The Gynecologist’s Role in Evaluation and Management of HMBfiles. · The Gynecologist’s Role in...
28
The Gynecologist’s Role in Evaluation and Management of HMB Andra H. James MD, MPH Consulting Professor, Obstetrics & Gynecology Duke University Medical Center
Transcript of The Gynecologist’s Role in Evaluation and Management of HMBfiles. · The Gynecologist’s Role in...
The Gynecologist’s Role in Evaluation and Management of HMB
Andra H. James MD, MPH Consulting Professor,
Obstetrics & Gynecology Duke University Medical Center

Sponsored by Texas Children’s Hospital & The Foundation for Women and Girls with Blood Disorders
Monday, May 18, 2015 Feigin Center, 14th Floor, Conference Room 14D
1:00pm – 5:00p.m.
Speaker: Andra H. James, MD, MPH
Duke Medicine, Consulting Professor
Topic: “Gynecologists Role in Evaluation and Management of HMD”
Planning Commi+ee DISCLOSURE: Dr. James is referencing an unlabeled/unapproved drug or product in her presenta9on. The drugs referenced are normal contracep9ves and proges9n contracep9ves for the treatment of heavy menstrual bleeding.
Overview
1. Establish the presence of HMB 2. Consider the possible causes 3. Evaluate for uterine pathology 4. Evaluate for systemic causes
-anovulation 2⁰ to systemic disease -underlying bleeding disorder
5. Utilize hormonal or surgical therapy as appropriate
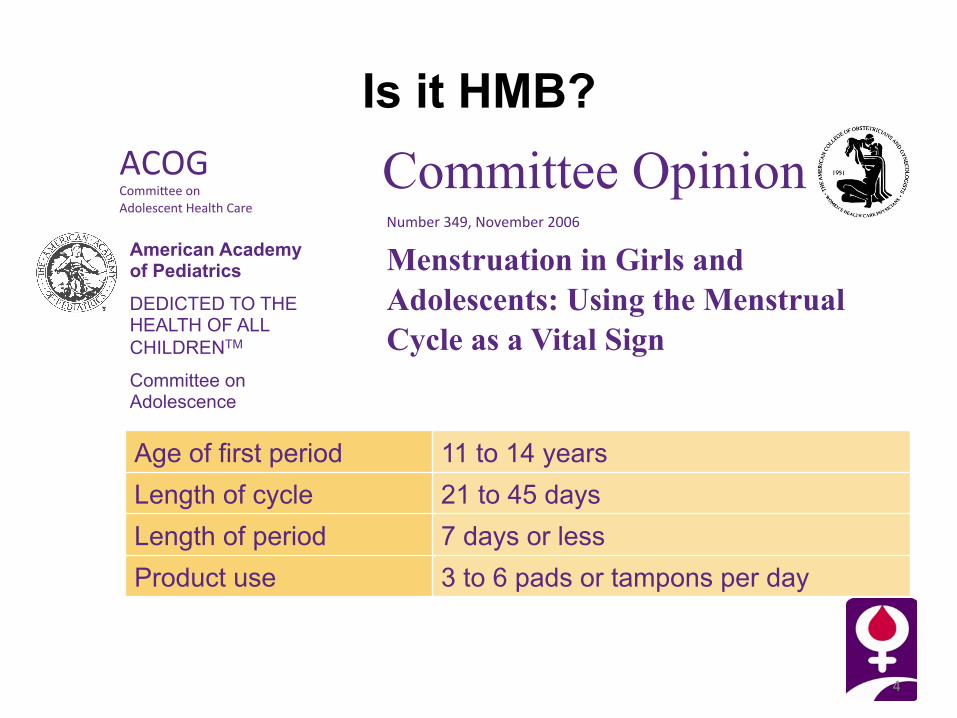
ACOG Commi@ee on Adolescent Health Care
American Academy of Pediatrics
DEDICTED TO THE HEALTH OF ALL CHILDRENTM
Committee on Adolescence
Is it HMB?
4
Committee Opinion Menstruation in Girls and Adolescents: Using the Menstrual Cycle as a Vital Sign
Number 349, November 2006
Age of first period 11 to 14 years Length of cycle 21 to 45 days Length of period 7 days or less Product use 3 to 6 pads or tampons per day
PALM-COEIN Classification of Abnormal Uterine Bleeding
5 Munro, et al. for the FIGO Working Group on Menstrual Disorder, Int J Gynaecol Obstet. 113:1-13, 2011
polyp adenomyosis leiomyoma (fibroids) malignancy and hyperplasia coagulopathy (bleeding disorder) ovulatory dysfunc9on (anovula9on) endometrial iatrogenic not yet classified
PALM-COEIN Classification of Abnormal Uterine Bleeding
6
polyp adenomyosis leiomyoma (fibroids) malignancy and hyperplasia coagulopathy (bleeding disorder) ovulatory dysfunc9on (anovula9on) endometrial iatrogenic not yet classified
Munro, et al. for the FIGO Working Group on Menstrual Disorder, Int J Gynaecol Obstet. 2011; 113:1-‐13

Netter medical illustration used with permission of Icon Learning Systems, LLC a subsidiary of MediMedia, USA, Inc. All rights reserved.
Fibroids as an Example of Local Pathology
7

PALM-COEIN Classification of Abnormal Uterine Bleeding
8 Munro, et al. for the FIGO Working Group on Menstrual Disorder, Int J Gynaecol Obstet. 2011; 113:1-‐13
polyp adenomyosis leiomyoma (fibroids) malignancy and hyperplasia coagulopathy (bleeding disorder) ovulatory dysfunc9on (anovula9on) endometrial iatrogenic not yet classified

The Menstrual Cycle
9

Cause Age 13-‐19
Age 20-‐34
Age 35-‐49
Age 50+
Adolescent anovula9on
Bleeding disorder
Local pathology
New systemic disease
An9coagulant therapy
Post-‐op complica9on
Hypothyroidism
Peri-‐menopausal anovula9on
Causes of Heavy Menstrual Bleeding
10

Evaluation of HMB: History
History • obstetrical
• currently pregnant?
• gynecological • menstrual • sexual • recent trauma?
• medical • bleeding history
Image source: Microso] Clip Art online

Evaluation of HMB: History
Medications • contraceptives and
hormones • anticoagulants and
antiplatelet agents • thyroid medications
Image source: Microso] Clip Art online

Evaluation of HMB: Examination • vital signs • oxygen saturation • speculum exam and pelvic examination
per gynecologist – depending on the age of the patient and the clinician’s judgement
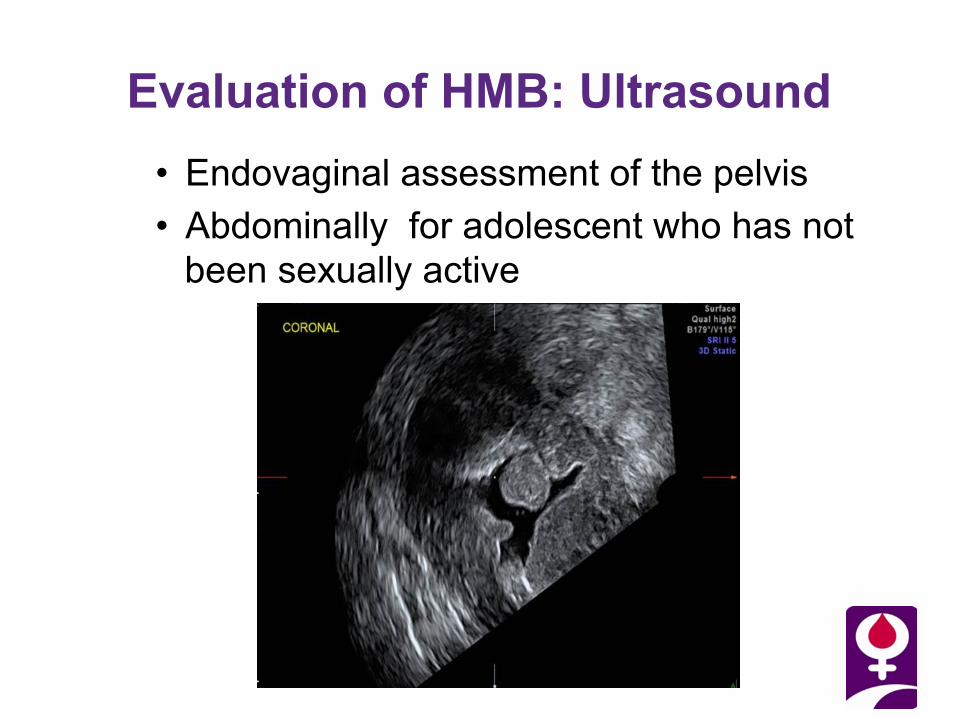
Evaluation of HMB: Ultrasound • Endovaginal assessment of the pelvis • Abdominally for adolescent who has not
been sexually active

Evaluation of HMB: Ultrasound
• Endometrial sampling if > age 45 • < age 45 if history of unopposed estrogen
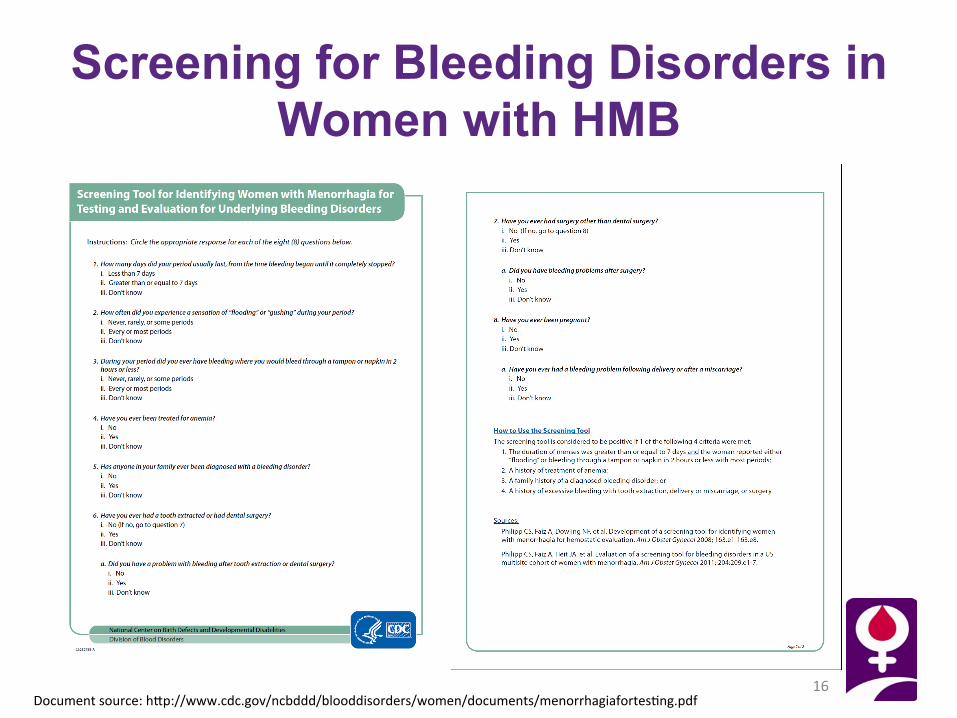
Screening for Bleeding Disorders in Women with HMB
16 Document source: h@p://www.cdc.gov/ncbddd/blooddisorders/women/documents/menorrhagiafortes9ng.pdf

How to use the screening tool
17
The screening tool is considered positive if: 1. The duration of menses was greater than or
equal to 7 days and the woman reported either “flooding” or bleeding through a pad or tampon in 2 hours or less with most periods
2. A history of treatment of anemia 3. A family history of a diagnosed bleeding
disorder, or 4. A history of excessive bleeding with tooth
extraction, delivery or miscarriage, or surgery

Laboratory Evaluation • pregnancy test
James et al. Von Willebrand disease and other bleeding disorders in women: consensus on diagnosis and management from an international expert panel. Am J Obstet Gynecol, 2009

Work-Up for a Bleeding Disorder
The laboratory assessment should include, as necessary:
• CBC • prothrombin time (PT) • activated partial thromboplastin time (aPTT) • VWF:RCo, VWF:Ag and FVIII • platelet function (platelet aggregation studies) • other clotting factors • other non-hematologic tests including, perhaps, tests
of thyroid function
James et al. Von Willebrand disease and other bleeding disorders in women: consensus on diagnosis and management from an international expert panel. Am J Obstet Gynecol, 2009

Types of Bleeding Disorders in Female UDC (n = 319)*
20
Total VWD 88.7% Type 1 61.1 % Type 2 7.8 % Type 3 4.4 % Type unknown 15.4 % Factor VIII 12.5% Platelet disorders 4.7% Missing diagnoses 6.9% Other bleeding disorders 15.4%
*19.4% had 2 or more hemosta9c defects *Byams et al, Haemophilia. 17(Suppl 1):6-13
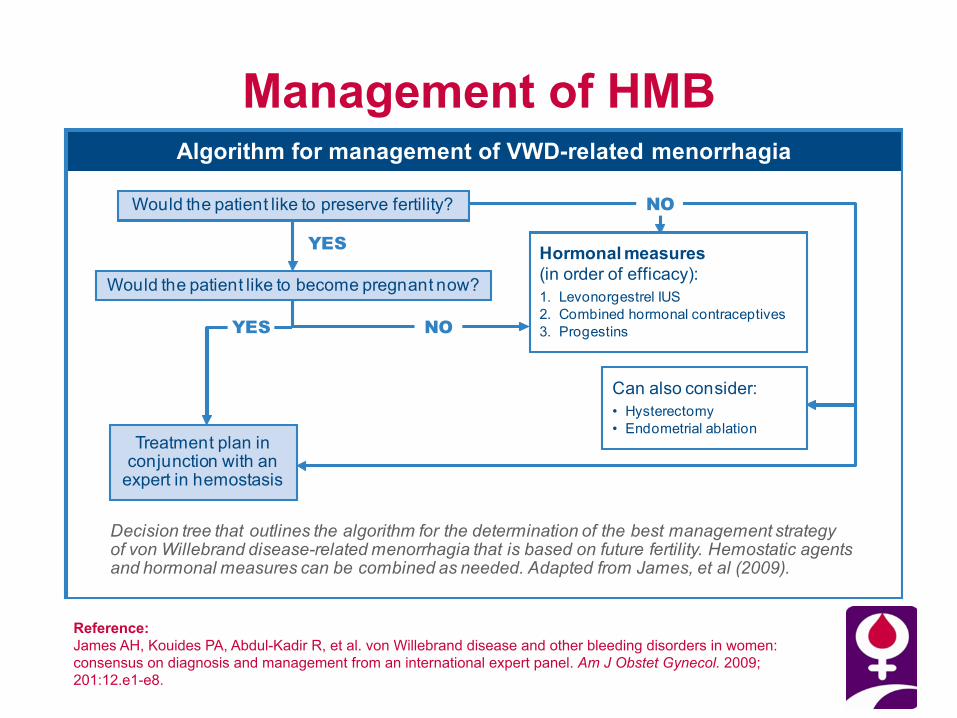
Management of HMB Algorithm for management of VWD-related menorrhagia
Hormonal measures(in order of efficacy):1. Levonorgestrel IUS2. Combined hormonal contraceptives3. Progestins
Treatment plan in conjunction with an
expert in hemostasis
Would the patient like to preserve fertility?
Would the patient like to become pregnant now?
Can also consider:• Hysterectomy• Endometrial ablation
YES
NO
NO
YES
Decision tree that outlines the algorithm for the determination of the best management strategy of von Willebrand disease-related menorrhagia that is based on future fertility. Hemostatic agents and hormonal measures can be combined as needed. Adapted from James, et al (2009).
Reference: James AH, Kouides PA, Abdul-Kadir R, et al. von Willebrand disease and other bleeding disorders in women: consensus on diagnosis and management from an international expert panel. Am J Obstet Gynecol. 2009; 201:12.e1-e8.

Watchful Waiting in the Adolescent
• Follow pubertal progression closely – Menarche is, on average, 2 years behind
telarche (growth velocity peak) – Maintaining fertility is critical
• Hysterectomy is not an option • Work with a hemostasis expert and have
a well-designed plan in place – Both hormones and hemostatic agents may
be necessary
James AH. Bleeding disorders in adolescents. Obstet Gynecol Clin N Am. 2009; 36(1):153-162.

Starting Hormones in Adolescents1,2
• Levonorgestrel intrauterine system (IUS)1,2
• Combined hormonal contraceptives1,2
• Progestins1,2
• Can be started at menarche, but not before
– Starting early may interfere with growth
References: 1. James AH. Bleeding disorders in adolescents. Obstet Gynecol Clin N Am. 2009;36(1):153-162. 2. Kadir RA. Menorrhagia: treatment options. Thromb Res. 2009;123(suppl 2):S21-S29.

Endometrial Ablation1,2
• Advantages compared with hysterectomy – Shorter procedure3
– Faster recovery3
– Reduced cost3
– Fewer adverse events3
• Disadvantages – Future surgery3
– Greater long-term blood loss References: 1. Sambrook AM, Bain C, Parkin DE, Cooper KG. A randomised comparison of microwave endometrial ablation with transcervical resection of the endometrium: follow
up at a minimum of 10 years. Br J Obstet Gynecol. 2009;116:1033-1037. 2. Chapa HO, Venegas G, Antonetti AG, Van Duyne CP, Sandate J, Bakker K. In-office endometrial ablation and clinical correlation of reduced menstrual blood loss
and effects on dysmenorrhea and premenstrual symptomatology. J Reprod Med. 2009;54:232-238. 3. Lethaby A, Shepperd S, Farquhar C, Cooke I. Endometrial resection and ablation versus hysterectomy for heavy menstrual bleeding (review). Cochrane Syst Data
Rev. 1999;2(1):1-60.

Hysterectomy1-4 • Patient satisfaction reported to be comparable to or
higher than that for other methods3 • Potential for serious morbidity, including perioperative
bleeding4 – Bleeding complications during hysterectomy occur in
3% of patients with VWD compared to <1% of women without VWD5
• Plan required to avoid/control bleeding • Aspirin and NSAIDs to be avoided post-op6 • Potential for complications should not keep women who
need the procedure from having it6
References: 1. Munro KG. The evolution of uterine surgery. Clin Obstet Gynecol. 2006;49(4):713-721. 2. Hoffman MS. Extent of radical hysterectomy: evolving emphasis. Gynecol Oncol. 2004;94:1-9. 3. Lethaby A, Shepperd S, Farquhar C, Cooke I. Endometrial resection and ablation versus hysterectomy for heavy menstrual bleeding (review). Cochrane Syst Data Rev. 1999;2(1):1-60. 4. Maresh MJA, Metcalfe MA, McPherson K, et al. The VALUE national hysterectomy study: description of the patients and their surgery. Br J Obstet Gynecol. 2002;109:302-312. 5. James AH, Myers ER, Cook C, Pietrobon R. Complications of hysterectomy in women with von Willebrand disease. Haemophilia. 2009;15(4):926-931. 6. National Heart, Lung, and Blood Institute. The Diagnosis, Evaluation, and Management of von Willebrand Disease. Bethesda, MD: US Department of Health and Human Services; 2008.

Treatment for HMB (n = 165) in the UDC
26
Oral contracep9ves 90 (54.5%) Desmopressin 56 (33.9%) An9fibrinoly9cs 40 (24.2%) Blood or plasma products 12 (7.3%) Cloang factor products 10 (6.1%) Endometrial abla9on 7 (4.2%) Levonorgestrel IUD 5 (3.0%) Uterine artery emboliza9on 3 (1.8%) Platelet transfusion 1 (0.6%)
21/198 (10.6%) menstrua9ng/menopausal women with HMB underwent hysterectomy specifically to control HMB
Byams, et al. Haemophilia, 17(Suppl 1):6-‐13
Summary
1. Establish the presence of HMB 2. Consider the possible causes 3. Evaluate for uterine pathology 4. Evaluate for systemic causes
-anovulation 2⁰ to systemic disease -underlying bleeding disorder
5. Utilize hormonal or surgical therapy as appropriate

Thank you Gracias Merci
fwgbd.org