QIPP Digital Technology Team EPaCCS Informatics Advisory and Support Group
Upload
cecil-hubbardCategory
view
214download
1

The LTC QIPP Development programme &Year of Care Funding Model

3
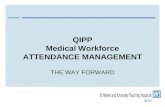
Annual HC spending per capita by age group2004, USD thousand
Aging populations
Source:UN population database, US Centers for Medicare and Medical services reproduced with kind permission of Novartis
1.5
0.4
2000 2050
+252%
WORLD
Aging Population Billion people >65 years
US
3
3
5
8
11
16
2685+
75–84
65–74
55–64
45–54
19–44
0–18
All ages = 5

– The majority of over-65s have 2 or more conditions, and the majority of over-75s have 3 or more conditions
– More people have 2 or more conditions than only have 1
Multimorbidity is common in Scotland

Records of 1.7 million patients showed
• Only 19% of patients with COPD have just COPD
• Only 14% of patients with Diabetes have just Diabetes
• Only 5% of patients with Dementia have just Dementia
• etc
Mercer Guthrie and Wyke Univ of Glasgow 2011



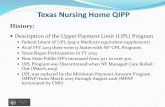
Team A
Team B
Team C
Team D
?

Integrated neighbourhood Care Team

Primary drivers
• Systematic risk profiling of population
• Integrated locality care teams including social care, community services, allied health professionals and general practice
• Maximising number of patients who can self manage through systematic transfer of knowledge, and care planning

Risk stratification
•Better targeted services improves outcomes
•Enhanced targeted assessment was associated with improved mortality and physical function after one year1
•Targeted activities to activate patients have the greatest impact when targeted a specific high risk groups2
•When integrated stroke care was targeted at highest risk, this increase survival and reduced need for institutional care3
Source: (1) Stuck, Siu, Whieland et al. “Comprehensive geriatric assessment: a meta-analysis of controlled trials. Lancet 1992; 342: 1032-6Source: (2) Conn, Valentine & Cooper “Interventions to increase physical activity among aging adults: a meta-analysis”. Ann Behav Med 2002; 24(3): 190-200Source: (3) Fagerberg, et al. “Effect of acute stroke unit care integrated with care continuum versus conventional treatment. Stroke 2000; 31(11): 2578-84

Integrated teams
• Improved health status, reduced weight and improved diet.1,4 • People were most likely to be alive, living independently at
home.6
• Improved symptoms and behaviours.5
• Improved health status & mental well-being. Outcomes for lower cost.3,7
• Source: (1) Kasper “A Randomized Trial of the Efficacy of Multidisciplinary Care in Heart Failure Outpatients at High Risk of Hospital Readmission”. Journal of the American College of Cardiology Vol. 39, No. 3, 2002
• Source: (2) Griffiths. “Cost effectiveness of an outpatient multidisciplinary pulmonary rehabilitation programme”. Thorax 2001;56:779–784
• Source: (3) van den Hout “Patient team care nurse specialist care, inpatient team care, and day arthritis: a randomised comparison of clinical multidisciplinary care in patients with rheumatoid”. Ann Rheum Dis 2003 62: 308-315
• Source: (4) Capomolla et al. “Cost/utility ratio in chronic heart failure: comparison between heart failure management programme delivered by day-hospital and usual care” J Am Coll Cardiol 2002; 40: 1259-66
• Source: (5) Opie, Doyle & O’Connor “Challenging behaviours in nursing home residents with dementia: a RCT of multidisciplinary interventions” Int J Geriatr Psychiatry 2002; 17(1):6-13
• Source: (6) Stroke Unit Trialists’ collaboration “Organised inpatient care for stroke” Cochrane Library, issue 2, 2004
• Source: (7) Ahlmen et al “Team vrs non-team outpatient care in rheumatoid arthritis” Arthritis Rheum 1988; 31(4): 471-9

Self Management
• reduce number of GP visits
• help to prevent unnecessary admissions to hospital
• reduce length of stay of necessary hospital admissions
• improve health status and self efficacy
• enable patients to remain in their homes and communities
• improve feeling of control in their condition
• increase choice for patients
• improve end of life care
• integrate all elements of care
• deliver better glycaemic control for diabetic patients
• lead to reduced stress for people with mental health conditions• 1 http://www.crd.york.ac.uk/CRDWeb/ShowRecord.asp?View=Full&ID=32006001556

Other literature
• 20% patients identified by risk stratification could not be identified in any other way
• Improving access to care for these people improves quality of care
• Large RCT in US (Boult) showed this approach reduced inpatient days (52%), Aand E visits (17%) and readmissions (49%)
• 16 other studies showed significant reductions in length of stay, admissions and Aand E visits

In other words ..
You need to do them all
.. And status quo is not an option

Risk Profiling
Milestone Two - By ....20% of practices covering a minimum 50% of the population within the CCG or cluster have committed to implementing a risk profiling tool and have a plan to systematically use the data with the integrated neighbourhood team
Milestone Three - By ....All practices that have implemented a risk profiling tool are systematically using the data with the integrated neighbourhood team to pro-actively manage patients identified 'at risk

National Average – Risk Profiling
Milestone 2 Achieved 56.35%Milestone 2 Date set 43.65%
Milestone 3 Achieved 18.54%Milestone 3 Date set 57.60%

Integrated Care Teams
Milestone Three - By....The implementation team have identified and engaged all relevant stakeholders/ clinicians and developed an action plan to embed the integrated neighbourhood team model in a minimum 20% of practices covering a minimum of 50% of the population within the CCG/ locality.Milestone Four - By....All integrated neighbourhood care teams attached to every practice / locality are using risk profiling data to case manage patients identified' at risk '

National Averages – Integrated Care Teams
Milestone 3 Achieved 50.73%Milestone 3 Date set 38.98%
Milestone 4 Achieved 11.00%Milestone 4 Date set 55.90%

Devon CCG -Rolling impact top cohort

Other European LTC financial models
• Alzira model Valencia; capitated payments single integrated provider. Significant shift from hospital to community 25% less cost – but
• CREG project Lombardy; multiple providers but common risk adjusted pathways developed reinforced by capitated contractual model ; still in pilot stage
• Netherlands; bundled payments but disease specific orientation, costs increased
• Gesundes Kinzigtal Germany; multiple providers and insurers, bundled capitation payments since 2007 but as part of care change; reduction in morbidity and mortality, morbidity adjusted efficiency gain 16%
Gesundes Kinzigtal Integrated Care: improving population health by a shared health gain approach and a shared savings contract, H. Hildebrandt, C. Hermann, R. Knittel, M. Richter-Reichhelm, A. Siegel, W. Witzenrath
Money for value: the Kinzigital -way to measure the produced value and health gain in a local area
Helmut Hildebrandt, CEO OptiMedis AG and CEO Gesundes Kinzigital GmbH, Germany

Scope of the Year of Care Funding Model

• PbR TIA• PbR same-
day EM• EL Medicine
Acute Community Mental Health Social Care Voluntary/ Independent
Primary care
GP services
• Special Serv• Surgery
• Cancer??• PbR excl drugs
• Crit. Care
Personal healthcare
budget
Specialised Services
Means-tested
services
Within tariff
Residential continuing healthcare
Palliative & end of life
• Alcohol-related care• Yearly cost > £50k
• Reablement• Adult Services
PbR MH clusters
Selection of Services
GP. prescribing

4 key elements
• Identifying and supporting people with LTCs
• Developing costed pathways of need
• Commissioning and contracting of the model
• Systems architecture

What LTCs Should be IncludedThe National Project Team Propose that the LTCs included should be based on the Scottish School of Primary Cares Multimorbidity Research Programme (excluding schizophrenia.)
These LTCs are: Coronary Heart Disease Hypertension Heart Failure Stroke/TIA Diabetes COPD Cancer as LTC (not chemo/radiotherapy) Depression Dementia

Achieving the future state – Primary Drivers
LTC Year of Care
Funding Model
Define the Year of Care Budget and Costing Pathways
Identifying and supporting patients
Systems architecture
Commissioning & Contracting
Define current spend on
LTCs
Agree an integrated needs led assessment framework
Agree categories of support
Define and agree a set of locally owned outcomes
Needs Assessment
Define Year of Care budget according to agreed scope of patient cohort and services
Costings Information
Integration for care co-
ordination
Practical Implementation
Identify population that would benefit from this model
Develop commissioning
mechanism
Developing contracting mechanism
Data Quality
Define typical pathways per category of support
Define methodologies and currencies to establish costs
Cost future pathway
Secure and Maintain agreement to test the implementation of the
Year of Care Funding Model
Identify and agree a model for effective stakeholder collaboration
Agree a high level strategic vision and direction