
The following program is co-provided by the American Heart ...wcm/... · Name: Bart Cox, MD, FACC...
27
3/20/2013 1 The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/20/2013 ©2010, American Heart Association 1
Transcript of The following program is co-provided by the American Heart ...wcm/... · Name: Bart Cox, MD, FACC...

3/20/2013
1
The following program is co-provided by the American Heart Association
and Health Care Excel, the Medicare Quality Improvement Organization for
Kentucky.
3/20/2013 ©2010, American Heart Association 1

3/20/2013
2

3/20/2013
3
3/20/2013 ©2011, American Heart Association 3
Presenter Disclosure InformationName: Bart Cox, MD, FACC
Title: Associate Professor of Medicine, Division of Cardiology,
Hospital: University of New Mexico School of Medicine, Albuquerque, NM
FINANCIAL DISCLOSURE: None
UNLABELED/UNAPPROVED USES DISCLOSURE: None
3/20/2013
4
3/20/2013 ©2011, American Heart Association 4
Presenter Disclosure InformationName: Diane M. Dodendorf, PhD
Title: Clinical Quality Manager/Anaylist, Internal Medicine
Hospital: University of New Mexico, Albuquerque, NM
FINANCIAL DISCLOSURE: None
UNLABELED/UNAPPROVED USES DISCLOSURE: None
3/20/2013
5
3/20/2013 ©2012, American Heart Association 5
3/20/2013
6
Target: Heart FailureUniversity of New Mexico School of Medicine
Division of Cardiology
Development of HF Performance Measures: Process, Barriers, and Spinoffs
3/20/2013
7
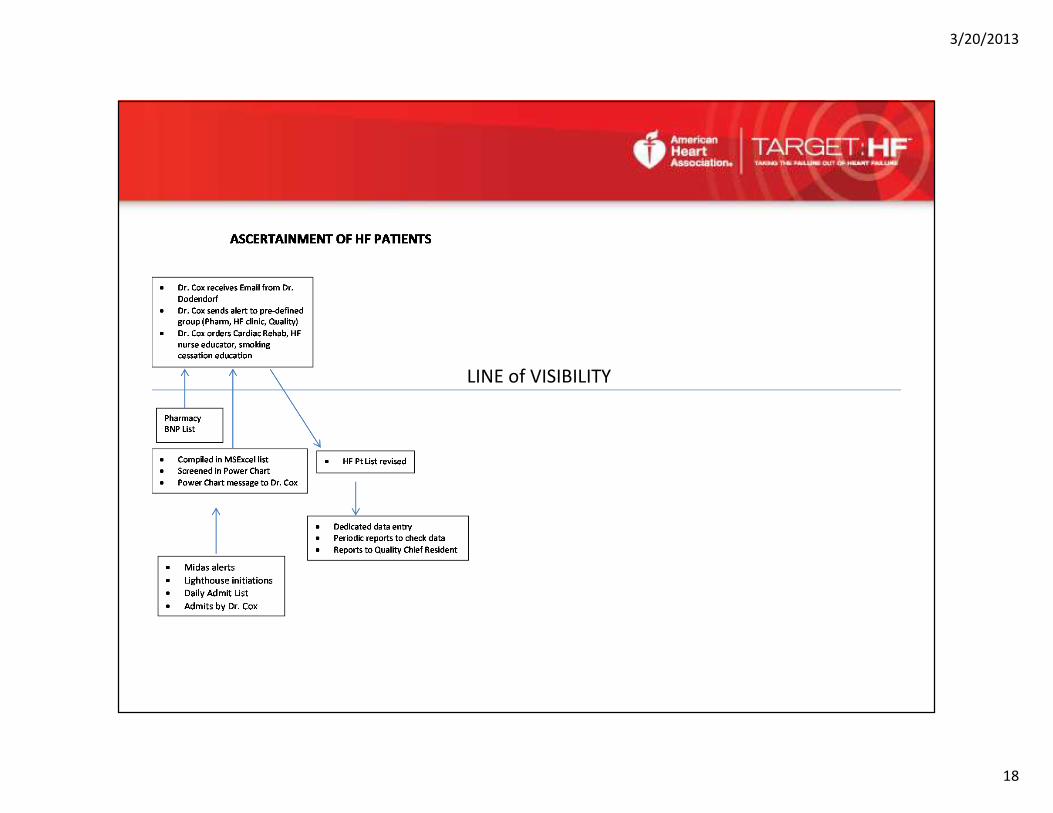
Objectives• Describe the individual components of our process for ascertainment,
clinical care, clinical follow-up (care transitions), data entry, and
monitoring of HF patients in the University of New Mexico Hospital
system.
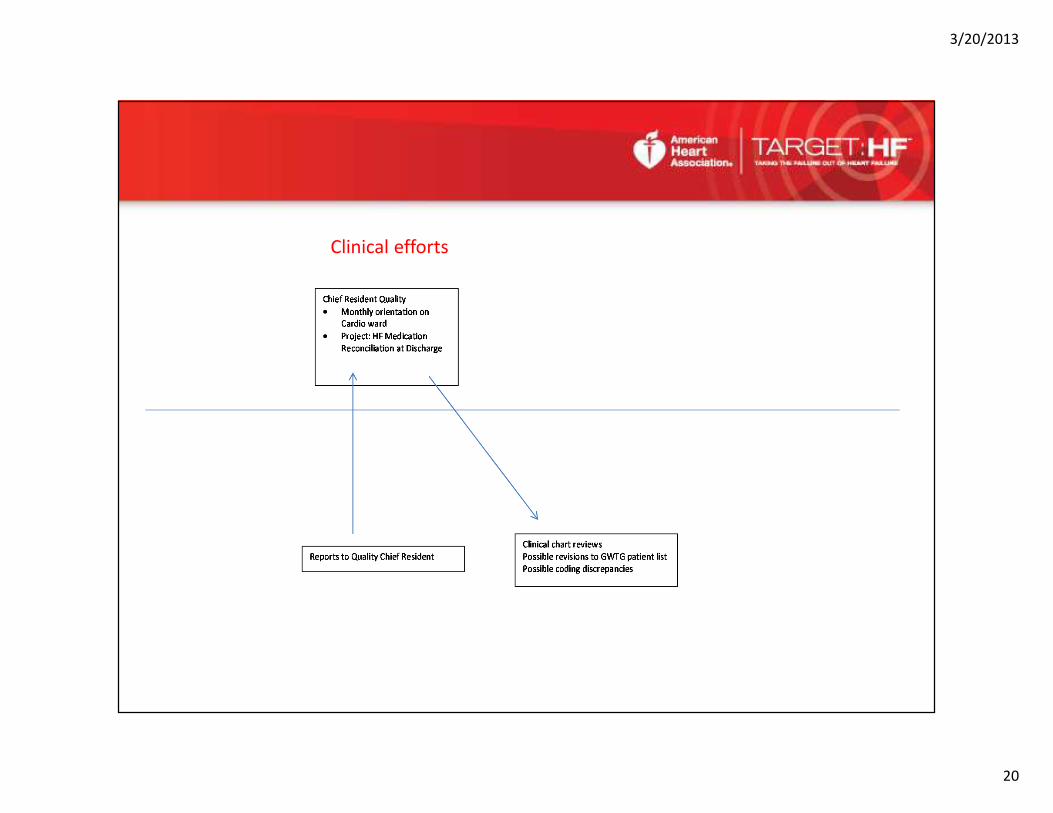
• Demonstrate how these independent “parts” function together –
collaboration and cooperation and communication.
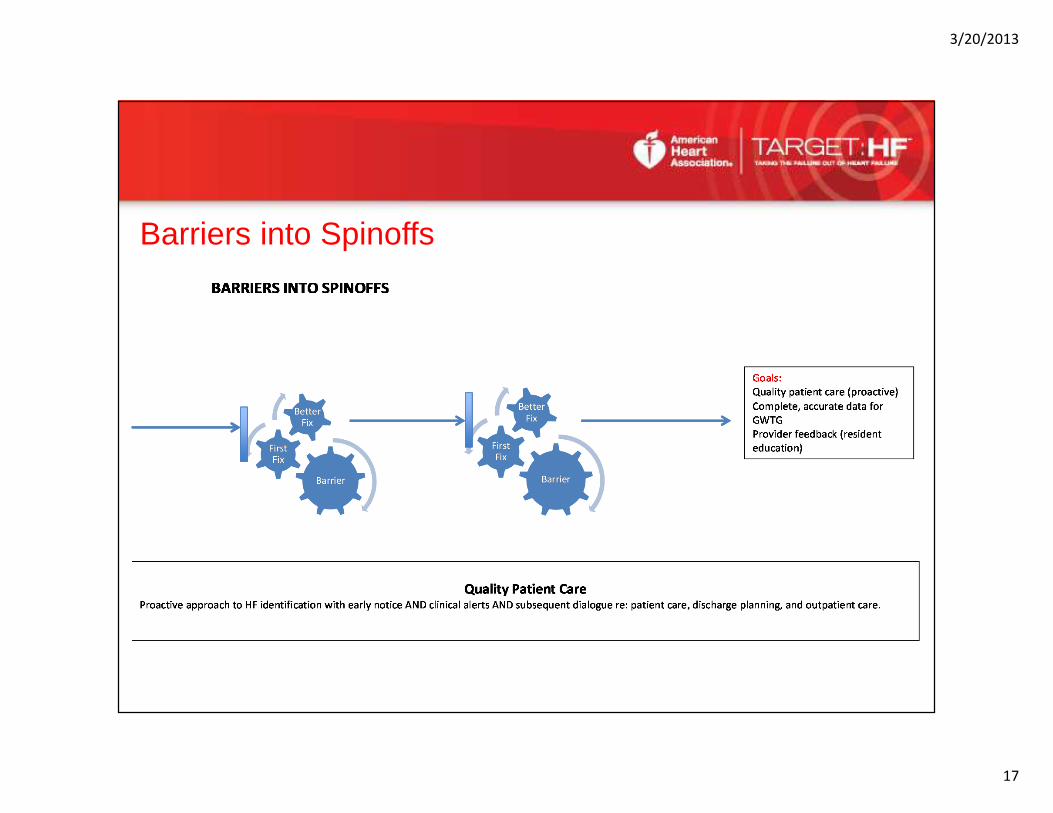
• Identify the early and late barriers and “spin-offs” with this process or
“What will get in your way!”
3/20/2013
8
Target: Heart Failure
• An AHA initiative launched in 2010 whose purpose is to improve quality, care
transitions, and outcomes for patients with heart failure with a targeted initiative and
leveraging the American Heart Association’s premier quality improvement suite of
resources including Get With The Guidelines-Heart Failure.
• Provide healthcare professionals with content-rich resources and materials designed to
help them advance heart failure awareness, prevention, treatment and recovery.
• Participants must demonstrate > 50% compliance on the following measures:
• Medication optimization
• Early follow-up and care coordination
• Enhanced patient education
3/20/2013
9
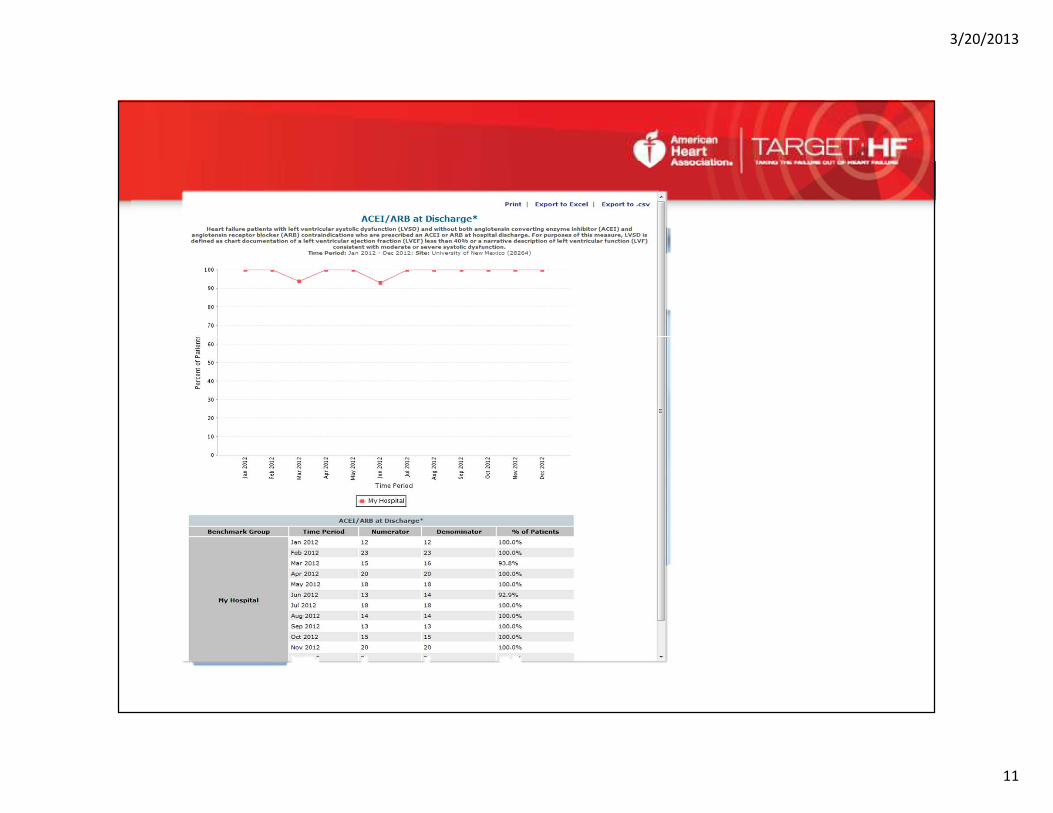
Target: Heart Failure• ACEI/ARB at discharge
• Evidence-based beta-blocker at discharge
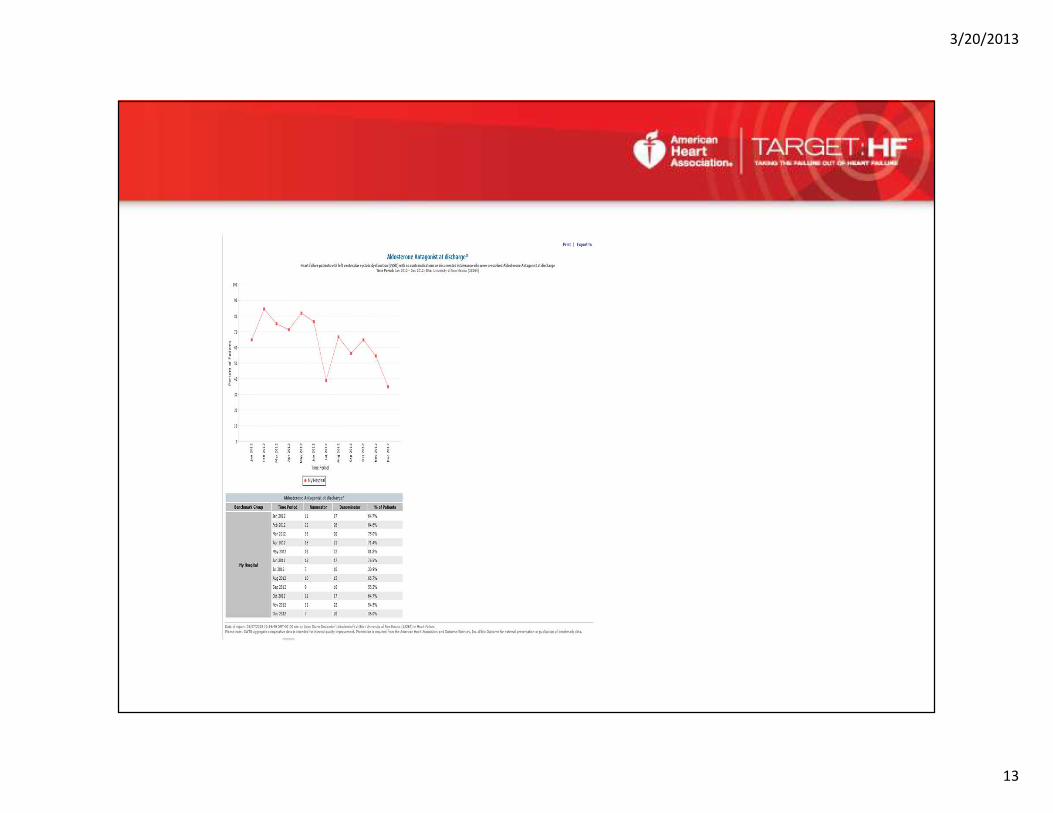
• Aldosterone Antagonist at discharge
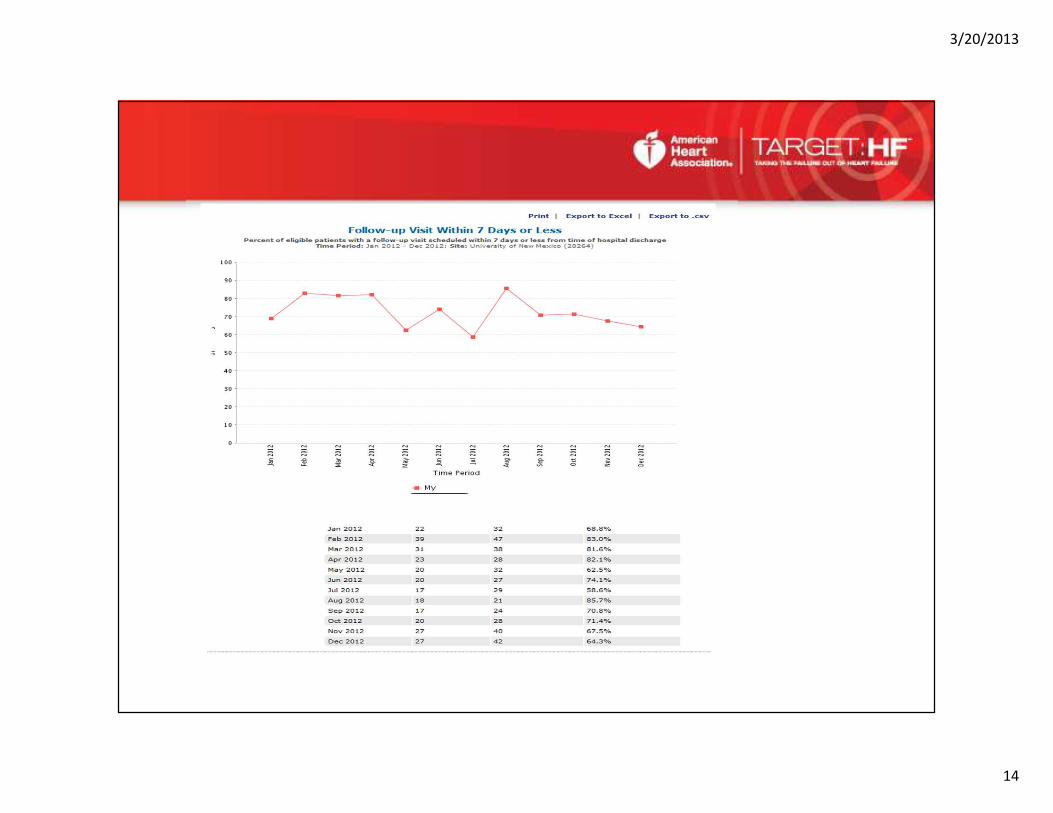
• Follow-up visit within 7 days
• Referral to disease management program
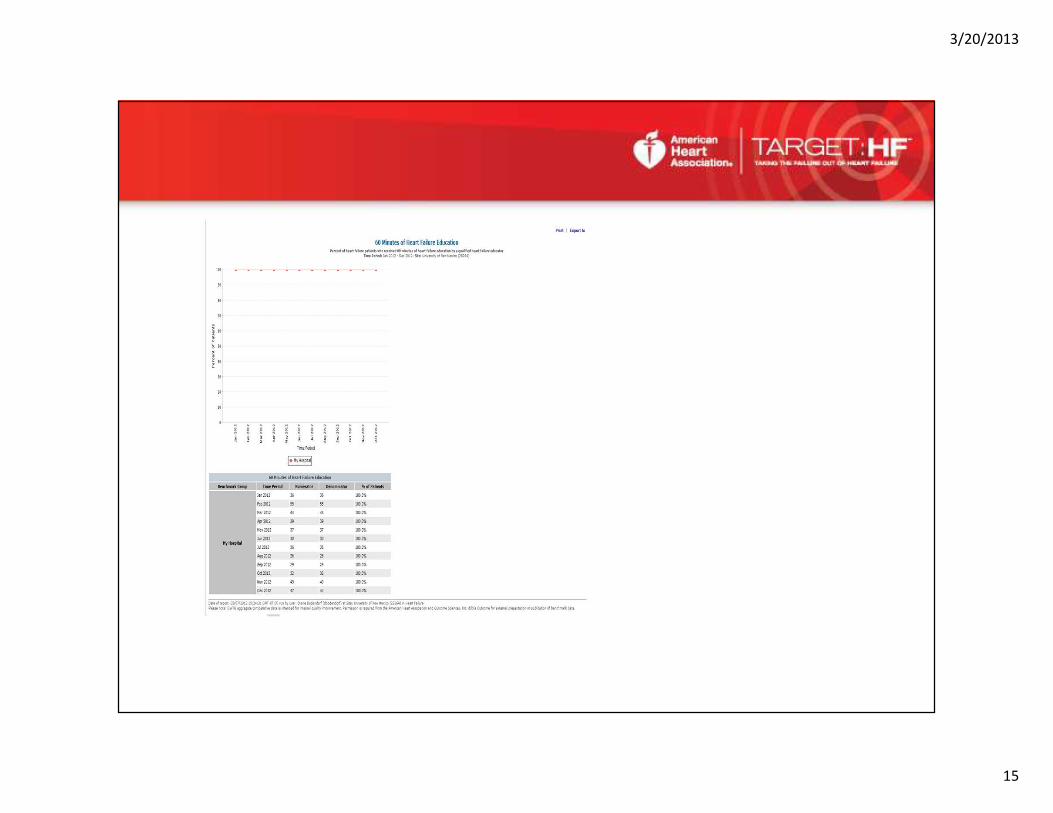
• Patient education (at least 60 min)
• Interactive workbook
3/20/2013
10
GWTG Target: HFUniversity of New Mexico Hospital
Performance
3/20/2013
11

3/20/2013
12
3/20/2013
13
3/20/2013
14
3/20/2013
15
3/20/2013
16
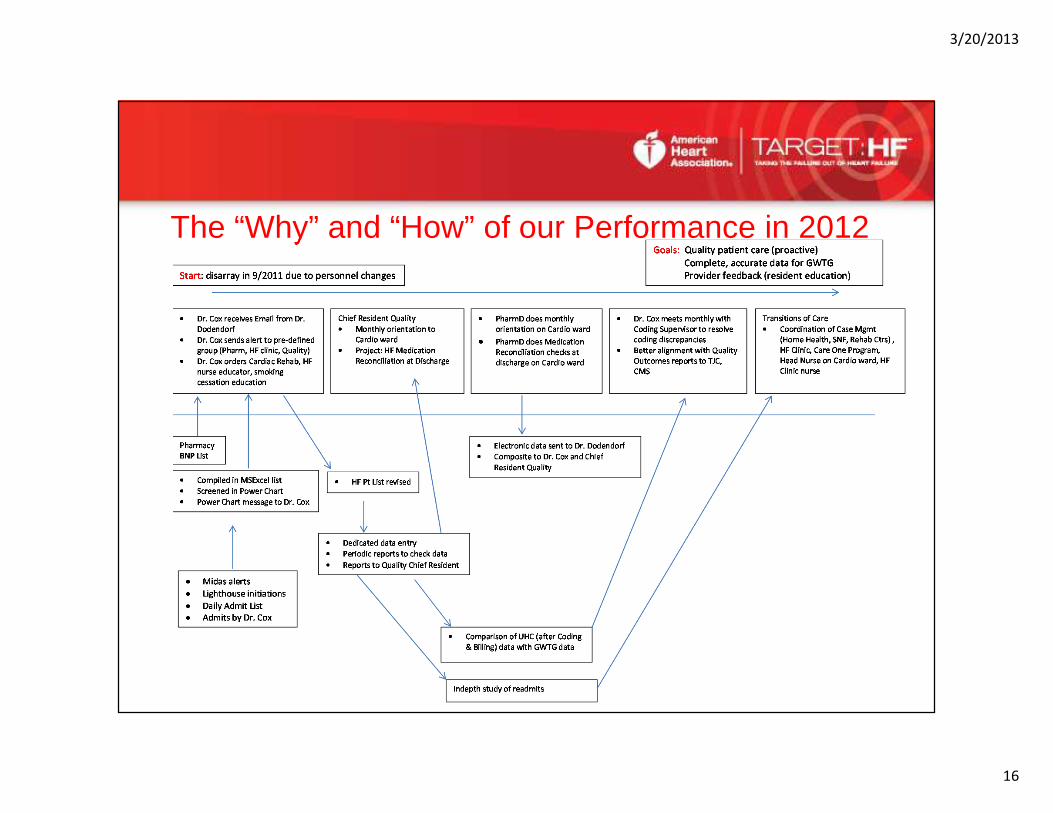
The “Why” and “How” of our Performance in 2012
3/20/2013
17
Barriers into Spinoffs
3/20/2013
18
LINE of VISIBILITY
3/20/2013
19
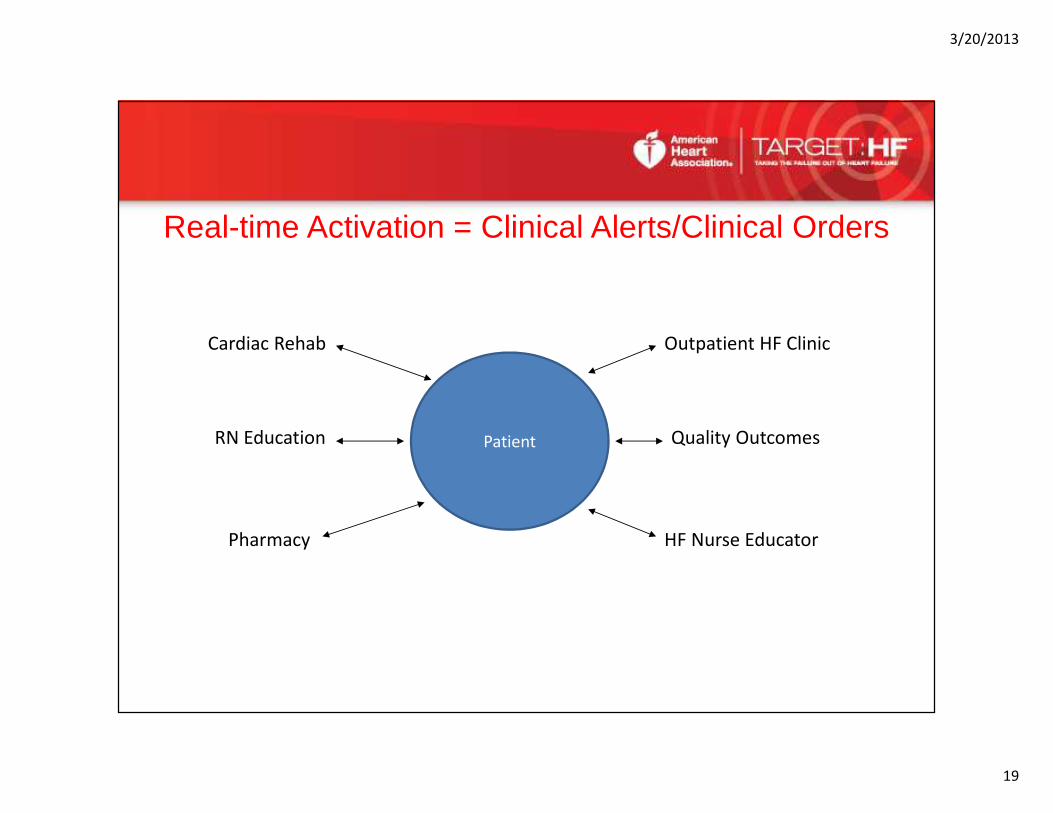
Real-time Activation = Clinical Alerts/Clinical Orders
Patient
Pharmacy
Cardiac Rehab
RN Education
HF Nurse Educator
Outpatient HF Clinic
Quality Outcomes
3/20/2013
20
Clinical efforts
3/20/2013
21
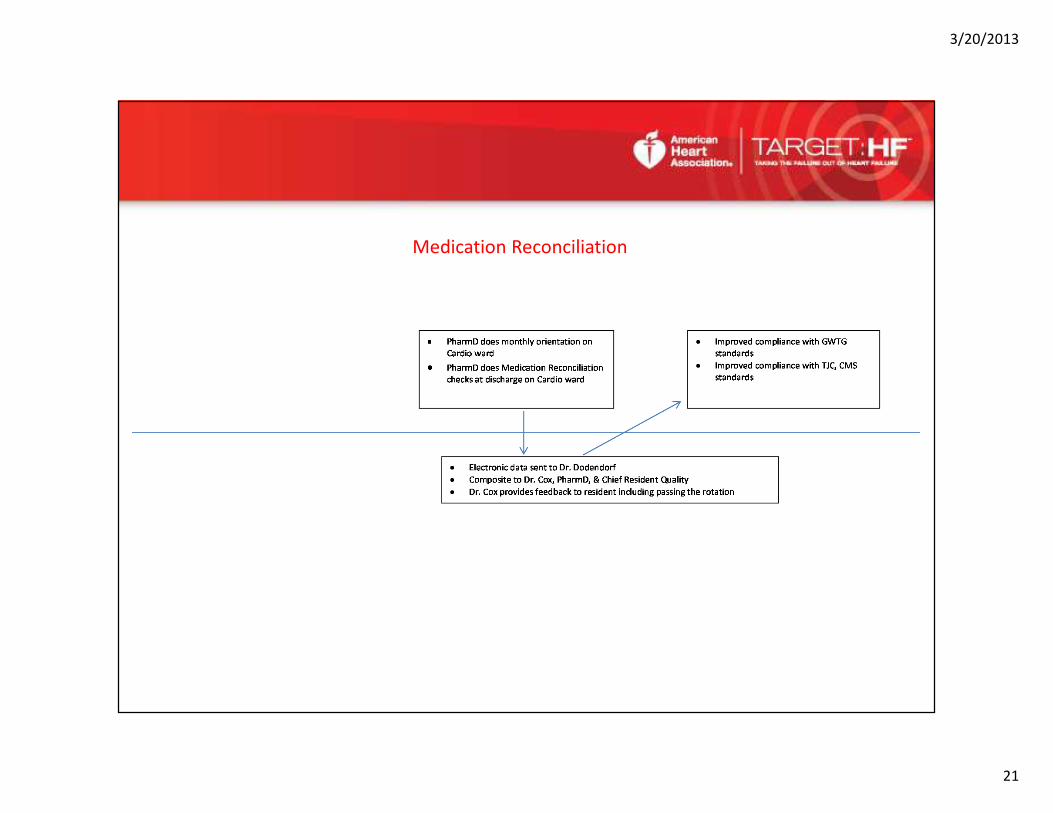
Medication Reconciliation
3/20/2013
22
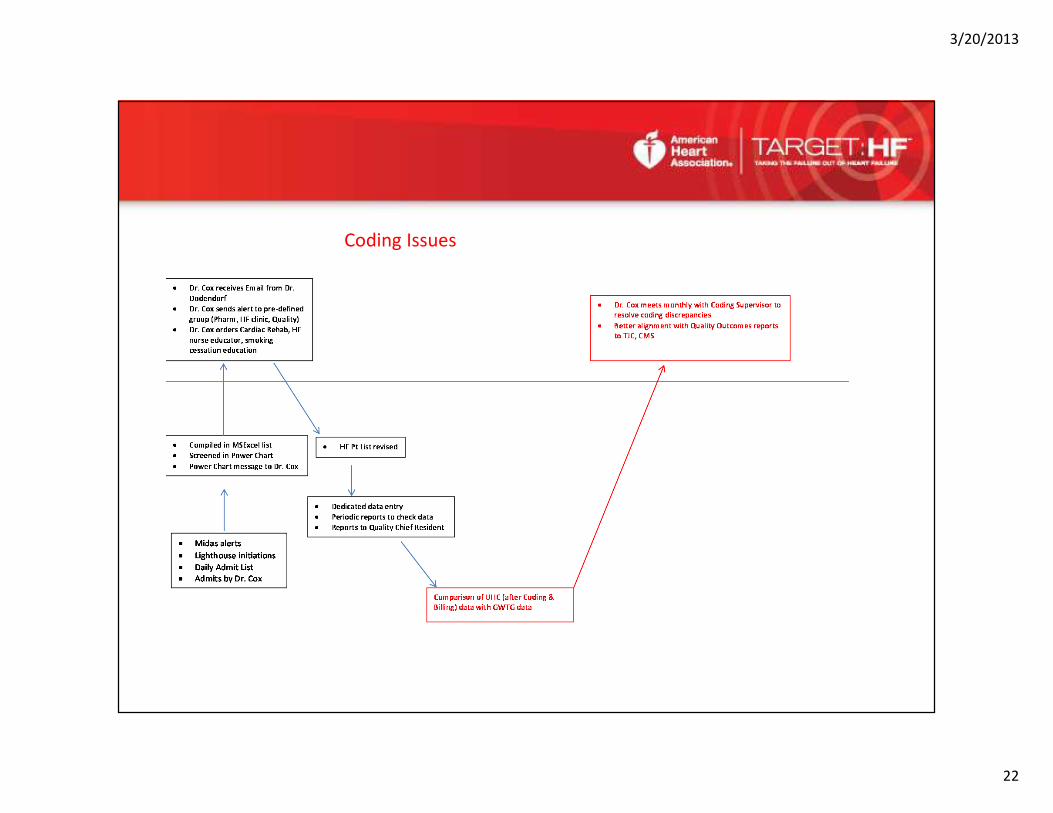
Coding Issues
3/20/2013
23
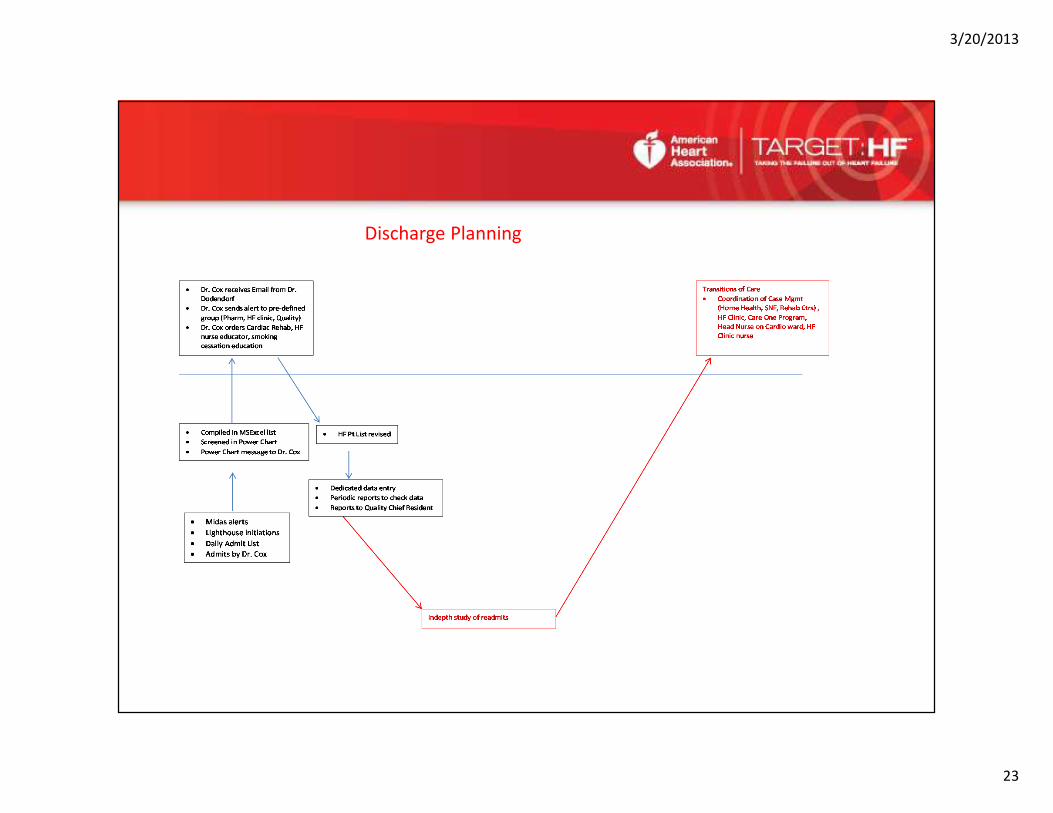
Discharge Planning

3/20/2013
24
Transition in Care• The 7- day follow-up scheduled at discharge
• The 30-day visit data are ensured by use of dictation template (created by NP at HF
Clinic) and the use of dedicated database (clinical outpatient database)
• Medication reconciliation at each step
• Role of out-patient pharmacy services at HF Clinic
• Cardiac Rehabilitation
• Nurse Education at HF Clinic (1/2 day/week)

3/20/2013
25
Repeat Look at Process

3/20/2013
26
This process is like “braiding” 3 railroad tracks• First “railroad track”: Clinical Processes
• Second “railroad track”: Identification and Ascertainment of HF Patients
• Third “railroad track”: Chart Abstraction and Data Entry (EMR and Outcomes software)
• Build in redundancy and backups
• Expect barriers… actually they are a good thing!!
3/20/2013
27
Questions? Comments? Reactions?


















