The impact of fluid therapy on microcirculation and tissue oxygenation in hypovolemic patients: a...
11
Joachim Boldt Can Ince The impact of fluid therapy on microcirculation and tissue oxygenation in hypovolemic patients: a review Received: 21 October 2009 Accepted: 7 March 2010 Published online: 26 May 2010 Ó Copyright jointly held by Springer and ESICM 2010 J. Boldt ( ) ) Department of Anesthesiology and Intensive Care Medicine, Klinikum der Stadt Ludwigshafen, Bremserstr. 79, 67063 Ludwigshafen, Germany e-mail: [email protected] Fax: ?49-621-5033024 C. Ince Department of Intensive Care, Erasmus MC University Hospital Rotterdam, Rotterdam, The Netherlands Abstract Purpose: An optimal volume replacement strategy aims to restore systemic hemodynamics with the ultimate goals of improving organ perfusion and microcirculation for sustaining adequate tissue oxygena- tion. This review presents the (patho)physiological basis of hypo- volemia, microcirculation, and tissue oxygenation and presents a literature review on the effects of plasma substitutes on microperfusion and oxygenation in the clinical setting. Methods: Literature review of the effects of fluid therapy on micro- circulation and tissue oxygenation using PubMed search including ori- ginal papers in English from 1988 to 2009. Results: We identified a total of 14 articles dealing with the effects of different crystalloids and colloids on organ perfusion, microcirculation, and tissue oxygenation in patients. The results are divergent, but there is a general trend that colloids are superior to crystalloids in improving organ perfusion, microcirculation, and tissue oxygenation. Due to the limited number of studies and different study conditions, a meta- analysis on the effects of the volume replacement strategies on micro- circulation is not possible. Conclusions: Improving the micro- circulation by volume replacement appears to be a promising issue when treating the critically ill. The growing insights from animal experiments have to be translated into the clinical setting to identify the optimal fluid regimen for correcting hypovolemia. New techniques for monitoring microcirculation at the bedside might provide such endpoints, although these have to be validated also in the clinical setting. Whether improved microperfusion and tissue oxygena- tion by fluid therapy will also improve patient outcomes will have to be proven by future studies. Keywords Volume replacement Á Crystalloids Á Albumin Á Gelatins Á Hydroxyethyl starch Á Microcirculation Á Tissue oxygenation Á Patients Introduction Circulating volume and microcirculatory deficits may occur in the surgical, trauma, burn, and intensive care patient. While bleeding causes absolute volume deficits, vasodilation mediated by vasoactive substances produces relative volume deficits. Hypovolemia may also develop in the absence of obvious fluid loss secondary to gen- eralized impairment of the endothelial barrier caused by inflammation resulting in capillary leakage and fluid shift from the intravascular to the interstitial space. Restoration of intravascular volume can be regarded as a cornerstone of therapy in the critically ill. Diagnosis, choice of fluids, and identification of hemodynamic targets, however, Intensive Care Med (2010) 36:1299–1308 DOI 10.1007/s00134-010-1912-7 REVIEW
-
Upload
fitrani-dwina -
Category
Documents
-
view
9 -
download
2
description
Intensive Care Med (2010)Penulis : Joachim Boldt Can Ince
Transcript of The impact of fluid therapy on microcirculation and tissue oxygenation in hypovolemic patients: a...
-
Joachim BoldtCan Ince
The impact of fluid therapy on microcirculationand tissue oxygenation in hypovolemicpatients: a review
Received: 21 October 2009Accepted: 7 March 2010Published online: 26 May 2010 Copyright jointly held by Springer andESICM 2010
J. Boldt ())Department of Anesthesiologyand Intensive Care Medicine,Klinikum der Stadt Ludwigshafen,Bremserstr. 79, 67063 Ludwigshafen,Germanye-mail: [email protected]: ?49-621-5033024
C. InceDepartment of Intensive Care,Erasmus MC University HospitalRotterdam, Rotterdam, The Netherlands
Abstract Purpose: An optimalvolume replacement strategy aims torestore systemic hemodynamics withthe ultimate goals of improving organperfusion and microcirculation forsustaining adequate tissue oxygena-tion. This review presents the(patho)physiological basis of hypo-volemia, microcirculation, and tissueoxygenation and presents a literaturereview on the effects of plasmasubstitutes on microperfusion andoxygenation in the clinical setting.Methods: Literature review of theeffects of fluid therapy on micro-circulation and tissue oxygenationusing PubMed search including ori-ginal papers in English from 1988 to2009. Results: We identified a totalof 14 articles dealing with the effectsof different crystalloids and colloidson organ perfusion, microcirculation,and tissue oxygenation in patients.The results are divergent, but there isa general trend that colloids aresuperior to crystalloids in improvingorgan perfusion, microcirculation,and tissue oxygenation. Due to thelimited number of studies and
different study conditions, a meta-analysis on the effects of the volumereplacement strategies on micro-circulation is not possible.Conclusions: Improving the micro-circulation by volume replacementappears to be a promising issue whentreating the critically ill. The growinginsights from animal experimentshave to be translated into the clinicalsetting to identify the optimal fluidregimen for correcting hypovolemia.New techniques for monitoringmicrocirculation at the bedside mightprovide such endpoints, althoughthese have to be validated also in theclinical setting. Whether improvedmicroperfusion and tissue oxygena-tion by fluid therapy will alsoimprove patient outcomes will haveto be proven by future studies.
Keywords Volume replacement Crystalloids Albumin Gelatins Hydroxyethyl starch Microcirculation Tissueoxygenation Patients
Introduction
Circulating volume and microcirculatory deficits mayoccur in the surgical, trauma, burn, and intensive carepatient. While bleeding causes absolute volume deficits,vasodilation mediated by vasoactive substances producesrelative volume deficits. Hypovolemia may also develop
in the absence of obvious fluid loss secondary to gen-eralized impairment of the endothelial barrier caused byinflammation resulting in capillary leakage and fluid shiftfrom the intravascular to the interstitial space. Restorationof intravascular volume can be regarded as a cornerstoneof therapy in the critically ill. Diagnosis, choice of fluids,and identification of hemodynamic targets, however,
Intensive Care Med (2010) 36:12991308DOI 10.1007/s00134-010-1912-7 REVIEW
-
remain controversial. One of the reasons for this uncer-tainty is that fluid resuscitation has traditionally beentargeted to correct macrocirculation, whereas the physi-ological impact of fluids at the microcirculatory level isstill unclear. Uncorrected microcirculatory alterationsresult in inadequate oxygen transport to achieve sufficientoxidative phosphorylation and, ultimately, cause tissuedamage and organ dysfunction [14]. The primary aim ofoptimal fluid resuscitation should be to achieve adequateperfusion without compromising oxygen transport byexcessive hemodilution. It still remains unclear whetherthis can be achieved by correction of hypovolemia itselfor whether the kind of volume replacement is alsoof importance. The ideal volume replacement strategyshould correct hypovolemia and restorate systemichemodynamics, but also improve microcirculatoryperfusion and tissue oxygenation [5, 6].
The purpose of this review is to consider the currentinsights into the effects of fluid therapy on microcircu-lation and oxygen transport to the parenchymal cells.A review of the literature will be given with regard to theeffects of commonly used plasma substitutes on organperfusion, microcirculation, and tissue oxygenation in theclinical setting.
Pathophysiology of the hypovolemic microcirculation
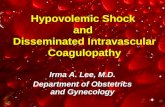
Hypovolemia leads to inadequate perfusion of themicrocirculation resulting in insufficient oxygen avail-ability to meet the needs of mitochondrial oxidativephosphorylation [2, 7]. Weil and Shubin [8] in theirkeynote paper classified the different types of shockinto four main categories: hypovolemic, cardiogenic,obstructive, and distributive shock (Fig. 1, 2). Hypovo-lemic shock can be described as the condition wherebythere is a decrease in circulating volume. Cardiogenicshock occurs where there is a loss of cardiac contractilitywith elevation of diastolic filling pressure and volume.Obstructive shock can occur as a result of massive pul-monary embolism, tension pneumothorax, or pericardialtamponade where there is a physical obstruction in thecirculation resulting in impaired diastolic filling andincreased afterload. Distributive shock involves a defectin the (micro)vascular distribution of a normal or even ofa supranormal cardiac output resulting in inadequateregional oxygen delivery. Hypovolemia induced by dis-tributive shock is highly heterogeneous and targets themicrocirculation. Its detection by measuring systemichemodynamics is complicated by shunting of the micro-circulation resulting in microcirculatory alterations andhypoxia with normal systemic hemodynamics and oxy-gen-derived variables [9]. Distributive shock especiallyoccurs under conditions of inflammation and infectionsuch as in sepsis and reperfusion injury. Inflammatory
mediators and hypoxemia result in abnormal blood flowdistributions and shunting leading to a mismatch betweenoxygen delivery and oxygen need by the parenchymalcells, and thus heterogeneous hypoxemia, and organdysfunction [9, 10].
Distributive shock provides the biggest challenge withregard to identifying endpoints for assessing an adequatefluid replacement [11]. Currently these endpoints areaimed at correcting changes in systemic hemodynamics.Fluid resuscitation can cause an apparent improvement insystemic circulation while leaving regional and micro-circulatory oxygenation and perfusion underresuscitated.In animal investigations it has been shown that fluidresuscitation improved organ blood flow of the gut andkidneys, while leaving other areas hypoxemic [12]. Thisis important in the light of recent clinical studies usingnew techniques for monitoring microcirculation, whichhave shown the persistence of microcirculatory underre-suscitation in the presence of normalized systemichemodynamic variables and association with adverseclinical outcome [5, 1315].
Adequate microcirculation relies on the function of thedifferent components of the microcirculation. Red andwhite blood cells, endothelial cells, and smooth musclecells have to function in close harmony to guaranteeadequate microcirculatory blood flow to transport oxygento the tissues. The function of each of these cellularand subcellular systems is affected by hypovolemia.
Fig. 1 The classification of shock according to Weil and Shubin[8]. I Normal conditions. II Cardiogenic shock, related to cardiacpump failure resulting from loss of the pump function of the heart.III Hypovolemic shock as a result of decreased circulating volumefrom, for example, hemorrhage. IV Obstructive shock as result ofan obstruction in the cardiovascular circuit as a result of, forexample, massive pulmonary embolism, tension pneumothorax, orpericardial tamponade. V Distributive shock where vasculardysfunction is unable to distribute a normal or even high cardiacoutput, resulting in underperfused microcirculatory areas beingshunted by well perfused areas
1300
-
Deleterious effects on the microcirculation include dys-function of endothelial signal transductory pathwaysby inflammatory mediators and reactive oxygen spe-cies, deterioration of endothelial barrier function (e.g.,glycocalyx), alterations in red blood cell function(deformability, aggregability), and increased leukocyteadhesion and activation [6, 9]. Any one of these altera-tions either alone or acting together can lead to a loss offunctional capillary density resulting in heterogeneousabnormalities in the distribution of blood to the micro-circulatory network, enhanced oxygen diffusion distancesfrom the perfused intracapillary lumens to the tissue cell,tissue hypoxemia, and finally organ dysfunction.
Administration of fluids to correct hypovolemia maymodulate microcirculatory function by various mecha-nisms. The most important is increasing flow by enhancedfilling of the vasculature, thus generating forcing pressurepromoting microcirculatory perfusion. Fluids also modifythe hemorheology of blood by decreasing viscosity, whichadditionally promotes blood flow. There are differenteffects of fluids on blood viscosity depending on thecomposition of the fluid; the microcirculation can be eitherimproved or impaired by these effects [16]. Excessivehemodilution can cause shunting of the microcirculationand impair regional tissue oxygenation [14]. This effectcan differ among the different organ systems [12].
Acid-base balance has been shown to be influenced bythe administration of fluids [17]. Alterations in acid-basestatus can cause deleterious effects on organ function(e.g., kidney function [18]). Saline solution appears tohave the most negative effect on the (micro)circulation
[19]. Infusion of large amounts of saline results inincreased plasma chloride concentration and causes areduction in the strong ion difference, which in turnproduces an increase in free hydrogen ions [20]. Thiseffect can be avoided when using more plasma-adapted(balanced) crystalloids [21].
Release of inflammatory mediators secondary tohypovolemia is another important factor contributing tomicrocirculatory dysfunction. The volume replacementstrategy can modulate inflammatory activation, genera-tion of reactive oxygen, and leukocyte adhesion to themicrocirculatory endothelium [22]. Saline solutionappears to be the most pro-inflammatory fluid, whereascertain colloids (especially when dissolved in a balancedsolution) may be more beneficial in controlling theinflammatory process [2325]. Studies using intravitalmicroscopy have shown this to be the case by imaging theeffects of different fluids on leukocyte adherence on organmicrovascular surfaces [26, 27]. In this context colloidsshowed more beneficial effects on the microcirculationthan saline resuscitation in a variety of experimentalmodels using direct observation of leukocyte endothelialinteraction [27, 28]. The use of crystalloids as volumereplacement has been shown to impair microcirculationand to cause vascular leakage resulting in fluid shift to theinterstitial space [29, 30]. The negative effects on oxygentransport pathways occur as a result of increased diffusionpath length and poor oxygen solubility in aqueous solu-tions causing reduced oxygen availability and impairedcellular respiration.
The glycocalyx is a gel-like structure that forms theinterface between the intracapillary lumen and the endo-thelial cells, and its integrity is highly sensitive tooxidative stress [31]. It is likely that endothelial dys-function and microcirculatory deterioration resulting fromhypovolemia and reperfusion injury are caused by a lossof the endothelial glycocalyx [32]. Depletion of thisbarrier results in leukocyte adhesions and loss of theendothelial barrier function [33, 34]. This in turn resultsin alterations of the Starling forces promoting tissueedema. The loss of this important supracellular compart-ment of the microcirculation may form an importantrationale for using colloids [32]. Of the colloids, starcheshave been shown to protect the glycocalyx barrier [35]. Itis expected that modifications of the molecular andpharmacological properties of colloids as well as of thesolvent may provide additional protection of the glyco-calyx and thereby of the microcirculation.
How can the effects of volume replacementbe monitored?
Currently, endpoints of volume replacement are aimed atcorrecting changes in systemic hemodynamic variables.
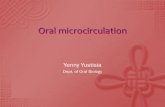
Fig. 2 The impact of fluid therapy on the microcirculation. Fluidadministration is the therapy of choice following shock. Theamount and/or composition of the fluids, however, can either havebeneficial or deleterious effects on the microcirculation
1301
-
These include giving volume challenges either byadministering a fluid bolus or by autotransfusion bypassive leg raising resulting in changes in systemichemodynamic variables such as stroke volume or venouspressure [11]. Fluid resuscitation can cause an apparentimprovement in systemic circulation while leavingregional and microcirculatory oxygenation and perfusionuncorrected [12]. New techniques have been introduced atthe bedside aimed at monitoring various aspects of themicrocirculation and tissue oxygenation. These have beenapplied to various areas of the body, and various param-eters related to microcirculatory function and tissueoxygenation have been measured. At present, no unifyingmonitoring technique exists that measures all aspects ofmicrocirculatory function in an integrated fashion, andeach technique has its limitations in this respect. It isworth noting that in fact all hemodynamic monitoringmodalities suffer from this drawback and that no singletechnique can be used to measure the integrative functionof the cardiovascular system to achieve hemodynamichomeostasis from lung to mitochondria. Thus eachmicrocirculatory monitoring technique should be inter-preted for its sensitivity and specificity in identifying aparticular physiological component and its ability topredict impending adverse events. It has to be emphasizedthat these microcirculatory monitoring techniques are atan early stage of development and have to be validated forguiding volume therapy in the clinical setting. Currentlyused bedside monitoring techniques for assessing theinfluence of volume therapy on microcirculation aredescribed below.
Laser Doppler flowmetry (LDF) is used for nonquan-titative assessment of blood flow and has been appliedmainly to the cutaneous microcirculation [36].
Tissue CO2 can be measured using gastric CO2tonometers or by tissue CO2 electrodes [37]. Thesemeasurements have been mostly applied either in thestomach or intestines or sublingually and are assumed tobe a measure of the adequacy of microcirculatory perfu-sion [3642]. In early studies such CO2 measurementsand arterial bicarbonate were entered into the Henderson-Hasselbalch equation to obtain intestinal mucosal pH(pHi). This calculation was later abandoned and insteadtissue-to-arterial gradient (pCO2 gap) was used.
A more direct method of evaluating microcirculatoryperfusion is by direct imaging of the microcirculationusing the recently introduced orthogonal polarizingspectrum (OPS) or sidestream dark field (SDF) imaging[43, 44]. These are optical techniques that are incorpo-rated into hand-held microscopes for direct visualobservation of the microcirculation on mucosal organsurfaces. In the perioperative setting these techniqueshave mainly been applied to study the sublingualmicrocirculation.
Tissue oxygenation has classically been measured byuse of Clark electrodes [45] although more modern
versions of such electrodes use solid state or oxygen-dependent fluorescence quenching methods. These elec-trodes are applied either trans- or subcutaneously, or asneedles that can be inserted into muscle tissue.
An alternative method to gain information about mi-crocirculatory oxygen availability is the use of theoxygen-dependent optical properties of microcirculatoryHb, which can be monitored using near infrared spec-troscopy (NIRS) [46]. This technique has been applied inthe thenar, calf, and forearm, and on the forehead.
A more comprehensive presentation of these tech-niques will be provided in another review paper to bepublished in Intensive Care Medicine as part of thiscurrent series dedicated to microcirculation.
Clinical studies on the effects of fluid therapyon microcirculation and tissue oxygenation
A PubMed analysis was carried out to investigate theliterature on the effects of fluids on the microcirculationand tissue oxygenation in the clinical setting. We includedall original studies published in English from 1988 to2009 and only studies in patients (no volunteer studies)were included (Table 1). Keywords for the search inclu-ded [microcirculation], [microperfusion] [tissue bloodflow] [organ perfusion] [tissue oxygenation] in connectionwith [hypovolemia], [volume therapy/replacement], [fluidtherapy/replacement], [crystalloids], [Ringers lactate],[saline solution], [normal saline], [(human) albumin],[gelatin(s)], [dextran(s)], [hydroxyethyl starch, HES], and[hypertonic solution]. Articles were only included whenthe methods for assessing organ perfusion, microcircula-tion, and tissue oxygenation were given. Obviously wemay have missed several ongoing studies and indeedseveral are currently under review, but nevertheless wefeel this overview gives a comprehensive review of thestate of the current art.
Crystalloids
In two prospective, randomized studies in patientsundergoing abdominal aortic and gynecologic surgery,the influence of Ringers lactate (RL) for intraoperativevolume replacement on gastric mucosal perfusion wasassessed by measuring gastric intramucosal pH (pHi) bytonometry [47, 48]. In one study, RL did not improvegastric mucosal perfusion [47], while in the other one RLalso increased gastric mucosal perfusion, but not nearly asmuch as HES 200/0.5 did [48]. In patients undergoingmajor abdominal surgery, volume replacement usingsaline solution resulted in decreased skeletal muscle tissuepO2 (ptiO2), whereas ptiO2 increased significantly in thepatients given HES 130/0.4 in saline [49]. This difference
1302
-
Table 1 Effects of volume administration on organ perfusion, microcirculation, and tissue oxygenation
Reference(year)
Patients Design Fluids Model Method Main results
Boldt [52] (1991) Cardiacsurgery
Pros rand 6% HES 200/0.5vs. HHES vs. nofluids
To doublereduction inPCWP
LDF skin Both increased LDF;HHES showedsignificantly higherincrease in LDF thanHES 200/0.5
Mythen [53] (1995) Cardiacsurgery
Pros HES 200/0.5 nocontrol
To increase strokevolume
pHi tonometry HES significantlyincreased gastricmucosal perfusion
Boldt [51] (1996) Trauma andsepsis ICU
Pros rand 10% HES 200 vs.20% HA
Volumereplacement onICU
pHi tonometry Trauma patients: nodifferences in pHi;septic patients:decrease in pHiblunted only byHES, decrease inpHi by HA
Marik [47] (1997) Abdominalaorticsurgery
Pros rand RL vs. HES 450/0.7
Perioperativevolumereplacement
pHi tonometry Only HES improvedmicrovascular bloodflow, RL did not
Asfar [54] (2000) Sepsis Pros rand HES 200/0.62 vs.gelatin
Hemodynamicstabilization
pHi tonometry pHi remainedunchanged withHES and slightlyincreased withgelatin (from 7.27 to7.31)
Forrest [55] (2000) Sepsis Pros 10% HES 264/0.45 Keep PAOP[15 mmHg
pHi tonometry No correction ofabnormalintramucosal pCO2gap by HES
Lang [49] (2001) Abdominalsurgery
Pros rand Saline vs. HES130/0.4
Perioperativevolumereplacement(PCWP 1216 mmHg)
Microsensory pO2catheters
RL decreased (muscle)tissue oxygenation,whereas it wasincreased by use ofHES 130/0.4
Wilkes [59] (2001) Electivesurgeries
Pros randdouble-blinded
Balanced vs.unbalancedvolume therapyHES ? cryst
Hemodynamicstabilization(using algorithm)
Gastric pHitonometry
CO2 gap lower inunbalanced volumegroup indicatingimproved gastricmucosal perfusionwith balancedvolume replacementstrategy
Rittoo [56] (2002) Abdominalaorticsurgery
Pros rand Gelatin vs. HES200/0.62
Volume expansion pHi tonometry pHi lower with gelatinthan with HES 200/0.62; HES reducedsplanchnic perfusionsignificantly less
Guo [48] (2003) Gynecology Pros rand Rl vs. HES 200/0.5 Intraoperativevolumereplacement
pHi tonometry HES significantlyimproved splanchnicblood flow; RL wasnot as effective asHES
Arkilic [50] (2003) Colonresectionsurgery
Pros rand Crystalloids 8 vs.1618 mL kg-1
h-1
Perioperative fluidreplacement
Polarographicsubcutaneoustissue O2tension
Both regimensincreased tissueoxygenation; morefluids were better forimproving tissueoxygenation;differences were notseen by systemichemodynamicmonitoring
1303
-
was not identified by monitoring only systemic hemody-namics. Arkilic et al. [50] investigated the effects ofconservative (2,183 972 mL) versus aggressive(3,815 1,853 mL) unspecified crystalloid resuscitationin elective colon resection surgery and measured subcu-taneous oxygen tension using oxygen electrodes andcapillary blood flow by a thermal diffusion system. Theyfound that supplemental fluid administration increasedboth tissue oxygen tension and capillary blood flowshowing the most increase with the higher doses of fluids.The difference between conservative and aggressivecrystalloid resuscitation seen in the microcirculation wasnot identified by monitoring systemic hemodynamics.
Colloids
Human albumin (HA)
In one study in trauma intensive care unit (ICU) patients,volume replacement with HA given over 5 days toguarantee stable hemodynamics assessed with the help ofa pulmonary artery catheter (PAC) did not change normalgastric mucosal perfusion measured by tonometry(no changes in pHi). In septic patients, however, pHi wassignificantly decreased by HA administration despiteadequate correction of hypovolemia, suggesting ongoingperfusion abnormalities in this area by volume resusci-tation with HA [51].
Dextrans
No study in the clinical setting during the past 20 yearswas found showing the effects of dextrans on organ per-fusion, microcirculation, or tissue oxygenation in patients.
Hydroxethyl starch (HES)
Hydroxyethyl starch (HES) refers to a class of syntheticcolloid solutions that are modified natural polysac-charides, similar to glycogen. HES is derived fromamylopectin, a highly branched starch that is obtainedfrom waxy maize or potatoes. Polymerized D-glucoseunits are joined primarily by 1-4 linkages with occasional1-6 branching linkages. Substituting hydroxyethyl forhydroxyl groups results in highly increased solubility andretards hydrolysis of the compound by amylase, therebydelaying its breakdown and elimination from the blood.The hydroxyethyl groups are introduced mainly at carbonpositions C2, C3, and C6 of the anhydroglucose residues.The available HES preparations are characterized byconcentration (hypooncotic: 3%; isooncotic: 6%; hyper-oncotic: 10%), molar substitution (MS; low: \0.5;medium: 0.5; high: [0.5), the mean molecular weight[Mw, low-molecular weight (LMW)-HES: 70 kD;medium-molecular weight (MMW)-HES: 130264 kD;high-molecular weight (HMW)-HES: [450 kD], the ori-gin (potato-derived versus maize-derived HES), and thesolvent (balanced and unbalanced HES preparations).
Eleven studies using HES in the clinical setting wereidentified [47, 49, 5157]. Two studies in septic [54, 55]and one study in cardiac surgery patients [57] showedunchanged organ perfusion by HES. In all of these stud-ies, pHi (or pCO2 gap) was measured by tonometry toassess the influence of volume replacement therapy ongastric mucosal perfusion. Eight studies in patientsundergoing cardiac, vessel, trauma, or gynecologic sur-gery showed that HES improved organ perfusion or tissueoxygenation or that decrease in perfusion was blunted byadminstration of HES [4749, 5153, 56, 58]. In sixof them, gastric mucosal perfusion (pHi) was mea-sured using tonometry and administration of HES was
Table 1 continued
Reference(year)
Patients Design Fluids Model Method Main results
Hofman [57](2005)
Cardiacsurgery
Pros HES 200/0.5 nocontrol
Postoperative fluidload
pHi tonometry HES increased cardiacoutput, but notsplanchnic mucosalperfusion
Al-Rawi [62](2005)
SAHpatients
Observational 23.5% HS Observation CPP, PbO2, FV Significant increase inCPP, PbO2, and FVby 23.5% saline
Mahmood [58](2009)
Abdominalaorticsurgery
Pros rand Gelatin, HES 200/0.62, HES 130/0.4
Perioperativevolumeexpansion over24 h
pHi tonometry Least drop in pHi withHES 200/0.62; mostpronounced drop inpHi with gelatin
HES Hydroxyethylstarch, HA human albumin, pHi gastric intra-mucosal pHi, RL Ringers lactate, HS hypertonic saline, HHEShypertonic saline plus hydroxyethylstarch, pros prospective, randrandomized, LDF laser Doppler flow, PCWP pulmonary capillarywedge pressure, SAH subarachnoid hemorrhage (SAH), CPP
cerebral perfusion pressure, PbO2 brain tissue oxygen, FV middlecerebral artery flow velocity, PAOP pulmonary artery occlusionpressure, pHi gastric intramucosal pH, ICU intensive care unit,pCO2 gap arterial-to-intramucosal pCO2 difference, ANH acutenormovolemic hemodilution
1304
-
associated with significantly improved gastric mucosalperfusion [47, 48, 51, 53, 56, 58]. In one study in cardiacsurgery patients, LDF was used to measure skin micro-circulatory perfusion [52]. Microcirculatory blood flowshowed better skin perfusion with HES 200/0.5 than withother HES preparations (HES 70/0.5 and HES 450/0.7).That the type of HES preparation seems to be of impor-tance concerning modulation of the microcirculation hasalso been shown in a study of patients undergoingabdominal aortic surgery [58]. When using HES 200/0.62,pHi was significantly less decreased compared to HES130/0.4. In a study in patients undergoing major abdom-inal surgery, the influence of 6% HES 130/0.4 on tissuepO2 was compared to patients who received saline solu-tion for volume replacement [49]. Skeletal muscle tissuepO2 (ptiO2) was monitored for 24 h after surgery usingflexible minimally invasive microsensory pO2 catheters.Although systemic hemodynamics and systemic oxygen-ation data were similar in both groups, ptiO2 increasedsignificantly in the HES 130/0.4-treated patients (?59%),but decreased in the RL group (-23%).
Gelatins
Three studies were found that used gelatins for improvingorgan perfusion [54, 56, 58]. Gelatin was given forhemodynamic stabilization in patients suffering fromsepsis or undergoing aortic surgery and compared to useof HES. pHi was measured by tonometry to assess gastricmucosal perfusion. In the hypovolemic septic patients[54], use of gelatin very moderately increased pHi (from7.27 to 7.31) suggesting improved splanchnic perfusion.Of particular importance was also that no difference insystemic hemodynamic variables was found between thetwo volume replacement strategies, but only on gastrictonometry data. In two other studies from one researchgroup performed in patients undergoing abdominal aorticsurgery, either gelatin or HES (HES 200/0.62 or HES130/0.4) was administered for volume expansion [56, 58].HES 200/0.62-treated patients showed significantly lessreduced splanchnic perfusion than those administeredgelatin.
Plasma-adapted versus non-plasma-adapted volumereplacement strategy
In a prospective, randomized, blinded trial in elderlysurgical patients, either a plasma-adapted (balanced)intraoperative fluid regimen consisting of Hartmannssolution and 6% HES preparation dissolved in a balancedelectrolyte solution (Hextend) or a nonplasma-adapted(unbalanced) regimen consisting of 0.9% sodiumchloride solution and 6% HES dissolved in 0.9%sodium chloride solution was given to guarantee stable
hemodynamics using a specific algorithm [59]. Similaramounts of HES (approximately 2,500 mL) and crystal-loids (approximately 1,500 mL) were given in bothgroups. Splanchnic perfusion was assessed by gastrictonometry. Systemic hemodynamics were without groupdifferences, while hyperchloremic acidosis was seen onlyin the non-plasma-adapted volume group, and bettergastric mucosal perfusion was provided by the balancedvolume replacement strategy compared with saline-basedfluids.
Hypertonic solutions
Great enthusiasm has been expressed for hypertonicsaline (HS) or hypertonic/colloid solutions (HCS) in thetreatment of hypovolemic shock (small volume resus-citation). Hypertonic volume replacement has beenproposed to correct microcirculatory dysfunction associ-ated with hypovolemia and its subsequent inflammatoryeffect. HS has been shown to increase perfusion pressure,improve capillary flow distribution, and offer endothelialde-swelling effects [60, 61]. Because hemodynamiceffects of HS solutions are reported to be rather transient,HS is often mixed with colloids [hypertonic saline plushyperoncotic dextran (HSD) or hypertonic saline plushypertonic HES (HHES)].
In a study in cardiac surgery patients using HHES todouble low pulmonary capillary wedge pressure (PCWP),skin microcirculatory blood flow measured by LDF wassignificantly increased in comparison to HES 200/0.5[52]. In an observational study in patients with sub-arachnoid hemorrhage, Al-Rawi et al. [62] administeredextremely hypertonic saline solution (23.5%). A signifi-cant increase in cerebral perfusion pressure, brain tissueoxygenation, and middle cerebral artery flow velocity wasfound accompanied by a significant decrease in intracra-nial pressure. An improvement in cerebral metabolicstatus in terms of lactate-pyruvate ratio was also seenafter infusion of this extreme hypertonic solution.
Discussion
In recent years, microcirculation has gotten increasedattention in the treatment of the critically ill patient. Thisincludes the choice for the ideal volume replacementstrategy to improve microcirculation. Interestingly, wefound only 14 papers on this issue over the past 20 years.This dearth of information on the different volumereplacement strategies for organ perfusion, microcircula-tion, or tissue oxygenation is remarkable as there is anongoing controversy concerning the ideal plasma sub-stitute to correct hypovolemia. Due to the small numberof studies and the divergent study designs, we decided not
1305
-
to perform a meta-analysis or a systematic review. Theidentified studies differed markedly with regard to thestudy design: (1) Plasma substitutes were used underdifferent conditions, e.g., in trauma, sepsis, hemorrhage orsurgery. (2) The amount of fluids that was administereddiffered widely among the studies making it difficult todistinguish between what effect is attributed to volumecorrection/expansion alone and what effect is specific fora certain plasma substitute. (3) Duration of volumeadministration differed; cases of single-shot versuscontinuous administration over hours were compared. (4)The endpoint of volume administration was not uniformlydefined. Mostly fixed amounts of volume were given.A goal-directed volume replacement strategy, how-ever, is a better approach than infusing a fixed amount ofvolume. (5) Although it is clear that measurement ofsystemic hemodynamic variables has limited sensitivityfor identifying hemodynamic alterations associated withshock and resuscitation, most of the techniques used forassessing microcirculation are still at the stage of devel-opment and not yet ready for routine clinical use.
Looking at the results of the 14 identified studies, thereappears to be a trend that colloids are more effective inbeneficially modifying organ perfusion and microcircu-lation than crystalloids. One important objection to theresults of these studies is that most of them used gastrictonometry to assess the effects of volume replacement onperfusiona surrogate marker of splanchnic perfusionwhose validity has often been doubted.
There is an urgent need for more information on theeffect of fluids on microcirculation as there is a currenttrend to keep the patients more on the dry side byrestricting volume administration. From the pathophysi-ological point of view, use of vasopressors in anhypovolemic patient to keep up blood pressure mayinitiate a fatal process on the microperfusion level withdetrimental sequel for organ function and even for thepatients outcome. It has been demonstrated that the useof vasopressors has no effect on prompting microcircu-latory flow, emphasizing that a guarantee of adequatemicroperfusion may not be reached simply by maintain-ing or even increasing arterial blood pressure.
Whether the effects of a certain volume replacementstrategy on microcirculation can be translated into itseffects on patients outcome (survival) was beyond thescope of this review. Up to now it has not been shownthat, by the choice of a certain volume replacement reg-imen, someones life was rescued, although beneficialeffects on inflammation, microcirculation, and tissueoxygenation have been shown. This experience is similarto the introduction of new monitoring techniques, anti-biotics, feeding strategies, or renal replacement strategiesthat have been shown to improve certain aspects in themanagement of the critically ill without improving overallsurvival. Our actual approach in the treatment of thecritically ill aims to improve different parts in the mosaic
of pathophysiology of critical illness; improving micro-circulation may be one important part in this therapeuticpuzzle.
As the commonly used plasma substitutes differ withregard to their physico-chemical characteristics, they alsomay differ with regard to their effects on organ perfusion,microcirculation, or tissue oxygenation. Based on theinsights received from animal studies, questions that haveto be addressed in the clinical setting will include how thedifferent fluids affect the determinants of microcirculatoryfunction. Important issues will be the effects on capillaryflow and capillary recruitment in terms of functionalcapillary density, the extent of leukocyte endothelialinteraction and glycocalyx determination, release ofinflammatory mediators and reactive oxygen species, andfinally the effects of the various fluid types on tissueoxygenation. These effects have to be determined for thedifferent types of shock and will have to be related toorgan function and clinical outcome.
Conclusions
Although it is clear from our literature search that the datathat are needed to draw definite conclusions concerningthe optimal fluid therapy and improvement in micro-circulatory perfusion are not yet available, we will drawsome careful conclusions from an evidence level Eperspective. These can be summarized as follows: (1) Arobust method or protocol for identifying hypovolemiaand guiding fluid resuscitation is yet being sought. (2)Although it is clear that fluid therapy should be effective incorrecting systemic hemodynamics, albeit based mainlyon experimental studies, it should also be successful incorrecting deficits in microperfusion and tissue oxygena-tion. (3) There is a need for bedside monitoring techniquesfor guiding fluid therapy integrating systemic, regional,microcirculatory, and oxygenation issues. (4) The choicebetween crystalloids and colloids is probably dependenton the patients condition and the cause of hypovolemia.(5) Compared to colloids, large amounts of crystalloids areneeded to achieve similar systemic and microcirculatoryendpoints leading to tissue edema and impaired tissueoxygenation. (6) It is expected that an optimal fluidcomposition for correction of hypovolemia may have toinclude additional components needed to support organperfusion, microcirculation, and tissue oxygenation.
We hope that with this paper we have set the scenefor important clinical investigations that will have to becarried out to find the optimal fluid composition andidentify the optimal (micro)hemodynamic targets forvolume resuscitation. We expect that protection of themicrocirculatory function will play an important role inthe future and will lead to improved treatment of thehypovolemic critically ill patient.
1306
-
Acknowledgments The authors gratefully acknowledge the talentsof Darryl Milstein who produced Figs. 1 and 2 in this paper. Thisstudy was supported only by an institutional grant.
Conflict of interest statement Boldt and his institution havereceived funding from B. Braun (Germany); Fresenius-Kabi
(Germany); Serumwerke Bernburg (Germany); Baxter (Europe).Ince holds a patent on SDF imaging, has stock in MicrovisionMedical, and has received educational grants from HutchinisonTechnology, Baxter, Novartis, and Eli Lilly.
References
1. Edouard AR, Degremont AC,Duranteau J, Pussard E, Berdeaux A,Samii K (1994) Heterogeneous regionalvascular responses to simulatedtransient hypovolemia in man. IntensiveCare Med 20:220414
2. Ince C (2004) Microcirculation indistress: a new resuscitation end point?Crit Care Med 32:19631964
3. Vollmar B, Menger MD (2004) Volumereplacement and microhemodynamicchanges in polytrauma. LangenbecksArch Surg 389:485491
4. Perret C, Feihl F (2000) Volumeexpansion during septic shock. BullAcad Natl Med 184:16211629
5. Sakr Y, Dubois MJ, De Backer D,Creteur J, Vincent JL (2004) Persistentmicrocirculatory alterations areassociated with organ failure and deathin patients with septic shock. Crit CareMed 32:18251831
6. Takala J, Jakob SM (2009) Sheddinglight on microcirculation. IntensiveCare Med 35:394396
7. Mythen MG, Salmon JB, Webb AR(1993) The rational administration ofcolloids. Blood Rev 7:223228
8. Weil MH, Shubin H (1971) Proposedreclassification of states of shock. AdvExp Med Biol 23:1323
9. Ince C (2005) The microcirculation isthe motor of sepsis. Crit Care9(Suppl 4):S13S19
10. De Backer D, Creteur J, Preiser JC,Dubois MJ, Vincent JL (2002)Microvascular blood flow is altered inpatients with sepsis. Am J Respir CritCare Med 166:98104
11. Vincent JL, Weil MH (2006) Fluidchallenge revisited. Crit Care Med34:13331337
12. Van Bommel J, Siegemund M, HennyCP, Ince C (2008) Heart, kidney, andintestine have different tolerances foranemia. Transl Res 151:110117
13. Trzeciak S, Dellinger RP, Parrillo JE,Guglielmi M, Bajaj J, Abate NL (2007)Early microcirculatory perfusionderangements in patients with severesepsis and septic shock: relationship tohemodynamics, oxygen transport, andsurvival. Ann Emerg Med 49:8898
14. Van Bommel J, Henny CP, TrouwborstA, Ince C (2001) Microvascularshunting in severe normovolemichemodilution. Anesthesiology 94:152160
15. Wang P, Hauptman JG, Chaudry IH(1990) Hemorrhage producesdepression in microvascular blood flowwhich persists despite fluidresuscitation. Circ Shock 32:307318
16. Ehrly AM, Landgraf H (1985) Influenceof intravenous infusions ofhydroxyethylstarch (HES) (MW 40,000and 450,000) on the blood flowproperties of healthy volunteers.Angiology 36:4144
17. Boldt J (2007) The balanced concept offluid resuscitation. Br J Anaesth99:312315
18. Powell-Tuck J, Gosling P, Lobo DN,Allison SP, Carlson GL, Gore M,Lewington AJ, Pearse RM, Mythen MG(2008) British consensus guidelines onintravenous fluid therapy for adultsurgical patients. http://www.bapen.org.uk/pdfs/bapen_pubs/giftasup.pdf
19. Kellum JA (2002) Fluid resuscitationand hyperchloremic acidosis inexperimental sepsis: improved short-term survival and acid-base balancewith Hextend compared with saline.Crit Care Med 30:300305
20. Scheingraber S, Rehm M, Sehmisch C,Finsterer U (1999) Rapid salineinfusion produces hyperchloremicacidosis in patients undergoinggynecologic surgery. Anesthesiology90:12651270
21. Boldt J (2008) Saline versus balancedhydroxyethyl starch: does it matter?Curr Opin Anaesthesiol 21:679683
22. Boldt J (2006) Do plasma substituteshave additional properties beyondcorrecting volume deficits? Shock25:103116
23. Kellum JA, Song M, Almasri E (2006)Hyperchloremic acidosis increasescirculating inflammatory molecules inexperimental sepsis. Chest 130:962967
24. Boldt J, Suttner S, Brosch C, LehmannA, Rohm K, Mengistu A (2009) Theinfluence of a balanced volumereplacement concept on inflammation,endothelial activation, and kidneyintegrity in elderly cardiac surgerypatients. Intensive Care Med 35:462470
25. Matharu NM, Butler LM, Rainger GE,Gosling P, Vohra RK, Nash GB (2008)Mechanisms of the anti-inflammatoryeffects of hydroxyethyl starchdemonstrated in a flow-based model ofneutrophil recruitment by endothelialcells. Crit Care Med 36:15361542
26. Kaplan SS, Park TS, Gonzales ER,Gidday JM (2000) Hydroxyethyl starchreduces leukocyte adherence andvascular injury in the newborn pigcerebral circulation after asphyxia.Stroke 31:22182223
27. Kupper S, Torge Mees S, Gassmann P,Brodde M, Kehrel B, Haier J (2007)Hydroxyethyl starch normalizes plateletand leukocyte adhesion withinpulmonary microcirculation duringLPS-induced endotoxemia. Shock28:300308
28. Inan N, Iltar S, Surer H, Yilmaz G,Alemdaroglu KB, Yazar MA, Basar H(2009) Effect of hydroxyethyl starch130/0.4 on ischaemia/reperfusion inrabbit skeletal muscle. Eur JAnaesthesiol 26:160165
29. Funk W, Baldinger V (1995)Microcirculatory perfusion duringvolume therapy. A comparative studyusing crystalloid or colloid in awakeanimals. Anesthesiology 82:975982
30. Hoffmann JN, Vollmar B, LaschkeMW, Inthorn D, Schildberg FW,Menger MD (2002) Hydroxyethylstarch (130 kD), but not crystalloidvolume support, improvesmicrocirculation during normotensiveendotoxemia. Anesthesiology 97:460470
31. Rubio-Gayosso I, Platts SH, Duling BR(2006) Reactive oxygen speciesmediate modification of glycocalyxduring ischemia-reperfusion injury. AmJ Physiol Heart Circ Physiol290:H2247H2256
1307
-
32. Chappell D, Jacob M, Hofmann-KieferK, Conzen P, Rehm M (2008) Arational approach to perioperative fluidmanagement. Anesthesiology 109:723740
33. Constantinescu AA, Vink H, Spaan JA(2003) Endothelial cell glycocalyxmodulates immobilization of leukocytesat the endothelial surface. ArteriosclerThromb Vasc Biol 23:15411547
34. Mulivor AW, Lipowsky HH (2002)Role of glycocalyx in leukocyte-endothelial cell adhesion. Am J PhysiolHeart 283:H1282H1291
35. Rehm M, Zahler S, Lotsch M, WelschU, Conzen P, Jacob M, Becker B (2004)Endothelial glycocalyx as an additionalbarrier determining extravasation of 6%hydroxyethyl starch or 5% albuminsolutions in the coronary vascular bed.Anesthesiology 100:12111223
36. Leslie SJ, Affolter J, Denvir MA, WebbDJ (2003) Validation of laser Dopplerflowmetry coupled with intra-dermalinjection for investigating effects ofvasoactive agents on the skinmicrocirculation in man. Eur J ClinPharmacol 59:99102
37. Dubin A, Edul VSK, Ince C (2009)Determinants of tissue pCO2 in shockand sepsis: relationship to themicrocirculation. In: Vincent JL (ed)Yearbook of intensive care andemergency medicine. Springer,Heidelberg, pp 195204
38. Russell JA (1997) Gastric tonometry:does it work? Intensive Care Med23:36
39. Vallet B, Lund N, Curtis S, Kelly D,Cain S (1994) Gut and muscle tissuePO2 in endotoxemic dogs during shockand resuscitation. J Appl Physiol76:793800
40. Dubin A, Edul VS, Pozo MO, MuriasG, Canullan CM, Martins EF, FerraraG, Canales HS, Laporte M, EstenssoroE, Ince C (2008) Persistent villihypoperfusion explains intramucosalacidosis in sheep endotoxemia. CritCare Med 36:535542
41. Creteur J, De Backer D, Sakr Y, KochM, Vincent JL (2004) Sublingualcapnometry tracks microcirculatorychanges in septic patients. Crit CareMed 32:516523
42. Weil MH, Nakagawa Y, Tang W, SatoY, Ercoli F, Finegan R (1999)Sublingual capnometry: a newnoninvasive measurement for diagnosisand quantification of severity ofcirculatory shock. Crit Care Med27:12251229
43. Goedhart PT, Khalilzada M, BezemerR, Merza J, Ince C (2007) Sidestreamdark field (SDF) imaging: a novelstroboscopic LED ring-based imagingmodality for clinical assessment of themicrocirculation. Opt Express15:1510115114
44. Groner W, Winkelman JW, Harris AG,Ince C, Bouma GJ, Messmer K, NadeauRG (1999) Orthogonal polarizationspectral imaging: a new method forstudy of the microcirculation. Nat Med5:12091212
45. Clark LC (1956) Monitor and control ofblood and tissue oxygen tension. TransAm Soc Artif Intern Org 2:4146
46. Jobsis FF (1977) Noninvasive, infraredmonitoring of cerebral and myocardialoxygen sufficiency and circulatoryparameters. Science 198:12641267
47. Marik PE, Iglesias J, Maini B (1997)Gastric intramucosal pH changes aftervolume replacement with hydroxyethylstarch or crystalloid in patientsundergoing elective abdominal aorticaneurysm repair. J Crit Care 12:5155
48. Guo X, Xu Z, Ren H, Luo A, Huang Y,Ye T (2003) Effect of volumereplacement with hydroxyethyl starchsolution on splanchnic oxygenation inpatients undergoing cytoreductivesurgery for ovarian cancer. Chin Med J116:9961000
49. Lang K, Boldt J, Suttner S, Haisch G(2001) Colloids versus crystalloids andtissue oxygen tension in patientsundergoing major abdominal surgery.Anesth Analg 93:405409
50. Arkilic C, Taguchi A, Sharma N,Ratnaraj J (2003) Supplementalperioperative fluid administrationincreases tissue oxygen pressure.Surgery 133:4955
51. Boldt J, Heesen M, Muller M, PabsdorfM, Hempelmann G (1996) The effectsof albumin versus hydroxyethyl starchsolution on cardiorespiratory andcirculatory variables in critically illpatients. Anesth Analg 83:254261
52. Boldt J, Zickmann B, Herold C,Ballesteros M, Dapper F, HempelmannG (1991) Influence of hypertonicvolume replacement on themicrocirculation in cardiac surgery. BrJ Anaesth 67:595602
53. Mythen MG, Webb AR (1995)Perioperative plasma volume expansionreduces the incidence of gut mucosalhypoperfusion during cardiac surgery.Ann Surg 130:423429
54. Asfar P, Kerkeni N, Labadie F, GouelloJP, Brenet O, Alquier P (2000)Assessment of hemodynamic andgastric mucosal acidosis with modifiedfluid gelatin versus hydroxyethyl starch:a prospective, randomized study.Intensive Care Med 26:12821287
55. Forrest DM, Baigorri F, Chittock DR,Spinelli JJ, Rusel JA (2000) Volumeexpansion using pentastarch does notchange gastric-arterial PCO2 gradient orgastric intramucosal pHi in patientswho have sepsis syndrome. Crit CareMed 28:22542258
56. Rittoo D, Gosling P, Bonnici C,Burnley S, Millns P, Simms MH, SmithSR, Vohra RK (2002) Splanchnicoxygenation in patients undergoingabdominal aortic aneurysm repair andvolume expansion with eloHAES.Cardiovasc Surg 10:128133
57. Hofmann D, Thuemer O, Schelenz C,van Hoot N, Sakka SG (2005)Increasing cardiac output by fluidloading: effects on indocyanine greenplasma disappearance rate andsplanchnic microcirculation. ActaAnaesthesiol Scand 49:12801286
58. Mahmood A, Gosling P, Barclay R,Kilvington F, Vohra R (2009)Splanchnic microcirculation protectionby hydroxyethyl starches duringabdominal aortic aneurysm surgery. EurJ Vasc Endovasc Surg 37:319325
59. Wilkes NJ, Woolf R, Mutch M, MallettSV, Peachey T, Stephens R, MythenMG (2001) The effects of balancedversus saline-based hetastarch andcrystalloid solutions on acid-base andelectrolyte status and gastric mucosalperfusion in elderly surgical patients.Anesth Analg 93:811816
60. Kreimeier U, Bruckner UB, NiemczykS, Messmer K (1990) Hyperosmoticsaline dextran for resuscitation fromtraumatic-hemorrhagic hypotension:effect on regional blood flow. CircShock 32:8399
61. Behrman SW, Fabian TC, Kudsk KA,Proctor KG (1991) Microcirculatoryflow changes after initial resuscitationof hemorrhagic shock with 7.5%hypertonic saline/6% dextran 70. JTrauma 31:589598
62. Al-Rawi PG, Zygun D, Tseng MY,Hutchinson PJ, Matta BF, KirkpatrickPJ (2005) Cerebral blood flowaugmentation in patients with severesubarachnoid haemorrhage. ActaNeurochir (Suppl) 95:123127
1308
-
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.
c.134_2010_Article_1912.pdfThe impact of fluid therapy on microcirculation and tissue oxygenation in hypovolemic patients: a reviewAbstractIntroductionPathophysiology of the hypovolemic microcirculationHow can the effects of volume replacement be monitored?Clinical studies on the effects of fluid therapy on microcirculation and tissue oxygenationCrystalloidsColloidsHuman albumin (HA)DextransHydroxethyl starch (HES)GelatinsPlasma-adapted versus non-plasma-adapted volume replacement strategyHypertonic solutions
DiscussionConclusionsAcknowledgmentsReferences