The impact of devolution: Long-term care provision in the UK
44
The impact of devolution Long-term care provision in the UK David Bell www.jrf.org.uk January 2010 A review of the evolution of long-term care policy during the first decade of devolved government in the UK. Devolution has given the constituent nations of the UK greater freedom to pursue different long-term care strategies. After ten years of devolution, this report looks at why, and how, long-term care policies have diverged in England, Scotland, Wales and Northern Ireland. It found: • Population ageing is common to all parts of the UK. • Levels of disability are somewhat higher in Wales and Northern Ireland than in Scotland and England. • There is a dual system of support for those with long-term conditions. One branch is largely run by local authorities and health authorities, funded by the devolved administrations. The other operates through the Department for Work and Pensions. There is little interaction between these. • In relation to the demand for long-term care, differences within UK countries are much greater than differences between them. • Levels of support for long-term care differ partly because of differences in funding. Those more generously treated by the Barnett Formula can afford to provide better services. • But, in reality, the devolved authorities cannot follow radically different long-term care policies. They are constrained by the UK structure of taxes and benefits, where power is ‘reserved’ to Westminster. • So far, UK nations have not been good at learning lessons from each others’ experiences of long-term care policies. • Scotland, Wales and Northern Ireland are at a disadvantage to England because they do not have the resources to conduct large-scale evaluations of policy effectiveness. • Much of the legislation that influences long-term care provision was passed before devolution. Changing this legislation to permit greater policy differentiation is not high on the legislative agenda.
Transcript of The impact of devolution: Long-term care provision in the UK

The impact of devolution
Long-term careprovision in the UK
David Bell
www.jrf.org.uk
January 2010
A review of the evolution of long-term carepolicy during the first decade of devolvedgovernment in the UK.
Devolution has given the constituent nations of theUK greater freedom to pursue different long-termcare strategies. After ten years of devolution, thisreport looks at why, and how, long-term carepolicies have diverged in England, Scotland,Wales and Northern Ireland. It found:
• Population ageing is common to all parts ofthe UK.
• Levels of disability are somewhat higher inWales and Northern Ireland than in Scotlandand England.
• There is a dual system of support for thosewith long-term conditions. One branch islargely run by local authorities and healthauthorities, funded by the devolvedadministrations. The other operates throughthe Department for Work and Pensions. Thereis little interaction between these.
• In relation to the demand for long-term care,differences within UK countries are muchgreater than differences between them.
• Levels of support for long-term care differpartly because of differences in funding. Thosemore generously treated by the BarnettFormula can afford to provide better services.
• But, in reality, the devolved authorities cannotfollow radically different long-term carepolicies. They are constrained by the UKstructure of taxes and benefits, where power is‘reserved’ to Westminster.
• So far, UK nations have not been good atlearning lessons from each others’ experiencesof long-term care policies.
• Scotland, Wales and Northern Ireland are at adisadvantage to England because they do nothave the resources to conduct large-scaleevaluations of policy effectiveness.
• Much of the legislation that influenceslong-term care provision was passed beforedevolution. Changing this legislation to permitgreater policy differentiation is not high on thelegislative agenda.

Contents
Executive summary 2
1 Introduction 4
2 Devolution: politics and finance 5
3 The demand for long-term care acrossthe UK 11
4 Ability to pay 17
5 Care provision in the UK 20
6 Long-term care policy since devolution 24
7 Long-term care policies across the UK 32
8 Conclusions and recommendations 34
Notes 37
Related reports 38
References 39
Acknowledgements 42
About the author 42
Contents

Executive summary
This report reviews the development of long-termcare policy for older people in the UK, in the decadesince the introduction of devolution in 1999.
Executive summary2
Key findings include:
• The challenges which different parts of theUnited Kingdom face in terms of populationageing and the demand for long-term care arenot hugely different: the proportion of thepopulation aged 65 plus will increase rapidlyover the next few decades throughout the UK;levels of disability are slightly higher in Walesand Northern Ireland than in England andScotland; the ability to pay for care privatelyis higher in England than in the devolvedterritories; there appears to have been someconvergence in rates of unpaid care provisionacross the UK in recent years. The differencesin the demand for care across the constituentparts of the UK are not large by internationalstandards. Nevertheless, if the devolvedbodies have different views about equity, ordifferent capacities to deliver care efficiently,one might expect to see some variation inlong-term care policy across the UK nations.
• It is widely assumed that policies for thelong-term care of older people are entirelyunder the control of the devolvedadministrations in Scotland, Wales andNorthern Ireland. The financial and politicalimportance of the ‘secondary’ social caresystem, which is funded by DWP benefitswhich are determined at Westminster, is oftenoverlooked.
• It is also important to understand that the‘primary’ care system, which is in the handsof the devolved bodies, is ultimately fundedthrough the Departmental Expenditure Limits(DEL) system, while the secondary caresystem is funded through Annually Managed
Expenditure (AME). Annual budget constraintsare binding on DEL, but less so on AME. Thisimplies that social care provided by the devolvedauthorities is more likely to be rationed than isthe case for the care provided by DWP.
• The delivery of long-term care is largely in thehands of local authorities, with the exception ofNorthern Ireland. There is a wide divergence inneeds, ability to pay and provision across localauthorities throughout the UK. Both thedevolved administrations and the WestminsterGovernment face a political dilemma indetermining the relative role of centraliseddirection and local autonomy over long-termcare policy.
• While devolution may have restructuredpolitical power within the United Kingdom,it did not fundamentally change the systemfor funding Scotland, Wales and NorthernIreland. As a result, there continue to besignificant differences in the amount of publicresources allocated to long-term care in thedifferent parts of the UK.
• The devolved territories cannot pursuelong-term care policies that are independentof the UK Government. This is partly becauseof the secondary care system comprisingAttendance Allowance, Disability LivingAllowance and Carers Allowance, which arefunded by the Department for Work andPensions in London. Any changes to thesebenefits are likely to be driven by Englishconcerns, but will have knock-on effects in thedevolved territories. Politicians in Scotland,Wales and Northern Ireland cannot afford toignore the possibility of such change in

designing their own long-term care policies.The ability to influence what may happen toDWP benefits is at present very limitedbecause of the weakness of the system ofintergovernmental relations, such as the JointMinisterial Committees which were supposedlyan important component of the devolutionarrangements.
• It is not clear, therefore, that the devolvedterritories have the capability to pursue aradically different strategic vision for long-termcare from that in England. Scotland and Waleshave produced older people’s strategies, butthese cannot carry the weight of documentslike Putting People First, which outlines a visionfor the future of adult social care in England.They tend to have fewer resources to devoteto strategic development and, crucially, theycannot sign up stakeholders that haveresponsibility for ‘reserved’ issues, as ispossible with policy development in England.
• One of the benefits of devolution may be thatit does help policy-makers compare the effectsof policy changes in different parts of the UK.Certainly other parts of the UK have learnedfrom Scotland’s experience of free personalcare. But without formal intergovernmentalmechanisms for knowledge exchange, suchknowledge has mostly been collected anddisseminated as a result of the activities ofresearchers and interested organisations,including the Joseph Rowntree Foundation.Policy-makers therefore tend to learn atsecond hand about policy changes elsewherein the UK. This may lead to misunderstandingof what is going on elsewhere. Again there isa clear need to improve interaction betweenpolicy-makers in London, Cardiff, Belfast andEdinburgh.
• In developing long-term care policy, thedevolved administrations are at a disadvantagecompared with England. This is because theydo not have the resources to conduct andassess large-scale evaluations. An example isthe piloting of individual budgets in 13 localauthorities in England by the Independent
Budgets Evaluation Network (IBSEN).Additionally, the devolved authorities do nottend to work with the Department for Workand Pensions in developing policy initiativesfor care for older people. An example is theStreamlined Assessment Project (StAP),which integrates assessment procedures forAttendance Allowance and local authority care.A further consequence is that the devolvednations do not build up the capacity to analyselarge-scale evaluations. In England, individualuniversities, or groups of universities, arecapable of high-quality policy evaluations.
• Much of the legislation which sets theframework under which long-term care isprovided pre-dates devolution. This inhibitsthe devolved nations from instigating radicalchange because the unravelling of thislegislation would be problematic andtime-consuming. Integral to this is the rolegiven by such legislation to local authoritiesfor the delivery of social care. As a result,social care policy is partly a product of theway that local government interacts with thedevolved administrations and with theDepartment of Health in England.
• Whether devolution has benefited care clientsis difficult to assess. In the last decade, therehas been a substantial increase in theresources allocated to health and careprovision throughout the UK, which will notbe repeated for the foreseeable future. Overthis period, opportunities for co-operation orco-ordination of social care policy across theUK have rarely been taken. The need tounderstand successful policy interventions indifferent parts of the UK will be much moreacute in the next decade.
Executive summary 3

Introduction4
The UK has long struggled with the problem ofdesigning an effective and fair long-term carepolicy for older people. In the last decade, withthe advent of devolution, the context for thedevelopment of such policy has changedsubstantially. As a result of the establishmentof the Scottish Parliament and the Welsh andNorthern Ireland Assemblies, the constituentparts of the UK (the devolved nations) were givengreater freedom to design and implement theirown long-term care policies. As a result, therehas been increasing policy diversity across theUK. But the development of policy also reflectsvariations in the finances available to the devolvedbodies, the demand for long-term care by olderpeople and the ability to pay for such care. Suchpolicies also have to take account of the widevariations in demand and in ability to pay thatexist within each part of the UK.
This report looks at the role of devolution inthe development of long-term care policy in thelast decade. It considers how far such policyin the devolved nations is constrained by policiescontrolled from Westminster. Next, it examinesdiversity in long-term care provision both withinand between the nations that comprise the UK.Finally, it discusses how devolution affects thepolitical and financial context within whichlong-term care policy is framed in the UK.
1 Introduction

Devolution: politics and finance 5
Politics
Devolution in the UK celebrated its tenth birthdayin 2009. On 1 July 1999, powers were transferredfrom Westminster to the Scottish Parliament andto the Welsh Assembly. In Northern Ireland, thetransfer took place on 2 December 1999. TheNorthern Ireland Assembly has not satcontinuously since then: its most recent spellbegan on 26 March 2007.
While many powers were transferred to thenew Parliament and Assemblies, others were‘reserved’ to Westminster. Reserved powersinclude social security, defence andmacroeconomic policy. Areas such as health,housing and local government came under thecontrol of the devolved bodies. The devolvedinstitutions enable the people of Scotland, Walesand Northern Ireland to exert greater control andscrutiny over a range of important public services.As a consequence, policy differences haveemerged.
One area where such divergence hasincreased is the provision of long-term careto older people. The Department of Health inEngland and the devolved nations provideresources for local authorities and health boards.These resources, in turn, support services forolder people requiring long-term care. Serviceswhich the local authority funds may be providedby the private sector, by the voluntary sector ordirectly by themselves. In the remainder of thisreport, this set of local authority-based activitiesis described as the primary care system. Its keyfeature is that the devolved nations and Englandhave some latitude to design and implement theirown long-term care policies in the primary caresector. These differences emerge partly becauseof institutional differences in delivery mechanismsfor long-term care in different parts of the UK.
Thus, in Wales, Scotland and England, localauthorities are primarily responsible for deliveringcare for older people, liaising with relevant health
boards. In Wales, health boards and localauthority boundaries are coincident. In NorthernIreland care is delivered by Health and Social CareTrusts (HSCs). The Minister of Health, SocialServices and Public Safety appoints the chairmanand the non-executive directors of the HSCs.Thus, in Northern Ireland, social care policy doesnot have a local democratic input. There arepositive and negative aspects of the Northern Irishstructure. It is easier to ensure uniformity inassessment, provision and charging when thereare no local political inputs. On the other hand,local care clients might wish to differentiateprovision from that in other parts of the Province.This issue of uniformity versus local discretionarises in many different guises in the debate onlong-term care policy in the UK.
There is another care system which is fundedby the public sector, but is entirely independent ofthe devolved bodies. The secondary care system,which is administered by the Department for Workand Pensions (DWP), provides direct cash benefitsto the disabled, carers and those with care needs.These benefits comprise Attendance Allowance(AA) and Disability Living Allowance (CareComponent) (DLA) and Carers Allowance (CA).AA and DLA are non-means-tested cash benefits.Older clients can use the cash as they see fit.Their assessment procedures differ from thoseused by the primary system.
AA is payable to those aged 65 and over whoneed help with their personal care because of anillness or disability. Similarly, DLA provides forthose aged under 65 with personal care needs.But if the claim was made before age 65 and thedisability has persisted, the benefit will continue tobe paid after the client reaches 65. Thus, DLAclaimants tend to be drawn from the ‘young’ old,while AA claims are typically made by the ‘oldest’old.
AA is paid at two rates depending on the levelof disability. The current higher rate is £70.35 andthe lower rate is £47.10. DLA (Care Component)
2 Devolution: politics andfinance

is payable at three weekly rates, £70.35, £47.10and £18.65. In November 2008, there were0.98 million individuals aged 65+ receiving DLAand 1.63 million receiving AA. The secondary caresystem supports more than 2.6 million individualsthroughout the UK. In 2008/9 the total cost of AAwas £4.7 billion. Assuming that the amount paidthrough DLA is on average the same irrespectiveof age then a further £2.7 billion can be added tothe DWP bill to support long-term care. Thisimplies that the average annual payment to
claimants through the secondary care system insupport of personal care needs is around £2,800per client.
Thus, the process of devolution has naturallyresulted in a focus on the primary system of careprovision because the devolved bodies can formtheir own policies for its delivery. But this hasperhaps resulted in a failure to appreciate theimportant contribution made by the secondarysystem in supporting older people with care needson a uniform basis throughout the UK. There was
Devolution: politics and finance6
Box 1: Attendance Allowancepayments to care home clients inScotland
Prior to 2001, care home residents could becharged for nursing care, subject to a meanstest. After the report of the Royal Commissionin 1999, the principle of free nursing care wasaccepted throughout the UK. But from July2002 the Scottish Parliament agreed to providefree personal care as well as nursing care forboth care home clients and those receivingcare at home. Weekly payments for nursingcare and personal care were set at £65 and£145 respectively. Payments were to be madeby the local authority. AA is specificallyintended to help ‘people aged 65 or over whohave an illness or disability and need help withpersonal care’. DWP rules prevent paymentof AA when a local authority is alreadycontributing towards the client’s personal carecosts. Hence AA was withdrawn from clients inScottish care homes who were receiving freepersonal care. Payments for nursing care,which form part of health care and so arewithin the scope of the NHS, are not affectedby this rule. In contrast, those who now receivefree personal care at home in Scotland, whomight have previously paid for this care,continue to receive AA.
England, Wales and Northern Irelandadopted more generous allowances for nursingcare than did Scotland. The current position isthat the allowance for nursing care in Scotlandis £69 per week; in England there are two
bands with a lower rate of £103.80 and higherrate of £142.80; in Wales there is a single bandof £119.66; and in Northern Ireland thecontribution is ‘up to’ £100 per week.
AA is payable at £70.35 at the higher rateand £47.10 at the lower rate. This means thata care home client in England could potentiallyreceive up to £213.15 per week from nursingcare and AA, while in Scotland the maximumpayable for both nursing and personal care is£222 per week – based on the currentpersonal care allowance of £153 per week. Thenumbers of clients eligible for such allowancesin both countries depend on many factorsincluding assessment procedures. But thedifference in the maximum contributionbetween Scotland and England is less than £9per week even though the headlines around‘free personal care’ suggest that the Scottishpolicy is much more generous. One importantdistinction is that all of the payments inScotland come from the Scottish budget,whereas in England they are funded in part bythe Department of Health and in part by theDepartment for Work and Pensions.
The introduction of free personal care inScotland has ‘saved’ DWP over £200 million inAA since 2002. Scottish politicians and mediahave felt that this was unjust. Lord Sutherland’srecent review of free personal care alsosuggested that this was an anomaly. It isunclear whether any radical change in thestructure of disability benefits will follow from therecent Green Paper. Until there is some radicalchange in AA, the status quo is likely to prevail.

one important difference of opinion as to whetherits application has always been uniform – thepayment of AA to care home clients in Scotlandwho were receiving free personal care. This provedan extremely controversial issue (see Box 1).
The primary and secondary care systems donot serve identical groups of clients, largely due todifferences in their assessment procedures. Thiscan be illustrated with data from Scotland. TheScottish Government collects data on those beingprovided with free personal care at home by localauthorities. These clients are in the primary caresystem. As shown in Box 1, AA is only paid tothose living at home in Scotland: care homeclients are excluded. Thus, one might expect alarge overlap between those receiving personalcare at home from their local authority (primarysystem) and those receiving AA (secondarysystem). But the populations served by the twosystems differ substantially in size. The numberof personal care clients being supported in theprimary system is around one-third of the numberbeing supported in the secondary system. If oneadds those receiving at least the lower carecomponent of DLA who are aged 65 and over, theshare receiving care from the primary sector fallsto 21 per cent. Thus, for older clients living athome, the secondary care system, which isentirely independent of the devolved institutions,serves almost five times as many clients as theprimary system.
This illustrates one of the main paradoxesof devolution and long-term care in the UK. Thereare two quite distinct systems: one is supportedby DWP, while the other is provided by localauthorities that are responsible to their respectiveadministrations. Provision by the devolvedauthorities through the primary system is strictlycash-limited, while that provided through thesecondary system is not subject to such stringentfinancial controls.
The secondary care system is subject to lessstringent financial control than the primary systembecause social security benefits form part ofAnnually Managed Expenditure (AME). AME is notdirectly cash-limited by HM Treasury since it isdifficult to precisely predict large elements ofsocial security spending. Rather, the Treasuryestimates the likely path of AME and determines
its other spending plans based on theseestimates. In particular, it determines aDepartmental Expenditure Limit (DEL) for eachspending ministry and for each of the devolvedbodies. The Department of Health and thedevolved bodies must stay within the DEL thatthey have been assigned. To stay within theselimits, the devolved bodies assign fixed budgets totheir local authorities and health boards.
At the level of the individual client requiringcare, this means that local authority social workdepartments will be working within budgets thatthey cannot breach, while the opportunity cost ofproviding Attendance Allowance or Disability LivingAllowance is much more nebulous. Assessing anadditional client as eligible for AttendanceAllowance does not appear to reduce the budgetof any other part of the public sector. Of course,in the long run, there is an equivalent cost togovernment, irrespective of whether the fundinghas come from the primary or secondary caresystem, but to those making the decisions aboutwhether to provide local authority-funded careservices on the one hand, or social securitybenefits on the other, this equivalence may not beat all clear.
There is also a ‘tertiary’ system of care supportcomprising unpaid care by friends and relativesand privately purchased care. It is not directlydependent on the public sector for funding, thoughthe supply of care by this route does interact withpublic provision. In the UK, there are around fivemillion relatives, friends and volunteers in the UKwho provide unpaid care to older people. Notmuch is known about this sector in the sense thatsurvey and administrative data on private careprovision tends to be limited for a variety ofreasons. Compared to the widespread availabilityof data on publicly provided health care, the dataon social care in the UK is much less complete,particularly that involving the tertiary sector wherethe public sector may have no role in assessment,commissioning or provision. Even where data isavailable, it is often collected in different ways inEngland, Wales, Scotland and Northern Ireland,making comparisons difficult. UK-wide data tendsto be only available from commercial organisationssuch as the UK Home Care Association and Laing& Buisson, who collect data on care homes.
Devolution: politics and finance 7

As we have just seen, the primary andsecondary systems do not serve the same set ofclients. DWP benefits are not means-tested, whileat least in England and Wales, local authoritypersonal care provision is subject to means-testing. And this affects the tertiary care sector,since clients who feel they receive inadequatepublicly funded support may seek care elsewhere.This may come from family, friends or charities,or it may be purchased from the private sector,provided that the client has the required resources.
Long-term care policy and devolution werelinked by one important coincidence. For theincoming Labour administration in 1997, bothdevolution and long-term care policy were close tothe top of the ‘to do’ list. There were manifestocommitments in both policy areas. Thus the RoyalCommission on Long-Term Care was establishedin 1997 with Sir Stewart Sutherland as chairman.Its report was published on 1 March 1999, only afew months before the establishment of thedevolved bodies.
A key recommendation in its report, supportedby a majority of the commissioners, was that‘personal care should be available after anassessment, according to need and paid for fromgeneral taxation’ (HMSO, 1999a,). But in a formalnote of dissent, two of the commissioners arguedthat this proposal was unaffordable. The devolvedbodies were thus established just as the report ofthe Royal Commission was stimulating an intensedebate on the future of long-term care.
Powers to influence long-term care variedacross the devolved bodies. This was becausedevolution was ‘asymmetric’: though they wereresponsible for largely the same policy areas, thedevolved bodies did not have the same powers tolegislate. For example, the Welsh Assembly didnot have the power to introduce primarylegislation: it could only build on existing Acts ofthe UK Parliament. This was partly responsible forthe decision of the Welsh Assembly not to goahead with the policy of free domiciliary care(see Box 2).
Devolution: politics and finance8
Box 2: Domiciliary care charges:the importance of the legislativeframework
The Welsh Assembly only had secondarylegislative powers when it was set up.It therefore had to work within the frameworkof UK statute. For non-residential care, this wasprovided by the National Assistance Act 1948,which makes local authorities responsible forthe provision of non-residential social services.In addition, the Health and Social Services andSocial Security Adjudication Act 1983 giveslocal authorities discretionary power to recovercharges for care services, including personalcare.
The Labour Party made a manifestocommitment in 2003 to provide free domiciliarycare to all adults (not just those aged 65+). Butthe Welsh Assembly could not pass a law toprevent local authorities charging for theseservices. This was because it only hadsecondary legislative competence. It could tryto persuade local authorities to stop chargingby compensating them for the loss in income,
but it did not have the powers to guarantee anend to charges. In contrast, with its primarylegislative powers, the Scottish Governmentcould, and did, force local authorities to stopcharging for personal care services delivered athome to those aged 65+.
The Government of Wales Act 2006enhanced the legislative powers of the WelshNational Assembly. It can now bring forward aLegislative Competence Order (LCO) thattransfers powers from the UK Parliament to theWelsh Assembly. This gives the Assembly theability to introduce primary legislation, thoughby a much more convoluted procedure than isrequired in Scotland. LCOs have to beapproved by the Assembly, the Secretary ofState for Wales and both Houses of the UKParliament. In 2008, the Assembly successfullyintroduced an LCO to ‘create a more levelplaying field in relation to charges for domiciliarycare services’ (WAG, 2009). During 2009, itconsulted on how this objective would best betaken forward, before introducing the necessarylegislation to effect a more uniform structure ofhome care charges throughout Wales.

In Northern Ireland, there are ‘excepted’powers over which the Assembly has no controland ‘reserved’ ones where legislation requires theconsent of the Secretary of State. The Assemblyhas powers to pass primary legislation in othermatters and therefore could have introduced freepersonal care to Northern Ireland.
Aside from the differences in the powers of thedevolved bodies, another set of contrasts existedbecause of the different ways in which long-termcare policy had evolved across the UK, evenwithin a common legislative framework. Thus, forexample, in 1999 more than 50 per cent ofcontact hours purchased or provided by localauthorities in England were supplied by theindependent sector; in contrast, in Scotland, only8 per cent of hours were not supplied exclusivelyby local authorities. Some local authorities inScotland had already effectively introduced freepersonal care before 1999. As we shall see, thiswas one of the reasons why there was so muchvariation across Scottish local authorities in thecosts of free personal care.
Finance
Devolution introduced new legal frameworkswithin which long-term care policy operated indifferent parts of the UK. But this was not the onlyreason why long-term care policy evolved indifferent ways: resources also played a key part.There have been significant differences ingovernment spending per head in different partsof the UK for many decades. These partly reflectvarying levels of need: where unemployment ishigh, per capita payments on unemploymentbenefits will be high. But differences in spendingpower between the devolved governments arelargely driven by the Barnett formula, an arcanedistribution formula devised in 1978 by JoelBarnett, then Chief Secretary to the Treasury. Itsoutcomes are largely driven by past history ratherthan by differences in need.
The Barnett formula passed unscathedthrough the devolution process. While the UKGovernment was willing to concede additionalpolitical powers to Wales, Northern Ireland and
Devolution: politics and finance 9
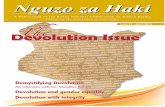
Figure 1: Real public expenditure per head by country 1998/9 to 2008/9 (2007/8 prices)
£0
1998
/99
1999
/00
2000
/01
2001
/02
2002
/03
2003
/04
2004
/05
2005
/06
2006
/07
2007
/08
2008
/09
£2,000
£4,000
£6,000
£8,000
£10,000
£12,000
Scotland
Wales
Northern Ireland
England
Source: Public Expenditure Statistical Analysis, HM Treasury

Scotland, it was unwilling to extend additionalfinancial powers.1 As we shall see later, proposalsfor changes to the funding system have recentlybeen made in both Scotland and Wales. Thus,while devolution increased the ability to exertpolitical control over long-term care policy, it didnot significantly increase the ability of the devolvedbodies to control the financial resources availableto them.
Figure 1 illustrates spending per head in realterms (2007/8 prices) in the devolved nations overthe period 1998/9 to 2008/9.2 The trends arealmost parallel, implying that there have beenminimal changes in relative public spending perhead between England, Scotland, Wales andNorthern Ireland since devolution was introduced.Thus, for example, public spending per head inScotland was 16 per cent above that in the UK asa whole in 1998/9; in 2008/9, it was still 16 percent above the UK average.
Figure 1 also illustrates a second majorcoincidence that affected both devolution andlong-term care policy in the last decade. Over thisperiod, there has been a period of unprecedentedreal increases in public spending. In the UK as awhole, the real value of public spending per headgrew by 55 per cent between 1998/9 and2008/9 – 3.6 per cent per annum – and well inexcess of the real growth of the UK economy.This meant a general loosening of budgetconstraints.
Many of the differences in long-term carepolicy among the devolved nations and Englandthat have emerged since 1999 can be more easilyinterpreted in the light of the differences in theirrespective financial settlements rather than as aresult of devolution itself. The UK may havebecome a ‘policy laboratory’ as a result ofdevolution. This might help explain the differencesin long-term care policy that have emerged since1998/9. But it is vital to bear in mind that thefreedom to pursue new policies within thislaboratory is constrained by available resources.And, as we have just seen, devolution did notsignificantly affect the distribution of public financeamong the different parts of the UK. But, whileresource availability may constrain policy variation,differences in care provision may reflectdifferences in the demand for care across the UK.In the next chapter, we examine the extent towhich such contrasts exist.
Devolution: politics and finance10

The demand for long-term care across the UK 11
Long-term care policy may have evolveddifferently in Scotland, Wales and Northern Irelandbecause of variations in the level and nature ofdemand for long-term care. The purpose of thischapter is to investigate differences in demand forlong-term care across the UK.
A good starting point is to look at differencesin the proportions of the population aged 65 andover. These are shown in Table 1 for variousyears. There has clearly not been any ‘devolution’effect that influenced the age structure of thepopulation in the devolved nations during thisshort period. Table 1 shows that NorthernIreland’s population is somewhat younger thanelsewhere. Thus, relative to its total population,the demand for long-term care in Northern Irelandis lower than in the rest of the UK. But theproportion of those aged 65+ in Northern Ireland(and Scotland and Wales) grew more rapidly thanin England between 1981 and 2007. This is partlythe outcome of higher rates of immigration fromoverseas by younger people into England, whichwill keep its population relatively young.
The demand for long-term care depends notonly on the size of the older population, but alsoon its health. One way to analyse this is to look atthe difference between overall life expectancy and‘healthy’ or ‘disability free’ life expectancy. TheOffice of National Statistics has analysedresponses to questions on health and disability inthe General Household Survey in Great Britain andthe Continuous Household Survey in NorthernIreland. Figure 2 shows the number of years inpoor health or with disability that someone aged65 can expect in different parts of the UK. ThusWelsh females will, on average, experience thelongest period of poor health – 6.2 years. Scottishmales aged 65 can expect a much shorter periodof poor health, 2.7 years, mainly reflecting theirshorter life expectancy. The disability data isbroadly consistent with that on poor health,though both males and females in Northern Irelandexperience longer periods of disability than malesand females elsewhere in the UK. This finding hasto be treated with care, given that the NorthernIreland data is drawn from a different survey.
3 The demand for long-termcare across the UK
Table 1: Share of older people (aged 65+) in total population (%)
Source: NOMIS (www.nomis.co.uk) and Northern Ireland Statistics and Research Agency (NISRA)
Year England Scotland Wales Northern Ireland
1981 23.5 22.1 24.6 11.8
1991 24.3 23.0 27.0 12.9
2001 24.2 24.1 27.3 13.1
2007 24.0 24.5 27.5 13.7

Taken together, this data suggests shorterperiods of poor health and disability in Scotland,both for males and females. At the other end ofthe spectrum, it appears that older people inWales and Northern Ireland experience longerperiods of poor health and disability. Thesedifferences are clearly influential in determiningdemand for long-term care.
Another way to review the demand forlong-term care across the UK is to analyse claimsfor disability-related benefits among those aged65 and over. Figures 3 and 4 show the proportionof those aged over 65 receiving AA and DLA,respectively, across the UK since 2002.1 Theyshow some distinct trends. First, in line with thedata on poor health and disability, the share ofolder people receiving DLA and AA is significantlyhigher in Wales and Northern Ireland than in eitherScotland or England. Second, DLA claims bythose over 65 are increasing much more rapidlythan AA claims. This reflects increasing numbersof those below pension age receiving DLA, whichthen continues beyond retirement age. Between2002 and 2008, there was a 14 per cent increasein the number of DLA claimants aged 50–64 and a34 per cent increase, to 2.1 million, in the numberof claims that had lasted at least five years.
The share of the older population receiving AAis more stable. As with DLA, among those agedover 65, a slightly larger share of older people inScotland than in England claim AA. But this is arelatively small difference compared with the muchhigher rate of claims for both AA and DLA inWales and Northern Ireland. In Wales more than20 per cent of those aged 65+ now claim AA andthis share is increasing, while in Northern Ireland,where almost 30 per cent of older people were AAclaimants in 2002, the share has recently fallen tojust over 25 per cent.
The data on AA and DLA suggests significantvariation between the devolved nations. But theyconceal much greater variation within theirboundaries. Figure 5 maps the proportion of thoseaged 65+ receiving AA by local authority acrossthe UK. This share varies between 4 per cent and37 per cent – much greater than the variationbetween the devolved nations. If benefit take-up isan objective indicator of long-term care needs,then each part of the UK experiences widevariation in the demand for long-term care withinits boundaries. Local authorities and health boardsin the devolved nations have widely differingresource needs if they are to provide a uniformlevel of support for long-term care clients.
The demand for long-term care across the UK12
Figure 2: Expected years with poor health/disability, 2004–06
Source: Health Statistics Quarterly No 40, Winter 2008, Office of National Statistics
Males, Northern Ireland
Males, Scotland
Females, Scotland
Females, Northern Ireland
Females, England
Males, Wales
Males, England
Females, Wales
0 2 4 6
Years of poor health/with disability
8 10 12
Poor health
Disability

These benefit statistics may not be unbiasedmeasures of the demand for long-term care. Theremay be differential take-up of AA and DLA acrossregions. Some regions may have more effectivesystems to assist claimants, as indicated by theHouse of Commons Work and PensionsCommittee (2009) in its recent report on pensioner
poverty. But while there is evidence of low take-upof some types of benefit, particularly by olderpeople, there is little evidence of regional variationin low take-up. Given that eligibility criteria are thesame throughout the UK, it is difficult to explain thevariation shown in Figures 3, 4 and 5 unless thereis a corresponding variation in disability rates.
The demand for long-term care across the UK 13
Figure 4: Proportion of over 65s receiving AA, 2002–07
02002
Source: Department for Work and Pensions and Social Security Agency, Northern Ireland
2003 2004 2005 2006 2007
5
10
15
20
25
30
35
Scotland
Wales
Northern Ireland
England
Per
cent
Figure 3: Proportion of over 65s receiving Disability Living Allowance, 2002–07
02002
Source: Department for Work and Pensions and Social Security Agency, Northern Ireland
Per
cent
2003 2004 2005 2006 2007
2
4
6
8
10
12
14
16
18
20
Scotland
Wales
Northern Ireland
England

The overall picture of the demand forlong-term care across the countries of the UKis complex. Northern Ireland has a youngerpopulation than the rest of the UK. Levels ofdisability are higher in Wales and Northern Ireland.Years of unhealthy life expectancy are shortest inScotland. There are some variations in levels ofdisability within the devolved nations. But byinternational standards, these differences are
relatively small. Further, there is much greatervariation in disability rates between localauthorities than between the constituent parts ofthe UK as a whole. And the secondary caresystem has a much larger client base than itsprimary equivalent.
To complete the picture of the demand forlong-term care for older people across the UK, wefinally focus on the tertiary care system – where
The demand for long-term care across the UK14
Figure 5: Proportion of over 65s receiving Attendance Allowance by local authority (November 2008)
David Bell, University of StirlingSource: NOMIS
[20, 37] (77)
[Range ofpercentagescovered]
(number of localauthorities fallingwithin that range)
[18, 20] (90)
[17, 18] (70)
[16, 17] (89)
[15, 16] (71)
[14, 15] (120)
[4, 14] (107)

paid and unpaid care is provided by friends,family, charities and private providers. As alreadymentioned, much of this activity is not wellmeasured.
One way to examine the unpaid carecomponent is to look at UK-wide householdsurveys which include questions on voluntary careprovision. The Family Resources Survey is aregular survey of representative households that
has been conducted each year since the mid1990s. Unfortunately data from Northern Ireland isonly available since 2003. Figures 6 and 7 showthe proportion of adults receiving care at homeand the proportion of adults giving care, either inthe home or outside the home, respectively.Figure 7 shows differences in levels of disabilityacross the UK. England has the lowest share ofolder people receiving care, while Northern Ireland
The demand for long-term care across the UK 15
Figure 7: Trends in care giving across the UK, 1997/8 to 2007/8
51997 1998 1999 2000 2001 2002 2003 2005 2006 2007
7
9
11
13
15
17
19
21
Scotland
Wales
Northern Ireland
England
Per
cent
Figure 6: Trends in care receiving across the UK, 1997/8 to 2007/8
41997 1998 1999 2000 2001 2002 2003 2005 2006 2007
5
6
7
8
9
10
11
12
13
14
Scotland
Wales
Northern Ireland
England
Per
cent

has the highest proportion. These rankings areconsistent with the findings from the AA data. Thedownward trend evident in the proportionreceiving care in Figure 6 and the simultaneousupward trend in the number of clients receiving AAand DLA may suggest that there is a shift awayfrom tertiary care to secondary care – from friendsand relatives to reliance on cash benefits fromDWP to purchase care services.
There is a higher proportion of adults givingcare than receiving care. This is because somecare clients receive care from more than oneindividual. Thus the proportion of the adultpopulation giving care in Figure 7 is significantlyhigher than the proportion receiving care asshown in Figure 6. In line with the general declinein the receipt of care, Figure 7 also showsa reduction in the share of adults giving careto friends and relatives in the ten years prior to2007/8. The downward trend seems commonto all parts of the UK: in fact, there appears tobe some convergence, with around 11 per centof adults in each part of the UK providing careto other adults in 2007/8. There is no evidenceof diverging trends in unpaid care provision thatmight be associated with differences in long-termcare policy across the UK.
The demand for long-term care across the UK16

Ability to pay 17
Older people’s ability to pay for long-term careservices varies substantially throughout the UK.There are three factors that affect the capacity todirect purchase care services:
1 Pensions – for those aged 65+, pensions arethe main source of income. Private pensionsdepend on contributions to pension schemesduring working life, while state pension isdependent on the history of National Insurancecontributions. High earners who have beenemployed for most of their adult life are likelyto have a higher pension than those who havebeen periodically outside the workforce forreasons such as unemployment, care-giving orbringing up a family.
2 Savings and investments – which reflectincome and consumption patterns. Those whohave consumed a large proportion of theirincome or have supported others with cashtransfers may not have assets that can easilybe liquidated to pay for care.
3 Housing equity – by international standards,the UK has a high proportion of homeownership. Thus, large numbers of UK citizenshave significant proportions of their wealth inthe form of housing equity rather than infinancial assets. Older people generally find theprocess of reducing their housing equity to payfor care distressing.
Each of these components of pensioner wealthvaries across the constituent parts of the UK.Table 2 shows data for weekly household incomeand non-housing capital which is drawn from theFamily Resources Survey 2007/8. Smallersamples in Wales and Northern Ireland mean thatresults for these areas must be treated withcaution. Nevertheless a consistent patternemerges. For households where the head is aged65 or above, household income is highest inEngland and lowest in Scotland. For working-agehouseholds, income in Scotland is generally higherthan in either Wales or Northern Ireland. For thoseof pension age, household incomes in Wales and
4 Ability to pay
Table 2: Ability to pay
Source: Family Resources Survey 2007/8 and Department of Communities and Local Government
England Wales Scotland Northern Ireland
Average weekly household incomeaged 65+
£375.6 £391.1 £346.7 £363.3
Households with > £23,000non-housing capital (%)
28.89 22.96 22.15 11.54
Owner-occupiers 1991 (%) 68.1 70.7 52.4 65.6
Owner-occupiers 2008 (%) 71.1 77.0 77.9 88.5
Average house price 2008 £237,112 £169,948 £168,593 £218,282

Northern Ireland are higher than those in Scotland.This is because higher rates of disability in Walesand Northern Ireland result in higher contributionsfrom AA, DLA and other social security benefits toweekly household income. For the UK as a whole,pensioner household incomes are higher whensomeone in the household receives care. But higherhousehold incomes in England also reflect higherlifetime earnings, and therefore higher pensions.
A higher proportion of pensioner householdsin England have more than £23,000 in financialassets. This limit is important because care clientswhose savings and investments exceed £23,000are normally expected to meet all of their carecharges. Scotland and Wales both have around22 per cent of households in this category, almosttwice the share in Northern Ireland, though thelatter figure should be treated with caution.
Ability to pay18
Figure 8: Proportion of over 65s receiving Pension Credit by local authority (November 2008)
David Bell, University of StirlingSource: NOMIS
[40, 75] (69)
[32, 40] (104)
[28, 32] (119)
[26, 28] (107)
[24, 26] (60)
[20, 24] (85)
[12, 20] (80)
[Range ofpercentagescovered]
(number of localauthorities fallingwithin that range)

Housing tenure varies across different parts ofthe UK. Currently, Scotland has the lowest shareof owner-occupiers, though the share ofowner-occupiers grew more rapidly in Scotlandbetween 1991 and 2007 than in other parts of theUK. Nevertheless, this means that a higherproportion of those entering residential care inScotland cannot use housing equity to pay forcare. The Care Development Group (2001) arguedthat the increasing proportion of home ownershipin Scotland would offset the costs of free personalcare because an increasing share of thoseentering residential care would have access tohousing equity and therefore would be able tocontribute towards their accommodation costs.
House prices are good indicators of housingequity, particularly for older people who havetypically fully repaid their mortgage. Table 2 showsthat house prices are highest in England, whilethose in Wales and Scotland are around 30 percent lower. House prices in Northern Ireland in2008 were above those in Scotland and Walesbut below those in England. Recent experiencewith the housing market shows that house pricescan be extremely volatile, suggesting that housingequity is not a low-risk method of fundinglong-term care.
Household income, financial assets andhousing assets can all be used to fund long-termcare. Clearly these vary between England andother parts of the UK. Devolution is not the causeof these differences: they are largely historical orreflect changes in economic circumstances sincedevolution. Differences in ability to pay may elicitdifferences in policy response across the devolvedinstitutions. In areas where pensioner income andassets are relatively low, one might expect greaterreliance on state provision of care and vice versa.But this will result in more affluent clients in poorerareas gaining while poorer clients in affluent areaslose in terms of state support for care provision.
What the data in Table 2 fails to reflect is thehuge variation in incomes and assets that existswithin each part of the UK. This can be illustratedwith measures of inequality. There is a class ofsuch measures which can be used to allocate theoverall inequality in pensioners’ household incomein the UK to that which arises between England,Scotland, Wales and Northern Ireland and that
which is due to variation within these areas. Usinga measure devised by Frick et al. (2006) incombination with the 2007/8 Family ResourcesSurvey, one can show that over 99 per cent of theinequality in pensioner household income in theUK is due to differences within the nations, whileless than 1 per cent of this inequality is due todifferences between average pensioner householdincome in England, Scotland, Wales and NorthernIreland. To reinforce the message that variationwithin is much more important than variationbetween, Figure 8 shows the proportion ofpensioners receiving Pension Credit by localauthority across the UK at the end of 2008. Theshare varies massively. Across UK localauthorities, a minimum of 12 per cent and amaximum of 75 per cent of pensioners receivePension Credit. The south of England hasgenerally lower proportions of pensioners receivingPension Credit, but it is also striking that there is agreat deal of variation in this share both withinEngland and within the devolved nations.
The conclusion from the analysis of ability topay is that though there are significant differencesin older people’s ability to contribute towards thecosts of long-term care between the componentparts of the UK, these are much less significantthan the differences within each part. Further, thedifferences in incomes, financial assets and thevalue of housing between the devolved nationsare not themselves the result of devolution, butlargely reflect past political and economicdecisions.
Ability to pay 19

Care provision in the UK20
In the UK, care is provided in a number ofsettings, including long-stay hospitals, carehomes, various forms of intermediate housing andclients’ homes. Of these, the most importantsettings in terms of numbers of clients are carehomes and care at home. The balance of carebetween these different forms of provision tendsto change slowly because of the organisationaland staffing costs associated with change.
Another dimension to care provision is theissue of the ownership of the organisationssupplying care. There is an ideological dividebetween those who believe that care should bedelivered by the state and those who favourprivate sector provision. The arguments of thosewho favour state provision generally emphasiseequity and quality, while those who supportprivate provision argue that this form of provisionmaximises efficiency and client choice.
Different parts of the UK had different policypositions with respect to these dimensions of careprior to devolution. There have been somechanges since 1999, particularly in Scotland, butthe changing role of the private sector andincreased personalisation are mainly attributableto policies developed at Westminster for England.For example, the debate between private andpublic sector provision has become less stark.The Blair Government moved towards increasedprivate sector delivery in England, aiming tocombine private sector efficiency with the publicsector acting as regulator and commissioner ofservices. Rather than focusing on an exclusivelypublic sector or private sector system, the debaterefocused on the respective roles of the privateand public sectors within that system. Increasedcommissioning of private sector providers by localauthorities underlies the rapid increase in privatesector delivery of home care services by localauthorities in England. Westminster has alsopromoted consumer choice by extending clients’rights to choose between service providers. Thisapproach is aligned with the general preference of
frail older people for care services to be deliveredat home. It also provides a rationale for theextension of direct payments, self-directed care,and personal and individual budgets.
The enthusiasm for extending consumerchoice was not shared to the same extent by thedevolved administrations, even those that wereLabour-dominated. Thus, as we shall see, theimplementation of consumer choice in careservices varies considerably across the UK. Fora variety of reasons the extension of client controlover care packages has been more limited in thedevolved administrations than in England.
But ideological differences at the national levelare not the only source of variance: social carepolicy is delivered by local authorities, which havetheir own policy agenda. They have always hadsome choice over the range and quality ofservices that they provide to older people. Even ifthe resources provided to local authorities by thedevolved authorities to support older people are‘ring-fenced’, they could decide to provideadditional services to older people by increasingtheir spending above the ring-fenced level.
Another aspect of policy in recent years hasbeen a drive to remove so-called ‘postcodelotteries’ in the provision of public services.Political parties have willingly or unwillingly beenforced to increase pressure on local servicedeliverers to conform to national standards. It ismost clearly exemplified by the use ofPerformance Indicators, particularly in England,to ensure that public bodies follow the policyobjectives set by government. This was anothercomponent of the New Labour philosophy andwas applied widely and rigorously in the early partof this decade. Recently, there has been someretreat from strong central direction fromWestminster. One signal of this has been thedecision to remove ring-fencing from SupportingPeople – the £1.7 billion programme aimed atsupporting vulnerable people in their own homes.
5 Care provision in the UK

Older care clients living at home were among themain beneficiaries from this programme.
For long-term care, the Department of Healthand devolved administrations have tried tointroduce a more uniform charging structure withintheir jurisdictions. This reduces local authorities’freedom to design their own charging policieswhich was granted to them under the 1948National Assistance Act. To illustrate how theseideological and practical differences across theadministrations have real effects, Table 3 showssome recent data on the structure of care indifferent parts of the UK. The statistics should beinterpreted as being broadly indicative rather thanprecise because of differences in the way thatcare statistics are collected across England,Scotland, Wales and Northern Ireland. Inparticular, the different approaches taken tomeasuring home care provision make theinterpretation of data relating to this topicproblematic.
The first row of Table 3 shows that a very highproportion of care home places are provided bythe independent (private and voluntary) sectorthroughout the UK. Northern Ireland has thehighest proportion of independent care homes,while Wales has the lowest share. There has been
a general policy preference towards a ‘hotel’model of residential care, and an acceptance thatthis implied increased scale – with around 40clients widely perceived as an appropriate size.The private sector has easier access to capitaland has therefore been in a better position tobuild homes that provide attractive environmentsand meet regulatory requirements. Therefore thebalance has shifted towards care homes ownedby the private sector.
Northern Ireland also has the highest shareof care home places per thousand populationaged 65+. This may reflect its higher level of percapita funding, higher levels of disability andcurrent or historic preferences over careprovision. England has by far the largest numberof domiciliary care clients aged 65+ whose caseshave been reviewed by local authorities. Thissimply reflects its much greater population: 83per cent of all UK citizens aged 65+ live inEngland. On a per capita basis, Northern Irelandhas the largest number of older clients receivinglocal authority home care, followed by Scotland,Wales and finally England. This does not tell thewhole story: in Northern Ireland, residential care ismore commonly used for clients with personalcare needs. Of the 21,400 clients receiving
Care provision in the UK 21
Table 3: Balance of care
England Scotland Wales Northern Ireland
Share of independent sector(care home places) (%)
83.0 81.0 77.4 93.0
Care home places per 1,000,population 65+
43 44 46 49
Number of older LA domiciliarycare clients
471,000 68,759 41,496 21,420
LA home care per 1,000aged 65+
58 81 78 88
Total home care per 1,000aged 65+
70
Direct payments hourly rate £8.87 £9.70 £6.74 £7.82
Private purchases of domiciliarycare (£m)
1,460 34
% of LA home care contractedout to independent sector
81 36 52 51

domiciliary care in Northern Ireland, only 5,600are receiving intensive home care. Compare thatwith Scotland: following the introduction of freepersonal care in 2002, there has been asignificant shift away from care home provisiontowards greater provision in clients’ own homes.Thus, for each older person receiving personalcare in a care home in Scotland at the start of2009, there were 4.7 individuals receivingpersonal care at home. When the policy wasintroduced at the beginning of 2002 there wereonly 3.4 individuals receiving personal care athome for each care home client receivingpersonal care. This is a very significant shift inthe balance of care. But the Scottish legislationthat introduced free personal care merelyprohibited local authorities from charging; it saidnothing about the balance of care. The impetustowards changing the balance of care towardscare at home began before devolution, but wascarried forward by the Care Development Group,which was commissioned by the ScottishExecutive after devolution to consider thefeasibility of introducing free personal care.
The definition of what constitutes a carepackage differs between Scotland and NorthernIreland. But in both, a high proportion of clientsreceive personal care and there is therefore asignificant overlap between the types of client. Thedata therefore suggests a substantial difference inthe balance of care between care homes anddomiciliary settings between Scotland andNorthern Ireland, with a greater proportion ofpersonal care being delivered at home inScotland.
Northern Ireland also has an extensive homehelp service. In 2006/7, 19,600 older clientsreceived a home help service. Such services havelargely disappeared in Great Britain, with localauthorities tending to provide services only tothose with substantial or critical needs. InEngland, around 73 per cent of councils only offerhome care services to those with ‘substantial’ or‘critical’ care needs (UKHCA, 2009). In Scotland,the total number of local authority social careclients fell by more than 3,000 between 2004 and2009. In 2004 at least 50 per cent of this groupwere receiving personal care; by 2009 this sharehad risen to 69 per cent.1
The proportion of those aged 65+ receivinghome care services is slightly lower in Wales thanin Scotland and considerably lower in England.This does not tell the whole story, however. While471,000 clients received home care packagesin England in 2007/8, just over one million ofthose aged 65+ had some interaction withcommunity-based services such as day care,meals and equipment and adaptations. Becausestatistics are not collected on the same basis inthe rest of the UK, it is not possible to make directcomparisons.
Nevertheless, the lower proportion of thoseaged 65+ receiving home care packages fromlocal authorities, shown in Table 3, may explainthe substantial expansion of the private home caremarket in England. The Commission for SocialCare Inspection (2009) estimated that 150,000clients in England buy domiciliary care privately,slightly more than the 146,000 who pay their carehome fees privately. Little is known about privatepurchasers of home care in Wales, Scotland andNorthern Ireland. UKHCA (2004) estimatessuggested that in Scotland in 2004, 16,000weekly care hours were purchased independentlyby clients, accounting for only 3 per cent of totalcare hours purchased that year. As in England,these hours may be used to replace serviceswhich local authorities are no longer prepared toprovide. But the scale is much larger in England.If private clients in Scotland purchased carepackages half as large as those being given to theaverage Scottish local authority home care clientreceiving personal care, there would only be2,800 such clients – less than 2 per cent of thenumber in England. While there is no data onexpenditure of clients in Wales and NorthernIreland, Wales has fewer than half as manyindependent home care providers as Scotlandhas, while Northern Ireland has less than 13 percent of the Scottish total. This suggests that themarket for private purchases of home care forolder people is much more developed in Englandthan in Scotland, Wales or Northern Ireland. Thismay reflect greater ability to pay in England, asalready discussed. It might also reflect strongerpreferences for home care in England. Finally,it may be a reflection of the differences ingovernment funding to the constituent parts of
Care provision in the UK22

the UK, with less pressure on local authoritiesin areas that are generously funded to withdrawfrom non-critical home care.
The last row in Table 3 shows the proportionof home care commissioned by local authoritieswhich is contracted out to independentsuppliers – charities and private providers. Again,there is a substantial contrast between Englandand the rest of the UK. Voluntary and privateproviders now supply 81 per cent of publiclyfunded home care in England, compared with5 per cent in 1993. This is a much higherproportion than in Wales and Northern Ireland,where independent suppliers provide just over52 per cent of state-funded home care. InScotland the share of independent provision iseven lower, with only 36 per cent of home caresupplied by independent providers in 2008, whilea further 11 per cent of provision involvedcombined working by local authorities and thevoluntary or private sectors. The low proportionof independent provision in Scotland may beindicative of political and staff resistance to privatesector care provision at home.
The evidence thus suggests that there aresignificant differences in the primary care systemin different parts of the UK.
Key differences include:
• the balance between home care and carehome provision;
• the ability of clients to design their own carepackages;
• the balance between care provided by thepublic sector on the one hand and theindependent sector on the other.
In the next chapter, we discover how some ofthese differences have emerged in relation to carepolicies that have been introduced in differentparts of the UK.
Care provision in the UK 23

Long-term care policy since devolution24
In this chapter we examine a number of cross-cutting themes in relation to long-term care forolder people and devolution. The first of these isfree personal care, which has not only had majorsignificance for the care of older people, but hasalso been one of the major policy divergencesresulting from the first decade of devolution.
Free personal care
The Royal Commission on Long-Term Carerecommended that personal care should be freeto those assessed as in need of such care. Itsrecommendation coincided with the establishmentof devolution. Since social care policy came underthe control of the devolved bodies, each of thesehad to determine whether to take this proposalforward. As we shall see, the results are quitediverse: though politically appealing, free personalcare has only been introduced in Scotland. In thissection, we examine the history of this policy ineach part of the UK. We start with Scotland.
ScotlandFree personal care for those aged 65+ wasintroduced in Scotland in July 2002 through anAct which prevented local authorities fromcharging for personal care. It had the support ofall of the major political parties and was stronglysupported by older people’s advocacy groups. Itshistory has been somewhat troubled, but it hashad a major impact on care provision in Scotland.It has also had a number of unintendedconsequences, some of which provide usefullessons for other parts of the UK. It has been thesubject of a major review (Scottish Government,2008), led by Lord Sutherland. It now has almostunanimous political support within Scotland. Thismay partly be because free personal care is notonly valued in its own right, but it is also perceivedas one of the best examples of how devolutionhas ‘made a difference’. Prior to its introduction,the support of the Labour Party was more
equivocal. Its eventual support for the policy waspartly driven by the need to maintain its coalitionwith the Liberal Democrats who were stronglycommitted to free personal care. We now examinesome aspects of the policy, including itsunintended consequences, having already dealtwith the issue of Attendance Allowance in Box 1.
Understanding of the policyThroughout its existence, understanding of thefree personal care policy has been limited. This istrue of the media, clients and carers. Themisapprehension has extended throughout theUK. Its most extreme version is that all social carefor older people in Scotland is free. In reality,accommodation charges are still charged in carehomes, using broadly the same means test thatapplies in the rest of the UK. Therefore, those onmedium or high household incomes may have toreduce their financial assets or housing equity topay for care. Non-personal care provided at homeis charged for, again using charging regimes thatdiffer little from those in the rest of the UK.
Allocations to local authoritiesEngland, Wales and Scotland have complexmechanisms to distribute funding from centralgovernment or the devolved bodies to localauthorities. In Northern Ireland, the range of localauthority functions is more limited, and thereforethe allocation mechanism is simpler. Localauthorities were compensated by the ScottishExecutive for loss of charge income when freepersonal care was introduced. But calculation ofthis loss was complex. Allocation mechanismstend to be weighted towards extra provision inareas of deprivation or in very rural areas. But theintroduction of free personal care meant that localauthority income fell most in relatively affluentareas. In poorer areas, funding had already beenincreased to pay for those who were unable tocontribute towards their care costs and thereforedid not benefit from free personal care. Thus the
6 Long-term care policysince devolution

allocation mechanism should have been biasedtowards higher-income authorities. Initially noseparate calculation for free personal care at homewas made, leaving some more affluent localauthorities arguing that the policy was underfunded(see, for example, East Renfrewshire, 2007).
Some local authorities had already movedtowards free personal care before 2002 byreducing or eliminating charges. These authoritiesthus had already absorbed the costs of the policybefore it was introduced and therefore found itrelatively easy to implement. Others had made nomove in this direction and found it much moredifficult to fund.
Variations in costsThe estimates of costs produced by the ScottishExecutive showed huge variation across localauthorities. Audit Scotland’s review of freepersonal care (2008) argued that local authoritieshad been given insufficient guidance to accuratelycost free personal care. Estimates of the percapita annual cost of free personal care at homevary widely across local authorities. AuditScotland’s revised cost estimates and thequarterly monitoring data collected by the ScottishGovernment suggest that in 2005/6, per headcosts varied by a factor of six across localauthorities. Argyll and Bute’s annual cost was£6,650 while that in Angus was £1,100. Theaverage for Scotland as a whole was £2,800. Thisis a huge variation in costs and well beyond whatone might expect from, say, variations in transportcosts. Given that service delivery is in the hands ofthe local authorities, the Scottish Government haslimited powers to reduce cost variation. It has,however, set up the Joint Improvement Team(2009), which is charged with improving jointworking between local health and social carepartnerships and so indirectly should exertdownward pressure on costs.
Single Outcome AgreementsThere is no ring-fencing of funding associated withthe free personal care policy. Instead localauthorities and the Scottish Government nowindividually agree Single Outcome Agreements(SOAs). These commit the local authority toactions that support the Scottish Government’s
overall strategy, but are the outcome of bilateralnegotiations. Thus, in some agreements, olderpeople’s issues may play a central part, while inothers such issues are peripheral. This contrastswith the more target-led culture in English localauthorities which embody much more centraldirection. The design of the SOAs naturally leadsto concerns that older people’s issues will playonly a minor role in local authority prioritiesbecause the National Performance Framework onwhich the SOAs are based only includes twoaspirations in relation to older people. These areto reduce the number of emergency inpatientadmissions and to increase the proportion withcomplex care needs who are cared for at home.
Unmet needThere was a substantial increase in demand forpersonal care shortly after the policy wasintroduced. This was not anticipated by the CareDevelopment Group. The number receiving freepersonal care at home rose from 26,000 in 2002to 44,000 in 2008. But the overall number ofhome care clients drifted slightly downwards to66,000 over the same period. Thus, many fewerclients now receive non-personal care fromScottish local authorities. Clients who wouldpreviously have received non-personal care fromthe local authority may now be purchasing suchcare elsewhere. There are many unsubstantiatedreports of clients asking for their free personalcare from the relevant local authority, whilepurchasing other components of their care fromthe private sector.
Local authority provision of personal care athome and AA/DLA are both addressed at clientswith personal care needs. We have shown thatthe AA/DLA client base is around five times largerthan the local authority client base, and thatAA/DLA claims in all parts of the UK, includingScotland, have increased somewhat during thisdecade. But the growth has been slower than theincrease in demand for free personal care at homein Scotland provided by local authorities. Theincrease in home care clients in Scotland seemsto be a response to previously unmet need fromclients who were assessed as requiring personalcare by local authorities. Although there was not asimilar proportionate rise in AA claimants, the
Long-term care policy since devolution 25

increase in local authority provision may haveoccurred because some clients who werereceiving AA but not local authority personal carewere given assessments which indicated that theywere entitled to receive local authority care. Thisillustrates the importance of the assessmentmechanism in determining eligibility for servicesthat are free at the point of delivery.
Care boundariesWhenever a service is provided free, disputes arelikely to arise both over the definition of the serviceand over eligibility for free provision. WithScotland, the key issue turned out to be foodpreparation. Local authorities claimed thatScottish Executive guidance on the circumstancesin which food preparation constituted personalcare was unclear, and they did not wish to risklitigation by taking a narrow view of eligibility.Following recommendations in the SutherlandReview of 2008, discussions between the ScottishGovernment and the Convention of Scottish LocalAuthorities (COSLA) resulted in the passing of aregulation (Scottish Statutory Instruments, 2009)which precisely specifies the nature of foodpreparation. Devolution has provided powers notonly to legislate in Scotland, but also to amendlegislation relatively easily.
Treatment of those aged under 65Eligibility for free personal care in Scotland isage-dependent. Those aged under 65 who areassessed as being able to contribute to the costsof care continue to be charged. Only those aged65+ receive free personal care. This has yet to bechallenged in the courts on the grounds of agediscrimination. If it were successfully challenged,there would be significant cost implications for theScottish Government. Evidence from Walessuggests that those aged under 65 tend to havemore complex care needs and are less able tofund their care.
WalesThe Welsh Assembly initially took a cautiousapproach to free personal care. But in 2003, theLabour Party manifesto for the Welsh Assemblypledged to introduce free domiciliary care servicesfor disabled people in Wales. Following this
commitment, in 2004, an expert group – the FreeHome Care for Disabled People Task and FinishWork Group (FHCTG) – was convened to consideroptions for implementation. This group examinedthe definitions of disability and types of servicethat might be eligible under the scheme. Thedefinition of domiciliary care was closely aligned tothe definition of personal care used in Scotland.Following this report, the Minister for Health andSocial Services announced that a final schemewould be released in 2006/7.
Local authorities in Wales have a statutoryright to charge for domiciliary care. Until recently,the Welsh Assembly Government did not have thelegislative powers necessary to set aside this rightexcept for the first six weeks. It could, however,try to persuade local authorities to stop chargingby reimbursing them for loss of charge income.
Research commissioned by the AssemblyGovernment (Bell, 2006) provided estimates offuture costs of free domiciliary care in Wales.These costings reflected higher levels of disabilityin Wales and the additional costs of providing freecare for those aged under 65. Wales is not asgenerously funded in relation to its level of needthrough the Barnett formula as is Scotland. Theadditional costs thus provided a significantchallenge to the Welsh Assembly’s budget. Thesecosts were forecast to increase substantially overtime as a result of demographic change.
The Assembly Government thereforeinvestigated alternative ways of reducing chargesto personal care clients in Wales. In 2006, itproposed an alternative scheme (Welsh AssemblyGovernment, 2006), which was specificallytargeted at those on modest incomes. Specifically,it increased the ‘buffer’ above Income Supportlevels from 25 per cent to 35 per cent beforecharges are made. This allowed those on incomesjust above Income Support levels to retain agreater share of this income. More affluent careclients would be unaffected by this measure andwould therefore continue to pay charges. The fullpackage included additional support for carers,greater provision of equipment and expansion oftelecare.
The Welsh experience is therefore quitedifferent from that in Scotland. Concerns overcosts and scarcity of resources led to a quite
Long-term care policy since devolution26

different policy from that envisaged by the RoyalCommission. Rather than treating personal careas equivalent to NHS provision, i.e. free at thepoint of delivery, the Welsh Assembly focusedassistance on those of modest means who pay amuch larger proportion of their income in chargesthan more affluent clients.
Northern IrelandPrior to devolution, care home clients in NorthernIreland were expected to contribute to the costsof personal care, subject to a means test. Thosereceiving care at home did not have to pay fortheir personal care; this was a more generousprovision than elsewhere in the UK. But, as wehave already seen, numbers receiving domiciliarycare in Northern Ireland were relatively low.
In 2001, the Northern Ireland Executivecommissioned a group to examine the costs ofintroducing free personal care. The Assembly wassuspended before the analysis was complete.Ministers were unwilling to take a decision duringthe period of direct rule, arguing that such adecision should be taken by a locally electedExecutive.
The Northern Ireland Assembly voted in favourof providing free personal care in 2007. Followingthis vote, it set up a review of the costs andbenefits of introducing free personal care inNorthern Ireland. The review argued that arelatively small number of clients would benefitfrom free personal care. This is partly because thecare needs of 70 per cent of care home clients inNorthern Ireland are fully funded by the state,reflecting the relatively low incomes of NorthernIrish pensioners, as mentioned previously.Accommodation charges are means-tested as inthe rest of the UK. Data on residents in privatecare homes is not collected systematically inNorthern Ireland. But the review estimated thatthere were around 1,600 such residents and afurther 1,900 self-funding residents that wereknown to the HSCs. However, based on estimatesof the weekly costs of personal care in carehomes, which were close to the estimates used inScotland, the review estimated that 1,900 self-funders and 230 residents who are part-funded bythe Northern Ireland Executive would benefitfinancially from the introduction of free personal
care. Just over a quarter of care home residents inNorthern Ireland would be better off as a result ofthe introduction of free personal care.
The review concluded that the relatively smallnumber of beneficiaries made it difficult to justifythe estimated initial cost of £30 million, whichwould rise to £45 million by 2026. In May 2009,the Northern Ireland Health Minister, MichaelMcGimpsey, announced that he would not beable to introduce free personal care in NorthernIreland for cost reasons.
Thus, both in Wales and Northern Ireland,initial political support for free personal care waseroded when the cost implications of the policywere analysed. This does illustrate that, even witha fixed budget, devolution has made localpoliticians accountable for the choices they make.In both areas, organisations that support theneeds of the disabled have made theirdisappointment very clear to the politicians whodecided not to proceed with free personal care.
EnglandIn its response to the Royal Commission onLong-Term Care, the Department of Health (2000)argued that making personal care free for everyonewould carry a very substantial cost and that it doesnot help the least well-off. They therefore rejectedits recommendation that personal care should befree, subject to assessment of need. Unlike inScotland, Wales and Northern Ireland, the policyof free personal care never commanded sufficientsupport in the major political parties to make itsintroduction in England likely.
Nevertheless, in all recent evaluations oflong-term care funding in England, free personalcare is invariably one of the options considered.For example, the Wanless Review (King’s Fund,2006) analysed current and potential future costsof free personal care alongside the ‘partnership’model which provides people with a free minimumguaranteed amount of care set at around two-thirds of a benchmark care package. Individualscan then contribute towards the cost of theirpackage with match-funding from the Governmentuntil the benchmark care package is achieved.Those on low incomes who could not contributewould receive state funding to pay for thebenchmark package. The partnership model is
Long-term care policy since devolution 27

preferred to free personal care in the WanlessReview, largely on the grounds of cost.With free personal care, the state has to provide78 per cent of total costs compared with justover 71 per cent in the partnership model.
The report also argues that both thepartnership and free personal care modelsundermine the logic of AA and DLA, and that thesebenefits might largely be discontinued. Clearly,should this come about, there would be significantimplications for the devolved nations, who mightwish to implement a different mechanism forfunding long-term care. They might be forced toaccept changes in the secondary care system as aresult of the introduction of, say, the partnershipmodel. This could undermine the funding basis oftheir long-term care policies, thus questioning theability of the devolved nations to follow a radicallydifferent approach to that in England.
A final aspect of the process of examining thecosts and benefits of free personal care is therelative size of the resources that each part of theUK has devoted to its evaluation. England’srelative size means that it can absorb the fixedcost of large-scale policy evaluations relativelyeasily. Scotland, Wales and Northern Ireland haveto design policy based on much more meagreanalytical resources. The same disparity inanalytical power has been evident in the next topicthat we discuss – the drive towards giving clientsgreater control over the care they receive.
Personalisation
In recent years, many industrialised countries havegiven disabled people greater control over theservices that they use. In the UK, direct payments(also described as self-directed care) haveincreased client control over care provision byallowing them to choose among care providers.The move towards personalisation began beforedevolution with the 1996 Community Care (DirectPayments) Act which allowed local authoritiesthroughout the UK to offer direct paymentsinstead of services. The devolved bodies havetherefore been able to control the rate at whichpersonalisation was introduced: they couldinfluence local authorities’ priorities and provideresources to meet implementation costs such as
training and arrangements for monitoring andmanagement. These costs are relatively greater inScotland, Wales and Northern Ireland because oftheir smaller scale than England.
In England there has been a sharp increase inthe number of clients receiving direct paymentssince 1997. But take-up in the devolved nationshas been much slower. This cannot be easilyexplained by differences in the regulatoryframework. In April 2003 regulations were put inplace requiring councils in England to offer directpayments to all people using community careservices.
Similar guidance was introduced in Scotland in2003, and then updated in 2007. The legislativecompetence for this guidance came from theSocial Work (Scotland) Act 1968. Anotherimportant input into the 2007 regulations was thereport of the Scottish Parliament HealthCommittee (2006) which stated that:
The Committee supports the concept of directpayments as a means of increasing theautonomy of those who receive them as wellas enabling care packages to be tailored moreclosely to their needs. Whilst not a solution foreveryone, they have the potential to improvethe care available to many and the Committeewishes to encourage the increase in theirtake-up.
The report also stressed the need for theguidance to encourage clear commitments fromlocal authorities to improve take-up. Thus, partlyas a result of this report, the 2007 guidanceproposed that local authorities should fund:
• independent, user-led, local support services;
• training for individuals making use ofself-directed support, including personalassistants;
• appointment of self-directed support leadofficers within each local authority;
• training on self-directed support for caremanagers, finance managers and localauthority directors.
Long-term care policy since devolution28

In England, Putting People First (Department ofHealth, 2007) marked a new commitment topersonalisation of adult social services.It embodied a new vision for the future of careservices:
The time has now come to build on bestpractice and replace paternalistic, reactive careof variable quality with a mainstream systemfocused on prevention, early intervention,enablement, and high quality personallytailored services. In the future, we want peopleto have maximum choice, control and powerover the support services they receive.
(Department of Health, 2007, p.2)
Putting People First introduced the concept ofpersonal budgets, which could be taken in theform of a direct payment or by asking the localcouncil to commission the service. A furtherextension was the introduction of individualbudgets, which cover a larger group of fundingstreams such as Supporting People, IndependentLiving Funds etc. First proposed in 2005, thesewere piloted across 13 councils in England by theIndividual Budgets Evaluation Network (IBSEN),which was based at five leading universities. A keyfinding of the evaluation was that, though somegroups reacted positively to individual budgets,older people were more likely to suggest thattaking control of their support was burdensome.
One aspect of this approach to policyformation is that it helps develop policy evaluationcapacity in English universities. With a lesswell-resourced approach to policy formation,universities in the devolved nations are unable toprovide such high quality policy analysis.
In Scotland, regulations for direct paymentswere introduced in June 2003. The duty to offerdirect payments was extended to all persons aged65+ assessed as needing a community careservice because of infirmity or old age. Unlike inthe rest of the UK, carers in Scotland were notoffered direct payments for their own services(Carers UK, 2009). In Wales, similar measureswere established in March 2005 (Welsh AssemblyGovernment, 2004). In Northern Ireland, theCarers and Direct Payments Act (Northern Ireland)2000 extended direct payments.
The extension of personalisation has been veryuneven across the UK. This was illustrated byRiddell et al. (2006), who conclude that by 2003the take-up of direct payments in England wastwice as high as in other parts of the UK. Theyprovide a number of explanations, including theeffectiveness of local disability advocates, fundingfor policy development, political culture, the supplyof social care and the appropriateness ofinfrastructure.
Before mandatory duties were placed on localauthorities, local interpretations of policy were animportant influence on direct payment provision(Priestley et al., 2006). Some local authoritieslacked the capacity to implement national policies.The smaller scale of the local authorities in thedevolved nations may have impeded their ability toimplement new policy initiatives. But also therewas local resistance to direct payments,particularly in Scotland. This may have come fromlocal politicians, managers or front-line staff(Priestley et al., 2007) and may stem from agreater commitment to collectivism and loyalty tothe welfare state in Scotland (Keating, 2003).
The resources and training allocated topersonalisation inevitably affect take-up. Smallerlocal authorities have more difficulty in absorbingthe fixed costs of implementation. Resourcesallocated to training varied widely across localauthorities. Training was vital given the novelty ofthe service and the large number of issues thathad to be resolved before an effective and efficientservice could be delivered. There is also evidenceof wide variation in the effectiveness of this training(Davey et al., 2007).
Recent data from Scotland and Englandshows a marked increase in take-up in recentyears. Between 2004 and 2009 the number ofself-directed support payments in Scotland morethan doubled. However, this data covers alladults, rather than those aged 65+. Similarly,Wales and Northern Ireland do not publish data onthose direct payments that are specificallydirected at those aged 65+. Only Englandpublishes data on direct payments by age group.
Personalisation posed a different challengethan did free personal care to the devolvedadministrations. Though it represented a majorchange in the philosophy of care provision, it did
Long-term care policy since devolution 29

not require legislative change. Rather, the issuewas the willingness of the administrations and localauthorities to prioritise personalisation. The 2007manifestos of the Labour Party, Liberal Democratsand Conservatives in Wales and Scotland did nothighlight personalisation. Only the Scottish NationalParty alluded to this issue, with a commitment tointroduce individual budgets. The generalimpression is that politicians in the devolved bodiesare lukewarm to the personalisation agenda andthat this has impeded its relatively slow extensioncompared with England.
Charging
All UK local authorities have the legal right to setcharges for long-term care under the 1948National Assistance Act. Differences in chargesbetween local authorities are criticised on thegrounds of both complexity and equity. TheDepartment of Health in England and the devolvedadministrations can issue guidelines to ensureconsistency of charging.
The broad principles of charging are commonto most local authorities, but details may differsignificantly. Thus, charges are generally based onability to pay rather than cost. The chargingprocess must therefore be based on anassessment of clients’ financial circumstances.The assessment of capital has an important role indetermining whether charges are levied at all.
If capital exceeds some limit, charges are setso that a client retains a minimum level of income.For those living at home, this minimum may reflectthe value of Income Support. To this is usuallyadded a ‘buffer’, set at a percentage of theseminimum income levels. This is ‘guaranteed’income. The person’s ‘assessable income’ wouldbe any income that exceeds the guaranteedincome. Charges are only levied against the‘assessable’ component of this income.
Charging for care is highly complex. For manyyears, local authorities determined chargeswithout reference to national guidance. But as thecosts and volume of care increased, the desire ofthe devolved authorities and the UK Governmentto have greater consistency has led to morepressure being put on local authorities to aligntheir charging policies.
For example, the Welsh Assembly Governmentissued statutory guidance on charging policy inJuly 2002. Fairer Charging Policies for Home Careand Other Non-Residential Social Services (WAG,2002) sets out a framework for ‘reasonable’charging policies. It considered issues such asmaximum charges, buffers, minimum residualincome and savings limits. When the WelshAssembly decided not to go ahead with the policyof free personal care, it partly offset the negativeimpact of this decision by increasing its grant tolocal authorities to allow them to reduce charges todomiciliary clients. Specifically, it increased the‘buffer’ so that a substantial number of less affluentclients would no longer have to pay charges.
In Scotland, guidance tends to come fromCOSLA. Thus, in January 2006, COSLA sent acircular letter to local authorities which was carefulnot to be seen to be interfering with localauthorities’ power to determine charges. It statedthat:
The Guidance does not take the form ofnational prescription. It provides a frameworkthat aims to maintain local accountability anddiscretion while encouraging councils todemonstrate that in arriving at charges theyhave followed best practice.
Although personal care is free at home in Scotland,councils can and do charge for day care, lunchclubs, domiciliary services, including meals onwheels, wardens in sheltered housing, communityalarms, laundry services, aids and adaptations.As council budgets have tightened, these chargeshave tended to increase significantly. This hasbeen understandably unpopular with clients. Forexample, the increase in charges for such servicesin Fife from £4 to £11 per hour in 2008 wascredited with having an impact on the Glenrothesby-election (The Courier, 2008).
In Northern Ireland, care is primarily deliveredby HSCs. No charges are made for domiciliarycare. As mentioned earlier, the balance of care inNorthern Ireland is weighted more towards carehomes than in other parts of the UK. Care homecharges are determined in a similar way to otherparts of the UK. Savings limits in Northern Irelandare the same as those in England.
Long-term care policy since devolution30

In England care charges are set by localcouncils, but should comply with the FairerCharging guidelines (Department of Health, 2003).As in the rest of Great Britain, local authorities inEngland have some autonomy to set their owncharges. There are ongoing concerns overdifferential charges across local authorities.Differences in policy priorities and views abouthow progressive charging should be, may partlyexplain some of these differentials, but they alsoreflect differences in local authorities’ financialsituations. These partly indicate the extent towhich central government grants accurately reflectlocal needs in each authority across all categoriesof spending. Unexpected overspends in otherparts of the local authority budget, including socialservices, may force local authorities to increasecare charges to older people.
Across the whole of the UK, care charges toolder clients are determined by an uneasy mixtureof local autonomy and central direction. Carecharges are widely perceived to be unfair in thatthey fall most heavily on those of modest meanswho are unlucky enough to require complexpackages of care, either at home or in aresidential setting. The two major impacts ofdevolution have been the removal of charges forpersonal care in Scotland and the changes to thestructure of charges in Wales as compensation fornot introducing free personal care.
While there has been pressure to reduce thevariability of charges across local authorities, thereis no enthusiasm for taking responsibility forcharging away from local authorities in eitherScotland or Wales. This may be a politicalcalculation, given the unpopularity of carecharges. But it would also remove local authorityfreedom to adjust charges in the light of their ownfinancial circumstances and so would furtherweaken the accountability of local government.
Relationship between localauthorities and devolved bodies
As implied by the previous discussion, therelationship between local authorities, devolutionand long-term care for older people is highlycomplex. This stems from (1) the legislative dutyon local authorities to provide social care and
from (2) the tension between national uniformityand local autonomy in assessment, deliveryand charging.
Devolution has added a new layer to thiscomplexity. Devolved authorities can establish adifferent working relationship with their localauthorities from that which exists between Englishlocal authorities and Westminster. For example, asmentioned previously, the SNP introduced anoutcomes-based governance model, the NationalPerformance Framework, in 2007 (ScottishGovernment, 2009a). Its constituent parts are asingle government Purpose, five StrategicObjectives, 15 National Outcomes and 45 NationalIndicators designed to track progress.Performance against these in relation to olderpeople is calibrated on the ‘Scotland Performs’website (Scottish Government, 2009b), and theSOAs ‘set out how each will work in the futuretowards improving national outcomes for the localpeople in a way that reflects local circumstancesand priorities’.
The effectiveness of joint working betweenhealth authorities and local government is alsoimportant for long-term care delivery. Healthauthorities are typically not elected. They have lessdemocratic legitimacy and therefore are less ableto contest policy initiatives from the devolvedbodies. This is important in Northern Ireland, wherelocal authority powers are much more limited thanin the rest of the United Kingdom and long-termcare for older people is delivered by HSCs.
Laffin et al. (2002) argue that the establishmentof the Welsh Assembly has not restricted localgovernment autonomy in Wales. As with itsequivalent, COSLA in Scotland, the WelshAssociation of Local Government (WLGA) hasdeveloped new policy networks as a result of theestablishment of the Assembly. Such networkscould potentially improve long-term care delivery.This reflects the benefits of the relative smallnessof the devolved authorities: it is easier to agreepolicy innovations when there are a small numberof parties involved. It is much more difficult inEngland where there are not only a large numberof local authorities but a complex structureinvolving metropolitan districts, shire counties andunitary authorities as well as the London boroughs.
Long-term care policy since devolution 31

Long-term care policies across the UK32
This chapter looks at the extent to which changesin long-term care policy are constrained orenhanced by the creation of the devolvedadministrations.
Social security
The UK has two care systems that are largelyfunded by the state. The primary system is largelyfunded by local government; the secondarysystem is paid for by DWP. In the devolvednations, local government is the responsibility ofthe respective administrations. Suppose that a UKgovernment wished to instigate a major reform ofwelfare benefits, including AA and DLA. Thiswould result in significant political difficulties underthe current structure, because changes to welfarebenefits might have implications for care provisionvia local government. Clearly this would involvesome mechanism for co-operation across the UK.Such a mechanism does in theory exist. The JointMinisterial Council was set up in 1999 ‘for thedevolved administrations to be involved by the UKGovernment at ministerial level when they considerreserved matters which impinge on devolvedresponsibilities’ (Scottish Executive, 1999). Inpractice, meetings of this committee have beenrelatively rare though they were revived in 2008.As yet, none of them have focused on social care,which clearly constitutes one of the mostimportant interactions between devolved andreserved matters in terms of both social welfareand fiscal sustainability.
Thus, for example, the StreamlinedAssessment Project (StAP) approach arose out ofUK government policy to ‘meet the challenges ofageing in the 21st century’ (Hilton, 2008). Itinvolves joint assessment of eligibility for AA andfor local authority social care. In the interests ofefficiency, it is sensible to streamline assessmentprocedures. All of the pilots for this project havebeen carried out in England. Assessment
procedures for the primary care system aredifferent in Scotland, Wales and Northern Ireland.
Funding mechanisms
The first decade of devolution has coincided witha benign public expenditure climate. While therehas been some dissatisfaction with levels offunding in the devolved nations, the decade has infact witnessed an unprecedented increase in thereal value of public expenditure across the UK.However, it has been clear for some time that thefinancial arrangements that currently underpindevolution are difficult to justify on grounds ofequity and have no international parallels.
Thus, and for different reasons, Wales andScotland have separately set up commissions toinvestigate the existing funding structure andsuggest alternatives. The IndependentCommission on Funding & Finance for Wales (theHoltham Commission) recently reported on theadvantages and disadvantages of the Barnettformula to Wales, and on possible alternativefunding mechanisms, including tax varying andborrowing powers (Independent Commission onFunding & Finance for Wales, 2009). Similarly, theCommission on Scottish Devolution (the CalmanCommission) examined the provisions of theScotland Act 1998 to determine if there was away to improve the financial accountability of theScottish Parliament within the United Kingdom.Developments such as these suggest thatdevolution should be regarded as a process,rather than an event. It is unclear where thisprocess may go, and at what speed.
Changes in the powers of the devolvedadministrations will mean further changes torelationships with Westminster ministries. Theirsuccess will therefore be contingent on goodwill inWestminster, which has not always been present,perhaps partly because these Westminsterdepartments are not compensated for the costs ofdealing with the devolved administrations.
7 Long-term care policiesacross the UK

Both commissions emphasise autonomy,equity and accountability as desirable featuresof any revised funding arrangements. Onemechanism for increasing autonomy andaccountability would be to confer tax powers fromLondon to Edinburgh and Cardiff. The CalmanCommission has proposed that the ScottishParliament retains around half of income taxrevenue and makes an explicit decision about theincome tax rate required to generate this revenue.(Commission on Scottish Devolution, 2009). Interms of long-term care, this would openopportunities to use either general orhypothecated taxes to fund long-term care, as isthe case in Germany and Japan.
However, the Calman Commission acceptedthat social security would continue to be availableon a uniform UK-wide basis. Thus, even ifScotland used additional tax-raising powers tofund long-term care, state support for care forolder people would still be partly provided byWestminster through AA and DLA. Since neitherthe Holtham nor the Calman Commission appearswilling to contemplate devolving social security, itseems likely that, for the foreseeable future, theprimary and secondary sources of support forlong-term care will continue to exist. Inevitably thisraises questions around whether this is an efficientuse of public resources when the two systemshave very limited joint communication. Whilegeneral principles of equity suggest that the socialsecurity system should be uniform across the UK,these efficiency arguments are perhaps too readilydismissed and might well be worth revisiting.
Our analysis of the structure of long-term careprovision in different parts of the UK suggests thatthere are relative differences in the demand forcare. These stem from differences in agestructure, healthy life expectancy and unpaid careprovision etc. But the Barnett formula, as we havepreviously described, is not responsive todifferences in need. In Wales, England andScotland, allocation mechanisms for funding localauthorities and health authorities do respond toindicators such as numbers of older people. Butthe mechanism which determines the overall grantby the Treasury to Scotland, Wales and NorthernIreland does not respond to differences in need.The Holtham Commission is likely to recommend
that a needs assessment should be undertaken,while the Calman Commission has accepted thatsuch an assessment may be necessary, thoughthis may well have negative effects on funding inScotland and Northern Ireland.
Political constraints
The UK has a very open and efficient mediaenvironment. Differences in the volume and qualityof public services across the UK are easilycommunicated. This creates difficulties forpoliticians who wish to emphasise constructingpolicy around local needs and aspirations, andhaving local accountability for these choices.
Similarly, aside from the nationalist parties, thepolitical structure of the UK is organised aroundthree major UK-wide parties, each of which isrepresented at the different levels of government.This inevitably causes tensions if a party wishes tofollow different policies at different levels ofgovernment. Thus, for example, the Labour Partyin Scotland has consistently supported freepersonal care since its introduction, whereas theUK Labour Party has argued that it is too costly,and also not sufficiently targeted at the poor.
These centralising forces make it difficult forthe devolved governments to introduce radicalpolicy initiatives. This is particularly true wherethere are significant funding consequences, giventheir almost complete dependence on a blockgrant from the UK Government. Aside from theissues that we have already discussed, such asthe UK-wide social security system, theimportance of pre-devolution legislation and thepolicy role of local authorities, the constraintsassociated with funding and the political culturealso inhibit the development of truly radicalapproaches to long-term care provision in thedevolved nations.
Long-term care policies across the UK 33

Conclusions and recommendations34
This report has looked at several different aspectsof the interaction between devolution and long-term care for older people in the last decade. It isevident that devolution has made a system thatthe public, politicians and clients found difficult tocomprehend even more complex. One of theprincipal reasons for confusion is the multiplicity ofagencies involved. The devolved institutions areresponsible for long-term care insofar as theylargely fund local authorities or, in the case ofNorthern Ireland, the Health and Social CareTrusts. These bodies provide the primary socialcare system that assesses and manages care forthose with assessed need. However, there is aparallel secondary system which provides cash tothose with care needs. They are assessed by adifferent mechanism and the client base is aroundfive times larger than that of the primary system.The secondary system is funded by DWP and isindependent of the devolved bodies. Finally, thereis a tertiary system associated with those whocannot, or do not wish to, access publiclyprovided care. In this system, clients, theirrelatives or friends pay for care privately or makeinformal arrangements to supply care. These threesystems interact, but these interactions are notwell understood. Their interdependence meansthat it is impossible to change the rules by whichone of them operates without having effects,sometimes unintended, on the others.
This poses a particular problem for devolutionbecause social care is one of the areas which isnot reserved to Westminster. But the socialsecurity system is reserved even though it includespayments to compensate for care needs –Attendance Allowance and Disability LivingAllowance. And because of the interdependencebetween the two systems, it is difficult to see howthese benefits could be altered without affectingthe funding of social care policy in the devolvednations. Indeed, this argument is implicitlyacknowledged, albeit weakly, in the recent GreenPaper on social care (HM Government, 2009).
In a paper of 132 pages, there is only one mentionof the devolved administrations. This is in relationto the possibility that moving funding from thesecondary to the primary system would affectpublicly funded care provision in the devolvednations. According to the Green Paper, thedevolved administrations may ‘choose to adoptthe new care and support system’ (p.104) that willbe implemented in England. Such treatment of thedevolved administrations tends to reinforcestereotypes held in Scotland, Wales and NorthernIreland that some of the Westminster ministries areunwilling to engage with the intricacies of thedevolution settlements.
The Green Paper is somewhat vague on whatthis system might be. But it does suggest thatthere will be further extension of client choicethrough mechanisms such as personal budgets.As we have seen, there has been much lessenthusiasm for this approach in the devolvednations than in England. Indeed, the whole pointof devolution was to allow different parts of the UKto formulate their own policies for a limited set ofpolicy areas, including social care. The sentimentsof the Green Paper seem at odds with this. Itdoes not reflect the possibility that the devolvedauthorities may have distanced their social carepolicy from that in England as a point ofprinciple – to demonstrate that devolution is ableto provide different policies from those in England.
The Green Paper makes it abundantly clearthat changes in the structure of the secondarycare system will be driven by the English policyagenda. This makes it difficult for the devolvedadministrations to embark on radical changes totheir own funding mechanisms. It is therefore notclear that the devolved nations can really pursuea wholly independent long-term care policy.Politicians in Scotland, Wales and Northern Irelandcannot afford to ignore the possibility of suchchange in designing long-term care policy.
For example, even if the devolvedadministrations are granted tax-raising powers,
8 Conclusions andrecommendations

it would be difficult to conceive how a Scottishadministration might operate its own long-termcare tax or insurance scheme unless it had greatercontrol over AA and DLA. But the CalmanCommission has explicitly ruled out the possibilityof varying the social security system across theUK. Paradoxically, it may be that the UKGovernment will be willing to consider suchvariation. This could happen if the implication ofthe Green Paper that greater alignment of theprimary and secondary care systems would bedesirable in England becomes part of UKgovernment policy.
What is clear is that there has been little jointlearning of social care policy lessons in the lastdecade. Although one could think of the UK nowbeing a ‘policy laboratory’, there do not seem tobe proper mechanisms where ideas andexperience can be transferred. Most importantly,the Joint Ministerial Committee mechanism doesnot seem to be functioning adequately. None of itsrelatively rare meetings have addressed the issueof social care, one of the most pressing policyissues currently facing the UK.
At a lower level, governmental evaluation andassessment of social care policy in the differentparts of the UK generally focus on England,Scotland, Wales and Northern Ireland separately.It is only charities, such as the Joseph RowntreeFoundation, that attempt to take a widerperspective. Understandably, the resourcesallocated to policy evaluation in Englandsubstantially exceed those deployed in the rest ofthe UK. This means that there is much lessevaluation capacity in the devolved nations. Thereis possibly a role for the Economic and SocialResearch Council, which has significantly moreresources than the charitable researchorganisations, to take a lead in enhancingknowledge exchange and capacity-building inrelation to social care policy across the UK.
Our research has indicated that there aredifferences in the demand for long-term care byolder people in different parts of the UK. Thesereflect differences in life expectancy, theprevalence of disability and the willingness ofunpaid carers to supply care, though rates ofunpaid care provision seem to be convergingacross the UK. What is clear is that variations in
the demand for long-term care between thecomponent parts of the UK are much smallerthan are the variations within each of these parts.Similarly, the ability to pay for care appears to varymore within than between England, Scotland,Wales and Northern Ireland. Variations in thedemand for long-term care for older people andin ability to pay between the component parts ofthe UK are relatively small in international terms.
While devolution may have restructuredpolitical power within the United Kingdom, it didnot fundamentally change the fundingmechanisms in Scotland, Wales and NorthernIreland. As a result, there continue to be significantdifferences in the amount of public resourcesallocated to long-term care in the different parts ofthe UK. In consequence, the tertiary sector, wherepeople pay for their own care, is much moredeveloped in England than in the devolvednations. Unfortunately, information on this sector isrelatively poor, and, given that it is likely to expandthroughout the UK in the future because of thesevere constraints on government spending thatare likely to apply for at least the next decade,there should be a priority to improve ourunderstanding of its operation.
As mentioned above, in Great Britain, the‘primary’ long-term care system is administeredby local authorities. This is partly because muchof the legislation which sets the framework underwhich long-term care is provided pre-datesdevolution. This inhibits the devolved authoritiesfrom instigating radical change because theunravelling of this legislation would be problematicand time-consuming. Thus local authorities inGreat Britain tend to be responsible forassessment, charging and, in some cases,provision. Clearly they have democratic legitimacy,and therefore the devolved administrations andthe Department of Health in England have to takecare not to interfere with legally established localauthority powers. However, the devolvedadministrations can legitimately influence theautonomy of local authorities by adjusting theirability to allocate funding towards their ownpriorities or towards those of the devolvedadministration. The Scottish Government hastaken a quite different approach to this issue tothat of the Westminster Government. However,
Conclusions and recommendations 35

both the devolved administrations and theWestminster Government face a political dilemmain determining the relative role of centraliseddirection and local autonomy in long-term carepolicy.
Health boards are not generally elected, butthey have an important interaction with localauthorities in supporting frail older people. There istherefore a complex political interaction inScotland and Wales between the devolvedadministration, health boards and local authorities.In Northern Ireland, local authorities do not have asignificant social care role. Nevertheless, all partsof the UK are introducing policy changes toimprove the joint working of the relevant publicagencies, including pooled budgeting. There mustbe lessons that can be learned from otherjurisdictions in seeking to effect these efficiencyimprovements, yet again there seems to be noappetite for joint evaluations in this area.
Ultimately, the key question is whetherdevolution has benefited care clients. This is noteasy to answer. The last decade has seen anunprecedented increase in public spending, whichhas significantly increased the amount ofresources allocated to health and care provisionthroughout the UK. This will not be repeated in thenext decade. It has been possible for the devolvedadministrations and the UK Government toimprove services, at least for some clients, withoutexperiencing a significant political cost. Theyhave done this without much co-operation orco-ordination across the UK. The need to learnfrom each other, even if policies differ somewhat,will become much more acute in the next decade.
Conclusions and recommendations36

Chapter 2
1 The Scottish Parliament was given the powerto vary income tax by 3p in the pound but thispower has never been exercised.
2 Data is taken from various volumes of PublicExpenditure Statistical Analysis (PESA), HMTreasury and chain-linked back to 1998/9.
Chapter 3
1 2002 is the first year for which consistent datais available.
Chapter 5
1 We do not have data on those aged under 65who receive personal care. Therefore thesepercentages represent lower bounds on theshare of clients receiving personal care.
Notes 37
Notes

Related reports38
Adamson, D. (2010) The Impact of Devolution:Area-based Regeneration Policies in the UK
Bivand, P., Bell, L., Vaid, L., Whitehurst, D. andWan, K. (2010) The Impact of Devolution:Employment and Employability
Palmer, G. (2010) The Impact of Devolution:Indicators of Poverty and Social Exclusion
Wilcox, S. and Fitzpatrick, S. (2010) The Impact ofDevolution: Housing and Homelessness
Related reports

References 39
Audit Scotland (2008) A Review of Free Personaland Nursing Care. Available atwww.audit-scotland.gov.uk/utilities/search_report.php?id=230 (accessedAugust 2009)
Bell, D.N.F. (2006) Estimating the Cost of FreeHome Care for Disabled People in Wales. Cardiff:Welsh Assembly Government
Care Development Group (2001) Fair Care forOlder People: Report. Available atwww.scotland.gov.uk/Publications/2001/09/10069/File-1 (accessed August 2009)
Carers UK (2009) ‘What are direct payments?’Available at www.carersuk.org/Information/Directpayments/Whataredirectpayments(accessed August 2009)
Commission for Social Care Inspection (2009)The State of Social Care in England 2007/8.Available at www.cqc.org.uk/_db/_documents/SOSC08%20Report%2008_Web.pdf(accessed August 2009)
Commission on Scottish Devolution (2009)Serving Scotland Better: Scotland and the UnitedKingdom in the 21st Century, Final Report.Available atwww.commissiononscottishdevolution.org.uk/uploads/2009-06-12-csd-final-report-2009fbookmarked.pdf (accessed August 2009)
Davey, V., Fernández, J., Knapp, M., Vick, N.,Jolly, D., Swift, P., Tobin, R. Kendall, J., Ferrie, J.,Pearson, C., Mercer, G. and Priestley, M. (2007)Direct payments: a national survey of directpayments policy and practice. London: PersonalSocial Services Research Unit
Department of Health (2000) ‘The NHS Plan, TheGovernment’s response to the Royal Commissionon Long Term Care’, Cm 4818-II, July. Available athttp://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/@dh/@en/documents/digitalasset/dh_4082154.pdf (accessedNovember 2009)
Department of Health (2003) Fairer ChargingPolicies for Home Care and Other Non-residentialSocial Services: Guidance for Councils with SocialServices Responsibilities. Available atwww.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_4117930 (accessed August 2009)
Department of Health (2007) Putting People First:A Shared Vision and Commitment to theTransformation of Adult Social Care. Available atwww.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_081118 (accessed August 2009)
East Renfrewshire (2007) Letter from the Directorof Finance to Lord Sutherland’s Review of FreePersonal Care. Available at www.scotland.gov.uk/Resource/Doc/924/0056697.pdf(accessed August 2009)
Frick, J.R., Goebel, J., Schechtman, E., Wagner,G.G. and Yitzhaki, S. (2006) ‘Using Analysis ofGini (ANoGi) for detecting whether twosub-samples represent the same universe: theGerman Socio-Economic Panel Study (SOEP)experience’, Sociological Methods & Research,Vol. 34, No. 4, pp. 427–68
Hilton, J. (2008) Streamlining the Assessment ofAttendance Allowance Applications with SocialCare Assessment: An Evaluation of Two LondonPilots, Department for Work and PensionsResearch Report No. 534. London: DWP
References

HM Government (2009) Shaping the Future ofCare Together, Cm 7673. Available atwww.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/documents/digitalasset/dh_102732.pdf (accessed August 2009)
HMSO (1999a) With Respect to Old Age: LongTerm Care – Rights and Responsibilities, A Reportby The Royal Commission on Long Term Care,Cm 4192-I. London: The Stationery Office
House of Commons, Work and PensionsCommittee (2009) Tackling Pensioner Poverty,Fifth Report of Session 2008–09. London: TheStationery Office
Independent Commission on Funding & Financefor Wales (2009) Funding Devolved Governmentin Wales: Barnett & Beyond, First Report.Available at http://wales.gov.uk/docs/icffw/report/090708barnettfullen.pdf (accessed August 2009)
Joint Improvement Team (2009) What is JIT?Available at www.jitscotland.org.uk/about/what-is-jit/ (accessed August 2009)
Keating, M. (2003) ‘Social Inclusion, Devolutionand Policy Divergence’, The Political Quarterly,74.4, pp.429–30
King’s Fund (2006) Securing Good Care for OlderPeople: The Wanless Review of Social Care.Available at www.kingsfund.org.uk/research/publications/securing_good.html(accessed August 2009)
Laffin, M., Taylor, G. and Thomas, A. (2002)The National Assembly for Wales and LocalGovernment. York: Joseph Rowntree Foundation
Priestley, M., Jolly, D., Pearson, C., Riddell, S.,Barnes, C. and Mercer, G. (2006) ‘Directpayments and disabled people in the UK: supply,demand and devolution’. British Journal of SocialWork, July
Riddell, S., Priestley, M., Pearson, C., Mercer, G.,Barnes, C., Jolly, D. and Williams, V. (2006) DirectPayments: A UK Comparative Study, ESRC EndOf Award Report, RES-000-23-0263. Available atwww.leeds.ac.uk/disability-studies/projects/UKdirectpayments/UKDPfinal.pdf(accessed August 2009)
Scottish Executive (1999) ‘Concordat Betweenthe Scottish Executive and the Lord Chancellor’sDepartment’, December. Available at http://www.scotland.gov.uk/Publications/1999/12/lcd(accessed November 2009)
Scottish Government (2008) Independent Reviewof Free Personal and Nursing Care in Scotland,A Report by Lord Sutherland. Available atwww.scotland.gov.uk/Publications/2008/04/25105036/0 (accessed August 2009)
Scottish Government (2009a) Scotland Performs.Available at www.scotland.gov.uk/About/scotPerforms (accessed August 2009)
Scottish Government (2009b) Scotland PerformsIndicators relating to older people. Available atwww.scotland.gov.uk/About/scotPerforms/indicators/CareAtHome (accessed August 2009)
Scottish Parliament Health Committee (2006)Care Inquiry Final Report, 10th Report (Session 2),Vol. 2. Available at www.scottish.parliament.uk/business/committees/health/reports-06/her06-10-vol01-01.htm#CaR5 (accessed August 2009)
Scottish Statutory Instruments (2009) No. 137,Social Care, The Community Care and Health(Scotland) Act 2002 (Amendment to schedule 1)Order. Available atwww.opsi.gov.uk/legislation/scotland/ssi2009/ssi_20090137_en_1 (accessed August 2009)
The Courier (2008) ‘Parties reflect as dust settles’.Available at www.thecourier.co.uk/output/2008/11/07/newsstory12209428t0.asp(accessed August 2009)
References40

UKHCA (United Kingdom Home Care Association)(2004) Who Cares Now? Available atwww.ukhca.co.uk/pdfs/whocaresnowscotland.pdf(accessed August 2009)
UKHCA (United Kingdom Home Care Association)(2009) An Overview of the UK Domiciliary CareSector. Available at www.ukhca.co.uk/pdfs/domiciliarycaresectoroverview.pdf(accessed August 2009)
Welsh Assembly Government (2002) FairerCharging Policies for Home Care and othernon-residential Social Services: Guidance for LocalAuthorities, July Available at http://wales.gov.uk/topics/health/publications/socialcare/guidance/2002/fairercharging?lang=en(accessed November 2009)
Welsh Assembly Government (2004) DirectPayments Guidance: Community Care, Servicesfor Carers and Children’s Services (DirectPayments) Guidance Wales 2004.Available at wales.gov.uk/docrepos/40382/dhss/socialservices/reportsenglish/Direct_Payments_2004-e.pdf?lang=en (accessed August 2009)
Welsh Assembly Government (2006) FreeHomecare for Disabled People, Cabinet Statementby Brian Gibbons, Minister for Health and SocialServices. Available atwales.gov.uk/about/cabinet/cabinetstatements/2006/950641/?lang=en (accessed August 2009)
Welsh Assembly Government (2009) ‘AssemblyMeasure on Charging for Non-residential SocialCare Task & Finish Group. Available athttp://wales.gov.uk/docs/dhss/report/090507taskgroupreporten.pdf(accessed November 2009)
References 41

Acknowledgements and About the author42
Acknowledgements
The author would like to thank Richard Humphriesat King’s Fund, Dean Looney, Elderly andCommunity Care Unit, Department of Health,Social Services and Public Safety, Northern IrelandAssembly and Gareth Griffiths, Older People andLong Term Care Policy Directorate, Health &Social Services Department, Welsh AssemblyGovernment.
About the author
David Bell is Professor of Economics at theUniversity of Stirling. He is also Budget Adviser tothe Finance Committee of the Scottish Parliament.
He was a member of the Care DevelopmentGroup which considered the policy of freepersonal care in Scotland, the Joseph RowntreeFoundation Policy and Practice Group onLong-Term Care and Lord Sutherland’sIndependent Review of Free Personal Care.
During 2009 he jointly authored a JRFViewpoint with Professor Caroline Glendinning(University of York) entitled Rethinking social careand support: What can England learn from othercountries? and another Viewpoint with ProfessorJustin Keen (Leeds) entitled Identifying a fairersystem for funding adult social care.
When not researching social care, David’scurrent research is mainly on unemployment.In 2009 he co-authored two papers with ProfessorDavid Blanchflower (Stirling and DartmouthCollege) entitled What should be done aboutunemployment in the UK? and What should bedone about unemployment in the OECD?

© University of Stirling 2010
First published 2010 by theJoseph Rowntree Foundation
All rights reserved.Reproduction of this report byphotocopying or electronicmeans for non-commercialpurposes is permitted.Otherwise, no part of this reportmay be reproduced, adapted,stored in a retrieval system ortransmitted by any means,electronic, mechanical,photocopying, or otherwisewithout the prior writtenpermission of the JosephRowntree Foundation.
ISBN: 978-1-85935-726-2 (pdf)
The Joseph RowntreeFoundation has supported thisproject as part of its programmeof research and innovativedevelopment projects, which ithopes will be of value to policy-makers, practitioners andservice users. The factspresented and views expressedin this report are, however,those of the authors and notnecessarily those of theFoundation.
Joseph Rowntree FoundationThe Homestead40 Water EndYork YO30 6WPwww.jrf.org.uk
This report, or any other JRFpublication, can be downloadedfree from the JRF website(www.jrf.org.uk/publications/).
A CIP catalogue record for thisreport is available from theBritish Library.