The Hillingdon Hospitals NHS Foundation Trust Meeting of ...
225
The Hillingdon Hospitals NHS Foundation Trust Meeting of the Board of Directors-Public Tuesday 02 November 2021 10:00 – 12:00 Via MS Teams AGENDA Items which have gone through a Board Sub Committee are marked with an * THHFT Chair: Lord Morse KCB Item Business Items Lead Format Indicative Timing Business Matters 1. Welcome and Apologies for Absence Chair Verbal 10.00 2. Declarations of Interest Chair Verbal - 3. Patient/Service story Medical Director Presentation 10.05 4. Minutes of the meeting held on 05 October 2021 for approval Chair Minutes 10.20 5. Matters Arising/Action Log for noting Chair Action Log - 6. Chair’s Report Chair Verbal 10.25 7. Chief Executive’s Report Chief Executive Report for information and noting 10.30 ITEMS FOR DISCUSSION/DECISION Quality 8. Integrated Quality & Performance Report * • 8.1 Operational recovery plan Chief Operating Officer Report for assurance and discussion 10.30 9. National A&E Survey Director of Nursing Report for assurance and noting 10.50 Workforce 10. People Strategy Update Report Chief People Officer Report for assurance and noting 11.00 11. Raising Concerns/Speaking Up: Six Monthly Report and FTSU Training Proposal FTSUP/CPO Report for assurance and noting 11.10 THHFT Board PUBLIC 02 Nov 2021 Page 1 of 225
Transcript of The Hillingdon Hospitals NHS Foundation Trust Meeting of ...

The Hillingdon Hospitals NHS Foundation Trust
Meeting of the Board of Directors-Public
Tuesday 02 November 2021 10:00 – 12:00
Via MS Teams
AGENDA
Items which have gone through a Board Sub Committee are marked with an *
THHFT Chair: Lord Morse KCB
Item Business Items Lead Format Indicative Timing
Business Matters
1. Welcome and Apologies for Absence Chair Verbal 10.00
2. Declarations of Interest Chair Verbal -
3. Patient/Service story Medical Director
Presentation 10.05
4. Minutes of the meeting held on 05 October 2021 for approval
Chair Minutes 10.20
5. Matters Arising/Action Log for noting Chair Action Log -
6. Chair’s Report Chair Verbal 10.25
7. Chief Executive’s Report Chief Executive
Report for information and noting
10.30
ITEMS FOR DISCUSSION/DECISION Quality
8. Integrated Quality & Performance Report *
• 8.1 Operational recovery plan
Chief Operating Officer
Report for assurance and discussion
10.30
9. National A&E Survey Director of Nursing
Report for assurance and noting
10.50
Workforce 10. People Strategy Update Report Chief People
Officer Report for assurance and noting
11.00
11. Raising Concerns/Speaking Up: Six Monthly Report and FTSU Training Proposal
FTSUP/CPO Report for assurance and noting
11.10
THHFT Board PUBLIC 02 Nov 2021 Page 1 of 225

Finance 12. Finance Reports Month 6*
Chief Finance Officer
Report for assurance and discussion
11.20
13. Charity Annual Report & Accounts 2020/21
Chief Finance Officer
For approval 11.35
Well-led - - - - -
OTHER MATTERS 14. Review of Human Tissue Authority
Guidance CFO For noting 11.40
15. Reports from the Chairs of the Sub-Committees
Trust Secretary
For noting -
ANY OTHER BUSINESS 11.45
Questions from Governors
Questions from the Public
Date of Next Meeting: (Public) Tuesday 02 December 2021 Exceptionally, and until further notice, due to the Covid-19 situation, members of the public have been asked to submit questions in writing to the Trust Secretary in advance of the meeting as the Board will be convening via MS TEAMS.
THHFT Board PUBLIC 02 Nov 2021 Page 2 of 225

1
Present voting: Catherine Jervis Non-Executive Director - Deputy Trust Chair CJ Dr Linda Burke SID/Non-Executive Director LB Neville Manuel Non-Executive Director NM Simon Morris Non-Executive Director SM Janet Campbell Non-Executive Director JC Dr Ayesha Akbar Non-Executive Director AA Patricia Wright Chief Executive Officer PW Jason Seez Deputy Chief Executive Officer and Director of Strategy Jon Bell Chief Finance Officer JB Melanie Van Limborgh Director of Nursing MvL Gubby Ayida Medical Director GA Tina Benson Chief Operating Officer TB Present non-voting: Sue Smith Chief People officer SS Tahir Ahmed Director of Estates & Facilities TA Apologies: Lord Morse KCB (Non-Executive Director - Trust Chair), David Searle (Director of Corporate Affairs) and Pippa Nightingale Chief Nurse, Chelsea and Westminster (Clinical Advisor to the Board) In attendance: Lesley Watts Special Advisor to the Board LW Graeme Wright Deputy Director of Nursing GW Catherine Holly Head of Patient Experience CH Alan Hayes Comms Team AH Chloe Jarvis Comms Team ChJ Debbie Wilson CQC, Relationship Manager DB Karen Blackbond Assistant Director of Service Development and
Implementation KB
Devangi Thakkar Ali Nobakht Narishma Gorsia Tristan Bate Consultant Paediatrician TBa Vikas Sharma Trust Secretary VS Governors: Des Brown Public Governor DB Rosemary Jenkins Public Governor RJ Ian Burnell Public Governor IB Ahmet Moustafa Public Governor AhM John Clark Public Governor JCl Stefan Krok-Paszkowski Staff Governor SK
THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST
DRAFT MINUTES OF THE BOARD OF DIRECTORS
Part-1 Meeting in public Tuesday 05 October 2021 11.00am
Via Microsoft Teams
THHFT Board PUBLIC 02 Nov 2021 Page 3 of 225

2
Members of the public: Armelle Thomas AT
Items marked with * have been through a sub-committee. 1
Welcome and Apologies for Absence Action
1.1 The Chair welcomed all to the meeting. 2. Declarations of Interest
2.1 No declarations of interest were made. 3 Patient/Service story 3.1 3.2
The Director of Nursing (MvL) presented the patient story via pre-recorded video to explain Hugo’s journey through the Neonatal Intensive Care Unit (NICU) at Hillingdon hospital, following transfer from Queen Charlotte’s’ (“QC”) after spent just over 4 weeks in the NICU unit there.
• Hugo Jonathan Peter Hedley arrived 13 weeks early at 26 + 6 weeks gestation. He was delivered naturally at QC on 13th February 2020 at 1:09am and weighing 825g.
• The story is unique as it was in the middle of an unprecedented global pandemic, the amazing staff at the NICU units were adapting to new ways of working in a live environment.
• There were concerns initially but by the end of journey at Hillingdon, the family recognised outstanding care and experience.
• All of the NICU Nurses were amazing and cared for Hugo wonderfully, and also empowered the parents to be able to care for him independently. They were able to assess the correct level of involvement to help parents progress at the same speed as the babies.
• They were good at celebrating key milestones, which was heart-warming and uplifting.
• Above all the care, love, attention, support that Hugo received (but also received as a family) was amazing and helped us navigate a very distressing time.
• Since leaving the NICU, the paediatric care by the consultant has been outstanding with the level of knowledge, professionalism, along with genuine ‘care’ for Hugo.
• Hugo’s journey had been long and hard but he is fighting fit now.
Feedback/suggestions from the family were noted:
• Expressing room / Breastfeeding rooms can be improved to reflect more warmth and inspiration. An in-house lactation
THHFT Board PUBLIC 02 Nov 2021 Page 4 of 225

3
3.3
specialist (even part-time) can be made available for the mothers.
• The family room needs to be better maintained and should have a non-medical fridge to store things and the TV must be working.
• Psychologist to provide psychological support for parents having a premature baby as a key part of mental health journey.
• Peer group sessions to meet parents in similar positions. The Board noted that a lot of work has been done to improve the patient experience/services and the above feedback should be considered to improve it further, for instance, by arranging an event with the friends and families or training the staff, as appropriate, to increase the skills in some of the above areas. The Board thanked the team for sharing the patient story and noted the learning.
4. Minutes of the last meeting and matters arising 4.1
The Minutes of the meeting held on 07 September 2021 were approved as an accurate record of the meeting, subject to the following amendment: TB has sent some minor amendments to the Trust Secretariat to be incorporated: Minute#3.5 – Line to read as: The Chief Operating Officer (TB) explained that some of the funding comes from specialist commissioning and the CCG, unfortunately, this does not always cover the cost of providing an individualised service to each patient.
5 Matters Arising/Action Log 5.1 There were no matters arising.
Action 13.3 – MvL informed that, assurance on the 2018 CQC actions and the CQC Key Lines of Enquiry (KLOE) gap analysis progress is scheduled to be received at the Quality and Safety Committee at its November meeting and the Board in December. PW clarified that this related to the formal closing down of the actions from the 2018 CQC inspections. The CQC KLOE element is the forward-looking gap analysis to enable a self-assessment of where the Trust is positioned against the CQC standards. The Board noted the action log.
Items for Discussion/Decision 6 Chair’s Report 6.1
The Chair (CJ) provided a verbal update noting in particular:
THHFT Board PUBLIC 02 Nov 2021 Page 5 of 225

4
6.2 6.3
With reference to the Recovery Support Programme which is progressing and aligning attention across a number of dynamics of what we do within the Trust. The Chair stressed that good management of resource goes hand in hand with good care. As we continue to implement and respond to the recovery support programme, the Board will be looking particularly to seek assurance that we are embedding best practice in resource management alongside quality improvement initiatives. Concerning the recruitment of an acute chair across North West London, CJ informed that headhunters had now been appointed to recruit and were beginning to source candidates for the role. Governors had been and would continue to be involved in the process.
7 Chief Executive’s Report 7.1
The Chief Executive (PW) drew attention to the following key issues of local, sector and national interest over the last month:
• Appointments in senior posts PW highlighted that Professor Julian Redhead has been appointed National Clinical Director for Urgent and Emergency Care, and will be responsible for helping the NHS to continue to improve 999, 111, A&E and other urgent care services, at the same time as the service faces record levels of pressure off the back of the pandemic.
• We have been notified of funding for the second half of the year with reference to items 1.2 (Funding for the second half of 2021/22 (H2)) & 1.3 (Build Back Better – our plan for health and social care) within the report. PW explained the emphasis over the next six months is to get on very strong trajectory of recovering from the COVID pandemic and in particular, tackling a backlog of patients on waiting lists.
• Work has started to recruit to the Chief Executive post within the Integrated Care System, and stakeholder events and interviews are taking place in October 2021.
• PW informed that COVID numbers within the Trust have settled, at around 7 - 8% of patients in the hospital testing positive. It is a virus which remains very infectious and we continue to implement strict Infection Prevention and Control measures. There has been some new guidance, and we are assessing whether or not we are able to relax some of our local measures. This will be reported back to the Board in due course.
• During October, the Trust has planned an extensive programme of activities in support of Black History and Freedom to Speak Up month. This is a great opportunity to celebrate the diversity of our staff and local population and
THHFT Board PUBLIC 02 Nov 2021 Page 6 of 225

5
7.2
to stress the importance of openness and transparency in all of the Trust’s activities.
The Board noted the update.
8 Integrated Quality & Performance Report * 8.1 8.2 8.3 8.4
The Chief Operating Officer (TB) presented the Integrated Quality & Performance Report (IQPR) and highlighted the following:
• The Month 4 (M4) IQPR is re-presented to the Trust Board following management and Board Committee review in September 2021, and to further enable a systematic governance flow of performance, assurance, scrutiny and challenge from management and the Board sub-committees.
• The M4 report does however; include an update on the Outpatient, and the Emergency Department (ED) Deep dive.
• Performance trajectories of the constitutional standards are not where we want them to be. We have a recovery plan, which will be reported to the board next month. Action: TB
• There are concerns with Pathology KPI's, under performing against trajectory.
• Histology recruitment remains a national challenge, is a key part of our cancer pathway recovery and is being monitored at the North West London Pathology Owners Committee.
• With regards to the ED deep dive further assurance is required in respect of the impact of performance on quality which will be overseen by the Quality and Safety Committee in October 2021.
• The maternity caesarean section deep will be included in M5 reporting.
TB informed on questions received from Non-Executive Director (NM) in relation to triangulation between the IQPR and the previous Chief Executives update. The Rapid Improvement Event for ED saw a 10% improvement in performance during the week in Type 1 ED attendances, which has not been sustained. We are seeing a small improvement in our type 1 attendances and that is where we are working to drive change. NM also asked in respect of the Outpatient first operational recovery, there seemed to be a fall off rather than increase and how that is being addressed? TB explained that for elective operational recovery we have had some challenges with our Did Not Attend (DNA) rates specifically around outpatients, despite booking at 100% or over by 10-12%. A review of our process highlighted some issues with our text system with regards to rescheduling, and also patient feedback indicated that some patients were reluctant to click links within the alerts due to fraud and scam awareness. A review of the text system is
TB
THHFT Board PUBLIC 02 Nov 2021 Page 7 of 225

6
8.5 8.6 8.7 8.8 8.9 8.10 8.11 8.12
underway and in the interim patients are being called to confirm appointments. We expect to reduce DNA rates to reduce to 8% by the end of the week. We are driving our theatre utilisation to ensure we are seeing as many patients as possible to reduce the backlog. There are approximately 62 slots a month that could be utilised. We have adopted a new IPC policy across the sector for patients, which accommodates for low risk/complexity patients to be swabbed on the day if they did not swab 3 days before and proceed with surgery. There is an Elective Recovery plan, which will flow through committees next month to enable oversight and progress. TB highlighted that for H2 focus will be on clearing long-waiters over 104 weeks down to pre-COVID levels, patients waiting over 52 weeks and getting back on track with our RTT. The Deputy CEO (JS) noted that the Rapid Improvement Week methodology encompasses interval reviews at 30, 60 and 90 days which iteratively review interventions, progress and learning. JS suggested the reviews are reported through the Boards Committees. Action: TB JS further added in terms of those improvement trajectories, the updated planning guidance means all trusts need to submit draft updated trajectories in October, with finalised trajectories submitted in November. Those trajectories will also need to go through a board or assurance committee in order to be signed off. TB informed the event yielded 150 opportunities for change improvement. 5 actions are being taken every week, with directional change if there is no value added improvement. We are also seeking support from the Emergency Care Intensive Support Team in terms of how we are measuring and making decisions on interventions/sustainable change i.e. whether to continue, stop or change. Non-Executive Director (SM) sought assurance in respect of stranded patients and highlighted that the board needed to see revised RTT trajectories that reflect actions, and adjustments to reflect where we are now and where we aim to get to. Action: TB TB informed the trajectories will be presented next month, highlighting the importance of them being owned at a local level. Non-Executive Director (LB) asked if learning and key messages from the discharge process and the Rapid Improvement event are
TB TB
THHFT Board PUBLIC 02 Nov 2021 Page 8 of 225
7
8.13 8.14 8.15 8.16
shared within the system? The impact discharge nurses will or have had? are we confident that internal processes are efficient as possible to support the process? TB informed that a second Rapid Improvement Event focused on discharge is taking place in October 2021. The areas of focus will be implementing the nationally recommended tool for discharge ‘SAFER’, which will support a more efficient, effective and standardised process. Alongside this, we will be working with our partner organisations with particular focus on improving in the area of 24 hours from medically optimised to being in your next place of care, working with the HHCP, CCG and local authority. Benchmark data for stranded patients, shows the Trust as an outlier, however, the rehabilitation unit is included when most other organisations, particularly, those in North West London, excluded this and the Trust is applying similarly to the national team for the exclusion to be applied. TB provided assurance that focused work and action are improving performance, but placement delays remains are area of focus and requires improvement with partner support. The Board noted the Integrated Quality Performance Report.
9 Winter Plan 2021/22 * 9.1
The Chief Operating Officer (TB) presented the Winter Plan 2021/22 as an update of where we are, highlighting the following:
• The plan has been developed working across the sector and locally (PLACE winter plan). Much of what we are trying to deliver is prevention of unnecessary attendances and admissions, streamlining of discharges and rapid care of patients in the Community.
• The board will recognise that failure to deliver scale that we are trying to achieve in the Community services or in prevention will result in increased pressure within the Trust.
• Our biggest scheme is to reduce our length of stay by one day and actions plans are in place to do that. Implementing the SAFER Bundles, good board rounds with less variation and good discharge processes all of which will be the areas of focus during the Rapid improvement event for discharge scheduled w/c 18th of October 2021,
• TB highlighted that even with that reduction there would still be a gap of approx. 44 beds, assuming that there will be a 20% increase in activity. TB alerted the board to papers within North West London suggesting a 37% increase and looking to a 92% occupancy, whereas the Trust have modelled at a
THHFT Board PUBLIC 02 Nov 2021 Page 9 of 225

8
9.2 9.3 9.4 9.5 9.6 9.7
20% increase and 95% occupancy. At worst-case scenario, the deficit would be over 100 beds.
• TB informed the modelling does not include an escalation ward to use, which would be unfunded, but a bid has been put forward into the sector for winter funding cost pressures which would fund an escalation ward, but alerted the committee of the associated risks in doing so in respect of quality and safety.
Non-Executive Director (NM) asked how the assumptions in respect of Flu have been compared to previous winters and given an expected increase this winter and secondly should the risk materialise how long would it take to mitigate those risks i.e. new staffed beds or alternatives. TB clarified, we have seen assumptions in terms of flu nationally as high as 37%. Previous increases within Hillingdon range between 9-11%. Therefore, we felt 20% reflected a significant increase. In terms of opening an additional ward, detailed planning is underway, with the aim of being able to enact those plans within 48 hours. The Chief Executive Officer (PW) added the gap analysis sits over a very detailed winter plan and an escalation plan that is in place for winter emergencies. During Covid, skills have been developed locally and at sector level, to support bed modelling and scenario planning. Working in PLACE will support forward planning to foresee risks and mitigations and is key in supporting how we ramp up as a sector to support winter pressures. The board noted the winter plan, lack of stretch within the system, potential risk and the need for us to work collaboratively as part of PLACE, and sought clarity about how the board will remain assured that the plan is being delivered and within our capabilities. Action: TB
TB
10 Safer Staffing update – Nursing- Establishment review * 10.1
The Director of Nursing (MvL) presented the Nursing Establishment review and highlighted the following:
• The establishment review is a mandated requirement presented to the board twice a year.
THHFT Board PUBLIC 02 Nov 2021 Page 10 of 225

9
10.2 10.3 10.4 10.5
• The paper presents the findings from the midterm Inpatient Nursing Establishment Review. It sets out the methodology and process used to ensure that establishments are adequate for patient need, in line with National Quality Board (NQB) standards.
• The aim of the review and triangulate information, to address safe staffing and the quality of care that comes through that staffing. There is also an element of professional judgment that is brought into this particular review of the report.
• MvL explained exclusions to this report are escalation wards, the new respiratory care unit and the Emergency Department, but assured the board that these will be reviewed in different ways and using alternative appropriate tools, highlighting the tool being developed by the Shelford Group which is expected later this year.
• The review demonstrated our funded ward establishments were in line with the patient need.
• The report highlights a reduction of beds within the Acute Medical Unit and the divisions are considering how they can release, redirect and align resources in relation to need within the division.
• The review recommends an Increase in headroom (provision for study leave, personal development, annual leave, maternity leave etc.) from 21% to 23% (nationally 24%). We are undertaking some further work to drive that forward to further support our staffing establishment.
In conclusion, MvL assured the board that our staffing changes are reviewed on a regular basis, needs are reviewed dynamically on a daily basis, and further assured the board that this report concludes that the inclusive funded wards have the required establishments to provide safe care. Non-Executive Director (LB), highlighted an action from the Quality and Safety Committee following their review and scrutiny of this report, regarding the need for more granular information to enable triangulation and early identification of hotspot and risk areas. The Chief People Officer (SS) provided assurance that work is already underway in this respect and will be brought to the next People Committee. The board noted the report, assurance with regard to our funded establishment, the further programme of work planned and for the board to receive a further update in six months’ time. Action: MvL
MvL
THHFT Board PUBLIC 02 Nov 2021 Page 11 of 225

10
11 People Strategy * 11.1 11.2 11.3 11.4 11.5
The Chief People Officer (SS) presented the Trust’s People Strategy highlighting:
• It outlines our ambition to be a great place to work. • Offers information about where we are, our workforce, and
strategic context. • The People Strategy has been designed to promote a
culture that reflects the Trust’s values, and 4 pillars which are:
o Looking after our people o Belonging in our Trust o New ways of working & delivering care o Growing for the future
• There are measurements of success within it. • Outlines our approach from a People in Organisational
Development (P&OD) perspective and the role of the P&OD team.
• It also outlines how staff can work with us to take this ambition forward.
• The Strategy has been subject to extensive consultation. • Applies to both staff and volunteers. • The strategy is three years in duration and we are already
working to year one. The Chair (CJ) noted the focus on new roles and skill mix, sought assurance on how we ensure staffing is benchmarked and reflects current practice. SS informed that a significant amount of work has been undertaken through the redevelopment programme, which is referenced throughout the strategy. SS provided assurance that we are considering this via the redevelopment work streams as part of the workforce redevelopment group to make sure that we have a clear workforce plan that reflects where we are now and where we want to be in the next five years. Non- Executive Director (SM) added that the Strategy had been considered and discussed at length via the People Committee and stressed the importance of now communicating and delivering the strategy. SM emphasised the need to start seeing some movement and progress and that the People Committee would be seeking some further granularity and assurance in terms of KPIs, costings given that one of the major drivers for the financial pressures on the trust is the use of agency staff. The People committee will be seeking assurance that we are on top of that and managing that through the review of the workforce plan and strategy.
THHFT Board PUBLIC 02 Nov 2021 Page 12 of 225
11
11.6 11.7 11.8 11.9 11.10 11.11 11.12
Non-Executive Director (LB) asked: 1 What rationale was applied to select the measures of
success? 2 How will we know that we are were making progress? What
would we expect to see? 3 How will that fit with other priorities i.e. finance?
In response to question 3, SS referred to the financial recovery board and programme of work underpinning that. SS added that she as lead for workforce and the COO (TB) as the lead for agency reduction are working in partnership. Our financial recovery is predicated by effective management of our long-term sickness and a significant reduction in our vacancies and in improvement in our relationship with agencies in terms of agency and bank fill, an enhancement in our bank fill as well. All aspects of workforce are monitored through the financial Recovery Board and we will be providing periodic updates to the People Committee. In response to question 1, SS explained that the four key themes correlate through to the NHS people plan that in turn underpins our NHS staff survey. The Hillingdon people promise correlates back through to the NHS people promise and we felt it was important that our measurements of success reflect our external reporting arrangements/agenda against which we will be monitored. In response to question 2, SS explained that the targets we are aiming for in our trajectory for improvement will be agreed through the People Committee. In terms of where we expect to be at the end of 2022, we have agreed KPIs. However, we may well decide as we go into the new calendar year and in agreement with Trust Management Board that we wish to amend those KPIs and make them tighter in order to meet our trajectory. The Chief Executive Officer (PW) thanked SS and her team and all contributors that have supported the development of the strategy. PW re-emphasized the need for effective communication and accessibility of the strategy. The strategy needs to be dynamic and we will need to review this every year. PW further supported the board to approve the strategy. The Board approved the Trust’s People Strategy.
12 Trust Seasonal Influenza and COVID vaccination plan * 12.1
The Chief People Officer (SS) presented the Trust’s Seasonal Influenza and COVID vaccination plan highlighting:
• The COVID booster campaign commenced on the 20th of September 2021.
THHFT Board PUBLIC 02 Nov 2021 Page 13 of 225

12
12.2
• 1417 staff had been vaccinated at the end of last week in terms of the COVID booster, with a further 2000 staff to vaccinate.
• It is expected that flu vaccinations available on site from the 18th of October 2021, and we do know that a number of staff are holding back for their double vaccination opportunity.
• The paper outlines our approach and we will be providing a monthly update within the Integrated Performance Report (IQPR) to provide assurance that we are progressing to plan.
The board received assurance on the Trust’s planned arrangements to deliver the seasonal influenza vaccination and COVID-19 booster programme and noted the Trust’s Influenza and COVID vaccination plan.
13 Finance Reports Month 5 13.1 13.2
The Chief Finance Officer (JB) presented the month 5 report and highlighted the following:
• Month 5 was a challenging month with an in month deficit of £1.7m.
• The year to date position is an adverse variance of £4.5m. • Drivers for the position continue to be:
o Pay as the main driver o Escalation ward open o ICU pressures o Sickness levels in nursing were around 6%, which
was the highest since January, with little headroom. • A combination of which, resulted in a significant amount of
agency spend, much of which was off-framework. • Expenditure on pay was the highest we have seen so far
this year at £17m. • We had predicted that we would see an improvement in
August with a forecast of £1.2m, but ended a drift by £0.5m. JB highlighted work underway to address the deficit including:
• Addressing pay o Sickness absence levels o Funding for ICU, through a sector approach o Escalation ward is now closed o Reduction in agency staff, particularly off-
framework. Analysis suggests that the premium we have paid so far off framework this year is an escalated rate.
• Non-delivery of TIP. Our plan was to delivery £10.3 million, however, year to date only 1.5m of TIP has been delivered which is £2.8m adrift of plan.
THHFT Board PUBLIC 02 Nov 2021 Page 14 of 225

13
13.3 13.4 13.5 13.6 13.7 13.8
• These are key areas of focus as part of the Recovery Support Programme and Financial Recovery Board.
• JB informed the Board that the Trust is an outlier nationally against the Better Payment Practice Code with 69% of invoices paid with 30 days. A remedial plan is in place with a trajectory for improvement to raise in month performance to 95% by year-end.
• The Trust has spent £6.7 m of Capital at the end of August 2021, against a plan of £23.7m. Much of this £17m underspend relates to HIP2 schemes (approximately £8.9m), where the Trust is awaiting confirmation that funding will be in place. The Trust continues to spend some of the HIP2 funding at risk, particularly the seed funding for completion of the outline business case.
• The other areas where there is significant underspend is the Digital Care Record project £2.7m, Fire remediation £2.1m and the Salix project £1.4m but at present there is no risk that these projects will not spend to plan by the end of the year.
• A re-profiling and re-budgeting exercise is underway with regards to Capital spend which will be reported to the Finance & Performance Committee October, and the Board in November, with an expectation that the HIP spend this year will be lower than planned.
The Non-Executive Director (NM) to what extent the Trust was using cost offsetting as a mitigation of the overspend, and are we being aggressive enough. JB confirmed the Trust was using cost-offsetting, a vacancy factor is within the TIP. Where we can we will hold vacancies, which are not required quickly or critical i.e. Nursing, but equally there is a need to recruit quickly in areas where agency spend is high. We have also been looking at variances within non-pay, and holding those variances where there is underspend. In terms of aggressiveness, JB agreed that there is potentially more we could do, but provided assurance that is an area of focus. The Chief Executive Officer (PW) added that discretionary spend is another area currently being explored. The Non-Executive Director (JC) sought assurance with regards to the use of off-framework as a recurring theme and the approach in terms of behavioural change. The Chief Operating Officer (TB) explained that the detailed work undertaken as part of the establishment review has been reported back to ward areas so there is absolute clarity on their
THHFT Board PUBLIC 02 Nov 2021 Page 15 of 225

14
13.9 13.10 13.11 13.12 13.13 13.14 13.15
establishments and what headroom is available in each budget (with the exception of the Emergency Department, The Acute Respiratory unit and ICU). For all wards where the correct establishment is in place, we will be stopping any off-framework requests, to support in tackling behavioural change. TB emphasised that we absolutely need to keep our wards safe, but greater support and scrutiny is being given to requests, to support managers in undertaking acuity assessments and utilising alternative staff to manage workload and maintain patient safety. In ICU, a full establishment is underway, and a new unit lead has commenced in post, which will support the review and reduction of the off framework nursing spend for ICU. We are also continuing to secure funding for three Level 3 beds. In the Acute respiratory Unit, we have gone from having 8 high acuity level 1 1/2 beds in the organisation to 20 on most occasions and we will be asking for the funding for those beds. Through the Workforce Recovery meetings, we have agreed to recruit additional band 5s and short-term band 6s. There is some additional funding available for the Emergency Department; a business case is being completed this week to ensure transparent governance for the change. Once we have understood the correct establishments for those areas we will be taking the same approach and setting a trajectory to stop/limit the use off-framework agency. The Chief People Officer added that we are working with the various suppliers of temporary staffing to be clear about what rates we will pay. We are also relaunching our bank offer so staff are aware that they can work extra on the bank. The Board remains extremely concerned with the financial position. There is an increased understanding of what the issues are with mitigations actions. We have yet to see those actions making a significant difference, or a trajectory for improvement and assurance is needed in respect of this. The Board will be working through the detail of the Recovery support programme in the month ahead.
14 H1 and Full Year Forecast* 14.1
The Chief Finance Officer (JB) presented the H1 and Full Year Forecast, highlighting:
• The position has moved on since last seen at Month 4 by the Board in Private, as now seen in the Month five position.
• We were predicting that we would have a forecast deficit of between £4.1 and 5.4 million for the first half of the year (H1)
THHFT Board PUBLIC 02 Nov 2021 Page 16 of 225

15
14.2 14.3
• The the worst case or the more likely case scenario now is around £6.1 million for the outturn for H1.
• In relation to the forecast for the second half of the year (H2). New guidance has recently been released, which is being reviewed to understand the impact. Particularly with the changes that have been proposed to the Elective Recovery Fund (ERF) and how the fund will work in the second half of the year.
• JB added that we are working through the planning guidance and it will be reflected in our new plan.
• If we can resolve the ITU funding issues, deliver some additional income from ERF and get a grip of the pay run rate then we should be able to see an improvement in the forecast outturn.
The Chair (CJ) highlighted the need for accurate and scenario based forecasting with greater granularity in the next iteration of forecasts. Action: JB The Board noted the H1 and Full Year Forecast.
JB
15 Reports from the Chairs of the Board Sub Committees 15.1
The Reports from the Chairs of Board Sub Committees were received by the Board. The Board noted the reports for assurance from the Chairs of the Board Sub Committees for the meetings convened in September 2021.
ANY OTHER BUSINESS - None Questions from Governors There were no questions from Governors Questions from the Public Armelle Thomas: Queried, the CEOs report reference to 78% COVID Patients? PW clarified, currently there are 7 to 8% of patients within the hospital have tested positive for COVID. These are not necessarily patients who are in hospital because they have COVID. Armelle Thomas: Last month the Trust reference 3.2% of staff were on long-term sick, and asked how the Trust was addressing this? SS responded that at the end of September we had 77 staff off long term sick. The top reason for absence was linked to stress, anxiety and depression, and reflects the very difficult 18 months that staff have been through. We have plans in place for every single member of staff and with the hope that we can return them to the workforce, but if not, we can support them in other ways. Armelle Thomas: Is the COVID booster being offered to every member of staff? SS clarified that the booster is being offered to every member of staff. The Chair thanked colleagues for their attendance and closed the meeting. END Next meeting: Tuesday 02 November 2021 at 11.00am
THHFT Board PUBLIC 02 Nov 2021 Page 17 of 225
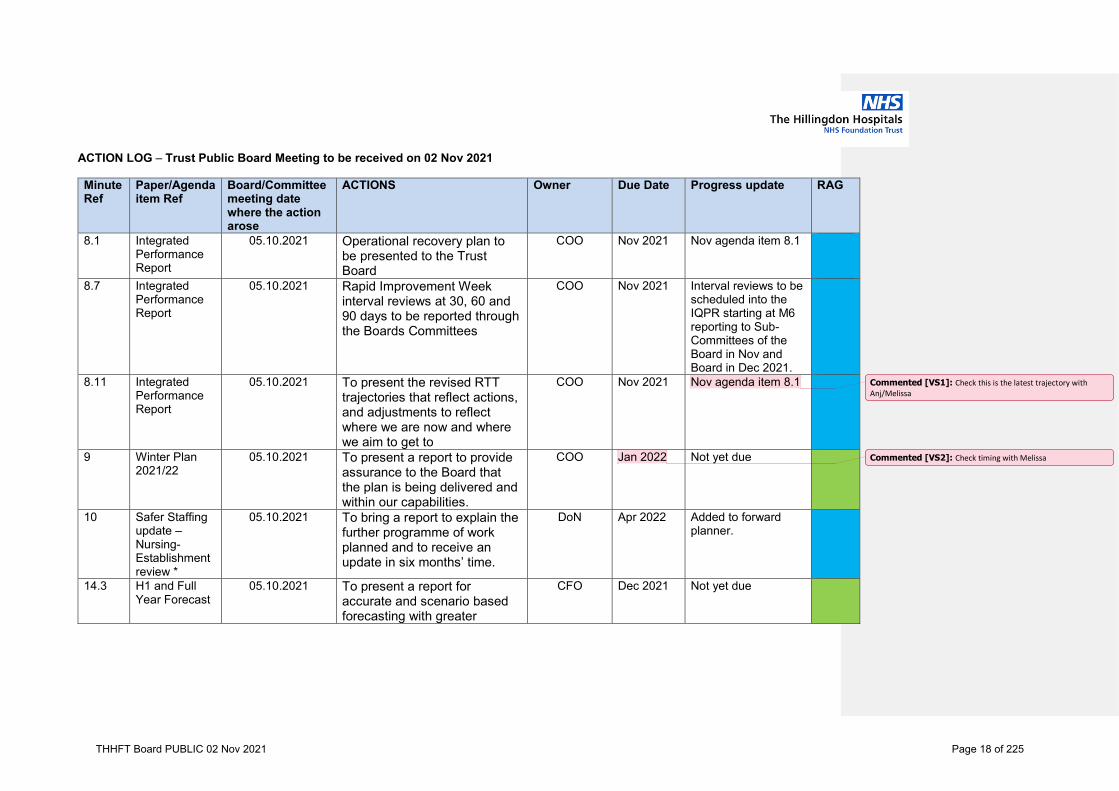
ACTION LOG – Trust Public Board Meeting to be received on 02 Nov 2021
Minute Ref
Paper/Agenda item Ref
Board/Committee meeting date where the action arose
ACTIONS Owner Due Date Progress update RAG
8.1 Integrated Performance Report
05.10.2021 Operational recovery plan to be presented to the Trust Board
COO Nov 2021 Nov agenda item 8.1
8.7 Integrated Performance Report
05.10.2021 Rapid Improvement Week interval reviews at 30, 60 and 90 days to be reported through the Boards Committees
COO Nov 2021 Interval reviews to be scheduled into the IQPR starting at M6 reporting to Sub-Committees of the Board in Nov and Board in Dec 2021.
8.11 Integrated Performance Report
05.10.2021 To present the revised RTT trajectories that reflect actions, and adjustments to reflect where we are now and where we aim to get to
COO Nov 2021 Nov agenda item 8.1
9 Winter Plan 2021/22
05.10.2021 To present a report to provide assurance to the Board that the plan is being delivered and within our capabilities.
COO Jan 2022 Not yet due
10 Safer Staffing update – Nursing- Establishment review *
05.10.2021 To bring a report to explain the further programme of work planned and to receive an update in six months’ time.
DoN Apr 2022 Added to forward planner.
14.3 H1 and Full Year Forecast
05.10.2021 To present a report for accurate and scenario based forecasting with greater
CFO Dec 2021 Not yet due
Commented [VS1]: Check this is the latest trajectory with Anj/Melissa
Commented [VS2]: Check timing with Melissa
THHFT Board PUBLIC 02 Nov 2021 Page 18 of 225

granularity in the next iteration of forecasts
8.1 Integrated Performance Report
03.08.2021 To undertake and present a local deep dive of our caesarean sections to identify any specific issues and recommendations for future practice
MD Nov 2021 Reported to the Quality and Safety Committee October 2021
9.2 Quality Priorities 2021-22
03.08.2021 The future reports to include the journey segregated into quarters of the year to understand the phased delivery of these priorities and what the Trust should expect to see in each quarter.
DoN December meeting
The QSC is receiving a detailed update on the Quality Priorities throughout October (x2) and November (x2), and subsequent reporting to the Board.
13.3 CQC/HSE action plan update (sec 29 & 31) (this action is in relation to the 2018 inspection)
01.06.2021 There were significant concerns about the number of actions still open from the previous inspection in 2018 and it was agreed that the progress on them would be discussed in the next meeting.
DoN December meeting
Assurance on the 2018 CQC actions, and the CQC Key Lines of Enquiry gap analysis progress scheduled to be received at the QSC at its November meeting, and Board in December.
RAG RATING OWNERS
Key Completed On Track Some slippage Serious Issues
Commented [VS3]: Check with Gubby re board
THHFT Board PUBLIC 02 Nov 2021 Page 19 of 225

Name initials Lord Amyas Morse Trust Chair Patricia Wright CEO Jason Seez Deputy CEO Tina Benson COO Jon Bell CFO Dr Gubby Ayida MD Melanie v Limborgh DoN Tahir Ahmed DoE Sue Smith CPO
THHFT Board PUBLIC 02 Nov 2021 Page 20 of 225

1
Chief Executive’s Report
THHFT Board Meeting-Public
Date of the meeting: 02 November 2021
ITEM: 7
Purpose of the Report/Paper: To provide an update from the Chief Executive on key issues of local, sector and national interest. For: Information Assurance Discussion and input Decision/approval Executive summary: This report provides an update from the Chief Executive on key issues of local, sector and national interest over the last month.
Sponsor (Executive Lead):
Patricia Wright, Chief Executive
Author:
Patricia Wright, Chief Executive
Author contact details:
Risk implications – Link to Board Assurance Framework or Corporate Risk Register:
All relevant
Legal/Regulatory/Finance/Quality & Safety/ HR/E&D/Engagement/Communications/Reputation or Sustainability implications:
All
Link to Relevant CQC Domain: Safe Effective Caring Responsive Well Led Link to relevant Corporate Objectives/strategic aims:
All
Document previously considered by: NA Recommendations: The Board is asked to note the information provided in the report.
THHFT Board PUBLIC 02 Nov 2021 Page 21 of 225

2
Chief Executive’s Report (November 2021)
Introduction This report provides an update from the Chief Executive on key issues of local, sector and national interest over the last month.
1. National 1.1 The government has announced an independent review of leadership in health
and social care, to be led by retired Vice Chief of the Defence Staff, General Sir Gordon Messenger.
1.2 On 27 October 2021 the Chancellor of the Exchequer delivered the Comprehensive Spending Review. Much of the detail in the review has been trailed in advance, with additional funding being allocated to the NHS to reduce waiting lists.
1.3 The Care Quality Commission (CQC) published its new State of Care report on 22 October 2021, The state of health care and adult social care in England 2020/21, setting out its annual assessment of the quality of health and social care in England over the past year. Key points include:
• CQC highlights the impact of COVID-19 on people’s experiences of care, with many struggling to access the care they need due to the strain on health and care services.
• It emphasises its concerns over adult social care services and warns of a “tsunami of unmet need across all sectors” unless workforce pressures in social care are reversed and capacity in the sector increased.
• It emphasises the challenges in access facing some groups over others, such as older people, people from Black and ethnic minority backgrounds, people from more deprived areas and those with a learning disability. It recognises that trusts are keen to tackle their waiting lists with a focus on health inequalities.
• CQC raises particular concerns around urgent and emergency services, ambulance handovers, a rise in demand for mental health services, and staffing pressures in adult social care. It recognises the impact of these ongoing pressures on the health and social care workforce.
• It singles out the benefits of the ‘discharge to assess’ model for managing transfers of care, and highlights that continued funding for it would support local partners to build relationships and increase capacity in rehabilitation and step-down services.
THHFT Board PUBLIC 02 Nov 2021 Page 22 of 225
3
• The report focuses on the significant quality concerns stemming from closed cultures, and noted a higher risk of closed cultures in mental health services. CQC also highlights its quality concerns in maternity services where it feels improvement has not been fast enough.
• CQC discusses the challenges for integrated care systems, including the need to better understand health inequalities, for better integration of health and social care, and the urgent need to prioritise workforce planning.
2. NWL Integrated Care System (ICS) 2.1 Dr Genevieve Smallwood has been appointed as ICS Medical Director
following the move of Dr Redwood to a national role. Dr Smallwood is a GP in Harrow.
3. Local 3.1 Regulation The Trust continues to work closely with the Recovery Support Programme
Team to address financial issues and awaits confirmation from the CQC about the removal of licence conditions.
3.2 COVID-19 The number people admitted who have tested positive for Covid-19 has
continued to drop during October 2021 with around 20-25 inpatients at any one time. Levels of infection in the wider population continue to increase, although the impact of this has not yet impacted on the Trust in terms of admissions although we are monitoring rates very closely. Pre-booked visiting recommenced in mid-October 2021.
3.3 Black History and Freedom to Speak Up month – October 2021 The extensive programme of activities in support of Black History and
Freedom to Speak Up month in October has been very well received and will be used as a platform to maintain our focus on speaking up and valuing diversity.
3.4 Awards and Accolades Our Estates & Facilities teams have won a number of awards in relation to
sustainability, waste management and partnership working.
The Finance Leadership Council has accredited the Finance team at Level 1 for achieving consistent good practice in Financial Skills Development.
3.5 Cares+ The Trust ran an ‘Improving Non Elective Patient Flow’ Discharge Rapid
Improvement Event from 18-22 October 2021.
Over 40 improvements were identified
THHFT Board PUBLIC 02 Nov 2021 Page 23 of 225

4
• Departure Lounge established
• New process to declare beds, supported by Standard Work
• Pharmacy runner introduced for TTAs
• ‘Green card’ system to improve visibility of medically optimised patients
• Improved communication with patients re discharge plans
• Real time access to Social Care records for Patient Flow Coordinators
The feedback session was attended by staff from Quality Improvement Teams from other Trusts in England as well as our own staff and the event was highly commended. The plan is to repeat the event to check that changes have been embedded and to look at different cohorts of patients who may benefit from a change in pathways.
THHFT Board PUBLIC 02 Nov 2021 Page 24 of 225

Integrated Quality Performance Report (IQPR)
THHFT Board Meeting-Public
Date of the meeting: 2 November 2021
ITEM: 8
Purpose of the Report/Paper: The IQPR is produced by the Trust on a monthly basis to monitor key clinical quality and patient safety indicators, national and local target performance, and financial performance. The IQPR provides assurance to the Board that all areas of performance are monitored with sentinel indicators, allowing the Board to gain assurance regarding actual performance, Trust priorities and remedial actions. This new version of the IQPR is continuing to be reviewed and adapted in line with feedback provided. Standards are being allocated to each indicator however for the quality standards, these are being worked through however due to current pressures these will be finalised over the next month. For: Information Assurance Discussion and input Decision/approval Executive summary: After reviewing the data indicators and information produced for the Integrated Quality and Performance Report, for August, there are a number of areas that prove to be a risk for the organisation and require actions to be undertaken to address.
• The opening of escalation beds to meet demand, vacancy, and staff unavailability (25.3%), sickness, turnover and the increased requirement for enhanced care all contributed to significant nurse staffing challenges during Aug 21.
• RMN usage remains high across clinical areas. RMN usage, vacancy rate and opened escalation is contributing to the high agency use and driving the increase in off framework requests – 8.8% (6.3% July 21).
• Cohort 3 of internationally recruited nurses landed 3rd September with a further 37 FTE to land before 31st December 21.
• Moisture lesions incidents has significant increased this month and have failed to meet the standard for the last five months. Further review and deep dive is required to provide greater assurance on a drive to improvement.
• A 35 point Fire Safety Action Plan for 2020 & 2021 was developed to pick up
on the actions from the Authorised Engineer Report and the LFB Enforcement Notice. Currently 23 of the 35 actions have been fully completed and the remaining 12 are on track. 10 of the 35 actions on the plan specifically relate to the LFB Notice. To date - 6 of the LFB actions have been completed with the remaining 4 actions being directly related to the completion of the capital programme on fire safety improvements in the Tower.
THHFT Board PUBLIC 02 Nov 2021 Page 25 of 225
• Respiratory Protective Equipment (RPE) compliance is currently at 81% with
a target of 90%. This dip is directly related to the new doctor induction and work is underway to ensure an appropriate process is put in place for our new intakes.
• VTE remains below target whilst the recent Trust audit demonstrated an improvement compared to the previous year more work is required to ensure we are meeting the standards. The action plan emphasises the need for training and focus through quality rounds.
• Whilst our complaints performance remains strong the volume of complaints and PALs have risen in month with key themes being around patient communication which reflects challenges faced by staffing gaps on wards but also with outpatient letters ans text messages being unclear and process needing to be improved.
• The Trust held a trust-wide Rapid Improvement Event from 16-22 August to help improve patient flow in the Urgent and Emergency Care setting. The week proved to be very successful. Some rapid improvements that were implemented in the week included the introduction of armbands for Nurse in Charge, the introduction of the ‘perfect shift’ in green Zone and Visual Management installed on flooring to guide patients from ED to SDEC – new black line on floor. The ongoing actions from this week are being monitored through the Non Elective Steering Group.
• August has been a challenging month across all elective operational performance indicators, with annual leave and sickness impacting significantly on the Trust’s ability to deliver against the constituitional standards and the operating plan trajectories. A detailed recovery plan which demonstrates the expected impact of the actions and when trajectories will be delivered is being produced. A high impact action plan can be found in the responsive section of the report.
• The newly recruited EDI Lead joined the Trust on 16th August. The Trust’s EDI strategy implementation is focused on the Year 1 objectives and actions of the three year EDI Plan. There are key actions taking place every month as part of this.
• Given some of the challenges around staff sickness, a Health and Wellbeing
Steering Group is being set up to commence in September, with a remit to develop a comprehensive staff health and wellbeing programme aligned to the national staff wellbeing framework.
Sponsor (Executive Lead):
Tina Benson, Chief Operating Officer
Authors:
Melissa Mellett, Director of Operations Anjali Joshi, Director of Operations Vikas Sharma, ADIG
THHFT Board PUBLIC 02 Nov 2021 Page 26 of 225

Tom Ijaz Yates, Head of Workforce Information
Author contact details:
[email protected] [email protected]
Risk implications – Link to Board Assurance Framework or Corporate Risk Register:
All
Legal/Regulatory/Finance/Quality & Safety/ HR/E&D/Engagement/Communications/Reputation or Sustainability implications:
Finance Quality and Safety HR
Link to Relevant CQC Domain: Safe Effective Caring Responsive Well Led Link to relevant Corporate Objectives/strategic aims:
All
Document previously considered by: Operational Management Group, Trust Management Board, Quality & Safety Committee, Finance & performance and People Committee
Recommendations: The Board is asked to note and discuss the IQPR.
THHFT Board PUBLIC 02 Nov 2021 Page 27 of 225
Integrated Quality and Performance Report
1
August 2021
THHFT Board PUBLIC 02 Nov 2021 Page 28 of 225

2
Is Care Safe?
Discharge Summaries
This project has developed into a concurrent 3-phase programme.
In-month progress has been impacted by leave in the PMO, ward staff capacitydue to leave, ward closures & the participation in the Trust-wide RapidImprovement Event.
Phase 1: Eliminate backlog• It has become apparent that ward processes have not established into
business as usual, there has been an increase in the number of ‘Ready notIssued’ discharge summaries. Improvements in practice have not beenmaintained in the absence of PMO support. Further work is required withwards to establish & embed processes during periods of leave, this willbecome a key focus for September & October.
Phase 2: Improve Standard (BAU) Processes• Again we have seen an increased backlog generated through late August &
early September where the new process to complete all RIP paperwork in theBereavement Suite have not been sustained. This in part will be due to thejunior doctor rotation in August. An improvement plan to recoverperformance will be agreed with the team.
Phase 3: Improve Timeliness of Completion• The Transformation Team are working with the Information Team to get
weekly KPI monitoring data and nursing staff will be supported andempowered to flag when summaries are not available to share with patientswho are ready to be discharged.
• We are also investigating possible data quality issues that may contributing tothe failure to meet targets.
• This work remains ongoing & will be picked up in September.
Pressure Ulcers
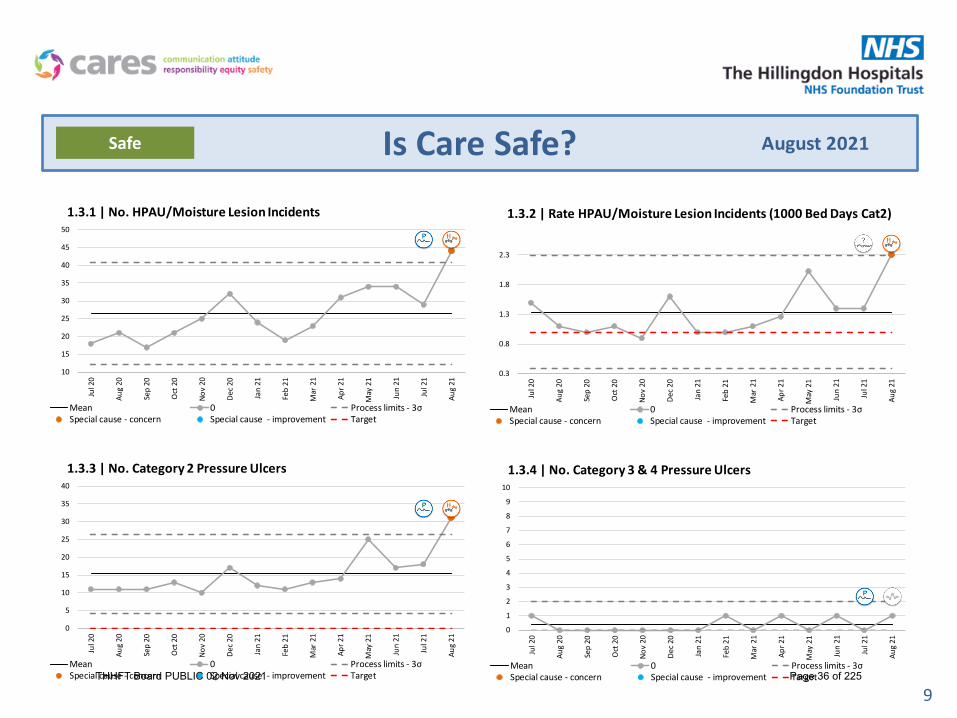
• There were 44 Hospital Acquired Pressure Ulcers/moisture lesions were recorded in August 2021; this is a slight reduction on the previous months reported incidents.
• The rate of pressure ulcers category 2+ was 2.3 per 1000 bed days which is a significant increase on the previous month.
• In August 2021 there were 1 Cat 3 or 4 HAPU reported, however there were 2 unstageable PU and 3 deep tissue injury– investigations into the themes and learning from these are underway.
• The Clinical governance team are sharing a weekly dashboard – highlighting the current focus of concerns for pressure ulcers.
• A weekly meeting between hospital and community TVN’s, clinical governance and the safeguarding team is now embedded allowing for open and shared information around patients transitioning between areas of care, with a reduction in delays of appropriate treatment of patients with complex wounds.
• A week focusing upon staff development and education is due to running from 13th September 2021, with a focus upon pressure ulcers on heels due to an increase in the number of this type of incident being reported. Ward based teaching is planned with good engagement from both divisions.
• A static mattress audit and replacement programme was undertaken at THH in August 2019 – with more than 90 mattresses being replaced. Dates are being planned for the same process at the MVH site.
Patient Falls
• 52 inpatient falls were recorded in August 2021 at a rate of 3.8 per 1000 bed days., and there we no falls with fracture.
• Falls prevention sensors are available in the equipment library for use in clinical areas for patients who are at high risk of falling.
• Two of our unplanned care frailty wards have purchased bathroom falls sensors – a positive response with the aim of reducing of falls in bathrooms.
• The Clinical Governance team are sharing a weekly dashboard highlighting the focus of concern for falls across the trust.
• Falls Awareness week is in September 2021 with a communication campaign being planned to enhance awareness trustwide.
• Visual aids to help identify patients at increased risk of falls are being explored – with areas to pilot these tools to be identified.
August 2021Safe
THHFT Board PUBLIC 02 Nov 2021 Page 29 of 225
3
Is Care Safe?
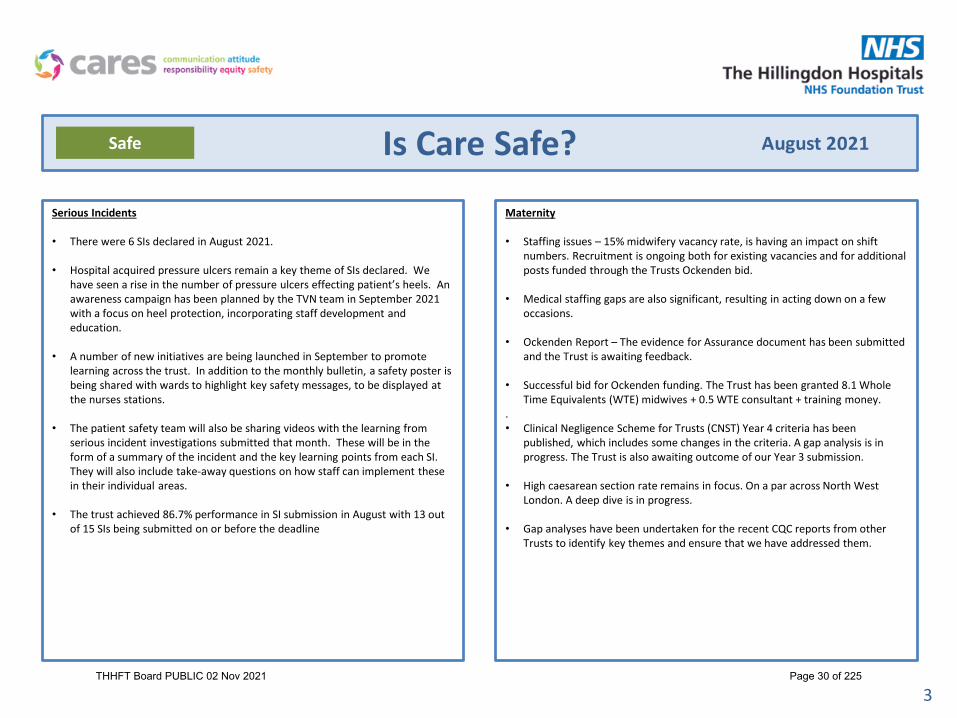
Serious Incidents
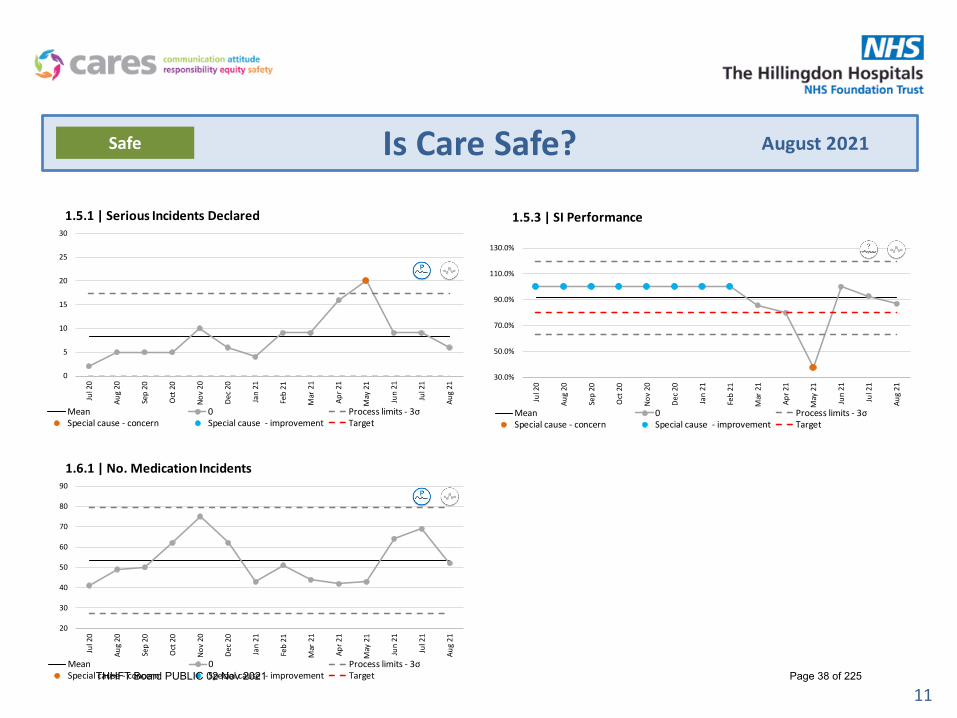
• There were 6 SIs declared in August 2021.
• Hospital acquired pressure ulcers remain a key theme of SIs declared. We have seen a rise in the number of pressure ulcers effecting patient’s heels. An awareness campaign has been planned by the TVN team in September 2021 with a focus on heel protection, incorporating staff development and education.
• A number of new initiatives are being launched in September to promote learning across the trust. In addition to the monthly bulletin, a safety poster is being shared with wards to highlight key safety messages, to be displayed at the nurses stations.
• The patient safety team will also be sharing videos with the learning from serious incident investigations submitted that month. These will be in the form of a summary of the incident and the key learning points from each SI. They will also include take-away questions on how staff can implement these in their individual areas.
• The trust achieved 86.7% performance in SI submission in August with 13 out of 15 SIs being submitted on or before the deadline
Maternity
• Staffing issues – 15% midwifery vacancy rate, is having an impact on shift numbers. Recruitment is ongoing both for existing vacancies and for additional posts funded through the Trusts Ockenden bid.
• Medical staffing gaps are also significant, resulting in acting down on a few occasions.
• Ockenden Report – The evidence for Assurance document has been submitted and the Trust is awaiting feedback.
• Successful bid for Ockenden funding. The Trust has been granted 8.1 Whole Time Equivalents (WTE) midwives + 0.5 WTE consultant + training money.
.• Clinical Negligence Scheme for Trusts (CNST) Year 4 criteria has been
published, which includes some changes in the criteria. A gap analysis is in progress. The Trust is also awaiting outcome of our Year 3 submission.
• High caesarean section rate remains in focus. On a par across North West London. A deep dive is in progress.
• Gap analyses have been undertaken for the recent CQC reports from other Trusts to identify key themes and ensure that we have addressed them.
August 2021Safe
THHFT Board PUBLIC 02 Nov 2021 Page 30 of 225

Safer Staffing
4
Reported concerns
k4.01 - Average fill
rate:RN
/Midwives %
k4.02 - Average fill
rate:Care Staff
%
k4.03 - Average fill
rate:RN
/Midwives %
k4.04 - Average fill rate:
Care Staff %
Ald 20 20 120.3% 95.1% 100.0% 141.9% 4.2 3.6 7.9 8.06 5.9% 6.2% 20.9% 22.5% 6.3% 8.3% 29.8% 14.6% 1 2 6/0 1 0% 0%B'East 20 20 86.6% 82.8% 101.6% 96.8% 2.9 2.5 5.5 7.59 0.0% 22.9% 29.2% -17.0% 6.9% 14.8% 30.2% 0.0% 1 3 1/0 0 100% 0%Bevan 24 24 50.7% 140.3% 54.4% 182.3% 4.5 4.2 8.6 8.37 2.6% 1.6% -28.3% -71.3% 29.8% 27.8% 16.5% 8.5% 2 3 9/2 1 50% 50%ECU 7 8 92.9% 62.2% 97.8% 45.2% 10.9 2.2 13.1 10.44 10.1% 1.6% 8.0% -100.0% 5.4% 0.0% 20.9% 5.4% 0 0 0/0 0 63% 27%Daniels 16 16 83.4% 91.9% 94.6% 97.0% 4.2 3.0 7.2 8.06 12.1% 15.1% 29.6% 25.2% 26.1% 34.8% 31.9% 5.7% 0 0 5/0 0 100% 0%Dray 18 18 106.3% 162.1% 129.0% 229.0% 5.5 3.7 9.1 7.48 12.0% 6.4% -10.3% 7.8% 4.4% 12.5% 27.2% 20.8% 1 4 2/0 5 100% 0%AMU 38 38 88.4% 99.5% 93.7% 96.8% 4.3 3.1 7.4 8.64 12.7% 3.7% 30.7% 5.5% 16.9% 13.6% 10.6% 26.5% 1 2 4/2 6 83% 6%Grange 30 30 88.1% 86.3% 98.9% 89.8% 2.7 4.2 6.9 7.59 10.8% 5.4% 23.6% 16.1% 10.8% 18.9% 26.2% 8.0% 1 7 4/1 0 50% 50%Franklin 28 28 104.5% 92.7% 114.0% 111.0% 3.4 4.7 8.2 7.49 4.6% 7.2% -6.5% 7.6% 9.1% 6.5% 19.2% 3.7% 3 3 2/0 3 80% 0%ARCU 26 26 67.9% 76.9% 79.5% 111.3% 6.3 2.2 8.5 8.37 3.4% 0.9% 57.4% 20.3% 8.0% 8.7% 21.9% 20.3% 0 1 1/1 4 82% 9%Lister 10 12 95.9% 98.1% 103.4% 109.7% 4.9 4.2 9.0 7.59 8.8% 14.3% 7.3% 1.1% 13.8% 8.7% 29.1% 6.6% 0 0 2/2 0 67% 0%Stroke 24 24 78.7% 108.4% 97.8% 111.3% 3.1 3.2 6.3 9.15 1.9% 0.6% 15.7% 7.8% 10.5% 6.7% 18.4% 0.8% 0 2 2/0 2 100% 0%Jersey 22 30 97.5% 92.9% 100.0% 128.4% 3.4 3.4 6.8 8.60 2.8% 5.0% 28.2% 9.1% 5.6% 13.3% 27.3% 11.6% 1 0 1/0 0 0% 0%Kennedy 30 30 89.7% 104.3% 98.2% 102.4% 3.1 3.9 7.0 8.59 4.0% 1.4% 17.5% 15.7% 0.0% 15.4% 24.7% 2.0% 0 1 2/1 2 87% 13%ITU/HDU 9 12 185.9% 8.1% 174.0% 12.9% 32.0 0.4 32.4 27.66 19.3% 1.1% 3.4% -147.9% 11.1% 0.0% 10.1% 54.2% 1 3 0/0 1 0% 0%Trinity 25 16 82.5% 48.3% 66.7% 100.0% 9.8 5.5 15.4 8.08 6.5% 3.7% 32.6% 19.9% 19.4% 11.1% 34.6% 4.0% 0 0 0/0 0 100% 0%Pagett 12 12 97.5% 96.8% 93.7% 100.0% 10.1 4.3 14.4 9.75 0.6% 0.6% 16.6% 3.8% 0.0% 0.0% 15.7% 1.7% 0 0 0/0 0 0% 0%Flem/Peter Pan 24 24 110.4% 51.8% 114.5% 13.5 1.3 14.7 13.95 2.0% 2.0% 10.6% -7.6% 28.6% 18.2% 7.0% 21.1% 1 0 0/0 3 76% 6%NNU 20 20 85.2% 109.3% 87.5% 96.8% 5.8 2.3 8.1 13.95 3.3% 9.5% 8.8% 11.3% 6.2% 15.4% 25.5% 0.0% 2 0 0/0 0 100% 0%Alex 22 22 85.3% 82.8% 81.7% 98.6% 3.9 2.5 6.3 13.51 7.7% 14.9% -32.0% 6.9% 21.1% 9.1% 31.8% 4.2% 5 0 0/0 2 63% 13%Kath 15 15 88.7% 91.6% 95.2% 96.8% 4.7 2.8 7.5 13.51 5.5% 23.7% 18.8% 31.6% 12.1% 15.4% 25.0% 0.0% 2 0 0/0 1 100% 0%Kath Mat Led 66.7% 43.0% 49.6 0.0 49.6 13.51 11.4% 13.1% 22.9% 13.3% 0.0% 90% 10%Labour 13 13 85.6% 99.2% 93.0% 96.3% 17.9 2.5 20.4 13.51 7.2% 3.9% 16.7% -0.5% 8.9% 37.0% 20.6% 2.5% 14 0 1/0 3 80% 20%
92.6% 92.4% 97.5% 105.5% 5.7 3.2 9.0 7.6% 6.6% 13.2% 5.5% 13.1% 15.0% 21.2% 13.4%
Data Sources:**E-rostering report, workforce report ***Incidents reported via datix**** Proportion of bank and agency nursing information provided by temporary staffing office and workforce information*****Reported occurences of specific events validated by NICE as indicating staffing may be inadequate to meet patient needs
Plan
ned
Care
Care Staff
Registered
Beds Open
k4.06 - Temporary Staffing
Proportion
Agency hours****
Environment
Unp
lann
ed C
are
Nurse Sensitive Outcome Indicators
Days Nights
Sickness Rate Vacancy Rate
Medication errors
****
Voluntary Turnover Rate
Registered
Care Staff
Registered
Overall Care Staff
National Median
Benchmark (Data May 21)
95.7%k4.05 - Overall Fill Rate
STAFFING LEVELS August 2021 Data
Total Beds
Hospital Acquired Pressure
Ulcers G2 and
above****
Falls with no harm /
Falls resulting
in harm****
FFT % of positive respons
es
Proportion Bank hours
FFT % of negative response
s
Fill Rates**
Suboptimal staffing
Directorate
Ward
Registered
midwives/ nurses
Care Staff
k4.07 - Care Hours Per Patient Day (CHPPD)
THHFT Board PUBLIC 02 Nov 2021 Page 31 of 225

Safer Staffing
5
Data:• Overall reduction in average fill rates (95.7%) from July 21 (101.4%)• Significant reduction in overall CHPPD 9.0, from 10.2 in July 21. This
is despite additional shifts above template to staff an escalation ward on Hayes and the continued requirement for enhanced care. Position is on a par with national benchmark 9.1 (data source Model Hospital –May 21).
• Slight increase in the proportion of Bank use - 21.2% (20.8% July 21) and proportion of agency use continued its upward trend to 13.4% (10% July 21)
• Sickness absence rates remained static at 6.0% across nursing and midwifery (6.1% July 21)
• Voluntary turnover in Registered Nursing and Midwifery staff is broadly unchanged at 12.8% (12.4% June 21)
Escalations:• The opening of escalation beds to meet demand, vacancy, staff
unavailability (25.3%), sickness, turnover and the increased requirement for enhanced care all contributed to significant nurse staffing challenges during Aug 21.
• Staffing challenges were not limited to THH, experienced London wide.• RMN usage remains high across clinical areas, most noticeably on
Flem/Peter. This is a national phenomenon.• High agency use continues in response to the above challenges with
substantial increase in off framework requests – 8.8% (6.3% July 21)• Background processes around cascade of shifts to framework agencies not
functioning within HealthRoster – manual process creating additional administrative burden.
• Roster lead times (>42 days) not met, affecting lead time for agency fill • Flexing inpatient capacity to accommodate increased demand causing
further staffing and quality challenges• Increased number of reported sub-optimal staffing incidents.
Exceptions:• Fill rates continued to vary from planned levels, due to adjusting staffing in
real time in line with actual need, bed occupancy in specific wards varying from template, sickness, ongoing service reconfigurations and the opening of additional beds to meet service demand.
• High CHPPD on Bevan due to change in patient profile and associated staffing template changes which are not yet reflected on E-roster system.
• High CHPPD on ICU associated with changed staffing demand in line with environment design of new ward and additional beds.
• ECU – high CHPPD. Warranted variation due to enhanced care of patients, requiring higher nurse:patient ratio.
• Service reconfigurations continued, impacting interpretability of data for e.g. for Jersey bed base above funded level; Churchill ward fluctuations due SAU. Acute Respiratory unit now included in reporting.
• Maternity CHHPD noted as significantly different to national benchmarks. Staffing challenges saw services closed (e.g. MLU) and dynamic redeployment of staff to ensure safety.
Actions:• Cohort 3 of Internationally recruited nurses landed 3rd September (9). Further 37
FTE to land before 31st December 21. • Successful bid submitted for further funding to support accelerated HCSW
recruitment• Roster KPI meetings reinstated to give scrutiny and oversight of rostering practice,
supported by NHSE/I. • Nursing Productivity Steering Group Meetings embedded to challenge and support
underpinning work streams to deliver stabilised, effective and responsive staffing.• Cross divisional working to maximise visible frontline nursing leadership • Corporate and Nurse Specialist support to clinical areas to ensure safety.• Daily staffing review, chaired by DoN to escalate and resolve issues with temporary
staffing in real time.• Temporary staffing Consultant employed to identify areas for improvement and
resolve issues within temporary staffing and HealthRoster processes.• Trust bank incentive scheme, to encourage bank staff to fill vacant shifts.• Pan London rate card introduced with reduced escalation rate.• Corporate risk register updated and risk level increased to reflect current staffing
position. THHFT Board PUBLIC 02 Nov 2021 Page 32 of 225

6
Domain Scorecard SummarySafeRolling 12 Months
to August 2021
KPI ID KPI Description Standard Sep 20 Oct 20 Nov 20 Dec 20 Jan 21 Feb 21 Mar 21 Apr 21 May 21 Jun 21 Jul 21 Aug 212021/2022
YTD
1.1.1 Discharge Summaries Not Issued n/a 396 438 637 995 1178 1612 708 66 78 127 132 187 590
1.1.2 Discharge Summaries Issued (within 24 hrs) >= 90% 80.3% 85.2% 80.9% 78.7% 82.0% 74.9% 85.8% 82.5% 85.0% 84.6% 84.6% 85.0% 84.2%
1.1.3 Discharge Summaries Issued (within 7 days) >= 100% 89.4% 89.9% 88.1% 84.6% 86.7% 82.3% 93.0% 89.6% 91.9% 92.6% 90.7% 91.1% 91.3%
1.2.1 No of Inpatient Falls n/a 48 46 45 55 41 40 31 36 46 59 44 52 237
1.2.2 Rate of Inpatient Fall (1000 Bed Days) <= 4.6 4.4 4.0 4.4 4.9 3.6 3.9 2.2 3.2 3.8 4.8 3.4 3.8 3.8
1.2.5 Falls With Fracture <= 10 0 1 2 0 2 1 1 1 1 0 0 0 2
1.3.1 No. HPAU/Moisture Lesion Incidents n/a 17 21 25 32 24 19 23 31 34 34 29 44 172
1.3.2 Rate HPAU/Moisture Lesion Incidents (1000 Bed Days Cat2) <= 1.0 1.0 1.1 0.9 1.6 1.0 1.0 1.1 1.3 2.0 1.4 1.4 2.3 1.7
1.3.3 No. Category 2 Pressure Ulcers n/a 11 13 10 17 12 11 13 14 25 17 18 31 105
1.3.4 No. Category 3 & 4 Pressure Ulcers n/a 0 0 0 0 0 1 0 1 0 1 0 1 3
1.3.5 No. Unstageable Pressure Ulcers n/a 2 1 0 5 1 0 0 1 2 4 2 2 11
1.3.6 No. Deep Tissure Injuries n/a 2 5 4 0 0 0 2 1 2 1 1 3 8
1.4.1 Patient Safety Incidents n/a 458 508 568 594 436 413 543 471 585 581 568 588 2793
1.4.2 Reporting Rate Patient Safety Incidents (KH03) >= 35 49 52 60 61 45 47 56 49 55 56 50 51 52
Discharge Summaries
Patient Falls
Hospital Aquired Pressure Ulcers / Moisture Lesions
Patient Safety Incidents
THHFT Board PUBLIC 02 Nov 2021 Page 33 of 225

7
Domain Scorecard SummarySafeRolling 12 Months
to August 2021
KPI ID KPI Description Standard Sep 20 Oct 20 Nov 20 Dec 20 Jan 21 Feb 21 Mar 21 Apr 21 May 21 Jun 21 Jul 21 Aug 212021/2022
YTD
1.5.1 Serious Incidents Declared n/a 5 5 10 6 4 9 9 16 20 9 9 6 60
1.5.2 Never Events n/a 0 0 0 0 1 0 0 0 0 0 0 0 0
1.5.3 SI Performance >= 80% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 85.7% 80.0% 37.5% 100.0% 92.9% 86.7% 73.0%
1.6.1 No. Medication Incidents n/a 50 62 75 62 43 51 44 42 43 64 69 52 270
1.6.2 Medicines Reconciliation Started Within 24 hours >= 70% 90.6% 95.0% 92.1% 93.9% 90.8% 88.6% 87.0% 91.0% 93.2% 86.4% 91.2% 79.3%
1.6.3 Omitted Dose In Last 24 Hrs <= 18% 6.8% 4.2% 4.5% 4.5% 5.4% 5.6% 4.1% 2.6% 4.5% 9.5% 9.3% 5.8%
1.7.1 MRSA (Trust Attributed) <= 0 0 0 0 0 0 1 0 0 0 0 0 0 0
1.7.2 C.diff Cases HOHA (Hospital Onset Hospital Aquired) <= 30 3 1 4 2 1 0 1 1 2 1 3 2 6
1.7.3 C.diff Cases COHA (Community Onset Hospital Aquired) n/a 1 0 1 2 1 1 0 1 1 1 1 0 4
1.7.4 E.Coli Blood Stream Infections (BSIs) <= 56 0 3 2 2 0 1 0 2 2 2 0 4 6
1.7.5 Hand Hygeine n/a 96% 97% 96% 95% 92% 98% 98% 94% 95% 97% 97% 98% 96%
1.8.1 Completed Patient Observations - Adult (NEWS) >= 95.8% 95.5% 95.3% 95.5% 95.4% 96.3% 96.1% 95.5% 95.5% 95.7% 95.4% 95.6% 95.4% 95.5%
1.11.1 Maternity (Caesarean Section Rate) < 29% 31.3% 32.0% 32.0% 34.3% 34.4% 36.1% 40.9% 40.6% 37.1% 41.7% 39.3% 36.0% 38.8%
1.11.2 Maternity (Postpartum Haemorrage >= 1500ml) < 0 1.4% 3.0% 2.8% 1.9% 1.7% 3.3% 1.3% 1.3% 2.4% 3.6% 1.4% 1.5% 2.0%
1.11.3 Maternity (1:1 Midwife in Labour) >= 100% 97.6% 95.8% 96.3% 96.7% 97.5% 97.7% 96.7% 96.7% 96.6% 95.3% 96.3% 96.3% 96.3%
1.11.4 Maternity (NICU Admissions) n/a 41 38 44 42 34 28 32 27 37 41 36 38 179
1.11.5 Maternity (3rd & 4th Degree Tears) n/a 1.7% 2.2% 3.1% 3.6% 0.7% 0.4% 1.6% 2.2% 2.7% 3.3% 0.8% 2.9% 2.4%
Infection Prevention and Control
Patient Observations
Maternity
Serious Incidents and Never Events
Medication Safety
THHFT Board PUBLIC 02 Nov 2021 Page 34 of 225
8
Domain Scorecard SummarySafeRolling 12 Months
to August 2021
KPI ID KPI Description Standard Sep 20 Oct 20 Nov 20 Dec 20 Jan 21 Feb 21 Mar 21 Apr 21 May 21 Jun 21 Jul 21 Aug 212021/2022
YTD
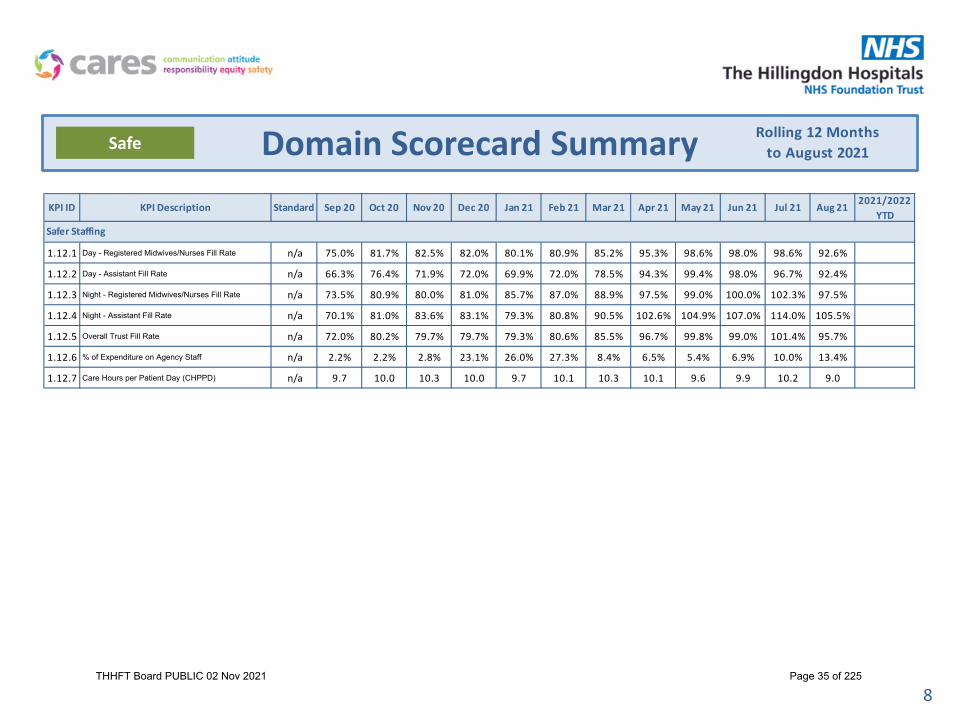
1.12.1 Day - Registered Midwives/Nurses Fill Rate n/a 75.0% 81.7% 82.5% 82.0% 80.1% 80.9% 85.2% 95.3% 98.6% 98.0% 98.6% 92.6%
1.12.2 Day - Assistant Fill Rate n/a 66.3% 76.4% 71.9% 72.0% 69.9% 72.0% 78.5% 94.3% 99.4% 98.0% 96.7% 92.4%
1.12.3 Night - Registered Midwives/Nurses Fill Rate n/a 73.5% 80.9% 80.0% 81.0% 85.7% 87.0% 88.9% 97.5% 99.0% 100.0% 102.3% 97.5%
1.12.4 Night - Assistant Fill Rate n/a 70.1% 81.0% 83.6% 83.1% 79.3% 80.8% 90.5% 102.6% 104.9% 107.0% 114.0% 105.5%
1.12.5 Overall Trust Fill Rate n/a 72.0% 80.2% 79.7% 79.7% 79.3% 80.6% 85.5% 96.7% 99.8% 99.0% 101.4% 95.7%
1.12.6 % of Expenditure on Agency Staff n/a 2.2% 2.2% 2.8% 23.1% 26.0% 27.3% 8.4% 6.5% 5.4% 6.9% 10.0% 13.4%
1.12.7 Care Hours per Patient Day (CHPPD) n/a 9.7 10.0 10.3 10.0 9.7 10.1 10.3 10.1 9.6 9.9 10.2 9.0
Safer Staffing
THHFT Board PUBLIC 02 Nov 2021 Page 35 of 225
9
Is Care Safe? August 2021Safe
10
15
20
25
30
35
40
45
50
Jul 2
0
Aug
20
Sep
20
Oct
20
Nov
20
Dec 2
0
Jan
21
Feb
21
Mar
21
Apr 2
1
May
21
Jun
21
Jul 2
1
Aug
21
Chart Title
Mean 0 Process limits - 3σSpecial cause - concern Special cause - improvement Target
1.3.1 | No. HPAU/Moisture Lesion Incidents1.3.1 | No. HPAU/Moisture Lesion Incidents
0.3
0.8
1.3
1.8
2.3
Jul 2
0
Aug
20
Sep
20
Oct
20
Nov
20
Dec 2
0
Jan
21
Feb
21
Mar
21
Apr 2
1
May
21
Jun
21
Jul 2
1
Aug
21
Chart Title
Mean 0 Process limits - 3σSpecial cause - concern Special cause - improvement Target
1.3.2 | Rate HPAU/Moisture Lesion Incidents (1000 Bed Days Cat2)1.3.2 | Rate HPAU/Moisture Lesion Incidents (1000 Bed Days Cat2)
0
5
10
15
20
25
30
35
40
Jul 2
0
Aug
20
Sep
20
Oct
20
Nov
20
Dec 2
0
Jan
21
Feb
21
Mar
21
Apr 2
1
May
21
Jun
21
Jul 2
1
Aug
21
Chart Title
Mean 0 Process limits - 3σSpecial cause - concern Special cause - improvement Target
1.3.3 | No. Category 2 Pressure Ulcers1.3.3 | No. Category 2 Pressure Ulcers
0
1
2
3
4
5
6
7
8
9
10
Jul 2
0
Aug
20
Sep
20
Oct
20
Nov
20
Dec 2
0
Jan
21
Feb
21
Mar
21
Apr 2
1
May
21
Jun
21
Jul 2
1
Aug
21
Chart Title
Mean 0 Process limits - 3σSpecial cause - concern Special cause - improvement Target
1.3.4 | No. Category 3 & 4 Pressure Ulcers1.3.4 | No. Category 3 & 4 Pressure Ulcers
THHFT Board PUBLIC 02 Nov 2021 Page 36 of 225

10
Is Care Safe? August 2021Safe
10
20
30
40
50
60
70
80
Jul 2
0
Aug
20
Sep
20
Oct
20
Nov
20
Dec 2
0
Jan
21
Feb
21
Mar
21
Apr 2
1
May
21
Jun
21
Jul 2
1
Aug
21
Chart Title
Mean 0 Process limits - 3σSpecial cause - concern Special cause - improvement Target
1.2.1 | No of Inpatient Falls1.2.1 | No of Inpatient Falls
1.5
2.5
3.5
4.5
5.5
6.5
Jul 2
0
Aug
20
Sep
20
Oct
20
Nov
20
Dec 2
0
Jan
21
Feb
21
Mar
21
Apr 2
1
May
21
Jun
21
Jul 2
1
Aug
21
Chart Title
Mean 0 Process limits - 3σSpecial cause - concern Special cause - improvement Target
1.2.2 | Rate of Inpatient Fall (1000 Bed Days)1.2.2 | Rate of Inpatient Fall (1000 Bed Days)
30
35
40
45
50
55
60
65
70
75
80
Jul 2
0
Aug
20
Sep
20
Oct
20
Nov
20
Dec 2
0
Jan
21
Feb
21
Mar
21
Apr 2
1
May
21
Jun
21
Jul 2
1
Aug
21
Chart Title
Mean 0 Process limits - 3σSpecial cause - concern Special cause - improvement Target
1.4.2 | Reporting Rate Patient Safety Incidents (KH03)1.4.2 | Reporting Rate Patient Safety Incidents (KH03)
THHFT Board PUBLIC 02 Nov 2021 Page 37 of 225
11
Is Care Safe? August 2021Safe
0
5
10
15
20
25
30
Jul 2
0
Aug
20
Sep
20
Oct
20
Nov
20
Dec 2
0
Jan
21
Feb
21
Mar
21
Apr 2
1
May
21
Jun
21
Jul 2
1
Aug
21
Chart Title
Mean 0 Process limits - 3σSpecial cause - concern Special cause - improvement Target
1.5.1 | Serious Incidents Declared1.5.1 | Serious Incidents Declared
30.0%
50.0%
70.0%
90.0%
110.0%
130.0%
Jul 2
0
Aug
20
Sep
20
Oct
20
Nov
20
Dec 2
0
Jan
21
Feb
21
Mar
21
Apr 2
1
May
21
Jun
21
Jul 2
1
Aug
21
Chart Title
Mean 0 Process limits - 3σSpecial cause - concern Special cause - improvement Target
1.5.3 | SI Performance1.5.3 | SI Performance
20
30
40
50
60
70
80
90
Jul 2
0
Aug
20
Sep
20
Oct
20
Nov
20
Dec 2
0
Jan
21
Feb
21
Mar
21
Apr 2
1
May
21
Jun
21
Jul 2
1
Aug
21
Chart Title
Mean 0 Process limits - 3σSpecial cause - concern Special cause - improvement Target
1.6.1 | No. Medication Incidents1.6.1 | No. Medication Incidents
THHFT Board PUBLIC 02 Nov 2021 Page 38 of 225

12
Is Care Safe? August 2021Safe
0
1
2
3
4
5
6
7
8
9
10
Jul 2
0
Aug
20
Sep
20
Oct
20
Nov
20
Dec 2
0
Jan
21
Feb
21
Mar
21
Apr 2
1
May
21
Jun
21
Jul 2
1
Chart Title
Mean 0 Process limits - 3σSpecial cause - concern Special cause - improvement Target
1.7.1 | MRSA (Trust Attributed)1.7.1 | MRSA (Trust Attributed)
0
5
10
15
20
25
30
35
40
Jul 2
0
Aug
20
Sep
20
Oct
20
Nov
20
Dec 2
0
Jan
21
Feb
21
Mar
21
Apr 2
1
May
21
Jun
21
Jul 2
1
Chart Title
Mean 0 Process limits - 3σSpecial cause - concern Special cause - improvement Target
1.7.2 | C.diff Cases HOHA (Hospital Onset Hospital Aquired)1.7.2 | C.diff Cases HOHA (Hospital Onset Hospital Aquired)
0
1
2
3
4
5
6
7
8
9
10
Jul 2
0
Aug
20
Sep
20
Oct
20
Nov
20
Dec 2
0
Jan
21
Feb
21
Mar
21
Apr 2
1
May
21
Jun
21
Jul 2
1
Chart Title
Mean 0 Process limits - 3σSpecial cause - concern Special cause - improvement Target
1.7.3 | C.diff Cases COHA (Community Onset Hospital Aquired)1.7.3 | C.diff Cases COHA (Community Onset Hospital Aquired)
0
10
20
30
40
50
60
Jul 2
0
Aug
20
Sep
20
Oct
20
Nov
20
Dec 2
0
Jan
21
Feb
21
Mar
21
Apr 2
1
May
21
Jun
21
Jul 2
1
Chart Title
Mean 0 Process limits - 3σSpecial cause - concern Special cause - improvement Target
1.7.4 | E.Coli Blood Stream Infections (BSIs)1.7.4 | E.Coli Blood Stream Infections (BSIs)
THHFT Board PUBLIC 02 Nov 2021 Page 39 of 225

13
Is Care Safe? August 2021Safe
20.0%
25.0%
30.0%
35.0%
40.0%
45.0%
50.0%
Sep
19
Oct
19
Nov
19
Dec 1
9
Jan
20
Feb
20
Mar
20
Apr 2
0
May
20
Jun
20
Jul 2
0
Aug
20
Sep
20
Oct
20
Nov
20
Dec 2
0
Jan
21
Feb
21
Mar
21
Apr 2
1
May
21
Jun
21
Jul 2
1
Aug
21
Chart Title
Mean 0 Process limits - 3σSpecial cause - concern Special cause - improvement Target
1.11.1 | Maternity (Caesarean Section Rate)1.11.1 | Maternity (Caesarean Section Rate)
0.0%
1.0%
2.0%
3.0%
4.0%
5.0%
6.0%
7.0%
8.0%
9.0%
10.0%
Sep
19
Oct
19
Nov
19
Dec 1
9
Jan
20
Feb
20
Mar
20
Apr 2
0
May
20
Jun
20
Jul 2
0
Aug
20
Sep
20
Oct
20
Nov
20
Dec 2
0
Jan
21
Feb
21
Mar
21
Apr 2
1
May
21
Jun
21
Jul 2
1
Aug
21
Chart Title
Mean 0 Process limits - 3σSpecial cause - concern Special cause - improvement Target
1.11.2 | Maternity (Postpartum Haemorrage >= 1500ml)1.11.2 | Maternity (Postpartum Haemorrage >= 1500ml)
90.0%
95.0%
100.0%
105.0%
110.0%
Sep
19
Oct
19
Nov
19
Dec 1
9
Jan
20
Feb
20
Mar
20
Apr 2
0
May
20
Jun
20
Jul 2
0
Aug
20
Sep
20
Oct
20
Nov
20
Dec 2
0
Jan
21
Feb
21
Mar
21
Apr 2
1
May
21
Jun
21
Jul 2
1
Aug
21
Chart Title
Mean 0 Process limits - 3σSpecial cause - concern Special cause - improvement Target
1.11.3 | Maternity (1:1 Midwife in Labour)1.11.3 | Maternity (1:1 Midwife in Labour)
20
25
30
35
40
45
50
55
60
Sep
19
Oct
19
Nov
19
Dec 1
9
Jan
20
Feb
20
Mar
20
Apr 2
0
May
20
Jun
20
Jul 2
0
Aug
20
Sep
20
Oct
20
Nov
20
Dec 2
0
Jan
21
Feb
21
Mar
21
Apr 2
1
May
21
Jun
21
Jul 2
1
Aug
21
Chart Title
Mean 0 Process limits - 3σSpecial cause - concern Special cause - improvement Target
1.11.4 | Maternity (NICU Admissions)1.11.4 | Maternity (NICU Admissions)
THHFT Board PUBLIC 02 Nov 2021 Page 40 of 225

14
Estates & FacilitiesWater SafetyAnnual water safety audits are carried out by the external Authorised Engineer looking at personnel/ risk assessments/control scheme/ remedial actions. Current compliance is 77% (Fair Compliance) at Hillingdon & 64% (Improvement needed) at MVH. Target compliance by May 2022 is expected to be Excellent at Hillingdon and Good at MVH – or possibly Excellent dependant on infrastructure/pipeline improvements. Next review in 02 months and expected score is 75-80%.
Control on Legionella and Pseudomonas Bacteria in both THH & MVH
Improvement in water system to reduce the risk of Legionella and Pseudomonas over 2021:-
• Dynamic approach for low use outlet flushing.• Legionella and pseudomonas sampling strategy in place.• Legionella and pseudomonas control by using Sodium Hypochlorite dosing system which works 24/7.• Low use taps flushed daily and bi weekly flushing in other places.• Thermostatic mixing valves cleaning and disinfection every month in different wards/department.• Monthly Sentinel temperature Monitoring and Chlorine checks.• Planned preventive maintenance remedial been carried out every month and recorded.• New Chemical Dosing unit installed in MVH Main Building.• Water Heaters installed in MVH where there is no access to return flow.
From Year 2019 – June 2020 there was a significant increase in usage of Point of Use (POU) filters in Hillingdon because of the high counts of Legionella and Pseudomonas. Because of corrective measures in 2021 we have seen an ongoing decrease in Legionella and Pseudomonas in the system and therefore a decreasing need for POU filters. Currently there are 300 POU filters in use, down from 400 in the same period in 2020.
Fire Safety
• Fire Safety is monitored through the Fire Safety Group, which meets monthly. Annual fire safety audits are carried out by the external Authorised Engineer looking at eg fire risk assessments, emergency lighting, fire doors, signage, fire and smoke dampers, and fire alarms. The finding in 2019 was Reasonable Assurance with a large number of actions required to improve compliance. The 2020/21 audit is underway currently.
• An Enforcement Notice was subsequently issued by the London Fire Brigade (LFB) in January 2020 and that also set out a number of remedial actions to be complied with by 23/12/2021. There has since been a lot of interaction with the LFB leading now to the signing of a Memorandum of Understanding to underpin the new relationship with them. A number of capital fire works were commissioned in 2020/21 and 2021/22 in the Tower building related to fire safety improvements and meeting the requirements of the LFB Enforcement Notice.
• A 35 point Fire Safety Action Plan for 2020 & 2021 was developed to pick up on the actions from the Authorised Engineer Report and the LFB Enforcement Notice. Currently 23 of the 35 actions have been fully completed and the remaining 12 are on track.
• 10 of the 35 actions on the plan specifically relate to the LFB Notice. To date - 6 of the LFB actions have been completed with the remaining 4 actions being directly related to the completion of the capital programme on fire safety improvements in the Tower.
Safety & Compliance
25 37 45 70 7737 53 53 63 64
2018 2019 2020 2021 JUN-21
Annual water safety auditTHH Compliance Score in % MVH Compliance Score in %
Cleaning Compliance
The Trust adheres to the National Specifications for Cleanliness in the NHS processes, target standards and technical audit frequencies. In the past quarter there were 218 technical cleaning audits undertaken across all clinical/non-clinical areas. The standards have been updated from April 2021.
August 2021
Fire Safety Action Plan Metrics (June 2021) Performance
Fire Risk Assessments completed 75Fire Safety Training (Level 1) – target 80% 82.5%Fire Safety Training (Level 2) – target 80% 93%
IPC Risk Category
NSC Target
HillingdonScore
MVHScore
Overall Trust Score
Very High 98% 99% 99% 99%High 95% 97% 99% 97%Significant 85% 93% 97% 93%Low 75% 94% 99% 94%
Jan Feb Mar April May June July AugLegionella 5 4 9 7 15 5 14 9Pesudomonas 10 8 4 3 1 0 0 8
01020Legionella & Pseudomonas positive results on monthly basis
THHFT Board PUBLIC 02 Nov 2021 Page 41 of 225

Health and Safety Dashboard
Data from 1st April – 31st August 2021
15
THHFT Board PUBLIC 02 Nov 2021 Page 42 of 225

SUMMARY
16
Slide Subject Comment
3 Incidents – By Division, Directorate and Top Locations (Excl. VA&S)
In August 21 there was a notable de-crease in incidents when compared to the previous 5 months (since 1st April 21). ED and Labour continue to be in the top two locations (as per previous months). Medical Devices availability followed by Contact with dirty sharps were the two most commonly reported incidents in these areas.
4 Incidents – by Category and Sub-Category (Excl. VA&S)
Top 5 Categories: “Medical Devices”, “Equipment (non-clinical)”, “Infrastructure (staff, facilities, environment)”, “Sharps and needle stick”, and “Working conditions”. No change from pervious month.Top 3 Sub-Categories: “Availability of device”, “Non Clinical-Equipment malfunction/failure” and “unsafe/unsuitable environment”. No change from pervious month.
5 (RIDDOR)- By Type and Cause 2 RIDDORs since 1st April 21. Over 7days the most common Type. No notable trend regarding causation.
6 STaM Training – H&S, M&H L1, M&H L2
Only Moving and Handling L2 is below the Trust target of 90% but slightly improved from 84% to 85% from last month. Issues include high cancellations and DNAs (particularly of bank and some managers), as well as loss of training room capacity due to Covid. Ongoing work to safely increase capacity, escalate attendance issues, and identifying staff who can potentially be stood down from L2 training.
7 Respiratory Protective Equipment (RPE)
The noticeable drop in compliance in relation to “One of Any RPE Solution” was attributed to the large intake of medics during this period. Work is underway to tighten the formal process for capturing new intakes of medics more quickly. Implementation plan for FFP3 resilience is close to full completion. Only slight slippage in closing out the final 6 actions, which are mostly administrative, but are expected to be fully completed within September 21.
8 Nominated H&S CoordinatorOut of 253 areas identified Trustwide, 83 are now covered by 46 nominated Health and Safety Coordinators. Training launched on the 24th of August, with 6 people in attendance. 8 sessions planned until 31st December (2 per month).
9 Nominated H&S Coordinator Training Feedback For information - Nominated H&S Coordinator Training being well received with generally good feedback
10 Risk AssessmentsA number of completed Covid risk assessments require updating. On-going escalations in regards to this. Note: The total number of completed risk assessments are subject to ongoing moves and changes across the Trust Further initiatives also underway towards identifying and addressing the Trust’s wider risk assessment gaps.
11 Workplace Self-Inspections Workplace Self-inspection piloted in 6 areas including Estates and Facilities. 10 clinical areas planned for September as well as full launch. Mostly positive reception and good feedback received thus, with adjustments being made as appropriate.
12 Health and Safety Related Audits COSHH audit to commence in Sep 21. Trust Gap Analysis Update Oct 21. Local area safety audits (including sharps) commences Nov 21
THHFT Board PUBLIC 02 Nov 2021 Page 43 of 225

0
20
40
60
80
100
Mar-21 Apr-21 May-21 Jun-21 Jul-21 Aug-21 Sep-21 Oct-21 Nov-21 Dec-21 Jan-22 Feb-22 Mar-22
Un-Planed Care
Planed Care
E&F
Others
Total
Incidents- By Division, Directorate and Top Locations (Excl. Violence, Aggression and Security)
In August 21 there was a de-crease in incidents when compared to the previous 5 months (since April) In August 21, ED and Labour continue to be in the top two locations (as per previous months). Medical Devices availability
followed by Contact with dirty sharps were the two most commonly reported incidents in these areas.
17
By Division / Directorate
Top 2 Locations Mar-21 Apr-21 May-21 Jun-21 Jul-21 Aug-21 Sep-21 Oct-21 Nov-21 Dec-21 Jan-22 Feb-22 Mar-221st ED Labour ED ED ED ED2nd AMU ED AMU,
Labour, Franklin, ICU/HDU, NNU
AMU, Labour
Labour Labour
THHFT Board PUBLIC 02 Nov 2021 Page 44 of 225

By Sub Category (from 1st Apr – Aug 31st)
Incidents –by Category and Sub-Category(Excl. Violence, Aggression and Security)
Top 5 Categories: “Medical Devices”, “Equipment (non-clinical)”, “Infrastructure (staff, facilities, environment)”, “Sharps and needle stick”, and “Working conditions”. No change from pervious month.
Top 3 Sub-Categories: “Availability of device”, “Non Clinical-Equipment malfunction/failure” and “unsafe/unsuitable environment”. No change from pervious month.
18
By Category (from 1st Apr – Aug 31st)
THHFT Board PUBLIC 02 Nov 2021 Page 45 of 225

Reporting of Injuries Diseases Dangerous Occurrences(RIDDOR)- By Type and Cause
2 incidents reported to the HSE under RIDDOR since 1st April 21, both of which were Over 7 day. Over 7 day is currently the most common Type of RIDDORs reported (2). Currently no trend regarding the Causes of RIDDORs.
19
from 1st Apr – Jul 31 from 1st Apr – Jul 31
THHFT Board PUBLIC 02 Nov 2021 Page 46 of 225

Health and Safety Moving and Handling L1 Moving and Handling L2
STaM Training (up to 14th Aug 21)
Health & Safety and Moving and Handling L1 continue to meet Trust Target of 90%. Moving and Handling L2 remains belowthe below the Trust target of 90% but slightly improved from 84% to 85% from last month. Issues include high cancellationsand DNAs (particularly of bank and some managers), as well as loss of training room capacity due to Covid. Ongoing work tosafely increase capacity, escalate attendance issues, and identifying staff who can potentially be stood down from L2 training.
20
THHFT Board PUBLIC 02 Nov 2021 Page 47 of 225

Respiratory Protective Equipment (RPE) 13 Month Compliance Summary
21
RPE summary for high risk areas Target Aug-20 Sep-20 Oct-20 Nov-20 Dec-20 Jan-21 Feb-21 Mar-21 Apr-21 May-21 Jun-21 Jul-21 Aug-21
One of Any RPE Solution 90% 97% 95% 96% 91% 92% 91% DNA 87% 86% 88% 88% 87% 81%
Hood Filter Changes 95% DNA DNA DNA DNA 100% 99% 85% 98% 97% 100% 98% 100% 100%
Hood Inspections 95% DNA DNA DNA DNA 19% 79% 44% 79% 90% 86% 91% 97% 98%
Resps Filter Changes + Inspections 90% DNA DNA DNA DNA 29% 48% 40% 68% 69% 69% 80% 90% 89%
The Trust has set ambitious internal targets to help drive improvements.
DNA (Data Not Available) indicates areas where the data was not explicitly monitored at the time or a different methodology was applied and therefore does not offer a suitable comparison toother months.
Ongoing Compliance Actions: Clear and ambitious targets, dedicated fit testing hub in place, provision of various RPE options to staff, mask posters and mask ID cards in place so staff can easilyidentify their personal RPE options, development of the Mask Tracker application for tracking all RPE compliance and reporting, robust procedures for fit testing and RPE maintenance, regularliaison with and compliance reporting to departments, and clear escalation routes to the executive team.
Further Comments 1: The noticeable drop in compliance in relation to “One of Any RPE Solution” was attributed to the large intake of medics during this period. Work is underway to tightenthe formal process for capturing new intakes of medics more quickly.
Further Comments 2: The FFP3 Resilience Principles in the Acute Setting (as per DHSC on 17th June 21) is close to full completion. Only slight slippage in closing out the final 6 actions, which aremostly administrative, but are expected to be fully completed within September 21.
THHFT Board PUBLIC 02 Nov 2021 Page 48 of 225

Nominated H&S Coordinator
22
Out of 253 areas identified Trustwide, 83 are now covered by 46 nominated Health and Safety Coordinators. Training launched on the 24th of August, with 6 people in attendance. 8 sessions planned until 31st December (2 per month)
4835
121132
0
20
40
60
80
100
120
140
Clinical Non-Clinical
Nominated H&S Coordinator
Depts covered by a H&S Coordinator No. of Depts
THHFT Board PUBLIC 02 Nov 2021 Page 49 of 225
Nominated H&S Coordinator Training Feedback
“…it's the correct direction for the Trust, given time and support ...”
23THHFT Board PUBLIC 02 Nov 2021 Page 50 of 225

Risk Assessments
24
A number of completed Covid risk assessments require updating as indicated by the chart on the left. On-going escalations in regards to this. Note: The total number of completed risk assessments are subject to ongoing moves and changes across the Trust.
Further initiatives underway towards identifying and addressing the Trust’s wider risk assessment gaps.
Other Risk Assessment Initiatives include
Risk assessment workshop covered in Nominated H&S coordinators training
Departments will need to maintain a risk assessment inventory, to help them monitor what risk assessment they should hold.
Further risk assessment templates being developed by the H&S to support completion
Departments assigned a member of the H&S Team to support with set-up where required.
Risk assessments will be covered as part of Local area H&S Auditing to commence in Q3 21
5845
121132
0
20
40
60
80
100
120
140
Clinical Non-Clinical
COVID-19 Risk Assessment Review
Covid RA Reviewed No. of Completed RA
THHFT Board PUBLIC 02 Nov 2021 Page 51 of 225

Workplace Self-Inspections
25
Pilot Activities
Workplace Self-inspection piloted in 6 areas including Estates and Facilities. 10 clinical areas planned for September as well as full launch.
Mostly positive reception and good feedback received thus, with adjustments being made as appropriate.
Planned for SeptemberUnplanned Care
Drayton WardBeaconsfield EastCardiologyAMUA&E
Planned Care
Elizabeth WardFleming WardTinkerbellRainbowKennedy
Completed
Security Catering Porters lodged and post roomParking and administration office Jersey Mortuary
THHFT Board PUBLIC 02 Nov 2021 Page 52 of 225

Health and Safety Related Audits
26
Planned Audits
COSHH audit to commence in Sep 21 Trust Gap Analysis Update Oct 21 Local area safety audits (including sharps) commences Nov 21
September 21 October 21 November 21 December 21
COSHH audits-prioritising clinical areas
Trust Gap Analysis Update
Local area safety audits (including sharps)
Local area safety audits (including sharps)
THHFT Board PUBLIC 02 Nov 2021 Page 53 of 225

27
Is Care Effective?
Mortality
• There is now a clear process to disseminate learning from the Structured Judgement Review process and to identify actions. The capturing of Structured Judgement Review actions on the GiveMeDatasystem will facilitate thematic reporting in the future. This new process has been agreed and will go live in September 2021.
• Dr Foster data has identified people who died with multiple sclerosis as an outlier. Although the numbers are small these cases are being reviewed to capture any concerns and learning about their care. A previous alert was raised for deaths with pathological fractures and a report following case review is due in September
• The in-hospital mortality statistics of HMSR and SHMI lie within the expected range from March 2020 to February 2021 and in line with NHS national mortality performance. Weekend and Weekday HSMR performance, as well as Emergency Weekend performance remain within the expected range. SMR was higher than expected for all months between December 2020 and February 2021 due to the impact of the Covid-19 pandemic.
• There will be a retrospective review of hospital acquired Covid-19 deaths for all cases involving probable and definite Covid-19 mortality from April 2020 to March 2021. This will be a significant piece of work as the numbers are thought to be potentially over 100. The Infection Protection Control (IPC) team have done ward-based RCAs, to consider the root causes and contributory factors on each ward (the meetings are still to be completed). The learning has been shared to prepare for wave 3 but this work will now need to be expanded to consider each case individually. A clear plan as to how this work will be undertaken will be developed at the Mortality Surveillance Group in September in conjunction with The IPC and Governance teams.
Improvement to prevention and management of VTE for our patients
• Recent trust audit of VTE conducted over the first half of 2021 from January to June 2021, showed that VTE risk assessments in adult inpatients were only completed within 24hours in 81% of patients (national target is >95%).
• Other findings from the audit highlighted that 61% of patients in medical wards and 81% in surgical wards were prescribed the correct dose of LMWH, based on blood tests and weight.
• Although targets are not being met adequately, when this audit data was compared to the same audit undertaken in 2019 there has been an improvement in rates of VTE risk assessment completion from 68% in 2019 to 81% in 2021.
• The audit has highlighted that emphasis around completion needs to be reiterated regularly to remind juniors of the importance. Education on correct dosing once assessment is complete is essential.
• Training module via iDevelop linking to E-learning for health is live and has been part of the recent induction for August 2021 intake of doctors.
• A quality round is planned for the end of the month to highlight these issues to nursing staff so that extra steps can be made to flag up incomplete risk assessments.
August 2021Effective
THHFT Board PUBLIC 02 Nov 2021 Page 54 of 225

28
Domain Scorecard SummaryEffectiveRolling 12 Months
to August 2021
KPI ID KPI Description Standard Sep 20 Oct 20 Nov 20 Dec 20 Jan 21 Feb 21 Mar 21 Apr 21 May 21 Jun 21 Jul 21 Aug 212021/2022
YTD
2.1.1 Crude Mortality Rate < 2.1% 1.0% 1.1% 1.3% 2.0% 4.4% 2.4% 0.9% 1.1% 1.3% 1.1% 1.0% 1.1% 1.1%
2.1.2 Number of Deaths n/a 41 50 61 92 163 88 45 49 57 51 48 54 259
2.1.3 SHMI n/a 98.5% 96.7% 96.3% 100.8% 102.3% 104.1% 102.0%
SHMI Banding As Expected As Expected As Expected As Expected As Expected As Expected As Expected
2.2.1 Sepsis (Eligible Patients Screened) >= 90% 94.5% 96.8% 96.1% 94.7% 94.6% 95.7% 94.1% 92.7% 95.6% 94.9% 93.9% 92.8% 94.1%
2.2.2 Sepsis (Antibiotics within 1 hour) >= 90% 95.4% 90.1% 94.8% 96.4% 94.4% 76.5% 76.9% 84.0% 92.9% 93.6% 84.6% 97.0% 91.0%
2.3.1 VTE Compliance >= 95% 92.0% 91.2% 90.3% 85.3% 82.1% 86.8% 88.9% 88.8% 91.6% 91.0% 90.2% 88.1% 89.9%
2.4.1 Dementia (Screening) >= 90% 90.2% 85.0% 83.2% 83.7% 90.9% 90.2% 96.9% 97.2% 98.1% 99.0% 93.9% 81.1% 94.4%
2.4.2 Dementia (Assessment) >= 90% 94.1% 100.0% 87.0% 100.0% 92.6% 95.2% 94.7% 95.0% 86.7% 75.0% 87.5% 94.4% 88.9%
2.4.3 Dementia (Referral for Specialist Diagnosis) >= 100% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0%
2.5.1 Readmission Rate < 9% 7.9% 8.6% 7.2% 8.2% 6.7% 7.5% 9.0% 8.0% 7.3% 7.5% 7.0% 7.2% 7.4%
2.5.2 A&E Reattendance Rate < 0 8.6% 7.8% 8.6% 8.5% 9.5% 9.4% 10.0% 8.2% 8.8% 9.4% 9.2% 9.9% 9.2%
Mortality
Sepsis
VTE
Dementia Screening
Readmissions
THHFT Board PUBLIC 02 Nov 2021 Page 55 of 225

29
Is Care Effective? August 2021Effective
0.0%
1.0%
2.0%
3.0%
4.0%
5.0%
6.0%
7.0%
8.0%
9.0%
10.0%
Sep
19
Oct
19
Nov
19
Dec 1
9
Jan
20
Feb
20
Mar
20
Apr 2
0
May
20
Jun
20
Jul 2
0
Aug
20
Sep
20
Oct
20
Nov
20
Dec 2
0
Jan
21
Feb
21
Mar
21
Apr 2
1
May
21
Jun
21
Jul 2
1
Aug
21
Chart Title
Mean 0 Process limits - 3σSpecial cause - concern Special cause - improvement Target
2.1.1 | Crude Mortality Rate2.1.1 | Crude Mortality Rate
0
20
40
60
80
100
120
140
160
180
Sep
19
Oct
19
Nov
19
Dec 1
9
Jan
20
Feb
20
Mar
20
Apr 2
0
May
20
Jun
20
Jul 2
0
Aug
20
Sep
20
Oct
20
Nov
20
Dec 2
0
Jan
21
Feb
21
Mar
21
Apr 2
1
May
21
Jun
21
Jul 2
1
Aug
21
Chart Title
Mean 0 Process limits - 3σSpecial cause - concern Special cause - improvement Target
2.1.2 | Number of Deaths2.1.2 | Number of Deaths
80.0%
85.0%
90.0%
95.0%
100.0%
105.0%
110.0%
Sep
19
Oct
19
Nov
19
Dec 1
9
Jan
20
Feb
20
Mar
20
Apr 2
0
May
20
Jun
20
Jul 2
0
Aug
20
Sep
20
Oct
20
Nov
20
Dec 2
0
Jan
21
Feb
21
Mar
21
Apr 2
1
May
21
Jun
21
Jul 2
1
Aug
21Chart Title
Mean 0 Process limits - 3σSpecial cause - concern Special cause - improvement Target
2.2.1 | Sepsis (Eligible Patients Screened)2.2.1 | Sepsis (Eligible Patients Screened)
60.0%
70.0%
80.0%
90.0%
100.0%
110.0%
120.0%
Sep
19
Oct
19
Nov
19
Dec 1
9
Jan
20
Feb
20
Mar
20
Apr 2
0
May
20
Jun
20
Jul 2
0
Aug
20
Sep
20
Oct
20
Nov
20
Dec 2
0
Jan
21
Feb
21
Mar
21
Apr 2
1
May
21
Jun
21
Jul 2
1
Aug
21
Chart Title
Mean 0 Process limits - 3σSpecial cause - concern Special cause - improvement Target
2.2.2 | Sepsis (Antibiotics within 1 hour)2.2.2 | Sepsis (Antibiotics within 1 hour)
THHFT Board PUBLIC 02 Nov 2021 Page 56 of 225
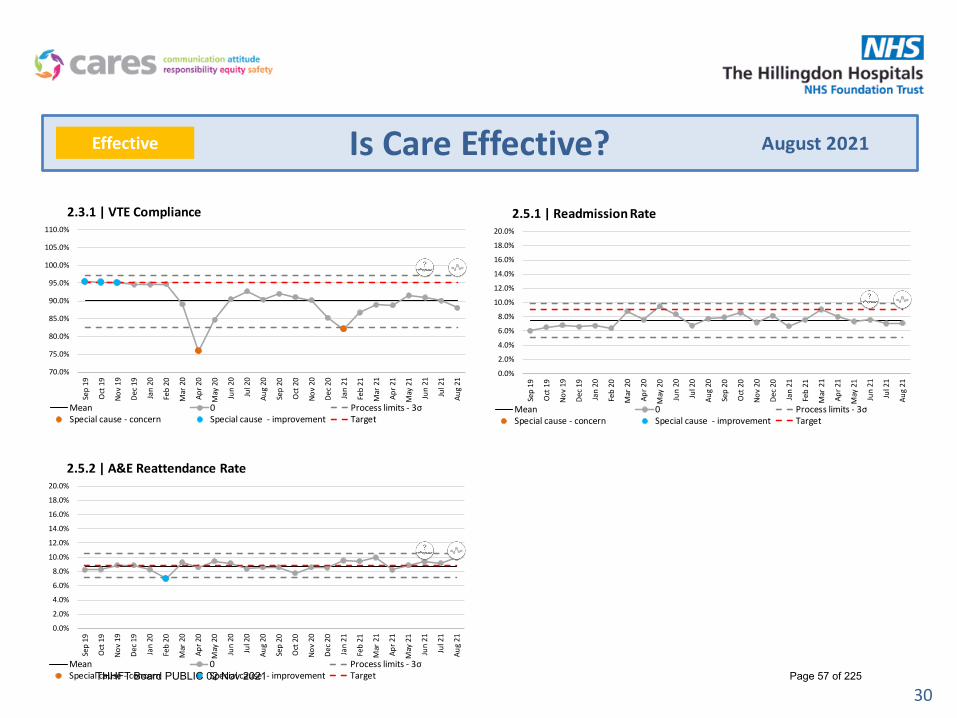
30
Is Care Effective? August 2021Effective
70.0%
75.0%
80.0%
85.0%
90.0%
95.0%
100.0%
105.0%
110.0%
Sep
19
Oct
19
Nov
19
Dec 1
9
Jan
20
Feb
20
Mar
20
Apr 2
0
May
20
Jun
20
Jul 2
0
Aug
20
Sep
20
Oct
20
Nov
20
Dec 2
0
Jan
21
Feb
21
Mar
21
Apr 2
1
May
21
Jun
21
Jul 2
1
Aug
21
Chart Title
Mean 0 Process limits - 3σSpecial cause - concern Special cause - improvement Target
2.3.1 | VTE Compliance2.3.1 | VTE Compliance
0.0%
2.0%
4.0%
6.0%
8.0%
10.0%
12.0%
14.0%
16.0%
18.0%
20.0%
Sep
19
Oct
19
Nov
19
Dec 1
9
Jan
20
Feb
20
Mar
20
Apr 2
0
May
20
Jun
20
Jul 2
0
Aug
20
Sep
20
Oct
20
Nov
20
Dec 2
0
Jan
21
Feb
21
Mar
21
Apr 2
1
May
21
Jun
21
Jul 2
1
Aug
21
Chart Title
Mean 0 Process limits - 3σSpecial cause - concern Special cause - improvement Target
2.5.1 | Readmission Rate2.5.1 | Readmission Rate
0.0%
2.0%
4.0%
6.0%
8.0%
10.0%
12.0%
14.0%
16.0%
18.0%
20.0%
Sep
19
Oct
19
Nov
19
Dec 1
9
Jan
20
Feb
20
Mar
20
Apr 2
0
May
20
Jun
20
Jul 2
0
Aug
20
Sep
20
Oct
20
Nov
20
Dec 2
0
Jan
21
Feb
21
Mar
21
Apr 2
1
May
21
Jun
21
Jul 2
1
Aug
21
Chart Title
Mean 0 Process limits - 3σSpecial cause - concern Special cause - improvement Target
2.5.2 | A&E Reattendance Rate2.5.2 | A&E Reattendance Rate
THHFT Board PUBLIC 02 Nov 2021 Page 57 of 225

31
Patient Experience
Complaints
Top five themes
Learning from complaints closed in August 2021
• Patient was admitted to Hillingdon Hospital Day Care Surgical Unit. He gave his details and got undressed ready for the procedure. Patient was then told by ward sister that there had been a mix up and that the surgeon was at Mount Vernon Hospital. Patient had to get dressed and travel to Mount Vernon Hospital. The investigation highlighted that the admissions team had entered the wrong location of the patient’s surgery. Booking staff have since had refreshed training on making the correct selection on the patient administration system.
• Patient attended clinic on the basis that a British Sign Language interpreter had been booked. A booking had been made by the clinic team but had not replied to a subsequent enquiry from the supplier of interpreting and translation services and so the booking was not confirmed. Staff have been reminded to ensure the correct process is followed through to completion so that interpreters are present when required to support patients.
OmbudsmanOne contact was received from the Ombudsman in August 2021 requesting medical notes and SI report.
Patient Engagement
Patient Engagement Forum
Third meeting of the Patient Engagement Forum (PEF) scheduled for Friday 29th October 2021. The agenda is not yet finalised but will include an update on the Hospital redevelopment project.
August 2021Caring
Clinical Care Medical Staff 21
Communication/ Information to Patients 21
Attitude (Nursing Staff) 8
Appointments (OPD & A&E) 6
Clinical Care Nursing Staff 7
THHFT Board PUBLIC 02 Nov 2021 Page 58 of 225
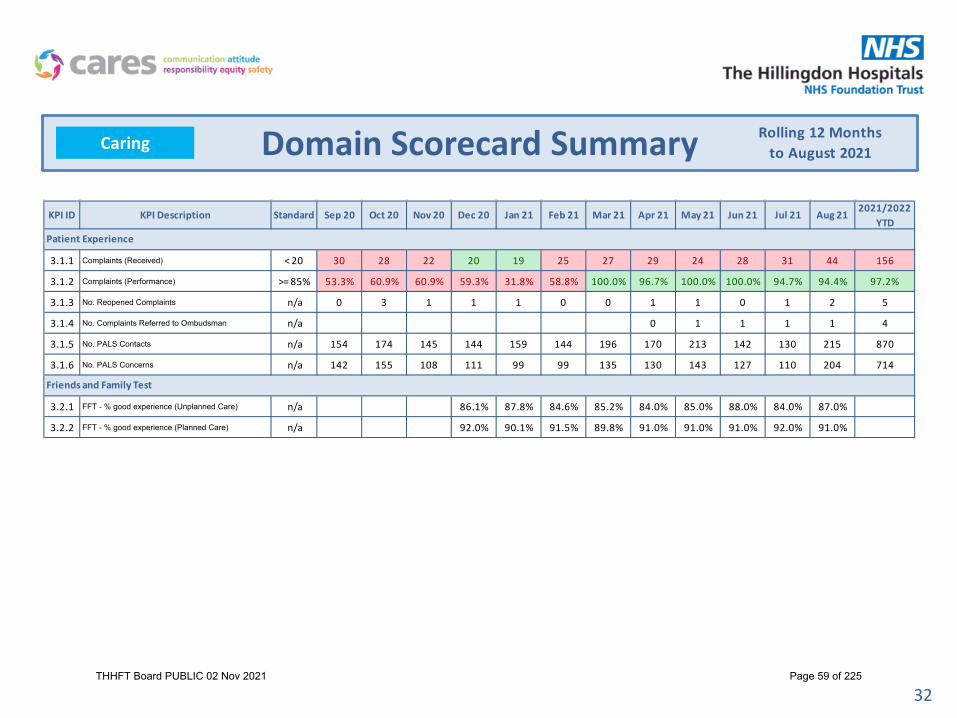
32
Domain Scorecard SummaryCaring Rolling 12 Monthsto August 2021
KPI ID KPI Description Standard Sep 20 Oct 20 Nov 20 Dec 20 Jan 21 Feb 21 Mar 21 Apr 21 May 21 Jun 21 Jul 21 Aug 212021/2022
YTD
3.1.1 Complaints (Received) < 20 30 28 22 20 19 25 27 29 24 28 31 44 156
3.1.2 Complaints (Performance) >= 85% 53.3% 60.9% 60.9% 59.3% 31.8% 58.8% 100.0% 96.7% 100.0% 100.0% 94.7% 94.4% 97.2%
3.1.3 No. Reopened Complaints n/a 0 3 1 1 1 0 0 1 1 0 1 2 5
3.1.4 No. Complaints Referred to Ombudsman n/a 0 1 1 1 1 4
3.1.5 No. PALS Contacts n/a 154 174 145 144 159 144 196 170 213 142 130 215 870
3.1.6 No. PALS Concerns n/a 142 155 108 111 99 99 135 130 143 127 110 204 714
3.2.1 FFT - % good experience (Unplanned Care) n/a 86.1% 87.8% 84.6% 85.2% 84.0% 85.0% 88.0% 84.0% 87.0%
3.2.2 FFT - % good experience (Planned Care) n/a 92.0% 90.1% 91.5% 89.8% 91.0% 91.0% 91.0% 92.0% 91.0%
Patient Experience
Friends and Family Test
THHFT Board PUBLIC 02 Nov 2021 Page 59 of 225

33
Patient Experience August 2021Caring
0
10
20
30
40
50
60
Sep
19
Oct
19
Nov
19
Dec 1
9
Jan
20
Feb
20
Mar
20
Apr 2
0
May
20
Jun
20
Jul 2
0
Aug
20
Sep
20
Oct
20
Nov
20
Dec 2
0
Jan
21
Feb
21
Mar
21
Apr 2
1
May
21
Jun
21
Jul 2
1
Aug
21
Chart Title
Mean 0 Process limits - 3σSpecial cause - concern Special cause - improvement Target
3.1.1 | Complaints (Received)3.1.1 | Complaints (Received)
10.0%
30.0%
50.0%
70.0%
90.0%
110.0%
130.0%
Sep
19
Oct
19
Nov
19
Dec 1
9
Jan
20
Feb
20
Mar
20
Apr 2
0
May
20
Jun
20
Jul 2
0
Aug
20
Sep
20
Oct
20
Nov
20
Dec 2
0
Jan
21
Feb
21
Mar
21
Apr 2
1
May
21
Jun
21
Jul 2
1
Aug
21
Chart Title
Mean 0 Process limits - 3σSpecial cause - concern Special cause - improvement Target
3.1.2 | Complaints (Performance)3.1.2 | Complaints (Performance)
THHFT Board PUBLIC 02 Nov 2021 Page 60 of 225

34
Is Care Responsive?
Overview of Planned Care
Key actions this month
RTT• All patients waiting 104 weeks plus to be dated• Patient by patient review of all patients over 78 weeks and next
step to be actioned• Additional WLIs in Dermatology & Paediatric T&O to commence• Patient by patient review of all patients over 78 weeks and next
step to be actioned• Additional WLIs in Pain to commence (6 day operating)• Specialty specific actions in order to reduce the numbers of
patient waiting over 52 weeks in ‘smaller services’
Cancer
• Urology additional diagnostic capacity for biopsies and scopes• Ring fence slots in Endoscopy for Colorectal/UGI STT pathway • Lung - Bundling of CT requests earlier in pathway
Diagnostic Performance
• Endoscopy patient by patient review of over 6 weeks and admin booking resource increase
• MRI Mutual aid plans with West Mid and LNW• Scoping Mobile scanner availability for MRIs
Overview of Unplanned Care
EDAugust Type 1 performance was 74.5%. This was driven by high activity across the whole emergency pathway, increased length of stay and higher levels of staff gaps in both medical and nursing workforce.
Key Actions this month:• Front end Senior Clinical Decision maker - from 16th September.
• Model Cubicle Role out – 16th September.
• Nurse in Charge/Consultant in Charge Zone created for oversight of shift - 1st September.
• Transformation programme to support culture of improvement following RIE and subsequent follow up event in October.
• Business Case for staffing associated with trajectory in final stage. September 24th.
• Third middle grade overnight – 20th September
Long Length of Stay
August has seen the biggest increase in our average length of stay – to 5.8 days and an increase in patients staying greater than 7 days – currently 185. There has been nursing home placement delays due to covid outbreaks in the community. The Hillingdon Care Partnership are working together to find solutions for this now and inevitably through the winter period.
A Rapid improvement Event for Discharge is being planned for the week of the 18th October and the Cares+ team are working with clinicians internally and in the community to scope for the event.
August 2021Responsive
THHFT Board PUBLIC 02 Nov 2021 Page 61 of 225

35
Domain Scorecard SummaryResponsiveRolling 12 Months
to August 2021
KPI ID KPI Description Standard Sep 20 Oct 20 Nov 20 Dec 20 Jan 21 Feb 21 Mar 21 Apr 21 May 21 Jun 21 Jul 21 Aug 212021/2022
YTD
4.1.1 A&E Performance (All Types) >= 95% 87.2% 84.9% 84.2% 77.6% 71.4% 80.3% 86.8% 84.0% 82.6% 78.2% 73.7% 74.5% 78.4%
4.1.2 A&E Performance (Type 1) >= 95% 75.2% 70.7% 70.5% 58.4% 49.4% 62.9% 76.4% 68.4% 66.6% 61.1% 54.4% 55.3% 60.9%
4.1.3 12 Hour Trolley Waits = 0 6 8 5 8 12 4 4 1 2 9 4 4 20
4.1.4 LAS Handover (Performance within 15 mins) = 100% 64.2% 66.3% 67.2% 57.3% 44.5% 51.9% 47.3% 47.4% 54.8% 49.3% 46.0% 49.6% 49.5%
4.1.5 LAS Handover (30 mins waits) < 83 55 72 73 159 182 160 67 104 159 231 275 217 986
4.1.6 LAS Handover (60 mins waits) < 9 1 0 8 56 18 12 0 1 7 18 67 33 126
4.1.7 Stranded Patients (>= 7 days) < 120 140 135 133 139 121 138 139 148 145 156 165 185 160
4.1.8 Super Stranded Patients (>= 21 days) < 39 50 49 48 54 31 38 50 53 56 55 56 74 59
4.1.9 Average Length of Stay (Emergency) < 5.0 4.72 5.24 4.48 5.08 5.48 4.55 4.05 5.17 5.14 5.47 5.32 5.84 5.39
4.2.1 RTT (Incomplete Performance) >= 92% 53.8% 64.4% 68.7% 67.4% 64.7% 62.8% 57.2% 61.0% 62.9% 60.2% 61.1% 62.0% 61.4%
4.2.2 RTT (52 Week Waiters) = 0 1,465 1,579 1,584 1,245 1,353 1,355 1,035 889 898 1,020 1,159 1,137 1,137
4.2.5 RTT (Total Waiting List) <= 18515 16,478 16,798 17,460 18,286 18,650 18,991 18,578 20,344 20,897 21,082 20,911 21,080 21,080
4.2.3 Diagnostics (6 Weeks Performance) >= 99% 66.4% 66.8% 73.5% 76.2% 71.2% 77.4% 80.6% 80.3% 74.7% 74.5% 69.9% 68.7% 73.4%
Emergency Care
Referral to Treatment
THHFT Board PUBLIC 02 Nov 2021 Page 62 of 225

36
Domain Scorecard SummaryResponsiveRolling 12 Months
to August 2021
KPI ID KPI Description Standard Sep 20 Oct 20 Nov 20 Dec 20 Jan 21 Feb 21 Mar 21 Apr 21 May 21 Jun 21 Jul 21 Aug 212021/2022
YTD
4.3.1 Cancer - 2 Week Wait (All) >= 93% 86.0% 94.6% 96.1% 94.1% 85.2% 94.6% 93.4% 86.9% 90.2% 69.7% 75.9% 73.0% 78.8%
4.3.2 Cancer - 2 Week Wait (Breast) >= 93% 5.0% 8.3% 16.5% 17.3% 50.7% 91.5% 65.9% 12.9% 18.2% 12.4% 14.2% 57.7% 23.7%
4.3.3 Cancer - 31 Day (1st Treatment) >= 96% 96.5% 100.0% 98.4% 96.7% 100.0% 94.9% 100.0% 98.4% 95.7% 98.5% 96.3% 94.8% 96.6%
4.3.4 Cancer - 31 Day (Subsequent Treatment - Surgery) >= 94% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0%
4.3.5 Cancer - 31 Day (Subsequent Treatment - Drug) >= 98% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 66.7% 100.0% 94.1%
4.3.6 Cancer - 62 Day (GP) >= 85% 66.7% 58.2% 72.1% 62.4% 52.4% 77.2% 72.6% 78.1% 74.7% 64.7% 71.3% 49.6% 67.1%
4.3.7 Cancer - 62 Day (Screening) >= 90% 100.0% 100.0% 100.0% 50.0% 100.0% 100.0% 100.0% 25.0% 100.0% 82.4%
4.3.8 Cancer - 62 Day (Upgrade) >= 95% 87.2% 100.0% 91.8% 90.4% 100.0% 91.3% 92.6% 83.3% 94.7% 98.3% 86.4% 71.8% 88.2%
4.4.1 Cancelled Ops (Performance) < 0.5% 0.9% 0.1% 0.1% 0.3% 0.1% 0.1% 0.1% 0.1% 0.4% 0.8% 0.2% 1.0% 0.5%
4.4.2 Cancelled Ops (28 Day Breaches) = 0 1 1 0 0 1 0 0 0 0 0 0 1 1
Cancer
Cancelled Operations
THHFT Board PUBLIC 02 Nov 2021 Page 63 of 225

London region – ED Comparison
37
89.00%
88.37%
86.59%
86.02%
85.44%
83.61%
83.12%
82.44%
81.24%
78.63%
76.43%
75.69%
74.01%
73.84%
68.88%
62.97%
0%10%20%30%40%50%60%70%80%90%
100%
Epsom and St Helier…
University College…
Lewisham
and Greenw
ich…
Homerton U
niversity…
St George's U
niversity…
London North W
est…
Croydon Health Services…
Guy's and St Thom
as'…
Barts Health NHS Trust
Whittington Health N
HS…
Royal Free London NHS…
North M
iddlesex…
The Hillingdon Hospitals…
Kingston Hospital NHS…
King's College Hospital…
Barking, Havering and…
4hr performance - all
4Hr % (all) System
88.39%
88.37%
86.02%
83.81%
79.58%
78.63%
75.98%
73.58%
72.08%
72.01%
69.87%
67.69%
65.52%
59.26%
56.94%
36.56%
0%10%20%30%40%50%60%70%80%90%
100%
Epsom and St Helier…
University College London…
Homerton U
niversity…
St George's U
niversity…
Lewisham
and Greenw
ich…
Whittington Health N
HS Trust
Guy's and St Thom
as' NHS…
Croydon Health Services NHS…
Royal Free London NHS…
London North W
est…
Barts Health NHS Trust
North M
iddlesex University…
Kingston Hospital NHS…
King's College Hospital NHS…
The Hillingdon Hospitals NHS…
Barking, Havering and…
4hr performance - type 1 only
4Hr % (Type1) System
THHFT Board PUBLIC 02 Nov 2021 Page 64 of 225

38
Is Care Responsive? August 2021Responsive
60.0%
65.0%
70.0%
75.0%
80.0%
85.0%
90.0%
95.0%
100.0%
Sep
19
Oct
19
Nov
19
Dec 1
9
Jan
20
Feb
20
Mar
20
Apr 2
0
May
20
Jun
20
Jul 2
0
Aug
20
Sep
20
Oct
20
Nov
20
Dec 2
0
Jan
21
Feb
21
Mar
21
Apr 2
1
May
21
Jun
21
Jul 2
1
Aug
21
Chart Title
Mean 0 Process limits - 3σSpecial cause - concern Special cause - improvement Target
4.1.1 | A&E Performance (All Types)4.1.1 | A&E Performance (All Types)
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
Sep
19
Oct
19
Nov
19
Dec 1
9
Jan
20
Feb
20
Mar
20
Apr 2
0
May
20
Jun
20
Jul 2
0
Aug
20
Sep
20
Oct
20
Nov
20
Dec 2
0
Jan
21
Feb
21
Mar
21
Apr 2
1
May
21
Jun
21
Jul 2
1
Aug
21
Chart Title
Mean 0 Process limits - 3σSpecial cause - concern Special cause - improvement Target
4.1.2 | A&E Performance (Type 1)4.1.2 | A&E Performance (Type 1)
20
70
120
170
220
270
320
Sep
19
Oct
19
Nov
19
Dec 1
9
Jan
20
Feb
20
Mar
20
Apr 2
0
May
20
Jun
20
Jul 2
0
Aug
20
Sep
20
Oct
20
Nov
20
Dec 2
0
Jan
21
Feb
21
Mar
21
Apr 2
1
May
21
Jun
21
Jul 2
1
Aug
21Chart Title
Mean 0 Process limits - 3σSpecial cause - concern Special cause - improvement Target
4.1.5 | LAS Handover (30 mins waits)4.1.5 | LAS Handover (30 mins waits)
0
10
20
30
40
50
60
70
80
Sep
19
Oct
19
Nov
19
Dec 1
9
Jan
20
Feb
20
Mar
20
Apr 2
0
May
20
Jun
20
Jul 2
0
Aug
20
Sep
20
Oct
20
Nov
20
Dec 2
0
Jan
21
Feb
21
Mar
21
Apr 2
1
May
21
Jun
21
Jul 2
1
Aug
21
Chart Title
Mean 0 Process limits - 3σSpecial cause - concern Special cause - improvement Target
4.1.6 | LAS Handover (60 mins waits)4.1.6 | LAS Handover (60 mins waits)
THHFT Board PUBLIC 02 Nov 2021 Page 65 of 225

39
Is Care Responsive? August 2021Responsive
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
Sep
19
Oct
19
Nov
19
Dec 1
9
Jan
20
Feb
20
Mar
20
Apr 2
0
May
20
Jun
20
Jul 2
0
Aug
20
Sep
20
Oct
20
Nov
20
Dec 2
0
Jan
21
Feb
21
Mar
21
Apr 2
1
May
21
Jun
21
Jul 2
1
Aug
21
Chart Title
Mean 0 Process limits - 3σSpecial cause - concern Special cause - improvement Target
4.2.1 | RTT (Incomplete Performance)4.2.1 | RTT (Incomplete Performance)
0
200
400
600
800
1,000
1,200
1,400
1,600
1,800
Sep
19
Oct
19
Nov
19
Dec 1
9
Jan
20
Feb
20
Mar
20
Apr 2
0
May
20
Jun
20
Jul 2
0
Aug
20
Sep
20
Oct
20
Nov
20
Dec 2
0
Jan
21
Feb
21
Mar
21
Apr 2
1
May
21
Jun
21
Jul 2
1
Aug
21
Chart Title
Mean 0 Process limits - 3σSpecial cause - concern Special cause - improvement Target
4.2.2 | RTT (52 Week Waiters)4.2.2 | RTT (52 Week Waiters)
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
110.0%
120.0%
Sep
19
Oct
19
Nov
19
Dec 1
9
Jan
20
Feb
20
Mar
20
Apr 2
0
May
20
Jun
20
Jul 2
0
Aug
20
Sep
20
Oct
20
Nov
20
Dec 2
0
Jan
21
Feb
21
Mar
21
Apr 2
1
May
21
Jun
21
Jul 2
1
Aug
21
Chart Title
Mean 0 Process limits - 3σSpecial cause - concern Special cause - improvement Target
4.2.3 | Diagnostics (6 Weeks Performance)4.2.3 | Diagnostics (6 Weeks Performance)
15,480
20,480
25,480
30,480
35,480
Sep
19
Oct
19
Nov
19
Dec 1
9
Jan
20
Feb
20
Mar
20
Apr 2
0
May
20
Jun
20
Jul 2
0
Aug
20
Sep
20
Oct
20
Nov
20
Dec 2
0
Jan
21
Feb
21
Mar
21
Apr 2
1
May
21
Jun
21
Jul 2
1
Aug
21
Chart Title
Mean 0 Process limits - 3σSpecial cause - concern Special cause - improvement Target
4.2.5 | RTT (Total Waiting List)4.2.5 | RTT (Total Waiting List)
THHFT Board PUBLIC 02 Nov 2021 Page 66 of 225

40
Is Care Responsive? August 2021Responsive
60.0%
70.0%
80.0%
90.0%
100.0%
110.0%
120.0%
Sep
19
Oct
19
Nov
19
Dec 1
9
Jan
20
Feb
20
Mar
20
Apr 2
0
May
20
Jun
20
Jul 2
0
Aug
20
Sep
20
Oct
20
Nov
20
Dec 2
0
Jan
21
Feb
21
Mar
21
Apr 2
1
May
21
Jun
21
Jul 2
1
Aug
21
Chart Title
Mean 0 Process limits - 3σSpecial cause - concern Special cause - improvement Target
4.3.1 | Cancer - 2 Week Wait (All)4.3.1 | Cancer - 2 Week Wait (All)
0.0%
20.0%
40.0%
60.0%
80.0%
100.0%
120.0%
Sep
19
Oct
19
Nov
19
Dec 1
9
Jan
20
Feb
20
Mar
20
Apr 2
0
May
20
Jun
20
Jul 2
0
Aug
20
Sep
20
Oct
20
Nov
20
Dec 2
0
Jan
21
Feb
21
Mar
21
Apr 2
1
May
21
Jun
21
Jul 2
1
Aug
21
Chart Title
Mean 0 Process limits - 3σSpecial cause - concern Special cause - improvement Target
4.3.2 | Cancer - 2 Week Wait (Breast)4.3.2 | Cancer - 2 Week Wait (Breast)
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
110.0%
120.0%
Sep
19
Oct
19
Nov
19
Dec 1
9
Jan
20
Feb
20
Mar
20
Apr 2
0
May
20
Jun
20
Jul 2
0
Aug
20
Sep
20
Oct
20
Nov
20
Dec 2
0
Jan
21
Feb
21
Mar
21
Apr 2
1
May
21
Jun
21
Jul 2
1
Aug
21
Chart Title
Mean 0 Process limits - 3σSpecial cause - concern Special cause - improvement Target
4.3.6 | Cancer - 62 Day (GP)4.3.6 | Cancer - 62 Day (GP)
80.0%
85.0%
90.0%
95.0%
100.0%
105.0%
110.0%
115.0%
120.0%
Sep
19
Oct
19
Nov
19
Dec 1
9
Jan
20
Feb
20
Mar
20
Apr 2
0
May
20
Jun
20
Jul 2
0
Aug
20
Sep
20
Oct
20
Nov
20
Dec 2
0
Jan
21
Feb
21
Mar
21
Apr 2
1
May
21
Jun
21
Jul 2
1
Aug
21Chart Title
Mean 0 Process limits - 3σSpecial cause - concern Special cause - improvement Target
4.3.3 | Cancer - 31 Day (1st Treatment)4.3.3 | Cancer - 31 Day (1st Treatment)
THHFT Board PUBLIC 02 Nov 2021 Page 67 of 225
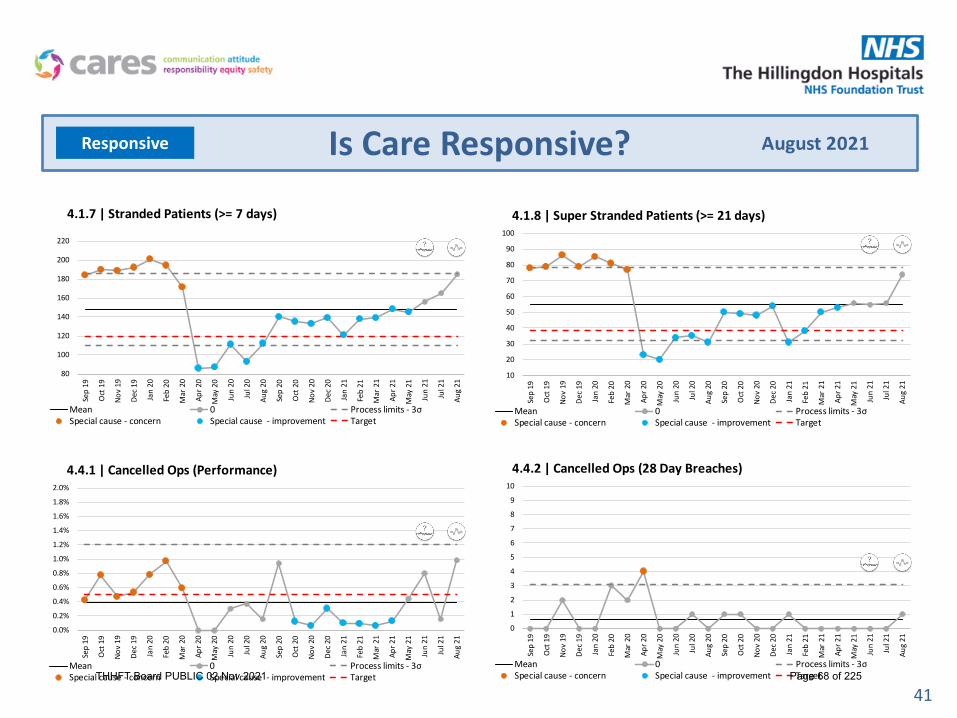
41
Is Care Responsive? August 2021Responsive
0.0%
0.2%
0.4%
0.6%
0.8%
1.0%
1.2%
1.4%
1.6%
1.8%
2.0%
Sep
19
Oct
19
Nov
19
Dec 1
9
Jan
20
Feb
20
Mar
20
Apr 2
0
May
20
Jun
20
Jul 2
0
Aug
20
Sep
20
Oct
20
Nov
20
Dec 2
0
Jan
21
Feb
21
Mar
21
Apr 2
1
May
21
Jun
21
Jul 2
1
Aug
21
Chart Title
Mean 0 Process limits - 3σSpecial cause - concern Special cause - improvement Target
4.4.1 | Cancelled Ops (Performance)4.4.1 | Cancelled Ops (Performance)
0
1
2
3
4
5
6
7
8
9
10
Sep
19
Oct
19
Nov
19
Dec 1
9
Jan
20
Feb
20
Mar
20
Apr 2
0
May
20
Jun
20
Jul 2
0
Aug
20
Sep
20
Oct
20
Nov
20
Dec 2
0
Jan
21
Feb
21
Mar
21
Apr 2
1
May
21
Jun
21
Jul 2
1
Aug
21
Chart Title
Mean 0 Process limits - 3σSpecial cause - concern Special cause - improvement Target
4.4.2 | Cancelled Ops (28 Day Breaches)4.4.2 | Cancelled Ops (28 Day Breaches)
80
100
120
140
160
180
200
220
Sep
19
Oct
19
Nov
19
Dec 1
9
Jan
20
Feb
20
Mar
20
Apr 2
0
May
20
Jun
20
Jul 2
0
Aug
20
Sep
20
Oct
20
Nov
20
Dec 2
0
Jan
21
Feb
21
Mar
21
Apr 2
1
May
21
Jun
21
Jul 2
1
Aug
21
Chart Title
Mean 0 Process limits - 3σSpecial cause - concern Special cause - improvement Target
4.1.7 | Stranded Patients (>= 7 days)4.1.7 | Stranded Patients (>= 7 days)
10
20
30
40
50
60
70
80
90
100
Sep
19
Oct
19
Nov
19
Dec 1
9
Jan
20
Feb
20
Mar
20
Apr 2
0
May
20
Jun
20
Jul 2
0
Aug
20
Sep
20
Oct
20
Nov
20
Dec 2
0
Jan
21
Feb
21
Mar
21
Apr 2
1
May
21
Jun
21
Jul 2
1
Aug
21
Chart Title
Mean 0 Process limits - 3σSpecial cause - concern Special cause - improvement Target
4.1.8 | Super Stranded Patients (>= 21 days)4.1.8 | Super Stranded Patients (>= 21 days)
THHFT Board PUBLIC 02 Nov 2021 Page 68 of 225

42
Benchmarking
Constitutional Standard
Period THHFTNorth West
LondonLondon England
91.9% 82.1% 79.1%
Ranked 5/5 Ranked 20/22 Ranked 157/194
0th percentile 10th percentile 20th percentile
74.2% 64.6% 62.4%
Ranked 8/8 Ranked 26/29 Ranked 140/171
0th percentile 10th percentile 20th percentile
88.5% 88.6% 85.6%
Ranked 6/6 Ranked 20/21 Ranked 124/142
0th percentile 0th percentile 10th percentile
80.8% 75.4% 72.1%
Ranked 5/6 Ranked 12/20 Ranked 83/143
20th percentile 40th percentile 40th percentile
81.9% 84.0% 76.5%
Ranked 5/6 Ranked 23/25 Ranked 266/340
20th percentile 10th percentile 20th percentile
RTT - 18 Week Performance
July 2021 60.9%
Last 12 Months
A&E - 4 Hour Performance
August 2021
71.8%
Diagnostics - 6 Week Performance
July 2021 69.8%
Cancer - 2 Week Wait Performance
July 2021 75.9%
Cancer - 62 Day Treatment Performance
July 2021 71.3%
60%
65%
70%
75%
80%
85%
90%
95%
100%
20%
30%
40%
50%
60%
70%
80%
90%
60%
65%
70%
75%
80%
85%
90%
95%
100%
40%
50%
60%
70%
80%
90%
100%
30%
40%
50%
60%
70%
80%
90%
100%
THHFTNorth West LondonLondonEngland
THHFT Board PUBLIC 02 Nov 2021 Page 69 of 225
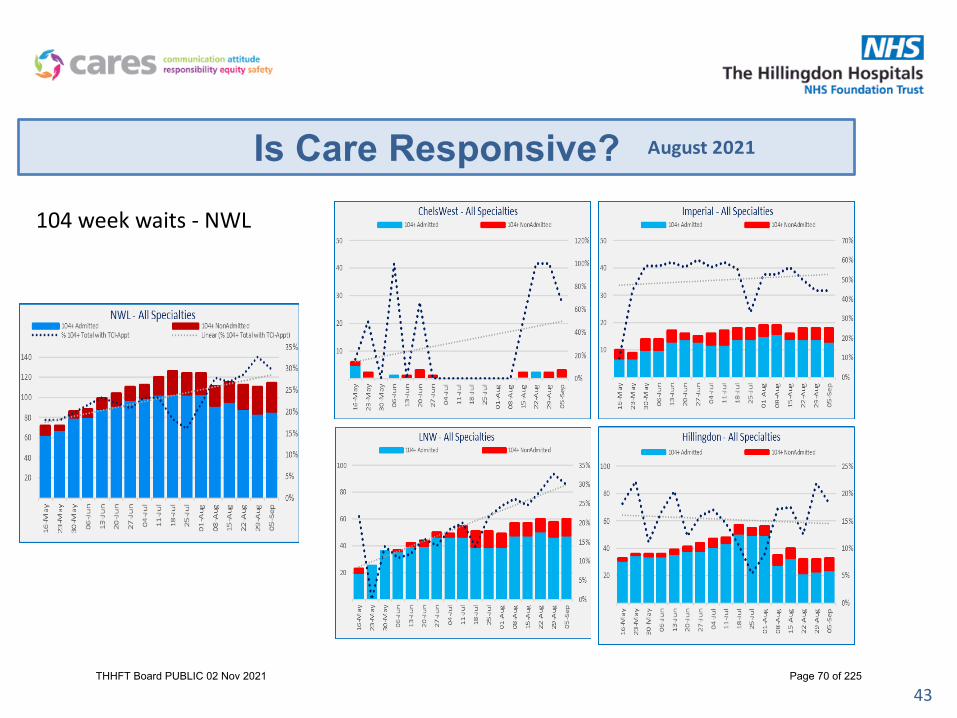
43
Is Care Responsive? August 2021
104 week waits - NWL
THHFT Board PUBLIC 02 Nov 2021 Page 70 of 225

44
Is Care Responsive? – RTT Augmented Standards positionAugust 2021
52 week Non – Admitted Actual vs Plan78 week waiters
Actual vs Plan
52 week Admitted Actual vs Plan
52 week Admitted - HVLC Actual vs Plan
THHFT Board PUBLIC 02 Nov 2021 Page 71 of 225

45
Operating Plan Compliance
50%
60%
70%
80%
90%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Elective Total
50%
60%
70%
80%
90%
100%
110%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Elective Inpatients
50%
60%
70%
80%
90%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Daycases
50%
60%
70%
80%
90%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Outpatients - Consultant Led - Total
50%
60%
70%
80%
90%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Outpatients - Consultant Led - First
50%
60%
70%
80%
90%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Outpatients - Consultant Led - Follow Up
THHFT Board PUBLIC 02 Nov 2021 Page 72 of 225

46
Operating Plan Compliance
50%
60%
70%
80%
90%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Magnetic Resonance Imaging
50%
60%
70%
80%
90%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Computed Tomography
50%
60%
70%
80%
90%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Non-obstetric ultrasound
50%
60%
70%
80%
90%
100%
110%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Endoscopy
50%
60%
70%
80%
90%
100%
110%
120%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Cardiology - Echocardiography
THHFT Board PUBLIC 02 Nov 2021 Page 73 of 225

47
Performance High Impact Actions and Trajectory
Action Expected Impact Measurable KPI Trajectory to be met by:RTT• All patients waiting 104 weeks plus to be
dated
All to have OPA, POA or TCI date:13 to be dated across the specialities 0 x 104 week waits 14th November 2021
• Patient by patient review of all patients over 78 weeks and next step to be actioned
• Additional WLIs in Dermatology & Paediatric T&O to commence
Clearance of 78 week Non-admitted patients in these specialities and robust tracking of next
events for each patient.0 x Non Admitted 78 week waits 31st October 2021
• Patient by patient review of all patients over 78 weeks and next step to be actioned
• Additional WLIs in Pain to commence (6 day operating)
All patients at 78 weeks plus to all have a next event booked Reduction in Admitted 78 week backlog to tip ins
only 30th November 2021
• Specialty specific actions in order to reduce the numbers of patient waiting over 52 weeks in ‘smaller services’
Number of patients over 52 week in smaller volume specialities will be treated or discharged as
appropriate0 x 52 weeks Non-Admitted
31st December 2021
CancerUrology additional diagnostic capacity Reduction in over 63 day wait and faster diagnosis
0 x 104 day waits< 20 over 63 day waits
30th November 2021
Ring fence slots in Endoscopy for Colorectal/UGI STT pathway Faster diagnosis FDS 75%
30th November 2021
Lung - Bundling of CT requests earlier in pathway Reduction in over 63 day wait and faster diagnosis0 x 104 day waits
< 20 over 63 day waits 30th November 2021
DM01Endoscopy patient by patient review of over 6 weeks and admin booking resource increase
Reduction in patients waiting over 6 weeks on DM01 DM01 99%
30th November 2021
THHFT Board PUBLIC 02 Nov 2021 Page 74 of 225

48
Operational Recovery High Impact actions and Trajectory
Action Expected Impact Measurable KPI Trajectory to be met by:Outpatients -Reduce DNA rate from 10% to 8%• Dedicated resource to be allocated to Envoy
system to ensure patient responses are actioned within 24 hours of receipt.
• HCAs to call patients within specialities with highest number of DNAs. Explore the use of volunteers or bank staff for this.
Reduction in DNAs and increase in activity towards activity plan.
8% DNA rate95% Outpatient Actvity - meeting the plan
30th September 2021
Outpatients -Reduce cancelled sessions from 27% to 10%• Ensure no more than 100 sessions lost per
week and monitor through OMM. • Ensure cancelled sessions are filled by
consultants using WLI and SPAs
Increase in activity towards plan 90% OPD session utilisation within clinics rooms 31st October 2021
• Fill unused sessions at Boundary House Increase in activity towards plan 100% utilisation of boundary house 14th October 2021
Theatres - Improve theatre utilisationIncrease in patients per list for Pain and Oral SurgeryPre-op telephone clinics to move to weekend to increase F2F capacity in the weekLA patients to move from pre-op to specialties
Increase in activity towards planReduction in short notice cancellations
85% utilisation by specialtyMeeting the 95% activity plan for electives 30th September 2021
Diagnostics - Increase MRI activityMutual aid being provided by West Middlesex and LNWUHChasing availability of a mobile scanner on THH site
Reduction in MRI backlogReduction in cancer diagnostic delays
Meeting 95% of operating planDM01 performance 99%FDS for cancer being met
31st October 2021
THHFT Board PUBLIC 02 Nov 2021 Page 75 of 225
Emergency Department Deep Dive Follow Up
THHFT Board PUBLIC 02 Nov 2021 Page 76 of 225

ED Performance
50
ED Actions
• Front end Senior Clinical Decision maker - from 16th September.
• Model Cubicle Role out – 16th
September.• NIC / CIC Zone created for oversight of
shift• Transformation programme to support
culture of improvement following RIE and subsequent follow up event in October.
• Business Case for staffing associated with trajectory in final stage. September 24th.
• Third middle grade overnight – 20th
September
SDEC Actions
SAU has now moved into its new space in The Wilson Unit so figures above reflect old capacity. AECU now has the whole of Churchill ward.A business case has been submitted for expansion of AECU nursing and admin staffing.Approval has been granted for the ED Lead to take on Clinical Leadership for the AECU
Non Admitted Actions
• Direct referrals to AMU and extended use of AECU – 28th August
• Enhanced MDV coverage – AMC / CT Control Room 28th August
• Go live with 1st clinician 28th October• CDU open 24/7 • Self Transfer for AECU
System support required• Continued demand management and increase hard stop at the front door.• RIE outputs from HHCP ED• UTC Streaming processes to be reviewed.
Type 1 (New Trajectory)
Aug Sept Oct Nov Dec Jan Feb March
Target 59.0% 71.0% 76.1% 83.6% 87.3% 91.0% 91.0%
Actual 55.3%
Same Day Emergency Care
Medical Surgical
750 ( 747) 170
Non Admitted
Breaches T1 Performance T1
1,562 62.4%
All Types
All Type 1
73.3% 55.3%
THHFT Board PUBLIC 02 Nov 2021 Page 77 of 225

Action Plan Summary
Action Deliverables/Intended Outcome Update since May Deep Dive Timescale Status Owner
PerformanceAchievement of the planned trajectory to meet the 90% type 1 performance.
New trajectory for ED performance written mapped to reflect staffing model and pathways
February2022 SLT
Rapid recruitment for Trust SHO gaps Appointment of 8 x SHO March 2021 Dr Khan
Business case for non-compliant SHO roster
Approved business case for compliantSHO roster Feb 2021 Dr Khan
Capacity & demand modelling to inform staffing model
Workforce model to support to activity levels which reflects improved SDEC & community provision
Capacity and demand modelling complete.Business case written and currently being reviewed.
October 2021
Jon Mitchell
Specialty doctor rotareview
Compliant roster with March 21 DHSC/NHSEI/BMA guidance May 2021 Dr Khan
Upskilling of middlegrade doctors Improved decision making Ongoing work to upskill middle grade
Doctors. Assessment days plannedOctober 2021 Dr Khan
Consultant recruitment & specialist doctor posts
Fully staffed consultant roster 2 Consultants recruited. 1 consultant non clinical (review of workforce underway)
October 2021 Dr Khan
Workforce & skill mixreview Recruitment & pipeline of PA & ANPs
Capacity and demand modelling complete.Business case written and currently being reviewed. Requirement for flexible working contracts to enable weekend cover
Jan 2022 Jon Mitchell
THHFT Board PUBLIC 02 Nov 2021 Page 78 of 225

Action Plan - continuedAction Deliverables/Intended Outcome Update since May Deep Dive Timescale Status Owner
Pathway review including SDEC & UTC
Improved flow & patient experience, removes current pathway blockages
Inclusion/ exclusion criteria for AECU & SAU written and in use June 2021 Team
CDU nurse-led discharge Improved flow & patient experience, removes current pathway blockages
Process written. To be reviewed with training
November2021
Dr Carruth
Workspace remodelbusiness case
Provision of patient toilet, sluice, socialdistancing & huddle/review area
Wider work being undertaken to reprovision workspace on the ground floor to provide capacity and flow
November2021 Division
Quality improvement informed byCARES+ methodologyAudit LeadIPC peer reviewRoyal College audits
Improved patient experience, reduced incidents & complaints
RIE undertaken with further events planned
October2021 SLT
Equipment reviewImproved utilisation of existing equipment business cases for identified requirements
September 2021 SLT
Right First Time (RFT) Improved patient experience & clinical outcomes, reduced re-admissions
Capacity and demand modelling complete.Business case written and currently being reviewed. Requirement for flexible working contracts to enable weekend cover
SLT
Training programme including;TraumaTinTATNCUSCATResus & Simulation
Supported, invested and engaged medic, nursing & AHP workforce Training ongoing October
2021 SLT
THHFT Board PUBLIC 02 Nov 2021 Page 79 of 225

53
Rapid Improvement Event 16-22 Aug
Purpose• To address high volumes of patients attending in the Urgent and
Emergency Care setting• Need to collectively focus on safety of care• Improve patient flow by implementing quick wins while
capturing future improvement opportunities and learning
Methodology & Aims• Run like major incident control room/command/daily briefings• 24/7 for 7 days• Allow clinical staff more time to focus on clinical duties• Enable support services to provide a rapid response to clinicians • Recalibrate (or reset) the system• Benefit from improved patient flow throughout the
organisation• Free up capacity earlier in the day (to prevent bottlenecks)• Learn from, and with each other to improve each day
Some Quick Wins-ED• Perfect shift introduced (Green Zone) with Consultant & Nurse in
Charge• Arm bands for Nurse and Consultant co-ordinators • MDV screens installed in Radiology • Agency ANP / ACP shifts offered to cover medics rota shortfalls • Frequent list reviews with UTC
Some Quick Wins-SDEC• Patients suitable for SDEC walk to unit unescorted • Trial of dedicated ultrasound capacity for SDEC• Visual Management installed on flooring to guide patients from ED
to SDEC – new black line on floor
154 issues logged to the Control Room• 36% issues requiring action have been resolved• 31% have actions underway to address them• 32% require development/ actions to be taken
HHCP Colleagues provided useful insights to support partnership working
THHFT Board PUBLIC 02 Nov 2021 Page 80 of 225

Current StateOutpatients• Operating plan achieved and ERF obtained.• 85% clinic utilisation• 30% of all outpatient activity to be virtual• 3% of FU waiting list on PIFU pathway• Low volume of un-outcomed activity
Theatres• Operating plan achieved and ERF obtained.• 85% utilisation• Full reconfiguration of theatre space to enable consistent treatment of THH only patients, paediatrics and provision
of additional recovery space.• Local anaesthetic pre-op pathway to be adopted as per best practice and optimisation of pre-op capacity via a digital
pre-op solution• Transformation of additional specialty pathways to convert procedures from theatres to outpatients.. • Development of a short notice patient pathway in line with IPC guidance
Future State
Risks Progress and Next Milestones
Key risks Mitigating actions Residual Score (Likelihood vs Impact)
Achievement of elective operating plan (outpatients and theatres).
Action plan in place for outpatients.Pre-op capacity work in progress for theatres.
3 x 4 = 12
27% unused sessions in Main OPD and Tudor clinic rooms.
Target to be agreed, action plan being addressed and transformation support in place.
2 x 4 = 8
Current RAG Status
Outpatients• Did not meet the operating plan for the month – action plan in place to address• Unused sessions in outpatient clinic rooms remains poor – Transformation support in place to look at OP
processes.• Over 1700 patients on PIFU pathway (1% of FU wait list – DQ issue in previous month where this was reported
higher) – highest uptake in Trauma & Orthopaedics, Ophthalmology and Gynaecology• e-COF form live and over 7000 completed in August with a decrease in missing outcomes.• e-TCI ready for trial
Theatres• Did not meet the operating plan for the month• Achieved 71.6% theatre utilisation • 7.9% of cases cancelled on the day and 15.7% of cases cancelled within 4 days. Sector looking at proposal for
short notice cancellations and how lists can be filled in line with IPC guidance.• Elective Surgical Unit (old ITU) being used for long waiting Hillingdon only patients (orthopaedics and paediatrics)• Working to increase pre-op capacity via local anaesthetic proposal, pre-op carried out prior to TCI and weekend
clinics from 28/8/21 onwards.
Elective Care Steering Group Highlight Report, August 2021
Next steps and key milestones
1 of 2
Outpatients• Transformation Team to look at outpatient processes to identify where issues are preventing optimum booking.• Adoption of specialty clinical guidelines from other Trusts to increase uptake of PIFU• e-TCI to be trialled by October.
Theatres• Exploration of digital pre-op questionnaire via CIE• Development of an information pack to inform patients what to expect re. swabbing, isolation and their TCI to reduce patient
cancellations within 4 days.• Surgical teams to approve local anaesthetic proposal.
THHFT Board PUBLIC 02 Nov 2021 Page 81 of 225
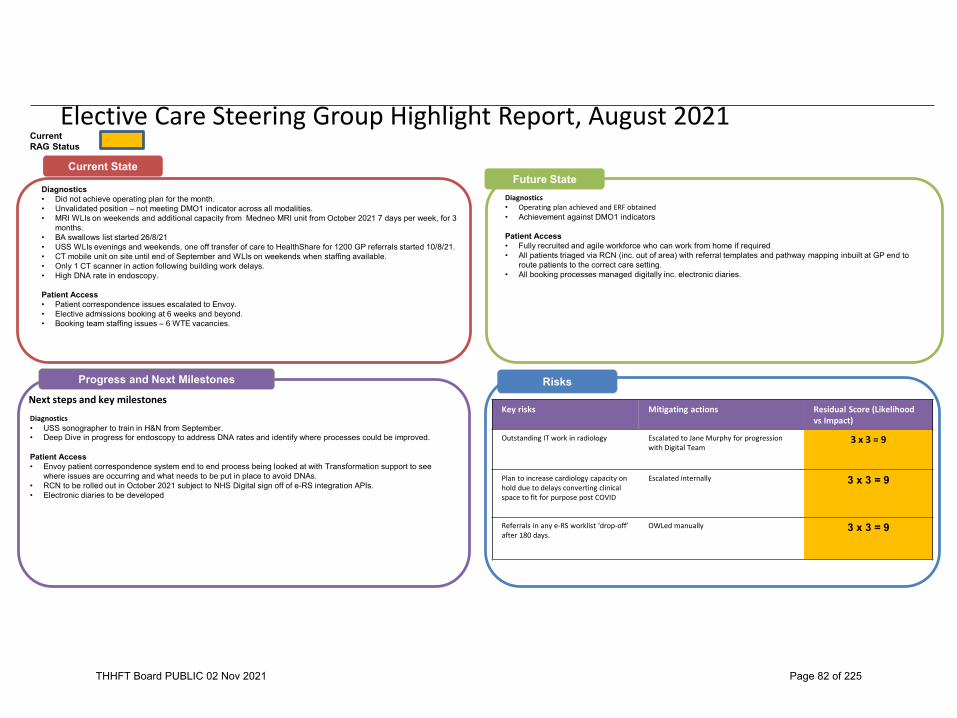
Current State
Diagnostics• Operating plan achieved and ERF obtained• Achievement against DMO1 indicators
Patient Access• Fully recruited and agile workforce who can work from home if required• All patients triaged via RCN (inc. out of area) with referral templates and pathway mapping inbuilt at GP end to
route patients to the correct care setting.• All booking processes managed digitally inc. electronic diaries.
Future State
Risks Progress and Next Milestones
Current RAG Status
Diagnostics• Did not achieve operating plan for the month.• Unvalidated position – not meeting DMO1 indicator across all modalities. • MRI WLIs on weekends and additional capacity from Medneo MRI unit from October 2021 7 days per week, for 3
months.• BA swallows list started 26/8/21• USS WLIs evenings and weekends, one off transfer of care to HealthShare for 1200 GP referrals started 10/8/21.• CT mobile unit on site until end of September and WLIs on weekends when staffing available. • Only 1 CT scanner in action following building work delays.• High DNA rate in endoscopy.
Patient Access• Patient correspondence issues escalated to Envoy.• Elective admissions booking at 6 weeks and beyond.• Booking team staffing issues – 6 WTE vacancies.
Elective Care Steering Group Highlight Report, August 2021
Next steps and key milestones
2 of 2
Diagnostics• USS sonographer to train in H&N from September.• Deep Dive in progress for endoscopy to address DNA rates and identify where processes could be improved.
Patient Access• Envoy patient correspondence system end to end process being looked at with Transformation support to see
where issues are occurring and what needs to be put in place to avoid DNAs. • RCN to be rolled out in October 2021 subject to NHS Digital sign off of e-RS integration APIs. • Electronic diaries to be developed
Key risks Mitigating actions Residual Score (Likelihood vs Impact)
Outstanding IT work in radiology Escalated to Jane Murphy for progression with Digital Team
3 x 3 = 9
Plan to increase cardiology capacity on hold due to delays converting clinical space to fit for purpose post COVID
Escalated internally 3 x 3 = 9
Referrals in any e-RS worklist ‘drop-off’ after 180 days.
OWLed manually 3 x 3 = 9
THHFT Board PUBLIC 02 Nov 2021 Page 82 of 225

Current State
Cancer• Achievement of the operating plan and national cancer standards.• No patients waiting 104+ days. • Achieving FDS from October 2021
RTT• No patients waiting over 52 weeks for non-admitted. • No patients waiting over 52 weeks for HVLC• No patients waiting over 78 weeks for both admitted and non-admitted pathways.
Future State
Risks Progress and Next Milestones
Current RAG Status
Cancer• 62 day cancer standard at 84% against a target of 85%• Unvalidated FDS standard at 59% against a target of 75%• Unvalidated 2WW at 72.6% against a target of 93%• 62 day+ backlog increased• Urology & Skin additional clinics taking place• Additional RMP funding for 2021/22 FDS.
RTT• Total incomplete RTT PTL:
• 33 patients over 104 weeks – not on track to have all treated by end of August but weekly patient by patient review over 104 weeks
• 307 over 78 weeks• 1174 over 52 weeks
• HVLC ahead of plan• Just over 100 out of 1152 clinical harm reviews completed – none have come to harm.• Independent Sector arrangements moving forward at pace and have successfully transferred over 600 patients.
Elective Care Steering Group Highlight Report, August 2021
Next steps and key milestones
2 of 2
Cancer• Additional capacity plan requested from H&N and Lung. • Theatre availability review for colonoscopy • MRIs for prostate to be confirmed for September. • Standardisation of process of informing patients of benign results in endoscopy.
RTT• Admin review of all patients in dermatology and allergy• Pain service looking to put on additional clinic capacity through increased clinic profiles.• Look at super lists for General Surgery to increase clearance rate further.• Well-being texts to be sent to all patients on FU waiting list to confirm appointment still required or whether
discharge/PIFU appropriate.
Key risks Mitigating actions Residual Score (Likelihood vs Impact)
Dermatology/Allergy currently unknown capacity gap
Demand and Capacity assessment being completed with support from NHSI/E
3 x 3 = 9
Uptake of IS by patients or rejection of patients by the private group.
Plan for additional WLI in house and consider insourcing opportunity with Chelsea & Westminster
1 x 3 = 3
Clinical harm reviews not completed. Clear definitions of harm outcomes from the sector to be shared with Clinicians.
5 x 3 = 15
THHFT Board PUBLIC 02 Nov 2021 Page 83 of 225

57
Is Care Responsive?Pathology Performance
Key performance Indicators Target % Sep-20 Oct-20 Nov-20 Dec-20 Jan-21 Feb-21 Mar-21 Aprl-21 May-21 Jun-21 July-21 Aug-21KPI1: A&E Renal, LFT & FBC within 1 hour 90% 88.8 92.7 91.6 91.7 88.2 89.6 88.1 79.1 80.3 84.3 86 85.1
KPI2: Histo biopsy reports within 7 calendar days 80% 68.4 56.1 18.3 8.9 56.5 24.5 19.9 36.1 62.1 62.6 57.7 54.1
KPI3: Histo & Cytology reports within 10 calendar days 90% 88 77.7 61.6 37.6 87.8 65.5 67.1 71.3 82.8 82.4 86.3 78.8KPI4: Antenatal screen (HIV, Hep B, Rubella& Syphilis) in 6
calendar days 90% 100 100 100 100 100 100 100 100 100 100 100 100
Responsive
THHFT Board PUBLIC 02 Nov 2021 Page 84 of 225

58
Pathology Performance• KPI 1 (A&E Renal, LFT & FBC within 1 hour) still remains below the target of 90% between July and
Aug 2021 due to IT issues and a new interface to transfer the results from the analyser middleware to the LIMS. Recurrent downtime of this interface is managed through routine downtime procedures, with results communicated manually to the requesting clinician and ensuring patient care is not impacted.
• KPI 2 (Histopathology biopsy reports within 7 calendar days) and KPI 3 (Histopathology & Cytology reports within 10 calendar days) did not meet the target since September 2020. Temporary investment in staffing supported by Royal Marsden Partners has supported some extended working days and six day working, however the increased service provision is reliant on availability of bank/agency staffing and the availability of staff to complete overtime. NWLP are now working on the service improvement action plan and associated business cases to re-present to the September Committee meeting.
• KPI 4 target of 90% of routine antenatal screening tests for Hepatitis B, HIV, Syphilis, and Rubella susceptibility reported within 6 calendar days was 100% for July and Aug 2021.
Is Care Responsive?Responsive
THHFT Board PUBLIC 02 Nov 2021 Page 85 of 225

59
Are We Well-Led? August 2021Well-Led
K7.02 - Voluntary Turnover
• Key intervention has been to promote the recently launched exit interview process. Managers are encouraged to inform P&OD regarding resignations straight away so that exit interviews can be undertaken with staff. The themes will then be analysed and actions taken forward• Within Planned Care Workforce KPI meetings have been rolled out in all the key specialities, to provide advice on staffing matters, analyse key metrics and agree interventions. Additionally staff health & wellbeing will be included in all divisional team meetings as an agenda item going forward• Within Unplanned Care retention Strategies are in development for B5 and B6 Nurses as this area over the last quarter has seen the highest turnover.
K7.03 - Sickness Absence
• The main reasons across the Trust for long-term sickness absence include anxiety/ stress/ depression, followed by Coronavirus and other MSK reasons. There is a specific focus on addressing and tackling long-term sickness absences with input from Occupational Health and support to management in managing individual cases.
• There are Bi weekly review meetings with managers to support them in managing sickness absence cases, ensuring cases appropriately progress through policy stages in a timely manner.
• Long Covid guidance is being implemented – which includes options of extended phased returns, reduced or amended duties, redeployment, ill health capability. Across the trust there are 12 members of staff absent as a result of Long Covid.
• The HRBPs are working with OD/OH on addressing issues associated with Stress and Wellbeing management. Additionally the HRBPs are working on specific interventions to ensure grip and control over Medical sickness absence logging, monitoring and processing.
THHFT Board PUBLIC 02 Nov 2021 Page 86 of 225
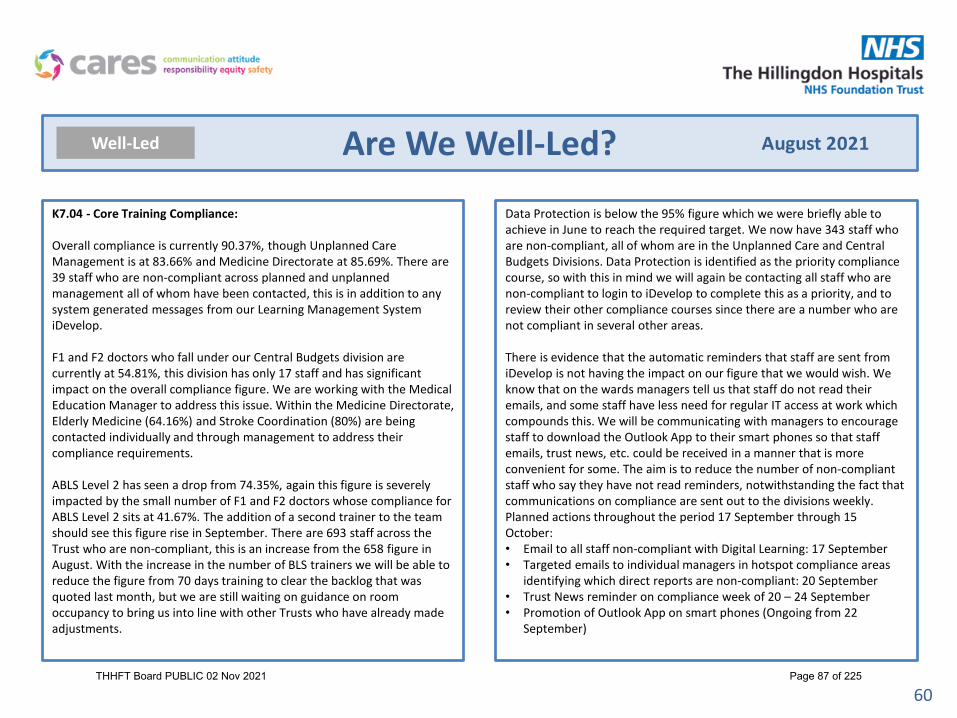
60
Are We Well-Led? August 2021Well-Led
K7.04 - Core Training Compliance:
Overall compliance is currently 90.37%, though Unplanned Care Management is at 83.66% and Medicine Directorate at 85.69%. There are 39 staff who are non-compliant across planned and unplanned management all of whom have been contacted, this is in addition to any system generated messages from our Learning Management System iDevelop.
F1 and F2 doctors who fall under our Central Budgets division are currently at 54.81%, this division has only 17 staff and has significant impact on the overall compliance figure. We are working with the Medical Education Manager to address this issue. Within the Medicine Directorate, Elderly Medicine (64.16%) and Stroke Coordination (80%) are being contacted individually and through management to address their compliance requirements.
ABLS Level 2 has seen a drop from 74.35%, again this figure is severely impacted by the small number of F1 and F2 doctors whose compliance for ABLS Level 2 sits at 41.67%. The addition of a second trainer to the team should see this figure rise in September. There are 693 staff across the Trust who are non-compliant, this is an increase from the 658 figure in August. With the increase in the number of BLS trainers we will be able to reduce the figure from 70 days training to clear the backlog that was quoted last month, but we are still waiting on guidance on room occupancy to bring us into line with other Trusts who have already made adjustments.
Data Protection is below the 95% figure which we were briefly able to achieve in June to reach the required target. We now have 343 staff who are non-compliant, all of whom are in the Unplanned Care and Central Budgets Divisions. Data Protection is identified as the priority compliance course, so with this in mind we will again be contacting all staff who are non-compliant to login to iDevelop to complete this as a priority, and to review their other compliance courses since there are a number who are not compliant in several other areas.
There is evidence that the automatic reminders that staff are sent from iDevelop is not having the impact on our figure that we would wish. We know that on the wards managers tell us that staff do not read their emails, and some staff have less need for regular IT access at work which compounds this. We will be communicating with managers to encourage staff to download the Outlook App to their smart phones so that staff emails, trust news, etc. could be received in a manner that is more convenient for some. The aim is to reduce the number of non-compliant staff who say they have not read reminders, notwithstanding the fact that communications on compliance are sent out to the divisions weekly.Planned actions throughout the period 17 September through 15 October:• Email to all staff non-compliant with Digital Learning: 17 September• Targeted emails to individual managers in hotspot compliance areas
identifying which direct reports are non-compliant: 20 September• Trust News reminder on compliance week of 20 – 24 September• Promotion of Outlook App on smart phones (Ongoing from 22
September)
THHFT Board PUBLIC 02 Nov 2021 Page 87 of 225

61
Are We Well-Led? August 2021Well-Led
K7.05 – PDRs
Compliance for 2020-21 is at 62.5%. Work is ongoing to review and cleanse data to address user queries. Paperwork for the proposed new format for PDRs to move away from the previous three-month window to align with the AfC pay progression rules is being reviewed which includes a new PDR form for staff to complete, plus guidance for managers, is currently under review. The purpose is to simplify the process and increase compliance.
A key part of the PDR process also focuses on regular 1:1s and managers having wellbeing conversations with staff as part of the NHS People Plan 2020-2021. NHSEI has started a roll out of wellbeing conversations training for staff and dates shared in Trust communications. The training has recently been extended until March 2022 and regular communications will be circulated to encourage colleagues to attend.
Work Experience
Face to face work experience is still suspended. The Trust currently has virtual Work Experience Programme through Spring Pod. The next programme will be in October 2020, during half-term, 5 Trusts in North West London are involved in this project. The Programmes that will be available in October are Allied Health Professional, Nursing & Midwifery, and Medicine.
Leadership and Development
Modules from the ChelWest Management and Fundamentals suite are now offered to Hillingdon staff and further dates are being finalised until March 2022. Anecdotal feedback has been positive for staff, though formal evaluation methods are being reviewed to ensure robust capture of the learner experience and aid regular review of the course content.A senior medical leadership development programme is underway.
Apprenticeships
There are currently 50 total apprentices in the Trust including 20 undertaking Level 7 Senior Leader Apprenticeship (MBA/MSc), 6 are currently paused in their programme.Last quarter, 24% of the Levy was utilised. The Trust aims to increase this utilisation by identifying more entry-level apprenticeship posts and introducing new Apprenticeship Programmes that will support the workforce and also develop into hard to recruit posts.
The following are the new Apprentice roles that started in the Trust this financial Year:• Apprentice Improvement Practitioner- Transformation Team• Operating Department Practitioner Apprentice- Theatres Department• Physiotherapy Degree Apprenticeship- Therapies TeamThe following Apprenticeship Programmes are currently being developed and waiting for approval:• Business Admin Apprenticeship- Recruitment Team• Data Analyst Apprentice- Information and Digital Services Team• Healthcare Support Worker Apprenticeship- Nursing, AHP and Midwifery (Target:
43 Apprentices)• Nursing Associate Apprenticeship- Nursing (Target: 14 Apprentices)
Functional Skills Course for Math and English, continues to be available in the Trust to assist current staff to get in to Higher, Degree, and Masters, Level Apprenticeship Programmes.
The Head of Apprenticeship continues to work with Department Heads to develop Career Pathways for their teams, using Apprenticeship routes. Pathways are currently being developed for the following teams: Radiology Team, Integrated Discharge Team, Information and Digital Services Team, Transformation Team, Recruitment Team, Facilities Team (Security), and a Trust-wide plan for Support Workers and Nursing.
THHFT Board PUBLIC 02 Nov 2021 Page 88 of 225

62
Are We Well-Led? August 2021Well-Led
Race Equality Plan & Inclusion
Danny Karystinos has started his new role, as EDI Lead on 16th August. The Trust’s EDI strategy implementation is focused on the Year 1 objectives and actions of the three year EDI Plan.The EDI communication strategy has been shared with the Communication & Engagement dept.
Our key actions for 2021 are:
SEPTEMBER• BAME network relaunch event on the 30th Sept.• Drop in sessions: speak to our EDI lead (first and last Friday of each
month).• In your shoes days: EDI lead to spend half day at each department and
support.
OCTOBER• BHM and FTSU series of events in October.• New posters: Networks, 78 Nationalities.• Celebrating Inclusion week by launching the 78 nationalities special
days.• LGBT+ badges scheme.• Promoting our networks via leaflets and stands, to improve
participation.
NOVEMBER• Launching of KUDOS days, when employees will praise a colleague for
an outstanding action.• New networks: Women’s network.
DECEMBER• New networks: Wellbeing support network.• Our WRES data has been submitted on the 26th August.
Health and Wellbeing
We are continuing to work with the NW London Sector Health and Wellbeing task and finish group to establish and deliver a sector health and wellbeing strategy. This includes reviewing our priorities in light of previous surges, agreeing a medium term direction, and ensuring there is a HWB plan in place in each Organisation.
We are in the process of setting up a Health and Wellbeing Steering Group to commence in September, with a remit to develop a comprehensive staff health and wellbeing programme aligned to the national staff wellbeing framework, with the three pillars of healthy mind, healthy body, and healthy living.
Recruitment is underway for an Engagement and Wellbeing Lead in the Trust to drive this agenda forward.
We now have 31 trained mental health first aiders, with another two cohorts planned for September and October. The Employee Relations team are also continuing to support our staff who remain off sick with long-Covid.
THHFT Board PUBLIC 02 Nov 2021 Page 89 of 225
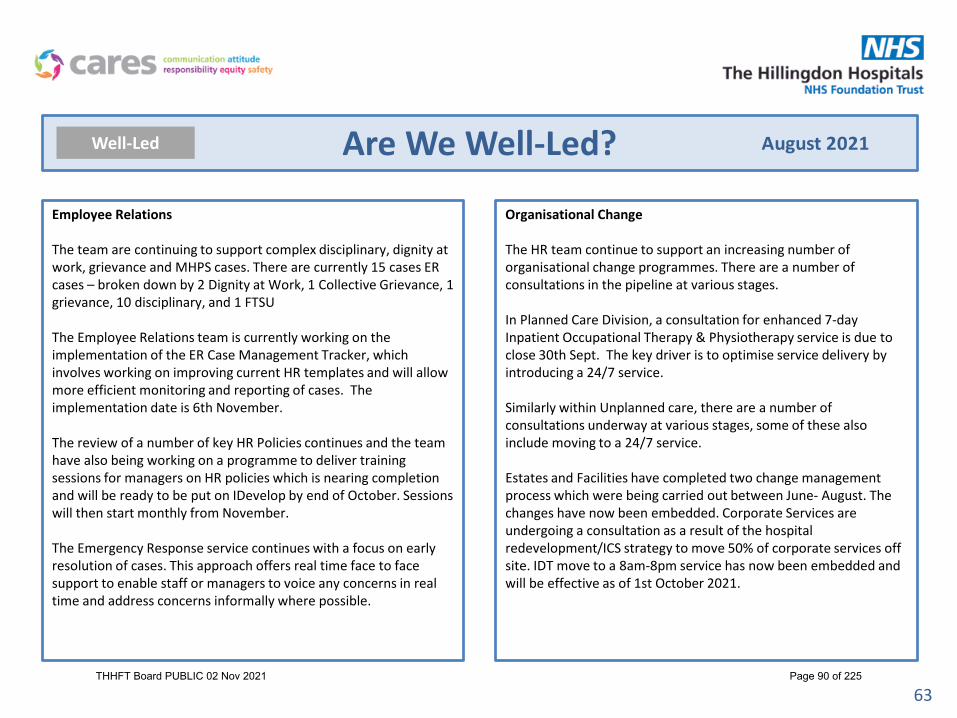
63
Are We Well-Led? August 2021Well-Led
Employee Relations
The team are continuing to support complex disciplinary, dignity at work, grievance and MHPS cases. There are currently 15 cases ER cases – broken down by 2 Dignity at Work, 1 Collective Grievance, 1 grievance, 10 disciplinary, and 1 FTSU
The Employee Relations team is currently working on the implementation of the ER Case Management Tracker, which involves working on improving current HR templates and will allow more efficient monitoring and reporting of cases. The implementation date is 6th November.
The review of a number of key HR Policies continues and the team have also being working on a programme to deliver training sessions for managers on HR policies which is nearing completion and will be ready to be put on IDevelop by end of October. Sessions will then start monthly from November.
The Emergency Response service continues with a focus on early resolution of cases. This approach offers real time face to face support to enable staff or managers to voice any concerns in real time and address concerns informally where possible.
Organisational Change
The HR team continue to support an increasing number of organisational change programmes. There are a number of consultations in the pipeline at various stages.
In Planned Care Division, a consultation for enhanced 7-day Inpatient Occupational Therapy & Physiotherapy service is due to close 30th Sept. The key driver is to optimise service delivery by introducing a 24/7 service.
Similarly within Unplanned care, there are a number of consultations underway at various stages, some of these also include moving to a 24/7 service.
Estates and Facilities have completed two change management process which were being carried out between June- August. The changes have now been embedded. Corporate Services are undergoing a consultation as a result of the hospital redevelopment/ICS strategy to move 50% of corporate services off site. IDT move to a 8am-8pm service has now been embedded and will be effective as of 1st October 2021.
THHFT Board PUBLIC 02 Nov 2021 Page 90 of 225

64
Are We Well-Led? August 2021Well-Led
Temporary Staffing
Demand for Temporary Staff had increased in August 2021 by 7.53 % (Total Demand: 11153 Shifts) in comparison to July 2021 (Total Demand: 10389).
The increased shift demand had meant a decreased utilization of Bank % Fill at 59 %, Increased Agency % Fill at 18.53 % and unfilled duties at 22.47%.The total demand for Nursing & Midwifery was 5944 shifts in August 2021. Out of which Bank had covered 2882 shifts (48.49 %). Framework approved agencies had covered 491 (8.26 %). Framework approved agencies where the rates were escalated had contributed 515 shifts (8.66%). Off-framework Suppliers had covered 523 shifts 8.80%). The remaining unfilled shifts for Nursing & Midwifery had contributed to 1533 (25.79 %). Framework Escalations and Off-framework suppliers were utilized to stabilize gaps across the organisation.
Top Three Areas: ITU & HDU had the largest utilization from Framework Escalations and Off-framework suppliers (335 shifts), followed by ED Nurses (60 shifts) & AMU (42 Shifts). Top Three Request Reasons Associated with Framework Escalations and Off-framework Usage: Vacancy (296 shifts), COVID-19 Additional Demand (81 shifts) & Additional Bed Capacity (71 shifts).
The overall Medical Staffing demand in August 2021 was 1657 shifts. Medical Bank filled 826 shifts (50%), Agencies had filled 459 shifts (28 %), Collaborative Bank filled 91 shifts (5 %) and the remaining unfilled were 281 shifts (17 %). Total medical staffing spend through patchwork was £861,056 in August 2021. Bank: £453,919.00 was spent on Medical Bank and £46,201.00 was spent on collaborative bank. A LLR Breach is defined as where there is an escalation of the initially advertised rate. This is a derived from pre-set rates associated with each medical grade. The total number of LLR Breach Bank hours was 5091.53 (63.9 %) of all shifts had breached the LLR rate.
A&E Medics had the highest bank spend with £142,400.00. Agency: £360,936.00 was spent on Agency. The top departments for agency spend for August 2021 were Microbiology Department Medics (£53,800.00), Medical On-Call Rota(£59,000.00) and Respiratory Medicine Medics (£68,000.00).
Recruitment and Vacancies
General Recruitment
Substantive recruitment time to hire for August is at 29.2 days, with a target of 33 days. This has decreased since last month. The overall vacancy rate for the Trust is at 9.5% with a target of 11%.The current vacancies activity being recruited to on TRAC for September onwards are below.
HCA Recruitment
The Trust has received an additional £40K funding from NHSEI to recruit to the HCA vacancies, we currently have 43.57FTE vacancies with 25 HCAs in the pipeline which are being progressed by the recruitment team.
THHFT Board PUBLIC 02 Nov 2021 Page 91 of 225

65
Are We Well-Led? August 2021Well-Led
Recruitment & Vacancies, Cont’d
Retention of Vaccinators
We have started working with the vaccination retention hub at Chelwest to match vaccinators to available positions and will be attending a careers day at the Old Vinyl factory to talk to people who may be interested in working at Hillingdon.
Midwifery International Recruitment
There has been funding made available to recruit international midwifes, which we are looking to recruit a small number of. We also have 5 student midwifes starting in October alongside 1 qualified midwife that started in September
Radiology International Recruitment
There is funding available from HEE to recruit international radiologists and we are meeting with HEE end of September to scope out a project plan for this initiative.We have also been working with radiology to reconcile establishment and vacant post’s to identify recruitment campaigns.
International Nurse Recruitment
We currently have 30 international nurses, and are expecting a further cohort of 5-8 nurses dependant on flights W/C 20th September and a further 20 in October. The nurses still need to isolate for 10 days as the majority are from Amber listed countries, this is putting a strain on the recruitment team, due to getting food supplies and bedding to the accommodation and providing pastoral support out of hours.
Volunteering
Training on the staging state has gone well. We are now on the ‘live’ site. We are slowly integrating ‘active volunteers’ on to the site and have sent existing volunteers an email informing them about the change.
We were able to contact volunteers who supported the vaccine hub earlier in the year about supporting booster jabs and 15 answered the call. These volunteers will make up the first cohort of volunteers using Assemble. Most of them have successfully logged on and we’ll provide further support to those who need it.
After integrating existing volunteers, we aim to start a ward companion recruitment via Assemble by the end of the month.
Two volunteers have been successful in gaining full time positions for the NHS (one at Hillingdon, another at Buckinghamshire NHS Trust). They both had a good experience volunteering and thanked the service and the Trust and we’ll endeavour to further enhance the service and make the NHS an attractive place to work.
A planning day is scheduled at Uxbridge Business Park on 20 September to plan volunteering activity, a strategy outline, and draft business case. The focus going forward will be supporting Care of the Elderly wards. A meeting with the Frailty Lead has taken place and Therapy leads contacted with the first meeting scheduled on 4 October.
THHFT Board PUBLIC 02 Nov 2021 Page 92 of 225

66
Domain Scorecard Summary August 2021Well-Led
KPI ID KPI Description Target Jun-20 Jul-20 Aug-20 Sep-20 Oct-20 Nov-20 Dec-20 Jan-21 Feb-21 Mar-21 Apr-21 May-21 Jun-21 Jul-21 Aug-21
k7.01 Substantive Vacancies <= 11% 10.7% 10.5% 10.2% 10.1% 10.0% 10.0% 10.3% 9.8% 10.1% 8.6% 8.9% 9.1% 8.9% 9.5% 9.5%
k7.02 Voluntary Turnover <= 11% 12.5% 12.3% 12.2% 12.2% 12.0% 11.9% 12.0% 12.0% 12.2% 11.7% 11.7% 11.9% 12.2% 12.3% 12.3%
k7.03 Sickness Absence(In-Month) <= 3% 4.8% 4.9% 4.2% 4.3% 4.5% 4.9% 5.9% 6.9% 5.3% 4.7% 4.4% 4.3% 4.7% 4.8% 4.9%
k7.04 Core Skills Training(Statutory/Mandatory) Training >= 90% 92.5% 91.3% 89.7% 90.8% 92.3% 92.4% 91.8% 90.4% 88.3% 89.0% 90.6% 91.1% 92.4% 92.4% 90.9%
k7.05 Time to Hire(non-Medical) 33 36.5 37.5 35.3 42.3 33.9 32.2 33.2 34.8 36.3 33.5 34.2 38.8 31.7 30.3 29.2
k7.06 Appraisals / PDRs Compliance >= 95% 98.2% 18.8% 25.1% 50.3% 72.5% 78.4% 80.4% 81.3% 81.4% 82.0% 82.8% 82.5% 79.2% 69.8% 62.5%
k7.07 Medical Appraisals >= 90% 74.5% 65.4% 65.6% 68.7% 57.1% 53.4% 52.8% 50.5% 45.2% 47.3% 52.0% 58.5% 76.2% 80.8% 84.2%
k7.08 Agency Spend n/a £309,870 £491,278 £433,803 £610,471 £694,098 £727,881 £630,726 £1,233,553 £1,179,819 £1,379,163 £1,006,394 £970,512 £1,147,576 £1,455,279 £1,646,246
THHFT Board PUBLIC 02 Nov 2021 Page 93 of 225

67
Are We Well-Led? August 2021Well-Led
THHFT Board PUBLIC 02 Nov 2021 Page 94 of 225

68
Are We Well-Led? August 2021Well-Led
THHFT Board PUBLIC 02 Nov 2021 Page 95 of 225

69
Are We Well-Led? August 2021Well-Led
Red Amber Green
1.1 Establishment # 3504.36 3587.47 3530.121.2 Staff in Post (Whole Time Equivalent) # 3135.41 3210.12 3196.161.3 Headcount # 3423.00 3462 3492.00
2.1 Sickness Absence % 4.2% 4.8% 4.9% 3.0%2.2 Long-Term Sickness Absence % 2.9% 3.2% 3.4%2.3 Short-Term Sickness Absence % 1.3% 1.6% 1.5%
2.5 Voluntary Turnover % 12.2% 12.3% 12.3% 11.0%
4.1 Total Requested Shifts # 5360 10348 111494.2 Bank Shifts Filled % 73.8% 64.0% 59.0%4.3 Agency Shifts Filled % 11.2% 16.8% 18.5%4.4 Unfilled Shifts Filled % 15.0% 19.2% 22.5%
5.1 Trust Vacancy Rate % 10.2% 9.5% 9.5% 11.0%5.2 Corporate % 15.0% 13.5% 10.9% 11.0%5.3 Planned Care % 10.7% 7.9% 8.0% 11.0%5.4 Unplanned Care % 6.1% 8.5% 10.4% 11.0%
6.1 Shortlisting # 8.5 7.8 7.7 36.2 Interview Outcome # 3.5 2.3 3.5 36.3 Conditional Offer # 2.6 1.5 2.3 26.4 Pre-employment Checks # 19.3 16.7 14.3 206.5 Time to Recruit # 37.5 30.3 29.2 33
7.1 Trust PDR Rate % 62.5% 69.8% 95.0%7.2 Corporate % 78.2% 74.7% 95.0%7.3 Planned Care % 73.1% 62.1% 95.0%7.4 Unplanned Care % 58.0% 52.1% 95.0%
6. Recruitment (non-medical) - average working days
7. PDRs (AfC staff over 6 months)
Item UnitsThis Month
Last YearLast Month This Month Target/Ceiling
RAG Status
1. Workforce
2. HR Indicators
3. Temporary Staffing Usage
4. Vacancy
THHFT Board PUBLIC 02 Nov 2021 Page 96 of 225

70
Are We Well-Led? August 2021Well-Led
Division Budget (WTE) Staff in Post (WTE) Vac. Diff. Aug % Jul % Division Aug % Jul %Corporate Services Division 841.13 749.42 91.71 10.9% 13.5% Corporate Services Division 10.7% 10.5%Planned Care Division 1458.86 1342.33 116.53 8.0% 7.9% Planned Care Division 11.6% 11.6%Unplanned Care Division 1238.79 1110.41 128.38 10.4% 8.5% Unplanned Care Division 14.2% 14.5%Grand Total 3538.8 3202.2 336.6 9.5% 9.5% Grand Total 12.3% 12.3%
Division Aug % Jul % % +/- Avail. WTE Hrs Abs WTE Hrs Episodes Long-Term (WTE Hrs) % Long-Term Sickness % Short-TermCorporate Services Division 4.8% 5.2% -0.4% 24853.85 1187.71 103 1010.97 4.1% 0.7%Planned Care Division 4.8% 5.0% -0.2% 40951.84 1966.14 270 1267.61 3.1% 1.7%Unplanned Care Division 5.0% 4.2% 0.8% 33487.22 1673.08 264 1056.10 3.2% 1.8%Grand Total 4.9% 4.8% 0.1% 99292.91 4826.93 637 3334.69 3.4% 1.5%
Division Aug (Avg Working Days) Jul (Avg Working Days)Corporate Services Division 30.5 31.1Planned Care Division 24.5 29.2Unplanned Care Division 30.2 36.7Grand Total 29.2 31.7
k7.07 Medical Appraisals, Aug 2021Division Aug % Jul % Division Aug % Jul %Corporate Services Division 74.7% 78.2% Corporate Services Division 100.0% 100.0%Planned Care Division 62.1% 73.1% Planned Care Division 100.0% 80.0%Unplanned Care Division 52.1% 58.0% Unplanned Care Division 70.0% 76.9%Grand Total 62.5% 69.8% Grand Total 84.2% 80.8%
k7.03 Sickness, Aug 2021
k7.05 Time to Recruit, Aug 2021
k7.01 Substantive Vacancy, Aug 2021 k7.02 Voluntary Turnover, Aug 2021
k7.06 Appraisal / PDR, Aug 2021
THHFT Board PUBLIC 02 Nov 2021 Page 97 of 225

71
Are We Well-Led? August 2021Well-Led
Course Planned Care Division Unplanned Care Division Corporate Services Division Central Budgets Division Temporary Staffing Division Grand TotalAdult Basic Life Support Level 1 [Once Only], 80% target 98.9% 96.7% 98.6% 100.0% 95.9% 98.1%Adult Basic Life Support Level 2 [1 Year], 80% target 78.1% 68.9% 72.4% 41.7% 80.8% 74.6%Blood & Blood - Transport Only [1 Year], 80% target #DIV/0! #DIV/0! 18.2% #DIV/0! #DIV/0! 18.2%Blood & Blood [2 Years], 80% target 90.0% 85.7% 79.3% 72.7% 94.1% 88.4%Conflict Resolution [3 Years], 80% target 94.3% 89.9% 93.2% 77.8% 98.0% 93.1%Data Security & Protection [1 Year], 95% target 93.0% 89.3% 94.8% 72.2% 94.2% 92.4%Equality & Diversity [3 Years], 80% target 94.5% 89.7% 94.7% 77.8% 98.0% 93.4%Fire Safety Level 1 [1 Year], 80% target 75.7% 73.5% 88.4% 75.0% 93.7% 82.4%Fire Safety Level 2 [1 Year], 80% target 94.3% 89.3% 86.1% 50.0% 97.5% 92.5%Health, Safety & Welfare [3 Years], 80% target 94.2% 90.4% 94.8% 72.2% 97.8% 93.5%Infection Control Level 1 [3 Years], 90% target 95.5% 95.6% 96.2% 100.0% 95.7% 96.0%Infection Control Level 2 [1 Year], 90% target 90.9% 86.4% 83.1% 66.7% 97.4% 89.7%Moving & Handling Level 1 [3 Years], 80% target 93.8% 84.1% 92.9% 73.3% 95.8% 91.3%Moving & Handling Level 2 [2 Years], 80% target 83.9% 83.0% 85.9% 100.0% 98.6% 85.1%Safeguarding Adults Level 1 [3 Years], 90% target 94.5% 91.2% 93.5% 72.2% 98.2% 93.6%Safeguarding Adults Level 2 [3 Years], 90% target 93.9% 90.3% 92.5% 58.3% 99.1% 92.9%Safeguarding Children Level 1 [3 Years], 90% target 94.0% 90.0% 93.3% 72.2% 98.2% 93.0%Safeguarding Children Level 2 [3 Years], 90% target 93.7% 88.2% 88.7% 58.3% 99.4% 92.0%Safeguarding Children Level 3 [3 Years], 90% target 90.8% 58.0% 77.3% #DIV/0! 100.0% 80.4%Safeguarding Children Level 4 [3 Years], 90% target 100.0% #DIV/0! #DIV/0! #DIV/0! #DIV/0! 100.0%Grand Total 91.5% 86.9% 93.2% 71.6% 96.3% 90.9%
THHFT Board PUBLIC 02 Nov 2021 Page 98 of 225

72
Are We Well-Led? August 2021Well-Led
THHFT Board PUBLIC 02 Nov 2021 Page 99 of 225

73
Benchmarking August 2021Well-Led
Jul-21KPI Hillingdon Imperial LNWUHT ChelWest HRCH CLCH CNWL West London NWL SectorVacancy Rate 9.5% 12.0% 10.7% 8.8% 11.6% 11.0% 11.6% 14.6% 11.4%Turnover (12-Month Rolling) 12.3% 10.4% 10.8% 11.3% 13.0% 12.4% 18.7% 9.4% 12.3%Sickness (In-Month) 4.8% 4.0% 4.0% 3.3% 4.2% 5.1% 3.1% 4.8% 4.2%Sickness (12-month Rolling) 4.9% 3.7% 3.4% 3.1% 3.9% 4.4% 3.1% 4.6% 3.9%Core Skills Training 92.4% 94.0% 85.5% 89.0% 92.1% 96.6% 92.0% 83.7% 90.2%
THHFT Board PUBLIC 02 Nov 2021 Page 100 of 225

COVID Lateral Flow Testing Update Report
Gubby Ayida 10 March 2021
THHFT Board PUBLIC 02 Nov 2021 Page 101 of 225

1. LFT Reporting Performance YTD (Combination of locally reported and centrally reported results)
Lateral Flow Testing (LFT) 6th September 2021
Output name Region Number of staff testing Expected number of tests reported AllTests % Start of Programme WeekTHE HILLINGDON HOSPITALS NHS FOUNDATION TRUST LONDON 2838 5676 964 17.0% Monday, April 5, 2021THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST LONDON 2838 5676 874 15.4% Monday, April 12, 2021THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST LONDON 2838 5676 831 14.6% Monday, April 19, 2021THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST LONDON 2838 5676 757 13.3% Monday, April 26, 2021THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST LONDON 2838 5676 801 14.1% Monday, May 3, 2021THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST LONDON 2838 5676 751 13.2% Monday, May 10, 2021THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST LONDON 2838 5676 752 13.2% Monday, May 17, 2021THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST LONDON 2838 5676 642 11.3% Monday, May 24, 2021THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST LONDON 2838 5676 582 10.3% Monday, May 31, 2021THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST LONDON 2838 5676 225 4.0% Monday, June 7, 2021THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST LONDON 2838 5676 598 10.5% Monday, June 14, 2021THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST LONDON 2838 5676 612 10.8% Monday, June 21, 2021THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST LONDON 2838 5676 597 10.5% Monday, June 28, 2021THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST LONDON 2838 5676 569 10.0% Monday, July 5, 2021THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST LONDON 2838 5676 568 10.0% Monday, July 12, 2021THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST LONDON 2838 5676 183 3.2% Monday, July 19, 2021THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST LONDON 2838 5676 403 7.1% Monday, July 26, 2021THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST LONDON 2838 5676 570 10.0% Monday, August 2, 2021THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST LONDON 2838 5676 540 9.5% Monday, August 9, 2021THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST LONDON 2838 5676 534 9.4% Monday, August 16, 2021THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST LONDON 2838 5676 492 8.7% Monday, August 23, 2021THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST LONDON 2838 5676 670 11.8% Monday, August 30, 2021THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST LONDON 2838 5676 235 4.1% Monday, September 6, 2021
THHFT Board PUBLIC 02 Nov 2021 Page 102 of 225

2. LFT Reporting Performance Benchmarking (locally reported results)
Sum of % tests reported Period
Trust28/06/2021 - 04/07/2021
05/07/2021 - 11/07/2021
12/07/2021 - 18/07/2021
19/07/2021 - 25/07/2021
26/07/2021 - 01/08/2021
02/08/2021 - 08/08/2021
09/08/2021 - 15/08/2021
16/08/2021 - 22/08/2021
23/08/2021 - 29/08/2021
30/08/2021 - 05/09/2021
CENTRAL AND NORTH WEST LONDON NHS FOUNDATION TRUST 45% 23% 1% 0% 0% 0% 0% 0% 0% 0%CENTRAL LONDON COMMUNITY HEALTHCARE NHS TRUST 46% 43% 43% 32% 38% 34% 32% 29% 26% 23%CHELSEA AND WESTMINSTER HOSPITAL NHS FOUNDATION TRUST 31% 35% 36% 35% 45% 37% 36% 36% 34% 34%HOUNSLOW AND RICHMOND COMMUNITY HEALTHCARE NHS TRUST 26% 25% 25% 24% 23% 21% 22% 23% 23% 20%IMPERIAL COLLEGE HEALTHCARE NHS TRUST 12% 12% 13% 13% 12% 12% 12% 11% 11% 10%LONDON NORTH WEST UNIVERSITY HEALTHCARE NHS TRUST 4% 4% 3% 0% 0% 0% 0% 0% 0% 0%THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST 10% 10% 9% 2% 7% 10% 9% 9% 8% 11%WEST LONDON NHS TRUST 11% 2% 0% 10% 9% 0% 0% 0% 0% 0%Grand Total 13% 12% 13% 11% 15% 13% 15% 15% 14% 14%
THHFT Board PUBLIC 02 Nov 2021 Page 103 of 225

Finance
77THHFT Board PUBLIC 02 Nov 2021 Page 104 of 225

78
Are we Using our resources effectively?Divisional Summary Month 5
1. Planned Care is reporting an adverse variance of £0.86m compared to plan. The pressure on pay from Critical Care has increased this month due to more beds being occupied and non-pay is high to clear backlog of patients.
2. Unplanned Care is reporting an adverse variance to plan of £1.55m. Pay is adverse to plan by £1.26m, with overspends on medical, nursing & HCA pay. The escalation ward has remained open all month. Pressure from escalated rates and sickness continue.
3. The Corporate Division is adverse to plan by £0.09m. The pay position has been impacted by a redundancy payment in month of £0.1m.
4. Central Budgets show a favourable variance of £0.80m. NHS Clinical Income is adverse in plan due to ERF not being earned in month. Pay and non-pay are showing favourable variances due to the centrally held cost pressure funding. THHFT Board PUBLIC 02 Nov 2021 Page 105 of 225

79
Are we Using our resources effectively?Transformation Improvement Programme
• The H1 plan for 2021/22 includes a TIP target of £5.1m.
• The tables left show the Month 5 position.
• In month 5 delivery was £0.40m against a target of £0.86m, an adverse variance of £0.45m.
• On a year to date basis, TIPs of £1.5m have been delivered against a budgeted target of £4.3m, an adverse variance of £2.8m.
THHFT Board PUBLIC 02 Nov 2021 Page 106 of 225

80
Report Glossary
Domain KPI ID KPI Description KPI Methodology Data Source
Safe 1.1.1 Discharge Summaries Not Issued Number of discharge summaries not issued at month end ePro
Safe 1.1.2 Discharge Summaries Issued (within 24 hrs) Percentage of discharge summaries issued within 24 hours ePro
Safe 1.1.3 Discharge Summaries Issued (within 7 days) Percentage of discharge summaries issued within 7 days ePro
Safe 1.2.1 No of Inpatient Falls Number of falls reported Datix
Safe 1.2.2 Rate of Inpatient Fall (1000 Bed Days)Number of inpatient falls reported divided by number of General and Acute occupied bed days
Datix / iReporter
Safe 1.2.3 No of Non-Inpatient Falls Number of falls reported Datix
Safe 1.2.4 Rate of All Patient Falls (1000 Bed Days) Number of falls reported divided by number of General and Acute occupied bed daysDatix /
iReporter
Safe 1.2.5 Falls With Fracture Number of falls reported that resulted in fracture Datix
Safe 1.3.1 No. HPAU/Moisture Lesion IncidentsNumber of hospital acquired pressure ulcers, moisture lesion, deep tissue injury incidents
Datix
Safe 1.3.2Rate HPAU/Moisture Lesion Incidents (1000 Bed Days Cat2)
Number of HPAU/Moisture lesions divided by number of General and Acute occupied bed days
Datix / iReporter
Safe 1.3.3 No. Category 2 Pressure Ulcers Number of patients with hospital acquired pressure ulcers (Category 2) Datix
Safe 1.3.4 No. Category 3 & 4 Pressure Ulcers Number of patients with a newly hospital acquired pressure ulcers Categories 3 & 4) Datix
Safe 1.3.5 No. Unstageable Pressure Ulcers Number of patients with hospital acquired pressure ulcers (Unstageable) Datix
Safe 1.3.6 No. Deep Tissure Injuries Number of patients with hospital acquired deep tissue injuries Datix
Safe 1.4.1 Patient Safety Incidents Number of patient safety incidents reported DatixTHHFT Board PUBLIC 02 Nov 2021 Page 107 of 225

81
Report Glossary
Domain KPI ID KPI Description KPI Methodology Data Source
Safe 1.4.2 Reporting Rate Patient Safety Incidents (KH03)Number of patient safety incidents divided by number of General and Acute occupied bed days with KHO3 exclusions
Datix / iReporter
Safe 1.4.3 No. Patient Safety Incidents Graded Moderate + Number of patient safety incidents resulting in moderate or above harm Datix
Safe 1.4.4 Rate of Patient Safety Incidents Graded Moderate +Number of patient safety incidents resulting in moderate or above harm divided by number of General and Acute occupied bed days
Datix / iReporter
Safe 1.5.1 Serious Incidents Declared Total number of serious untoward incidents declared Datix
Safe 1.5.2 Never Events"Never events" are very serious, largely preventable patient safety incidents that should not occur if the relevant preventative measures have been put in place.
Datix
Safe 1.5.3 SI PerformancePercentage of Serious incidents (SIs) submitted to the Clinical Commissioning Group with 60 working days.
DATIX / GMD
Safe 1.6.1 No. Medication IncidentsThe number of incidents which caused harm or potential to cause harm involving an error in administrating, prescribing, preparing, dispensing or monitoring medication.
Datix
Safe 1.6.2 Medicines Reconciliation Started Within 24 hours Percentage of medicines reconciliation started within 24 hours Pharmacy
Safe 1.6.3 Omitted Dose In Last 24 Hrs Percentage of ommitted does in last 24 hours Pharmacy
Safe 1.7.1 MRSA (Trust Attributed) Number of hospital assigned MRSA bacteraemia. IPC
Safe 1.7.2 C.diff Cases HOHA (Hospital Onset Hospital Aquired) Number of hospital acquired C diff bacteraemia. IPC
Safe 1.7.3 C.diff Cases COHA (Community Onset Hospital Aquired) Number of community onset hospital acquired C diff bacteraemia. IPC
Safe 1.7.4 E.Coli Blood Stream Infections (BSIs) Number of hospital acquired E.Coli Blood Stream Infections IPC
Safe 1.7.5 Hand Hygeine Compliance rate with the Infection Control Saving Lives Audit GMD
Safe 1.8.1 Completed Patient Observations - Adult (NEWS) Percentage of adults who received a completed set of NEWS observations hObsTHHFT Board PUBLIC 02 Nov 2021 Page 108 of 225

82
Report Glossary
Domain KPI ID KPI Description KPI Methodology Data Source
Safe 1.11.1 Maternity (Caesarean Section Rate) Percentage of caesarean sections relative to all registerable births Euroking
Safe 1.11.2 Maternity (Postpartum Haemorrage >= 1500ml) Percentage of Postpartum Haemorrage >= 1500ml relative to all registerable births Euroking
Safe 1.11.3 Maternity (1:1 Midwife in Labour) Percentage of women in labout with a 1:1 midwife Euroking
Safe 1.11.4 Maternity (NICU Admissions) Number of admission to neonatal unit PAS
Safe 1.12.1 Day - Registered Midwives/Nurses Fill Rate Actual hours over planned hours Healthroster
Safe 1.12.2 Day - Assistant Fill Rate Actual hours over planned hours Healthroster
Safe 1.12.3 Night - Registered Midwives/Nurses Fill Rate Actual hours over planned hours Healthroster
Safe 1.12.4 Night - Assistant Fill Rate Actual hours over planned hours Healthroster
Safe 1.12.5 Overall Trust Fill Rate Actual hours over planned hours Healthroster
Safe 1.12.6 % of Expenditure on Agency Staff Agency hours over total actual hours Bank Staff
Safe 1.12.7 Care Hours per Patient Day (CHPPD) Total actual hours over cummulative count of patients each dayHealthroster/P
AS
Effective 2.1.1 Crude Mortality Rate Percentage of patients who died in hospital PAS
Effective 2.1.2 Number of Deaths Number of patients who dies in hospital PAS
Effective 2.1.3 SHMIThe ratio between the actual number of deaths following hospital care in relation to the no of patients who were expected to die based on the patient's comorbidities
NHS Digital
Effective 2.1.4 HSMR (Aggregate)The ratio of observed deaths to expected deaths for a basket of 56 diagnosis groups, which represent approximately 80% of in hospital deaths
Dr FosterTHHFT Board PUBLIC 02 Nov 2021 Page 109 of 225

83
Report Glossary
Domain KPI ID KPI Description KPI Methodology Data Source
Effective 2.1.5 HSMR (Weekend)The ratio of observed deaths to expected deaths for a basket of 56 diagnosis groups, which represent approximately 80% of in hospital deaths
Dr Foster
Effective 2.2.1 Sepsis (Eligible Patients Screened)The percentage of patients sampled who met the criteria of the local protocol and were screened for sepsis
hObs
Effective 2.2.2 Sepsis (Antibiotics within 1 hour)The total number of patients sampled who received antibiotics within 1 hour of arrival as a percentage of those who should have received antibiotics within 1 hour of arrival.
hObs
Effective 2.3.1 VTE CompliancePercentage of patients risk-assessed for Venous-Thromboembolism within 24 hours of admission
PAS
Effective 2.4.1 Dementia (Screening)Of the patients who were eligible to be screened for dementia (aged 75 and with a length of stay of 72 hours or greater), how many were screened
PAS/ePro
Effective 2.4.2 Dementia (Assessment)Of the patients who were identified using the dementia screening assessments, how many were appropriately assessed.
PAS/ePro
Effective 2.4.3 Dementia (Referral for Specialist Diagnosis) PAS/ePro
Effective 2.5.1 Readmission RateNumber of hospital readmission within 30 days of original admission as a percentage of all admissions
PAS
Effective 2.5.2 A&E Reattendance RateNumber of A&E reattendances within 7 days of original attendance as a percentage of all attendances. Excluding planned attendances.
PAS
Caring 3.1.1 Complaints (Received) Number of complaints received this month DATIX
Caring 3.1.2 Complaints (Performance)Percentage of complaints that have received a response within the agreed time frame, based on the month in which the response was due
DATIX
Caring 3.1.3 No. Reopened Complaints Number of complaints reopened this month DATIX
Caring 3.1.4 No. Complaints Referred to Ombudsman Number of complaints referred to ombudsman this month DATIX
Caring 3.1.5 No. PALS Contacts Total number of contacts via the Patient Advice and Liasion Service (PALS) Datix
Caring 3.1.6 No. PALS Concerns Number of contacts via PALS of which were expressions of concern DatixTHHFT Board PUBLIC 02 Nov 2021 Page 110 of 225

84
Report Glossary
Domain KPI ID KPI Description KPI Methodology Data Source
Caring 3.2.1 FFT - % good experience (Unplanned Care)Number of patients who would recommend the Trust to friends and family, as a percentage of all respondents.
Caring 3.2.2 FFT - % good experience (Planned Care)Number of patients who would recommend the Trust to friends and family, as a percentage of all respondents.
Responsive 4.1.1 A&E Performance (All Types) Percentage of all A&E attendances discharged within 4 hours of arrival PAS
Responsive 4.1.2 A&E Performance (Type 1) Percentage of type 1 A&E attendances discharged within 4 hours of arrival PAS
Responsive 4.1.3 12 Hour Trolley Waits Number of A&E 12 hour trolley waits CSPs
Responsive 4.1.4 LAS Handover (Performance within 15 mins) Percentage of Ambulance handovers completed within 15 minutes of Arrival at A&E LAS Portal
Responsive 4.1.5 LAS Handover (30 mins waits) Number of LAS Ambulance Handovers - 30 min waits LAS Portal
Responsive 4.1.6 LAS Handover (60 mins waits) Number of LAS Ambulance Handovers - 60 min waits LAS Portal
Responsive 4.1.7 Stranded Patients (>= 7 days) Number of patients in hospital over 7 days PAS
Responsive 4.1.8 Super Stranded Patients (>= 21 days) Number of patients in hospital over 21 days PAS
Responsive 4.1.9 Average Length of Stay (Emergency) Average length of stay for emergency admission PAS
Responsive 4.2.1 RTT (Incomplete Performance) Percentage of open RTT pathways waiting under 18 weeks LUNA
Responsive 4.2.5 RTT (Total Waiting List) Number of patients on RTT waiting list LUNA
Responsive 4.2.2 RTT (52 Week Waiters) Number of open RTT pathways waiting over 52 weeks LUNA
Responsive 4.2.3 Diagnostics (6 Weeks Performance) Percentage of diagnostics waiters within 6 weeksPAS/Infoflex/Auditbase/SolitonTHHFT Board PUBLIC 02 Nov 2021 Page 111 of 225
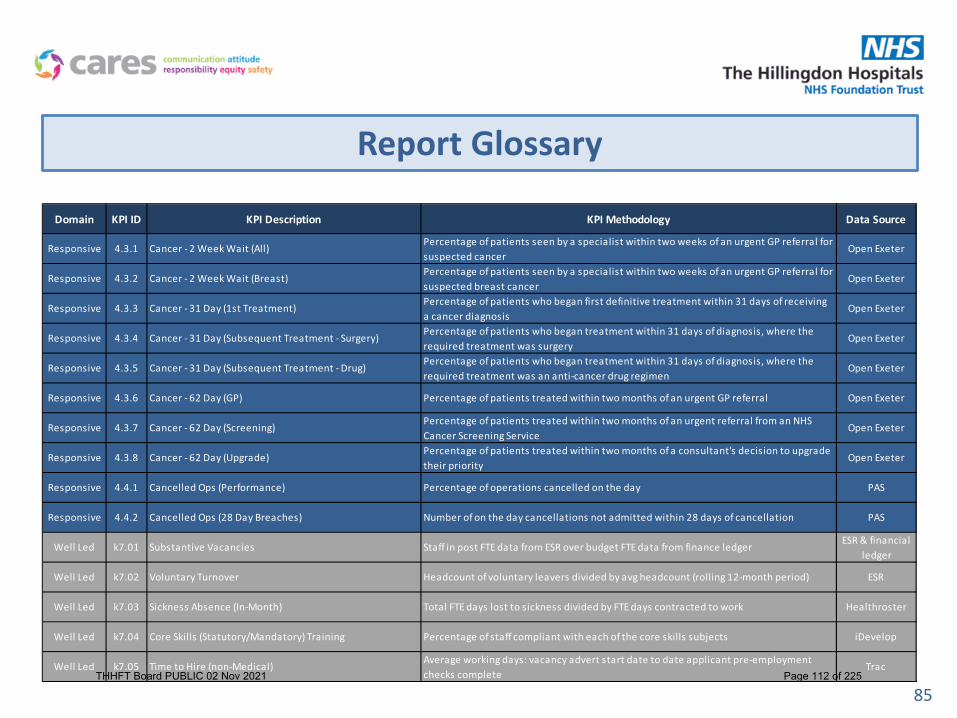
85
Report Glossary
Domain KPI ID KPI Description KPI Methodology Data Source
Responsive 4.3.1 Cancer - 2 Week Wait (All)Percentage of patients seen by a specialist within two weeks of an urgent GP referral for suspected cancer
Open Exeter
Responsive 4.3.2 Cancer - 2 Week Wait (Breast)Percentage of patients seen by a specialist within two weeks of an urgent GP referral for suspected breast cancer
Open Exeter
Responsive 4.3.3 Cancer - 31 Day (1st Treatment)Percentage of patients who began first definitive treatment within 31 days of receiving a cancer diagnosis
Open Exeter
Responsive 4.3.4 Cancer - 31 Day (Subsequent Treatment - Surgery)Percentage of patients who began treatment within 31 days of diagnosis, where the required treatment was surgery
Open Exeter
Responsive 4.3.5 Cancer - 31 Day (Subsequent Treatment - Drug)Percentage of patients who began treatment within 31 days of diagnosis, where the required treatment was an anti-cancer drug regimen
Open Exeter
Responsive 4.3.6 Cancer - 62 Day (GP) Percentage of patients treated within two months of an urgent GP referral Open Exeter
Responsive 4.3.7 Cancer - 62 Day (Screening)Percentage of patients treated within two months of an urgent referral from an NHS Cancer Screening Service
Open Exeter
Responsive 4.3.8 Cancer - 62 Day (Upgrade)Percentage of patients treated within two months of a consultant's decision to upgrade their priority
Open Exeter
Responsive 4.4.1 Cancelled Ops (Performance) Percentage of operations cancelled on the day PAS
Responsive 4.4.2 Cancelled Ops (28 Day Breaches) Number of on the day cancellations not admitted within 28 days of cancellation PAS
Well Led k7.01 Substantive Vacancies Staff in post FTE data from ESR over budget FTE data from finance ledgerESR & financial
ledger
Well Led k7.02 Voluntary Turnover Headcount of voluntary leavers divided by avg headcount (rolling 12-month period) ESR
Well Led k7.03 Sickness Absence (In-Month) Total FTE days lost to sickness divided by FTE days contracted to work Healthroster
Well Led k7.04 Core Skills (Statutory/Mandatory) Training Percentage of staff compliant with each of the core skills subjects iDevelop
Well Led k7.05 Time to Hire (non-Medical)Average working days: vacancy advert start date to date applicant pre-employment checks complete
TracTHHFT Board PUBLIC 02 Nov 2021 Page 112 of 225

86
Report Glossary
Domain KPI ID KPI Description KPI Methodology Data Source
Well Led k7.06 Appraisals / PDRs Compliance Percentage of non-medical staff compliant with their appraisal iDevelop
Well Led k7.07 Medical Appraisals Percentage of Medics compliant with their annual appraisalMedical Staffing
Team
Well Led k7.08 Agency Spend Total sum of agency spend (actuals)Financial
Ledger
THHFT Board PUBLIC 02 Nov 2021 Page 113 of 225

87
SPC Chart Symbol Description
Source: NHS Improvement SPC Tool
Perform Assure DescriptionSpecial cause of a concerning nature where the measure is significantly HIGHER. This occurs where there is higher pressure in the system or deteriorating performance. This system is not capable. It will FAIL the target without system change.
Special cause of a concerning nature where the measure is significantly HIGHER. This occurs where there is higher pressure in the system or worse performance. However despite deterioration the system is capable and will consistently PASS the target.
Special cause of a concerning nature where the measure is significantly HIGHER. This occurs where there is higher pressure in the system or worse performance. This system will not consistently hit or miss the target. (This occurs when target lies between process limits).
Special cause of a concerning nature where the measure is significantly LOWER. This occurs where there is deteriorating performance. This system is not capable. It will FAIL the target without system change.
Special cause of a concerning nature where the measure is significantly LOWER. This occurs where there is deteriorating performance. However the system is capable and will consistently PASS the target.Special cause of a concerning nature where the measure is significantly LOWER. This system will not consistently hit or miss the target. (This occurs when target lies between process limits).
Common cause variation, no significant change.This system is not reliably capable. It will FAIL to consistently meet target without system change.
Common cause variation, no significant change. The system is capable and will consistently PASS the target.
Common cause variation, no significant change. This system will not consistently hit or miss the target. (This occurs when target lies between process limits).
Perform Assure DescriptionSpecial cause of an improving nature where the measure is significantly HIGHER. This occurs where there improving performance. However the system is still not capable. It will FAIL the target without system change.
Special cause of an improving nature where the measure is significantly HIGHER. This occurs where there is improving performance. The system is capable and will consistently PASS the target.
Special cause of an improving nature where the measure is significantly HIGHER. This occurs where there improving performance. This system will not consistently hit or miss the target. (This occurs when target lies between process limits).
Special cause of an improving nature where the measure is significantly LOWER This occurs where there improving performance. However the system is still not capable. It will FAIL the target without system change.
Special cause of an improving nature where the measure is significantly LOWER. This occurs where there is improving performance. The system is capable and will consistently PASS the target.Special cause of an improving nature where the measure is significantly LOWER. This occurs where there improving performance. This system will not consistently hit or miss the target. (This occurs when target lies between process limits).
THHFT Board PUBLIC 02 Nov 2021 Page 114 of 225

Operational Recovery Plan
THHFT Board Meeting-Public
Date of the meeting: 2 November 2021
ITEM: 8.1a
Purpose of the Report/Paper: The Operational recovery plan provides assurance to the committee that all areas of operational performance are monitored with key actions in place, allowing the committee to gain assurance and information regarding actual performance and remedial actions. This operational recovery plan will continue to be revised with new actions added as required to achieve the operational performance and recovery trajectories, that were set out in the H1 operating plan. For: Information Assurance Discussion and input Decision/approval Executive summary: The report focuses on the high impact actions that will be taken in order to meet the agreed standards for areas in non elective care such as for ED performance, same day emergency care, early discharge. The report also highlights key actions for meeting the HI operational plan standards in elective care such as RTT, Cancer, DM01, Outpatient and Theatre recovery. The report also sets out timelines for when the expected standards and trajectories will be met. Sponsor (Executive Lead):
Tina Benson, Chief Operating Officer
Authors:
Melissa Mellett, Director of Operations Anjali Joshi, Director of Operations
Author contact details:
[email protected] [email protected]
Risk implications – Link to Board Assurance Framework or Corporate Risk Register:
All
Legal/Regulatory/Finance/Quality & Safety/ HR/E&D/Engagement/Communications/Reputation or Sustainability implications:
Finance Quality and Safety Reputation
Link to Relevant CQC Domain: Safe Effective Caring Responsive Well Led Link to relevant Corporate Objectives/strategic aims:
All
Document previously considered by: Operational Management Group
Recommendations: The Committee is asked to note the Recovery plan
THHFT Board PUBLIC 02 Nov 2021 Page 115 of 225

Operating Recovery Plan
Melissa Mellett & Anjali Joshi
THHFT Board PUBLIC 02 Nov 2021 Page 116 of 225
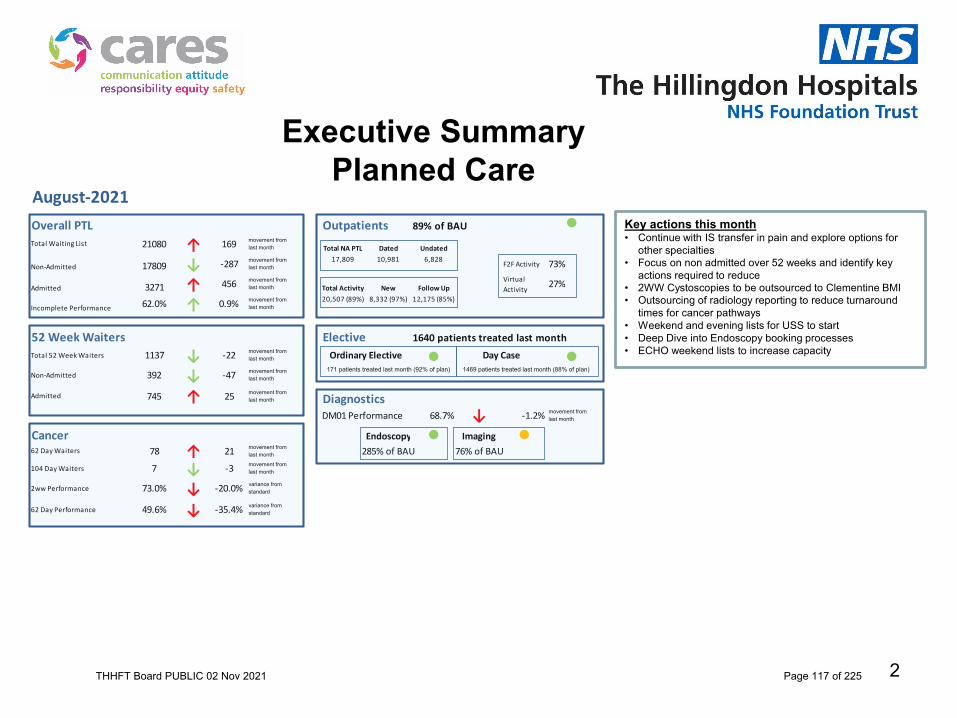
2
Executive SummaryPlanned Care
Overall PTL Outpatients 89% of BAU ●21080 ↑ 169 movement from
last month Total NA PTL Dated Undated
17809 ↓ -287 movement from last month
17,809 10,981 6,828F2F Activity 73%
3271 ↑ 456 movement from last month Total Activity New Follow Up
Virtual Activity
27%
62.0% ↑ 0.9% movement from last month
20,507 (89%) 8,332 (97%) 12,175 (85%)
52 Week Waiters Elective 1640 patients treated last monthTotal 52 Week Waiters 1137 ↓ -22 movement from
last month ● ●Non-Admitted 392 ↓ -47 movement from
last month
Admitted 745 ↑ 25 movement from last month Diagnostics
DM01 Performance 68.7% ↓ -1.2% movement from last month
Cancer Endoscopy ● Imaging ●62 Day Waiters 78 ↑ 21 movement from
last month 285% of BAU 76% of BAU
104 Day Waiters 7 ↓ -3 movement from last month
2ww Performance 73.0% ↓ -20.0% variance from standard
62 Day Performance 49.6% ↓ -35.4% variance from standard
Incomplete Performance
Ordinary Elective Day Case171 patients treated last month (92% of plan) 1469 patients treated last month (88% of plan)
Admitted
August-2021
Total Waiting List
Non-Admitted
Key actions this month• Continue with IS transfer in pain and explore options for
other specialties• Focus on non admitted over 52 weeks and identify key
actions required to reduce• 2WW Cystoscopies to be outsourced to Clementine BMI• Outsourcing of radiology reporting to reduce turnaround
times for cancer pathways• Weekend and evening lists for USS to start• Deep Dive into Endoscopy booking processes• ECHO weekend lists to increase capacity
THHFT Board PUBLIC 02 Nov 2021 Page 117 of 225

Executive SummaryUnplanned Care
10.0% ↓ -0.8% 81 ↑ 5
Performance 21 Days and Over
New
Follow Ups
0.6% 5.7 ↑ 0.1
DischargeBed Occupancy
-24
Discharges Before 12pm Long Length of Stay
Average LOS
Surgical
Readmissions
347 ↓
150 ↓ -3 344 ↓ -15
66
19↑↑406
110
Discharges 7 Days and Over
↑
48.4% ↓ -0.3% 80.0% ↑ 8.2%
Adults Paeds
326.4 ↓ -19.3
3484 ↓ -145 2119 ↓ -52
Walk In's Ambulances Total
●Attendances
Mental HealthAttendances
60 Minutes 33 ↓ -34 98.3% ↑ 1.7%
12 Hour Breaches Avg LOS (minutes)
-82 49.6%
94.5%
Avg LOS In Department (minutes)
Ambulance HandoverBreaches Performance
15 Minutes 963 ↓
-0.4 137.1 ↑ 0.1
↑ 3.6%
5603 ↓ -197
Avg Initial Assess Avg Treatment Time
58.8 ↓
August-2021
Same Day Emergency CareType 1 All Types
55.3% ↑ 0.9% 74.5% ↓ -13.5%
Overall ED Performance ●-64
-29
New
Follow UpsMedical
↓↓460
172
99 ↑ 6 4 ↑ 1 478.8 ↓ -2.5
THHFT Board PUBLIC 02 Nov 2021 Page 118 of 225

Unplanned Care Recovery
ED Actions
• Front end Senior Clinical Decision maker - from 16th September.
• Model Cubicle Role out – 16th
September.• NIC / CIC Zone created for
oversight of shift• Transformation programme to
support culture of improvement following RIE and subsequent follow up event in October.
• Business Case for staffing associated with trajectory in final stage. September 24th.
• Third middle grade overnight – 20th
September
SDEC Actions
SAU has now moved into its new space in The Wilson Unit so figures above reflect old capacity. AECU now has the whole of Churchill ward.A business case has been submitted for expansion of AECU nursing and admin staffing.Approval has been granted for the ED Lead to take on Clinical Leadership for the AECU
Non Admitted Actions
• Direct referrals to AMU and extended use of AECU – 28th August
• Enhanced MDV coverage – AMC / CT Control Room 28th August
• Go live with 1st clinician 28th October
• CDU open 24/7 • Self Transfer for AECU
System support required• Continued demand management and increase hard stop at the front door.• RIE outputs from HHCP ED• UTC Streaming processes to be reviewed.
Type 1 (New Trajectory)
Aug Sept Oct Nov Dec Jan Feb March
Target 59.0% 71.0% 76.1% 83.6% 87.3% 91.0% 91.0%
Actual 55.3%
Same Day Emergency Care
Medical Surgical
750 ( 747) 170
Non Admitted
Breaches T1 Performance T1
1,562 62.4%
All Types
All Type 1
73.3% 55.3%
THHFT Board PUBLIC 02 Nov 2021 Page 119 of 225

5
NWL 104ww- 110pts 05/09/21
THHFT Board PUBLIC 02 Nov 2021 Page 120 of 225
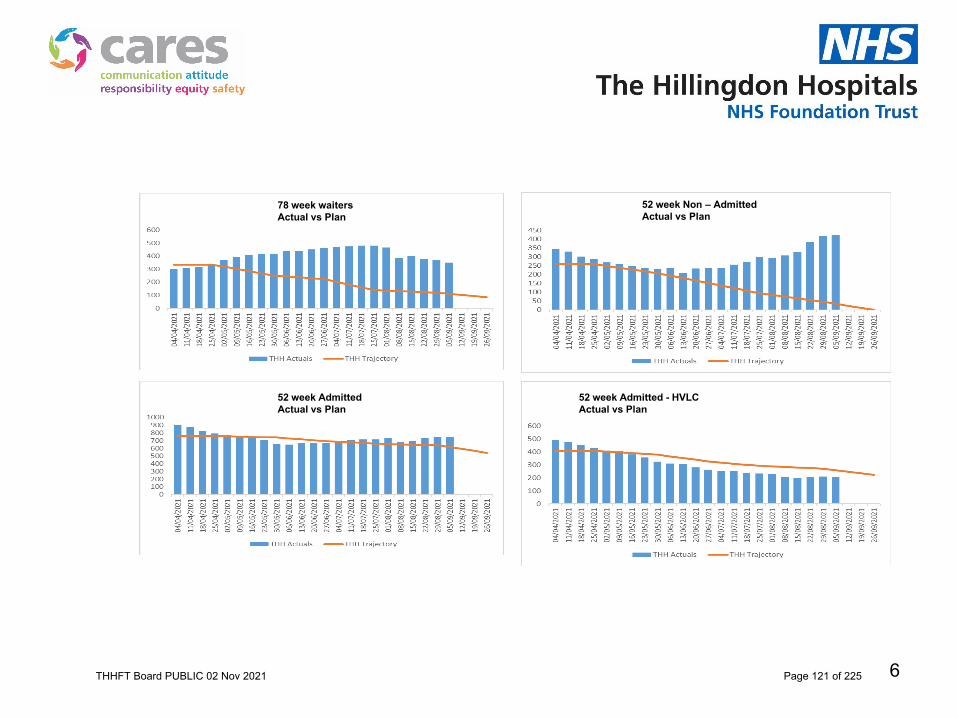
6
THH 52 week Actuals vs Trajectories
52 week Non – Admitted Actual vs Plan
78 week waitersActual vs Plan
52 week Admitted Actual vs Plan
52 week Admitted - HVLC Actual vs Plan
THHFT Board PUBLIC 02 Nov 2021 Page 121 of 225

Operating Plan
50%
60%
70%
80%
90%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Elective Total
50%
60%
70%
80%
90%
100%
110%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Elective Inpatients
50%
60%
70%
80%
90%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Daycases
50%
60%
70%
80%
90%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Outpatients - Consultant Led - Total
50%
60%
70%
80%
90%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Outpatients - Consultant Led - First
50%
60%
70%
80%
90%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Outpatients - Consultant Led - Follow Up
THHFT Board PUBLIC 02 Nov 2021 Page 122 of 225

Operating Plan
50%
60%
70%
80%
90%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Magnetic Resonance Imaging
50%
60%
70%
80%
90%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Computed Tomography
50%
60%
70%
80%
90%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Non-obstetric ultrasound
50%
60%
70%
80%
90%
100%
110%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Endoscopy
50%
60%
70%
80%
90%
100%
110%
120%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Cardiology - Echocardiography
THHFT Board PUBLIC 02 Nov 2021 Page 123 of 225
Operational Recovery Action Plan
Progress against actions set.October 2021
THHFT Board PUBLIC 02 Nov 2021 Page 124 of 225
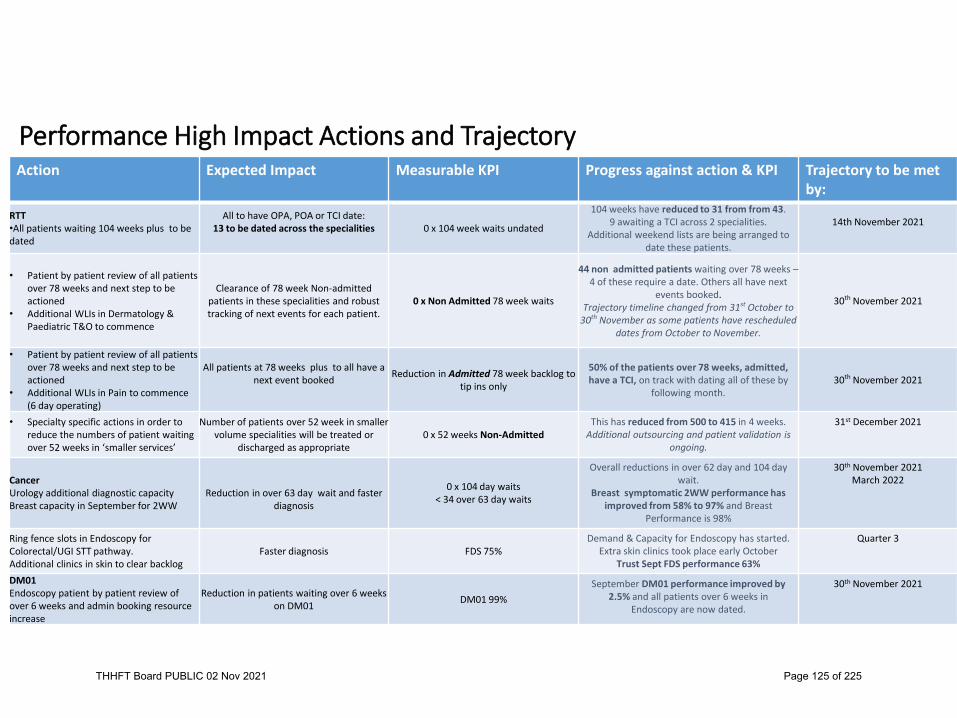
Performance High Impact Actions and TrajectoryAction Expected Impact Measurable KPI Progress against action & KPI Trajectory to be met
by:RTT•All patients waiting 104 weeks plus to be dated
All to have OPA, POA or TCI date:13 to be dated across the specialities 0 x 104 week waits undated
104 weeks have reduced to 31 from from 43.9 awaiting a TCI across 2 specialities.
Additional weekend lists are being arranged to date these patients.
14th November 2021
• Patient by patient review of all patients over 78 weeks and next step to be actioned
• Additional WLIs in Dermatology & Paediatric T&O to commence
Clearance of 78 week Non-admitted patients in these specialities and robust tracking of next events for each patient.
0 x Non Admitted 78 week waits
44 non admitted patients waiting over 78 weeks –4 of these require a date. Others all have next
events booked.Trajectory timeline changed from 31st October to
30th November as some patients have rescheduled dates from October to November.
30th November 2021
• Patient by patient review of all patients over 78 weeks and next step to be actioned
• Additional WLIs in Pain to commence (6 day operating)
All patients at 78 weeks plus to all have a next event booked Reduction in Admitted 78 week backlog to
tip ins only
50% of the patients over 78 weeks, admitted, have a TCI, on track with dating all of these by
following month.30th November 2021
• Specialty specific actions in order to reduce the numbers of patient waiting over 52 weeks in ‘smaller services’
Number of patients over 52 week in smaller volume specialities will be treated or
discharged as appropriate0 x 52 weeks Non-Admitted
This has reduced from 500 to 415 in 4 weeks.Additional outsourcing and patient validation is
ongoing.
31st December 2021
CancerUrology additional diagnostic capacityBreast capacity in September for 2WW
Reduction in over 63 day wait and faster diagnosis
0 x 104 day waits< 34 over 63 day waits
Overall reductions in over 62 day and 104 day wait.
Breast symptomatic 2WW performance has improved from 58% to 97% and Breast
Performance is 98%
30th November 2021March 2022
Ring fence slots in Endoscopy for Colorectal/UGI STT pathway.Additional clinics in skin to clear backlog
Faster diagnosis FDS 75%Demand & Capacity for Endoscopy has started.
Extra skin clinics took place early OctoberTrust Sept FDS performance 63%
Quarter 3
DM01Endoscopy patient by patient review of over 6 weeks and admin booking resource increase
Reduction in patients waiting over 6 weeks on DM01 DM01 99%
September DM01 performance improved by 2.5% and all patients over 6 weeks in
Endoscopy are now dated.
30th November 2021
THHFT Board PUBLIC 02 Nov 2021 Page 125 of 225

Operational Recovery High Impact actions and TrajectoryAction Expected Impact Measurable KPI Progress against action &
KPITrajectory to be met by:
Outpatients -Reduce DNA rate from 10% to 8%• Dedicated resource to be allocated to
Envoy system to ensure patient responses are actioned within 24 hours of receipt.
• HCAs to call patients within specialities with highest number of DNAs. Explore the use of volunteers or bank staff for this.
Reduction in DNAs and increase in activity towards activity plan.
8% DNA rate95% Outpatient Activity - meeting the plan
Total Outpatient Actvity has improved to average of 92% for the previous 4 weeks.Actions have been put in place however
DNA rate hasn’t reduced.Discussions in place with Dr Doctor to
implement solution in place at C&W and ICHT, which has reduced DNA rates.
30th September 2021
Outpatients –Review of templates and increasing bookings.Ensure all attendances are marked to ensure activity is captured
Increase in activity towards plan 95% Outpatient Activity - meeting the plan
Increase in template slots seen and improvements in ‘unmarked’ backlog
clearance has improvement outpatient activity by approx. 2% a week.
31st October 2021
Theatres - Improve theatre utilisationIncrease in patients per list for Pain and Oral SurgeryPre-op telephone clinics to move to weekend to increase F2F capacity in the weekLA patients to move from pre-op to specialties
Increase in activity towards planReduction in short notice cancellations
85% utilisation by specialtyMeeting the 95% activity plan for electives
Total Elective performance has improved since August.Week ending 3rd Oct total elective activity was 91% of 19/20 baseline.
Activity through theatres has increased every week for the last 5 weeks and w/e 3rd Oct, the Trust was 4th highest in London for HVLC activity.
30th September 2021
Diagnostics - Increase MRI activityMutual aid being provided by West Middlesex and LNWUHChasing availability of a mobile scanner on THH site
Reduction in MRI backlogReduction in cancer diagnostic delays
Meeting 95% of operating planDM01 performance 99%FDS for cancer being met
Mobile MRI unit in place and operating from 11th October and future bookings have increased by 100 cases per week.
31st October 2021
THHFT Board PUBLIC 02 Nov 2021 Page 126 of 225

Caesarean Section Report – November 2021 THHFT Board meeting- Public
Date of the meeting: 02 November 2021
ITEM: 8.2
Purpose of the Report/Paper: To provide an update on Caesarean Sections Rates
For: Information Assurance Discussion and input Decision/approval Executive summary: This report includes the following:
• Current caesarean section rates at Hillingdon • Northwest London Sector caesarean section rates • Reasons for increased caesarean section rates • July caesarean section audit information • Recommendations from caesarean section audit
Sponsor (Executive Lead):
Ms Gubby Ayida, Medical Director
Author:
Julie Cooper, Director of Midwifery and colleagues
Author contact details:
Risk implications – Link to Board Assurance Framework or Corporate Risk Register:
BAF risk 1 BAF1.1, 1.2, 1.3, 1.4, 1.5, 1.6, 3.1, 3.2 & 3.3
Legal/Regulatory/Finance/Quality & Safety/ HR/E&D/Engagement/Communications/Reputation or Sustainability implications:
Regulatory
Link to Relevant CQC Domain: Safe Effective Caring Responsive Well Led Link to relevant Corporate Objectives/strategic aims:
Quality – We will deliver consistent high quality care Performance – we will deliver the right care at the right time or our patients
Document previously considered by: Quality & Safety Committee
Recommendations: The Board is invited to note the findings of the report.
THHFT Board PUBLIC 02 Nov 2021 Page 127 of 225

Update on Caesarean Section Rates
October 2021
1THHFT Board PUBLIC 02 Nov 2021 Page 128 of 225
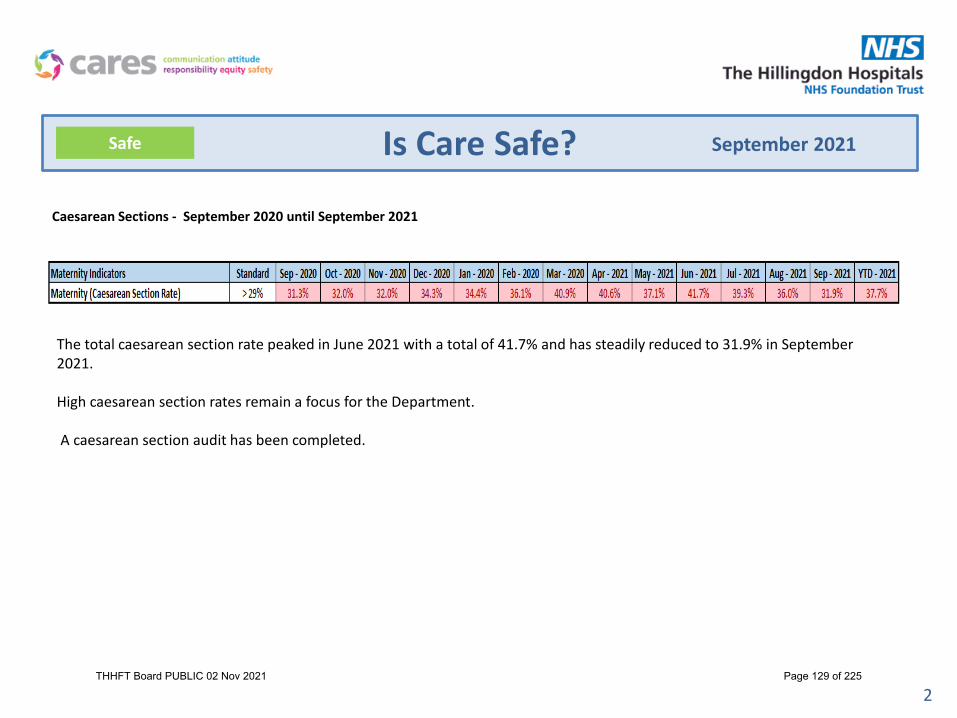
2
Is Care Safe?Safe September 2021
Caesarean Sections - September 2020 until September 2021
The total caesarean section rate peaked in June 2021 with a total of 41.7% and has steadily reduced to 31.9% in September 2021.
High caesarean section rates remain a focus for the Department.
A caesarean section audit has been completed.
THHFT Board PUBLIC 02 Nov 2021 Page 129 of 225

3
Is Care Safe?
Caesarean Sections 2021The caesarean section rate is on a par with the rest of the North West London Sector. See below.
Safe September 2021
THHFT Board PUBLIC 02 Nov 2021 Page 130 of 225

4
Is Care Safe?
Caesarean Sections 2021
Safe September 2021
THHFT Board PUBLIC 02 Nov 2021 Page 131 of 225
5
Is Care Safe?Safe September 2021
Reasons for increased Caesarean Section*VBAC= vaginal birth after CS
THHFT Board PUBLIC 02 Nov 2021 Page 132 of 225

6
Is Care Safe?Safe September 2021
Audit into Caesarean Sections 2021
THHFT Board PUBLIC 02 Nov 2021 Page 133 of 225

7
Is Care Safe?
Recommendations following the Audit 2021 - Elective (planned) Caesarean Sections
1. Accept user expectations
2. VBAC clinics more accessible in different stages of pregnancy
3. Macrosomia stickers for consistent advice and offer earlier Induction rather than CS (As suggested by new NICE guidelines)
4. Streamline CS pathway as services need to change to accommodate our increased elective CS demand
VBAC= Vaginal birth after Caeserean Section
Macrosomia= Big Baby
Induction =starting labour
Recommendations following the 2021 Audit - Emergency Caesarean Sections
1. Timely booking for elective Caesarean Sections
2. CTG teaching of pathological CTG-indicated CS (Fetal monitoring lead)
3. Induction process not delayed as high CS rate after 42 weeks
4. Avoid early Vaginal examinations and inappropriate use of Syntocinon
CTG-=Cardiotocograph (electronic fetal heart rate monitoring)
Safe September 2021
THHFT Board PUBLIC 02 Nov 2021 Page 134 of 225

1
2020 Urgent & Emergency Care (UEC) Survey
THHFT Board Meeting-Public Date of the meeting: 02 November 2021
ITEM: 9 Purpose of the Report/Paper: To provide an update on the trust’s results of the 2020 Urgent & Emergency Care (UEC) Survey. The results were published on the CQC website on 15th September 2021 For: Information Assurance x Discussion and input Decision/approval Executive summary: This report provides an overview of the trust’s performance in the 2020 Urgent & Emergency Care (UEC) Survey. The report highlights areas where patients reported positive aspects of patient experience and outlines the next steps to address areas for improvement. Main points to note:
• 322 patients returned a completed questionnaire, giving a response rate of 27% compared to 30.5% nationally
• When compared with other organisations, the trust performed ‘about the same’ as most other trusts that took part in the survey in all 9 sections
• The Trust scored “better” than other trusts in one question: o Were you able to get suitable food and drink when you were in A&E?
• The Trust scored “worse” than other trusts in three questions: o Did doctors or nurses talk to each other about you as if you weren’t
there? o How clean was the A&E department? o After leaving A&E, was the care and support you expected available
when you needed it? • 79% of patients felt overall, they had a good experience • Overall, the Trust’s 2020 scores are an improvement compared to the 2018
report • When comparing the trust with 9 other similar hospitals in Model Hospital
peer group, 1 hospital scored better, 7 hospitals scored the same and 1 hospital scored worse than our trust.
Sponsor (Executive Lead):
Melanie Van Limborgh, Director of Nursing
Author:
Catherine Holly, Head of Patient experience
Author contact details:
THHFT Board PUBLIC 02 Nov 2021 Page 135 of 225

2
Risk implications – Link to Board Assurance Framework or Corporate Risk Register:
BAF Risks 1 & 4 & 5
Legal/Regulatory/Finance/Quality & Safety/ HR/E&D/Engagement/Communications/Reputation or Sustainability implications:
Regulatory, Quality & Safety, Reputation
Link to Relevant CQC Domain: Safe x Effective x Caring x Responsive x Well Led x Link to relevant Corporate Objectives/strategic aims:
Quality – We will deliver good care every day Workforce – We want empowered, committed people with the right skills and attitude
Document previously considered by: N/A Recommendations: The Board is invited to note and comment on the content of this report.
THHFT Board PUBLIC 02 Nov 2021 Page 136 of 225

3
1. Introduction The 2020 Urgent and Emergency Care Survey surveyed patients who were aged 16 or older and who had attended the UEC services (Type 1 accident and emergency (A&E) department) in September 2020. The results of the Urgent & Emergency Care survey were published on the CQC website on 15th September 2021. As in previous years, the trust appointed Picker to deliver the 2020 national A&E survey on its behalf. Patients were sent by post a questionnaire, a covering letter from the trust, a multiple language sheet offering help with the survey and a CQC flyer. A Freepost envelope was also supplied in which those who wished could return their completed questionnaire. Non-responders were sent a reminder letter after 2-3 weeks and a further reminder with another copy of the questionnaire after a further 2-3 weeks. Picker ran a Freephone helpline for patients who had queries or concerns about the survey. Access to Language Line was also available with interpreters in over 100 languages. A total of 1250 patients who were discharged from the A&E department were sent a postal questionnaire inviting them to take part in the survey. 322 patients returned completed questionnaires. The survey response rate was 27%. 2. Results There are 9 sections in the National A&E Survey. These are: • Arrival • Waiting times • Doctors and nurses • Care and treatment • Tests
• Hospital environment & facilities • Leaving A&E • Respect & dignity • Experience overall
The results show that the trust performed ‘about the same’ as most other trusts that took part in the survey in all 9 sections. 2.1. Breakdown of results by questions There are 38 comparative questions in the survey. • The Trust scored “better” than other trusts in one question:
o Were you able to get suitable food and drink when you were in A&E?
• The Trust scored “worse” than other trusts in three questions as follows: o Did doctors or nurses talk to each other about you as if you weren’t there? o How clean was the A&E department? o After leaving A&E, was the care and support you expected available when
you needed it? The trust scored about the same in all remaining 34 questions. The survey highlighted many positive aspects of patient experience:
THHFT Board PUBLIC 02 Nov 2021 Page 137 of 225

4
• Handover from ambulance to A&E - for those taken to A&E in an ambulance not having to wait too long with the ambulance crew before care was handed to A&E staff (80%)
• Time to talk - for feeling they had enough time to discuss their condition with a doctor or nurse (82%)
• Being listened to - for feeling the doctor or nurse listened to what they had to say (87%)
• Confidence and trust - for having confidence and trust in the doctors and nurses examining and treating them (84%)
• Acknowledging patients - for doctors and nurses not talking in front of them, as if they weren't there (82%)
• Information about condition or treatment - for being given the right amount of information about their condition or treatment (84%)
• Privacy when examined or treated - for being given enough privacy when being examined or treated (88%)
• Communication - for not being told one thing by a member of staff and something quite different by another (86%)
• Cleanliness - for describing A&E as clean (85%) • Safety - for not feeling threatened by other patients or visitors (95%) • Clear explanations about medication purpose - for those prescribed new
medications, having the purpose of new medications explained to them in a way they could understand (94%)
• Respect and dignity - for being treated with respect and dignity (87%) 3. Comparison with the 2018 survey results Surveys are refined year-to-year but overall are comparable. The 2020 survey results show an improvement compared to the 2018 report. The 2018 survey had 30 questions: • The Trust’s results were significantly higher in 2020 in 8 questions
o How long did you wait before you first spoke to a nurse or doctor? o Sometimes, people will first talk to a doctor or nurse and be examined later.
From the time you arrived, how long did you wait before being examined by a doctor or nurse?
o Sometimes, people will first talk to a doctor or nurse and be examined later. From the time you arrived, how long did you wait before being examined by a doctor or nurse?
o Sometimes, people will first talk to a doctor or nurse and be examined later. From the time you arrived, how long did you wait before being examined by a doctor or nurse?
o If you needed attention, were you able to get a member of medical or nursing staff to help you?
o Sometimes, a member of staff will say one thing and another will say something quite different. Did this happen to you?
o In your opinion, how clean was the A&E department? o Overall, I had a very good experience.
THHFT Board PUBLIC 02 Nov 2021 Page 138 of 225

5
• The Trust’s results were significantly lower this year in 0 questions: • There was no statistically significant differences between the 2018 results and
2020 results for 22 questions. 4. Comparison with 9 similar trusts, (from Model Hospital peer group),
selected by NHSEI
Trust Better About the
same
Worse Score unavailable
Current CQC rating
Airedale NHS FT 0 9 0 Requires improvement
Bedfordshire Hospitals NHS FT
0 8 0 1 Good
Croydon Health Services NHS Trust
0 9 0 Requires improvement
Dartford and Gravesham NHS Trust
0 3 6 Good
George Elliot Hospital NHS Trust
0 9 0 Requires improvement
Kettering General Hospital NHS FT
0 9 0 Requires improvement
Mid and South Essex NHS FT
0 9 0 Requires improvement
The Princess Alexandra Hospital NHS FT
0 9 0 Requires improvement
Somerset NHS FT
5 4 0 Good
The Hillingdon Hospitals NHS FT
0 9 0 Requires improvement
5. Action The Emergency Department management team will review the results and agree actions required that are likely to have the highest impact on experience for the largest group of patients. Progress will be monitored via divisional reporting at the Patient Experience Review Group.
6. Conclusion The survey provides useful insight into a patient’s A&E experience as reported by patients. When compared with other organisations, the trust performed ‘about the same’ as most other trusts that took part in the Urgent and Emergency Care Survey. Whilst it is pleasing to note that 79% of patients felt overall, they had a good experience, there is scope for improvement.
THHFT Board PUBLIC 02 Nov 2021 Page 139 of 225

People Strategy Update Report THHFT Board meeting- Public
Date of the meeting: 02 November 2021 ITEM: 10
Purpose of the Report/Paper: This purpose of this report is to provide an update on progress to date against the Year One action plan within newly approved People Strategy. For: Information Assurance x Discussion and input Decision/approval Executive summary: Our new People Strategy was approved last month and is written around four key themes: • Looking after our people • Belonging in our trust • New ways of working and delivering care • Growing our workforce We have an ambitious three year action plan underpinning these four themes and this is the first update provided to Board regarding progress being made and some of the challenges we face. In light of our Recovery Support Programme and as we plan for the second half of the year (H2), the focus for the past month has been the establishment of an affordable workforce plan, with an initial focus on the nursing workforce where we have established clarity about numbers, options regarding new roles and different ways of working such as the Registered Nursing Associate role, and therefore a clear plan to recruit both through the UK and internationally. Our newly appointed Diversity & Inclusion Lead has put in place a robust programme of staff engagement as demonstrated by the re-launch of the BAME network, and the excellent Freedom to Speak Up and Black History Month programme throughout October. As we prepare for winter, our newly appointed Health & Wellbeing Lead has also begun work to refresh and communicate our health and wellbeing offer, alongside the delivery of our Covid booster and Flu vaccination programme. Running alongside this is also the need to encourage staff to complete their NHS Staff Survey.
Sponsor (Executive Lead):
Sue Smith Chief People Officer
Author:
Jo Fanning Deputy Chief People Officer
Author contact details:
THHFT Board PUBLIC 02 Nov 2021 Page 140 of 225
Risk implications – Link to Board Assurance Framework or Corporate Risk Register:
BAF risks 2.1-2.9
Legal/Regulatory/Finance/Quality & Safety/ HR/E&D/Engagement/Communications/Reputation or Sustainability implications:
Finance HR
Link to Relevant CQC Domain: Safe Effective Caring Responsive Well Led Link to relevant Corporate Objectives/strategic aims:
Workforce- Great Place to work! (we want empowered, committed people with the right skills and attitude) Well Led- we will empower our people to deliver
Document previously considered by: People Committee Recommendations: The Board is invited to note the information provided and be assured that appropriate action is being taken to address risks and challenges identified against delivery of the Year One action plan.
THHFT Board PUBLIC 02 Nov 2021 Page 141 of 225

THHFT Board PUBLIC 02 Nov 2021 Page 142 of 225
People & OD Update
1
September 2021
THHFT Board PUBLIC 02 Nov 2021 Page 143 of 225

2
Looking after our people
Promote health and wellbeing to all our people to ensure they are safe and well to work:The P&OD team have now appointed an Engagement and Wellbeing Lead, who isin post and will be a key role in supporting to develop a comprehensive staffhealth and wellbeing programme.
We are continuing to work with the NW London Sector Health andWellbeing task and finish group, and internally are setting up our Healthand Wellbeing Steering Group as well as reviewing the role that CARESChampions may have in driving this agenda forward:
• Healthy Body• Healthy Mind• Healthy Living• Keeping Safe
We now have 63 trained mental health first aiders following additionalcohorts held during September and October. Monthly meetings are heldwith this group supported by our psychological services team and we arereviewing how best to utilise this role within the Trust.
The Covid booster and Flu vaccination programmes are now live - ourtarget is 90% and current compliance for the Covid booster is 34.8% of allstaff (of which 33.1% are front line clinical staff) and for flu is 11.8% of allstaff (of which 8.4% are front line staff).
We are seeking an IT solution to establish which staff have received dualvaccinations outside of the Trust, but until this option is effective we willbe contacting staff directly to establish this information and if not alreadyvaccinated, the importance of keeping both themselves and our patientssafe.
Improve the learning & development experience:The Education Strategy Board met for the first time in October – its corepurpose is to oversee the delivery of learning and development across allstaff groups at the Trust, shape the provision of a multi-disciplinaryfacilities within the new hospital development, and ensure arrangementswithin the interim as the site undergoes re-development are fit forpurpose.
The Management Fundamentals’ virtual training is now being offered tostaff at Hillingdon in collaboration with Chelsea and Westminster. Dateshave been shared with Divisional Leads and HRBPs and included withinTrust communication.
This is a modular programme and sessions are bookable either via theEventbrite platform, or by contacting the L&OD team. Sessions includetopics such as Management vs. Leadership, Time Management, andCommunication all of which are delivered by the L&OD team. Other topicssuch as planning for retirement are available and delivered by an externalfacilitator.
Work is on-going to launch the “Embracing Leadership” programme inJanuary, which will offer a wider variety of open programmes andmasterclasses as well targeted team development opportunities.
Improvements have also been made in the take-up of the Apprenticeship Levy we are now at 25% utilisation which is double what it has been. Work is underway to introduce radiography apprenticeships and to continue to support HCSW in undertaking their level 2 qualification which will increase the levy uptake further.
THHFT Board PUBLIC 02 Nov 2021 Page 144 of 225

3
Belonging in our trust
Ensure best managerial and leadership practice:The team are continuing to support complex disciplinary, dignity at work,grievance and MHPS cases. There are currently 15 ER cases, three ofwhich are expected to close by the end of the month. The team is alsocontinuing to focus on the management of sickness absence, workingclosely with Divisional Leads to support staff and to manage absences inline with the policy. There is a specific focus currently on those off withlong term sickness.
Since launching the new policy and the additional fact finding step, therehave been 6 fact finding cases this month; 4 of which has been resolved atthis fact finding stage without progressing to a formal investigation. OurHead of Employee Relations is commencing a programme of‘Transforming Organisational Culture - Principles and Practises ofRestorative Just Culture’, to further enhance developing, implementingand evaluating a restorative just culture in our Trust.
The team have also being working on a programme to deliver trainingsessions for managers on key ER policies, with an initial focus onPerformance Management, Managing Conduct and Sickness Absence.
There will be training uploaded to i-develop from end of October, andvirtual manager training sessions held through November and December.The Employee Relations team is continuing to work on theimplementation of the ER Tracker and the review of templates letter isnow complete, with an implementation date is 6th November.
Secure equity for everyone and recognise, reward, and celebrate our people:During October we celebrated Black History Month and our Freedom toSpeak Up, culminating in a music al event on the 29th October by theMusic in Hospitals Charity.
In addition a range of other activities have taken place this month:
• Promoting our networks via leaflets and stands, to improveparticipation
• In your shoes days: Hayes, Facilities & Catering, Kennedy, Franklin• EDI awareness training @ Theatres• Drop in session: first and last Friday of the month• Walk and Talk: discuss with our EDI lead• EDI Roll Up banner• LGBT network posters.• Wellbeing support network: Introduction meeting on the 19th October
Two radio shows were also recorded (Radio Hillingdon and MVH radio),introducing the new Diversity & Inclusion Lead and our strategy, toincrease awareness and engagement.
Additionally, the Trust is due to launch long service awards to ensure oursubstantive staff who have been employed within the NHS for a longperiod receive positive recognition for this service. From November 2021we will commence this roll out, awarding staff who reach key length ofservice milestones with a pin badge highlighting their years of service anda certificate of appreciation.
THHFT Board PUBLIC 02 Nov 2021 Page 145 of 225

4
New ways of working & delivering care
Understand supply changes and analyse current and future workforceneeds:It is essential that the trust has an affordable workforce plan and a draftreturn was made this week as part of the wider North West LondonIntegrated Care System workforce plan in line with our H2 funding:
Engage fully with the workforce to seek their input into solutions,innovations and improvements:The NHS staff Survey 2021 was launched on 20th Sept 2021. As at 18thOctober 2021 24.5% of our staff have responded to the Staff Survey, thisis broken down by 33% Corporate Services, 25% Planned Care, and 17.4%Unplanned Care.
HRBPs are working with the Divisions to encourage staff to complete thesurvey. Across services in both Planned and Unplanned Care, weekly dropin sessions for staff have been set up to allow staff dedicated time tocomplete the survey. In addition, promotional work is being conductedthrough Trust wide communications, walkabouts and engaging with staffon various Divisional forums.
We are holding weekly staff survey meetings between P&OD and theCommunications Team to review response rates and feedback receivedfrom staff on the walkabouts. Following this we are due to launch bothteam and individual level incentives to encourage further participation inthe survey. We are also providing managers with key pointers to helpsupport them explain to staff why they should complete their staff surveyand the key actions we have taken as a result of last year’s staff survey.
The consultation for a third division, Mount Vernon and Clinical SupportServices, closed on 6th October 2021, and the new division will beimplemented on the 1st November 2021.
The Redevelopment consultation to move corporate services off site hasalso concluded and the first moves will take place in November.
Establishment Baseline Actual Actual Plan Plan Establishment
2020/21End of Year
Staff in Post20/21 End of
Year
Q1(End of Jun '21)
Q2(End of
Sept '21)
Q3(End of Dec '21)
Q4(End of
Mar '22)
2021/22Whole Year
Substantive (FTE) 3457.51 3160.42 3087.05 3102.36 3094.71 3094.71 3578.58Bank (FTE) 386.48 347.93 340.03 343.98 343.98
Agency (FTE) 235.04 188.05 229.95 209.00 209.00Total Provider
Workforce (FTE) 3457.51 3781.94 3623.03 3672.34 3647.69 3647.69 3578.58
Registered Nursing & Midwifery
1039.36 944.70 938.73 917.36 928.05 928.05 1110.82
Allied Health Professionals (AHP)
194.56 170.26 165.40 170.78 168.09 168.09 209.36
Other Sci/Thera/Tech Staff (STT)
68.14 75.19 22.52 23.89 23.21 23.21 70.99
Healthcare Scientists (HCC)
22.30 20.09 22.66 24.41 23.54 23.54 19.32
Support to Nursing 433.51 375.99 442.47 470.32 456.40 456.40 452.48Support to AHP 46.37 34.39 33.61 36.08 34.85 34.85 46.98
Support to STT/HCC 83.25 64.69 67.12 60.61 63.87 63.87 84.25Total Non-Med Staff 5345.00 1685.31 1692.51 1703.45 1697.98 1697.98 1994.20
Consultants 197.36 185.22 184.42 182.51 183.47 183.47 199.86Staff/Career Grades 67.17 49.81 52.28 48.26 50.27 50.27 64.52
Trainee Grades 246.15 268.14 252.97 262.97 257.97 257.97 262.09Total Medical & Dental
Staff 510.68 503.17 489.67 493.74 491.71 491.71 526.46
NHS Infrastucture Support 1059.34 971.94 904.87 905.17 905.02 905.02 1057.92
THHFT Board PUBLIC 02 Nov 2021 Page 146 of 225
5
Growing for the future
Embed a strong, unique employer brandTraining on the volunteer management system has progressed. We arenow working off two websites. (one staging to test what we put on thelive site). Most of the volunteers have migrated and are interacting withthe app. The first role is ‘live’ though currently only available via emailinvite, until the web teams link our website to the Go Assemble platform.This gives us time to test the process fully before making the offer public.Once completed, interviewing and processing volunteers will take up mytime.
We completed all the risk assessments for ‘inactive volunteers’ as well ascontacting them to find out if they were returning. There are now 70active volunteers down from 200 March 2020.
Pressure is on to recruit volunteers ahead of winter pressures. Fundingfor the current part time coordinator post is due to finish in November butwe will be submitting an application for the Volunteer Service Fund fromNHS E/ I on 18 October 2021 to extend this role on a full time basis.
If successful, the aim is to scale up the volunteer offer in three main areas:
• Outpatients Appointment Centre: Appointment reminder volunteers• Therapy Service Volunteers: SALT• Ward Companions: Care of the Elderly Services
In the meantime, we continue to support existing projects e.g. infantfeeding volunteers and volunteers on the post labour ward and the Careof the Elderly service.
Deliver targeted and streamlined recruitmentIn support of the Recovery Support Programme, a nursing workforceaction plan has been developed, the overall aims being:
• Ensure safe and effective nursing & midwifery staffing• Reduce reliance on costly temporary staffing solutions• Provide a sustainable nursing and midwifery model• Meet the needs of our workforce and our patients
Short term actions:• Rapid review undertaken of ward budgets, rosters and ESR to provide
assurance that wards have adequate funding to provide safe staffing and to ensure that all stakeholders agree on the current bed base.
• Work underway with NHSE/I to ensure optimal use of HealthRoster and Allocate software to support staffing decisions. E-rostering lead nurse appointed on temporary basis to work with wards and TSO to support improvements.
• Vacancy report generated identify high-risk areas, develop action plans and track progress.
Medium term actions:• On-going international recruitment and planning for future fit.• Establishment of a guaranteed h job scheme for N&M graduates
Long term actions:• Work with divisions to undertake skill-mix reviews of all areas.• Embed the use of nursing associates within ward establishments• Establish appropriate education programmes to ensure corrects kills
within the nursing workforce (including clinical skills, leadership, PDRs etc.)
THHFT Board PUBLIC 02 Nov 2021 Page 147 of 225

Raising Concerns/Speaking Up: Six Monthly Report
THHFT Board meeting- Public Date of the meeting: 02 November 2021 ITEM: 11
Purpose of the Report/Paper: To provide the Trust Board with an update on Freedom To Speak Activities for the period April 2021 to September 2021, includes the Trust events to celebrate FTSU Month and recommendation for discussion and formal decision. Please note, this paper comprises of quarter 1 and 2 reports presented to Trust Management Board and the Peoples committee in July and October 2021. For: Information Assurance Discussion and input Decision/approval Executive summary: Speaking Up or raising concern keeps workers and patients safe. All workers are encouraged to raised concerns that they may have relating to actual or potential risk, malpractice, wrongdoing and or suggestions to make improvements. Listening Up is critical to hearing and understanding the concerns raised that should be considered as gifts, to be handled effectively and timely. Following Up is to handle the matter or escalate further, give feedback to acknowledge that the worker have been listened to and heard even if resolution hasn’t yet happened and keep up to date on progress. Only then, we will demonstrate learning and culture change. This is the ninth bi-annual FTSU report to the board informing of qualitattive and quauntative FTSU activities within the Trust. Sponsor (Executive Lead):
Sue Smith, Chief People Officer
Author:
Cherma St Clair, Freedom To Speaking Up (FTSU) Guardian
Author contact details:
Risk implications – Link to Board Assurance Framework or Corporate Risk Register:
BAF
Legal/Regulatory/Finance/Quality & Safety/ HR/E&D/Engagement/Communications/Reputation or Sustainability implications:
Quality and Safety/ Regulatory
Link to Relevant CQC Domain: Safe Effective Caring Responsive Well Led Link to relevant Corporate Objectives/strategic aims:
Relevant to all
THHFT Board PUBLIC 02 Nov 2021 Page 148 of 225

Ensuring safe, high quality and sustainable Acute Services
Document previously considered by: Recommendations: The Trust Board is requested to discuss the report, and agree the recommendations made.
Raising Concerns/Speaking Up Report:
THHFT Board PUBLIC 02 Nov 2021 Page 149 of 225

1. Introduction
It is five years since Sir Francis’s Freedom To Speak Up review into whistleblowing culture within the NHS, yet many do not know that Freedom to Speak Up is part of a national initiative to help improve patient and workers safety; that guidance is taken from the National Guardians Office, which then reports to Parliament every year.
Speaking Up protects patients and workers, but is only effective if leaders Listen Up and Follow Up. Leaders must set the tone from the top, where compassionate and inclusive leadership are role modelled, where our organisational values is articulated at every opportunity so that they are meaningful and lived by all workers. Leader’s commitment to listen up and follow up enables Freedom To Speak Up Guardians to support workers efficiently. In practice this result in learning, continuous improvement and the ability to share with others to deliver high quality care.
Adhering to the NHS standard contract and the National Guardian Office Guidelines, recruitment of the Freedom to Speak up Guardian (FTSU) and FTSU Champions are critical to providing an additional confidential and safe route for workers to speak up. We know that Speaking Up saves lives. It is about patient safety, staff safety, negative behaviours and or anything that prevents the delivery of safe excellent care as well as ideas for improvement.
It must be noted that the Care Quality Commission (CQC) have been ask to consider leadership, organisational culture, resources available to FTSU Guardians, FTSU training and processes for tackling barriers to speaking up as important elements in their assessment of well-led (Key lines of Enquiry 3). This ninth bi-annual report aims to update on FTSU activities from April 2021 to September 2021, includes events during October.
2 Update on FTSU Nationally (April to September 2021) The National Guardian, Henrietta Hughes, has now stepped down after five years. We await the appointment of her successor. The National Guardian Office continues with FTSU agenda nationally. One recommendation made is for all organisations to review their FTSU status regularly, two to three yearly, to strengthen strategies towards cultural change. The recommendation states that the FTSU self-review tool and Guidance for Trust boards published in 2018, should be used to review status. Important publications for this period are as follows:-
• FTSU Index – May 2021 FTSU-Index-Report-2021.pdf (nationalguardian.org.uk)
• Revised Guidelines for recording cases for FTSU Guardians – July 2021 Recording Cases and Reporting Data (nationalguardian.org.uk)
• Five-year National Strategic Framework for FTSU – July 2021 NGO-Strategic-Framework-2021.pdf
• Case Review: Blackpool Teaching Hospitals – October 2021 Blackpool_Teaching_Hospitals_FT_case_review.pdf (nationalguardian.org.uk)
3. Local Update from FTSU Guardian
THHFT Board PUBLIC 02 Nov 2021 Page 150 of 225

3.1 Review of recommendation in the last paper (April 2021) a) Communication – Feedback informs some improvement. Leaders who
participated in the FTSU events demonstrated compassionate leadership through reflection of lived experience.
b) An Executive lead is assign to every concern to assure that all issues raised are handle according to best practice. This includes tackling potential barriers to speaking up.
c) FTSU Training modules are accessible via IDevelop. Workers are encouraged to complete. Around 40 workers have undertaken this training. For those who completed the training feedback inform that training should be mandatory. The appropriate committee or forum will assess the briefing paper (appendix 1) and make decision.
d) Review of our FTSU status is yet to be completed. This is a need to review and update the Trust FTSU vision and strategy, which need to be align with our Peoples strategy and the National Strategic Framework for FTSU.
e) Workers are not yet confident to tell their stories – working progress.
3.2. Policy Update
To reflect best practice the Trust FTSU policy has been up-dated, ratified by JNCC and published on the intranet. Summary of changes are as follows:-
• Quick reference guide – replace flow charts for raising and handling concerns with two simpler flowcharts
• link to relevant policy and well-being hub inserted • Update compliance and mentoring • Update Appendices A, C, D. • Duties and responsibilities – move to Appendix –B, also reference role of the
FTSU Champions • Executive team names and e-mail addresses are remove from appendix D1,
and link inserted to the FTSU intranet page where these details can be located.
3.3 Celebrating FTSU and Black History Month
Now an annual event, October is FTSU and Black History month. Both equally important, enabling inclusive and expansive opportunities, to reflect on the past, to raise awareness, celebrate progress and address identified gaps.
We celebrated FTSU and BH month with a number of events (Appendix 2). We heard from Trust Leaders, workers and guest speakers. Feedback from the events were consistent, inspiring, thought provoking, glimmer of hope for the future. Focusing on the BH we gathered toolkit of nuggets for development. For FTSU, Leaders made pledged. All recorded sessions are available on the Trust U-tube channel. 3.4 Concerns & Themes: (April to September 2021) Forty workers contacted the FTSU Guardian and Champions with their concerns during this period; 16 in Q1 and 24 in Q2. This brings the total amount of cases
THHFT Board PUBLIC 02 Nov 2021 Page 151 of 225

recorded to 407. Many concerns are multi-thematic comprising of mix elements. Main themes include safety, negative behaviours, work life balance and flexible working pattern, recruitment and pay dispute. Analysis in accordance with national categories are detailed below:- Graph (a) Professional group, graph (b) professional level, graph (c) ethnic group and graph (d) types of concerns.
Analysis of data illustrated in all graphs shows actual numbers. The cases categorised as other in graph (d) consist of workers making contact for information, advice and signposting. As mentioned above, also included are flexible working, recruitment, increment suspensions and mandatory updates.
3.5 Workers’ Feedback (Q1 &Q2)
63 3 2 2
0 0 0
63
8
1 2 2 1 102468
10
Graph (a)
Q1 Q2
11
5 0 0
119
2 2
MANAGER WORKER SENIOR LEADER
UNKNOWN
Graph (b)
Q1 Q2
02
3
6
0
5
1
57
10
0
8
ANONYMOUS PT SAFETY WORKERS SAFETY
BAHAVIOUR DETRIMENT OTHER
Graph (d)
Q1 Q2
Q1 = 16; Q2 = 24
Equal number of nurses and midwives raised concern in Q1 & Q2.. There was an increase in the number of admin / Clerical workers speaking up during
113 2
105
9
BAME NON BAME UNKNOWN
Graph (C)
Q1 Q2
Open / Cases
Q2 – 15 Open cases of which 3 -HR investigation, 2 –no response re follow up actions. 9 cases closed.
Q1- 4 cases open of which 1 is been investigated at department level.
THHFT Board PUBLIC 02 Nov 2021 Page 152 of 225

Nearly all workers who raise concern to the FTSU Guardian and Champions give informal feedback expressing thanks for listening, for providing a safe platform to speak up, for advice and direction, support and taking their concerns seriously to stages of facilitation or escalation. However, most do not complete the formal feedback request. Alternative strategies is been considered to address this. 4. Conclusion Progress to make speaking up business as usual are been made; still, we have much more to do. Workers continue to speaker up about safety, their day-to-day experiences and negative behaviours that they encounter, including incivility and mirco-aggressions. Many have given positive feedback resulting from speaking up. Nonetheless, there are many who do not feel safe to do so. We believe that in order to deliver excellent quality care for our patients, our staff need to feel safe in their workplace. Leaders and managers are listening more as well as following up with actions, but this needs to be consistent. When things go wrong, have the potential to go wrong or needs improvement, we need to make sure that actions are taken, lessons are learnt and improvements are made. Giving feedback remains an identified gap that require addressing by both workers raising concerns and handling concerns raised. 5. Recommendations
1) Decision regarding the status of FTSU Training. 2) Promote psychology safety for worker to facilitate them to rely their experiences 3) Complete review of our FTSU status. Used the findings to review and update
the Trust FTSU vision and strategy ensuring that it is aligned with our Peoples strategy and the National Strategic Framework for FTSU
4) FTSU Guardian and Champions aims to undertake audit FTSU service and gap analysis of the recommendation of the last case review.
Appendix 1- Training proposal for FTSU Training Appendix 2 – Programme for October 2021
THHFT Board PUBLIC 02 Nov 2021 Page 153 of 225

FTSU Training Proposal
THHFT Board meeting-Public Date of meeting: 02 November 2021
ITEM: 11
Purpose of the Report/Paper: This paper is a proposal outlining the background, underpinning guidelines together with regional and local progress for FTSU training to be considered as mandatory. Executive summary: Speaking up saves lives and improves the wellbeing of workers. It is essential that workers are adequately prepared to raise concerns that they may have and for managers and leaders to be equiped to handle workers concerns in accordance to best practice to effect learning and change. This can only be accomplished through recommended training to gain the right knowledge and skills. Sponsor (Executive Lead):
Sue Smith, Chief People Officer
Author:
Cherma St Clair, Freedom To Speaking Up (FTSU) Guardian
Author contact details:
Risk implications – Link to Board Assurance Framework or Corporate Risk Register:
All BAF risks
Legal/Regulatory/Finance/Quality & Safety/ HR/E&D/Engagement/Communications/Reputation or Sustainability implications:
Quality and Safety/ Regulatory
Link to Relevant CQC Domain: Safe ☐ Effective ☐ Caring ☐ Responsive ☐ Well Led ☐ Link to relevant Corporate Objectives/strategic aims:
Train and develop our workforce
Recommendations for Freedom to Speak Up Training e-Learning: Module 1: Speaking Up - mandatory for all workers
Module 2: Listening Up - mandatory for all workers with line management
responsibilities.
THHFT Board PUBLIC 02 Nov 2021 Page 154 of 225

1. Introduction
The National Guardian’s Office (NGO) was established following recommendations made in the Freedom To Speak Up Review by Sir Robert Francis QC. The NGO works to effect cultural change in the NHS so that speaking up becomes business as usual. This Office leads, trains and supports a network of Freedom to Speak Up Guardians (FTSUGs) nationally, conducts case reviews within organisations, and works in partnership with the wider health system to support learning and improvement.
2. Background and Underpinning Guidelines From case reviews conducted, the NGO observed that training on Freedom to Speak Up had not kept up pace with developments in the field and did not fully reflect the NHS’s approach to speaking up. The NGO therefore undertook to develop national guidelines, designed to improve the quality, clarity and consistency of training on speaking up across the health sector to support those commissioning and delivering training. These guidelines were published in August 2019, detailing the level of training that is needed for different levels of staff on speaking up throughout organisations. The guideline outlined format, principles, and methodology to be used to develop for FTSU training together with learning objectives. In the NGO guidance under the “principle” section it stipulates that Freedom To Speak Up Training should follow the following principles: All workers are required to complete training on Speaking Up. That FTSU training should be treated with the same priority as other mandatory training
that organisations may have such as risk management or safeguarding. That workers should repeat this training regularly enough to reinforce its key messages
and to provide assurance that changes in organisational policies and procedures are properly disseminated and understood
In the NHS Standard Contract 2021/22 section 5.10.1 it supports this training requirement in reference to Freedom to Speak Up and states: The provider must appoint one or more Freedom to Speak up Guardians to fulfil the
role and to comply with the requirements of the National Guardian Office. In addition, having completed my Health and safety mandatory update training, it occurred to me (which I now believe) that there is a lot of links to FTSU, in particular ensuring safety of all workers. FTSU play a crucial role in ensuring the legal duties of both the employer and employee can be met, to foster a safer workplace for all. Remember also, if employees (or others) think that their concerns have not met with a suitable response, they can make a complaint directly to the Health and Safety Executive. This training is therefore vital to preparing workers with knowledge to speak, listen and follow up effectively and appropriately.
3. Regional Progress Many organisations have developed their own training based on the NGO’s ‘National guidelines on Freedom to Speak Up training within the health sector in England, since this was published in August 2019. For one Trust within the London region, the Core training has been included within their statutory and mandatory training to be completed annually and by all new starters and the for line and middle managers’ training has been incorporated within the e-learning Leadership and People Development Programme, which all managers are required to complete.
THHFT Board PUBLIC 02 Nov 2021 Page 155 of 225
Since the development and publication of the HEE/NGO e-learning modules (October 2020), many organisations have implemented these in various ways. For some Module 1 “Speaking Up” was introduced as mandatory for all new starters, whilst Module 2 “Listen Up” was incorporated in management training. Others have used the workers video within the core training as mandatory for all.
4. Local Progress The publication of the NGO guidelines on FTSU training was presented to Trust Board in October 2019 (FTSU paper) with a recommendation that all workers should undertake training, acknowledging that no funding came with this recommendation. This training was crucial to all workers base on FTSU data and staff survey results. Equipping workers with knowledge in raising concerns is at the core of culture change and promotes patient safety. In addition for those with, line manager’s responsibilities, enabling active listening and giving timely feedback appropriately were equally as important. At the time of reporting to the board, work had begun with the Learning and Development team to develop an e-learning FTSU training package for all staff, with additional interactive session for senior managers and a draft outline was produced. However, this did not progress beyond the initial stage; reasons were multifaceted and included priorities, staffing and the impact of the pandemic. The approach to implement e-learning modules developed by the NGO in collaboration with Health Education England in October 2020, removed the need to develop our own and enable the Trust to be in adherence with this national mandate. Details of the e-learning modules were presented to various committees, including the executive team and the Board (FTSU paper April 2021). The training was launched on IDevelop in March 2021 and a briefing went out to all staff through the communication in April 2021. . Module 1 “Speaking Up” - is aimed at all workers including volunteers, students and
those in training. Module 2 “Listen Up” – is aimed at all workers with line management responsibilities. Module 3 “Follow Up” – is aimed at all senior leaders and should be undertaken in
conjunction with module 1 and 2 (when it becomes available).
In line with the recent guidance on Champion networks, established FTSU Champions have been asked to complete both the HEE/NGO core and managers’ training. Feedback received from those who have completed this training was that Module 1 “Speaking Up” should be included in the Trust’s mandatory training profile at the very least and should be completed by all workers.
5. Recommendations
Module 1 “Speaking Up” should be mandatory for all workers and updated every 3 years. The length of this e-learning is approximately 20 minutes.
Module 2 “Listen Up” should be mandatory for all new managers in post and for existing managers with updates every three years.
The Videos within both modules should be accessible as a stand-alone via the FTSU webpage and the wellbeing hub.
THHFT Board PUBLIC 02 Nov 2021 Page 156 of 225
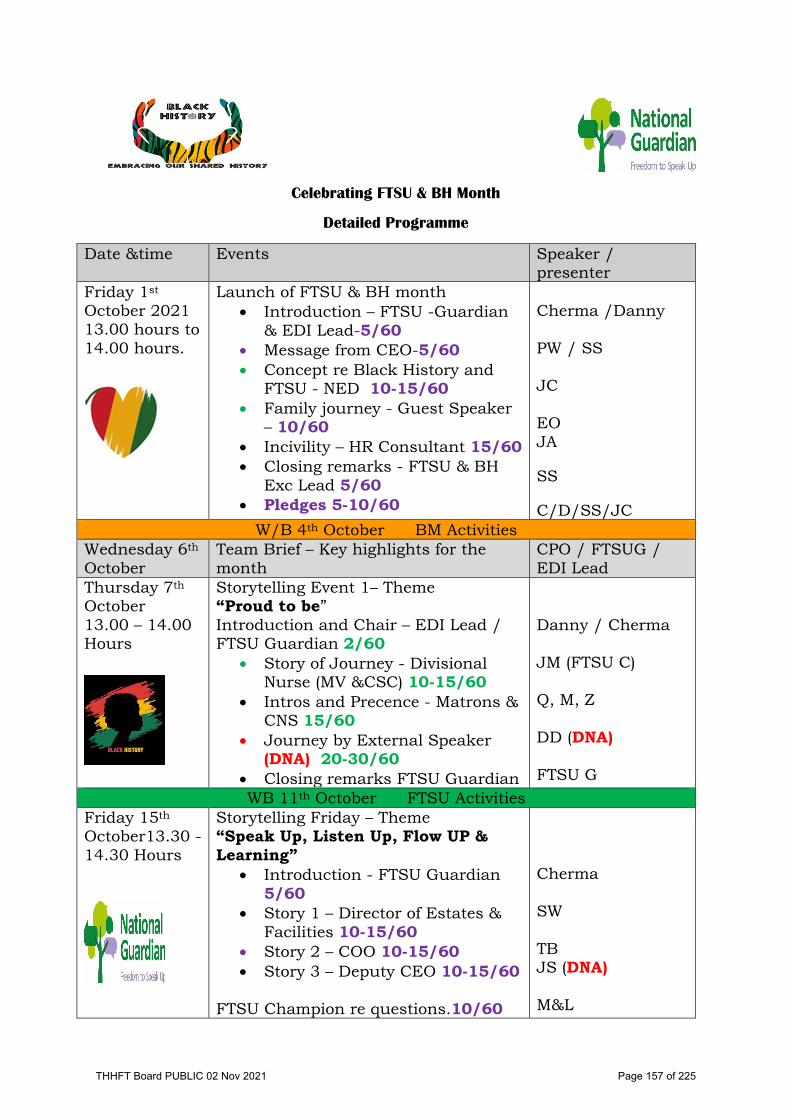
Celebrating FTSU & BH Month
Detailed Programme
Date &time Events Speaker / presenter
Friday 1st October 2021 13.00 hours to 14.00 hours.
Launch of FTSU & BH month • Introduction – FTSU -Guardian
& EDI Lead-5/60 • Message from CEO-5/60 • Concept re Black History and
FTSU - NED 10-15/60 • Family journey - Guest Speaker
– 10/60 • Incivility – HR Consultant 15/60 • Closing remarks - FTSU & BH
Exc Lead 5/60 • Pledges 5-10/60
Cherma /Danny PW / SS JC EO JA SS C/D/SS/JC
W/B 4th October BM Activities Wednesday 6th October
Team Brief – Key highlights for the month
CPO / FTSUG / EDI Lead
Thursday 7th October 13.00 – 14.00 Hours
Storytelling Event 1– Theme “Proud to be” Introduction and Chair – EDI Lead / FTSU Guardian 2/60
• Story of Journey - Divisional Nurse (MV &CSC) 10-15/60
• Intros and Precence - Matrons & CNS 15/60
• Journey by External Speaker (DNA) 20-30/60
• Closing remarks FTSU Guardian
Danny / Cherma JM (FTSU C) Q, M, Z DD (DNA) FTSU G
WB 11th October FTSU Activities Friday 15th October13.30 -14.30 Hours
Storytelling Friday – Theme “Speak Up, Listen Up, Flow UP & Learning”
• Introduction - FTSU Guardian 5/60
• Story 1 – Director of Estates & Facilities 10-15/60
• Story 2 – COO 10-15/60 • Story 3 – Deputy CEO 10-15/60
FTSU Champion re questions.10/60
Cherma SW TB JS (DNA) M&L
THHFT Board PUBLIC 02 Nov 2021 Page 157 of 225

FTSU Guardian – Closing remarks 5/60 Pledges-10/60
Cherma SW, JS, TB
WB 18th October BH Activities
Thursday 21st October 12.30 to 13.30 hours
Storytelling Friday – Theme “Proud to be”
• Introduction 5/60 • Workers journey 15/60 • External Speaker Via pre recorded
video 10-15 • Worker’s journey 15/60 • Intros and presence 10/60 • Closing remarks 5/60
Danny Robert Prof J.D-B. OBE DL Discussion Cherma
WB 25th October FTSU Activities
Thursday 28th October 13.30 – 2.30 hours
Storytelling Friday Theme “Speak up, Listen up, Follow up” & Learning
• Introduction 5/60 • CEO – 10/60 • FTSU Champions 10/60 • HR Relations case 10/60 • Medical Director – 10/60 • Closing remarks 5/60 • Pledges 10/60
Cherma PW MM GA NK Cherma PW, GA, MV
Friday 29th October 12.30 – 13.30
Closing events- Music African / Caribbean music 60/60
Guest
THHFT Board PUBLIC 02 Nov 2021 Page 158 of 225

Page 1 of 2
Finance Report - Month 6
THHFT Board meeting - Public
Date of the meeting: 02 November 2021 ITEM: 12 Purpose of the Report/Paper: To provide the Trust Board with an update on Trust’s financial position as at Month 6. For: Information Assurance Discussion and input Decision/approval Executive summary: The month 6 position was a deficit of £1.6m, against the breakeven plan. The year to date position is an adverse variance of £6.1m. In month, a 3% pay increase has been awarded to all staff groups except doctors in training, with the increase and the back pay to April being paid. This has increased pay costs in month by £2.4m. As per guidance, the impact on the position has been neutralised with an equal and opposite income accrual of £2.4m. The key driver of the year to date variance is pay costs which, at £103m, are £8.2m adverse to plan. This includes £2.4m for the pay award which was not in the plan. Adjusting for the impact of the pay award in month 6, the year to date variance is £5.8m adverse to plan. Pay costs were £19.6m in month, of which £2.4m was due to the pay award. The underlying pay position is similar to that in August, but pay costs have increased by £0.75m since May. The main drivers of this variance continue to be undelivered TIP (£2.1m), increases in nursing agency premiums (£1.0m), high use of RMNs (£0.6m), costs of running the vaccination centres (£0.6m), Hayes escalation ward (£0.4m), and pressures in Critical Care (£0.8m) from additional beds and staff sickness. Non-Pay spend year to date of £44m is £2.4m adverse to plan. This includes £1.2m of undelivered TIP. Year to date, Drugs are now £0.7m adverse to plan, despite the activity delivered being significantly below the budgeted level. Clinical Supplies & Services are close to plan. The year to date adverse variance is largely driven by Other Operating Expenses, which is £1.4m adverse. Within this the main variances other than TIP are from Patient Transport (£0.13m) which is driven by Covid-19 social distancing guidance, Recruitment Expenses for the international nurse recruitment programme (£0.2m), bad debts provision movements (£0.2m) and IT costs (£0.16m). Income is £4.2m favourable year to date, of which £2.4m relates to the pay award. A further £0.6m is due to Elective Recovery Funding earned for activity in months 1-3, however the increased thresholds means that no further income from this source is expected. In addition income for staffing the vaccination centres accounts for a further £0.6m. The plan has an overall TIP target of £10.3m for 2021-22 (£5.1m in H1). This is made up of a combination of 2% in-year target (£5.8m), £2.0m carried forward from 2020-21 and a Vacancy Management Factor of £2.5m. The year to date delivery of £1.7m is £3.4m behind plan. The report outlines the actions the Trust is taking to address the key drivers of the adverse financial position.
THHFT Board PUBLIC 02 Nov 2021 Page 159 of 225
Page 2 of 2
The Trust has spent £9.2m of Capital at the end of September 2021, against a plan of £30.7m for the same period. Much of this £21m underspend relates to HIP2 schemes (approximately £13m), where there has been slippage on original plans with some of the planned expenditure now not expected until 2022/23. A reforecast exercise has been undertaken, this has reduced forecast expenditure in Estates by £7.5m. The other areas where there is significant underspend is the Digital Care Record project £2.5m, Fire remediation £2.6m and the Salix project £1.8m. Project managers are reporting back to Finance that all of these projects will be completed by the end of the financial year. Sponsor: Jon Bell, Chief Financial Officer Author: Stephen Jones, Deputy Director
of Finance Author contact details:
Risk implications – Link to Board Assurance Framework or Corporate Risk Register:
BAF Risks 3.1 – 3.6
Legal/Regulatory/Finance/Quality & Safety/ HR/E&D/Engagement/Communications/Reputation or Sustainability implications:
Finance
Link to Relevant CQC Domain: Safe Effective Caring Responsive Well Led Link to relevant Corporate Objectives/strategic aims:
Money – we will live within our means
Document previously considered by: Finance & Performance Committee
Recommendations: The paper is for information and discussion by the Trust Board.
THHFT Board PUBLIC 02 Nov 2021 Page 160 of 225

Contents
1. Summary of Month 6 Financial Position: Income & Expenditure position Financial Headlines Pay, Non-Pay & WTE Trend Reports Divisional Summary Overall TIP Position
1. Financial reporting: Balance sheet Debtors & Creditors Cash flow Capital Report
2. Appendices: Activity and income report
1THHFT Board PUBLIC 02 Nov 2021 Page 161 of 225

Summary of Month 6 Financial Position
2
H1 Plan Actual Variance Plan Actual VariancePlan In Month In Month In Month to-date to-date to-date£m £m £m £m £m £m £m
Operating IncomeNHS Clinical Income 133.12 22.24 24.67 2.43 133.12 136.80 3.67Non-NHS Clinical Income 1.30 0.22 0.28 0.06 1.30 1.35 0.06Other Operating Income 10.58 1.76 1.94 0.17 10.58 11.08 0.50Total Operating Income 145.00 24.22 26.89 2.67 145.00 149.22 4.23Medical Pay (26.14) (4.36) (5.20) (0.84) (26.14) (27.84) (1.70)Nursing Pay (30.61) (5.13) (6.55) (1.42) (30.61) (33.63) (3.01)HCAs & Other Support Staff Pay (10.83) (1.81) (2.46) (0.66) (10.83) (12.44) (1.61)Other Staff Pay (26.90) (4.48) (5.44) (0.96) (26.90) (28.76) (1.86)Employee Expenses (94.49) (15.77) (19.64) (3.87) (94.49) (102.67) (8.18)Drugs - PbR Excluded (5.55) (0.92) (1.07) (0.14) (5.55) (5.79) (0.24)Drugs - In Tariff (2.83) (0.47) (0.58) (0.11) (2.83) (3.32) (0.49)Clinical Supplies and Services (12.85) (2.14) (2.21) (0.07) (12.85) (13.14) (0.29)Other Operating Expenses (20.32) (3.42) (3.57) (0.16) (20.32) (21.70) (1.38)Total Non-Pay (41.55) (6.95) (7.43) (0.48) (41.55) (43.95) (2.40)Total Operating Expenses (136.04) (22.72) (27.07) (4.35) (136.04) (146.62) (10.58)EBITDA 8.96 1.50 (0.19) (1.69) 8.96 2.60 (6.35)Depreciation (4.97) (0.83) (0.84) (0.01) (4.97) (5.03) (0.06)Interest Income/Expense (1.25) (0.21) (0.12) 0.09 (1.25) (0.92) 0.33PDC Dividend Expense (2.75) (0.46) (0.46) (0.00) (2.75) (2.75) (0.00)
Surplus(Deficit) before Exceptionals (0.00) 0.01 (1.60) (1.61) (0.00) (6.09) (6.09)Financial Recovery Fund 0.00 0.00 0.00 0.00 0.00 0.00 0.00Surplus(Deficit) after Exceptionals (0.00) 0.01 (1.60) (1.61) (0.00) (6.09) (6.09)
( ) variance indicates it is adverseTHHFT Board PUBLIC 02 Nov 2021 Page 162 of 225
Month 6 Financial Headlines
Overview• The Trust has submitted a breakeven H1 plan to NHSIE.• The month 6 position was a deficit of £1.6m, against the breakeven plan. The year to date position is an adverse variance of
£6.1m.• In month, a 3% pay increase has been awarded to all staff groups except doctors in training, with the increase and the back
pay to April being paid. This has increased pay costs in month by £2.4m. As per guidance, the impact on the position has been neutralised with an equal and opposite income accrual of £2.4m.
• The majority of the year to date variance is on pay - £8.2m year to date, however adjusting for the impact of the pay award gives an adverse variance of £5.8m. Non-pay is £2.4m adverse to plan. These adverse variances are offset by over-performance on ERF income of £0.6m, and pay award income of £2.4m, with income overall favourable to plan by £4.2m.
Income• NHS Clinical Income is better than plan by £3.7m year to date. In month there is a favourable variance of £2.4m, this is
because, as per guidance, income equal to the cost of the pay award paid in month has been accrued. Year to date ERF is giving a favourable variance of £0.6m. No ERF income was earned in the period as the threshold to earn ERF was increased to 95%.
• A further £0.6m is due to funding for the vaccination centre - this is offset in pay. • ERF income of £2.3m was reported YTD, for activity in quarter one. The thresholds have been reviewed, and as a result, the
thresholds for earning ERF have been adjusted to 95% of 2019/20 activity levels from 1 July 2021. Month 6 activity and income was 84% against the threshold of 95%, therefore no further ERF income has been recorded for month 6.
• Non-NHS Clinical Income is favourable to plan in month (£0.1m) as high overseas visitor income in month more than offset the adverse variance on ICR income.
• Other Operating Income is favourable in month (£0.2m), with favourable variances on car parking and income for international nurse recruitment programme, however the latter is offset in non-pay.
3THHFT Board PUBLIC 02 Nov 2021 Page 163 of 225
Pay• Pay is £8.2m adverse to plan year to date, and £3.9m adverse in month. Adjusting for the impact of the pay award in
month 6, these become £5.8m adverse to plan year to date, and £1.5m adverse in month. Pay costs were £19.6m in month, of which £2.4m was due to the pay award. The underlying pay position is similar to that in August, but pay costs have increased by £0.75m since May. The main drivers of this variance are:– Undelivered TIP £2.1m: Further to Financial Recovery Board, an Executive led group will review pay costs with the
aim of reducing the pay run-rate. In addition the savings scheme relating to the commercial arrangements for bank and agency spend is completed and in review.
– Pressures in Critical Care, which is in its new location in Seacole Building, where there are 16 beds spaces available. There were 29 out of the 30 days in September (up from 28/31 in August) when more than the 9 funded beds were open. The new layout includes a mix of single and double rooms, and depending on the number of HDU patients, their bed location and the mix of Covid and non-Covid patients, it is necessary to move the nursing of HDU patients to a 1:1 ratio, instead of the usual 2:1. In addition staff sickness in September was 13%. These factors have combined to give a year to date pay overspend of £1.38m, of which £0.54m is the increased agency premium.
– Increase in agency premium due to the significant number of nursing shifts going to off-framework agencies. This is estimated to have increased cost by £1.0m year to date. Measures introduced in August to reduced agency rates have had some success, with the average rate being lower than in August, and total agency nursing spend reducing despite the small increase in WTEs. The additional cost of off-framework and over-cap agency shifts, as compared to bank rates, has been £2.5m year to date.
– In September agency nurse WTEs increased by 4 to 137, from the already high level seen in August. Substantive WTEs were down by 10, and bank WTEs down by 2, giving a net reduction of 9 WTEs for qualified nursing staff. Substantive WTEs are down by 28 WTEs compared to May, which saw the highest number of substantive nursing staff in post.
Month 6 Financial Headlines
4THHFT Board PUBLIC 02 Nov 2021 Page 164 of 225

Pay (Cont.)– High use of RMNs, which are adverse to plan by £0.6m: There were 1,886 shifts in the period April to September 21,
compared to 604 in the same period in 2019. The cost increased from £0.23m to £0.83m. There has been a significant increase (£0.1m) in Alderbourne Ward during August & September due to the high acuity of two patients, one of whom needed 2:1 care. Whilst reducing, this will continue into October.
– Pay costs for the vaccination centres of £0.6m. This is offset in income.– Hayes Escalation ward shut on 20 September, but cost £0.1m in the month.– The Trust sickness rate has increased from an average of 4.0% for April to September 19/20, to 4.7% in the same period
in 21/22. Sickness increased from 4.9% in August to 5.4% in September, the highest rate this year.
Non-pay• The year to date position is an adverse variance of £2.4m. This includes £1.2m of undelivered TIP.• Year to date, Drugs are now £0.73m adverse to plan, despite the activity delivered being significantly below the budgeted level.
The Finance, Divisional and Pharmacy teams are working together to understand this variance better, but an initial review shows that increased activity in radiology in driving an adverse variance. In Medical Haematology, in response to NHSE commissioning guidelines, there has been a switch to more expensive oral medicines rather than admitting patients for intravenous medication.
• Clinical Supplies & Services are £0.3m adverse to plan, but this includes £0.4m of undelivered TIP.• The year to date adverse variance is largely driven by Other Operating Expenses, which is £1.4m adverse. Within this the main
variances are on undelivered TIP (£0.7m), Patient Transport (£0.13m) which is driven by Covid-19 social distancing guidance, Recruitment Expenses for the international nurse recruitment programme (£0.2m), bad debts provision movements (£0.2m) and IT costs (£0.16m). A review of maintenance costs identified £0.1m of costs that could be charged to capital, and this has brought this area of cost back in line with plan. The cost of the international recruitment programme is currently offset with income from NHSIE.
Month 6 Financial Headlines
5THHFT Board PUBLIC 02 Nov 2021 Page 165 of 225

TIP• The H1 plan includes a TIP target of £2.9m (2%) for 21/22. In addition there is £1m of undelivered TIP carried forward from
20/21 and a Vacancy Management target of £1.25m, a total efficiency requirement in H1 of £5.1m. This is phased equally across the months, giving an in-month target of £0.86m. Year to date delivery was £1.7m against a target of £5.1m, an adverse variance of £3.4m
Actions Being Taken To Address Key Drivers of Deficit To Plan
Income• NWL ICS will provide funding for the increased capacity required within our ICU however, details are still being worked through
and are not yet finalised.
Pay• Pay is the largest driver for the Trust’s adverse position (£5.8m adverse year to date excluding pay award).• A Workforce Run Rate committee has been established which reports into the Financial Recovery Board. Actions being taken to
reduce the level of agency spend include:– Working with NHSEI to optimise our use of Healthroster– Review of establishments, ESR and Rosters to ensure alignment– Increased scrutiny of off-framework requests to reduce the number going off-framework– On-going international recruitment– Targeted bank recruitment for ITU– Guaranteed job scheme for nursing & midwifery students– RMN shifts being pro-actively booked with framework agencies to avoid going off-framework at the last minute & there is
on-going recruitment of RMNs to our bank
Month 6 Financial Headlines
6THHFT Board PUBLIC 02 Nov 2021 Page 166 of 225

Actions Being Taken To Address Key Drivers of Deficit (cont.)
Non Pay• A group has been established which is chaired by the Deputy CEO on a monthly basis which reviews all budget overspends
with budget managers and finance to understand and where possible tackle the underlying causes.
• The Trust has also established a Grip and Control Task and Finish group which reports into the Financial Improvement Working Group which is reviewing control measures across all areas within the Trust including income, costs, cash, workforce, estatesand capital.
TIP• TIP progress is reported at the Financial Recovery Board and divisions are being challenged to identify mitigations for schemes
which are not delivering to plan.• The Recovery Support Team are carrying out a review of the PMO function within the Trust and their findings will be reported
through the appropriate committee when finalised. Additional finance resource is being provided on a non-recurrent basis pending the outcome of that review.
Month 6 Financial Headlines
7THHFT Board PUBLIC 02 Nov 2021 Page 167 of 225

Pay and WTE Trends
8
These graphs show the pay costs and WTEs since April 2019.
September pay has been adjusted to remove the impact of the pay award.
THHFT Board PUBLIC 02 Nov 2021 Page 168 of 225

Pay Expenditure Trend April 20 to September 21
• This report shows the actual pay expenditure run-rate.• There was significant increase in pay costs in September due to the pay award, backdated to April, being paid. The underlying
position is similar to the August position. The position on Nursing pay has improved slightly in month, with costs being lower by £0.1m, partly driven by lower WTEs (9 fewer WTEs) but also a reduction in the average agency rate since August.
• The pay run-rate for M1-6 of £16.7m (excluding pay award) is £0.9m above the 2019-20 & 2020-21 averages (£15.9m). However, the 2020-21 average pay run rate was lowered during the first wave of the pandemic in Q1 & Q2 as there was a step down in much of the elective activity, especially at the Hillingdon site which meant staff were re-assigned to provide sickness cover on wards.
• Pay rates started to increase from Q3 with the step up in elective activity and actually averaged £16.6m in Q4.• Although the numbers of Covid patients in the hospital are down considerably from the January peak there are still considerable
pressures driven by A&E attendances, bed occupancy and staff sickness cover. 9
Staff Group Apr-20 May-20 Jun-20 Jul-20 Aug-20 Sep-20 Oct-20 Nov-20 Dec-20 Jan-21 Feb-21 Mar-21 Apr-21 May-21 Jun-21 Jul-21 Aug-21 Sep-21 Trend Line£ms £ms £ms £ms £ms £ms £ms £ms £ms £ms £ms £ms £ms £ms £ms £ms £ms £ms £ms £ms £ms Apr20-Sep21
1.SubstantiveMedical Pay 3.70 3.91 3.81 3.92 3.73 3.64 3.62 3.72 3.80 3.70 3.73 3.78 3.54 44.91 3.84 3.67 3.63 3.67 3.68 4.18 22.67Nurses & Midwives Pay 3.98 4.08 4.30 4.35 4.26 4.21 4.28 4.23 4.25 4.25 4.28 4.25 4.17 50.92 4.25 4.20 4.28 4.26 4.18 4.93 26.09Hcas & Support Staff Pay 1.65 1.68 1.55 1.85 1.70 1.67 1.67 1.56 1.56 1.57 1.59 1.63 1.61 19.65 1.67 1.68 1.68 1.72 1.72 2.08 10.55Other Staff Pay 4.09 4.05 4.20 4.23 4.12 4.25 4.15 4.08 4.11 4.15 4.11 4.13 4.04 49.63 4.13 4.02 4.01 4.08 4.14 4.81 25.181.Substantive Total 13.42 13.73 13.87 14.35 13.82 13.77 13.73 13.58 13.72 13.67 13.71 13.80 13.37 165.11 13.88 13.57 13.60 13.72 13.72 16.00 84.49
2.BankMedical Pay 0.56 0.42 0.37 0.48 0.52 0.46 0.69 0.58 0.51 0.66 0.21 0.48 0.53 5.91 0.55 0.51 0.48 0.58 0.50 0.62 3.24Nurses & Midwives Pay 0.46 0.30 0.20 0.14 0.18 0.29 0.34 0.39 0.52 0.49 0.63 0.63 0.69 4.78 0.49 0.52 0.53 0.51 0.54 0.59 3.19Hcas & Support Staff Pay 0.27 0.17 0.08 0.07 0.07 0.14 0.17 0.18 0.29 0.26 0.29 0.26 0.31 2.30 0.25 0.24 0.26 0.25 0.29 0.33 1.62Other Staff Pay 0.29 0.27 0.21 0.25 0.24 0.21 0.24 0.29 0.32 0.34 0.36 0.35 0.45 3.54 0.35 0.32 0.40 0.39 0.35 0.42 2.232.Bank Total 1.59 1.17 0.87 0.93 1.02 1.10 1.43 1.44 1.64 1.74 1.50 1.72 1.98 16.53 1.64 1.59 1.67 1.73 1.68 1.96 10.28
3.AgencyMedical Pay 0.24 0.15 0.16 0.13 0.20 0.20 0.27 0.29 0.26 0.12 0.31 0.27 0.33 2.70 0.26 0.24 0.30 0.39 0.34 0.40 1.94Nurses & Midwives Pay 0.39 0.19 0.03 0.02 0.02 0.02 0.10 0.11 0.14 0.25 0.58 0.62 0.71 2.80 0.47 0.40 0.57 0.78 1.11 1.02 4.35Hcas & Support Staff Pay 0.04 0.07 0.07 0.03 0.09 0.04 0.04 0.07 0.06 0.03 0.10 0.07 0.08 0.75 0.03 0.07 0.02 0.04 0.05 0.05 0.27Other Staff Pay 0.15 0.14 0.11 0.13 0.18 0.17 0.19 0.22 0.27 0.23 0.24 0.22 0.26 2.37 0.25 0.26 0.25 0.24 0.14 0.21 1.353.Agency Total 0.83 0.56 0.37 0.31 0.49 0.43 0.61 0.69 0.73 0.63 1.23 1.18 1.38 8.62 1.01 0.97 1.15 1.46 1.65 1.68 7.91Grand Total 15.84 15.46 15.11 15.59 15.33 15.31 15.77 15.71 16.09 16.04 16.44 16.70 16.72 190.26 16.53 16.13 16.42 16.91 17.05 19.64 102.67
Total Medical Pay 4.51 4.48 4.35 4.53 4.46 4.31 4.58 4.59 4.57 4.47 4.26 4.54 4.39 53.52 4.65 4.42 4.41 4.64 4.52 5.20 27.84Total Nurses & Midwives Pay 4.83 4.58 4.53 4.50 4.46 4.51 4.72 4.73 4.91 4.99 5.48 5.50 5.57 58.50 5.20 5.12 5.38 5.55 5.82 6.55 33.63Total Hcas & Support Pay 1.97 1.93 1.69 1.96 1.86 1.85 1.89 1.81 1.90 1.86 1.99 1.95 2.00 22.69 1.94 1.98 1.97 2.02 2.07 2.46 12.44Total Other Staff Pay 4.53 4.47 4.53 4.60 4.54 4.64 4.58 4.59 4.70 4.72 4.71 4.71 4.75 55.54 4.73 4.60 4.66 4.71 4.64 5.44 28.77Grand Total 15.84 15.46 15.11 15.59 15.33 15.31 15.77 15.71 16.09 16.04 16.44 16.70 16.72 190.26 16.53 16.13 16.42 16.91 17.05 19.64 102.67
2021-22 Total
2020-21 2020-21 Total
2019-20 Average (Inflated)
2021-22
THHFT Board PUBLIC 02 Nov 2021 Page 169 of 225
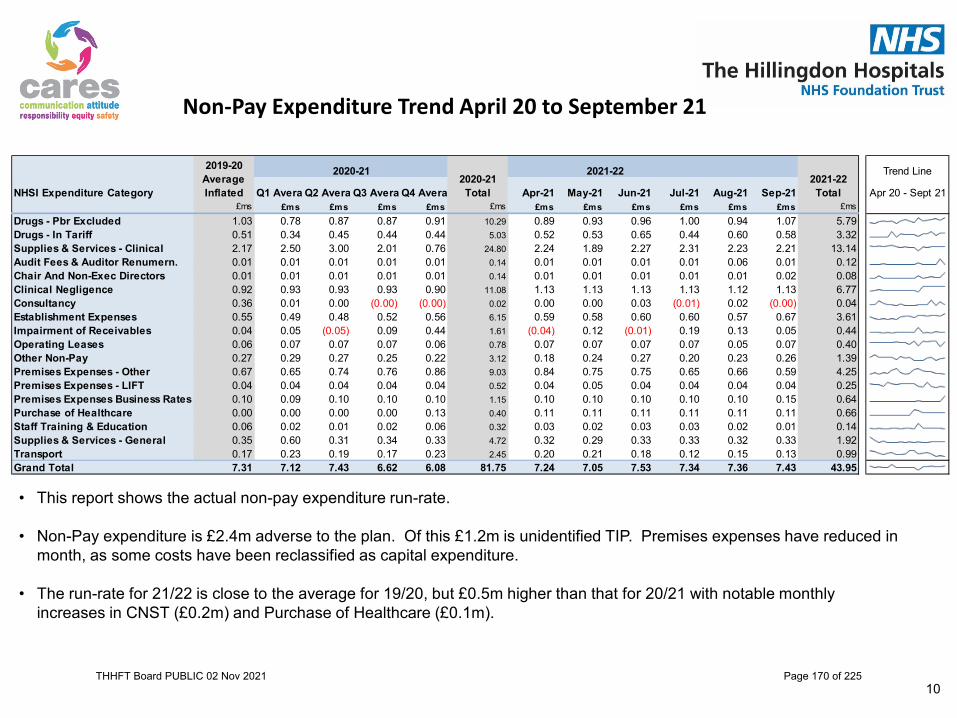
Non-Pay Expenditure Trend April 20 to September 21
• This report shows the actual non-pay expenditure run-rate.
• Non-Pay expenditure is £2.4m adverse to the plan. Of this £1.2m is unidentified TIP. Premises expenses have reduced in month, as some costs have been reclassified as capital expenditure.
• The run-rate for 21/22 is close to the average for 19/20, but £0.5m higher than that for 20/21 with notable monthly increases in CNST (£0.2m) and Purchase of Healthcare (£0.1m).
10
Trend Line
NHSI Expenditure Category Q1 Avera Q2 Avera Q3 Avera Q4 Avera Apr-21 May-21 Jun-21 Jul-21 Aug-21 Sep-21 Apr 20 - Sept 21£ms £ms £ms £ms £ms £ms £ms £ms £ms £ms £ms £ms £ms
Drugs - Pbr Excluded 1.03 0.78 0.87 0.87 0.91 10.29 0.89 0.93 0.96 1.00 0.94 1.07 5.79Drugs - In Tariff 0.51 0.34 0.45 0.44 0.44 5.03 0.52 0.53 0.65 0.44 0.60 0.58 3.32Supplies & Services - Clinical 2.17 2.50 3.00 2.01 0.76 24.80 2.24 1.89 2.27 2.31 2.23 2.21 13.14Audit Fees & Auditor Renumern. 0.01 0.01 0.01 0.01 0.01 0.14 0.01 0.01 0.01 0.01 0.06 0.01 0.12Chair And Non-Exec Directors 0.01 0.01 0.01 0.01 0.01 0.14 0.01 0.01 0.01 0.01 0.01 0.02 0.08Clinical Negligence 0.92 0.93 0.93 0.93 0.90 11.08 1.13 1.13 1.13 1.13 1.12 1.13 6.77Consultancy 0.36 0.01 0.00 (0.00) (0.00) 0.02 0.00 0.00 0.03 (0.01) 0.02 (0.00) 0.04Establishment Expenses 0.55 0.49 0.48 0.52 0.56 6.15 0.59 0.58 0.60 0.60 0.57 0.67 3.61Impairment of Receivables 0.04 0.05 (0.05) 0.09 0.44 1.61 (0.04) 0.12 (0.01) 0.19 0.13 0.05 0.44Operating Leases 0.06 0.07 0.07 0.07 0.06 0.78 0.07 0.07 0.07 0.07 0.05 0.07 0.40Other Non-Pay 0.27 0.29 0.27 0.25 0.22 3.12 0.18 0.24 0.27 0.20 0.23 0.26 1.39Premises Expenses - Other 0.67 0.65 0.74 0.76 0.86 9.03 0.84 0.75 0.75 0.65 0.66 0.59 4.25Premises Expenses - LIFT 0.04 0.04 0.04 0.04 0.04 0.52 0.04 0.05 0.04 0.04 0.04 0.04 0.25Premises Expenses Business Rates 0.10 0.09 0.10 0.10 0.10 1.15 0.10 0.10 0.10 0.10 0.10 0.15 0.64Purchase of Healthcare 0.00 0.00 0.00 0.00 0.13 0.40 0.11 0.11 0.11 0.11 0.11 0.11 0.66Staff Training & Education 0.06 0.02 0.01 0.02 0.06 0.32 0.03 0.02 0.03 0.03 0.02 0.01 0.14Supplies & Services - General 0.35 0.60 0.31 0.34 0.33 4.72 0.32 0.29 0.33 0.33 0.32 0.33 1.92Transport 0.17 0.23 0.19 0.17 0.23 2.45 0.20 0.21 0.18 0.12 0.15 0.13 0.99Grand Total 7.31 7.12 7.43 6.62 6.08 81.75 7.24 7.05 7.53 7.34 7.36 7.43 43.95
2020-21 Total
2021-22 Total
2020-212019-20 Average Inflated
2021-22
THHFT Board PUBLIC 02 Nov 2021 Page 170 of 225
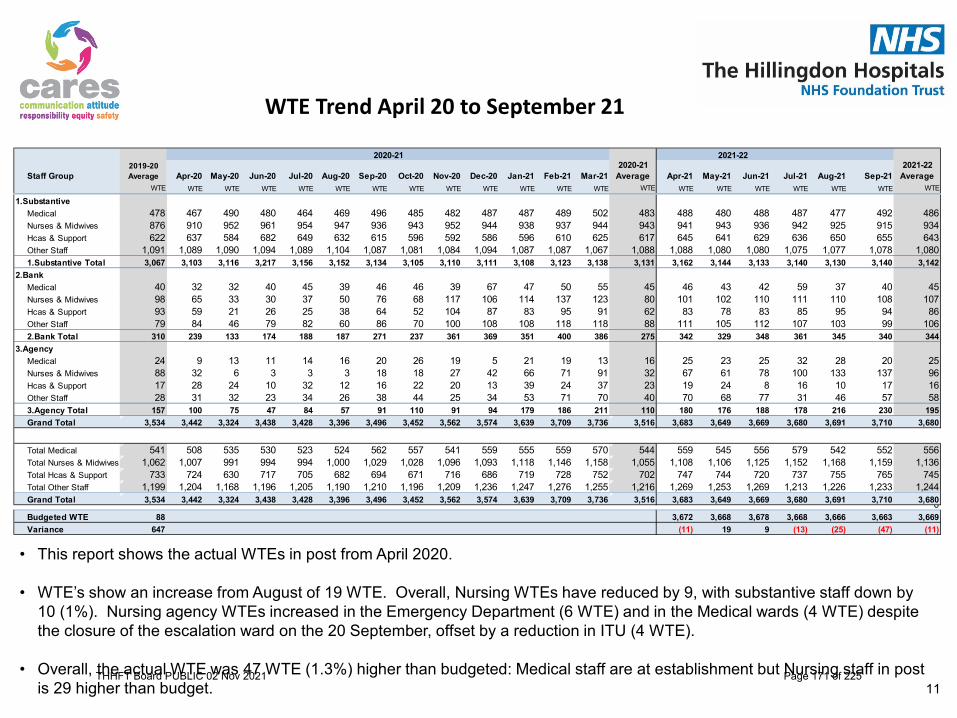
WTE Trend April 20 to September 21
• This report shows the actual WTEs in post from April 2020.
• WTE’s show an increase from August of 19 WTE. Overall, Nursing WTEs have reduced by 9, with substantive staff down by 10 (1%). Nursing agency WTEs increased in the Emergency Department (6 WTE) and in the Medical wards (4 WTE) despite the closure of the escalation ward on the 20 September, offset by a reduction in ITU (4 WTE).
• Overall, the actual WTE was 47 WTE (1.3%) higher than budgeted: Medical staff are at establishment but Nursing staff in post is 29 higher than budget. 11
Staff Group Apr-20 May-20 Jun-20 Jul-20 Aug-20 Sep-20 Oct-20 Nov-20 Dec-20 Jan-21 Feb-21 Mar-21 Apr-21 May-21 Jun-21 Jul-21 Aug-21 Sep-21WTE WTE WTE WTE WTE WTE WTE WTE WTE WTE WTE WTE WTE WTE WTE WTE WTE WTE WTE WTE WTE
1.SubstantiveMedical 478 467 490 480 464 469 496 485 482 487 487 489 502 483 488 480 488 487 477 492 486Nurses & Midwives 876 910 952 961 954 947 936 943 952 944 938 937 944 943 941 943 936 942 925 915 934Hcas & Support 622 637 584 682 649 632 615 596 592 586 596 610 625 617 645 641 629 636 650 655 643Other Staff 1,091 1,089 1,090 1,094 1,089 1,104 1,087 1,081 1,084 1,094 1,087 1,087 1,067 1,088 1,088 1,080 1,080 1,075 1,077 1,078 1,0801.Substantive Total 3,067 3,103 3,116 3,217 3,156 3,152 3,134 3,105 3,110 3,111 3,108 3,123 3,138 3,131 3,162 3,144 3,133 3,140 3,130 3,140 3,142
2.BankMedical 40 32 32 40 45 39 46 46 39 67 47 50 55 45 46 43 42 59 37 40 45Nurses & Midwives 98 65 33 30 37 50 76 68 117 106 114 137 123 80 101 102 110 111 110 108 107Hcas & Support 93 59 21 26 25 38 64 52 104 87 83 95 91 62 83 78 83 85 95 94 86Other Staff 79 84 46 79 82 60 86 70 100 108 108 118 118 88 111 105 112 107 103 99 1062.Bank Total 310 239 133 174 188 187 271 237 361 369 351 400 386 275 342 329 348 361 345 340 344
3.AgencyMedical 24 9 13 11 14 16 20 26 19 5 21 19 13 16 25 23 25 32 28 20 25Nurses & Midwives 88 32 6 3 3 3 18 18 27 42 66 71 91 32 67 61 78 100 133 137 96Hcas & Support 17 28 24 10 32 12 16 22 20 13 39 24 37 23 19 24 8 16 10 17 16Other Staff 28 31 32 23 34 26 38 44 25 34 53 71 70 40 70 68 77 31 46 57 583.Agency Total 157 100 75 47 84 57 91 110 91 94 179 186 211 110 180 176 188 178 216 230 195Grand Total 3,534 3,442 3,324 3,438 3,428 3,396 3,496 3,452 3,562 3,574 3,639 3,709 3,736 3,516 3,683 3,649 3,669 3,680 3,691 3,710 3,680
Total Medical 541 508 535 530 523 524 562 557 541 559 555 559 570 544 559 545 556 579 542 552 556Total Nurses & Midwives 1,062 1,007 991 994 994 1,000 1,029 1,028 1,096 1,093 1,118 1,146 1,158 1,055 1,108 1,106 1,125 1,152 1,168 1,159 1,136Total Hcas & Support 733 724 630 717 705 682 694 671 716 686 719 728 752 702 747 744 720 737 755 765 745Total Other Staff 1,199 1,204 1,168 1,196 1,205 1,190 1,210 1,196 1,209 1,236 1,247 1,276 1,255 1,216 1,269 1,253 1,269 1,213 1,226 1,233 1,244Grand Total 3,534 3,442 3,324 3,438 3,428 3,396 3,496 3,452 3,562 3,574 3,639 3,709 3,736 3,516 3,683 3,649 3,669 3,680 3,691 3,710 3,6800Budgeted WTE 88 3,672 3,668 3,678 3,668 3,666 3,663 3,669Variance 647 (11) 19 9 (13) (25) (47) (11)
2021-22 Average
2019-20 Average
2020-21 Average
2020-21 2021-22
THHFT Board PUBLIC 02 Nov 2021 Page 171 of 225

Divisional Summary
12
1. Planned Care is reporting an adverse variance of £0.94m compared to plan. The pressure on pay from Critical Care has increased this month due to more beds being occupied and non-pay is high to clear backlog of patients.
2. Unplanned Care is reporting an adverse variance to plan of £1.64m. Pay is adverse to plan by £1.32m, with overspends on medical, nursing & HCA pay. The escalation ward was open for 3 weeks. Pressure from escalated rates and sickness continue.
3. The Corporate Division is adverse to plan by £0.17m. There are pressures on pay from agency staff, and non-pay from IT costs and recruitment expenses.
4. Central Budgets show a favourable variance of £1.14m. NHS Clinical Income includes £2.4m for the pay award. The pay budget & variance is unusual –this is a result of funding the divisions for the pay award, as this is not in our plan (as per guidance).THHFT Board PUBLIC 02 Nov 2021 Page 172 of 225

• The H1 plan for 2021/22 includes a TIP target of £5.1m.• The tables below show the Month 6 position. This month, schemes that improve the run-rate but which are not TIPs have
been shown separately.• In month 6 delivery was £0.39m against a target of £0.86m, an adverse variance of £0.46m.
Transformation Improvement Programme
13
Divisional Schemes Plan Actual Variance Plan Actual Variance Plan Actual VariancePlanned Care 76 26 (50) 261 56 (205) 733 177 (556)Unplanned Care 47 6 (41) 145 57 (88) 503 452 (51)Corporate 185 156 (29) 709 644 (65) 1,870 1,796 (74)
Total Divisional 308 188 (120) 1,115 757 (358) 3,106 2,424 (682)
Transformational Schemes Plan Actual Variance Plan Actual Variance Plan Actual VariancePeople and OD 81 21 (60) 367 127 (240) 855 615 (240)Procurement 111 77 (34) 319 173 (146) 987 1,008 21Improving Models of Care 141 0 (141) 281 0 (281) 1,125 0 (1,125)ICS Collaboration 0 0 0 0 0 0 0 0 0Total Transformational 333 99 (235) 967 301 (667) 2,967 1,623 (1,344)
Vacancy Factor Plan Actual Variance Plan Actual Variance Plan Actual VariancePlanned Care 91 38 (53) 548 396 (152) 1,095 868 (227)Unplanned Care 76 35 (40) 455 125 (329) 909 216 (693)Corporate 41 31 (10) 248 156 (92) 496 404 (92)
Total Vacancy Factor 208 105 (104) 1,250 677 (573) 2,500 1,489 (1,011)
Trust Total TIP Schemes 850 391 (459) 3,332 1,734 (1,598) 8,573 5,536 (3,037)
Actual versus Target 856 391 (464) 5,135 1,734 (3,400) 10,269 5,536 (4,733)
Unidentified TIP (Gap) 6 0 (6) 1,802 0 (1,802) 1,696 0 (1,696)
Run Rate Plan Actual Variance Plan Actual Variance Plan Actual VarianceRun Rate 81 71 (10) 325 238 (87) 813 805 (7)Total Run Rate Schemes 81 71 (10) 325 238 (87) 813 805 (7)
Plan - TIP schemes identified/developedTarget - TIP in the operating plan and budget
In Month £000s Year To Date £000s Forecast Outturn £000s
In Month £000s Year To Date £000s Forecast Outturn £000s
In Month £000s Year To Date £000s Forecast Outturn £000s
Performance - Scheme Plans versus Actual Delivery
In Month £000s Year To Date £000s Forecast Outturn £000s
THHFT Board PUBLIC 02 Nov 2021 Page 173 of 225

Financial Reporting
31THHFT Board PUBLIC 02 Nov 2021 Page 174 of 225

Balance Sheet as at 30 September 2021
32
Key ratios M6
Month 6 commentary on significant movements
The significant movements on the balance sheet between years are as follows: • Cash and cash equivalents has decreased
by £14m between August and September. This resulted from significant outflows on capital creditors (c. £7m), PDC dividends (£3m). As stated elsewhere in the pack, the Trust paid the backdated pay award to all staff in September, which resulted in a payroll run £1.4m higher than any other month this financial year.
• In the year to date, creditors have fallen by over £20m in line with the decline in cash.
Current month Prior monthCurrent ratio 0.80 0.89Quick ratio 0.72 0.81Cash / liquidity ratio 0.32 0.48
31-Mar-21 30-Sep-21 MovementActual Actual Actual
£m £m £mNon-Current Assets
Intangible Assets 7.76 7.52 (0.24)Plant, Property and Equipment (Owned) 207.98 212.55 4.57Investment Property 49.86 49.86 0.00Prepayments 0.81 0.81 0.00Trade and other receivables 0.65 0.59 (0.06)
Total Non-Current Assets 267.06 271.33 4.27
Current AssetsInventories 4.67 4.78 0.11NHS Trade Receivables 16.69 12.61 (4.09)Non-NHS Trade Receivables 4.40 3.62 (0.78)Prepayments and Accrued Income 4.49 7.16 2.67Cash and Cash Equivalents 47.40 18.45 (28.96)
Total Current Assets 77.65 46.61 (31.04)Total Assets 344.71 317.94 (26.77)Current Liabilities
Trade Payables 3.11 (2.66) (5.77)Capital Payables 33.51 12.60 (20.91)Other Payables 11.02 11.88 0.87Accruals and Deferred Income 26.03 27.34 1.32Provisions 0.16 0.16 0.00Other Liabilities 2.84 7.33 4.50Financing <1 year 1.24 1.40 0.16Capital Investment Loans 0.40 0.40 0.00Working Capital Loan 0.00 0.00 0LIFT 0.29 0.29 0.00Finance Leases 0.55 0.71 0.16
Net Current Assets/(Liabilities) (0.24) (11.43) (11.20)Total Assets Less Current Liabilities 266.82 259.89 (6.93)Non-Current Liabilities (amounts falling due after more than one year)
Provisions 1.67 1.61 (0.06)Financing > 1 year 15.86 15.25 (0.61)Capital Investment Loans 3.96 3.76 (0.19)Deficit Support Loans 0.00 0.00 0.00LIFT Contract 10.92 10.77 (0.15)Finance Leases 0.98 0.72 (0.26)
Total Assets Employed 249.30 243.03 (6.26)
Taxpayers EquityPublic Dividend Capital 247.72 247.72 0.00Retained Earnings (51.55) (57.82) (6.26)Revaluation Reserve 53.13 53.13 0.00
Total Taxpayers' Equity 249.30 243.03 (6.26)THHFT Board PUBLIC 02 Nov 2021 Page 175 of 225

Debtors and Creditors as at 30 September 2021
33
The analysis shows ageing of the Trust's outstanding creditors at the end of September 2021. It is noticeable that creditors are ageing, and the Trust is taking urgent action to clear these in line with the agenda on improving performance against the Better Payment Practice Code (BPPC) target. More information on that is included on the next slide.
The analysis shows ageing of the Trust's outstanding debtor invoices at the end of September 2021 compared to August 2021. Overall system debt is £0.7m lower than in August. A key part of that movement was the write off of £759k of old debt in relation to the RAFT charity. This was approved by the Board in early October.
THHFT Board PUBLIC 02 Nov 2021 Page 176 of 225

Better Payment Practice Code (BPPC)
34
• The graph above shows the Trust’s performance against the BPPC target for the last 12 months, as well as forecast performance for the remaining months in 2021-22. The Trust is required to pay 95% of valid invoices within 30 days.
• The Trust is currently reporting 68%. In response to an urgent request from NHSEI to improve performance, the Trust is currently implementing a range of measures including the implementation of a no PO no pay policy and electronic invoice management software. We are also rolling out the receipting of purchase order items by end users. All of these will be implemented by the end of October and should start to have a positive impact on performance once these arrangements bed in. We are also taking other actions, such as focused effort on items about to breach the 30 day limit, and consistent use of disputes where invoices do not appear to be valid.
• As stated on the previous slide, the Trust is currently targeting the clearance of aged creditor balances. As shown in the graphabove, this may mean that performance deteriorates in the short term before improving after that.
THHFT Board PUBLIC 02 Nov 2021 Page 177 of 225

Cash Flow Forecast - September 2021
The analysis shows a rolling cash flow including forecasts up to the end of Mar 2022. Key points to note are: 1. At the end of September 2021, the Trust is holding £18.45m, down by £14m from August. As stated on the balance sheet slide, this was partly due to paying
significant capital creditors, PDC dividends and the impact of the pay award.2. The Trust’s cash forecast currently shows that the Trust is currently forecasting to have sufficient cash until m11, this is consistent with the previous month. This is an
improved position from that reported earlier in the year – this is due to updated assumptions around likely funding streams in H2. H2 forecasting is underway and we will update cash flow to ensure it is consistent with movements in the forecast financial position.
3. There is still uncertainty around the timing of receipts for year-end accruals for Annual Leave and Lost Income from NHSI (£1.5m and £2.7m). The Trust is working to resolve these uncertainties and develop mitigation actions should these receipts be further delayed. 35
Cash Flow Forecast 21-22 Cash flow forecast September 2021ACT ACT ACT ACT ACT ACT FCT FCT FCT FCT FCT FCT
Apr-21 May-21 Jun-21 Jul-21 Aug-21 Sep-21 Oct-21 Nov-21 Dec-21 Jan-22 Feb-22 Mar-22INCOME £000s £000s £000s £000s £000s £000s £000s £000s £000s £000s £000s £000s
Clinical Income 21.38 19.84 22.88 21.82 22.21 22.91 21.79 21.03 21.03 21.74 21.38 21.38 Education and Training 2.67 - - 1.64 0.19 - 2.03 - - 1.70 - - Other Income 0.95 6.38 0.28 0.82 1.39 1.74 4.70 1.12 1.16 1.09 1.09 1.92 Lost Income - - - - 3.48 - 1.92 - - - - - Annual Leave accrual - - 1.37 - - - 1.52 - - - - - HMRC - 1.45 0.47 - 2.18 - 0.88 0.60 0.60 0.60 0.60 0.60 STF - - - - - - - - - - - - ERF funding - - - - 1.45 - 0.84 - - - - - ICS Loan - - 4.00 2.98- 2.98 - 4.00- - - - - - Other Receipts 0.56 0.38 0.29 - 0.29 0.19 0.07 0.06 0.09 0.07 0.07 0.07 TOTAL RECEIPTS 25.56 28.05 29.31 21.31 34.15 24.83 29.75 22.81 22.88 25.20 23.14 23.98 PAYMENTSPay Costs 16.19- 15.84- 15.99- 16.30- 16.29- 17.67- 17.09- 15.99- 16.49- 15.99- 15.99- 15.99- Creditors 7.67- 13.42- 5.50- 8.55- 6.53- 9.56- 4.58- 7.00- 6.84- 6.84- 6.84- 6.84- Capital Creditors PDC 4.00- 15.36- 2.02- 0.49- 1.69- 6.50- 13.91- - - - - - Capital credtitors internally generated - 0.59- 0.93- 0.87- 0.73- 0.44- 2.52- 1.14- 1.14- 1.14- 0.77- - NHSLA 1.41- 1.41- 1.41- 1.41- 1.41- 1.41- 1.41- 1.41- 1.41- 1.41- - - PDC Dividends - - - - - 2.61- - - - - - 3.89- ITFF Loan Interest payments - - - - - 0.08- - - - - - 0.08- Loan Repayments - - - - - 0.20- - - - - - 0.20- Other Payments 0.00- 0.00- 0.00- 0.00- 0.00- 0.00- 0.02- - - - 0.02- 0.02- Total Payments 29.27- 46.61- 25.87- 27.62- 26.66- 38.48- 39.53- 25.55- 25.88- 25.38- 23.62- 27.02- NET CASH FLOW IN PERIOD 3.71- 18.56- 3.44 6.32- 7.49 13.64- 9.78- 2.73- 3.00- 0.18- 0.47- 3.04- OPENING CASH BALANCE 48.39 44.67 26.11 29.55 23.24 30.73 17.09 7.30 4.57 1.57 1.39 0.92
CLOSING CASH BALANCE 44.67 26.11 29.55 23.24 30.73 17.09 7.30 4.57 1.57 1.39 0.92 2.12-
Timing difference between statement & ledger RBS 0.01 0.00HSBC 0.72 0.92 1.24 1.28Petty cash 0.08 0.08 0.08 0.08Total cash Balance 30.35 24.24 32.05 18.45
THHFT Board PUBLIC 02 Nov 2021 Page 178 of 225

Capital Update and Month 6 Position
• The Trust has available capital funding of £57.2 million to fund its 2021/22 capital plan, and (as stated in month 1 capital report and other papers) has set a plan to spend £58.6 million against that available funding. This over commitment reflects the risks faced in each individual area (Estates, Medical Equipment, IT). The Trust has clearly communicated this risk to the ICS and expects that the over commitment will be funded through slippage in the wider ICS later in the financial year.
• The forecast spend is split by area as follows:– Estates £48.8m– IT £6.1m– Medical Equipment £3.7m
• The Trust has spent £9.2m at the end of September 2021, against a plan of £30.7m for the same period. The key reasons behind the underspend against plan are: – Much of this £21.5m underspend relates to HIP2 schemes (approximately £13m), where there has been slippage on
original plans with some of the planned expenditure now not expected until 2022/23. A reforecast exercise has been undertaken, this has reduced forecast expenditure in Estates by £7.5m. This has been presented and agreed at FPC.
– The other areas where there is significant underspend is the Digital Care Record project £2.5m, Fire remediation £2.6m and the Salix project £1.8m. Project managers are reporting back to Finance that all of these projects will be completed by the end of the financial year.
19THHFT Board PUBLIC 02 Nov 2021 Page 179 of 225
Month 6 Activity and Income Report
Appendix 1:
36THHFT Board PUBLIC 02 Nov 2021 Page 180 of 225

Trust Activity and Income Month 6 YTD
Income Commentary
• The Trust will receive block payments from 1 April 2021 to 30 September 2021. This is based on 2020/21 payments made in Qtr. 3 times 2, adjusted for any known changes or service developments. The focus is delivering a balanced plan for H1. There have been discussions relating to H2, and it is likely that block payments will continue.
• We will continue to review activity inline with our internal plan based on 2019/20 activity and top-up the divisions from the block payments to their respective plans for H1 (April 21 – September 21). The divisional top-ups to date are as follows:
• Unplanned Care Ytd £6.9m• Planned Care Ytd £5.3m
• The clinical income position for M6 is £1.2m above the Trust plan. The favourable variance relates to ERF over performance against the YTD plan of £960k, and the retrospective top-up of £634k. The block payment received for M6 of £21.3m has been fully recognized in the position, and £128.2m YTD.
• Elective Recovery Fund (ERF) is £2.23m YTD. The income is based on whole system (NWL) delivery. The plan for H1 is £1.3m. The gateway for further ERF achievement has been changed to 95% activity delivery, making any additional income from ERF maybe challenging. The £2.23m has been agreed with NWL, the divisional split has been estimated as the full data set has not been received from NHSE.
37THHFT Board PUBLIC 02 Nov 2021 Page 181 of 225

ERF - Month 6 YTD
38
Activity by POD70% 75% 80% 95% 95% 95%
POD Name 1 2 3 4 5 6 Grand Total 1 2 3 4 5 6 Grand Total 1 % 2 % 3 % 4 % 5 % 6 % Grand TotalDaycase 1,238 1,323 1,655 1,676 1,633 1,646 9,171 1,243 1,317 1,523 1,534 1,408 1,489 8,514 5 70% -6 75% -132 74% 0 78% 0 73% 0 77% -133 Elective 144 158 190 164 182 157 995 138 170 203 225 162 174 1,072 -6 67% 12 81% 13 86% 0 117% 0 76% 0 94% 19OP Procedures 3,589 3,901 4,927 5,091 4,753 5,154 27,415 4,335 3,969 4,472 4,132 3,926 4,386 25,220 746 85% 68 76% -455 73% 0 69% 0 70% 0 72% 358OP Attendances 12,870 13,430 16,462 17,527 14,862 17,776 92,927 16,074 16,324 18,394 17,226 15,694 18,370 102,082 3,204 87% 2,895 91% 1,932 89% 0 84% 0 90% 0 88% 8,030
Grand Total 17,842 18,812 23,234 24,458 21,430 24,732 130,509 21,790 21,780 24,592 23,117 21,190 24,419 136,888 3,948 85% 2,968 87% 1,358 85% 0 80% 0 84% 0 84% 8,274
Income by POD70% 75% 80% 95% 95% 95%
POD Name 1 2 3 4 5 6 Grand Total 1 2 3 4 5 6 Grand Total 1 % 2 % 3 % 4 % 5 % 6 % Grand TotalDaycase 1,026,751 1,148,780 1,430,014 1,507,405 1,378,250 1,387,366 7,878,565 1,057,232 1,133,834 1,445,510 1,337,712 1,153,364 1,203,282 7,330,936 30,481 72% -14,945 74% 15,497 81% 0 75% 0 71% -184,084 74% -153,050 Elective 661,963 688,922 757,111 692,923 823,108 629,581 4,253,607 543,427 912,895 909,256 956,016 676,238 783,714 4,781,546 -118,536 57% 223,973 99% 152,145 96% 0 117% 0 70% 154,134 106% 411,715OP Procedures 585,613 613,593 781,005 805,534 749,370 823,509 4,358,624 818,974 771,318 869,501 744,852 700,360 777,194 4,682,199 233,361 98% 157,725 94% 88,496 89% 0 79% 0 79% -46,315 80% 433,267OP Attendances 1,848,561 1,924,431 2,393,009 2,537,988 2,138,014 2,591,693 13,433,696 2,386,851 2,513,022 2,812,017 2,482,129 2,248,010 2,675,147 15,117,177 538,289 90% 588,591 98% 419,008 94% 0 83% 0 89% 83,454 88% 1,629,343
Grand Total 4,122,888 4,375,726 5,361,138 5,543,850 5,088,742 5,432,149 29,924,492 4,806,484 5,331,069 6,036,284 5,520,710 4,777,973 5,439,337 31,911,858 683,596 82% 955,344 91% 675,146 90% 0 85% 0 80% 7,189 85% 2,321,274
Threshold Actual Elective Recovery Fund ActivityYTD YTD
Threshold Actual Elective Recovery Fund ActivityYTDYTD
THHFT Board PUBLIC 02 Nov 2021 Page 182 of 225

Trust Activity and Income Month 6 YTD
39
Board Report PODIn Month
Plan Activity
In Month Actual
Activity
In Month Activity Variance
%In Month
Plan Income
In Month Actual Income
In Month Income
Variance%
YTD Plan Activity
YTD Actual
Activity
YTD Actual
Variance%
YTD Plan Income
YTD Actual Income
YTD Variance
%
A&EHillingdon A&E 6,059 5,851 -208 -3% 1,111,814 825,946 -285,868 -26% 34,700 33,510 -1,190 -3% 6,367,664 4,905,290 -1,462,374 -23%CDU 0 0 0 0% 212,611 212,611 0 0% 0 0 0 0% 1,217,679 1,217,679MIU 2,602 1,020 -1,582 -61% 199,698 87,188 -112,510 -56% 14,900 4,858 -10,042 -67% 1,143,726 415,255 -728,471 -64%
A&E Total 8,660 6,871 -1,789 -21% 1,524,123 1,125,745 -398,378 -26% 49,600 38,368 -11,232 -23% 8,729,068 6,538,224 -2,190,844 -25%Critical Care
Adult CC 448 361 -87 -19% 527,398 656,495 129,097 24% 2,568 2,876 308 12% 3,020,552 3,619,182 598,630 20%Neonatal 662 519 -143 -22% 341,743 289,013 -52,730 -15% 3,790 3,345 -445 -12% 1,957,255 1,803,945 -153,310 -8%
Critical Care Total 1,110 880 -230 -21% 869,141 945,508 76,367 9% 6,358 6,221 -137 -2% 4,977,808 5,423,127 445,320 9%Inpatients
Delivery 352 358 6 2% 1,159,519 1,270,038 110,519 10% 2,018 2,125 107 5% 6,640,880 7,626,166 985,286 15%Chemotherapy 131 100 -31 -23% 28,261 24,890 -3,371 -12% 749 639 -110 -15% 161,860 139,336 -22,524 -14%Daycase 2,036 1,582 -454 -22% 1,629,945 1,215,457 -414,488 -25% 11,661 9,143 -2,518 -22% 9,335,141 7,065,222 -2,269,919 -24%Elective 217 193 -24 -11% 829,413 790,594 -38,819 -5% 1,243 1,158 -85 -7% 4,750,273 4,571,390 -178,883 -4%Emergency 2,466 2,136 -330 -13% 4,603,689 3,596,866 -1,006,823 -22% 14,123 12,881 -1,242 -9% 26,366,582 22,452,655 -3,913,928 -15%Excess Beddays 732 623 -109 -15% 233,232 203,235 -29,997 -13% 4,194 4,038 -156 -4% 1,335,783 1,273,489 -62,295 -5%Ambulatory Care 1,056 1,436 380 36% 429,976 620,030 190,054 44% 6,048 7,429 1,381 23% 2,462,588 3,286,368 823,780 33%
Inpatients Total 6,990 6,428 -562 -8% 8,914,035 7,721,110 -1,192,925 -13% 40,035 37,413 -2,622 -7% 51,053,107 46,414,624 -4,638,483 -9%Other
Block 0 0 0 0% 322,336 322,336 0 0% 0 0 0 0% 1,877,208 1,877,208 0 0%Direct Access 8,673 6,697 -1,976 -23% 472,988 377,189 -95,799 -20% 49,674 36,505 -13,169 -27% 2,708,933 2,027,361 -681,573 -25%Operational Resilience 0 0 0 0% 246,938 246,938 0 0% 0 0 0 0% 1,481,628 1,481,628 0 0%Rehab Beddays 1,747 1,461 -286 -16% 566,589 497,608 -68,981 -12% 10,005 8,163 -1,842 -18% 3,245,011 2,813,321 -431,690 -13%Excluded Drugs 0 0 0 0% 961,402 987,674 26,273 3% 0 0 0 0% 5,768,410 5,926,047 157,637 3%Other 0 0 0 0% 2,812,536 678,423 -2,134,113 -76% 0 0 0 0% 22,891,511 3,503,026 -19,388,485 -85%Other Contract Income 0 0 0 0% -383,815 -383,815 0 0% 0 0 0 0% -2,302,891 -2,302,891 0 0%
Other Total 10,420 8,158 -2,262 -22% 4,998,974 2,726,354 -2,272,620 -45% 59,679 44,668 -15,011 -25% 35,669,811 15,325,700 -20,344,111 -57%CQUIN
CQUIN 0 0 0 0% 208,940 208,940 0 0% 0 0 0 0% 1,253,641 1,253,641 0 0%CQUIN Total 0 0 0 0% 208,940 208,940 0 0% 0 0 0 0% 1,253,641 1,253,641 0 0%Outpatients
Outpatients 40,147 37,454 -2,693 -7% 4,592,829 3,977,512 -615,317 -13% 229,931 215,905 -14,026 -6% 26,301,201 21,986,851 -4,314,351 -16%Community 1,508 794 -714 -47% 184,754 93,342 -91,412 -49% 8,634 4,729 -3,905 -45% 1,058,138 556,892 -501,246 -47%
Outpatients Total 41,654 38,248 -3,406 -8% 4,777,583 4,070,854 -706,729 -15% 238,565 220,634 -17,931 -8% 27,359,339 22,543,742 -4,815,597 -18%Income Earned Total 68,835 60,585 -8,250 -12% 21,292,796 16,798,510 -4,494,286 -21% 394,238 347,304 -46,934 -12% 129,042,774 97,499,059 -31,543,715 -24%
Divisional Top-up 0 0 0 0% 0 2,374,535 2,374,535 0% 0 0 0 0% 0 12,244,898 12,244,898 0%Block Adjustment 0 0 0 0% 0 2,455,441 3,022,077 0% 0 0 0 0% 0 18,964,055 18,964,055 0%Elective Recovery Fund 0 0 0 0% 496,000 40,590 -455,410 -92% 0 0 0 0% 1,354,000 2,314,086 960,086 71%Lost Income 0 0 0 0% 450,000 450,000 0 0% 0 0 0 0% 2,700,000 2,700,000 0 0%Retrospective Top-Up 0 0 0 0% 0 114,647 114,647 0% 0 0 0 0% 0 634,317 634,317 0%Pay Award Funding 0 0 0 0% 2,406,361 2,439,000 32,639 1% 0 0 0 0% 2,428,548 2,439,000 10,452 0%Other Income Total 0 0 0 0% 3,352,361 7,874,213 4,521,852 135% 0 0 0 0% 6,482,548 39,296,356 32,813,808 506%
Grand Total 68,835 60,585 -8,250 -12% 24,645,157 24,672,723 27,566 0% 394,238 347,304 -46,934 -12% 135,525,322 136,795,415 1,270,093 1%
THHFT Board PUBLIC 02 Nov 2021 Page 183 of 225

Charity Annual Report and Accounts 2020-21
THHFT Board meeting- Public Date of the meeting: 02 November 2021 ITEM: 13
Purpose of the Report/Paper: To present the Charity Annual Report and Accounts to the Board for approval as recommended by the Charitable Funds Committee at its meeting on 15th October 2021; following which the Annual Report and Accounts can be submitted to the Charity Commission by the 31 January 2022 deadline. For: Information Assurance Discussion and input Decision/approval Executive summary: This paper accompanies the 2020-21 Annual Accounts and Annual Report. The key headlines are:
• The total value of the Charity’s funds as at 31 March 2021 is £1,117,000. This represents an increase in funds in the year of £250k, largely as a result of increased small-scale donations in response to the COVID-19 pandemic in recognition of the work done by the NHS. The Charity also received some individually significant legacies and donations.
• Income for the year is £685k, compared with £927k in 2019-20. While the pandemic offered new opportunities for fundraising, it also significantly reduced the opportunities for more traditional fundraising. It is also worth mentioning that the Charity received one donation of £500k in 2019-20, which skews the comparison somewhat. Overall, fundraising has remained strong.
• Expenditure on charitable activities for the year is £547k compared with £395k in 2019-20. It has been important for the charity to spend the additional funds received through public generosity. Much of the spend has been on staff welfare.
• The fund recorded a gain on investments of £111k, compared with a £51k loss in 2019-20.
• No significant adjustments were made to the 2020-21 financial statements or annual report as a result of the independent examination.
Sponsor (Executive Lead):
Jon Bell, Chief Finance Officer
Author:
Jonathan Ware, Head of Financial Services
Author contact details: [email protected] Risk implications – Link to Board Assurance Framework or Corporate Risk Register:
N/A
Legal/Regulatory/Finance/Quality & Safety/ HR/E&D/Engagement/Communications/Reputation or Sustainability implications:
Financial & Sustainability
THHFT Board PUBLIC 02 Nov 2021 Page 184 of 225

Link to Relevant CQC Domain: Safe Effective Caring Responsive Well Led Link to relevant Corporate Objectives/strategic aims:
• Performance - We will deliver the right care at the right time for our patients
• Money - We will live within our means
• Well Led - We will empower our people to deliver
Document previously considered by: Charitable Funds Committee Recommendations: The Board is asked to approve the Charity Annual Report and Accounts 2020-21.
THHFT Board PUBLIC 02 Nov 2021 Page 185 of 225

1. BACKGROUND
The 2020-21 annual accounts for Hillingdon Hospitals NHS Trust Charitable Funds have been prepared. In line with the terms of reference of this Committee, they are now being presented for recommendation of onward approval at Trust Board in November.
The draft financial statements have been independently examined by Moore Kingston Smith (MKS) over the last few weeks, and the output of that process will be discussed during this Committee meeting. Examination work on the financial statements is complete, and the independent examiners expect to give a conclusion that the accounts give a “true and fair” view of the financial position of the Charity in the year.
After the accounts have been signed on behalf of the Charity, the independent examiners will sign their statement. Once that is complete, the annual report and accounts will be submitted to the Charity Commission before their 31 January reporting deadline.
2. DETAIL AND COMMENTARY ON MAIN STATEMENTS
Statement of Financial Activity (SOFA) The impact of the COVID-19 pandemic on the SOFA has been two-fold:
• At £685k, overall income is lower than in 2019-20 (£927k). This is because the Charity received a large individual donation of £500k in 2019-20, whereas the largest donation in 2020-21 was £125k. However, small-scale donations through JustGiving and NHS Charities Together were much higher than in previous years, and partly offset the impact of reduced traditional fundraising.
• Expenditure was £150k higher than in 2019-20. Almost all of this increase resulted from additional spend on staff welfare, such as:
o Funding the provision of a luxury coach as a staff breakout area; and o Funding vouchers for all staff to thank them for their work through the
pandemic.
Investment outcomes were significantly better in this financial year. Investments managed by Brewin Dolphin recorded a gain of £111k in 2020-21, compared with a £51k loss in 2019-20.
Balance sheet Overall, funds increased by £250k, driven primarily by the events mentioned above. Most of the gain was in unrestricted funds, as most donations in 2020-21 were given
THHFT Board PUBLIC 02 Nov 2021 Page 186 of 225

for the general benefit of the Charity (in particular hospital staff), rather than for a specific purpose.
Annual report The review of the Annual Report is also complete. No significant issues were found in the Annual Report’s compliance with Charity Statement of Recommended Practice (SORP) guidance.
Key amendments made to the financial statements As in previous years, no significant amendments have been made to the financial statements as part of the independent examination process. Independent examiners from MKS suggested some minor disclosure amendments, which were processed by the team. No changes have been made that have resulted in a change to fund balances.
3. RECOMMENDATION AND NEXT STEPS
We ask the Board to note and approve the Annual Report and Accounts. Following approval and certification by the Trust Board, we will obtain signatures from the independent examiners and make the submission to the Charity Commission ahead of the 31 January 2022 deadline.
THHFT Board PUBLIC 02 Nov 2021 Page 187 of 225

THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST
GENERAL AMENITIES FUND AND OTHER RELATED CHARITIES (Registered Charity No 1056493)
Annual Report and Accounts For the year ended 31 March 2021
THHFT Board PUBLIC 02 Nov 2021 Page 188 of 225

1 | P a g e
THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST
GENERAL AMENITIES FUND AND OTHER RELATED CHARITIES
ANNUAL REPORT LEGAL AND ADMINISTRATIVE SUMMARY 1. Nature of Governing Instrument A Trust Deed dated 15 November 1995 governs The Charity. The
Charity Commission have approved this Deed. Full details can be accessed at their website www.charity-commission.gov.uk.
2. Registered Charity Number The Registered Number of the Charity is 1056493. 3. Trustee
The Hillingdon Hospitals NHS Foundation Trust is the corporate trustee of the Charity, appointed in accordance with clause B of the Declaration of Trust. Non-Executive members of the Board of Directors are appointed by the Foundation Trust’s Council of Governors and Executive members are recruited by the Board of Directors Nominations Committee. A Charitable Funds Committee has been established to assist the corporate trustee in the management of the funds. The Board appoints Committee members to the Charitable Funds Committee, taking into account the particular skills and experience of the individuals and the requirements of the role.
4. Management of Funds The Board of The Hillingdon Hospitals NHS Foundation Trust has put in
place a Charitable Funds Committee to oversee the governance of funds. The Committee is chaired by a Non-Executive Director of the Trust and reports to the full Trust Board.
THHFT Board PUBLIC 02 Nov 2021 Page 189 of 225

2 | P a g e
5. Principal Address The principal address of the Charity is: The Hillingdon Hospitals NHS Foundation Trust, Pield Heath Road,
Uxbridge, Middlesex UB8 3NN 6. Professional Organisations (a) The bankers for the Charity are:
HSBC Bank plc, PO Box 41, High Street, Uxbridge, Middlesex, UB8 1BY.
(b) The investment advisers for the Charity are:
Brewin Dolphin Securities Ltd, 12 Smithfield Street, London, EC1A 9BD.
(c) The Independent Examiners for the Charity are:
Moore Kingston Smith LLP, Devonshire House, 60 Goswell Road, London, EC1M 7AD, United Kingdom.
(d) The internal auditors for the Charity are:
KPMG LLP, 15 Canada Square, London, E14 5GL.
7. Powers of Investment The trustee may invest the funds or part thereof in the purchase of or at
interest upon the security such stocks, funds, shares, securities or other investments as the trustee in their discretion think fit.
THHFT Board PUBLIC 02 Nov 2021 Page 190 of 225

3 | P a g e
OBJECTIVES The objectives of the Charity are to hold funds upon trust and to apply the income and, at the trustee’s discretion, the capital for any charitable purpose or purposes relating to the National Health Service wholly or mainly for the services provided by The Hillingdon Hospitals NHS Foundation Trust. REVIEW OF THE YEAR’S ACTIVITIES Principally, the Charity receives donations from patients and the general public and aims to utilise them primarily to enhance the welfare and amenities of patients and staff above and beyond the levels the NHS can fund. By focussing on these areas the Charity complies with its framework classification as determined by the Charity Commission. 2020/21 proved to be an extraordinary year for the Charity. The global COVID-19 pandemic started affecting the Charity almost immediately and has had a dramatic impact on our activities. Once the extent of disruption became clear, the Charity immediately made £10,000 available to the Trust to support staff in whatever way was needed. The Charity Office itself was taken over itself to be used as the staff sickness reporting hub, so all Charity staff started working from home. Almost immediately the public started delivering large quantities of food, toiletries and other gifts to the Hospital which we were able to have distributed, ensuring all staff received some of the items. Whilst the public, Faith groups and local and national companies showed enormous generosity during this time, the negative impact on the Charity was that all of our normal fundraising activities stopped. The pandemic served to increase awareness of our Charity, and NHS Charities more widely, but has severely interrupted normal Charity business. The key events that we normally attend, such as the Hillingdon Half Marathon and the Uxbridge Business Expo were cancelled. Despite the disruption, during this time:
• We sourced numerous coffee machines, kettles and microwaves free of charge to give to staff for use in their staff rooms.
• We funded the provision of a luxury coach for 6 weeks to be used a staff break-out area. This included all drinks and snacks.
• Whilst all face-to-face fundraising and engagement events stopped
immediately, we set up a staff wellbeing appeal on JustGiving, generating significant funds.
• We stewarded a single £125,000 corporate donation through to completion.
THHFT Board PUBLIC 02 Nov 2021 Page 191 of 225
4 | P a g e
• We received the first grants from NHS Charities Together to
support our COVID response.
• We launched our first major Fundraising appeal, aiming to raise c. £400,000 to build a bespoke Maternity Bereavement Suite.
• We launched our first Virtual event, a half-marathon to be run over
the course of February. This raised £20,000.
• We successfully used our Social Media channels to encourage the public to raise money to support our staff, including 24 hour dancing, knitting, pebble-painting and many more activities.
• We funded the celebrations for International Nurses Day in May.
• We purchased and paid to have 6 benches installed around the
hospital grounds, for staff to use during breaks.
The trustee reviews the aims, objectives and activities of the Charity on a periodic basis. This covers what has been achieved in relation to the outcomes of the work of the Charity in the previous year. The review assesses the success of key activities and the benefits that have been delivered against the objectives set by the trustee. The review also helps to ensure the aims, objectives and activities remain focused on the Charity’s stated aims and legal purpose. The majority of fund balances are held in investments. The Trust’s investment portfolio is constructed in a prudent way appropriate to a charity of this type and is managed by the fund managers Brewin Dolphin Securities Ltd. A balanced approach is taken between growth and income and for the year the portfolio performed in line with The Association of Private Client Investment Managers and Stockbrokers (APCIMS) benchmark. The Charity has continued to consolidate its position in the Hospitals and in the wider community. Our research has shown that knowledge of the Charity and its objectives is limited and this has a consequent impact on our ability to raise funds. The focus this year has been to greatly increase visibility and knowledge of the Charity throughout the Borough of Hillingdon, this visibility being key to more successful fundraising as we go forward. Our main focus in 2021/22 is to rebuild the resources of the Charity, to deliver the Maternity Bereavement Suite funding and create a solid foundation for a less disrupted fundraising future. OBJECTIVES AND ACTIVITIES FOR THE PUBLIC BENEFIT The trustee confirms it has complied with its duty under section 17 of the Charities Act 2011, the Accounting and Reporting for Charities; Statement of recommended practice (SORP), revised 2015. It has considered the public benefit guidance published by the Charity Commission and believes that it has followed it.
THHFT Board PUBLIC 02 Nov 2021 Page 192 of 225
5 | P a g e
The funds have been applied towards benefiting the public in accordance with the objectives of the charity. This is achieved by the Charity supporting a range of charitable and health related activities that included the purchase of additional goods and services above and beyond what is usually provided by the NHS. Spend on staff welfare and amenities was £179k (2019/20: £20k) and includes mainly cost towards staff awards & annual membership. Spend on patients' welfare and amenities were £353k (2019/20:£362k). The Charity purchased specific equipment to meet its obligation of public benefit such as a purchase of a Sonosite Ultrasound system & C-Mac system. FINANCIAL REVIEW The Annual Accounts show the financial position of the Charity for the year ending 31 March 2021. The total income for the year was £685k (2019/20: £927k) this includes some of the major donations as below, £100k from NHS Charities for Covid, Legacy donation £87k, £125k from international warehouse & logistics company, £110k through Just Giving, £10k was from dividends on investments (2019/20: £10k). Total expenditure for the year was £547k (2019/20: £395k) with the majority of this on charitable activities £532k (2019/20: £383k). To further encourage expenditure, the committee has decided that where funds are non-active for a certain amount of time then they will be amalgamated to a general fund where they are more likely to be utilised. The total balance of funds as at 31 March 2021 was £1,117k (2019/20: £867k) reflecting a net increase of £249k. This balance of funds is considered by the trustee to be sufficient to meet the known obligations of the Charity. The majority of fund balances are held as investments, either shares or stocks, with the remainder in interest bearing accounts. No other fixed assets are held by the Charity. The investments are managed by the fund managers Brewin Dolphin Securities Ltd and are valued using mid-market Stock Exchange prices. The Trust has requested Brewin Dolphin manage the Charity investment funds on a “category risk level 5” basis – cautious with risk; the appropriate investment benchmark being WMA (Wealth Management Association). The Charity also benchmarks with members of the NHS Association of Charities to ensure it adopts the appropriate balance of risk and return.
Investments were valued at £792k as at 31 March 2021 representing an in year gain of £104k (2019/20: £42k loss) due to depreciation in investment market conditions.
The Trustee has established an ethical consideration for investments and has directed Brewin Dolphin to act ethically when investing; this excludes investing into tobacco and alcohol. GOVERNANCE The Hillingdon Hospitals NHS Foundation Trust is the corporate trustee for the Charity. The Board members of the NHS Foundation Trust are therefore jointly responsible (on behalf of the NHS Foundation Trust) for the management of the Charity. Collectively the Board contains a wide range of business skills,
THHFT Board PUBLIC 02 Nov 2021 Page 193 of 225
6 | P a g e
including accountancy and governance that assist Board members in the oversight of the Charity. The Board delegates responsibility for the management of the Charity to an officially constituted Board committee; The Charitable Funds Committee. This meets a minimum of three times a year, is chaired by the Chair of the Trust Board and holds to account those staff that have direct financial and administrative responsibility for charitable funds. Appropriately skilled and qualified staff of The Hillingdon Hospitals NHS Foundation Trust performed the supporting management and administration of funds, including the accounting and fundraising, for a total cost of £180k (this included a charge of £27k related to governance). Additionally, a fee of £4k was charged for an independent examination on the annual report and accounts. Fundraising will increase over time to offset these costs and put the Charity on a positive footing for the future. The Charity Director and the Community Fundraiser are members of staff employed by The Hillingdon Hospitals NHS Foundation Trust that is fully funded by the Charity. Remuneration and salary was set by benchmarking against other not for profit organisations. No trustee received any remuneration in respect of his or her services to the Charity during the year. The Committee puts policy and procedures in place to ensure income is spent in accordance with donors’ wishes, in line with the charitable objectives and within a reasonable period of time. This includes an authorisation process of requests for grants and support, which always involves a member of the Charitable Funds Committee. At an appropriate level of detail at each of its meetings the Committee also reviews expenditure decisions taken. Reserves Policy The Trustee has adopted a reserves policy where they consider £300k an appropriate level to ensure the continuing ability of the Charity to meet its objectives and obligations. The value of unrestricted reserves as at 31 March 2021 was £686k (2019/20: £372k), therefore the reserves policy has been exceeded. It is the intention of the trustee to continue to run the Charity in line with its current aims and objectives. Risk Management Board members recognise they are responsible for the Charity’s investments and cash assets. The Charitable Funds Committee has delegated responsibility from the Trust Board and this is set out in a Terms of Reference document. The Committee regularly reviews the activities of the Charity and assesses the major risks to which the Charity is potentially exposed, i.e. financial, operational and
THHFT Board PUBLIC 02 Nov 2021 Page 194 of 225

7 | P a g e
reputational and is satisfied that systems are in place to mitigate exposure to those risks. The Charity’s accounts and financial procedures are subject to internal reviews and any audit recommendations are implemented. Investments are managed by professional advisors, Brewin Dolphin and have been classified at a level appropriate to this sector, caution with risk including income return. This effectively means the Charity retains a degree of protection in its investment strategy but is also looking for a higher rate of return than would be expected with the lowest risk classification. In doing so the corporate trustee acknowledges the values of the investments are not guaranteed and will fluctuate, but over the medium-term expects an above inflation level of return. Going Concern After making enquiries the trustee has a reasonable expectation that the Charity has adequate resources to continue its activities for the foreseeable future. Day to day working capital requirements are managed without the use of an overdraft facility. Although expenditure may exceed income in line with the Charity’s aim to reduce reserves this is supported by a strong investment portfolio. Accordingly, they continue to adopt the going concern basis in preparing the financial statements. Grants Distribution Policy The Charity has both restricted and unrestricted funds. Restricted funds are given to the Charity for purposes specified by the donor and used in accordance with the donor’s wishes. These restricted funds are spent mainly on research and medical equipment. Unrestricted funds are used for general purposes for the benefit of the hospitals not otherwise funded by the NHS. The Charity’s £431k restricted funds at the end of the accounting period were 44% of total funds available. Of this and in accordance with the donor’s wishes £20.5k is available to be spent on additional staffing to enhance services and research, £2.7k for the purchase of radiology equipment for the investigation and diagnosis of cancer and £406k is towards the building of a new Rehab unit at Mount Vernon. Unrestricted funds at the end of the accounting period were £687k. There are no specific guidelines attached to the utilisation of these funds In some cases individual project grants are made over a period of more than one year. In this instance under the Statement of Recommended Practice (SORP), the grant is fully recognised in the year it is committed. The Trust applies to the Charity for internal investment funding as part of its annual business planning process. From these applications, the Trust selects items it considers eligible for funding by the Charity. The selection is submitted to the Corporate Trustee that considers the merits of each project and chooses the most appropriate.
THHFT Board PUBLIC 02 Nov 2021 Page 195 of 225

8 | P a g e
The Charity’s policy only provides grant funding to Hillingdon and Mount Vernon Hospitals and not to any other individual or organisation. Signed on behalf of the trustee Chair-Non Executive Member of the Hillingdon Hospitals NHS Foundation Trust Board Date:
THHFT Board PUBLIC 02 Nov 2021 Page 196 of 225

9 | P a g e
THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST GENERAL AMENITIES FUND, No. 1056493
Statement of trustee’s responsibilities
The trustee is responsible for preparing the Trustee’s Annual Report and the financial statements in accordance with applicable law and United Kingdom Accounting Standards (United Kingdom Generally Accepted Accounting Practice).
The law applicable to charities in England and Wales requires the trustee to prepare financial statements for each financial year which give a true and fair view of the state of affairs of the charity and of the incoming resources and application of resources of the charity for that period. In preparing these financial statements, the trustee is required to:
• select suitable accounting policies and then apply them consistently; • observe the methods and principles in the Charities SORP; • make judgments and estimates that are reasonable and prudent; • state whether applicable accounting standards have been followed; and • prepare the financial statements on the going concern basis unless it is
inappropriate to presume that the charity will continue in business.
The trustee is responsible for keeping proper accounting records that disclose with reasonable accuracy at any time the financial position of the charity and enable them to ensure that the financial statements comply with the Charities Act 2011, the Charity (Accounts and Reports) Regulations 2008 and the provisions of the trust deed. They are also responsible for safeguarding the assets of the charity and hence for taking reasonable steps for the prevention and detection of fraud and other irregularities.
The trustee is responsible for the maintenance and integrity of the charity and financial information included on the charity's website. Legislation in the United Kingdom governing the preparation and dissemination of financial statements may differ from legislation in other jurisdictions.
By order of the Trustee
Signed:
Chair-Non Executive member of The Hillingdon Hospitals NHS Foundation Trust Board
Date:
THHFT Board PUBLIC 02 Nov 2021 Page 197 of 225
10 | P a g e
Independent examiner’s report to the trustees of The Hillingdon Hospitals NHS Foundation Trust General Amenities Fund and Other Related Charities I report to the trustees on my examination of the accounts of The Hillingdon Hospitals NHS Foundation Trust General Amenities Fund and Other Related Charities for the year ended 31 March 2021. Responsibilities and basis of report As the charity trustees you are responsible for the preparation of the accounts in accordance with the requirements of the Charities Act 2011 (‘the Act’). I report in respect of my examination of the Charity’s accounts carried out under section 145 of the 2011 Act and in carrying out my examination I have followed all the applicable Directions given by the Charity Commission under section 145(5)(b) of the Act. Independent examiner’s statement I have completed my examination. I confirm that no material matters have come to my attention in connection with the examination giving me cause to believe that in any material respect:
1. accounting records were not kept in respect of the Charity as required by section 130 of the Act; or
2. the accounts do not accord with those records; or 3. the accounts do not comply with the applicable requirements concerning
the form and content of accounts set out in the Charities (Accounts and Reports) Regulations 2008 other than any requirement that the accounts give a ‘true and fair view which is not a matter considered as part of an independent examination.
I have no concerns and have come across no other matters in connection with the examination to which attention should be drawn in this report in order to enable a proper understanding of the accounts to be reached. Date: Luke Holt FCA For and on behalf of Moore Kingston Smith LLP Devonshire House 60 Goswell Road London EC1M 7AD
THHFT Board PUBLIC 02 Nov 2021 Page 198 of 225
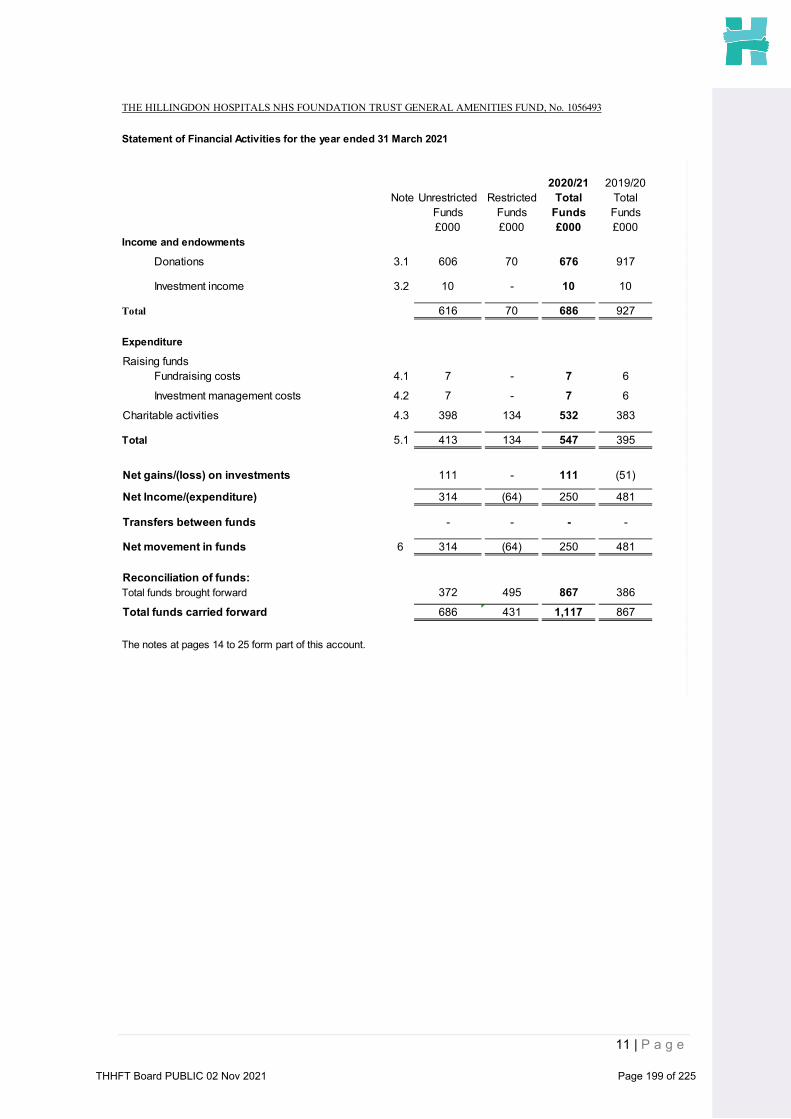
11 | P a g e
THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST GENERAL AMENITIES FUND, No. 1056493
Statement of Financial Activities for the year ended 31 March 2021
2020/21 2019/20Note Unrestricted Restricted Total Total
Funds Funds Funds Funds£000 £000 £000 £000
Income and endowments
Donations 3.1 606 70 676 917
Investment income 3.2 10 - 10 10
Total 616 70 686 927
Expenditure
Raising funds Fundraising costs 4.1 7 - 7 6
Investment management costs 4.2 7 - 7 6
Charitable activities 4.3 398 134 532 383
Total 5.1 413 134 547 395
Net gains/(loss) on investments 111 - 111 (51)
Net Income/(expenditure) 314 (64) 250 481
Transfers between funds - - - -
Net movement in funds 6 314 (64) 250 481
Reconciliation of funds: Total funds brought forward 372 495 867 386
Total funds carried forward 686 431 1,117 867
The notes at pages 14 to 25 form part of this account.
THHFT Board PUBLIC 02 Nov 2021 Page 199 of 225

12 | P a g e
THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST GENERAL AMENITIES FUND, No. 1056493
Balance Sheet as at 31 March 2021
NoteUnrestricted Restricted Total at 31 UnrestrictedRestricted Total at 31Funds Funds March 21 Funds Funds March 20£000 £000 £000 £000 £000 £000
Fixed assets:
Investments 7 487 305 792 293 395 688Total fixed assets 487 305 792 293 395 688
Current assets:
Debtors 8 1 - 1 1 - 1
Cash at bank and in hand 8.1 238 126 364 127 100 227Total current assets 239 126 365 128 100 228
9 (40) - (40) (49) - (49)
Net current assets/ (liabilities) 199 126 325 79 100 179
Net assets 686 431 1,117 372 495 867
The funds of the charity:Restricted income funds 10.2 - 431 431 - 495 495
Unrestricted income funds 686 - 686 372 - 372
Total charity funds 686 431 1,117 372 495 867
Approved by the Board on ____________________ and signed on its behalf:
Chairperson
Creditors: Amounts falling due within one year
THHFT Board PUBLIC 02 Nov 2021 Page 200 of 225

13 | P a g e
THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST GENERAL AMENITIES FUND, No. 1056493
Statement of Cash Flows for the Year Ended 31 March 2021
Note 2021 2020£ £
Cash flow/(outflow) from operating activities
Net cash (used in)/provided by operating activities 127 548
Cash flows from investing activities10 10
Interest paid - -7 82 (106)
Payments to acquire investments 7 (82) (289)Net cash (outflow)/Inflow from investing activities 10 (384)
Increase/(Decrease) in cash and cash equivalents in the year 137 164
Cash and cash equivalents at beginning of the year 226 62Cash and cash equivalents at end of the year 363 226
Reconciliation of net income/ (expenditure) to net cash flow from operating activities
2021 2020£ £
250 481
Adjustments for:
Net (gains)/ losses on investments (104) 51Investment income (10) (10)(Decrease)/ Increase in debtors (0) (0)(Decrease)/Increase in creditors (9) 26
Net cash used in operating activities 127 548
Please note: The Charity has no debt & accordigly no net debt note is presented
Investment income and interest received
Proceeds from disposal of fixed asset
Net Income
THHFT Board PUBLIC 02 Nov 2021 Page 201 of 225

14 | P a g e
THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST GENERAL AMENITIES FUND, No. 1056493
Notes to the Account
Accountin 1.1 Basis of preparation Policies
The principal accounting policies adopted in the preparation of the financial statements are setout below
1.2 Going Concern
Accordingly, they continue to adopt the going concern basis in preparing the financial statements.
1.3 Income
a)
i) entitlement - arises when a particular resource is receivable or the charity's right becomes legally enforceable;
ii) probability - when it becomes probable that the incomewill be received;
iii) measurement - when the monetary value of the income canbe measured with sufficient reliability.
b) Legacies & Bequests
Legacies and Bequests are accounted for as an incoming resource once the receipt becomes probable. This will be once confirmation has been received from the representatives of the estates that payment of the legacy will be made or that property bequeathed will be transferred and once all associated conditions have been fulfilled.
These financial statements are prepared on a going concern basis, under the historical cost convention, as modified by the revaluation of investments being measured at fair value through income and expenditure within the Statement of Financial Activities.
The financial statements have been prepared in accordance with the Financial Reporting Standard applicable in the UK and Republic of Ireland (FRS 102). The Charity is a public benefit company for the entity of FRS 102 and therefore the Charity also prepared its financial statements in accordance with the Statement of Recommended Practice applicable to charities preparing their accounts in accordance with the Financial Reporting Standard applicable in the UK and Republic of Ireland (The FRS 102 Charities SORP) and the Charities Act 2011.
After making enquiries, the trustees have a reasonable expectation that the Charity has adequate resources to continue its activities for the foreseeable future.
Day to day working capital requirements are managed without the use of an overdraft facility. Although expenditure may exceed income in line with the Charity's aim to reduce reserves this is supported by a strong investment portfolio.
All income is included in full in the Statement of Financial Activities as soon as the following three factors can be met:
The financial statements are prepared in sterling, which is the functional currency of the charity. Monetary amounts in these financial statements are rounded to the nearest one
THHFT Board PUBLIC 02 Nov 2021 Page 202 of 225
15 | P a g e
THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST GENERAL AMENITIES FUND, No. 10
1.4 Expenditure
a)Cost of raising funds
b)Grants payable
c) Support costs
d) Governance costs
1.5 Structure of funds
1.6 Investment Fixed Assets
Investment fixed assets are shown at market value.
a)Quoted stocks and shares are included in the balance sheet at mid-market price, ex-dividend.
b)Other investment fixed assets are included at trustees' best estimate of market value.
With effect from 1 April 2020, the Charity has adopted a revised allocation methodology for support costs and investment income. It is now allocating income relating to gains on investments and costs relating to the running of the Charity across all funds pro-rata by size. This change in policy has no impact on the opening
The Charity accounts are prepared in accordance with the accruals concept. All expenditure is recognised once there is a legal or constructive obligation to make a payment to a third party.
These are accounted for on an accruals basis. The cost of raising funds are the costs associated with generating income for the funds held on trust.
Grants payable are payments, made to third parties in the furtherance of the charitable objectives of The Hillingdon Hospitals NHS Foundation Trust General Amenities Fund to relieve those who are sick. They are accounted for on an accruals basis where the conditions for their payment have been met or where a third party has a reasonable expectation that they will receive the grant. This includes grants paid to NHS Bodies.
These are accounted for on an accruals basis and are recharges of appropriate proportions of costs from The Hillingdon Hospitals NHS Foundation Trust. These costs are allocated between Charitable Activities and Costs of raising funds based
These are accounted for on an accruals basis. The governance costs comprise all costs attributable to ensuring the public accountability of the charity and its compliance with regulation and good practice. These costs include costs related to the audit together with an apportionment of support costs.
Where there is a legal restriction on the purpose to which a fund may be put, the fund is classified in the accounts as a restricted fund. Funds where the capital is held to generate income for charitable purposes and cannot itself be spent are accounted for as endowment funds. Other funds are classified as unrestricted funds. Funds which are not legally restricted but which the Trustees have chosen to earmark for set purposes are classified funds. The major funds held within these categories are disclosed on notes 10.1 to 10.3.
THHFT Board PUBLIC 02 Nov 2021 Page 203 of 225
16 | P a g e
THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST GENERAL AMENITIES FUND, No. 1056493
1.7 Realised gains and losses
1.8 Cash and cash equivalents
1.9 Financial instruments
1.10 Legal status of the charity
2 Critical accounting estimates and areas of judgement
In the view of the trustees in applying the accounting policies adopted, no judgements were required that have a significant effect on the amounts recognised in the financial statements nor do any estimates or assumptions made carry a significant risk of material adjustment in the next financial year.
All gains and losses are taken to the Statement of Financial Activities as they arise. Realised gains and losses on investments are calculated as the difference between sales proceeds and opening market value (or date of purchase if later). Unrealised gains and losses are calculated as the difference between market value at the year end and opening market value (or date of purchase if later).
The Hillingdon Hospitals NHS Foundation Trust General Amenities Fund is a charity domiciled and registered in England and Wales. The registered office is The Hillingdon Hospitals NHS Foundation Trust, Pield Heath Road, Uxbridge, Middlesex, UB8 3NN.
Cash and cash equivalents include cash in hand, deposits held at call with banks, other short-term liquid investments with original maturities of three months or less.
The charity has elected to apply the provisions of Section 11 ‘Basic Financial Instruments’ of FRS 102 to all of its financial instruments. Financial instruments are recognised in the charity's balance sheet when the charity becomes party to the contractual provisions of the instrument. Financial assets and liabilities are offset, with the net amounts presented in the financial statements, when there is a legally enforceable right to set off the recognised amounts and there is an intention to settle on a net basis or to realise the asset and settle the liability simultaneously.
All other debtor and creditor balances are considered to be basic financial instruments under FRS 102. See notes 8 and 9 for the debtor and creditor notes.
In preparing financial statements it is necessary to make certain judgements, estimates and assumptions that affect the amounts recognised in the financial statements.
THHFT Board PUBLIC 02 Nov 2021 Page 204 of 225

17 | P a g e
THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST GENERAL AMENITIES FUND, No. 1056493
Details of 3.1 Unrestricted Restricted 2020/21Other Funds Funds TotalMaterial FundsIncome And £000 £000 £000Endowments Material income and endowments
1 Donations 606 70 676
Total donation income 606 70 676
Unrestricted Restricted 2019/20Funds Funds Total
Funds£000 £000 £000
Material income and endowments
1 Donations 416 501 917
Total donation income 416 501 917
THHFT Board PUBLIC 02 Nov 2021 Page 205 of 225

18 | P a g e
THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST GENERAL AMENITIES FUND, No. 1056493
Investment 3.2 UnrestrictedRestricted 2020/21Income Funds Funds Total
Funds£000 £000 £000
1 Dividends 10 - 10
Total Investment Income 10 - 10
UnrestrictedRestricted 2019/20Funds Funds Total
Funds£000 £000 £000
1 Dividends 10 - 10
Total Investment Income 10 - 10
THHFT Board PUBLIC 02 Nov 2021 Page 206 of 225

19 | P a g e
THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST GENERAL AMENITIES FUND, No. 1056493
Expenditure
Costs of 4.1 Unrestricted Restricted 2020/21Raising Funds: Funds Funds TotalFundraising Costs Funds
£000 £000 £000
Fundraising costs 7 - 7
7 - 7
Unrestricted Restricted 2019/20Funds Funds Total
Funds£000 £000 £000
Fundraising costs 6 - 6
6 - 6
Investment 4.2 Unrestricted Restricted 2020/21Management Funds Funds TotalCosts Funds
£000 £000 £000
Fees payable 7 - 7
7 - 7
Unrestricted Restricted 2019/20Funds Funds Total
Funds£000 £000 £000
Fees payable 6 - 6
6 - 6
Charitable 4.3 Unrestricted Restricted Support Cost 2020/21Activities Funds Funds Unrestricted Total
Funds Funds£000 £000 £000 £000
Patients welfare and amenities 163 83 107 353
Hillingdon Hospitals staff welfare 100 51 28 179
263 134 135 532
The Charity’s policy only provides grant funding to Hillingdon and Mount VernonHospitals and not to any other individual or organisation.
THHFT Board PUBLIC 02 Nov 2021 Page 207 of 225

20 | P a g e
THHFT Board PUBLIC 02 Nov 2021 Page 208 of 225

21 | P a g e
THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST GENERAL AMENITIES FUND, No. 1056493
Governance 4.5 Unrestricted Restricted 2020/21Costs Funds Funds Total
Funds£000
Management charge 9 14 23Independent examination of the charity's annual accounts 1 3 4
10 17 27
Unrestricted Restricted 2019/20Funds Funds Total
Funds
Management charge 19 - 19Independent examination of the charity's annual accounts 4 - 4
24 - 24
Analysis of 5.1 Costs of Costs of Investment 2020/21Total Generating Activities for Managers TotalResources Funds Charitable Cost FundsExpended Activities
£000 £000 £000 £000Examiners remuneration - 1 - 1
Charitable Objectives 7 531 7 546
7 532 7 547
Costs of Costs of Investment 2019/20Generating Activities for Managers Total
Funds Charitable Cost FundsActivities
£000 £000 £000 £000Examiners remuneration - 4 - 4
Charitable Objectives 6 379 6 391
6 383 6 395
Analysis of 5.2Staff There were no staff employed directly by the Charity. A Management charge of £152,940Costs (2019/20: £129,695) was made by The Hillingdon Hospitals NHS Foundation Trust to reflect the
use of Trust resources on the activities of The Hillingdon Hospitals NHS Foundation TrustGeneral Amenities Fund
THHFT Board PUBLIC 02 Nov 2021 Page 209 of 225

22 | P a g e
THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST GENERAL AMENITIES FUND, No. 1056493
Changes in 6 Unrestricted Restricted Endowment 2020/21Resources TotalAvailable Funds Funds Funds Fundsfor Charity £000 £000 £000 £000Use
Net movement in funds for the year 313 (64) - 249Net movement in funds availablefor future activities 313 (64) - 249
Unrestricted Restricted Endowment 2019/20Total
Funds Funds Funds Funds£000 £000 £000 £000
Net movement in funds for the year 12 469 - 481Net movement in funds availablefor future activities 12 469 - 481
THHFT Board PUBLIC 02 Nov 2021 Page 210 of 225

23 | P a g e
THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST GENERAL AMENITIES FUND, No. 1056493
2021 2020Analysis of 7.1 Fixed Asset Investments: £000 £000Fixed AssetInvestments Opening Market Value 1st April 2020 689 346
Less: Disposals at carrying value (110) (52)Cash Movnt on Dealing and Deposits Account 28 158Add: Acquisitions at cost 82 289Net gain/(loss) on revaluation 104 (53)Closing Market value at 31 March 2021 792 688
Historic cost at 31 March 2021 695 721
7.2 Market value at 31 March 2021 Held 2021 2020in UK Total Total£000 £000 £000
Investments listed on Stock Exchange 554 554 481
Cash held as part of the Investment portfoli 238 238 207
792 792 688
£554,000 of investments listed on the stock exchange are held in the UK (2020:£481,000). £238,000 of cash held as part of the investment portfolio is held in the UK (2020: £207,000).
Analysis of 7.3 Total gross income Held 2021 2020gross income in UK Total Totalfrom £000 £000 £000investments
Income from investment portfolio 10 10 10
10 10 10
£10,287 of income from the investment portfolio is held in the UK (2020: £10,000).
Analysis of 8 Debtors 2021 2020Current Assets Total Total
Amounts falling due within one year: £000 £000Other debtors 1 1
Total debtors falling due within one year 1 1
8.1 2021 2020Total Total£000 £000
Cash at bank and in hand 364 227
364 227
THHFT Board PUBLIC 02 Nov 2021 Page 211 of 225

24 | P a g e
THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST GENERAL AMENITIES FUND, No. 1056493
Analysis of 9 2021 2020Creditors Total Total
Amounts falling due within one year: £000 £000Other creditors (40) (49)
Total creditors falling due within one year (40) (49)
Analysis of 10.1Funds
There are no Endowment Funds.
10.2 Balance Income Expenditure Balance31 March 31 March
2021 2020£000 £000 £000 £000
Material Restricted funds
A Donaldson Bequest 3 0 (1) 3-
B Rheumatology Nurse Fund 20 3 (6) 23-
c Rehabilitation Unit 408 66 (127) 469
Total 431 69 (134) 495
Balance Income Expenditure Balance31 March 31 March
2020 2019£000 £000 £000 £000
Material Restricted funds
A Donaldson Bequest 3 - - 3
B Rheumatology Nurse Fund 23 - - 23
c Rehabilitation Unit 469 501 (32) -
Total 495 501 (32) 26
Details of 10.3 Name of fund Description of the nature and purpose of each fundMaterial A Donaldson Bequest radiological equipment for the investigation and diagnosis of cancerFunds B Rheumatology Nurse Fund funding an additional Rheumatology Nurse for 1 year to enhance services
C Rehabilitation Unit Potential for building a new Rehab unit at Mount vernon
THHFT Board PUBLIC 02 Nov 2021 Page 212 of 225
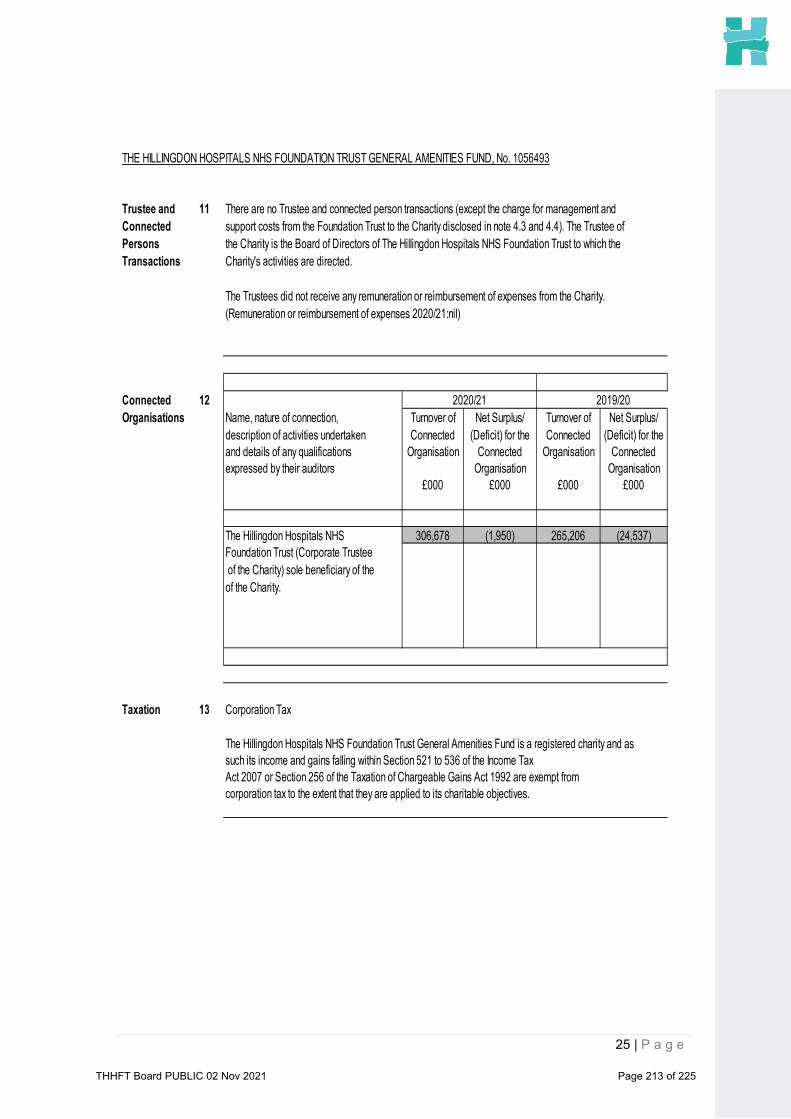
25 | P a g e
THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST GENERAL AMENITIES FUND, No. 1056493
Trustee and 11 There are no Trustee and connected person transactions (except the charge for management andConnected support costs from the Foundation Trust to the Charity disclosed in note 4.3 and 4.4). The Trustee of Persons the Charity is the Board of Directors of The Hillingdon Hospitals NHS Foundation Trust to which the Transactions Charity's activities are directed.
The Trustees did not receive any remuneration or reimbursement of expenses from the Charity. (Remuneration or reimbursement of expenses 2020/21:nil)
Connected 12 2020/21 2019/20Organisations Name, nature of connection, Turnover of Net Surplus/ Turnover of Net Surplus/
description of activities undertaken Connected (Deficit) for the Connected (Deficit) for theand details of any qualifications Organisation Connected Organisation Connectedexpressed by their auditors Organisation Organisation
£000 £000 £000 £000
The Hillingdon Hospitals NHS 306,678 (1,950) 265,206 (24,537)Foundation Trust (Corporate Trustee of the Charity) sole beneficiary of the of the Charity.
Taxation 13 Corporation Tax
The Hillingdon Hospitals NHS Foundation Trust General Amenities Fund is a registered charity and as such its income and gains falling within Section 521 to 536 of the Income TaxAct 2007 or Section 256 of the Taxation of Chargeable Gains Act 1992 are exempt from corporation tax to the extent that they are applied to its charitable objectives.
THHFT Board PUBLIC 02 Nov 2021 Page 213 of 225
Page 1 of 4
Review of Human Tissue Authority Guidance
THHFT Board Meeting- Public Date of the meeting: 02 November 2021 ITEM: 14 Purpose of the Report/Paper: This paper provides an update on the recent request for the Boards of NHS organisations who have a mortuary or body store to ensure they are compliant with existing Human Tissue Authority (HTA) guidance. A review was required to be undertaken and a return made by 16 November 2021. For: Information Assurance Discussion and input Decision/approval
Executive summary: This paper provides an update on the review undertaken to ensure that the HTA requirements have been met in relation to security of our mortuary facilities on both hospital sites. The requirement was:
• To ensure all access points to the mortuary are controlled by swipe card security access or with alterative sufficient mitigation– which they are
• To have effective and regularly reviewed CCTV coverage in mortuary areas – which is in place
• To have documented risk assessments undertaken with regard to the operation, security and construction of the mortuary facilities. These have been completed.
• To ensure there is a consistent application of appropriate levels of DBS checks for all Trust and contracted employees.
A return was committed with the required details following the review on 20th October 2021. The Trust fully complies with the requirements set by the HTA. Sponsor (Executive Lead):
Jon Bell, Chief Financial Officer
Author:
Steve Wedgwood, Deputy Director of Estates & Facilities
Author contact details: [email protected] Risk implications – Link to Board Assurance Framework or Corporate Risk Register:
Risk assessments have been carried out as required by the review.
Legal/Regulatory/Finance/Quality & Safety/ HR/E&D/Engagement/Communications/Reputation or Sustainability implications:
• Regulatory • Legal • Reputation • Quality & Safety
THHFT Board PUBLIC 02 Nov 2021 Page 214 of 225

Page 2 of 4
Link to Relevant CQC Domain: Safe Effective Caring Responsive Well Led
Link to relevant Corporate Objectives/strategic aims:
Quality- We will deliver consistent high quality care
Document previously considered by: N/A
Recommendations: The Trust Board is asked to note the report, actions taken and receive assurance that the Trust fully complies with the requirements set by the HTA.
THHFT Board PUBLIC 02 Nov 2021 Page 215 of 225

Page 3 of 4
Review of Human Tissue Authority (HTA) Guidance in relation to the security of mortuaries and body stores
1.Background
1.1 A letter was issued to all Trusts on 12th October 2021 by NHSE/I requesting that all NHS Boards of organisations that have either a mortuary of body store ensure that they are compliant with existing guidance and take the additional steps set out in the letter. A return was required to be submitted by 16th November confirming that the areas had been reviewed and compliance adhered to.
2. Actions taken to provide assurance 2.1 A review was undertaken by Robert Street, Facilities Manager (Security
Management Specialist) and carried out in partnership with the Mortuary Services Manager.
2.2 The review covered the specific questions detailed below:
Ensure all access points to the mortuary or body store are controlled by swipe card security access. Where this is not immediately possible, organisations must assure themselves that there is sufficient mitigation in place to ensure the facilities are secure and there is auditable access.
Review outcome:
• At Hillingdon all doors to the mortuary from outside are controlled via access control, and therefore self-auditing in terms of who has access at what time/day etc. There is also a key log for Porters and Mortuary staff for out of hours services, which is supported by an authorised signatory list.
• At Mount Vernon – The facility does not have electronic access control, the security of the mortuary is via mechanical locks. This is supported by an auditable signatory system held centrally with the Portering Department, also supported by an authorised signatory list and provides the required mitigation.
There must be effective CCTV coverage in mortuary areas and this should be reviewed on a regular basis by an appropriately trained and authorised individual. Specialist training and mental health support may be required to support staff to undertake this task.
Review outcome:
• At Hillingdon – External and internal CCTV is in situ and can be reviewed when required, it is a system that is password protected and can only be reviewed by staff privy to the password. Weekly checks of functionality are also being introduced.
THHFT Board PUBLIC 02 Nov 2021 Page 216 of 225
Page 4 of 4
• At Mount Vernon the same system is in place - linked from MVH to the
main system. A documented risk assessment of the facilities should be undertaken with regard to the operation, security and construction of the mortuary or body store area. Review outcome:
• Both sites were risk assessed and the Risk Lead is the Mortuary Services Manager. These are also supported by the internal risk assessments undertaken as part of the HTA accreditation process.
Ensure there is consistent application of appropriate levels of DBS checks for all Trust and contracted employees, specifically in line with requirements of the NHS Standard Contract. Employers are required to pay attention to the security features of a DBS certificate, and support on DBS checks can be found here.
Review outcome:
• At Hillingdon all staff that enter or work in the facility are DBS checked to the appropriate level at the start of their employment. DBS checks are carried out according to the Recruitment Policy and are only carried out at the commencement of a member of staff or if a job is changed.
• The same process is in place at Mount Vernon.
3. Summary 3.1 The review was carried out as required and the return provided before the due
date. It showed that we comply fully with the requirements set by the HTA.
THHFT Board PUBLIC 02 Nov 2021 Page 217 of 225

1
REPORT FROM CHAIRS OF THE BOARD SUB COMMITTEES
THHFT Board Meeting - Public
Date of the meeting: 02 November 2021 ITEM: 15
Purpose of the Report/Paper:
To provide the Board with an update from the Chairs of the Board Sub Committee meetings held in October 2021. For: Information Assurance Discussion and input Decision/approval Executive summary:
The Board is asked to receive and note for assurance the updates provided from the Chairs of the Board Sub Committees convened in September 2021. Sponsor (Executive Lead): • Lord Morse KCB, Chair of
the Redevelopment Committee
• Neville Manuel, Chair of the Audit and Risk Committee;
• Simon Morris, Chair of the Charitable Funds Committee;
Author: Vikas Sharma, Trust Secretary
Author contact details: [email protected]
Risk implications – Link to Board Assurance Framework or Corporate Risk Register:
All BAF risks apply
Legal/Regulatory/Finance/Quality & Safety/ HR/E&D/Engagement/Communications/Reputation or Sustainability implications:
All may apply
Link to Relevant CQC Domain: Safe Effective Caring Responsive Well Led Link to relevant Corporate Objectives/strategic aims: • Quality –we will deliver
consistent high quality care• Performance – we will deliver
the right care at the right timefor patients
• Money – we will live within ourmeans
• Well led – we will empower ourpeople to deliver
• Partnership working – we willdevelop sustainable models of
THHFT Board PUBLIC 02 Nov 2021 Page 218 of 225

2
care centred around our patients
Document previously considered by: NA Recommendations: The Board is asked to receive and note for assurance the updates provided from the Chairs of the Board Sub Committees held in October 2021.
THHFT Board PUBLIC 02 Nov 2021 Page 219 of 225

3
Report from the Chair of the Redevelopment Committee Amyas Morse The following items were received and discussed at the meeting held on 7th October 2021:
• Terms of Reference: The Committee noted the Terms of Reference, which had been
agreed previously by the Trust Board on 06 July 2021. The Chair reiterated that the Committee has been established to provide oversight and scrutiny to the redevelopment programme and to provide assurance to the Trust Board. It was agreed to review the membership of the Redevelopment Committee in the future in reference to representation from local stakeholders. The Committee noted that key stakeholders are fully engaged in the programme at an assurance level through the Redevelopment Partnership Board and at a management level through the Redevelopment Steering Group, Redevelopment Programme Board, Strategy and Transformation Group and Finance and Activity Group.
• Summary report on progress: The Committee noted the continued excellent progress of the Hillingdon Hospital redevelopment programme and noted the key next steps and overall risk status of the programme. In line with the Collaboration Agreement between the Trust and the New Hospital Programme (NHP) team, Lesley Watts, as Accountable Officer for the redevelopment programme, and Jason Seez, as Senior Responsible Officer for the redevelopment programme, are working closely with national and London leads to jointly address the key risks to the programme. It was noted that the NHP team has undertaken a Phase 2 digital assessment of the Trust’s scheme, which has seen the RAG status against key digital criteria significantly improve from the Phase 1 review position. Feedback from the NHP team suggests the Trust’s digital progress is strong.
• Refreshed schedule of accommodation, 1:500 designs, cost plan and Outline
Business Case delivery programme: The Committee approved the revised schedule of accommodation, 1:500 designs, cost plan and Outline Business Case delivery programme. The Committee noted the next steps, including commencement of the more detailed 1:200 design stage from mid-October 2021, alongside continued engagement with the NHP to confirm support for the design, key milestones and 2021/22 programme costs.
• Finance report: The Committee noted the current financial performance of the redevelopment programme; noted the changes to budget forecasts across decant and enabling costs, design fees and programme costs; and noted the current funding position.
• Decant and enabling progress update: The Committee noted the decant and enabling progress update.
THHFT Board PUBLIC 02 Nov 2021 Page 220 of 225

4
Report from the Chair of the Charitable Funds Committee Simon Morris The following items were received and discussed at the meeting held on 15th October 2021:
• Presentation from investment managers & Ethical Standards of Investments: The Committee noted the update and advised that a report is brought to the next meeting in order to review the portfolio options and come back with a recommendation
• Report on Investments: An update on investments was noted and that the value of investments has increased by £31k for the period ending June 2021 which is continuing that upward trend that was seen throughout 2021
• Charity Director’s Report: The Committee noted the report and supported the idea of launching public lottery in March/April 2022, subject to the open tendering process and the board being made aware of the launch of the lottery in its role as trustee of the charity. The Committee made a recommendation to the Board to approve the Lottery proposal. Appendix 1
• Charity Strategy and Budget: The Committee noted the Charity Strategy and Budget and advised to bring a progress report on objectives set for 2021/22
• Charity Annual Accounts 2020-21: The Committee noted and approved the Charity’s Annual Report and Accounts 2020-21 for onward sharing with the Board in November for approval. The Committee thanked the finance team for their efforts and work towards Charity Annual Accounts 2020-21
• Income and Expenditure for the Charitable Fund and summary of balances: The Committee noted the report
• Health and Wellbeing update: The Committee noted the update and discussed that there is a need to be an open and close dialogue so as to ensure the charity was able to support initiatives as they developed. Staff wellbeing being one of the priorities for the charity’s funding.
• CFC Forward Planner 2021-22: The Committee noted the draft CFC Forward Planner 2021-22
THHFT Board PUBLIC 02 Nov 2021 Page 221 of 225

5
Report from the Chair of the Audit and Risk Committee Neville Manuel The following items were received and discussed at the meeting held on 20th October 2021:
• Internal Audit progress report • Review of the factors that contributed to the year-end issues on capital
expenditure and the audit • Soft controls analysis of the staff survey
The Committee noted the internal audit progress report including the factors that contributed to the year-end issues on capital expenditure and Soft controls analysis of the staff survey and in response to the internal audit report on the Trust’s capital procurement an additional Audit and Risk Committee meeting will convened in December 2021 to cover the following areas of assurance:
- Individual accountability and disciplinary review - Coverage of proposed actions - Timeliness of proposed actions - Depth of assurance of proposed actions - Internal and external assurance as to the impact and effectiveness of
proposed actions
• LCFS progress report: The Committee noted the report from LCFS.
• Progress from External Auditors: The Committee noted that the final Annual Auditors Report on last year's audit has been issued and the external auditors are preparing and planning work for this year’s audit.
• Financial report including Review of Creditors and Debtors position, Reference costs and Better Payment Practice Code BPPC: The Committee noted the report.
• Update on Grip and Control Task and Finish Group: The Committee noted the report and advised to provide assurance report in the next meeting on targeted and achieved impacts of various interventions as mentioned in the report.
• Review of the 31 March 2021 Statement of Financial Position: The Committee noted the report
• Capital Governance Update: The Committee noted the report and for the assessment on recommendations from the report to be brought to the additional ARC meeting in December 2021.
• Quarterly Estates and Facilities Update - Estates Risks and Issues: The Committee noted the report and discussed the risks around
• Health & Safety Progress Report: The Committee noted the Health & Safety Progress report
• ARC Terms of Reference: The review of Terms of Reference were deferred to the last quarter of the year and will be reviewed in consistency with the ToRs of other sub-committees.
THHFT Board PUBLIC 02 Nov 2021 Page 222 of 225

6
• ARC Draft Forward Plan: The Committee noted the ARC forward planner.
THHFT Board PUBLIC 02 Nov 2021 Page 223 of 225

Charity Public Lottery
THHFT Board meeting- Public Date of the meeting: 02 November 2021 ITEM: 15.1
Purpose of the Report/Paper: To inform the Trust Board of plans to develop a Public Lottery For: Information Assurance Discussion and input Decision/approval Executive summary: The Charity’s fundraising activities tends to lead to peaks and troughs of income, based on our events and publicity. We have been exploring the benefits of a Public Lottery to provide a more consistent income pattern and a level of ‘base’ fundraising, so our events become the top-up, rather then the core income. The CFC has approved the development of this Lottery which we will seek to develop alongside London North West Charity. We have already received Board approval to proceed there and pending approval from the THH Board plan to launch the Lottery in April 2022. Sponsor (Executive Lead):
Sue Smith, Chief People Officer
Author:
David Jenkins, Charity Director
Author contact details:
[email protected] 07811 735083
Risk implications – Link to Board Assurance Framework or Corporate Risk Register:
N/A
Legal/Regulatory/Finance/Quality & Safety/ HR/E&D/Engagement/Communications/Reputation or Sustainability implications:
N/A
Link to Relevant CQC Domain: Safe Effective Caring Responsive Well Led Link to relevant Corporate Objectives/strategic aims:
Document previously considered by: Charitable Funds Committee
Recommendations: To Board is asked to approve the Lottery proposal.
THHFT Board PUBLIC 02 Nov 2021 Page 224 of 225

Many charities rely on Regular Giving programmes to provide their core, base level funding. Hillingdon Hospital Charity does not have a large enough database of donors to support this activity. The introduction of a Public Lottery can address this and help create a stable monthly income, so smoothing the peaks and troughs of our normal fundraising. The key points of the public lottery are: • It is a simple number matching lottery with the possibility of winning between £5
and £10,000 per week • Tickets are £1, with players limited to two entries per week. • Based on similar sized Trusts, within three years we should be earning c. £130k
annually (assuming signing 2,400 new players per annum) • Players sign up for a weekly Direct Debit; sales are through a combination of face-
to-face, online through a bespoke website, via social media and through the Charity office.
Other considerations: • The day-to-day administration and licensing are all managed by the 3rd party
provider • All prizes are paid from the management fee, HHC keep 60% all ticket sales • All player data is collected in accordance with GDPR legislation and owned by the
Charity • They are a proven success in other Hospital Trusts • The public desire to support the NHS has never been higher • It can be developed alongside London North West Healthcare Charity to dilute
costs
THHFT Board PUBLIC 02 Nov 2021 Page 225 of 225