
The last days of life of people with ID living in residential services Stuart Todd ©University of...
20
The last days of life of people with ID living in residential services Stuart Todd ©University of Glamorgan
-
Upload
shanon-jones -
Category
Documents
-
view
213 -
download
0
Transcript of The last days of life of people with ID living in residential services Stuart Todd ©University of...
The last days of life of people with ID living in residential
services
Stuart Todd
©University of Glamorgan

Death and ID• Death and dying have become more visible and salient
features of ID research.• Changes in policy rhetoric about ‘full and meaningful
life’ have drawn attention to the lower life expectancy for people with ID.
• Research on ‘avoidable deaths’ and ‘disadvantaged living’.
• In historical terms, people with LD are living longer than before.
• However, a longer life will likely imply a ‘longer dying’• How do people with LD spend their lives- all of their
lives?
Dying and ID
• There is an everyday belief that ‘we are equal in the end’
• Yet inequalities are not washed away at the end of life
• Everyday concerns are now more focused on our pre-mortem rather than post-mortem fates
• Dying is the new death

Dying and ID• End of life care is a major emergent policy concern
generally• Seymour (2005) described how older people might
experience ‘disadvantaged dying’ – provision of a good quality of care at the end of life in inequitable
• The prospect of ‘disadvantaged dying’ has emerged an organising theme of ID death related research
• But this is based on several small scale, qualitative studies.
• There is a strong desire for people with ID to die at home but no evidence of the extent to which this is achieved
Research difficulties
• Death is not always mentioned on death certificates
• How would we find a large enough sample• What would we want to know and how would
we measure it?• Welsh pilot, New Zealand follow up, a large
UK ‘last months of life study’
Narrowing the population: Death in ID services
With increasing age, more people live in service based accommodation than with families
These will be services were many people with ID will undergo the important socially managed transitions from living to dying, from dying to death, from being present to being absent but ‘still present’ (remembered)
Increasing attention to QoL in services should be matched with a growing interest in quality of EoLC in those services.

Death in services Recent attention to the way care settings
manage death and dying The attention to ‘dying at home’ has led to a
discussion about care settings as ‘home for an individual’
Death in care settings, mainly for older people, has indicated that care settings may be inadequately resourced to manage dying.
Just over 50% of care home residents die ‘at home’ and that hospital deaths could be avoided for many more.
Basic research questions
• Where do people with ID die?• What factors might influence where people
die? For example, gender, cause of death• To what extent is ‘place of death’ consistent
with individual choice?

Method• Exploratory studies• 5 service providers in Wales providing care to between
85 and 127 people (n= 520)• Data were to be extracted from service records• However, low death rate (3%) and lack of records
relating to deaths of residents meant that data were obtained from service managers for a five year period in Wales
• In New Zealand we had a two year period of study .• Data were obtained on 78 deaths in Wales, and 64 in
New Zealand
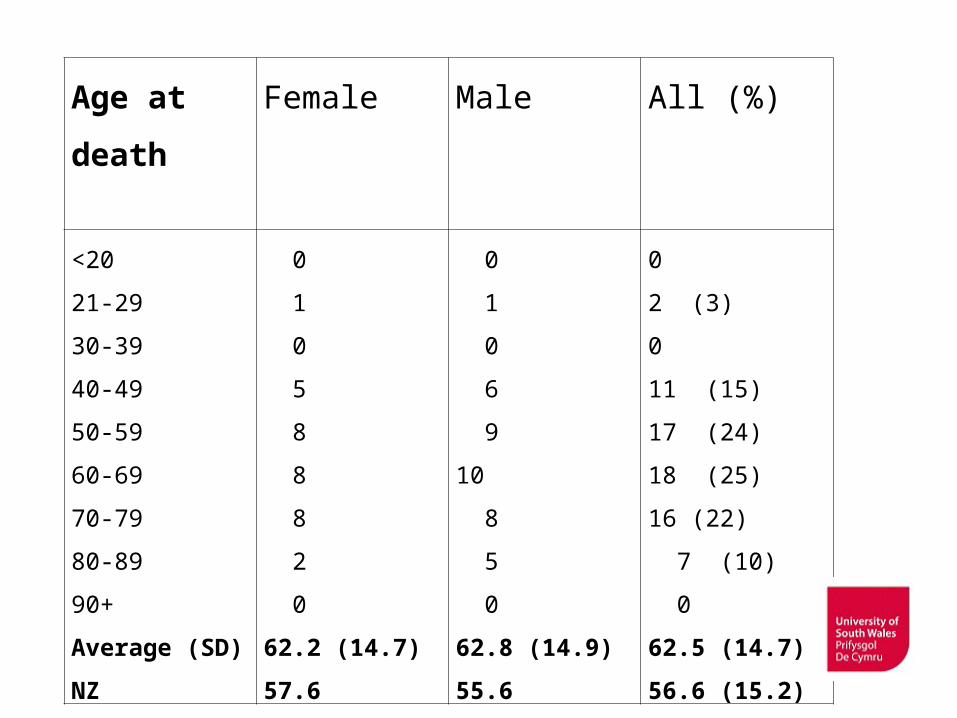
Age at death Female Male All (%)
<20
21-29
30-39
40-49
50-59
60-69
70-79
80-89
90+
Average (SD)
NZ
0
1
0
5
8
8
8
2
0
62.2 (14.7)
57.6
0
1
0
6
9
10
8
5
0
62.8 (14.9)
55.6
0
2 (3)
0
11 (15)
17 (24)
18 (25)
16 (22)
7 (10)
0
62.5 (14.7)
56.6 (15.2)

%
Age at death

Age specific annual death rates (NZ)

Age and death
• There is a similar relationship in ID services as found in the general population
• However, given the age profile of people living in services and the risk of younger dying, services will experience a higher number of younger deaths
• What happens when people with LD age? Where are they? Where and how do they die?

Reported cause of deathWales New Zealand
NZ+
• Respiratory failure 44% 26%• Cancer 27% 16% 26%• Heart disease 8% 11%• Epilepsy 5% 12%• Organ Failure 5% 5%• Stroke 5% -• Others 7% 12%• Dementia - 8% 32%• Missing n= 15

Dying out of home• Average length of stay in residence prior to death
was 8 years and 4 months (SD = 4 years)• However, only 31% of deaths occurred at home.
67% of deaths occurred in hospital.• 60% of cancer deaths were hospital deaths. 25%
of deaths frommore acute illnesses occurred in a hospital.
• Average length of stay in hospital prior to death was 44 days (SD 82 days). Only 22% of hospital deaths occurred within a week of admission.

Awareness of death• Confusing data• Only 4 people who died from cancer (n=20) were
reported to have been told that they were dying• Three of those four died at home – (compared to
5 out of fifteen people who were reported to be not aware)
• In New Zealand, we found that 25% of people reported to be aware that they were dying
• Awareness did not influence place of death

Discussion
• Although findings are tentative they support further study
• Methodological challenges – low levels of death and lack of recorded information will require a larger study of recent deaths in a greater number of service agencies
• Recent funding support to obtain data from services supporting
• Using a nationally used measure – VOICES II – to allow comparison with other populations
©University of Glamorgan

Disadvantaged and unique dying• Data suggest that models for improving EoLC on
other care settings (typically for older people) may not translate well into ID services where deaths are of younger people living in, settings that are more ‘home’ and where issues of ‘awareness’ more challenging.
• Is there a missing intermediate transition?• Are people with ID more likely to experience
‘disadvantaged dying’ – not dying at home or having less of the dying phase at home, little involvement in care decisions? Maybe.
THE LAST DAYS OF LIFE OF PEOPLE WITH LEARNING DISABILITIES LIVING IN SERVICES IN
THE UKLDoL (Services) Study
3 phases• To date recruited about 40 independent
service providers across the UK• Providing support to, at least, 6000 people
with LD• 100-200 deaths?• (i) Describing the population• (ii) Characteristics of the decedent and their
lives and deaths• (iii) Quality of care at the end of life


















