The lungs and their relations
3
THORACIC ANAESTHESIA AND INTENSIVE CARE MEDICINE 9:11 459 © 2008 Elsevier Ltd. All rights reserved. The lungs and their relations John Craven Abstract The anatomy of the lungs is described with particular reference to its sur- face markings and those of the pleural sac. The lung’s blood supply and lymphatic drainage are summarized. Keywords blood supply; costal surface; fissures; hilus; lungs; lymphatic drainage; lobes; mediastinal surface; pleural sac Each lung lies in a pleural sac (see pages 462–63, in this issue) attached by the pulmonary vessels to the mediastinum. Each is cone-shaped to conform to the contours of the thoracic cavity and is spongy and elastic in texture. The right lung is slightly larger (620 g) than the left (560 g). Each lung has an apex in the root of the neck and a base resting on the diaphragm. The base is separated by a sharp inferior border from a lateral con- vex surface and a medial concave mediastinal surface. In the centre of the mediastinal surface the structures forming the root of the lung are surrounded by a collar of reflected pleura. The medial surface of the left lung is concave to accommodate the left ventricle of the heart and the anterior border of the left lung is indented by the heart to form the cardiac notch. In both lungs the posterior border is rounded and lies in the paravertebral sulcus. Each lung is divided into lobes by fissures that extend deeply into their substance. An oblique fissure divides the left lung into an upper and a lower lobe. In the right lung, oblique and hori- zontal fissures divide the right lung into upper, middle and lower lobes (Figure 1). In both lungs the surface marking of the oblique fissure is a line extending round the chest wall from the spine of the third thoracic vertebra to the sixth costochondral junction. The horizontal fissure is marked on the surface by a horizontal line passing laterally to the oblique fissure from the fourth right costochondral junction (Figure 2). The lower lobes of both lungs lie below and behind the oblique fissure and comprise most of the posterior and inferior borders and parts of the medial and costal surfaces. The upper lobe of the left lung lies above and in front of the oblique fissure and comprises the apex, large parts of the mediastinal and costal surfaces and the whole of the anterior border. The equivalent part of the right lung is divided by the horizontal fissure into a John Craven, MD, FRCS, was formerly Consultant Surgeon at York District Hospital, York, UK. He is past chairman of the primary examiners of the Royal College of Surgeons of England. Conflicts of interest: none declared. large upper lobe and a smaller, wedge-shaped, anteriorly placed middle lobe. Some variation exists in this lobar pattern. Fissures may be missing or incomplete. The hilus of each lung contains a main bronchus, pulmonary artery, two pulmonary veins, the pulmonary nerve plexus and lymph nodes. It is surrounded by the collar of pleura reflected from the lung onto the mediastinum, the narrow inferior extension of which is known as the pulmonary ligament. Parietal relations The borders of the lungs closely follow the lines of pleural reflection on the chest wall except where the inferior border of the lung lies about two intercostal spaces above the infe- rior limit of the pleura and in front on the left side where the cardiac notch lies about 3 cm lateral to the pleural reflection (Figure 2). The costal surface is related to the thoracic wall. The base is separated by the diaphragm, on the right side from the right lobe of the liver, and on the left side from the left lobe of the liver, the stomach and the spleen. The apex is covered by the dome of the pleura and the suprapleural membrane and above them arch the subclavian vessels. Posteriorly the apex is separated from the neck of the first rib by the anterior primary ramus of the first thoracic nerve, the superior intercostal artery, the sympathetic trunk and the pleura. Medial relations The medial relations of the two lungs differ (Figures 3 and 4). On the left lung there is a concavity anteroinferiorly for the left ventricle, which is continuous superiorly with a groove for the Lobes and fissures of the lungs Horizontal fissure Oblique fissure Oblique fissure Upper lobe Right lung Left lung Upper lobe Lower lobe Lower lobe Middle lobe Figure 1
-
Upload
john-craven -
Category
Documents
-
view
216 -
download
2
Transcript of The lungs and their relations

Thoracic
The lungs and their relationsJohn craven
AbstractThe anatomy of the lungs is described with particular reference to its sur-
face markings and those of the pleural sac. The lung’s blood supply and
lymphatic drainage are summarized.
Keywords blood supply; costal surface; fissures; hilus; lungs; lymphatic
drainage; lobes; mediastinal surface; pleural sac
Each lung lies in a pleural sac (see pages 462–63, in this issue) attached by the pulmonary vessels to the mediastinum. Each is cone-shaped to conform to the contours of the thoracic cavity and is spongy and elastic in texture. The right lung is slightly larger (620 g) than the left (560 g). Each lung has an apex in the root of the neck and a base resting on the diaphragm. The base is separated by a sharp inferior border from a lateral con-vex surface and a medial concave mediastinal surface. In the centre of the mediastinal surface the structures forming the root of the lung are surrounded by a collar of reflected pleura. The medial surface of the left lung is concave to accommodate the left ventricle of the heart and the anterior border of the left lung is indented by the heart to form the cardiac notch. In both lungs the posterior border is rounded and lies in the paravertebral sulcus.
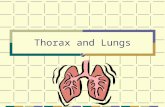
Each lung is divided into lobes by fissures that extend deeply into their substance. An oblique fissure divides the left lung into an upper and a lower lobe. In the right lung, oblique and hori-zontal fissures divide the right lung into upper, middle and lower lobes (Figure 1). In both lungs the surface marking of the oblique fissure is a line extending round the chest wall from the spine of the third thoracic vertebra to the sixth costochondral junction. The horizontal fissure is marked on the surface by a horizontal line passing laterally to the oblique fissure from the fourth right costochondral junction (Figure 2).
The lower lobes of both lungs lie below and behind the oblique fissure and comprise most of the posterior and inferior borders and parts of the medial and costal surfaces. The upper lobe of the left lung lies above and in front of the oblique fissure and comprises the apex, large parts of the mediastinal and costal surfaces and the whole of the anterior border. The equivalent part of the right lung is divided by the horizontal fissure into a
John Craven, MD, FRCS, was formerly Consultant Surgeon at York District
Hospital, York, UK. He is past chairman of the primary examiners of
the Royal College of Surgeons of England. Conflicts of interest: none
declared.
aNaESThESia aND iNTENSiVE carE MEDiciNE 9:11 4
large upper lobe and a smaller, wedge-shaped, anteriorly placed middle lobe. Some variation exists in this lobar pattern. Fissures may be missing or incomplete.
The hilus of each lung contains a main bronchus, pulmonary artery, two pulmonary veins, the pulmonary nerve plexus and lymph nodes. It is surrounded by the collar of pleura reflected from the lung onto the mediastinum, the narrow inferior extension of which is known as the pulmonary ligament.
Parietal relations
The borders of the lungs closely follow the lines of pleural reflection on the chest wall except where the inferior border of the lung lies about two intercostal spaces above the infe-rior limit of the pleura and in front on the left side where the cardiac notch lies about 3 cm lateral to the pleural reflection (Figure 2).
The costal surface is related to the thoracic wall. The base is separated by the diaphragm, on the right side from the right lobe of the liver, and on the left side from the left lobe of the liver, the stomach and the spleen. The apex is covered by the dome of the pleura and the suprapleural membrane and above them arch the subclavian vessels.
Posteriorly the apex is separated from the neck of the first rib by the anterior primary ramus of the first thoracic nerve, the superior intercostal artery, the sympathetic trunk and the pleura.
Medial relations
The medial relations of the two lungs differ (Figures 3 and 4). On the left lung there is a concavity anteroinferiorly for the left ventricle, which is continuous superiorly with a groove for the
Lobes and fissures of the lungs
Horizontal
fissure
Oblique fissure
Oblique
fissure
Upper lobe
Right lung Left lung
Upper lobe
Lower
lobe
Lower
lobe
Middle lobe
Figure 1
59 © 2008 Elsevier Ltd. all rights reserved.

Thoracic
Surface anatomy of pleurae and lungs
Horizontal fissure
Cardiac notch
Oblique
fissure
Lung base
Lower extent
of the pleural
cavity
Anterior view Posterior view
Figure 2
aortic arch passing in front of and above the hilum. Above this groove the surface is in contact with the left brachiocephalic vein, left common carotid and left subclavian arteries and the oesophagus.
aNaESThESia aND iNTENSiVE carE MEDiciNE 9:11 46
On the right lung there is a shallow concavity in front of the hilum for the right atrium which is continuous above and below with shallow grooves for the superior and inferior venae cavae. Above the superior groove the surface is in contact with the left
Medial surface of the left lung
The hilus is surrounded by the cut edges of the pleura and
pulmonary ligament (inferiorly)
Groove for the left
common carotid artery
Groove for the left
subclavian artery
Impression for
the aortic arch
Bronchus
Pulmonary
ligament
Oesophageal
impression
Cardiac notch
Left ventricular
impression
Pulmonary
veins
Pulmonary artery
Figure 3
Medial surface of the right lung
Superior vena
caval impression
Pulmonary
arteries
Pulmonary
veins
Right atrial
impression
Oesophageal
impression
Groove for
azygos vein
Bronchi
Pulmonary
ligament
Oesophageal
impression
Figure 4
0 © 2008 Elsevier Ltd. all rights reserved.

Thoracic
brachiocephalic vein, the left common carotid and subclavian arteries and the oesophagus.
Blood supply
The heart returns mixed venous blood to the lungs by the pulmo-nary trunk. After respiratory exchange the blood is then returned by the pulmonary veins.
The pulmonary trunk is a wide vessel, about 5 cm long. It begins at the pulmonary valve, ascends posteriorly to the left of the aorta and bifurcates under the concavity of the aortic arch into right and left pulmonary arteries.
The right pulmonary artery passes horizontally to the hilus of the right lung behind the ascending aorta and in front of the oesophagus and right main bronchus before dividing into branches that follow the segmental bronchi, ending in a capillary network within the alveolar walls.
The left pulmonary artery passes to the left lung hilus in front of the left bronchus and the descending aorta. It is connected by the ligamentum arteriosum, normally fibrosed shortly after birth, to the lower surface of the aortic arch. It also divides within the sub-stance of the lung, its branches following the segmental bronchi.
Bronchial arteries: lung tissue is supplied not by the pulmonary arteries but by the bronchial arteries, which are small branches of the descending thoracic aorta. The corresponding bronchial veins drain into the azygos or hemiazygos veins. Some of the bronchial arterial blood drains back to the heart in the pulmo-nary veins.
The pulmonary veins are short, wide vessels that pass directly horizontally into the left atrium. There are usually two (upper
aNaESThESia aND iNTENSiVE carE MEDiciNE 9:11 4
and lower) from each lung. In the lung hilus they lie below the pulmonary artery; on the right, they lie behind the superior vena cava and the right atrium, and, on the left, behind the left atrium and in front of the aorta. The pulmonary veins are formed by the union of smaller veins that drain oxygenated blood from the capillary bed in the alveolar walls.
Lymphatic drainage
Lymphatic drainage of the lungs is via a superficial subpleural lymph plexus and a deep plexus of lymph vessels accompanying the bronchi. Both groups drain through hilar or bronchopulmo-nary nodes to tracheobronchial nodes and thence to mediastinal lymph trunks.
The tracheobronchial nodes lie alongside the trachea and bronchi and receive afferents from the lungs, bronchi, trachea and heart. Their efferents drain to the bronchomediastinal lymph trunks which ascend alongside the trachea to end in the right lymph duct and, on the left, the thoracic duct.
Nerve supply
Innervation of the lung is by the pulmonary plexus, which conveys both the sympathetic (bronchodilator) fibres from the upper four thoracic sympathetic ganglia and the parasympathetic (bronchoconstrictor) fibres from the vagus. Sensory fibres pass largely in the vagus nerves. ◆
FurTher reAdiNg
abrahams P, craven J, Lumley J. illustrated clinical anatomy. London:
hodder arnold, 2005
(The anatomy, relations and surface anatomy of the lungs are
described).
61 © 2008 Elsevier Ltd. all rights reserved.