The influence of high body mass index on the prognosis of patients with esophageal cancer after...
9
The Influence of High Body Mass Index on the Prognosis of Patients With Esophageal Cancer After Surgery as Primary Therapy Yuki Hayashi, MD, PhD 1 ; Arlene M. Correa, PhD 2 ; Wayne L. Hofstetter, MD 2 ; Ara A. Vaporciyan, MD 2 ; David C. Rice, MD 2 ; Garrett L. Walsh, MD 2 ; Reza J. Mehran, MD 2 ; Jeffrey H. Lee, MD 3 ; Manoop S. Bhutani, MD 3 ; Alexander Dekovich, MD 3 ; Stephen G. Swisher, MD 2 ; and Jaffer A. Ajani, MD 1 BACKGROUND: High body mass index (BMI), a prevalent condition in the United States, is associated with esopha- geal adenocarcinoma (EAC). Its influence on a patient’s outcome remains unclear. In the current study, the authors examined the impact of BMI on survival and complications in patients with esophageal cancer (EC) who underwent surgery as their primary therapy. METHODS: The authors retrospectively reviewed 301 consecutive EC patients who underwent surgery but received no adjunctive therapy. Patients were segregated into 2 subgroups based on their baseline BMI: normal/low (<25 kg/m 2 ) and high (25 kg/m 2 ). RESULTS: Seventy-six (25%) patients had a BMI <25 kg/m 2 and 225 (75%) patients had a BMI 25 kg/m 2 . In the high BMI group, there were more men (P < .001), fewer upper ECs (P ¼ .021), a lower baseline clinical stage (P ¼ .006), and frequent EAC (P < .001). Postoperative morbidity was similar in both groups, with the exception of gastrointestinal complications (P ¼ .016). The 5-year overall survival (OS) rates were 44% in the normal/low BMI group and 60% in the high BMI group (P ¼ .017). The 5-year disease-free survival (DFS) rates were 41% in the normal/low BMI group and 60% in the high BMI group (P ¼ .005). On multivari- able analysis, age, weight loss, peripheral vascular disease (PVD), and both clinical and pathological stage of disease were found to be independent prognosticators for OS. Older age (hazard ratio [HR], 1.029; 95% confidence interval [95% CI], 1.009-1.049 [P ¼ .004]), weight loss (HR, 1.525; 95% CI, 1.034-2.248 [P ¼ .033]), and PVD (HR, 2.325; 95% CI, 1.039-5.204 [P ¼ .040]) were found to be associated with poor OS. CONCLUSIONS: High BMI is common in EC patients and the better OS/DFS noted in patients with a high BMI is because of the diagnosis of a low baseline clini- cal stage. Confirmation of these findings is warranted. Cancer 2010;116:5619–27. V C 2010 American Cancer Society . KEYWORDS: body mass index, prognostic factors, esophageal cancer, surgery, stage.. High body mass index (BMI) is a serious health problem in the United States. According to the National Health and Nutrition Examination Survey, approximately 65% of adults were overweight (defined as a BMI of 25 to 30 kg/m 2 ) and 30% were obese (defined as a BMI of 30 kg/m 2 ). 1 These numbers are increasing gradually. High BMI is associated with an increased risk of malignancies that are contributing to 14% to 20% of cancer-related deaths. 2 The influence of high BMI on outcome in patients with cancer is an unsolved question. Recent studies demonstrated no significant correlation between BMI and survival rate in patients with ovarian, colon, and prostate cancer. 3-6 In 2009, approximately 16,000 new cases and 14,000 deaths from esophageal cancer (EC) were estimated to have occurred in the United States. 7 In the West, the incidence of esophageal adenocarcinoma (EAC) has been rising dramati- cally and that of squamous cell carcinoma (SCC) has been subsiding, with approximately 80% of new cases being diag- nosed as EAC. 8 High BMI is a risk factor for gastroesophageal reflux disease (GERD) and, consequently, for EAC. 9-11 Several studies have reported that high BMI was not associated with improved or reduced overall survival (OS) after esophagectomy, 12-14 although increased postoperative morbidity, such as respiratory complications, anastomotic leaks, and length of hospital stay, have been associated with high BMI in patients with gastroesophageal cancer who are DOI: 10.1002/cncr.25745, Received: May 3, 2010; Revised: August 10, 2010; Accepted: August 18, 2010, Published online November 8, 2010 in Wiley Online Library (wileyonlinelibrary.com) Corresponding author: Jaffer A. Ajani, MD, Department of Gastrointestinal Medical Oncology, Mail Stop 426, The University of Texas M. D. Anderson Cancer Center, 1515 Holcombe Boulevard, Houston, TX 77030; Fax: (713) 745-1163; [email protected] 1 Department of Gastrointestinal Medical Oncology, The University of Texas M. D. Anderson Cancer Center, Houston, Texas; 2 Department of Thoracic and Cardio- vascular Surgery, The University of Texas M. D. Anderson Cancer Center, Houston, Texas; 3 Department of Gastroenterology, Hepatology, and Nutrition, The Uni- versity of Texas M. D. Anderson Cancer Center, Houston, Texas. Cancer December 15, 2010 5619 Original Article
-
Upload
yuki-hayashi -
Category
Documents
-
view
213 -
download
1
Transcript of The influence of high body mass index on the prognosis of patients with esophageal cancer after...
The Influence of High Body Mass Index onthe Prognosis of Patients With EsophagealCancer After Surgery as Primary TherapyYuki Hayashi, MD, PhD1; Arlene M. Correa, PhD2; Wayne L. Hofstetter, MD2; Ara A. Vaporciyan, MD2; David C. Rice, MD2;
Garrett L. Walsh, MD2; Reza J. Mehran, MD2; Jeffrey H. Lee, MD3; Manoop S. Bhutani, MD3; Alexander Dekovich, MD3;
Stephen G. Swisher, MD2; and Jaffer A. Ajani, MD1
BACKGROUND: High body mass index (BMI), a prevalent condition in the United States, is associated with esopha-
geal adenocarcinoma (EAC). Its influence on a patient’s outcome remains unclear. In the current study, the authors
examined the impact of BMI on survival and complications in patients with esophageal cancer (EC) who underwent
surgery as their primary therapy. METHODS: The authors retrospectively reviewed 301 consecutive EC patients who
underwent surgery but received no adjunctive therapy. Patients were segregated into 2 subgroups based on their
baseline BMI: normal/low (<25 kg/m2) and high (�25 kg/m2). RESULTS: Seventy-six (25%) patients had a BMI <25
kg/m2 and 225 (75%) patients had a BMI �25 kg/m2. In the high BMI group, there were more men (P < .001), fewer
upper ECs (P ¼ .021), a lower baseline clinical stage (P ¼ .006), and frequent EAC (P < .001). Postoperative morbidity
was similar in both groups, with the exception of gastrointestinal complications (P ¼ .016). The 5-year overall survival
(OS) rates were 44% in the normal/low BMI group and 60% in the high BMI group (P ¼ .017). The 5-year disease-free
survival (DFS) rates were 41% in the normal/low BMI group and 60% in the high BMI group (P ¼ .005). On multivari-
able analysis, age, weight loss, peripheral vascular disease (PVD), and both clinical and pathological stage of disease
were found to be independent prognosticators for OS. Older age (hazard ratio [HR], 1.029; 95% confidence interval
[95% CI], 1.009-1.049 [P ¼ .004]), weight loss (HR, 1.525; 95% CI, 1.034-2.248 [P ¼ .033]), and PVD (HR, 2.325; 95%
CI, 1.039-5.204 [P ¼ .040]) were found to be associated with poor OS. CONCLUSIONS: High BMI is common in EC
patients and the better OS/DFS noted in patients with a high BMI is because of the diagnosis of a low baseline clini-
cal stage. Confirmation of these findings is warranted. Cancer 2010;116:5619–27. VC 2010 American Cancer Society.
KEYWORDS: body mass index, prognostic factors, esophageal cancer, surgery, stage..
High body mass index (BMI) is a serious health problem in the United States. According to the National Health andNutrition Examination Survey, approximately 65% of adults were overweight (defined as a BMI of 25 to 30 kg/m2) and30% were obese (defined as a BMI of�30 kg/m2).1 These numbers are increasing gradually. High BMI is associated withan increased risk of malignancies that are contributing to 14% to 20% of cancer-related deaths.2 The influence of highBMI on outcome in patients with cancer is an unsolved question. Recent studies demonstrated no significant correlationbetween BMI and survival rate in patients with ovarian, colon, and prostate cancer.3-6
In 2009, approximately 16,000 new cases and 14,000 deaths from esophageal cancer (EC) were estimated to haveoccurred in the United States.7 In the West, the incidence of esophageal adenocarcinoma (EAC) has been rising dramati-cally and that of squamous cell carcinoma (SCC) has been subsiding, with approximately 80% of new cases being diag-nosed as EAC.8 High BMI is a risk factor for gastroesophageal reflux disease (GERD) and, consequently, for EAC.9-11
Several studies have reported that high BMI was not associated with improved or reduced overall survival (OS) afteresophagectomy,12-14 although increased postoperative morbidity, such as respiratory complications, anastomotic leaks,and length of hospital stay, have been associated with high BMI in patients with gastroesophageal cancer who are
DOI: 10.1002/cncr.25745, Received: May 3, 2010; Revised: August 10, 2010; Accepted: August 18, 2010, Published online November 8, 2010 in Wiley Online
Library (wileyonlinelibrary.com)
Corresponding author: Jaffer A. Ajani, MD, Department of Gastrointestinal Medical Oncology, Mail Stop 426, The University of Texas M. D. Anderson Cancer
Center, 1515 Holcombe Boulevard, Houston, TX 77030; Fax: (713) 745-1163; [email protected]
1Department of Gastrointestinal Medical Oncology, The University of Texas M. D. Anderson Cancer Center, Houston, Texas; 2Department of Thoracic and Cardio-
vascular Surgery, The University of Texas M. D. Anderson Cancer Center, Houston, Texas; 3Department of Gastroenterology, Hepatology, and Nutrition, The Uni-
versity of Texas M. D. Anderson Cancer Center, Houston, Texas.
Cancer December 15, 2010 5619
Original Article

undergoing surgery.14,15 Many of these studies includedsmall number of patients, in whom adjunctive therapy(preoperative chemotherapy and/or radiotherapy) wasused.
The goal of the current analysis was to learn aboutthe impact of high or low BMI on long-term outcome aswell as surgical complications in 301 patients with ECwho underwent surgery as their primary therapy at TheUniversity of Texas M. D. Anderson Cancer Center(MDACC) but did not receive any adjunctive therapy.
MATERIALS AND METHODS
Patients
We searched the EC database in the Department of Tho-racic and Cardiovascular Surgery at MDACC to find 301consecutive patients who were fully staged and had under-gone surgery as their primary therapy and received no ad-junctive therapy. Patients who did not undergo surgery atMDACCwere not included in this database.
Patients were included if they had histologic docu-mentation of EAC or SCC histology and computed to-mography scans of the chest and abdomen. All eligiblepatients were aged �18 years. Staging was determinedbased on the American Joint Committee on CancerTNM staging system.16 No other selection criteria wereimplemented. Stored information regarding alcohol con-sumption, smoking (ever smoker), surgical complications,and other parameters such as length of hospital stay andmortality were captured and analyzed. The InstitutionalReview Board of MDACC approved this analysis.
Surgery
Types of esophagectomy included Ivor-Lewis, transhiatal,total esophagectomy, and minimally invasiveesophagectomy.
Follow-Up and Survival
Patients were followed periodically for at least 5 years oruntil death. Additional follow-up data were obtainedfrom review of the MDACC tumor registry and the hos-pital records or Social Security database. Follow-up timewas calculated from the date of surgery to the event ordate of the last contact.
Statistical Analysis
The data in the EC database were collected in a prospec-tive manner with a standardized approved protocol. Allstatistical analyses were performed using the SPSS Statisti-
cal Software Package (version SPSS 15.0; SPSS Inc, Chi-cago, Ill). The differences between groups were tested forsignificance using the Student t test for continuous varia-bles and the Fisher exact test or chi-square test for categor-ical variables. Univariable Cox regression analyses wereperformed using death and disease recurrence or death asthe outcomes with a significance level of P � .05. Covari-ates that were significant at P � .25 were included in themultivariable Cox regression analyses. Backward stepwiseWald elimination at P ¼ .10 was used to find a finalmodel. Death and disease recurrence or death functionswere calculated according to the Kaplan-Meier methodand differences were assessed using the log-rank test.
RESULTS
Patient Characteristics
A total of 301 consecutive EC patients who underwentsurgery as their primary therapy (and received no adjunc-tive therapy) were analyzed. Among these, 266 (88%)patients had EAC and 35 (12%) patients had SCC.Patient characteristics are summarized in Table 1. Menpredominated the group as expected (P � .001) and ade-nocarcinoma histology was common (P� .001).
Patient Characteristics by BMI
Patients were divided into 2 groups according the tradi-tional BMI cutpoints (<25 kg/m2 or �25 kg/m2). Therewere 76 patients (25.2%) with a pretreatment BMI <25kg/m2 and 225 patients (74.8%) with a pretreatmentBMI�25 kg/m2. As shown in Table 1, the 2 groups werewell matched with regard to age, Zubrod performance sta-tus, past medical history except for sex, diabetes, and his-tological type. However, in the high BMI group, male sex,a primary tumor in the lower esophagus (with or withoutgastroesophageal junction [GEJ] involvement), EAC, andlower baseline clinical stage were represented at a statisti-cally significantly higher rate than in patients in the lowBMI group (P� .001, P¼ .021, P� .001, and P¼ .006,respectively). Patients who lost weight during the preced-ing 3 months from the date of surgery or who smokedtobacco were more likely to be in the normal/low BMIgroup compared with the high BMI group (P� .001 andP¼ .031, respectively).
Surgical Outcomes
Ivor-Lewis esophagectomy was performed in 132patients, transhiatal esophagectomy was performed in125 patients, total esophagectomy was performed in 24
Original Article
5620 Cancer December 15, 2010
patients, and minimally invasive esophagectomy was per-formed in 17 patients. Outcomes of surgery are shown inTable 2. The 30-day surgical mortality rate was 2.6% (2patients) in the normal/low BMI group and 1.8% (4patients) in the high BMI group (P ¼ .473). Althoughgastrointestinal complications (diarrhea, dumping syn-drome, gastric outlet/conduit obstruction, ileus, and smallbowel obstruction) were more frequent in the high BMIgroup, there was no significant difference noted with
regard to other postoperative complications, such aspulmonary (P ¼ .796), cardiovascular (P ¼ .271), andwound-related/infectious complications (P ¼ .509) andanastomotic leak (P ¼ .786). The median postoperativehospital stay was 11 days in the normal/low BMI groupand 12 days in the high BMI group.
Disease recurrence after surgery developed in 25patients (32.9%) in the normal/low BMI group and 53patients (23.6%) in the high BMI group. The type of
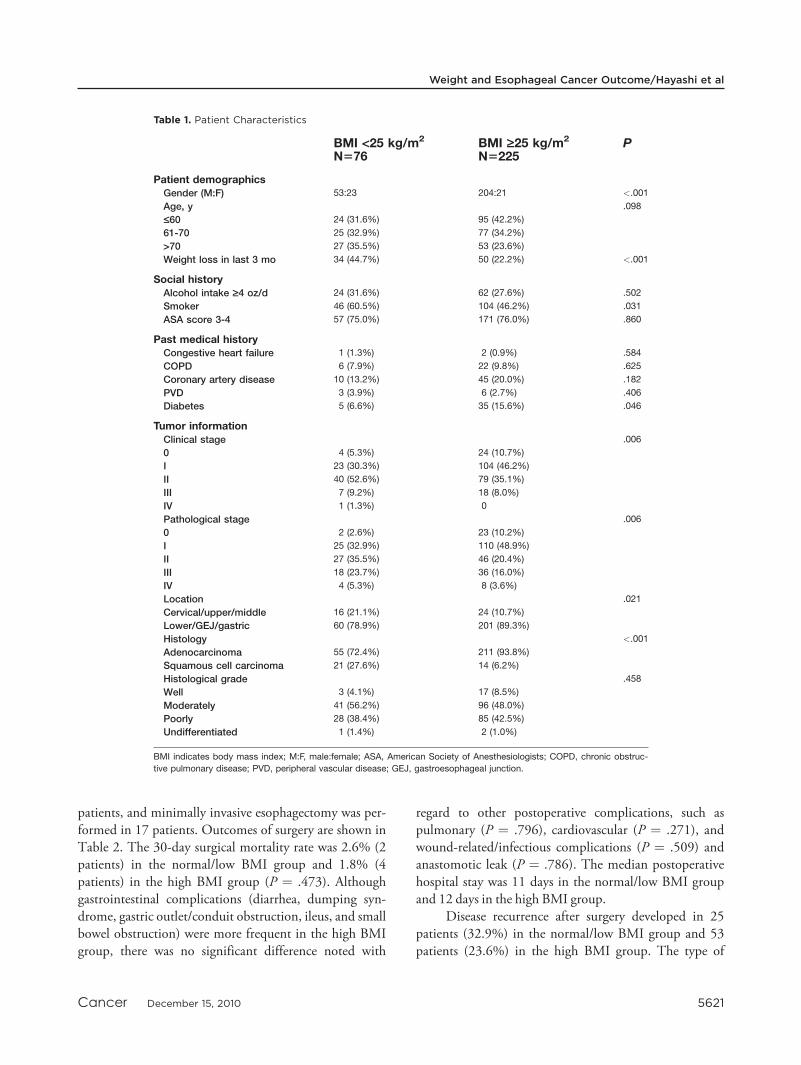
Table 1. Patient Characteristics
BMI <25 kg/m2
N576BMI ‡25 kg/m2
N5225P
Patient demographicsGender (M:F) 53:23 204:21 <.001
Age, y .098
£60 24 (31.6%) 95 (42.2%)
61-70 25 (32.9%) 77 (34.2%)
>70 27 (35.5%) 53 (23.6%)
Weight loss in last 3 mo 34 (44.7%) 50 (22.2%) <.001
Social historyAlcohol intake ‡4 oz/d 24 (31.6%) 62 (27.6%) .502
Smoker 46 (60.5%) 104 (46.2%) .031
ASA score 3-4 57 (75.0%) 171 (76.0%) .860
Past medical historyCongestive heart failure 1 (1.3%) 2 (0.9%) .584
COPD 6 (7.9%) 22 (9.8%) .625
Coronary artery disease 10 (13.2%) 45 (20.0%) .182
PVD 3 (3.9%) 6 (2.7%) .406
Diabetes 5 (6.6%) 35 (15.6%) .046
Tumor informationClinical stage .006
0 4 (5.3%) 24 (10.7%)
I 23 (30.3%) 104 (46.2%)
II 40 (52.6%) 79 (35.1%)
III 7 (9.2%) 18 (8.0%)
IV 1 (1.3%) 0
Pathological stage .006
0 2 (2.6%) 23 (10.2%)
I 25 (32.9%) 110 (48.9%)
II 27 (35.5%) 46 (20.4%)
III 18 (23.7%) 36 (16.0%)
IV 4 (5.3%) 8 (3.6%)
Location .021
Cervical/upper/middle 16 (21.1%) 24 (10.7%)
Lower/GEJ/gastric 60 (78.9%) 201 (89.3%)
Histology <.001
Adenocarcinoma 55 (72.4%) 211 (93.8%)
Squamous cell carcinoma 21 (27.6%) 14 (6.2%)
Histological grade .458
Well 3 (4.1%) 17 (8.5%)
Moderately 41 (56.2%) 96 (48.0%)
Poorly 28 (38.4%) 85 (42.5%)
Undifferentiated 1 (1.4%) 2 (1.0%)
BMI indicates body mass index; M:F, male:female; ASA, American Society of Anesthesiologists; COPD, chronic obstruc-
tive pulmonary disease; PVD, peripheral vascular disease; GEJ, gastroesophageal junction.
Weight and Esophageal Cancer Outcome/Hayashi et al
Cancer December 15, 2010 5621
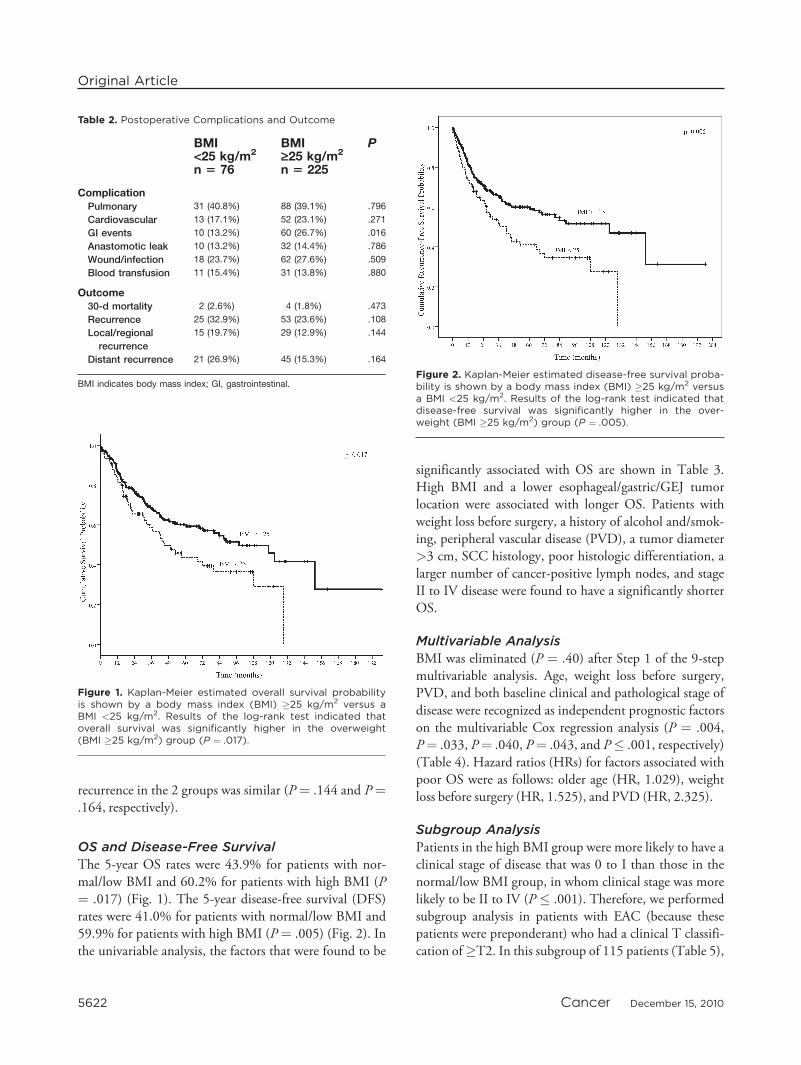
recurrence in the 2 groups was similar (P ¼ .144 and P¼.164, respectively).
OS and Disease-Free Survival
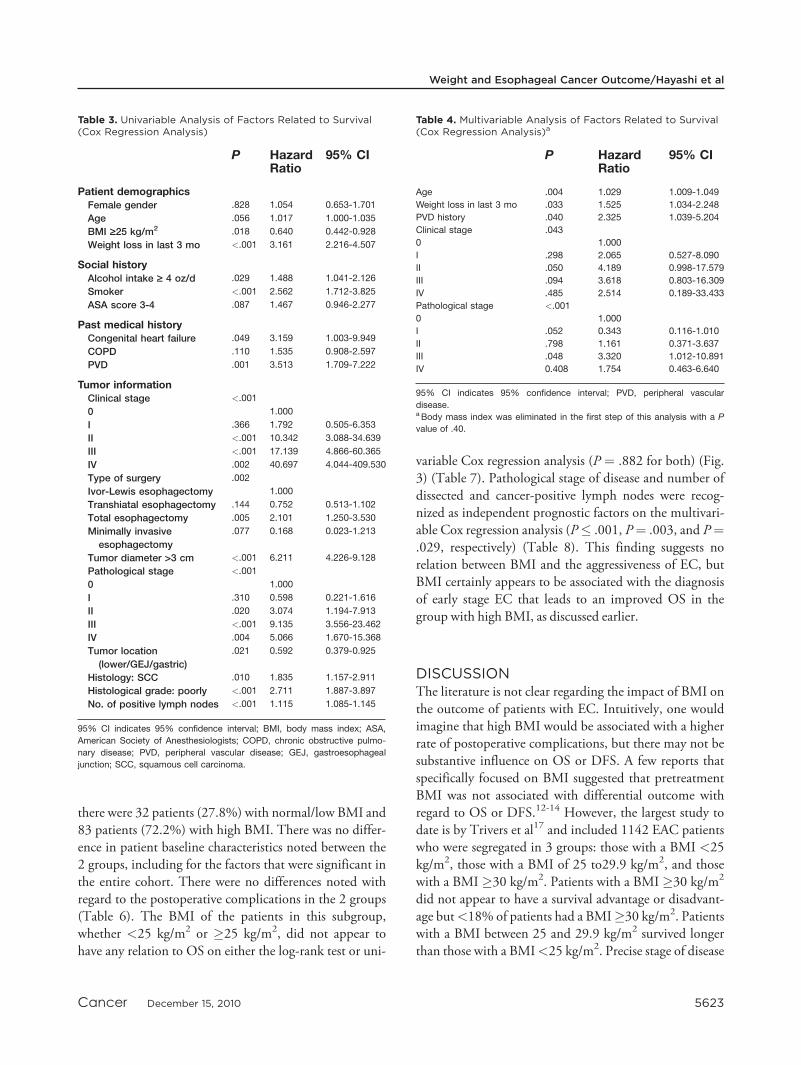
The 5-year OS rates were 43.9% for patients with nor-mal/low BMI and 60.2% for patients with high BMI (P¼ .017) (Fig. 1). The 5-year disease-free survival (DFS)rates were 41.0% for patients with normal/low BMI and59.9% for patients with high BMI (P ¼ .005) (Fig. 2). Inthe univariable analysis, the factors that were found to be
significantly associated with OS are shown in Table 3.High BMI and a lower esophageal/gastric/GEJ tumorlocation were associated with longer OS. Patients withweight loss before surgery, a history of alcohol and/smok-ing, peripheral vascular disease (PVD), a tumor diameter>3 cm, SCC histology, poor histologic differentiation, alarger number of cancer-positive lymph nodes, and stageII to IV disease were found to have a significantly shorterOS.
Multivariable Analysis
BMI was eliminated (P ¼ .40) after Step 1 of the 9-stepmultivariable analysis. Age, weight loss before surgery,PVD, and both baseline clinical and pathological stage ofdisease were recognized as independent prognostic factorson the multivariable Cox regression analysis (P ¼ .004,P¼ .033, P¼ .040, P¼ .043, and P� .001, respectively)(Table 4). Hazard ratios (HRs) for factors associated withpoor OS were as follows: older age (HR, 1.029), weightloss before surgery (HR, 1.525), and PVD (HR, 2.325).
Subgroup Analysis
Patients in the high BMI group were more likely to have aclinical stage of disease that was 0 to I than those in thenormal/low BMI group, in whom clinical stage was morelikely to be II to IV (P � .001). Therefore, we performedsubgroup analysis in patients with EAC (because thesepatients were preponderant) who had a clinical T classifi-cation of�T2. In this subgroup of 115 patients (Table 5),
Table 2. Postoperative Complications and Outcome
BMI<25 kg/m2
n 5 76
BMI‡25 kg/m2
n 5 225
P
ComplicationPulmonary 31 (40.8%) 88 (39.1%) .796
Cardiovascular 13 (17.1%) 52 (23.1%) .271
GI events 10 (13.2%) 60 (26.7%) .016
Anastomotic leak 10 (13.2%) 32 (14.4%) .786
Wound/infection 18 (23.7%) 62 (27.6%) .509
Blood transfusion 11 (15.4%) 31 (13.8%) .880
Outcome30-d mortality 2 (2.6%) 4 (1.8%) .473
Recurrence 25 (32.9%) 53 (23.6%) .108
Local/regional
recurrence
15 (19.7%) 29 (12.9%) .144
Distant recurrence 21 (26.9%) 45 (15.3%) .164
BMI indicates body mass index; GI, gastrointestinal.
Figure 1. Kaplan-Meier estimated overall survival probabilityis shown by a body mass index (BMI) �25 kg/m2 versus aBMI <25 kg/m2. Results of the log-rank test indicated thatoverall survival was significantly higher in the overweight(BMI �25 kg/m2) group (P ¼ .017).
Figure 2. Kaplan-Meier estimated disease-free survival proba-bility is shown by a body mass index (BMI) �25 kg/m2 versusa BMI <25 kg/m2. Results of the log-rank test indicated thatdisease-free survival was significantly higher in the over-weight (BMI �25 kg/m2) group (P ¼ .005).
Original Article
5622 Cancer December 15, 2010
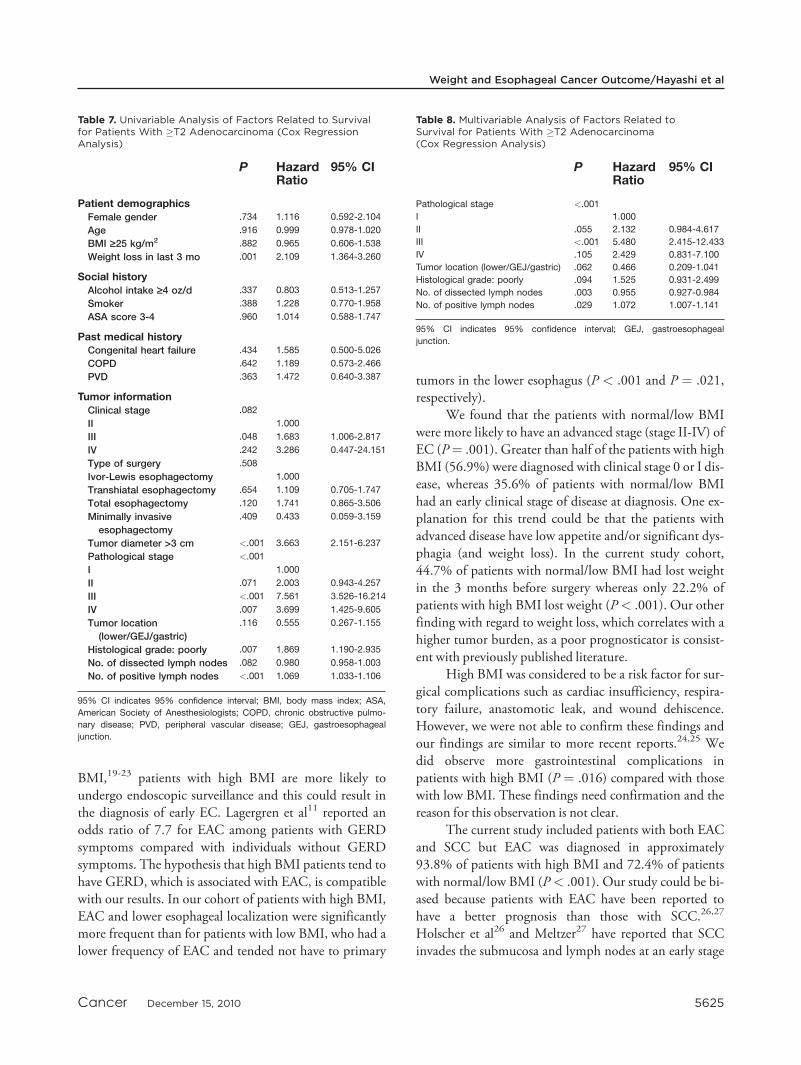
there were 32 patients (27.8%) with normal/low BMI and83 patients (72.2%) with high BMI. There was no differ-ence in patient baseline characteristics noted between the2 groups, including for the factors that were significant inthe entire cohort. There were no differences noted withregard to the postoperative complications in the 2 groups(Table 6). The BMI of the patients in this subgroup,whether <25 kg/m2 or �25 kg/m2, did not appear tohave any relation to OS on either the log-rank test or uni-
variable Cox regression analysis (P ¼ .882 for both) (Fig.3) (Table 7). Pathological stage of disease and number ofdissected and cancer-positive lymph nodes were recog-nized as independent prognostic factors on the multivari-able Cox regression analysis (P� .001, P¼ .003, and P¼.029, respectively) (Table 8). This finding suggests norelation between BMI and the aggressiveness of EC, butBMI certainly appears to be associated with the diagnosisof early stage EC that leads to an improved OS in thegroup with high BMI, as discussed earlier.
DISCUSSIONThe literature is not clear regarding the impact of BMI onthe outcome of patients with EC. Intuitively, one wouldimagine that high BMI would be associated with a higherrate of postoperative complications, but there may not besubstantive influence on OS or DFS. A few reports thatspecifically focused on BMI suggested that pretreatmentBMI was not associated with differential outcome withregard to OS or DFS.12-14 However, the largest study todate is by Trivers et al17 and included 1142 EAC patientswho were segregated in 3 groups: those with a BMI <25kg/m2, those with a BMI of 25 to29.9 kg/m2, and thosewith a BMI �30 kg/m2. Patients with a BMI �30 kg/m2
did not appear to have a survival advantage or disadvant-age but<18% of patients had a BMI�30 kg/m2. Patientswith a BMI between 25 and 29.9 kg/m2 survived longerthan those with a BMI<25 kg/m2. Precise stage of disease
Table 3. Univariable Analysis of Factors Related to Survival(Cox Regression Analysis)
P HazardRatio
95% CI
Patient demographicsFemale gender .828 1.054 0.653-1.701
Age .056 1.017 1.000-1.035
BMI ‡25 kg/m2 .018 0.640 0.442-0.928
Weight loss in last 3 mo <.001 3.161 2.216-4.507
Social historyAlcohol intake ‡ 4 oz/d .029 1.488 1.041-2.126
Smoker <.001 2.562 1.712-3.825
ASA score 3-4 .087 1.467 0.946-2.277
Past medical historyCongenital heart failure .049 3.159 1.003-9.949
COPD .110 1.535 0.908-2.597
PVD .001 3.513 1.709-7.222
Tumor informationClinical stage <.001
0 1.000
I .366 1.792 0.505-6.353
II <.001 10.342 3.088-34.639
III <.001 17.139 4.866-60.365
IV .002 40.697 4.044-409.530
Type of surgery .002
Ivor-Lewis esophagectomy 1.000
Transhiatal esophagectomy .144 0.752 0.513-1.102
Total esophagectomy .005 2.101 1.250-3.530
Minimally invasive
esophagectomy
.077 0.168 0.023-1.213
Tumor diameter >3 cm <.001 6.211 4.226-9.128
Pathological stage <.001
0 1.000
I .310 0.598 0.221-1.616
II .020 3.074 1.194-7.913
III <.001 9.135 3.556-23.462
IV .004 5.066 1.670-15.368
Tumor location
(lower/GEJ/gastric)
.021 0.592 0.379-0.925
Histology: SCC .010 1.835 1.157-2.911
Histological grade: poorly <.001 2.711 1.887-3.897
No. of positive lymph nodes <.001 1.115 1.085-1.145
95% CI indicates 95% confidence interval; BMI, body mass index; ASA,
American Society of Anesthesiologists; COPD, chronic obstructive pulmo-
nary disease; PVD, peripheral vascular disease; GEJ, gastroesophageal
junction; SCC, squamous cell carcinoma.
Table 4. Multivariable Analysis of Factors Related to Survival(Cox Regression Analysis)a
P HazardRatio
95% CI
Age .004 1.029 1.009-1.049
Weight loss in last 3 mo .033 1.525 1.034-2.248
PVD history .040 2.325 1.039-5.204
Clinical stage .043
0 1.000
I .298 2.065 0.527-8.090
II .050 4.189 0.998-17.579
III .094 3.618 0.803-16.309
IV .485 2.514 0.189-33.433
Pathological stage <.001
0 1.000
I .052 0.343 0.116-1.010
II .798 1.161 0.371-3.637
III .048 3.320 1.012-10.891
IV 0.408 1.754 0.463-6.640
95% CI indicates 95% confidence interval; PVD, peripheral vascular
disease.a Body mass index was eliminated in the first step of this analysis with a P
value of .40.
Weight and Esophageal Cancer Outcome/Hayashi et al
Cancer December 15, 2010 5623

at diagnosis was not reported in this analysis and theauthors, unfortunately, did not analyze the relationbetween ‘‘stage’’ at diagnosis and BMI. In a much smallerstudy, Di Fiore et al18 demonstrated that a BMI of >18kg/m2was one of the independent prognostic factors in105 patients treated with definitive chemoradiotherapy (P¼ .003). However, in this study, the cutpoint for BMIwas nontraditional and the sample size was small.
In the current study, 74.8% of EC patients had highBMI and had better OS and DFS compared with thosewith normal/low BMI. However, high BMI, per se, wasnot found to be an independent prognosticator. Further
analyses of our data revealed a finding that has not yetbeen reported in the literature, namely that high BMI wasassociated with early baseline stage EC. Thus, the betterOS and DFS reported in the high BMI group is attributedto lower EC stage and high BMI does not appear to influ-ence the aggressiveness of established EC. Why wouldhigh BMI be associated with a diagnosis of early stage EC?An answer to this intriguing finding remains unclear. Wespeculate that because patients with high BMI are diag-nosed with GERD more often than those with low
Table 5. Patient Characteristics for Patients With �T2Adenocarcinoma
BMI<25 kg/m2
n532
BMI‡25 kg/m2
n583
P
Patient demographicsGender (M:F) 27:5 73:10 .758
Age, y .038
£60 8 (25.0%) 34 (41.0%)
61-70 9 (28.1%) 30 (36.1%)
>70 15 (46.9%) 19 (22.9%)
Weight loss in last 3 mo 17 (53.1%) 34 (41.0%) .239
Social historyAlcohol intake ‡4 oz/d 11 (34.4%) 27 (32.5%) .850
Smoker 23 (71.9%) 53 (63.9%) .416
ASA score 3-4 26 (81.3%) 67 (80.7%) .949
Past medical historyCongestive heart failure 1 (3.1%) 2 (2.4%) .628
COPD 3 (9.4%) 6 (7.2%) .481
Coronary artery disease 5 (15.6%) 17 (20.5%) .553
PVD 2 (6.3%) 5 (6.0%) .630
Diabetes 5 (15.6%) 14 (16.9%) .872
Tumor informationClinical stage .349
II 26 (81.3%) 67 (80.7%)
III 5 (15.6%) 16 (19.3%)
IV 1 (3.1%) 0
Pathological stage .762
I 5 (15.6%) 16 (19.3%)
II 14 (43.8%) 28 (33.7%)
III 10 (31.3%) 32 (38.6%)
IV 3 (9.4%) 7 (8.4%)
Location .519
Cervical/upper/middle 2 (6.3%) 7 (8.4%)
Lower/GEJ/gastric 30 (93.8%) 76 (91.6%)
Histological grade .148
Well 1 (3.1%) 4 (4.9%)
Moderately 17 (53.1%) 25 (30.5%)
Poorly 14 (43.8%) 51 (62.2%)
Undifferentiated 0 2 (2.4%)
BMI indicates body mass index; M:F, male:female; ASA, American Society
of Anesthesiologists; COPD, chronic obstructive pulmonary disease; PVD,
peripheral vascular disease; GEJ, gastroesophageal junction.
Table 6. Postoperative Complications and Outcome forPatients With �T2 Adenocarcinoma
BMI<25 kg/m2
n532
BMI‡25 kg/m2
n583
P
ComplicationPulmonary 15 (46.9%) 28 (33.7%) .192
Cardiovascular 7 (21.9%) 15 (18.1%) .642
GI events 1 (3.1%) 22 (26.5%) .005
Anastomotic leak 3 (9.4%) 9 (10.8%) .559
Wound/infection 6 (18.8%) 20 (24.1%) .539
Blood transfusion 6 (18.8%) 12 (14.5%) .570
Outcome30-d mortality 1 (3.1%) 2 (2.4%) .628
Recurrence 13 (40.6%) 44 (53.0%) .234
Local/regional recurrence 6 (18.8%) 25 (30.1%) .218
Distant recurrence 12 (37.5%) 39 (47.0%) .359
BMI indicates body mass index; GI, gastrointestinal.
Figure 3. Kaplan-Meier estimated overall survival probabilityis shown by a body mass index (BMI) �25 kg/m2 versus aBMI <25 kg/m2 in patients with clinical T2 and higher adeno-carcinoma. Results of the log-rank test indicated that therewas no significant difference in overall survival between the 2groups (P ¼ .882).
Original Article
5624 Cancer December 15, 2010
BMI,19-23 patients with high BMI are more likely toundergo endoscopic surveillance and this could result inthe diagnosis of early EC. Lagergren et al11 reported anodds ratio of 7.7 for EAC among patients with GERDsymptoms compared with individuals without GERDsymptoms. The hypothesis that high BMI patients tend tohave GERD, which is associated with EAC, is compatiblewith our results. In our cohort of patients with high BMI,EAC and lower esophageal localization were significantlymore frequent than for patients with low BMI, who had alower frequency of EAC and tended not have to primary
tumors in the lower esophagus (P < .001 and P ¼ .021,respectively).
We found that the patients with normal/low BMIwere more likely to have an advanced stage (stage II-IV) ofEC (P¼ .001). Greater than half of the patients with highBMI (56.9%) were diagnosed with clinical stage 0 or I dis-ease, whereas 35.6% of patients with normal/low BMIhad an early clinical stage of disease at diagnosis. One ex-planation for this trend could be that the patients withadvanced disease have low appetite and/or significant dys-phagia (and weight loss). In the current study cohort,44.7% of patients with normal/low BMI had lost weightin the 3 months before surgery whereas only 22.2% ofpatients with high BMI lost weight (P< .001). Our otherfinding with regard to weight loss, which correlates with ahigher tumor burden, as a poor prognosticator is consist-ent with previously published literature.
High BMI was considered to be a risk factor for sur-gical complications such as cardiac insufficiency, respira-tory failure, anastomotic leak, and wound dehiscence.However, we were not able to confirm these findings andour findings are similar to more recent reports.24,25 Wedid observe more gastrointestinal complications inpatients with high BMI (P ¼ .016) compared with thosewith low BMI. These findings need confirmation and thereason for this observation is not clear.
The current study included patients with both EACand SCC but EAC was diagnosed in approximately93.8% of patients with high BMI and 72.4% of patientswith normal/low BMI (P< .001). Our study could be bi-ased because patients with EAC have been reported tohave a better prognosis than those with SCC.26,27
Holscher et al26 and Meltzer27 have reported that SCCinvades the submucosa and lymph nodes at an early stage
Table 7. Univariable Analysis of Factors Related to Survivalfor Patients With �T2 Adenocarcinoma (Cox RegressionAnalysis)
P HazardRatio
95% CI
Patient demographicsFemale gender .734 1.116 0.592-2.104
Age .916 0.999 0.978-1.020
BMI ‡25 kg/m2 .882 0.965 0.606-1.538
Weight loss in last 3 mo .001 2.109 1.364-3.260
Social historyAlcohol intake ‡4 oz/d .337 0.803 0.513-1.257
Smoker .388 1.228 0.770-1.958
ASA score 3-4 .960 1.014 0.588-1.747
Past medical historyCongenital heart failure .434 1.585 0.500-5.026
COPD .642 1.189 0.573-2.466
PVD .363 1.472 0.640-3.387
Tumor informationClinical stage .082
II 1.000
III .048 1.683 1.006-2.817
IV .242 3.286 0.447-24.151
Type of surgery .508
Ivor-Lewis esophagectomy 1.000
Transhiatal esophagectomy .654 1.109 0.705-1.747
Total esophagectomy .120 1.741 0.865-3.506
Minimally invasive
esophagectomy
.409 0.433 0.059-3.159
Tumor diameter >3 cm <.001 3.663 2.151-6.237
Pathological stage <.001
I 1.000
II .071 2.003 0.943-4.257
III <.001 7.561 3.526-16.214
IV .007 3.699 1.425-9.605
Tumor location
(lower/GEJ/gastric)
.116 0.555 0.267-1.155
Histological grade: poorly .007 1.869 1.190-2.935
No. of dissected lymph nodes .082 0.980 0.958-1.003
No. of positive lymph nodes <.001 1.069 1.033-1.106
95% CI indicates 95% confidence interval; BMI, body mass index; ASA,
American Society of Anesthesiologists; COPD, chronic obstructive pulmo-
nary disease; PVD, peripheral vascular disease; GEJ, gastroesophageal
junction.
Table 8. Multivariable Analysis of Factors Related toSurvival for Patients With �T2 Adenocarcinoma(Cox Regression Analysis)
P HazardRatio
95% CI
Pathological stage <.001
I 1.000
II .055 2.132 0.984-4.617
III <.001 5.480 2.415-12.433
IV .105 2.429 0.831-7.100
Tumor location (lower/GEJ/gastric) .062 0.466 0.209-1.041
Histological grade: poorly .094 1.525 0.931-2.499
No. of dissected lymph nodes .003 0.955 0.927-0.984
No. of positive lymph nodes .029 1.072 1.007-1.141
95% CI indicates 95% confidence interval; GEJ, gastroesophageal
junction.
Weight and Esophageal Cancer Outcome/Hayashi et al
Cancer December 15, 2010 5625

and the 5-year OS rate of patients with stage I disease whoundergo surgery was 82.5% in patients with EAC and59.2% in patients with SCC. However, this finding is notgeneralizable and further studies are warranted.
There are weaknesses to the current study: 1) it is aretrospective review; 2) we included a relatively smallnumber of patients; 3) we cannot explain why patientswith high BMI had earlier stage EC at diagnosis; and 4)some of our findings are not consistent with the literature.The strengths of the current study are 1) a homogeneousstudy population (surgery only as therapy and no adjunc-tive therapy received); 2) detailed analysis is provided; 3)many findings are consistent with the literature; and 4) ithas novel findings.
BMI was not an found to be an independent prog-nostic factor, but it was associated with a lower baselinestage of EAC. It appears that BMI itself has no influenceon the clinical aggressiveness of EC and in the currentanalyses; it was found to have no adverse influence withregard to surgical complications as a whole. The incidenceof GERD and EAC is high in patients with high BMI andour novel findings present an opportunity for detectingEAC at an early stage if patients with high BMI can be sur-veyed more aggressively.
In conclusion, high BMI is common in patientswith EC and patients with high BMI are diagnosed withearly stage EC and therefore tend to have better survivalthan those with low/normal BMI.
CONFLICT OF INTEREST DISCLOSURESSupported in part by grants from The University of Texas M.D. Anderson Cancer Center; the Dallas, Park, Cantu, Smith,and Myers families; and the River Creek Foundation. Alsosupported by National Cancer Institute (NCI) GrantsRO1CA138671, R21CA127672, and R21CA129906. Tissuesfrom some patients presented in this article were used to gener-ate preliminary data for the above NCI grants.
REFERENCES
1. Ogden CL, Carroll MD, Curtin LR, McDowell MA, TabakCJ, Flegal KM. Prevalence of overweight and obesity in theUnited States, 1999-2004. JAMA. 2006;295:1549-1555.
2. Calle EE, Rodriguez C, Walker-Thurmond K, Thun MJ.Overweight, obesity, and mortality from cancer in a pro-spectively studied cohort of U.S. adults. N Engl J Med.2003;348:1625-1638.
3. Barrett SV, Paul J, Hay A, Vasey PA, Kaye SB, GlasspoolRM. Does body mass index affect progression-free or overallsurvival in patients with ovarian cancer? Results from SCO-TROC I trial. Ann Oncol. 2008;19:898-902.
4. Matthews KS, Straughn JM Jr, Kemper MK, Hoskins KE,Wang W, Rocconi RP. The effect of obesity on survival in
patients with ovarian cancer. Gynecol Oncol. 2009;112:389-393.
5. Meyerhardt JA, Niedzwiecki D, Hollis D, et al. Impact ofbody mass index and weight change after treatment on can-cer recurrence and survival in patients with stage III coloncancer: findings from Cancer and Leukemia Group B89803. J Clin Oncol. 2008;26:4109-4115.
6. Siddiqui SA, Inman BA, Sengupta S, et al. Obesity and sur-vival after radical prostatectomy: a 10-year prospectivecohort study. Cancer. 2006;107:521-529.
7. Jemal A, Siegel R, Ward E, Hao Y, Xu J, Thun MJ. Cancerstatistics, 2009. CA Cancer J Clin. 2009;59:225-249.
8. Brown LM, Devesa SS, Chow WH. Incidence of adenocar-cinoma of the esophagus among white Americans by sex,stage, and age. J Natl Cancer Inst. 2008;100:1184-1187.
9. Hampel H, Abraham NS, El-Serag HB. Meta-analysis: obe-sity and the risk for gastroesophageal reflux disease and itscomplications. Ann Intern Med. 2005;143:199-211.
10. MacDonald WC, MacDonald JB. Adenocarcinoma of theesophagus and/or gastric cardia. Cancer. 1987;60:1094-1098.
11. Lagergren J, Bergstrom R, Nyren O. Association betweenbody mass and adenocarcinoma of the esophagus and gastriccardia. Ann Intern Med. 1999;130:883-890.
12. Morgan MA, Lewis WG, Hopper AN, et al. Prognostic sig-nificance of body mass indices for patients undergoingesophagectomy for cancer. Dis Esophagus. 2007;20:29-35.
13. Skipworth J, Foster J, Raptis D, Hughes F. The effect ofpreoperative weight loss and body mass index on postopera-tive outcome in patients with esophagogastric carcinoma.Dis Esophagus. 2009;22:559-563.
14. Healy LA, Ryan AM, Gopinath B, Rowley S, Byrne PJ,Reynolds JV. Impact of obesity on outcomes in the manage-ment of localized adenocarcinoma of the esophagus andesophagogastric junction. J Thorac Cardiovasc Surg.2007;134:1284-1291.
15. Fujitani K, Ajani JA, Crane CH, et al. Impact of inductionchemotherapy and preoperative chemoradiotherapy on oper-ative morbidity and mortality in patients with locoregionaladenocarcinoma of the stomach or gastroesophageal junc-tion. Ann Surg Oncol. 2007;14:2010-2017.
16. Greene FL, ed. AJCC Cancer Staging Atlas/American JointCommittee on Cancer. New York, NY: Springer; 2006.
17. Trivers KF, De Roos AJ, Gammon MD, et al. Demo-graphic and lifestyle predictors of survival in patients withesophageal or gastric cancers. Clin Gastroenterol Hepatol.2005;3:225-230.
18. Di Fiore F, Lecleire S, Pop D, et al. Baseline nutritional sta-tus is predictive of response to treatment and survival inpatients treated by definitive chemoradiotherapy for a locallyadvanced esophageal cancer. Am J Gastroenterol.2007;102:2557-2563.
19. Ayazi S, Hagen JA, Chan LS, et al. Obesity and gastro-esophageal reflux: quantifying the association between bodymass index, esophageal acid exposure, and lower esophagealsphincter status in a large series of patients with refluxsymptoms. J Gastrointest Surg. 2009;13:1440-1447.
20. Friedenberg FK, Xanthopoulos M, Foster GD, Richter JE.The association between gastroesophageal reflux disease andobesity. Am J Gastroenterol. 2008;103:2111-2122.
21. Bytzer P, Christensen PB, Damkier P, Vinding K, Seer-sholm N. Adenocarcinoma of the esophagus and Barrett’sesophagus: a population-based study. Am J Gastroenterol.1999;94:86-91.
Original Article
5626 Cancer December 15, 2010

22. Lagergren J, Bergstrom R, Lindgren A, Nyren O. Sympto-matic gastroesophageal reflux as a risk factor for esophagealadenocarcinoma. N Engl J Med. 1999;340:825-831.
23. Ye W, Chow WH, Lagergren J, Yin L, Nyren O. Risk ofadenocarcinomas of the esophagus and gastric cardia inpatients with gastroesophageal reflux diseases and after anti-reflux surgery. Gastroenterology. 2001;121:1286-1293.
24. Kilic A, Schuchert MJ, Pennathur A, et al. Impact of obe-sity on perioperative outcomes of minimally invasive esopha-gectomy. Ann Thorac Surg. 2009;87:412-415.
25. Mullen JT, Davenport DL, Hutter MM, et al. Impact ofbody mass index on perioperative outcomes in patientsundergoing major intra-abdominal cancer surgery. Ann SurgOncol. 2008;15:2164-2172.
26. Holscher AH, Bollschweiler E, Schneider PM, Siewert JR.Prognosis of early esophageal cancer. Comparison betweenadeno- and squamous cell carcinoma. Cancer. 1995;76:178-186.
27. Meltzer SJ. The molecular biology of esophageal carcinoma.Recent Results Cancer Res. 1996;142:1-8.
Weight and Esophageal Cancer Outcome/Hayashi et al
Cancer December 15, 2010 5627