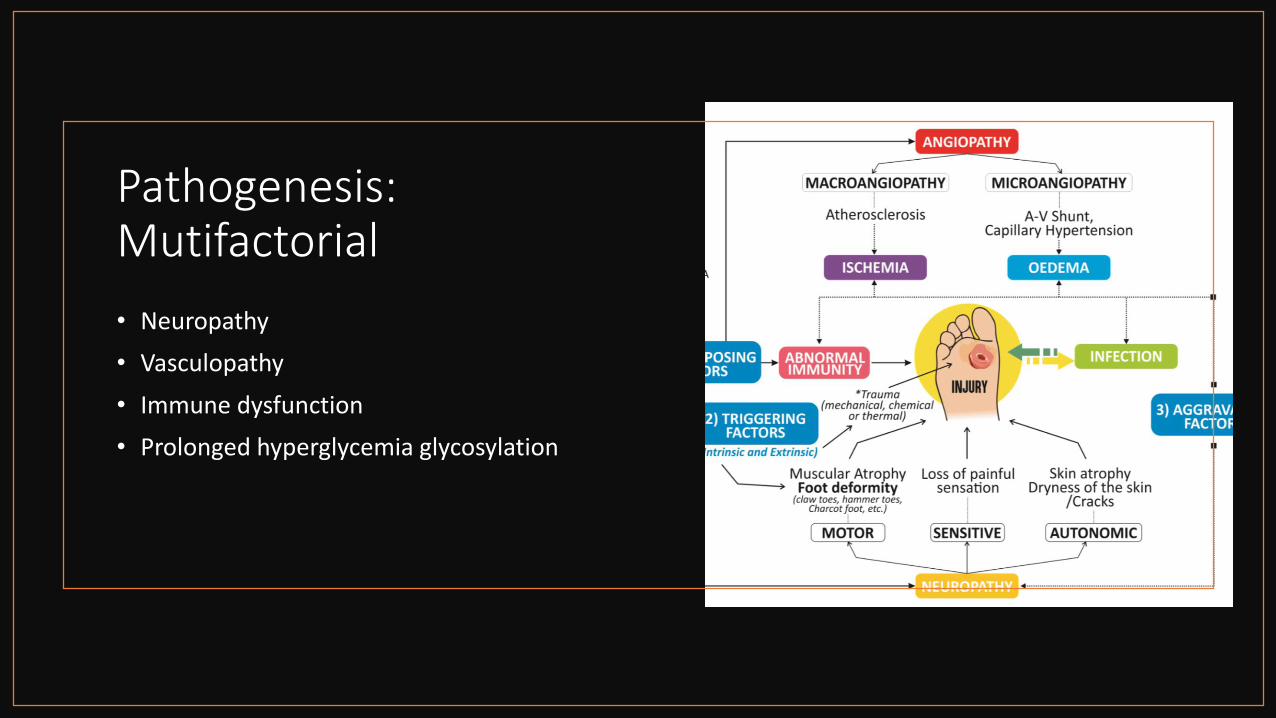
Pathogenesis: Mutifactorial
• Neuropathy
• Vasculopathy
• Immune dysfunction
• Prolonged hyperglycemia glycosylation

Sensory Neuropathy• Loss of pain
• Unnoticed trauma
• Lesion unchecked
• Callus formation
• Tissue necrosis
• Ulcerformation
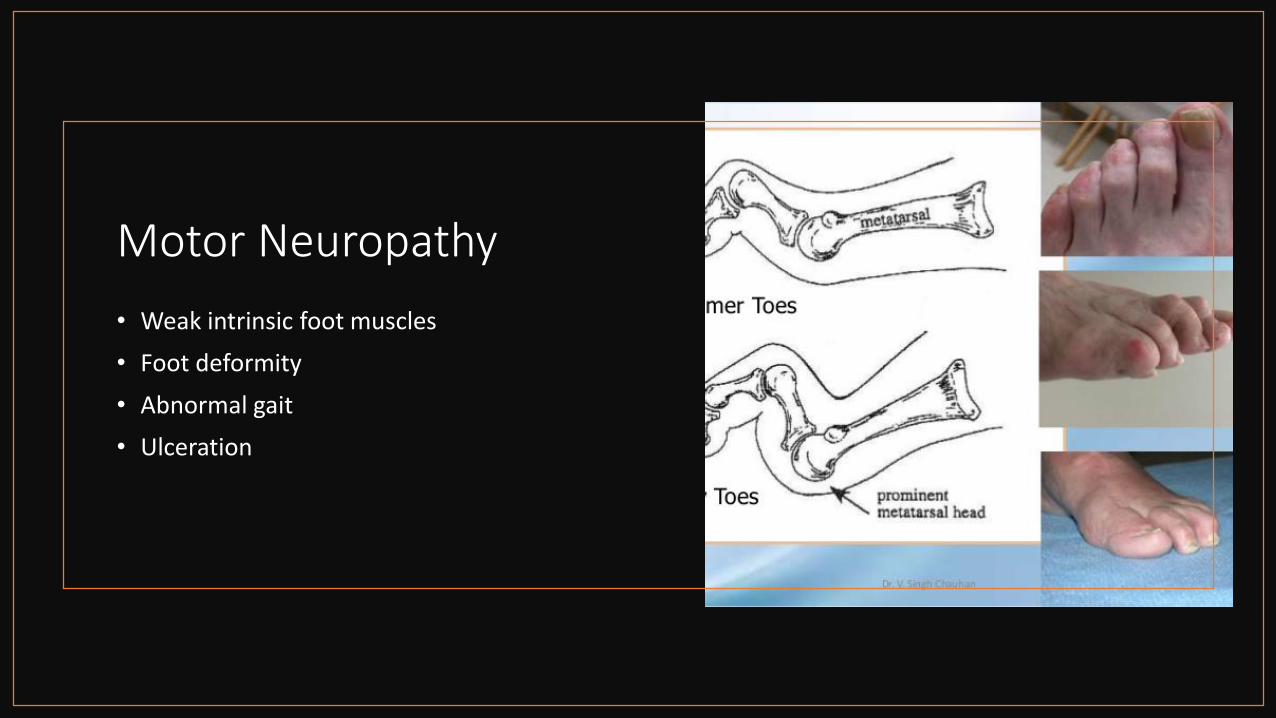
Motor Neuropathy
• Weak intrinsic foot muscles
• Foot deformity
• Abnormal gait
• Ulceration

Automomic neuropathy:
• Decrease sweating
• Dry brittle skin
• Fissures cracks
• Infection
• Ulceration

Vasculopathy:
• Macroangiopathy: artherosclerosis of large arteries
• Microangiopathy: capillary damage

Charcot Foot:
• Differentiate from infected foot: challenge for the PCP and ER.
• Always remain a high suspicion in any diabetic patient with PND with red, hot, swollen foot.
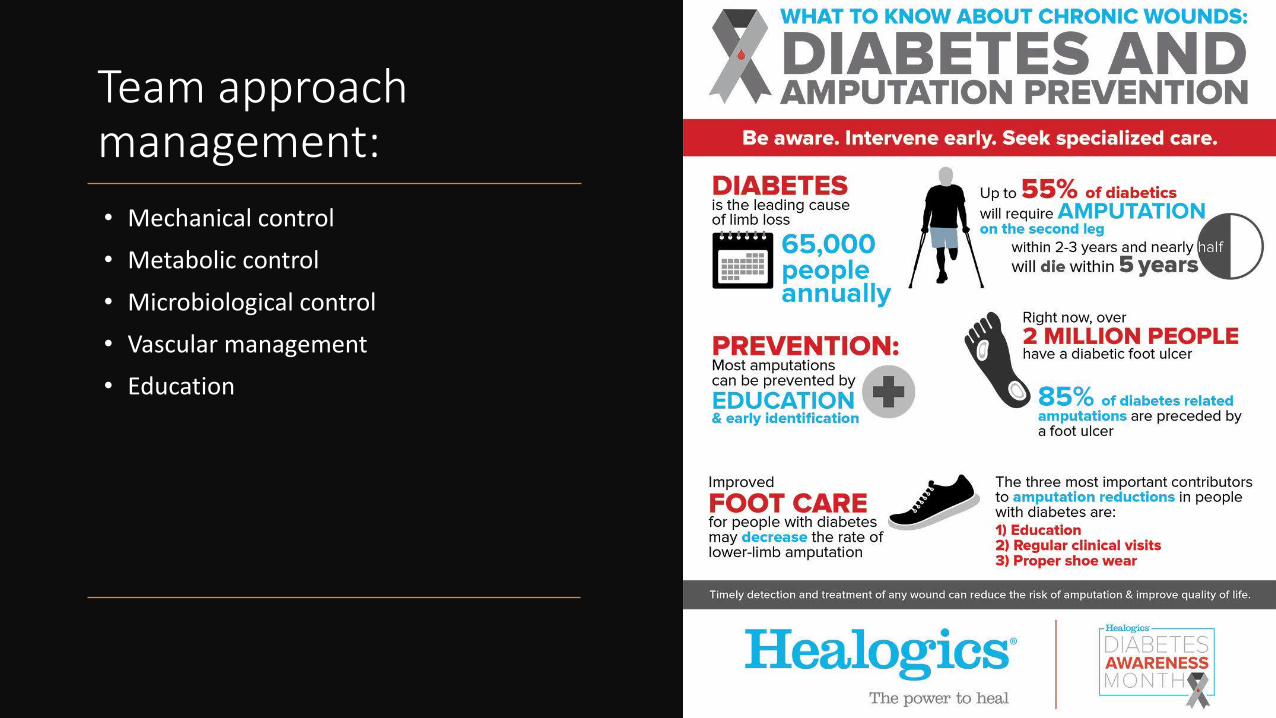
Team approach management:
• Mechanical control
• Metabolic control
• Microbiological control
• Vascular management
• Education
To Catch a Tumor: lumps and bumps



REFER TO THE SPECIALIST!!!
• SOME GENERAL PRACTITIONERS AND GENERAL SURGEONS ARE NOTORIOUSLY NOT GOOD AT REFERRING OUT.
• WHEN IN DOUBT, REFER IT OUT.
Thanks for your attention: