The Intrathymic Pathogenesis of Myasthenia Graviset al., 1977), thymocytes (Fuchs et al., 1980), and...
7
The Intrathymic Pathogenesis of Myasthenia Gravis ARNOLD I. LEVINSON a, *, DECHENG SONG a , GLEN GAULTON b and YI ZHENG a a Allergy and Immunology Section, University of Pennsylvania School of Medicine, Room 1014 BRB II/III, 421 Curie Boulevard, Philadelphia, PA 19104, USA; b Department of Pathology and Laboratory Medicine, University of Pennsylvania School of Medicine, Room 357 BRB II/III, 421 Curie Boulevard, Philadelphia, PA 19104, USA The thymus is considered to play an important role in the pathogenesis of Myasthenia gravis, an autoimmune disease characterized by antibody-mediated skeletal muscle weakness. However, its role is yet to be defined. The studies described herein summarize our efforts to determine how intrathymic expression of the neuromuscular type of acetylcholine (ACh) receptors is involved in the immunopathogenesis of this autoimmune disease. We review the work characterizing the expression of neuromuscular ACh receptors in the thymus and advance a new hypothesis that examines the intrathymic expression of this autoantigen in disease pathogenesis. Keywords: Myasthenia gravis; Thymus; Acetylcholine receptor; Intrathymic expression INTRODUCTION Myasthenia gravis (MG) is a disease characterized by weakness of striated muscles. The weakness is due to impaired neuromuscular transmission resulting from a reduction of the number of receptors for the neurotrans- mitter, acetylcholine (ACh) at the postsynaptic myoneural junction. This reduction is caused by the action of anti- acetylcholine receptor (anti-AChR) antibodies, reviewed in Levinson et al. (1987). MG is a prototypic autoimmune disease; the immune effector mechanisms and autoanti- genic target have been delineated. However, the events leading to the abrogation of self-tolerance to the neuromuscular type of AChR (nAChR) remain a mystery. The thymus gland has long been considered to hold the key to solving this mystery, although the nature of its involvement remains to be elucidated. Interest in a pathogenic role for the thymus in MG has been fueled by pathologic, clinical and immunologic lines of evidence as reviewed by Levinson and Wheatley (1995). Briefly, thymus glands of 60 – 70% of MG patients demonstrate the histological pattern of germinal center hyperplasia whereas another 10% display cortical epithelial cell thymomas. Thymectomy, particularly in young patients (, 40 years of age) with thymic hyperplasia, is followed by clinical improvement and remains a first-line therapeutic intervention. nAChR- specific B and T cells have been recovered from MG thymus specimens but not control thymus tissue. This indicates that the autoimmune effector cells populate the diseased thymus. EXPRESSION OF nAChR IN THYMUS A major feature of the thymus that very likely represents an important pathogenic link to MG is the expression of nAChRs on cells in this organ as reviewed in Levinson and Wheatley (1995). The issue of thymic expression of AChR has attracted considerable interest, in part, because of the pivotal role that self-antigen expression in the thymus plays in tailoring the T cell repertoire. Moreover, the expression of nAChRS on thymic cells represents the first description of the “promiscuous” intrathymic expression of an organ-specific self-antigen that is the target of an autoimmune attack in the periphery. The early reports prompted some investigators to propose that the thymus might actually serve as a site of sensitization for this autoantigen (Wekerle et al., 1978). Taken at face value, this idea might be viewed as being incongruent with the cardinal immunologic construct, noted above, namely that thymic self-proteins, particularly those expressed on epithelial cells orchestrate the induction of self-tolerance (Klein and Kyewski, 2000). The nAChRs are expressed in two major forms as reviewed in Levinson (2001a). The so-called mature or junctional form is expressed on innervated muscles and the immature or fetal form is expressed on non-innervated tissue. At the mature (innervated) myoneural junction, nAChRs are comprised of four subunits labeled a, b, d and 1. Two alpha subunits and one each of the other subunits are assembled, like the whalebone in a corset, to form an asymmetric hourglass channel spanning the membrane. Two alternatively spliced alpha subunit ISSN 1740-2522 print/ISSN 1740-2530 online q 2004 Taylor & Francis Ltd DOI: 10.1080/17402520400001769 *Corresponding author. E-mail: [email protected] Clinical & Developmental Immunology, September/December 2004 Vol. 11 (3/4), pp. 215–220
Transcript of The Intrathymic Pathogenesis of Myasthenia Graviset al., 1977), thymocytes (Fuchs et al., 1980), and...
-
The Intrathymic Pathogenesis of Myasthenia Gravis
ARNOLD I. LEVINSONa,*, DECHENG SONGa, GLEN GAULTONb and YI ZHENGa
aAllergy and Immunology Section, University of Pennsylvania School of Medicine, Room 1014 BRB II/III, 421 Curie Boulevard, Philadelphia, PA19104, USA; bDepartment of Pathology and Laboratory Medicine, University of Pennsylvania School of Medicine, Room 357 BRB II/III, 421 Curie
Boulevard, Philadelphia, PA 19104, USA
The thymus is considered to play an important role in the pathogenesis of Myasthenia gravis,an autoimmune disease characterized by antibody-mediated skeletal muscle weakness. However, itsrole is yet to be defined. The studies described herein summarize our efforts to determine howintrathymic expression of the neuromuscular type of acetylcholine (ACh) receptors is involved in theimmunopathogenesis of this autoimmune disease. We review the work characterizing the expression ofneuromuscular ACh receptors in the thymus and advance a new hypothesis that examines theintrathymic expression of this autoantigen in disease pathogenesis.
Keywords: Myasthenia gravis; Thymus; Acetylcholine receptor; Intrathymic expression
INTRODUCTION
Myasthenia gravis (MG) is a disease characterized by
weakness of striated muscles. The weakness is due to
impaired neuromuscular transmission resulting from a
reduction of the number of receptors for the neurotrans-
mitter, acetylcholine (ACh) at the postsynaptic myoneural
junction. This reduction is caused by the action of anti-
acetylcholine receptor (anti-AChR) antibodies, reviewed
in Levinson et al. (1987). MG is a prototypic autoimmune
disease; the immune effector mechanisms and autoanti-
genic target have been delineated. However, the events
leading to the abrogation of self-tolerance to the
neuromuscular type of AChR (nAChR) remain a mystery.
The thymus gland has long been considered to hold the
key to solving this mystery, although the nature of its
involvement remains to be elucidated.
Interest in a pathogenic role for the thymus in MG has
been fueled by pathologic, clinical and immunologic lines
of evidence as reviewed by Levinson and Wheatley
(1995). Briefly, thymus glands of 60–70% of MG patients
demonstrate the histological pattern of germinal center
hyperplasia whereas another 10% display cortical
epithelial cell thymomas. Thymectomy, particularly in
young patients (,40 years of age) with thymichyperplasia, is followed by clinical improvement and
remains a first-line therapeutic intervention. nAChR-
specific B and T cells have been recovered from MG
thymus specimens but not control thymus tissue. This
indicates that the autoimmune effector cells populate
the diseased thymus.
EXPRESSION OF nAChR IN THYMUS
A major feature of the thymus that very likely represents
an important pathogenic link to MG is the expression of
nAChRs on cells in this organ as reviewed in Levinson and
Wheatley (1995). The issue of thymic expression of AChR
has attracted considerable interest, in part, because of the
pivotal role that self-antigen expression in the thymus
plays in tailoring the T cell repertoire. Moreover, the
expression of nAChRS on thymic cells represents the first
description of the “promiscuous” intrathymic expression
of an organ-specific self-antigen that is the target of an
autoimmune attack in the periphery. The early reports
prompted some investigators to propose that the thymus
might actually serve as a site of sensitization for this
autoantigen (Wekerle et al., 1978). Taken at face value,
this idea might be viewed as being incongruent with the
cardinal immunologic construct, noted above, namely that
thymic self-proteins, particularly those expressed on
epithelial cells orchestrate the induction of self-tolerance
(Klein and Kyewski, 2000).
The nAChRs are expressed in two major forms as
reviewed in Levinson (2001a). The so-called mature or
junctional form is expressed on innervated muscles and
the immature or fetal form is expressed on non-innervated
tissue. At the mature (innervated) myoneural junction,
nAChRs are comprised of four subunits labeled a, b, dand 1. Two alpha subunits and one each of the othersubunits are assembled, like the whalebone in a corset, to
form an asymmetric hourglass channel spanning the
membrane. Two alternatively spliced alpha subunit
ISSN 1740-2522 print/ISSN 1740-2530 online q 2004 Taylor & Francis Ltd
DOI: 10.1080/17402520400001769
*Corresponding author. E-mail: [email protected]
Clinical & Developmental Immunology, September/December 2004 Vol. 11 (3/4), pp. 215–220
-
isoforms have been characterized, P3A2 and P3Aþ. Thelarger P3Aþ isoform, which includes an additionalsequence of 25 amino acids between exons 3 and 4, is
found only in humans and other primates. In fetal muscle,
as in adult denervated muscle or nonjunctional membrane,
a g subunit replaces the 1 subunit found in mature,innervated muscle endplates.
In the analysis of nAChRs in the thymus, many
investigators have focused on the nAChR alpha subunit
(nAChRa) since it is the source of the important pathogenicT and B cell epitopes for the pathogenic autoimmune
response in MG (Oshima et al., 1990; Zhang et al., 1990;
Conti-Fine et al., 1998; Fuji and Lindstrom, 1988).
Expression of this subunit was originally reported on a
variety of thymic cells including epithelial cells (Engel
et al., 1977), thymocytes (Fuchs et al., 1980), and myoid
cells (Kao and Drachman, 1977; Schluep et al., 1987).
Myoid cells, which share phenotypic properties with
skeletal muscle cells, were originally viewed as the
principal AChR-expressing cells in thymus (Schluep et al.,
1987). They are found in the medulla of both normal and
MG thymus.
In the past several years, there has been renewed interest
in thymic cells as a source of nAChR expression. Several
investigators, including ourselves, have taken a molecular
approach in characterizing thymic AChRs and identifying
cell populations expressing them. Using reverse-transcrip-
tion-PCR (RT-PCR) technology, we reported that mRNA
for the AChRa was expressed in normal mouse(Wheatley et al., 1992), normal human and MG thymus
(Wheatley et al., 1993; Zheng et al., 1999). We also
reported that AChRa mRNA was expressed on trans-formed murine thymic cortical and medullary epithelial
cell lines and thymic dendritic cell lines (Wheatley et al.,
1992). We found that mRNAs encoding both major
isoforms of the human AChRa, i.e. P3Aþ and P3A2, wereexpressed in normal and MG thymus and normal human
thymic epithelial cells (Wheatley et al., 1993; Zheng et al.,
1999). Sequencing of P3Aþ and P3A2 cDNA clonesrecovered from control and MG thymus indicated that
they share the same nucleotide sequence as their
respective counterparts at the myoneural junction. Thus,
unless there are posttranslational changes, the structure of
the AChRa proteins expressed in the thymus and theperiphery are likely to be identical. These results provided
a structural basis for proposing that an immune response
directed at thymic nAChRa may be responsible forinitiating or perpetuating disease. Berrih-Aknin sub-
sequently reported that AChRa protein as well as mRNAwas expressed on human thymic epithelial cells (Wakkach
et al., 1978).
However, there is still a controversy over the expression
of the other subunits on thymic cells and whether they are
expressed as components of intact receptors. Some of the
reported discrepancies may reflect differences in the ages
of the thymus donors and differences in the design of the
RT-PCRs. At this time, it appears as if 1 and b mRNAs areexpressed in most normal and MG thymus specimens with
variable expression of d and g subunits (Naveneethamet al., 2001; Bruno et al., 2004). Expression of the AChR
subunits appears to be concentrated in the thymic
medullary compartment.
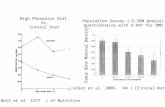
To gain a better understanding of how intrathymic
expression of nAChRa might be linked to the developmentof disease, we addressed additional features of nAChRaexpression in the thymus. We observed that the smaller
P3A2 isoform is present in approximately a five-fold
excess in both MG and control thymic tissue and a 2.5-fold
excess in a non-transformed human thymic epithelial cell
(TEC) line relative to the larger P3Aþ isoform (Fig. 1)(Zheng et al., 1999). The greater expression of the P3A2
isoform in thymus does not parallel its expression in
healthy and MG muscle tissue where both isoforms show
equivalent expression (Beeson et al., 1990). These
observations suggest that the expression of mRNAs
encoding the P3A2 and P3Aþ isoforms is regulateddifferently in human thymus and muscle. Since the same
disproportionate expression of P3A2 was observed in
control and MG thymus, it appears that the differential
pattern of expression observed in thymus relative to muscle
is not a manifestation of thymic pathology in MG. Rather,
this pattern may reflect control processes that are unique to
these two distinct tissue compartments. Presently, it is not
known whether the disproportionate expression of P3A2
vs. P3Aþ isoforms has pathogenic significance.We also observed that expression of both P3Aþ and
P3A2 mRNAs are increased in MG thymus compared to
control thymus (Fig. 2) (Zheng et al., 1999). This finding
parallels that reported for skeletal muscle where AChR
mRNA expression was found to be greater in MG muscle
than in control muscle (Guyon et al., 1993). The finding of
increased AChRa mRNA expression in MG thymus mayrepresent an attempt to compensate for the destructive
action of locally secreted anti-AChR antibodies. It is also
possible that the increased AChR mRNA expression may
reflect the antecedent action of other local environmental
factors, e.g. cytokines.
FIGURE 1 Relative expression of AChRa P3A2 and P3Aþ isoforms inthymus and TEC. Compilation of data from 14 MG thymuses, 7 controlthymuses, and 4 separate TEC experiments. The signals for the P3A2 andP3Aþ bands on Southern blots were quantitated on a phosphorimager.The P3A2/P3Aþ ratios are shown. Expression of P3A2 exceeded that ofP3Aþ by a factor of 5.5 ^ 0.9 (mean ^ SEM) in Control thymus,4.7 ^ 0.05 in MG thymus, and 2.8 ^ 0.2 in TEC. (Copyright: ClinicalImmunology, 1:1999).
A.I. LEVINSON et al.216
-
REGULATION OF INTRATHYMIC nAChRaEXPRESSION
IL-1 and IL-6 production by epithelial cells is increased in
hyperplastic thymic tissue obtained from MG patients
compared to thymus from control subjects (Cohen-
Kaminsky et al., 1978; Emilie et al., 1991). Since
cytokines produced in vitro by thymic epithelial cell
(TEC) lines demonstrate autocrine function (Galy and
Spits, 1991), it seemed plausible that these cytokines or
perhaps others produced by cells in the thymus might
regulate TEC expression of AChR. We examined this
possibility by incubating a human non-transformed TEC
line with either IL-1b, IL-4, IL-6 and interferon-g(IFN-g). We found that neither IL-1, IL-4, nor IL-6altered the expression of AChRa mRNA by this cell line(Zheng et al., 1999). By contrast, IFN-g increasedexpression of the P3A2 and P3Aþ isoforms by factors of2.7 and 2.8, respectively. It is known that IFN-gup-regulates the expression of MHC class II antigens on
thymic epithelial cells (Berrih-Aknin et al., 1985; Galy
and Spits, 1991). This dual effect of IFN-g on AChRa andMHC antigens raises the possibility that this cytokine, and
perhaps others, may alter expression of thymic AChRain vivo in a manner that leads to the development or
perpetuation of MG. Before addressing this idea, it would
be helpful to briefly review the role of self-antigen
expression in thymus plays in the development of T cell
tolerance and consider how the thymus could serve as a
site of immune activation.
INTRATHYMIC EXPRESSION OF SELF
ANTIGEN AND THE DEVELOPMENT OFT CELL TOLERANCE
The thymus plays a fundamental role in the generation of
the peripheral T cell repertoire as reviewed in Klein and
Kyewski (2000), Sprent et al. (1988), Kisielow and
Boehmer (1990), Alam et al. (1996) and Anderson et al.
(1996). It is generally believed that thymocytes with low
affinity receptors for self are positively selected for export
to the peripheral lymphoid tissues where they comprise the
T cell repertoire that recognizes exogenous antigens
(Kisielow and Boehmer, 1990; Anderson et al., 1996).
By contrast, T cell tolerance to self is effected largely by the
process of central deletion/inactivation. Developing
thymocytes with high affinity receptors for self-peptide
are silenced by apoptosis or anergy. There is widespread
agreement that presentation of self-peptides by cortical
epithelial cells is necessary for positive selection
(Kisielow and Boehmer, 1990; Alam et al., 1996;
Anderson et al., 1996). Thymic medullary epithelial cells
and to a lesser extent, bone marrow-derived macrophages
and dendritic are considered to be the major APCs
involved in negative selection (Blackman et al., 1990;
Bonomo and Matzinger, 1993; Hugo et al., 1994;
Hoffmann et al., 1995; Klein and Kyewski, 2000).
However, central deletion is not complete even though a
broad array of self-peptides is “promiscuously” expressed
on medullary thymic epithelial cells (Klein and Kyewski,
2000). Self-reactive T cells escape from the thymus in
small numbers, perhaps due to the fact that limiting levels
of self-antigen limit the efficiency of tolerance induction
(Adelstein et al., 1991; Iwabuchi et al., 1992; Oehen et al.,
1994). However, such self-reactive T cells are silenced by
their anergic or ignorant status, i.e. they never encounter
self-antigen in the periphery in a manner that leads to
immune activation, or they are suppressed by regulatory
T cells (Shevach, 2000).
FIGURE 2 Semiquantitative RT-PCR: compilation of results fromthymus specimens of seven control subjects and fourteen MG patients.The signal intensity of the AChRa bands is normalized to the signalintensity of the standard by calculating the ratio of thymicAChRa/AChRa standard. The expression of P3A2 and P3Aþ isoformsin MG thymus is 2.5- and 2.8-fold greater, respectively, than that incontrol thymus. (Copyright: Clinical Immunology, 1:1999).
FIGURE 3 Semiquantitative RT-PCR: compilation of results from sixTEC experiments depicting the effect of IFN-g on expression of AChRaisoforms in TEC. To determine the effect of IFN-g on the expression ofAChRa P3A2 and P3Aþ isoforms, we compared the normalized signalintensities of the isoforms (ratio of thymic AChRa/AChRa standard)detected in untreated and IFN-g treated TEC9 cultures. Expression ofP3A2 mRNA was significantly greater in IFN-g treated (2.19 ^ 0.75,mean þ SEM) than in untreated cultures (0.89 ^ 0.36, p , 0:05;student’s t-test). Likewise, expression of P3Aþ mRNA wassignificantly greater in IFN-g treated (0.9 ^ 0.31) than in untreatedcultures (0.36 ^ 0.15, p , 0:05). (Copyright: Clinical Immunology,1:1999).
PATHOGENESIS OF MYASTHENIA GRAVIS 217
-
THE THYMUS AND T CELL TRAFFICKING
Based on the classic studies of Gowans, traffic of
lymphocytes is generally considered to be unidirectional,
i.e. out of the thymus into the blood and peripheral
lymphoid organs (Gowans and Knight, 1964). However,
small numbers of peripheral immunocompetent T cells
migrate to the thymus, entering via the medulla
(Naparstek et al., 1982,1993; Michie et al., 1988;
Hirokawa et al., 1989; Agus et al., 1991; Gossmann
et al., 1991; Westermann et al., 1991). Most of the thymic
immigrants are T cells activated in the peripheral immune
system although even resting T cells may gain access to
the thymus (Hirokawa et al., 1989; Agus et al., 1991;
Gossmann et al., 1991; Westermann et al., 1991). It is not
known if the rate or number of thymic immigrants is
increased by an inflammatory reaction in the thymus.
Furthermore, it is not known if self-reactive T cell
immigrants are activated when they encounter their
specific antigens in the thymus. Thymus T cell immigrants
specific for the lymphocytic choriomeningitis virus
(LCMV) clear infectious foci from the thymus (Gossmann
et al., 1991). This observation indicates that peripheral T
cells can be activated when they engage specific foreign
antigens in the thymus in an appropriate context. When
self-reactive T cells encounter their antigens in other
tissue compartments in the presence of requisite
co-stimulatory signals, they can be activated to express
their differentiation program, reviewed in Mondino et al.
(1996). One mechanism that leads to a milieu that
promotes the abrogation of tolerance peripherally is
infection. Local infection can lead to the upregulation of
MHC antigens and co-stimulatory molecules on cells that
express low levels of self-antigens and thereby lead to
activation of autoreactive T cells (Mondino et al., 1996).
A NEW MODEL OF THYMIC INFLAMMATIONAND ITS IMPACT ON “RETROGRADE” T CELL
MIGRATION
Delineation of the molecular events, particularly in the
thymus, that trigger MG has been hampered by the lack of
a model system. Thymic pathology is not a feature of
experimental models of MG in rodents. Although such
models have provided insight into the pathogenesis of
MG, they have not served to elucidate the role played by
the thymus (Christadoss et al., 2000). To address this issue
we have developed a model of inflammation targeted to
the thymic medulla, the site of thymic entry by peripheral
T cells (Levinson et al., 2001b). We generated molecular
variants of the well characterized thymotrophic Gross
murine leukemia virus (G-MLV), GD17, that had
previously been shown to exclusively infect medullary
thymic epithelium following their intrathymic injection in
naı̈ve mice. The variants were constructed to allow for
easy casetting of a broad array of genes of interest. The
thymo-tropic MLV vectors were created by ligating a
425 bp fragment containing the U3 region of GD-17 into
the LTR backbone of the well defined M-MLV vector
LXSH.
The vectors used in our studies are presented in
linear form in Fig. 4. The parental LXSH vector includes
50 M-MSV LTR, the psi packaging site and 50 gagregion, the hygromycin resistance gene under control of
the SV40 promoter, and the 30 LTR of M-MLV. For ourexperimental protocol, we modified this vector by
insertion of the Lac z gene (LBSHG). We utilized
LBSHG and LXSHG as our experimental and control
vectors, respectively. As was true for GD17, we found that
these vectors also target expression of encoded genes to
the thymic medullary epithelium.
Balb/c mice were immunized to b-galactosidase (b-gal)and then injected intrathymically (i.t.) with the b-galencoding vector LBSHG or the control vector LXSHG.
Hematoxylin and eosin stained sections of thymus
obtained four days after i.t. injection of LBSHG, but not
LXSHG, showed obliteration of the cortical/medullary
architecture with marked cellular expansion of the
medulla. To determine whether this local inflammatory
reaction non-specifically augmented the entry of peri-
pheral T cells into the thymus, b-gal immunized micewere injected i.v. with a population of CFSE-labeled
CD4þ T cells specific for an unrelated antigenfour days after i.t. injection of LBSHG or LXSHG. The
CD4þ T cells were derived from a transgenic mouse
FIGURE 4 Schematic diagram of MLV-based vectors. The vectors used in these studies are presented in linear form. The parental LXSH vector includesthe 50 M-MCV LTR, the psi packaging site and the 50 gag region, the hygromycin resistance gene under the control of the SV40 promoter, and the 30 LTR ofM-MLV. Vectors are modified by insertion of either GD-17 U3 or LacZ. (Copyright: Annals of the New York Academy of Sciences, 998:2003).
A.I. LEVINSON et al.218
-
bearing a T cell receptor that recognized an influenza
hemagglutinin peptide. Animals that received LBSHG had
4.2-fold more CFSE-labeled CD4þ thymic immigrantsthan animals that received the control vector.
Using this model, we have begun to examine a new
hypothesis bearing on the intrathymic pathogenesis of MG.
(Fig. 5). The hypothesis posits that an inflammatory
reaction to an unrelated antigen within the medulla of the
thymus facilitates entry of peripheral AChRa-reactiveCD4þ T cells that escaped central deletion. These cellsenter the thymus in the medullary compartment where they
encounter AChRa expressed on antigen presenting cells.The concomitant intrathymic inflammatory reaction
creates a milieu that favors activation of these cells, i.e.
upregulation of MHC class II antigens, co-stimulatory
molecules on APCs, and perhaps upregulation of
AChR expression. Presentation of AChRa epitopes to theCD4þ thymic immigrants leads to their activation, help forlocally stimulated aAChR-reactive B cells, the productionof anti-AChR antibodies, and the development of MG. The
rationale for this hypothesis is outlined in Table I.
CONCLUSION
There is considerable circumstantial evidence that the
thymus plays a pivotal role in the pathogenesis of MG.
Nevertheless, the pathogenic link remains to be forged.
We are re-examining the hypothesis that AChR expressed
in the thymus drives the pathogenic autoimmune response.
We have established a model of intrathymic inflammation
that is localized to the thymic medulla and demonstrated
that such an inflammatory process promotes the
nonspecific entry of peripheral CD4þ T cells into thethymus. We are currently exploiting this model to
determine whether (1) AChR-reactive CD4þ T cellhoming to the thymus is also augmented by a concurrent
intrathymic inflammatory response to an unrelated antigen
and (2) AChR-reactive T cell immigrants undergo
activation following their engagement of autoantigen in
this inflammatory milieu, provide help for the production
of anti-AChR antibodies by immigrant autoreactive B
cells, and thereby promote the development of a
myasthenic syndrome.
Acknowledgements
Studies described in this report were supported by a grant
from the Muscular Dystrophy Association and National
Institutes of Health grant AI 50058. The authors thank
Cecelia Willitt for assistance in preparation of the
manuscript.
References
Adelstein, S., Pritchard-Briscoe, H., Anderson, T.A., et al. (1991)“Induction of self-tolerance in T cells but not B cells of transgenicmice expressing little self-antigen”, Science 251, 1223–1225.
Agus, D., Surh, C.D. and Sprent, J. (1991) “Reentry of T cells to the adultthymus is restricted to activavted cells”, J. Exp. Med. 173,1039–1046.
Alam, S.M., Travers, P.J., Wung, J.L., Nasholds, W., Redpath, S.,Jameson, S.C. and Gascoigne, N.R. (1996) “T-cell-receptor affinityand thymocyte positive selection”, Nature 381, 616–620.
Anderson, G., Moore, N.C., Owen, J.J. and Jenkinson, E.J. (1996)“Cellular interactions in thymocyte development”, Ann. Rev.Immunol. 14, 73–99.
Beeson, D., Morris, A., Vincent, A. and Newsom-Davis, J. (1990)“The human muscle nicotinic acetylcholine receptor a-subunit existsas two isoforms: a novel exon”, EMBO 9, 2101–2106.
Berrih-Aknin, S., Arenzana-Seisdedos, F., Cohen, S., Devos, R., Charron,D. and Virelizier, J. (1985) “Interferon-gamma modulates HLA classII antigen expression on cultured human thymic epithelial cells”,J. Immunol. 35, 1165–1171.
Blackman, M., Kappler, J. and Marrack, P. (1990) “The role of the TCRin positive and negative selection of developing cells”, Science 248,1335–1341.
Bonomo, A. and Matzinger, P. (1993) “Thymus epithelium inducestissue-specific tolerance”, J. Exp. Med. 177, 1153–1164.
Bruno, R., Sabater, L., Tolosa, E., et al. (2004) “Different patterns ofnicotinic acetylcholine receptor subunit transcription in humanthymus”, J. Neuroimaging 149, 147–159.
Christadoss, P., Poussin, M. and Deng, C. (2000) “Animal models ofmyasthenia gravis”, Clin. Immunol. 94, 75–87.
Cohen-Kaminsky, S., Delattre, R., Devergne, O., et al. (1978) “Syn-ergistic induction of interleukin-6 production and gene expression inhuman thymic epithelial cells by LPS and cytokines”, Cell Immunol.138, 79–93.
Conti-Fine, B.M., Navaneetham, D., Karachunski, P.L., Raju, R.,Diethelm-Okita, B., Okita, D., Howard, J. and Wang, Z. (1998) “T cellrecognition of the acetylcholine receptor in myasthenia gravis”, Ann.Acad. Sci. 841, 283–308.
Emilie, D., Creven, M.C., Cohen-Kaminsky, S., et al. (1991) “In situproduction of interleukins in hyperplastic thymus from myastheniagravis patients”, Hum. Pathol. 22, 461–468.
TABLE I Rationale for intrathymic pathogenesis hypothesis
nAChRa-reactive CD4+ T cells can be found in the blood of healthydonors as well as MG patients.
nAChRa-reactive T and B cells are recovered from MG thymus but not“control” thymus.
nAChRa is constitutively expressed on thymic myoid cells and thymicepithelial cells.
nAChRa mRNA and MHC class II protein expression on human thymicepithelial cells is upregulated by interferon-g.
Peripheral T cells traffic to thymus where they enter the medulla.
(Copyright: Annals of the New York Academy of Sciences, 998:2003).
FIGURE 5 A new hypothesis bearing on the intrathymic pathogenesisof MG. Please see text for details. (Copyright: Annals of the New YorkAcademy of Sciences, 998:2003)
PATHOGENESIS OF MYASTHENIA GRAVIS 219
-
Engel, W., Trotter, J.L., MacFarlin, D.E. and McIntosh, C.L. (1977)“Thymic epithelial cells contain acetylcholine receptor”, Lancet 1,1310–1311.
Fuchs, S., Schmidt-Hopfeldd, I. and Tridente, G. (1980) “Thymiclymphocytes bear a surface antigen which cross-reacts withacetylcholine receptor”, Nature 287, 162–164.
Fuji, Y. and Lindstrom, J. (1988) “Specificity of the T cell immuneresponse to acetylcholine receptor in experimental autoimmunemyasthenia gravis”, J. Immunol. 140, 1830–1837.
Galy, A.H. and Spits, H. (1991) “IL-1, IL-4, and IFN-g differentiallyregulate cytokine production and cell surface molecule expression incultured human thymic epithelial cells”, J. Immunol. 147,3823–3830.
Gossmann, J., Lohler, J. and Lehmann-Grube, F. (1991) “Entry ofantivirally active T lymphocytes into the thymus of virus-infectedmice”, J. Immunol. 146, 293–297.
Gowans, J.L. and Knight, E. (1964) “The route of re-circulation oflymphocytes in the rat”, Proc. R. Soc. Lond. B 159, 257–282.
Guyon, T., Levasseur, P., Truffault, F., Cottin, C., Ohta, K., Itoh, N. andOhta, M. (1993) “Nicotinic acetylcholine receptor a subunit variantsin human myasthenia gravis: quantification of steady-state levels ofmessenger RNA in muscle biopsy using the polymerase chainreaction”, J. Clin. Investig. 94, 16.
Hirokawa, K., Utsuyama, M. and Sado, T. (1989) “Immunohistologicalanalysis of immigration of thymocyte-precursors into the thymus:evidence for immigration of peripheral T cells into the thymicmedulla”, Cell Immunol. 119, 160–170.
Hoffman, M.W., Heath, W.R., Ruschmeyer, D. and Miller, J.F. (1995)“Deletion of high-avidity T cells by thymic epithelium”, Proc. Nat.Acad. Sci. USA 92, 9851–9855.
Hugo, P., Kappler, J.W., Godfrey, D.I. and Marrack, P.C. (1994)“Thymic epithelial cell lines that mediate positive selection can alsoinduce thymocyte clonal deletion”, J. Immunol. 152, 1022–1031.
Iwabuchi, K., Nakayama, K.I., Mc Coy, R.L., et al. (1992) “Cellular andpeptide requirements for in vitro clonal deletion of immaturethymocytes”, Proc. Natl Acad. Sci. 89, 9000–9004.
Kao, I. and Drachman, D.B. (1977) “Thymic muscle cells bearacetylcholine receptors: possible relation to myasthenia gravis”,Science 195, 74–75.
Kisielow, P. and Boehmer, M.V. (1990) “Negative and positive selectionof immature thymocytes: timing and the role of the ligand for T cellreceptor”, Semin. Immunol. 2, 35–44.
Klein, L. and Kyewski, B. (2000) “Promiscuous expression of tissueantigens in the thymus: a key to T-cell tolerance and autoimmunity?”,J. Mol. Med. 78, 483–494.
Levinson, A.I. and Wheatley, L. (1995) “The thymus and the pathogenesisof myasthenia gravis”, Clin. Immunol. Immunopathol. 78, 1–5.
Levinson, A.I., Zweiman, B. and Lisak, R.P. (1987) “Immunopatho-genesis and treatment of myasthenia gravis”, J. Clin. Immunol. 7,187–197.
Levinson, A.I. (2001a) “Myasthenia Gravis”, In: Rich, R., et al., eds,Principles and Practice of Clinical Immunology (St. Louis), Vol. 2.
Levinson, A.I., Zheng, Y., Gaulton, S., Moore, J., Pletcher, C.H., Song, D.and Wheatley, L.M. (2001b) “A new model linking intrathymicacetylcholine receptor expression and the pathogenesis of myastheniagravis”, Ann. Acad. Sci. 998, 257–265.
Marshall, D.J. and Gaulton, G.N. (1996) “The role of the immuneresponse in MuLV-induced lymphomagenesis”, Leukemia 10,1860–1866.
Michie, S.A., Kirkpatrick, E.A. and Rouse, R.V. (1988) “Rare peripheralT cells migrate to and persist in normal mouse thymus”, J. Exp. Med.168, 1929–1934.
Mondino, A., Khourts, A. and Jenkins, M.K. (1996) “The anatomyof T-cell activation and tolerance”, Proc. Natl Acad. Sci. 3,2245–2252.
Naparstek, Y., Holoshitz, J., Eissenstein, S., et al. (1982) “Effector Tlymphocyte line cells migrate to the thymus and persist there”, Nature300, 262–264.
Naparstek, Y., Ben-Nun, A., Holoshitz, J., et al. (1993) “T lymphocytelines producing or vaccinating against autoimmune encephalo-myelitis (EAE). Functional activation induces peanut agglutininreceptors and accumulation in the brain and thymus of line cells”,Eur. J. Immunol. 13, 418–423.
Naveneetham, D., Penn, A.S., Howard, J.F. and Conti-Fine, B.M. (2001)“Human thymuses express incomplete sets of muscle acetylcholinereceptor subunit transcripts that seldom include the d subunit”,Muscle Nerve 24, 203–210.
Oehen, S.U., Ohashi, P.S., Burki, K., Hengartner, H., Zinkernagel, R.M.and Aichele, P. (1994) “Escape of thymocytes and mature T cellsfrom clonal deletion due to limiting tolerogen expression levels”, CellImmunol. 158, 342–352.
Oshima, M., Ashizawa, T., Pollack, M.S. and Atassi, M.Z. (1990)“Autoimunne T cell recognition of human acetylcholinereceptor: the sites of T cell recognition in myasthenia gravis onthe extracellular part of the a-subunit”, Eur. J. Immunol. 20,2563–2569.
Schluep, M.N., Wilcox, N., Vincent, A., Dhoot, G.K. and Newsom-Davis, J. (1987) “Acetylcholine receptor in human thymic myoid cellsin situ: an immunologic study”, Ann. Neurol. 22, 212–222.
Shevach, E. (2000) “Regulatory T cells in autoimmunity”, Adv. Rev.Immunol. 18, 423–449.
Sprent, J., Lo, D., Gao, E.K. and Ron, Y. (1988) “T cell selection in thethymus”, Immunol. Rev. 101, 173–190.
Wakkach, A., Guyon, T., Bruand, C., Tzartos, S., Cohen-Kaminsky, S.and Berrih-Aknin, S. (1978) “Expression of acetylcholine receptorgenes in human thymic epithelial cells. Implications for myastheniagravis”, J. Immunol. 157, 3752–3760.
Wekerle, H., Ketelson, U.P., Zurn, A.D. and Fulpius, B.W. (1978)“Intrathymic pathogenesis of myasthenia gravis: transient expressionof acetylcholine receptors on thymus-derived myogenic cells”, Eur.J. Immunol. 8, 579–582.
Westermann, J., Smith, T., Peters, U., et al. (1991) “Both activated andnonactivated leukocytes from the periphery continuously enter thethymic medulla of adult rats: phenotypes, sources and magnitude oftraffic”, Eur. J. Immunol. 26, 1866–1874.
Wheatley, L.M., Urso, D., Tumas, K., Maltzman, J., Loh, E. andLevinson, A.I. (1992) “Molecular characterization of the nicotinicacetylcholine receptor alpha chain in mouse thymus”, J. Immunol.148, 3105–3109.
Wheatley, L.M., Urso, D., Zheng, Y., Loh, E. and Levinson, A.I. (1993)“Molecular analysis of intrathymic nicotinic acetylcholine receptor”,Ann. NY Acad. Sci. 681, 74–82.
Zhang, Y., Schluep, M., Frutiger, S., Hughes, G.J., Jeannet, M., Steck, A.and Barkas, T. (1990a) “Immunologic heterogeneity of autoreactiveT lymphocytes against the nicotinic acetylcholine receptor inmyasthenic patients”, Eur. J. Immunol. 20, 2577–2583.
Zhang, Y., Schluep, M., Frutiger, S., Hughes, G.J., Jeannet, M., Steck, A.and Barkas, T. (1990b) “Immunologic heterogeneity of autoreactiveT lymphocytes against the nicotinic acetylcholine receptor inmyasthenic patients”, Eur. J. Immunol. 20, 2577–2583.
Zheng, Y., Wheatley, L.M., Liu, T. and Levinson, A.I. (1999)“Acetylcholine receptor alpha subnit mRNA expression in humanthymus: augmented expression in myasthenia gravis and upregulationby interferon-g”, Clin. Immunol. 1, 170–177.
A.I. LEVINSON et al.220
-
Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com