
The Journal of Bangladesh Orthopaedic Society (JBOS)
95
Published by BANGLADESH ORTHOPAEDIC SOCIETY The Journal of Bangladesh Orthopaedic Society (JBOS)
Transcript of The Journal of Bangladesh Orthopaedic Society (JBOS)

Published by
BANGLADESH ORTHOPAEDIC SOCIETY
The Journal of
Bangladesh Orthopaedic Society (JBOS)
The Journal of
Bangladesh Orthopaedic Society (JBOS)
JOURNAL COMMITTEE 2012 - 2014
Chairman Dr. Ramdew Ram Kairy
Editor : Dr. Md. Golam Sarwar
Associate Editor : Dr. Mohammad Mahfuzur Rahman
Assistant Editor : Dr. Md. Wahidur Rahman
Dr. Md. Jahangir Alam
Members : Dr. Nakul Kumar Datta
Dr. Sajedur Reza Faruquee
Dr. ABM Golam Faruque
Dr. Kazi Shamim Uzzaman
Dr. Mohammad Khurshed Alam


The Journal of Bangladesh Orthopaedic Society is
published twice in a year in the month of January and July.
Articles are received throughout the year in the office of
BOS, NITOR, Dhaka. Acknowledgement receipt may be
taken from the office. Letter of acceptance will be given on
demand after initial scrutiny of the paper by the Journal
committee. If any paper is found to be copied, pirated or
not a genuine works as claimed by the author, will be
discarded automatically without information. Authors are
requested to follow the instructions outlined below:
Preparation of manuscript:
Manuscript should be typed on white A4 size paper with
liberal margins and double spacing and on one side of the
paper only. Pages are to be numbered consecutively
beginning with the title page & not exceeding six (6) pages.
Title page:
The title page should contain the title of the study of
investigation and abstract, mentioning basic procedures,
main findings, principal conclusions and keywords.
Text:
The text of the article should be divided into introduction,
materials & methods, results, discussion and conclusion.
Tables & Illustrations:
Each table or illustration is to be typed on a separate sheet
& numbered in roman numbers & attached at the end of
the text.
Photographs should be clear, glossy and in black & white
preferably. Top of the picture should be indicated by arrow
sign (T). Diagrams & graphs are to be drawn by jet black
ink or printed by laser printer in white sheet.
References:
References are to be numbered consecutively in the order
in which they appear in the text. The form of references
should be as per examples below:
a) References for journal:- References should be written
according to the following sequenceauthors name,
topic, name of the journal with year of publication,
INFORMATION TO CONTRIBUTORS
volume number, page numbers e.g: Ratliff ABC.
Truamatic Separation of the upper femoral epiphysis
in Children. J.B.J.S. (Br.) 1968. 5013:57507-70.
When there are seven authors or more the first three
names will be listed & then the word ‘et. al’ to be
added.
b) References for Complete books:
Sequence for references are - authors name, name of
book, number of edition, Publishers name, Year of
Publication, Page e.g: Adams J.C. Outline of
Orthopaedic. 9th edition Churchill Livingstone
1981. 347.
c) Reference of articles of Magazines
Sequence of reference are - authors name, name of subject,
name of magazine, year & date, Pages e.g: Zachary R.B.
Result of nerve suture M. Seddon H.S. Ed. Perpheral Nerve
injuries. MRC Special Report Series No. 282. London. 1954
3 5c4-88.
Authors may submit the article composed in Microsoft
Word as in the journal format in two columns with pictures
and diagrams. 3 copies of printed article to be submitted at
Bangladesh Orthopaedic Society office along with soft
copy composed in Microsoft Word in a CD or data can be
transferred by pendrive or by e-mail. Original copies &
digital photos in JPEG format to be attached in a separate
folder.
Articles are accepted for Publication on the condition that
they are contributed solely to this journal.
Address of Bangladesh Orthopaedic Society Office:
National Institute of Traumatology & Orthopaedic
Rehabilitation (NITOR)
Sher-e-Bangla Nagar, Dhaka-1207, Bangladesh.
Tele-Fax: +88 - 02 - 9135734
PABX: +88 - 02 - 9144190-4, Ext-280
Mobile: +88 - 01917-665140
web: www.bosbd.org
e-mail: [email protected],
FORWARDING LETTER FOR SUBMISSION TO JBOS
Date.................................................................................
To
The Editor
Dr. .....................................................................................................................
The Journal of Bangladesh Orthopaedic Society (JBOS)
Sub: Submission of manuscript
Dear Sir,
We are submitting our manuscript entitled, ........................................... by, ........................................... 1, ..........................................
2, ......................................... 3, ......................................... 4, .......................................... 5. for publication in your journal. This
article has not been published or submitted for publication elsewhere.
We believe that this article may be of value to medical professionals engaged in Orthopaedic Surgery & related
subjects/................................... We are submitting 3 copies of manuscript along with an electronic version (CD).
We therefore, hope that you would be kind enough to consider our manuscript for publication in your journal as
original / Review article / Case Report.
Thanks and best regards
(2)
Associate Professor,
Department of ......................................... BSMMU/NITOR/
Medical College. .............................
(1)
Professor,
Department of ......................................... BSMMU/NITOR/
Medical College. .............................
(3)
Assistant Professor
Department of ......................................... BSMMU/NITOR/
Medical College. .............................
(4)
Consultant /.........................................../..................................
.....................................................................................................
....................................................................................................

Date : .................................................
To
...........................................................................................
...........................................................................................
...........................................................................................
...........................................................................................
Subject : Acceptance of the Article for publication
Dear Author
Your article Titled “...................................................................................................................................”
has been accepted for publication by the Editorial Board of the The Journal of Bangladesh Orthopaedic
Society (JBOS)
Your article will be published in any of the coming issues.
Thanking you.
...........................................................
Editor
The Journal of Bangladesh Orthopaedic Society (JBOS)
The Journal of
Bangladesh Orthopaedic Society (JBOS)

CONTENTS
EDITORIAL
l How to publish your journal paper 111
Md. Golam Sarwar
ORIGINAL ARTICLES
l Functional outcome of intraarticular fractures of the distal humerus following both column 117
fixation by tension band wire
Kamruzzaman, Ripon Kumar Das, Asit Baran Dam, Swapon Kumar Paul, Zahid Ahmed,
Mohammad Khurshed Alam
l Results of One Stage Surgical Correction of Congenital Vertical Talus in Children 122
Dipankar Nath Talukder, M.A. Hannan, Ishtiaque Ul Fattah, Faruqul Islam, Mohsenuzzaman Khan
l Management of Traumatic Orbital Wall Fracture with Titanium Mesh 126
Kazi Lutfor Rahman, Ismat Ara Hayder, Mohammad Ghulam Rasul,
Anjal Lal Ghosh, Shibasis Basak
l Evaluation of the Outcome of Proximal Femoral Locking Compression Plate for the 132
Treatment of Comminuted Trochanteric and Subtrochanteric Femoral Fractures
MM Hossain, QS Alam, MFH Qasem, MTI Noman, Md. Golam Sarwar, Md. Golam Mostofa
l Result of Arthroscopic Anterior Cruciate Ligament Reconstruction by Semitendinosus & 137
Gracillis Tendon Graft
Md. Harun-Or-Rashid Khan, Mohammad Serajus Saleheen, M. Muniruzzaman,
Md.Aminul Haque Pathan, Md. Abdus Sabur, Md. Iqbal Qavi
l Management of Complex (Schatzker-Type V And VI) Tibial Plateau Fractures 142
by Ilizarov Method
Mir Hamidur Rahman, Gazi Md. Enamul Kabir, Monaim Hossen, Shaymol Deb Nath,
Md. Mofakhkharul Bari
l Management of Diabetic Foot 147
Noor Mohammad, Md. Golam Sarwar, Anjon Lal Ghosh, MA Sabur, Shibasis Basak,
Mollah Eshadul Haq, Shahidul Haq
l Removal of Dead and Infected Bone in Chronic Osteomyelitis is the Prime factor to 151
Control Infection – Early Removal Decreases Morbidity
AHM Rezaul Haque, Debashis Biswas, Shakeel Akter, Takbirul Islam, Debashis Ghosh
l Old Achilles Tendon Injury Reconstruction with Flexor Hallucis Longus Tendon-a Prospective Study 155
Md. Abdul Gani Ahsan, Kazi Md Salim, Ishtiaque-Ul-Fattah, AKM Zahir Uddin
THE JOURNAL OF BANGLADESH ORTHOPAEDIC SOCIETY
VOLUME 28 NUMBER 2 JULY 2013

l Anterolateral Chest Wall Flap as a salvage for composite wound coverage of 159
the elbow, forearm and hand
A.B.M. Golam Faruque, A.H.M. Tanvir Hasan Siddiquee, Uttam Kumar Saha, A K M Zohiruddain,
Md. Mohabbatullah, Md Zahid Ahmed
l Minimally invasive plate osteosynthesis (MIPO) for fracture of distal tibia in 18 patients 163
at BIRDEM Hospital
Anwar Ahmed, Ahmed Suparno Bahar Moni, MKI Quayyum Choudhury, M Golam Sarwar,
Anjan Lal Ghosh
l Functional Outcome of Minimally Invasive Percutaneous Plate Osteosynthesis Using Locking 167
Condylar Plates In Distal Femoral Fractures
Md. Saidul Islam, Md. Golam Mostafa, Shah Jawaher Jahan Kabir, Shahidul Haq
l Posterior Long Segment Transpedicular Screw Fixation for Unstable Thoracolumbar 170
Fractures with Incomplete Spinal Cord Injury
Syed Shahidul Islam, M R Karim, Purnendu, Meraj, Azad, Swapan, Rahman,
Rayhan Hamid, Susmita
l Management of Open Gustilo IIIB Tibia-Fibula Fractures by Soleus Muscle Flap and 174
Locally Made AO External Fixator
Abdullah Al-Mahmood Bilal, Mir Hamidur Rahman, Mohammed Abdus Sobhan,
Milon Krishna Sarker, Md.Wahidur Rahman, M Monaim Hossen
l Evaluation of Outcome of Open Intramedullary Interlocking Nailing in 181
Tibial Shaft Fracture in Adults
Mohammed Abdus Sobhan, Mir Hamidur Rahman, Abdullah Al-Mahmood Bilal,
Milon Krishna Sarker, Md.Wahidur Rahman, M Monaim Hossen
Review Article
l Upper Cervical Spinal Injuries : A Review 187
Ghosh JC, Mollah Ershadul Haq, Dulal Datta, Monaim Hossen, Noor Mhammad, Lokman Hossain
Case Report
l Health Seeking Behaviour of Road Traffic Accident Victims: A Qualitative Study among the Slum 192
Dwelling Disabled People of Dhaka City
Mohammad Mahbub Alam Talukder, Md. Ali Imam, Nasrin Akter, Nasir Uddin Sheikh
Book Review 197
Iqbal Qavi

Editorial
This paper focuses on preparing articles for publication in
journals. You must have a focus and a vision. The key to
successfully publishing an article is to get a vision-a reason
and purpose for writing. Once you have a vision, write
down and keep it in constant view to remind you of your
mission. Four areas of article preparation are to be covered:
a. When selecting a journal for your paper, what you
should be thinking about;
b. You need to follow in journal style guides;
c. Simple ways when writing paper for better clarity;
d. What happens to your paper once you send it to the
journal and the various types of responses you can
expect to receive?
1. SELECTING A JOURNAL
Ideally , you should be thinking about the journal you
want to submit your paper to before you even write the
paper, that is, when you’re still conducting the research.
It makes sense to select a journal before you commence
writing up the results of your research, given that you can
then familiarize with the journal’s format before you start
to write, these ensuring that your paper complies with
their required format. The journal’s style guide, which is
covered in more detail later, will also help you to focus
your paper and keep it within manageable word limits.
But how do you select a journal for you’re yet to be written
article?
There are thousands of academic journals out there of
varying levels of quality and reach, so below are a few
questions you can ask yourself to limit your search.
i . Will my paper appeal to a domestic or international readers?
ii. What sort of paper am I going to write ?
Main stay is to write clearly. There is no substitute for a
good idea for excellent research or for good, clean, clear
writing. Will it be a qualitative or quantitative study, a
literature review, a brief report, a meta-analysis or a
discussion of a current issue? In other words, what sort
How to publish your journal paper
Md. Golam Sarwar
Associate Professor of Orthopaedic Surgery, DMCH, Dhaka
of focus/ scope am I looking for in a journal? Journal
scopes are usually given on the imprint page of a journal.
You need to align your journal before you submit it or you
will be wasting your time!
An example is:
The journal of Bangladesh Orthopaedic Society is a fully
referred journal publishing original scholarly works in
orthopaedic surgery and development of our professional
discussion papers referring scientific, theoretical or
philosophical base.
The primary criteria for acceptance are excellence and
clarity. Papers are published in BJOS under the following
categories: research papers, scholarly articles, clinical
reports, international reviews and book reviews.
iii. Send your manuscript to the right journal.
Does my paper/research relate only to my discipline or
can I look at journal outside my discipline i.e. Who am I
trying to communicate with/who is my reader?
Knowing your audience is an important element not only
of selecting your journal, but of writing you paper. Also it
will help you to choose the style of your paper and
language.
For example, if you are going to write an article on about
orthopaedics, which you want as many orthopaedicians
as possible to read. A good way to reach these to get your
paper published in the JBOS; 6 monthly journals.
iv. What database is the journal indexed and abstracted in
i. e. how easily the other academics are able to access my
article through searches?
v. What is the journal impact factor?
The impact factor is a calculation based on the number
of times a piece of research is cited in the research of
other academics. Basically the impact factor gives you
an idea of the journal’s prestige or academic weight (found
in ISI (Institute for Scientific Information-Ref 016.5 Ins/
Sjc).
VOL. 29, NO. 2, JULY 2014 111

vi. Is the journal peer-reviewed?
Most academics will only be interested in publishing in
peer-reviewed academic journals. A simple way to check
is to go to the first database. (www.insinet.com/isi/journals)
or non-peer-reviewed in www.ulrichsweb.com
vii. Am I realistic?
Once you know the type of journal you want to target, it’s
a matter of talking to your colleagues to utilize your
knowledge of journals doing website searches of journal
lists, or browsing the shelves of the library.
It is important that you build up a knowledge-based and a
feel for the journals in your area of research. This obviously
involves not only reading the scope section of journals,
but also reading papers from the journals. Academics who
plan to publish should regularly read several journals in
their own field and at least two from related fields.
When you do read those journals, you should be looking
at the content and style of each journal. Therefore, you
will be able to determine which subjects are currently of
interest and which research topics are generating
discussion in that particular journal. Looking at writing
style will help you to familiarize yourself with the technical
language used in the journal and the level of details given
in the paper.
Finally reading other academics writing will also help you
to improve your own writing.
2. STYLING TO JOURNAL GUIDELINES
A journal guideline gives all the information you need
about writing and presenting a paper.
While editors and reviewers are most interested in the
substance of a paper, they can become distracted if you
have not followed the journals’ style requirements. Your
paper might even be rejected straight out if certain basic
requirements are not followed. So, basically, you put
yourself at a disadvantage if you do not follow journal
guidelines when writing your paper.
Journal guidelines really just provide simple points about
how to write your paper. An easy way to attach journal
guidelines is, before writing your paper, to go through the
selected journal’s guidelines and jot down the main
requirement you need to follow when writing your article.
These will include the followings:
- Maximum length of the paper
- Referencing style to follow
- Type and length of abstract to be included (that is
structured or unstructured)
- Whether keywords should be provided
- How tables and graphs should be styled and presented
- Spelling (that is US, British or Australian)
- System of units to use (e.g. SI units)
- Format to use (e.g. typeface, font size)
- Layout of the text (e.g. double spacing)
- The process of review that will take place
- Author details (e.g. address, phone and fax numbers,
email)
- How many copies of ms should be submitted and
where to send the paper
Given that most these requirements are fairly
straightforward excepts- word length, referencing and
abstracts.
I. WORD LENGTH
There are 3 reasons-
The first relates to journal budgets. Basically, it is very
expensive to publish a journal. Journal editors will set the
page extents for an issue of journal long before that issue
is printed. Because a couple of extra pages in any one
issue can totally blow out the journal budget.
The Second reason, in every paper you write, you should
be aiming to write tightly and to get rid of excess words. A
classic writing text will be; “Aim for brevity in your writing.
Omit needless words. A sentence should contain no
unnecessary words, a paragraph no unnecessary
sentences”.
The third, and perhaps most important, nobody will want
to read your paper, not the editor; not the reviewer and
finally not the reader. Therefore, a quick tip on sticking to
word limits is to do a plan so you do not go over the limit.
II REFERENCING
There are two types of referencing to which you will be
asked to adhere: The Vancouver system or the Harvard
system. For more details- Publication manual of the
American Psychological Association (5th edition, 2001) or
Australian Government Publishing Services style manual
for Authors, Editors and Printers (6th edition, 2002)
Below I will cover a couple of tricky aspects of referencing:-
The first is what to do about unpublished material that
have been sent to a journal but not yet accepted, should
not be included in the reference list. But you can include
as follows
Roy and Ram found similar discrepancies in a study of 20
dementia sufferers (R. Ram, unpublished data, 2001).
112 Editorial
The Journal of Bangladesh Orthopaedic Society

Another problematic aspect of referencing is how to
reference information downloaded from internet. For an
internet article based on a print source you can reference
the online article in the same way that you would the print
version, except that you would add “Electronic version”
in brackets after the article title, as in the followings:
e.g. Parker, G., & Roy, K. 2001. Adolescent Depression: A
review (Electronic version), Australian and New Zealand
journal of Psychiatry, 35: 572-580.
For an article in an internet- only journal, you should style
the reference in the same way as the previous example,
except that instead of using volume numbers, the online
journal might use a different numbering system.
It is important that you pay attention to the referencing
style of the journal when writing or formatting a paper.
You should Endeavour to copy it as closely as possible
and include all of the necessary information. Missing
information will result in delays once your paper has been
accepted for publication, as will use of the incorrect system
of referencing.
III. ABSTRACTS
Given that the abstract or summary may be all that most
people will ever read of a paper, it’s surprising that so little
attention is paid by authors to writing the abstract. Writing
a clear concise abstract that accurately presents the
essence of your paper will take time and thought.
What should an abstract include? It should include the
purpose of the study; a brief description of the methods
used; the key results; the main conclusion; and possibly
some recommendations, depending on the journal
requirements. A good way to learn to write an effective
abstract is to read some sample abstracts from the journal
you are targeting.
3 IMPROVING THE CLARITY OF YOUR PAPER-
I. Avoid wordiness in writing
Your aim should be to keep sentences short and to
the point. How do you keep sentences short? By
being concise and getting rid of excess words. Take
this example of unnecessary and redundant language:-
e.g. “We shout to explore …”- May right- “We
explored…”
Do not spent many words going off the tract. You do
not have to say everything about your chosen topic,
but should be confining yourself to what is relevant
to your reader.
II. Keep Jargon to a minimum
Any article or publication in a journal should be
written so that it is understandable to an intelligent
reader who is not a specialist in your particular field.
Try not to use too much Jargon, and try to write in
plain English. Your aim in writing is to communicate
your message of ideas and in accessible language
will mean that your ideas are disseminated to a wider
range of people.
III. Make sure pronouns are no ambiguous
You know, a pronoun is a word that takes the place of
a noun (This, That, It, His etc). An antecedent is the
word that the pronoun refers back to.
e.g. The decision is significant because it reflects the
splits developing within the groups.
“It” = the pronoun
“The Decision” = the antecedent
However pronoun is very obvious. Papers can
become very confusing if the antecedent for each
pronoun is not obvious.
IV. Use the definite/indefinite article correctly
The indefinite article-‘a’- is used to introduce someone
or something for the first time.
e.g. A study was conducted by Brierly and Jones…
This implies that it’s the first time that you have
mentioned that study in your paper
The definite article-‘the’- is used to refer to one or
more people or things that have already been
mentioned or that are assumed to be common
knowledge.
e.g. the study conducted by Sarwar and Gani…
This implies that you have already mentioned the
study earlier in your paper
It can be very confusing to readers if “a” and “the”
are incorrectly used !
V. Don.’t use anthropomorphism
Anthropomorphism is a literary device used to
attribute human characteristics to non-human things.
- the study said..
- environmental designs will need to consider..
Obviously, a study cannot speak and an
environmental design cannot consider..so these types
of statements need to be rephrased:
-It was apparent from the study…
-Researchers planning environmental designs will
need to consider…
How to publish your journal paper 113
VOL. 29, NO. 2, JULY 2014

VI. Avoid shortcuts in writing
By avoiding shortcuts in writing,
e.g. Making a copy..
This is a lazy approach to writing, and can result in
ambiguities. A better approach is;
Making a copy involves making an exact replica of
the article…
VII. Be consistent
When writing your paper, try to stick to the one term
to describe groups of people; that is, don’t jump from
“subject” to “respondents” to “patients” to “clients”
as this is confusing to the reader.
VIII. Use the appropriate tense
Use the past tense (e.g. “Jones showed”) or the
present perfect tense (“researchers have shown”) for
the literature review and for describing your
procedure if the discussion is of past event-but stay
within your chosen tense.
Again you may use past tense (e.g. depression
decreased significantly) to describe the results of your
study.
Use the present tense (e.g. “the results indicate”) in
the discussion to discuss your results and to detail
your conclusion, using present tense in the
discussion section allows readers to join in your
deliberation of the results.
Do not write about the study as if you are just about
to conduct it (do not use the future tense). It’s
assumed that you are writing your paper after the
study has taken place and that you are describing
things that occurred in the past not that will occur in
the future.
e.g. “our sample will consist of 25 women…”= incorrect
“Our sample consisted of 25 women…”= correct
IX. Avoid generalization
Generalizations are often used in paper based on
qualitative studies
e.g. the respondents said they were distressed…
This leaves you asking the question, “Did they all
say this or did only some say this?”Statements like
the above should be qualified so that the reader
knows whether in fact all respondents made a certain
comment or only some.
X. Be aware of time factors
You need to be careful when using terms like “recent/
recently” and “over the past decade” as these terms
date.
e.g. Recent research has indicated…. (Smith, 1995)
Obviously, 1995 is not “recent”, so the sentence would
need to be amended to:-
e.g. Research has indicated….(Smith, 1995)
Avoid finishing your paper with a long , clinched,
jumbled or sentimental last line-leaders are left with a
better impression if you finish with a short clear
sentence.
Following the above tips when writing a paper will
help you to ensure that your paper is clear and that
readers will be able to read through your paper
without having to stop to work out what you are
trying to say. Or same reviewers may recommend
submitting your paper to a different journal. “They
are not saying the article is hopeless, instead of they
are just saying that it may not be right for that journal”.
If the research needs more studies and you have a
sincere interest in that area, you can resubmit it as a
new paper, noting the differences in the cover letter.
Also keep in mind that quite often, unfortunately, a
journal will reject an article because its’ navel or new
for its time. But if you feel that it is valid and good,
then by all means, send it off to another journal.
Don’t put off the revisions
If you are invited to revise, “do it, do it fast and don’t
procrastinate”.
Ultimately, it is good to keep in mind that the road to
being published is not a langely one. All authors get
lots of rejections-including senior authors. The
challenge is to preserve and improve one’s paper over
time.
XI. Don’t panic
The overwhelming majority of initial journal
manuscripts are rejected at first. Remember to get a
lot of publications , you also will need to get lots of
rejections.
XII. Beef up your cover letter
Many authors do not realize the usefulness of cover
letter; the letter can contain the author’s rationale for
choosing the editor’s journal-especially if it is not
immediately apparent.
114 Editorial
The Journal of Bangladesh Orthopaedic Society

3. WHAT TO EXPECT WHEN YOU SEND YOUR PAPER
TO A JOURNAL
There are four possible responses that you could receive
from a journal’s editor after your paper has been through
that journal’s review process:-
i. The paper is accepted as it is (very rare which almost
nobody gets)
ii. The paper is accepted on the proviso that minor
decisions be made-20%. Just make some minor
changes.
iii. The paper is rejected as it is because it needs some
major revisions-
The most usual response is about 60%, the’re still
interested in you ! This means, the paper might be accepted.
If this happens, do not be discouraged. Address the
reviewer’s comments and send a detailed letter back to the
editor.
iv. The paper is rejected outright-about 20% of papers.
Or some reviewers may recommend submitting your paper
to a different journal. “they are not saying the article is
hopeless, instead of they are just saying that it may not be
right for that journal.”
If this is happened, take the reviewer’s advice and submit
your revised paper to another journal. And, again, if this
happens, do not be discouraged as it may well be that you
have aimed to high in sending your paper to a particular
journal. Remember-Though not as good as revise and
resubmit “they still want the paper!”
REFERENCES:
1. American Psychological association, Publication Manual
of the American Psychological Association, 5th edn,
Washington, DC: American Psychological Association,
2001
2. James R & durston B, Instuctions to Contributors: Writing
for Publication, Health Promotion Journal of Australia,
accssed 20/11/01, http://vhpax.vichealth. vic.gov.au/hpja/
writing.html.
3. McInerney DM, Publishing Your Psychology Research:
A Guide to Writing for Journals in Psychology and Related
Fields, Crows Nest: Allen & Unwin, 2001
4. Saeck L & Lowe JB, Instuctions to Contributors: Writing
to be Read-Publishing the Results of Health Promotion
Activities, Health Promotion Journal of Australia,
accessed20/11/01, http://vhpax.vidhealth. vic.gov.au/hpja/
writing02.html.
5. Strunk W & White EB, The Elements of style, New York:
Macmillan Publishing Co,1972.
6. Van Teijlingen E & Hundley V, Getting Your Paper to the
Right Journal: A Case Study of an Academic Paper. Journal
of Advanced Nursing,37(6),506-511.
7. Kathryn Hewlett ,How to publish Jour Journal
Paper.sept2002, vol33, No. 8 Print version: Page 50 http:/
/www.apa.org/monitor/sep02/publish.aspx
8. Rowena Murray, Top Tips for How To start Writing
That paper, Friday 6 Sept,2013 15.30 BST, 3rd edition,
How to publish your journal paper 115
VOL. 29, NO. 2, JULY 2014

Original Article
Functional outcome of intraarticular
fractures of the distal humerus
following both column fixation by
tension band wire
Kamruzzaman1, Ripon Kumar Das2, Asit Baran Dam3, Swapon Kumar Paul4, Zahid Ahmed5,
Mohammad Khurshed Alam6
ABSTRACT
The aim of this study was to evaluate the functional outcome following internal fixation of intraarticular fractures
of the distal humerus with a minimum follow-up of one year. A retrospective evaluation with prospective clinical
review was carried out at Trauma Center, Shyamoli, Dhaka during January 2012 and june 2013.Twenty one
consecutive patients with fractures of the distal humerus were treated over a 24-month period. Their mean age
was 39 years (range, 18-68). Male-Female ratio was 3.2:1. Road traffic accident (RTA) was the most common
cause of injury in this study (57.7%) and next was fall on slippery ground (26.9%) and fall from height (15.7%).Two
patients were not available for final clinical review. Analysis of the results were based on the medical records,
pre-operative and postoperative radiographs of all 21 patients and clinical review of 19 patients at a mean follow-
up of 18 months (range,12-30 months). Twenty-0ne fractures were operated by both column fixation with tension
band wire technique. Radiographic evaluation of the quality of reduction was carried out using a grading system.
Clinical outcome was assessed using the Broberg and Morrey functional rating index. thirteen patients (70%) had
an excellent or good outcome, five patients (25%) a fair outcome and one patient (5%) had a poor result. The mean
arc of flexion was 112° (range, 85 to 122). Mean pronation was 75° (range, 60-82) and supination was 76° (range,
60-80). Fifteen patients (75%) were able to return to their pre-injury level of occupation and activity. Seventeen
patients (85%) were satisfied with the final outcome. We conclude that internal fixation of intraarticular fractures
of the distal humerus by double tension band wiring is an effective procedure with an excellent or good functional
outcome in most patient age groups. Patients have a high level of satisfaction and the majority return to their
previous level of activity.
1. Associate Professor, Bangladesh Medical College, Dhaka.
2. Junior Consultant, NITOR, Dhaka.
3. Assistant Professor, NITOR, Dhaka.
4. Assistant Professor, NITOR, Dhaka.
5. Junior Consultant, NITOR, Dhaka
6. Assistant Professor, Department of Orthopaedic Surgery, DMCH, Dhaka
Correspondence: Dr. Kamruzzaman, Associate Professor, Bangladesh Medical College, Dhaka.
INTRODUCTION
Complex intraarticular distal humerus fractures are a
considerable challenge to even the most experienced
surgeon. Previous treatment methods of closed reduction
with immobilisation, traction and limited internal fixation
have lead to significant functional impairment with loss of
range of movement4,12,17.
The functional outcome of distal humerus fractures is
related to the ability to restore the normal anatomy and to
allow early movement. Various methods of limited internal
fixation have been described using Kirchner wires, screw
fixation and single plates2,3,10. Fractures of the distal
humerus are relatively rare and large case series are rarely
reported. Comparison between the various studies is
difficult owing to the variation in fracture classification,
operative techniques and outcome measures used15.
The aim of our study was to evaluate the functional
outcome of intraarticular distal humerus fractures treated
by both column fixation with tension band wiring with a
minimum of one year follow-up.
VOL. 29, NO. 2, JULY 2014 117

PATIENTS AND METHODS
Twenty-one consecutive patients with 21 fractures of the
distal humerus seen in Tauma Center over a 30-month
period underwent internal fixation of their fracture. Same
consultant trauma surgeon with his team performed
surgery . The choice of fixation was the double column
fixation by tension band wire based on the pattern of the
fracture and presence of associated injuries as seen on
standard antero-posterior and lateral radiographs of the
elbow. All the fractures were displaced intraarticular
fractures.
Surgical Technique:
The operation is carried out under general anaesthesia in
lateral decubitus.Torniquet is applied for all patients
undergoing operation. Esmarch tourniquet is applied at
the upper arm after exsanguination of blood from hand
and forearm. A midline posterior incision was made over
the distal humerus, curving around the tip of the olecranon.
The ulnar nerve was identified and protected. An olecranon
osteotomy was used for adequate exposure of the joint
surface . The osteotomy was started with an oscillating
saw but completed using a fine osteotome through the
subchondral bone.
Reduction And Fixation of The Condyles: Fragments of
the condyle are reduced and held together firmly by towel
clip or reduction clump. 1.5mm Kirschner wire is used for
reduction and temporary fixation. Parallel to the wire,
2.5mm hole is drilled from radial to ulnar fragment or ulnar
to radial side (depending on the fracture fragment) and a
4.5 mm partial threaded cancellous screw is introduced.
Reduction And Fixation Of Reassembled Condyle To The
Diaphysis: After the articular fragments have been
anatomically reduced to form an articular block, proper
reassembly of the medial and lateral columns are resumed
and these are fixed with the diaphysis of the humerus by
bilateral cross tension band wire.
Postoperative x-ray
Table I
AO classification of intra-articular fractures of the
distal humerus
Clinical Evaluation No Follow Up
C1 6 1
C2 9 1
C3 4 O
Total 19 2
There were 2O closed fractures and one open fractures.
The mean age for the surgery group was 39 years (range
18 to 68 years). There were 16 male patients and 5 female
patients. The results were analysed using clinical and
radiographic evaluation at a mean follow-up of 18 months.
The quality of reduction was graded (A to C), based on
the postoperative radiographs by the senior author. Grade
A was an anatomical reduction, grade B a step or gap of
the articular surface of less than 2 mm and grade C
involved a step or gap of more than 2 mm. The quality of
reduction was based on the immediate postoperative plain
radiographs and operative findings. Data from the clinical
records, clinical review and examination were summarised
in a weighted grading scale (Broberg and Morrey
functional rating index) (8) as shown in table II. The grading
scale was weighted as follows : normal motion, 40 points ;
no pain, 35 points ; normal strength, 20 points ; and normal
stability, 5 points.
Olecranon osteotomy was repaired using partial threaded
cancellous screw. The stability and range of motion was
assessed per operatively. Wound is closed in layers,
keeping a drain tube. A long arm posterior slab is fixed
with the elbow at right angle.Drain is removed after 48
hours postoperatively.Stiches are removed after 14
days.Triangular sling or elbow bag is applied to each and
every patient after removal of back slab at 2 weeks. Patient
is advised to continue this sling for further 2 weeks and to
allow active limited exercise of the elbow within the sling.
After removal of the sling, range of motion was gradually
increased depending on the documented stability and
postoperative range of motion achieved.
118 Kamruzzaman, Ripon Kumar Das , Asit Baran Dam, Swapon Kumar Paul, Zahid Ahmed, Mohammad Khurshed Alam
The Journal of Bangladesh Orthopaedic Society

RESULTS:
Two patients were lost to follow up. The clinical records
and radiographs were available for all 21 patients. 19
patients were assessed clinically and radiographically at a
mean of 18 months postoperative (range 12 to 30 months).
thirteen out of 19 patients (68.4%) had an excellent or a
good functional result. Five patients (26.3%) had a fair
functional outcome and one patient (5.3%) had a poor
result.
Table II
Broberg and Morrey functional rating index
Variable Points value
Motion
Degree of flexion (0.2 3 arc) 27
Degree of pronation (0.1 3 arc) 6
Degree of supination (0.1 3 arc) 7
Strength
Normal 20
Mild loss (appreciated but not limiting, 13
80% of opposite side)
Moderate loss (limits some activity, 5
50% of opposite side)
Severe loss (limits everyday tasks, disabling) 0
Stability
Normal 5
Mild loss (perceived by patient, no limitation) 4
Moderate loss (limits some activity) 2
Severe loss (limits everyday tasks) 0
Pain
None 35
Mild (with activity, no medication) 28
Moderate (with or after activity) 15
Severe (at rest, constant medication, disabling) 0
Excellent 95-100 points
Good 80-94 points
Fair 0-59 points 60-
Poor 79 points
The mean arc of movement was 112° (range 85- 122°). The
mean pronation was 75° (range, 60-82°) and supination
was 76° (range, 60-80°). The mean functional score for the
group was 85 (range, 55 to 100).
The quality of reduction based on the immediate
postoperative plain radiographs and operative findings
was grade A (15 cases), grade B (5 cases) and grade C (1
case). On the functional rating index, 11 out of 15 fractures
with an anatomical reduction (grade A) had an excellent
outcome ; three had a good outcome and one a fair
outcome. Out of five patients with a grade B reduction,
two had a good outcome and three had a fair functional
result. The one patient with loss of reduction (grade C)
had a poor result. Fourteen patients (73.6%) were able to
return to their preinjury level of occupation and activity.
Seventeen patients (89.4%) were satisfied with the final
outcome.
Table III
Complications
Number Percentage
Metalwork Prominence 5 26
Heterotopic Ossification 2 11
Wound Infection 2 11
Suture Irritation 1 5
Ulnar Nerve Palsy 1 5
Osteotomy non-union 0 0
The complications are shown in table III. Two patients
developed an early superficial wound infection. There was
one case of ulnar nerve neurapraxia, which resolved within
6 months. There was evidence of moderate osteoarthrosis
in one elbow. There were no case of olecranon osteotomy
nonunion.
DISCUSSION:
Complex intraarticular fractures of the distal humerus are
still a considerable challenge to the experienced surgeon.
Prior to the 1970’s great emphasis was laid on
conservative treatment of these fractures either by the
use of plaster or by traction on the olecranon, which led
to considerable stiffness and poor functional results12,17.
However with advances in implants and surgical
techniques, many surgeons have moved towards surgical
reconstruction of these complex fractures2,12. Many
methods of internal fixation have been described. The
results of the various treatment methods are difficult to
compare owing to the variability of the outcome scoring
systems used.
Total joint arthroplasty as a primary modality of treatment
is also an option in the elderly when the extent of
Functional outcome of intraarticular fractures of the distal humerus following both column fixation by tension band wire 119
VOL. 29, NO. 2, JULY 2014

fragmentation is beyond surgical reconstruction, when
the quality of bone stock is poor due to osteoporosis or
when antecedent arthritis (usually rheumatoid) is present
in the joint5. In our series no cases required arthroplasty.
The majority of patients had mild or no pain (85%), there
were no cases of severe pain. There were good forearm
rotational movements in these patients, the main restriction
was in flexion to extension. The mean arc of movement
was 112°, which is consistent with other studies2,3,9. There
was no correlation between age and the final functional
outcome achieved. Patients with open fractures had a lower
mean functional score, which is similar to previous
studies15.
Fourteen patients (70%) had an excellent or good
functional outcome after these complex fractures. This is
comparable with other series in the literature although
there is considerable variation depending on the outcome
scoring system used (9, 11, 13, 14, 20). There was one poor
result in a 68 year-old lady who sustained a grade 2 open
injury. She had an arc of flexion of 85° with considerable
weakness and moderate pain at latest follow-up. She was
unable to achieve her pre-injury level of activity. Overall,
five patients (25%) were unable to return to their previous
level of activity. Seventeen patients (85%) were satisfied
with their final outcome.
Olecranon osteotomy for exposure and fixation of the
distal humeral fracture was initially popularized by
Cassebaum3. Henley et al reported a 57% incidence of
complications with the transverse osteotomy, including
symptomatic prominence of the K-wire, broken tension
band wire, delayed union and non-union8. In 1982 Heim et
al described the chevron osteotomy with the point of the
“V” turned distally. In addition to providing mechanical
stability to rotational stresses the larger area of contact
between the ends of the osteotomy enhances bony
union7. We used the technique of transverse osteotomy
in our study ; we had five cases of metalwork prominence
but no cases of non-union.
Wang et al recommend routine anterior subcutaneous
transposition of the ulnar nerve using a posterior approach
(20). We have not found it necessary to perform a routine
anterior transposition and have performed an adequate
mobilisation as described by Jupiter et al11. Sodergard et
al reported a 12.5% neural complication following the
surgical fixation, 3.1% of the patients had a permanent
dysfunction of the ulnar nerve in a series of 96 adult
patients at an average follow-up of 6 years19. There was
one case of ulnar nerve palsy in our series, which recovered
by 6 months. Heterotopic ossification was seen in two
cases although much higher rates have been reported in
similar series. We believe that the olecranon osteotomy
minimizes triceps muscle trauma and combined with early
mobilisation reduces this complication.
Fratures of the distal humerus are relatively rare and large
case series are rarely reported. Comparison between the
various studies is difficult due the variation in fracture
classification, operative techniques and outcome measures
used. There is considerable variation depending on the
outcome measures used.
Internal fixation of intra-articular distal humerus fractures
using double column fixation by tension band wire is an
effective procedure with an excellent or good functional
outcome in most patient age groups. There is a long-term
reduction in grip strength in the injured arm, however
patients have a high level of satisfaction and the majority
return to their previous level of activity.
REFERENCES
1. Broberg MA, Morrey BF. Results of delayed excision of
the radial head after fracture. J Bone Joint Surgery 1986 ;
68-A : 669-674.
2. Burri C, Henkemeyer H, Spier W. Results of operative
treatment of intraarticular fractures of the distal humerus.
Acta Orthop Belg 1975 ; 41 : 227-234.
3. Cassebaum WH. Open reduction of T- and Y-fractures of
the lower end of the humerus. J Trauma 1969 ; 9 : 915-
925.
4. Charnley J. The Closed Treatment of Common Fractures,
3rd ed, 1961. Williams & Wilkins, Baltimore, pp 70-71.
5. Cobb TK, Morrey BF. Total elbow arthroplasty as primary
treatment for distal humeral fractures in elderly patients.
J Bone Joint Surg 1997 ; 79-A : 826-832.
6. Gabel GT, Hanson G, Bennett JB, Noble PC, Tullos HS.
Intraarticular fractures of the distal humerus in the adult.
Clin Orthop 1987 ; 216 : 99-108.
7. Helfet DL, Hotchkiss RN. Internal fixation of the distal
humerus : a biomechanical comparison of methods. J
Orthop Trauma 1990 ; 4 : 260-264.
8. Henley MB. Intra-articular distal humeral fractures in
adults. Orthop Clin North Am 1987 ; 18 : 11-23.
9. Holdsworth BJ, Mossad MM. Fractures of the adult distal
humerus. Elbow function after internal fixation. J Bone
Joint Surg 1990 ; 72-B : 362-365.
10. Johannson H, Olerud S. Operative treatment of
intercondylar fractures of the humerus. J Trauma 1971 ;
10 : 836-843.
120 Kamruzzaman, Ripon Kumar Das , Asit Baran Dam, Swapon Kumar Paul, Zahid Ahmed, Mohammad Khurshed Alam
The Journal of Bangladesh Orthopaedic Society

11. Jupiter JB, Neff U, Holzach P, Allgower M. Intercondylar
fractures of the humerus. An operative approach. J Bone
Joint Surg 1985 ; 67 : 226-239.
12. Keon Cohen BT. Fractures at the elbow. J Bone Joint Surg
1966 ; 48-A : 1623-1639.
13. Kundel K, Braun W, Wieberneit J, Ruter A. Intraarticular
distal humerus fractures. Factors affecting functional
outcome. Clin Orthop 1996 ; 332 : 200-208.
14. Letsch R, Schmit-Neuerburg KP, Sturmer KM, Walz M.
Intraarticular fractures of the distal humerus. Surgical
treatment and results. Clin Orthop 1989 ; 241 : 238-244.
15. Nadim A,Keith W. Functional outcome following internal
fixation of intra-articular fractures of distal humerus (AO
type C).Acta Orthop. Belg.,2004, 70, 118-122.
16. McKee MD, Jupiter JB. A contemporary approach to
the management of complex fractures of the distal end of
the humerus. Hand Clin 1994 ; 10 : 479-494.
17. Riseborough EJ, Radin EL. Intercondylar T fractures of
the humerus in adult. J Bone Joint Surg 1969; 51A: 130.
18. Self J, Viegas SF, Buford WLJr, Patterson RM. A comparison
of double-plate fixation methods for complex distal
humerus fractures. J Shoulder Elbow Surg 1995 ; 4: 10-16.
19. Sodergard J, Sandelin J, Bostman O. Postoperative
complications of distal humeral fractures. 27/96 adults
followed up for 6 (2-10) years. Acta Orthop Scand 1992;
63 : 85-89.
20. Wang KC, Shih HN, Hsu KY, Shih CH. Intercondylar
fractures of the distal humerus : routine anterior
subcutaneous transposition of the ulnar nerve in a posterior
operative approach. J Trauma 1994 ; 36 : 770-773.
Functional outcome of intraarticular fractures of the distal humerus following both column fixation by tension band wire 121
VOL. 29, NO. 2, JULY 2014

Original Article
Results of One Stage Surgical
Correction of Congenital Vertical Talus
in Children
Dipankar Nath Talukder1, M.A. Hannan2, Ishtiaque Ul Fattah3, Faruqul Islam4, Mohsenuzzaman
Khan5
ABSTRACT
Congenital vertical talus(CVT) is a well known cause of severe rigid flatfoot deformity if it is left untreated. It is
more commonly associated with other neuromuscular disorders with less favourable outcome.
The aim of our study is to find out the clinical and radiological outcome of one stage surgical correction in children
having congenital vertical talus. The goal is to restoration of normal shape and function of the foot.
We report our experience of a one-stage surgical procedure for correction of congenital vertical talus. This
series consisted of 10 congenital vertical tali in 8 patients. Syndromes such as arthrogryposis multiplex congenital
and other neurological abnormality were excluded from this study. So,all are belonged to isolated CVT. All feet
were treated by 2 or 3 serial plaster prior to surgery. The male-to-female ratio was 1:1. The mean operative age
was 28.88 (13-48) months. All patients were available for clinical and radiological follow-up for a mean period of
3.1 (1.1-6) years.Colton scoring system was utilized for assessment of final outcomes.
The outcomes of 8 feet (70%) were excellent, 2 (20%) good and 1(10%) fair. All patients wear normal shoes and
were satisfied by their functional results and appearance. No talar avascular necrosis was encountered. None
required further operation. Radiologically there was a statistically significant difference of postoperative
improvement of measured angles compared to preoperative values (P < 0.005). All radiological parameters were
within normal ranges.
As a complex deformity, isolated CVT may be effectively managed with one-stage procedure for surgical correction
before the age of 4 years. The results of this study indicate that single stage surgical procedure is sufficient for
correction of deformity and no need for excision of talus or navicular.
Keywords: congenital vertical talus, single stage surgery.
1. Associate professor of ortho surgery,Sylhet MAG Osmani medical College Hospital
2. Registrar of ortho surgery,Sylhet MAG Osmani medical College Hospital
3. Associate professor of ortho surgery,Sylhet MAG Osmani medical College Hospital
4. Consultant of ortho surgery,Sylhet MAG Osmani medical College Hospital
5. Registrar of ortho surgery,Sylhet MAG Osmani medical College Hospital
Correspondence: Dr. Dipankar Nath Talukder, M.A. Hannan, Email: [email protected], [email protected]
INTRODUCTION
Congenital vertical talus is a rare foot deformity with an
incidence of 1 in 10,000.1 It is also called congenital convex
pes valgus, Persian slipper, congenital rigid rocker bottom
foot and dislocated navicular and both sexes are equally
affected. It is bilateral in 50% of cases.2,3 The exact etiology
of vertical talus is unknown and possible causes include
muscle imbalance, especially overpull of the anterior tibial
tendon in paralytic disorders, and intrauterine
compression, particularly when coupled with
arthrogryposis.4 Autosomal dominant transmission
through three generations of a family has been reported5,6.
Suggested causes include defects in central nervous
system, muscle abnormalities, genetics and acquired
deformities7,8,9.
The main pathology of congenital vertical talus is the
dorsolateral dislocation of the navicular in relation to the
talus and usually articulates with the dorsal aspect of the
122 The Journal of Bangladesh Orthopaedic Society

neck of the talus and is locked there.(1,10) The navicular
adapts to this position by becoming wedge shaped with a
hypoplastic plantar segment.(9) The talar head and neck
are flattened dorsally and deviated medially, the calcaneus
is displaced posterolaterally in relation to the talus and is
tilted into equinus.4 The talus becomes hourglass shaped
and remain in marked equinus position. So its longitudinal
axis is almost the same as that of the tibia.(11) The
talonavicular joint capsule is dorsally contracted and both
the calcaneonavicular (spring) ligament and the anterior
fibers of the deltoid ligament are stretched. There are
corresponding contractures of the tibialis anterior, long
toe extensors, peroneus brevis, and triceps surae. The
posterior tibial and peroneal tendons may be displaced
anteriorly so that they act as dorsiflexors rather than plantar
flexors5,9,12, the peroneal and tibialis anterior tendons are
contracted, and the foot is everted into a valgus, externally
rotated position1,4,9 It is characterized by hindfoot equines
and valgus, forefoot abduction, and forefoot dorsiflexion
at the midtarsal joint, this is usually recognized in the
newborn period by the rigidity of the foot.1 In congenital
vertical talus, the plantar surface of the foot is convex
creating a rocker bottom appearance.
In addition to the clinical examination, the diagnosis should
be confirmed by radiological examination.1 Congenital
vertical talus is difficult to correct and tends to recur, and
serial casting has been recommended and attempted by
many but ineffective because of the rigidity of the
deformity.9
Surgical correction is the mainstay of treatment. The exact
upper age limit for a successful open reduction is debatable.
The difficulty of surgical correction depends on the
severity of the deformity, the associated diagnosis, and
the age of the patient. Childrens are best treated by open
reduction and realignment of the talonavicular and subtalar
joints which can be performed through either a one-stage
or two-stage operation1,12 The single-stage correction can
be done through dorsal, posterior and medial approach.(1)
METHODS
A prospective study was conducted in Sylhet MAG
Osmani Medical CollegeHospital between September 2007
and August 2013, with 8 patient (10 feet) of isolated CVT
and treated with one stage surgical procedure for
correction of the deformity. After surgery, all cases were
followed up regularly for a mean period of 3.1 years
(minimum 13 months and maximum 6 years), during this
period they were clinically evaluated for subjective
complaints and objective findings focused on the range
of movement at the ankle,subtalar and midtarsal joints,
equines deformity, position of the hindfoot and the lateral
and medial boarders of the foot. Colton (1973)15 scoring
was used as a baseline indicator for the clinical
improvement. AP and lateral radiographs was for
radiological assessment of the talocalcaneal angle and
tibiocalcaneal angle. Statistical analysis was done by using
paired t test.
OPERATIVE PROCEDURE
One staged surgical procedure was used for all patients.(16)
Peritalar soft tissue release with tendons lengthening and
fixation of talonavicular joint by k wire and sometimes
tibialis anterior transfer to talar neck for elderly children
was done. With the 5cm medial straight incision parallel to
the sole of the foot, subcutaneous dissection was done
and incising the talonavicular capsule, head of the talus
was exposed, subtalar release along with division of spring
Table-I
Colton Clinical scores
Topics 4 points 3 points 2 points 1 point
Equinus Dorsiflexion above Dorsiflexion to Slight equinus Gross equinus
square square
Lateral boarder Convex Straight Slight concavity Gross forefoot
abduction
Medial talar prominence None Slight prominence Callosity over Ulceration over
prominence prominence
Mobility Useful range all tarsal Subtalar joint stiff, Stiffness of whole Rigidity of
joints Other tarsal joints mobile tarsus whole tarsus
Range of plantar-flexion Over 20 11 to 20 0 to 10 Fixed dorsiflexion
(degrees)
Lateral boarder Convex Straight Slight concavity Gross forefoot
abduction
Excellent (21 24 points), Good (16 20 points), Fair (14 15 points) and Poor (13 points or less).
Results of One Stage Surgical Correction of Congenital Vertical Talus in Children 123
VOL. 29, NO. 2, JULY 2014

ligament was done, if contracted the tibialis anterior tendon
was lengthened by Z plasty and also the contracted dorsal
talonavicular ligament was divided. Then wide posterior
capsulotomy of ankle and subtalar joints, the contracted
calcaneofibular ligament should be divided to correct the
valgus heel preserving the neurovascular bundle. By using
5cm posterior incision on medial boarder of Achilles
tendon, lengthening was done by z plasty.Lateral incision
was performed for lateral subtalar release, divide the
ligament in sinus tarsi and peroneal z plasty was done if
needed.
A k wire is then inserted in the talus in a retrograde manner
and then used as a joystick to reduce the talonavicular
joint by molding the longitudinal arch and manipulation
of forefoot into plantar flexion and inversion, after that the
k wire is advanced to secure the talonavicular joint then
advanced more to the middle or medial cuneiform. A second
k wire in some cases inserted from the posterior end the
heels through calcaneus to the reduced talus to fix the
subtalar joint.
Reconstruction of the talonavicular ligament and tight
closure of the talonavicular capsule was done.
Six weeks after the surgery the k wires were removed but
the cast were put for further 2 weeks. Then an Ankle Foot
orthosis or a Shoewear with medial arch support was
applied and encourage the child for walk.
RESULTS
There were 8 cases (10 feet), 4 boys and 4 girls and only 2
cases were bilateral. The ages ranged from 13 to 48 months
and the mean was 28.88 months. All the patients had
improvement of their foot deformities based on the
significant differences between the pre and post operative
measurements of radiological talocalcaneal and
tibiocalcaneal angles and also the significant improvement
in the clinical scores.
The results showed highly significant decrease in both
lateral talocalcaneal and tibiocalcaneal angles after surgery.
The mean of lateral right and left talocalcaneal angles
decreases from (41.90°) and (38.00°) before surgery to
(24.70°) and (25.78°) respectively on last follow up, while
the mean of right and left tibiocalcaneal angles decreases
from (122.80°) and (128.80°) before surgery to (88.90°) and
(92.67°) respectively. These difference in mean value are
significant.(p < 0.005)
The clinical picture in all cases were improved and showed
significant increase in the result of clinical scores compared
to the preoperative assessment by the same system.
Preoperatively there were only 3 feet with fair grade while
the rest 7 feet were graded as poor. After performing the
one stage surgical treatment, overall results were 70%
excellent, 20% good and 10% fair. The results is highly
significant.(paired t test, p < O.005)
One case developed superficial wound infection which
was controlled by additional antibiotic support. Pin tract
Preoperative tibio and talocalcaneal angle
Postoperative
124 Dipankar Nath Talukder, M.A. Hannan, Ishtiaque Ul Fattah, Faruqul Islam, Mohsenuzzaman Khan
The Journal of Bangladesh Orthopaedic Society

infection followed by k-wire loosening and auto removal
occured in a patient. After controlloing infection, cast was
applied for 3 weeks followed by orthosis.That patient feft
pain on walking 5 months postoperatively and recovered
after 1 year with fair outcome.
During our follow up period , no patient had worsening or
recurrence of the deformity and no AVN of talus developed.
DISCUSSION:
A high index of CVT is suspected when examining any
child or infant with severe flatfeet. We found 25% cases
were bilateral where as incidence in most literature was
50%.1,9,17
Conservative treatment by serial casting should be
attempted if the child is as young as 3 4 months but we
performed surgical treatment with 2 preoperative casting
as all of our sample were between 13 to 48 months.
Our study showed highly significant decrease in both
lateral talocalcaneal and tibiocalcaneal angles post
operatively. Our results were similar or close to the study
of Saini et. al(17) , Raap and krauspe from Germany (1997)18.
In current study, satisfactory(excellent & good) outcome
was 90% and statistically significant improvement was
observed postoperatively by using Colton score. Similarly,
AAOS instructional series, Clark et al. (1977)19, Striker
and Rosen(1997)20 studies showed more than 80%
satisfactory outcome.
CONCLUSION
We can concluded from our study that one stage surgery
is very useful in children up to 4 years of age, but when
done earlier it will help to avoid a 2nd surgery with its
complication and like naviculectomy and talectomy .
Posterior ankle and subtalar capsulotomy is a keystone in
the treatment along with the division of the contracted
calcaneofibular ligament and adding a tibialis anterior
element in elderly children to the single stage surgery
obviates the need for extra-articular subtalar fusion.
REFERENCES
1. Alaee F, Dobbs M : A new approach to the treatment of
congenital vertical talus. J Child Orthop 2007; 1:165–74.
2. Lamy L, Weissman L: Congenital convex pes valgus. J
Bone Joint Surg 1939;21:79.
3. Osmond Clarke H: Congenital vertical talus. J BoneJoint
Surg Br 1956;38: 334.
4. Herring J. A. : Tachdjian s Pediatric Orthopedics, vol 2,
4thed, Saunders Elsevier, 2008.
5. Stern HJ, Clark RD, Stroberg AJ,et al. : Autosomal
dominant transmission of isolated congenital vertical talus.
Clin Genet 1989;36:42Z .
6. Seimon LP. Surgical correction of congenital vertical talus
under the age of 2 years. J Pediatr Orthop 1987;7:405 11.
7. Stanton, R. P.; Rao,N.; and Scott, C. I., Jr.: Orthopaedic
manifestations in de Barsy syndrome. J. Pediat. Orthop.,
1994;14: 60 62.
8. Södergård, J., and Röyppy, S.: Foot deformities in
arthrogryposis multiplex congenita. J. Pediat. Ortinop.,
1994;14: 768 72.
9. Drennan J. C.: Congenital vertical talus. J BoneJoint Surg
1995; 77 A .
10. Sarsam IM: A one stage operation to correct congenital
vertical talus deformity.Pan ArabJOrth.Traum1995;2; 667
11. Moore, Keith L.:Clinically Oriented Anatomy, 5th
Edition.2006.
12. Canale and Beaty, Campbell’s Operative Orthopaedics,
2008;11th ed.
13. Weinstein S. : Turek’s Orthopaedics: Principles and Their
Application, 6th Ed, Lippincott Williams & Wilkins 2005.
14. Szendrõi, F.and Sim, F. H. Color Atlas of Clinical
Orthopedics, 1st ed , 2009:252.
15. Christopher L. Colton: The Surgical management of
congenital vertical talus. J BoneJoint Surg 1973; 55 B.
16. Bosker B. et al.: Congenital convex pes valgus (congenital
vertical talus)The condition and its treatment : A review
of the literature. Acta Orthopædica Belgica, 2007;73 3 .
17. Saini R. et al: Results of dorsal approach in surgical
correction of congenital vertical talus: an Indian experience.
J. P iat. Orthop.B March 2009;8:63 68 .
18. P.Raap and R.Krauspe :One stage procedure for surgical
correction of congenital vertical talus. Foot and ankle
surgery , 1997;3: 71 76.
19. Clark W. et al: Congenital vertical talus treatment by open
reduction and navicular excision. J BoneJoint Surg 1977;59
A.
20. Stricker SJ, Rosen E Early one stage reconstruction of
congenital vertical talus. Foot Ankle Int 1997; 18:
535–43.
Results of One Stage Surgical Correction of Congenital Vertical Talus in Children 125
VOL. 29, NO. 2, JULY 2014

Original Article
Management of Traumatic Orbital Wall
Fracture with Titanium Mesh
Kazi Lutfor Rahman1, Ismat Ara Hayder2, Mohammad Ghulam Rasul3, Anjal Lal Ghosh4, Shibasis Basak5
ABSTRACT
The management of orbital injuries is one of the most interesting and difficult areas in maxillofacial surgery. The
improper reconstruction of the orbit frequently results in ophthalmic complications. Though a number of materials
are available for the use in orbital wall reconstruction, at present titanium mesh could be considered to be the ideal
orbital floor repair material. Ten cases of internal orbital wall defects were reconstructed by titanium mesh at the
Dept. of Oral and Maxillofacial Surgery, Dhaka Dental College and Hospital, Dhaka from January, 2013 to December,
2014 were considered for this study. The study involved patients with symptomatic zygomatico-orbital fractures
requiring orbital wall reconstruction. Under general anaesthesia the floor of orbit was explored and reconstructed
with contoured titanium mesh after repositioning of the entrapped orbital contents.The patients were on periodic
follow- up for 3 months where clinical and radiographic data were recorded. Ten male patients age ranging from
18 to 50 years ( mean 30.50 years) received titanium mesh for impure orbital fractures ( eight patients) and pure
orbital floor fractures ( two patients). The main cause of fractures was road traffic accidents. They also complained
of enophthalmos (n = 9), diplopia (n = 8), infraorbital nerve paresthesia (n = 4), dystopia (n = 1) and epiphora (n= 2).
No implant extrusion or infection was seen. The symptoms were corrected in eight patients with enophthalmos,
seven with diplopia, three with infraorbital nerve paresthesia and all patients with epiphora. Dystopia persisted
post-surgically in one patient. Titanium orbital implants were used to confirm titanium as a useful repair material
for orbital floor fractures. Their use leads to less morbidity as no donor site operation is needed. Titanium mesh
provides favourable healing as it is biocompatible.
Keywords: Orbital floor fractures · Titanium mesh · Enophthalmos · Reconstruction of floor.
1. Researcher, Dept. of Oral and Maxillofacial Surgery, Dhaka Dental College Hospital
2. Professor & Head, Department of Orthopaedic Surgery, Dhaka Dental College Hospital
3. Associatge Professor, Department of Orthopaedic Surgery, NITOR, Dhaka
4. Assistant Professor, Department of Orthopaedic Surgery, ZH Sikder Medical College
5. Registrar, Department of Orthopaedic Surgery, Dhaka Medical College, Dhaka
Correspondence to : Dr.Kazi Lutfor Rahman, M.S (Oral and Maxillofacial Surgery), PhD Researcher, Fellow IAOMS (USA),Department
of Oral and Maxillofacial Surgery, Dhaka Dental College and Hospital, Dhaka, Bangladesh, Cell: +8801711235845, E-mail:
INTRODUCTION
The management of orbital injuries is one of the most
interesting and difficult areas in maxillofacial surgery. The
consequences of an orbital injury are dramatic. They vary
from loss of vision, enophthalmos, diplopia,loss of an
eye, epiphora, a disturbing loss of facial sensation to an
unsightly and unacceptable appearance of the eye and
the hard and soft tissues around it.These injuries demand
careful attention to detail but they are often
underestimated and undertreated1.
Damage to the orbital walls themselves can cause
disorders such as enophthalmos, diplopia and much less
frequently vertical dystopia. It is therefore mandatory to
reconstruct the orbital floor and also repair of orbital rims
in the same time2.
Numerous materials - both naturally occurring and
synthetic substances - are available for reconstructing
damaged internal orbital walls to restore orbital volume.
This is a prospective study for the management of post-
traumatic orbital internal wall defect reconstruction by
titanium mesh implants to provide long term chemically
inert, biocompatible material which can replace autogenous
bone grafts. The demerits include the need for a donor
site and its complications.
MATERIALS AND METHODS
Ten patients (ten male patients between 18 to 50 years
of age) with internal orbital wall fractures were randomly
selected and treated at the Department of Oral and
Maxillofacial Surgery, Dhaka Dental College and Hospital,
126 The Journal of Bangladesh Orthopaedic Society

Dhaka after obtaining ethical clearance between January,
2013 to December, 2014. The study involved patients with
symptomatic zygomatico-orbital fractures requiring
orbital wall reconstruction.
Patients presented with orthoptic symptoms including
enophthalmos, diplopia,and dystopia or other associated
symptoms like nerve paresthesia or epiphora.
All patients were operated under general anaesthesia
through nasoendotracheal tube.
All patients were evaluated by the ophthalmologist for
errors in vision, presence of enophthalmos, diplopia or
dystopia and a through clinical history was recorded.
Routine presurgical blood investigations and radiographs
or computed tomography ( CT) scans were obtained.
Diplopia charting was done clinically in all nine cardinal
positions of gaze pre- operatively and post- operatively.
Following thorough skin preparation with betadine and
sprit, tarsorrhaphy was done. Infraorbital incision was
given in eight patients and subcilliary incision was given
in two patients. Dissection layer by layer done and fracture
site was exposed. The entrapped orbital tissues were
repositioned and walls were reconstructed using cut and
contoured 0.2 mm titanium mesh [Medicon Mesh
Plate,contourable, Pure Titanium]. The mesh was fixed to
the infraorbital rim using 2 mm screws to ensure graft
stability.
The surgical skin defect was closed primarily in layers
taking care to prevent any tension across suture line.
All patients were evaluated for the correction of their
preoperative complaints through clinical and radiological
Fig.-1: Case 1 pre-operative and post-operative profile
view
Fig.-2: Case1 preoperative and postoperative coronal
CT scan
Fig.-3: Case 1 before and after intra operative reconstru-ction
examinations for a period of 3 months. Coronal CT scans
with 3D reconstruction was done in all cases
postoperatively following reconstruction ( Figs. 1,2, 3, 4,
5, 6, 7, 8, 9,10 ).
Management of Traumatic Orbital Wall Fracture with Titanium Mesh 127
VOL. 29, NO. 2, JULY 2014

RESULTS
The main aim of the investigation was to evaluate clinically
the efficiency of use of titanium mesh for the
reconstruction of orbital floor post traumatically.
In this study, the most common mode of injury causing
orbital wall fractures were associated with road traffic
accidents ( 80%), followed by assault (20%).
Majority of fractures involving orbit were caused by
indirect forces associated with fractures of zygomatico -
maxillary complex with 80% of the study sample being
orbital fracture of impure type and two patients with pure
orbital blow out fractures. Minimum time lapse between
trauma and surgery was 7 days and maximum period was
27 days.
This study showed no cases with infection of the surgical
site.None of cases showed any other complications
associated with the use of alloplastic materials like implant
migration, extrusion of implant or hypersensitivity.
Epiphora was noted in two patients (20%) preoperatively
on fractured side which resolved considerably over the
period of 3 weeks. None of the patients complained of
epiphora upto 8 weeks following surgery.
Enophthalmos was seen in 90% of patients included in
the study preoperatively. Correction of enophthalmos was
seen in 88.9% of our patients, on the 8th week following
surgery only one patient showed signs of enophthalmos.
Though the possibility of late post- operative
enophthalmos is a possible sequale, all our patients were
reviewed after 1 year and did not show any signs of
enophthalmos to date.
This study showed correction of diplopia in 87.5% of
patients. Persistance of double vision was only noted in
one patient in extreme upward gaze, this error in the vision
did not affect the patient’s day to day activities.
Dystopia was present in one patient preoperatively which
corrected after surgery. In this study 40% of the patients
reported numbness over the infraorbital and lateral part
of the nose following trauma. Patients showed
considerable improvement over time and 80% of patients
involved in the study had no complaints of paresthesia
over 8 weeks of surgery.
None of cases showed any obvious entrapment of the
orbital muscles on surgical exposure. Though orbital
connective tissue and fat were noticed to be entrapped in
the fracture site none of the cases showed any obvious
restriction of globe movement.
Fig,-4: Case 1 post operative 3D reconstruction scan Fig.-5: Case 1 post-operative 3 months follow up
Fig.-6: Case 2 preoperative and post-operative profile
view
128 Kazi Lutfor Rahman, Ismat Ara Hayder, Mohammad Ghulam Rasul, Anjal Lal Ghosh, Shibasis Basak
The Journal of Bangladesh Orthopaedic Society
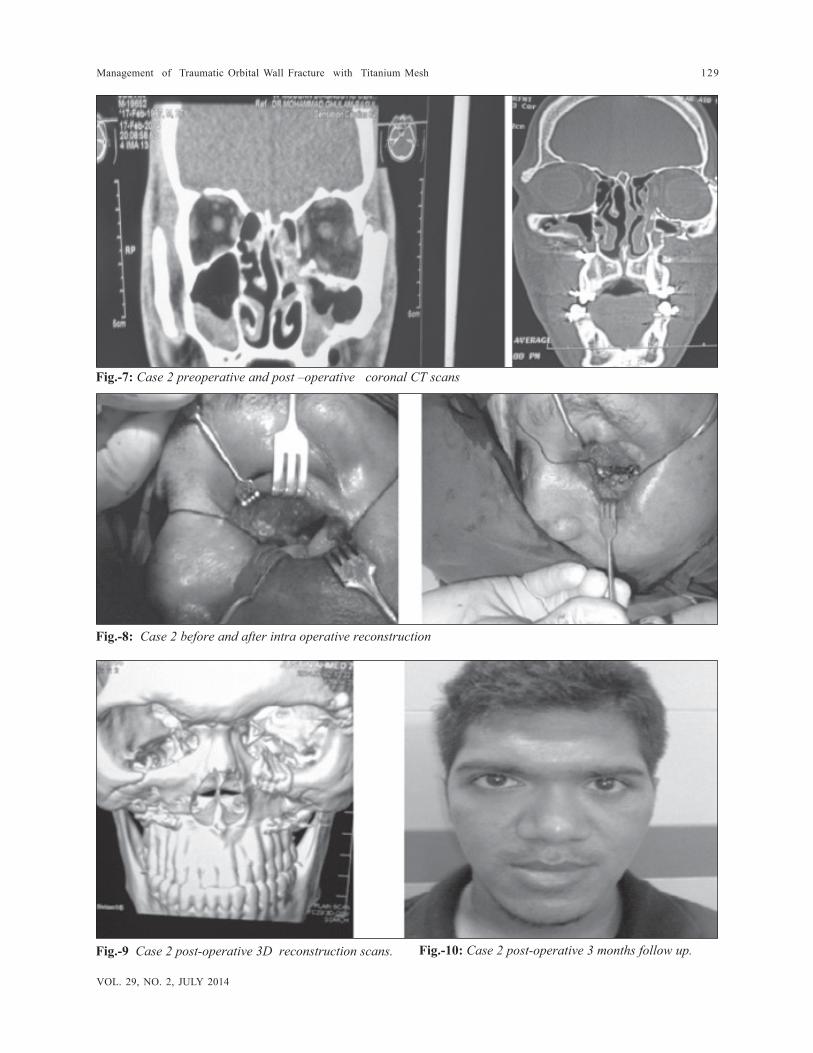
Fig.-7: Case 2 preoperative and post –operative coronal CT scans
Fig.-9 Case 2 post-operative 3D reconstruction scans.
Fig.-8: Case 2 before and after intra operative reconstruction
Fig.-10: Case 2 post-operative 3 months follow up.
Management of Traumatic Orbital Wall Fracture with Titanium Mesh 129
VOL. 29, NO. 2, JULY 2014

DISCUSSION
The orbital floor is most vulnerable to fracture because of
thinness of the maxillary roof, existence of the infraorbital
canal and curvature of the floor. Immediately behind the
orbital rim, the floor is concave, whereas further back , it
becomes convex and is called posterior ledge or bulge,
where the bony structure becomes thicker and less
deformed in the orbital floor fracture3.
Reconstruction of this posterior bulge or retrobulbar bulge
by proper contouring of this titanium mesh before insertion
into the defect has to be strictly followed to ensure that
the antero – posterior globe position is maintained after
reconstruction (Fig. 5). Failure to achieve this step during
surgery could result in late post- operative enophthalmos.
There has been extensive debate over the standard of
care of orbital floor and wall fractures. Recommendations
of treatment range from exploration to observation. Clinical
indicators such as enophthalmos, persistent diplopia,
infraorbital nerve paresthesia, muscular entrapment or
incarceration, hypoglobus, potentiation of the
oculocardiac reflex, severe orbital emphysema, as well as
various radiographic criteria have all been proposed as
indications for surgical intervention. Of these, diplopia,
entrapment and hypoglobus, with or without
enophthalmos, seem to be the most common clinical signs
for surgical intervention4.
The ideal material for orbital reconstruction remains
controversial. It should be cheap, biocompatible, readily
available, easy to manipulate and insert in the operating
room and it should allow fixation to the host bone by
screws, wire or sutures.
The more elastic materials are unable to withstand the
dynamic stresses of large defects. Resorbable implants
may be prone to foreign- body reaction, implant exposure
and having only fibrinous connective tissue remains after
resorption. The disadvantages of autogenous bone grafts
include minimal contourability and a donor site defect. In
addition, implant resorption can occur.
High complication rates have been reported in use of some
alloplastic materials5-8.
In the present study showed excellent biocompatibility
with no post surgical infection with the use of titanium
mesh and shows excellent results in correction of post
traumatic orthoptic problems with titanium mesh for orbital
floor fractures. Only one patient showed persistence of
double vision at the end of 8 weeks following
reconstruction in only extreme upward gaze. Some
alloplastic materials like porous polyethylene implants have
shown persistence of diplopia in 25- 30% of patients5-9.
Correction of enophthalmos yielded excellent results with
titanium mesh with 88.9% of the test sample showing
resolution of the symptoms. One patient who showed
persistent enophthalmos presented with extensive injury
(panfacial trauma) to surrounding bony structures with
loss of bony architecture. At the 8 week following surgery
there was significant improvement in globe position and
volume with mild persistent enophthalmos compared to
the uninjured eye. Extensive injury could be postulated to
be the reason for difficulty to correct the globe volume
satisfactorily.
Numbness over the skin in the infraorbital region was
noticed in 40% of the patients which was seen to persist
over a period of 3 weeks following surgery and slowly
resolved over 8 weeks with 80% of patients showing no
symptoms of paresthesia.
CONCLUSION
Titanium mesh has a long track record of reconstruction
of large orbital floor defects and correction of globe
malposition. Care has to be taken in reconstruction of the
retrobulbar bulge with titanium mesh by adequate
contouring of the mesh in this critical area to ensure proper
globe position.
Some advantages of titanium mesh plates are availability,
biocompatibility, easy intraoperative contouring and rigid
fixation. Disadvantages are difficulties with ease of
insertion.Any rough edges on the mesh tend to catch on
prolapsed orbital fat. Removal of the titanium mesh after
the healing period is challenging due to scar tissue that
grows through the mesh perforations.
This study highlights the ability of the alloplastic mesh to
satisfactorily correct post traumatic orbital sequel including
enophthalmos and diplopia.
Titanium mesh can be considered to be the ideal orbital
floor repair material.
REFERENCES
1. Leo FA, CyrusJK (2007) Peri and intraorbital trauma and
orbital reconstruction.In: Booth PW, Schendel SA,
Hausmen JE( ed) Maxillofacial surgery, vol 1, 2nd edn.
Churchil Livingstone, Edinburg, p 205-222
2. Metzger MC, Schon R, Schulze D, Carvalho C, Gutwald
R, Schmelzeisen R (2006) Individual preformed titanium
meshes for orbital fractures. Oral Surg Oral Med Oral
Pathol Oral Radiol Endod 102: 442 – 447
3. Stanley RB (2002) Treatment of orbitozygomatic fractures.
In: Papel ID et al (ed) Facial plastic and reconstructive
surgery, vol 1, 2nd edn. WB Saunders, Philadelphia,p
746-748
130 Kazi Lutfor Rahman, Ismat Ara Hayder, Mohammad Ghulam Rasul, Anjal Lal Ghosh, Shibasis Basak
The Journal of Bangladesh Orthopaedic Society

4. Mazock JB, Schow SR, Triplett RG (2004) Evaluation of
ocular changes secondary to blow- out fractures. J Oral
Maxillofac Surg 62:02-1298.
5. Villarreal PM et al (2007) Porous polyethylene implants
in orbital floor reconstruction. Plast Reconstr Surg 109
:877-885.
6. Baumann A, Burggasser G,Gauss N,Ewers R (2002)
Orbital floor reconstruction with an alloplastic resorbable
polydioxanone sheet. Int J Oral Maxillofac Surg 31: 367-
373.
7. Tuncer S et al (2007) Reconstruction of traumatic orbital
floor fractures with resorbable mesh plate. J Craniofac
Surg 18: 598 – 605.
8. Lee S et al (2005) Porous high- density polyethylene for
orbital reconstruction. Arch Otolaryngol Head Neck Surg
131: 446 – 450.
9. Hidding J, Deitmer T, Hemprich A,Ahrberg W (1991)
Primary correction of orbital fractures using PDS-
foil.Fortschr Kiefer Gesichtschir 36 :195 - 196.
Management of Traumatic Orbital Wall Fracture with Titanium Mesh 131
VOL. 29, NO. 2, JULY 2014

Original Article
1. Assistant Professor (Arthroplasty Orthopaedic Surgery), DMCH, Bangladesh
2. Assistant registrar , Orthopaedic Surgery , Dhaka Medical College Hospital. Bangladesh.
3. Assistant Professor (Orthopaedic Surgery), Dhaka Medical College and Hospital, Dhaka, Bangladesh.
4. Assistant registrar , Orthopaedic Surgery, Mymensing Medical College Hospital. Bangladesh.
5. Associate Professor, Department of Orthopaedic Surgery, Dhaka Medical College Hospital, Bangladesh
Correspondense: Dr. Mobarak Hossain. Assistant Professor (Arthroplasty Orthopaedic Surgery), Dhaka Medical College Hospital.
Bangladesh. Tel=+88-01715784628, Email. [email protected]
Evaluation of the Outcome of Proximal
Femoral Locking Compression Plate for
the Treatment of Comminuted
Trochanteric and Subtrochanteric
Femoral Fractures
MM Hossain1, QS Alam2, MFH Qasem3, MTI Noman4, Md. Golam Sarwar5, Md. Golam Mostofa5
ABSTRACT
The Comminuted trochanteric and subtrochanteric femoral fractures are considered as one of the most difficult
fractures to treat in the orthopaedic surgery and they associated with high incidence of nonunion, malunion.
Various implants, both intramedullary and extramedullary, are available for their fixation.
To assess the success rate of proximal femoral locking compression plate osteosynthesis in comminuted
trochanteric and subtrochanteric femoral fracture.
20 consecutive patients with comminuted Trochanteric and subtrochanteric fractures were operated upon with
PF-LCP. Detailed clinical conditions of all patients, duration of operation, technical difficulty with the implant,
hospital stay period were recorded. Patients were visited at 6 weeks interval till union then 3 monthly. The Harris
Hip Score was used to document hip function at final follow-up.
There were fifteen excellent (75%), two good (10%), two fair (10%) and one poor (5%) results according to Harris
hip score. No instance of implant failure was recorded.
Fixation of comminuted trochanteric and subtrochanteric fractures with PF-LCP provides stable fixation with
high union rate and fewer complications.
Keywords: Proximal femoral locking compression plate, Femoral Comminuted trochanteric and subtrochanteric
fracture, plate osteosynthesis
INTRODUCTION
Trochanteric and subtrochanteric femoral fractures
account for 10% to 34% of all hip fractures. They have a
bimodal age distribution and different mechanism of injury.
Older patients typically sustain low-velocity trauma, where
as in younger patients these fractures commonly result
from high-energy trauma and often are associated with
other fractures and injuries. (Lavelle, 2008).
Comminuted Trochanteric and subtrochanteric femoral
fractures are high-energy injuries in adults. In the proximal
part of the femur the medial cortex is subjected to
compressive loads and the lateral cortex to tensile forces
during weight bearing. Comminution of medial cortex may
lead difficulty in anatomic reconstruction of this area. The
blood supply of the comminuted fragments may be
compromised in subtrochanteric region with predominantly
cortical bone which has less healing capacity than
metaphyseal region. Therefore, one should consider the
biomechanics of mechanism of injury and preoperative
plan for stability based on those assumptions. (Kayali, et
al., 2008)
132 The Journal of Bangladesh Orthopaedic Society

The management of these fractures is challenging for 2
reasons: (1) the inherent instability of the fracture pattern
and (2) the forces of the muscles acting on the proximal
and distal fragments. Fracture patterns at the
subtrochanteric level are typically transverse or run
obliquely in an inferolateral direction from the lesser
trochanter. Thus, the fracture line runs parallel to the
direction of movement of the lag screw in a sliding hip
screw (SHS) implant, rendering this implant ineffective.
Often, the medial calcar is comminuted, giving the fracture
a tendency to collapse into varus. Medial comminution
and the strong pull of the adductor musculature promote
medialization of the shaft. The powerful abductor and
iliopsoas muscles insert on the proximal fragment and force
it into abduction, flexion, and external rotation. This makes
closed reduction of this fracture difficult and pushes the
proximal fragment into a malreduced position. (Kuzyk, et
al., 2009)
Over the last few years, there has been a shift in the
principles of management of these fractures from rigid
anatomic reduction to relative biological fixation which
preserves the vascularity of bone fragments and enhances
their callus-forming abilities. Biological fixation, in
comparison to traditional open plating, has produced good
results for these fractures. (Saini, et al., 2013)
The proposed three requirements for an ideal internal
fixation for pertrochanteric fracture: (1) femoral neck screw
with at least three dimensional structures of the fixed
system; (2) minimal angle between the femoral neck screw
axis and the femoral shaft and thus maximum alignment
between the angle of normal hip joint weight-bearing line
and the femoral graft axis and (3) ability of the implant to
prevent the rotation of the femoral head. Unfortunately,
none of the currently used devices can fully meet these
three criteria. Future studies should be conducted to
determine the optimal implant for the internal fixation of
pertrochanteric fractures that can maximally meet the three
criteria described above. (Zha, et at., 2011).
METHOD:
This is a prospective interventional study (Quasi
experimental type) done From December 2013 to May 2014
at department of Orthopaedic Surgery, DMCH. All patients
with clinical and radiological evidence of comminuted
trochanteric and subtrochanteric fracture admitted in
Hospitals for operation within three weeks of incidence.
Active or latent infection, Pathological fracture other than
osteoporotic fracture, Open fracture, Non-united fracture
were excluded from the study.
Surgery was performed with the patient supine on a fracture
table. Length restoration and fracture reduction was done
either direct or indirect method. In highly comminuted and
unstable fractures that cannot be adequately reduced by
traction on a fracture table, we preferred free draping of
the lower extremity in the supine position on a radiolucent
operating table for open reduction. The operative area
was scrubbed first with hexiscrub and painted with
povidone iodine. Then draping was made. A lateral
approach typically is performed by a straight incision from
the greater trochanter, extending approximately 10 cm
distally. For more complex and comminuted fractures, the
plate can be used as a reduction tool. In this case, the
proximal fragment is first fixed to the plate, and the plate is
then reduced to the femoral shaft. After ensuring perfect
anatomic placement of the plate to the proximal fragment,
a 2.5-mm drill tip guide wire is inserted through a wire
sleeve that is threaded to the most proximal hole at a
predetermined 95° angle. A second guide wire is then
inserted through the drill sleeve of the second hole in a
120° angle. Finally, a third guide wire is inserted through
the sleeve on the third hole above the calcar in a 135°
angle. The plate was then distally fixed with at least 3
bicortical locking head screws. After proper haemostasis
a drain was placed at appropriate site and wound was
closed in layers with vicryl. The skin was closed with skin
stapler.
Fig. 1: The locking compression plate for the proximal
femur is a precontoured, angular stable, with large
fragment screw (7.3/5.0/4.5mm).
Evaluation of the Outcome of Proximal Femoral Locking Compression Plate for the Treatment 133
VOL. 29, NO. 2, JULY 2014

RESULTS
The patients started static quadriceps exercises after 24
hours. Drain tube was removed after 48 hours. Stitches
were removed on 14th postoperative day. Postoperatively
antibiotics were given routinely for 2 weeks. The Patients
was allow moving out of bed using crutch and without
bearing weight on operated limb as pain permits. Knee
bending was allowed as pain permits. The patients was
discharged with the advice to walk on crutch non - weight
bearing on affected side for 6 weeks and then to report to
the outpatient department. Partial weight bearing was
allowed as soon as the patient could tolerate it with
considering the fracture configuration, bone quality and
the stability of the fixation. Full weight bearing was started
when the fracture showed complete union clinically by
absence of limb pain when standing upon the fracture
limb alone and radiologically by the presence of the
abundant callus at least in two views.
Table- I
Distribution of patient according to bony union time .
Evidence of bony union shown on plain radiograph
Time (weeks) Number of Percentage Mean
patients (%) ±SD
12-18 16 80 17.79±2.89
19-24 02 10
25-30 02 10
Among 20 patients mean time to union was 17.79±2.89
weeks. Four cases were of delayed union.
Table-II
Postoperative complication
Postoperative complication No. of Percentage
patient (%)
Infection 1 5
Screw cutout 0 0
Implant failure 0 0
Limb shortening 1cm 2 10
Postoperative complications were minimum.
Table-III
Comparison of ROM and SNA
Outcome Injuried Hip Healthy Hip P-
(Mean±SD) (Mean±SD) value
Range of Motion 139.47±4.04 142.37±2.57 p>.05
Shaft Neck Angle 133.58±1.07 134.32±0.94 p>.05
Table- IV
Distribution of the results according to the final
outcomes (n=20).
Result Number of Percentage
patient
Satisfactory 18 90%
(Excellent & Good)
Unsatisfactory 02 10%
(Fair & Poor)
Total 20 100%
Confidence level of the final outcome:
Range of Motion and Shaft Neck Angle of the hip joint of
the injured and healthy side were measured at the last
follow-up. Paired t- test was done for calculation of test
statistic and there was no significant difference between
them (p>0.05).
Chart-1: Harris Hip Score
Mean Harris Hip Score was 92.05±7.85.
So, among the population we will find almost 70% to 100%
satisfactory result by this procedure. It is quite acceptable
outcome.
134 MM Hossain, QS Alam, MFH Qasem, MTI Noman, Md. Golam Sarwar, Md. Golam Mostofa
The Journal of Bangladesh Orthopaedic Society

Case-1
Pre-operative x-ray on
25/03/2014
Post operative x-ray on
20/04/2014
Post operative x-ray on
20/04/2014
Case-2
Pre-operative x-ray on
12/10/2013Pre-operative x-ray on 12/10/2013 Follow up x-ray on
Case-3
Pre-operative x-ray on
20/05/2014
Follow up x-ray on 07/
06/2014
Follow up x-ray on
19/07/2014
Follow up x-ray on
19/10/2014
Evaluation of the Outcome of Proximal Femoral Locking Compression Plate for the Treatment 135
VOL. 29, NO. 2, JULY 2014

DISCUSSION
Comminuted Trochanteric and subtrochanteric femoral
fractures are considered as one of the most difficult fracture
to treat for the orthopaedic surgeons. It was found that
indirect reduction and biological fixation method with the
dynamic condylar screw and plate is considered as a
valuable cheap fixation method for the management of
comminuted subtrochanteric fractures of femur especially
in the young patient’s populations. (Elzohairy, 2012)
In our study we evaluated the result of proximal femoral
locking compression plate osteosynthesis for the treatment
of comminuted Trochanteric and subtrochanteric fracture
and we did a prospective study. Out of our 20 patients,
age range from 21-70 years with a mean age of 41.35 years.
Among them maximum were between 31-40 years (35%).
Like all trauma cases comminuted Trochanteric and
subtrochanteric fracture is more common in male due to
more activities and traveling. In our study, out of 20
patients, male patients were 17 (85%).
High velocity trauma due to road traffic accidents was the
main cause of these fractures seen in our study. The mean
duration of follow up was 39.70 weeks (24-58 weeks).
Average time to union was 17.35 weeks (14-28 weeks).
Partial weight bearing (15-20kg) was allowed as soon as
the patient could tolerate it and full weight bearing was
started when the fracture showed complete union clinically
by absence of limb pain when standing upon the fracture
limb alone and radiologically by the presence of the
abundant callus at least in two views. Sixteen patients had
union within 18 weeks, 4 patients had delayed union (28
weeks). One centimeter shortening was seen in two
patients. No patient had significant rotational malalignment
as determine by clinical examination. There were no cut-
outs, breakage or pull-out of screws.
Shaft-neck angle and range of motion of hip joint of the
injured and healthy sides were measured at the last follow
up, and there was no significant difference between them
(p>0.05). Harris Hip Score was used for clinical assessment,
as per Harris Hip Score 18 patients (90%) had good or
excellent outcome with two fair result (10%).
CONCLUSION
The present study conclude, with proper patient selection,
good instrumentation, image intensifier and surgical
technique, proximal femoral locking compression plate is
the implant of choice in the management of comminuted
Trochanteric and subtrochanteric fracture.
Large scale studies with longer follow up are essential
requirement for an optimum outcome measurement.
Though the study was small which may not represent the
whole scenario but the results of the study can be utilized
for future large study.
REFERENCES
1. Anglia Ruskin University Library, 2011. Guide to the
Harvard Style of Referencing, 3rd edition, [PDF] London.
Anglia Ruskin University. Available at: <http://
libweb.anglia.ac.uk/referencing/harvard.htm> [Accessed 29
March 2012]
2. Elzohairy, M.M., 2012. Management of Comminuted
Subtrochanteric Femur Fractures by Indirect Reduction
and Biological Fixation with Dynamic Condylar Screw. J
Trauma Treat, 1, pp.1-3
3. Kuzyk, P.R.T., Bhandari, M., McKee, M.D., Russell,
T.A., Schemitsch, E.H., 2009. Intramedullary Versus
Extramedullary Fixation for Subtrochanteric Femur
Fractures. J Orthop Trauma, 23, pp.465–70
4. Kyle, R.F., 1993, Fracture of the hip. In R.B. Gustilo,
R.F. Kyle and D. C. Templeman, eds. 1993. Fractures and
Dislocations, volume 2, St. Louis, Mosby, Ch.23, pp.
783-854.
5. Lavelle, D.G. 2008. Fracture and Dislocation of the Hip.
In: S.T. Canale and Beaty J. H. eds. 2008. Campbell’s
Operative Orthopaedics, Volume III: 11th Ed. Philadelphia,
PA: Mosby, Elsevier, Ch. 52. pp. 3237-309.
6. Saini, P., Kumar, R., Shekhawat, V., Joshi, N., Bansal,
M., Kumar, S., 2013. Biological fixation of comminuted
subtrochanteric fractures with proximal femur locking
compression plate. Injury International Journal of the Care
of the Injured, 44, pp.226–31
7. Zha G.C., Chen Z.L., Qi X.B., Sun J.Y., 2011. Treatment
of pertrochanteric fractures with a proximal femur locking
compression plate. Injury International Journal of the Care
of the Injured, 42, pp.1294 – 99.
136 MM Hossain, QS Alam, MFH Qasem, MTI Noman, Md. Golam Sarwar, Md. Golam Mostofa
The Journal of Bangladesh Orthopaedic Society

Original Article
Result of Arthroscopic Anterior Cruciate
Ligament Reconstruction by
Semitendinosus & Gracillis Tendon
Graft
Md. Harun-Or-Rashid Khan1, Mohammad Serajus Saleheen2 ,M. Muniruzzaman3, Md.Aminul
Haque Pathan 4, Md. Abdus Sabur 5, Md. Iqbal Qavi6
ABSTRACT
This clinical study is the results of ACL injury reconstructed by quadruple semitendinosus & gracillis graft on 10
patients over a period of two years from January 2011 to December 2012 at National Institute of Traumatology and
Orthopaedic Rehabilitation (NITOR) Dhaka. The objective of this study was to evaluate the outcome of ACL
reconstruction. In this study purposive sampling method was followed irrespective of sex. ACL injury which had
persisted at least 3 months and was not improved by conservative treatment and patient with no history of
previous reconstructive surgery of ACL were included in this study. Data were collected by structured questionnaire
which includes all the variables of interest. The test statistics used to analyze the data were descriptive statistics
paired “t” test. Result shows all the patients were male with mean age 26.10 (±6.56 ) years. About half of the
subjects were student & service holder. Right knee was affected in 30% and left knee in 70% patients. Associated
meniscus injury was in 40% cases. Preoperative all patients had positive anterior drawer test. They had either
grade II or grade III positive Lachman test. Pivot shift test was positive in 60% cases. Preoperative Lysholm score
was 55.30 (±5.05). Mean hospital stay after operation was 4.90(±1 .66) days. Post operative subjective outcome
6 months after operation including influence of activity level, knee function, pain, recurrent swelling, and giving
way improved significantly. Post operative objective outcome including Lachman test, Anterior drawer test and
Pivot shift test were improved significantly. Preoperative versus post operative Lysholm score show a significant
improvement (p< 0.001). Final out come of this study shows 80% satisfactory and 20% unsatisfactory result.
1. Jr. Consultant of Orthopaedics (cc), NITOR.
2. Jr. Consultant of Orthopaedics (c.c), NITOR.
3. Jr. Consultant of Orthopaedics, Sadar Hospital, Jhalokathi.
4. Assistant Professor, NITOR, Dhaka
5. Assistant Professor, NITOR, Dhaka
6. Professor of Orthopaedic Surgery, NITOR.
Correspondence to: Dr. Md. Harun- Or- Rashid Khan, MBBS (DU), D ortho, MS (Ortho), Jr. Consultant of Orthopaedics(c.c)., NITOR,
Cell: 01711977642.
INTRODUCTION
The knee is the largest joint in the body. It is also the most
frequently injured joint due to its anatomy, exposure and
the demand placed upon it. Function and stability of the
knee depend upon a complex interrelationship of bony
and soft tissue anatomy 1.
The anterior cruciate ligament is on of the major stabilizing
ligament of the knee. It is a strong rope like structure
located in the centre of the knee running from the femur to
the tibia. It prevents the tibia moving abnormally on the
femur. When this abnormal movement occurs it is referred
to as instability and the patient is aware of this abnormal
movement2. The cruciate ligaments provide both
anteroposterior and rotatory stability; they also help to
resist excessive valgus varus angulations. Injuries of these
ligaments are on, particularly in sporting pursuits but also
in road accidents where they may be associated with
VOL. 29, NO. 2, JULY 2014 137

fractures or dislocations. They vary in severity from a
simple sprain to complete rupture3.
The importance of the anterior cruciate ligament (ACL) in
the maintenance of stability of the knee is well-known.
Active individuals who have a torn anterior cruciate
ligament are frequently troubled by chronic instability and
recurrent episodes of giving-way, which often are
associated with intra-articular injuries4.
The exact incidence of anterior cruciate ligament injuries
is unknown; however, it has been estimated that 100,000
are torn each year, and 50,000 anterior cruciate ligament
reconstructions are done each year in the United States.
The controversy for managing this injury now centers
more on the choice of graft selection for reconstruction
instead of whether surgery is necessary2.
Reconstructions of the anterior cruciate ligament (ACL)
are frequently performed procedures in knee surgery
nowadays. Looking at the history of ACL surgery since
its advent in antiquity, it is amazing to see how long it took
for some diagnostic and management techniques to
establish themselves. However since the early 20th
century, there has been increasing awareness of and
interest in the ligament and its lesions5. Numerous authors
have described successful reconstruction of the ACL with
use of a myriad of donor auto graft Patellar, hamstring or
quadriceps and allograft (Achilles, patellar, hamstring or
tibialis anterior) tendons. A statistical survey was carried
out at NITOR, Dhaka between January 2011 and December
2012 in the patients admitted with anterior cruciate ligament
insufficiency. Effort has been made in this work to extract
certain relevant facts in connection with ACL insufficiency
and the mode of their management and finally to evaluate
the outcome of reconstruction of ACL injury by quadruple
semitendinosus & gracillis tendon graft using arthroscopic
assisted ACL Reconstruction with the hope that it will
impart us a better understanding of further treatment of
this particular trauma in our country.
Reconstruction of ACL by BTB gained popularity but
donor site morbidity, anterior knee pain and stiffness are
major drawback. For this reason semitendinosus & gracillis
graft can be a good alternative for ACL reconstruction.
In this context we are doing ACL reconstruction by
semitendinosus & gracillis using quadruple graft at NITOR
for last few years. But we did not have any study regarding
this technique. So, the purpose of my study is to evaluate
the outcome after reconstruction of ACL injury by
quadruple semitendinosus & gracillis graft.
METHODOLOGY
The study was carried out at National Institute of
Traumatology and Orthopaedic Rehabilitation (NITOR),
Dhaka, Bangladesh from January 2011 to December
2012.The study populations were the patients attending
at the above place for the treatment of torn anterior cruciate
ligament.A total of 10 patients met the following selection
criteria were selected consecutively from the study
population.Inclusion criterias were:Patients with ages
ranging from 15 - 40 years,
ACL injury leading to instability of knee which had
persisted for at least 01 month and failed to respond to
adequate conservative treatment.In doubtful cases
diagnosis confirmed by MRI. Exclusion criterias
were:Patients with a history of previous reconstruction of
the anterior cruciate ligament (ACL),Patients who had a
reconstruction for posterior, posterolateral or lateral
instability of the knee,Osteoarthritis of knee.
OBSERVATIONS AND RESULTS
This prospective study was carried out from January 2011
to December 2012 at NITOR. A total of 10 cases were
selected for the study, all these patients were male and
followed up for 6 months to 12 months. In this present
series the following results were obtained.
Age frequency.
Fig-1: Age distribution of the patients (n-10)
Mean age = 26.10±6.56. Out of the ten patients with ACL
injury the age range was 15-40 years and mean age was
26.10± 6.56 years. Among them 20% were more than 31
years of age and 20% were less than 20 years.
This bar chart describes the distribution of the subjects
by occupation. About one third (30%) subjects were
student, 60% were player, service holder and businessman
(20% each). Only 10% were day labour.
138 Md. Harun-Or-Rashid Khan, Mohammad Serajus Saleheen, M. Muniruzzaman, Md.Aminul Haque Pathan et al
The Journal of Bangladesh Orthopaedic Society

Right side involvement was 30% and left side involvement
was 70%.
Table-I
Associated injury of the subjects.
Associated injury No. of patients Percentage
Lateral collateral ligament 3 30
Medial collateral ligament 3 30
Medial meniscus injury 4 40
Total 10 100
This table describes associated injury along with ACL
injury. 30% were lateral collateral injury, 40% were medial
meniscus injury and another 30% were medial collateral
injury.
Table-II
Duration of suffering from injury to operation
(in months)
Duration of suffering Number of Percentage
thepatients
<5 3 30
5-10 3 30
11-15 2 20
21-25 1 10
25-30 1 10
Total 10 100
Mean-10.4 (±9.53) months.The outcome of ACL
reconstruction greatly depends upon time interval between
injury and operation. So duration of suffering was studied.
Data shows 30% patients have been suffering less than 5
months and 10% patients were suffering for 25-30 months.
Mean duration of suffering was 10.4 (±9.53) months.
Table-III
Hospital stay after operation (in days).
Hospital stay(days) Number of thepatients Percentage
<4 2 20
4-6 6 60
7-9 2 20
Total 10 100
Table shows 20% patient stayed in hospital after operation
less than 4 days. 60% patients stayed 4-6 days and only
20% patients stayed 7-9 days.
Table-IV
Complications of the patients.
Complication Number of thepatients Percentage
Infection 1 10
Endo button slippage 1 10
at femoral site.
Total 2 20
Early post operative period was uneventful in 80% cases.
One patient had infection at tibial screw site and the other
patient had endo button slippage at femoral site.
Tab1e-V
Functional score and result (n-10) Distribution of
patients according to Lysholm score
Case no. Result Functional score
1 Excellent 96
2 Poor 60
3 Good 85
4 Excellent 95
5 Good 85
6 Excellent 96
7 Good 85
8 Excellent 96
9 Fair 67
10 Excellent 97
In the present series excellent result were achieved in 5
patients, good results were achieved in 3 patients and fair
result was achieved in 01 patient, poor result were achieved
01 patient.
Bar Chart-1: Occupational distribution of patient (n-
10)
Result of Arthroscopic Anterior Cruciate Ligament Reconstruction by Semitendinosus & Gracillis Tendon Graft 139
VOL. 29, NO. 2, JULY 2014

Table-VI
Comparison of pre-operative and postoperative
Lysholm knee score.
Number of Mean ±SD p
the patients value
Pre-operative 10 55.30±5.05 0.001*
Postoperative 10 86.20 ±13.08
* Significant
Paired sample ‘t’ test.
Preoperative Lysholm knee score was 55.30 (SD±5.05) and
post operative score was 86.20 (SD± 13.08). Preoperative
versus postoperative Lysholm scores showed significant
improvement (p<0.001).
Outcome of the clinical evaluation after six months:
Preoperative clinical evaluation showed that all patients
had mild to moderate pain. Lachman test was positive in
all patients among them grade II was 70% and grade three
was 30%. All patients had anterior drawer test positive.
80% patient complained of giving way. Pivot shift test
was positive in 40% cases. Mc Murray test was positive
in 30% cases. 60% patients had less than 135° knee flexion
and 40% had 130° flexion preoperatively.
Postoperatively Lachman test improved significantly.
Grade I was in 80% cases and grade II was in 20% cases.
Anterior drawer was positive in 20% cases. Pivot shift
test was positive in only 10% cases. After operation 70%
had 135° knee flexion and 30% had 130° flexion.
Table-VII
Final outcome of the patients.
Final outcome Number of Percentage
thepatients
Satisfactory 8 80
Unsatisfactory 2 20
Total 10 100
This table demonstrates the final outcome of the patients.
Out of 10 patients, 8 (80%) were satisfactory, 2 were
unsatisfactory (20%) result.
DISCUSSION:
The importance of the ACL in the maintenance of the
stability of knee is well known. Active individual who have
a torn ACL are frequently troubled by chronic instability
and recurrent episode of giving way, which often are
associated with intra-articular injuries4.
In the present study, all the subjects were male with mean.
age 26.10 (± 6.56) years and the minimum and maximum
ages were 15 and 40 years respectively.
Eriksson et al6 made study over 164 patients. In his study
age ranges were between 15 and 45 years. (Mean 25.7±
6.9years) which is comparable with present study.
In the present study more two third (70%) of the patients
were Students, service holder and business men. 20%
were player in these group. Only 10% patients were day
labour.
The cause of injury was sporting activity in 70% cases
and 30% was due to accidental fall.
Out of 10 patients right knee involvement was 3 (30%) and
left knee involvement was 7 (70%). In the present study
30% had medial collateral ligament injury, 30% had lateral
collateral injury and 40% had medial meniscus injury. Those
patients who had meniscal injury and underwent partial
menisectomy shows poor results. In my study mean
duration of the suffering from the injury to operation were
10.4 (± 6.56) months ranging from 3 and 30 months.
In this study mean hospital stay after operation was 4.9 (±
1.66) days. Buss et al (1993) investigated 67 ACL
reconstructions and found mean hospital stay was 5 days
(range 3 to 8 days).
Preoperative versus post operative Lysholm knee score
in this series shows significant improvements (p<0.001).
Preoperative and postoperative Lysholm scores were 55.30
(±5.05) and 86.20 (±13.08) respectively.
Wagner et al.7 also showed significant improvement of
the Lysholm score in his study (P<0.001). According to
Williams et al.8 study mean Lysholm score improved from
55 points preoperative to 91 points after 2 year follow-up
over 120 patients. This is comparable with present study.
Regarding final outcome of the patients, present series
shows out of 10 patients 8 (80%) were satisfactory and 2
(20%) were unsatisfactory result. In the 90s, hamstring
reconstruction with double and quadrupled
semitendinosus and gracillis tendons gained popularity
as a result of decreased graft harvesting morbidity and
smaller incisions. It was also shown that biomechanically,
double and quadruple tendons have superior strength
and stiffness compared with bone patellar tendon-bone
grafts and the native ACL5.
140 Md. Harun-Or-Rashid Khan, Mohammad Serajus Saleheen, M. Muniruzzaman, Md.Aminul Haque Pathan et al
The Journal of Bangladesh Orthopaedic Society

CONCLUSION
ACL injury frequently occurs in young adult population,
which reduces activity level and become economic burden.
So, early reconstruction of the ACL is necessary to make
them fit and return to their original activity level.
Graft choice is crucial in reconstruction of ACL injury.
Quadruple semitendinosus& gracillis tendon graft has an
ultimate tensile load to be as high as 4108N.
Quadruple semitendinosus & gracillis graft has got
advantages over other grafts in respect of strength,
stability, less donor site morbidity and anterior knee pain.
The procedure can be done by, where arthroscopic
facilities are available.
REFERENCES
1. Reckling FW, Munns SW 1990, ‘Knee’ in Reckling FW,
Reckling JB, Mohn MP (eds), Orthopaedic Anatomy
and ‘Surgical Approaches, Mosby Year Book, St. Louis,
U.S.A. pp. 357.
2. Miller III RH 2003, ‘Knee injuries’ in Canale ST, Daugherty
K, Jones L, Campbell’s Operative Orthopaedics, 10th ed.
Vol.3, Mosby Yearbook, Philadelphia, USA, pp.2278-80.
3. Solomon L 2001, ‘injuries of the knee and Leg, in Louis
Solomon, David J, Warwick, Selvenduria Nayagum, Apley’s
System of Orthopaedics and Fracture, 8th ed, Arnold,
London, pp. 705.
4. Buss DD, Warren RF, Wickiewicz TL, Galinat BJ,
Panariello R 1993, ‘Arthroscopically Assisted
Reconstruction of the Anterior Cruciate Ligament with
use of Autogenous Patellar-Ligament Graft’, The Journal
of Bone and Joint Surgery, Vol. 75-A, No. 9, pp. 1346.
5. Leong DKH, Lee WP, Low BY 2005, ‘A Historical Review
of ACL Surgery’, The Journal of the Asean Orthopaedic
Association, Vol. 17, No. 1, pp. 9-14.
6. Eriksson k, Anderberg P, Hamberg P, Bredenberg M,
Westman I, Wredmark T 2001, “A comparison of
quadruple semitendinosus and patellar tendon graft in
reconstruction of the Anterior cruciate ligament” , The
Journal of Bone and Joint Surgery, Vol.83B, pp.348-354.
7. Wagner M, Kaab MJ, Schallock J, Haas NP, Weiler A
2005, ‘Hamstring Tendon Versus Patellar Tendon ACL
Reconstruction Using Biodegradable Interference Fit
Fixation,, The American Journal of Sports Medicine, Vol.
33, No. 9, pp. 1327.
8. Williams III RJ, Hyman J, Petrigliano F, Rozental ‘I.
Wickiewicz TL 2004, ‘ACL Reconstruction with a Four-
Strand Hamstring Tendon Auto-graft’, The Journal of
Bone and Joint Surgery, Vol. 86-A, No. 2, pp 225.
Result of Arthroscopic Anterior Cruciate Ligament Reconstruction by Semitendinosus & Gracillis Tendon Graft 141
VOL. 29, NO. 2, JULY 2014

INTRODUCTION
In 1979, Schatzker et al. introduced a clsssification for
tibial plateau fractures that distinguished low –energy split
depression fractures from high energy bicondylar
(Schatzker type V and VI) fractures. Complex tibial plateau
fractures (Schatzker type V and VI) are one of the most
challenging problems in orthopaedic surgery. The Ilizarov
technique solves many of these problems encountered in
the management of such fractures and provides a method
for closed reduction and fixation that does not necessitate
excessive soft tissue stripping3,12.
These fractures involve both medial and lateral condyles
with various amount of articular surface comminution are
often associated with severe soft tissue injury that can
frequently result in compartment syndrome and are
frequently open fractures. Operative management of these
injuries is invariably complicated by the condition of the
soft tissue envelop of the proximal tibia.
Original Article
Management of Complex (Schatzker-
Type V And VI) Tibial Plateau Fractures
by Ilizarov Method
Mir Hamidur Rahman1, Gazi Md. Enamul Kabir2, Monaim Hossen3, Shaymol Deb Nath4, Md.
Mofakhkharul Bari5
ABSTRACT
We studied 46 tibial plateau fractures (Schatzker Type V and VI), managed by Ilizarov fixator in National Institute
of Traumatology & Orthopaedic Rehabilitation (NITOR), Pink unit-II (Ilizarov, Deformity Correction and Reconstruction
Unit), Dhaka, Bangladesh. All fractures were the result of high energy trauma. Duration of study was 6 and a half
years. Using The Knee Society Clinical Rating System, 32 knees were rated as excellent, 13 as good and 1 as fair.
Pin sites inflammation and pin loosening were the commonest complications in our study. This study emphasizes
the clinical success and low morbidity associated with the use of Ilizarov external fixatior.
Key ward: Tibial plateau fracture, Soft tissue injury, External fixator, Functional outcome.
The risk of wound complication following open reduction
and internal fixation is notably high owing to extensive
soft tissue dissection. Alternatively application of Ilizarov
technique minimizes soft tissue dissection and provides
adequate fracture stabilization to allow early movement of
joint and correction of any malalignment. With this
technique soft tissue complication particularly surgical
site infections are expected to be significantly reduced.
The purpose of this study is to evaluate the management
of these complex injuries with the Ilizarov technique,
functional outcome and complications associated with this
treatment method2,6.
The treatment goal for bicondylar tibial plateau fracture
with Ilizarov method is to obtain a stable, aligned, painless
and mobile knee and to minimize the risk of post-traumatic
osteoarthritis. Ring fixator like Ilizarov system, with
tensioned fine wires, utilizes beam loading to creat
uniformed support for the joint and stable fracture
immobilization to achieve fracture union.3,4,5
1. Asst. Professor, OSD, DGHS Attached Abdul Malek Ukil Medical College, Norshidi
2. Junior Consultant, 250 Beded General Hospital, Narayangonj
3. Assistant Professor, Department Orthopaedic Surgery, NITOR, Dhaka
4. Associate Professor, Department Orthopaedic Surgery, NITOR, Dhaka
5. Professor, Department Orthopaedic Surgery, NITOR, Dhaka
Correspondence: Dr. Mir Hamidur Rahman, Asst. Professor, OSD, DGHS Attached Abdul Malek Ukil Medical College, Norshidi
142 The Journal of Bangladesh Orthopaedic Society

MATERIALS & METHODS
This retrospective study was conducted at Pink Unit –II
(Ilizarov, Deformity Correction & Reconstruction
Unit),NITOR, Dhaka, Bangladesh. Number of total patient
was 46. The duration of study was 6 and half years from
January, 2006 to, July, 2012. All fractures occurred after
high energy trauma including RTI and falls from height of
>2.5 meter. There were 44 male and 2 female with an average
age of 40 years (range 21 to 62 years). 34 were closed
fractures and 12 were open fractures. Soft tissue injury
for the closed fractures was classified according to
Tscherne and Gotzen, and open fracture was classified
according to Gustilo and Anderson. Inclusion criteria were
patients of skeletal maturity with complex tibial plateau
fractures that were treated with Ilizarov external fixator.
Patients were excluded if they had any of the following:
(1) a condition that would impede the rehabilitation process
of the patient – for example, acetabulum fracturs that
would require prolonged immbolization; (2) concomitant
injuries that could alter the functional outcome of the
patient- for example, ipsilateral femoral shaft fractures; (3)
previous major trauma, surgery or deformity of the affected
knee. The preoperative diagnostic approach was to
determine the severity and the extension of the osseous
damage. Plain radiograph were supplemented in all cases
by biplane tomograms. Computed tomography scan was
used in 30 fractures and magnetic resonance imaging was
used in 4 fractures.
Surgical Technique:
The objective was to accurately reduce the condyles in
relation to one another and to reduce and stabilize the
tibial shaft beneath the reduced condyles. Anatomical
reduction of the joint surface was a secondary goal
that was often accomplished percutaneously or
through limited approach. Condylar reduction was
assisted by longitudinal traction on the fracture table
with application of the varus or vulgus forces. Large
pointed reduction forceps applied percutaneously help
to obtain accurate condylar reduction and compression
(Ligamentotaxis).
After reduction of the condyles, counter-opposed olive
wires through the fragments were used to achieve
interfragmentary compression. Three to four wires at least
1.5 cm. from the joint line, with an overall divergence of an
angle at least 60 degree, were introduced for stabilization
of the condylar and metaphyseal fragments. Frequently
we used an olive wire through the fibular head obliquely
into the lateral tibial condyle, taking advantages of the
buttress effect that fibular head offers to the lateral column
of the tibia. A 5/8 ring was attached to allow greater knee
flexion and wire tensioning was performed under C-ARM
guide to directly view the adequacy of the reduction and
avoid over-compression.
Middle construct was made with a full ring two to three
cm. distal to diaphyseal fracture site and distal ring was
placed at a lower level and secured to a transfixation
reference wire positioned parallel to the ankle joint to
ensure mechanical axis of the tibia. Now second and third
ring were joined by four connecting rods, then metaphysio-
diaphyseal alignment was corrected under C-ARM
control. Finally 1st and 2nd ring were joined by four
connecting rods.
Post-Operative Care:
All patients were instructed on fixator care and taught to
do daily pin sites cleansing with rectified sprit and started
on passive range of motion exercise on the 2nd post-
operative day and active motion by 1 week. Ankle equinus
deformity was prevented by meticulous wire placement
technique, active joint mobilization post-operatively and
splinting of the foot in a neutral position. Early range of
movement exercise for the knee and mobilization with
crutches was encouraged in all cases. Partial to full weight-
bearing was increased as tolerated. Patients with marked
articular comminution were kept partial-weight bearing for
6 weeks.
OBSERVATION AND RESULTS
The mean patient’s age at the time of injury was 40 years
(range 22-62 years). Average duration of hospitalization
was 10 days (6 to 14 days).The average follow-up was 14
months (range- 12 to 18 months). All fractures united in
an average time of 14 weeks (ranges 10 to 20 weeks).
Fixators were removed after union of fractures. The
radiographic reduction of fractures was rated as excellent
in 38 and good in 8 according to Rasmussen’s criteria.
Using The Knee Society Clinical Rating system, 34 were
rated as excellent, 11 as good and 1 as fair. The average
total range of knee flexion was 120 degree (range 0 to 140
degree). 34 patients had a normal walking pattern and
were able to climb stairs normally. Five patients had
clinically demonstrable grade 2+ medial-lateral instability.
Only two were symptomatic but had no functional
handicap. 8 had mild or occasional pain. In 4 patients,
walking was limited, and needed walking aids. Pin-tract
infection was mild and common but controlled by
dressing and antibiotics
Management of Complex (Schatzker-Type V And VI) Tibial Plateau Fractures by Ilizarov Method 143
VOL. 29, NO. 2, JULY 2014

Fig.-1: Complex (Schatzker-Type VI) tibial plateau
fractures of a 24 years old boyFig: 2. 2 weeks after application of Ilizarov external
fixator.
Fig.-3: 16 weeks after application of Ilizarov external
fixator.
Fig.-4: After removal of Ilizarov external fixator (at 20
weeks)
144 Mir Hamidur Rahman, Gazi Md. Enamul Kabir, Monaim Hossen, Shaymol Deb Nath, Md. Mofakhkharul Bari
The Journal of Bangladesh Orthopaedic Society

Follow-Up:
After discharge, patients attended the Ilizarov clinic in
NITOR held on every Sunday. During follow-up, the
patients were assessed in term of range of motion, fracture
union clinically and radiologically, any loss of reduction
radiologically, any hardware related complications like wire
breakage, surgical sites infection, complications related
to the surgery like nerve injury from inadvertent pin
placement. Serial standing radiograph of the knee and leg
in antero-posterior and lateral plane were performed at 6th
week, 12th week, 18th week, 24th week and 28th week post-
operatively. The Ilizarov fixator was removed once
radiographic evidence of union was established. Functional
outcome was determined using The Knee Society Clinical
Rating Score.
DISCUSSSION
The goals of operative treatment of these fractures include
anatomic reduction for restoration of articular congruity
and alignment, and stable fixation to allow early motion.
However the classic dual plate osteosynthesis has been
associated with potentially devastating complications such
as fixator failure, malunion, nonunion, joint stiffness,
secondary post-traumatic osteoarthritis, infection, and
most importantly severe soft tissue complications ranging
from 23 to 87.5%2,9,12.
The management of intraarticular fractures in the tibial
plateau is inherently complex. The restoration of articular
congruity is mandatory, and careful treatment of soft tissue
is as important as bone. Over the past few decades, a
number of evolving treatment modalities ranging from
traction to cast immobilization to open reduction and
internal fixation have been used with mixed results. No
treatment modality has been produced consistently good
results, nor has any allowed both stable fixation and
preservation of remaining soft tissues. In an attempt to
achieve both stable fixation and preserving the remaining
soft tissue many surgeons have chosen to use indirect
reduction and external fixation. Ilizarov external fixation
has been introduced and shown to be effective in the
treatment of these difficult fractures3,8,12.
The Ilizarov fixator offers several advantages that include
minimizing further injuries to soft tissue envelop, feasible
surgery even in the presence of badly injured soft tissue,
adequate stability to allow early post-operative
mobilization, and minimizing risk of joint stiffness. The
disadvantages include the need for constant pin site care,
pin sites infection and risk of septic arthritis from incidental
intracapsular pin placement and potential risk of common
peroneal nerve injury from poor pin placement3,9.
Using Rasmussen criteria for radiographic assessment,
excellent to good reduction was achieved in all our cases,
which is superior to all similar series. The mean range of
movement reported by Guadinez et al. was 85 degree and
by Morandi and Pearse was 113 degree (9).All patients
reported by Zecher et al. achieved at least 90 degree.The
average knee range of movement in our study was greater
than comparable studies, despite the presence of 2 cases
of knee stiffness. When applying The Knee Society Rating
System, the average knee score in our study was 80.2 and
average functional score was 83.8, and the average knee
rating was 82.5. Mikulak et al. reported a mean score of
78.5, a mean functional score of 81.9, and an average knee
rating of 80.2 in their 24 patients8. Kumar and Whittle
reported a mean score of 83 and a mean functional score
of 69 (79%) in 45 patients6.
Several published studies have shown decreased
complication with treating bicondylar tibial plateau
fractures with the fine-wire external fixator. Kataria et al.
reported on a series of 38 patients treated with small wire
external fixator and had no incidences of non-union or
septic arthritis. In series by Dendrinos 24 patients were
treated with Ilizarov circular external fixator, and there was
no incidence of non-union, osteomyelitis or septic arthritis.
Chin et al. reported similar results of 18 patients, none of
whom developed wound dehiscence, infection,
osteomyelitis or septic arthritis1. The current series is
comparable to these studies in that no cases of wound
dehiscence, infection, osteomyelitis or septic arthritis were
encountered.
Pin tract infection was the main drawback when using an
external fixator to treat fractures. In meta-analysis of 10
studies with a total of 381 patients, Hutson et al.
encountered 38 cases superficial pin tract infection (10%),
5 septic arthritis (1%), and 13 deep infection (4%).
Limitations of this study include the small number of cases
and the retrospective nature of the review. Also, the
exclusion of patients with certain concomitant injuries
could lead to a selection bias, possibly omiting patients
with more severe injuries.
CONCLUSION
Complex tibial plateau fractures fixation by Ilizarov
technique has become increasingly popular over the past
decade. The degree of soft tissue injury associated with
these fractures is an important determinant for both the
choice of treatment modality and prediction of treatment
outcome. Ilizarov method is a safe and effective option for
the treatment of difficult Schatzker type V & VI tibial
Management of Complex (Schatzker-Type V And VI) Tibial Plateau Fractures by Ilizarov Method 145
VOL. 29, NO. 2, JULY 2014

plateau fractures. This method minimizes soft tissue
complication and favours bony union with an acceptable
return of function. Complications are mainly related to pin
tract sepsis. We feel that the technique merits a place in
the armamentarium for managing.
REFERENCES
1. Chin TYP, Bardana D, Bailey M, Williamson OD, Miller
R, Edward ER, Esser MP. Functional outcome of tibial
plateau fractures treated with the fine-wire fixator. Injury
Int. J. Care Injured 2005;36:1467-75.
2. Dendrinos GK, Kontos S, Katsenis D ,Dalas A. Treatment
of High energy tibial plateau fractures by the Ilizarov
Circular fixator. J Bone Joint Surg 1996;78-B:710-17.
3. El Barbary H, Abdel Gani H, Misbah H, Salem K. Complex
tibial plateau fractures treated with Ilizarov external fixator
with or without minimal internal fixation. International
Orthopaedics (SICOT) 2005;29:182-185.
4. Ilizarov G.A. The treatment of fractures, theoretical
considerations, experimental studies and clinical
application of the apparatus. In: Ilizarov G. A., Green
SA, eds. Transosseous osteosynthesis: theoretical and
clinical aspects of the regeneration and growth of tissues.
Berlin: Springer-Verlog 1992:369-452.
5. Katsenis D, Dendrinos G, Kouris A, Savas N,
Schoinochoritis N, Pogiatzis K. Combination of fine wire
fixation and limited internal fixation for high energy tibial
plateau fractures: functional results at minimum 5-year
follow-up.J Orthop Trauma 2009; 23: 493-501.
6. Kumar A, Whittle AP. Treatment of complex (Schatzker
type-VI) fractures of tibial plateau with circular wire
external fixator: retrospective case review. J Orthop Trauma
2000;14(5):339-44.
7. Marsh JL, Smith ST, Do TT. External fixation and limited
internal fixation for complex fractures of the tibial plateau.
J Bone Joint Surg Am 1995;77:661-173.
8. Mikulak SA, Gold SM, Zinar DM. Small wire external
fixation with high-energy tibial plateau fractures. Clin
Orthop Relat Res 1998;365:230-238.
9. Morandi MM, Pearse MF. Management of complex tibial
plateau fractures with the Ilizarov external fixator. Thec
Orthop. 1996; 11:125-131.
10. Rasmussen PS.Tibial condylar fractures: Impairment of
knee joint stability as indication for surgical treatment. J
Bone Joint Surg. 1975;55(A):1331-1350.
11. Rationale of The Knee Society Clinical Rating System.
Clin Orthop. 1989;248:13-14.
12. Young MJ, Barrack RL. Complications of internal fixation
of tibial plateau fractures. Orthop Trauma 2005;19:
241-48.
146 Mir Hamidur Rahman, Gazi Md. Enamul Kabir, Monaim Hossen, Shaymol Deb Nath, Md. Mofakhkharul Bari
The Journal of Bangladesh Orthopaedic Society

Original Article
A diabetic foot is a foot that exhibits any pathology
resulting directly from diabetes mellitus. Presence of
several characteristic diabetic foot pathologies is called
diabetic foot syndrome.
The most serious foot complications in diabetes are:
• Diabetic foot ulceration. It occurs in 15% of all patients
with diabetes and precedes 85% of all diabetes-related
lower leg amputations.
• Diabetic foot infections
• Neuropathic osteoarthropathy of the foot
Wound healing assessment of diabetic ulcers:
• Damage to blood vessels and impairment of the
immune system from diabetes makes it difficult to heal
diabetic ulcers. Bacterial infection of the skin,
connective tissues, muscles and bones then occur.
These infections can develop into gangrene.The only
treatment for this isamputation of the foot or leg. If
the infection spreads to the bloodstream, this process
can be life-threatening.
• People with diabetes must be fully aware ofhow to
prevent foot problems before they occur, to recognize
problems early, and to seek the right treatment when
problems do occur. Although treatment for diabetic
foot problems has improved, prevention - including
good control of blood sugar level - remains the best
way to prevent diabetic complications.
Causes of Diabetic Foot:Several risk factors causing
diabetic foot are -
• Footwear: Poorly fitting shoes are a common cause
of diabetic foot problems.
- If the patient hasred spots, blisters, corns,
calluses, or consistent pain associated with
wearing shoes, new properly fitting footwear
must be obtained as soon as possible.
Management of Diabetic Foot
Noor Mohammad1, Md. Golam Sarwar2, Anjon Lal Ghosh3, MA Sabur4, Shibasis Basak5, Mollah
Eshadul Haq6, Shahidul Haq7
1. Associate Professor, BIHS General Hospital, 125/A, Darus Salam Road, Mirpur-1,Dhaka-1216
2. Associate Professor, Department of Orthopaedic Surgery, DMCH, Dhaka
3. Assistant Professor, Department of Orthopaedic Surgery, NITOR, Dhaka
4. Assistant Professor, Department of Orthopaedic Surgery, ZH Sikder Women’s Medical College Hospital
5. Registrar, DMCH, Dhaka
6. Assistant Professor, Department of Orthopaedic Surgery, SSMCH, Dhaka
7. Asst. Professor, Department of Surgery, Cox’s Bazar Medical College, Chittagong
Correspondence: Dr. Noor Mohammad, Associate Professor, BIHS General Hospital, 125/A, Darus Salam Road, Mirpur-1,Dhaka-1216,Mobile: +8801710562467, E-mail: [email protected]
- If the patient has common foot abnormalities such
as flat feet,bunions, or hammertoes etc. prescription
shoes or shoe inserts may be necessary.
• Nerve damage: People with long-standing or poorly
controlled diabetes are at risk for having damage to
the nerves in their feet (peripheral neuropathy).
• Because of the nerve damage, the patient is unable to
feel their feet normally. Also, they may be unable to
sense the position of their feet and toes while walking
and balancing.
• A person with diabetes may not properly sense minor
injuries (such ascuts, scrapes, blisters), signs of
abnormal wear and tear (that turn into calluses and
corns), and foot strain.
• Poor circulation: When poorly controlled, diabetes
can lead to atherosclerosis causing poor blood flow to
injured tissues.Thus healing does not occur properly.
• Trauma to the foot: Any trauma can increase the risk
for a more serious problem to develop.
• Infections Athlete’s foot, a fungal infection of the
skin or toenails, can lead to more serious bacterial
infections. Ingrown toenails should be treated by an
appropriate doctor.
• Smoking: Smoking causes damage to smallblood
vessels in the feet and legs. This damage can disrupt
the healing process and can be a major risk factor for
infections and amputations.
Symptoms of Diabetic Foot:
• Persistent pain is a symptom ofsprain, strain, bruise,
improperly fitting shoes, infection etc.
• Redness can be a sign of infection, especially when
surrounding a wound.
VOL. 29, NO. 2, JULY 2014 147

• Swelling of the feet or legs can be a sign of underlying
inflammation or infection or poor venous circulation.
Other signs of poor circulation include:
- Pain in legs or buttocks that increases with
walking but improves with rest (claudication).
- Hair no longer growing on the lower legs and feet
- Hard shiny skin on the legs
• Localized warmth can be a sign of infection or
inflammation.
• Any break in the skin canresult from abnormal wear
and tear, injury, or infection. Calluses,corns may be a
sign of chronic trauma.
• Drainage of pus from a wound is usually a sign of
infection.
• A limp can be sign of joint problems, serious infection,
or improperly fitting shoes.
• Fever or chills in association with an wound can be a
sign of a limb-threatening infection.
• Redness spreading out from a wound is a sign of a
progressively worsening infection.
• New or lasting numbness in the feet or legs can be a
sign of nerve damage from diabetes.
Exams and Tests:
Medical evaluation should include a thorough history and
physical examination and may also include laboratory tests,
x-ray studies of circulation in the legs, and consultation
with specialists.
• History and physical examination:Detailed personal
family and clinical history is very important for
diagnosis. The examination should include the
patient’s vital signs, examination of the sensation in
the feet and legs, an examination of the circulation in
the feet and legs.
• Laboratory tests include :
1. Complete blood cell count which will assist in
determining the presence and severity of infection. A
very high or very low white blood cell count suggests
serious infection.
2. Random blood sugar,FBS with 2 hrs. PP either by
fingerstick or by a laboratory test. Depending on the
severity of the problem, the doctor may also order.
3. Kidney function tests.
4. Blood chemistry studies (electrolytes)
5. Liver enzyme tests.
6. Heart enzyme tests to assess whether other body
systems are working properly in the face of serious
infection.
• X-rays of the leg and footto assess the condition of
bones andjoints, damage from infection, foreign
bodies in the soft tissues. Gas in the soft tissues
indicates gangrene - a very serious, potentially life-
threatening or limb-threatening infection.
• Ultrasound: Doppler ultrasound to see the blood flow
through the arteries and veins.
• Consultation:The vascular surgeon and/or an
orthopedic surgeon may be asked for consultation.
• Angiogram: If the vascular surgeon determines that
the patient has poor circulation in the lower
extremities, an angiogram may be performed in
preparation for surgery to improve circulation.
DIABETIC FOOT CARE AND TREATMENT:
Self-Care at Home:
A person with diabetes should do the following:
• Foot examination:The patient should examine his foot
daily after any trauma, no matter how minor the trauma
is. A water-based moisturizer should be used every
day to prevent dry skin and cracking. He should wear
cotton or wool socks and avoid elastic socks,
• Eliminate obstacles: Remove any objects he islikely
to trip over or bump his feet on. Keep the sharp objects
on the floor picked up. Light the pathways used at
night - indoors and outdoors.
• Toenail trimming should be done with a safety
clipper leaving plenty of room out from the nail
bed.Help from a family member can be sought.
• Footwear: Wear sturdy, comfortable shoes whenever
feasible to protect your feet. If you have flat feet,
bunions, or hammertoes, you may need prescription
shoes or shoe inserts.
• Exercise: Regular exercise will improve bone and joint
health in your feet and legs, improve circulation to
your legs, and will also help to stabilize your blood
sugar levels.
• Smoking: Smoking accelerates damage to blood
vessels, especially small blood vessels leading to poor
circulation, which is a major risk factor for foot
infections and ultimately amputations.
• Diabetes control: Following a reasonable diet, taking
medications, checking blood sugar regularly and
maintaining good communication with your physician
are essential in keeping your diabetes under control.
Consistent long-term blood sugar control to near
normal levels can greatly lower the risk of damage to
your nerves, kidneys, eyes, and blood vessels.
MEDICAL TREATMENT:
• Antibiotics: If the doctor determines that a wound or
ulcer on the patient’s feet or legs is infected, antibiotics
will be prescribed to treat the infection or the potential
infection. It is very important that the patient take the
148 Noor Mohammad, Md. Golam Sarwar, Anjon Lal Ghosh, MA Sabur, Shibasis Basak, Mollah Eshadul Haq, Shahidul Haq
The Journal of Bangladesh Orthopaedic Society

entire course of antibiotics as prescribed. For limb-
threatening or life-threatening infections, the patient
will be admitted to the hospital and given IV
antibiotics. Less serious infections may be treated
with pills as an outpatient. The doctor may give a
single dose of antibiotics as a shot or IV dose prior to
starting pills in the clinic or emergency department.
• Referral to wound care center: Many of the larger
community hospitals now have wound care centers
specializing in the treatment of diabetic lower extremity
wounds and ulcers. In these multidi ciplinary centers,
professionals of many specialties work as members
of a team in developing a treatment plan for the wound.
Treatment plans may include surgical debridement of
the wound, improvement of circulation through
surgery or therapy, special dressings, and antibiotics.
The plan may include a combination of treatments.
Referral to podiatrist or orthopedic surgeon: If the patient
has bone-related problems, toenail problems, corns and
calluses, hammertoes, bunions, flat feet, heel spurs,
arthritis, or have difficulty with finding shoes that fit, a
physician may refer you to one of these specialties.
Care of the Diabetic Foot:
Diabetic foot problems are a major health concern and are
a common cause of hospitalization.Most foot problems
that people with diabetes face arise from two serious
complications of the disease: nerve damage and poor
circulation. The lack of feeling and poor blood flow can
allow a small blister to progress to a serious infection in a
matter of days. Chronic nerve damage (neuropathy) can
cause dry and cracked skin, which provides an opportunity
for bacteria to enter and cause infection. The
consequences can range from hospitalization for
antibiotics to amputation of a toe or foot. For people with
diabetes, careful daily inspection of the feet is essential to
prevent damaging foot problems.
General Care of the Diabetic Foot:
• Never walk barefoot. Thus decrease the chances of
injuries leading to infection.
• Wash your feet every day with mild soap and warm
water. Test the water temperature with your hand first.
Dry the feet & toes with a clean towel.
• Use lotion to keep the skin soft and moist. This
prevents cracks & decreases the risk of infection.
• Trim toe nails carefully & avoid cutting corners. If
you find an ingrown toenail, seek advice.
• Do not use antiseptic solutions orheating pads.
• Do not put your feet on radiators or in front of the
fireplace.
• Keep your feet warm. Do not wet your feet in snow or
rain. Wear socks & shoes in winter.
• Do not smoke. Smoking damages blood vessels and
decreases theavailability of oxygen to the feet. In
combination with diabetes, it significantly increases
the risk of amputation.
Inspection:
• Inspect your feet every day.
• Look for puncture wounds, bruises, pressure areas,
redness, warmth, blisters, ulcers, scratches, cuts, and
nail problems.
• Get someone to help you or use a mirror. You may not
feel that damage has occurred to the skin.
• Look at and feel each foot for swelling. Swelling in
one of the feet and not the other is an early sign that
you may be experiencing early stages of Charcot foot.
This can occur in people with nerve damage. It can
destroy the bones and joints.
• Examine the bottoms of your feet and toes.
A few typical diabetic lesions in feet:
Management of Diabetic Foot 149
VOL. 29, NO. 2, JULY 2014

150 Noor Mohammad, Md. Golam Sarwar, Anjon Lal Ghosh, MA Sabur, Shibasis Basak, Mollah Eshadul Haq, Shahidul Haq
The Journal of Bangladesh Orthopaedic Society
Shoe wear: Choose & wear the proper shoes. Poor fitting
shoes cause ulcers leadingto infection.
• Buy new shoes late in the day when your feet are
larger. Buy shoes that are comfortable without a
“breaking in” period.
• Check how your shoe fits in width, length, back,
bottom of heel, and sole. Have your feet measured
every time you buy new shoes. Your foot will change
shape over the years and you may not be the same
shoe size you were 5 years ago.
• Avoid pointed-toe styles and high heels. Try to get
shoes made with leather upper materias.l
• Wear new shoes for only 2 hours or less at a time. Do
not wear the same pair every day.
• Inspect the inside of each shoe before putting it on.
Do not lace your shoes too tightly or loosely.
• Avoid long walks without taking a break, removing
your shoes and socks and checking for signs of
pressure (redness) or ulcers.
ORTHOTICS
An accommodative orthotic made from a soft material called
plastizote is commonly prescribed. The orthotics should
not be hard, as this will increase the risk of a pressure
ulcer. The orthotic can be transferred from shoe to shoe
and should be used at all times when standing or walking.
REFERENCES:
1. Reiber, G.E., Boyko, E.J., and Smith, D.G. 1995. Lower
extremity foot ulcers and amputations in diabetes.In
Diabetes in America.M.I. Harris and M.P. Stern, editors.
U.S. Government Printing Office. Bethesda, Maryland,
USA. 409–428.
2. Falanga V. Wound healing and its impairment in the diabetic
foot. Lancet.2005;366:1736–1743.
3. Boulton A.J., Vileikyte L., Ragnarson-Tennvall G.,
Apelqvist J. The global burden of diabetic foot
disease.Lancet.2005;366:1719–1724.
4. Ramsey SD, Newton K, Blough D, et al. Incidence,
outcomes, and cost of foot ulcers in patients with diabetes.
Diabetes Care 1999;22:382–387.
5. Bartus CL, Margolis DJ. Reducing the incidence of foot
ulceration and amputation in diabetes.CurrDiab Rep
2004;4:413–418.
6. Apelqvist J, Bakker K, van Houtum WH, Nabuurs-
Franssen MH, Schaper NC, International Working Group
on the Diabetic Foot International consensus and practical
guidelines on the management and the prevention of the
diabetic foot. Diabetes Metab Res Rev 2000;16(Suppl.
1):S84–S92.
7. Singh N, Armstrong DG, Lipsky BA. Preventing foot
ulcers in patients with diabetes.JAMA 2005;293:217–
228.

INTRODUCTION
The management of chronic osteomyelitis continues to
pose a major challenge for orthopaedic surgeons. Chronic
Osteomyelitis of child is most commonly of
haematogenous origin but in adult it is commonly occur
after trauma in relation with either open # or to internal
fixation.
Because of the avascular nature of sequestrum,
osteomyelitis is difficult to treat and can be associated
with high morbidity and possible mortality for the patient.
Treatment is aimed at resolution of infection and
maximization of patient function.
The treatment of chronic osteomyelitis significantly
advanced with the use of muscle flaps and vascularized
bone transfer to manage large open defect after
debridement.
Further advancement have included –
1. Antibiotic beads to manage dead space in staged
reconstruction.
2. The use of ext. fixator in the illizarov technique of SK
reconstruction.
Original Article
We studied prospectively a consecutive series of 16 patients with chronic osteomyelitis. All patients had a
surgical intervention before coming to the hospital. All patients had open wound. After doing culture & sensitivity
and antibiotics accordingly patient didnot improved satisfactorily but after removal of dead and infected bone
patient improved dramatically and only one patient developed recurrence. There is always controversy about the
removal of sequestrum. We preferred to remove the dead and infected bone when there is line of demarcation
between living and dead bone.
Removal of Dead and Infected Bone in
Chronic Osteomyelitis is the Prime
factor to Control Infection – Early
Removal Decreases Morbidity
AHM Rezaul Haque,1 Debashis Biswas2, Shakeel Akter3, Takbirul Islam4, Debashis Ghosh5
Abstract
1. Assistant Professor, Dept. of Orthopaedics, Uttara Adhunik Medical College, Uttara, Dhaka.
2. Associate Professor, Dept. of Orthopaedics, Uttara Adhunik Medical College, Uttara, Dhaka.
3. Associate Professor, Dept. of Orthopaedics, Uttara Adhunik Medical College, Uttara, Dhaka.
4. Assistant Registrar, Dept. of Orthopaedics, Uttara Adhunik Medical College, Uttara, Dhaka.
5. Assistant Registrar, Dept. of Orthopaedics, Uttara Adhunik Medical College, Uttara, Dhaka.
Correspondence: Dr. A.H.M Rezaul Haque, Assistant Professor, Department of Orthopaedics, Uttara Adhunik Medical College,
Uttara, Dhaka.
3. There advancement has led to increased success in
the management of Chronic Osteomyelitis with success
rates > 90% in the literature2.
Principle of treatment is eradication of infection by
thorough debridement and appropriate antibioticcoverage.The main part of debridement is sequestrectomy.There is debate about the timing of sequestrectomy.Herewe have removed the sequestrum when there is line ofdemarcation between living and dead bone. The extent ofbone removal was decided during operation. We followpaprika technique. Early sequestrectomy causesimprovement of local wound, control of infection andgeneral condition of patient.
Patient & Method:
There were 10 men and 6 women with a mean age at
presentation of 20 (2- 52) years. The diagnosis of chronic
osteomyelitis was made on the basis of clinical presentation
and imaging. The aetiology of chronic osteomyelitis was
post traumatic in 6 patients, post traumatic post-operative
in 1 patient and haematogenous in 4 patients.
Depending on the anatomical location of disease the extent
of osteomyelitis, the patients’ age and comorbidity and
their preference of treatment option a decision was made
about surgical intervention.
VOL. 29, NO. 2, JULY 2014 151

Radiographs were done before operation for determining
the line of demarcation. The actual extent of bone resection
was determined at the time of surgery.
Debridement is aimed at removing all infected or necrotic
bone and soft tissues. All sinus tracts, scar tissues and
wound edges were excised and the adjacent soft tissues
were resected back to the tissue the bleed briskly. In
general, scalpel was used.
Bone was exposed to in extra periosteal. Periosteal
stripping avoided. Involucrum was kept in situ. Precise
bone debridement was performed until the paprika sign.
For endosteal infection debrided with curate and reamer.
In some situations, debridement of intramedullary canal
done by means of a trough in the bone.
In patient with extensive or circumferential involvement
of cortical bone, extensive resection of the involved area
was done. Infected perioseum was removed. In these
situations, stabilization done.
Tissue obtained at the time of debridement was sent for
culture and pathology. In some cases serial debridement
is done. After closing the wound, closed irrigation and
suction system, temporary antibiotic laden polymethyl
methacrylate beads, given in some cases. Bony defect
can be corrected by fibula graft and illizarov external
fixator.
After surgery, broad spectrum antibiotics were
administered I/V to all patients, this was modified after the
result C/S.
All patients were followed up regularly, with a mean length
of follow up of 20 months. Recurrence of infection was
diagnosed by local signs and symptom of infection, sinus
formation or drainage, a raised level of C reactive protein
or E S R or of systemic symptom such as fever for which
no other cause could be found.
RESULTS:
The clinical details and the outcome of treatment for all
patients are given in table. Despite accurate
microbiological diagnosis from intralesional biopsy and
of antibiotic therapy all patients had a recurrence of
infection.There were only one case of recurrence in
patients after removal of infected bone after one year.
In some patients, 2/3 times operations had to be
performed.
Mean age at first surgical intervention was 20 yrs (2 – 52),
75% (12) of the patients with chronic osteomyelitis came
from the rural community while 25% (4) came from urban
or common. Other bones involved are humerous and ulna.
The duration of osteomyelitis was determined as the time
from the first onset of symptom to the time of surgical
intervention.
Other determinant factor which might affect the likelihood
of recurrence of infection are aetiology, site of infection,
host comorbidity, duration of infection and causative
organism.
It is showing that most of the chronic osteomyelitis of
femur is of post traumatic. After accident, proper
surgical toileting is not done in remote area. First
surgical toileting and wound care is the most important
factor to prevent development of chronic osteomyelitis
after open fracture.
Fig.-1: Preoperative x-ray Fig.-2: Post operative x-ray Fig.-3: Bones to be removed during operation
152 AHM Rezaul Haque, Debashis Biswas, Shakeel Akter, Takbirul Islam, Debashis Ghosh
The Journal of Bangladesh Orthopaedic Society

Table 1
Pt/ Sl Age Aetiology Site Duration Stabilisation Follow up Recurrence Complication
1 20 PT & PO femur 6months Nail, Ext. fixator, illizarov* 4years No Knee stiffness
2 2 H tibia 3months LLBS 1year No Fibula Migration
3 24 PT femur 1year Illizarov 1year No Limb Shortening
4 12 H tibia 6months LLBS 1year No Nil
5 40 PT & PO tibia 8months Illizarov* 1year No Skin
6 10 PT & PO femur 3years Nail 1year No Ugly scar
7 12 PT Ulna 4years Graft and nail 6months No Nil
8 40 PT Humerous 1year Ext. Fixator 1year No Nil
9 3 H Tibia 6months LLBS 1year No Fibula migration
10 18 PT & PO Femur 10months Ext. Fixator 2years Once Nil
11 25 PT Tibia 1year Illizarov 3years No Nil
12 9 H Humerous 6months LABS 2years No Nil
13 19 PT Tibia 1year ORIF* 2year No Nil
14 52 PT Femur 2year ORIF* 1year No Nil
15 24 PT & PO R&U 6months Nail/Ext. 1year No Nil
16 16 PO Femur 2year IM Nail* 1year No Nil
PT- Post traumatic; PO- Post Operative; H- Haematogenous
*Final Fixation
Fig.-4: Segmental Bones remove Fig.-5: X Ray film before removal
DISCUSSION
It is essential to remove all necrotic and infected bone
when treating osteomyelitis. Many techniques have been
used to determine whether bone is alive or dead. The
technique most commonly used is the presence of bone
at the time of surgery and the presence of punctuate
bleeding. We used this technique to assess whether or
not the bone was viable.
In post -traumatic osteomyelitis where repeated surgical
clearance done chance of involucrum formation is
negligible. Repeated surgical clearance causes increased
local tissue scarring, decreased local vascularity, decreases
chance of neovascularisation so there by healing and union.
Waiting for separation of sequestrum makes the surgery
late.
Prolonged use of antibiotic causes antibiotic causes
antibiotic resistance, renal impairment, increases morbidity
and increased financial loss.
The duration of the infective process also adversely
affected the prognosis. It has been suggested that
Removal of Dead and Infected Bone in Chronic Osteomyelitis is the Prime factor to Control Infection 153
VOL. 29, NO. 2, JULY 2014

prolonged infection causes increased sclerosis and
scarring of the soft tissue envelope, making the infection
more resistant to treatment6.
The local or systemic immune response of some patient
may be suboptimal which may lead to higher recurrence
ratio7. It is very difficult to remove all dead and necrotic
material in a single sitting. After removing the main bulk of
infective foci body’s immune system can remove small
infective foci. This was seen in haematogenous
osteomyelitis.
It is showing that most of the chronic osteomyelitis of
femur is of post traumatic. After accident, proper surgical
toileting is not done in remote area. First surgical toileting
and wound care is the most important factor to prevent
development of chronic osteomyelitis.
CONCLUSION
Chronic osteomyelitis is a condition associated with
potentially high morbidity and has historically been very
difficult to cure. Treatment is geared toward resolution of
infection, while maintaining optimal function of the
patients’ extremity.
Although a variety of treatment options are available, no
set guideline or algorithm is available for treating patients
with chronic osteomyelitis. The main factor to control of
infection is removal of dead infected bone. As early as the
dead and infected bone can be removed as early as
infection can be controlled, so the morbidity decreases
and gives near normal function of extremity.
Ciernyand others stress that treatment should be
individualized to the patient. Management should take
into account the anatomic aspects of the patients’
infection, morbid medical condition and patients perception
of the expected outcome. This will allow the optimum
outcome in the management of these patients.
REFERENCES
1. Mathes SJ, Alpert BS, Chang N. Use of muscle flap in
chronic osteomyelitis: experimental and clinical correlation.
Plast Reconstr. Surg. 1982;69: 815-829.
2. Patazakis MJ, Mazur K, Wilkins J, Sherman R, Holtom
P. Septopal beads and autogenous bone grafting for bone
defects in patients with chronic osteomyelitis. Clin
Orthop 1993; 295: 112-118.
3. Cierny G, Mader JT, Penninck JJ. A clinical staging system
for adult osteomyelitis. Contemp Orthop 1985; 10:
17-37.
4. Mader JT, Cripps MW, Calhoun JH. Adult post-traumatic
osteomyelitis of the tibia. Clin Orthop 1999; 360: 14-21.
5. Daoud A, Saighi- Bouaouina A. treatment of sequestra,
pseudarthroses, and defects in the long bones of children
who have chronic hematogenous osteomyelitis. J Bone
Joint Surg. [AM] 1989; 71: 1448-1468.
6. West WF, Kelly PJ, Martin WJ. Chronic osteomyelitis:
factors affecting the results of treatment in 186 patients.
JAMA 1970; 213: 1837-42.
7. Kelly PJ. Infected non-union of the femur and tibia. Clin
Orthop North Am 1985; 15:1481-90.
154 AHM Rezaul Haque, Debashis Biswas, Shakeel Akter, Takbirul Islam, Debashis Ghosh
The Journal of Bangladesh Orthopaedic Society

Original Article
INTRODUCTION
Achilles tendon (AT) injuries may occur due to sports
injuries and about 10% to 25% of the complete AT ruptures
are not diagnosed1; accidental cuts by sharp household
tools, penetrating injuries, road traffic accidents, slipping
of the foot in toilet pans and spontaneous rupture; local
corticosteroid injection causes rupture after minimal
trauma2,3. Acute AT injury may be managed either
operatively or non-operatively. However, generally 6 weeks
following an injury of AT (old/neglected) a direct repair
opposing the tendon ends becomes increasingly difficult.
Through this time scar tissue forms, disuse leg muscles
atrophy and the tendon ends weaken4. The old AT injury is
debilitating; their optimal management is surgical3,4,5. The
purpose of this series was to evaluate clinical result of old AT
injury reconstruction by FHL tendon.
MATERIAL AND METHODS
This prospective study was conducted in the department
of orthopaedic surgery in Sylhet MAG Osmani Medical
College, Sylhet Women’s Medical College Hospital and
other private hospital in Sylhet, science January 2007 to
June 2014. Each patient had an old AT injury, whereby all
Achilles tendons tear were presented and/or treated more
than 6 weeks after the index lesion (Fig-1). We have
performed 10 cases of old AT injury. All age and sex, patient
Old Achilles Tendon Injury
Reconstruction with Flexor Hallucis
Longus Tendon-a Prospective Study
Md. Abdul Gani Ahsan1, Kazi Md Salim2, Ishtiaque-Ul-Fattah3, AKM Zahir Uddin4
Abstract
The optimal management of old Achilles tendon (AT) injury is surgical reconstruction. In case of wide gap between
tendon’s ends of old AT injury, need long tendon for reconstruction. Flexor hallucis longus (FHL) tendon can serve
this type of reconstruction. We describe 10 cases of Achilles tendon reconstruction by FHL tendon with satisfactory
outcome. This technique allows reconstruction of the old AT injury with any length of gap using FHL.
Key wards: Achilles tendon, flexor hallucis longus, reconstruction.
1. Associate Professor, Department of Orthopaedics, Sylhet Women’s Medical College, Sylhet.
2. Professor and Head, Department of Orthopaedics, Sylhet Women’s Medical College, Sylhet.
3. Associate Professor, Department of Orthopaedics, Sylhet MAG Osmani Medical College, Sylhet.
4. Associate Professor, Department of Orthopaedics, NITOR, Dhaka
Correspondence: Dr. Md Abdul Gani Ahsan, Associate Professor, Department of Orthopaedics, Sylhet Women’s Medical College, Sylhet.
with old (neglected) AT injury, re-rupture after primary
repair of AT injury were included in this study. Fallow-up
time was 6 to 12 months.
Surgical procedure: Surgery was performed under spinal
anaesthesia, in prone lateral position. A tourniquet was
applied to the thigh. After usual antiseptic preparation,
the limb was draped in a sterile field. A longitudinal skin
incision was given in between Achilles tendon (AT) and
posterior border of medial malleolus and tibia (Fig-2).The
paratenon was incised, tenolysis performed and the AT
was inspected. Debridement of tendon fibrosis was
performed with conservation of a distal and a proximal
tendon stump. The average AT defect after fibrosis
debridement was 6.2 cm (range, 4–10). After incision of
the deep fascia of the leg and having located and retracted
the posterior tibial bundle, the FHL muscle belly and
tendon were identified and isolated. To harvest the distal
portion of the FHL, a second short medial arch incision
was performed (Fig.-2,3). The flexor digitorum longus
(FDL) tendons were identified and connections between
FHL and FDL were freed. FHL tendon was divided distally
and pulled out through the proximal approach (Fig-3).
Reconstruction techniques include passing the tendon
(FHL) through tenotomy in the distal and the proximal
tendon stumps 3, 6 or through a tunnel drilled through the
posterior calcaneal cortex and a tenotomy in the proximal
VOL. 29, NO. 2, JULY 2014 155

Achilles tendon stump7 (Fig- 4). Next the FHL tendon was
tenodesed to itself with a tension fixed at 40° of plantar
flexion (Fig- 4). Wound closure was performed carefully
to avoid subsequent skin necrosis. A well padded cotton
bandage with a short anterior plaster slab was applied
with the ankle in maximum plantar flexion for 6 weeks. Post
operatively, patients are allowed to toe touch walking with
the help of elbow crutches. After 6 weeks, the plaster slab
is removed and physiotherapy is commenced focusing on
proprioception, plantar and dorsi flexion of the ankle,
inversion and eversion for reduce further muscle atrophy.
During this period of rehabilitation the patient is permitted
to weight bear as comfort allows. Athletic activities were
restricted for six months after surgery (Fig-5).
RESULTS
A series of 10 patients (eight men, two women) with age
distribution was 32.3 years (18 to 52) in our study. All 10
patients presented with a limp, inability to run and AT
gap, among them 6 had a scar overlying skin. Causes of
AT injury were Indian type broken toilet pan 3 (30%),
spontaneous rupture 2(20%), local corticosteroid injection
2(20%), motor vehicle accident 2 (20%) and 1(10%) with
an Achilles tendon (AT) re-rupture. The AT defect after
fibrosis debridement averaged 5.4 cm (range, 3.5–8).
All patients were inadequately treated previously and
lastly present minimum after 6 weeks for reconstructive
surgery. Left sided AT injury is predominant (70%) in our
study. The mean follow-up was minimum 6 months (range,
6–18). All the patients were evaluated according to Nada
criteria 8. Functional outcome was satisfactory (excellent
and good). Average delay of work and sports recovery
was 6 months (range, 5–8). All patients returned to a sports
activity within minor limitations. No re-rupture has been
described. No major complication was observed
particularly on wound healing. Two patients developed a
small skin necrosis and a mild discharging sinus. Both
were healed spontaneous after 2-3 weeks. All patients
presented with a loss of active flexion of great toe without
subsequent hyperextension. However, no patient
presented with functional weakness of the great toe during
athletic or daily life activities.
Fig- 1 Old AT injury (left); before operation Fig-2 Incision site Fig- 3 Delivery of FHL (left)
Fig-4 Complete TA reconstruction Fig- 5 Eight months later of AT reconstruction
156 Md. Abdul Gani Ahsan, Kazi Md Salim, Ishtiaque-Ul-Fattah, AKM Zahir Ueddin
The Journal of Bangladesh Orthopaedic Society

DISCUSSION
In 1993 Wapner et al. 9 first described the use of FHL as a
graft for reconstruction of AT. Many procedures have
been described in the literature for old AT injury
reconstruction with different local autologous material
such as the gastrocnemius soleus complex with V-Y
myotendinous advancement 10 or a “turn-down” of
proximal AT tissue11. Other surgical techniques used
tendon transfer of peroneus brevis (PB) 3, 6, 7, flexor
digitorum longus (FDL) 12 or flexor hallucis longus (FHL)9, 13 tendons.
Compared to PB or FDL, the FHL is a stronger plantar
flexor, its axis of contractile force more closely reproduces
that of the AT, it fires in phase with the gastrocnemius-
soleus complex and its anatomical proximity avoids the
neurovascular bundle. Another benefit of FHL transfer is
the plantar flexion strength reinforcement which is almost
always compromised with fascial advancement alone 15.
With regards to vascularisation of AT, the FHL muscle
belly extends distally into the avascular zone of AT and
allows recruitment of an increased blood supply to the
repaired AT. Furthermore, FHL transfer maintains the
normal muscle balance of the ankle by transferring a muscle
with the same function. In a recent study using MRI
evaluation, Hahn et al. showed a complete integration of
the FHL tendon in 60% of the patients 16. The FHL was
free of degeneration in all patients and more than 15%
hypertrophy of the FHL was observed in 80% of the
patients which suggests functional incorporation into
plantar flexion after the transfer of FHL16.
Excision of degenerative part of the AT due to chronic
rupture was complete to improve pain relief 9. Some
authors proposed preservation of fibrous scar tissue at
the stumps of the ruptured AT to keep its original length,
make length adjustment easier and to use it as a scaffold
for the FHL transfer 15, 16, 18. In our series, fibrous scar
tissue of AT stumps was not preserved. Another authors
describe FHL transfer alone was insufficient for
reconstruction of defects greater than 5 cm; a V-Y
myotendinous advancement or a fascial turn-down flap
was required 14,15,17. The main morbidity of FHL harvesting
is the loss of active interphalangeal plantar flexion strength
of great toe. According to our results and those of other
studies, FHL transfer morbidity is clinically insignificant,
even for good push-off or balance in running sports 9, 14,
19. Therefore, alternatives to FHL such as FDL or PB appear
less advantageous in these respects. In our study and
other previous series, when using FHL tendon transfer
for AT rupture reconstruction, no case of re-rupture has
been reported at latest follow-up 9, 14. However, account
all other surgical procedures, the incidence of AT re-rupture
following acute or chronic rupture reconstruction has been
reported to be 1.4–3.7% 20. In our study no re-rupture of
Achilles tendon after reconstruction. The main limitation
of our series is the small number of patient’s included.
CONCLUSION
For old Achilles tendon injury with a wide gap, surgical
reconstruction by FHL tendon transfer achieved excellent
outcome with a neglected drawback.
Table-I
Clinical characteristics of the patients
Patient no. Age/Sex/Side Cause of AT Injury to operation AT defect after Complication Outcome
involved injury AT duration fibrosis
(Weeks) debridement(cm)
1 25/M/L TP 12 4 None Excellent
2 18/F/L TP 10 3.5 None Excellent
3 20/M/R MVA 16 6 None Excellent
4 52/M/L SR 24 7.5 None Excellent
5 24/M/L RR 13 4.5 None Excellent
6 35/M/L TP 14 5 Skin necrosis Good
7 45/F/R LSI 18 6.5 None Excellent
8 25/M/R MVA 15 5 None Excellent
9 32/M/L LSI 12 4 None Excellent
10 47/M/L SR 20 8 Discharging sinus Good
Abbreviations: M-Male; L- Left; R-Right; TP-Toilet pan; MVA- Motor vehicle accident; LSI- Local steroid injection;
SR- Spontaneous rupture; RR-Re rupture.
Old Achilles Tendon Injury Reconstruction with Flexor Hallucis Longus Tendon-a Prospective Study 157
VOL. 29, NO. 2, JULY 2014

REFERENCES
1. Thermann H, Hufner T, Tscherne H. Achilles tendon
rupture. Orthopade. 2000; 29: 235-50.
2. Chatterjee SS, Sarkar A, Misra A. Management of acute
open tendo-Achilles injuries in Indian lavatory pans. Indian
J Plast Surg 2006; 39(1):29-33.
3. Ahsan MAG, Fattah IU, Hasan SM, Salim KM. Evaluation
of result of peroneus brevis tendon transfer in the
management of neglected tendo Achilles Injury. Osmani
Medical Teachers Association Journal 2011; 10(2):98-101.
4. Carmont M, Maffulli N: Less invasive Achilles tendon
reconstruction. BMC Musculoskelet Disord. 2007, 8: 100.
5. Leslie HD, Edwards WH: Neglected ruptures of the Achilles
tendon. Foot Ankle Clin 2005, 10(2):357-70.
6. Turco VJ, Spinella AJ: Achilles tendon ruptures-peroneus
brevis transfer. Foot Ankle 1987, 7(4):253-59.
7. Pérez Teuffer A: Traumatic rupture of the Achilles Tendon.
Reconstruction by transplant and graft using the lateral
peroneus brevis. Orthop Clin North Am 1974, 5(1):89-
93.
8. Nada A. Rupture of calcaneus tendon treatment by external
fixator. J Bone Joint Surg (Br) 1985; 67(3):449-53.
9. Wapner KL, Pavlock GS, Hecht PJ, Naselli F, Walther R:
Repair of chronic Achilles tendon rupture with flexor
hallucis longus. Foot Ankle 1993, 14(8):443-49.
10. Abraham E, Pankovich AM . Neglected rupture of the
Achilles tendon by V-Y tendinous flap. J Bone Joint Surg
(Am) 1975; 57: 253–56.
11. Bosworth DM. Repair of defects in the Tendo Achilles. J
Bone Joint Surg (Am) 1956; 38:111–14.
12. FDL Mann RA, Holmes GB, Seale KS, Collins DM.
Chronic rupture of the Achilles tendon: a new technique
of repair. J Bone Joint Surg (Am)1991; 73-A:214–19.
13. Wilcox DK, Bohay DR, Anderson JG: Treatment of
chronic Achilles tendon disorders with flexor hallucis
longus tendon transfer/augmentation. Foot Ankle Int 2000,
21(12):1004-10.
14. Kann JN, Myerson MS. Surgical management of chronic
ruptures of the Achilles tendon. Foot Ankle Clin
.1997;2:535-45.
15. Hartog BD. Surgical strategies: delayed diagnosis or
neglected Achilles tendon ruptures. Foot Ankle Int. 2008;
29: 456-63.
16. Meyer P, Maiwald C, Zannetti M, Vienne P. Treatment
of chronic Achilles tendinopathy and ruptures with flexor
hallucis longus tendon transfer: Clinical outcome and MRI
findings. Foot Ankle.2008; 794-802.
17. Kissel CG, Blacklidge DK,Crowley DL. Repair of
neglected Achilles tendon rupture: procedure and functional
results. J Foot Ankle Surg. 1994; 33:46-52.
18. Park YH, Yoon TR, Chung JY. Reconstruction of neglected
Achilles tendon rupture using the flexor hallucis longus
tendon.Knee Surg Traumatol Arthrosc. 2008; 17:316-20.
19. Coull R, Flavin R, Stephens MM. Flexor hallucis longus
tendon transfer: evaluating of postoperative morbidity;
24: 931-34.
20. Linden-vander Zwang HMJ, Nelissen RGHH, Sintenie
JB. Results of surgical versus non-surgical treatment of
Achilles tendon rupture. Int Orthop.2004; 28:370-73.
158 Md. Abdul Gani Ahsan, Kazi Md Salim, Ishtiaque-Ul-Fattah, AKM Zahir Ueddin
The Journal of Bangladesh Orthopaedic Society

Original Article
Anterolateral Chest Wall Flap as a
salvage for composite wound coverage
of the elbow, forearm and hand
A.B.M. Golam Faruque1, A.H.M. Tanvir Hasan Siddiquee2, Uttam Kumar Saha3, A K M Zohiruddain4,
Md. Mohabbatullah5, Md Zahid Ahmed6
ABSTRACT
Anterolateral chest wall flap has a significant effect on the patient’s aesthetic and functional outcome, especially
in the cases of the soft tissue defects in the elbow, forearm and hand. The surgical procedure must be tailored to
the needs of the wound and the patient.
This prospective study was carried out on 10 patients with post traumatic soft tissue defects over the elbow,
forearm and hand. The duration of this study was 2 years. Average age of the patients was 28.5 years, ranging
from 6 to 60 years. 6 were males and 4 were females, with a male female ratio of 3:2. 6 patients had soft tissue
loss over forearm with exposed bone; 3 had exposed bones and tendons at the elbow and 1 had lost skin and soft
tissue over the dorsum of the hand with exposed, infected 2nd & 3rd metacarpals. All patients were treated with
inferiorly based anterolateral chest wall flap. 1 case developed marginal necrosis, which was overcome by
debridement and dressings. A follow up ranging from 2 to 24 months (mean 12 months) showed that patients
achieved a good aesthetic and functional outcome.
Key words : Anterolateral chest wall flap, reconstruction, soft tissue defect.
1. Associate Professor, Orthopaedic Surgery, National Institute of Traumatology & Orthopaedic Rehabilitation (NITOR), Dhaka
2. Junior Consultant, Orthopaedic Surgery, Govt. Emplyees Hospital, Dhaka.
3. Junior consultant, Orthopaedic Surgery ,Louhajonj UHC, Munsighonj
4. Associate Professor, Orthopaedic Surgery, National Institute of Traumatology & Orthopaedic Rehabilitation (NITOR), Dhaka
5. Assistant Professor, Orthopaedic Surgery, National Institute of Traumatology & Orthopaedic Rehabilitation (NITOR), Dhaka.
6. Junior Consultant, Orthopaedic Surgery, National Institute of Traumatology & Orthopaedic Rehabilitation (NITOR), Dhaka
Correspondence: Dr. A.B.M. Golam Faruque, Associate Professor, Orthopaedic Surgery, National Institute of Traumatology &
Orthopaedic Rehabilitation (NITOR), Dhaka
INTRODUCTION
Flap surgery is a technique in plastic and reconstructive
surgery where any type of tissue is lifted from a donor site
and moved to a recipient site with an intact blood supply.
Soft tissue reconstruction in the upper limb is a common
challenge following trauma, burns, tumour resection and
infection. The quality of the reconstruction has a significant
effect on the patient’s aesthetic and functional outcome.
The options for soft tissue reconstruction in the upper
extremity include skin grafting, local flaps, regional flaps
and free flaps. The preferred approach is the simplest
method which can provide the most stable coverage. The
mechanism, time, location and extent of soft tissue injury,
severity of contamination, nature of the structure exposed
and expected outcomes of spontaneous healing of the
defect will dictate the soft tissue reconstruction options
used in the upper limb.1 Successful soft tissue coverage
requires removal of all necrotic tissue, control of
contamination and confirmation of a good blood supply.2,3
Soft tissue restoration will take place as early as possible
to prevent wound infection and allow earlier patient
recovery and rehabilitation.4,5,6
Several factors, including the patient’s age, sex,
occupation, and general health status before injury or an
operation, should be considered before choosing the
method of wound closure. The surgical procedure must
be tailored to the needs of the wound and the patient.7
Anterolateral chest wall flap gets blood supply from the
intercostals and the thoraco-epigastric vessels. The skin
in this area has great mobility. This skin is more pliable,
sub cutaneous tissue is thinner and the surrounding skin
VOL. 29, NO. 2, JULY 2014 159

is more elastic, thinner tissue provides accurate fitting of
the flap, minimizing the need for secondary defatting,
scanty hair on the skin is an additional benefit. The donor
site usually is bounded superiorly by the nipple line,
inferiorly the umbilicus and laterally by the mid-axillary
line. The inferiorly based flap is the preferred orientation,
because it minimizes venous congestion and edema
formation in the flap by permiting dependent drainage.
This transversely oriented flap should not extend across
the ventral midline, since the collateral blood supply of
the skin across the midline is poor. The approximate length
to width ratio should be 1.5:1, not exceeding 7-8 cm in
width and 10-12 cm in length.8
Anterolateral chest wall flaps may be contralateral or
ipsilateral. Contralaterl anterolateral chest wall flaps are
ideal source for application to the digits, palm, dorsum of
the hands and occasionally to the wrist. Ipsilateral
anterolateral chest wall flaps are best suited for coverage
about the elbow, forearm and proximal wrist.8
MATERIALS AND METHODS
This prospective study was carried out at NITOR and
some other private hospitals from May 2013 to May 2015.
10 patients with post traumatic soft tissue injury of the
elbow, forearm and hand were included in this study. 6
patients had soft tissue loss over forearm with exposed
bone; Among them, 2 were with degloving injury of forearm
with open fracture of radius & ulna, 2 with fractured radius;
1 open & 1 closed, with compartment syndrome, being
treated initially by a traditional bone setter; 1 with fractured
ulna with dislocated elbow and 1 without fracture. 3 patients
were with exposed elbow and 1 patient with wound at the
dorsum of the hand, with lost skin, muscle & tendon over
infected 2nd & 3rd metacarpals. Fractured bones were were
internally fixed by Rush nail and K wire, although 1 was
treated initially by external fixator, which was later fixed by
rush nail. All patients were treated with inferiorly based
anterolateral chest wall flap for wound coverage.
OPERATIVE TECHNIQUE
Under general anesthesia, the patient was placed supine.
After sterile drapping, a marking line was drawn on the
upper border of the flap on the donor site, above the
umbillicus. A fasciocutaneous flap of appropriate size was
then elevated. Meticulous hemostasis was ensured.
Wound gap on the donor site was minimized by skin
mobilization and direct closure. Then the recipient site
was prepared and wound coverage was done without
undue tension over the flap. The vascularity of the flap
was checked. After application of sterile dressing, The
arm was held flush with the trunk.
Early in the postoprative period, the operated extremity was
immobilized by dressing and elastic bandages. A light plaster
covering was added over the bandages in 4 cases, especially
in the children, to ensure more secure mobilization.
In all cases, the flaps were divided 3 weeks after application.
The donor site was then covered by direct closure of the
pedicle, or by split thickness skin grafting.
Thereafter dynamic splintage and physiotherapy was
instituted.
The patients were followed up regularly at every month
for the first 3 months, then at every 3 months at the
outpatient department.
RESULTS
The duration of this study was 2 years; from May 2013 to
2015. Total 10 cases of soft tissue injury over the elbow,
forearm and the hand were included. Average age of the
patients was 28.5 years, ranging from 6 to 60 years. Among
the 10 cases, 6 were males and the rest 4 were females,
with a male female ratio of 3:2. All patients were treated
with inferiorly based anterolateral chest flap.
Adequate functional restoration was achieved in all 10
cases. A follow up ranging from 2 to 24 months (mean 12
months) showed that patients achieved a good aesthetic
outcome, satisfactory elbow and wrist movement,along
with good thumb-index pinch, chuck pinch, hook and
grasp. The donor area is concealed and there has been no
hypertrophic scarring or spreading of the scar.
Regarding complication, 1 case with open fracture radius
& ulna, developed marginal necrosis, which was overcome
by debridement and dressings.
Fig 1 : Dosum of the hand defect with exposed 2nd and 3rd metacarpals; before & after surgery
160 Anterolateral Chest Wall Flap as a salvage for composite wound coverage of the elbow, forearm and hand
The Journal of Bangladesh Orthopaedic Society

DISCUSSION
Trauma to extremities often results in complex bony and
soft tissue injuries, that require free flap reconstruction.9,10,11,12 But, free flaps are prone to vascular thrombosis
at the recipient area in cases of traumatic injury.13 In
cases of trauma, the status of recipient vessels is directly
related to the magnitude of the injury. 14 Although
microsurgical techniques are well developed and can be
used in one stage operations to provide good contour,
the distant pedicle flap is still the method of choice for
reconstruction of upper extremity defects. Pedicled flaps
are good to cover the forearm and elbow defects, as free
flaps may fail due to trauma induced thrombosis.15
The advantages of this flap are :
- The blood supply is reliable and the elevation of the
flap is easy and quick.
- Major arteries are not sacrificed.
- Easy identification of the perforator vessel using
Dopplar ultrasound.
- The perforator vessel need not to be exposed.
- Adequate vascular network for covering large soft
tissue defects.
- Can cover forearm and elbow defects without
tension.
The disadvantages are :
- Inevitable ugly scar,
- Bulkiness of flap in overweight patients,
- Needs a second procedure for pedicle separatiion.16
A study on 8 patients of post burn contracture affecting
dorsum of the hand, treated by contralateral anterolateral
chest wall flap showed satisfactory outcome in all 8
patients, and all the patients could return to their previous
vocation within a follow up period of 5 to 12 months.17
Similarly, in this study on 10 patients with post traumatic
elbow, forearm and hand defects, which were treated by
inferiorly based anterolateral chest wall flaps, adequate
functional restoration was achieved in all 10 cases within
a follow up period of 2 to 24 months.
CONCLUSION
Anterolateral chest wall flap is useful for covering severe
crush injury defects of the forearm, elbow and even hands
that have a high risk of free flap necrosis because of
inadequate recipient vessels. The flap procedure is easily
performed and the site of the flap can be raised safely .
The chest flap can be used as salvage flap to cover the
forearm and elbow defects, where free flap surgery is not
possible because of a poor armamentarium.
REFERENCES
1. Levin LS, Erdmann DE. Primary and secondary
microvascular reconstruction of the upper extremity. Hand
Clinics. 2001;17: 447–55.
2. Lister G, Scheker L. Emergency free flaps to the upper
extremity. J Hand Surg Am. 1988; 13: 22–8.
3. Godina M. Early microsurgical reconstruction of complex
trauma of the extremities. Plast Reconstr Surg. 1986; 78:
285–92.
4. Chen S, Tsai YC, Wei FC , et al. Emergency free flaps to
the type IIIC tibial fracture. Ann Plast Surg. 1990; 25:
223–9.
5. Chen SHT, Wei FC, Chen HC , et al. Emergency free flap
transfer for reconstruction of acute complex extremity
wounds. Plast Reconstr Surg. 1992; 89: 882–8.
6. Chen ZW, Yan W. The study and clinical application of
the osteocutaneous flap of the fibula. Microsurgery. 1983;
4: 11–6.
7. Russell RC, Zamboni WA. Soft tissue reconstruction.
Coverage of the elbow and forearm. Orthop Clin North
Am. 1993 Jul; 24(3): 425-34.
8. Griffin M, Hindocha S, Malahias M, Saleh M, Juma A.
Flap Decisions and Options in Soft Tissue Coverage of
the Upper Limb. Open Orthop J. 2014; 8: 409–14.
(A)
Fig.-2 : Degloving injury with fractured radius and ulna with dislocated right elbow; A. Initial appearance, B. After
debridement, C. After wound coverage, D. Final appearance
(B) (C) (D)
A.B.M. Golam Faruque, A.H.M. Tanvir Hasan Siddiquee, Uttam Kumar Saha, A K M Zohiruddain, Md. Mohabbatullah et al 161
VOL. 29, NO. 2, JULY 2014

9. Howard TW, James WF, Detlev E, Scott L. Use of the
anterolateral thigh free flap for upper extremity
reconstruction. J Hand Surg . 2005; 30: 859-64.
10. Chen SL, Chen TM, Wang HJ. Free thoracodorsal artery
perforator flap in extremity reconstruction: 12 cases. Br J
Plast Surg. 2004; 57: 525-30.
11. Schenck RR. Rectus femoris muscle and composite skin
transplantation by microneurovascular anastomosis for
avulsion of forearm muscles: a case report. J Hand Surg .
1973; 3: 60-9.
12. Wei CY, Chuang DC, Chen HC, Lin CH, Wong SS, Wei
FC. The versatility of free rectus femoris muscle flap: an
alternative flap. Microsurgery . 1995; 16: 698-703.
13. Yunchuan P, Jiaqin X, Sihuan C, Zunhong L . Use of the
lateral intercostal perforator-based pedicled abdominal flap
for upper limb wounds from severe electrical injury. Ann
Plast Surg. 2006; 56: 116-21.
14. Khouri RK, Shaw WW. Reconstructionof the lower
extremity with microvascular free flap : a 10- year
experience with 304 consecutive patients. J Traum. 1989;
29: 1086-94
15. Acland RD. Refinement in lower extremity free flap. Clin
Plast Surg. 1990; 17: 733-44
16. Tzeng Y, Yu C, Dai N, Chen T, Chen S. The Abdomino-
hypogastric flap as a salvage flap for composite wound
coverage of the forearm and elbow. J Med Sci. 2007; 27(4):
185-8
17. Bhattacharya S, Pandey SD, Chandra R, Bhatnagar SK.
Lateral chest wall fasciocutaneous flaps in the management
of burn contractures on the dorsum of the hand. Eur J
Plast Surg . 1988; 11: 8-11.
162 Anterolateral Chest Wall Flap as a salvage for composite wound coverage of the elbow, forearm and hand
The Journal of Bangladesh Orthopaedic Society

Original Article
Minimally invasive plate osteosynthesis
(MIPO) for fracture of distal tibia in 18
patients at BIRDEM Hospital
Anwar Ahmed1, Ahmed Suparno Bahar Moni2, MKI Quayyum Choudhury3, M Golam Sarwar4,
Anjan Lal Ghosh5
ABSTRACT
The treatment of distal tibia fracture by minimally invasive locking plate osteosynthesis (MIPO) was a prospective
study carriedout at BIRDEM Hospital in Dhaka, Bangladesh, between August 2008 to July 2014.Total 18 patient
were included in the study. Among them 14 cases were male, four were female. The age range of patients was 18
to 75 year. Mean age is 28.5 years. Majority of the patient was in the age group of 30 -55 years (50%). 14 patient
were injured from road traffic accident, four cases due to fall. The mean time of union was 18 weeks. Very few
complications were observed, among which ankle stiffness was common. Satisfactory results (Excellent and
good) were in 83.33% cases and unsatisfactory results in 16.67%.
1. Associate Professor of Orthopaedics, BIRDEM General Hospital and Ibrahim Medical College.
2. Assistant Professor (Orthopaedics), BIRDEM General Hospital and Ibrahim Medical College.
3. Professor of Orthopaedics, BIRDEM General Hospital and Ibrahim Medical College.
4. Associate Professor of Orthopaedic Surgery, DMCH, Dhaka
5. Assistant Professor of Orthopaedic Surgery, ZH Sikder Medical College
Correspondence: Dr. Anwar Ahmed, D.Ortho, MS (Ortho), MchOrth, Associate Professor of Orthopaedics, BIRDEM Hospital and
Ibrahim Medical College, E-mail: [email protected]
INTRODUCTION
Distal tibial fractures show some characteristics as:
hardship regarding reduction and stabilization, an
increased local complication rate following classic
osteosynthesis by metallic plates (nonunions, infections,
tegumentary necrosis) and also consecutively to
intramedullary osteosynthesis (malalignment) or to external
fixation (healing delay).
Poor soft tissue coverage and blood supply act as a
deterrent to quick healing of fracture. Alternative for
management of distal third tibial fracture are diverse and
modalities of treatment is influenced by its integrity of the
soft tissue, open fracture, presence or absence of infection.
Conservative treatment of these fracture often results in a
number of complications including malunion, non-union
and ankle stiffness1,2. Intramedullary nailing is not suitable
for all distal tibial fracture3,4. External fixation can be used
as either a temporary or definitive method of
treatment.Open plating of the medial aspect of the distal
tibia causes greater disruption of the extraosseous blood
supply leading to higher incidence of non-union, infection,
skin necrosis and implant failure
On one side, MIPO shows the advantage of periosteal
circulation preservation with positive effect on bone
healing5,6, and on the other side, it provides a good
stability for the fracture site.
It is with these background, treatment of distal tibial
fracture by minimally invasive locking plate osteosynthesis
has been evaluated in this study from August 2008 to
July2014.
MATERIALS AND METHOD
This was a prospective study carried out at BIRDEM
hospital in Dhaka, Bangladesh.during the period from
August 2008 to July 2014. A total number of 18 patient
were selected.
This study comprising 18 cases for follow-up for a period
of 6 to 24 months. Patient with open fracture were excluded
from study. Among these 18 cases, 14 cases were male, 4
cases were female. 14 patientwere injured after road traffic
accident and 4 patient had a fall. The average age of the
patient was 38 years (range 18 to 75 years). The fracture
were classified according to the Muller’s AO classification
system. There were type A (5 in A1,6inA2,4 inA3)
VOL. 29, NO. 2, JULY 2014 163

andtypeB(2in B1,linB2). Surgery was performed as soon
as the swelling subsided. When indicated, the fibula was
fixed initially by using standard AO technique. Through a
small curve incision behind the medial malleolus an
extraperiosteal or subcutaneous tunnel was created along
the medial aspect of tibia by blunt dissection, using
periosteal elevator. The distal tibial medial
anatomicallocking plate was then inserted extraperiosteally.
Initially fixation was carried out with a distal screw under
the guidance of image intensifier. And the fracture was
indirectly reduced on to the plate. Axial traction on the
foot or application of the reduction forceps was used to
obtain acceptable reduction. Once the sagital, coronal and
rotational alignment appeared to be satisfactory, the
proximal screws were passed percutaneously under image
intensifier.
RESULT
All the 18patients were reviewed clinically and
radiologicaly at regular interval: 6 week interval for 6 month,
12 week interval onward. Follow up period was between 6-
24 month (average 14.6 month). Evaluation of results of the
study was done on the basis of criteria followed by Tucker
et.al (1992) (7) Patient were graded into excellent, good, fair
and poor depending onunion, pain, shortening, angulation,
range of ankle and knee movement. Any angulation of more
than 5 degrre of varus valgus and 10 degree of anterior-
posterior angulation and over 1cm. of shortening were
considered to be radiologically fair to poor result. Mean
time of union was 18 weeks.
Table-I
Post operative complications
Case Ankle Knee Flexion Deficit varus valgus Antro- Rotation Shortening
no pain on pain deficit knee Ankale posterior In degre
weight ROM Angulation
1. + - - - - - - - -
2. - - - l0® - - - 5® -
3. - - - 8® - - 8® 5® -
4. - - - 5® - - - - -
5. - - - - - - - - -
6. - - - 5® - - - - -
7. - - — 4® - — 8® — —
8. + - - 5® - - - - -
9. + - - - - - - - -
10. + - - S® - - - - -
11. + - - 8® - - - - -
12. - - - 5® - - - - 1.5 cm
13. - - - 5® - - - - -
14. - - - - - - - - -
15. - - - l0® - - - - -
16. - - - 5® - - - - -
17. + - - 10® - - 4® - -
18. - - - - - - - - -
Table-II
Results according to tucker criteria
Grading Number of Percentage
Patient
Satisfactory Excellent 7 38.89
Good 8 44.44
Unsatisfactory Fair 2 11.11
Poor 1 5.56 Fig.-1: Insertion of LCP
164 Anwar Ahmed, Ahmed Suparno Bahar Moni, MKI Quayyum Choudhury, M Golam Sarwar, Anjan Lal Ghosh
The Journal of Bangladesh Orthopaedic Society

DISCUSSION
MIPO shows the advantage of periosteal circulation
preservation with positive effect on bone healing5,6, and
on the other side, it provides a good stability for the fracture
site.
According to Helfet8, the standard protocol that precedes
MIPO procedure includes: a. tibial fracture alignment with
external triangular temporary fixation, extended from
heelbone to tibia; b. reduction of the fibular fracture and
plate fixation by a precontoured one third tubular plate or
by a small DCP. MIPO by medial approach is recommended
at 5-7 days from accident.It is more advantageous over
IM nailing or by open reduction and internal fixation using
plates in respect of non-union, skin problems, local septic
complications and stiffness of adjacent joints9,4.
In our study 18 patients were treated by this method.All
fractures healed, within a mean time of 18 weeks. No bone
grafting is required. No incidence of nonunion but 2 cases
of delayed union was observed.There wereno infections.
In several series of minimally invassive plate
osteosynthesisno infection was reported 10,4. Jensen
et.al.11 reported 9% superficial infection treated by open
method.
In our study, there were wound necrosis in 2 cases. But it
is common in medial plating by open method (12.5%)
because open plating of the medial aspect of distal tibia
caused massive disruption of the extraosseous blood
supply of the metaphysical region.12
All patients had a satisfactory knee and ankle range of
motion.There were no implant failures
CONCLUSION
MIPO is a safe and effective procedure to preserve bone
biology and minimise surgical soft tissue trauma.It is a
demanding technique in cases of lower tibia fracture,
which requirescautious intraoperative clinical and
fluoroscopic control in order to reestablish limb axis,
rotation and length.
REFERENCES
1. Digby JM, Holloway GM, Webb JK. A study offunction
after tibia! cast bracing. Injury.1983;14(5):432439. doi:
10.1016/0020-1383(83)90094-3. [RefMed] [Cross Ref]
2. Oh OW, Kyung HS, Park lH, Kim PT, lhn JC. Distal
tibialmetaphyseal fractures treated by percutaneous plate
osteosynthesis. C/in Orthop Re/at Res. 2003;408:286291.
Doi: 10.1097/00003086-200303000-00038. [RefMed]
[Cross Ref]
Fig.-2: Insertion of distal and proximal screws
Fig.-3: Preoperative x - ray
Fig.-4: Post operative x - ray (after 4 months)
Minimally invasive plate osteosynthesis (MIPO) for fracture of distal tibia in 18 patients at BIRDEM Hospital 165
VOL. 29, NO. 2, JULY 2014

3. Dickson KF, Montgomery S, Field J. High energyplafond
fractures treated by a spanning external fixator initially
and followed by a second stage open reduction internal
fixation of the articularsurface preliminary report. Injury.
2001 ;32(Suppl4):5D925D98. [PubMed]
4. Krackhardt T, Dilger J, Flesch I, Höntzsch D, Eingartner
C, Weise K. Fractures of the distal tibia treated with closed
reduction and minimally invasive plating. Arch Orthop
Trauma Surg. 2005; 1 25(2):8794. doi: 10.1 007/s00402-
004- O778-y[RefMed] [Cross Ref].
5. Baumgartel, F.; Buhl, M. &Rahn, B.A. (1998). Fracture
healing in biological plate osteosynthesis. Injury, Vol.29,
Suppl.3, pp. C3-6, ISSN 0020-1383
6. Farouk, O.; Krettek, C.; Miclau, T.; Schandelmaier, P.;
Guy, P. &Tscherne, H. (1997). Minimally invasive plate
osteosynthesis and vascularity: preliminary results of a
cadaver infection study. Injury, Vol.28, Suppl.1, pp. 7-12,
ISSN 0020-1383
7. Tucker HL and Kendra JC(1992),management of unstable
open and closed tibial fractures using llizarov method. C/
in Orthop 280:125
8. Helfet, D.L.; Shonnard P.Y.; Levine, D. &Borrelli, J. (1997).
Minimally invasive plate osteosynthesis of distal fractures
of the tibia. Injury, Vol.28, Suppl.1, pp. 42-48, ISSN 0020-
1383.
9. Fisher WD, Hamblen DL. Problems and pitfalls of
compression fixation of long bone fractures: a review of
results and complications. Injury1978;10(2):99107. dol:
10.1016/S0020- 1383(79)80069-8. [RefMed] [Cross Ref]
10. Collinge C, Kuper M, Larson K, Protzman R.Minimally
invasive plating of high-energymetaphyseal distal tibia
fractures. J OrthopTrauma. 2007;21(6):355361. doi: 10.1
097/BOT. 0b013e3180ca83c7. [PubMed][Cross Ref].
11. JensenJS,HansenFW,JohansenJ.Tibialshaftfractures.A
comparison of conservative treatment and internal fixation
with conventional plates or A0 compression plates.
ActraOrthopScandd. 1977 48(2):204-21 2.
12. Hasenboehler E, RikIl D, Babst R. Locking compression
plate with minimally invasive plate osteosynthesis in
diaphyseal and distal tibial fracture: a retrospective study
of 32 patients. Injury. 2007;38(3):365370. Doi: 10.1 016/
j.injury. 2006. 10.024. [RefMed] [Cross Ref]
166 Anwar Ahmed, Ahmed Suparno Bahar Moni, MKI Quayyum Choudhury, M Golam Sarwar, Anjan Lal Ghosh
The Journal of Bangladesh Orthopaedic Society

Original Article
Functional Outcome of Minimally
Invasive Percutaneous Plate
Osteosynthesis Using Locking Condylar
Plates In Distal Femoral Fractures
Md. Saidul Islam1, Md. Golam Mostafa2, Shah Jawaher Jahan Kabir3, Shahidul Haq4
ABSTRACT
Minimally Invasive Percutaneous Plate Oseosynthesis for distal femoral fractures is a type of Biological
osteosynthesis which preserve biological environment at the fracture site and vascularity of fracture fragment
and thus improved fracture healing.Distal femoral fractures are associated with high energy trauma and
osteoporotic bone . Metaphyseal comminution and osteoporotic bone is a challenge to conventional plate
fixation.The present study was carried out for evaluation and analysis of the role of Minimall invasive percutaneous
plate osteosynthesis with locking condylar plate for distal femoral fractures.Total 20 cases ,aged more than 18
years were included in this study. .According to AO/OTA classification,the fractures were classified as types
A1(n=7 )A2 (n=6) A3(n= 3),C1(n=3),C2(n=1).All the fracture were closed.The result in all the 20 cases ,17 cases
had acceptable result (i.eExcellent and good) and 3 cases had poor result. MIPPO with Locking condylar
plate(LCP) achieves favorable biological fixation for distal femoral fractures for early fracture union and less
complications especially when fracture is comminuted and osteoporotic.
Key words: Distal femoral fractures,Indirect reduction, Minimally Invasive technique.
1. Associate Professor, Department of Orthopaedic Surgery , Dhaka Medical Collge,Dhaka.
2. Associate Professor, Department of Orthopaedic Surgery , Dhaka Dhaka Medical Collge,Dhaka.
3. Assistant Professor, NITOR,Dhaka
4. Assistant Professor, Department of Surgery, Cox’s Bazar Medical College, Chittagong
Correspondense to: Dr. Md. Saidul Islam, Associate Professor, Department of Orthopaedic Surgery, Dhaka Medical College, Dhaka
E-mail: [email protected]
INTRODUCTION
Distal femoral fractures are associated with high energy
trauma in young adults and osteoporotic bone in elderly1.
and are frequently comminuted and intra-articular.
Metaphysial comminuttion is a challenge to conventional
plate fixation.The locking condylar plate (LCP) forms a fixed
angle construct and enables placement of the plate without
any contact to the bone2,3. It can therefore be used in
metaphysical comminution. The pull-out strength of the
locking screw is substantially higher than that of
conventional screws and it is difficult for one screw to pull-
out or fail unless all adjacent screw do so4. This enables a
better hold in osteoporotic bones.LCP is anatomocally
precontoured ,so it reduces soft tissue problem and act as
internal external fixator5. LCP is suitable for minimal invasive
percutaneous plate osteosynthesis (MIPPO) for distal
femoral fracture. MIPPO is a type of biological plate
osteosynthesis, is important to preserve bone
vascularization, to improve consolidation, to decrease
infection rate, and bone grafting.
Our goal of this study was to assess the functional
outcome of MIPPO technique using Locking condylar
plate for distal femoral fractures.
MATERIAL AND METHOD
This was a prospective study which was carried out at
Orthopaedic department of Dhaka Medical college and
different private clinic in Dhaka,Bangladesh during the
period from July 2o12 to June 2014. Our study comprising
20 patient of either sex with distal femoral fractures
underwent minimally invasive percutaneous plate
osteosynthesis using LCP . Age range of the patient was
18 to 65 years, mean age was 48 year. 16 patient were
male , 4 patient were female.The causes of injury were
vehicular accidents(n=18),falls(n=2).According to AO/
OTA classification,the fractures were classified as types
VOL. 29, NO. 2, JULY 2014 167

A1(n=7 )A2 (n=6) A3(n=3 ),C1(n=3),C2(n=1) (Table -1).All
the fractures were closed.Two patient had contralateral
femer fractures ,one patient had ipsilateral middle tthird
fracture of tibial and fibular shaft which were treated with
intramedullary interlocking nailing. 13patient were rihgtt
side 7 were left sided .
The method used for fracture fixation was minimally
invasive percutaneous plate osteosynthesis (MIPPO)
with locking condylar plate . ( Fig I and 2)
Inclusion Criteria
1. Those patients who were above the age of 18 yrs of
either sex.
2. Type A, Type C1,C2 according to AO/OTA classification
system ,both closed and Gustillo type -1.
3. Patient willing for treatment and given informed written
consent.
Exclusion criteria
1. Patient aged below 18.
2. Fractures more than 3 wks old.
3. Gustillo type II and III fractures,pathological fracture
other than osteoporotic fractures and fractiure types
B and C3 of AO/OTA classification were excluded.
RESULTS
The mean operating time was 80 (range 60-110 )
minutes.The mean length of hospital stay was 14(8- 21 )
days. The mean follow-up period was 14 months (range 4-
24 monthes).
Partial weight bearing was usually achieved at 8 wks
and full weight bearing was started around 18 weeks
according to signs of union on follow-up.Follow-up was
given for 2 years with evaluation at 2 weeks , 4 weeks , 6
weeks ,12 weeks and then every 6 weeks interval upto 6
months and thereafter 3 monthly interval onward. (Fig.-
3 and 4)
The average time to union was 18.5 weeks. The mean
flexion was 105egrees. (range 85-140)The extensor lag
ranged from 0 degree to 10 degree with an average of 4
degree. Out of 20 patient 2 had leg length discrepancy.
One patient had shortening of <1 cm and another patient
had shortening 1.5 cm.Two patient had 05degree varus
and one patient had 06 degree valgus malalignment. One
patient had superficial infection.
Functional outcome was assessed using Schatzker et al.(7)
scoring system. Excellent in 5 patients(25%),good in 12
patients (60%), fair in 3 patients (15%) (Table-I).
Table –I
Functional outcome and fracture type
Type of Excellent Good Fair Failure Total
fracture
A1 4 3 0 0 7
A2 1 5 0 0 6
A3 0 2 1 0 3
C1 0 2 1 0 3
C2 0 0 1 0 1
Total 5 12 3 0 20
Table-II
Radiological union
Union (Weeks) No. of cases Percentage
< 16 1 5%
16-18 14 70%
19-20 3 15%
21-22 2 10%
Non-union Nil Nil
Table-III
Knee flexion
Knee Flexion (Degrees) No. of cases Percentage
>90 02 10
91-109 06 30
11o and more 12 60
Fig.-1: (a) Distal and proximal incision, (b) Pre-operative x-ray, (c) X-rray at 12 Wks (d) X-ray at 18 wks
(a) (b) (c) (d)
168 Functional Outcome of Minimally Invasive Percutaneous Plate Osteosynthesis Using Locking Condylar Plates
The Journal of Bangladesh Orthopaedic Society

DISCUSSION
There are different modalities of treatment for distal femoral
fractures.They include direct reduction and internal fixation
with condylar buttress plates, retrograde nailing,dynamic
condylar screws , external fixators, open minimal invasive
approaches,Indirect reduction and plate osteosynthesis
using a locking condylar plate by MIPPO technique or by
less invasive stabilization system (LISS). (6).Good fixation
outcomes depends on bone quality,fracture complexity
and surgical techniques.
Conventional screw-plate systems (condylar buttress
plates and dynamic condylar screws) depends on the bone
–plate interface for stability1,7,8. When screw are
tightened,the plate compresses against the cortex and
maintain stability.The stability of the standard screw
depends on bone quality. So in metaphysical
comminution,in osteoporotic bone ,the holding power of
the screw is compromised leading to failure of screw –
plate system.More over fixation with DCS requires at least
4 cm of uncomminuted bone in the femoral condyles above
the intercondylar notch9. This limits its use in more distal
extr-articular fractures.Soft tissue striping during
conventional plating adds a biological insults to the poor
bone quality as in metaphyseal comminution and
osteoporotic bones.These may lead to poor outcomes such
as non-union,implant failure,malunion and infection10.
Retrograde intramedullary nailing involves joint opening
and is associated with joint stiffness,protrusion of nail in
the joint,patellofemoral problems and knee sepsis9.
Locking plate system such as the LCP have been
extensively used for distal femoral fractures.It has a lower
risk of early implant loosening than DCS and promote
early mobilistion and rapid healing without bone grafts
.The LCP differ from LISS in that the LCP has combination
holes (6) and does not have a jig.
LCP acts on the internal fixator principle 9 and enables
percutaneous plating.The LCP is compatible with MIPPO.
Many studies combining the LCP and MIPPO/MIPO have
shown improved results.
In our study all the 20 fractures were treated by indirect
reduction and internal fixation by LCP . The size of the
plate was selected based on the type of fracture. Of 20
patient 14 patient (70%) showed radiological union within
18 weeks. Sk Venkatesh et al. showed 73% radiological
union within 18 weeks, J.P.S et al(11). showed 100% mean
time of radiological union 16.2 weeks. Normal knee flexion
is 140 degrees.Thus ,acceptable knee flexion compatible
with daily activity would be 110 degree.Average flexion in
this study was 105 degree with 60% patient having range
of knee flexion more than 110 degrees. Sk Venkatesh et al.
showed 50 % patient with more than 110 degreeknee flexion
and J.P.S et al showed 36 % patient with more than 110
degree knee flexion. This difference may be due to we had
given early knee movement, no post operative back slub
given.
In this study , overall results were tabulated in four groups
i.e Excellent, good ,fair and failure according to the criteria
Schatzker et al.(7 ) scoring system.Out of 20 cases 17
cases had acceptable result (i.eExcellent and good) and 3
cases had poor result. Ravi Nayak et al. (12). obtained
excellent and good outcomes in 29 out of 31 cases.19
CONCLUSION
MIPPO with Locking condylar plate achieves favorable
biological fixation for distal femoral fractures for early
fracture union and less complications especially when
fracture is comminuted and osteoporotic.
REFERENCES
1. T.F Higgins. Distal femoral fracture. The Journal of Knee
Surgery, Vol 20,No 1 p 56-66,2007.
2. Mast J,Jakob R, Genz R.Planing and reduction technique
in fracture surgery.Springer- Verlage,New yourk 1989.
3. Brunner CF,Weber BG.Antiglide plate ,In:mBrunner
CF,Weber BG;eds Osteosynthesis technique,Berlin:
Springer 1982.
4. Scultz M,Sudkamp NP; Revolution in plate
osteosynthesis: New internal fixator system. J. Orthop
Sci. 2003; 8:252-8.
5. Close reduction by manipulation and minimally invasive
percutaneous plate osteosynthesis for the treatment of
supracondylar femer fracture .Orthopaedic Hospital of
Sichuan, Chengdu 610041,Sichuan China,2011.
6. Hontzsch D. Distal femoral fracture - technical
possibilities(In German),Kongressbd Dtsch Ges Chir
Kongr 2001;118:371-4.
7. Schatzker J,Tile M. The rationale of operative fracture
care.Berlin: Springer Verlage;1987.
8. Klaue K.Principles of plate and screw osteosynthesis.In
Bulstrode C, Buckwalter J, Carr A, editor. Oxford textbook
of orthopaedics and trauma. Oxford: oxford University
press; 2002:1697-710.
9. Whittle AP, Wood II GW.Fracture of the lower
extremity.In: canale ST,editor. Campbell’s operative
orthopaedics. Vol 3, Philadelphia:Mosby; 2003;2725.
10. Grewiwer RM.Archdeacon MT.Locking plate technology:
current concepts. J knee surg 2007; 20; 50-5.
11. J.P.S et al. Minimally Invasive Plate Osteosynthesis for Distal
femoral Fractures.JIMSA Oct-Dec.2014 Vol. 27 No 4.
12. Ravi Nayak, MR Koichade,Alok N. Minimally Invasive
Plate Osteosynthesis for Distal femoral Fractures. J Orthop
Surg 2011;19 (2): 185-90.
Md. Saidul Islam, Md. Golam Mostafa, Shah Jawaher Jahan Kabir, Shahidul Haq 169
VOL. 29, NO. 2, JULY 2014
Original Article
Posterior Long Segment Transpedicular
Screw Fixation for Unstable
Thoracolumbar Fractures with
Incomplete Spinal Cord Injury
Syed Shahidul Islam1, M R Karim2, Purnendu3, Meraj 4, Azad5, Swapan 6, Rahman7,
Rayhan Hamid8, Susmita9
ABSTRACT
Prospective study. To evaluate the outcome after long segment pedicle instrumentation in unstable fractures of
the thoracolumbar spine with incomplete neurological deficits.
We reviewed the outcome in 40 patients (32 males and 8 females) of unstable thoracolumbar fractures with
incomplete neurological deficits who underwent long segment pedicle screws & rod fixation and fusion from
January 2009 to January 2013 at National Institute of Traumatology and Orthopaedic Rehabilitation (NITOR),
Dhaka, Bangladesh. Mean age was 33.3years (range 14-55 years). Leading cause of fracture was motor vehicle
accident. Involvement of T12, LI & L2 was noted, respectively in 12, 17 and 11 patients. According to the ASIA
impairment scale 5 patients had B, 25 patients had C, 9 patients had D and 1 patients had E scale. The mean
follow-up was 13.2 months (Range 10-42 months).
According to Modified Macnab criteria functional result were excellent in 22 patients (55%) good in 14 patients
(35%). fair in 3 patients (7.5%) & poor in 1 patients (2.5%). Neurological recovery of one or more ASIA Impairment
Scale was seen in all patients. There is no implant failure, correction loss and complication.
Long segment pedicle screw fixation for unstable thoracolumbar fracture with incomplete neurological deficit
achieves adequate fixation without implant failure and correction loss and gives satisfactory results.
Keywords: Thoracolumbar fracture, Unstable, incomplete neurological deficits, long segment instrumentation.
1. Associate Professor, National Institute of Traumatology & Orthopaedic Rehabilitation (NITOR), Dhaka, Bangladesh.
2. Asst. Professor, National Institute of Traumatology & Orthopaedic Rehabilitation (NITOR), Dhaka, Bangladesh.
3. Asst. Professor, National Institute of Traumatology & Orthopaedic Rehabilitation (NITOR), Dhaka, Bangladesh.
4. Registrar,, National Institute of Traumatology & Orthopaedic Rehabilitation (NITOR), Dhaka, Bangladesh.
5. Asst. Registrar, National Institute of Traumatology & Orthopaedic Rehabilitation (NITOR), Dhaka, Bangladesh.
6. Asst. Professor, National Institute of Traumatology & Orthopaedic Rehabilitation (NITOR), Dhaka, Bangladesh.
7. Medical Officer, National Institute of Traumatology & Orthopaedic Rehabilitation (NITOR), Dhaka, Bangladesh.
8. Registrar, National Institute of Traumatology & Orthopaedic Rehabilitation (NITOR), Dhaka, Bangladesh.
9. Lecture, Physiotherapy. National Institute of Traumatology & Orthopaedic Rehabilitation (NITOR), Dhaka, Bangladesh.
Correspondence: Dr. Syed Shahidul Islam, Associate Professor, National Institute of Traumatology & Orthopaedic Rehabilitation
(NITOR), Dhaka, Bangladesh.
INTRODUCTION
Thoracolumbar junction is the mechanical transition zone
between rigid thoracic and more mobile lumbar spine which
predispose to failure. Injury to the cord or cauda equina
associated with 14 to 38% .25
The treatment of thoracolumbar fractures remains
controversial15,22. Although most authors believe that
surgical treatment is needed for unstable fractures, the choice
for operative approaches remains disputed2,5,22. Common
opinion is to obtain the most stable fixation by fixating as few
vertebrae as possible and neural canal decompression1,2.
Short-segment posterior instrumentation (SSPI) is the most
common and simple treatment, offering the advantage of
incorporating fewer motion segments in the fusion18. A
170 The Journal of Bangladesh Orthopaedic Society

review of the literature showed that SSPI alone led to a 9-
54% incidence of implant failure and re-kyphosis in the
long-term, and 50% of the patients with implant failure
had moderate-to-severe pain2: To prevent this, several
techniques have been developed to augment the anterior
column in burst fractures, such as transpedicular bone
grafting2, 18, 19, placement of body augmenter5,
polymethylmethacrylate (PMMA) injection6, anterior
instrumentation and strut grafting17, or long-segment
posterior fixation (LSPF)1,6.
There are few controlled studies explaining the reasons
for implant failure and re-kyphosis for thoracolumbar
fractures2. In the current study, only patients with
thoracolumbar junction (T12-L2), fractures were included.
The aim of the present study was to determine the proper
treatment choice for thoracolumbar junction fracture.
MATERIAL AND METHODS
Between January 2009 and January 2013, 40 patients with
acute, traumatic fractures of the thoracolumbar junction
were treated with long-segment transpedicular screw
fixation.
In LSP screw fixation we applied eight screws: two levels
above and below the fracture. All the operations were
performed by us without any discriminations according
to the fixation type. The authors had decided to apply
long-segment posterior instrumentation during the
operation, till January 2013.
Screws were 40 or 45 mm long, depending on the level and
size of the vertebra. At the tenth and eleventh thoracic
levels, 5.5 or 6.5-mm-diameter multiaxial screws and at the
twelfth thoracic level and caudally 6.5-mm-diameter
multiaxial screws were used. The instrumentation was
applied by laterally and cross-links were used to augment
torsional rigidity. Reduction of the fracture was
accomplished by the rod contouring and extension and
compression-distraction forces before tightening the
screws. Patients were a thoracolubar brace for two months.
Complete clinical and radiologic examinations were done on
admission. Clinical and radiographic follow-up was at 1, 3, 6,
and 12 months and every year thereafter. Data were collected
concerning age, sex, localization, presence of neurological
deficits, pain and work status, mobility complications and
radiologic parameters. Correction loss was defined as an
increase of more than 10R” SI in the latest follow-up
radiographs compared with the measurement on the initial
post-operative radiographs. Neurologic assessment was
done using ASIA Impairment scale. Modified Macnab Criteria
is used for categorizing the outcome of surgery.
RESULTS
Postoperatively, kyphosis was corrected by more than
10° in 33 (82.05%). Last follow-up values showed a
correction of more than 10° in 26 patients (26%) Correction
loss more than 10° was found 4 (10%). All patients with
incomplete neurologic injuries improved. In ASIA Impairment
scale two grade of improvement in 23 (57.5%) patients and
one grade of improvement in 17 (42.5%) patients.
Male, Age 30 yrs, L1 Fracture with incomplete SCI Preoperative X-ray and MRI
Immediate post operative X-ray and follow up X-ray after 1 year
Posterior Long Segment Transpedicular Screw Fixation for Unstable Thoracolumbar Fractures 171
VOL. 29, NO. 2, JULY 2014

corrective force over multiple levels and the reduction of
the likelihood of implant failure.
Serin et al.23 reported that four level posterior fixation is
superior to two level posterior fixation. Tezeren et al[25
demonstrated that final outcome regarding sagital index
and anterior body compression is better in the long
segment instrumentation group than short segment
instrumentation group.
In this surgical method we need the statistical analysis of
cobb angle, Kyphotic deformity anterior body compression.
The thoracolembar junction contributes the transitions
zone between the rigid thoraces and mobile lumbar spine.
Vertebral fracture in this area are usually extremely unstable
and Kyphotic deformity is often significant degree
therefore inserting the screw only one level above and
below the fractured segment might not have provided
adequate stability Gurr et al[14 found that two level above
and below the injured level in an unstable calf spine model
provided more stiffness than the intact spine. Carl et al4
reported that segmental pedicular fixation two level above
the kyphosis should be used at the thoracolumbar junction,
where compression force act more antereorly.
Post operative correction loss after posterior
instrumentation has been reported by many authors. The
mean correction loss ranged from 0.3º to 15.4º has been
reported in may authors. In our study mean correction
loss is 3.2º. In our study no there were no instrument
failure.
Selection of the surgical method in the treatment of
thoracolumbar fractures remains a matter of
discussion2,5,6,8. Multiple parameters have to be
considered, such as the type and stability of the fracture,
degree of CC, and neurological status26. SSPF is frequently
regarded as the procedure of choice because it offers
advantages such as incorporating fewer motion segments
in the fusion, shorter operative time and fewer blood
transfusions. But without body reconstruction, many
authors believe that transpedicular bone grafts have not
prevented early implant failure and correction loss, and
may lead to low anterior inter body fusion rates in the long
term2,18,21. Recently, PMMA was reported to strengthen
the fractured body and prevent instrument failure, but the
long-term result is unknown6. Injection of PMMA into a
fractured vertebral body may lead to cement extrusion
into the spinal canal, particularly if the posterior
longitudinal ligament is torn. Anterior instrumentation and
strut grafting have proven to be effective17, but require a
more invasive approach, prolonged operation may cause
blood loss and morbidity.
Table-I
Neurological recovery after surgery
ASIA Scale Preoperative Latest Follow-up
A B C D E
B 5 - - 2 3 -
C 25 - - - 5 20
D 9 - - - - 9
E 1 - - - - 1
*Two grade of improvement in 23 (57.5%) patients*One grade
of improvement in 17 (42.5%) patients.
Table-II
Surgical outcome with modified Macnab criteria
Excellent 22 patients (55%)
Good 14 patients (35%)
Fair 3 patients (7.5%)
Poor 1 patients (2.5%)
In the last follow-up visit, all 40 patients there were no
implant failures, including no screw breakage, or loosening.
According to Modified Macnab criteria functional result
were excellent in 22 patients (55%) good in 14 patients
(35%). fair in 3 patients (7.5%) & poor in 1 patients (2.5%).
Neurological recovery of one or more ASIA Impairment
Scale was seen in all patients. There is no implant failure,
correction loss and complication.
DISCUSSION
It is widely accepted that thoracolumbar frature should be
addressed surgically2. The goals of treatment of
thoracolumbar fracture regardless of the selected method
are the restoration of the stability of the vertebral column,
prevention and correction of collaps and deformity, the
decompression of the spinal canal, protection of intact or
incompletely injured neural element leading to earlier
mobilization of the patient. Short segment pedicle
instrumentation is popular since Dick et al10 have
developed the SS stabilization. However there is a
controversy as far as the result of this instrumentation are
concerned. There are studies that report high rate of failure
because of proximal screw pullout, screw breakage and
loss of correction even if material failure does not always
affect the clinical outcome21.
The advantage of long segment instrumentation that used
in this study is the immediate mobilization of the patient
with less depending of bracing, the distribution of
172 Syed Shahidul Islam, M R Karim, Purnendu, Meraj, Azad5, Swapan, Rahman, Rayhan Hamid, Susmita
The Journal of Bangladesh Orthopaedic Society

CONCLUSION
The recent literature does not provide a gold standard for
the treatment of thoracolumbar fractures. Therefore, the
choice of therapy should be made individually, considering
the type and severity of fracture, the neurological status
and the patient’s condition as well as the skill of the
surgeon. LSPS fixation of unstable thoracolumbar spine
fracture can provide more secure fixation & better
correction of deformity and avoiding correction loss with
patients’ satisfaction. Long-term follow-up needed for
clear evaluation.
REFERENCES
1. Akbarnia BA, Crandall DO, Burkus K et al (1994) Use of
long rods and a short arthrodesis for burst fractures of
thethoracolumbar spine. A long-term follow-up study. J
Bone Joint Surg Am 76(11):1629-1635
2. Alanay A, Acarolu E, Yazici M et al (2001) Short-segment
pedicle instrumentation of thoracolumbar burst fractures:
does transpedicular intracorporeal grafting prevent early
failure. Spine 26(2):213-217
3. Boerger TO, Dickson RA (2000) Does canal clearance
affect neurological outcome after thoracolumbar burst
fractures? J Bone Joint Surg Br 82(5):629-635
4. Carl AL, Tromanhauser SG, Roger DJ (1992) Pedicle screw
instrumentation for thoracolumbar burst fractures and
fracture-dislocations. A calf spine model. Spine 17:317-
324
5. Chen HH, Wang WK, Li KC et al (2004) Biomechanical
effects of the body augmenter for reconstruction of the
vertebral body. Spine 29(18):382-387
6. Cho DY, Lee WY, Sheu PC (2003) Treatment of thoraco
lumbar burst fractures with polymethyl methacrylate
vertebroplasty and short-segment pedicle screw
fixation. Neurosurgery 53(6):1354-1360
7. Dall BE, Stauffer ES (1988) Neurologic injury and recovery
patterns in burst fractures at the T12 or LI motion segment.
Clin Orthop 233:171-176
8. De Peretti F, Howorka I, Cambas PM et al (1996) Short
device fixation and early mobilization for burst fractures
of the thoracolumbar junction. Eur Spine J 5:112-120
9. Denis F, Armstrong GWD, Searls K et al (1984) Acute
thoracolumbar burst fractures in the absence of neurologic
deficit: a comparison between operative and nonoperative
treatment. Clin Orthop 189: 142-149
10. Dick W, Kluger P, Magerl F, Woersdorfer O, Zach G. A
new device for internal ‘fixation interne’. Paraplegia 1985:
23(4): 225-32.
11. Farcy JP, Weidenbaum M, Classman SD (1990) Sagittal
index in management of thoracolumbar burst fractures.
Spine 15(9):958-965
12. Frankel HL, Hancock DO, Hyslop G et al (1969) The
value of postural reduction in the initial management of
closed injuries of the spine with paraplegia and tetraplegia.
Para plegia 7:179-192
13. Gertzbein SD, Court-Brown CM, Marks P et al (1988)
The neurologic outcome following surgery for spinal
fractures.Spine 13:641-644
14. Gurr KR, McAfee PC (1988) Cotrel-Dubousset instrumen
tation in adults. A preliminary report. Spine 13:510-520
15. Kaneda K, Taneichi H, Abumi K et al (1997) Anterior
decompression and stabilization with the Kaneda device
for thoracolumbar burst fractures associated with
neurological deficits. J Bone Joint Surg Am 79(l):69-83
16. Katonis PG, Kontakis GM, Loupasis GA et al
(1999) Treatment of unstable thoracolumbar and lumbar
spine injuries using Cotrel-Dubousset instrumentation.
Spine 24(22):2352-2357
17. Kim NH, Lee HM, Chun IM (1999) Neurologic injury
and recovery in patients with burst fracture of the
thoracolumbar spine. Spine 24:290-293
18. Knop C, Bastian L, Lange U et al (2002) Complications in
surgical treatment of thoracolumbar injuries. Eur Spine J
ll(3):214-226
19. Knop C, Fabian HF, Bastian L et al (2002) Fate of the
transpedicular intervertebral bone graft after posterior
stabilisation of thoracolumbar fractures. Eur Spine J
11(3):251-257
20. Knop C, Fabian HF, Bastian L et al (2001) late results of
thoracolumbar fractures after posterior instrumentation
and transpedicular bone grafting. Spine 26(l):88-99It)
spring.
21. Kramer DL, Rodgers WB, Mansfield FL. Transpedicular
instrumentation and short-segment fusion of
thoracolumbar fractures: A prospective study using a single
instrumentation system, J Orthop Trauma 1995; 9(6):
499-506.
22. McLain RF, Sparling E, Benson DR. Early failure of short
segment pedicle instrumentation for thoracolumbar burst
fractures. A preliminary report, J Bone Joint Surg Am
1993; 75(2): 162-7.
23. Serin E, Karakurt L, Yilmaz E, Belhan O, Varol T, Effectys
of two- levels, four-levels, and four-levels plus offset-
hook posterior fixation techniques on protecging the
surgical correction of unstable thoracolumbar vertebral
fractures: a clinical study. Eur J Orthop Surg Traumatol
2004; 14 (I): 1-6.
24. Saboe, Limda; Reid, David; Davis; Lylea Warrer, Sharon,
Grace. Spine Trauma and Associate injuries. Journal of
Trauma & Acute care surgery, January 1991.
25. Tezeren G, Kuru I. Posterior fixation of thoracolumbar
burst fracture: Short-segment pedicle fixation versus long-
segment instrumentation. J Spinal Disord Tech 2005;
18(6): 485-8.
26. Wenger DR, Carollo JJ. The machanism of thoracolumbar
fractures stabilized by segmental fixation. Clin Orthop
1984; (189):89-96.
Posterior Long Segment Transpedicular Screw Fixation for Unstable Thoracolumbar Fractures 173
VOL. 29, NO. 2, JULY 2014

Original Article
Management of Open Gustilo IIIB Tibia-
Fibula Fractures By Soleus Muscle Flap
and Locally Made AO External Fixator
Abdullah Al-Mahmood Bilal1, Mir Hamidur Rahman2 , Mohammed Abdus Sobhan3 Milon Krishna
Sarker4, Md.Wahidur Rahman5 M Monaim Hossen6
ABSTRACT
This prospective study of ‘‘ Management of open Gustilo IIIB tibial fractures by soleus muscle flap and locally
made AO external fixator produce good success rate’’ was carried out with 26 patients of Gustilo, type IIIB open
fracture of the tibia-fibula during the period of July 2000 to June 2002 at NITOR. Out of 26 patients, 4 patients were
lost from the follow up. So ultimately the final result based on the results of 22 patients. In this study patients were
randomly selected irrespective of age and sex. Open fracture type IIIB (middle 1/3rd) were selected only. Polytrauma
patients were excluded from the study. Most common age group in this series were 26-35 years (41%) age group.
Lowest age was 16 years and highest age was 52 years with mean age 30 years. Male were more commonly
affected than female with a ratio of 9:2. Most common fracture were comminuted (63%). Right side involvements
were more (55%). Soleus muscle flap coverage with external fixator was done in all cases. Partial flap failure in
8 cases (36%) which were managed by cross leg fasciocutaneous flap in 6 cases and split thickness skin graft
in 2 cases. Various complications were observed. Commonest one was infection. Out of these bone infection
55%, soft tissue infection 36%, pin tract infection 10%. Non union was observed in 12 cases (55%). Out of these 8
were managed by BMP, 3 cases by bone graft and 1 by Illizarov external fixator. Leg length discrepancy in 7 cases
(32%) of which 5 was acceptable managed by heel raised shoe and other two by Illizarov external fixator. Varus
angulation of about100 in 1 case (4%),50 in 1 case (4%) and 100 valgus in 1 case (4%) was observed. None of the
cases developed compartment syndrome. Stiffness of ankle were observed in 6 cases (27%).According to
criteria of Tucker et al. (1992) final results of treatment were analyzed. Acceptable results were in 72.73% of
cases ( Excellent 22.73% and good 50%), 27.27% cases were not acceptable (Fair 9.09% and poor 18.18%)
1. Assistant Professor (C,C) OSD, DGHS, attached Abdul Malek
Ukil Medical College, Noakhali
2. Assistant Professor, OSD, DGHS, attached Abdul Malek Ukil
Medical College, Noakhali
3. Senior Consultant, 250 bedded General Hospital Noakhali,
4. Assistant Professor, OSD, DGHS, attached Abdul Malek Ukil
Medical College, Noakhali
5. Associate Professor, NITOR, Dhaka
6. Associate Professor, NITOR, Dhaka
Correspondence: Dr. Abdullah Al-Mahmood Bilal, Assistant
Professor (C,C) OSD, DGHS, attached Abdul Malek Ukil Medical
College, Noakhali
INTRODUCTION
An open tibia-fibula fracture has been the most challenging
problem of all long bone injuries (Gustilo, 1993). Gustilo
(1993) Developed the historiocal and world wide accepted
classification system of open fractures of Tibia-Fibula that
is relevant to both treatment and outcome. The problem is
challenging because high incidence if sepsis and other
complications like chronic osteomyelitis, malunion,
nonunion and amputation. Among the trauma patients
open fracture of the tibia fibula comprises a substantial
group who requires careful attention to prevent mortality
as well morbidity. Because one third of its surface is
subcutaneous throughout most of its length, open
fractures are more common in the tibia than in any other
major long bones. Furthermore the blood supply to the
tibia is more precarious than that of bones enclosed by
muscles. The emergency department of National of
Traumatology and Orthopaedic Rehabilitation (NITOR) is
to manage huge number of open tibia-fibula fracture of
different types each and everyday. It is also a common but
sorrow picture to have a good number of patients occupying
the hospital beds for long duration. Their broken pieces of
bones smiling at the surgeons are surrounded by hundreds
of thousands of bacteria along with devitalizing tissues
resulting from open fracture tibia-fibula.
174 The Journal of Bangladesh Orthopaedic Society

The goal of treatment of an open fracture are prevention
of infection, healing of the fracture and restoration of
function of the extremity.
Gustilo type IIIB open fractures are characterized by:
(1) Extensive soft tissue loss.
(2) Extensive periosteal stripping with a large fragment
of bone exposed.
(3) Massive contamination.
(4) Severe fracture Comminution
The essential criterion is that after adequate debridement
and irrigation, a segment of bone exposed that requires
flap coverage . Regarding the timing of wound closure,
there is no place primary closure in open fractures
irrespective of any because of increased sepsis and the
risk of gas gangrene(Gustilo,1993) suggested wound
closure in type lllB fractures within three to five days.
Adequate debridement and early assessment of the soft
tissue defect are necessary so that appropriate soft tissue
coverage can be provided within first one to two weeks
(Fisher et.al.,1991).In present study the badly
contanminated wounds were covered, when judged to
be clinically & bacteriologically fit for ,between 5 th to 21st
trauma. According to the just mentioned study early
muscle-flap coverage has been termed when done within
ten days after injury. It usually took at least 3-5 days to
stabilize both the wound and the patient. Why muscle-
flaps has been selected ? The advantages of muscle flaps
are:
(1) Muscle have a rich blood supply with distinct vascular
pedicle which enhance fracture union
(2) The vascular pedicle is often located outside the
surgical defect owing to the are of rotation and the
length of the muscle
(3) The muscle provides bulk for deep , extensive defects
and protective padding for exposed vital structures
(4) Muscle can be mainpulated to prouduce a desired
shape or volume
(5) well-vascularized muscle is resistant to bacterial
inoculation and infection
(6) Reconstruction using muscle is often a one stage
procedure
(7) The reliability and availability of soleus muscle make
them an excellent alternative means of reconstruction
when the method of choice for a particular defect is
unavailable or inadequate
(8) Negligible morbidity of donor site (Mc Carthy, 1990).
AIMS AND OBJECTIVES OF THE STUDY
Aims:
To find out the bitter method of management of open
Gustilo IIIB fracture of the tibia in context of our socio-
economic condition
Objectives :
1. Union of open Gustilo IIIB fracture of fibula after solues flap.
2. To evaluate the success rate of soleus muscle flap
transposition for coverage.
3. Soft tissue healing
Functional assessment of the survived limb with or without
complications
Patients and methods
Type of the Study
This prospective study was carried out to evaluate the
results of management of open Gustilo IIIB tibia-fibula
fractures by soleus muscle flap coverage and locally made
AO external fixator.
Place and period of study
This study was carried out at National Institute of Trauma
and Orthopaedic Rehabilitation, Dhaka; during the period
of July 2000 to June 2002.
Sample Size
A sample size of 26 patients were taken. Out of 26 cases
four cases were dropped out from the follow-up. Hence,
this study comprises 22 cases.
Sampling Technique
Sampling was purposive as guided by some inclusion and
exclusion criteria.
Criteria for selection of patients
Inclusion Criteria
These were as follows :
1. Cases were randomly selected between 16-50 years
2. facture of any side of tibia and fibula.
3. Only open fracture shaft of the tibia and fibula (Middle
1/3 rd )
4. Only open fracture-Gustilo type IIIB irrespective of
fracture configuration viz oblique, transverse, spiral
segmental, comminuted or with loss of bone.
5. Open fracture on same day of injury.
EXCLUSION CRITERIA
1. Polytrauma patients
2. Diabetic patients
3 Patients of peripheral vascular disease
4. Any open fracture except type IIIB (Middle 1/3 rd )
5. General condition of patient not fit for general or spinal
anaesthesia
Management of Open Gustilo IIIB Tibia-Fibula Fractures By Soleus Muscle Flap and Locally Made AO External Fixator 175
VOL. 29, NO. 2, JULY 2014

Data Collection Protocol
A questionnaire and checklist was designed consisting of
variables related to patients , treatment timing, soft tissue
management fracture management. Data protocol includes
history, physical examination, clinical examination,
radiological assessment, wound care and management.
Data Analysis
Once data collection was completed, data were complied
manually according to the key variable .All statistical
analysis of different variable were analyzed according to
standard statistical method and calculation done by using
scientific Calculator.
Observation and Result
In the present series, the following observations were noted:
Age Incidence : in this study there were 22 patients with
age range 16-52 years . Mean age 30 years. Maximum
incidence was in 26-35 years age group.
Table-I
Showing different age group in the present series.
(Age in year) Number of patients Percentage (%)
16-25 07 31.82%
26-35 09 40.90%
36-45 05 22.73%
46-60 01 4.55%
N=22
Sex Distribution: In the present series, 18 were male and 4
female. Male female ratio 9:2
Table-II
Showing sex distribution of patients in present series.
Sex Number of patients Percentage (%)
Male 18 81.82%
Female 04 18.18%
N=22
Side Involved:
In the present series, right side involvement were in 12
cases and left side involvement ni 10 cases.
Table-III
Showing side of the injury in this series.
Side Number of patients Percentage (%)
Right 12 54.55%
Lift 10 45.45%
N = 22
Location of fracture: in this series all 22 (100%) cases of
open gustilo IIIB fracture were in the middle 1/3 rd of the
shaft of tibia.
Gusstilo Type of feacture: in this series all 22 (100%)
cases were type iiiB:
Causes of injury : in this series, motor vehicle accident
were found in 17 cases, assault in 2 cases, machinery
injury in 3 cases.
Table-IV
Showing causes of injury in this series.
Causes of Injury Number of patients Percentage (%)
Motor Vehicle Accident 17 77.27%
Assault 2 9.09%
Occupational 3 13.64%
N = 22
Configuration of Fracture:
In the present series, fractures configuration were comminuted
in 14, oblique in 5, transverse 1 and segmental in 2.
Table-V
Showing configuration of fracture in this series.
Fracture Configuration No. of patients Percentage
Comminuted 14 63.64%
Oblique 5 22.72%
Segmental 2 9.09%
Transverse 1 4.55%
N=22
Occupation of Patients:
People of different occupations were patients of open
fractures tibia- fibula found in this study.
Table-VI
Showing occupation of patients in this series.
Occupations Number of patients Percentage (%)
Farmer 3 13.64%
Labour 7 31.82%
Businessman 2 9.09%
House wife 4 18.18%
Student 2 9.09%
Govt. Service 2 9.09%
Technician 2 9.09%
N = 22
176 Abdullah Al-Mahmood Bilal, Mir Hamidur Rahman, Mohammed Abdus Sobhan, Milon Krishna Sarker, Md.Wahidur Rahman et al
The Journal of Bangladesh Orthopaedic Society

Soft tissue and fracture healing :
Table- XI
Showing incidence of Soft Tissue and fracture healing .
Healing Procedure employed Number of patient Percentage (%)
A. Soft Tissue Soleus Flap only 14 63.64%
Soleus Flap (>25%-50% failure) followed by cross leg flap 6 27.28%
Soleus flap (25% failure) followed by split thickness skin graft 2 9.08%
B. Fracture Primary healing Nil 0%
Secondary healing 10 (without bone graft/BMP) 45%
8 BMP 36.87%
3 (Bone graft) 13.63%
1 Ilizarov 4.54%
Incidence of Complications :
Table-XII
Showing incidence of complications in the present series
Complication Number of patient Percentage (%)
Infection
Soft tissue 8 36.37%
Pin-tract 2 9.09%
Bone 12 54.54%
Delayed union 8 36.37%
None Union 4 18.19%
Restriction of knee 6 27.28%
and ankle movement
Angulations 3 13.63%
Leg length discrepancy 7 31.82%
RESULTS
To choose an unique parameter for analysis of results is a
difficult task in open tibia fibula shaft fractures. These
injuries are associated with moderate to severe
complications because soft tissue, bone and adjacent joint
movements, all contributes to the final out come of the
result.Bony unions take much longer time than any
other bones body (Edward, 1988). Most difficult part of
the evaluation was the limited time of follow up for this
type of study. Gustilo et al. (1993) used following criteria
to define a satisfactory result:-
i) Fracture healing without sepsis.
ii) No mal alignment or angulatory deformity in excess of
valgus angulation 10 degrees, varus angulation 5
degrees, Anteroposterior angulation of 10 degrees
and shortening lcm.
iii) Near or near-normal joint motion of both knee and
ankle. Main disadvantage of this parameter is, they
did not graded their results. so, statistical analysis
and comparison of results of treatment is not possible.
Karlstrom et sl. (1975) used following parameters for
evaluation of their results of severe open fractures of tibia.
They graded the result as A, B, and C . (Table No. XIII)
Preoperative X-ray after injury Application of external fixator in open Gustillo IIIB fracture
tibia-fibula
Management of Open Gustilo IIIB Tibia-Fibula Fractures By Soleus Muscle Flap and Locally Made AO External Fixator 177
VOL. 29, NO. 2, JULY 2014

DISCUSSION
This study was carried out in order to find out an easy,
appropriate and well accepted technique for solving
prolonged suffering and complication of patients with
Gustilo type IIIB open tibia-fibula fractures involving
middle 1/3 rd . As a tertiary hospital like NITOR the
incidents of open fracture shaft of tibia-fibula are not
negligible encountered in daily practice in the casualty
department.
Out of 22 cases, all were type IIIB involving middle 1/3 rd
of shaft of the tibia-fibule. In this type cast immobilization
is very troublesome and difficult to maintain. Cast does
not allow access for serial debridement and dressing. It
soaks readily and needs frequent change which is quite
costly, time consuming and hampers maintenance of
fracture reduction. More over cast immobilization for
prolonged time leads to joint stiffness, muscle atrophy
and diffuse osteoporosis.
Most of our patients reported to hospital after golden
hours (>8 hours). Internal fixation in this situation by intra
medullary nailing or plating carries consequences of high
risk of bone infection (Edward, 1988) and in this cases
external fixation is this treatment of choice (Seligson, 1990;
Gustilo, 1993) for early wound care, sequential debridement
and early wound coverage.
In this study wound could not be covered within three
days, Possible causes were : a) All the cases were badly
Soleus muscle flap separation with
external fixation.
Check X-ray after external fixation
3 weeks after soleus muscle flap surgery Patient with partial
weight bearing at 8 weeks
178 Abdullah Al-Mahmood Bilal, Mir Hamidur Rahman, Mohammed Abdus Sobhan, Milon Krishna Sarker, Md.Wahidur Rahman et al
The Journal of Bangladesh Orthopaedic Society

contaminated and potentially infected b) Exact nature and
velocity of injury could not be ascertained c) correct
evaluation of local circulation of deep soft tissues is
unpredictable d) lack of sufficient operation theatre (O.T)
available which is overburdened with disproportionately
huge number of patients.
Definitely there is relationship between early wound
coverage and better results. In this study 10 cases (45%)
were covered at 5-10 days after injury and 12 cases (55%)
after 10 days of injury/. Flap success rate is 80% in early
covered cases and success rate dropped to 50% in late
covered cases. Out of 10 cases done within 5 to 10 days
extent of flap
Among the complications out of 22 cases, 12 developed
bone infection, 8 cases soft tissue infection, 2 pin tract
infection and 7 developed limb length discrepancy. No
specific infection (Gas gangrene, tetanus) were noted.
Wound swab yields growth of mixed bacteria (staph. aureus,
E.coli, Pseudomonas) which were resistant to almost all
usual antibiotics. They are very sensitive to Ciprofloxacin,
ceftriaxone, netilmycin.
Of the 12 cases of chronic osteomyelitis, sequestrectomy
done in all cases. After 6-8 weeks of sequestrectomy 11
cases developed aseptic nonunion and one infected
nonunion. Out of 11 aseptic nonunion cases 8 were treated
by BMP and 3 cases by autogenous bone graft. One
infected nonunion case was treated by Ilizarov extetnal
fixator.
Pin tract infection was managed by daily cleaning with
povidone iodine scrub and dressed with povidone iodine
ointment. Antibiotics were given according to culture and
sensitivity report. In one case external fixator was removed.
Soft tissue infection were managed by daily flushing with
normal saline followed by povidone iodine dressing.
Antibiotic was given according to culture and sensitivity
report till infection controlled.
After control of infection bony procedures (Bone graft,
BMPP) were done. necrosis was 25% occurred in 2 cases
(20%) and out of 12 eases done after 10 days extent of flap
necrosis was > 25%-50% occurred in 6 cases (50%).
Out of 10 soleus muscle flaps done earlier( within 10 days),
3 casses (30%) (case no.4,6,16) developed chronic
osteomyelities. so 70% open fractura can be protected
from infection. Out of 12 soleus muscle flaps done after 10
days, 9 cases (75%) developed chronic osteomyelities.
only 30% open fracture can be protected from infection in
late wound covered cases. In the study of fishier et al.(1991)
82% in early covered cases .(within 10 days) can be
protected from deep bone infection. After 10 days
protection rate dropped to 25%. so fisher et al. (1991) study
is nearly similar to this study.
Fracture union occurred unevently in 10 cases (45%). Bony
procedures (BMP/ bone graft) were done in rest of the 12
cases(55%). These results are comparable with Eshaque
et al. (2001) study.
In this series time of fracture healing was 5.5 to 12 months
with a mean of 7.5 months which is nearly similar to
Eshaque et al. (1991) study where time of fracture healing
is 5 to 10 months.
None of the patient developed neurovascular or
compartment injury during the study of this series. In this
series locally made AO external fixator was applied in 22
cases for stabilization of fracture on the same day of injury.
AO/ASIF External fixator, Hoffmann fixator, Ilizarov ring
fixators are costly and most of our patient can not afford
to purchase such set. So AO external fixator can be made
locally and cost is cheap which our patient can afford. So,
in other word cost benefit ratio is higher with locally made
AO external fixator than standard external fixators.
At the end of discussion I would like to express my overall
impression that early the wound was covered with muscle
flap and stabilization of fracture, the better was the
prognosis.
CONCLUSION
Open fracture in leg in mid third with exposed tibia, Gustilo
type IIIB can be better managed by immediate reduction
of fracture and immobilization by AO external fixator after
surgical toileting and application of soleus flap over the
exposed bone in due time. Post-operative care is very
important for soft and hard tissue healing.
REFERENCES
1. Connolly,TF 1085, ‘C0mmon available problems in
nonunions’, clin orthop, vol.194,no.2, pp.226-35.
2. Cove,JA, Llowe,DW, Jupiter,JB & Silsk,JM 1997, ‘The
management of femoral diaphyseal nonunions’, J. Orthop
Trauma ,voi11, no .4 ,pp.513-20.
3. Crawford,RA 1973, ‘A history of the treatent of nonunion
of fractures in 19 th century in the united states’, J. Bone
Joint Surg., vol. 55-A, no. 11, pp. 1685-97.
4. Curylo, LJ & Lindsey, RW 1984, ‘Shaft nonunions current
etiology & outcome of treatment”,Orthop Int, vol.2, no.5,
pp.465-73.
Management of Open Gustilo IIIB Tibia-Fibula Fractures By Soleus Muscle Flap and Locally Made AO External Fixator 179
VOL. 29, NO. 2, JULY 2014

5. Evans,F, Pederson, H & Lossiner, H 1951, “The role of
tensile stress in the mechanism of femoral fracture’, J.
Bone Joint surg, vol.33-A, no.3 , pp.485-501.
6. Furlong, AJ, Giannoudis, PV, DeBoer,P, Mathews,Sj,
MacDonal, DA & Smith, RH 1999 , ‘Exchange nailing for
femoral shaft aseptic nonunion’, INJURY, vil.30,
pp. 245-9.
7. Grosse,A, Kempf, I & Lafforgne, D 1978, ‘Treatment of
femoral fractures with interlocking imtramedullary nails :
A report of 40 cases’, Rev clin orthop, vol.64 (suppl.2),
pp.333-5.
8. Hak,DJ, Lee,SS & Goulet, JA 2000, ‘Success of Exchange
Reamed Intramedullary Nailing for Femoral shaft nonunion or
Delayed union’, J. orthop trauma, vol.14 ,no.3 ,pp.178-82.
9. Haper, M & Carson, W 1987, ‘Curvature of the femoral
and the proximal entry point for an intramedullary rod’,
Clin. orthop, vol.220,no.1, pp.155-6.
10. Heiple, KG, Figgi, HE, Lacey, SH & Figgie, MP 1985,
‘Femoral shaft nonunion treated by a fluted intramedullary
nail’, Clin. ortho, vol.194, no.2, pp. 218-25.
11. Heppenstall,RB 1984, ‘The present role of bone graft
surgery in treating nonunion’, Orthop clin North Am, vol.
15, no.1, pp.113-23.
12. Jhonson, KD, Tencer, AF & Blumenthal,S 1986,
‘Biomechanical performances of locked intramedullary nail
systems in comminuted femoral shaft fractures’, clin.
orthop, vol. 206,n.1, pp.151-61.
13. Caudle R. J. and Stern P. J. Severe open fractures of the
tibia. J. Bone and joint Surg. July 1987, 69-A : 801 807.
14. Chapman M. W. The role of intramedullary fexation in
open fractures,clin Orthop 1986; 212 : 26-34.
15. Charnley J. The Closed treatment of Common Fractures
(3rd ed), Livingstone, Edinburgh, 1961, P: 105.
16. Cierny, George HI, Byrd H. S. and Jones R. E. Primary
versus delayed soft tissue coverage for severe open
tibialfractures. A comparison of result. Clin. Orthop. 1983,
178 : 54-63.
17. De Bastiani G, Aldegheri R, Brivio LR. The treatment of
fractures with a dynamic axial fixator. J Bone joint Surg
(Br) 1984; 66-45.
18. Eggers G. W. N. Internal Contact Splint, Journal of Bone
and Joint Surgery 1948, 30-A : 40.
19. Grosse A, Kempf I Lafforgue D. Treatment of femoral
fractures with interlocking intramedullary nails. Rev. Clir
Orthop 1978, 64 (Suppl 2) : 33-5.
20. Gustilo R.B. Fractures of Tibua and Fibula. In -. Gustilo
RB, Kyle R.F, Tempeman D.C editors. Fracture and
Dislocation. St. Louis, Mosby, Year Book Inc, 1993 :
901-941 Open fractures p. 169-195
21. Haq. Z. Evaluation of Treatment of Open Tibial Shaft
Fracture by llizarov Technique. MS. thesis 1996;
University of Dhaka, Bangladesh.
22. Islam R. Result of Management of Open Tibial Shaft
Fracutres with External Skeletal Fixation in Adults. MS.
thesis 11989; University of Dhaka., Bangladesh.
23. Karlstrom G . and Olernd S. Percutaneous Piu Fixation of
Open Tibial Fractures J Bone Joint Surg. 1975, 57: 91 5-
923.
24. Heating J. F, O’Brien P. L,Blacuhut P . A , Meak R. N,
Brockhuyse H. M. Reamed interlocking intramedullary
nailing of open fracture of the tibia. Clin orthop 1997
May, 338: 182-91.
25. Klein M. P. M, Rahn B. A, Frigg R, Kessler S, Perren
S.M, Reaming versus non-reaming in medullary nailing :
Interference with cortical circulation of the canine tibia.
Arch Orthop Traumat. Surg 1990, 109: 314-316.
26. Krehek C, Gluer S, Schandelmaier P, Tscherne H,
Intramedullaty nailing of open fractures, orthopadics 1996,
25 (3).
27. Lottes J. O. Closed reduction, plate fixation and medullary
nailing of fracture of both bones of the leg. J Bone Joint
Surg (A) 1952, 34A:861 Medullary nailing of the tibia
with the triflange nail. Clin Orthop 1974, 105 : 253.
28. Holbrook J. L, swiontkowski M. F, Sander S. R. Treatment
of open fractures of the tibial shaft: Endcr nailing versus
external fixation. A randomized prospective comparison,
J Bone joint surg [Am|1989, 71 (A):1231-1238.
29. Thunold J, Varhaug Je, Bjerkeset T. Tibial shaft fractures
treated by rigid internal fixation: the early results in a 4-
year series. Injury 1975-76,:125-133.
180 Abdullah Al-Mahmood Bilal, Mir Hamidur Rahman, Mohammed Abdus Sobhan, Milon Krishna Sarker, Md.Wahidur Rahman et al
The Journal of Bangladesh Orthopaedic Society

Original Article
Watson Jones.Chamley (1961).Sarmiento (1967), and Nicoll (1974). The cast through dose not provide great
stability and there is a chance of shortening and malunion. Moreover incases of open fractures soft tissue care
is difficult.Application of a plate and screws provides right internal fixation and has shown comparatively less
incidence of non-union. But the high rate of infection has left much to be desired.
ABSTRACT
This prospective study of” Evaluation of outcome of open intramedullary interlocking nailing in tibial shaft
fracture in adults” carried out at CMCH between January 2007 to July 2008, involving 40 patients with
fractures of shaft of tibia. The aim of this study was to compare the outcome of treatment of closed tibial
fractures by interlocking nail. There were 23 patients with closed tibial shaft fractures and 17 patients
with open tibial shift fractures . 6 patients with closed fractures and 2 patients with open fractures were
lost at subsequent follow up so ultimately there were 32 cases ; 17 with closed fractures and 15 with open
fractures. In this study purposive sampling method was followed irrespective of sex .In open fracture
cases only types I, II and IIIA were selected .Two cases amongst the closed tibial fractures group had
associated ipsilateral femoral fractures and one had an ipsilateral fracture of the radius. Most common
age group in this series was 18-25 years (43.75%). The mean age of occurrence was 31.16 years for
closed fracture and 29.85 years for open fracture. Right side involvement was more (59.37%), while the
middle third of the shaft (59.4%) was the commonest site of fracture followed by the distal third (28.1%). In
cases with open fracture, the wound in 7 (46.66%)cases were closed by delayed primary suture, 5(33.3%)
healed up by granulation ,2 (13.3%) were managed by secondary suture and 1 (6.6%)case was managed by
slit thickness skin graft Mean time of union was 16.5 weeks incase of closed fracture and 26.5 weeks in
case of open fracture various complication were noticed such as, infection (12.54%),leg length discrepancy
(6.27%), knee pain (18.75%), knee and ankle stiffness. There were two cases of delayed union (table
XVIII).The final outcome of treatment was analyzed according to the criteria set by Tucker et al. 1992.
Acceptable results in close fracture were 82.3%while in case of open fracture79.9%were found acceptable
.17.6% of results were graded unsatisfactory in close fracture while 19.9% were unacceptable in open
fracture. So Intramedullary interlocking nailing is a modern, safe and appropriate technique regarding the
management of close and open tibial shaft fracture in adults.
Evaluation of Outcome of Open
Intramedullary Interlocking Nailing In
Tibial Shaft Fracture In Adults
Mohammed Abdus Sobhan1, Mir Hamidur Rahman2, Abdullah Al-Mahmood Bilal3, Milon Krishna
Sarker4, Md.Wahidur Rahman5 , M Monaim Hossen6
1. Senior Consultant, 250 bedded General Hospital Noakhali,
2. Assistant Professor, OSD, DGHS, attached Abdul Malek Ukil
Medical College, Noakhali
3. Assistant Professor (C,C) OSD, DGHS, attached Abdul Malek
Ukil Medical College, Noakhali
4. Assistant Professor, OSD, DGHS, attached Abdul Malek Ukil
Medical College, Noakhali
5. Associate Professor, NITOR, Dhaka
6. Associate Professor, NITOR, Dhaka
Correspondence: Dr. Mohammed Abdus Sobhan, Senior
Consultant, 250 bedded General Hospital Noakhali, Dhaka
INTRODUCTION
Fractures of the Shaft of tibia constitute the commonest
diaphyseal fractures amonogst all long bones. By this
very location , the tibia is exposed to frequent injury and
because 1/3rd of its surface is subcutaneous throughout
most of its length. Open fracture are more common in the
tibia than in any other bone.
Treatment of tibial fracture continues to pose a challenge
to orthopedic surgeons. Poor soft tissue coverage and
VOL. 29, NO. 2, JULY 2014 181

blood supply act as a deterrent to quick recovery.
Moreover, neuro-vascular injury, compartment syndrome
and infection (more so in open fractures) might add to the
burden. Later, delayed union nonunion and malunion may
complicate a tibial fracture.
The indication for operative and conservative treatment
of tibial shaft fracture has not been well defined. Early
workers advocated conservative management with close
reduction and piaster cast immobilization. Most prominent
amongst these were
Currently for open tibial fractures (Gustilo type II and
Gustilo type III) external fixator seen to be widely accepted.
It provides a right fixation with a relatively low rate of
deep infection, although the problems of pin tract infections
and malunions coupled with a low acceptability to patients,
remain. Over the last couple of decades intrameculiary
nailing of both closed and open fractures of tibial shaft
have come to gain acceptance and popularity.Herzog (1951)
was the first to modify the strainght Knail to accommodate
the eccentric proximal pole. Since then various authores
have reported their work on intramedullary nailing of tibial
fracture. Lottes (1974). Sedlin and Zitner, and d’ Aubigne
et al. (1974) reported encouraging results in the treatment
of both closed and open tibtal fractures.
The management of tibial fracture, both closed and open
by SIGN nailis still in its early stages in Bangladesh. The
study is based on the intrameduilary fixation of closed
and open tibial shaft fractures by IM interlocking nail
PATIENTS AND METHODS
Type of the study :
this was is prospective randomized analysis on the
outcome of intramedullary interlocking nailing in closed
and open tibial shaft fractures in adults.
Place of Study :
Orthopedic units of Chittagong Medical College Hospital
and deferent clicnics in Chittagnog Metropolitan Area,
Chittagong.
Study Duration:
January 2007 to July 2008 ( Year)
Study Population
All the patents above 18 years of age with closed and
open fracture ( upto Gustillo IIIB) of the Shaft of tibia
admitted in the different units of Chittagong Medical
College Hospital Chittagong and deferent clinics in
Chittagong Metropolitan Area, Chittagong.
Inclusion criteria :
· Age – above 18 years of age
· Sex _ patients were selected irrespective of sex
· Site _ diaphyseal (fractures of the tibia ) Shaft,4” below
the knee and 3” above the ankle joint
· Type of fractures
· Closed displaced fractures of the tibia Shaft either
fresh, or those in which initial conservation
management was unsatisfactory ( eg.-lost reduction in
a cast)
· Open fractures, Gustilo typel to type IIIB irrespective
of fracture configuration viz oblique, transverse, spiral,
segmentai and corn minuted. open fractures treated
within 7 days of injury and without any infection will
be included in this study.
· Associated injuries-
Other long bone injuries like fracture of femur, or of the
Humerus, radius and ulna.
Exclusion Criteria :
· Fractures in children
· Gustilo type IIIC
· Active or latent infection
Observation
During the period extending form January’ 07 to June 2008
a total of 32 patients wear studied. Seventeen patients
had close fractures and fifteen suffered open fractures of
tibia.
Occupation of the patients:
people from various walks of life were victims of tibial
fracture..
Age incidence :
in the study age range was form 18 to 55 yes. Maximum
incidence was found in 18 to 25 yrs age group.
Sex distribution:
In this series, 27 cases (84.37%) were, ales and 5 cases
(15.62%) were females.
Causes of injury:In this study motor vehicle accident (
MVA) accounted for 21 cases (65.62%) fall form height for
7 cases (21.8%) and 4 cases (21.5%) were due to assault.
Side involved:
In this study right side involvement was seen in 19 cases
( 59.37%) and left side in 13 cases (40.6%)
182 Mohammed Abdus Sobhan, Mir Hamidur Rahman, Abdullah Al-Mahmood Bilal, Milon Krishna Sarker, et al
The Journal of Bangladesh Orthopaedic Society

Both or single bone involvement:
Both bones were involved in 29 cases (90.6%) 3 cases
(9.3%) had only tibial fractures.
With associated other long bone fractures (other than
fibula):
2 cases (6.2%) had ipsilateral femoral fractures and one
case (6.26%) had a radial fracture.
All associated fractures occurred in cases with closed
tibial fractures only .
Level of fractures :
In this series there were 17 cases (53.1%) involving the
middle i/3. followed by 11 cases (33.3%) in the lower 1/3
and 4 cases (12.5%) in proximal 1/3 of the tibial shaft.
Pattern of fracture (fracture configuration):
In this series, fracture pattern was comminuted in 14 cases
(43.7%), oblique in 9 cases (28.1%), transverse in 7 cases
(21.8%) and segmental in 2 cases (6.25%)
Static or Dynamic nailing of tibial shaft fracture:
In the series 12 closed fracture cases and 12 open fracture
cases were managed by static nailing, 5 closed fracture
cases and 3 open fracture cases were managed by dynamic
locking.
Types of open fractures (Gustilo):
In this study the open fracture types were as follow: 8
were type 1.5 were type II and 2 were type III A.
Soft tissue management (with reqard to wound closure)
in case of open fractures:
In this series, delayed primary suture was applied in 7
patients, in 5 patients wound was left to heal by secondary
intention, secondary sutures were applied in 2 cases and
in 1 case skin graft was applied.
Duration of hospital stay:
Maximum and minimum hospital stay in this series was 7
and 15 days respectively for closed fractures and 10 and
25 days respectively for open fractures.
Time taken for union:
In this series, the minimum time for union in closed fracture
was 14 weeks and maximum was 27 weeks with a mean of 16.5
weeks. In case of open fractures, the minimum time for union
17 weeks and maximum was 35 weeks with a mean of 26.
Time taken for union as per fracture site:
In this series, for the closed group fractures in the distal 1/3
of tibial shaft took the longest to union with a mean of 18.5
weeks while. for the proximal 1/3 fractures had a mean union
time of 15.5 weeks. In case of open fractures distal 1/3 fractures
had a mean union time 29.2 weeks while the proximal 1/3
fractures showed the earliest mean union rate of 20.5 weeks.
Fracture union as per fracture pattern (in weeks):
In this study. In the closed fracture group, comminuted
fracture took the longest to union with a mean of 17.7
weeks, while oblique fracture were the earliest to unite
with a mean of 15.6 weeks. In the open grope, comminuted
fractures had a mean union of 26.57 weeks while. oblique
fracture had a mean of 21.7 weeks
Incidence of complication:
In this series 2 cases had post-operative superficial in
both groups. There was knee stiffness in 3 cases in both
groups. Delayed union was seen in 1 case in each group.
Shortening was observed in 1 case in each group. Other
complication were knee and ankle pain.
Table XVIII. Showing incidence of complications.
Incidence of Infection in the post operative period and
the causative organism:
Post- operative wound infection showed staphylococcal
and pseudomonal infections
Evaluation of Outcome of Open Intramedullary Interlocking Nailing In Tibial Shaft Fracture In Adults 183
VOL. 29, NO. 2, JULY 2014
X-ray after 20 WeeksPost Operative X-ray Preoperative X-ray

RESULTS
Analysis of results of tibial fractures is difficult task.
Besides the fracture itself ,soft tissue healing and
adjacent joint movements, greatly affect the final
outcome.The number of different grading systems is a
proof of lack of one single universally accepted grading
criterion .On this back drop, this study has attempted to
draw a comparative analysis on the outcome of closed
and open tibial fractures when treated by IM interlocking
nail.All the 32 patients in the study were followed up for
at least 6 months and upto a maximum of 12 months. In
fact the most worrisome part of the evaluation was the
time constraint for this type of study.The final result of
the study was analyzed by observng the outcome of
treatment of 32patients,which were included in this study.
For evaluation of results, Tuckers criteria was considered
for both closed and open fractures. A single grading
system for both types of fractures was used to have
uniformity while comparing the outcome of treatment in
bothclosed and open fractures. Moreover this system
included infection as one of the parameters for
assessment of outcome. Excellent and good results were
accepted as satisfactory, while fair and poor results were
regarded as being unsatisfactory. In this series ,for closed
fractures there were satisfactory results in
14cases(82.35%)and unsatisfactory in 3cases (17.64%).
For open fractures there were 12 cases(80%) as
satisfactory and 3(20%)unsatisfactory. Analysis was
done by applying the Chi-square test to compare the
outcome of the results of closed and open groups. There
was no significant difference in the results between the
two groups.
Table XX a.
Results of closed fractures (n=17)
Grading of result No. of patients %
Excellent 8 47.05
Good 6 35.29
Fair 1 5.88
Poor 2 11.76
Satisfactory result (Excellent + Good )= 82.35% Unsatisfactory
result (Fair + Poor) = 17.64%.
Table XX b
For Results of open fractures (n=15)
Grading of result No. of patients %
Excellent 5 33.33
Good 7 46.66
Fair 2 13.33
Poor 1 6.66
Satisfactory result (Excellent + Good )= 80% Unsatisfactory
result (Fair + Poor) = 20%
DISCUSSION
The fractures of the tibial shaft constitute the commonest
diaphyseal fractures amongst all long bones. But in spite
of the vast experience gained over the last 50 years, the
treatment of tibial fractures still can’t be governed by a
given set of rules. A number of treatment methods have
been well documented. The advocates of plaster cast
application have been well (1958) , Nicoll (1964) and
Sarmiento (1967). The main drawback of plaster cast
treatment has been shortening and malunioin. It would
probably be better indicated in cases with stable fractures
with minimal soft tissue injury.Interest in internal fixation
has centered round the use of the AO dynamic
compression plate and this has been well documented
(Thunold et al; 1975). The relatively hih rate of infection
makes the use of a plate an unattractive treatment
option.External fixator provides a rigid fixation with a
relatively low rate of deep infection, but prolonged
application, unsightly appearance and inconvenience to
the patient has limited its use for the treatment of severe
compound fractures, although its use has been
documented in the management of closed and minor
compound fractures of shaft of the tibia (De Bastiani et al.
1984; Court-Brown and Hughes, 1985; Evans. 1988)
Intramedullary devices have been used to stabilize tibial
184 Mohammed Abdus Sobhan, Mir Hamidur Rahman, Abdullah Al-Mahmood Bilal, Milon Krishna Sarker, et al
The Journal of Bangladesh Orthopaedic Society
Final Outcome

fractures for many years. Kuntscher (1958) was the first to
document the treatment of tibial fractures with IM nailing.
Since then a lot of authors have come up with their
observations.Most used the Lottes nail. Aubigne et at.
(1988), Lottes (1974) and Velasco et al. (1997), showed
commendable results in treating tibial fractures with Lottes
nail. The major drawback of simple IM nailing has been
malunion, as demonstrated by Swansonetal.
(1990).Interlocking IM nailing solver the problem of
malunion because it provides the ability to control length,
angulation and rotation. IM nailing of closed tibial fractures
has been an accepted treatment modality for sometime
now. Its use in open tibial fractures has been a more recent
innovation.Ekeland et al. (1987), Court-Brown et al. (1990),
and more recently Keating et al. (1997), have documented
good results in the treatment of open tibial fractures with
interlocking nail. Grosse-Kempf interlocking tibial nail was
used by these workers.While reamed nailing has gained
acceptance in closed tibial fractures, its use in open
fractures is still not considered favourable, due to an
increased incidence of complications.At NITOR the
treatment of tibial fractures with IM interlocking nail has
gradually come to gain acceptance over the last couples
of years. Alam 2002, and Chowdhury 2002, both showed
acceptable results in their study of treating closed and
open tibial fractures respectively with SIGN nail.The
present study has been undertaken in CNCH, Chittagong
to do a comparative analysis on the outcome of treatment
of both closed and open fractures by IM interlocking nail.
In this study, most victims fell under the 18-25 years group
(41.17% for closed fractures and 46.66% for open
fractures), while the next common age group being 26-35
years group (35.29% and 33.33% respectively for closed
and open fractures). The mean age of incidence was 31.16
years for closed fractures and 29.85 for open fractures.
These figures compare favorably with those shown by
other workers. The high incidence of young adult age
group points to the higher rate of mobility as well as social
violence in this age group. Male population in this study
constituted 84.81% of cases, while the females made up
the remaining 15.62%. Bone and Johnson (1986), observed
a male predominance of 81.81%, while Court-Brown et al.
(1990), showed males to make up 81.30% of the cases in
his study. Males being the major working force of a society
and are thus more consistently exposed to the external
environment, which probably accounts for this
discrepancy.Motor vehicle accidents were found to be
the most common causative factor of the injury in this
study (75%).Bone and Johnson (1986),-90%, and Court-
Brown et al. (1991), - 66.6%, both observed motor vehicle
accidents as the major reason for tibial fractures . Gustilo
1993,described road traffic accident as the commonest
cause of open tibial fractures. In this study, motor vehicle
accidents made up a slight higher percentage of victims in
case of open fractures (86.66) as compared to close
fractures (64.70).Most Fractures occurred in the middle
third of the shaft of tibia (53.12), f0llowed by distal third
(34.37) in this series. the incidence of facture level was
more or less similar in both closed and open fractures. this
is consistent with the observations of Bone and Johnson
(1946), Smet et al. (2000), and choudhury (2002).court –
Brown et al. (1990). found a greater incidence of fracture at
the distal third (51%). At its middle third the tibia is slender,
with a subcutaneous anterior-medial surface and lacks
muscle coverage, with a subcutaneous anterior-medial
surface and lacks muscle coverage. which exposes it to
injury. in this series most factures were comminuted (44%).
High velocity trauma results in comminution of bone
(Apley and Solomon 1993). In the study of Blachut et al.
(1997, 71% of fractures were comminuted.The tiba of the
right side fractured in 19 (59.37%)was injured in 13 (40.62)
cases. Both tibia and fibula were fractured in 29 (90.62)
cases of while the tibia alone was fractured in only 3 (9.37%)
cases. in two cases of closed tibial fractures, an ipsilateral
femoral fracture (closed) which was managed by
conservatively.
CONCLUSION
As can be seen from the study, interlocking IM nailing of
tibial fractures is a safe technique with a commendable
performance regarding soft tissue management as well as
fracture healing.After comparing the results of closed and
open tibial shaft fractures when treated with intramedullary
interlocking nail, it can be recommended to be used safely
for both closed and open (type l, ll and lllA) fractures.
REFERENCES
1. Gustilo R. B, Mendoa R. M and Williams D. N Problems
in the management of type 111 (severe) open fractures : A
new classification of type 111 open fractures. J Trauma
1984,24:742-746.
2. Ellis H. The speed of healing after fracture of the tibial
shaft.J Bone Joint Sueg (Br) 1958, 40-B : 42-6
3. Nicoll E. A. Fracture of the tibial shaft a survey of 705
cases. J Bone Joint Surg (Br) 1964,46-8:373-87.
4. Sarmiento A. A functional below-the –knee brace for tibial
fractures Bone Joint Surg (Am)\97Q; 52A: 295-311.
5. Court-Brown C. M, Christie J, Mcqueen M. M. Closed
intramedullary tibial nailing, J Bone Joint Surg (Br) 1990;
72^B: 605-11.
Evaluation of Outcome of Open Intramedullary Interlocking Nailing In Tibial Shaft Fracture In Adults 185
VOL. 29, NO. 2, JULY 2014

6. Allen. w, Piotrowsky G, Burnstein A, Frankel V.
Biomechanical principles of intramedullary fixation. Clin
Orthop. 1968; 60:13-20.
7. Brown P. W, Urban J. G, Early weight-bearing treatmrnt
of open fractures of the tibia : An end-result study of
sixty-three cases. J Bone Joint Surg. 1969, 51A, 59-75.
8. Wenger H. l. Shaft Fracture Immobilizstion with plaster,
American Journal of Surgery 1944, 66, 382.
9. Edwards C. C, Simmon S. C, Browner J. d, Weigel M. C.
Severe Open Tibial Fractures; Result Treating 202 Injuries
withy External Fixation. Clin. Orthop 1988, 230: 98.
10. Lottes J. O. Closed reduction, plate fixation and medullary
nailing of fracture of both bones of the leg. J Bone Joint
Surg (A) 1952, 34A:861 Medullary nailing of the tibia
with the triflange nail. Clin Orthop 1974, 105 : 253.
11 Holbrook J. L, swiontkowski M. F, Sander S. R. Treatment
of open fractures of the tibial shaft: Endcr nailing versus
external fixation. A randomized prospective comparison,
J Bone joint surg [Am|1989, 71 (A):1231-1238.
12. Thunold J, Varhaug Je, Bjerkeset T. Tibial shaft fractures
treated by rigid internal fixation: the early results in a 4-
year series. Injury 1975-76,:125-133.
13. Christensen J, Greiff J, Rosendahl S. Fractures of the
shaft of the tibia treated with AO-compression
osteosynthesis./n/ury 1982 ; 13:307-14.
14. Allo A, Molster A, Thoresen BO, Gjerdej NR, Ekeland
A, Polleras G, etal. Effect of rotational stability of
intramedullary nailing on bone healing. Acta Orthop Scand
1991;62:573-6.
15. Hindley C. J. Closed medullaery nailing for recent fractures
of the tibia. Injury 1988,19:180-4
16. Appley A. G. and Solomon L. Apleys System of
Orthopaedics and Fractures 7th ed. Butterworth-
Heinemann Ltd. Oxford. 1993,P:532-533,544,689-693.
17. Helfet D. L, Dipasquale T. G, Howey T.D, Sander R,Zinar
D, PopmanD. The treatment of open and or unstable tibial
fractures with an unreamed double locked tibial nail. In :
Proceedings of the American Association of Orthopaedic
Surgeons Conference, New orleans, Feb 1990.
18. Bach A. W, Hansen S.T. Plates versus external fixation in
severe open tibial fractures: A randomized trial, Clin.
Orthop. 1989,241:89-94.
19. Bonatus T, Olsan S. A, Lee S, Chapman M. W. Nonreamed
Locking intramedllary nailing for open fracturesn of the
tibia, Clin orthop 1997, juni; (339):58-64.
186 Mohammed Abdus Sobhan, Mir Hamidur Rahman, Abdullah Al-Mahmood Bilal, Milon Krishna Sarker, et al
The Journal of Bangladesh Orthopaedic Society

Review Article
Upper Cervical Spinal Injuries : A
Review
Ghosh JC1, Mollah Ershadul Haq2, Dulal Datta3, Monaim Hossen4, Noor Mhammad5, Lokman Hossain6
Abstract:
This study was done to review the management of upper cervical spinal injuries, so that the recent management
trends along with pitfall in management can be utilized for better patient management. Methods: This is a review
study done by searching the literature through pubmed using the key words; injury , upper cervical spine and
management. Correct diagnosis and classification of a lesion is the first step for determining the most appropriate
form of treatment. The emergent evaluation of patient who are at risk of cervical spinal injury relies on standardized
clinical and radiographic protocol to identify and classify injury and predict instability. Upper cervical spinal
injuries are frequently missed and the most common reason is in inadequate radiological examination.
Ligamentous injuries usually require surgical intervention although bony injuries can mostly be managed
conservatively. The indication for operative treatment or significant injuries to cervical spine is basically determined
by instability and dislocation and urgency of operative treatment in based on neurological status. Upper cervical
spinal injuries are commonly associated with trauma and which require significant force to produce. Significant
upper cervical spinal injuries are potentially life threatening injuries that may cause immediate death as a
consequences of complete respiratory arrest due to brain stem compression.
Key word: Upper cervical, Spinal injury, Management.
1. Associate professor (ortho -surgery), Gopalgonj Medical College, Gopalgonj
2. Assistant Professor of Orthopaedic Surgery, Shiheed Suhrawardy Medical College Hospital, Dhaka
3. Assistant Professor of Orthopaedic Surgery, NITOR, Dhaka
4. Associate Professor of Orthopaedic Surgery, NITOR, Dhaka
5. Associate Professor, BIHS General Hospital, Mirpur, Dhaka
6. Assistant Professor, Department of Orthopaedics, NITOR, Dhaka
Correspondence: Dr. Jagodish Chandra Ghosh, Associate Professor (ortho -surgery), Gopalgonj Medical College, Gopalgonj, Email:
INTRODUCTION
Cervical spine trauma is a common problem with wide range
of severity from minor ligamentous injury to frank osteo-
ligamentous instability with spinal cord injury.12
Approximately 5-10% of patient who are unconscious and
present on emergency basis as a result of motor vehicle
accident or fall have major injury to the cervical spine. The
cervical spine is conventionally divided into upper and lower
cervical spine . The upper cervical spine extend from occipital
to 2nd cervical vertebrae and lower cervical spine from C3-C7
vertebrae. The anatomy of upper cervical spine is unique in
its structural design This distinctive anatomy the upper
cervical spine leads injuries to occur in a predictable pattern.4
Most of the upper cervical spinal injuries are due to high
energy trauma and among all the cervical spinal injuries about
one third occurs at the level C2. Common injuries of upper
cervical spine include occipital condylar fracture, atlanto
occipital dislocation fracture of the ring of C1, ligamentous
injuries, odontoid fracture and C2 body fracture.4 The
integrity of upper cervical spine is essential for survival and
function because of the neurovascular structure contained
within its bony elements.1 The skull base with its bony and
ligamentous elements surrounding the foramina magnumplays an integral part in maintenance of normal functionalalignment of these two cervical vertebrae. Bony injuries canbe treated either by conservative or surgical interventiondepending on the fracture stability but significantligamentous injury needs surgery. Atlanta-occipitaldislocation is uncommon injuries and usually fatal injuriesbut there are reports of survival of such patient with urgentand appropriate management.
RESULTSDislocation of atlanta-occipital joint:Atlanta-occipital dislocation are uncommon injury. Thisinjury is rarely seen even in a level1 trauma centre and it isassociated with high morbidity and mortality. It may beeither anterior or posterior but usually fatal. Bone fracturemay accompany atlatooccipital dislocation . Althoughmost of the patient die immediately of complete respiratoryarrest caused by brainstem compression but, there arereports in the literatures in of patient who survived thisinjury..6 Survival in atlantooccipital dislocation is possible
in patient with minimum neurological deficit and if
VOL. 29, NO. 2, JULY 2014 187

diagnosed quickly and treated appropriately. Treatment
of this injury consist of reduction of dislocation and
stabilization of the atlanto occipital joint. Rapid diagnosis
by CT scan is so called gold standard and treatment
initiation using occipitocervical stabilization if possible or
temporary application of a halo fixator is crucial because it
is possible for adults to survive this injury.7Cervical
traction is contraindicated because instability. Immediate
application of a halo vestis recommended to stabilize the
joint. Patient’s respiratory and neurological status must
be carefully monitored. Occipital condylar fracture:
Occipital condylar fractures are rare.19 This injury
infrequently missed on initial evaluation. The first
description of occipital condylar fracture inliterature was
provided by Bell in 1817.18 These injuries usually results
from axial loading andlateral bending during which force
is applied to the head and neck .Stable occipital
condylerfracture can be treated in a rigid cervical orthoses
or halo vest. Potentially unstableinjury needs
immobilization in a halo vest for 12 weeks. After an
adequate period of immobilization in a halo vest if
instability is indicated by flexion and extension imaging
film then occipital C2 fusion may be necessary. If atlanto-
occipital dislocation has been diagnosed in addition to
fracture then it require surgical stabilization independent
of occipital condylar fracture andit is a significant predictor
for outcome. 24 Atlas fracture: Atlas fracture represent 2%
of all vertebral spine fracture and occur when an axial
compression of the skull on the atlas forces it into the axis
resulting in a fracture at the weakest point. Most fracture
in the atlas can be treated with immobilization in a rigid
cervical orthosis or in halo vest. Isolated posterior arch
fracture are stable injuries that can be treated in a cervical
collar for 8-12 weeks. Levine and Edward found that53%
of patient with atlas fracture had additional cervical spinal
injuries in their series. Non displaced or minimally displaced
fracture of the lateral mass and Jefferson fracture can be
treated by collar immobilization to prevent displacement
and allow fracture healing. Fracture in which the lateral
mass of atlas is displaced laterally more than 7mm beyond
the articular surface of the axis should be reduced with
halo traction .Halo traction should be maintained for 3-
6weeks before application of a halo vest if the lateral mass
is severely displaced, since displacement may recur if a
halo vest is applied immediately after reduction. Rupture
of transverse ligament: This is a purely Ligament us injury
and different from other injuries involving C1-C2 complex.
It is most commonly results from a fall with blow to the
back of the head. The transverse ligament may be avulsed
with a bony fragement from the lateral mass on either side
or it may rupture in its midsubstances. Because rupture of
the transverse ligament is primarily a ligamentous injury ,
nonoperative treatment is ineffective in obtaining stability.
Surgical stabilization of the C1 complex is the treatment of
choice. Axis fracture: The mechanism of axis fracture is
hyperextension injury. Among the axis fracture odontoid
fracture most often result from trauma.tic flexion In young
patient these injury require a good deal of forces such as
motorvehicle collision, skiing or fall from a height.
Immediate death from medullary injury may occur. Fracture
through the base of the dens neck are the most common
type of dens injury and are usually unstable injury. ,fracture
displaced beyond 6mm in old or that are unstable even in
halo vest require surgery. Fracture through the body of
the axis may be displaced or undisplaced. Undisplaced
fracture are stable injuries that heal with 8-12 weeks of
immobilization in either a halo vest or cervical collar.
Displaced fracture may have multiple combination of
angulations and translation although most of these fracture
could be reduced with halo traction, continuous traction
with extension is required to maintain reduction. Traumatic
spondylolisthesis of axis (Hangman fracture) : Hangman
fracture was originally described as those neck injuries
that incurred during hanging of criminals. Their most
common cause now a days are motor vehicle accident
with hyperextension of the head on neck. The occiput is
forced down against the posterior arch of the atlas which
in turn is forced against the pedicle of C2. Minimally
displaced and stable Hangman fracture usually heal within
12 weeks of immobilization in a rigid cervical orthosis.
Hangman fracture with more than 3mm of anterior
translation and significant angulations require application
of skull traction through tong or halo ring with extension
of the neck over a rolled up towel. Immobilization in a halo
vest does not achieve or maintain reduction and halo
traction with slight extension may be necessary for 3-6
weeks to maintain anatomical reduction , then the patient
can be mobilized into a halo vest for the rest of the 3
months period. In more severe form of this fracture there
may be a combination of bipedicular fracture with posterior
facet injuries.This injuries are the only type of Hangman
fracture that require surgical stabilization .Open reduction
and internal fixation are generally required and treated
appropriately. Treatment of this injury consist of reduction
of dislocation and stabilization of the atlanto occipital joint.
Rapid diagnosis by CT scan is so called gold standard
and treatment initiation using occipitocervical stabilization
if possible or temporary application of a halo fixator is
crucial because it is possible for adults to survive this
injury.7Cervical traction is contraindicated because
188 Ghosh JC, Mollah Ershadul Haq, Dulal Datta, Monaim Hossen, Noor Mhammad, Lokman Hossain
The Journal of Bangladesh Orthopaedic Society

instability. Immediate application of a halo vestis
recommended to stabilize the joint. Patient’s respiratory
and neurological status must be carefully monitored.
Occipital condylar fracture: Occipital condylar fractures
are rare.19 This injury infrequently missed on initial
evaluation. The first description of occipital condylar
fracture inliterature was provided by Bell in 1817.18 These
injuries usually results from axial loading andlateral
bending during which force is applied to the head and
neck .Stable occipital condylerfracture can be treated in a
rigid cervical orthoses or halo vest. Potentially
unstableinjury needs immobilization in a halo vest for 12
weeks. After an adequate period of immobilization in a
halo vest if instability is indicated by flexion and extension
imaging film then occipital C2 fusion may be necessary. If
atlanto-occipital dislocation has been diagnosed in
addition to fracture then it require surgical stabilization
independent of occipital condylar fracture andit is a
significant predictor for outcome.24 Atlas fracture: Atlas
fracture represent 2% of all vertebral spine fracture and
occur when an axial compression of the skull on the atlas
forces it into the axis resulting in a fracture at the weakest
point. Most fracture in the atlas can be treated with
immobilization in a rigid cervical orthosis or in halo vest.
Isolated posterior arch fracture are stable injuries that can
be treated in a cervical collar for 8-12 weeks. Levine and
Edward found that53% of patient with atlas fracture had
additional cervical spinal injuries in their series. Non
displaced or minimally displaced fracture of the lateral mass
and Jefferson fracture can be treated by collar
immobilization to prevent displacement and allow fracture
healing. Fracture in which the lateral mass of atlas is
displaced laterally more than 7mm beyond the articular
surface of the axis should be reduced with halo traction
.Halo traction should be maintained for 3-6weeks before
application of a halo vest if the lateral mass is severely
displaced, since displacement may recur if a halo vest is
applied immediately after reduction. Rupture of transverse
ligament: This is a purely Ligament us injury and different
from other injuries involving C1-C2 complex. It is most
commonly results from a fall with blow to the back of the
head. The transverse ligament may be avulsed with a bony
fragement from the lateral mass on either side or it may
rupture in its midsubstances. Because rupture of the
transverse ligament is primarily a ligamentous injury ,
nonoperative treatment is ineffective in obtaining stability.
Surgical stabilization of the C1 complex is the treatment of
choice. Axis fracture: The mechanism of axis fracture is
hyperextension injury. Among the axis fracture odontoid
fracture most often result from trauma.tic flexion In young
patient these injury require a good deal of forces such as
motorvehicle collision, skiing or fall from a height.
Immediate death from medullary injury may occur. Fracture
through the base of the dens neck are the most common
type of dens injury and are usually unstable injury. ,fracture
displaced beyond 6mm in old or that are unstable even in
halo vest require surgery. Fracture through the body of
the axis may be displaced or undisplaced. Undisplaced
fracture are stable injuries that heal with 8-12 weeks of
immobilization in either a halo vest or cervical collar.
Displaced fracture may have multiple combination of
angulations and translation although most of these fracture
could be reduced with halo traction, continuous traction
with extension is required to maintain reduction. Traumatic
spondylolisthesis of axis (Hangman fracture) : Hangman
fracture was originally described as those neck injuries
that incurred during hanging of criminals. Their most
common cause now a days are motor vehicle accident
with hyperextension of the head on neck. The occiput is
forced down against the posterior arch of the atlas which
in turn is forced against the pedicle of C2. Minimally
displaced and stable Hangman fracture usually heal within
12 weeks of immobilization in a rigid cervical orthosis.
Hangman fracture with more than 3mm of anterior
translation and significant angulations require application
of skull traction through tong or halo ring with extension
of the neck over a rolled up towel. Immobilization in a halo
vest does not achieve or maintain reduction and halo
traction with slight extension may be necessary for 3-6
weeks to maintain anatomical reduction , then the patient
can be mobilized into a halo vest for the rest of the 3
months period. In more severe form of this fracture there
may be a combination of bipedicular fracture with posterior
facet injuries.This injuries are the only type of Hangman
fracture that require surgical stabilization .Open reduction
and internal fixation are generally required .
DISCUSSION
Upper cervical spinal injuries are potentially life threatening
injuries and most of them are associated with high energy
trauma.4 In older patient stiffness of the lower cervical
spine caused by degenerative changes and osteopenia
might contribute to upper cervical spinal injury in response
to low energy trauma.20 Achieving the correct diagnosis
and classification of a lesion is the first step towards
identifying the most appropriate form of treatment.19 ,23
Current protocol for evaluation of suspected cervical spinal
injury include combine information from history, clinical
examination and imaging evaluation to predictthe
instability ,identify neurological deficit and the need for
Upper Cervical Spinal Injuries : A Review 189
VOL. 29, NO. 2, JULY 2014

surgical intervention.12 The immediate clinical examination
of the spine should include inspection and palpation of
the spine as well as the complete neurological examination
.In addition cranial nerve examination should always be
performed. Nerve palsies related to cranial
nerves6,7,9,10,11,12 can occur in association with upper
cervical spinal injuries.13,14 There is a significant chance
of missing upper cervical spinal injury during evaluation
of the patient.23 The reported frequency of missed injury
in the cervical spine varies from 4%-30%.12 The most
common reason cited for missed injuries is an inadequate
radiological examination. 10,11,12 The complex regional
anatomy and overlying structure make plain radiological
images difficult to interpret these injuries adequqtely.21
CT and MRI are required in the course of diagnosis for the
traumatic injury of the upper cervical spine Management
of patient with cervical spine injuries is urgent as there
might be immediate death from some upper cervical spinal
injury , so early recognition and prompt treatment can
reduce the mortality and morbidity. The treatment option
may be either conservative or surgical depending on
fracture stability, status of the relevant ligamentous
structure , fracture pattern and alignment .3 Bony injuries
including occipital condylar fracture, atlas fracture ,most
odontoid fracture and traumatic spondylolisthesis of the
axis generally respond well to nonsurgical treatment .19
The indication for operative treatment of significant
injuries to cervical spine is basically determined by
instability and dislocation. Urgency of operation is based
on neurological status, if there is chance of recovery
operative treatment is urgent.4,5
REFERENCES
1. Jackson RS, Banit DM, Rhyne AL, 3rd,Darden
BV2nd.Upper cervical, spine injuries.J Am Acad Orthop
Surg , 2002 Jul-Aug; 10(4): 271-80
2. Seljeskok EL,Chou SN. Spectrum of the hangman’s fracture.
J Neurosurg 1976Jul; 45(1):3-8
3. Joaquim AF ,Ghizoni E, Tedeschi H, Lawrence B, Brooke
DS, Vaccaro AR,Patel AA.Upper cervical injuries A
rational approach to guide surgical management. J spinal
cord 2014Mar; 37(2):139-51
4. Syre P, Petrov. Management of upper cervical spinal
injuries: a review. J Neurosurg sci 2013 Sep; 57:219-40
5. Buhren V, Hofmeister M, Potulskim. Indication for
surgical management of injuries of the cervical spine.
Zentralbl chir 1998; 123(80: 907-13
6. Chatter-cora D,Valenziano CP.Atlanto- occipital
dislocation :A report of three patients and a review. J
orthop Trauma 2000 June-July; 14(5): 370-5
7. Muller FJ, Kinnel B, Neumann C,Nerlich M, Fuechtmeier
B. Incidence and outcome of atlanto-occipital dissociation
at a level1 trauma centre: a prospective study of five cases
within 5 years. Euro Spine J. Jan 2013;22(1):65-71.
Published online Oct 18,2012. doc 101007/s00586- 012-
2543-1.
8. Jefferson G. Fracture of the atlas vertebrae. Report of
four cases and review of those previously recorded.
British Journal of Surgery.1919;7(27):407-22. Avilable
from http/onlinelibrary.wiley.com/doi/101002/bjs.
1800072713/abstract. Accessedin 2012(Oct 30)
9. LiLB,Shen YX, Fan ZH, Shanq P,Wang LL.Surgical
management of traumatic injury of upper cervical spine.
Zhonqqoo Gu Shang.2009 May;22(5):387-8.
10. Bohlmann HH. Acute fracture and dislocation of the
cervical spine: An nalysis of three hundred patient and
review of literature. J Bone Joint Surg Am. 1979;61:1119-
42.
11. Gerrelts BD, Petersen EU, Mabry J, Petersen SR. Delayed
diagnosis of cervical spinal injuries. J
Trauma.1991;31:1622-6.
12. Joel A, Torretti and Dilip sengupta. Cervical spine trauma.
Indian J Orthop. 2007 Oct- Dec;41(4):255-267. doc
104103/0019-36985
13. Arias MJ. Bilateral traumatic abducens nerve palsy with
skull fracture and w ith cervical spine fracture: case report
and review of literature. Neurosurgery. 1985;16:232-4.
14. Mc Cleary AJ. A fracture of the odontoid process
complicated by tenth and twelveth cranial nerve palsies:
A case report. Spine 1993;18:932-5.
15. Strohm PC1 ,Muller ChA, Kostler W, Reising K, Sudkamp
NP. Halo- fixator vest: indication and complications.
Zentralbl Chir .2007 Feb;132(1):54-9.
16. Basu S, Chatterjee S, Bhattacharaya MK, Seal K. Injuries
of the upper cervical spine:A series of 28 cases. Indian J
Orthop. 2007 Oct; 41(4): 305-11. doc 10.4103/0019-
5413.36992
17. Danerymez M, Kahraman S, Gezen F, Sirin S. Cervical
spine injuries and Management experiences with 235
patients in 10 years. Minim invasive Neurosurg. 1999
Mar; 42(1):6-9.
18. Bell C. Surgical observations. Middlesex Hospital Journal.
1817;4:469-70.
19. Kandziora F1, Schnake K, Hoffmann R. Injuries to cervical
spine . Part2:Osseous injuries. Unfallchir surg. 2010 Dec;
113(12):1023-39;quiz 1040. doc 10.1007/s00113-010-
1896-3
190 Ghosh JC, Mollah Ershadul Haq, Dulal Datta, Monaim Hossen, Noor Mhammad, Lokman Hossain
The Journal of Bangladesh Orthopaedic Society
20. Watanabe M1 ,Sakai D, Yamamto Y, Sato M, Mochida J.
Upper cervical spine injuries: age specific clinical feature.
J rthop Sci.2010 Jul;15(4):485-92. doc 10.1007/s00776-
010-1493-x Epub 2010 Aug 19
21. Kontautas E1 , Ambroozaitis KV, Spakauskas B,
SmailysA. Upper cervical spinal injuries and their
diagnostic features. Medicina(Kaunas) 2005; 41: 802-9.
22. Daentzer D1 ,Flokemeier T . Conservative treatment of
upper cervical spinal injuries with halo vest:an appropriate
option for all patient for all patient independent of their
age. J Neurosurg Spine. 2009 Jun;10(6):443-50. doc
10.317/2009.2 SPINE 08484
23. Macron RM1, Cristante AF, Teixeira WJ, Narasaki
DK,Oliveira RP, de Barros Filho TE. Fractures of cervical
spine. Clinics. 2013 Nov; 68(11): 455-61. doc 10.6061/
clinics/ 2013(11) 12.
24. Muller FJ, Fuechtmeier B, Rosskopf M, Neumann C,
Nerlich M, Englert C. Occipital condyle fracture:
prospective follow up of 31 cases within 5 years at a
level 1 trauma centre. Euro Spine J.2012 Feb; 21(2): 289-
9. doc 10.1007/s 00586-011963-7. Epub 2011
Aug 11.
25. Greene KA,Dickman CA, Mariaano , FF,Drabier JB,
Hadley MN, Sonntag VK. Acute axis fracture: analysis of
management and outcome in 340 consecutive cases. Spine.
1997 Aug15; 22(16): 1843-52.
Upper Cervical Spinal Injuries : A Review 191
VOL. 29, NO. 2, JULY 2014

Case Report
Health Seeking Behaviour of Road
Traffic Accident Victims: A Qualitative
Study among the Slum Dwelling
Disabled People of Dhaka City
Mohammad Mahbub Alam Talukder1, Md. Ali Imam2, Nasrin Akter3, Nasir Uddin Sheikh4
ABSTRACT
Road traffic accident is a global problem which is severe in the developing countries like Bangladesh. In
consequence, in developing countries road trauma has now been recognized as an increasing public health
hazards and economic burning issue. And after road traffic accidents the lack of management and economic
costs related with health seeking behabiour have a disproportionate impact on lower income groups, thus
contributing to the persistence of poverty in conjunction with disability. This cross sectional study, carried out
during July 2012 to June 2013, aimed to explore health seeking decision and culture of handling the road traffic
accident related victims, as taken from experiences of the poor disabled people of slum dwellers of Dhaka city.
The present study has been designed based on qualitative techniques such as in-depth interview and case
studies. Additionally, a survey questionnaire was used to collect the demographic characteristics of the study
population (n=150) and to select participants purposively for in-depth interview (n=50) and case study (n=30).
Content analysis of qualitative data was done through theme coding and matrix analysis of case study was done
to use relevant verbatim. Most of the time the health seeking decision totally depended on the surrounded people
of the accidental place, their knowledge, awareness and remaining facility and capacity regarding proper
management of the victims. However, most of the cases the victims did not get any early treatment and it took 2-
12 hours to get even the first aid because of distance, shortage of money, lack of availability of getting the aid, lack
of mass awareness etc. Under the reality of discriminated and unaffordable health service provision better
treatment couldn’t turn out due to economic inability of the poor victims. To avoid the severe trauma, treatment
delay must be reduced by providing first aid within very short time and to do so mass awareness campaign is
necessary for handing the victims. Moreover, necessary measures should be taken to ensure cost free health
service provision to treat the chronic disabled condition of the road traffic accident related poor victims.
Key words: Accident, Injury, Disabled, Qualitative, Slum.
INTRODUCTION
Road traffic accident is a ‘global tragedy’ with ever-rising
trend and represents a major cause of premature deaths
and disabilities worldwide. Each year, 1.3 million people
are killed and 50 millions are injured by road accidents all
over the world. (iRAP, 2008a). Road trauma has now been
recognized as one of the significant diseases of industrial
societies and is an increasing public health hazards and
economic burning issue in developing countries.
Accidents are particularly prevalent in low and middle
income countries- around 88 percent of the world’s deaths
occur in developing countries (Mackay, 2003). According
to a study, the numbers of fatalities have been increasing
from 1009 in 1982 to 2082 in 2011 in Bangladesh (ARI
Database, 2012). It is estimated that by 2020 about two-
thirds of the world’s traffic fatalities might be in the Asian-
Pacific region. The economic costs of road crashes, which
range from 1 percent to 3 percent of GDP in Asia, have a
disproportionate impact on lower income groups, thus
contributing to the persistence of poverty. Also it has
been observed from the studies that up to 62 percent of
urban road accident deaths are pedestrians alone and in
1. Professor of Accident & Research Institute, BUET, Dhaka
2. Research Investigator, ICDDR,B, Dhaka
3. Operation Research Manager, Consult AID, Bangladesh\
4. Research Manager, Consult AID, Bangladesh
Correspondence: Dr. Mohammad Mahbub Alam Talukder, Professor of Accident & Research Institute, BUET, Dhaka
192 The Journal of Bangladesh Orthopaedic Society

Dhaka city, they represented nearly 70 percent. Almost 80
percent of fatalities are vulnerable road users e.g.
pedestrians, bicyclists and motorcyclists (Hoque, 2006).
According to the World Health Organization report on
road traffic injury prevention (WHO, 2004), for every death,
there are far greater numbers of injuries- 04 persons with
severe/permanent disabilities, 10 persons requiring
hospital admission, and 30 persons were requiring
emergency room treatment. These facts demanded that
there is indeed an urgent need to develop an appropriate
and co-operative health system response to this man-made
epidemic by implementing strategic programs that will
effectively address such a major growing issue of road
traffic accidents and injuries.
In these circumstances this study aims to explore the
healthcare seeking decision and culture of handling the
road traffic accident related victims in the light of their
existing experiences. The study also tried to assess socio-
economic and demographic characteristics of the victims
who are the slum dwellers of Dhaka city. Simultaneously,
an attempt was made to explore the knowledge, beliefs,
norms, attitudes, behavior and practices related to health
seeking decision of the victims.
METHODS
This is a cross sectional descriptive study among poor
slum dwelling disable peoples of Dhaka city that had been
conducted during July 2012 to June 2013. The present
study was designed based on qualitative methods and to
do so qualitative techniques such as in-depth interviews
and case studies were used. Additionally, a survey
questionnaire was used to collect the socio-economic
background and demographic characteristics of the study
population. The study area included three differently
located slums of Dhaka city (Duaripara, Vasan tek and
Korail slums). The study populations were the poor
disabled persons and the victims of traffic related accidents
and their household members living with him/her in the
selected slum locations.
Participants were selected purposively to ensure both male
and female and to ensure category of the research
participants (road traffic accident victims). For interview
we also sought to enroll 150 road traffic accident victims’
those were generally disabled and aged between 21-60
years. It was a small survey of traffic accident related 150
disabled in slum community of Dhaka city and survey
interview was used for collecting the socio-economic
background and demographic characteristics of the study
population as well as to identify more vulnerable
participants for in depth interview. Based on survey
interview more disabled were invited to attend one to one
in depth interview and 50 qualitative interviews were
conducted by skilled research assistant and sequentially
identified 30 most disable victims for case study. Selection
was again purposive and was designed to reflect the views
of traffic accident related disabled of both the sexes and
their willingness to talk openly to the research team.
Diagram 1: Sampling, Sample size and Research tools
Mohammad Mahbub Alam Talukder, Md. Ali Imam, Nasrin Akter, Nasir Uddin Sheikh 193
VOL. 29, NO. 2, JULY 2014

Before interviewing with the informants the researchers
built rapport and described the objectives of the study.
The investigator sought the verbal consent from the
individuals to provide their personal information and their
related practices in the relevant study field and ensured
the confidential issues of their information that used only
for this research purpose.
Analysis of data was begun with the first field activities
and led to refinements as the study proceeded. The field
notes were regularly reviewed with the field team (initially
daily). The field team met the Principal Investigator (PI)
every other day to discuss the results of their activity
sessions/interviews and to determine the best practices
for further activity sessions/ interviews and note-taking.
From the beginning, thematic analysis took place to
understand the health seeking decision and culture of
handling road traffic accident related victims. The process
followed a sequence of interrelated steps recommended
by Ulin et al. that include reading, coding, displaying,
reducing, and interpreting. (Ulin 2002). Thus, data were
organized according to a sequence. After that, qualitative
findings were presented and discussed compared with
existing relevant studies and literature on this topic.
Moreover, the personal narratives presented in this report
are literal translations of the same language that was
delivered at the time of the interview. To present the
complex view of most disable victims verbatim from case
studies were used that were directly translated from the
transcripts. The triangulation of methods and comparison
of various accounts by different FROs were employed to
improve the quality of research results, which is also
recommended by Denzin (Denzin 1989). Cross tabs were
made to present the demographic characteristics of the
informants.
RESULTS AND DISCUSSION
The presentation of the findings is organized in three
different sections. The first section report from the finding
of survey interview and illustrates the major information
of the disabled person’s demographic characteristics. The
second section reports from the findings of the case
studies conducted among poor road traffic accident related
victims of slum of Dhaka city. This section focuses on
describing the (i) factors associated with health care
seeking behaviour. The second section reports from the
findings of in-depth interviews and focuses on explaining
(ii) first aid and culture of handling road traffic accident.
Verbatim quotations are used to illustrate findings in the
both sections. Speech reported in the article was translated
into English by the both first and second authors.
DEMOGRAPHIC CHARACTERISTICS:
There was preponderance of male (97 %%) and female
(3%) children with an age range from 21-60 years and
among them 50%% were 31-40 years aged. Of the 150
participants of both categories who participated in survey
interview, 38 (25%) never went to school and 56 (71%)
only got primary education. 33% of the victims reported
that in consequence of road accident they bound to take
begging as their main occupation 31% of them were
involved in small business to survive. All female victims
who participated in the research were housewife. A
significant number of families 80 (53%) had taka 2001-4000
per month income.
Table-I
Socio-demographic Characteristics of the informants
Characteristics Frequency (n) Percentage
(N=150) (%)
Sex
Male 145 97
Female 05 03
Age (years)
21-30 09 06
31-40 75 50
41-50 46 31
51-60 20 13
Education
Illiterate 38 25
primary 76 51
Secondary 30 20
SSC 03 02
HSC 02 01
BA 01 0.67
Occupation
Small Business 47 31
House wife 03 02
Beggar 50 33
Farmer 05 03
Government Service 04 03
Private Service 20 13
Unemployment 21 14
Income (monthly)
Up to 2000 24 16
2001-4000 80 53
4001-6000 25 17
6001-8000 15 10
194 Health Seeking Behaviour of Road Traffic Accident Victims: A Qualitative Study among the Slum Dwelling Disabled People
The Journal of Bangladesh Orthopaedic Society

Factors associated with health care seeking decision:
The result of the study shows that most of the time the
health seeking decision totally depended on the
surrounded people of the accidental place, their knowledge,
awareness and remaining facility and capacity regarding
proper management of the victims. By analyzing the in
depth interview findings this study identified four causes
that hinders the health seeking behavior of the victims for
acute conditions and for injuries; these are lack of
opportunity even to get first aid due to limitations of
transport and weak communication systems, long distance
of the health facilities, poor victim’s shortage of money
and eventually lack of mass awareness about rapid
management of road traffic accident victims. Moreover,
from the case studies the scenario of health seeking
behavior of the victims has been explored to understand
the accidental incidents and the way of being gone under
any sort of treatment.
Limitations of transport and weak communication systems:
Lack of proper transportation and immediate
communication systems leads treatment delay which in
consequence forces the victims to accept the chronic
disability in life time.
CASE: 1
“One day I was going to bus stand by rickshaw to go to
my village. All of a sudden a truck stroked my rickshaw
and I fell down in road side and lost my sense. Few minutes
later I found that few people were carrying me to hospital
by van (one type of three wheelers). They admitted me in
a private medical hospital. I told everything to doctor about
the accident then they phoned my relatives and later my
mother and brother came and broke down into tears. But it
was too late. I tried to seat but could not, severe pain
graved me, and one of my hands was bended with bed.
Doctor confirmed to my elder brother that my right hand
had been damaged. As it was deteriorating day by day
lastly it had to cut. Till then I am fully crippled and have
been bearing disable life (Male, age-50, married).”
Long distance of the injury service health facilities:
The long distance of the health facilities related with road
traffic injury has been found in the study as hindering to
get proper treatment in proper time to avoid long term
disability.
CASE: 2
“Near about one year ago, one morning I was going to my
working station. As I was so busy at bus stand, so to ride
the bus suddenly I fell down. Last wheel of the bus ran
over on my two legs. I was groaning “mother, mother”. I
lost my sense. When I got back my sense I was in a nearby
private clinic at Savar. Taking consideration of my severity
the hospital authority sent the message to my guardian.
Later I was sent to the trauma Hospital in Dhaka. Lastly
my legs were cut out. After 10 months treatment I came
back at home. I am now physically challenged person (Male,
age-23, unmarried).”
CASE: 3
“Three years ago I was going to Comilla with my husband
during Eid –Ul-Azha. Our bus stroke another truck and
our bus turned out. I and my husband both were injured
but I was severely injured. I felt a severe pain in my waist
and legs. Passersby rushed me to a nearest hospital by
tempo. As my condition was deteriorating day by day
then I admitted into a clinic in Dhaka. Doctors decided to
cut off my ankle by a surgery. After the surgery I was
crippled (Female, age-35, married).”
Lack of affordability of poor victims:
The result of the study finds disability as consequence
the poor victims’ shortage of money to get proper
treatment from proper health facility. In addition, due to
the decision often taken by the strangers with minimal
knowledge, the victims often had been shifted to
commercial private clinics rather than shifted to
Government trauma hospitals.
CASE: 4
“Five years ago, one day I was crossing the busy road of
Shewrapara, Mirpur. Unexpectedly a rushed private car
stroked me and I fell down following senseless. Pedestrians
carried away me to Showrowardy Hospital and later I was
shifted to a private clinic and not to the pongu haspatal
(Public Orthopedic hospital). As I was not capable to
bear the cost of treatment, so my operation was not
successful. One of my legs had to cut. Later because of
lethal infection I fully lost my one leg. In this way I lost my
leg forever. It is my fate I have lost my leg now I am helpless
(Male, age-40, married).”
Lack of mass awareness about rapid management of road
traffic accident victims:
Most of the time the health seeking decision totally
depended on the surrounded people of the accidental
place, their knowledge, awareness and remaining facility
and capacity regarding proper management of the victims.
Mohammad Mahbub Alam Talukder, Md. Ali Imam, Nasrin Akter, Nasir Uddin Sheikh 195
VOL. 29, NO. 2, JULY 2014

Often the lack of taking the right decision makes the poor
disable.
CASE: 5
“Just after accident local people shifted me to Dhaka
Showrowardy Hospital that was 8 kilometer away from the
accident spot. After almost 3 and half hours I got my first
aid in that hospital by the doctor of the hospital who was
on duty. (Male, age-40, married).”
Whereas, the study also finds some positive cases since
the road traffic accident related victims were managed
properly by the appropriate health seeking decision of
mass people. And it could assist the victims to recover
injury.
CASE: 6
“One day morning I was going to my office by bus. After
one kilometer ahead a truck stroke heavily to my bus, in
consequence the bus lost its way and hit the island on the
road. One of the heavy parts of the bus falls on my leg and
my ankle was broken. One passer-by took me to a private
hospital, later he took me disability hospital. I took
treatment seven days there and came back home (Male,
age-50, married).”
CASE: 7
“One day I determined to go Farmgate from Shahbagh.
When I was waiting for a bus, suddenly a microbus strokes
me from my back. I fell down on the street. People rushed
me into nearest pharmacy for first aid .They also collected
some money for me. As I had no money I came back home
by taking some medicine and I did not able to go to hospital
further. At last I lost both of my legs. Now I can’t walk
(Male, age-42, married).”
The study saw the sights of the depriving experiences of
the road traffic accident related victims since the moment
of accidental incident to health seeking behavior follows
to disability. This study reveals the facts how the
interviewees had to face these incidents. All the informants
of the study were sufferer but their experiences of health
seeking behavior and sufferings were not same. These
unexpected incidents came as a nightmare to their life.
The unbearable sorrows, thousands of adverse situations
and dependency to others started from the health seeking
moment to the lifelong passage of life.
First Aid and handling road traffic accident:
Distance, shortage of money, lack of opportunity of getting
the aid, lack of mass awareness again has been identified
as the main obstacles of getting the first aid assistance.
Most of the cases it took 2 to even 12 hours to get the first
aid. And findings of treatment seeking reveals the facts
that most often the victims did not get any early treatment
even the first aid. Moreover, in many cases it took more
and more time to get first aid. As one of the victims said-
“Few people took me away by helping me hand to hand
to hospital by CNG vehicle after my accident which is 12
km away from the accident spot. I took the first aid only
after reach at that hospital. “
Whereas, some victims would able to get the first aid
facilities and their recovery rate was higher. As one said-
“First the people of surroundings shifted me to a nearest
private clinic, 2 km away from the spot, by taxi. I got my
first aid immediately in that hospital and then they shifted
me to disability hospital.”
Diagram 2: First aid services in handling road traffic
accident related victims
In case of any road traffic accident first aid is the most
valuable issue after the accident. If the victim gets the
immediate first aid then the possibility of curing is higher.
However, the study explores the cause of treatment delay
that leaded to severe chronic disable condition of the
victims.
CONCLUSIONS AND RECOMMENDATIONS
The results of the study explore the health seeking
behavior after an incident of road traffic accident which
helps us to understand the context of existing first aid
facility and injury management. In Bangladesh, people are
vulnerable to different types of disability but treatment
facilities are not available to them. A large proportion of
196 Health Seeking Behaviour of Road Traffic Accident Victims: A Qualitative Study among the Slum Dwelling Disabled People
The Journal of Bangladesh Orthopaedic Society

people do not get treated because they cannot afford it.
Eventually, the lack of productivity caused by disability
and high medical treatment costs drive them towards
poverty, and poverty makes people ill. However, less
attention is paid to factors influencing medical treatment
seeking patterns or economic impoverishment of the
household, which are also important factors. Broadly,
by understanding the health seeking behavior and
health system response to the victims of traffic related
accident this research has created opportunity to
develop more fruitful ways of new intervention
designing to diminish the road accidents as well as to
reduce the sufferings of the disabled people.
It can be concluded that treatment delay must be reduced
by providing first aid within very short time and mass
awareness raising campaign is necessary to avoid the
severe trauma. Moreover, necessary measures should be
taken to ensure cost free public health service provision
to treat the long term disabled condition.
REFERENCES
1. Accident Research Institute –ARID (2012), Database.
2. Hoque MM. (2006), Understanding Road Accident
Problems and their Remedies, Road Safety Training
Course, ARC, BUET.
3. International Road Assessment Program- iRAP (2008)
Country Report.
4. Mackay M. (2003). Global Road Traffic Injuries: An
Overview of the Problem, UN Technical Briefings on the
Global Road Safety Crisis.
5. World Health Organization-WHO (2004). Injury Report.
Mohammad Mahbub Alam Talukder, Md. Ali Imam, Nasrin Akter, Nasir Uddin Sheikh 197
VOL. 29, NO. 2, JULY 2014

Book Review
Dr. Iqbal Qavi
“Current Progress in Orthopaedics” edited by Ashok Johar,i
MS(Orth), MCh (Orth), FRCS (Lo), FAMS from India, Keith DK
Luk, MD from Hong Kong and James P Wadell, MD, FRCSC from
Canada. List of contributors include 58 eminent academician,
clinicians and researchers from renowned institutes from different
parts of the world. The book has been endorsed by the
International Society of Orthopaedic Surgery and Traumatology,
SICOT.
Medical Knowledge is constantly changing. As new information
becomes available, changes in treatment, procedures, equipment,
and the use of drugs become necessary. The authors, editors, and
contributors have , as far as possible, taken care to ensure that the
information given in the text is accurate and up-to-date.
The book contains 24 chapters on different topics. The topics
include present status of treatment modules like Ponseti
management of clubfoot, management of cerebral palsy, and
brachial plexus birth palsy. The book includes difficult problems
in trauma such as management of open fractures, treatment of
displaced femoral neck fractures, operative management of distal
radial fractures in adults, and functional non-surgical treatment of
humeral fractures. Topics related to joint replacement surgery are role of joint registries in implant selection, role of
osteotomy, unicondylar arthroplasty and total knee arthroplasty in osteoarthritis of knee, role of cemented stem in total
hip replacement surgery, and role of hip resurfacing surgery. Topics related to arthroscopy are cartilage repair and
regeneration, advances in arthroscopic rotator cuff repair, and anatomic double-bundle ACL reconstruction. Spine
related topics include early onset scoliosis, sagittal alignment in degenerative lumber spine disease, prosthetic total disc
replacement, treatment of TB spine, and management of spinal metastasis. Other miscellaneous interesting topics are
femoroacetabular impingement, progress in limb lengthening, and joint preservation and biological reconstruction for
osteosarcoma around the knee.
The book is an interesting reading for update knowledge on recent developments in the above mentioned topics. The
authors hope to bring many more volumes in this series in the coming years.
The book is published by TreeLife Media, Kothari Medical Subscription Services Pvt. Ltd., Mumbai, India.
198 The Journal of Bangladesh Orthopaedic Society


















