

The HIV Pandemic 2008 Where Do We Go From Here? Myron S. Cohen, MD J. Herbert Bate Professor...
86
The HIV Pandemic 2008 Where Do We Go From Here? Myron S. Cohen, MD J. Herbert Bate Professor Medicine, Microbiology, Public Health Director, UNC Institute of Global Health The University of North Carolina-CH
-
Upload
asher-booker -
Category
Documents
-
view
214 -
download
4
Transcript of The HIV Pandemic 2008 Where Do We Go From Here? Myron S. Cohen, MD J. Herbert Bate Professor...

The HIV Pandemic 2008Where Do We Go From Here?
Myron S. Cohen, MD
J. Herbert Bate Professor
Medicine, Microbiology, Public Health
Director, UNC Institute of Global Health
The University of North Carolina-CH

Critical Issues in HIV
• The Pandemic
• Global Treatment
• Prevention
…and UNCs role
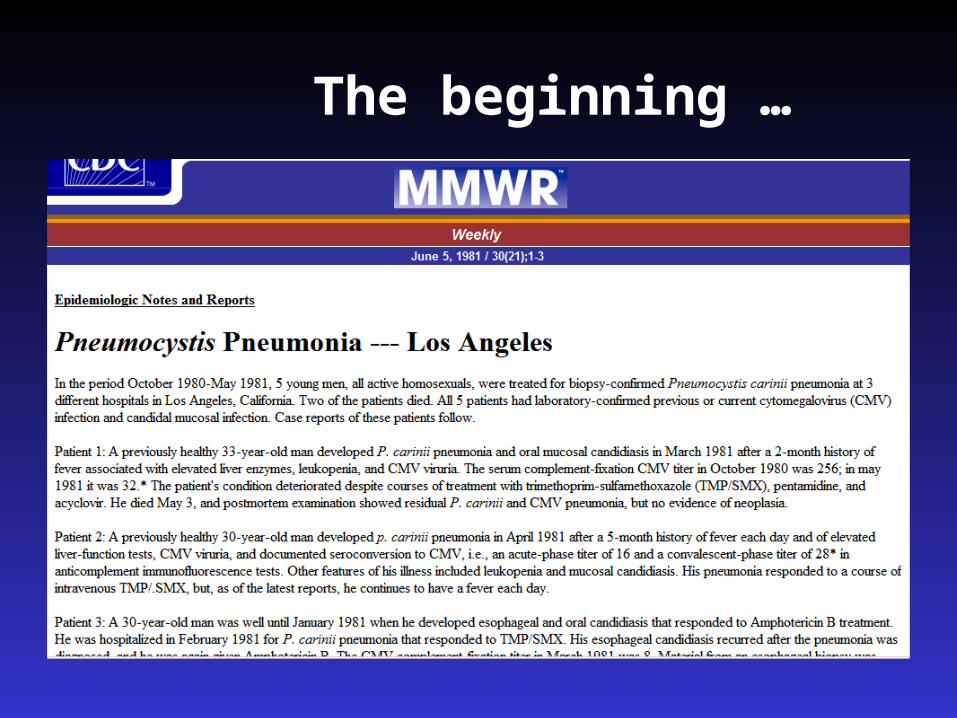
The beginning …

Hubei Medical College, 1979
Me

A global view of HIV infectionA global view of HIV infection38.6 million people [33.4‒46.0 million] living with HIV, 2005
2.4

Where is HIV Going Next?
• HIV is STAYING in Africa
• India
• China
• Russia
• ????

About 14,000 new HIV infections dailyAbout 14,000 new HIV infections daily
• >95%95% new infections in developing countries.
• 2,0002,000 in children under 15 years of age.
• 12,00012,000 are in people aged 15-49 years
* about 50% are 15–24 year olds.
* almost 50% are in women
4 new people infected for every person treated!



Epidemic Spread of Disease
Ro = bDC
When Ro >1 epidemic is sustained
b = Efficiency of transmission (…a biological event)
D = Duration of infectiousness
C = Number of people (partners) exposed

Transmission of Infectious Diseases:Biological Requirements
Infectious SusceptibilityInoculum (concentration)Hereditary resistance
Phenotypic factors Innate resistance
Acquired (immune)
resistance
*communicability and virulence are two different concepts

Routes of Exposure and H.I.V. INFECTION ROUTE RISK OF INFECTION
Sexual Transmissiona. Female-to-male transmission………..1 in 700 to 1 in 3,000b. Male-to-female transmission……...….1 in 200 to 1 in 2,000c. Male-to-male transmission………...….1 in 10 to 1 in 1,600d. Fellatio??…………………………….. 0 (CDC) or 6% (SF)
Parenteral transmissiona. Transfusion of infected blood………….95 in 100b. Needle sharing………………………….1 in 150c. Needle stick…………………………..…1 in 200d. Needle stick /AZT PEP…………………1 in 10,000
Transmission from mother to infanta. Without AZT treatment………...…….1 in 4b. With AZT treatment………………….Less than 1 in 10
Royce, Sena, Cates and Cohen, NEJM 336:1072-1078, 1997

Coital Frequency per Month by Age
10.02
8.98 9.11
7.44
15-24 25-29 30-34 35-59
Age
4
5
6
7
8
9
10
11
Co
ital
fre
qu
ency
per
Mo
nth

Hypothesis
1) Estimated transmission rates are too low to explain the epidemic
2) HIV transmission is intermittently AMPLIFIED by increased genital tract shedding3) AMPLIFIED transmission is critical to the
spread of HIV 4) OTHER Sexually Transmitted diseases play
a key role
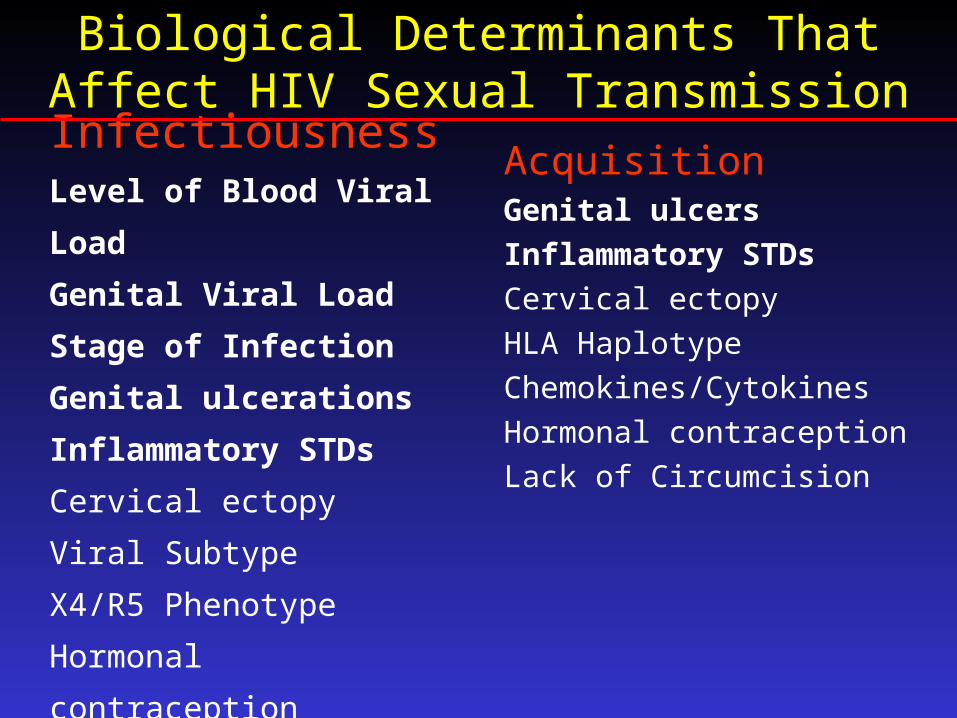
Biological Determinants That Affect HIV Sexual Transmission
InfectiousnessLevel of Blood Viral Load
Genital Viral Load
Stage of Infection
Genital ulcerations
Inflammatory STDs
Cervical ectopy
Viral Subtype
X4/R5 Phenotype
Hormonal contraception
AcquisitionGenital ulcers
Inflammatory STDs
Cervical ectopy
HLA Haplotype
Chemokines/Cytokines
Hormonal contraception
Lack of Circumcision

HIV
RN
A in
Sem
enH
IV R
NA
in S
emen
(Log
(Log
1010
copi
es/m
l) c
opie
s/m
l)
Acute Infection
Acute Infection
3 wks3 wks Asymptomatic
Asymptomatic
InfectionInfection
HIV Progression
HIV ProgressionAIDSAIDS
00
22
44
66
1/1000 - 1/1000 - 1/10,0001/10,000
1/500 - 1/500 - 1/20001/2000
1/100-1/100-1/10001/1000
Risk of TransmissionRisk of TransmissionReflects Reflects Genital Genital Viral Burden Viral Burden
1/30-1/30-1/701/70
Big Idea I: Transmission in Clusters

HIV
RN
A in
Sem
enH
IV R
NA
in S
emen
(Log
(Log
1010
copi
es/m
l) c
opie
s/m
l)
Acute HIV Infection
Acute HIV Infection
& STD Coinfection
& STD Coinfection
STD Episode
STD Episode
STD Episode
STD EpisodeAIDSAIDS
22
33
44
55
Big Idea II: “Classical” STDs Drive HIV
1/30 or greater odds of transmission 1/30 or greater odds of transmission to a susceptible partner per coital actto a susceptible partner per coital act

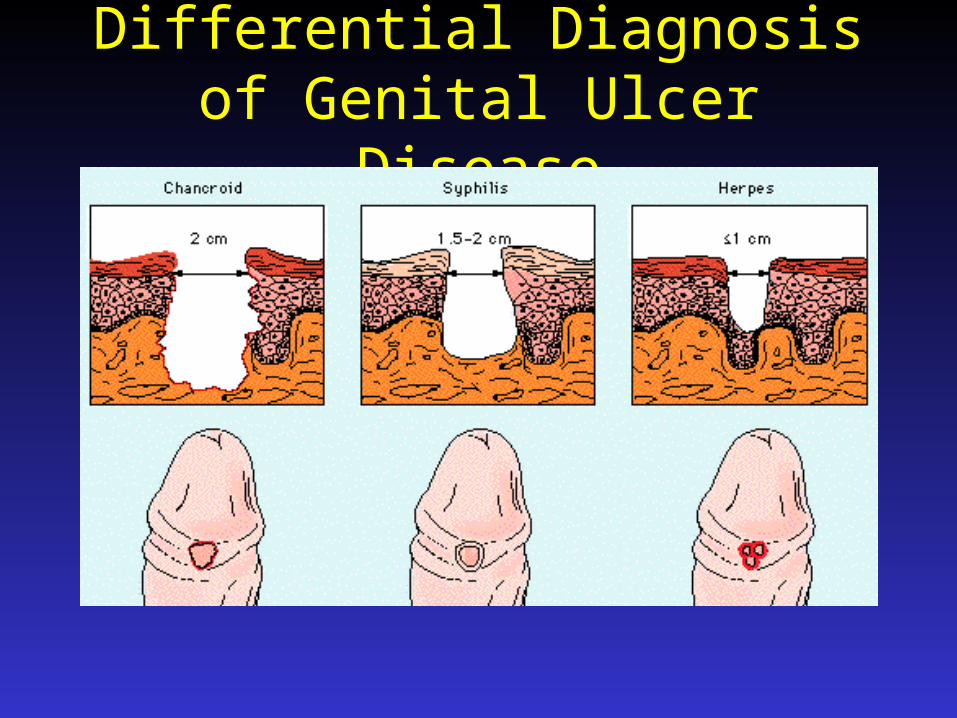
Differential Diagnosisof Genital Ulcer Disease

"The Tip of the Iceberg"
90.8%Unrecognized and asymptomatic infection
9.2%Recognized infection
Iceberg represents all those withHSV-2 antibody

UNC Global Health Research Sites“TO BE AND NOT TO SEEM”

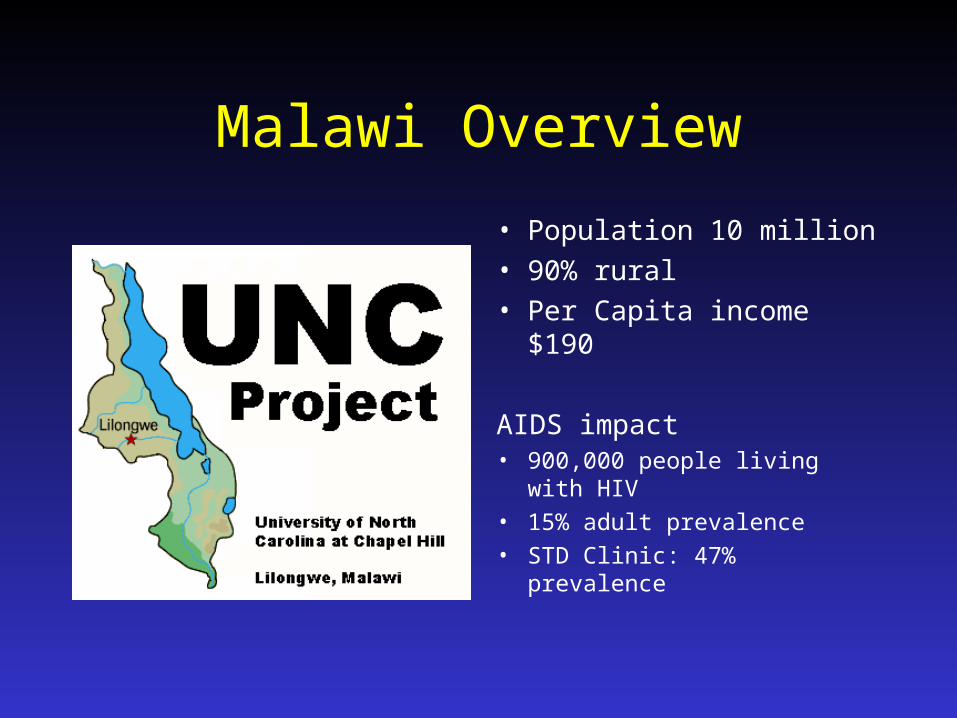
Malawi Overview
• Population 10 million• 90% rural• Per Capita income $190
AIDS impact• 900,000 people living with
HIV• 15% adult prevalence• STD Clinic: 47% prevalence







HIV-1 Viremia and SheddingPilcher et al. AIDS, 2007
wk4 wk8 wk16
Established HIV Infection
CD4<350
1
3
5
7
9
CD4>350
Acute HIV Infection
log
10H
IV-1
RN
A c
opie
s p
er m
L

01 July 2002 slide number SSA-7
Number of people who died from HIV/AIDS in sub-Saharan Africa, 1980-2001
0
500
1,000
1,500
2,000
2,500
1980 1983 1986 1989 1992 1995 1998 2001
Thousan
ds
Source: UNAIDS, 2002

Projected life expectancy in African countries with high HIV prevalence, 1995–2000
Source: United Nations Population Division
1955 1960 1965 1970 1975 1980 1985 1990 1995 2000
Average life expectancy at birth, in years65
60
55
50
45
40
35
ZimbabweZimbabwe
ZambiZambiaaUgandaUganda
BotswanaBotswana
MalawiMalawi

In 9 Sub-Saharan African countries, one-fifth to one-third of all children under the age of 15
Were orphaned by the year 2000 34.3
27.4 26.9 27.425.5
23.421.7 20.9 20.3
0
5
10
15
20
25
30
35
Zambia
Malawi
Rwanda
Zimbabwe
Uganda
Botswana
Tanzania
Burkina Faso
Central African Rep.
US Census Bureau


0
5
10
15
20
25
30
35
40
1995 1996 1997 1998 1999 2000 2001
Dea
ths
per
100
per
son
-yea
rs
0
25
50
75
100 Percen
tage o
f patien
t-days o
n A
RT
DEATHS
USE OF ART
Mortality vs ART utilization
Palella F, et al. 2001; 8th CROI. Abstract 268b.
AIDS Mortality Rates: 1996-2001
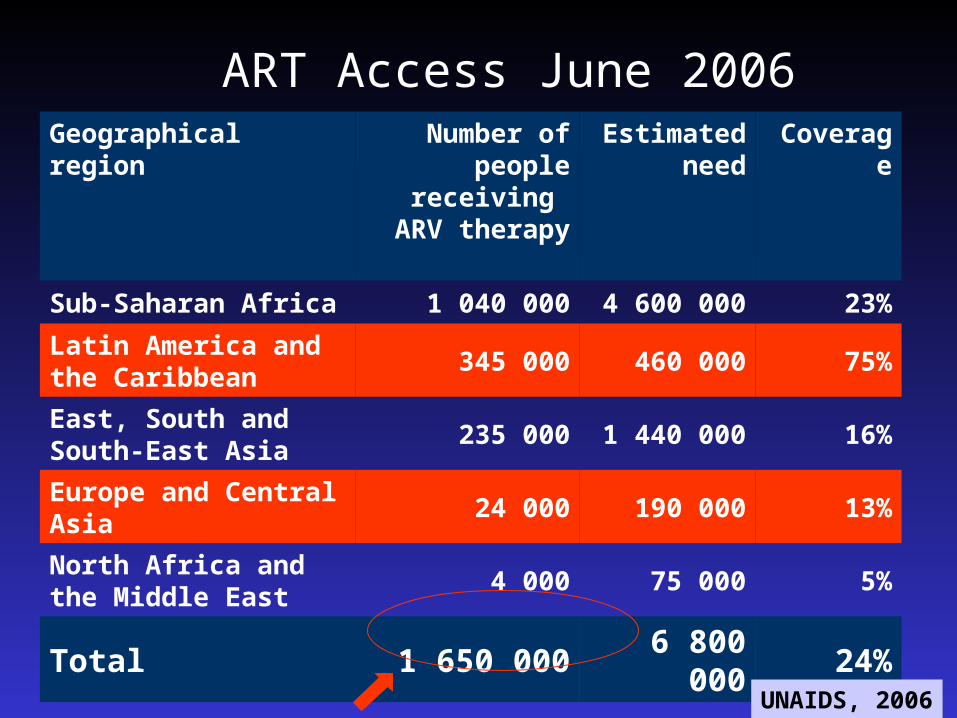
ART Access June 2006Geographical region Number of
people receiving ARV
therapy
Estimated need
Coverage
Sub-Saharan Africa 1 040 000 4 600 000 23%
Latin America and the Caribbean
345 000 460 000 75%
East, South and South-East Asia
235 000 1 440 000 16%
Europe and Central Asia
24 000 190 000 13%
North Africa and the Middle East
4 000 75 000 5%
Total 1 650 000 6 800 000 24%
UNAIDS, 2006

Presidential Emergency Plan for AIDS Relief (PEPFAR)
• 15 “focus” countries…(but funds in > 120)• Trained lab personnel, counselors,
infrastructure, distribution/management of ART and other drugs
• Care provided to 3,000,000 people• >600,000 provided ART • $15,000,000,000 over 5 years (maybe more!) ….and The Global Program, Three x Five and
others! As of 2007…THE US IS PRIVIDING 1/3 of ALL
PLANETARY HIV TREATMENT AND CARE
Opportunities to Prevent HIV
1) BEFFORE EXPOSURE
2) AT EXPOSURE (PrEP)
3) AFTER EXPOSURE (PEP)
4) SECONDARY TRANSMISSION
“positive prevention”

Prevention of HIV
1. STD control, behavior change, condom2. Topical microbicides (Trials ongoing)3. The diaphragm (Trial completed!)4. Male circumcision (Trials completed!)5. Antiviral therapy (Trials ongoing) - for HIV (treat both HIV+ or HIV-) - for HSV to prevent HIV (treat HIV+ or-) 2. Societal (Structural) Change: Incentives for
safer sex, needle exchange?

Vaccines for Prevention of HIV Infection
Good News:HIV proteins are immunogenicAnimal success stories with clues to immunity
Bad News:No reliable surrogates of immunity
Short-lived immunity VAXGEN Failure Merck 502,503 Failure (Sept 22,2007)!!!
The Cost : Benefit ratio-Disinhibition

Potential end-points of HIV-vaccine efficacy trials
UNAIDS–97100 1 August 1998
“normal” infectionwith variable levels
of viral load
no protection
no infection
protection against HIVsterilizing immunity
protection against disease (modification of the course of HIV infection in vaccine recipients)
initial infection“controlled”
establishment of chronic infection with low viral load

Merck 502
• AD5, HIV CTL stimulation, no envelope
• Study stopped in September 2007 for FUTILITY!!
• No protection from HIV acquisition
• No reduction in viral load set point
WHATS NEXT?????


Relationship Between HIV and Male Circumcision
0
5
10
15
20
25
0 20 40 60 80 100
% Circumcised males
HIV
Ser
op
reva
len
ce (
%)
Bongaarts AIDS 1989
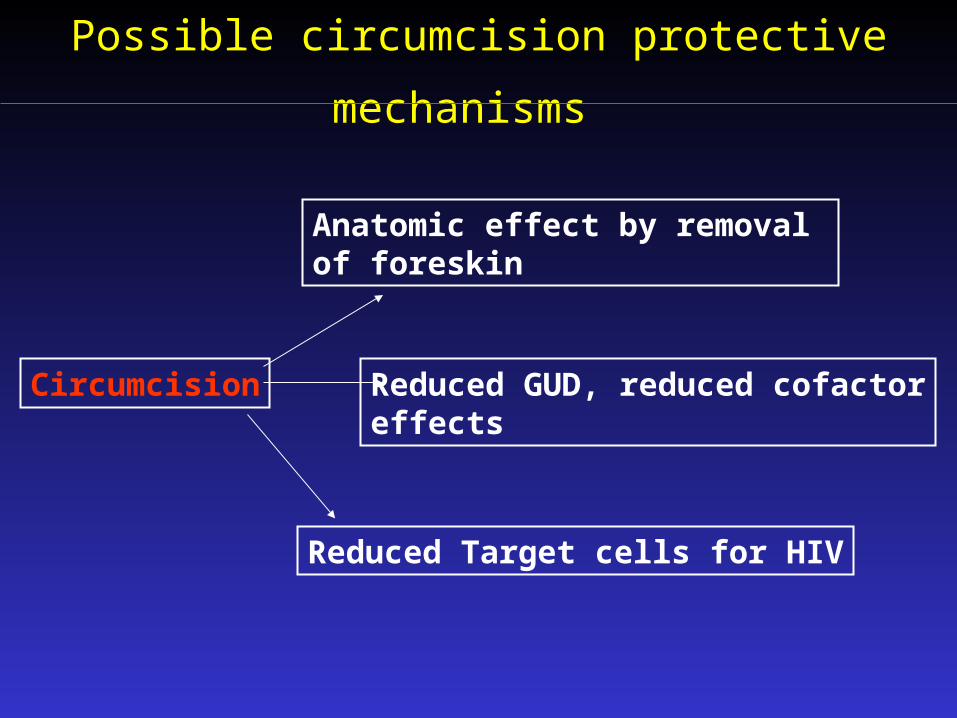
Possible circumcision protective mechanisms
Circumcision
Anatomic effect by removal of foreskin
Reduced GUD, reduced cofactoreffects
Reduced Target cells for HIV

Impact of MC on HIV : Evidence from observational studies and RCTs
85 80 70 60 .50 1
Reduction of risk
(95% CI)
South Africa (RCT) 60 ( 76, 33)
Kenya (RCT) 59 ( 76, 30)
Uganda (RCT) 51 ( 82, 14)
Overall 58 ( 66, 48)15
17
1
1
Reduction of risk (0%)
Bailey et al. Lancet 2007; 369: 643–56
Weiss et al. AIDS 2000, 14:2361-70
Auvert et al. PLoS Med 2005(11): e298.2006
Gray et al. Lancet, 2007, 657–66
gramjee
again is this referring to MC?
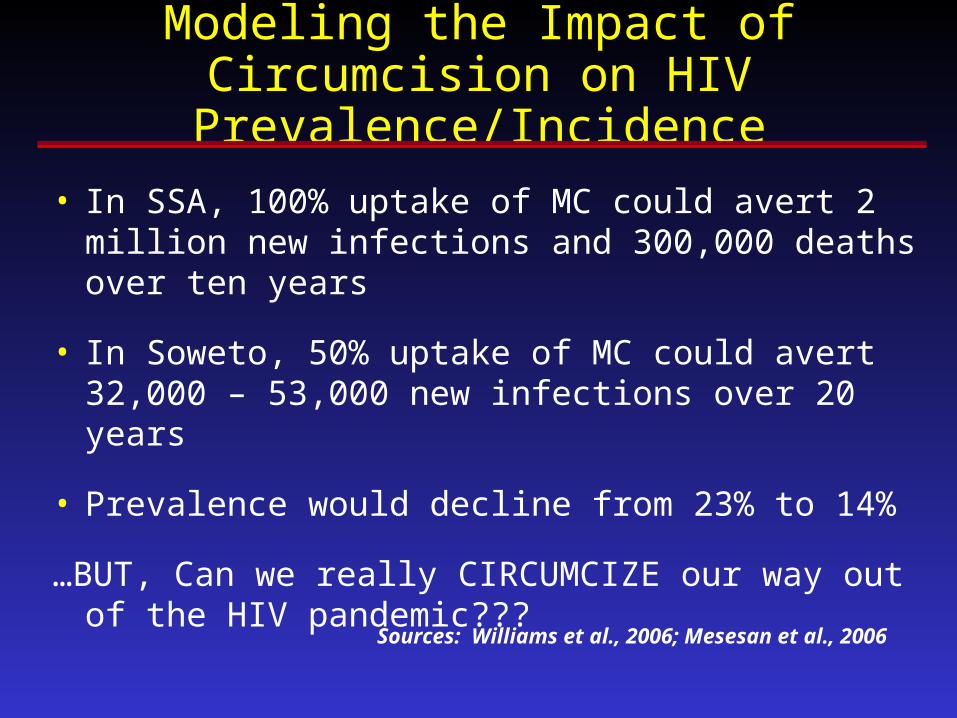
Modeling the Impact of Circumcision on HIV Prevalence/Incidence
• In SSA, 100% uptake of MC could avert 2 million new infections and 300,000 deaths over ten years
• In Soweto, 50% uptake of MC could avert 32,000 – 53,000 new infections over 20 years
• Prevalence would decline from 23% to 14%
…BUT, Can we really CIRCUMCIZE our way out of the HIV pandemic???
Sources: Williams et al., 2006; Mesesan et al., 2006

Antiretroviral Therapy
Effect on HIV Transmission
?
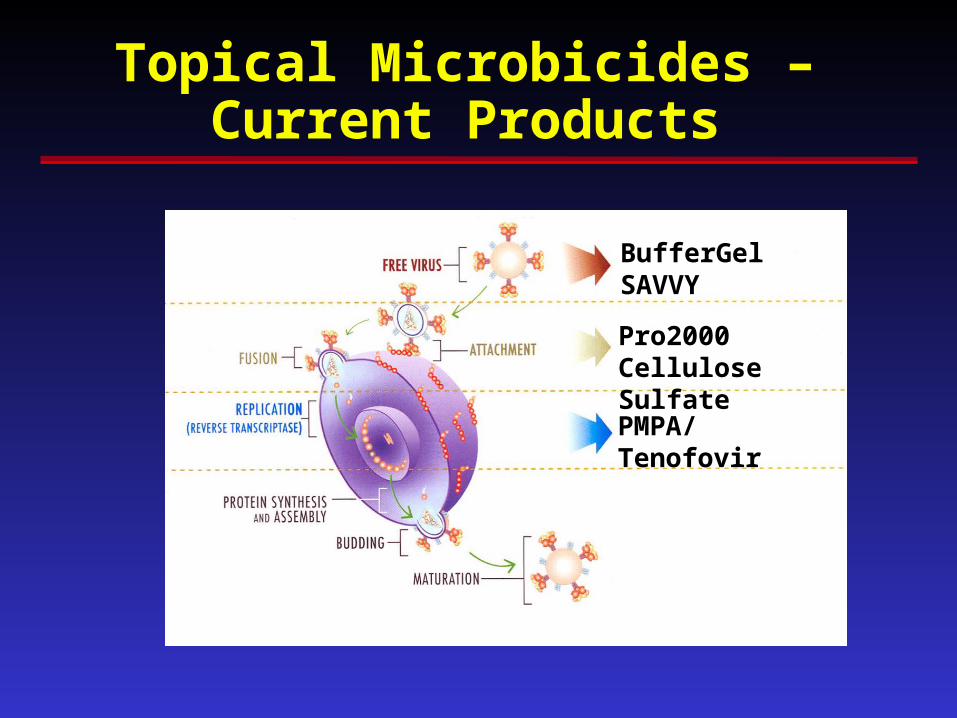
Topical Microbicides –Current Products
BufferGelSAVVY
Pro2000Cellulose Sulfate
PMPA/Tenofovir
ART to Prevent Transmission of HIVCohen et al. Annals Int Med, 2007
• Post-exposure prophylaxis (nPEP)
USPH Guidelines 2005
• Pre-Exposure Prophylaxis (PrEP)
• Treatment of the infected person
nPEP US Guidelines• A clinical trial to PROVE that nPEP works cannot
be developed (and it sometimes fails!!)
• CDC Guidelines generated based on consensus, lessons from macaques
MMWR Jan 21, 2005 Vol 54: 1-20 “Antiretroviral Postexposure Prophylaxis After
Sexual, Injection-Drug Use, or Other Nonoccupational Exposure to HIV in the United States”
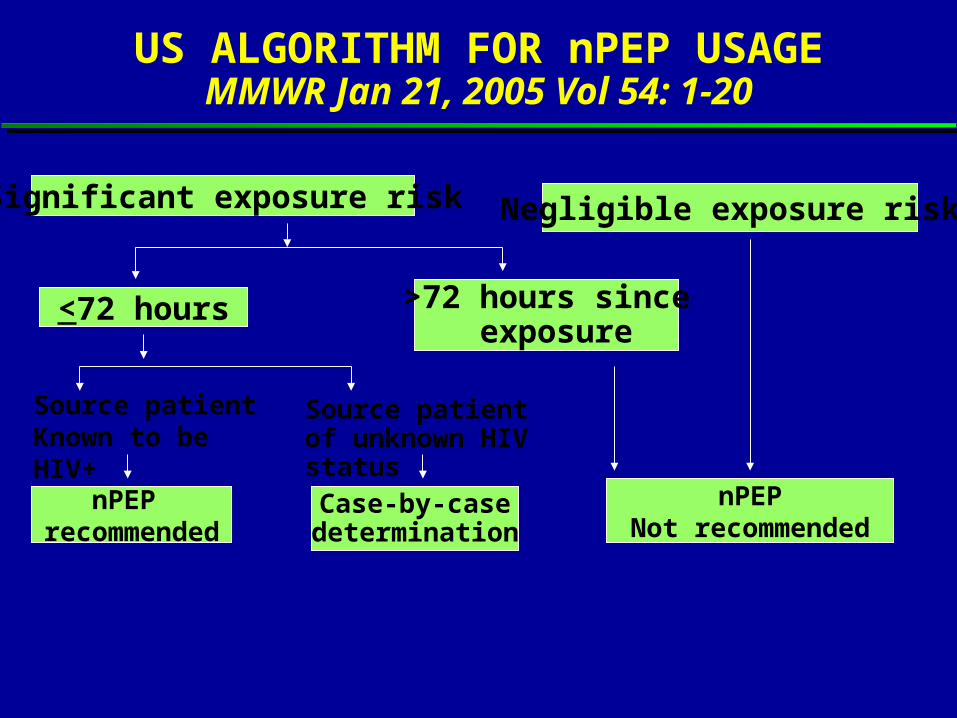
US ALGORITHM FOR nPEP USAGEMMWR Jan 21, 2005 Vol 54: 1-20
Significant exposure risk Negligible exposure risk
<72 hours >72 hours since exposure
Source patientKnown to be HIV+
Source patient of unknown HIV status
nPEP recommended
Case-by-casedetermination
nPEPNot recommended

NVP (80%)
APV (50%)
ABC (40%)
ABC (150%)
Female Genital Tract Exposure(% blood plasma)
Dumond et al. AIDS 2007
ZDV (200%)
IDV (200%)
0 200% 400% 600%
TDF (400%)
3TC (400%)
NNRTIPINRTI
LPV (30%)
ATV (30%)
RTV (20%)
DLV (20%)
FTC (600%)ddI (100%)
SQV(ND)
EFV (0.6%)
d4T (4%)

0 2 4 6 8 10 12 140
25
50
75
100
Number of rectal exposures
% U
nin
fect
ed a
nim
als
Controls (n = 18)
Injectable FTC (n = 6)
Injectable Truvada (n = 6)
Oral Truvada (n = 6)
Oral TDF (n = 4)
PrEP in Macaques
Garcia-Lerma et al PLoS Medicine in pressGarcia-Lerma et al PLoS Medicine in press
Cohen and Kashuba PLoS Medicine inn press (editorial) Cohen and Kashuba PLoS Medicine inn press (editorial)

HIV PrEP Safety Trial CompletedPeterson et al PLoS Clin Trials 2007
• Limited toxicity, good reported adherence
• 8 on-product seroconversions observed:
2 TDF/6 placebo (p = 0.24)
• A blood specimen obtained from one of the two participants on TDF showed no evidence of resistance
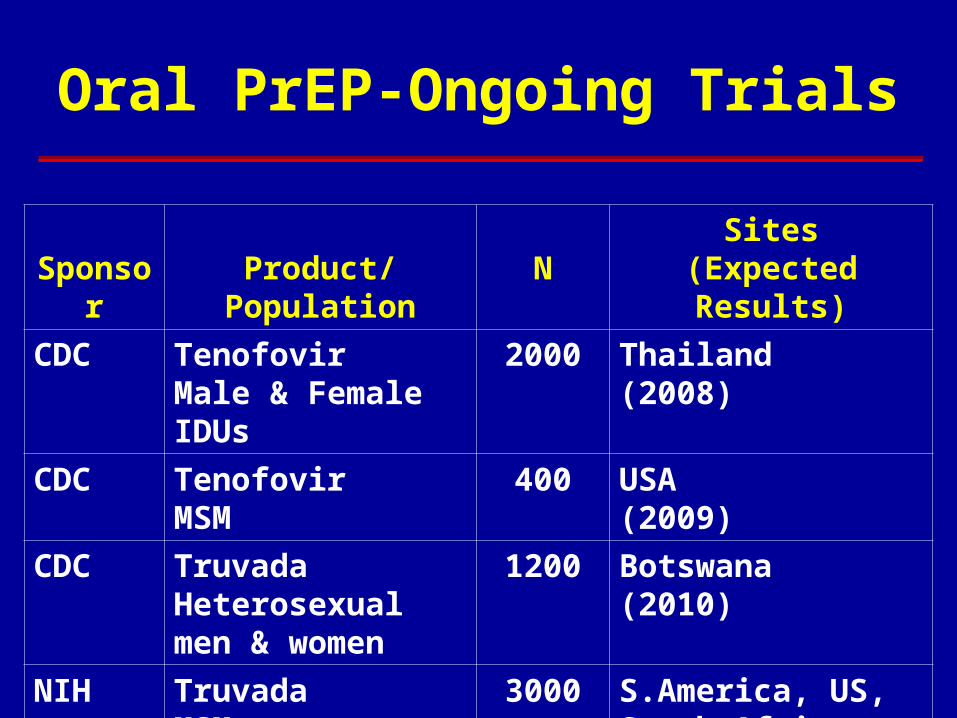
Oral PrEP-Ongoing Trials
Sponsor Product/Population NSites
(Expected Results)
CDC TenofovirMale & Female IDUs
2000 Thailand (2008)
CDC TenofovirMSM
400 USA (2009)
CDC TruvadaHeterosexual men & women
1200 Botswana (2010)
NIH TruvadaMSM
3000 S.America, US, South Africa, Thailand(2011)

Oral PrEP – Planned Trials
Sponsor Product/Population N Sites
Gates Tenofovir/TruvadaDiscordant couples
2000 men,2000 women
Eastern Africa
NIH/
MTN
Tenofovir/TruvadaWomen
2400 Southern/Eastern Africa
USAID TruvadaHigh-risk women
3900 Southern/Eastern Africa

ART PrEP Human trials with TDF focused on “very high risk”
subjects hindered or stopped because of….
i) “Ethical” Considerations (Cambodia, Cameroon) Grant et. al. Science, September 30, 2005 Page-Shafer et. al. Lancet, September 2005
ii) Resistance (Malawi) Tenofovir (k65r) resistance with monotherapy
iii) Public health relevance? J. Cohen, New York Times Sunday Magazine, Jan. 2006

ART to Prevent Sexual Transmission of HIV:COUPLES REALLY MATTER!!!!!
1. Biological plausibility
-HIV SUPPRESSION in the blood and the genital tract are readily achieved
2. Expectations from “the literature”
3. HPTN052: A Clinical Trial

HIV-RNAHIV-RNA HIV-DNAHIV-DNA
00
2020
4040
6060
8080
100100
Pa
tient
s (%
) w
ithP
atie
nts
(%)
with
det
ect
ab
le H
IV in
se
me
nd
ete
cta
ble
HIV
in s
em
en
n=55n=55
n=114n=114
Controls (drug naive) Controls (drug naive)
Potent ARTPotent ART
p<0.0001p<0.0001
p=0.025p=0.025
Semen HIV in patients with suppressed Semen HIV in patients with suppressed viral loadviral load
Vernazza, Cohen Vernazza, Cohen et al.,et al., AIDS, 2000 AIDS, 2000

March 2007, Slide 62
ART Prevents HIV Transmission? Retrospective Analysis
Musicco et al. Archives Int Med 154: 1971; 1994 Castilla et al. JAIDS 40, 96, 2005
Observational Studies Kayitenkore et al. IAS, 2006 Bunnell et a. AIDS 20: 85-92, 2006
Ecological Analysis Katz et al. Am J. Public Health 92: 388, 2002 (-) Porco et al. AIDS 18:81, 2004 (+) Fang et al. JID, September 2004 (++ Montaner et al. Lancet, August 2006 (??)

March 2007, Slide 63
Bunnell et a. AIDS 20: 85-92, 2006ART offered May, 2004 in Uganda454 subjects and co-habiting partners
available for 24 month follow-upBaseline viral load (122,500 copies)
“suppressed” Increased sex, but reduced risky behaviorHIV Seroconversions reduced from
45.7/1000 py to 1/1000 pyOnly one seroconversion in 2 years
March 2007, Slide 64
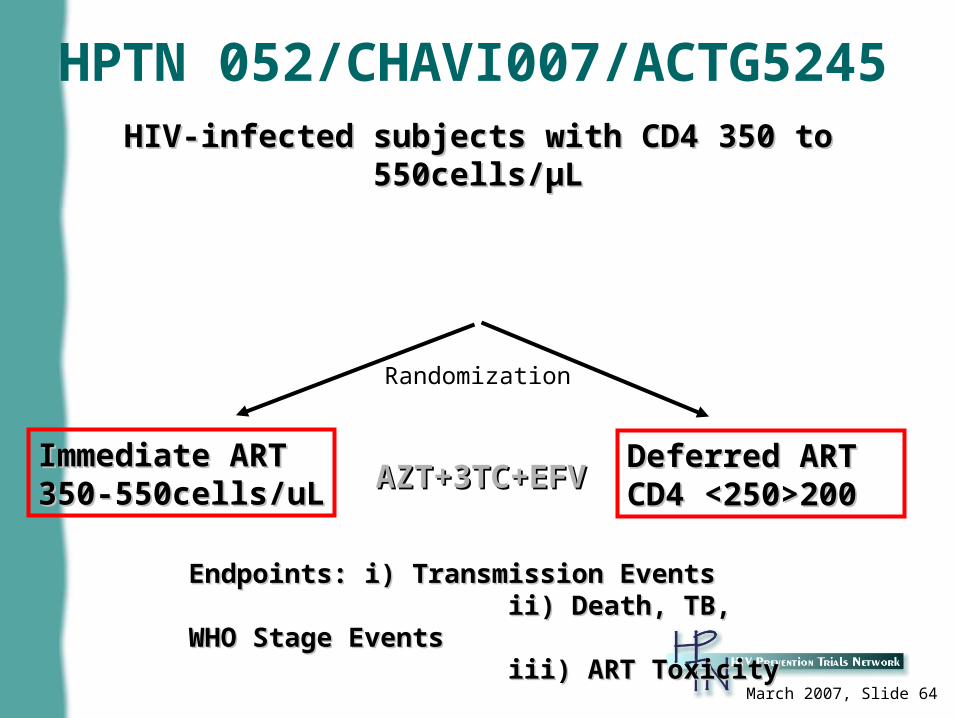
HPTN 052/CHAVI007/ACTG5245HIV-infected subjects with CD4 350 to 550cells/HIV-infected subjects with CD4 350 to 550cells/µLµL
Immediate ARTImmediate ART350-550cells/uL350-550cells/uL
Deferred ART Deferred ART CD4 <250>200CD4 <250>200AZT+3TC+EFVAZT+3TC+EFV
Endpoints: i) Transmission Events Endpoints: i) Transmission Events ii) Death, TB, WHO Stage Eventsii) Death, TB, WHO Stage Events iii) ART Toxicityiii) ART Toxicity
Randomization

Timing of Trial Results
2006 2008 2009
Female Barrier- Diaphragm
Male Circumcision - Susceptibility
20102007
Microbicides – CS-1CS-2
Carraguard
Male Circumcision - Infectiousness
Microbicides• BG/Pro2000
•Pro2000• TDF
Oral PrEP - IDU
HSV-2 Treatment - Infectiousness
HSV-2 Treatment –
Susceptibility
Oral PrEP• MSM
• Heterosexual
2012
IndexPartner
Treatment
Vaccines -Adenovirus-5Vaccines -
Prime/Boost
Community VCT and HIV
Support
Oral PrEP -West Africa

Prevention of HIV
1. STD control, behavior change, condoms2. Treatment of genital herpes (Trials onging)3. Topical microbicides (Trials ongoing)4. The diaphragm (Trial completed)5. Male circumcision (Trials completed)6. Antiviral therapy (trials ongoing)7. Societal (Structural) Change: Incentives for
safer sex?

Ode to a Condom
by Myron S. Cohen
Ode to a Condom
by Myron S. Cohen

O translucent, latex sheath
You snugly guard the sword beneath
To hear your name can cause a smirk
The question is, how well you work?

But for what purpose one must ask
For you can accomplish many tasks
To prevent conception has been your goal
But to prevent infection is your truer role.

For birth control you are not great
Pregnancy can occur at a 10% rate
But for STDs let's take a look
At news not found in a medical book.


There are some differences depending on the bug
In risks for men and women after "the hug"
For gonorrhea, chlamydia, and bacterial things
The risk goes down for a man's fling

For women, alas, the news is less good
Even in the face of your mighty latex hood.
Why is this so? It is a serious plight --
Men must be taught condom wrong from condom right!
Condoms can’t work,
If they’re not put on.
Insertion sans condom,
Has no pro, only con.

TABLE 1. Problems Experienced by 47 Men During 270 Cumulative Episodes of Condom Use in the Last Month, Stratified by Risk of Transmission for STDs, HIV Infection, and Pregnancy
No. of No. of Men Events Occurrence 95% Experiencing
Problem (n=270) (%) Cl (n=47)
No direct penile-vaginal contactPut on inside-out, then flipped over and used 35 13.0 5.2-20.7 15 (31.0%)Lost erection before or after condom was put on 33 12.2 3.2-21.1 11 23.4%)Experienced allergic reaction or irritation from condom 6 2.2 0.0-5.3 3 (6.4%)Completely unrolled condom before putting on 2 0.7 0.0-2.2 1 (2.1%)Removed defective condom from package 0 -- -- 0 (0%)Tore condom with finger, jewelry or ring 0 -- -- 0 (0%)
Direct penile-vaginal contactStarted intercourse without a condom, then stopped to put on 21 7.8 2.7-12.8 8 (17.0%)Broke condom during intercourse or withdrawal 11 4.1 0.8-7.3 6 (12.8%)Started intercourse with a condom, then removed it and 7 2.6 0.2-5.0 4 (8.5%) continued intercourseCondom fell off during intercourse or withdrawal 4 1.5 0.0-3.2 3 (6.4%)
STDs = Sexually transmitted diseases; HIV = human immunodeficiency virus, CI = confidence interval
Warner L, Clay-Warner J, Boles J, Williamson J. Assessing condom use practices. Sex Transm Dis 1998; 25(6):273-277.


Look at your package, look at your date;
If you are damaged one tempts the fates
Roll you on smoothly, expunge air at your tip,
Take you off if there is the smallest rip (drip).

And latex is tricky;
It’s destructible stuff.
So don’t lubricate with oil;
Water is enough.

And after the "love", while you are still in place,
You must be removed at a rapid pace
Gently unrolled and safely tied
Access for the milky elixir completely denied.

AND WHAT ABOUT AIDS, THE ULTIMATE FOE
Can you help? Is it so?
The answer is clear,
And should bring great cheer.
The spread of the virus has been carefully reviewed
In couples who used you and those who eschew you
When you are used transmission nears zero
Your rubbery face has the smile of a hero
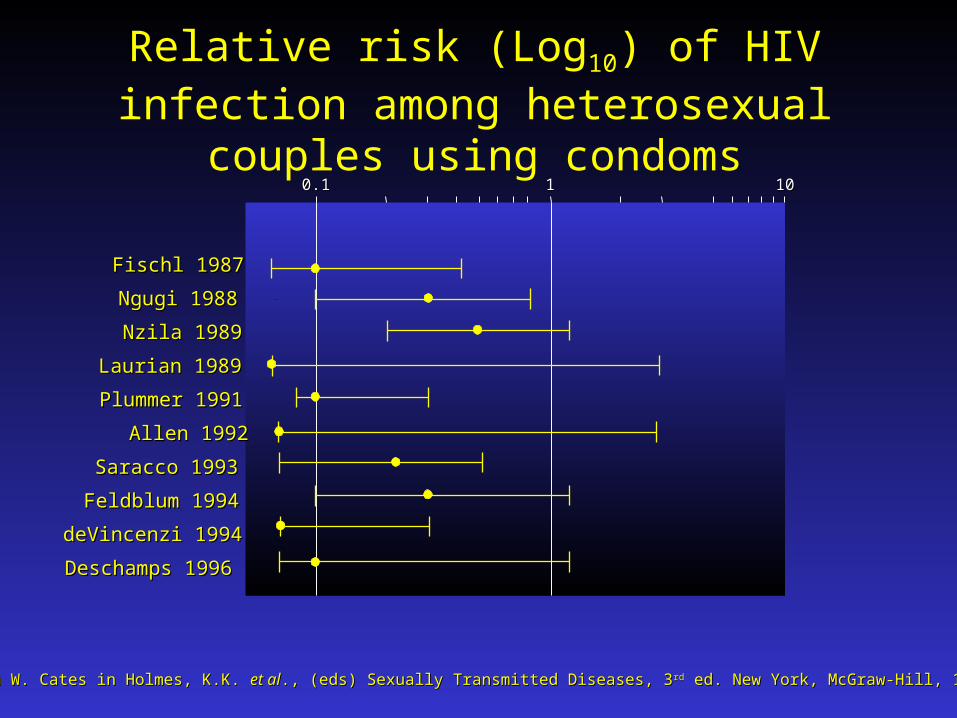
0.10.1 11 1010
Fischl 1987Fischl 1987
Ngugi 1988Ngugi 1988
Nzila 1989Nzila 1989
Allen 1992Allen 1992
Laurian 1989Laurian 1989
deVincenzi 1994deVincenzi 1994
Saracco 1993Saracco 1993
Plummer 1991Plummer 1991
Deschamps 1996Deschamps 1996
Feldblum 1994Feldblum 1994
Relative risk (Log10) of HIV infection among heterosexual couples using condoms
From W. Cates in Holmes, K.K. From W. Cates in Holmes, K.K. et alet al., (eds) Sexually Transmitted Diseases, 3., (eds) Sexually Transmitted Diseases, 3 rdrd ed. New York, McGraw-Hill, 1998. ed. New York, McGraw-Hill, 1998.

Monogamy is good, abstinence is best
You can't catch disease, if you give sex a rest.
But if "love" is your destiny, and you are fated to “dance”
Take heed because condoms are better than chance.

A. Fauci, 2006


















