The health hazards of depleted uranium munitions (c)

of 23
Transcript of The health hazards of depleted uranium munitions (c)
-
8/8/2019 The health hazards of depleted uranium munitions (c)
1/23
1
The health hazards of depleted uranium munit ions
ANNEXE C Assessments of depleted uranium intakes from use of depleted uranium on
the battlefield
M R Bailey (NRPB), J Marriage (AWE), J Shaw (AWE) and C Walsh (NRPB)
C1 Introduction
To make the assessment manageable, a set of specific scenarios was defined to be representative
of the various exposures. In each scenario only the exposure pathways considered to dominate
were assessed. For short -term exposures it seemed reasonable to use the three generic situations
(Level I, II and III exposures) used in OSAGWI (2000); these are defined in section 2.2 of appendix 1,
Battlefield exposure scenarios. Assessments of Level I and II exposures were based mainly on data
from trials of DU penetrators. Assessments of Level III intakes by inhalation outside vehicles
resulting from penetrator impacts, and fires involving DU, were based on modelling of dispersion of
aerosols. It was beyond the scope of this assessment to develop and validate a suitable model. Theapproach taken was to review, and then use, published models that have been applied to DU
dispersed from impacts or f ires. Assessments of intakes from inhalation of resuspended soil were
based on existing models used for environmental impact assessments. In each case, central
estimate and worst-case assessments were made, as described in section 2.2 of appendix 1.
C2 Level I exposures
C2.1 Introduction
Level I exposures are considered to be potentially the highest, eg being in a vehicle struck by a DU
penetrator, or soldiers entering a struck vehicle immediately to assist injured comrades. It is
assumed that such exposures are dominated by inhalation of the aerosol formed by the impact and
by embedded DU shrapnel fragments. The latter are considered separately in annexe B. The rest of
this section is concerned only with inhalation of the aerosol formed by the impact.
Inhalation f rom nominal sources of DU are calculated below, using clearly defined assumptions,
which may be challenged and changed. The calculations do not rely on any expert knowledge, but
contain referenced data where appropriate.
Such scenarios cover a very wide potential range of exposures. As described in annexeE, section
E2.3, the large calibre munitions fired by tanks have DU projectile masses of 45 kg, whereas the
small calibre munitions to be used in Bradley Fighting Vehicles (BFV) have projectile masses of 0.09
kg. The munitions fired by aircraft have a DU projectile mass of about 0.3 kg. In tests against
armour plate (annexe G) the estimated fraction of the penetrator aerosolised varied from 0.25% to
70%. (The value of 70% is disputed, and a more realistic upper bound may be about 20%.) It is
reported that if a large calibre round strikes a lightly armoured vehicle such as a BFV, and does not
hit a massive object such as the engine block, it may well pass straight through, with little
aerosolisation.
There are two potential sources of information:
test firings of DU penetrators against hard targets, such as armour plate, and in particular
-
8/8/2019 The health hazards of depleted uranium munitions (c)
2/23
2
against armoured vehicles;
measurements made on soldiers involved in Level I incidents in the Gulf War.
C2.2 Information from test firings
According to OSAGWI (2000, tab O), for estimating Level I exposures, given the lack of any
measurements of DU levels in air during the Gulf War, CHPPM (1998) considered the best data
source to be Fliszar et al (1989). We were unable to obtain this report, but it is summarised in
OSAGWI 2000 (Tab L, research report summary #27). Since it is particularly relevant, a summary of
the part relevant to Level I exposures (based on that in OSAGWI 2000) follows. (More details are
given in CHPPM 2000.)
The tests measured DU aerosol levels generated inside and outside a heavy (ie DU) armour Abrams
tank hit by various types of round. Interior air was sampled during three impact tests when
breakthrough into the crew compartment occurred. Limited data were collected in the first two of
those tests but not for the last test because all the air samplers were destroyed. During the first two
tests, most air samplers shut down soon after impact.
Intakes were estimated based on the conservative assumption that the samplers shut off within the
first second after impact. In the first test, the highest DU mass on a filter (3.7 mg total dust) was at
the gunners position, which gave an intake of 26 mg DU. In the second test, the highest DU mass
on a filter (4.6 mg) was at the drivers position. This sampler, however, continued to run for about
16 minutes. The drivers projected intake (breathing at 30 litres per minute) over that 16 minutes
would have been 28 mg DU. The highest filter reading in the main crew compartment was 2.4 mg,
presumably collected in the moments before the sampler shut off. This suggests an appreciably
higher concent ration of DU might have arisen in the main crew compartment than in the drivers
compartment.
For the sampler (projected flow rate: 5.0 litres per minute) in the main crew compartment where
the largest DU mass was recovered (3.7 mg), researchers estimated the amount of DU initially inthe air inside the vehicle (interior air volume of 268.5 ft
3) conservatively assuming a 1-second
sampling time after impact. They also conservatively assumed uniform DU distribution in the
vehicles air at the time of sample collection. Their estimate of 338 grams (total DU dust), would be
about 8.5% of the original DU mass of the penetrator hitting the vehicle (approximately 4000
grams for the 120 mm DU-KE), much lower than that reported in previous non-vehicular hard-
target impact aerosol tests. In addition, the projected 338 grams includes the unknown
contribution to that aerosol from the DU armor itself.
Using the information quoted above, we inferred the following. The volume assumed to be
sampled (5 litres per minute for 1 sec) = 8.3 x 105 m3. Since 3.7 mg was sampled, the
concentration measured = 44,400 mg m3
. The tank volume (268.5 f t3) = 7.6 m
3. Hence total DU
dust airborne, assuming uniform distribution in the air = 44.4 x 7.6 = 338 g. This initial
concentration i s extremely high. However, since the amount on the one sampler that did not shut
down was similar, it suggests that either the assumed run time (1 second) was too short, and/or
that the concentration fell very rapidly. An intake of 28 mg was calculated based on breathing at
30 litres per minute for 16 minutes (volume 0.48 m3), which gives an average concentration over
the 16 minutes of 58 mg m3
. GAO (2000) noted concerns about the reliability of CHPPMs dose
estimates for Level I veterans. A major factor was the actual time for which air samplers ran in the
key impact tests (Fliszar et al 1989). GAO (2000) refers to other sources of uncertainty, including
-
8/8/2019 The health hazards of depleted uranium munitions (c)
3/23
3
assumed breathing rates, and types of armour. (Some of the friendly-fire incidents in the Gulf War
involved lightly armoured BFVs.) Hence, OSAGWI directed the US Army to undertake tests to
characterise fully the likely exposure to DU, and its health and safety aspects, in combat vehicles
struck by DU munitions. This testing is expected to be completed in 2002. This situation illustrates
the difficulties involved in assessing such exposures.
The studies reviewed and summarised in annexe Ginvolved impacts of penetrators against armour
plate and hence are more relevant to worst -case than central estimate assessments. The studies
provide two types of information: measurements of the air concentration and estimates of the
fraction of the penetrator aerosolised (table C1). One report (Hansen et al 1974) relates to small-
calibre munit ions, the others to large-calibre munit ions. In one case (Hansen et al 1974) the impact
was largely contained by enclosures, but their combined volume (~0.5 m3) was much smaller than
that of a vehicle, which would tend to overestimate the initial concentration. The others seem to
have been conducted outdoors, or in enclosures considerably larger than a vehicle, and so might
tend to underestimate the initial concentration in a confined space.
Table C1. Summary of air concentrat ions and fraction aerosolised from DU penet ratorimpacts
Report Mass concentration (mg m3
) Fraction of penetratoraerosolised (%)
Reports obtainedHansen et al 1974 5001700 (exit chamber)
70600 (entrance chamber)
0.25a
Glissmeyer and Mishima
1979
835 70
Chambers et al 1982 130 (average) 3 (1.55)
Brown 2000 1360 (inside, at 3 m)717 (outside, at 7 m)
Reports not obtained (OSAGWI 2000, tab L)Gilchrist et al 1979 Near target, >0.3 for 5 min and >15
min (dry surface); but
-
8/8/2019 The health hazards of depleted uranium munitions (c)
4/23
4
According to CHPPM (2000, p.125) the most likely value for an exposure time was 60 seconds
(range 10120 seconds), although it acknowledges (p.151) that for one BFV crew it was
substantially longer. For the purpose of this assessment it is assumed that the central estimate of
exposure time is 60 seconds and the worst -case is one hour. CHPPM (2000, p.151) reports
unpublished test data showing that the concentration inside a tank fell by about a factor of 10
every 10 minutes (falling to about 0.02% of the initial amount at 30 minutes). Therefore it is
assumed here that the initial concentration is maintained for 1 minute, that it is a factor 10 lower
for 10 minutes and a further factor of 10 lower for 10 minutes, and so on (table C2).
The studies summarised in annexe G indicate that a large proportion of the aerosol (about 50%) is
respirable. Here the term respirable is used to mean small enough to be readily resuspended and
inhaled, ie less than about 10 m dae, and not , as usually defined for occupational health purposes,
to mean the fraction of the aerosol that if inhaled could reach the alveolar region, ie the deep
lungs. In this assessment a size distribution is applied to this respirable fraction to determine the
fraction deposited in each part of the respiratory tract. This is consistent with the use of cascade
impactor measurements of this size distribution, since the cascade impactors were often fit ted with
a precutter that allowed only particles with dae less than about 10 m to enter.
To estimate intake rates (mg h1
), these concentrations are multiplied by breathing rates (m3
h1
).
ICRP (1994a, table 6) defines four reference levels of exercise for which it gives reference breathing
parameter values: sleep, sitt ing, li ght exercise and heavy exercise. Clearly heavy exercise should be
assumed in this situation, for which the breathing rate is 3.0 m3
h1
(0.05 m3
min1
). Intakes based
on this are derived in table C2.
Table C2. Estimated intakes from Level I exposures
Central estimate Worst-caseDuration
minutes Concentrationof respirableDU, mg m
3
Ratea
ofintake ofDU, mgmin
1
Intakeof DU,mg
Concentrationof respirableDU, mg m
3
Ratea
ofintake ofDU, mgmin
1
Intakeof DU,mg
1 5000 250 250 50,000 2500 2500
1 11 5000 250 250011 21 500 25 25021 31 50 2.5 25
31 41 5 0.25 2.5
Total (rounded) 250 5000
a Breathing rate 0.05 m3 per minute
These intakes are higher than those estimated by CHPPM (2000) as reported in OSAGWI (2000), up
to about 30240 mg (annexe E, section E4.4). It is emphasised that the assumptions made here are
not based on good experimental data or expert knowledge, but the assumptions and their basis are
stated. According to DRPS (1993): In the unlikely event of personnel in a vehicle surviving the
impact of a DU round it is calculated that they could possibly inhale larger quantities of DU
particulate, in the order of 3mg per second. This corresponds to about 200 mg per minute, close
to the central estimate initial concentration, but DRPS (1993) does not estimate the total intake.
-
8/8/2019 The health hazards of depleted uranium munitions (c)
5/23
5
C2.3 Measurements made on soldiers involved in Level I incidents in the Gulf War
It is possible to make an assessment based on the measured excretion rates in the friendly fire
victims, but it will not be precise, because the measurements were made after such a long delay,
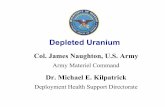
and were of total uranium, not specifically of DU. Figure C1 gives predicted urinary excretion rates
for default type M and type S uranium aerosols inhaled under reference conditions (light work,
AMAD 5 m etc) as used in ICRP publications 68 and 78, and for central estimate Level I and Level
II inhalation exposures (tables 14 and 15 of appendix 1).
Figure C1. Predicted daily ur inary excretion (gram U d1) follow ing acute intake of 1 gramU. Input parameter values given in tables 14 and 15 of appendix 1
Fetter and von Hippel (1999, note 40) made such an assessment as follows using data which was
then unpublished. Urine uranium concentrations were measured in 1994 and 1997, about 1100
and 2300 days after exposure; the highest level measured amongst the 14 veterans who did not
have shrapnel was 0.14 g U per gram creatinine. (Concentrations in unexposed controls were
0.010.05 g U per gram creatinine.) Assuming an excretion rate of 2.2 gram creatinine d1
gave
an excretion rate of 0.3 g U d1
. Using the ICRP model (presumably ICRP publication 54,
1988b, which uses the ICRP publication 30, 1979, Lung Model) they calculated that for a single
inhalation of one gram U, excretion rates at 1100 and 2300 days would be about 23 and 13 g U
d1
for insoluble compounds and 4.4 and 2.6 g U d1
for soluble compounds. Thus if the
aerosol was 30% soluble an excretion of 0.3 g U d1
would imply an intake of 1730 mg U in
1991. The estimated amount would be up to two times smaller for a finer, less soluble aerosol andup to two times greater for a coarser, more soluble aerosol. According to OSAGWI (2000, Tab H)
the friendly-fire incidents occurred in February, 1991. Hooper et al(1999) reported that urine
samples were collected and measured in 1993/4 (about 3 years later, ie 1095 days), and in
July/August 1995 (about 4 years 5 months later, ie 1580 days). Information on excretion rates is
given in tables 3 and 4 of Hooper et al. Table 3 states that in subjects with no suspected shrapnel,
the concentration (presumably the average for the group) was 0.07 g litre1
or 0.03 g U per gram
creatinine in 1993/4 (n=10), and 0.04 g litre1 or 0.01 g U per gram creatinine in 1995 (n= 3).
1.E-08
1.E-07
1.E-06
1.E-05
1.E-04
1.E-03
1.E-02
1.E-01
1 10 100 1000 10000
Time after intake, days
Dailyurin
aryexcretion,gra
Impact (Level I)
Resuspension (Level II)
Type S
Type M
-
8/8/2019 The health hazards of depleted uranium munitions (c)
6/23
6
Table 4 gives three values for subjects with no shrapnel: 0.03, 0.03 and 0.08 g U per gram
creatinine.
McDiarmid et al (2000) reported measurements made in spring/summer 1997 (about 6 years 3
months later, ie about 2200 days). Information on excretion rates is given in figure 2. In 14 subjects
who were exposed to DU, but with no suspected shrapnel, the concentration was in the range
from just below 0.01 g U per gram creatinine to just above 0.1 g U per gram creatinine.
As a worst-case for this group, assume that the highest level of excretion is mainly DU, ie that there
is excretion of 0.1 g DU per gram creatinine, or about 0.2 g DU per day, after 1095, 1580, or
2200 days. Table C3 gives the predicted excretion rate following inhalation of 1 gram DU, for
default type M and default type S uranium inhaled by a reference worker (as in ICRP publication
78), and for the central estimate parameter values for Level I exposure (table 14 of appendix 1).
Table C3 also gives the relevant input parameter values.
Table C3. Predicted urinary excretion rates follow ing inhalation of 1 gram DU for Level I
inhalation of impact aerosol (table 14), and for reference occupational exposure to type Mand type S uranium aerosols. Relevant input parameter values are also given.
Type M Type S Level I impact
(table 14)
Input parameterSubject exercise level Light work Light work Heavy exercise
AMAD, m 5 5 2GSD 2.5 2.5 13
Density , g cm3 3 3 9Rapid dissolution fraction, f
r0.1 0.001 0.3
Rapid dissolut ion rate, sr, d
1100 100 1
Slow dissolution rate, ss, d
10.005 0.0001 0.001
Gut uptake factor, f1
0.02 0.002 0.002
Urinary excretion rate, g d1
1095 days 0.9 1.4 101580 days 0.5 1.0 5
2200 days 0.4 0.7 2
The excretion rates are lower than those calculated by Fetter and von Hippel (1999) for a number
of reasons, including:
Lung deposition is considerably lower for a 5 m AMAD aerosol in the ICRP publication 66
model used here than for a 1m AMAD aerosol in the ICRP publication 30 model presumably
used by Fetter and von Hippel (1999).
There is less absorption to blood for an ICRP publication 66 type S insoluble aerosol than for an
ICRP publication 30 class Y insoluble aerosol.
Thus depending on the time, an excretion rate of 0.2 g DU per day corresponds to:
for type M, an intake of 220 500 mg DU;
for type S, an intake of 140 280 mg DU;
for the central estimate impact aerosol parameter values an intake of 20 100 mg DU.
These are broadly consistent with the central estimate intake assessment of 250 mg (table C2).
-
8/8/2019 The health hazards of depleted uranium munitions (c)
7/23
7
C3 Level II exposures
C3.1 Introduction
Both Level II and Level III scenarios involve entry into DU-contaminated vehicles, which have been
struck by one or more DU penetrator rounds, or which caught fire while carrying DU penetrator
ammunition. In both cases intake may be by inhalation of dust resuspended by the actions of the
person entering the vehicle, and by ingestion through hand-to-mouth transfer.
In Level II it is envisaged that the person is engaged in work on the vehicle (eg recovery of
equipment, repairs etc), while in Level III entry is brief (eg inspection, souvenir hunting). The only
distinction made is the duration of exposure and hence intake, which can be achieved by simple
scaling. As a unit of exposure, 1 hour is considered. In both cases it is assumed that the person
entering the vehicle is unaware of the presence of the DU or of its potential hazard and takes no
precautions to avoid contamination, which may well make the assessment overestimate any future
intakes where gloves and respiratory protection would almost certainly be used.
As for Level I, intakes from a nominal source of DU are calculated below, using clearly defined
assumptions, which may be challenged and changed. The calculations do not rely on any expert
knowledge, but contain referenced data, where appropriate. A worst-case and a more
representative central estimate are assessed. Assessments of occupational internal doses are not
generally made on the basis of surface contamination levels. With regard to inhalation, if clean up
were impractical, then respiratory protection or air sampling would be used in preference. Ingestion
would similarly be controlled by occupational hygiene (clean up or protective clothing, ie gloves).
There appear to be few relevant measurements of contamination levels (surface concentrations in a
vehicle contaminated with DU or air concentrations during entry to such a vehicle). OSAGWI (2000)
and CHPPM (2000) cite Fliszar et al (1989) as the most useful source in this context, but that report
was not available to us.
C3.2 Source termClearly the extent of contamination could vary enormously. The worst-case is easier to consider as it
is simulated in some of the reported trials, ie penetration of heavy armour by a large calibre
penetrator. Penetration of heavy armour results in a large fraction aerosolised, up to about 20%,
but more typically about 5% (table C1), and of that a large proportion (around 50%) is respirable
(CHPPM 2000, annexe G). (Here the term respirable is again used loosely to mean small enough to
be readily resuspended and inhaled, ie less than about 10 m dae
, and not, as usually defined for
occupational health purposes, to mean the fraction of the aerosol that if inhaled could reach the
alveolar region, ie the deep lungs.) Note that very small particles (
-
8/8/2019 The health hazards of depleted uranium munitions (c)
8/23
8
C3.3 Surf ace contamination
The contaminated vehicle is assumed to be a box of dimensions 3 x 2 x 2 m, having a volume of 12
m3and an inside surface area of 32 m
2. Thus for the worst-case the surface concentration is
2000/32 = 62.5 g m2
(= 62,500 mg m2
or 6.25 mg cm2
), and for the central estimate 100/32 =
3.1 g m2 (= 3100 mg m2 or 0.31 mg cm2). Surface concentrations of respirable DU are taken to be
50% of these values.
C3.4 Inhalation
Although not all the DU oxide inside the vehicle will be resuspended by the work being carried out,
it is assumed that material made airborne will be close to the operator and available for inhalation.
One approach is to use a resuspension factor (K), to calculate the air concentration, CA
(mg m3
),
resulting from the surface contamination, CS (mg m2
):
CA
= KCS
(C1)
Resuspension factors have been obtained empirically, but vary enormously according to the type of
surface, dust, time since deposition of the dust, activity, wind etc. A resuspension factor
appropriate to vigorous working on a contaminated surface (ie a relatively high value) is assumed tobe 0.001 m
1(Fish et al 1967, Mitchell and Eutsler 1967). Then:
for the worst-caseCA = 0.001 x 62,500 x 0.5 = 31 mg m3
;
for the central estimateCA
= 0.001 x 3100 x 0.5 = 1.5 mg m3
.
An alternative approach, which is also commonly used in environmental assessments (eg Wilkins et
al 1994, Simmonds et al 1995) is to consider dust loading. This approach assumes that the
radionuclide activity concentration in the airborne dust at a particular location is the same as that in
the surface layer of soil. Thus estimates are made of (i) t he total concentration of dust in the air,
and (ii) the fraction of the airborne dust that is DU. A dust loading of 10 mg m3
is suggested for
estimating individual doses in areas of high resuspension due to man-made activities in the absence
of site-specific data (Simmonds et al 1995, p.47). (However, higher values may arise in arid, dustyenvironments.) In the UK, the Control of Substances Hazardous to Health (COSHH) regulations
define a substance hazardous to health as including dust of any kind when present at a
concentration in air equal to or greater than 10 mg m3
8-hour time-weighted average (TWA) of
total inhalable dust, or 4 mg m3
8-hour TWA of respirable dust. This means that any dust will be
subject to COSHH if people are exposed above these levels. It is considered that in the great
majority of workplaces reasonable control measures will normally keep exposure below these levels.
For comparison, in non-urban areas, the particulate concentration in air is in the range
550 g m3, and in large industrial areas it can range between 100800 g m3 (Wilkins et al
1994).
For the worst-case, assume dusty air (10 mg m3), and 100% DU, giving 10 mg DU m3.
For the central estimate, assume a dust loading intermediate between dusty and ambient, ie 1 mg
m3
, and 50% DU, giving 0.5 mg DU m3
.
This approach gives values somewhat lower, but broadly consistent with the resuspension
approach. Hence, take as rounded values 10 mg DU m3
and 1 mg DU m3
, for worst-case and
central estimate, respectively. To estimate intake rates (mg h1
), these concentrations are
multiplied by breathing rates (m3
h1
). ICRP (1994a, table 6) defines light work on the basis of a
working day of 5.5 hours light exercise and 2.5 hours sitting, with an average breathing rate of 1.2
-
8/8/2019 The health hazards of depleted uranium munitions (c)
9/23
9
m3
h1
, and heavy work on the basis of a working day of 7 hours light exercise and 1 hour heavy
exercise, with an average breathing rate of 1.7 m3h
1. Light work is assumed for a reference worker
for whom dose coefficients are calculated (ICRP 1994b). As rounded values, take 2 m3
h1
as the
worst -case and 1 m3
h1
as the central estimate, giving intake rates of 20 mg h1
, and 1 mg h1
,
respectively.
C3.5 Ingestion
This intake is also estimated for working in a contaminated vehicle on an hourly basis. The first
approach is the methodology described in CHPPM (2000, pp. F10-13). It uses an effective transfer
rate of loose removable DU surface contamination (104
m2h
1), which assumes the area of the
palms of both hands is 0.042 m2. For a worst-case of vehicle surface contamination (2 kg over 32
m2
= 62.5 g m2
), the hand to mouth transfer = 62.5 x 104
g h1
, ie 6 mg h1
. For the central
estimate of vehicle surface contamination (0.1 kg over 32 m2
= 3.1 g m2
), the hand to mouth
transfer = 3.1 x 104
g h1
, ie 0.3 mg h1
.
An early approach (Dunster 1962) to assessment of surface-to-hand-to-mouth transfer in areas that
were not identified as being contaminated with radioactive material was to make the cautious
assumption that a person might ingest all the contamination from 10 cm2
(the approximate area ofthe fingert ips) of surface per day. Scaling to one hour, it is assumed that the subject ingests all the
contamination from 1 cm2
per hour. (This is the same as the transfer rate above: 104
m2
h1
.) On
this basis, intake rates by ingestion would be 6 mg h-1
(worst-case) and 0.3 mg h-1
(central estimate)
respectively. Another approach used is to apply habit data that are used for general radiological
assessment purposes for members of the public (Robinson 1996). Although they were intended
mainly for outdoor exposures, they have also been used for occupational exposures (eg Penfold et
al 1997, p C6). Rates for inadvertent ingestion of soil and sand by an adult are 10 mg d1 (average)
and 30 mg d1
(critical group), ie about 1 and 3 mg h-1, respectively. These values were based on
studies conducted on children aged 6 months to 5 years and extrapolated assuming an exponential
decrease with age up to 18 years. Values assumed for children range up to 100 mg d1
(average)
and 300 mg d
1
(critical group), for a 1-year-old. WHO (1994) uses a similar value of 20 mg soil d
1
ingested by adults when site specific data are unavailable. On this basis, intake rates by ingestion by
adults would be 3 mg h-1
(worst-case, assuming 3 mg h-1
and 100% DU) and 0.5 mg h-1
(central
estimate, assuming 1 mg h-1
and 50% DU). However an hourly rate for adults spending a small
fraction of the year at a particular location is given as 5 mg h-1. The three approaches give broadly
consistent results. Take as a central estimate 0.5 mg h-1, and as a worst-case 5 mg h
-1.
Table C4. Summary of Level II exposure rates for entry into contaminated vehicles (mg h-1)
Central estimate Worst-case
Inhalation 0.1 20Ingestion 0.5 5
C3.6 Measurements made on soldiers involved in Level II incidents in the Gulf War
As for Level I, it is possible to make an assessment based on a small number of measured excretion
rates. OSAGWI (2000 Tab J) describes four accidental tank fires. The fourth (section D, April 13,
1991) is significant in that the crew had urine samples collected at the time, the only reported urine
-
8/8/2019 The health hazards of depleted uranium munitions (c)
10/23
10
samples measured for uranium directly after exposure in the Gulf War. (The next were in 1992, see
below.) The following account is given.
Tank A31 was being towed by another tank (A32), when several rounds of its ammunition exposed
to the heat of A-32s exhaust suddenly blew up A-31 was allowed to burn out and recovery
operations began the next day. A-31 had 24 DU sabot rounds, and the propellant charges on all of
them had ignited. All 24 penetrators were located. The tank commander indicated that while they
showed signs of having been exposed to significant heat from the fire, he did not notice any
appreciable reduction in their size. The DU armour was intact.
On April 14, a three-man AMCCOM RADCON team arrived. DU penetrators and high explosive
rounds lay on the ground around the tank. Crew members had been working on the tank, in the
ammunition compartment, and on the ground around the tank. The RADCON team confirmed
alpha contamination on the ground beside the tank, on the tanks front surface, and on the inside
and top of the ammunition compartment. One RADCON team member stated people were hip
deep in DU. The team found DU contamination on several crew members hands and one crew
members coveralls. One crew member had radiological contamination in an open wound.
Seven soldiers who worked around A-31 provided urine samples for uranium evaluation on April
15, 1991. The samples subsequently were shipped to Germany and on to the Armys
Environmental Hygiene Agency (now USACHPPM) for analysis. All the samples were below the
method detection levels of 2.0 g/l, which is below the action level for class D and W compounds
in the Health Physics Society standard, HPS N13.22-1995, Bioassay Programs for Uranium, An
American National Standard.
To obtain an upper estimate of their intakes, assume that the measurements were made at 2 days
after intake and that the amount of DU being excreted was 2.0 g per day. Table C5 gives the
predicted excretion rate following inhalation of 1 gram DU, for default type M and default type S
uranium inhaled by a reference worker (as in ICRP publication 78), and for the central estimateparameter values for Level II exposure to aerosol resuspended inside vehicles (table 15 of appendix
1). Table C5 also gives the relevant input parameter values.
For an intake of 1 mg by inhalation, the daily urinary excretion predicted at 2 days is:
for type M uranium, 1.1 g; hence 2.0 g per day corresponds to an intake of ~2 mg;
for type S uranium, 0.044 g; hence 2.0 g per day corresponds to an intake of ~45 mg;
for central estimate aerosol, as described in table 15 of appendix 1, 3.3 g; hence 2.0 g per
day corresponds to an intake of ~1 mg.
-
8/8/2019 The health hazards of depleted uranium munitions (c)
11/23
11
Table C5. Predicted urinary excretion rates follow ing inhalation of 1 gram DU for Level II
inhalation (table 14), and for reference occupational exposure to t ype M and t ype S
uranium aerosols. Relevant input parameter values are also given.
Type M Type S Level II inhalation
(table 14)
Input parameter
Subject exercise level Light work Light work Heavy work
AMAD,m 5 5 5GSD 2.5 2.5 2.5
Density , g cm3 3 3 9Rapid dissolution fraction, f
r0.1 0.001 0.2
Rapid dissolut ion rate, sr, d1 100 100 1
Slow dissolution rate, ss, d1 0.005 0.0001 0.001
Gut uptake factor, f1
0.02 0.002 0.002
Urinary excretion rate, g d1
2 days 1100 44 3000
365 days 22 2.6 15
730 days 3.2 1.9 8.0
These are not inconsistent with the Level II inhalation assessments above (central estimate 0.1 mg
h1
, worst-case 20 mg h1
) assuming 110 hours exposure. OSAGWI 2000 (Tab P) also records that a
follow-up programme (separate from that on the friendly-fire victims) was initiated in 1992 to
evaluate the exposures of the 144th
Service and Supply Company, the unit that operated the
damaged equipment yard at King Khalid Military City. About 27 members of this unit were
exposed to DU for several weeks before being informed that some of the equipment was
contaminated. Twelve were evaluated in 1992. All underwent whole-body counting and 8 of the
12 also u nderwent urine testing. The tests showed no residual body-burdens of DU above
background levels . In 1993, thirteen members of the 144th
also provided urine samples to the
CHPPM. Both USACHPPM and the Environmental Measurements Laboratory of New York, New
York analysed these samples. Uranium levels were within normal background levels. However,
these measurements do not seem to have been published elsewhere. The limits of detection are
not given, nor the times between potential intakes and measurements, and so upper levels on
intakes and doses cannot readily be assessed. For the purposes of this assessment, assume that the
detection limit was similar to that used for the tank crew above, so that an upper limit on the DU
excretion rate is about 2.0 g per day. For the central estimate exposure an intake of 1 gram would
give an excretion rate of about 10 g per day at 1 -2 years after intake (table C5). Hence an
excretion rate of 2 g per day would correspond to an intake of ~200 mg. Assumption of default
type M and type S exposures leads to lower predicted excretion rates, down to about 2 g per day
per gram inhaled, and hence leading to an upper limit on intake of about 1 gram. The limit of
detection may have been lower than 2 g litre1
; Hooper et al (1999) reported measurements below
0.1 g litre1 made in 1993/4. In that case upper limits on intake would have been correspondingly
lower.
C4 Level III exposures
As noted in section 2.2 of appendix1 Battlefield exposure pathways, consideration is given to five
pathways: ingestion by hand to mouth transfer in contaminated vehicles, and inhalation of four
types of aerosols:
-
8/8/2019 The health hazards of depleted uranium munitions (c)
12/23
12
plume from impact;
plume from fire;
resuspension within contaminated vehicle;
resuspension from contaminated ground.Two of these (ingesti on by hand to mouth transfer in contaminated vehicles, and resuspension
within contaminated vehicles) were considered in the previous section (table C4).
C4.1 Inhalation of smoke plumes from impacts and fires
Because there was little useful information from the reports on DU penetrator trials, a modelling
approach was used. Such an approach was taken by Fetter and von Hippel (1999) to assess both
individual and population doses. Their methodology is critically reviewed in this section. Comments
have been restricted to specific aspects of their report, most notably the calculation of intakes and
radiation doses to the public from the atmospheric dispersal of DU. Intakes and radiation doses
from non-accident pathways have not been considered, nor has any treatment of chemical toxic
dose.
Critique of methodology used by Fetter and von Hippel (1999)
The critique includes independent verification of the results using the US dispersion modelHOTSPOT, and comparison against the AWE nuclear accident dispersion model DIFFAL, where
appropriate.
HOTSPOT (Homann 1999) is a US Gaussian model developed at Lawrence Livermore National
Laboratory (LLNL). It is very similar to the model described in report NRPB-R91 (Clarke 1979) with a
slightly different description of the standard deviations of cloud width and depth. The model also
includes pre-dispersion processing that modif ies the initial geometry of the release, and a post-
processing element that converts the raw dispersion output values into radiation dose estimates,
based on ICRP publication 30 dosimetry (ICRP 1979).
DIFFAL, the AWE dispersion model, is also a simple Gaussian model, but includes gravitational
sett ling as a dispersing mechanism. It also has similar pre- and post -processing components to
HOTSPOT. The det ails of the geometries and parameters are somewhat different however, and
these differences will be further described where pertinent to the comparison.
Although the dosimetry used in the report has not been reviewed in any great detail, where AWE
has default dosimetry factors relevant to the paper, they have been compared and contrasted with
those in the report.
Fetter and von Hippel (1999) estimate radiation and chemical toxicity intakes to individuals and
populations in the Gulf War. As the vast majority of DU ammunition expended in the Gulf War was
of US origin, the isotopic composition for DU has been assumed to be as stated by Fetter and von
Hippel. The composition assumes only uranium-234, -235, -236 and -238 isotopes. No plutonium
or fission products were assumed to be part of the composition (annexe D, section D2).
Individual intake
For impacts of DU ammunition against hard targets, Fetter and von Hippel assume that some of the
kinetic energy of the shell is converted into heat energy available for buoyant rise, and the energy
equated to a TNT equivalent explosive release. Exposures (time-integrated concentrations) for
explosive releases with varying high explosive (HE) masses (accounting for different ammunition
types and kinetic energy transfers) are calculated giving cloud top heights up to approximately
-
8/8/2019 The health hazards of depleted uranium munitions (c)
13/23
13
100 m.
AWE has no experimental data on release fractions for DU ammunition impacting against hard or
soft targets. Therefore release fractions for these scenarios are used directly from the Fetter and
von Hippel report.
In Fetter and von Hippel (1999), the smouldering and hot fires used to estimate the radiation
dose from burning of munitions at the ammunition store at Doha in Kuwait produces effective
release heights under 10 m. These values are low since the area over which the fire is spread, a
radius of 50 m, is relatively large. However, the calculations will produce fairly conservative results
due to this.
The reported 0.025% released and the respirable fraction for the DU fire is not inconsistent with
experimental data.
Using the HOTSPOT model with parameter values suitable for impacts and fires as described by
Fetter and von Hippel, it is easy to reproduce the figures published in tables 5 and 6 of their report.
To compare and contrast the results for impact and fire, the AWE dispersion model DIFFAL was alsorun using identical parameters where sensible and possible. It was not always possible to match the
parameters identically as some are calculated within the code itself, and are not available for
alteration by the user.
For the explosive releases in typical weather conditions, DIFFAL and HOTSPOT agree very well, there
being a factor of 2 3 difference at most.
For the explosive releases in worst -case weather conditions, DIFFAL and HOTSPOT dif fer somewhat,
the ratio of the DIFFAL result to the HOTSPOT result increasing with distance and reaching an order
of magnitude at approximately 10 kilometres. This difference is explained partly by the different
source geometries and dispersion parameters assumed by the two models, but mostly due todifferent deposition velocities. Fetter and von Hippel use the HOTSPOT default deposition velocity
value of 1 cm s1
whereas DIFFAL calculates a deposition velocity based on the gravitational settling
velocity as determined by the particle size. This results in smaller deposition velocities for the
aerosol in DIFFAL leading to increased exposures further downwind.
Running the HOTSPOT code with the scenarios as described above, but replacing the 1 cm s1
deposition velocity by 0.1 cm s1
, a value commonly used in the UK for 1 m AMAD particulate,
increases the longer-range exposure to values comparable to DIFFAL.
DIFFAL results for the explosive releases are summarised in table C6. The HE equivalent, W, in table
C6 has been converted from lbs in the Fetter and von Hippel paper to kgs, but the quantit ies are
the same.
The same differences are reflected in the fire scenarios, to a greater degree because the effective
cloud heights for the two cases of smouldering and hot fires are much lower than those calculated
for the explosive releases and hence deposition velocity is a greater factor. Also the DIFFAL
geometry assumes a greater amount of material nearer the ground and a much smaller initial
vertical spread. The latter factor accounts for the main difference at short ranges and especially in
the worst-case weather condit ions. The result is that DIFFAL predicts exposures orders of
-
8/8/2019 The health hazards of depleted uranium munitions (c)
14/23
14
magnitude greater at the shorter ranges becoming less signif icant at longer distances, especially
when the DIFFAL effective height is raised slightly or the HOTSPOT deposition velocity is decreased.
Table C6. Individual DIFFAL inhalation estimates (in micrograms) for an explosiverelease of 1 kg respirable material
Worst-case weather Typical weatherDistance(km)
W=0.013 kg W=0.13 kg W=1.3 kg W=0.013 kg W=0.13 kg W=1.3 kg0.1 6.8x10
21.8x10
25.4x10
12.4x10
18.2x10
02.7x10
0
0.2 6.4x102
1.8x102
5.8x101
2.1x101
7.5x100
2.5x100
0.5 5.2x102 1.6x102 5.6x101 1.4x101 5.7x100 2.1x100
1 3.5x102
1.3x102
5.0x101
6.8x100
3.8x100
1.6x100
2 1.4x102
8.7x101
3.9x101
2.2x100
1.6x100
9.6x10-1
5 2.6x101
2.3x101
1.7x101
3.8x10-1
3.3x10-1
2.6x10-1
10 6.5x100
6.2x100
5.3x100
9.6x10-2
8.5x10-2
7.3x10-2
W = High Explosive equivalent (kg of TNT)
To illustrate this, replacing the 1 cm s1
deposition velocity by 0.1 cm s1
in the HOTSPOT code
increases the longer-range exposure values up to nearly two orders of magnitude in the case of theworst -case weather and smouldering fire.
DIFFAL results for a fire are shown in table C7.
Table C7. Individual DIFFAL inhalation estimates (in micrograms) for fire release of 1 kgrespirable material
Worst-case weather Typical weather
Distance (km) Smouldering Hot Smouldering Hot
0.1 5.2x103
8.6x102
3.1x102
2.1x102
0.2 2.6x103
8.2x102
1.2x102
1.1x102
0.5 7.8x102
6.2x102
2.6x101
2.9x101
1 2.7x102 3.0x102 7.1x100 8.4x100
2 7.9x101
1.0x102
1.8x100
2.2x100
5 1.3x101
1.8x101
2.6x10-1
3.5x10-1
10 3.0x100
4.3x100
5.7x10-2
8.0x10-2
Collective dose
(The following discussion of collective doses forms part of the review of the models used by Fetter
and von Hippel. The collective doses are not used in the assessment.) The collective effective dose is
a quantity defined by ICRP which can be regarded as representing the total consequence (in terms
of radiation risks) of the exposure of a population (ICRP 1990). It is obtained by multiplying the
average dose to the members of the exposed population by the number of people in that
population. It thus has the unit man sievert (man Sv). Its use is limited to situations in which the risk
to an individual is proportional to the dose, which is generally regarded as reasonable at low doses.
In effect it relies on the assumption that, for example, a dose of 1 mSv to 1,000 people would
theoretically induce the same number of cancers as 10 mSv to 100 people. In each case the
collective dose is 1 man Sv. (The associated risk, assuming a risk of fatal cancer in an individual of
5% Sv1
would be 0.05, ie a 1 in 20 chance that 1 cancer would be induced.)
-
8/8/2019 The health hazards of depleted uranium munitions (c)
15/23
15
Using the default AWE ground shine (external irradiation from activity deposited on the ground)
dosimetry factor of 8.5 x 1019
(Sv s1
)/(Bq m2
) with no decrease due to weathering, tilling or
decontamination, and assuming that there are 300 tons of DU dispersed over an area with an
average population density of 50 km2
, then over 50 years the collective dose would be:
Collective dose = (3.0 x 105) x (1.4 x 107) x (8.5 x 1019) x (1.58 x 109) x 50 x (1 x 106) = 0.3 man Sv
This can be compared to the value of 2 man Sv as calculated by Fetter and von Hippel (1999).
Fetter and von Hippel calculate a collective inhalation dose using a simple atmospheric dispersion
model known as a wedge model, and a uniform population density. The late cancer fatality model
used in the report is identical to that used in DIFFAL. The results were compared and contrasted
against DIFFAL, the AWE dispersion model. Population densities as defined in the report seem
reasonable when compared against data available at AWE.
Collective dose from inhalation of the primary cloud in DIFFAL is calculated as:
Collective dose = i
ii Nd (C2)
wheredi is the inhalation dose received by a population of Ni persons.
Further, the inhalation dose di
= Cibdf (C3)
whereCiis the time-integrated concentration,bis the breathing rate and dfis a dosimetry factor
suitable for DU.
Assuming that the population has a constant density value of , then
Ni= A
i (C4)
whereAi is the area associated with a population receiving the dosedi
Then collective dose = b df i ii AC (C5)
Assuming the Fetter and von Hippel source term of 3.0 x 104
kg DU (10% of 300 tons), breathing
rate 3.3 x 104
m3
s1
, population density of 50 km2
and a default DIFFAL dosimetry factor of 8.0 x
106
Sv Bq1
(similar to the 1 m AMAD insoluble value in the report), Cican be calculated using a
single DIFFAL run, say an explosive release in typical meteorological conditions. This results in a
calculated collective dose of 0.6 man Sv, a figure within the range calculated by Fetter and von
Hippel, from 0.4 to 200 man Sv (4020,000 person-rem). The value at the upper end of this range
assumes conservative dosimetry (approximately a factor of two greater than the DIFFAL default
value), a higher release fraction and a smaller deposition velocity.
Fetter and von Hippel then go on to calculate radiation dose from inhalation of resuspended
material. The default resuspension factor used in the DIFFAL model is identical to the second
resuspension factor mentioned by Fetter and von Hippel up to 1000 days after deposition, but does
not remain constant thereafter as it does in the report. However, the result is that the Fetter and
von Hippel 50 year integrated resuspension factor is only a factor of 2 greater than that used in
DIFFAL. DIFFAL also contains an older resuspension model, described in NRPB-DL10 (Linsley et al
1986). Again, Fetter and von Hippel calculate the collective radiation dose from inhalation of the
resuspended material using the wedge model. An even simpler calculation can be performed
-
8/8/2019 The health hazards of depleted uranium munitions (c)
16/23
16
assuming that all of the 30 tonnes of DU is deposited on the ground and available for inhalation via
resuspension. Assuming the same dosimetry factors and population density as used in the
calculation of collective dose from inhalation of the primary cloud with a range of Fetter and von
Hippel integrated resuspension factors (2 to 800 s m1
), then it is easy to calculate a collective dose
from 0.1 to 45 man Sv, somewhat less than the reported 0.3 to 140 man Sv. Using the same
parameters, but replacing the integrated resuspension factors with those used within the DIFFAL
model (1 to 10 s m1), the collective dose ranges from 0.06 to 0.6 man Sv.
Collective dose estimates from Fetter and von Hippel and DIFFAL are summarised in table C8.
Table C8. Collective dose estimatesa
Scenario Mass(tonnes)
Dosimetry Resuspension(s m
-1)
Collective Dose(man Sv)
Ground shine
Fetter and von Hippel 300b
7.2x10-18
(Sv s1
)/(Bq m2
)c
- 2d
DIFFAL 300 8.5x10 -19 (Sv s1)/(Bq m2) - 0.3
InhalationFetter and von Hippel 30
e1.4x10
-61.4x10
-5Sv Bq
1(f)
- 0.4200g
DIFFAL 30 8x10-6
Sv Bq1
- 0.6
Resuspension
Fetter and von Hippel 30 6x10-6
Sv Bq1
2800 0.3140
DIFFAL 30 8x10-6
Sv Bq1
110 0.060.6
a Population density 50 km-2; Fetter and von Hippel (1999) DU specific activity of 1.4 x 107 Bq kg-1b 11,000 tank rounds5 kg + 800,000 A10 rounds 0.3 kgc Equivalent to 1.3 mrem y1 per tonne of DU per km2
d Collective dose for a year 10 to account for contamination being heaviest in remote arease 300 tonnes 20% conversion into respirable aerosol given a strike on a hard target 50% of rounds hitting a
hard targetf Assuming different uranium solubilities and particle sizesg Assuming different uranium solubilities and deposition velocities from 0.002 to 0.05 m s1
Assessed Level III intakes for inhalation of plumes
As discussed above, assessments made by Fetter and von Hippel (1999) were checked and appear
satisfactory, and are therefore used for these inhalation pathways. Tables C9 and C10 give intakes
calculated by Fetter and von Hippel for a person breathing at 3.3 x 104
m3s1
(1.2 m3
h1
), directly
downwind of a release of 1 kg DU, from impacts and fires respectively. Central estimate and worst-
case values from these tables are given in table C10.
For impacts:
central estimate take typical weather and an intermediate explosive yield;
worst-case take the highest values in table C9.
For fires:
central estimate take typical weather and rounded average of smoking and hot fires the
results are similar for the two cases;
worst-case take the highest values in table C10.
-
8/8/2019 The health hazards of depleted uranium munitions (c)
17/23
17
Table C9. Estimated DU inhaled (micrograms) for an individual directly dow nw ind f rom
release of 1 kg respirable DU generated by explosive impacts (Fetter and von Hippel 1999)
Worst-case weathera
Typical weatherb
Distance
(km) W=0.013 kg W= 0.13 kg W=1.3 kg W=0.013 kg W=0.13 kg W=1.3 kg
0.1 200 59 18 54 22 8.4
0.2 120 42 13 32 15 5.90.5 54 22 7.4 11 6.9 3.4
1 26 12 4.5 4.3 3.2 1.9
2 8.8 5.4 2.3 1.5 1.3 0.93
5 1.4 1.3 0.74 0.4 0.36 0.30
10 0.32 0.37 0.30 0.15 0.14 0.13a Class F stability, 1 m s-1 wind speed, 250 m mixing heightb Class D stability, 5 m s-1 wind speed, 1000 m mixing heightW = High Explosive equivalent (kg of TNT)
Table C10. Estimated DU inhaled (micrograms) by an indiv idual directly dow nw ind f romrelease of 1 kg respirable DU generated by a fire (Fetter and von Hippel 1999)
Worst-case weathera Typical weatherb
Distance (km) Smouldering Hot Fire Smouldering Hot Fire
0.1 25 54 11 14
0.2 16 44 7.9 10
0.5 6.9 25 3.8 4.9
1 3.1 13 1.8 2.4
2 1.1 4.6 0.79 0.98
5 0.18 0.79 0.23 0.30
10 0.04 0.16 0.09 0.12
a Class F stability, 1 m s-1 wind speed, 250 m mixing heightb Class D stability, 5 m s-1 wind speed, 1000 m mixing height
Table C11. Central estimate and worst -case estimates of DU inhaled (micrograms) by an
individual directly dow nw ind f rom release of 1 kg respirable DU generated by explosive
impacts or fi res
Central estimate Worst -case
Distance (km) Impacts Fire Impacts Fire
0.1 22 13 200 54
0.2 15 9.0 120 44
0.5 6.9 4.4 54 25
1 3.2 2.1 26 13
2 1.3 0.89 8.8 4.6
5 0.36 0.27 1.4 0.7910 0.14 0.11 0.32 0.16
C4.2 Resuspension from contaminated ground
The procedure used was (a) to estimate the initial surface concentration resulting from a battle and
(b) to apply an appropriate resuspension factor (K) and a dust loading approach to assess intakes
resulting from unit ground surface concentration. The latter will depend on the material, the
-
8/8/2019 The health hazards of depleted uranium munitions (c)
18/23
18
surface, activities taking place and the weather. Uncertainties associated with estimates of
resuspended air concentrations are large, and are discussed later.
Initial surface concentration
AMCCOM (1990) postulated a major tank battle scenario in which 600 5-kg penetrators are fired
and 25% aerosolised (750 kg DU), which is spread over 50 hectares (500,000 m2) giving a surface
concentration of 1.5 g m2
(annexe F, section F1).
Fetter and von Hippel (1999) considered 1000 kg DU per square km (1,000,000 m2) as a reasonable
upper limit for a battlefield area, giving a surface concentration of 1 g m2
.
UNEP (1999) proposed a hypothetical scenario in wh ich 3 aircraft attack a few vehicles, resulting in
10 kg DU spread over 1000 m2, giving a surface concentration of 10 g m
2.
OSAGWI (2000) Tab H notes that A-10 pilots usually fire a 23 second burst, which at 6000 rounds
per minute means 200300 rounds. At 0.3 kg per round, this gives about 60100 kg used in an
attack. Since most rounds (~90%) probably would not hit armour, only about 1% would be
dispersed, giving about 1 kg of dust. If the aircraft flies at 800 km h1
, ie about 200 m s1
, it travels
about 500 m during the attack. The rounds might therefore be dispersed over an area of about
500 x 10 m, ie about 5000 m2. If 1 kg is dispersed over this area, the initial concentration is
0.2 g m2
.
CHPPM (2000, appendix M) postulates a theoretical tank batt le scenario similar to that in
AMCCOM (1990). It is assumed that 300 4.7-kg penetrators hit tanks and 35% of the DU is
aerosolised (490 kg), which is spread over 50 hectares, giving a surface concentration of ~1 g m2
.
Doses are assessed for a 1-hour exposure within the area and before any rain (resuspension factor
104
m1
) and for a 5-day exposure at distances 0.1100 km downwind of a 50 m radius
contaminated area.
Taking these together, an initial surface concentration of 1 g DU m2 is assumed here.
The scenario
It is assumed that:
soldiers spend 4 weeks in an area, starting from the time it is contaminated with 1 g m -2 DU;
all the DU is respirable;
the soldiers activities cause enhanced resuspension of the DU owing to normal heavy vehicle
movements, but the soldiers are not undertaking digging, ploughing or clearance operations.
The central estimates assume UK-like conditions and soldiers with breathing rates typical of average
European adults engaged in a general range of activit ies. The worst -case estimates assume arid,
dusty conditions and soldiers with enhanced breathing rates during the working day. Estimates
were made for intakes over each one-week period during the 4-week exposure.
Resuspension factor approach
The resuspension factor, K, is defined as:
)mg(depositsurfaceofionconcentrat
)m(gonresuspensitodueairinionconcentrat)(mK
2
-31-
= (C6)
This is a convenient way of expressing the observed relationship between surface and air
-
8/8/2019 The health hazards of depleted uranium munitions (c)
19/23
19
concentrations, but with a number of limitations. There is an implicit assumption that the measured
airborne concentration originates solely from an area local to the surface sampling position. In
practice, the airborne contamination at any location will include resuspended material from a range
of upwind sources, which may be contaminated at varying levels. Also, reported resuspension
factors tend to be t ime averaged. They may give erroneous predictions of instantaneous air
concentrations, for example, in conditions when there is little or no wind or other disturbances. K
has the drawback that it must depend on the variation of the surface deposit with distance from
the point of measurement. The value of Kwill depend also on the depth of surface material
sampled in order to determine surface contamination. Since the processes of transfer up into the
atmosphere and down into the soil are poorly understood there is no obvious basis for choice, and
some of the variations in the values of Kreported in the literature might be due to the adoption of
different sampling depths.
A variation of resuspension rate with particle size wo uld be expected because aerodynamic lift
force will increase with wind speed and particle area. A change in chemical form of contaminant
may have the effect of increasing or decreasing the effective size distribution of the contaminant.
Chemical form may also dictate whether particles remain unattached, or attach to host material,
effectively increasing their aerodynamic diameters. However, the magnitude of variations in Kdueto particle size and chemical form has not been quantified in the literature and has not been
modelled here. For these estimations of intake, the assumption has been made that all the
deposited material is resuspended equally, and that it is all of a respirable size.
Garland (1979, 1982) carried out studies on grassland and bare soil at controlled wind speeds in a
wind tunnel, and found that an inverse power law fitted his wind tunnel data for experiments
which ran for times varying from several minutes to a number of months. Nevertheless, the Garland
resuspension factor has been applied to Chernobyl data and has been found to be a good fit
(Garland 1992, Garger 1997)even 8 years later, although in one of these studies (Garger 1997),
which examined data up to 1994, the Garland factor tended to overestimate by up to one order of
magnitude. The Garland resuspension factor is given by:
K(t)=1.2 x 10-6
t-1
m-1
(C7)
where tis the time after deposition in days.
Integrated resuspended air concentrations were calculated using the following formula:
=2
1
t
tairdtdepositsurfacex(t)KC (C8)
where:
Cair
is the integrated air concentration due to wind driven resuspension. Resuspension can be
divided into two types: wind-driven and mechanical or anthropogenic. Wind-driven resuspension
assumes that the only disturbance to the surface is as a result of natural weathering while
mechanical resuspension includes mechanical disturbances by pedestrians or vehicles and
agricultural operations (taken into account using Rscale
, see below);
t1
to t2is the period of integration;
K(t) is found from equation (C7);
the surface deposit is assumed to be 1 g m-2
;
average resuspended air concentrations and calculated time-integrated air concentrations are given
-
8/8/2019 The health hazards of depleted uranium munitions (c)
20/23
20
in table C12.
Table C12. Weekly average, and t ime-integrated resuspended air concentrat ions
calculated using the resuspension approach
Integration Time
Average air concentration
(g m-3
per g m-2
)
Integrated air concentration
(g s
m-3
per g m-2
)
0 to 6 days 3.6 x 10-7 2.2 x 10-1
7 to 13 days 1.1 x 10-7 6.5 x 10-2
14 to 20 days 6.4 x 10-8
3.9 x 10-2
21 to 27 days 4.8 x 10-8
2.9 x 10-2
The soldiers integrated intake of DU was calculated using the following formula:
IntakeDU
= [Cair
x Iinh
x Rscale
x (1-Occrate
)] + [Cair
x Iinh
x Rscale
x Occrate
x I/O] (C9)
where:
Iinh is the inhalation rate (24-hour average), as recommended by the International Commission onRadiological Protection (ICRP 1994a);
Rscale is the scaling factor for resuspension. Because the air concentrations have been calculated for
wind-driven resuspension in UK conditions, a scaling factor must be applied to scale for desert
conditions and for mechanical resuspension;
Occrate is the indoor occupancy, assumed to be 50%, ie the outdoor worker value from habit
surveys (Robinson 1996), for both the central estimate and worst-case;
I/O is the indoor:outdoor concentration ratio to scale indoor:outdoor concentrations by outdoor
concentrations. It is known that small particles can penetrate effectively into buildings, and the
degree of equi librium between indoor and outdoor air is dependent on particle size. Because, in
this study, the range of particles sizes which can be resuspended spans the full range of respirable
particle sizes, a value of 0.5 is chosen for both the central estimate and worst-case, on the basis ofa dose conversion factor suggested in Brown (1989). This is strictly applicable to active sheltering
for limited periods. However, given the uncertainties on the resuspension factor adopted, the
uncertainty associated with thi s reduction factor is considered unimportant.
Central estimate
Iinh
: outdoor worker rate = 2.92 x 10-4
m3s
-1.
Rscale: UK conditions, mechanical resuspension. Linsley (1978)recommended that in conditions of
moderate activity (regular disturbance of the surface by vehicles or pedestrians) a resuspension
factor of 10-5
m-1
may be more applicable. Hence Rscale = 10.
Worst -case
Iinh:heavy worker rate = 3.10 x 10-4
m3s
-1.
Rscale
: desert conditions, high mechanical resuspension. Because it has been suggested (Cohen 1977)
that humidity would be likely to reduce resuspension, a higher resuspension factor is assumed in
desert conditions. Also, because it is assumed in the worst -case that the soldiers are working in an
area close to heavy vehicular movement, high mechanical resuspension needs to be considered.
Rscale was taken to be 100 on the basis of measurements of Stewart (1964) in Australia. These
measurements were made on the Maralinga test site, 0.3 m from a moving vehicle. The
resuspension factors quoted ranged from 5.0 x 10-7
m-1
to 1.0 x 10-3
m-1, and so by using R
scale=
100, the effective resuspension factor used is 1.2 x 10-4
m-1.
-
8/8/2019 The health hazards of depleted uranium munitions (c)
21/23
21
The soldiers estimated intakes of resuspended DU are given in table C13.
Table C13. Intake of resuspended DU using the resuspension factor approach
Intake (mg)
Integration time Centralestimate
Worst-case
0 to 6 days 0.47 5.07 to 13 days 0.14 1.5
14 to 20 days 0.085 0.9
21 to 27 days 0.064 0.68
Total 0 to 27 days 0.8 8
Dust Loading Approach
The dust loading or equivalent soil concentration approach can also be used to relate the
concentration of a radionuclide in soil to that in the air. The resuspended air concentration can be
expressed as:
Ca (g m-3) = Cs (g kg
-1) SE (kg m
-3) (C10)
where Ca
is the estimated concentration of the radionuclide in air, Csis the concentration in soil
(g of DU per kg of soil) and SE is the equivalent soil concentration or dust-loading in air.
There are recognised dif ficulties using the dust-loading approach. The soil concentration is
expressed in terms of g kg1
, or Bq kg1
. As measurements are generally reported as g m2
or Bq m2
,
knowledge of the depth of contamination is required. For fresh deposits, it is diff icult to define the
depth of the layer of surface soil and this will change with time. Most measurements and estimates
given in the literature relate to aged deposits. This implies that the radionuclide is closely associated
with the soil and so therefore not necessarily appropriate for use with fresh d eposits. It is assumedthat the contaminant and soil are resuspended equally, which will not be the case for many soil
types. Vegetation cover is another important controlling factor in resuspension, and many dust-
loading measurements have been made on land with sparse vegetative cover. There is no time
dependence modelled; account is not taken of loss of activity through weathering. To model the
transport of radionuclides in the soil, a compartmental soil model was set up, using a generic
undisturbed soil model (Brown 1995). This is based on migration in soil for a limited number of
elements, particularly plutonium, caesium and strontium. The rate of movement into the soil of
these elements is slow, although there is significant variation between the results of the various
observations owing to differences in soil composition and annual rainfall. The soil model consists of
four compartments or boxes, representing soil depths of: 01, 15, 515 and 1530 cm. There
are rate constants to express transfer between boxes, and losses from boxes. Resuspension is
assumed to occur only from the top 1 cm of soil, iethe top box in the model.
To calculate the concentration of DU in the top box at time zero, following deposition of
1 g DU m2
in unit area (1 m2), i t is assumed that the DU is uniformly distributed in the top box. The
volume of the top box (with dimensions 1 m x 1 m x 0.01 m) = 0.01 m3, and therefore the density
of DU in the top box = 102
g DU m3
.
It is assumed that the density of soil (generic dry soil) = 1.25 g cm3
= 1.25 x 102
kg m3
, and
-
8/8/2019 The health hazards of depleted uranium munitions (c)
22/23
22
therefore the concentration of DU in the top box = 8.0 x 102
g kg1
(ie g of DU per kg of soil). The
time-integrated concentration of DU in the top box (ie the layer of soil available for resuspension)
Csoil
, over a week is therefore 4.83 x 104
g kg1
s. The model predicts a negligible change in Csoil
over
the f irst four weeks.
The integrated air concentration due to resuspension is defined as:
Cair (g m-3
s)=Csoil (g kg-1
s) x SE (kg m-3) (C11)
where SE
is the dust loading. The integrated intake of DU can then be calculated from:
IntakeDU
= [Cair
x Iinh
x (1-Occrate
)] + [Cair
x Iinh
x Occrate
x I/O] (C12)
where the parameters Iinh and Occrate have the same values as for the resuspension factor approach
above.
Central estimate
For UK conditions, and soldiers carrying out a range of activities, SE
= 100g m-3 = 1.0 x 107 kg m-3
as used by Wilkins et al 1994 as a reasonably cautious dust-loading. Hence over one week, Cair
=
4.8 x 103
g sm
-3, and the intake = 1.1 x 10
3mg DU.
Worst -case
For desert conditions and vehicular movements, SE = 30,000g m-3
= 3.0 x 10-5
kg m-3
based on
measurements from the Maralinga and Emu nuclear test sites in Australia (Haywood and Smith
1990) which quoted values of SE from 370 to 65,000 g m-3
for sitting in or near a moving vehicle.
A value mid-range is assumed, as the soldiers will not spend 24 hours a day close to the vehicles.
Hence over one week, Cair = 1.4 g sm
-3, and the intake = 0.34 mg DU.
These estimates are substantially lower than those made with the resuspension factor approach
(table C13), particularly for the central estimate, and during the first week. (The worst-case
estimates from the two approaches differ by only a factor of two in the fourth week.) This is
primarily due to the assumption in the dust loading approach that the DU is dispersed uniformly in
the top 1 cm of soil as this is a requirement of the generic soil model used. However, over short
time scales, the concentration in the upper few millimetres will be significantly higher than in the
next few millimetres, and therefore the resuspended air concentrations could well be higher than
those predicted using the dust loading approach. The results of the resuspension factor approach
rather than the dust loading approach were therefore used in the overall assessment.
Uncertainties in intake estimates
The uncertainties in the estimates of intake are at least 2 to 3 orders of magnitude, as discussed
below.
The resuspension factor approach is useful in localised situations for characterisation of the
relationship between surface and airborne contamination. In practice, however, there are no
homogeneously contaminated surfaces, and the airborne concentration is a sum of the local
resuspended contamination and contamination carried from upwind resuspension (Smith et al
1982), minus that carried away by the wind. Another deficiency is that resuspension factors are
applicable only for the conditions for which they were determined. In a recent paper (Garger et al
1997), it was found that even where local conditions such as vegetative cover and climate were
taken into account, the calculated values of Kmight differ from measured values by over one order
of magnitude. In that study, uncertainty in Khas been found to reach 23 orders of magnitude for
-
8/8/2019 The health hazards of depleted uranium munitions (c)
23/23
calculations where Khas been determined in a generic way, such as in this study.
The large uncertainty in the resuspension factor approach is the resuspension at time zero, ie K(0),
which can range from 10-9
to 10-5
m-1
(Linsley 1978). In the resuspension factor approach adopted
here, K(0)is initially assumed to be 10-6
m-1, indicating that while the intake calculation may be 2 to
3 orders of magnitude lower than calculated, it is unlikely to be more than 2 orders of magnitude
higher than calculated. Several studies (Garland et al 1992, BIOMOVS II 1996, Garger et al 1999)
have been carried out to test existing resuspension models against experimental data. In each of
these studies, Garlands resuspension factor has been found to overpredict the resuspended air
concentration. Another source of uncertainty i s transport of resuspended material from the
contaminated area. This has not been modelled here. Studies (Garger et al 1998, Underwood
1990) indicate that small particles (