The Global Health Workforce Alliance 2011 Annual Report … · 6 Message from the Chair and...
48
Enabling solutions, ensuring healthcare The Global Health Workforce Alliance 2011 Annual Report
Transcript of The Global Health Workforce Alliance 2011 Annual Report … · 6 Message from the Chair and...

Enabling solutions, ensuring healthcare
The Global Health Workforce Alliance 2011 Annual Report

This report was produced by the Global Health Workforce Alliance (the Alliance). The Alliance is hosted by the World Health Organization. All rea-sonable precautions have been taken by the Alliance to verify the informa-tion contained in this publication. Notwithstanding, the Secretariat of the Alliance welcomes any comments, suggestions and notification of errors or inconsistencies, which can be submitted to [email protected]. The respon-sibility for the interpretation and use of the material lies with the reader.
Requests for permission to reproduce or translate this publication – whether for sale or for non-commercial distribution – should be addressed to [email protected].
Photo credits
> Cover: © Thomson Reuters> Page 6: Masato Mugitani / ©WHO> Page 6: Mubashar Sheikh / © GHWA / Eric Williams> Page 8: © UN photo / Eskinder Debebe> Page 10: © GHWA / OnAsia / L.Duggleby> Page 12: © Touch Foundation> Page 21: © Thomson Reuters> Page 31: © UN photo / Eskinder Debebe> Page 32: © UN photo / O.Chassot> Page 36: © UN photo / Sophia Paris> Page 37: © GHWA / OnAsia / L.Duggleby> Page 44: © UN photo / Sophia Paris

6 MessagefromtheChairandExecutiveDirector
8 Healthworkforceattheheartofglobalagendas8 Maintaining momentum for the WHO Code of Practice
8 Second Global Forum on Human Resources for Health
11 Noncommunicable diseases policy processes
13 Recognition for HRH at the G8, Deauville
13 Maternal and child health
16 HIV and AIDS
16 Civil society partners driving global HRH advocacy
18 Improving conditions for health workers: 2011 Review of
the Positive Practice Environments Campaign
20 Acceleratingcountryactions20 Greater stakeholder engagement in HRH development:
the Country Coordination and Facilitation approach
23 Examples of progress through CCF support to countries
25 Drawing lessons from the CCF process in countries
28 Promoting HRH policy dialogue at regional level
32 Promotingevidence-basedHRHsolutions32 Systematic review and case studies of mid-level health providers
32 Joint statement on Scaling-up the Community-Based Health
Workforce for Emergencies
33 Private sector role in HRH development
35 UN OneHealth Costing Tool
36 Supportingcoremanagementfunctions36 Governance
36 Membership and partnership issues
36 Corporate communications
38 External evaluation
39 Budget and finance
44 TowardsthesecondphaseoftheAlliance

List of Figures, Boxes and Tables
Figure 1. PPE Campaign EvaluationFigure 2. Bringing HRH stakeholders together through the CCF processFigure 3. Results of CCF support (2009–2011)Figure 4. Alliance catalytic support through distributions to countries and regions, 2011Figure 5. Funding contributions to the Alliance from 2006 to 2011 (Dec)
Box 1. Second Global Forum Outcome StatementBox 2. Political declaration on noncommunicable diseases and the health workforceBox 3. Recognition of the value of the Alliance in increasing the quantity and quality of HRHBox 4. CCF process supports reproductive, maternal, newborn and child health goalsBox 5. Alliance support to High Burden Country InitiativeBox 6. State of the World’s Midwifery reportBox 7. 2011 Campaign: Health Workers Count CoalitionBox 8. Integrating HRH into wider health sector planning: Joint Assessment of National Health Strategies/IHP+ process in MaliBox 9. Engaging members, partners and national institutions in support of the CCF approachBox 10. Master of Public Health with focus on HRH for francophone countriesBox 11. Alliance members contribute global public goods for HRH developmentBox 12. Results of a 2011 survey among Alliance members and partnersBox 13. External evaluation key findings
Table 1. Annual Financial Statement of the Alliance as of 31 December 2011

List of acronyms and abbreviations
AAAH Asia-Pacific Action Alliance on Human Resources for Health AFD French Development Cooperation AgencyAlliance The Global Health Workforce AllianceAMREF African Medical and Research FoundationAPHA Africa Public Health Alliance and 15%+ CampaignAPHRH African Platform on Human Resources for HealthCCF Country Coordination and Facilitation approach CHW Community health workerDFID Department for International Development (United Kingdom)G8 Group of eight large economies (Canada, France, Germany, Italy, Japan, Russian Federation, United Kingdom, United States of America)GIZ Deutsche Gesellschaft für Internationale ZusammenarbeitGlobal Fund Global Fund to Fight AIDS, Tuberculosis and MalariaHHA Harmonization for Health in AfricaHIV/AIDS Human immunodeficiency virus/acquired immunodeficiency syndromeHRH Human resources for healthHWAI Health Workforce Advocacy InitiativeIHP+ International Health Partnership and related initiativesJANS Joint Assessment of National Health StrategiesJICA Japan International Cooperation AgencyMDG Millennium Development GoalMoHProf Mobility of Health Professionals NCD Noncommunicable diseaseNGO Nongovernmental organizationPATHS2 Partnership for Transforming Health Systems Phase IIPMAC Prince Mahidol Award ConferencePPE Positive Practice Environments Campaign UN United NationsUNFPA United Nations Population FundUNICEF United Nations Children’s FundUN Women United Nations Entity for Gender Equality and the Empowerment of WomenUSAID United States Agency for International DevelopmentWHO World Health Organization

6
The Global Health Workforce Alliance celebrated its fifth anniversary in May 2011, which marked the mid-point in our initial ten-year mandate. In this spirit, 2011 signalled a need for reflection and assessment; a time to consider the positive contributions the Alliance made over the course of the last five years and refocus on what remains to be done.
There were a number of high points in the year. In January, the Alliance showcased its role as a pow-erful and effective convenor at the Second Global Forum on Human Resources for Health in Bang-kok. The Forum brought together more than 1000 individuals dedicated to the human resources for health (HRH) cause, representing the broad spec-trum of actors, organizations and governments engaged in finding solutions to health worker challenges. The Alliance reinforced the momentum that was built at the Forum by taking its key messages and recommendations out to the wider world, capital-izing on several opportunities for policy dialogue at the global level throughout the year, most nota-bly in the realms of noncommunicable diseases, maternal and child health and HIV/AIDS. Each opportunity was used to position HRH firmly on the agenda, and sustain high-level political com-mitment and goodwill to strengthen the health workforce.
The Alliance continued to extend its direct support to countries facing critical HRH challenges through the Country Coordination and Facilitation process. This approach has already started to show results in terms of greater inclusiveness in health work-force coordination and planning, greater integra-tion of health workforce objectives in national health strategies, and accelerated implementation of HRH plans.
Message from the Chair and Executive Director
DrMubasharSheikh – Executive DirectorGlobal Health Workforce Alliance
DrMasatoMugitani– Chair Assistant Minister for Global Health, Ministry of Health, Labour and Welfare, Japan

6 7
Work was also initiated on a number of activities that will contribute to policy dialogue on priority HRH topics. These include the role of front-line mid-level health workers, the contribution of the private sector, and specific tools to support national health workforce policy and planning processes.
The solid achievements and progress of 2011 illustrate the many contributions and value added by the Alliance over the past five years, and are intrinsically linked to the accomplishments and contributions of more than 300 member and part-ner organizations that, together, constitute the global network of the Alliance.
In 2012, the Alliance will embark on a new cycle with a new strategy for its second phase (2013–2016), taking into account the successes and lessons learnt over its first five years of operation, and the findings of an external evaluation commissioned by the Board, conducted in the second half of 2011. The Alliance has an ongoing obligation and responsibility to tackle the unfinished HRH agenda during the next phase of its mandate, which it will strive to do while anticipating, responding to and monitoring key developments and challenges in the evolving HRH environment.
Dr Masato Mugitani, ChairDr Mubashar Sheikh, Executive Director
Global Health Workforce Alliance
Message from the Chair and Executive Director
“The unsung heroes, health workers, are in desperately short
supply”.Ban Ki-moon, UN Secretary General,
opening the Every Woman, Every Child event on September 20, 2011.

Health workforce at the heart of global agendas
> advocating for the Code implementation at the Second Global Forum on HRH;
> supporting a briefing on the implementation of the Code at the World Health Assembly;
> providing suggestions and inputs into the consultation process coordinated by WHO on the development of guidelines and tools for countries to report back on Code imple-mentation; supporting the renewal and the definition of a new role for the Health Worker Migration Global Policy Advisory Council, on which the Executive Director of the Alliance is a member, and with whom the Alliance will cooperate in future advocacy related to Code implementation.
Second Global Forum on Human Resources for Health
The year 2011 opened with the largest global gath-ering since 2008 of HRH experts in Bangkok, Thai-land, in January. Convened by the Alliance, WHO, JICA and the Prince Mahidol Award Conference
The Alliance actively led and engaged in major global events and policy processes throughout 2011 to ensure that the global and national shortfall of health workers received prominent attention. In particular, the vital link between health workers and the achievement of health and development goals was advocated at every key opportunity, and concrete solutions proposed on specific aspects of health workforce development.
Maintaining momentum for the WHO Code of Practice
If 2010 saw the historic adoption of the WHO Global Code of Practice on International Recruitment of Health Personnel, it was in 2011 that work actually got under way to put in practice its provisions. The Alliance supported a number of low- and middle-income countries through the CCF approach (seeSection 2) to gear up to the reporting require-ments. These engagements in specific countries were complemented by a series of activities at the global level, including:

1Health workforce at the heart of global agendas
(PMAC), the Second Global Forum was supported by many sponsors,1 and attended by delegates representing all constituencies involved in HRH at global level and in priority countries in particular.
The centrepiece of the event was the opportunity to share progress made in tackling health work-force challenges through the implementation of the strategies of the Kampala Declaration and Agenda for Global Action, adopted at the First Global Forum on HRH. The publication Reviewing progress, renewing commitment, the Alliance’s first progress report on the Kampala Declaration, represented a new milestone in HRH and provided the basis and a framework for discussions. Over 1000 representatives from more than 100 countries attended the conference, shared experiences and best practices, and reviewed results and further action needed.
Sessions and side events were organized by WHO, the Alliance Secretariat and a number of members and partners on a variety of aspects relating to the health workforce, including leadership, education and training, financing, appropriate skills mix, and health workforce implications of the United Nations Global Strategy for Women’s and Chil-dren’s Health.
A highlight was the awards ceremony during which the Alliance honoured individual health workers and institutions promoting HRH interventions at country level that are having positive results.
The momentum in mobilizing country leadership and stakeholders generated through the Second Global Forum was maintained through follow-up actions including the development and dissemina-tion to Forum participants and beyond of relevant
1 China Medical Board; Deutsche Gesellschaft für Internationale Zusammenarbeit GmbH; European Commission; Ministry of Foreign and European Affairs, France; Ministry of Health and Ministry of External Relations, Brazil; Norwegian Agency for Development Cooperation; The Rockefeller Foundation; United States Agency for International Development; World Health Organization Regional Office for South-East Asia.

10
communications and advocacy materials emerging from the conference. Alliance members and partners also played a proactive role in ensuring the wide dissemination of messages and materials developed in the context of the Forum, for example through the translation and dissemination through a variety of fora and activities of the animated film ‘Imagine’.
More importantly, the recommendations of the Forum were captured in an outcome statement (Box 1), which called for increased adoption of policies and investment decisions conducive to health workforce develop-ment; these recommendations were also widely distributed, and formed the basis for the Alliance engagement at other key events and processes throughout the year.
Snapshot from the Imagine video
Winners of the Special Recognition Award and Awards of Excellence – at the Second Global Forum on Human Resources for Health, Bangkok.

10 11
1. Health workforce at the heart of global agendas
2. Accelerating country actions
3. Promoting evidence-based HRH solutions
4. Supporting core management functions
5. Towards the second phase of the Alliance
Civil society organizations also made their voice heard through a state-ment by the Health Workforce Advocacy Initiative (HWAI), a global advo-cacy network supported by the Alliance. The statement, endorsed by allied civil society organizations, called for bolder leadership, clear, time-specific targets, and increased financial resources at global and national levels.
Noncommunicable diseases policy processes
Noncommunicable diseases (NCDs) received greater attention in 2011 than ever before, and the Alliance worked closely with the WHO NCD cluster in the preparation of key HRH messages that formed the background to the First Global Ministerial Conference on Healthy Lifestyles and Noncommu-nicable Disease Control in Moscow, Russian Federation, on 28 – 29 April. Through this engagement and through attendance at the event itself, the Alliance conveyed the following messages:
> much-needed progress in addressing NCDs will require adapting health worker education and training in low- and middle-income countries to the evolving burden of disease in these contexts, thereby ensuring that they possess the requisite competence;
> potential models used in other service delivery areas can be emu-lated, e.g. innovative skills mix approaches where simple tasks are shared among cadres with shorter training, such as community-based and mid-level health workers;
> NCD health workforce needs cannot be tackled in isolation, but should rather be integrated in all phases of health workforce training, devel-opment and management.
SecondGlobalForumOutcomeStatement Box1
The outcome statement of the Second Global Forum on Human Resources for Health reiterated the relevance of
the Kampala Declaration and Agenda for Global Action, recognized the WHO Code of Practice on International
Recruitment of Health Personnel as a critical reference framework, and called upon countries, partners and
other relevant stakeholders:
> to strengthen leadership by all state and non‐state actors for greater commitment and action on the
health workforce, and to ensure policy coherence across sectors;> to bolster the supply, training, retention and management of health workers, for improved availability,
quality and performance;> to scale up investment in HRH, ensuring that resources are sufficient, efficiently used and aligned to
national needs, and that there is full complementarity between international and domestic funding flows.

12
The issue of HRH featured prominently in the Declaration from the ministe-rial meeting, recognizing that treating NCDs requires an adequate health workforce equipped with the necessary skills and working within an effec-tive health system. The Declaration also emphasized the need to integrate NCD-related services into primary health care services and in the wider health systems strengthening agenda.
Building on the ministerial conference, the Alliance engaged in the United Nations General Assembly High-level Meeting on Non-communicable Dis-eases in New York, USA on 19 September 2011. Together with civil society members, the Alliance hosted a side event entitled Addressing Noncom-municable Diseases – It Takes a Workforce as part of a wider process of advocacy with countries.
These engagements contributed to bringing health workforce issues to the fore in the policy process focusing on NCD, as reflected in the politi-cal declaration issued by the United Nations General Assembly (Box2). Secretary-General Ban Ki-moon praised health workers and the indispen-sable role they play in achieving the MDGs and other health goals.
Alliance hosted side event at the UN General Assembly, September 2011 - “Addressing Noncommunicable Diseases - It Takes a Workforce”.

12 13
1. Health workforce at the heart of global agendas
2. Accelerating country actions
3. Promoting evidence-based HRH solutions
4. Supporting core management functions
5. Towards the second phase of the Alliance
Recognition for HRH at the G8, Deauville
In the run-up to the May 2011 G8 summit in Deauville, France, the Alli-ance worked with partners to promote the importance of HRH. Its efforts ensured that the global community and world leaders publicly recognized the need to increase the quantity and quality of health workers to ensure continued progress on health. Most significant was the commitment of G8 leaders, outlined in the Deauville Accountability Report: G8 Commitments on Health and Food Security,2 to remain accountable in health and support continued efforts to address weaknesses in the health workforce, particu-larly in African countries.
Recognizing the critical role of the Alliance in facilitating sustainable solu-tions to improve the health workforce in priority countries and globally, the Deauville Report stressed the need for equitable distribution of health workers and access to skilled health care. It made explicit reference to the Second Global Forum recommendation on accountability in HRH, as noted in Box3.
The renewed commitment of G8 countries opens the door for future dia-logue and opportunities to call for further support, including for increased efforts to track health workforce investments in line with the G8’s account-ability agenda.
Maternal and child health The Country coordination and Facilitation (CCF) approach, while aimed at strengthening HRH in an integrated fashion, can be instrumental – and
Politicaldeclarationonnoncommunicablediseasesandthehealthworkforce Box2
Commits to “Promote the production, training and retention of health workers with a view to facilitating
adequate deployment of a skilled health workforce within countries and regions, in accordance with the World
Health Organization Global Code of Practice on the International Recruitment of Health Personnel.”
United Nations General Assembly, New York, USA, September 2011.
2 Deauville Accountability Report – G8 Commitments on Health and Food Security: Status of Delivery and Results: http://www.g20-g8.com/g8-g20/root/bank_objects/Rapport_G8_GB.pdf.

14
valued by countries and development partners alike – in accelerating actions specifically geared towards the specific priorities of health MDGs (seeBoxes4and5).
Aside from this, the Alliance engaged in a series of dedicated advocacy and policy dialogue opportunities throughout the year related to reproductive, maternal, newborn and child health services (seeSection2), and its work to realize the United Nations Global Strategy for Women’s and Children’s Health. These included:
> Devoting a session in the Second Global Forum on HRH to follow-up to the United Nations Global Strategy for Women’s and Children’s Health, which was also explicitly referenced in the Forum outcome statement.
> Engaging in early consultations of the High Burden Country Initiative, spearheaded by the H4+ agencies (seeBox5) and supporting the
CCFprocesssupportsreproductive,maternal,newbornandchildhealthgoals Box4
In 2011 the Alliance began its involvement in a 5-year initiative promoted by the French Development Agency, as
part of France’s commitment to the Muskoka Initiative and to the United Nations Global Strategy for Women’s
and Children’s Health. This initiative targets several countries in sub-Saharan Africa, and focuses on reproduc-
tive, maternal, newborn and child health.
In the context of a larger programme involving UNFPA, UNICEF, UN Women and WHO, the Alliance has taken
the lead in the health workforce component of a multi-country programme to accelerate progress towards
the achievement of MDGs 4 and 5. Here, it provides a common framework for integration of HRH components
carried out by other agencies, through the CCF process, and ensures that maternal and child health needs are
mainstreamed into health workforce planning and development processes.
RecognitionofthevalueoftheAllianceinincreasingthequantityandqualityofHRH Box3
“The Second Global Forum on Human Resources for Health, convened by the Global Health Workforce Alliance,
has recommended the need for mutual accountability taking into consideration that international support
must be fully additional, aligned to countries’ needs, predictable, long term, and flexible, and must allow for
investment in training, equitable deployment, and ongoing and effective retention of health personnel along
the continuum of care.”
Deauville Accountability Report – G8 Commitments on Health and Food Security: State of Delivery and Results.

14 15
1. Health workforce at the heart of global agendas
2. Accelerating country actions
3. Promoting evidence-based HRH solutions
4. Supporting core management functions
5. Towards the second phase of the Alliance
United Nations Global Strategy, particularly in relation to strengthen-ing midwifery.
> Contributing to the development of the first-ever State of the World’s Midwifery report (Box6), by taking responsibility for the chapter on management and support of this cadre, including examples of best practices. The report was instrumental in highlighting the critical need for investment in midwives and in advocating for policies to facilitate their work at the Sixty-fourth World Health Assembly and at the 29th Triennial Congress of the International Confederation of Midwives in Durban, South Africa.
> Facilitating the nomination of the Alliance Board member Professor Miriam K Were to the Expert Review Group of the United Nations Com-mission on Information and Accountability for Women’s and Children’s Health (the Commission), tasked with reporting regularly to the Secretary-General on the results related to the Global Strategy and on progress in implementing the Commission’s recommendations.
AlliancesupporttoHighBurdenCountryInitiative Box5
As part of its support to the United Nations Global Strategy for Women's and Children's Health, the Alliance is
also engaged in a new initiative, led by UNFPA with UNAIDS, UNICEF, WHO and the World Bank (the H4+ agen-
cies), to strengthen maternal and newborn health in eight countries (Afghanistan, Bangladesh, DRC, Ethiopia,
India, Mozambique, Nigeria and Tanzania) that account for the bulk of the global burden of morbidity and
mortality. The Alliance will actively participate in a Technical Working Group developing tools for comprehen-
sive National Needs Assessments, aimed at better understanding gaps in the availability of health workers
with midwifery competency at the community level.
StateoftheWorld’sMidwiferyreport Box6
The Alliance contributed, along with many other partners, to the production and
launch of the first-ever State of the World’s Midwifery Report, in June 2011. The
report unveiled new data confirming the significant shortage of midwives and
called for an additional 112 000 to be trained and deployed. The shortfall means
that almost two-thirds of the 58 countries surveyed may fail to meet MDG 5 targets
for births attended by skilled birth attendants by 2015. The report represents a
milestone in recognizing midwives as key players within well-functioning health
systems.

16
HIV and AIDS
The Alliance, in partnership with the African Medical and Research Foun-dation (AMREF), the Government of Brazil, the Commonwealth Secretariat and UNAIDS, worked to mainstream HRH at the United Nations High-Level Meeting on AIDS in New York, USA in June 2011. The high-level meeting provided an opportunity to take stock of the progress and challenges of the last 30 years and shape the future response to AIDS. Can we achieve MDG 6 with the health workforce we have? – the only side event on HRH – succeeded in bringing HRH issues to the fore and attracting high-level speakers and participants. Hosted by the Alliance, the event sought to underline and build wide consensus on HRH as an indispensable element of an effective HIV/AIDS and MDG 6 response. Speakers, including heads of state, senior representatives from donor and international organiza-tions, civil society and the private sector, emphatically highlighted the critical link between HRH and meeting MDG 6, and shared relevant best practices and lessons learnt.
The side event was accompanied by more informal advocacy around the issue to Member States and civil society observers attending the Sum-mit, aimed at ensuring the appropriate recognition of HRH in the final proceedings.
The General Assembly adopted a Political Declaration on HIV/AIDS3 which commits to redouble the strengthening of health systems and increasing human resource capacity for the AIDS response, by scaling up the train-ing and retention of HRH policy and planning, and health-care personnel, consistent with the WHO Code of Practice on the International Recruitment of Health Personnel.
Civil society partners driving global HRH advocacy
The civil society-led HWAI supported by the Alliance transitioned to a new hosting arrangement with Wemos, a leading Netherlands-based right-to-health nongovernmental organization (NGO) which now serves as the Secretariat. Previously hosted by US-based Physicians for Human Rights, HWAI seeks to bring together civil society organizations with an interest in HRH to harmonize and reinforce their advocacy messages in support of coherent health workforce development solutions.
3 Political Declaration on HIV/AIDS: Intensifying our Efforts to Eliminate HIV/AIDS (http://daccess-dds-ny.un.org/doc/UNDOC/LTD/N11/367/84/PDF/N1136784.pdf?OpenElement).

16 17
1. Health workforce at the heart of global agendas
2. Accelerating country actions
3. Promoting evidence-based HRH solutions
4. Supporting core management functions
5. Towards the second phase of the Alliance
In 2011, HWAI member organizations played an especially active and influ-ential role in a global health worker campaign (seeBox7), led by Save the Children UK and supported by hundreds of organizations worldwide. The campaign, which encouraged popular mobilization for HRH, reached a climax at the United Nations General Assembly in New York, USA in Sep-tember 2011, where the scale of the health worker shortfall was exposed and urgent action by governments sought to close the gap.
Campaign:HealthWorkersCountCoalition Box7
Following on from the Global Forum on Human Resources for Health in Bangkok, a powerful global civil society
campaign, spearheaded by Alliance member Save the Children UK, drew attention to the health worker crisis
and catalysed action by governments and others to call for ‘a health worker within reach of everyone ’. More
than 300 organizations and many thousands of individuals united for the campaign from international organi-
zations, NGOs, ministries and the private sector. They took part in public hearings, rallies, online petitions,
Facebook and Twitter discussions, pop concerts, seminars, and parliamentary discussions with the aim of rais-
ing health worker issues to the top of the agenda and rallying support for investment in HRH and saving lives.
www.healthworkerscount.org

18
Improving conditions for health workers: 2011 Review of the Positive Practice Environments Campaign
The Positive Practice Environments (PPE) Campaign, funded by the Alli-ance and implemented by professional associations, aims to improve work environments for health professionals and thereby strengthen staff reten-tion and recruitment as well as quality of care. To date the campaign has focused on supporting activities in three pilot countries: Morocco, Uganda and Zambia. A detailed evaluation of the PPE campaign took place in 2011.
The evaluation identified as key strengths of the campaign its multi-disciplinary nature, high levels of commitment generated by campaign partners, and the relevance of the topic. Key recognized achievements include awareness in all contexts (global and in the three target countries) as well as successful collaboration by different categories of health work-ers towards the achievement of one common goal, particularly in Uganda and Zambia. In these two countries, the campaign also led to encouraging changes in policy and practice.
Besides these outcomes, a number of outputs were created, such as Cam-paign tools and materials and a web site. The tools and materials gener-ated appear to be widely used and appreciated. Improvements suggested relate particularly to making better use of the web site as a cost-effective core tool for campaigning.

18 19
1. Health workforce at the heart of global agendas
2. Accelerating country actions
3. Promoting evidence-based HRH solutions
4. Supporting core management functions
5. Towards the second phase of the Alliance
Increasing financial resources forimproving practice environments
Influencing practice
Mobilising communities and the wider public
Influencing policy
Creating pressure on government
Building alliances amongkey stakeholders
Disseminating materials andsharing information on PPE
Developing high-qualityadvocacy materials on PPE
Raising awareness ofissues relating to PPE
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Poor I cannot sayGoodExcellent Fair
Figure 1: PPE Campaign Evaluation

Accelerating country actions
on health workforce solutions (Figure2). The CCF approach helps countries to develop, implement and monitor an evidence-based and costed HRH plan that involves all stakeholders. In other words, the process is a trigger for countries to advance in the right direction to address their health workforce challenges, which ultimately leads to improved health of their populations.
To date, the CCF approach has succeeded, inter alia, in mobilizing the following support from part-ners at country level:
> The Department for International Development (DFID) of the United Kingdom complemented the Alliance efforts in Nepal and supported the HRH situation analysis and planning.
> The Japan International Cooperation Agency (JICA) is supporting South Sudan in its HRH information system and hosting the HRH Coor-dination Committee Secretariat; South Sudan has reviewed the curriculum for midwives, and increased their enrolment from 90 (2010) to
The ultimate scope of the Alliance work is to con-tribute to redressing health workforce imbalances in countries where these hinder progress in scaling up access to essential health services. In 2011, the Alliance continued to mobilize country leadership to improve the HRH situation, as an integral part of the health systems strengthening agenda. This has been accomplished through a variety of initia-tives, some targeting individual countries, others in collaboration with regional networks, and oth-ers still focusing on global level policy dialogue and advocacy processes.
Greater stakeholder engagement in HRH development: the Country Coordination and Facilitation approach
The CFF approach enables countries to align their HRH coordination mechanisms with their health systems. The added value of this process is to bring together the key stakeholders necessary for a joint identification of challenges, and to create collaborative platforms to develop and act

Accelerating country actions
181 (2011) and that of nurses from 60 (2010) to 91 (2011).
> The Partnership for Transforming Health Systems Phase II (PATHS2) is a partner in CCF implementation in Lagos State of Nigeria.
> The French Development Cooperation Agency (AFD) is collaborating in Cameroon with the Alliance and the World Health Organization (WHO) to support HRH development through the CCF process and related HRH planning activities.
CCF support to the countries also created synergy and mutual benefit among the initiatives of part-ners in a number of cases, such as the following:
> The Alliance supported the situation analysis in Sindh province of Pakistan with the con-tribution of the WHO country office; building on that, the United States Agency for Interna-tional Development (USAID) is supporting the development of the HRH plan.
> The Alliance supported the CCF process in Indonesia, which led the Ministry of Health to generate additional domestic resources for HRH planning and implementation, and to carry forward the approach.
> The Alliance supported a community health workers (CHW) situation analysis and policy development process in Zambia; since then, partners like WHO, the Clinton Health Access Initiative and the Global Fund to Fight AIDS, Tuberculosis and Malaria (Global Fund) are supporting the scaling-up of the Community Health Assistants programme in 7 provinces and 48 districts of the country.
> In Sudan, the annual enrolment capacity of the Academy of Health Sciences has risen from 2000 in 2005 to about 5000 in 2011. This has made it possible to enrol over 18 000 can-didates in each year of study in 14 different disciplines.
2

22
The Alliance has vital partnerships with the WHO country offices, which in most cases are the focal and entry points for the catalytic support. They also provide operational support for the CCF process and technical assistance to the HRH committees under the leadership of the Ministry of Health.
The National HRH Observatory of Sudan, which has been strengthened by the Alliance, provides the Secretariat to the CCF/HRH committee. In some countries where national HRH observatories are not established or fully functional, CCF mechanisms facilitate their establishment. This has been the case in Afghanistan, Cameroon, Indonesia, Nepal and Pakistan. By 2011, the CCF approach had proved its credentials: support to exist-ing countries was consolidated, and the key advances in their health workforce planning processes highlighted. In addition, five new countries joined the process (Burkina Faso, Chad, Congo, Guinea, Djibouti), bringing the total number of countries supported to 20.
Figure 2. Bringing HRH stakeholders together through the CCF process
HRHPLANEvidence basedComprehensive Costed
HRHcrisisreduced
HRHCOMMITTEE
CoordinationandStewardship
Membership from Line ministries, Academia, Professional associations, Regulating bodies,Private sector,Civil society, NGOs, andPartners
Stakeholders analysis and identification
Other Coordinationmechanisms supporting Health System Strengthening
DesignFinanceImplementMonitor Evaluate
KEYSTRATEGIES: Scaling up education, Task shifting, Skills mix, New cadres, Retention measures, Working conditions

22 23
1. Health workforce at the heart of global agendas
2. Accelerating country actions
3. Promoting evidence-based HRH solutions
4. Supporting core management functions
5. Towards the second phase of the Alliance
Examples of progress through CCF support to countries
Afghanistan• Afghanistan has increased investment in HRH and is undertaking the develop-
ment of a HRH plan. Salaries of health workers are being increased at both central and peripheral levels.
Nepal• Alliance partnership with DFID, Deutsche Gesellschaft für Internationale
Zusammenarbeit (GIZ) and WHO supported the development of the HRH plan through the CCF process, which is embedded in the national health strategy.
Pakistan• Pakistan has developed its first report on the implementation of the WHO
Global Code of Practice on the International Recruitment of Health Personnel. • Two provinces are developing an HRH situation analysis and a strategic plan.
Indonesia• With Alliance support, Indonesia has developed its HRH plan; started to
implement the WHO Global Code of Practice on the International Recruitment of Health Personnel; developed guidelines on the migration of nurses; and initiated a rural retention scheme.
Sudan
• With support from the Alliance, WHO and the Global Fund, Sudan began train-ing more than 300 CHWs across two states. Training capacity of the Academy of Health Sciences increased from 2000 (in 2005) to about 5000 (in 2011).
• After development of the HRH plan supported by the Alliance, additional resources for HRH development are being mobilized from global health initiatives.
Djibouti• The Alliance is supporting the HRH situation analysis with the involvement of
all key stakeholders to develop evidence-based information for the HRH plan, linked to the national health strategy.
SouthSudan• The Alliance supported the stakeholder analysis, consolidating the coordina-
tion process, HRH situation analysis and strategic planning. The WHO country office is the main partner and focal point, while JICA provides the secretariat to the HRH committee.
• South Sudan has revised the curriculum of midwives and increased the enrol-ment of nurses and midwives.

24
Chad• Thanks to advocacy efforts by the country’s parliamentarians, who are actively
represented on the HRH committee, the number of health workers in Chad steadily increased from 2008 to 2011.
• Chad is now working on the development of an HRH plan and a strategy for retention in rural areas.
Zambia• Since initial Alliance assessment support in 2009, Zambia has extended its
CHW programme across 7 provinces and 48 districts.• The country has developed its second HRH plan through the CCF approach.
Zimbabwe• Zimbabwe has developed its second HRH plan and scaled up its HRH reten-
tion scheme to cover 52% of the health workforce.
Guinea• A labour market study funded by the Alliance revealed that large numbers
of doctors are currently unemployed. Advocacy efforts by HRH committee members resulted in the recruitment of many additional medical doctors for service in rural areas during 2011.
Nigeria• The first National Conference on HRH in Abuja in October 2011 demonstrated
growing commitment, ownership and leadership on HRH by the Federal Government.
• The CCF approach was adopted by Lagos State. • Lessons learnt can be applied to other countries operating on a federal sys-
tem, such as India and Pakistan.
Cameroon• The Alliance collaborated with WHO and AFD to support Cameroon to
strengthen its HRH coordination and information base. • Effective HRH committee coordination resulted in re-opening of midwifery
schools and enrolment of 200 midwives, supported by the United Nations Population Fund (UNFPA) and other partners, leading to the development of a national HRH plan with input from diverse stakeholders.
• The Alliance and WHO partnership with AFD resulted in a highly informative study on health worker needs and workload to aid HRH planning.
Guinea,Togo,Mali,DemocraticRepublicoftheCongo• A joint programme, funded by France, between the Alliance, WHO, UNFPA,
the United Nations Children’s Fund (UNICEF) and the United Nations Entity for Gender Equality and the Empowerment of Women (UN Women) supported the “Every Woman, Every Child” initiative.
• The Alliance is facilitating the development of maternal, newborn and child health workforce strategies to be included in national health strategies, through CCF mechanisms.

24 25
1. Health workforce at the heart of global agendas
2. Accelerating country actions
3. Promoting evidence-based HRH solutions
4. Supporting core management functions
5. Towards the second phase of the Alliance
The outcome of the CCF approach can be summarized as follows: > greater inclusiveness in health workforce coordination and planning
processes; > greater integration of HRH in national health systems strategies and
plans; and > improved quality of HRH situation analyses, development plans and
strategies.
Accelerated implementation of HRH plans and strategies is also evident, particularly on:> scaling up training and production of health workers; > establishing or revamping training centres; > improving health worker capability through revision of training
curricula;> creating continuous professional development initiatives; > increasing levels of resource allocation to HRH from both domestic
and international sources.
CCF support has contributed to strengthening collaborative platforms at the national level, operating in synergy with existing health sector coor-dination processes. These include the International Health Partnership and related initiatives (IHP+), which aims to improve coordination and effectiveness of external assistance to countries (Box8).
A critical aspect to underscore is the complementarity of the CCF approach with work undertaken by members and partners. Firstly, the process sup-ported by the Alliance builds on, and relies on the technical assistance provided by partners like WHO and Capacity Plus. In addition, the relation-ship with the national health workforce observatories is one of mutual benefit, as they are instrumental in generating a better evidence base to feed into health workforce planning and development. And finally, in sev-eral cases nongovernmental national institutions also play a critical role in driving forward national HRH policy dialogue (Box9).
Drawing lessons from the CCF process in countries
Progress and feedback from Alliance-supported countries in 2010 and 2011 confirmed the value and important role of the Alliance in promoting the CCF approach, and that its technical and financial support has brought positive changes in the health workforce, ultimately resulting in lives saved and improved health.

26
Figure 3. Results of CCF support (2009–2011)
Embedded and integrated in national health policy dialogue and national health strategy.
Major steps on HRH in the CCF process
Step 2HRHSituationanalysis
Step 1HRHcoordinationmechanism
Step 3HRH plandevelopment
Step 4Resourcemobilization
Step 5HRH planimplemen-tation
Step 6M&Eof HRH plan
S1
S2
S3
S4
S5
S6
0
5
10
15
20
Basline 2009 end 2011
2
5
3
0 0 0 0
18
9 9
12
17
Countries at advancing levels of implementing the CCF approach, as at December 2011:
Step 1: Afghanistan, Burkina Faso, Cameroon, Chad, Comoros, El Salvador, Guinea, Indonesia, Mali, Nepal, Nigeria,
Pakistan, Paraguay, Peru, South Sudan, Sudan, Zambia and Zimbabwe.
Step 2: Afghanistan, Burkina Faso, Cameroon, Chad, Congo, Comoros, El Salvador, Guinea, Indonesia, Mali, Nepal,
Nigeria, Paraguay, Peru, Sudan, Zambia and Zimbabwe.
Step 3: Chad, Congo, El Salvador, Indonesia, Mali, Nepal, Nigeria, Paraguay, Peru, Sudan, Zambia and Zimbabwe.
Step 4: Chad, El Salvador, Indonesia, Mali, Paraguay, Peru, Sudan, Zambia and Zimbabwe.
Step 5: Chad, El Salvador, Indonesia, Mali, Paraguay, Peru, Sudan, Zambia and Zimbabwe.
Step 6: No country has yet reached this stage.

26 27
1. Health workforce at the heart of global agendas
2. Accelerating country actions
3. Promoting evidence-based HRH solutions
4. Supporting core management functions
5. Towards the second phase of the Alliance
These findings were reiterated in rapid assessments and case studies on CCF support, developed by the Secretariat in Sudan, Zambia and Zimbabwe. They were also corroborated through the external evaluation (seeSection4), which looked specifically at the results of CCF support in Cameroon, Indonesia and Zambia.
The findings of both the Secretariat assessments and the independent external evaluation are consistent, and point towards a positive impact on HRH coordination, policy dialogue and planning processes at national level, which is valued by countries and often results in increased alloca-tion of resources to HRH.
At the same time, the assessments revealed that the success of the process is dependent on national leadership, as very limited progress was made in a few countries where commitment appeared to be wavering. Moreover, the real test of the CCF approach will be whether it succeeds in catalysing improvement in HRH availability and distribution, beyond strengthening coordination and facilitating policy dialogue.
Early results of the CCF process in 10 countries were documented and disseminated as case studies, posters and presentations, and formed the basis of a dedicated CCF side event at the Second Global Forum in January
IntegratingHRHintowiderhealthsectorplanning:JointAssessmentofNationalHealthStrategies/IHP+processinMali Box8
The Alliance participated in the joint evaluation of the 10-year health plan in Mali, led by the Ministry of
Health and facilitated by WHO headquarters and the Country Office. The Joint Assessment of National Health
Strategies (JANS) framework and tools, a cornerstone of the IHP+ approach, was used for this activity. Such
joint assessments are an inclusive and participatory approach to analyse the strengths and weaknesses of a
national strategy. The goal is that national planning processes will be strengthened and partner confidence
increased to invest in the strategies, thereby contributing to more predictable and better aligned funding.
The JANS assessment in Mali was carried out in May 2011 with participation of national stakeholders, including
HRH committee members and international partners such as European Commission, Global Fund, GAVI, World
Bank, and the Alliance Secretariat. The health plan was evaluated, including its HRH components. The exercise
was conducted with the full engagement of related stakeholders such as ministry of finance, ministry of educa-
tion, private sector, NGOs, NGOs and academic institutions, in line with the CCF process. As a result of the JANS
and based on its findings, a roadmap was defined for the health plan with a strengthened HRH component.

28
2011. These materials4 continue to be used for advocacy and promotion of the CCF process in the 10 countries and others.
Promoting HRH policy dialogue at regional level
In addition to its work providing direct catalytic support to individual coun-tries, the Alliance has continued promoting policy dialogue and exchange of best practices through the work of several regional networks and part-nerships, including WHO regional offices, the African Platform on Human Resources for Health (APHRH), the Africa Public Health Alliance and 15%+ Campaign (APHA), the Asia-Pacific Action Alliance on Human Resources for Health (AAAH), and the Harmonization for Health in Africa (HHA).
In partnership with WHO, the Alliance Secretariat worked to mainstream an HRH perspective in the regional conference on Partners for Health in South-East Asia, held in New Delhi, India in March 2011. The major find-ings relative to this region of the progress report on the Kampala Declara-tion and Agenda for Global Action were shared, along with key messages emerging from the Second Global Forum on HRH.
The African Platform on Human Resources for Health is a continent-wide network with an all-inclusive, open membership of organizations, institu-tions and agencies interested in HRH from public, private and civil society, whose mandate is supported by the African Union and other major African
4 These materials are available on the Global Health Workforce Alliance web site at http://www.who.int/workforcealliance/knowledge/resources/ccfresources/en/index.html
Engagingmembers,partnersandnationalinstitutionsinsupportoftheCCFapproach Box9
The Alliance acts as a backstop to countries both directly, through WHO country offices, and by engaging
national research, academic or training institutions in countries such as Afghanistan, Burkina Faso (Institute
of Research in Health Sciences), Cameroon (Centre for the Development of Best Practices in Health), Nigeria
(Foundation for Sustainable Health Development) and Pakistan (Health Services Academy). The engagement
of national institutions was instrumental in providing advice and support on all the steps in the CCF approach;
these include establishing and/or strengthening multi-stakeholder coordination mechanisms on HRH; stake-
holder analyses; updating situation analyses; and evidenced-based HRH planning and costing, along with its
implementation and monitoring, with proactive engagement of the HRH stakeholders.

28 29
1. Health workforce at the heart of global agendas
2. Accelerating country actions
3. Promoting evidence-based HRH solutions
4. Supporting core management functions
5. Towards the second phase of the Alliance
stakeholders. The year 2011 witnessed renewed strengthening of this important regional body: with support from the Alliance, the Platform was revamped and a Governing Board under new leadership was announced. The African Platform has also started outlining a vision and a plan of action for its work in the years to come.
The Alliance has also partnered with the civil-society led APHA and the 15% Campaign to appeal to African leaders, through African ministerial meetings, to influence the agenda and proceedings of the African Union Summit with a view to increasing investment in health, and in HRH in particular. This advocacy work was supported by fact sheets illustrating the levels of financial investment and of HRH access in the region, which have proven to be effective communication tools.
In 2011 the Alliance joined the HHA initiative, a regional mechanism through which partners5 harmonize their assistance in Africa towards strengthened health systems and reaching the Millennium Development Goals (MDGs). The HHA also offers a platform for operational support and capacity-building in countries. The Alliance wholeheartedly supports the mission of improving harmonization and alignment spearheaded by the HHA, and is specifically involved in its HRH Community of Practice.
The AAAH was established in 2005 in response to international recogni-tion of the need for global and regional action to strengthen HRH plan-ning at the country level and change in health workforce systems. The AAAHRH continued to flourish in 2011, gaining importance in the region and increasing its membership to 16 countries. It has been an implement-ing partner of the Alliance in the Asia-Pacific region since 2007.
The annual conference of the Organization took place in Cebu, the Philip-pines in November 2011, focusing on the theme of capacity-building for HRH management and development to support universal health cover-age. The conference reviewed the HRH situation in member countries and showcased interventions for specific HRH problems. These included country examples of successful roll-out of the CCF approach and its impact on HRH development.
5 Partners include the African Development Bank, Japan International Cooperation Agency, Norwegian Agency for Development Cooperation, Joint United Nations Programme on HIV/AIDS, United Nations Population Fund, United Nations Children’s Fund, United States Agency for International Development, World Health Organization and World Bank.

30
2011AfricaHumanResourcesforHealthScorecard–IncorporatingSkilledHealthPersonnel,MaternalMortality,ReproductiveHealthandFemaleLifeExpectancyatBirth
SummaryofFindings:> Absence of skilled health personnel at birth is strongest contributing factor to Maternal
Death. In 5 most affected countries only 6% to 33% of births had skilled attendant present, compared to 93% to 99% in 5 least affected countries.
> Antenatal Coverage (by at least 4 visit), which is affected by health work force, is poorest in the 5 most affected countries.
> Access to Reproductive & Sexual Health Advice & Commodities (also affected by health workforce) is vital to progress. In 5 most affected countries a poor 2.8% – 14.7% of couples report use of family planning. In 5 least affected countries 44,4% – 75.8% of couples report use of family planning.
> 4 of the most affected countries have adolescent fertility rates of between 109 and 199 per 1,000 girls aged 15 – 19, higher than those of the 5 least affected countries which ranges between 4 and 59. This indicates that more young persons get pregnant at shool age due to early marriage and/or poor contraceptive availability. This high birth rate puts further pres-sure on the already over burdened health workforce.
> Main causes of Maternal Death are: Hemorrhage; Hypertensive disorders; Sepsis infec-tions; Anemia; Obstructed labour; Complications of abortion; & increasingly HIV/AIDS related complications in expectant mothers.
> No quick fix. Poor ratio of health workforce (doctors, nurses & midwives and pharmacists) to population means most countries will need to double, triple or even quadruple numbers of health workforce to make long term & sustainable progress on Maternal Health (& other health needs). Rapid changes in long term, education, & labour policies (training & reten-tion) are required, including integration with health planning.
> Crucial combination of policy as well as budget interventions is required in countries to reverse the trend and improve training and retention of Health Workforce.
Full Health Scorecard is available at:http://www.who.int/workforcealliance/media/news/2012/2012AfricaHRHScorecard.pdf

30 31
1. Health workforce at the heart of global agendas
2. Accelerating country actions
3. Promoting evidence-based HRH solutions
4. Supporting core management functions
5. Towards the second phase of the Alliance

Promoting evidence-based HRH solutions
other leading academic institutions in the south, to develop a systematic review and country case studies on the role and contribution of mid-level health providers. This endeavour builds on and complements prior Alliance work on CHWs, and is expected to feed into the guidelines on task shifting of essential services for MDG 4 and 5, cur-rently under development by WHO. The systematic review was finalized and country case studies con-ducted in Latin America (El Salvador and Peru), in Africa (Mozambique, United Republic of Tanzania, and Zambia), and Asia (Bangladesh, Indonesia, and Pakistan). The report, consolidating the find-ings of the systematic review with the country case studies, is expected to be finalized by mid-2012.
Joint statement on Scaling-up the Community-Based Health Workforce for Emergencies
The Alliance dedicated attention in 2011 to the critical issue of responding to emergency situa-tions. Joining forces with a number of partners,6
In 2011 substantive progress was made on activi-ties supported by the Alliance to promote adop-tion of evidence-based HRH solutions. Areas of focus included the role of CHWs in emergency settings; analytical work on the role and integra-tion in health systems of mid-level health provid-ers; the private sector contribution to strengthen the health workforce; and support to leadership development in francophone countries (Box 10). Many of these initiatives represent endeavours with a medium-term horizon; thus, some that came to a conclusion in 2011 were initiated much earlier, while others that commenced in 2011 are due for completion only in 2012.
Systematic review and case studies of mid-level health providers
Robust evidence is required on the use of different health workforce cadres for an appropriate and cost-effective skill mix to address priority health problems. To this end, the Alliance commissioned a consortium led by Aga Khan University, involving

3Promoting evidence-based
HRH solutions
the Alliance developed a joint statement on Scal-ing-up the Community-Based Health Workforce for Emergencies. The statement highlights the vital role of community health workers in building local resilience to disasters, and calls for greater emphasis on front-line health workers in health-system planning and preparedness for all phases of emergency risk management. It also provides a range of concrete country examples of community-based health workforce in action.
Private sector role in HRH development
The private sector (defined as domestic for-profit, domestic not-for-profit, faith-based, multinational corporate, foundations and universities, etc.) provides a significant proportion of health-care services and products in the least and less devel-oped countries of the world.
6 These partners included the International Federation of Red Cross and Red Crescent Societies, the United Nations High Com-missioner for Refugees, UNICEF and WHO, with support from the Asian Disaster Preparedness Centre, the International Medical Corps, the United Nations International Strategy for Disaster Reduction, Merlin and Save the Children.

34
The private health sector in the developing world is poorly under-stood, best practices are not documented, promising initiatives are not scaled for broader application, and there is sometimes mistrust between the public and private sectors. To address some of these issues, the Alliance has supported since 2009 the work of a multi-agency task force7 (whose Secretariat is hosted by Duke University) on private sector involvement in HRH development.
The work of the task force was instrumental in identifying promis-ing innovative private sector models that could be scaled up and replicated in other contexts, with the overall goal of increasing the supply of new workers, improving the efficiency and effectiveness of existing health workers, and reducing the attrition of health workers out of the field of practice or the region. The task force completed its work in late 2011, and the launch of its final report is expected to take place at the Sixty-fifth World Health Assembly in May 2012.
MasterofPublicHealthwithfocusonHRHforfrancophonecountries Box10
After preparations in 2009 – 2010, the Masters Programme in Public Health with a focus on HRH leadership and
management taught in French was finally launched, with the first cohort of 37 distance learning students start-
ing the course in 2011. These students originated from 10 French-speaking countries, namely Burkina Faso,
Burundi, Cameroon, Central African Republic, Chad, Congo, Côte d’Ivoire, Democratic Republic of the Congo,
Mali and Senegal. This initiative is implemented in collaboration with the University of Geneva (Switzerland)
and WHO.
7 Private Sector Task Force Members: Elizabeth Ashbourne, World Bank; Wolfgang Bichmann, KfW Entwicklungsbank; Brian Brink, Anglo American plc (Co-Chair); Kathy Cahill, Harvard Global Equity Initiative; Collin Chansa, Ministry of Health, Zambia; Delanyo Dovlo, WHO; Manuel Dayrit, WHO; Renuka Gadde, Becton Dickinson and Company; Yacouba Koné, Aga Khan Develop-ment Network, Mali; Christophe Lemière, Africa Region, World Bank; Marty Makinen, Results for Development Institute; Jeff Moe, Duke Global Health Institute (Taskforce Director); Michael Merson, Duke Global Health Institute (Co-Chair); John and Viv-ian Mthetwa, Master Trainers, Consultants, Zambia; Stefan Nachuk, Rockefeller Foundation; Maureen Nafula, Kenya Health Ser-vice; Peter Ngatia, AMREF, Kenya; Francis Omaswa, African Centre for Global Health and Social Transformation: Srinath Reddy, Public Health Foundation of India; Ken Sagoe, Ghana Health Service; Neeraj Sood, Leonard D. Schaeffer Center for Health Policy and Economics, University of Southern California; Marie-Odile Waty, Agence Française de Développement.

34 35
1. Health workforce at the heart of global agendas
2. Accelerating country actions
3. Promoting evidence-based HRH solutions
4. Supporting core management functions
5. Towards the second phase of the Alliance
UN OneHealth Costing Tool
The Alliance contributed technically and financially to the development of an integrated UN OneHealth planning and costing tool (formerly the Unified Health Module). Following a desk review and consultations of an interagency working group composed of UNAIDS, UNDP, UNFPA, UNICEF, WHO and the World Bank, a capacity-building programme commenced to train various UN agency technical officers and selected consultants who will provide support to countries. The HRH module of the tool builds on the Resource Requirement Tool developed by the Alliance, and will sup-port country efforts to make realistic forecasts of the cost implications and requirement of their HRH scale-up plans.
AlliancememberscontributeglobalpublicgoodsforHRHdevelopment Box11
Alliance members and partners contribute to building evidence on HRH solutions. In 2011, Capacity Plus – a
USAID-funded global project uniquely focused on the health workforce needed to achieve the MDGs – pro-
duced tools such as the Pre-Service Education Toolkit, an HRH Indicator Compendium and Guidelines for
Forming and Sustaining Stakeholder Leadership Groups. It also hosts the HRH Global Resource Centre which
is a global library of HRH resources focused on developing countries, where these and other tools contributed
by members are posted. Capacity Plus also runs an e-learning programme that offers free courses developed
by technical experts in the fields of HRH, health informatics and health service delivery, to build the capacity
of country-based users in critical skills.
The results of the multi-year and -country research on Mobility of Health Professionals (MoHProf ) were
presented at the international conference Ensuring Tomorrow’s Health: Workforce Planning and Mobility in
Brussels in December 2011, organized by an Alliance partner, the International Organization for Migration. The
research studied current trends of mobility of health professionals to, from and within the European Union.
The Alliance contributed to the research as a member of its Advisory Board. MoHProf contributes to improving
the knowledge base for, and facilitates European policy on human resource planning as well as on managing
migration of health professionals.

Supporting core management functions
members of the Alliance were given a stronger voice: two dedicated sessions for membership issues were organized on the occasion of the Second Global Forum, giving Alliance members an opportunity to interact with one another and to convey their suggestions on HRH in general, and Alliance work in particular, directly to the Board and Secretariat.
The findings of the survey fed into Alliance man-agement decisions on implementation of the Secretariat activities with a renewed emphasis on empowering members, and provided input into early discussions at Board level on the develop-ment of the new Alliance strategy (seeSection5).
Corporate communications
A number of initiatives were undertaken in 2011 to keep Alliance members, partners and other stake-holders abreast of Alliance work. The Alliance expanded its use of social media and established Facebook and Twitter accounts with the aim of targeting broader and younger audiences. A flickr
Governance
Throughout 2011 the Alliance ensured adequate governance of its structures, in line with the provi-sions of its governance handbook.
The Board met twice, holding its 11th and 12th meetings in January and June, respectively, where important decisions included the commissioning of an external evaluation.
Furthermore, the Board agreed to revisions in its own composition, including the creation of posi-tions for ‘Associate Board members’ for partners providing support to the Alliance in excess of US$ 300 000 per year, additional Board seats for representatives of the private for-profit sector, and for individual health workers beyond the existing seats for professional associations.
Membership and partnership issues
Membership continued to grow steadily, crossing the 400 mark by the end of 2011. More importantly,

Supporting core management functions
account, housing photographs of various events, was revamped and updated to include photo gal-leries of events at the Second Global Forum and other meetings held throughout the year. The Alliance multimedia gallery was continuously updated to include new health worker videos from partner organizations working on HRH.
With the aim of improving communications, the Secretariat revisited its news services to its sub-scribers. A new e-mail-based monthly newsletter was introduced, which replaced the quarterly newsletter. A survey on the new format and regu-larity of the newsletter was conducted received positive feedback. Web site content continued to
4
Post forum members session, at the Second Global Forum on Human Resources for Health, Bangkok, Thailand.

38
diversify with new material available in the core languages of French and Spanish. Work also commenced on the creation of dedicated CCF country profile pages. Several corporate products were developed and dissemi-nated, including an advocacy brochure following the Second Global Forum and the 2010 Annual Report. Work on the production and dissemination of several other knowledge products was also undertaken.
External evaluation
The end of 2011 marked the conclusion of the Alliance’s three-year strat-egy Moving Forward from Kampala, and the completion of its first five years of existence. This intermediate milestone warranted an analysis of its achievements, strengths, weaknesses, opportunities and threats for
Resultsofa2011surveyamongAlliancemembersandpartners Box12
A survey conducted in 2011 indicated that members and partners: > value the Alliance as a collaborative mechanism, and see its key strength as the ability to convene all
stakeholders, catalyse action, and generate consensus on important policy and technical HRH issues; > expect, at the same time, greater coordination and stewardship of their efforts in terms of joint messag-
ing, communications, tools, advocacy targets and benchmarks;> seek more venues and mechanisms for regular interaction and networking, and encourage the Board and
Secretariat to galvanise more effectively the involvement of the wider Alliance membership to address the
HRH crisis.
Snapshot of a CCF country page from the Alliance website

38 39
1. Health workforce at the heart of global agendas
2. Accelerating country actions
3. Promoting evidence-based HRH solutions
4. Supporting core management functions
5. Towards the second phase of the Alliance
the years to come, and preparation of its next strategic plan. As part of this process, the Alliance commissioned an external evaluation, which was conducted by the UK-based firm Oxford Policy Management, a con-tractor selected on the basis of a competitive tendering process overseen by a task team of Board members. The independent evaluation entailed an analysis of literature and documentation, interviews, focus group discussions and questionnaires sent to key informants, and country case studies.
The external evaluation, completed in late 2011, highlighted both strengths and areas requiring improvement (Box13).
Budget and finance
In the course of 2011, the aggregated Alliance income of US$ 3 955 301 (net of programme support costs), along with its carry-forward funding from the previous year, resulted in fund availability of US$ 8 988 699. Of this income, recorded expenditures amounted to US$ 6 779 159. The balance as of 31 December 2011 of US$ 2 209 540 is the projected carry forward into 2012. The composition of the 2011 income and breakdown of expenditures is reflected in Table1.
Externalevaluationkeyfindings Box13
In reviewing the areas where the Alliance has exceeded, met or not met initial expectations, the external
evaluation:> concluded that the Alliance work in its first five years represented good value for money; > recognized the critical contributions made by the Alliance Secretariat in moving forward the health
workforce agenda at global and country levels through its advocacy, knowledge brokering and convening
functions;> noted that the work of the Alliance Secretariat was highly relevant at all levels, and considered its support
to countries through the Country Coordination and Facilitation approach to be highly effective.
At the same time, the evaluation identified areas that required improvement, including:> better harnessing of Alliance member contributions; > ensuring wider use of knowledge products and gaining better visibility and brand recognition;> reviewing the Board’s effectiveness;> streamlining administrative procedures and the relationship with WHO; and> securing more stable income flows.

40
The Alliance acknowledges the following donors whose collective fund-ing contributed to the implementation of the Alliance 2011 workplan: Agence Française de Développement, Canadian International Develop-ment Agency, Department for International Development of the United Kingdom, Deutsche Gesellschaft für Internationale Zusammenarbeit, European Commission, Irish Aid, Japan Ministry of Health, Labour and Wel-fare, Norwegian Agency for Development Corporation, and United States Agency for International Development.
Table 1. Annual Financial Statement of the Alliance as of 31 December 2011
Financialoverview2011 US$
Income
Opening balance at 1 January 2011 4 588 878
Reserved funds – contingent liability 444 520
New grants in 2011 (net of PSC) 3 955 301
Totalavailablefunds2011 8 988 699
Expenditure
2011 Workplan expenditure and encumbrances 5 587 706
2nd Global Forum expenditure and encumbrances 849 453
Accrued liability 342 000
2011expenditure(netofProgrammeSupportCosts) 6 779 159
WHO Programme Support Cost (13%) 881 290
2011TotalExpenditures 7 660 450
Closingbalanceat31December2011 2 209 540

40 41
1. Health workforce at the heart of global agendas
2. Accelerating country actions
3. Promoting evidence-based HRH solutions
4. Supporting core management functions
5. Towards the second phase of the Alliance
2011WorkplanExpenditureandEncumbrances US$
Expendituresandencumbrances
Objective1:
Within the context of the Kam-
pala Declaration and Agenda
for Global Action, country
leadership mobilized to improve
the HRH situation and response
to shortages, mal-distribution,
weak management and support
of skilled and motivated health
workforce.
1.0 Mobilize political leadership 1 3372.0 Ensure an evidence- and needs-
based response
59 831
3.0 Support selected priority
countries to address HRH crisis
805 096
SubtotalObjective1 866 264
Objective2:
Effective and synergistic partner-
ships mobilized to address
transnational policy challenges
through evidence-informed
actions
4.0 Strengthen partnerships of
entities involved in HRH
145 477
5.0 Mobilize political leadership 229 309 6.0 Address HRH challenges 211 601
SubtotalObjective2 586 387
Objective3:
The Alliance Secretariat and
workplans effectively and
efficiently managed, monitored
and assessed
7.0 Ensure good governance and
management
157 605
8.0 Evaluate Alliance operations 106 401
Staff costs 3 871 049
SubtotalObjective3 4 135 055
SubtotalObjective1,2,3 5 587 706
Accrued liability 342 000 2nd Global Forum 849 453
2011 Total Alliance expenditure
andencumbrances(netofPSC)
6 779 159

42
Figure 4. Alliance catalytic support through distributions to countries and regions, 2011 *
* see task 3.0 in table1
Zambia6%
Republic ofthe Congo
7%
Chad7%
Burkina Faso14%
Guinea12%
Pakistan10%
Indonesia8%
Afghanistan10%
Nepal2%Nigeria
10%
Peru / Paraguay
14%
42 43
1. Health workforce at the heart of global agendas
2. Accelerating country actions
3. Promoting evidence-based HRH solutions
4. Supporting core management functions
5. Towards the second phase of the Alliance
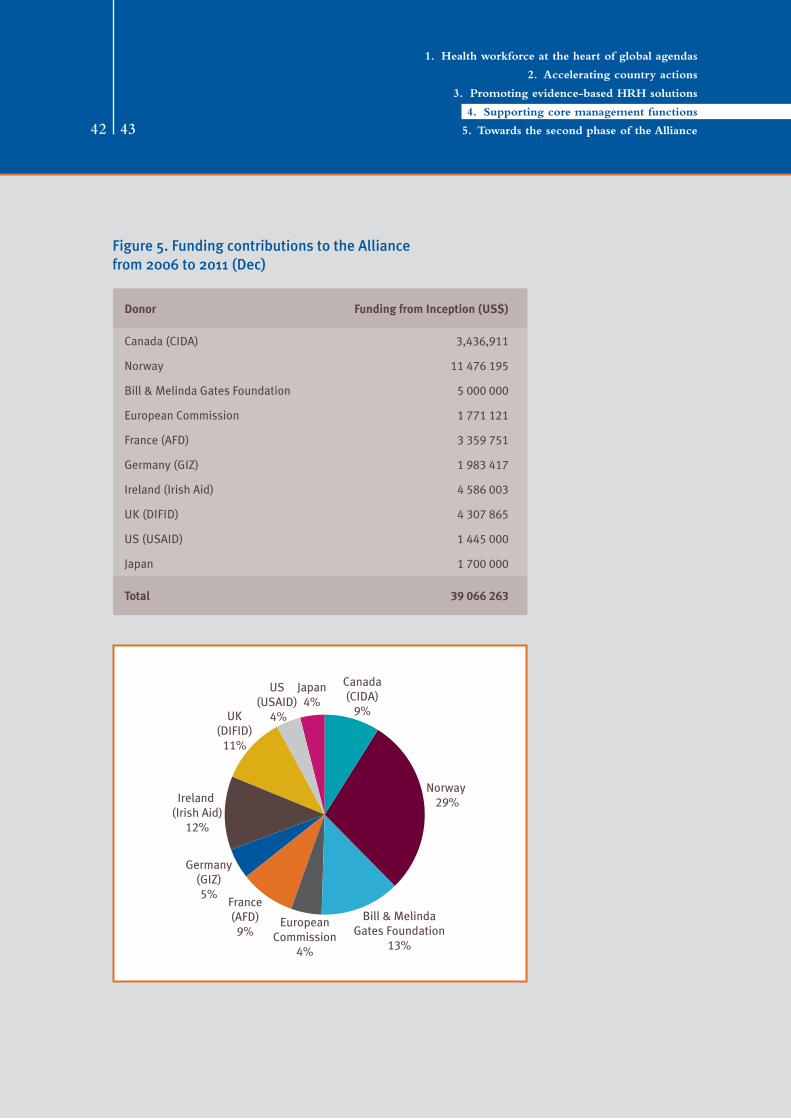
Figure 5. Funding contributions to the Alliance from 2006 to 2011 (Dec)
Donor FundingfromInception(US$)
Canada (CIDA) 3,436,911
Norway 11 476 195
Bill & Melinda Gates Foundation 5 000 000
European Commission 1 771 121
France (AFD) 3 359 751
Germany (GIZ) 1 983 417
Ireland (Irish Aid) 4 586 003
UK (DIFID) 4 307 865
US (USAID) 1 445 000
Japan 1 700 000
Total 39 066 263
EuropeanCommission
4%
France(AFD)
9%
Germany(GIZ)5%
Ireland (Irish Aid)
12%
UK(DIFID)
11%
US(USAID)
4%
Canada(CIDA)
9%
Norway 29%
Bill & MelindaGates Foundation
13%
Japan4%

Towards the second phase of the Alliance
> As knowledge broker, the Alliance developed innovative knowledge products on diverse themes which directly contributed to the HRH policy discourse at global and national levels.
> The Alliance Country Coordination and Facilita-tion approach, created as a collaborative plat-form at the national level, allows all relevant HRH players to join together to identify health workforce challenges and collaborate in the development and implementation of solutions, embedded in national health strategies. This generated great demand for support from countries, and is yielding results in terms of new and updated HRH situation analyses and country profiles; HRH coordination commit-tees; HRH plans; additional resources for HRH by development partners; and accelerated implementation of health workforce strategies and initiatives.
As a result of these efforts, national, regional and global leaders now recognize the critical
In 2012, building on the review of progress, achievements and challenges to date and find-ings from the external evaluation, the Alliance will embark on the development of a new strategic plan for 2013–2016.
The foundations laid over the past five years, in partnership with several hundred national, regional and global partners, serve as a strong basis for the Alliance’s future work:
> In convening two landmark meetings on HRH, the First and Second Global Forums in 2008 and 2011, the Alliance drew much needed attention on the the health workforce, main-streaming key issues in health and develop-ment agendas at all levels.
> In developing the Kampala Declaration and Agenda for Global Action, the Alliance created a unique global framework to tackle prob-lems, monitor implementation and encourage accountability.

5Towards the second
phase of the Alliance
importance of investing in and developing a sup-ported health workforce to improve health out-comes. These gains are, however, vulnerable: without sustained efforts, the relatively good recognition of HRH risks being diluted to just one of several elements of the health systems strengthening agenda.
Indeed, the HRH crisis is still an acutely limiting factor in countries’ attempts to reduce maternal and child mortality, to control priority infectious and noncommunicable diseases, and to attain the broader target of universal health coverage. This is due to persisting gaps in support to, and the train-ing and deployment of health workers. The development of the new strategic framework will outline a roadmap to address the HRH gaps, ensuring that the Alliance remains relevant to, and influences the evolving global health and develop-ment landscape.
Much more needs to be done and the Alliance remains in a strong position to tackle the unfinished
HRH agenda with renewed vigour and dedication, even against a backdrop of stagnating resources for global health and its evolving landscape.
The Alliance will develop its strategy for the second phase (2013–2016) through an inclusive consultation process led by its governing Board, and directly involving its members and partners.
Through its new strategy, built on the principle of greater harnessing of member and partner strengths, the Alliance will enable more countries to progress in planning, mobilizing resources and implementing a response to their health workforce challenges. It will enable health workforce issues to remain prominent on national and global agen-das. It will encourage further synergy among part-ners, better information, and result in improved policy-making and accountability. Ultimately, these efforts will pave the way for further improve-ments in the health workforce, and progress towards the universal health coverage goal for all citizens around the world.

4646

4646 47
TheAllianceisgratefultothefollowingdonorsfortheirsupportin2011:
> Canadian International Development Agency (CIDA)> European Commission> France/French Development Agency (AFD)> Deutsche Gesellschaft für Internationale Zusammenarbeit (GIZ) Gmbh,
Germany > Irish Aid, Department of Foreign Affairs, Ireland > Ministry of Health, Labour and Welfare, Japan> Norwegian Agency for Development Cooperation (NORAD)> United Kingdom Department for International Development (DFID)> United States Agency for International Development (USAID)

48
Launched in 2006, the GlobalHealthWorkforceAlliance is a partnership dedicated to iden-tifying and coordinating solutions to the health workforce crisis. It brings together a variety of actors, including national governments, civil society, finance institutions, health workers, international agencies, academic institutions and professional associations. The Alliance is hosted by the World Health Organization.
Forfurtherinformation,pleasecontact:
GlobalHealthWorkforceAllianceWorld Health OrganizationAvenue Appia 201211 Geneva 27SwitzerlandTel: +41 22 791 26 21 Fax: +41 22 791 48 41Email: [email protected]: www.who.int/workforcealliance