
The FQHC Advantage - aachc.org
41
THE FQHC ADVANTAGE IN THE TRANSITION TO VALUE-BASED CARE ORAL HEALTH VALUE-BASED CARE METHODOLOGY AND PREPARATION BOB RUSSELL DDS, MPH, MPA, CPM, FACD, FICD
Transcript of The FQHC Advantage - aachc.org
THE FQHC ADVANTAGE IN THE TRANSITION TO VALUE-BASED CAREORAL HEALTH VALUE-BASED CARE METHODOLOGY AND PREPARATION
BOB RUSSELL DDS, MPH, MPA, CPM, FACD, FICD
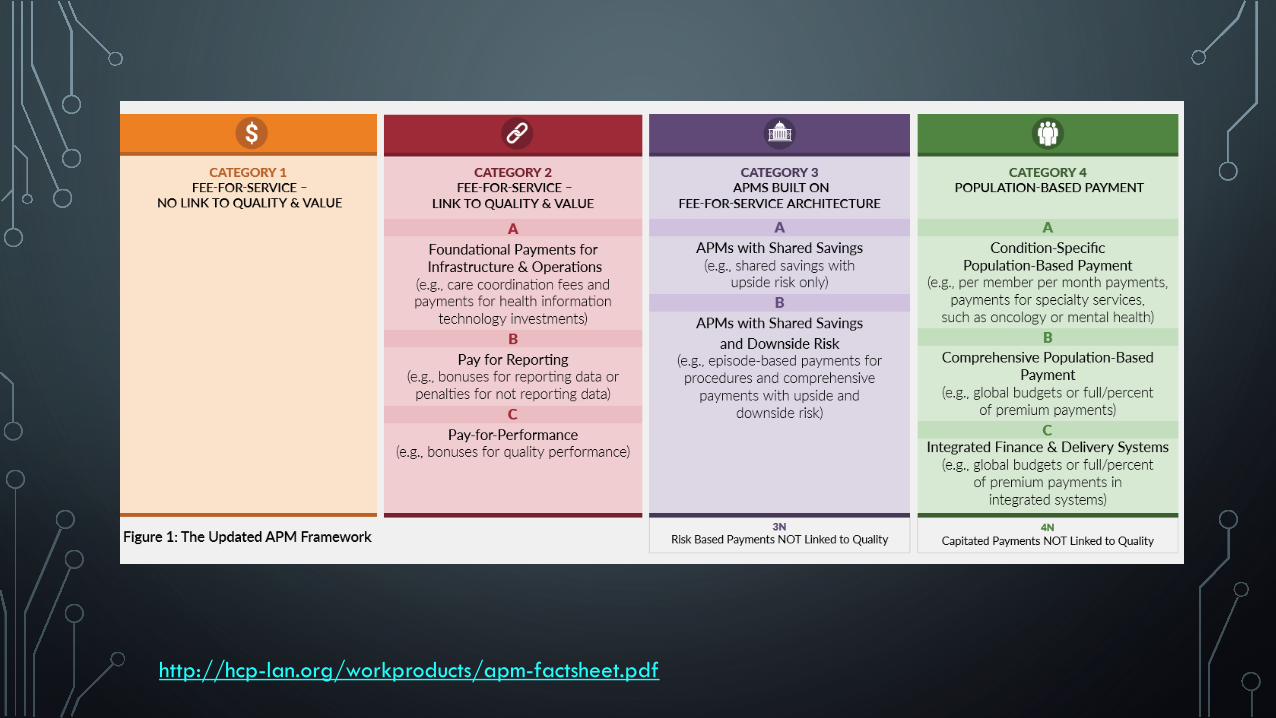
For an FQHC that demonstrates attainment of the Minimum Performance Standard (MPS) for one or more clinical quality measures, as reported for each FQHC in the Uniform Data System (UDS) Report to the Bureau of Primary Health Care of the Health Resources and Services Administration (HRSA), the baseline PPS rate will be adjusted by a Differential Adjusted Payment (DAP) factor.
ARIZONA SPA #18-009, FQHC ALTERNATIVE PAYMENT MODEL; 2018
*Slide updated 2/13/2020
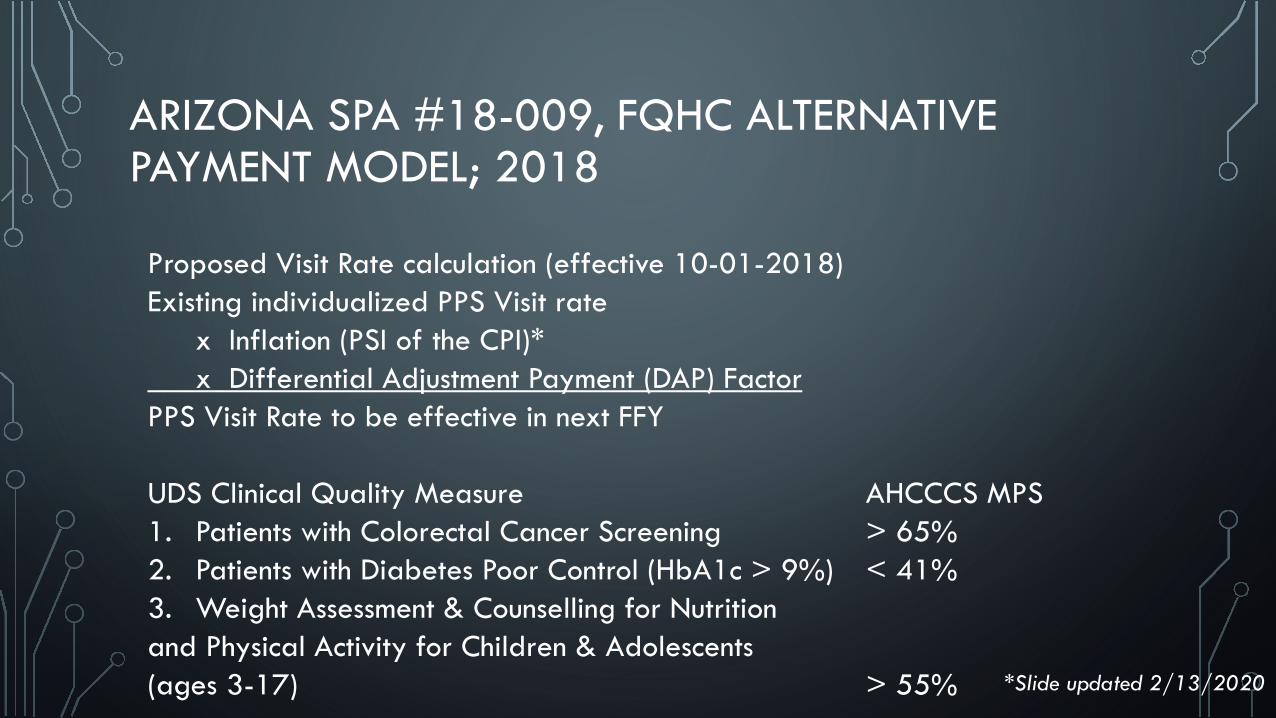
ARIZONA SPA #18-009, FQHC ALTERNATIVE PAYMENT MODEL; 2018
Proposed Visit Rate calculation (effective 10-01-2018) Existing individualized PPS Visit rate
x Inflation (PSI of the CPI)* x Differential Adjustment Payment (DAP) Factor
PPS Visit Rate to be effective in next FFY
UDS Clinical Quality Measure AHCCCS MPS 1. Patients with Colorectal Cancer Screening > 65% 2. Patients with Diabetes Poor Control (HbA1c > 9%) < 41% 3. Weight Assessment & Counselling for Nutrition and Physical Activity for Children & Adolescents (ages 3-17) > 55% *Slide updated 2/13/2020
A NATIONAL PLAN FOR FQHCS?
• Healthy Adult Opportunity Fact Sheet, Jan 30, 2020 Coverage
• States will have the opportunity to design Federally Qualified Health Center (FQHC) coverage and payment in order to facilitate the use of value-based payment design among safety-net providers.
• https://www.cms.gov/newsroom/fact-sheets/healthy-adult-opportunity-fact-sheet?utm_medium=email&utm_source=govdelivery
ORAL DISEASE IS THE 4TH MOST EXPENSIVE DISEASE TO TREAT IN MOST INDUSTRIALIZED COUNTRIES
World Health Organization. Oral health: what is the burden of oral disease? http://www.who.int/oral_health/disease_burden/global/en/; http://www.worldoralhealthday.com/wp-content/uploads/2014/03/FDIWhitePaper_OralHealthWorldwide.pdf
SIGNS OF CHANGE…
• Focus on prevention and early intervention with increased focus from industry on prevention agents and devices
• Continued efforts for Medical-Dental Integration (MDI) and interprofessional practice
• Efforts to increase diagnostic codes utilization in dentistry• Increased use of electronic records and practice management• Continued consolidation of care delivery systems• Changing dental workforce environment• Care being delivered outside of the traditional brick and
mortar dental office
www.oralhealthworkforce.org

WHERE IS THE TREND IN VALUE-BASED CARE HEADED?
• Promoting Better Outcomes = Better Health
• Improved Quality = Better Care
• Controlled Cost = Lower Cost
• Provider Satisfaction = Clinician Experience
MEDICAL PRIMARY CARE ADVANTAGE IN VBC
• Annual Wellness Visits
• https://www.cdc.gov/policy/hst/HRA/FrameworkForHRA.pdf
• Accustomed to Disease Treatment Protocols
• Long history in using risk assessments
• Detailed Health History
• Regular use of diagnostic codes
• Most EHRs are medical focused
• Many protocols are evidence-based
• 1 Health Risk Assessment completed
• 2 Feedback received
• 3 Shared decision making to develop goals and prevention plan 4 Referrals provided
• 5 Progress monitored
• 6 Follow-up regularly
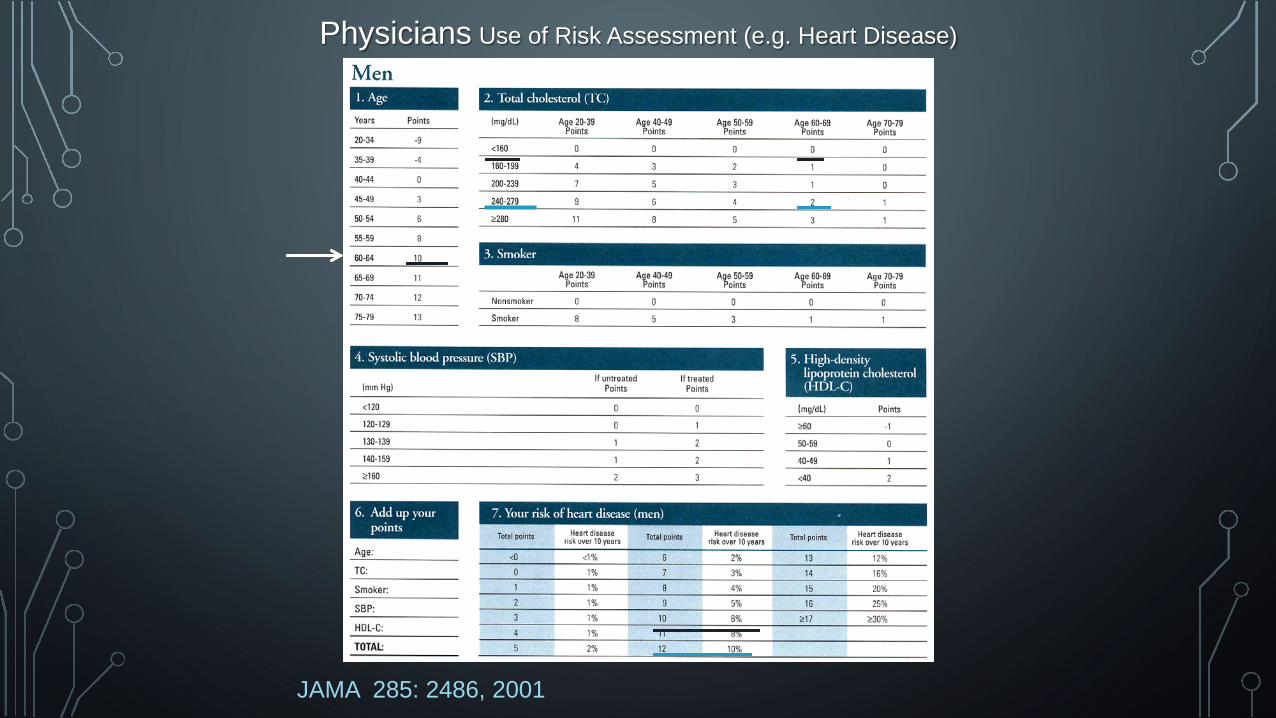
JAMA 285: 2486, 2001
Physicians Use of Risk Assessment (e.g. Heart Disease)
THE FQHC ADVANTAGE IN MEDICAL AND DENTAL
• POTENTIAL FOR INTEGRATION HEALTH CARE
• MULTIDISCIPLINE HEALTHCARE ON SITE
• ACCUSTOM TO ELECTRONIC HEALTH RECORDS
• POTENTIAL FOR EASY INTERNAL REFERRALS
• NNOHA QUALITY PRACTICE GUIDELINES (Dental)
• http://www.nnoha.org/nnoha-content/uploads/2019/10/NNOHA-Quality-Manual_V2Final.pdf
• BEGINNING TO TRACK OUTCOMES IN UDS REPORTING
• ACCUSTOM TO USING CLINICAL PROTOCOLS IN PATIENT MANAGEMENT (Medical)
• EVOLVING PATIENT CARE TRACKING CAPACITY AND USE OF SCORECARDS
• USE TO USING MEASURES AND PROTOCOLS
• LEADING IN THE USE OF DENTAL SEALANT AND FLUORIDE VARNISH MEASURES (Dental)
FQHC MEDICAL AND DENTAL DISADVANTAGES
• No standard coding language between medical and dental
• Lack of consistent data sharing in health records, if any
• Some FQHC dental and medical programs are physically separated
• Most FQHCs are different and differing levels of efficiencies
• Less Medicaid and no Medicare in dental
• Dental has roughly one-fifth or 17% (in Arizona) the patient capacity compared to medical
• All medical users may not have access to dental due to disproportion of capacity
• Lack of knowledge how value-based payment systems and care in dental can work in an FQHC
CRITICAL COMPONENTS TO VALUE-BASED CARE
• Risk Assessment Protocol
• Individualized treatment planning with emphasis on long-term prevention
• Patient tracking systems to monitor progress
• Care coordination/referral protocols that are tracked and monitored
• Multidiscipline care teams based on identified needs and risks
• Electronic Health Records that communicate across health disciplines
• Planning on resource utilization based on practice matrices and levels of compliance
• Education and training for Primary Care Providers- must see the mouth as an integral part of the body
• Training for general dentists to treat small children, pregnant women and patients with other health issues
• Patient communication – low literacy, culturally appropriate education materials
CHALLENGES
• Policies defining key processes• Case management system
designated access appointments
• Time availability in medical• User-friendly Clinical Risk
Assessment (CRA) tool• Reimbursement issues• Services not co-located
13
ORAL HEALTH HAS IMPLICATIONS IN CHRONIC DISEASE MANAGMENT
• Potential to increase morbidity in some medical chronic disease cases
• Related to a growing number of health related conditions
• Potential to save costs in chronic disease management
• Oral tissues are aids to medical diagnosis
• Mouth and body are fully integrated; why not our health care system?
• FQHCs have an opportunity to demonstrate the potential of integrated health care
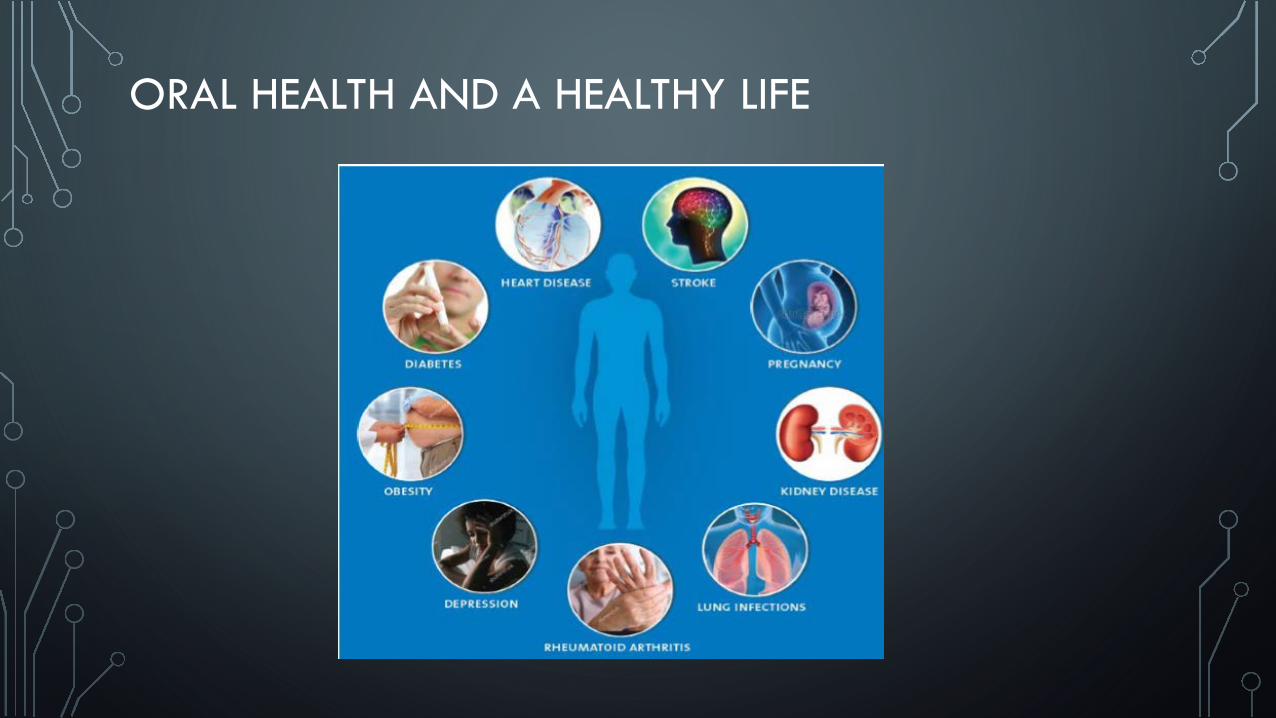
ORAL HEALTH AND A HEALTHY LIFE
https://www.dentaquestpartnership.org/system/files/April%2025%20IPP%20Webinar.pdf
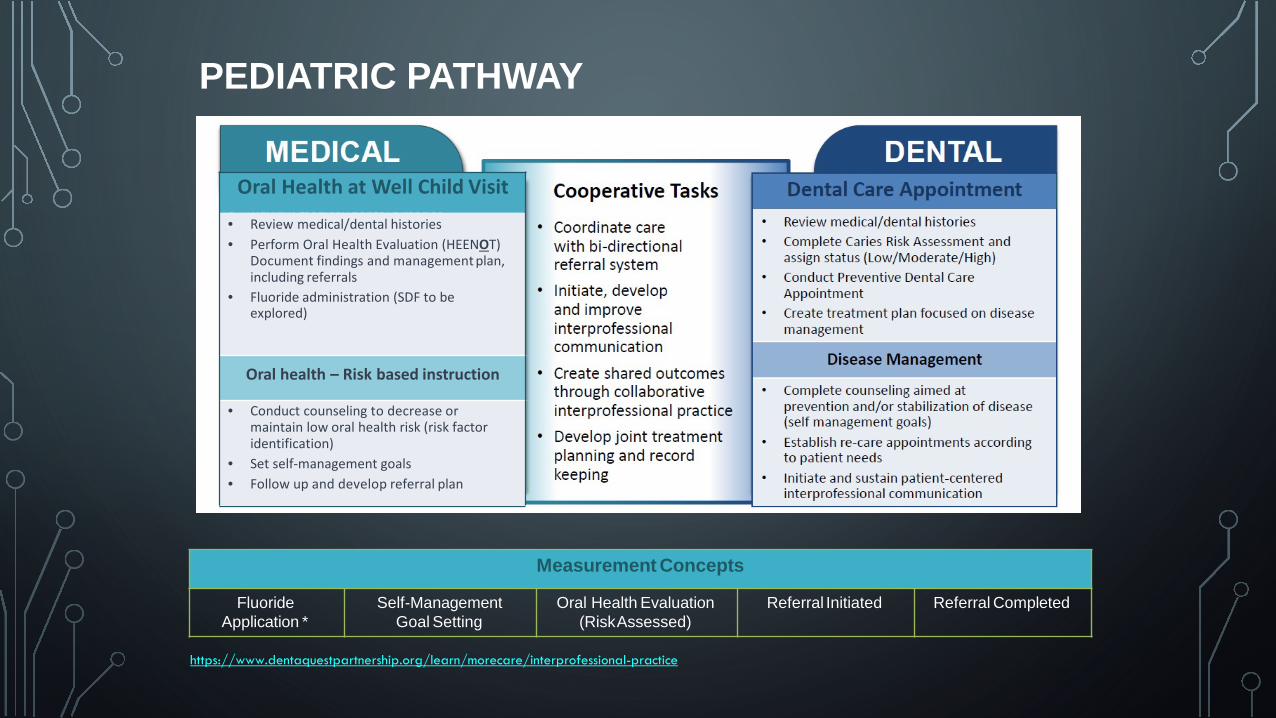
Oral Health at Well Child Visit• Review medical/dental histories• Perform Oral Health Evaluation (HEENOT)
Document findings and management plan, including referrals
• Fluoride administration (SDF to be explored)
Oral health – Risk based instruction
• Conduct counseling to decrease or maintain low oral health risk (risk factor identification)
• Set self-management goals• Follow up and develop referral plan
Oral Health at Well Child Visit
• Review medical/dental histories• Perform Oral Health Evaluation (HEENOT)
Document findings and management plan, including referrals
• Fluoride administration (SDF to be explored)
Oral health – Risk based instruction
• Conduct counseling to decrease or maintain low oral health risk (risk factor identification)
• Set self-management goals• Follow up and develop referral plan
Measurement Concepts
Fluoride Application *
Self-Management Goal Setting
Oral Health Evaluation (RiskAssessed)
Referral Initiated Referral Completed
PEDIATRIC PATHWAY
https://www.dentaquestpartnership.org/learn/morecare/interprofessional-practice
RESOURCES:
https://www.dentaquestpartnership.org/rural-ipp
https://www.hrsa.gov/sites/default/files/hrsa/oralhealth/integrationoforalhealth.pdf
http://www.qualish ealth.org/sites/defa ult/files/White-Paper-Oral-Health-Primary-Care.pdf
http://www.nnoha. org/nnoha-content/uploads/2 015/01/IPOHCCC-Users-Guide-Final_01-23-2015.pdf
ARIZONA HAS ENTERED A CATEGORY 2B/3A HYBRID
• Alternative Payment Methodology (APM) linked to UDS process measure reporting bonus
• No downside risks
• Only one to two indicators required
Value-based healthcare is a healthcare
delivery model in which providers are paid
based upon making patients healthier while
reducing costs of care.
EARLY ADOPTION OF VALUE –BASED CARE & PAYMENT PROTOCOLS IN DENTISTRY
Value-based Care Scorecard
• Provider Performance Reporting (Metrics & Measures)
• Prevention: Risk Assessments,• Sealants, Fluorides
• Access to Care & Cost of Care
• Incentives: Monetary and Non-Monetary Rewards
• Reimbursement for meeting metrics
Making it Happen
• Need for education, resources and leadership support
• Setting the right metrics that lead to measurable outcomes
• Creating an environment of change and responsibility
STEPS TO VALUE-BASED CARE IN DENTISTRY
• Start small
• Update knowledge on what VBC and VBP are and how they work
• Build on current practice efficiencies and monitoring capacity
• Get healthcare teams on board
• Get used to using metrics and monitoring as a tool to measure outcomes
SAMPLE PROCESS MEASURES
• Annual Oral Health Visit (populations)
• Treatment Plan Completed
• Topical Fluoride Treatment
• Dental Sealants https://bphc.hrsa.gov/sites/default/files/bphc/programopportunities/fundingopportunities/sac/performance-measures-crosswalk.pdf
• Oral Health Education (medical setting)
• Periodontal Exam (i.e HIV, diabetic)
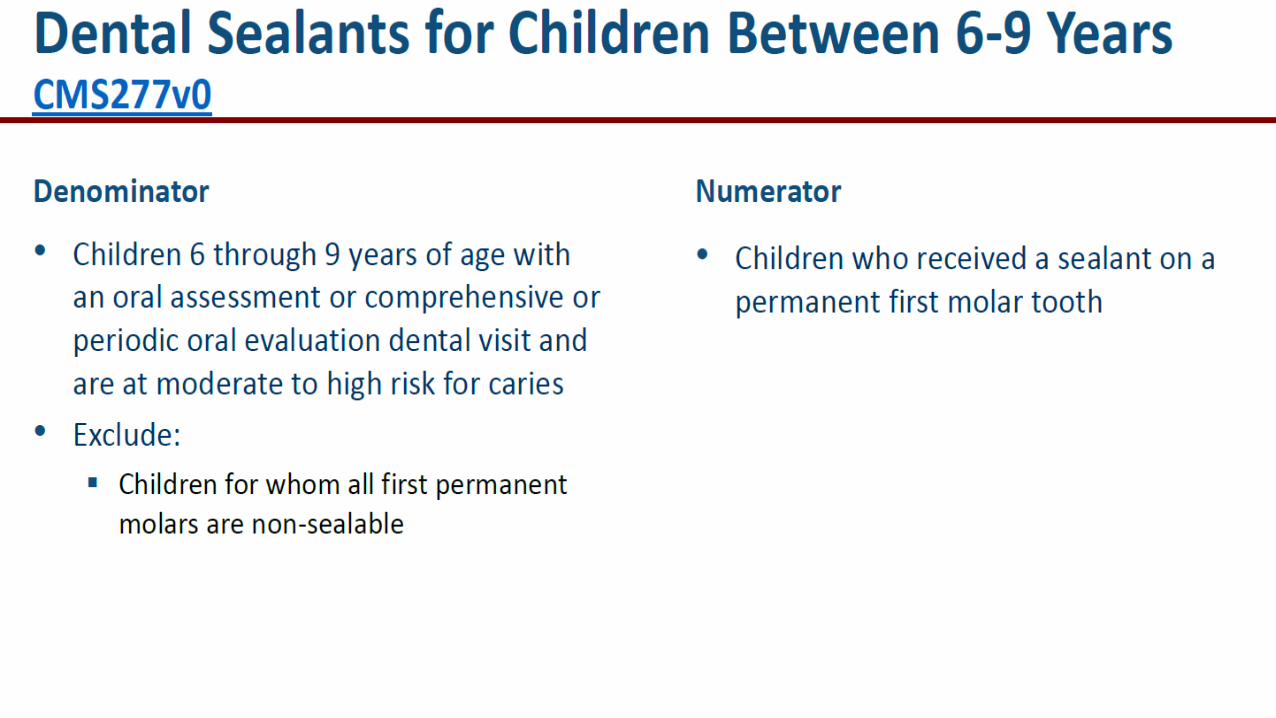
UDS DENTAL SEALANT MEASURE
• Retaining CMS277v0—Dental Sealants for Children Between 6-9 years: Based upon public feedback, HRSA has decided to retain the dental sealant measure for 2020 UDS reporting. HRSA has also decided to not add the fluoride varnish measure for 2020 UDS
• https://www.federalregister.gov/documents/2019/12/13/2019-26876/agency-information-collection-activities-submission-to-omb-for-review-and-approval-public-comment
DENTAL RISK ASSESSMENT TOOLS
• CAMBRA
• https://www.cdafoundation.org/Portals/0/pdfs/cambra_handbook.pdf
• American Academy of Pediatric Dentistry
• https://www.aapd.org/media/Policies_Guidelines/BP_CariesRiskAssessment.pdf
• American Dental Association Caries Risk Assessment
• https://www.ada.org/en/member-center/oral-health-topics/caries-risk-assessment-and-management
• PreViser (electronic risk assessment tool
• https://www.previser.com/
• American Academy of Pediatrics/Bright Futures
• https://www.aap.org/en-us/Documents/oralhealth_RiskAssessmentTool.pdf
• There is inconsistency in the use of risk assessment tools and none are completely validated in the literature
• https://www.ada.org/en/publications/ada-news/2019-archive/january/february-jada-efficacy-of-caries-risk-assessment-tools-compared
• Some are for caries only and some include periodontal assessments
https://www.dentaquestpartnership.org/system/files/DQP%20June%2027%20Webinar_ValueofOralHealth_FINAL.pdf
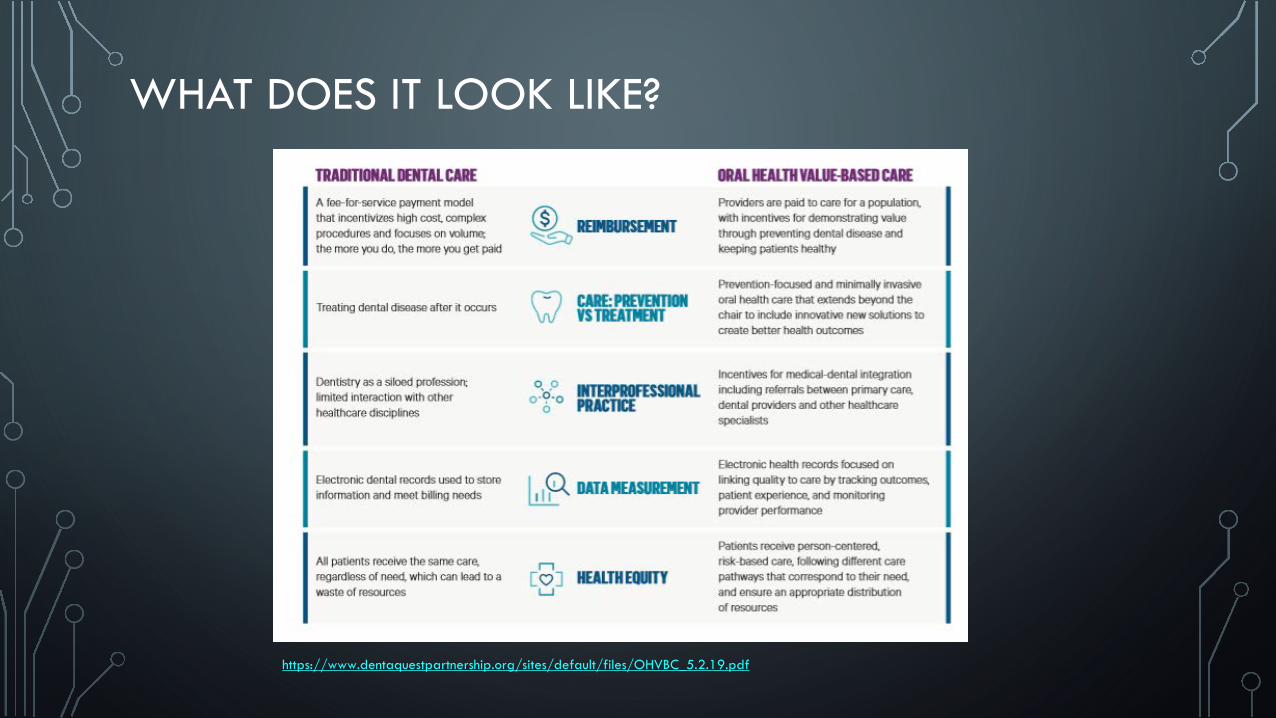
WHAT DOES IT LOOK LIKE?
https://www.dentaquestpartnership.org/sites/default/files/OHVBC_5.2.19.pdf
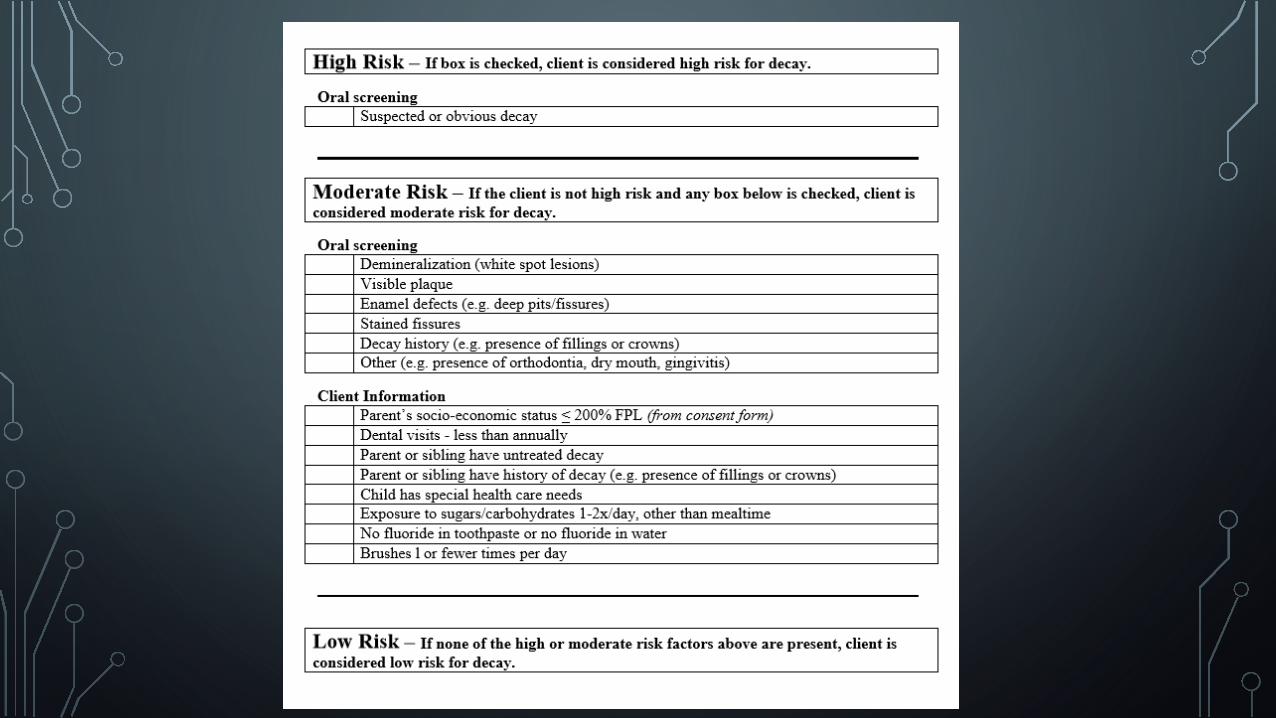
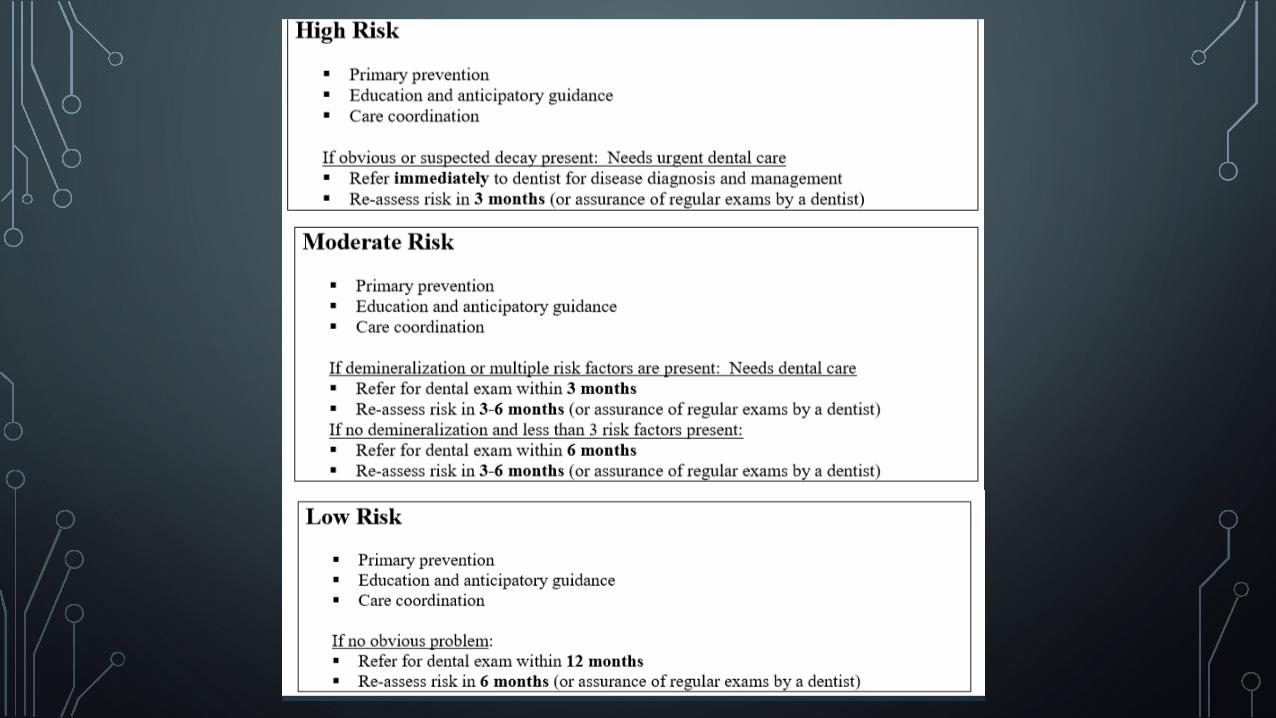
RISK ASSESSMENT USE IN DENTISTRY
• Iowa’s I-Smile Example (Used since 2006)• https://ismile.idph.iowa.gov/Portals/11/Files/Risk%20assessment%20I-Smile.7.1.08.pdf
• Simple: Mostly used in care/referral prioritization
• Based on a dental provider’s visual inspection
• Care Plan linked to the assessment
• Used as a statewide care coordination system linking medical to dental
MORE COMPLEX RISK ASSESSMENTS
• More details
• More protocols
• More risk factors
• More potential benefits
• More provider training and standardization needed
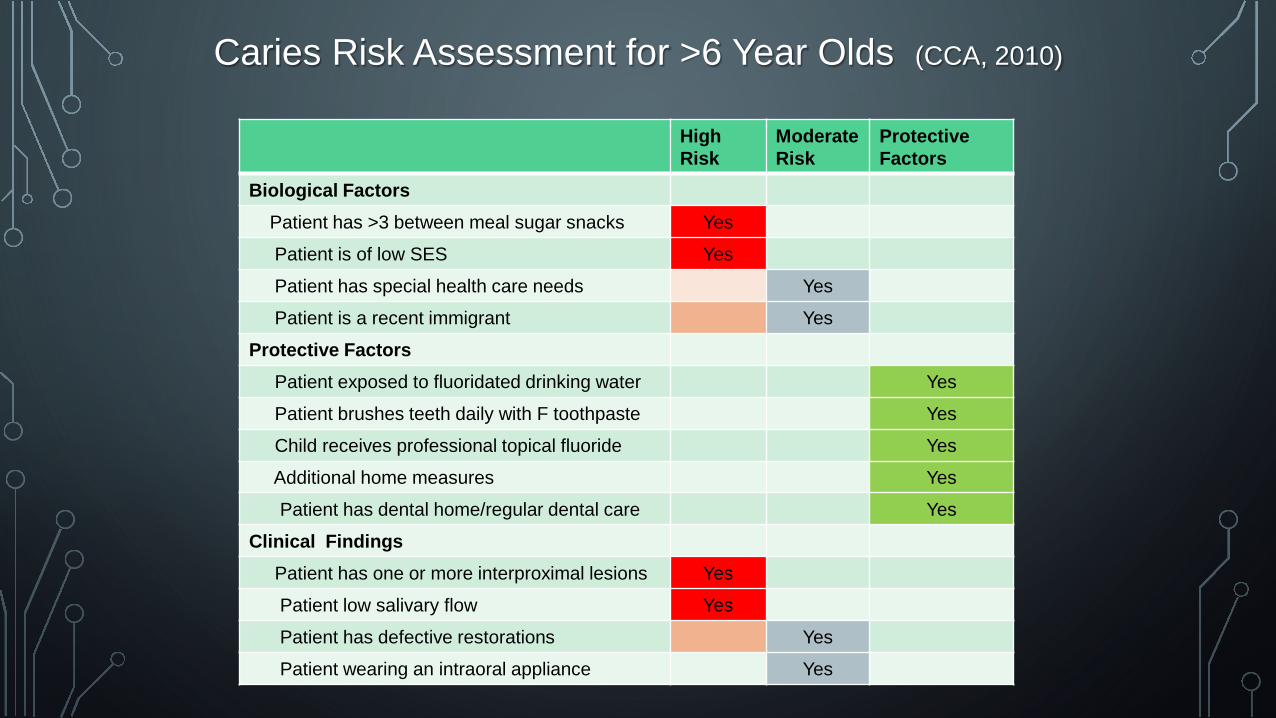
HighRisk
Moderate Risk
Protective Factors
Biological FactorsPatient has >3 between meal sugar snacks Yes
Patient is of low SES Yes
Patient has special health care needs Yes
Patient is a recent immigrant Yes
Protective FactorsPatient exposed to fluoridated drinking water Yes
Patient brushes teeth daily with F toothpaste Yes
Child receives professional topical fluoride Yes
Additional home measures Yes
Patient has dental home/regular dental care Yes
Clinical FindingsPatient has one or more interproximal lesions Yes
Patient low salivary flow Yes
Patient has defective restorations Yes
Patient wearing an intraoral appliance Yes
Caries Risk Assessment for >6 Year Olds (CCA, 2010)
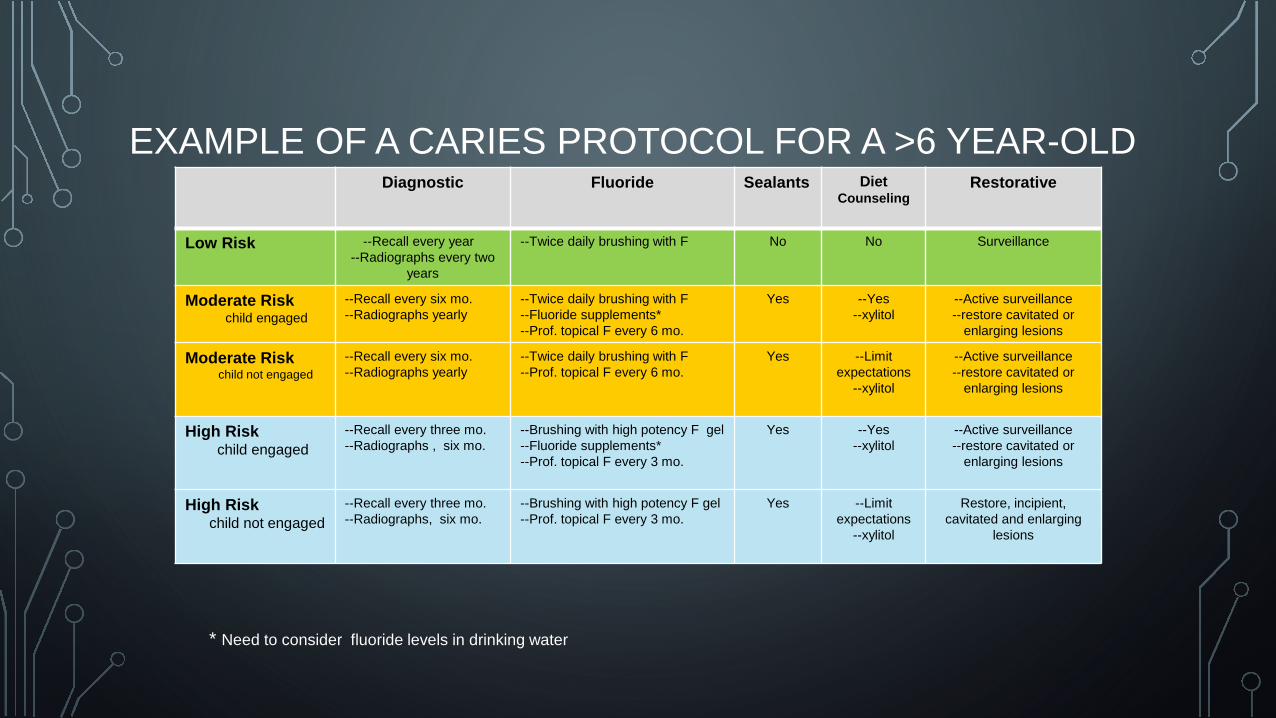
EXAMPLE OF A CARIES PROTOCOL FOR A >6 YEAR-OLDDiagnostic Fluoride Sealants Diet
CounselingRestorative
Low Risk --Recall every year--Radiographs every two
years
--Twice daily brushing with F No No Surveillance
Moderate Riskchild engaged
--Recall every six mo.--Radiographs yearly
--Twice daily brushing with F--Fluoride supplements*--Prof. topical F every 6 mo.
Yes --Yes--xylitol
--Active surveillance --restore cavitated or
enlarging lesions
Moderate Riskchild not engaged
--Recall every six mo.--Radiographs yearly
--Twice daily brushing with F--Prof. topical F every 6 mo.
Yes --Limitexpectations
--xylitol
--Active surveillance --restore cavitated or
enlarging lesions
High Riskchild engaged
--Recall every three mo.--Radiographs , six mo.
--Brushing with high potency F gel--Fluoride supplements*--Prof. topical F every 3 mo.
Yes --Yes--xylitol
--Active surveillance --restore cavitated or
enlarging lesions
High Riskchild not engaged
--Recall every three mo.--Radiographs, six mo.
--Brushing with high potency F gel--Prof. topical F every 3 mo.
Yes --Limit expectations
--xylitol
Restore, incipient, cavitated and enlarging
lesions
* Need to consider fluoride levels in drinking water
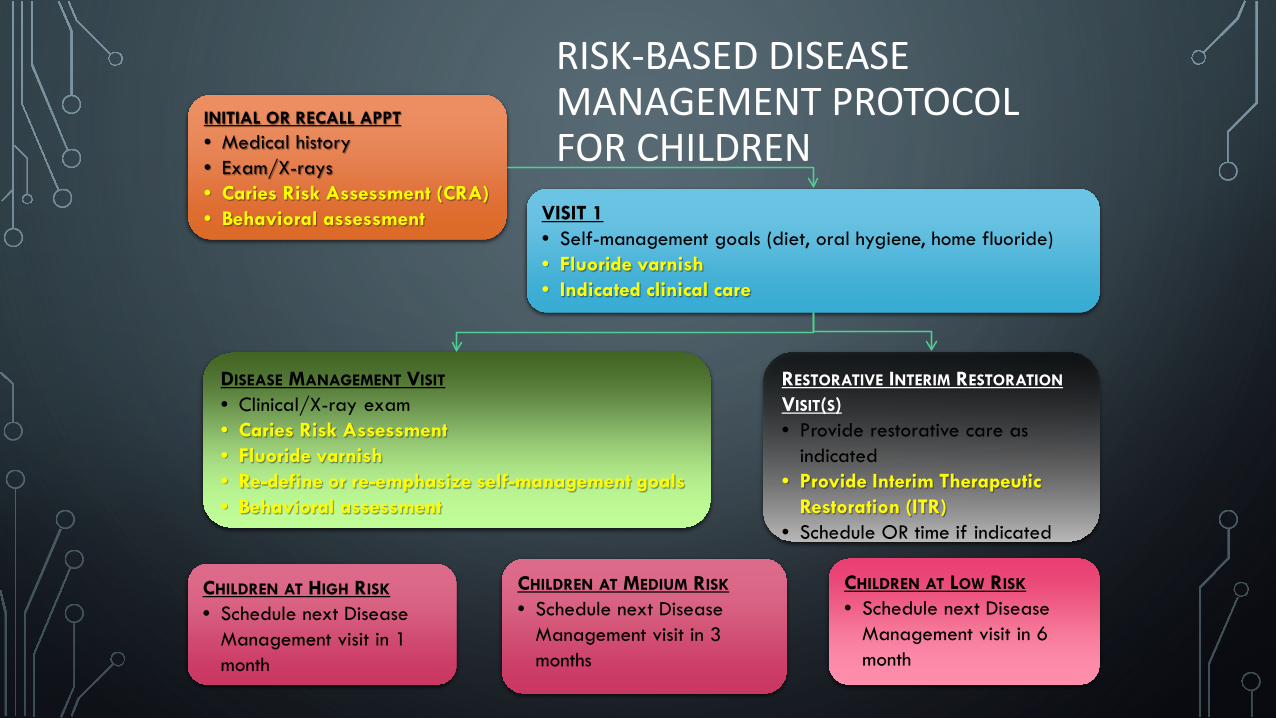
RISK-BASED DISEASE MANAGEMENT PROTOCOL FOR CHILDREN
INITIAL OR RECALL APPT• Medical history• Exam/X-rays• Caries Risk Assessment (CRA)• Behavioral assessment VISIT 1
• Self-management goals (diet, oral hygiene, home fluoride)• Fluoride varnish• Indicated clinical care
DISEASE MANAGEMENT VISIT
• Clinical/X-ray exam• Caries Risk Assessment• Fluoride varnish• Re-define or re-emphasize self-management goals• Behavioral assessment
RESTORATIVE INTERIM RESTORATION
VISIT(S)• Provide restorative care as
indicated• Provide Interim Therapeutic
Restoration (ITR) • Schedule OR time if indicated
CHILDREN AT HIGH RISK
• Schedule next Disease Management visit in 1 month
CHILDREN AT MEDIUM RISK
• Schedule next Disease Management visit in 3 months
CHILDREN AT LOW RISK
• Schedule next Disease Management visit in 6 month
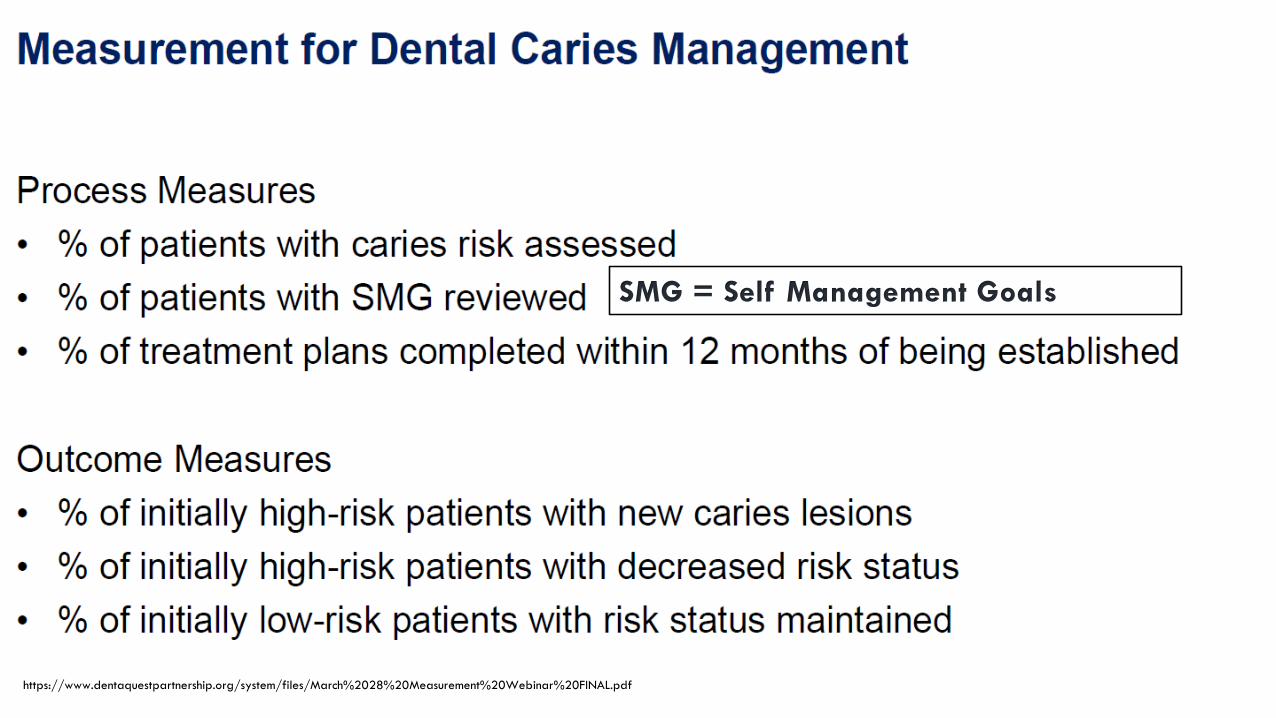
SMG = Self Management Goals
https://www.dentaquestpartnership.org/system/files/March%2028%20Measurement%20Webinar%20FINAL.pdf
TEXAS – A STATE WITH VALUE-BASED PAYMENT MODEL• Requires a caries risk assessment or exam claim not paid
• Includes a downside risk proportion of payment to Medical Management (MCO) and Dental Management Plans (DCO) for underperformance
• No provider downside risk when initiative first launched, but later incorporated
• Each MCO’s targets began for calendar year 2018, beginning at 25% of provider payments in any type of VBP and 10% of provider payments in risk-based VBP
• Dental Managed Care Organizations (DMOs), these targets are set at 25% VBP and 2% risk-based VBP in 2018
https://hhs.texas.gov/sites/default/files/documents/about-hhs/process-improvement/quality-efficiency-improvement/VBP-portal-webinar-040418.pdf
*Slide updated 2/13/2020
TEXAS DENTAL MANAGED CARE MEASURES• DentaQuest
• Measures Used -Medicaid: PreventiveMedicaid: Sealant 6-9Medicaid: Sealant 10-14Medicaid: 90-Day Checkup
• MCNA (Managed Care Network of America)• Evaluation of the number of members assigned to the Dental Home provider who receive
key preventive dental services.
• Fluoride services; 6 month dental visit completion; prophylaxis; sealants on permanent molars; and 1st dental home initiative services (D0145)
• D0145 includes the following diagnostic services:• Counseling with the child's primary caregiver: Instructions for cleaning the child's teeth. ... Once the
child reaches three years of age, periodic oral evaluation (D0120) is typically reported.
METRICS AND MEASURES IN TRANSITION
Moving To A Learning Measurement System (LMS)
“We need a national measurement system that can bridge sectors to advance health, well-being, and equity. The time is right to move away from a fractured, uncoordinated, and complex measurement development system to one that is streamlined, provides more timely and granular information, is accountable to communities, and has clear leadership and accountability to improve outcomes. This will require a substantial shift in who we work with, how we work together, and the establishment of a LMS to support unprecedented learning and collaboration to bring health and well-being to all."
https://www.healthaffairs.org/do/10.1377/hblog20200102.85377/full/?utm_source=Newsletter&utm_medium=email&utm_content=A+Learning+Measurement+System%3B+Medicaid+Financing%3B+Public+And+Private+Hospital+Payment+Rates%3B+Marketplace+Zero-Dollar+Premium+Plans&utm_campaign=HAT+1-8-20
QUESTIONS?


















