The Modern Science of Addiction - Food and Drug … Modern Science of Addiction Mary Jeanne Kreek,...
37
The Modern Science of Addiction Mary Jeanne Kreek, M.D. Patrick E. and Beatrice M. Haggerty Professor Head of Laboratory The Laboratory of the Biology of Addictive Diseases The Rockefeller University Senior Physician, The Rockefeller University Hospital Science Board – Food and Drug Administration Silver Spring, Maryland March 1, 2016 Funded primarily by NIH-NIDA (P50-05130), The Adelson Medical Research Foundation, NIH-NCRR (RUH – Dr B. Coller)
Transcript of The Modern Science of Addiction - Food and Drug … Modern Science of Addiction Mary Jeanne Kreek,...

The Modern Science of Addiction Mary Jeanne Kreek, M.D.
Patrick E. and Beatrice M. Haggerty Professor Head of Laboratory
The Laboratory of the Biology of Addictive Diseases The Rockefeller University
Senior Physician, The Rockefeller University Hospital
Science Board – Food and Drug Administration Silver Spring, Maryland
March 1, 2016
Funded primarily by NIH-NIDA (P50-05130), The Adelson Medical Research Foundation, NIH-NCRR (RUH – Dr B. Coller)
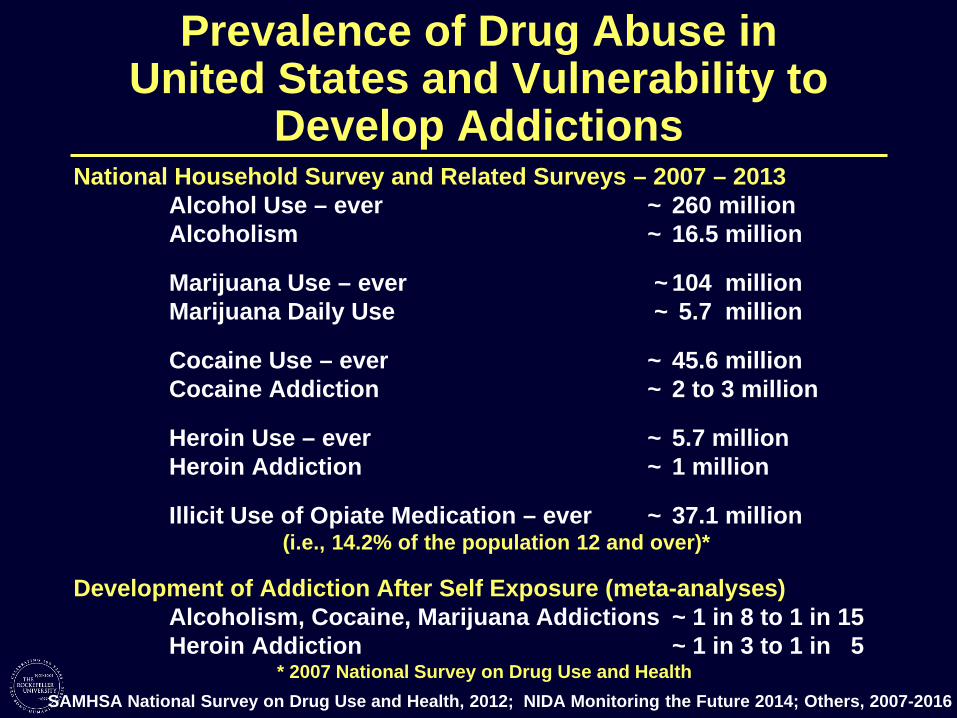
Prevalence of Drug Abuse in United States and Vulnerability to
Develop Addictions National Household Survey and Related Surveys – 2007 – 2013
Alcohol Use – ever ~ 260 million Alcoholism ~ 16.5 million
Marijuana Use – ever ~ 104 million Marijuana Daily Use ~ 5.7 million
Cocaine Use – ever ~ 45.6 million Cocaine Addiction ~ 2 to 3 million
Heroin Use – ever ~ 5.7 million Heroin Addiction ~ 1 million
Illicit Use of Opiate Medication – ever ~ 37.1 million (i.e., 14.2% of the population 12 and over)*
Development of Addiction After Self Exposure (meta-analyses) Alcoholism, Cocaine, Marijuana Addictions ~ 1 in 8 to 1 in 15 Heroin Addiction ~ 1 in 3 to 1 in 5
* 2007 National Survey on Drug Use and Health SAMHSA National Survey on Drug Use and Health, 2012; NIDA Monitoring the Future 2014; Others, 2007-2016

Number of Unintentional Drug Overdose Deaths Involving Prescription Opiates, Heroin, and Cocaine (United States,1999-2007) and Rate of Heroin Overdose Deaths (2002-13)
1.9 people die every day from heroin overdoses in New York City. (NYC Dept of Health – 2013)
23.5 million persons aged 12 and older needed treatment for an illicit drug or alcohol abuse
problem. Only 2.6 million received treatment at a specialized facility. (SAMHSA 2009)
47,000 persons (15 per 100,000) in the United States died of overdose deaths in 2014.
More than 3 people die every hour in the United States from illicit opiate overdose (2014).
(T Frieden, Center for Disease Control and Prevention, 2015)
National Vital Statistics System; MMWR 61:1, 2012; CDC Vitalsigns (online), July 7, 2015

PREVENT People From Starting Heroin
Reduce prescription opioid painkiller abuse. Improve opioid painkiller prescribing practices and identify high-risk individuals early:
REDUCE Heroin Addiction
Ensure access to Medication-Assisted Treatment (MAn. Treat people addicted to heroin or prescription opioid painkillers with MAT which combines the use of medications {methadone, buprenorphine, or naltrexone) with counseling and behavioral therapies.
REVERSE Heroin Overdose
Expand the use of naloxone. Use naloxone, a life-saving drug that can reverse the effects of an opioid overdose when administered in time.
CDC Vitalsigns (online), July 7, 2015
• • • • • •
•
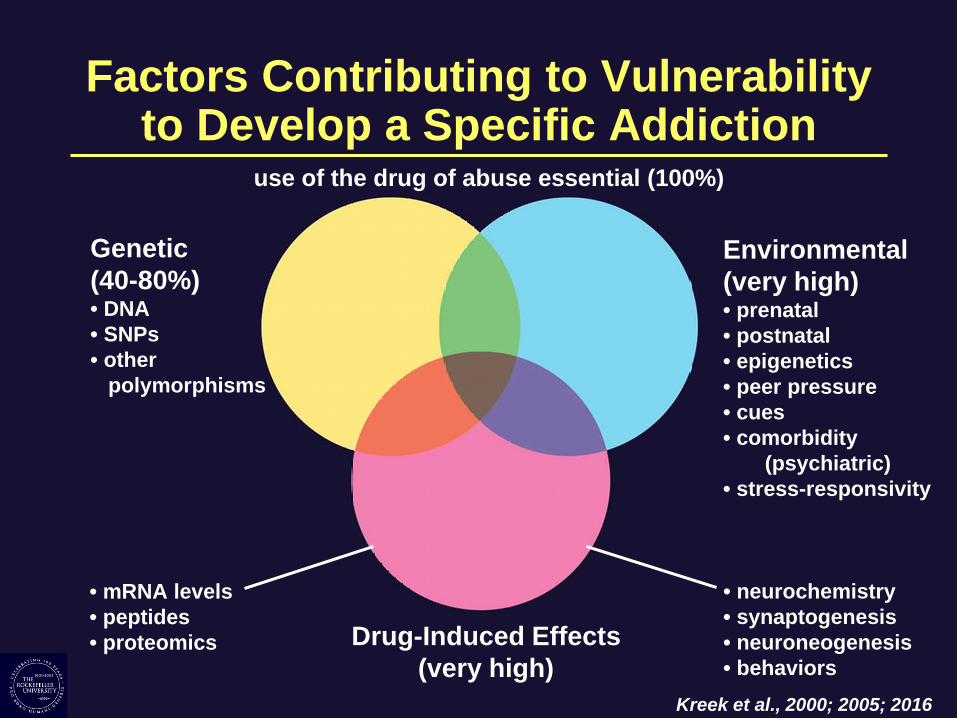
Factors Contributing to Vulnerabilityto Develop a Specific Addiction
use of the drug of abuse essential (100%)
Genetic (40-80%) • DNA • SNPs • other
polymorphisms
• • •
Environmental (very high)
prenatal postnatal epigenetics peer pressure cues comorbidity
(psychiatric) stress-responsivity
mRNA levels peptides proteomics Drug-Induced Effects
(very high)
• neurochemistry • synaptogenesis • neuroneogenesis • behaviors
Kreek et al., 2000; 2005; 2016
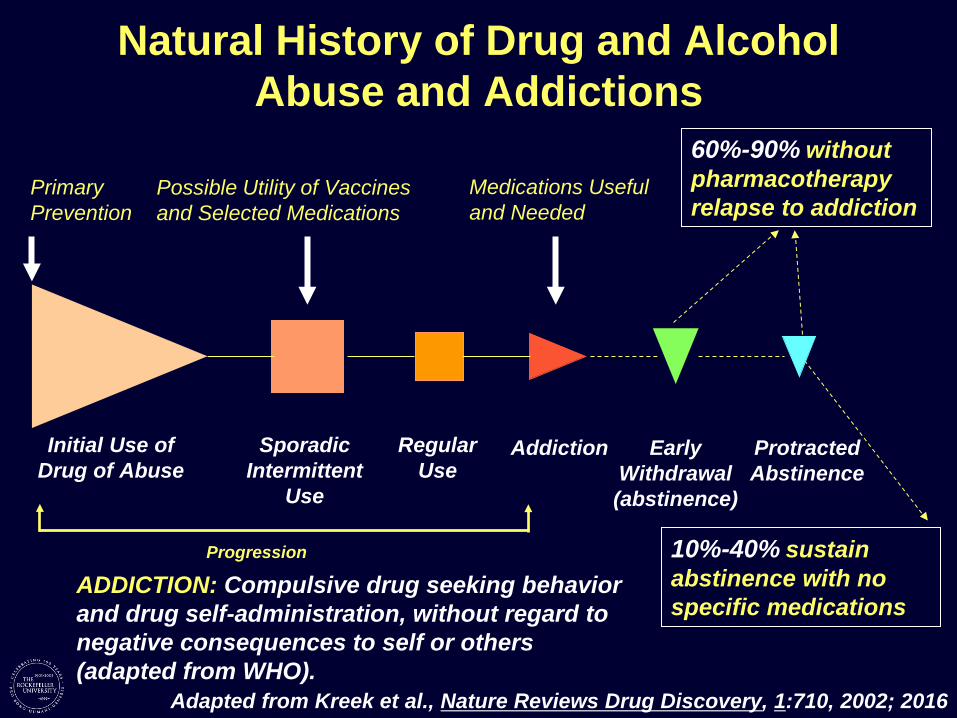
Natural History of Drug and Alcohol Abuse and Addictions
Primary Prevention
Possible Utility of Vaccines and Selected Medications
Medications Useful and Needed
60%-90% without pharmacotherapy relapse to addiction
Initial Use of Drug of Abuse
Sporadic Intermittent
Use
Regular Use
Addiction Early Withdrawal (abstinence)
Protracted Abstinence
Progression
ADDICTION: Compulsive drug seeking behavior and drug self-administration, without regard to negative consequences to self or others (adapted from WHO).
10%-40% sustain abstinence with no specific medications
Adapted from Kreek et al., Nature Reviews Drug Discovery, 1:710, 2002; 2016
50th Anniversary of First Research Paper onDeveloping Methadone Maintenance Treatment
HYPOTHESIS: Heroin (opiate) addiction is a disease – a “metabolic disease” – of the brain with resultant behaviors of “drug hunger” and drug self-administration, despite negative consequences to self and others. Heroin addiction is not simply a criminal behavior or due alone to antisocial personality or some other personality disorder. Vincent P. Dole, Jr., MD; Marie Nyswander, MD; and Mary Jeanne Kreek, MD
1964: Initial clinical research on development of treatment using methadone maintenance pharmacotherapy and on elucidating mechanisms of efficacy performed at The Rockefeller Hospital of The Rockefeller Institute for Medical Research:
First research paper describing methadone maintenance treatment research Dole, V.P., Nyswander, M.E. and Kreek, M.J.: Narcotic blockade: a medical technique for stopping heroin use by addicts. Transactions of the Association of American Physicians (May 1966), 79:122-136, 1966. (including discussion) Dole, V.P., Nyswander, M.E. and Kreek, M.J.: Narcotic blockade. Arch. Intern. Med., 118:304-309, 1966. Dole, Nyswander and Kreek, 1966, 2006, 2016

Impact of Short-Acting Heroin versus Long-Acting Methadone Administered on a Chronic Basis in Humans –
1964 through 1978 Studies: Opioid AgonistPharmacokinetics – Heroin Versus Methadone
Func
tiona
l Sta
te(H
eroi
n)
"High"
"Straight"
"Sick"
AM PM AM PM AM Days
Systemic Bioavailability
After Oral Apparent Plasma
Terminal Half-life Major Route of Biotrans-
Administration (t1/2 Beta) formation
Limited 3min Successive (<30%) (30min for active
- -6 acetyl morphine metabolite;
deacetylation and morphine
glucuronidation - 4 6h for morphine
and active - -morphine 6
glucuronide metabolite)
"High"
"Straight"
"Sick"
AM PM AM PM AM Days H
Func
tiona
l Sta
te(M
etha
done
)
Essentially 24h - N demethylation Complete (48h for active
(>70%) - [R](l) enantiomer)
Dole, Nyswander and Kreek, 1966; Kreek et al., 1973; 1976; 1977; 1979; 1982; Inturrisi et al, 1973; 1984
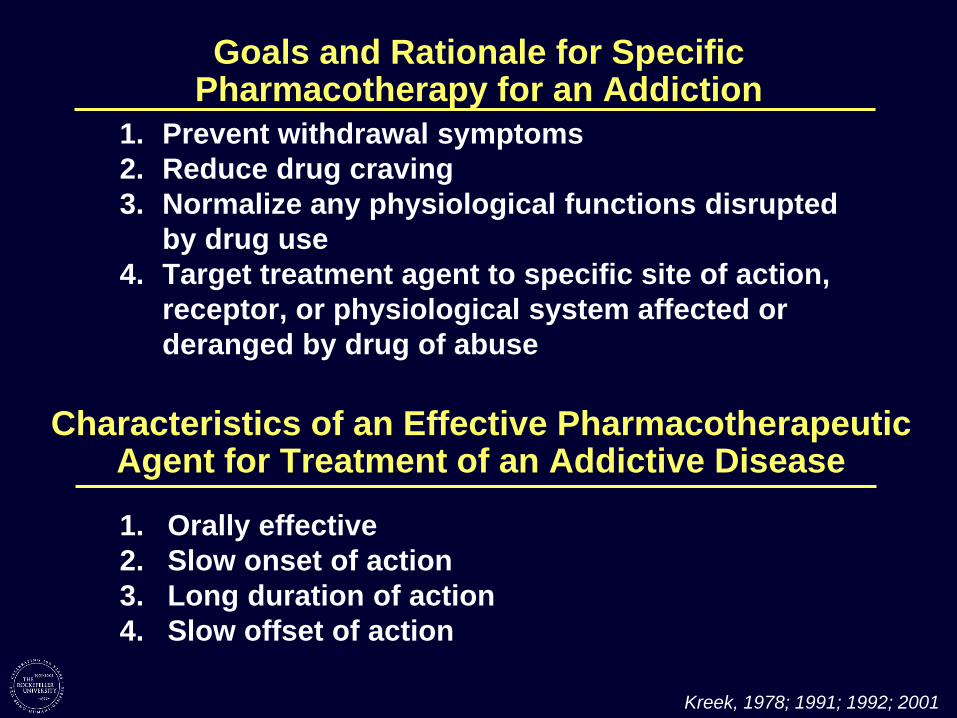
Goals and Rationale for SpecificPharmacotherapy for an Addiction
1. Prevent withdrawal symptoms 2. Reduce drug craving 3. Normalize any physiological functions disrupted
by drug use 4. Target treatment agent to specific site of action,
receptor, or physiological system affected or deranged by drug of abuse
Characteristics of an Effective PharmacotherapeuticAgent for Treatment of an Addictive Disease
1. Orally effective 2. Slow onset of action 3. Long duration of action 4. Slow offset of action
Kreek, 1978; 1991; 1992; 2001
•
•
•
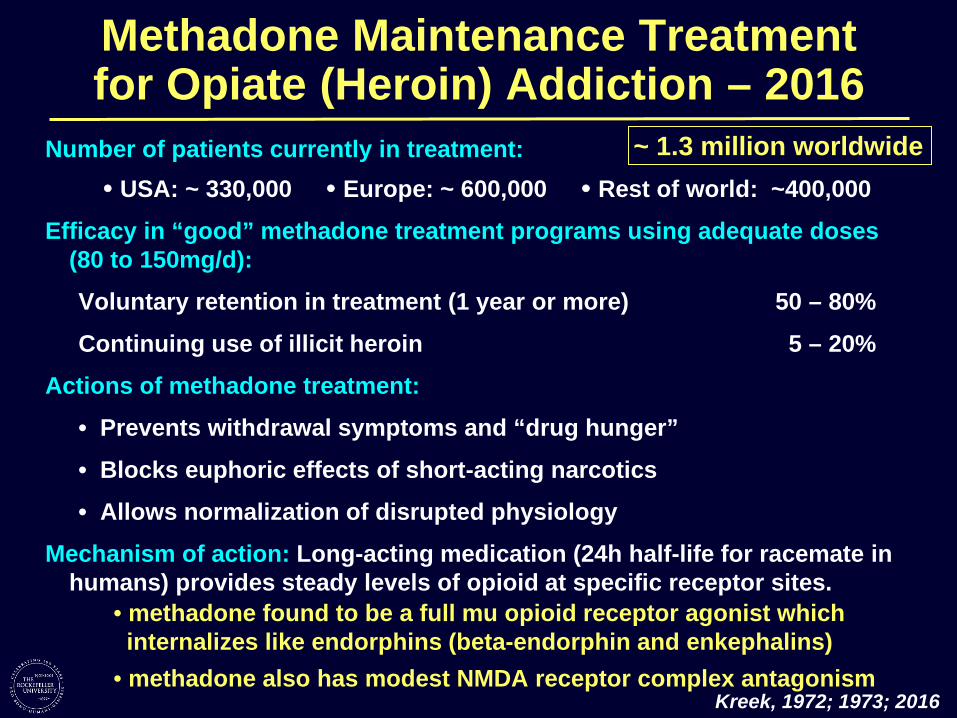
Methadone Maintenance Treatment for Opiate (Heroin) Addiction – 2016
Number of patients currently in treatment: ~ 1.3 million worldwide USA: ~ 330,000 Europe: ~ 600,000 Rest of world: ~400,000
Efficacy in “good” methadone treatment programs using adequate doses (80 to 150mg/d):
Voluntary retention in treatment (1 year or more)
Continuing use of illicit heroin
50 – 80%
5 – 20%
Actions of methadone treatment:
Prevents withdrawal symptoms and “drug hunger”
Blocks euphoric effects of short-acting narcotics
Allows normalization of disrupted physiology
Mechanism of action: Long-acting medication (24h half-life for racemate in humans) provides steady levels of opioid at specific receptor sites.
• methadone found to be a full mu opioid receptor agonist which internalizes like endorphins (beta-endorphin and enkephalins)
• methadone also has modest NMDA receptor complex antagonism Kreek, 1972; 1973; 2016

- -
Status of Methadone, Buprenorphine, andExtended Release Naltrexone Treatments in
the United States – 2013 (SAMHSA, 2015) Methadone Maintenance Treatment
Facilities 1,282
Patients 330,308
Buprenorphine Maintenance Treatment Facilities 3,113
Patients 48,148
Extended Release Naltrexone Treatment Facilities 1,718
Patients 3,781
Source: Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration. National Survey of Substance Abuse Treatment Services (N SSATS), 2003 2014
Communication from: Cathie E. Alderks, PhD, Federal Project Officer, Behavioral Health Services Information System, Center for Behavioral Health Statistics and Quality, SAMHSA, 2015

Limited Targeted PharmacotherapiesAvailable for Specific Addictive Diseases I. Opiate Addiction (Heroin and Illicit Use of Opiates)
a. METHADONE (50-80%)** b. BUPRENORPHINE (+ NALOXONE) (40-50%)* [c. NALTREXONE / SUSTAINED RELEASE NALTREXONE (<15%)*]
II. Alcoholism a. NALTREXONE (30-40%)* b. NALMEFENE (approved in Europe only, 2012) c. ACAMPROSATE (low in USA)
III. Nicotine Addiction (Primarily Tobacco Smoking) a. NICOTINE – DIVERSE DELIVERY SYSTEMS (?) b. BUPROPRION (?) c. VARENICLINE (?)
IV. Cocaine, Amphetamines and Other StimulantsNONE
(%) is % of unselected persons with specific addictions who can be retained voluntarily in treatment for 3 months (*) or 12 months (**), with success in eliminating specific drug use. Kreek, 2016
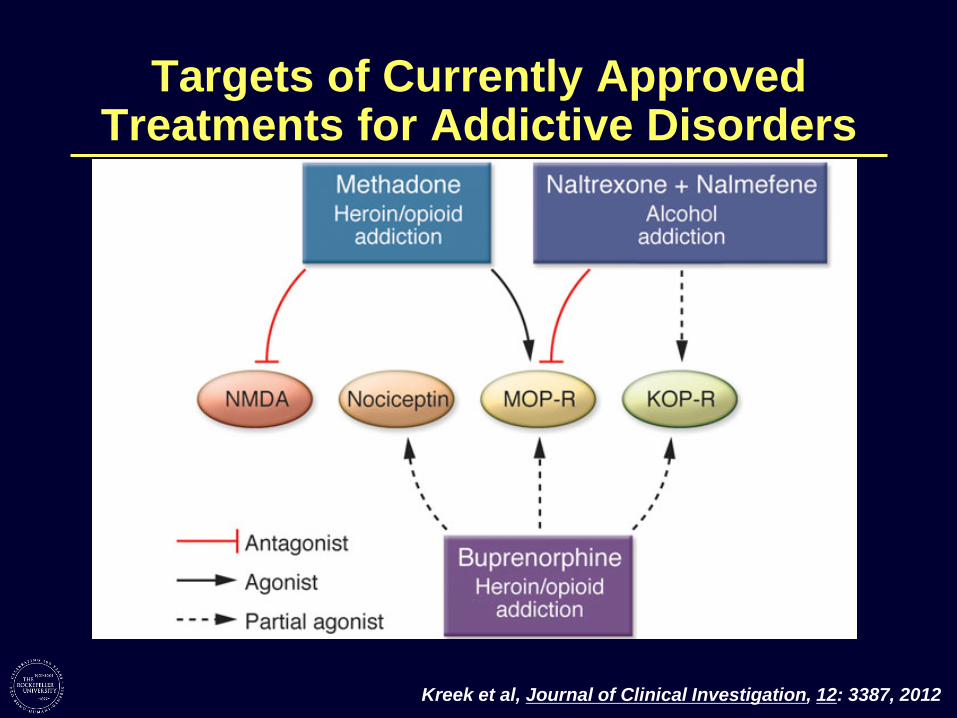
Targets of Currently ApprovedTreatments for Addictive Disorders
Kreek et al, Journal of Clinical Investigation, 12: 3387, 2012

•
•
•
Development of an Addiction:Neurobiology
Drugs alter normal brain networks and chemicals
“Rewarding” or “pleasurable” effects of drugs (the so-called “reinforcing effects”) involve: – –
Dopamine Endorphins (acting at Mu Opioid Receptors)
“Countermodulatory” response to reward involves: – Dynorphins (acting at Kappa Opioid Receptors)

•
•
•
•
•
•
Bidirectional-Translational Research: Novel and Conventional Animal Models
to Mimic Human Patterns of Abuse “Binge” Pattern Cocaine Parenteral Administration Model: Constant or Ascending Dose (mimics most common pattern of human use in addiction)
Intermittent Heroin (Morphine) Parenteral Administration Model: Constant or Ascending Dose (mimics most common pattern of human use in addiction)
“Binge” Pattern Oral Ethanol Administration Model: (mimics common pattern of human excessive use)
Intravenous Pump Methadone Administration Model: (converts short-acting pharmacokinetic properties of opioid agonist in rodent to long-acting human pharmacokinetic profile)
Intravenous Self-Administration (Mouse) Without or With High-Dose (also, extended access 4 h)
Extended Access (10 or 18 hours) Intravenous Self-Administration (Rat) with Individual Selection of Dose Escalation
Kreek et al., 1987; 1992; 2001; 2005; 2015
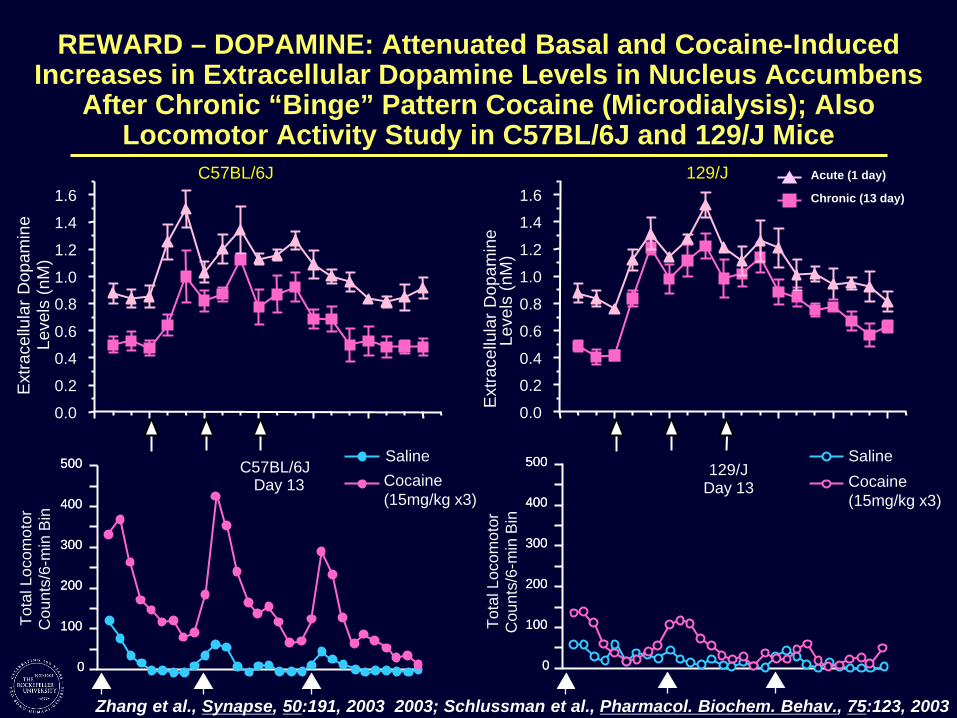
REWARD – DOPAMINE: Attenuated Basal and Cocaine-Induced Increases in Extracellular Dopamine Levels in Nucleus Accumbens
After Chronic “Binge” Pattern Cocaine (Microdialysis); AlsoLocomotor Activity Study in C57BL/6J and 129/J Mice
0.0
0.2
Leve
ls (n
M)
C57BL/6J
Saline
1.61.6
1.4
1.4
Acute (1 day)
Chronic (13 day)
129/J
Saline
Tota
l Loc
omot
orE
xtra
cellu
lar D
opam
ine
Leve
ls (n
M) 1.2 1.2
1.0
0.8
0.6
1.0
0.8
0.6
0.4 0.4
0.2
0.0
500500500500 C57BL/6J Day 13 Cocaine
(15mg/kg x3)
129/J Day 13 Cocaine
(15mg/kg x3)400400400400
Cou
nts/
6-m
in B
in
Cou
nts/
6-m
in B
in
300300300300
200200 200200
100100 100100
0000
To
tal L
ocom
otor
Ext
race
llula
r Dop
amin
e
Zhang et al., Synapse, 50:191, 2003 2003; Schlussman et al., Pharmacol. Biochem. Behav., 75:123, 2003
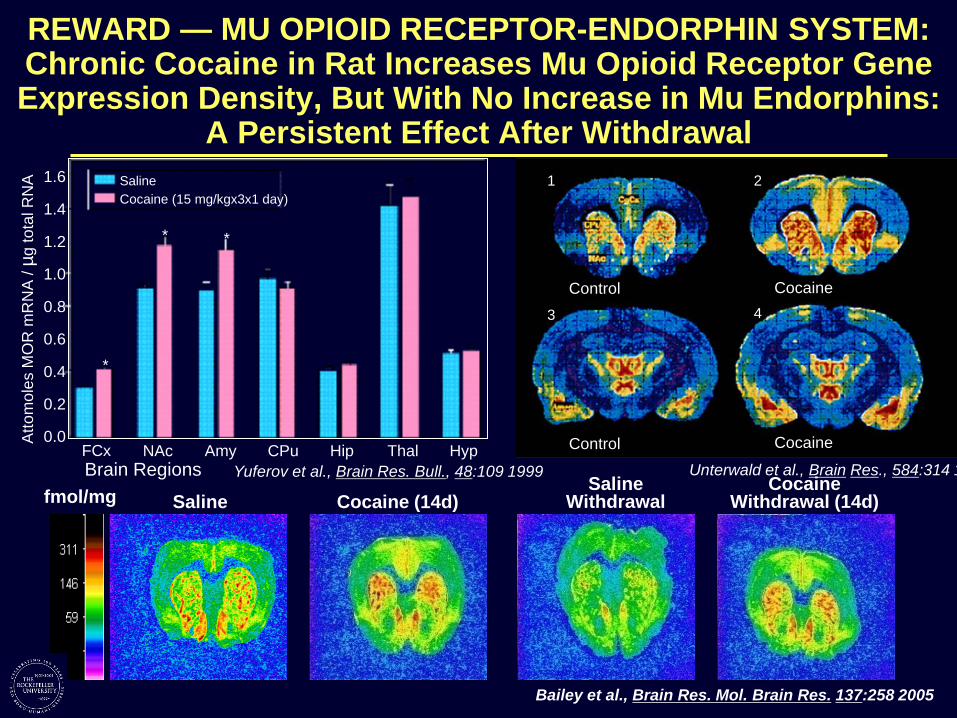
REWARD — MU OPIOID RECEPTOR-ENDORPHIN SYSTEM: Chronic Cocaine in Rat Increases Mu Opioid Receptor Gene Expression Density, But With No Increase in Mu Endorphins:
A Persistent Effect After Withdrawal
Control
1
Control
3
Cocaine
2
Cocaine
4
Atto
mol
es M
OR
mR
NA
/ µg
tota
l RN
A
FCx Brain Regions
Saline Cocaine (15 mg/kgx3x1 day)
0.0
0.2
1.0
1.2
1.4
0.4
0.6
0.8
1.6
NAc Amy CPu Hip Thal Hyp
*
**
fmol/mg Saline Cocaine (14d) Saline
Withdrawal Cocaine
Withdrawal (14d) Yuferov et al., Brain Res. Bull., 48:109 1999 Unterwald et al., Brain Res., 584:314 1
Bailey et al., Brain Res. Mol. Brain Res. 137:258 2005
REWARD — MU OPIOID RECEPTOR-ENDORPHIN SYSTEM: Mu Opioid Receptor Knock-Out Mice
•••
••
No morphine or other mu agonist analgesia No heroin or morphine self-administration No heroin or morphine induced conditioned place preference Attenuated self-administration of cocaine Attenuated self-administration of alcohol
[Different knock-out constructs and multiple research groups, including Kieffer,Uhl, Yu, Pintar, Loh, with, e.g., Maldonado, Pasternak, Hoellt, Roberts]
Reviewed in Kreek et al., Nature Reviews Drug Discovery, 1:710-726, 2002; 2010
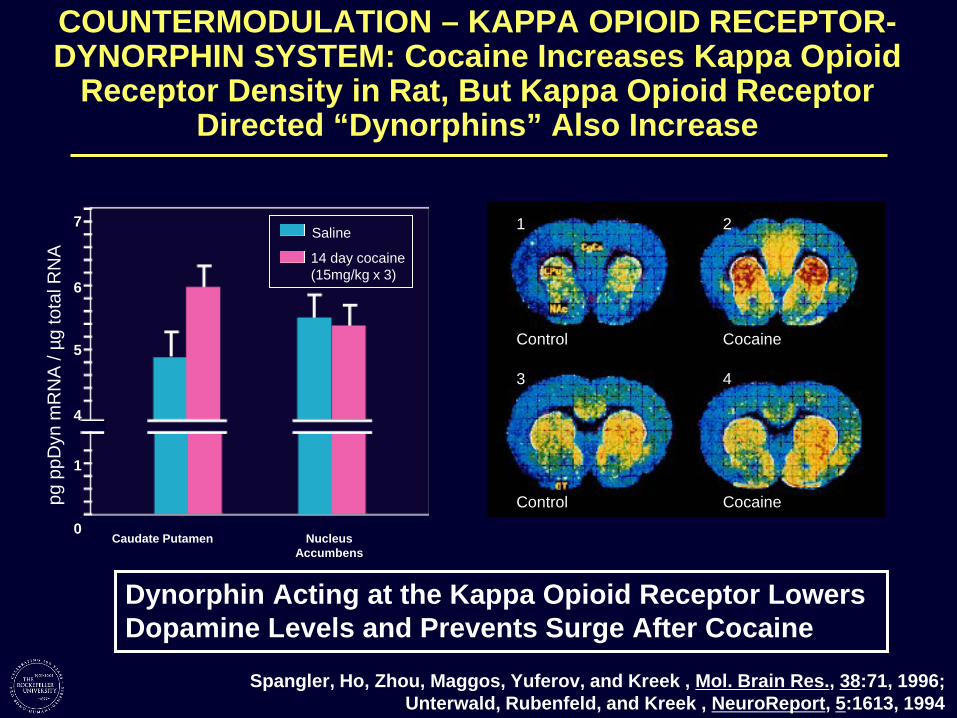
COUNTERMODULATION – KAPPA OPIOID RECEPTORDYNORPHIN SYSTEM: Cocaine Increases Kappa Opioid
Receptor Density in Rat, But Kappa Opioid ReceptorDirected “Dynorphins” Also Increase
0
pg p
pDyn
mR
NA
/ µg
tota
l RN
A
Control
1
Control
3
Cocaine
2
Cocaine
4
7
6
5
4
1
Caudate Putamen Nucleus
Saline
14 day cocaine (15mg/kg x 3)
Accumbens
Dynorphin Acting at the Kappa Opioid Receptor Lowers Dopamine Levels and Prevents Surge After Cocaine
Spangler, Ho, Zhou, Maggos, Yuferov, and Kreek , Mol. Brain Res., 38:71, 1996; Unterwald, Rubenfeld, and Kreek , NeuroReport, 5:1613, 1994
% o
f Sal
ine
Con
trol
ppDyn mRNA KOR mRNA
*
200 200
150
100
50 % o
f Sal
ine
Con
trol
150
100
50
*
0 0 Saline Morphine Saline Morphine
Saline
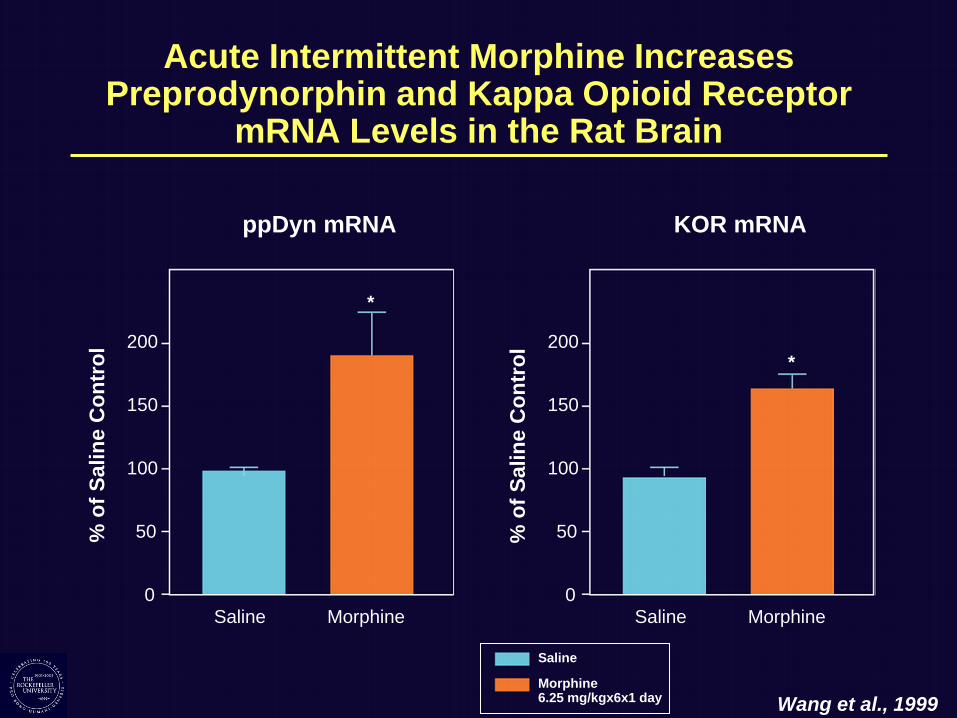
Morphine6.25 mg/kgx6x1 day Wang et al., 1999
Acute Intermittent Morphine IncreasesPreprodynorphin and Kappa Opioid Receptor
mRNA Levels in the Rat Brain

Natural Dynorphin A Lowers Basal and Cocaine Induced Dopamine Levels in Mouse Striatum
1-17
10 10
8
6
4
2
Dop
amin
e in
D
ialy
sate
(nM
) 8
6
4
2
0 0 60 120 180 60 120 180 Infusion Infusion Injection
20-min Sample 20-min Sample Dynorphin Dose (nmol)
0 1.0
2.0 4.4 4.4+nBNI (antagonist)
Dynorphin (4.4nmol) + Cocaine (15mg/kg)
Infusion and Injection Control Cocaine (15mg/kg)
D
ialy
sate
(nM
) D
opam
ine
in
Zhang, Butelman, Schlussman, Ho, and Kreek, Psychopharmacology, 172:422, 2004
•
•
•
•
Potential Biological Target Identifiedfor Novel Pharmacotherapies
(KOPr-Dynorphin System)
Need: Compounds selective for this target KOPr (agonist, biased agonist, partial agonist, and antagonist).
Major Clinical Concern with High Efficacy Kappa Agonist: Dysphoria; psychotomimesis
Actual Concern of Research Clinician: None. Tolerance develops to psychotomimetic effects. One recent study showed little to no problems in persons with long term addictions.
Potential Use in Treatments: Cocaine addiction; alcoholism; opiate addiction with concomitant cocaine or alcohol addiction
Kreek 2016

STRESS RESPONSIVITY – Dissecting the Hypothalamic-Pituitary-Adrenal Axis in
Humans: Selective Opioid Antagonist Testing
Endogenous Opioids
(mu – inhibition) (kappa – ? activation)
β-End (↑)
hypothalamus
anterior pituitary
POMC
Cortisol (↑) ACTH (↑)
CRF
Mu Opioid Receptor Antagonists
adrenal
Arginine Vasopressin
++
+
Kreek, 1984; 1998; 2006; 2014
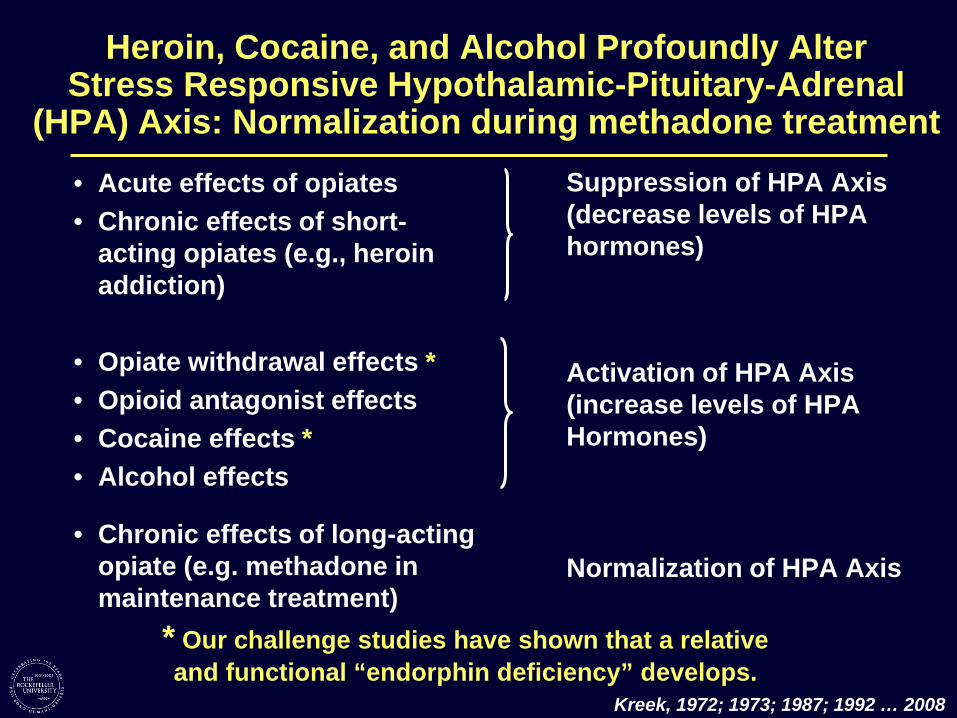
Heroin, Cocaine, and Alcohol Profoundly AlterStress Responsive Hypothalamic-Pituitary-Adrenal
(HPA) Axis: Normalization during methadone treatment • •
• • • •
•
Acute effects of opiates Chronic effects of short-acting opiates (e.g., heroin addiction)
Suppression of HPA Axis (decrease levels of HPA hormones)
Opiate withdrawal effects * Opioid antagonist effects Cocaine effects * Alcohol effects
Chronic effects of long-acting opiate (e.g. methadone in maintenance treatment)
Activation of HPA Axis (increase levels of HPA Hormones)
Normalization of HPA Axis
* Our challenge studies have shown that a relative and functional “endorphin deficiency” develops.
Kreek, 1972; 1973; 1987; 1992 … 2008

Nalmefene (mu/kappa Directed) Causes GreaterHPA Axis Activation Than Naloxone (mu Directed)
in Normal Human Volunteers (n=23)
=
40
35
30
25
20
15
AC
TH (p
g/m
l)
ACTH Cortisol 50 50
45 45
Cor
tisol
Lev
els
(µg/
dL)
40
35
30
25
20
15
10 10
0 10 20 30 40 50 60 75 90 120 150 180 240 0 10 20 30 40 50 60 75 90 120 150 180 240
Time after injection (min) Time after injection (min)
30 mg nalmefene 30 mg naloxone placebo (n 23) 10 mg nalmefene 10 mg naloxone (n=10 for each antagonist condition) (mu and kappa opioid (mu opioid receptorreceptor directed) directed)
Schluger, Ho, Borg, Porter, Maniar, Gunduz, Perret, King, and Kreek, Alcohol. Clin. Exp. Res., 22,1430, 1998

•
•
•
Genetic Variants of the Human Mu Opioid Receptor:Single Nucleotide Polymorphisms in the Coding Region
Including the Functional A118G (N40D) Variant
HYPOTHESIS
Gene variants:
Alter physiology “PHYSIOGENETICS”
Alter response to medications
“PHARMACOGENETICS”
Are associated with specific addictions
(A118G)
(C17T)
Bond, LaForge… Kreek, Yu, PNAS, 95:9608, 1998; Kreek, Yuferov and LaForge, 2000
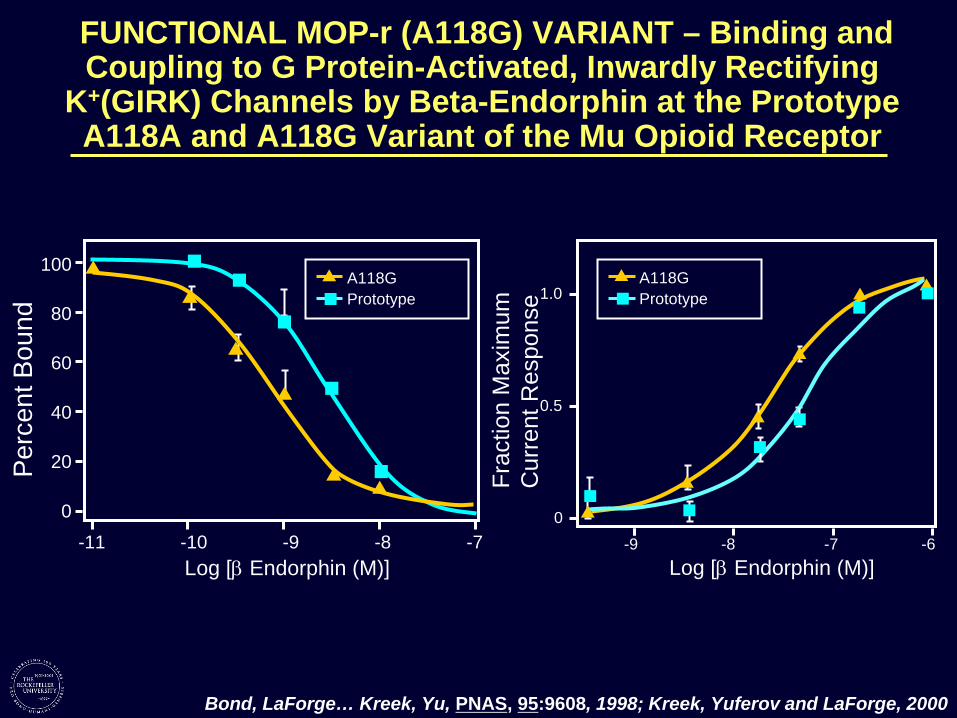
FUNCTIONAL MOP-r (A118G) VARIANT – Binding and Coupling to G Protein-Activated, Inwardly Rectifying
K (GIRK) Channels by Beta-Endorphin at the Prototype A118A and A118G Variant of the Mu Opioid Receptor
+
100
1.0
0.5
Cur
rent
Res
pons
e Fr
actio
n M
axim
um
A118G Prototype
-11 -10 -9 -8 -7
80
60
40
20
0
A118G Prototype
-9 -8 -7 -6
0
Log [β Endorphin (M)] Log [β Endorphin (M)]
Perc
ent B
ound
Bond, LaForge… Kreek, Yu, PNAS, 95:9608, 1998; Kreek, Yuferov and LaForge, 2000

FUNCTIONAL MOP-r (A118G) VARIANT – “Physiogenetics” Related to A118G Variant of Human
Mu Opioid Receptor Gene – Altered Stress Responsivity in Healthy Control Volunteers
P = Placebo
24 22 20 18 16 14 12 10 8Se
rum
Cor
tisol
(ug/
dl) N = Naloxone
P I
A/A (n=29)A/G (n=7) N N
N
N
Cor
tisol
Lev
els
-AU
C
(9:3
0am
-10:
30am
+ 9
0min
) 2500 Cortisol
(no
food
for 9
hou
rs)
0
2000
1000
1500
40 19
Prototype A118G
P < 0.05
500
50 0 50 100 150 200
Time (min)
Bart et al. Neuropsychopharmacology, Wand et al., Neuropsychopharmacol, 26:106, 2002 31:2313-2317, 2006 Chong…Wand, Neuropsychopharmacology, 31:204, 2006

FUNCTIONAL MOP-r (A118G) VARIANT –“Pharmacogenetics” Relatedto A118G Variant of Human Mu Opioid Receptor Gene, Which AltersStress Responsivity: Positive Predictor of Response to Naltrexone
Treatment of Alcoholics
0 Cum
ulat
ive
Surv
ival
(Tim
e to
Rel
apse
) 1.0 0.9 0.8 0.7 0.6 0.5
0.2
0.4 0.3
0.1 0.0
Naltrexone/ A/G, G/G (n=23) Naltrexone/ A/A (n=48)
Placebo/ A/A (n=41) Placebo/ A/G, G/G (n=18)
% W
ith G
ood
Clin
ical
Out
com
e
Placebo 100 Naltrexone hydrochoride
90 80 70 60 50 40
n=126 n=115 n=35 n=31
Asn40 Asp40
30 20 10
0 14 28 42 56 70 84
Days OPRM1 Genotype
Oslin et al., Neuropsychopharmacology, 28: 1546, 2003; Anton… Goldman et al., Arch Gen Pscyh, 65:135, 2008

Association Between a Functional Polymorphism in the mu Opioid Receptor Gene and Opiate Addiction and
also Alcoholism in Central Sweden Opiate Dependent (n=139) Control (n=170)
G/G; A/G 41 23 A/A 98 147
118G Allele Frequency 0.155 0.074
Thus, in the entire study group in this central Swedish population: Attributable Risk due to genotypes with a G allele: 18%
(with confidence interval ranges from 8.0 to 28.0%) Bart G , Heilig M, LaForge KS… Ott J, Kreek MJ, et al., Molecular Psychiatry, 9:547-549, 2004
Alcohol Dependent (n=389) Control (n=170) G/G; A/G 90 23
A/A 299 147 118G Allele Frequency * 0.125 0.074
* Overall 118G Allele Frequency = 0.109 Thus, in the entire study group in this central Swedish population:
Attributable Risk due to genotypes with a G allele: 11.1% (with confidence interval ranges from 3.6 to 18.0%)
Bart G , Kreek MJ, LaForge KS… Ott J, Heilig M, Neuropsychopharmacology, 30:417, 2005

Heroin Self-Administration (10 d; 4h/d) in Male and Female Wild-Type (A/A) and Genetically Modified
A112G (G/G) Mice: A Model of the Human A118G Mu Opioid Receptor Functional Variant
N o
se p o
kes
4 0 1 0 4 0 1 0
8
6
4
2 D
ai l
y H
er o
i n D
o s
e (
m g
/ kg
)
N o
se
p o
ke
s
M a l e s F e m a l e s
D a
i l y
H e
r o i n
S A
( m
g / k
g )
A A ( 1 5 ) G G ( 1 2 )
3 0
2 0
1 0
3 0
A A ( 12)
G G ( 1 2 )
2 0
1 0
0 0 0 0 1 2 3 4 5 6 7 8 9 1 0 1 2 3 4 5 6 7 8 9 1 0
D a y D a y
2
4
6
8
Zhang et al., Neuropsychopharmacology, 40:1091, 2015

Microdialysis in Striatum of Prototype A112A versus Genetically Modified G112G Mice: Absolute Dopamine
Levels of Three Baseline Samples and Levels ofDopamine after Heroin Injections
14
8 6 4 2
Females Males 14
GG (6) 12
Dop
amin
e (n
M) 12 GG (6)
10 10
AA (7) 2
8 6 4AA (6)
0 0
10mg/kg 20mg/kg 10mg/kg 20mg/kg Heroin Heroin Heroin Heroin
Dop
amin
e (n
M)
Zhang et al., Neuropsychopharmacology, in press, 2015

AIMS Markers and Gene Variants Associated with Long-Term Severe Opioid Addiction
African African cluster Descent
European European cluster Descent 12 genes
European sample
(24 genes)
African sample
(35 genes)
12 genes
Shared SNPs: DRD2: rs1076563
rs2587546
Kreek 2016, after Levran 2015

Variants of Opioid and Stress Related Genes Associated with Opiate Addiction in Caucasians
Which Have Been Replicated (7 of over 15) Genes
OPRM1 (mu opioid receptor)
OPRD1 (delta opioid receptor)
OPRK1 (kappa opioid receptor)
PDYN (dynorphin peptide)
Variant A118G (rs1799971)
rs2236861, rs3766951, rs2236857
NSV*
NSV*
Refs e.g, Bond… Kreek and Yu, 1998;
Stadlin et al., 2001; Haerian and Haerian, 2013 Levran et al., 2008; Beer et al., 2013;
Nelson et al., 2014 Yuferov et al., 2004; Levran et al., 2009;
Kumar et al., 2012 Wei et al., 2011; Clarke et al., 2012
AVPR1A (arginine vasopressin
receptor 1A)
FKBP5 (FK506-binding protein
51/ corticosterone chaperone)
GAL (galanin)
*NSV – N
rs11174811; rs1587097; rs10784339
rs1360780; rs3800373
rs694066
o Single Variant; replic
Maher et al., 2011; Levran et al., 2014
Levran et al., 2014a; Levran et al., 2014b
Maher et al., 2011, Levran et al., 2014
ation is on association of entire genes
Kreek 2016; adapted from Reed et al., Current Psychiatry Reports,16(11): 504, 2014

PHARMACOGENOMICS – CYP2B6 SNPs are Associated with Effective Methadone Dose (n=74) (516G>T and 785A>G)
(Replication)
50
10
0 15
0 20
0 25
0
GGGT
TT
GG GT
250 30 60 90 120 150 180 210 240 270
Met
hado
ne d
ose
(mg/
d)
25
20
150
Num
ber o
f sub
ject
s
mg/day 15
CYP2B6 rs3745274 (516G>T) G/G G/T T/T 10
rs3745274 (516G>T) 5
0
Methadone dose (mg/day)
50
100
150
200
A/A A/G G/G
GG
AA AG
AA AG
Met
hado
ne d
ose
(mg/
d)
150 mg/day
Rs2279343 (785A>G)
Levran … Kreek, Addiction Biology, 18: 709, 2012 Dobrinas…Eap, Pharmacogenet Genomics, 23:84, 2013
Gadel et at., Drug Metab Dispos, 41: 709, 2013
September 10, 2003 – FDA Presentation“Major Issues Related to Physician Prescribing of
Long-Acting Mu Opioid Receptor Agonists”
A. Lack of adequate or updated medical education concerning pharmacokinetics and pharmacodynamics of long-acting (intrinsic or by formulation) mu opioid receptor agonists and partial agonists.
B. Lack of adequate (or any) medical school education concerning any of the specific addictions and also medical approaches to assessing persons with ongoing misuse, abuse, or addiction to drugs.
C. Stigma, ingrained in physicians and other healthcare workers by their formal health-related education, against the addictive diseases, the persons suffering from addictive diseases, the providers of healthcare services to those with addictive diseases, and the medications used to treat addictive diseases (e.g., methadone and buprenorphine-naloxone).
Kreek, adapted from Long Acting Opioids: Challenges in Pharmacotherapy presented at the FDA September 10, 2003