The impact of antiretroviral drugs on renal...
28
The impact of antiretroviral drugs on renal function 1 Professor Bruce Hendry Renal Medicine King’s College London King’s College Hospital NHS Foundation Trust
Transcript of The impact of antiretroviral drugs on renal...
-
The impact of antiretroviral drugs on renal function
1
Professor Bruce HendryRenal Medicine
Kings College London Kings College Hospital NHS Foundation Trust
-
DISCLOSURES: BRUCE HENDRY
I have received research support and/or honoraria from Abbvie, AstraZeneca, Gilead Sciences, Otsuka and Viiv Pharmaceuticals
The opinions expressed in this lecture are entirely my own
-
Overview
Renal Disease: Basic Considerations Renal Disease in PLWHIV Anti Retroviral Therapy (ART) and the kidney Delivering Tenofovir: TAF versus TDF Key conclusions
-
Stratification of Renal Risk
1Consider using eGFRcystatinC for people with CKD G3aA1
ACR, albumin:creatinine ratio; CKD, chronic kidney disease; GFR, glomerular filtration rate
NICE clinical guideline CG182. https://www.nice.org.uk/guidance/cg182. Accessed 07 February 2017
https://www.nice.org.uk/guidance/cg182
-
Renal Concerns in HIV care
Present function eGFR < 75 ml/min Proteinuria
Future risk Age over 50 Diabetes Hypertension Cardiovascular disease (strong reciprocal relationship) Nephrotoxic medications Renal safety of ART
The information portrayed on this slide is attributed to the presenters expert opinion
-
HIV: Impact of CKD Stage G3-G5 (CRF)
p
-
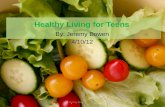
HIV+ vs HIV-Onset of Age-Related Comorbidities
HIV+ individuals vs age-matched HIV- controls have more individual noninfectious comorbidities and at an earlier age (all P < 0.001)
7Guaraldi G, et al. Clin Infect Dis. 2011;53:1120-1126.
Prevalence of Individual Noninfectious Comorbidities HIV+ (N=2854) vs HIV- (N=8562)
Com
orb
idit
y S
tatu
s, %
40 Years
HIV+ HIV-
41 to 50 Years
HIV+ HIV-
51 to 60 Years
HIV+ HIV-
> 60 Years
HIV+ HIV-
Chart1
801631
9091
603181
801721
4235176
652861
213129154
40421520.25
No Age-Related Diseases
1 comorbidity
2 comorbidities
3 comorbidities
4 comorbidities
80
90
60
80
42
65
21
40
16
9
31
17
35
28
31
42
3
8
17
6
29
15
1
1
1
2
6
1
15
2
1
4
0.25
Sheet1
No Age-Related Diseases1 comorbidity2 comorbidities3 comorbidities4 comorbiditiesSeries 6
801631100
9091100
0
603181100
801721100
0
4235176100
652861100
0
213129154100
40421520.2599.25
To resize chart data range, drag lower right corner of range.
-
In the ageing HIV+ population the incidence of CKD CVD and related comorbidities is increasing
*Comorbidities were considered if the patients either had the diagnosis or current treatment Adapted from Bonnet F, et al. HIV Drug Therapy 2016; Glasgow, UK; #O212.
Comorbidities and risk factors, in 2004 and 2014
Bonnet. Glasgow 2016
-
Incident CKD in EuroSIDA
CKD defined as: Confirmed eGFR 60 >25% decline if baseline
eGFR
-
Factors associated with CKD in the EuroSIDA cohort
Mocroft et al. AIDS 2010
-
Renal Signal of ATV/r with TDFmedian change in creatinine clearance
Daar, E et al. 17th CROI 2010. Abstract 59LB
-4
-2
0
2
4
6
8
10
Chan
ge in
cal
cula
ted
crea
tinin
e cl
eara
nce,
(mL/
min
)
ATV/r EFV
ATV/r
EFV
ABC/3TC TDF/FTC
377 330 338 287 394 352 360 327n=
Wk 48, p=0.17
Wk 96, p=0.33
Wk 48, p=0.001
Wk 96, p
-
PI and renal riskRisk of CKD: multivariate analysis
*Adjusted for gender, age at start of HAART, baseline eGFR, Hep B SAg, prior exposure to TFV and IND and total duration of TFV exposure.
Hazard Ratio (95% CI) P value
ATV/r 1.52 (1.14-2.03) 0.004
DRV/r 1.31 (0.94-1.81) 0.108
LPV/r 1.61 (1.1-2.6) 0.017
EFV 1
Rockwood N, et al. Oral presentation IAS; 2011. Rome.
Patients on ATV/r or LPV/r were significantly more likely to develop eGFR
-
ARV exposure and chronic kidney disease
Lancet HIV. 2016; 3:e23-32
-
Risk factors for CKD: data from the D:A:D study
PLoS Med 2015; 12: e1001809
-
Some ARV therapies increase the risk of CKD
15ATV, atazanavir; ATV/r, atazanavir/ritonavir; BPI, other ritonavir-boosted protease inhibitor
(excluding lopinavir/ritonavir and atazanavir/ritonavir); LPV/r, lopinavir/ritonavir; TDF, tenofovir. 1. Mocroft A et al. PLoS Med 12(3): e1001809.
Cumulative effects of ARVs on underlying CKD risk
Num
ber n
eede
d to
har
m
Years of ARV exposure
Low risk (
-
Renal Risk Calculators in HIV care
Copenhagen University http://www.chip.dk/TOOLS (D:A:D) Simple binary input (e.g. diabetes yes or no) Risk of CKD within 5 years Underestimates risk if moderate or severe comorbidity Includes ART risk modification (TDF etc)
UCSF http://hivinsite.ucsf.edu/InSite?page=md-calculator(VA) More sophisticated input (continuous variable) Includes proteinuria Less quick and easy Risk of CKD within 5 years Includes ART risk modification (TDF)
The information portrayed on this slide is attributed to the presenters expert opinion
http://www.chip.dk/TOOLShttp://hivinsite.ucsf.edu/InSite?page=md-calculator
-
Tubulopathy (acute tubular injury/Fanconi syndrome)
AIDS 2016; 30: 1311-3, HIV8, Glasgow 2008
-
TFV (TDF) exposure and kidney disease
Scherzer et al, AIDS 2012
-
Rapid eGFR decline and CKD in patients with subsequent TDF-associated Renal Tubulopathy
eGFR pattern on TDF Cases Controls P valueeGFR decline >3 mL/min/1.73m2/year 69.6% 7.9% 5 mL/min/1.73m2/year 55.4% 3.5%
-
eGFR slopes in patients who discontinued TDF
JID 2014; 210: 363-373
-
Factors associated with incomplete recovery of renal function after TDF discontinuation
JID 2014; 210: 363-373
-
Pharmacokinetics of Tenofovir alafenamide (TAF)
10/25 mg
1. SmPC DESCOVY. Available at https://www.medicines.org.uk/emc/medicine/31764. Accessed 3 May 2016. 2. Lee WA, et al. Antimicrob Agents Chemother 2005; 49(5): 18981906. 3. Birkus G, et al. Antimicrob Agents
Chemother 2007; 51(2): 543550. 4. Babusis D, et al. Mol Pharm 2013; 10(2): 459466.
https://www.medicines.org.uk/emc/medicine/31764
-
Plasma tenofovir concentrations (TDF vs. TAF)
-
eGFR through 96 weeks with ECF-TAF in patients with renal impairment (GS-0112)
Primary end point was eGFR change at Week 24 (primary endpoint met; no statistically significant difference in eCrCl)
Post, F. Boston, USA, CROI 2016 (P680)
-
Switching from TDF to TAF improves total and tubular proteinuria (GS-0112)
Post, F. Boston, USA, CROI 2016 (P680)
-
Comparison of renal events with ECF-TAF vs. ECF-TDF in ART-nave patients (GS-0104/0111)
TAF vs. TDF: P
-
ART and the kidney KEY points
PLWHIV should have baseline and ongoing assessment of renal function and risk (eGFR and proteinuria)
Signals of renal toxicity have been associated with certain ART notably TDF, ATV, LPV/r and boosted PI regimes in general.
ART not associated with renal risk include ABV, TAF, NNRTI and Integrase Inhibitors
Renal Risk assessment should be used to guide choice of ART using national and international guidelines
For patients with established CKD the future use of unboosted ART is of great potential benefit in avoiding DDI
Bruce Hendry, personal communication,
-
Thanks
28The author has permission to use this image
Dianummer 1DISCLOSURES: BRUCE HENDRYOverviewStratification of Renal RiskRenal Concerns in HIV careDianummer 6HIV+ vs HIV-Onset of Age-Related ComorbiditiesIn the ageing HIV+ population the incidence of CKD CVD and related comorbidities is increasingDianummer 9Dianummer 10Renal Signal of ATV/r with TDFmedian change in creatinine clearancePI and renal riskRisk of CKD: multivariate analysisDianummer 13Dianummer 14Some ARV therapies increase the risk of CKDRenal Risk Calculators in HIV careTubulopathy (acute tubular injury/Fanconi syndrome)TFV (TDF) exposure and kidney diseaseRapid eGFR decline and CKD in patients with subsequent TDF-associated Renal Tubulopathy Dianummer 20Dianummer 21Dianummer 22Dianummer 23eGFR through 96 weeks with ECF-TAF in patients with renal impairment (GS-0112) Dianummer 25Dianummer 26ART and the kidney KEY pointsDianummer 28