The Lancashire Quality of Life Profile: data and experiences with 58 detained mentally disordered...
13
The Lancashire Quality of Life Profile: data and experiences with 58 detained mentally disordered offenders JULIAN WALKER and GISLI GUDJONSSON Department of Psychology, Institute of Psychiatry, Kings College, De Crespigny Park, Denmark Hill, London SE5 8AF, UK ABSTRACT Objectives This study evaluates the quality of life (QOL) of a group of detained mentally disordered offenders (MDOs) from high- and medium-security institutions using the Lancashire Quality of Life Profile (LQOLP). It was predicted that they would show a poorer QOL on the LQOLP when compared with published data on patients using general psychiatric services. Design A cross-sectional study was undertaken using a clinician administered ques- tionnaire. Method The LQOLP was conducted with 58 detained forensic patients: 19 regional secure unit (RSU) patients, 20 high-security recently admitted patients, and 19 high-security pre-discharge patients. Results Contrary to predictions, it was found that there was no significant differ- ence in overall QOL (measured using the LQOLP) between detained forensic patients and published LQOLP data on psychiatric outpatients in general services. Nor was there a difference observed between these two groups on several major life domains. However, there were several domains in which detained patients had signif- icantly worse QOL ratings; these included: living situation (including living arrange- ments, independence, control and privacy); legal and safety; and health. It was also found that detained patients rated their social relations as significantly better than their non-detained counterparts. Conclusions The LQOLP is a viable instrument to use for evaluating the QOL of detained MDOs. QOL is an important outcome to measure in addition to the usual evaluation of symptoms and patient satisfaction. For detained forensic patients QOL assessment may represent the only way of measuring the totality of their experience in secure environments. QOL data may be used to compare service provision and to help guide the development and improvement of patient care. Future work may involve forensic outpatient and prison populations. Criminal Behaviour and Mental Health, 10, 123–135 2000 © Whurr Publishers Ltd 123
-
Upload
julian-walker -
Category
Documents
-
view
215 -
download
2
Transcript of The Lancashire Quality of Life Profile: data and experiences with 58 detained mentally disordered...
The Lancashire Quality of LifeProfile: data and experiences with58 detained mentally disorderedoffenders
JULIAN WALKER and GISLI GUDJONSSON Department of Psychology,Institute of Psychiatry, Kings College, De Crespigny Park, Denmark Hill,London SE5 8AF, UK
ABSTRACTObjectives This study evaluates the quality of life (QOL) of a group of detainedmentally disordered offenders (MDOs) from high- and medium-security institutionsusing the Lancashire Quality of Life Profile (LQOLP). It was predicted that theywould show a poorer QOL on the LQOLP when compared with published data onpatients using general psychiatric services.Design A cross-sectional study was undertaken using a clinician administered ques-tionnaire.Method The LQOLP was conducted with 58 detained forensic patients: 19 regionalsecure unit (RSU) patients, 20 high-security recently admitted patients, and 19high-security pre-discharge patients.Results Contrary to predictions, it was found that there was no significant differ-ence in overall QOL (measured using the LQOLP) between detained forensicpatients and published LQOLP data on psychiatric outpatients in general services.Nor was there a difference observed between these two groups on several major lifedomains. However, there were several domains in which detained patients had signif-icantly worse QOL ratings; these included: living situation (including living arrange-ments, independence, control and privacy); legal and safety; and health. It was alsofound that detained patients rated their social relations as significantly better thantheir non-detained counterparts.Conclusions The LQOLP is a viable instrument to use for evaluating the QOL ofdetained MDOs. QOL is an important outcome to measure in addition to the usualevaluation of symptoms and patient satisfaction. For detained forensic patients QOLassessment may represent the only way of measuring the totality of their experiencein secure environments. QOL data may be used to compare service provision and tohelp guide the development and improvement of patient care. Future work mayinvolve forensic outpatient and prison populations.
Criminal Behaviour and Mental Health, 10, 123–135 2000 © Whurr Publishers Ltd 123
CBMH 10.2 1st Proof 8/6/00 4:08 pm Page 123
Introduction
For over a decade now, quality of life has been regarded as an important issue inpatient care by governments as well as researchers and clinicians. In the UKGovernment green paper The Health of the Nation (1991), mental health wasidentified as one of five key areas that caused substantial ill health and cost tothe country. In response to this paper, Thornicroft and Strathdee (1991)detailed the mental health targets and indicators for patients, including qualityof life measures under the target ‘Measure user assessments of services’.
Quality of life (QOL) has eluded definitive description, with a single defin-ition being an ideal but not a practical reality. Walker and Rosser (1988)describe QOL as: ‘A concept encompassing a broad range of physical and psy-chological characteristics which describe an individual’s ability to functionand to derive satisfaction from doing so’ (p. 383). This definition of quality oflife implies that it may be regarded as an all-encompassing variable, contin-gent on many subordinate variables to different degrees. As an overall evalua-tion, QOL measurement allows everyone, regardless of illness, intervention orother patient or situational characteristics to be assessed on a common andhighly relevant outcome indicator. Furthermore, the shift away from a purelybiomedical viewpoint (that symptom reduction is the only goal of interven-tion) is reflected in the move by pharmaceutical companies to incorporatequality of life assessment as an important outcome variable in the evaluationof medicines in both physical and mental illness.
A literature search surprisingly revealed an absence of work on QOL indetained forensic psychiatry patients. Coid (1993) noted that many detainedpatients experience poor QOL, but that objective and subjective measuresneeded to be developed. In the related area of adult mental health, Lehmanand Burns (1996) recommend that QOL measures should be used to providebaseline data; for monitoring change; as an outcome measure for the effective-ness of intervention; and for cross-sectional comparisons of groups of patients.
Lehman and Burns (1996) reported that several measures are available forthe assessment of QOL in adults with mental health problems in both clinicaland research environments. Although they particularly recommended theQuality of Life Interview and the Lancashire Quality of Life Profile (LQOLP),they reviewed several other recognized measures.
The LQOLP was developed by Oliver et al. (1996) for use with psychiatricpatients from general services. So far, its use with detained patients has notbeen reported. Given its use with psychiatric patients and the unavailabilityof any reasonably comparable measures, it was chosen as an appropriate mea-sure to use with this new population.
This study was designed to evaluate the QOL of a group of detained men-tally disordered offenders and to provide normative data on the LQOLP forthis group. It was predicted that detained mentally disordered offenders withrestricted liberty would have worse QOL ratings than outpatients using gener-al psychiatric services.
124 Walker, Gudjonsson
CBMH 10.2 1st Proof 8/6/00 4:08 pm Page 124

Method
Sample
A total of 58 forensic psychiatry patients were selected who were detained inEngland and Wales under the Mental Health Act (1983). Patients wereincluded who were classified as having mental illness (n = 35, 60%), psycho-pathic disorder (n = 19, 33%) or both (n = 4, 7%). Patients were not excludedon the basis of ethnic group, which section of the Mental Health Act theywere detained under, or on the basis of offence history. The total number ofparticipants was restricted by the time limits of the study. Thirty-eightpatients from Broadmoor Hospital represented approximately a 7% sample ofthat population at the time the study was completed.
Patients were excluded if their mental state was too unstable for them to beinterviewed, as assessed by their responsible medical officer and the nursingstaff on the day of the interview.
Patients were interviewed in two different settings under conditions of medium (n = 19) and high security (n = 39). Nineteen patients from aregional (medium) secure unit (RSU) were interviewed at various stages inthe admission/discharge process. Within the high-security setting (BroadmoorHospital), patients were further separated into one group who had beenrecently admitted (n = 20) and a second group who were soon to be dis-charged, i.e. completing the last two years of their detention in a special (highsecurity) hospital (n = 19). These three groups of detained mentally disor-dered offenders were chosen to capture a sample which included patients fromdiverse settings within the target population in order to allow limited general-ization from the findings. Recently admitted and pre-discharge patients repre-sent the extreme ends of a special hospital sample, thus including the broadestrange of living conditions in order to maximize the discriminant validity ofthe questionnaire. All secure institutions differ and even two wards within thesame institution may differ significantly from one another.
Design
In this observational study, the three groups of detained patients were com-pared cross-sectionally with one another, and then whole-group comparisonswith existing normative data were made. QOL was measured using theLancashire Quality of Life Profile (LQOLP), which provides several scores.These include global well-being scores (range of values 1–7, a higher scoreindicates better subjective QOL/satisfaction) and scores for nine life domains(range of values 1–7): work; leisure; religion; finance; living situation; legaland safety; family relations; social relations; health. The LQOLP also includestwo subscales for affect balance.
Additional information gathered included: date of birth, age and ethnicgroup; Mental Health Act Section for current detainment; diagnosis; indexoffence.
The Lancashire Quality of Life Profile 125
CBMH 10.2 1st Proof 8/6/00 4:08 pm Page 125

Materials
The LQOLP is a clinician-administered questionnaire consisting of 105 ques-tions including yes/no responses, ratings of subjective well-being on a seven-point scale (from 1 = ‘couldn’t be worse’ to 7 = ‘couldn’t be better’, the mid-point 4=’mixed, equally satisfied and dissatisfied’), Cantril’s ladder (Lehman,1983), free-response questions, and background information. Oliver et al.(1996) reported an average completion time of 36.6 minutes. The question-naire was developed from a sound theoretical basis and includes a collectionof accepted measures from recognized research. It was refined using a system-atic approach, and data are available for a conglomerate group of outpatientsfrom general psychiatric services (total n = 1575, males = 807) who participat-ed in a series of studies conducted by several groups of researchers (Oliver etal., 1996). Because the LQOLP is really a collection of measures covering sev-eral key areas of life that may or may not be related to one another, thedomain results were analysed and reported separately. A few minor wordchanges were made to the original questionnaire following piloting. Thesewere designed to improve the application and understanding for detainedpatients.
Procedure
Suitable patients were seen by the researcher (JW) for 5 minutes in order toexplain to them the purpose and requirements of the study, provide them withan information sheet and give them an opportunity to ask questions and con-sider taking part. Those patients who agreed to take part arranged with theresearcher a mutually convenient time to be interviewed. The emphasisremained on patient empowerment and control, aimed at improving coopera-tion by encouraging patients to make and own the decision to take part. Eachpatient was interviewed in a single session with a break if necessary.Additional background information was collected from case notes and thedata were analysed using a computer-based statistical package (SPSS). T-testsfor independent samples were used to compare published norms (means andstandard deviations) with those obtained in this study.
Results
Table 1 shows the mean, standard deviation and range for age (in completedyears), and time elapsed since admission (in months) for the three groupsstudied.
The results show that the groups were similar in terms of age. However, ananalysis of variance (ANOVA) was run to compare age in completed years bygroup, which suggested that the mean age of the special hospital admissiongroup was significantly lower than the mean ages in the special hospitaladmission and RSU groups (F = 4.675, df = 2, p = 0.013).
126 Walker, Gudjonsson
CBMH 10.2 1st Proof 8/6/00 4:08 pm Page 126
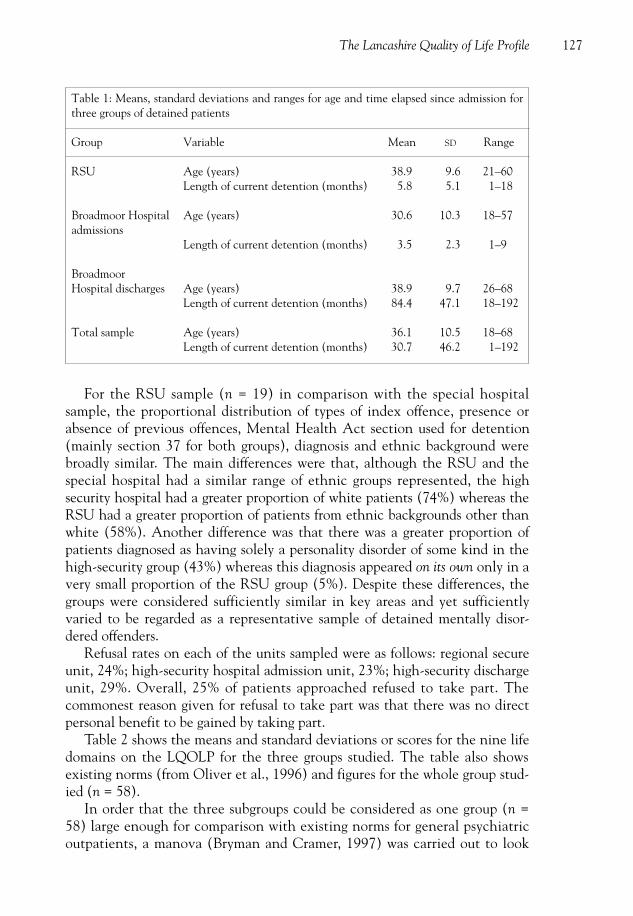
For the RSU sample (n = 19) in comparison with the special hospital sample, the proportional distribution of types of index offence, presence orabsence of previous offences, Mental Health Act section used for detention(mainly section 37 for both groups), diagnosis and ethnic background werebroadly similar. The main differences were that, although the RSU and thespecial hospital had a similar range of ethnic groups represented, the high security hospital had a greater proportion of white patients (74%) whereas theRSU had a greater proportion of patients from ethnic backgrounds other thanwhite (58%). Another difference was that there was a greater proportion ofpatients diagnosed as having solely a personality disorder of some kind in thehigh-security group (43%) whereas this diagnosis appeared on its own only in avery small proportion of the RSU group (5%). Despite these differences, thegroups were considered sufficiently similar in key areas and yet sufficientlyvaried to be regarded as a representative sample of detained mentally disor-dered offenders.
Refusal rates on each of the units sampled were as follows: regional secureunit, 24%; high-security hospital admission unit, 23%; high-security dischargeunit, 29%. Overall, 25% of patients approached refused to take part. Thecommonest reason given for refusal to take part was that there was no directpersonal benefit to be gained by taking part.
Table 2 shows the means and standard deviations or scores for the nine lifedomains on the LQOLP for the three groups studied. The table also showsexisting norms (from Oliver et al., 1996) and figures for the whole group stud-ied (n = 58).
In order that the three subgroups could be considered as one group (n =58) large enough for comparison with existing norms for general psychiatricoutpatients, a manova (Bryman and Cramer, 1997) was carried out to look
The Lancashire Quality of Life Profile 127
Table 1: Means, standard deviations and ranges for age and time elapsed since admission forthree groups of detained patients
Group Variable Mean SD Range
RSU Age (years) 38.9 9.6 21–60Length of current detention (months) 5.8 5.1 1–18
Broadmoor Hospital Age (years) 30.6 10.3 18–57admissions
Length of current detention (months) 3.5 2.3 1–9
BroadmoorHospital discharges Age (years) 38.9 9.7 26–68
Length of current detention (months) 84.4 47.1 18–192
Total sample Age (years) 36.1 10.5 18–68Length of current detention (months) 30.7 46.2 1–192
CBMH 10.2 1st Proof 8/6/00 4:08 pm Page 127
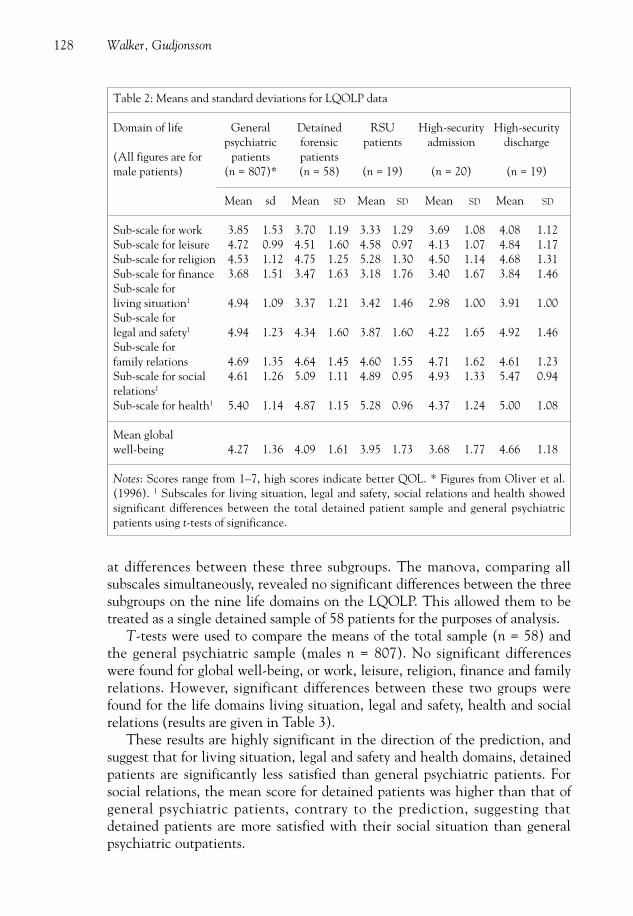
at differences between these three subgroups. The manova, comparing all subscales simultaneously, revealed no significant differences between the threesubgroups on the nine life domains on the LQOLP. This allowed them to betreated as a single detained sample of 58 patients for the purposes of analysis.
T-tests were used to compare the means of the total sample (n = 58) andthe general psychiatric sample (males n = 807). No significant differenceswere found for global well-being, or work, leisure, religion, finance and familyrelations. However, significant differences between these two groups werefound for the life domains living situation, legal and safety, health and socialrelations (results are given in Table 3).
These results are highly significant in the direction of the prediction, andsuggest that for living situation, legal and safety and health domains, detainedpatients are significantly less satisfied than general psychiatric patients. Forsocial relations, the mean score for detained patients was higher than that ofgeneral psychiatric patients, contrary to the prediction, suggesting thatdetained patients are more satisfied with their social situation than generalpsychiatric outpatients.
128 Walker, Gudjonsson
Table 2: Means and standard deviations for LQOLP data
Domain of life General Detained RSU High-security High-security psychiatric forensic patients admission discharge
(All figures are for patients patientsmale patients) (n = 807)* (n = 58) (n = 19) (n = 20) (n = 19)
Mean sd Mean SD Mean SD Mean SD Mean SD
Sub-scale for work 3.85 1.53 3.70 1.19 3.33 1.29 3.69 1.08 4.08 1.12Sub-scale for leisure 4.72 0.99 4.51 1.60 4.58 0.97 4.13 1.07 4.84 1.17Sub-scale for religion 4.53 1.12 4.75 1.25 5.28 1.30 4.50 1.14 4.68 1.31Sub-scale for finance 3.68 1.51 3.47 1.63 3.18 1.76 3.40 1.67 3.84 1.46Sub-scale forliving situation1 4.94 1.09 3.37 1.21 3.42 1.46 2.98 1.00 3.91 1.00Sub-scale forlegal and safety1 4.94 1.23 4.34 1.60 3.87 1.60 4.22 1.65 4.92 1.46Sub-scale forfamily relations 4.69 1.35 4.64 1.45 4.60 1.55 4.71 1.62 4.61 1.23Sub-scale for social 4.61 1.26 5.09 1.11 4.89 0.95 4.93 1.33 5.47 0.94relations1
Sub-scale for health1 5.40 1.14 4.87 1.15 5.28 0.96 4.37 1.24 5.00 1.08
Mean globalwell-being 4.27 1.36 4.09 1.61 3.95 1.73 3.68 1.77 4.66 1.18
Notes: Scores range from 1–7, high scores indicate better QOL. * Figures from Oliver et al.(1996). 1 Subscales for living situation, legal and safety, social relations and health showedsignificant differences between the total detained patient sample and general psychiatricpatients using t-tests of significance.
CBMH 10.2 1st Proof 8/6/00 4:08 pm Page 128

In general terms, detained forensic psychiatry patients showed a similarprofile of satisfaction/dissatisfaction with the various life domains when com-pared with existing data from outpatients using general psychiatric services.Both groups were generally satisfied (i.e. a mean satisfaction score of greaterthan 4) with leisure, religion, living situation, family, social relations, healthand global well-being. Both groups were generally dissatisfied (i.e. a mean sat-isfaction score of less than 4) with work and finance domains. The differencesin these domains were in the degree of satisfaction or dissatisfaction ratherthan in the direction of the mean response, i.e. satisfied versus dissatisfied.The only domain where a disagreement was apparent and significant was inthe living situation domain where outpatients using general psychiatric ser-vices were generally satisfied and detained forensic psychiatry patients weregenerally dissatisfied.
Discussion
In a continually developing health service where evidence-based medicine isconsidered vital to successful treatment, and the monitoring of outcomes is afundamental element of future healthcare, it was timely to examine the quali-ty of life (QOL) in a population which has so far been under-researched inthis area, namely detained mentally disordered offenders. QOL is regarded byboth governmental agencies and healthcare professionals as one of the keyoutcomes to measure in addition to mortality, morbidity, symptoms and satis-faction with services. For detained forensic psychiatry patients QOL assess-ment may represent the only way of measuring the totality of what may be adistressing and disempowering experience in secure environments. Resultingdata may be used to compare service provision and to help guide the develop-ment and improvement of patient care.
The importance of QOL assessment and adequately describing outcomehas been underlined by several authors (Lehman, 1983; Walker and Rosser,1993; Oliver et al., 1996; Orley et al., 1998). However, for detained mentally
The Lancashire Quality of Life Profile 129
Table 3: T-test results (one-tailed) comparing life domain subscale scores of two groups:detained patients (n = 58) and general psychiatric patients (n = 807)
Life domain d.f. t value Significance
Living situation 863 9.605 p = 0.0005Legal and safety 863 2.797 p = 0.005Social relations1 863 3.151 p = 0.005Health 863 3.392 p = 0.0005
Notes: 1Significant but in the opposite direction to the prediction, i.e. for the social relationsdomain detained patients scored higher than general psychiatric patients. Hence the report-ed significance is for a two-tailed t-test.
CBMH 10.2 1st Proof 8/6/00 4:08 pm Page 129

disordered offenders QOL may be considered a somewhat controversial issue.Society in general may be unconcerned with the QOL of those regarded as toodangerous to remain at large in the community. However, detained mentallydisordered offenders suffer on several counts. These include the effects of theirdisorder and subsequent medication where relevant, stigmatization by societyand also the restriction of their freedom. For these reasons they constitute avulnerable group of patients who require high levels of care and containmentrather than custody and punishment.
A severe and chronic mental illness may disrupt any area of life includingwork, with subsequent financial difficulties, and may cause problems withfriends and family resulting in a decreasing social support network, etc. Suchpatients may be unable to pursue a career, home life may lack stability andthere may be frequent hospitalization, interventions on offer may not makesense to the patient and the side-effects of medication can be extremelyunpleasant. The treatment of such individuals needs to go beyond symptomcontrol and compliance with medication, to include the many variables andindividual priorities that impact on the totality of the patient’s well-being andQOL as well as the management of his/her illness.
Patients have certain biological and psychological characteristics that maynot be amenable to change, they may have certain abilities or weaknesses, andthey may or may not have a supportive family or be financially secure.Individuals prioritize these issues differently: for one patient psychologicalsupport may be the most pressing need, another may be concerned aboutfinances and another troubled by medication side-effects. QOL assessmentoffers a systematic way of covering many aspects of life and satisfaction thatmay or may not have meaning or importance for the patient; it also providesan outcome measure appropriate to a range of illnesses and problems, inter-ventions and situations. QOL assessments may be used to track a patient’s pro-gression through services, through their illness or through life. QOL assess-ments can be used to identify problem areas and help to ascertain which areamenable to intervention and which are outside health care services andpatients’ control.
This study was an attempt to use the LQOLP to evaluate the QOL of agroup of detained mentally disordered offenders. QOL instruments are usuallymade up of several measures assessing different aspects of life; the LQOLP isno exception, so the domain results must be analysed and reported separately(Orley et al., 1998). The results showed that there was no significant differ-ence in overall QOL (as measured using the LQOLP) between detainedpatients and outpatients using general psychiatric services. Nor was there adifference observed between these two groups on several major life domains,including work; leisure; religion; finance; and family relations. This was con-trary to the prediction that detained patients would have a worse QOL incomparison with non-detained psychiatric patients. The general agreementbetween the two groups on relative satisfaction with life domains may reflect
130 Walker, Gudjonsson
CBMH 10.2 1st Proof 8/6/00 4:08 pm Page 130

several underlying issues. It could be that the LQOLP is insensitive to the dif-ferences between these groups, except perhaps for the living situation, legaland safety, and health domains, but a much larger sample, perhaps with sub-groups from different types of forensic setting, would be required to concludereliably that the measure is insensitive. Second, it may be that detention isnot a crucial differentiating factor when QOL is the outcome variable,although there were differences between groups within the detained sampleon some life domains. Third, this questionnaire may not be assessing trulymeaningful issues, particularly for detained patients, indicating that it may beinappropriate for this population as it was originally developed for outpatients.Fourth, there may be overriding factors – such as the presence of a psychiatricdiagnosis – which are having a main effect that obscures other subtle differ-ences between the groups. Last, as Orley et al. (1998) suggest, it may be diffi-cult to show differences between the QOL of patients in institutions and thatof patients in the community, because of the nature of QOL. QOL is a subjec-tive evaluation based on perceptions and expectations, and for QOL in aninstitution to be relatively worse, the expectation for community life must berelatively high (and vice versa). If this relative difference does not exist, thensatisfaction with life and subsequent QOL may be largely similar.
Despite non-significant differences in several life domains and a differencecontrary to the prediction in the social relations domain, several significantdifferences, in accordance with the predictions, did emerge. There were threedomains in which detained forensic psychiatry patients had significantly worseQOL ratings than general psychiatric outpatients: legal and safety, living situ-ation, and health. Greater dissatisfaction amongst detained patients in theselife domains may be due to a number of issues.
The observed relative dissatisfaction with the ‘legal and safety’ domain oflife may reflect detained patients’ frustrations with a legal system which theyperceive to be unjust or disempowering. Furthermore, this subsection alsoassesses how safe a person feels generally and in particular on the ward inwhich they are detained. It is possible that an unsettled ward that houses regu-larly violent patients constitutes a potentially unsafe place to live. Rates ofviolence are reported to be higher on inpatient units (Coid, 1996). This mayaccount for detained forensic psychiatry patients feeling less satisfied withtheir safety than psychiatric patients from general services, in accordance withthe predictions. It is also possible that when a ward contains mainly stablepatients with only a few patients who are disturbed, the result is the percep-tion of a less safe environment.
All three groups were generally dissatisfied with the living situation in hos-pital, compared with outpatients using general psychiatric services, who weregenerally satisfied with their living situation. Living situation includes livingarrangements generally; independence and freedom; influence and control;cohabitants in the unit; privacy afforded; and how they felt about the prospectof living in that situation for a long time. Detention in hospital, in particular
The Lancashire Quality of Life Profile 131
CBMH 10.2 1st Proof 8/6/00 4:08 pm Page 131

a high-security hospital, involves a marked difference in living arrangementscompared with community living. It is not surprising that the measure pickedup detained patients’ dissatisfaction in this area. This finding may be regardedas evidence for the discriminant validity of this section of the questionnairefor this population, and is further support for the prediction stated at the out-set that QOL is worse for detained forensic psychiatry patients than outpa-tients using general psychiatric services.
All three detained groups were generally satisfied rather than dissatisfiedwith their physical health. However, the results suggested that psychiatricpatients in the community were significantly more satisfied with their healththan detained forensic psychiatry patients. It is possible that detained patientsare more preoccupied with physical ailments when in hospital and they mayhave less control over their access to pharmacy, general hospital and generalpractice services than patients in the community.
Finally, contrary to predictions, the social relations domain revealed signif-icantly higher ratings by detained forensic patients compared with patientsfrom general psychiatric services. Although both groups were generally satis-fied with their social situation, the observed difference implies that detainedpatients are more satisfied with their social situation and performance thantheir non-forensic counterparts in the community. This finding may reflectthe relative isolation of psychiatric patients in the community, or the fact thatpatients in hospital are almost forced to get along with each other due to theamount of time they spend in each other’s company and the close proximity oftheir existence, or even a basic difference between patients who get into trou-ble (with the law) and those who do not.
The LQOLP was generally well received by patients, with 75% ofpatients in the present study agreeing to take part. Anecdotal evidence frommany of those who participated in the study showed that they found theexperience of being interviewed to be helpful and interesting. Perhaps thequestion of why some patients refused to be interviewed should be consid-ered, as this amounted to a sampling bias. When asked why they had refusedto take part, most patients reported that there was ‘nothing in it’ for them.It is possible that some patients suffering from paranoid illnesses did notwish to be interviewed by anyone, and that these research interviewsappeared to be prying into their lives with no perceived personal benefit,perhaps even at a cost to themselves. Oliver et al. (1996) recommended thatQOL interviews be conducted by a healthcare professional known to thepatient who has already built up some rapport, particularly when interview-ing inpatients. The researcher’s disadvantage in this study was beingunknown to patents on the high-security hospital wards. However, interest-ingly there was no difference between refusal rates on the RSU (where theresearcher had worked for 6 months) and the high-security hospital wards.In voluntary participation studies there will always be patients who refuse to
132 Walker, Gudjonsson
CBMH 10.2 1st Proof 8/6/00 4:08 pm Page 132
take part; given that this study was conducted with detained patients whoare typically difficult to engage, a refusal rate of 25% could be regarded asrespectably low.
Several patients in this study reported spontaneously that the experienceof the interview had been a positive one and had encouraged them to thinkabout aspects of life they had not considered before. Out of 58 patients, 56agreed that they would be happy to be interviewed again in six months’ timeif necessary. This is evidence that the interview procedure amounted to a posi-tive, or at least non-aversive, experience for patients. This finding is similar tofindings amongst patients in general psychiatric services assessed using theLQOLP (Oliver et al., 1996).
A larger sample would greatly improve the research. If data had been col-lected over a longer time period, some patients could also have been re-inter-viewed, or interviewed by another interviewer – for test–retest and inter-raterreliability respectively. Additional comparison groups may have included non-detained psychiatric inpatients, outpatients with forensic as well as psychiatrichistories, prison inmates and further RSU or high-security hospital samplesfrom other units (in particular long-stay wards where patients are in the mid-dle of an admission to special hospital). This will also allow further qualifiedcomments on the discriminant reliability of the LQOLP. The comparison ofpatients in different levels of security and the effects of the relative restric-tions on their liberty between different levels of security is a complex issue.This issue has also been researched by the authors and will be addressed in aforthcoming publication.
Additional data collected from the patients’ notes (psychiatric history,etc.) may have been useful to establish patients’ self-report reliability. Oliveret al. (1996) alluded to the possible effects of social desirability on theLQOLP, and a measure of deception such as the Self and Other DeceptionQuestionnaires (Sackeim and Gur, 1979) may have provided useful additionalinformation on this variable.
Half the high-security hospital patients (n = 39) were classified as havingmental illness under the Mental Health Act 1983 and half as having psycho-pathic disorder. Owing to higher prevalence rates of mental illness comparedwith personality disorders in secure hospitals, it is usual to find a skewed distri-bution as in the RSU sample (n = 19) where 84% of patients were classified ashaving mental illness. Taylor (1997) reported that patients classified as havingmental illness under the Mental Health Act 1983 constitute 75% of the spe-cial hospital (high-security) population in England. However, the high-securi-ty hospital admission data showed a greater proportion of patients classified ashaving psychopathic disorder. The reason for this bias is unclear, but possiblecauses may include: a higher proportion of patients with psychopathic disorderclassification being present on the unit during the period of the study; morepatients with psychopathic disorder classification agreeing to be interviewed;
The Lancashire Quality of Life Profile 133
CBMH 10.2 1st Proof 8/6/00 4:08 pm Page 133

patients with mental illness, who may be more likely to be disturbed onadmission, being excluded from the study from the beginning; or a combina-tion of these or other factors.
To the authors’ knowledge, this was the first time the LQOLP has beenused with detained patients; however, similar research by Joseph Oliver is cur-rently under way at another high-security hospital. Given the small samplesize, conclusions about the statistical performance of the measure may not bedrawn, and collaboration on similar research projects would benefit thisendeavour. This study underlined the importance of several aspects of QOLassessment in detained forensic psychiatry patients and in particular the valueof a broad approach, which is necessary to cover all aspects of life and restric-tions (Oliver et al., 1996). An individualized approach is one important wayto assess QOL reliably because of the multidimensional nature of QOL andthe variables that affect it. Therefore the QOL measures used should incorpo-rate the opportunity for patients’ issues and priorities to be considered. Theimportance of individual meaning and significance can never be underesti-mated, particularly for mentally disordered offenders.
Acknowledgements
This study was only possible with the cooperation of patients from the DenisHill Unit and Broadmoor Special Hospital. The authors are grateful to thestaff at both institutions for their help; in particular Dr E. Moore, Dr J.MacKeith and Dr A. Maden for their helpful comments and facilitation of thestudy. We also wish to thank Dr J. Oliver for his help in providing the measureand supporting information.
References
Bryman A, Cramer D (1997) Quantitative Data Analysis with SPSS for Windows. London:Routledge.
Coid JW (1993) Quality of life for patients detained in hospital. British Journal of Psychiatry 162:611–620.
Coid JW (1996) Dangerous patients with mental illness: increased risks warrant new policies,adequate resources, and appropriate legislation. British Medical Journal 312: 965–969.
Lehman AF (1983) The well-being of chronic mental patients: assessing their quality of life.Archives of General Psychiatry 40: 369–373.
Lehman AF, Burns BJ (1996) Severe mental illness in the community. In Spilker N, ed. Qualityof Life and Pharmacoeconomics in Clinical Trials, 2nd edn. Philadelphia: Lippincott-Raven.
Megargee EI (1995) Assessment research in correctional settings: methodological issues andpractical problems. Psychological Assessment 7(3): 359–366.
Oliver J, Huxley P, Bridges K, Mohammad H (1996) Quality of Life and Mental Health Services.London: Routledge.
Orley J, Saxena S, Herrman H (1998) Quality of life and mental illness. British Journal ofPsychiatry 172: 291–293.
134 Walker, Gudjonsson
CBMH 10.2 1st Proof 8/6/00 4:08 pm Page 134
Sackheim HA, Gur RC (1979) Self deception, other deception and self reported psychopathol-ogy. Journal of Consulting and Clinical Psychology 447: 213–215.
Secretary of State for Health (1991) The Health of the Nation. London: HMSO.Taylor PJ (1997) Damage, disease and danger. Criminal Behaviour and Mental Health 7(1):
19–48.Thornicroft G, Strathdee G (1991) The Health of the Nation: responses. Mental health. British
Medical Journal 303: 410–412.Walker SR, Rosser RM (1988) Quality of Life: Assessment and Application. Lancaster: MTP
Press.Walker SR, Rosser RM (1993) Quality of Life, Key Issues in the 1990s. Dordrecht: Kluwer.
Address correspondence to: Julian Walker, Dept of Psychology, Institute ofPsychiatry, Kings College, De Crespigny Park, Denmark Hill, London SE5 8AF, UK.
The Lancashire Quality of Life Profile 135
CBMH 10.2 1st Proof 8/6/00 4:08 pm Page 135