The International Treatment Preparedness Coalition What is to be done? What is to be done?
51
The International Treatment Preparedness Coalition What is to be What is to be done? done?
-
Upload
phillip-freeman -
Category
Documents
-
view
218 -
download
0
Transcript of The International Treatment Preparedness Coalition What is to be done? What is to be done?

The International Treatment Preparedness Coalition
What is to be done?What is to be done?

What is ITPC?
• A coalition of over 700 people with HIV/AIDS and their advocates, from over 125 countries, promoting universal access to comprehensive AIDS treatment, through local, national, regional and global treatment advocacy and literacy projects
• ITPC was born out of the 2003 International Treatment Preparedness Summit in Cape Town, South Africa
• We have a governance structure of Regional Advisory Committees and an International Steering Group.

Why treatment advocacy?

You never get anything unless you ask for it!
If there is no struggle there is no progress.
Power concedes nothing without a demand. It never did and it never will.
- Frederick Douglass, 1857
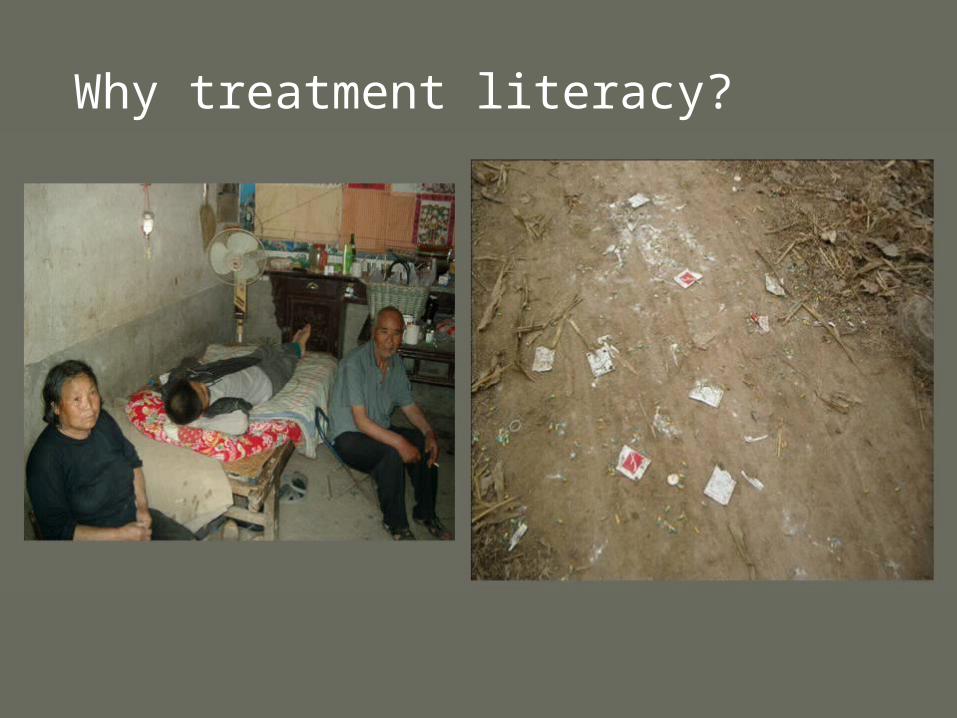
Why treatment literacy?
In one village, almost 90% of people stopped taking the ARVs within a short period of time. The main reason is because of the way they distributed the drugs without any education. They just passed them out with no information. So some of the people had side effects and the others watched them and stopped. So there is a lack of understanding and no treatment literacy and rumours start to come out of the village, “the government is trying to poison us." There is a lot of misunderstanding.
Thomas Cai, China
What has ITPC done so far?
• First meeting between Director-General of WHO, Executive Director of UNAIDS and GFATM and a delegation of PWLHAs in the history of the epidemic.
• Inclusion of Methadone on the WHO’s List of Essential Drugs and Medicines.
• Revision of Procurement Policy in Moldova• WHO’s Key Support for the Collaborative Fund

What has ITPC done so far?
• World Community Advisory Board (WorldCAB) meetings with originator and generic pharmaceutical companies.
• Days of Solidarity with the Treatment Action Campaign, Thai Drug Users Network, Front AIDS.
• Report Card on 3x5 - Missing the TargetKenya, Nigeria, South Africa, Russia, India,
Dominican Republic

Missing the target
Report on the progress of treatment rollout in 6 countries from people with HIV and their advocates
Missing the target
The following are key action points from the ITPC plan that we wholly endorse: resources not only pledged by donor governments but dispersed as well; better collaboration between WHO, UNAIDS, bilateral donors, and funding bodies such as the Global Fund to Fight AIDS, Tuberculosis, and Malaria, with clear assignment of responsibilities; detailed national plans for treatment scale-up that governments, WHO, and UNAIDS can be held accountable for meeting; and improved in-country visibility of WHO and UNAIDS, with these agencies acting as problem solvers.
- The Lancet, Moving up from 3 by 5
WorldCAB
Meetings between advocates and
generic and originator companies
WorldCAB
30 people with HIV and their advocates from all over the world

WorldCAB
At the meeting in India we met with the top management of Cipla and found out that Cipla doesn’t influence the prices of ARV drugs in the countries and that prices are formed locally…Comparison of the prices showed a difference between them of up to 27 times!…After finding out such outrageous facts we started an advocacy
campaign.

WorldCAB cont.
We prepared and distributed press releases among NGOs and government institutions in order to inform the public about severe violation of tender procedures.
The All-Ukrainian Network demanded that the government revise the tender for purchase of ARVs at world prices. As a result the tenders were cancelled.
- Hanna Khodas, WorldCAB 2 Report
What does ITPC want to do next?
Treatment AdvocacyOverview• Missing the Target 2. Expanded to 20-30 countries,
and including paediatrics, MTCT, OI treatment, 2nd line and vulnerable groups (women,
IDU, MSM. CSW)ARVs• WorldCAB 3 focusing on 2nd line treatment, develop
this working group (ITPC recently met with Abbott and Gilead to discuss access to 2nd line drugs)
• Technical assistance on registration, pricing etc to national groups

What does ITPC want to do next?
Diagnostics• Diagnostics report card• Diagnostics CAB
Ois • Short report top 5 OI drug needs
Treatment literacy• Diagnostic literacy booklet• Paediatric tx literacy booklet• Online tx literacy library (website)
What does ITPC want to do next?
Communications
• Regional email lists• Monthly reports from regions to ITPC list• Monthly translations in 4-6 languages of ITPC
digest (and emergency translations where necessary)

What does ITPC want to do next?
Collaborative Fund
As operational partner with Tides in the Collaborative Fund has distributed $4 million in small grants in 10 regions for local/regional mobilisation, tx literacy and advocacy. The grant programme will expand to cover HIV/TB and we will explore the possibility for two more regions (Middle East and North Africa and Southeast Europe).

Collaborative Fund for HIV Treatment PreparednessA Partnership of Tides Foundation and the International Treatment Preparedness Coalition

The Collaborative Fund: A community-driven funding mechanism that provides:
• Small grants to community organizations for treatment education, mobilization, and advocacy projects;
• Funding for regional coordination and networking to share information and advocacy strategies;
• Funding for technical assistance to support grantees;
• Program evaluation.


Funding in 10 regions:
• CIS/Baltics
• Caribbean
• Latin America
• Southeast Asia
• China
• South Asia
• Southern Africa
• West/Francophone Africa
• East Africa
• Women in Africa

How does it work:• Each region conducts a planning process,
including a workshop to develop a treatment preparedness agenda. ITPC regional members lead this process.
• Community Review Panels (CRP) are selected by workshop participants.
• CRPs are geographically diverse, have good gender balance, and majority are people living with HIV/AIDS.
• CRPs set funding priorities based on workshop discussion, develop an RFP, review grant applications, and decide which projects to fund.
• Tides Foundation collects organizational information and disburses funds.
A global structure for local impact:
• Small grants serve local level needs• ITPC Regional Advisory Committees develop
networking and TA activities on a regional level
• ITPC International Steering Committee provides global program direction
• Regional Coordinators in each region staff the CRP and implement TA and networking approaches
• GNP+ and ICW regional networks provide some of the regional coordination.

Regional Coordinators

2003
• February - Pilot project begins in CIS/Baltics region
• March - International Treatment Preparedness Summit held in Cape Town
• May - 1st Treatment Preparedness Workshop held in Minsk and CRP selected
• October - First round of grant making completed in CIS
• November - ITPC and Tides agree to develop global program



2004• February – Treatment Preparedness Conference in
Zimbabwe• May - ITPC meets with WHO and UNAIDS to
advocate for funding to communities as part of “3 by 5” initiative.
• October - Collaborative Fund is awarded $1 million from WHO
• November – Second round of CIS grant making completed
• Over $3 million is raised from other donors• Activities begin in Asia, Caribbean, Africa and
Latin America
2005• Treatment Preparedness workshops held in all 10
regions• Community Review Panels and Regional
Coordinators selected in all 10 regions• $200,000 is distributed in small grants in each of 9
regions• Technical assistance, network support and
program monitoring funds distributed in 9 regions totaling $630,000
• A total of $500,000 distributed for regional coordination and CRP support
• Program evaluation funded by WHO begins

TOTAL SPENDING - Breakdown by Activity
Community Networks 7%
Grants 43%
M&E 3%
Other 0%
Technical Assistance 6%
Workshops 8%
Indirect Admin 9%
Direct Admin 13%Reg. Coordination
11%
Community Networks
CRP Coordination
Grants
M&E
Other
Technical Assistance
Workshops
Indirect Admin
Direct Admin



Grant Application Process
• CRP develops funding priorities based on workshop discussion and develops an application form.
• Simple format in dominant languages of region.• Support is available to answer questions. The
application provides guidance and explains the program priorities.
• The application is broadly distributed. • People living with HIV/AIDS are involved in
every aspect of the process and all funded programs.
Grants Analysis - Subject
• Support groups, peer associations, and peer resource networks (>50%)
• Education and improved literacy about HIV/AIDS treatment options (>50%)
• Improved access and engagement with health care (>25%)
• Monitoring and advocacy of public and private sector efforts related to treatment (>15%)

Grant analysis - Demographic
• Grants made to 60 countries• Approximately 200 projects funded to date• PLWHA organizations (>50%)• Specific populations – women, drug users,
migrants, MSM, children, ethnic minorities, sex workers, prisoners
• Estimated 40 grantees working on national-level advocacy projects
• Over 50% of projects based in rural areas or small cities



A Commitment to Accountability and Transparency• CRP members selected through open
process with term limits and terms of reference.
• Each CRP develops conflict-of-interest and confidentiality policies
• A funding mechanism based on GIPA principles.
• All documents, including policies, reports, grant lists, budgets are available on the website – www.hivcollaborativefund.org

Technical Assistance and Network Support
• Each region determines technical assistance and network support needs.
• In China, each project was assigned a TA budget.
• In CIS, a website providing treatment information is in development
• In Latin America, workshops were held to increase capacity of non-funded organizations.
• In South Asia, a technical assistance workshop will bring all grantees together.
Monitoring and Evaluation
• Grantees submit six-month and year end reports. Simple reporting process.
• CRP develops other methods to monitor and evaluate programs.
• WHO funding an independent program evaluation.
• Developing operational research programs to evaluate program outcomes.
• No one has a greater stake in good evaluation than our grantees and the people they serve.

A Collaboration of Funders:There are currently 20 contributing partners to
the Collaborative Fund, including:
• World Health Organization
• Rockefeller Foundation• Ford Foundation• Stephen Lewis
Foundation• Johnson & Johnson • UNAIDS• Levi Strauss
Foundation
• AIDS Fonds Netherlands
• Open Society Institute• Pfizer Foundation• Overbrook Foundation• American Jewish World
Services• Pfizer Foundation• Tides Foundation
donors


Tides Foundation
• Administers grants• Ensures accountability and
transparency of process• Assists in developing policies of equity,
diversity, and openness• Raises funds • Assists Community Review Panels in
their work• Report to donors

Plans for 2006• A minimum of $200,000 in treatment
preparedness grants in each of 10 regions• $100,000 per region for network support and
technical assistance• $60,000 for regional coordination and CRP
support• $10,000 per region for program monitoring• Grant making for HIV/TB advocacy and education• Start of operational research to evaluation
treatment literacy programs• Strengthening partnerships with ICW and GNP+
The Collaborative Fund: A community-driven funding mechanism
that provides:
• Small grants to community organizations for treatment education, mobilization, and advocacy projects;
• Funding for regional networks to share information and advocacy strategies;
• Funding for technical assistance to support grantees;
• Program evaluation.
How does it work:
• Each region conducts a planning process, including a workshop to develop a treatment preparedness agenda. ITPC regional members lead this process.
• Community Review Panels (CRP) are selected by workshop participants.
• CRPs are geographically diverse, have good gender balance, and include people living with HIV/AIDS.
• CRPs set funding priorities based on workshop discussion, develop an RFP, review grant applications, and decide which projects to fund.
• Tides Foundation collects organizational information and disburses funds.
Grant analysis - Demographic
• Grants made to 60 countries• PLWHA organizations (>50%)• Specific populations – women, drug users,
migrants, MSM, children, ethnic minorities, sex workers
• Estimated 40 grantees working on national-level advocacy projects
• Over 50% of projects based in rural areas or small cities
TREATMENT FOR ALL!