
Ce 2008 m Lekic Use of Functional Appliances in Interceptive Orthodontics

Editor-in-Chief Prof. Dejan Marković, DDS, PhD, School of Dental Medicine, University of Belgrade, Serbia [email protected]
Guest EditorProf. Anastasios Markopoulos, School of Dentistry, Aristotle University, [email protected]
Associate Editors Prof. Ruzhdie Qafmolla, DDS, PhD, Faculty of Dentistry, University of Medicine-Tirana, [email protected]. Maida Ganibegović, DDS, PhD, Faculty of Dentistry, University of Sarajevo, Bosnia and [email protected] Assoc. Prof. Nikolai Sharkov, DDS, PhD, Faculty of Dental Medicine, Medical University, Sofia, [email protected]. Prof. George Pantelas, DDS, PhD, The School of Medicine, European University Cyprus, [email protected]. Ana Minovska, DDS, PhD, Department of Dentistry, Goce Delcev University of Štip, [email protected] Prof. Anastasios Markopoulos, DDS, PhD, School of Dentistry, Aristotle University, [email protected]. Prof. Mirjana Đuričković, Faculty of Medicine, University of Montenegro, [email protected]. Forna Norina Consuela, DDS, PhD, Faculty of Dentistry, Grigore T. Popa U. M. Ph. Iasi, [email protected]. Slavoljub Živković, DDS, PhD, School of Dental Medicine, University of Belgrade, [email protected]. Ender Kazazoglu, DDS, PhD, Dental School, University of Yeditepe, [email protected]
Editorial BoardAssoc. Prof. Dorjan Hysi, DDS, PhD, Faculty of Dentistry, University of Medicine-Tirana, AlbaniaProf. Virgjini Mulo, DDS, PhD, Faculty of Dentistry, University of Medicine-Tirana, AlbaniaAssoc. Prof. Naida Hadžiabdić, DDS, PhD, Faculty of Dentistry, University of Sarajevo, Bosnia and HerzegovinaDr. Mihael Stanojević, DDS, MSc, Medical Faculty Foca, Bosnia and HerzegovinaProf. Andon Filtchev, DDS, PhD, Faculty of Dental Medicine, Medical University, BulgariaProf. Georgi Todorov, DDS, PhD, Faculty of Dental Medicine, Medical University, BulgariaDr. Huseyn Biçak, DDS, General Hospital Nicosia, CyprusDr. Aikaterine Kostea, DDS, General Hospital Nicosia, Cyprus Assoc. Prof. Ilijana Muratovska, DDS, PhD, Department of Dentistry, Goce Delcev UN of Štip, FYROMAssoc. Prof. Vera R. Nikolovska, DDS, PhD, Department of Dentistry, Goce Delcev UN of Štip, FYROMProf. Lambros Zouloumis, DDS, PhD, School of Dentistry, Aristotle University, GreeceProf. Athanasios Poulopoulos, DDS, PhD, School of Dentistry, Aristotle University, GreeceAssoc. Prof. Zoran Vlahović, DDS, PhD, Faculty of Medicine, University of Priština, MontenegroProf. Andrei Iliescu, DDS, PhD, Faculty of Dentistry, Grigore T. Popa U. M. Ph. Iasi, RomaniaAssoc. Prof. Paula Perlea, DDS, PhD, Faculty of Dentistry, Carol Davila University of Medicine and Pharmacy, RomaniaAssoc. Prof. Tamara Perić, DDS, PhD, School of Dental Medicine, University of Belgrade, SerbiaDr. Slobodan Anđelković, DDS, Private Dental Practice- Belgrade, SerbiaProf. Gül Işik Özkol, DDS, PhD, Istanbul University, TurkeyAssoc. Prof. Zeynep Ozkurt Kayahan, DDS, PhD, Dental School, University of Yeditepe, Turkey
The first issue of the Balkan Journal of Dental Medicine was published in 2014The Journal continues the tradition of the Balkan Journal of Stomatology which was published between 1997 and 2013
Publisher: DE GRUYTER OPEN

II Balk J Dent Med, Vol 21, 2017
International Editorial Board Prof. Nitzan Bichacho, DDS, PhD, The Hebrew University, Hadassah School of Dental Medicine, IsraelDr. Borko Čudović, DDS, Angle Society of Europe, GermanyProf. George Freedman, DDS, PhD, BPP University School of Health, Faculty of Dentistry, United KingdomAssoc. Prof. Alex Grumezescu, PhD, Polytechnic University of Bucharest, RomaniaProf. James Gutmann, DDS, PhD, Texas A&M University Baylor College of Dentistry, USAProf. Christoph Hämmerle, DDS, PhD, Center of Dental Medicine, University of Zurich, GermanyDr. Chris Ivanoff, College of Dentistry, University of Tennessee Health Science Center, USADr. Barrie Kenney, DDS, Private practice- Los Angeles, USADr. Predrag Charles Lekic, DDS, PhD, University of Manitoba, CanadaProf. Joshua Moshonov, DDS, PhD, Hadassah School of Dental Medicine, IsraelJohn Nicholson, PhD, DSc, Bluefield Centre for Biomaterials, United KingdomProf. Kyösti Oikarinen, DDS, PhD, University of Oulu, FinlandAssoc. Prof. Sangwon Park, DDS, PhD, Chonnam National University, South KoreaProf. George Sandor, PhD, University of British Columbia, CanadaProf. Ario Santini, DDS, PhD, Faculty of General Dental Practice, United KingdomProf. Riitta Suuronen, DDS, PhD, Institute for Regenerative Medicine, University of Tampere, FinlandDr. Michael Weinlaender, DDS, Private Practice- Vienna, Austria
Publications CommitteeChairProf. Ljubomir Todorović, DDS, PhD, Academy of Medical Sciences, Serbian Medical Society, [email protected]
Editorial Medical StaffAssoc. Prof. Elizabeta Gjorgievska, DDS, PhD, Faculty of Dentistry, Ss. Cyril and Methodius UN, FYROMProf. Bojan Petrović, DDS, PhD, Faculty of Medicine, University of Novi Sad, SerbiaDr. Marijan Denkovski, DDS, FYROMDr. Georgios Tsiogas, DDS, GreeceDr. Ana Jotić, DDS, Private Dental Practice, Belgrade, SerbiaDr. Raša Mladenović, DDS, Faculty of Medicine, University of Priština, Serbia
Translations supervisorGordana Todorović
Technical EditingDr. Milica Cindrić, DDS
Publishing ManagersJelena Jaćimović, PhD, School of Dental Medicine, University of Belgrade, [email protected]. Asst. Bojana Ćetenović, DDS, PhD, Institute for Nuclear Sciences „Vinca“[email protected]. Ana Vuković, DDS, PhD, School of Dental Medicine, University of Belgrade, [email protected]
Statistical AdvisorProf. Biljana Miličić, MD, PhD, School of Dental Medicine, University of Belgrade, Serbia [email protected]
Editorial Office: School of Dental Medicine, Clinic for Paediatric and Preventive Dentistry, Dr. Subotića 11, 11000 Belgrade, Serbia
e-mail: [email protected], Tel: +381641149773, Fax: +381112685361
Papers published in the Balkan Journal of Dental Medicine are indexed in: Baidu Scholar, Case, Celdes, CNKI Scholar (China National Knowledge Infrastructure), CNPIEC, EBSCO Discovery Service, Google Scholar, J-Gate, JournalTOCs, KESLI-NDSL (Korean National Discovery for Science Leaders), Naviga (Softweco), Primo Central (ExLibris), ReadCube, Sherpa/RoMEO, Summon (Serials Solutions/ProQuest), TDOne (TDNet), WorldCat (OCLC).

BALKAN JOURNAL OF DENTAL MEDICINE ISSN 2335-0245
RA A.Grbović PracticalAspectsofFiniteElementMethodApplicationsinDentistry 69 D.MihajlovićRA Z.Vulićević ProstheticsinPaediatricDentistry 78 M.Beloica D.Kosanović I.Radović J.Juloski D.IvanovićRA E.M.Kalogirou IsDentalImplantationIndicatedinPatientswith 83 A.Sklavounou OralMucosalDiseasesOP M.Lalić OralHealthRelatedQualityofLifeand 93 I.Melih DentalStatusofAdultPatients E.Aleksić M.Gajić K.Kalevski A.ĆukovićOP A.Altındağ IncidentalFindingsinCone-BeamComputedTomographicImages: 100 H.Avsever CalcificationsinHeadandNeckRegion O.Borahan M.Akyol K.OrhanOP D.Trišić DiodeLaserIrradiationinEndodonticTherapythroughCycles 108 B.Ćetenović -in vitroStudy I.Jovanović E.Gjorgievska B.Popović D.MarkovićOP S.E.Gültekin MolecularProfilingofOdontogenicTumors-PilotStudy 112 B.Sengüven R. Aziz C.Heydt R.BuettnerCR P.Karakostas OralGranularCellTumor:ReportofCaseSeriesanda 116 A.Matiakis BriefReviewoftheLiterature E.Anagnostou A.KolokotronisCR A.Poulopoulos IntraoralMyeloidSarcomawithBilateralInvolvement-CaseReport 119 F.Iordanidis D.Andreadis K.AntoniadisCR D.T.Budanur OrofacialCrohn’sdisease:aCaseReport 123 M.Şirin E.Sepet M.Ünür M.Güllüoğlu M.S.Cantez Ö.D.Uğurcan
Contents
VOLUME 21 NUMBER 2 JULY 2017 PAGES 70-127
STOMATOLOGICA
L SO
CIE
TY

BALKAN JOURNAL OF DENTAL MEDICINE ISSN 2335-0245 STOMATOLOGIC
AL
SO
CIE
TY
Welcome Message
It is a great honor for me to edit this special issue of Balkan Journal of Dental Medicine for the selected revised papers presented in the 22nd BaSS Congress held on May 4-6, 2017, at the Makedonia Palace Hotel, in Thessaloniki, Greece.
As a guest editor of this issue, I was glad to see a variety of articles focusing on various fields of Dentistry, such as Endodontology, Implantology, Laser applications, Hospital dentistry, Oral Medicine/Oral Pathology, Orthodontics, Pediatric Dentistry, Periodontology, Preventive dentistry, Prosthodontics, Restorative Dentistry, Oral Radiology Oral & Maxillofacial Surgery and Biomaterials.
Scholars from many Balkan countries contributed to this issue of the Journal. All the submitted papers have been reviewed by reviewers specialized in the related field. In this issue we present you the selected papers after the end of the review process.
I would like to express my special thanks to all the reviewers, the Editor-In-Chief,and those involved in technical processes.
I hope that you will enjoy reading the papers.
Sincerely,
President of the Scientific Committee of 22nd BaSS Congress, Thessaloniki 2017
Anastasios Markopoulos, DMD, MS, PhD

SUMMARYThe use of numerical methods, such as finite element method (FEM),
has been widely adopted in solving structural problems with complex geometry under external loads when analytical solutions are unachievable. Basic idea behind FEM is to divide the complex body geometry into smaller and simpler domains, called finite elements, and then to formulate solution for each element instead of seeking a solution for the entire domain. After finding the solutions for all elements they can be combined to obtain a solution for the whole domain. This numerical method is mostly used in engineering, but it is also useful for studying the biomechanical properties of materials used in medicine and the influence of mechanical forces on the biological systems. Since its introduction in dentistry four decades ago, FEM became powerful tool for the predictions of stress and strain distribution on teeth, dentures, implants and surrounding bone. FEM can indicate aspects of biomaterials and human tissues that can hardly be measured in vivo and can predict the stress distribution in the contact areas which are not accessible, such as areas between the implant and cortical bone, denture and gingiva, or around the apex of the implant in trabecular bone. Aim of this paper is to present – using results of several successful FEM studies – the usefulness of this method in solving dentistry problems, as well as discussing practical aspects of FEM applications in dentistry. Some of the method limitations, such as impossibility of complete replication of clinical conditions and need for simplified assumptions regarding loads and materials modeling, are also presented. However, the emphasis is on FE modelling of teeth, bone, dentures and implants and their modifications according to the requirements. All presented studies have been carried out in commercial software for FE analysis ANSYS Workbench.Key words: Finite Element Method, Biomechanical Systems, Computer Simulations, Stress Analysis
Aleksandar Grbović, Dimitrije Mihajlović
Faculty of Mechanical Engineering, University of Belgrade, Serbia
REVIEW PAPER (RP) Balk J Dent Med, 2017;69-77
BALKAN JOURNAL OF DENTAL MEDICINE ISSN 2335-0245
Practical Aspects of Finite Element Method Applications in Dentistry
STOMATOLOGICA
L S
OC
IET
Y
Introduction
Finite element method (FEM) is one of the most widely used numerical methods for solving the problems of mechanics of continuum. FEM is method of discrete analysis and – unlike other numerical methods which are based on mathematical discretizationa of equations of boundary problems – it is based on physical discretization
a Discretization is the process of transferring continuous functions, models, and equations into discrete counterparts. This process is usually carried out as a first step toward making them suitable for numerical evaluation and implementation on digital computers.
of considered domain. Basis for all calculations is represented by the part of the domain (so called sub-domain) which has finite dimensions, also known as finite element. From the perspective of physical interpretation this means that the observed real physical domain with infinite number of degrees of freedomb (DOF) can
b In engineering, the degree of freedom (DOF) of a mechanical system is the number of independent parameters that define its configuration. It’s the number of parameters that determine the state of a physical system. For example, the position and orientation of a rigid body in space is defined by three components of translation and three components of rotation, which means that it has six degrees of freedom.
10.1515/bjdm-2017-0011

70 Aleksandar Grbović, Dimitrije Mihajlović Balk J Dent Med, Vol 21, 2017
The power of the FME resides primarily in its adaptability: analyzed structure might have arbitrary shape, materials, loads and supports. Also, the mesh may consist of elements of diverse types, shapes and physical properties. This great adaptability is usually achieved within a single computer program and the definition of all necessary input variables is controlled by user.
Finite element analysis (FEA) can provide detailed quantitative data at any location within mathematical model; therefore, FEA has become a valuable analytical tool in dentistry. FEM can indicate aspects of biomaterials and human tissues that can hardly be measured in vivo and can predict the stress and straine distribution in the contact areas which are not accessible, such as areas between the implant and cortical bone, denture and gingiva, or around the apex of the implant in trabecular bone. In general, research fields in which FEM is implemented can be classified as follows1:
- Investigation of improved shape and design of fillings, crowns, dental implants, removable dentures, dental bridges, etc.;
- Examination of mutual interaction of stomatognathic system supporting structures;
- Study of residual stresses which occur as consequence of mechanical and thermal extension in crowns and dental fillings;
- Research of physiological and biochemical effects of chewing forces, teeth reactions to occlusal forces, their interaction and stress concentration;
- Research and application in orthodontics; - Research and application in implantology.
In practice, applications of FEM in dentistry implies creation of virtual computer model with properly defined geometry and material properties, precisely defined loads and boundary conditions. These four parameters essentially define numerical model and the accuracy of the results is directly linked to them.
Geometry of the model must be close to the actual structure and unreasonable simplifications will unavoidably result in significant inaccuracy: experience and good judgment are needed to define adequate geometry. To decrease time to numerical solutions, researchers are often performing a two-dimensional (2D) instead of three-dimensional (3D) analyses because a 2D model is as efficient and accurate as a 3D model if it’s well defined (Figure 2).
required to interpolate (i.e. estimate) a value within two known values in a sequence of values. Polynomial interpolation is a widely-used method of estimating values between known data points.e In continuum mechanics stress is a physical quantity that expresses the internal forces that neighboring particles of a continuous material exert on each other, while strain is the measure of the deformation of the mate-rial. The dimension of stress is that of pressure, and therefore is com-monly measured in the same units as pressure (pascals), while strain is unitless quantity.
be replaced with discretized geometrical model with finite number of DOF. Such model consists of elements interconnected by finite number of points known as nodes (Figure 1). These finite elements have defined dimensions, physical properties and simple geometry, and together they can “simulate” the behavior of complex physical system. As a part of the process of discretization, choice of shape of finite element and number of elements used in numerical simulation is influenced by the nature of the analyzed problem and the required accuracy of solution.
Figure 1. Approximation of the real object using FEM
By analyzing the individual elements along with the characteristics of their mutual connections, the whole complex system can be analyzed. The approach where universal solution is obtained from the individual solutions is known as inductive method. This method is of the greatest importance for solving the problems where exact solutions cannot be achieved directly1.
Figure 1 shows the sketch of the real object and equivalent mathematical model after one possible discretization. Set of subdomains for the entire domain is called finite element mesh. Each node in mesh has finite number of degrees of freedom. Forces cannot act on the surface of the finite element or edge but only in nodes. After carried out calculations, each node will be assigned displacement values that represent the reaction of the entire system to given loads and boundary conditionsc. Values of displacements on the finite elements between the nodes are determined by means of mathematical interpolationd.
c The set of conditions specified for the behavior of the solution to a set of differential equations at the boundary of its domain. Boundary conditions are important in determining the mathematical solutions to physical problems.d In engineering, interpolation is a method of constructing new data points within the range of a discrete set of known data points. It is often

Balk J Dent Med, Vol 21, 2017 Finite Element Method Applications in Dentistry 71
In most reported investigations in dentistry materials were modelled as homogenous and linearly isotropic for two main reasons: 1) It is not easy to accurately determine orthotropic, anisotropic or hyperelastic properties of material, and 2) If material is isotropic analysis is linear, otherwise it is non-linear and convergencef problem may arise. There are several methods to determine the physical properties of bone or tooth, such as tensile, compressive, bending and torsion testing, pure shear tests, micro- and nano- indentation tests, acoustic tests, etc. For example, the values from 13.7 to 20.7 GPa and 1.37 to 14.8 GPa have been frequently used for the Young’s modulus of cortical and cancellous bone, respectively, and Poisson’s ratio was assumed to be 0.3 for both2. But, bone is an anisotropic material with properties being directionally dependent. To incorporate realistic material for bone tissues in maxilla or mandible, the FEM may employ full orthotropy for cortical bone as the elastic behavior in cortical bone approximates to an orthotropic material and transversely isotropic for cancellous bone.
Selecting appropriate loading conditions is also of immense importance for productive FEA. In general, loads used in FE simulation can be divided into axial forces and horizontal forces (or moment-causing loads). Combinations of these forces (termed as mixed loading) define oblique occlusal loads which are more realistic and usually generate considerable localized stresses in compact bone. An axial force acts down the long axis of the tooth or implant and hence produces compression (which is favorable), whereas horizontal loading transmits tensile stresses and induces a bending (which is considered undesirable). For example, when a crown is to be fabricated for an implant, its shape must be without any cantilevers (which can contribute to torsional or bending movement) and should distribute biomechanical forces in a such way to produce favorable compressive stresses.
Extensive studies of masticatory (bite) force revealed significant variations in magnitude which were related to the area of the mouth, muscle size, bone shape, sex, age and many other factors. In the premolar region, values of masticatory force range from 40 to 600 N, forces from 50 to 400 N have been recorded in the molar region for young adults while forces from 25 to 170 N have been measured in the incisal region3,4,5. Clinical studies revealed that the average masticatory force transmitted to implant range between 90 N and 280 N, depending on the location, diameter, length of the implant and the kind of abutment used6,7. The choice of point of loading is also very important for successful FE analysis. Loading
f Convergence is a major issue with the use of FEM software. When FE problem is non-linear, solution techniques are based on iterative process to successively improve a solution, until ‘convergence’ is reached. The exact solution to the iterative problem is unknown, but numerical result must be sufficiently close to the solution for required level of accuracy. This requirement depends upon the purpose to which the solution will be applied.
However, 2D models cannot simulate the 3D complexity of the structures and hence results might be of minor clinical values. Time needed to create FE models and obtain results is decreasing with advances in computer technology; thus, three-dimensional FE models are becoming dominant. With the development of digital imaging techniques more efficient methods are available for the direct transformation of 3D information from computed tomography (CT) or magnetic resonance imaging (MRI) into FE mesh. Solid models of a mandibula, crowns, teeth or dental implants may be obtained directly from 3D scanners or constructed using the computer-aided design (CAD) software such as CATIA or SolidWorks.
Figure 2. Two-dimensional model (left) vs. three-dimensional model (right)
Material properties considerably influence the stress and strain distribution in a structure. These properties can be modeled as isotropic, orthotropic, anisotropic, hyperelastic, viscoelastic, plastic (plasticity), etc. When the properties are the same in all directions material is linearly isotropic and only two independent material constants (Young’s modulus E and Poisson’s ratio ν) must be defined. In contrast to isotropic, orthotropic materials have properties that differ along three mutually-orthogonal axes of rotational symmetry. This results in unique elastic behavior along the three orthogonal axes of the material, thus three elastic (E) and shear modulus (G) and six Poisson’s ratios (ν) must be known for model input. Orthotropic materials are a subset of anisotropic materials which are directionally dependent, which implies different properties in different directions. Anisotropy can be defined as a difference, when measured along different axes, in a material’s physical or mechanical properties such as absorbance, refractive index, tensile strength, etc. Hyperelastic material model is used to describe the non-linear stress-strain behavior of complex materials such as rubbers, polymers, biological tissue, etc. Plasticity describes the deformation of a (solid) material undergoing non-reversible changes of shape in response to applied forces.

72 Aleksandar Grbović, Dimitrije Mihajlović Balk J Dent Med, Vol 21, 2017
should be modeled to reduce the analysis run time and RAM memory required. The lines or planes of symmetry in a FE model can be simulated by providing proper BCs to the symmetrical faces or edges of the geometry, while loads must be completely symmetric, too. The general rule for a symmetry displacement condition is that the displacement vector component perpendicular to the symmetry plane is zero and the rotational vector components parallel to the plane are zero. Figure 3 shows two-dimensional FE model of one half of dental assembly with symmetric BC (named Frictionless Support) and displacement of 1 mm used as a load. Frictionless support is applied along the axis of symmetry (position C in Figure 3), while Fixed Support is applied along edge A (which is the part of the assembly with restricted displacement in all directions). Finally, vertical upward displacement (represented by arrow) of 1 mm is applied along edges denoted by B and D. As it can be seen, no forces were used in this FE simulation.
To conclude, with rapid improvements of digital technologies and user friendly software interfaces, the FEM has become available not only to aerospace and civil engineers but to doctors and dentists who can use this powerful technique to analyze complex biomechanical structures. The modeling and simulation save time and money for conducting the live experiment or clinical trials. By understanding the basic theory, method, application, and limitations of FEA, the clinicians will be better equipped to interpret results of FE studies and apply these results to clinical situations.
The following four case studies – based on the results of FE simulations carried out in collaboration with professors from the Faculty of Dental Medicine, University of Belgrade – demonstrate the full potential of FEM application in dentistry. These studies have proved robustness of FEM in addressing biomedical problems that are challenging for conventional methods.
Case study 1: Evaluation of stress distribution under FPD supported in three different ways
In this study9 FEA was carried out to evaluate stress distributions in supporting tissues in four-unit tooth-tooth, implant-implant and tooth-implant supported dentures. The section contours of the alveolar bone, teeth, and fixed prosthesis were obtained from ATOS scanner and imported into CAD/CAM software CATIA where three different solid models were obtained. Solid model of the implant was constructed in CATIA and imported – along with bone, teeth and prosthesis models – into the software for FEA Ansys Workbench. After meshing the models, setting up material characteristics, boundary and loading conditions, calculations were performed. Materials were assumed homogenous, elastic and isotropic (with Young’s moduli and Poisson’s ratios taken from10), and 300 N axial and oblique load (making an angle of 30° to the long axis) were applied on pontic and all four units.
point changes in accordance to the modeled morphology of the restoration. FEA studies have loaded the cusp tips, distal and mesial fossae of the crowns with the objective of simulating the contact path followed by the functional cusps of a tooth.
It’s important to emphasize that all loads can be classified as either static or dynamic. Masticatory forces are dynamic loads, but since these loads are difficult to numerically model most FEA use static loads8. However, as an illustration that this modelling is possible, FE simulation with dynamic load will be presented in this paper.
The last but not less crucial step in defining FE model is determination of boundary conditions. The boundary conditions (BCs) are the specified values of the field variables (or related variables such as derivatives) on the boundaries of the field of interest. In other words, physical constraints such as displacements and supports must be applied on boundaries of the virtual model to ensure an equilibrium solution. The constraints are placed on nodes and they can prevent displacement and rotation in all directions (so called fixed support) or in some directions only (for example, displacement in X direction is allowed, while displacements in Y and Z direction and rotations about all three axes are not allowed). Boundary conditions can sometimes play the role of loads: instead of applying forces (whose magnitudes might be hard to evaluate) displacement on nodes in given direction is applied to simulate the effect of loading (Figure 3).
Figure 3. 2D FE model with symmetrical BCs and applied displacement
One method for efficient use of FE modeling is to exploit the planes of symmetry in an assembly or a part being analyzed. To take the advantage of symmetry, only a portion (a half, or a quarter) of the actual structure

Balk J Dent Med, Vol 21, 2017 Finite Element Method Applications in Dentistry 73
partial denture (Figure 4 and Figure 5). After reviewing all load combinations and fixtures it was concluded that implant-implant supported fixed partial denture had a better stress distribution compared to tooth-implant fixture.
FEA showed that maximum stress values occurred at the neck of implant and tooth in all models for occlusal forces, while in a case of axial and oblique loading on the pontic the highest stress value was located at the implant neck for tooth-implant supported fixed
Figure 4. Stress distribution in supporting tissue of four-unit tooth-tooth (I), implant-implant (II) and tooth-implant support under axial load (III)
Figure 5. Stress distribution in supporting tissue of four-unit tooth-tooth (I), implant-implant (II) and tooth-implant support under oblique load (III)
Case study 2: Analysis of stress distribution and deformation under FPD for two diverse types of tooth-implant connection
In this case, FEM was used to compute stress distribution in surrounding tissue of a fixed partial denture with tooth-implant connection for two diverse types of implants: resilient Titan Shock Absorber (TSA) abutment was compared to conventional non-resilient abutment11.
Two 3D models were created for this purpose. It was assumed that first and second molar were missing and implant was mounted in the second molar position for both cases. Modelling of the implant and abutment was performed in accordance with dimensions and
recommendations obtained from the manufacturer. Virtual model was comprised of tooth contours, periodontal ligament, mucous membranes, implant, cortical bones and spongiosa, abutment and suprastructure. Figure 6. shows model of tooth-implant supported fixed partial denture.
Again, all used materials were assumed homogenous, linear elastic and isotropic with exception of periodontal ligament which was modelled with 3D non-linear highly elastic spring elements to better replicate its real properties in the FE model. Finite element mesh is shown in Figure 7.
Three different load conditions were taken into consideration with vertical force of 500 N. In first case force was introduced on the tooth, in second above the

74 Aleksandar Grbović, Dimitrije Mihajlović Balk J Dent Med, Vol 21, 2017
Figure 7. Finite element mesh of the fixed partial denture
implant and in third case above all three units. Such models were analyzed using Ansys Workbench software which provided stress distribution for both models and all three load cases. It was observed that the resilient TSA abutment helped load dissipation and that the stress values are lower compared to non-resilient abutment. Deformation results for one type of the load are displayed in Figures 8 and 9 below.
Figure 6. 3D model of tooth-implant supported fixed partial denture
Figure 8. Total deformation in case of force acting above implant with resilient TSA abutment
Figure 9. Total deformation in case of force acting above implant with non-resilient abutment
Case study 3: Analysis of stress distribution in adhesive inlay bridge
Adhesive fixed partial dentures are a part of a group of minimally invasive fixed constructions, with inlay retainers instead of classic-shell retainers. Reduced contact area, however, weakens the retention and makes dentures prone to separation from teeth over time. Since this is a consequence of extensive pressure on the cement layer, stress states of this layer and surrounding elements can be observed, analyzed and interpreted using FME12.
Two extracted teeth were selected and scanned to simulate a lateral dental segment with partial edentulism13. A space of 13 mm was left between the teeth which were prepared with interproximal slots of specific dimensions. The corresponding fixed partial denture (FPD) made of ZirCAD was digitized with a scanner and imported into Ansys Workbench. An assumption was made that the teeth are not fixed and that the root is allowed a certain amount of vertical displacement equal to approximate distance between the alveolus and the root (about two hundredths of a millimeter). Therefore, the whole model was supported by elastic springs, which can simulate assumed behavior.
To simulate masticatory force three areas on the outer inclines of the buccal cusps were loaded (Figure 10). The total load of 225 N was applied along three directions in three successive simulations: at 900 to the tooth long axis (horizontal force), at 450 to the long axis (oblique force) and along the tooth axis (vertical force). Figures 11 and 12 shows stress distributions in the most critical case when horizontal load was applied.
As it can be seen in Figures 11 and 12, maximum stress occurs at contact areas of the bridge and supporting teeth. Stress is concentrated along the edges and over time this stress concentration may lead to tooth damage and, consequently, separation of the denture from tooth. Fatigue cracks always start at stress raisers, so removing them the fatigue strength of the system increases. To prevent cracks or, at least, to reduce the probability of their initiation the fillets at the sharp edges should be created. FEM might be very useful tool in determination of the optimized radii of these fillets.

Balk J Dent Med, Vol 21, 2017 Finite Element Method Applications in Dentistry 75
Figure 13. 3D model of full denture with two mini dental implants
Before adding implants, calculations were performed with denture being supported by the alveolar ridge only. Results showed high displacements which indicated denture non-stability. Then, calculations were carried out with denture supported by MDIs and obtained stress distributions on alveolar ridge and implants can be seen in Figure 14 and 15 respectively. It was obvious that the MDIs were asymmetrically loaded which was caused by asymmetry of the 3D model and loads applied. Only in a case of completely symmetrical model stress distributions would be the same on both MDIs. Since the stress values did not exceed the limits defined by material characteristics, it was concluded that two MDIs could provide substantial support for lower complete denture.
Figure 10 Loads used in FEA of adhesive inlay bridge
Figure 11 Stress distribution in the case of horizontal loading
Figure 12 Stress distribution on the second molar and premolar in the case of horizontal loading
Case study 4: Optimization of the number of MDIs to support complete denture. Simulation of crack growth in MDI under dynamic load.
The main goal of this FE study14 was to determine required number of mini dental implants (MDI) needed to fix complete denture in a case of poorly developed alveolar ridge. MDIs play key role in stabilization of complete dentures, especially lower ones. Due to small dimensions, MDIs can easily be applied even in extremely narrow and small ridges which are common with patients using dentures for a longer period. They contribute to solving problems of retention and stabilization, speech difficulties, etc.
3D model used in this study can be seen in Figure 13. Denture and plaster model of poorly developed alveolar ridge were scanned and imported into CATIA v5, while MDIs were constructed directly in software.
Figure 14. Stress distribution on alveolar ridge
Figure 15. Stress distribution in mini dental implants
Occasionally, during the installation of MDI micro cracks may be initiated on the implant’s surface and their growth can cause – after a certain number of chewing cycles – fatigue failure of MDI in cyclic stress

76 Aleksandar Grbović, Dimitrije Mihajlović Balk J Dent Med, Vol 21, 2017
Figure 17 Steps of crack growth in MDI
environment. To investigate this phenomenon existing FE model of MDI has been used and crack growth in more stressed implant (right MDI in Figure 15) was analyzed15. To simulate fatigue crack growth in implant, it is necessary to define realistic dynamic loads. In this study, horizontal and vertical forces of magnitudes 0.005 N were applied on spherical part of MDI during two consecutive time intervals (each interval was 1 second long). Later, these values were multiplied by cyclic load of amplitude 20000 N to simulate fully reversed load with constant amplitude of approximately 100 N. Since load on MDI, caused by changeable masticatory force acting on the denture, is mostly less than 100 N and varies with time, a random load spectrum (maximum amplitude of 20000 N) was used for crack initiation predictions (Figure 16). Time defined for this spectrum was 94 seconds.
Figure 18. Crack length as a function of number of chewing cycles
The plot in Figure 18 shows crack length versus cycle number. It must be noted that the final crack length was found to be just over 1 mm after 500000 cycles. This result confirmed the expectation that even damaged implant would work well for an extended period. This also concurs with clinical practice experiences, which show that the fatigue failure of MDI rarely occurs during the exploitation. Given that the worst load case scenario was used (load spectrum was very abrupt and rather long), it can be concluded that the least designed life of slightly damaged MDI of 500000 cycles is acceptable.
Discussion
FEM has been shown to be a useful tool when investigating complex systems that are difficult to standardize during in vitro and in vivo studies. It has been used mostly to evaluate the influence of the type of material and geometry on the stress distribution and deformation during chewing cycles. Most of the studies employed linear static models which are valid if the structure exhibits a linear stress–strain relationship and all the volumes are bonded as one unit. However, realistic testing situations give rise to dynamic models and nonlinearities, which can be classified in two main categories: (1) material nonlinearities (that cause the stiffness to change with different load levels) and (2) geometric nonlinearities (such as nonlinearities in the vicinity of a crack tip).
Main dilemma in application of FEM in dentistry is to which extent is the numerical model equivalent to the real biological system. Many studies have shown significant trend regarding advancements and
Figure 16 Random load spectrum used for crack initiation analysis
After the horizontal and vertical force had been applied, FE analysis was performed and obtained stress values were 0.0459 MPa and 0.00639 MPa, respectively. This is because small loads (0.005 N) were applied on MDI. But, during the second phase of the simulation these loads were multiplied by previously described random spectrum to get realistic dynamic loads. In Figure 15 the critical area of MDI (in terms of crack appearance) is showed in red color and the number of blocks of load spectrum which would initiate the crack was found to be between 533 and 20000. This means that total time before crack would start to grow is between 14 and 500 hours (total time depends on number of appearances of peak values during chewing).
The first step in setting the crack growth properties was to define the initial crack length. The value of 0.05 mm was chosen. The second step was to define crack geometry. It is assumed that the crack in the implant is much like a semi-circular crack in tension. Once the model was created in ANSYS, the steps necessary to perform crack growth analysis were: read the mesh information, rebuild the mesh around the crack, perform the Ansys analysis and compute new crack length16.
The program begins the process of inserting the flaw into the original model and then meshes the resulting cracked model. Figure 17 display the computed crack front in the model after five and ten steps of calculation. After each step the extension was scaled, polynomial was adjusted to fit through the new crack front points and the polynomial extrapolation was adjusted to ensure intersection with the model surface.

Balk J Dent Med, Vol 21, 2017 Finite Element Method Applications in Dentistry 77
4. Duygu Koc, Arife Dogan, and Bulent Bek, Bite Force and Influential Factors on Bite Force Measurements: A Literature Review. Eur J Dent, 2010;4:223-232.
5. Olmsted MJ, Wall CE, Vinyard CJ. Human bite force: the relation between EMG activity and bite force at a standardized gape. Am J Phys Anthropol, 2005;40:160-161.
6. Rangert B, Jemt T, Jörneus L. Forces and moments on Branemark implants. Int J Oral Maxillofac Implant, 1989;4:241-247.
7. Mericske-Stern R, Piotti M, Sirtes G. 3-D in vivo force measurements on mandibular implants supporting overdentures. A comparative study. Clin Oral Implants Res, 1996;7:387-396.
8. Akyuz E, Braun JT, Brown NA, Bachus KN. Static versus dynamic loading in the mechanical modulation of vertebral growth. Spine, 2006;31:952-958.
9. Erić J, Tihaček Šojić Lj, Lemić A, Bjelović Lj, Grbović A. Evaluation of stress distributions in supporting tissues in four-unit tooth, implant-implant and tooth-implant supported dentures by finite element analysis, Belgrade, 2016.
10. Lin ChL, Wang JCh, Chang WJ. Biomechanical interactions in tooth– implant-supported fixed partial dentures with variations in the number of splinted teeth and connector type: a finite element analysis. Clin Oral Impl Res, 2008;19:107-117.
11. Glišić M, Stamenković D, Grbović A, Todorović A, Marković A, Trifković B. Analysis of load distribution on tooth-implant supported fixed partial dentures by the use of resilient abutment. Srp Arh Celok Lek, 2016;144:188-195.
12. Grbović A, Vidanović N, Čolić K, Jevremović D. The use of finite element method (FEM) for analyzing stress distribution in adhesive inlay bridges, Third Serbian (28th Yu) Congress on Theoretical and Applied Mechanics, Vlasina lake, Serbia, 5-8 July 2011.
13. Jevremović D. Distribucija i koncentracija napona u adhezivnim mostovima, Doctoral Thesis, Belgrade, 2008.
14. Grbović A, Tanasković M, Vidanović N. Comparative analysis of stress distribution on the toothless alveolar ridge at the bottom of the complete denture prosthesis and overdenture retained with mini implants, 2nd International Congress of Serbian Society of Mechanics, D-14, 2009.
15. Grbović A, Rašuo B, Vidanović N, Perić M. Simulation of crack propagation in titanium mini dental implants (MDI). FME Transactions, 2011;39:165-170.
16. Kastratović, G. Determination of Stress Intensity Factors of Supporting Aero Structures with Multiple Site Damage, PhD thesis, Faculty of Mechanical Engineering, University of Belgrade, Belgrade, 2006.
Received on May 1, 2017.Revised on May 11, 2017.Accepted on May 22, 2017.
Correspondence:
Aleksandar Grbović Faculty of Mechanical Engineering University of Belgrade, Serbia е-mail: [email protected]
optimizations of FE models. Enhancements in software and hardware have significant positive impact on this trend. However, it is important to emphasize that even with all improvements, it is still impossible (and will be impossible in near future) to fully replicate the complexity of the human body.
Bone, mucoperiosteum or teeth are complex non-homogenous and anisotropic structures that are simplified in FEA to be adapted for calculations. These simplifications do not imply that the results obtained from such models are useless, but should be taken with caution. They are not conclusive and must be supported with clinical researches. Examples presented in this paper showed that the most valuable result of FEA was identification of critical (high stress) areas of the physical model.
Resulting stress distributions are useful, but the stress values that would lead, for example, to the mandible fracture are still not unquestionably defined and there is no evidence of bone rupture due to implant overload in clinical practice. Vast number of researches was pointed to the prediction of bone mass loss in the implant surroundings due to overload. It must be borne in mind that this concept is still insufficiently explored and that there is no reliable evidence of connection between these phenomena. Bone resorption is a dynamic process primarily influenced by biological factors.
For the aforementioned reasons, it can be concluded that the finite element method should be used as a tool for comparison and analysis of similar cases and not as a tool for drawing final conclusions. Future applications should be focused to optimization and verification of bone models, temporo-mandibular joint, teeth, implants, dentures, etc. Usefulness of FEM should be reflected in testing the new hypotheses which can be later confirmed in vivo. Differences (or similarities) in hypotheses identified by means of finite element calculations can be solid foundation for further clinical researches.
Note: The results of this paper were presented as a part of an invited lecture at the 22nd BaSS Congress.
References
1. Stomatološki fakultet. Stomatološki materijali knjiga 2: Beograd; 2012.
2. Ming-Lun Hsu, Chih-Ling Chang, Application of Finite Element Analysis in Dentistry, Finite Element Analysis, ed. David Moratal, 2010.
3. Geng J, Yan W, Xu W (Eds.). Application of the Finite Element Method in Implant Dentistry, ISBN: 978-3-540-73763-6, Springer, 2008.

SUMMARYPremature loss of teeth in children may lead to both functional and
esthetic problems. Missing teeth in both anterior and posterior regions may cause malfunctions in mastication and proper pronunciation. If the missing teeth are not replaced, further complications may occur, including adjacent tooth migration, loss of alveolar bone, and irregular occlusion. Considering the sensitive nature of children, loss of teeth may cause the development of insecurities and low self esteem problems. Due to dynamic nature of growth in children and adolescents, prosthetic appliances must not hinder development of orofacial system, and must meet adequate esthetic and functional standards. Dental prosthetic appliances in paediatrics must be planned with respect to the special conditions that led to tooth loss or damage. Multi-disciplinary approach is needed, under constant supervision of paediatric dentist and orthodontist, as well as regular checkups with clinical and radiographical examinations. Key words: Prosthetic, Child, Dental Crown, Adhesive Bridge, Denture
Zoran Vulićević1, Miloš Beloica1, Dušan Kosanović1, Ivana Radović1, Jelena Juloski1, Dragan Ivanović2
1 Clinic for Pediatric and Preventive Dentistry Faculty of Dental Medicine University of Belgrade, Serbia 2 Faculty of Medicine, University of East Sarajevo Republic of Srpska, Bosnia and Herzegovina
REVIEW PAPER (RP)Balk J Dent Med, 2017;78-82
BALKAN JOURNAL OF DENTAL MEDICINE ISSN 2335-0245
Prosthetics in Paediatric Dentistry
STOMATOLOGICA
L S
OC
IET
Y
Introduction
Premature teeth loss, both deciduous and permanent, may cause functional problems in children, such as malfunctions in mastication, improper teeth placement or eruption and hindered pronunciation. Esthetical issues are also present, as child may be mocked or bullied, leading to insecurity, development of complexes and low self esteem.
Modern dental prosthetic appliances need to fulfill several important criteria in order to be considered as an adequate treatment options in children:1. Rehabilitation of masticatory functions and efficiency:
Prosthetic appliance needs to be able to replace missing teeth without hindering child’s ability to chew. They must be designed properly to avoid or minimize wear on the opposing dentition.
2. Protection of dental pulp: Vitality of dental pulp should be preserved whenever possible. Prosthetic restoration must be made with great care not to disturb vitality of the tooth it is on (if vital), as well as adjacent or opposite teeth. Prosthetic restoration needs to be regularly checked and adjusted accounting for child’s growth and development.
3. Esthetic criteria: Restoring esthetics is one of the pillars of modern dentistry. Caring about personal appearance is very important to children, especially in adolescence1. However, there are recent studies showing that even children in preschool period (age 3-5) have a developed consciousness about their body image, and do care about how they are perceived by other children and adults alike2.
4. Proper speech function: Missing teeth, especially in anterior regions, may cause improper speech. Missing incisors often lead to a child being unable to properly pronounce dental consonants such as “t”, “d”, “n” and in some languages “l”. Similar problems may develop in children with cheilo-gnato-palatoschisis. This may lead to development of improper speech patterns that need to be corrected with the aid of speech therapist after the missing teeth or defects are taken care of with adequate prosthetic appliance.
5. Prosthetic appliance must support optimal and proper development of teeth and their eruption, as well as support growth of the dental arches, and facial bones. Prosthetic appliances need to be regularly maintained, adjusted and checked in order to prevent
10.1515/bjdm-2017-0012

cause a variety of unwanted clinical symptoms, mostly due to allergenic potential of nickel. Since then, design of the crowns as well as metals used significantly changed5. Nowadays stainless steel crown consist of blend of metals that includes iron, chromium, carbon and 9% nickel, similar to orthodontic wires (Figure 1). Stainless steel crowns are known for their durability, as shown by Prabhakar et al in their in vitro study6. Longevity of the crown mainly relies on following proper protocols for crown placement, especially in relation to margins. If it is possible, crown margin should rest on healthy tooth substance, and if it is not, then on amalgam or glass ionomer restorative material, as studies have shown these two material demonstrate least amount of microleakage7. Possibly the greatest issue with stainless steel crowns is their poor esthetical appearance, which limits their use to restoration of primary first and second molars. Nevertheless, these crowns may be esthetically satisfactory when veneered using composite materials in frontal teeth.
them from inhibiting proper orofacial development. In that sense, considering the fluid and changing environment of a child’s oral cavity, all dental prosthetic appliances have a temporary function.
6. Prevention of harmful habits: missing teeth or improper teeth alignment may cause the child to develop bruxism (teeth grinding), or to repeatedly clench their jaws. These habits can also develop in some children as a response to pain, sometimes during teeth eruption. Also, kids with certain medical condition, such as cerebral palsy, are also prone to develop bruxism. The purpose of the adequate prosthetic appliance in these cases is to prevent harmful habit by stabilizing occlusion and preventing painful sensations.
7. Provision of space maintenance: If the missing teeth are not replaced with a prosthetic appliance, adjacent teeth can migrate towards the toothless alveolar ridge, leading to occlusion problems and issues with dental eruption.
8. Fixation of loosened teeth after trauma: Splints, both wire and composite or fiber, perform a crucial role in saving teeth that have been loosened by trauma. Detailed examination with x-rays must be performed before splinting the teeth, and regular dentist supervision and checkups must be maintained for the duration of the splint, to avoid ankylosis.All of these criteria must be fulfilled in order to
create appropriate conditions for definite prosthodontics once the adult age is reached.
In the past, when deciduous tooth was suffering from extensive decay, most often outcome for such tooth was extraction. Pulpotomytreatment, and large carious lesions on primary teeth often led to failure of direct restorations, due to inability provide adequate, saliva free working environment and sufficient retention. Nowadays, crowns are considered a viable alternative3. Indications for use of dental crowns on deciduous teeth are:
1. developmental defects2. fractured teeth3. teeth after pulpal therapy4. restoring multisurface caries, especially in patients
with high caries risk5. teeth with extensive wear6. teeth that need to function as an abutment for space
maintainerMaterials and designs used for such crowns varied
greatly over the years, and recent improvements in design of dental materials have provided a variety of different dental crowns. Most important factors considered by dentists when choosing adequate crowns are durability, esthetics, retentiveness, adaptability, placement time, allergenicity and cost.
Stainless steel crowns first appeared as a full-tooth-coverage treatment option as early as 1950’s4. These first crowns, composed of nickel-chromium, were known to
Figure 1. Stainless Steel. Crown cemented in place
Zirconia crowns are relatively new in dentistry, firstly introduced in 2001. by Suttor et al8. However, the material itself has been in use in medicine since 1960’s, in orthopedic application during hip surgeries. Zirconia used in dental crowns is yttrium stabilized zirconia9. This provides the dental zirconia with highest flexural strength of all zirconia based materials, alongside high chemical and erosion resistance. Furthermore, material is biocompatible, hypoallergenic, and with similar durability as natural enamel. As they cannot be adjusted (unlike stainless steel crowns), zirconia crowns for primary teeth come prefabricated with specific attributes. It is therefore important to trial-fit using the mock-up crown before cementing, to ensure proper tooth preparation, margin and occlusion (Figure 2). Unlike traditional ceramic, zirconia crowns for primary teeth demonstrate low wear on the opposing dentition. Choi et al. in their in vitro study
Balk J Dent Med, Vol 21, 2017 Prosthetics in Paediatric Dentistry 79

80 Zoran Vulićević et al. Balk J Dent Med, Vol 21, 2017
show that zirconia and stainless steel crowns demonstrate lowest wear rates amongst materials for full coverage paediatric dental crowns, and as such should be primary choice, compared tolithium-disilcate glass ceramic and leucite glass-ceramic10. Excellent esthetical appearance of prefabricated zirconia crowns makes them fully usable in restorations in both anterior and posterior regions (Figure 2), with good durability and lifespan, as shown by Ashima et al.11.
Figure 2. Trial fitting with mock-up crowns before cementing
Partial removable dentures in children must be planned with child growth and development in mind. Design of dentures must be such that it allows for modification when teeth erupt or migrate. That said, long periods without a tooth (or tooth replacement) lead to narrowing of alveolar processes and vertical alveolar defects at sites with missing teeth, over eruption of unopposed permanent teeth, and tipping of adjacent teeth12.
Tissue supported partial dentures are indicated when we expect a child to be without a tooth for a prolonged period of time, or when bone resorption and remodeling is anticipated immediately following extraction or traumatic tooth loss. They are also indicated in severe cases of hypodontia, weather hereditary (like ectodermal dysplasia) or after cyst or tumor operations. Denture fabrications in early age, especially in cases of hypodontia, may lead to significant improvements in appearance, speech and masticatory functions. Such positive changes may increase the self-confidence of the child and aid in establishing proper dietary patterns. Balla et al. showed that wearing tissue supported dentures does not inhibit maxillar or mandibular growth13 .
Figure 3. Cemented zirconia crowns
Figure 4. Edentuous state in deciduous dentition, central incisors about to erupt
Figure 5. Tissue supported denture

Balk J Dent Med, Vol 21, 2017 Prosthetics in Paediatric Dentistry 81
All dentures designed must allow for proper hygienic maintenance of both denture and child’s oral cavity, and insure no damage to surrounding tissues. Regular checkups and recalls must be made every 3-6 months, and modifications must be made to match and accommodate to child’s growth and development.
Loss of anterior teeth in children and adolescents is more often a result of injury and/or complication from previous trauma (like ankylosis or root resorption). Central maxillary incisors are teeth most frequently affected by trauma15. During period of childhood, and especially in puberty, a non-invasive long term interim restoration should be designed until implant is indicated. Because of risk of complications such as implant infraposition, implant therapy should be postponed until adulthood is reached16.
Resin bonded or resin retained bridges represent a minimally invasive option for replacing missing teeth. This type of restoration was first described in 1970’s, and since then, they have evolved significantly in both design and materials used. First type of resin bonded bridge was known as Rochettebridge, which generated its retention through resin cement bonding through characteristic perforated metal retainer. The commonly used nickname for resin retained bridges “Maryland bridge” results from the type of electrochemical etching developed at university of Maryland, which improved and enhanced resin bonding to the metal alloy.
In recent years, with development of new materials, traditional metal-resin restorations are starting to slowly be abandoned in favor of modern fiber reinforced composites. Evolution of fiber products for dental use has transitioned from plain fibers, over pre-impregnated fibers to fully resin impregnated fibers. Most common types of fibers for use in resin bonded bridges are polyethylene, Kevlar and glass based fibers. Also, the fibers may be unidirectional, braid, mesh/network or woven. Different types of fibers and weaves create different adaptability and manageability, as well as different capabilities to distribute the force multidirectional. Majority of clinical studies of resin bonded bridges report on unidirectional fibers, and out of those, most used areglass fibers, mainly due to their strength and aesthetics17. The use of fiber reinforced composites in resin bonded restorations is advised for their favorable elastic module in comparison to metal, and better adhesion of the composite to the framework18.
Main advantages of resin bonded bridges are their preservance of healthy tooth substance, needing no or minimal preparations, reduced costs and generally good patient acceptance19. Also, they tend to remove pressure from mucosae and alveolar ridge (unlike tissue supported partial denture), therefore reducing the risk of alveolar bone resorption and possible complications with future implant therapy. Careful planning is needed in order properly distribute masticatory pressure on the adjacent teeth. Resin bonded bridges are relatively easy
Retention of tissue supported dentures in children is most often achieved by extended body of acrylic base of the denture, resting on alveolar ridge and palate (Figures 4 & 5). Clasps are only used when necessary, due to force they administer to teeth, but some orthodontic springs may be incorporated in the design of the denture to facilitate necessary tooth movement (if needed).
In recent years, polyamide based dentures have started to be more frequently used in paediatric dentistry, mainly due to its higher elasticity, toxicological safety and good esthetic14. Their high adaptability and elasticity makes them especially suited for use in deciduous and mixed dentition period.
Teeth supported dentures can be designed in edentuous states following cyst or tumor operations in mandibular or maxillar region (Figure 6). In these cases, it would not be advisable to apply pressure on compromised gingival or bone tissues, as that could lead to post-operative complications, ulcerations and infections. Retention of teeth supported dentures is achieved via dental clasps and occlusal rests, minimizing as much as possible contact with mucosae, while rigidity of the denture is ensured by the supportive metal frame (Figure 7).
Figure 7. Teeth supported denture, retention with occlusal rests and dental clasps
Figure 6. A 12 year old girl, status post osteosarcoma and mandibular resection.

82 Zoran Vulićević et al. Balk J Dent Med, Vol 21, 2017
3. Innes NP, Ricketts D, Chong LY, Keightley AJ, Lamont T, Santamaria RM. Preformed crowns for decayed primary molar teeth. Cochrane Database Syst Rev, 2015;12:CD005512.
4. Engel RJ. Chrome steel as used in children’s dentistry. Chron Omaha Dist Dent Soc, 1950;13:255-258.
5. Noble J, Ahing SI, Karaiskos NE, Wiltshire WA. Nickel allergy and orthodontics, a review and report of two cases. Br Dent J, 2008:204:297-300.
6. Prabhakar AR, Yavagal CM, Chakraborty A, Sugandhan S. Finite element stress analysis of stainless steel crowns. J Indian Soc Pedod Prev Dent, 2015;33:183-191.
7. Memarpour M, Derafshi R, Razavi M. Comparison of microleakage from stainless steel crowns margins used with different restorative materials: An in vitro study. Dent Res J (Isfahan), 2016;13:7-12.
8. Suttor D, Bunke K, Hoescheler S, Hauptmann H, Hertlein G. LAVA-the system for all-ceramic ZrO2 crown and bridge frameworks. Int J Comput Dent, 2001;4:195-206.
9. Available at: http://www.ceramics.net/services/materials-engineering-expertise/ytzp-yttria-stabilized-zirconia. Accessed 03/18/2017
10. Choi JW, Bae IH, Noh TH, Ju SW, Lee TK, Ahn J et al. Wear of primary teeth caused by opposed all-ceramic or stainless steel crowns. J Adv Prosthodont, 2016;8:43-52.
11. Ashima G, Sarabjot KB, Gauba K, Mittal HC. Zirconia crowns for rehabilitation of decayed primary incisors: an esthetic alternative. J Clin Pediatr Dent, 2014;39:18-22.
12. Jepson NJ, Nohl FS, Carter NE, et al. The interdisciplinary management of hypodontia: restorative dentistry. Br Dent J, 2003;194:299–304.
13. Bhalla G, Agrawal KK, Chand P, Singh K, Singh BP, Goel P et al. Effect of Complete Dentures on Craniofacial Growth of an Ectodermal Dysplasia Patient: A Clinical Report. J Prosthodont, 2013;22:495-500.
14. Vojdani M, Giti R. Polyamide as a Denture Base Material: A Literature Review. J Dent, 2015;16:1-9.
15. Borum MK, Andreasen JO. Therapeutic and economic implications of traumatic dental injuries in Denmark: an estimate based on 7549 patients treated at a major trauma centre. Int J Paediatr Dent, 2001;11:249-258.
16. Zitzmann NU, Özcan M, Scherrer SS, Bühler JM, Weiger R, Krastl G. Resin-bonded restorations: A strategy for managing anterior tooth loss in adolescence. J Prosthet Dent, 2015;113:270-276.
17. Dyer SR, Lassila LV, Jokinen M, Vallittu PK. Effect of fiber position and orientation on fracture load of fiber-reinforced composite. Dent Mater, 2004;20:947-955.
18. Burke FJ. Resin-retained bridges: fibre-reinforced versus metal. Dent Update, 2008;35:521-522.
19. Vallittu PK, Sevelius C. Resin-bonded, glass fiber-reinforced composite fixed partial dentures: a clinical study. J Prosthet Dent, 2000;84:413-418.
20. Wolff D, Schach C, Kraus T, Ding P, Pritsch M, Mente J et al. Fiber-reinforced composite fixed dental prostheses: a retrospective clinical examination. J Adhes Dent, 2011;13:187-194.
Received on May 1, 2017.Revised on Jun 1, 2017.Accepted on Jun 12, 2017.
Correspondence:
Zoran Vulićević Clinic for Pediatric and Preventive Dentistry Faculty of Dental Medicine, University of Belgrade, Serbia e-mail: [email protected]
to install, rarely require local anesthesia, and are therefore appropriate for patients who may have increased anxiety in dental chair, or are unable to devote themselves to multiple dental appointments. Patients should, however, be properly introduced and motivated of the importance of adequate oral health and hygiene, as poor maintenance of resin bonded bridge may lead to gingivitis, periodontal issues, and failure of the restoration.
Most common reasons of failure of resin bonded bridge are de-bonding, and discoloration and chipping, especially in areas where fibers have been exposed to oral cavity. Majority of the studies show that the expected survival rate of resin bonded bridge to be around 72-74% after the period of 3-5 years20. Also, it is reported that anterior restorations can be expected to last longer than posterior ones, as well as that survival rate of resin bonded bridges in maxilla is higher as opposed to mandible (81% vs 56% after 2.5 years). There is however a definite lack of detailed, standardized information in the literature concerning longevity of resin bonded bridges. It is also important to note that developments of new generations of composite restoration materials and bonding agents can possibly question validity of the results of the older publications.
Conclusion
Childhood and adolescence represent a period of intense growth and development of orofacial system. In such gentle period, replacement of missing teeth is of vital clinical importance, and variety of materials and restoration design options exist to ensure that proper chewing, aesthetics and pronunciation are achieved. Adequate prosthetic restoration in children or adolescents must not in any way hinder proper development of jaw bones, dental arches and permanent teeth, but rather guide and preserve oral tissues in a minimally invasive way to ensure that satisfactory definite restoration can be achieved once adulthood is reached. Frequent checkups and careful clinical supervision are advised, as well as maintaining adequate oral hygiene of the patient.
Note: The results of this paper were presented as a part of an invited lecture at the 22nd BaSS Congress.
References
1. Di Blasio A, Mandelli G, Generali I, Gandolfini M. Facial aesthetics and childhood. Eur J Paediat Dent, 2009;10:131-134.
2. Tremblay L, Lovsin T, Zecevic C, Larivière M. Perceptions of self in 3-5-year-old children: a preliminary investigation into the early emergence of body dissatisfaction. Body Image, 2011;8:287-292.

SUMMARYBackground/Aim: Dental implants are a reliable treatment choice
for rehabilitation of healthy patients as well as subjects with several systemic conditions. Patients with oral mucosal diseases often exhibit oral mucosal fragility and dryness, erosions, blisters, ulcers or microstomia that complicate the use of removable dentures and emphasize the need for dental implants. The aim of the current study is to review the pertinent literature regarding the dental implantation prospects for patients with oral mucosal diseases. Material and Method: The English literature was searched through PubMed and Google Scholar electronic databases with key words: dental implants, oral mucosal diseases, oral lichen planus (OLP), epidermolysis bullosa (EB), Sjögren’s syndrome (SS), cicatricial pemphigoid, bullous pemphigoid, pemphigus vulgaris, scleroderma/systemic sclerosis, lupus erythematosus, leukoplakia, oral potentially malignant disorders, oral premalignant lesions, oral cancer and oral squamous cell carcinoma (SCC). Results: Literature review revealed dental implantation in patients with OLP (14 articles), EB (11 articles), pemphigus vulgaris (1 article), SS (14 articles), systemic sclerosis (11 articles), systemic lupus erythematosus (3 articles) and oral SCC development associated with leukoplakia (5 articles). No articles regarding dental implants in patients with pemphigoid or leukoplakia without SCC development were identified. Most articles were case-reports, while only a few retrospective, prospective or observational studies were identified. Conclusions: Dental implants represent an acceptable treatment option with a high success rate in patients with chronic mucocutaneous and autoimmune diseases with oral manifestations, such as OLP, SS, EB and systemic sclerosis. Patients with oral possibly malignant disorders should be closely monitored to rule out the development of periimplant malignancy. Further studies with long follow-up, clinical and radiographic dental data are required to predict with accuracy the outcome of dental implants in patients with oral mucosal diseases.Key-words: Dental Implants, Oral Lichen Planus, Epidermolysis Bullosa, Pemphigus Vulgaris, Sjögren’s Syndrome, Systemic Sclerosis, Leukoplakia, Oral Carcinoma
Eleni-Marina Kalogirou, Alexandra Sklavounou
Department of Oral Medicine and Pathology Faculty of Dentistry National and Kapodistrian University of Athens Athens, Greece
REVIEW PAPER (RP) Balk J Dent Med, 2017;83-92
BALKAN JOURNAL OF DENTAL MEDICINE ISSN 2335-0245
Is Dental Implantation Indicated in Patients withOral Mucosal Diseases
STOMATOLOGICA
L S
OC
IET
Y
Introduction
Dental implants are a reliable treatment choice for rehabilitation of partially or completely edentulous patients1. On the basis of the implant failure factors that have been proposed, i.e. clinical or/and radiographic findings that require implant extraction- pain or mobility
during clinical examination or periimplant radiolucency in dental x-rays2, the success rate of dental implantation surpasses 90% during a 10-year-observation period3.
This high success rate generally refers to subjects with unremarkable medical history. On the other hand, medically compromised subjects, with systemic diseases such as diabetes mellitus, osteoporosis, cardiovascular
10.1515/bjdm-2017- 0013

84 Eleni-Marina Kalogirou, Alexandra Sklavounou Balk J Dent Med, Vol 21, 2017
Data retrieved included number of patients, patients’ demographics, history of autoimmune disorders, oral manifestations, number of inserted implants and type of prosthodontic restoration, implants success rate and follow-up period. Implants were considered as successful in case there was no need for removal at the study end point; thus, the implant success rate coincided with the survival rate. In cases with oral carcinoma development, information about the time interval between the placement of implants and cancer diagnosis, the site and clinical presentation of cancer, prior positive oral cancer history and smoking habits were also recorded. Studies regarding dental implants in patients with de novo oral cancer, i.e. without history of oral mucosal disease, were excluded.
Results
The literature review yielded 50 studies with regards to dental implants in patients with oral mucosal diseases; in particular, 14 studies referred to OLP13,17-29, 11 studies to EB15,30-39, 1 study to pemphigus vulgaris40, 14 studies to SS11-14,21,41-49, 11 studies to systemic sclerosis13,48-57, 3 studies to systemic lupus erythematosus (SLE)1429,44 and 5 studies to oral SCC development associated with leukoplakia27,58-61. Five studies presented patients with more than one oral mucosal disease13,21,27,29,48. Studies regarding dental implants in patients with cicatricial or bullous pemphigoid, as well as in patients with leukoplakia that did not progress into oral malignancy, were not identified.
Oral Lichen PlanusOur review identified 14 studies from the English
literature with 87 OLP patients (63 females and 24 males, female to male ratio: 2.63:1) who have received more than 313 dental implants13,17-29. In 3 patients information on the number of implants inserted was not available27. In particular, 9 case reports13,19-22,25,26,28,29, 3 retrospective studies18,24,27 and 2 prospective controlled studies17,23 were retrieved. In the majority of the patients, OLP was diagnosed prior to implants’ insertion13,17-26; in two studies implants were placed before and after the diagnosis of OLP18,25, while in two studies information regarding to exact time of implant insertion was missing27,29. One OLP patient also suffered from SS21 and another from SLE29. At the time of first examination OLP type was predominantly reticular or plaque-type in 19 (21.8%) patients, erosive or atrophic in 38 (43.7%) patients and unspecified in 30 (34.5%) patients (Table 1). In 32 cases with available information on the intraoral site of OLP lesions, the buccal mucosa and the gingiva were mainly involved, followed by the tongue and palate (Table 1). In 9 patients OLP lesions were noticed in close proximity to the dental implants18,24. Desquamative
disease, immunosuppression etc. were considered to be at an increased risk for implant placement and a number of relative and absolute contraindications have been suggested4-6.
Recently, investigators have proposed that head and neck radiotherapy at a dose > 50Gy, intravenous bisphosphonates therapy and chronic systemic treatment with hormonal agents, corticosteroids or immunosuppressive drugs may be considered to be contraindications for implant placement7. Other studies have stated that positive history for hepatitis, cardiovascular diseases, rheumatic disorders and osteoporosis are significantly associated with increased rates of implant failure. However there is no consensus on those issues, which still remain controversial8,9. Therefore nowadays, the spectrum of indications for dental implants in medically compromised patients has undergone many modifications and has been widened.
In addition to the impact of systemic diseases, the possible effect of oral mucosal diseases on the successful rehabilitation with dental implants has attracted increasing interest during the last decade1,10. The oral mucosal soreness observed in several mucocutaneous diseases and the oral dryness in patients with autoimmune disorders, such as Sjögren’s syndrome (SS) or lupus erythematosus, complicates the proper oral hygiene and predisposes to increased dental caries, periodontal disease and infections leading to further tooth loss11-13. Except for the oral mucosal fragility and xerostomia in those subjects, patients with rare diseases, such as epidermolysis bullosa (EB) and scleroderma, are characterized by various oral complications, e.g. blisters, tissue scars, induration and microstomia, which hinder the use of removable dentures and render dental implants not only a promising therapeutic solution, but occasionally the single treatment of choice12,14-16.
The aim of the present study is to review the pertinent literature regarding the dental implant treatment prospects for patients with oral mucosal diseases.
Materials and Methods
PubMed and Google Scholar electronic databases were searched in April 2017 with the following key words: dental implants, oral mucosal diseases, oral lichen planus (OLP), EB, SS, cicatricial pemphigoid, bullous pemphigoid, pemphigus vulgaris, scleroderma/systemic sclerosis, lupus erythematosus, leukoplakia, oral premalignant lesions, oral cancer, oral squamous cell carcinoma (SCC). Only studies from the English literature were selected. Prospective or retrospective clinical studies, case studies or case-reports were included in the current analysis. Review papers were excluded.

Balk J Dent Med, Vol 21, 2017 Dental Implantation and Oral Mucosal Diseases 85
insertion and oral cancer development was unspecified29. Three OLP subjects with SCC were smokers19,27, 2 had a history of oral cancer22,27 and one had been also diagnosed with oral leukoplakia27. Dental implants in close proximity to the oral malignancy were removed19,22,26,27. In contrast, 244/288 implants survived in 79 OLP patients without SCC development during a follow up period ranging from 21 months to 13 years (success rate = 84.7%)13,17,18,21,23-25,28. Two implants failed in a patient with bruxism 32 and 60 months after their insertion20, while 42 implants were lost in 20 patients with active OLP within the first year of their placement17. These 42 implants were replaced with absolute success for a 3-year-observational period17.
gingivitis was reported in 16 subjects23,24. In symptomatic OLP cases, a steroid-based therapy either topical or systemic usually preceded implants insertion17,18,21-23,26. Moreover, disease exacerbations during the postoperative and the follow-up period were managed with topical corticosteroids, antifungal agents or retinoids18,21,23,24. The type of prosthodontic restoration was reported in 73/87 (83.9%) OLP patients and in the majority of the cases (64/73, 87.7%) represented a fixed prosthesis13,17,19,23-29.
Among 87 OLP patients with dental implants, 8 women (9.2%) developed oral SCC, which presented as a mandibular exophytic mass; two of them within the first year following implant insertion27 and four 319,22 or 4 years26,27 post-insertion. In two patients the interval between implant
Table 1. Demographics and clinical data of OLP patients, number of implants, implants success rate, duration of follow-up and oral SCC development
Reference Patients Gender Age (years) OLP type* OLP Site* Implants Success
rate (%)Follow-up (months)**
SCC development
Esposito et al 200020 1 F 69 erosive NA 2 0 32, 60 no
Esposito et al 200321 2
F 72 erosivebuccal
mucosa, gingiva
2 100 21 no
F 78 erosive NA 2 100 21 noOczakir et al 200513 1 F 74 NA NA 4 100 72 no
Reichart 200625 3
F 63 reticular (and atrophic) gingiva 4 100 156 (2), 24
(1), NA(1) no
F 68 reticular (and atrophic)
buccal muco-sa, gingiva 1 100 36 no
F 79 atrophic gingiva 5 100 NA noCzerninksi et al 200619 1 F 52 NA NA 3 0 36 yes
Gallego et al 200622 1 F 81 plaque-type (and
erosive)palate, buccal
mucosa, tongue
4 0 36 yes
Hernandez et al 201223 18 14F, 4M mean:
53.7 erosive (18)buccal
mucosa (18), gingiva (11)
56 100 mean: 53.5 no
Czerninksi et al 201318 14 11F, 3M mean:
59.5erosive (6), atrophic (5), reticular (3)
buccal mucosa, gingiva (mainly)
54 100 12 to 24 no
Marini et al 201326 1 F 51 plaque-type NA 2 0 108 yes
Moergel et al 201327 3
F 54 NA NA NA NA 7 m yes
F 69 NA NA NA NA 6 m yes
F 80 NA NA NA NA 51 m yesLopez-Jornet et al 201424
16 10F, 6M mean: 64.5
erosive/atrophic (5), reticular (11) NA 56 100 mean: 42 no
Silva et al 201428 1 F 54 plaque-type,
reticular tongue 5 100 24 noRaiser et al 201629 2 2F 55, 70 NA NA 16 <100 36, 96 yes
Aboushelib & Elsafi 201717
23 12F, 11M mean: 56.7 NA NA 55 23.6 8-11 no
42 100 36 noAbbreviations: OLP, oral lichen planus; F, female; M, male; NA, not available; SCC, squamous cell carcinoma* Numbers in parentheses represent patients** Numbers in parentheses represent implants

86 Eleni-Marina Kalogirou, Alexandra Sklavounou Balk J Dent Med, Vol 21, 2017
microstomia, buccal and vestibular sulci obliteration, jaw atrophy and formation of soft tissue scars15,30-39. Fixed prostheses15,30-36,38,39 and removable overdentures35,37 were used in 22 and 7 patients, respectively, while in five subjects with atrophic jaws implants were inserted simultaneously with bone grafts31,38. During an observational period ranging from 1 to 9 years, 177/180 (98.3%) implants were successfully retained (Table 2).
Epidermolysis BullosaThe first case of dental implants in EB patients
was published37 in 2000. To date, 11 studies (6 case-reports15,30-34, 3 prospective35-37 and 2 retrospective studies38,39) could be disclosed reporting rehabilitation of 29 EB patients (19 females, 9 males, 1 gender not specified) with 180 dental implants. EB patients exhibited multiple bleeding blisters or ulcers, ankyloglossia,
Table 2. Demographics of EB patients, number of implants, implants success rate and duration of follow-up
Reference Patients Gender Age (years) Implants Success rate (%) Follow-up (months)
Penarrocha-Diago et al 200037 4
M 30 3 100 36F 35 2 100 12F 30 6 100 24F 26 4 100 48
Penarrocha et al 200736 3M 29 9 100 36F 44 9 100 60F 43 9 88.9 24
Penarrocha et al 200735 6
F 23 2 100 108F 36 6 100 96M 28 3 100 84M 29 9 100 36F 44 9 100 60F 43 9 88.9 24
Lee et al 200732 1 M 29 8 100 17Larrazabal-Moron et al 200931 1 F 52 2 100 18Oliveira et al 201034 1 F 17 2 100 30Müller et al 201033 1 NA NA, ≥20, <25 10 100 NA, ≤60
Penarrocha-Oltra et al 201139 6
F 24 4 100 24F 34 8 100 36M 55 8 100 12F 51 4 100 24F 33 4 100 12M 27 8 100 48
Penarrocha-Oltra et al 201238 4
M 27 9 100 24M 55 8 100 12F 51 4 100 48F 44 2 100 24
Agustín-Panadero et al 201530 1 F 19 8 87.5 18Letelier et al 201615 1 F 31 11 100 6 (6), <12 (5)*
Abbreviations: EB, epidermolysis bullosa; F, female; M, male; NA, not available* Numbers in parentheses represent implants
Pemphigus Vulgaris, Cicatricial Pemphigoid, Bullous Pemphigoid
In contrast to OLP and EB, literature data on dental implants in patients with other mucocutaneous disorders are scarce. Literature review yielded only one case report of a female patient with pemphigus vulgaris, medicated with systemic corticosteroids and azathioprine, who had received two implants and has been successfully followed up for 32 months40. No case regarding dental implants in patients with cicatricial or bullous pemphigoid has been found in the literature.
Sjögren’s SyndromeImplant rehabilitation in a SS patient was initially
reported62 in 1993 and since then more than 428 dental implants have been placed in 115 SS subjects (105 females, 5 males, 5 gender not specified), documented by 10 case-reports11,13,14,21,41-46, 3 retrospective studies12,48,49 and 1 observational cohort study47. In one study, information on the number of implants inserted was not available42. Forty seven (40.9%) patients were diagnosed with primary SS12,13,21,41,45,46, one of whom also suffered from OLP21. Dental implants were also placed in thirty

Balk J Dent Med, Vol 21, 2017 Dental Implantation and Oral Mucosal Diseases 87
in 12 studies involving 81 SS subjects; in particular, fixed prostheses were selected in 6 studies14,41,43-46, removable overdentures in 1 study21 and both prosthodontic restoration types were used in 5 studies11-13,48,49. Of the 407 dental implants with available survival rates, 22 failed during a follow-up period ranging from 1 to 13 years, corresponding to a success rate of 94.6 % (Table 3).
three patients (28.7%) with SS associated with other autoimmune diseases (20 with rheumatoid arthritis-RA11,43,45,48,49, 2 with SLE14,44, 1 with scleroderma13, 1 with RA and scleroderma48, 9 unspecified12). In 35 (30.4%) An SS case, information about concomitant connective tissue diseases was not available11,42,47. Data regarding the prosthodontic rehabilitation was available
Table 3. Demographics of SS patients, number of implants, implants success rate and duration of follow-up
Reference Patients Gender Age (years) Implants Success rate (%) Follow-up (months)
Payne et al 199745 3F 38 12 75 96F 38 6 100 12F 40 8 100 12
Isidor et al 199911 8
F 53-70 6 50 48F NA 5 60 48F NA 10 100 48F NA 6 100 48F NA 4 100 48F NA 7 57.1 48F NA 6 100 48F NA 8 75 24
Esposito et al 200321 1 F 72 2 100 21Binon et al 200541 1 M 76 6 100 156
Oczakir et al 200513 2F 63 4 100 24F 64 8 100 60
Weinlander et al 201049 4
NA NA 6 NA 91NA NA 3 NA 46NA NA 4 NA 48NA NA 8 NA 42
Spinato et al 201046 1 F 62 6 100 12Ergun et al 201044 1 NA NA 6 100 24
Krennmair et al 201048 8
F 68 6 100 96F 48 3 100 48F 42 4 100 50F 72 8 100 44F 41 3 100 49F 52 4 100 52F 55 4 100 34F 41 7 100 42
de Mendonça Invernici et al 201443 1 F 58 3 100 72 (2), NA (1)*Korfage et al 201512 50 46F, 4M mean: 67 144 97 mean: 46Chochlidakis et al 201614 1 F 71 6 100 14Albrecht et al 201647 32 32F mean: 64.5 105 99 mean: 59
Chatzistavrianou and Shahdad 201642 2F NA NA 100 18F NA NA 100 24
Abbreviations: SS, Sjögren’s syndrome; F, female; M, male; NA, not available* Numbers in parentheses represent implants
Systemic Lupus ErythematosusLimited literature data exist regarding dental
implants in SLE patients. Ergun et al.44 reported the successful placement of six dental implants in a patient with dry mouth, diagnosed with SLE and SS, who was followed for 2 years. Moreover, one OLP patient treated with dental implants had a positive history for SLE and ultimately developed a mandibular SCC29.
Systemic SclerosisEleven studies (9 case reports13,50-57 and 2 retrospective
studies48,49) reported rehabilitation of 11 systemic scleroderma patients (6 females, 1 male, 4 with unknown gender) with more than 61 dental implants. Microstomia, difficulty in mastication, root resorptions and advanced periodontal disease were observed in most patients50-55,57. Five patients suffered from systemic sclerosis alone50-53,55,

88 Eleni-Marina Kalogirou, Alexandra Sklavounou Balk J Dent Med, Vol 21, 2017
overdentures13,53,56. Forty one out of 42 dental implants in 6 patients with known outcome13,48,49,52,56,57 were successfully followed up for a period of 2 to 5 years (success rate= 97.6%, Table 4).
one was diagnosed with concomitant SS13, one with SS and RA48, whereas in 4 cases there was no information13,48,49,56. Eight scleroderma patients were rehabilitated with a fixed implant-supported prosthesis48-52,54,55,57 and three with
Table 4. Demographics of systemic sclerosis patients, number of implants, implants success rate and duration of follow-up
Reference Patients Gender Age (years) Implants Success rate (%)
Follow-up (months)
Jensen & Sindet-Pedersen 199052 1 M 41 9 88.9 24Langer et al 199253 1 F 54 2 NA NARaviv et al 199656 1 NA 65 3 100 24Patel et al 199855 1 F 54 4 NA NAHaas 200251 1 F 49 7 NA NAOczakir et al 200513 1 F 64 8 100 60Krennmair et al 201048 1 F 55 4 100 34Weinlander et al 201049 1 NA NA 6 100 46Zigdon et al 201157 1 NA 45 12 100 36Nam et al 201254 1 NA NA NA NA NABaptist 201650 1 F 61 6 NA NA
Abbreviations: F, female; M, male; NA, not available
Leukoplakia/Oral SCCThe review of the pertinent literature revealed 16 patients
with clinically diagnosed leukoplakia who had developed SCC in the vicinity of dental implants (9 females, 7 males, female to male ratio= 1.3:1; age range= 42-88 years, mean age= 69.4 years)27,58-61. In 14/16 patients implant rehabilitation was established with removable prostheses27,58,59, in one subject with a fixed prosthesis61, while in one case information regarding prosthodontic restoration was missing60. Twelve out
of the 16 subjects (75%) had a positive history of oral cancer (Table 5). At the time of periimplant carcinoma diagnosis, 5/16 (31.3%) patients were current smokers, 3/16 (18.6%) past smokers, 4/16 (25%) non-smokers, whereas data about smoking habits were missing in 4 (25%) cases (Table 5). Periimplant cancer predominantly involved the mandible (15/16-93.6% cases), mainly as an exophytic mass or gingival hyperplasia mimicking periimplantitis, and less often as an ulcer (Table 5).
Table 5. Demographics, smoking habits and positive oral SCC history in patients with leukoplakia who developed SCC after implant placement, number of implants, interval between implants insertion and SCC diagnosis, SCC site and clinical picture
Reference Patients Gender Age (years) Implants
Interval between implant insertion and
SCC diagnosis
SCC clinical picture
SCC site
Smoking habits
History of oral SCC
Block and Scheufler 200158 1 M 72 8 5 peri-
implantitis man past yes
Shaw et al 200461 1 F 69 3 60 (1st SCC), 84 (2nd SCC)
ex, peri-implantitis man NA yes
Gulati et al 200959 1 F 72 5 96 peri-implantitis man past yes
Moergel et al 201327 12
F 63 NA 42 ex man no yesF 70 NA 48 ex man yes yesM 72 NA 43 ex man no yesM 57 NA 120 ex man yes yesM 72 NA 43 ex man NA noM 88 NA 115 ulcer man no noF 42 NA 42 ulcer man NA yesF 59 NA 29 ulcer man NA yesM 73 NA 97 ex max past yesM 77 NA 43 ex man yes noF 68 NA 110 ex man yes yesF 80 NA 51 ex man yes no
Kaplan et al 201660 1 F 77 NA NA ex man no yesAbbreviations: SCC, squamous cell carcinoma; F, female; M, male; NA, not available; ex, exophytic mass; man, mandible; max, maxilla

Balk J Dent Med, Vol 21, 2017 Dental Implantation and Oral Mucosal Diseases 89
implant restoration in SS subjects has shown favorable results. According to a retrospective study evaluating the implant outcome in SS patients and healthy controls, the survival rates of dental implants, the incidence of periimplant mucositis, periimplantitis and several periimplant clinical indices (bleeding index, plaque index etc.), were comparable between the two groups12. A subsequent observational cohort study provided similar results47. According to the reviewed literature, in the present study no significant differences in the implant survival rates between patients with primary or secondary SS associated with other autoimmune disorders, could be detected, which is in accordance with previous reports12.
Data on dental implants in patients with other autoimmune diseases, including pemphigus vulgaris, SLE or pemphigoid, as well as in patients with leukoplakia without malignant transformation are scarce or missing29,40,44. In contrast, implants have been evaluated in patients with rare disorders involving oral mucosa, such as EB and systemic sclerosis10. The severe microstomia, which is a common complication of both aforementioned diseases, and the tendency for blister formation after minor trauma seen in EB, cause significant difficulties in the use of conventional prostheses and, therefore, stress the need of a therapeutic alternative.
Despite the small number of patients treated, literature favors dental implantation in EB subjects15,30-39. Precautionary measures during implant surgery in EB patients include lubrication of lips and intraoral tissues with petroleum jelly and close contact of the aspirator with the bone rather than the mucosa. Local anesthesia is preferable versus general to avoid intubation-induced ulcers and should be performed slowly and deeply into the oral soft tissues to reduce the risk of blistering30,31,35-37,39. Bone grafting simultaneously to implant placement is effective in case of severe jaw atrophy31,38 and fixed prostheses are preferred compared to overdentures35 in order to avoid irritation of the fragile oral mucosa during mastication37.
Dental implants have also been considered a viable therapeutic solution in patients with systemic sclerosis, who have difficulty to handle and tolerate the removable dentures, because of limited mouth opening and finger deformities52,53,55. Implant-supported prostheses contribute decisively to the improvement of function, aesthetics and sociability of these patients50. In particular, implant placement in the anterior maxillary and mandibular portion between the canines is indicated to ensure stability of the prosthetic restoration and the improvement of facial aesthetics67. However, due to the scarce literature on dental implantation in scleroderma subjects, and the lack of detailed information on the observational period and the success rates13,48-57, further studies are warranted to propose specific treatment recommendations50.
Discussion
The present study summarizes the current evidence regarding dental implantation in patients with oral mucosal diseases. It was interesting to note that the number of studies available on this topic is constantly increasing which can be possibly explained by the functional, esthetic, and psychological benefits that these patients experience, which urge investigators to explore the implant treatment prospects in this group of individuals.
OLP and SS represent the two disease entities that have been more extensively investigated so far10,14,63, although concerns have been raised in the past about the long-term success of dental implantation in those patients. It has been speculated that the health of the periimplant tissues in OLP patients may be compromised by the impaired attachment of the oral epithelium to the titanium surface, leading to a defective mucosal block to microorganisms64. Moreover, it has been suggested that upregulated pro-inflammatory cytokines induced by oral epithelial cells in OLP subjects stimulate resorption of the periimplant alveolar bone65,66. In contrast, the current literature seems to encourage dental implantation in OLP patients. According to three studies which compared the outcome of dental implants between OLP subjects and healthy controls18,23,24, no difference was detected between the two groups in terms of implant stability and development of periimplant mucositis or periimplantitis. These findings suggest that the disease severity or the intraoral site of involvement do not seem to affect the survival of dental implants18,23,24. However, detailed description of the clinical forms of the disease and information on the site affected is missing in several studies. Furthermore the number of cases with desquamative gingivitis23,24 is quite small or information on implant placement adjacent to OLP lesions18,24 is scarce and thus a protocol on clinical management of these cases cannot be established. Dental implants should not be inserted during the acute phase of the disease17,23 and caution should be exercised in patients with parafunctional habits, due to an increased risk for failure20. Treatment with topical (e.g. clobetasol propionate mouthwashes or ointment, dexamethasone, triamcinolone acetonide) or systemic corticosteroids (e.g. oral prednisone) should precede the placement of implants in symptomatic OLP cases and medication should be re-implemented in case of exacerbations during the follow-up period17,18,21,23. Long term systemic steroid therapy, although rare, may lead to immunosuppression and subsequently interfere with the mucosal healing capacity18.
The long-term survival of dental implants in SS patients has been previously challenged by the disturbed immune response caused by the disease itself and the chronic immunosuppressive therapy4. However, to date,

90 Eleni-Marina Kalogirou, Alexandra Sklavounou Balk J Dent Med, Vol 21, 2017
5. Donos N, Calciolari E. Dental implants in patients affected by systemic diseases. Br Dent J, 2014;217:425-430.
6. Hwang D, Wang HL. Medical contraindications to implant therapy: part I: absolute contraindications. Implant Dent, 2006;15:353-360.
7. Gomez-de Diego R, Mang-de la Rosa Mdel R, Romero-Perez MJ, Cutando-Soriano A, Lopez-Valverde-Centeno A. Indications and contraindications of dental implants in medically compromised patients: update. Med Oral Patol Oral Cir Bucal, 2014;19:e483-489.
8. Neves J, de Araujo Nobre M, Oliveira P, Martins Dos Santos J, Malo P. Risk Factors for Implant Failure and Peri-Implant Pathology in Systemic Compromised Patients. J Prosthodont, 2016; doi: 10.1111/jopr.12508.
9. Guobis Z, Pacauskiene I, Astramskaite I. General Diseases Influence on Peri-Implantitis Development: a Systematic Review. J Oral Maxillofac Res, 2016;7:1-16.
10. Reichart PA, Schmidt-Westhausen AM, Khongkhunthian P, Strietzel FP. Dental implants in patients with oral mucosal diseases - a systematic review. J Oral Rehabil, 2016;43:388-399.
11. Isidor F, Brondum K, Hansen HJ, Jensen J, Sindet-Pedersen S. Outcome of treatment with implant-retained dental prostheses in patients with Sjogren syndrome. Int J Oral Maxillofac Implants, 1999;14:736-743.
12. Korfage A, Raghoebar GM, Arends S, Meiners PM, Visser A, Kroese GMF et al. Dental Implants in Patients with Sjogren’s Syndrome. Clin Implant Dent Relat Res. 2016;18:937-945.
13. Oczakir C, Balmer S, Mericske-Stern R. Implant-prosthodontic treatment for special care patients: a case series study. Int J Prosthodont, 2005;18:383-389.
14. Chochlidakis K, Ercoli C, Elad S. Challenges in implant-supported dental treatment in patients with Sjogren’s syndrome: A case report and literature review. Quintessence Int, 2016;47:515-524.
15. Letelier MG, Jara CC, Penarrocha-Oltra S, Gomar-Vercher S, Diago MP. Fixed Implant-Supported Full-Arch Prosthesis in Epidermolysis Bullosa With Severe Symptoms. J Oral Implantol, 2016;42:498-505.
16. Leung WK, Chu CH, Mok MY, Yeung KW, Ng SK. Periodontal status of adults with systemic sclerosis: case-control study. J Periodontol, 2011;82:1140-1145.
17. Aboushelib MN, Elsafi MH. Clinical Management Protocol for Dental Implants Inserted in Patients with Active Lichen Planus. J Prosthodont, 2017;26:29-33.
18. Czerninski R, Eliezer M, Wilensky A, Soskolne A. Oral lichen planus and dental implants--a retrospective study. Clin Implant Dent Relat Res, 2013;15:234-242.
19. Czerninski R, Kaplan I, Almoznino G, Maly A, Regev E. Oral squamous cell carcinoma around dental implants. Quintessence Int, 2006;37:707-711.
20. Esposito M, Thomsen P, Ericson LE, Sennerby L, Lekholm U. Histopathologic observations on late oral implant failures. Clin Implant Dent Relat Res, 2000;2:18-32.
21. Esposito SJ, Camisa C, Morgan M. Implant retained overdentures for two patients with severe lichen planus: a clinical report. J Prosthet Dent, 2003;89:6-10.
22. Gallego L, Junquera L, Baladron J, Villarreal P. Oral squamous cell carcinoma associated with symphyseal dental implants: an unusual case report. J Am Dent Assoc, 2008;139:1061-1065.
Patients with oral potential malignant disorders, such as leukoplakia and OLP, are at risk for cancer development. Prior to case selection for implant therapy, factors, e.g. tobacco or alcohol consumption, should be modified68. Short-interval follow-up examinations are crucial after implant rehabilitation to early detect possible malignant transformation68,69. Implant-supported prostheses should be regularly removed in order to clinically evaluate the periimplant soft tissues and, thus, fixed prostheses should be selected with caution, especially in patients with a positive history of cancer and risk for recurrence27,61. A carcinoma adjacent to dental implants may manifest as an exophytic mass mimicking an inflammatory reactive lesion of the gingivae or periimplantitis27,58, and efforts to manage through periodontal treatment may cause delay in diagnosis59. Thus, tumors and ulcers arising in the proximity of dental implants, resistant to conventional therapeutic measurements, should be biopsied and submitted to histopathological examination27,59,69.
Conclusion
In conclusion, based on the reviewed literature, dental implants represent an acceptable and reliable treatment option with a high success rate in patients with chronic mucocutaneous diseases and autoimmune diseases with oral manifestations. However, further well-designed prospective studies, with long meticulous follow-up, are required to define treatment guidelines and recommendations and predict with accuracy the implant outcome in this group of patients.
Note: The results of this paper were presented as a part of an invited lecture at the 22nd BaSS Congress.
References
1. Candel-Marti ME, Ata-Ali J, Penarrocha-Oltra D, Penarrocha-Diago M, Bagan JV. Dental implants in patients with oral mucosal alterations: An update. Med Oral Patol Oral Cir Bucal, 2011;16:787-793.
2. Alsaadi G, Quirynen M, Komarek A, van Steenberghe D. Impact of local and systemic factors on the incidence of late oral implant loss. Clin Oral Implants Res, 2008;19:670-676.
3. Meijer HJ, Raghoebar GM, Batenburg RH, Vissink A. Mandibular overdentures supported by two Branemark, IMZ or ITI implants: a ten-year prospective randomized study. J Clin Periodontol, 2009;36:799-806.
4. Diz P, Scully C, Sanz M. Dental implants in the medically compromised patient. J Dent, 2013;41:195-206.
Balk J Dent Med, Vol 21, 2017 Dental Implantation and Oral Mucosal Diseases 91
diagnosed with recessive dystrophic epidermolysis bullosa. J Oral Maxillofac Surg, 2012;70:51-57.
39. Penarrocha-Oltra D, Penarrocha-Diago M, Balaguer-Martinez J, Ata-Ali J, Penarrocha-Diago M. Full-arch fixed prosthesis supported by four implants in patients with recessive dystrophic epidermolysis bullosa. Oral Surg Oral Med Oral Pathol Oral Radiol Endod, 2011;112:4-10.
40. Altin N, Ergun S, Katz J, Sancakli E, Koray M, Tanyeri H. Implant-supported oral rehabilitation of a patient with pemphigus vulgaris: a clinical report. J Prosthodont, 2013;22:581-586.
41. Binon PP. Thirteen-year follow-up of a mandibular implant-supported fixed complete denture in a patient with Sjogren’s syndrome: a clinical report. J Prosthet Dent, 2005;94:409-413.
42. Chatzistavrianou D, Shahdad S. Implant Treatment in Patients with Sjogren’s Syndrome: A Review of the Literature and Two Clinical Case Reports. Eur J Prosthodont Restor Dent, 2016;24:40-46.
43. de Mendonca Invernici M, Finger Stadler A, Vale Nicolau G, Naval Machado MA, Soares de Lima AA, Compagnoni Martins M. Management of Sjogren’s Syndrome Patient: A Case Report of Prosthetic Rehabilitation with 6-Year Follow-Up. Case Rep Dent, 2014;2014:1-5.
44. Ergun S, Katz J, Cifter ED, Koray M, Esen BA, Tanyeri H. Implant-supported oral rehabilitation of a patient with systemic lupus erythematosus: case report and review of the literature. Quintessence Int, 2010;41:863-867.
45. Payne AG, Lownie JF, Van Der Linden WJ. Implant-supported prostheses in patients with Sjogren’s syndrome: a clinical report on three patients. Int J Oral Maxillofac Implants, 1997;12:679-685.
46. Spinato S, Soardi CM, Zane AM. A mandibular implant-supported fixed complete dental prosthesis in a patient with Sjogren syndrome: case report. Implant Dent, 2010;19:178-183.
47. Albrecht K, Callhoff J, Westhoff G, Dietrich T, Dorner T, Zink A. The Prevalence of Dental Implants and Related Factors in Patients with Sjogren Syndrome: Results from a Cohort Study. J Rheumatol, 2016;43:1380-1385.
48. Krennmair G, Seemann R, Piehslinger E. Dental implants in patients with rheumatoid arthritis: clinical outcome and peri-implant findings. J Clin Periodontol, 2010;37:928-936.
49. Weinlander M, Krennmair G, Piehslinger E. Implant prosthodontic rehabilitation of patients with rheumatic disorders: a case series report. Int J Prosthodont, 2010;23:22-28.
50. Baptist BA. Fixed Implant Supported Rehabilitation of Partially Edentulous Posterior Maxilla in a Patient With Systemic Scleroderma: A Case Report. Implant Dent, 2016;25:155-159.
51. Haas SE. Implant-supported, long-span fixed partial denture for a scleroderma patient: a clinical report. J Prosthet Dent, 2002;87:136-139.
52. Jensen J, Sindet-Pedersen S. Osseointegrated implants for prosthetic reconstruction in a patient with scleroderma: report of a case. J Oral Maxillofac Surg, 1990;48:739-741.
53. Langer Y, Cardash HS, Tal H. Use of dental implants in the treatment of patients with scleroderma: a clinical report. J Prosthet Dent, 1992;68:873-875.
54. Nam J, Janakievski J, Raigrodski AJ. Complete transition from failing restorations to implant-supported fixed prostheses in a patient with scleroderma. Compend Contin Educ Dent, 2012;33:746-756.
23. Hernandez G, Lopez-Pintor RM, Arriba L, Torres J, de Vicente JC. Implant treatment in patients with oral lichen planus: a prospective-controlled study. Clin Oral Implants Res, 2012;23:726-732.
24. Lopez-Jornet P, Camacho-Alonso F, Sanchez-Siles M. Dental implants in patients with oral lichen planus: a cross-sectional study. Clin Implant Dent Relat Res, 2014;16:107-115.
25. Reichart PA. Oral lichen planus and dental implants. Report of 3 cases. Int J Oral Maxillofac Surg, 2006;35:237-240.
26. Marini E, Spink MJ, Messina AM. Peri-implant primary squamous cell carcinoma: a case report with 5 years’ follow-up. J Oral Maxillofac Surg, 2013;71:322-326.
27. Moergel M, Karbach J, Kunkel M, Wagner W. Oral squamous cell carcinoma in the vicinity of dental implants. Clin Oral Investig, 2014;18:277-284.
28. Silva RH, Paleari AG, Brito Cde A, Rocha JF, Massucato EM, Quishida CC. A clinical report of an oral lichen planus associated to epidermoid carcinoma in contact with metallic restorations. J Contemp Dent Pract, 2014;15:651-653.
29. Raiser V, Abu-El Naaj I, Shlomi B, Fliss DM, Kaplan I. Primary Oral Malignancy Imitating Peri-Implantitis. J Oral Maxillofac Surg, 2016;74:1383-1390.
30. Agustin-Panadero R, Gomar-Vercher S, Penarrocha-Oltra D, Guzman-Letelier M, Penarrocha-Diago M. Fixed full-arch implant-supported prostheses in a patient with epidermolysis bullosa: a clinical case history report. Int J Prosthodont, 2015;28:33-36.
31. Larrazabal-Moron C, Boronat-Lopez A, Penarrocha-Diago M, Penarrocha-Diago M. Oral rehabilitation with bone graft and simultaneous dental implants in a patient with epidermolysis bullosa: a clinical case report. J Oral Maxillofac Surg, 2009;67:1499-1502.
32. Lee H, Al Mardini M, Ercoli C, Smith MN. Oral rehabilitation of a completely edentulous epidermolysis bullosa patient with an implant-supported prosthesis: a clinical report. J Prosthet Dent, 2007;97:65-69.
33. Muller F, Bergendal B, Wahlmann U, Wagner W. Implant-supported fixed dental prostheses in an edentulous patient with dystrophic epidermolysis bullosa. Int J Prosthodont, 2010;23:42-48.
34. Oliveira MA, Ortega KL, Martins FM, Maluf PS, Magalhaes MG. Recessive dystrophic epidermolysis bullosa--oral rehabilitation using stereolithography and immediate endosseous implants. Spec Care Dentist, 2010;30:23-26.
35. Penarrocha M, Larrazabal C, Balaguer J, Serrano C, Silvestre J, Bagan JV. Restoration with implants in patients with recessive dystrophic epidermolysis bullosa and patient satisfaction with the implant-supported superstructure. Int J Oral Maxillofac Implants, 2007;22:651-655.
36. Penarrocha M, Rambla J, Balaguer J, Serrano C, Silvestre J, Bagan JV. Complete fixed prostheses over implants in patients with oral epidermolysis bullosa. J Oral Maxillofac Surg, 2007;65:103-106.
37. Penarrocha-Diago M, Serrano C, Sanchis JM, Silvestre FJ, Bagan JV. Placement of endosseous implants in patients with oral epidermolysis bullosa. Oral Surg Oral Med Oral Pathol Oral Radiol Endod, 2000;90:587-590.
38. Penarrocha-Oltra D, Aloy-Prosper A, Ata-Ali J, Penarrocha-Diago M, Penarrocha-Diago M. Implants placed simultaneously with particulated bone graft in patients

92 Eleni-Marina Kalogirou, Alexandra Sklavounou Balk J Dent Med, Vol 21, 2017
65. Lodi G, Scully C, Carrozzo M, Griffiths M, Sugerman PB, Thongprasom K. Current controversies in oral lichen planus: report of an international consensus meeting. Part 1. Viral infections and etiopathogenesis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod, 2005;100:40-51.
66. Taubman MA, Kawai T. Involvement of T-lymphocytes in periodontal disease and in direct and indirect induction of bone resorption. Crit Rev Oral Biol Med, 2001;12:125-135.
67. Alantar A, Cabane J, Hachulla E, Princ G, Ginisty D, Hassin M al. Recommendations for the care of oral involvement in patients with systemic sclerosis. Arthritis Care Res (Hoboken), 2011;63:1126-1133.
68. Salgado-Peralvo AO, Arriba-Fuente L, Mateos-Moreno MV, Salgado-Garcia A. Is there an association between dental implants and squamous cell carcinoma? Br Dent J, 2016;221:645-649.
69. Jane-Salas E, Lopez-Lopez J, Rosello-Llabres X, Rodriguez-Argueta OF, Chimenos-Kustner E. Relationship between oral cancer and implants: clinical cases and systematic literature review. Med Oral Patol Oral Cir Bucal, 2012;17:23-28.
Received on May 1, 2017.Revised on May 30, 2017.Accepted on May 31, 2017.
Correspondence:
Alexandra Sklavounou Department of Oral Medicine and Pathology Faculty of Dentistry National and Kapodistrian University of Athens, Greece e-mail: [email protected]
55. Patel K, Welfare R, Coonar HS. The provision of dental implants and a fixed prosthesis in the treatment of a patient with scleroderma: a clinical report. J Prosthet Dent, 1998;79:611-612.
56. Raviv E, Harel-Raviv M, Shatz P, Gornitsky M. Implant-supported overdenture rehabilitation and progressive systemic sclerosis. Int J Prosthodont, 1996;9:440-444.
57. Zigdon H, Gutmacher Z, Teich S, Levin L. Full-mouth rehabilitation using dental implants in a patient with scleroderma. Quintessence Int, 2011;42:781-785.
58. Block MS, Scheufler E. Squamous cell carcinoma appearing as peri-implant bone loss: a case report. J Oral Maxillofac Surg, 2001;59:1349-1352.
59. Gulati A, Puthussery FJ, Downie IP, Flood TR. Squamous cell carcinoma presenting as peri-implantitis: a case report. Ann R Coll Surg Engl, 2009;91:W8-10.
60. Kaplan I, Zeevi I, Tal H, Rosenfeld E, Chaushu G. Clinicopathologic evaluation of malignancy adjacent to dental implants. Oral Surg Oral Med Oral Pathol Oral Radiol, 2017;123:103-112.
61. Shaw R, Sutton D, Brown J, Cawood J. Further malignancy in field change adjacent to osseointegrated implants. Int J Oral Maxillofac Surg, 2004;33:353-355.
62. Binon PP, Fowler CN. Implant-supported fixed prosthesis treatment of a patient with Sjogren’s syndrome: a clinical report. Int J Oral Maxillofac Implants, 1993;8:54-58.
63. Pons-Fuster A, Jornet PL. Dental implants in patients with oral lichen planus: a narrative review. Quintessence Int, 2014;45:599-603.
64. Lekholm U. The surgical site. In: Lindhe J, editor. Clinical Periodontology and Implant Dentistry. 3rd ed. Copenhagen: Munksgaard; 1997.

SUMMARYBackground: The aim of this study was to assess the oral health-
related quality of life in adult patients who visit the Dental Clinic of the Faculty of Stomatology, Pancevo, using a Serbian version of 14-items Oral Health Impact Profile (OHIP14) Questionnaire. Material and Methods: A total of 89 respondents (42 women and 47 men, mean age 52.83 ± 13.74 years) filled in the questionnaire themselves. Three calibrated dentists recorded the oral health status of the respondents (number of healthy, decayed, filled and missing teeth), the type and time of wearing prosthodontic replacements, if they existed, and assessed the need for prosthodontic treatment. The total OHIP-14 score was calculated by adding scores for all fourteen items; OHIP-14 subscale scores were calculated by adding the scores for the two items in each of the seven subscales. Results: Mean total OHIP score was 10.25 ± 8.89. Patients with less than eight extracted teeth, wearers of fixed prosthodontic appliances and patients without replacements who did not need prosthodontic treatment reported better oral health-related quality of life. The most severe oral impacts assessed by the subscale OHIP14 scores were recorded in psychological discomfort (2.44 ± 2.18), physical pain (1.87 ± 1.73) and psychological disability subscale (1.83 ± 1.88). Women more often than men were dissatisfied with their diet and had been irritable in contact with other people. Conclusion: Further studies using the OHIP14 questionnaire in a larger sample will permit identification of key factors related to poor oral health and planning of treatment protocols and preventive programs for the adult population in Serbia.Key words: Oral Health-Related Quality Of Life, OHIP14, Oral Health, Missing Teeth, Prosthodontics
Maja Lalić, Irena Melih, Ema Aleksić, Milica Gajić, Katarina Kalevski, Anika Ćuković
Faculty of Stomatology Pancevo University Business Academy Novi Sad, Serbia
ORIGINAL PAPER (OP)Balk J Dent Med, 93-99
BALKAN JOURNAL OF DENTAL MEDICINE ISSN 2335-0245
Oral Health Related Quality of Life and Dental Status of Adult Patients
STOMATOLOGICA
L S
OC
IET
Y
Introduction
Oral diseases are significant public health burden worldwide but often not given adequate attention in many low and middle income countries. Oral diseases affect people’s everyday lives subtle but pervasive, disrupting eating, sleep, work and social roles. Oral health is essential to overall health, well-being and quality of life. Health-related quality of life (HRQoL) is multidimensional concept which includes patients’ physical, psychological and social well-being. A major factor that can strongly affect the overall HRQoL is the oral health of the individual1, 2.
Although a relatively new concept, oral health-related quality of life (OHRQoL) receives rapidly growing attention. The concept of OHRQoL is of special interest for oral health promotion and access to oral health care in the community3. At the clinical research level, this concept is used to determine the patient’s treatment needs, the specific type of treatment and to evaluate treatment outcome.
Since the quality of life is found to be an important outcome of dental care, a need for developing a range of instruments to determine oral health-related quality of life has arisen. OHRQoL can be measured using twenty indexes developed in the original English version, with numerous translations into other world languages4. The
10.1515/bjdm-2017-0014

94 Maja Lalić et al. Balk J Dent Med, Vol 21, 2017
To assess the impact of oral health status on health-related quality of life, we used the Serbian version of the OHIP-14 index7. Additionally, data about age, educational and occupational background were recorded.
The respondents filled in a questionnaire themselves. Three previously trained and calibrated dentists were at their disposal to provide explanations regarding the questions, without suggesting the answers. These dentists conducted the clinical examination in a dental surgery, under artificial light, using a dental mirror and probe. They recorded the dental status of each patient (numbers of healthy, decayed, extracted or filled teeth), as well as the presence, type and approximate time of wearing prosthetic replacements. It was noted whether the patient had an adequate prosthetic appliance, and whether he or she needed prosthetic treatment. How long patients without any replacements but who needed prosthodontic treatment had been without their teeth was also recorded.
OHIP-14 scores were calculated in two ways12: first, the total OHIP-14 score was calculated by summing responses over all fourteen items, with possible scores ranging from 0 to 56; secondly, OHIP-14 subscale scores were calculated for each of seven dimensions indicated in Table 5 by adding scores for the two items in each subscale.
Statistics
Statistical analyses were performed using SPSS for Windows (release 17.0, SPSS, Chicago, IL). Mean differences in OHIP-14 scores according to age, sex, educational level, occupation and the presence of different prosthetic appliances were assessed by ANOVA. Differences in dental status expressed by the number of healthy, decayed, extracted or filled teeth between the sexes were evaluated using the t-test. Statistical significance was based on probability values of less than 0.05.
Results
This study included 42 women and 47 men. The mean age of the patients was 52,83 ± 13,74 years (range 19 to 72 years, median 56). Mean total OHIP-14 score (Table 1) in the whole sample was 10.25 ± 8.89 (95% confidence interval – 8.38 to 12.12). Total OHIP score was 9.06 ± 8.38 for men and 11.57 ± 9.35 for women (p>0.05). Data pertaining to age, educational level and occupation were missing for ten (11.24%), three (3.37%) and nine (10.11%) patients, respectively. This loss of data could be expected and tolerated when self-complete form of questionnaire is used. No significant differences in total OHIP score related to sex, age, education and employment status of the subjects were detected.
Oral Health Impact Profile (OHIP) measures peoples’ subjective perceptions of disability and discomfort caused by oral conditions5. The OHIP-49 contains 49 questions that refer to functional limitation, physical pain, psychological discomfort, physical disability, psychological disability, social disability, and handicap. The OHIP-14 was developed as a shorter version expressing good reliability, validity and precision6. For each question, the subjects are asked how frequently they had experienced the problem in the last month. Responses are rated using a Likert-type scale (0 = never, 1 = hardly ever, 2 = occasionally, 3 = fairly often, 4 = very often). Zero indicates the absence of any problems, while high scores point to severely impaired oral health5.
Studies in the field of oral health in Serbian population are relatively new and few. The Serbian version of the OHIP-14 index was introduced in the pilot study of Stancic et al.7, who found that 60% of elderly people felt that life was generally less satisfying as a result of impaired oral health. The other pilot study of OHRQoL, measured using the Oral Impacts on Daily Performances (OIDP) index, reported that impaired oral health dominantly affected eating, speaking, social and emotional well-being of Serbian elderly adults8.
One of the instruments developed for the assessment the oral health problems of older adults was the Geriatric Oral Health Assessment Index (GOHAI)9. The pilot study of oral health related quality of life in Serbian geriatric patients before and after prosthodontics rehabilitation showed that the Serbian preliminary version of the GOHAI questionnaire confirmed the consistency, stability, and validity of the questionnaire and revealed the causal relation between the quality of life and the characteristics of oral health of the patients with dentures10. Studies applying Serbian version of OHIP-14 and GOHAI questionnaire provided more in-depth analysis of patients’ condition and could be very useful for treatment planning and estimation of dental treatment outcome11.
The aim of our study was to apply the OHIP-14 questionnaire to determine the incidence and extent of oral impacts on quality of life related problems among patients who visited the Dental Clinic of the Faculty of Stomatology Pancevo for the first time, prior to any treatment, and to assess the relations between their dental status, treatment needs and OHRQoL.
Material and Methods
This study included a suitable sample of 89 urban adults who visited the Dental Clinic of the Faculty of Stomatology, Pancevo, during March - April 2015, seeking restorative or prosthodontic treatment. Patients with a medical history of chronic or systemic diseases and disabilities, and those with acute dental symptoms/pain were not included in the investigation. All patients signed an informed consent form. The study was approved by Ethical committee of Faculty of Stomatology Pancevo.

Balk J Dent Med, Vol 21, 2017 Quality of Life and Dental Status 95
Table 1. The sample characteristics and differences in total OHIP-14 scores according to gender, age, educational and working status
N χ͞ SD SE
95% Confidence interval for mean
Min MaxLower limit
Upper limit F p
Gender:
male 47 9.06 8.38 1.222 6.60 11.52 0 35
female 42 11.57 9.35 1.442 8.66 14.48 0 35
Total 89 10.25 8.89 .942 8.38 12.12 0 35 1.782 ns
Age (years):
30 to 45 17 10.76 7.45 1.806 6.94 14.59 0 21
46 to 65 50 10.96 10.04 1.419 8.11 13.81 0 35
over 65 12 8.42 7.63 2.204 3.57 13.27 1 23 0.375 ns
Education:
elementary 10 9.20 7.69 2.430 3.70 14.70 1 23
high school 48 10.27 9.43 1.361 7.53 13.01 0 35
university 28 10.46 8.80 1.664 7.05 13.88 0 33 0.074 ns
Employment status:
employed 27 10.11 10.01 1.927 6.15 14.07 0 35
unemployed 21 9.52 8.57 1.870 5.62 13.43 0 26
retired 32 9.81 8.98 1.587 6.58 13.05 0 35 0.024 nsχ͞ - mean OHIP score; SD – Standard deviation; SE – standard error; p – statistical significance; ns-not significant
The average number of healthy (untereated) teeth was 9.41 ± 6.63 in the whole sample, while the mean number of decayed teeth was 2.52 ± 3.22; 12.75 ± 8.39 had been extracted and 6.11 ± 4.15 filled (Table 2). No statistically significant differences in dental status between men and women were found.
Table 2. The mean number of healyhy, decayed, missing and filled teeth according to gender
Total (n = 89)
Men (n = 47)
Women (n = 42) p
Healthy teeth 9.41(±6.63) 8.57(±6.45) 10.37(±6.79) ns
Decayed teeth 2.52(±3.22) 2.35(±3.48) 2.71(±2.93) ns
Missing teeth 12.75(±8.39) 13.91(±8.90) 11.44(±7.68) ns
Filled teeth 6.11(±4.15) 6.37(±4.37) 5.83 (±3.92) ns
p – statistical significancens-not significant
The differences in total OHIP scores according to the number of missing teeth are given in Table 3. Patients with more than eight teeth missing had the highest total OHIP score (11.94 ± 9.29), while it was 9.47 ± 8.37 for those with up to four and 5.44 ± 6.21 for patients with five to eight missing teeth (F = 3.60, p = 0.03).
Among all subjects, 42 (47%) had no prosthetic appliances, 19 (21%) had fixed prosthetic appliances (crowns and bridges), 8 (9%) had a combination of fixed appliances and/or partial dentures, 15 (17%) had immediate partial dentures, while 5 patients (6%) wore complete dentures. We found that 34 out of 42 patients (81%) who had no prosthetic appliances needed prosthetic rehabilitation. The average period of time that they had been without teeth was 3.19 ± 2.55 years. Among 43 respondents who already had replacements 29 (67%) required new ones. On average, the replacements were 7.77 ± 5.51 years old.
The presence and type of prosthetic replacement affected the total OHIP score (Table 4). Patients with crowns and/or bridges had the lowest total OHIP score (5.00 ± 5.82), while the highest scores were recorded among wearers of immediate partial (17.14 ± 8.88) and complete dentures (16.00 ± 11.58), with a significant difference between the groups (F = 5.002; p = 0.001).

96 Maja Lalić et al. Balk J Dent Med, Vol 21, 2017
Table 3. Mean OHIP-14 score according to the number of missing teeth
Number ofmissing teeth N χ͞ SD SE
95% Confidence interval for mean
Min MaxLower limit Upper limit
0 - 4 19 9.47 8.37 1.92 5.44 13.51 0.00 26.00
5 - 8 16 5.44 6.21 1.55 2.13 8.74 0.00 21.00
> 8 54 11.94 9.29 1.26 9.41 14.48 0.00 35.00
F = 3,60; p = 0,03χ͞ - mean OHIP score; SD – Standard deviation; SE – standars error
Table 4. Total OHIP-14 score according to the type of prosthetic replacement
95% Confidence Interval for Mean
N χ͞ SD SE Lower limit Upper limit Min Max
Without replacements 42 9.32 8.45 1.320 6.65 11.99 0 35
Crowns/bridges 19 5.00 5.82 1.372 2.11 7.89 0 21
Fixed partial denture 8 10.43 8.66 3.272 2.42 18.44 1 22
Immediate partial denture 15 17.14 8.88 2.374 12.01 22.27 5 33
Complete denture 5 16.00 11.58 5.177 1.63 30.37 7 35
df = 4; F = 5,002; p = 0,001χ͞ - mean OHIP score; SD – Standard deviation; SE – standard error
Table 5. Mean subscales OHIP-14 scores and frequencies of “often” or “very often” responses
OHIP-14 item
Distribution of “often”
or “very often" answers (%)
Mean Subscale OHIP score
(±SD)Men Women p
Functional limitation 1 Trouble pronouncing any words2 Sense of taste has worsened 1.18% 0.71
(±1.02)0.74
(±1.13)0.67
(±0.90) ns
Physical pain 3 Had painful aching in your mouth4 Uncomfortable to eat any foods 12.91% 1.87
(±1.73)1.96
(±1.91)1.76
(±1.53) ns
Psychological discomfort
5 Been self conscious6 Felt tense 22.35% 2.44
(±2.18)2.21
(±2.00)2.69
(±2.36) ns
Physical disability 7 Diet has been unsatisfactory8 Had to interrupt meals 10.59% 1.52
(±1.83)1.10
(±1.52)1.95
(±2.06) 0.032
Psychological disability
9 Difficult to relax10 Been a bit embarrassed 9.41% 1.83
(±1.88)1.57
(±1.79)2.12
(±1.95) ns
Social disability 11 Been a bit irritable with other people12 Had difficulty doing your usual jobs 5.88% 1.01
(±1.51)0.68
(±1.12)1.38
(±1.79) 0.033
Handicap 13 Felt that life in general was less satisfying14 Been totally unable to function 2.35% 0.89
(±1.13)0.79
(±1.10)1.00
(±1.17) ns
SD – standard deviation; p – statistical significance; ns-not significant

Balk J Dent Med, Vol 21, 2017 Quality of Life and Dental Status 97
pronouncing words (n = 67) or ability to function (n = 66) and no changes of taste sense (n = 62).
Mean OHIP-14 scores calculated separately for each item (Table 6), were significantly higher in women than in men concerning unsatisfactory diet (item 7; 1.17 ± 1.46 vs 0.55 ± 1.02, p = 0.022) and being somewhat irritable with other people (item 11; 0.79 ± 1.02 vs 0.36 ± 0.82, p = 0.030).
The most severe oral impacts assessed by the subscale OHIP-14 scores were recorded in psychological discomfort (2.44 ± 2.18), physical pain (1.87 ± 1.73) and psychological disability (1.83 ± 1.88) subscale, while the least severe impacts (0.71 ± 1.02) were in the functional limitation subscale (Table 5). Oral pain frequently affected 3.37% of respondents, while 50.56% of the subjects reported occasional painful aching in the mouth. The majority of respondents reported no oral impacts on
Table 6. Distribution of OHIP items, ranging from 0 (never), 1 (hardly ever), 2 (occasionally), 3 (very often) to 4 (fairly often) and mean OHIP-14 scores
Question 0 1 2 3 4 Total OHIP score (SD)
Men OHIP score (SD)
WomenOHIP score (SD) p
1 67 16 5 1 0 0. 33 (0.64) 0.36 (0.70) 0.29 (0.55) ns
2 62 21 5 1 0 0. 38 (0.65) 0.38 (0.64) 0.38 (0.66) ns
3 41 39 6 3 0 0. 68 (0.75) 0.72 (0.85) 0.62 (0.62) ns
4 41 15 15 7 10 1. 22 (1.40) 1.26 (1.42) 1.14 (1.39) ns
5 30 12 22 16 9 1. 57 (1.38) 1.49 (1.30) 1.67 (1.48) ns
6 44 24 13 5 3 0. 87 (1.08) 0.72 (0.90) 1.02 (1.24) ns
7 57 6 15 5 6 0. 84 (1.28) 0.55 (1.02) 1.17 (1.46) 0.022
8 48 29 7 4 1 0. 66 (0.89) 0.55 (0.88) 0.79 (0.90) ns
9 49 23 12 3 2 0. 72 (0.98) 0.62 (0.90) 0.83 (1.06) ns
10 32 26 22 7 2 1. 11(1.06) 0.96 (1.02) 1.29 (1.09) ns
11 57 22 4 4 2 0. 56 (0.94) 0.36 (0.82) 0.79 (1.02) 0.030
12 59 23 4 3 0 0. 45 (0.74) 0.32 (0.56) 0.60 (0.89) ns
13 53 23 10 1 2 0. 61 (0.90) 0.51 (0.93) 0.71(0.86) ns
14 66 22 0 1 0 0. 28 (0.52) 0.28 (0.45) 0.29 (0.60) ns
p – statistical significance; ns-not significant
Discussion
The convenient, small sample of patients examined here, may be considered a limitation of this study. Most of these patients visited the Dental Clinic of the Faculty of Stomatology, Pancevo due to the possibility of receiving free dental care. This includes not only prosthetic rehabilitation, but also conservative, endodontic, periodontal and surgical treatment. In most dental clinics, both private and public, dental treatment is not fully covered by standard health insurance. Certainly, the part of the population that can afford adequate and prompt dental treatment and, therefore, probably with better oral health-related quality of life, was not in the majority in
our research, so these results cannot be generalized and applied to the entire adult population of Vojvodina. Due to these limitations, this study should be considered a prospective one.
We used the self-completion questionnaire format of the Serbian version of the OHIP-14 index. The method of administration did not significantly influenced total OHIP14 scores, although more severe impacts were reported in some studies that used the interview compared to the questionnaire format of this index13. The use of the OHIP14 in the questionnaire format may result in loss of data and omission of answers. In our study the proportion of respondents who answered all the questions regarding age and social status was 88.76%. Although Stancic et

98 Maja Lalić et al. Balk J Dent Med, Vol 21, 2017
to interrupt meals and that their diet was unsatisfactory, while 19.10% of them stated that problems with their mouth or dentures interfered eating of any food. Women, significantly more often than men, were dissatisfied with their diet due to oral health problems.
The type of replacement significantly affected oral health-related quality of life. The greatest oral impacts were recorded in patients with immediate partial or complete dentures. Many patients with immediate dentures often use these appliances for a longer period than functionally acceptable24, probably due to their financial inability to afford a more sophisticated solution. This could be the main reason for the high oral impacts on quality of life among these patients. Krunić et al. suggested that relining of complete dentures with silicone may improve the patient’s satisfaction with dentures25. Many reports suggested that technically advanced appliances, i.e. implant overdentures, provided better function and oral health-related quality of life compared with conventional dentures26, 27, 28.
Better scores for self-reported oral health in the group of patients with fixed appliances than in the group without any replacements, could be explained by the finding that 81% of those without prosthodontic replacements needed prosthetic rehabilitation.
The data collected in this study revealed the most common oral impacts in adult patients and could help dentists to plan individual treatment aimed to improvement of patient’s oral and general health. We used only clinical data to assess different oral impacts on quality of life, while Slovenian and Croatian authors used self-reported oral health scores, which correlated with the scores in the Croatian and Slovenian versions of the 14-item Oral Health Impact Profile (OHIP-CRO14 and OHIP-SVN14) questionnaires29, 30.
Conclusions
Future research should be directed towards the assessment of psychometric properties of the Serbian version of the OHIP14 Questionnaire by including both clinical and subjective, patient-reported variables in a larger sample, in order to assess the causal determinants of oral health in adult patients and include these findings in planning treatment protocols and preventive programs.
References
1. McGrath C, Bedi R. The importance of oral health to older people’s quality of life. Gerodontol, 1999;16:59-63.
al.7 suggested that item nr. 5 should be omitted in Serbian version of OHIP 14 questionnaire, participants of this study answered it without asking for clarification.
We found that psychological discomfort, physical pain, physical and psychological disability were the most common oral impacts, frequently affecting 9.41% to 22.35% of the respondents. Functional limitations and handicaps were the least severe oral impacts.
No significant differences in total OHIP scores according to the respondents’ age, sex, educational level and occupation were noted in our study, although others indicated a considerable impact of social determinants on self-perceived oral health-related quality of life14,
15. Consistent with the results of earlier studies16, 12, we found that women perceive that oral health affects quality of life to a greater extent compared to men. Respondents older than 65 years of age subjectively perceived oral health problems less frequently than the younger participants, although the differences in total OHIP scores between different age groups were not statistically significant. Slade and al.17 reported that negative subjective perception of oral health problems is more common early in adulthood than in old age. This pattern probably indicates that young people have high expectations regarding oral health, while elderly express greater resilience. The older respondents more often seek medical than dental care, and dental treatment was mostly needed due to pain.
Summarized, the oral characteristic of our sample was a great number of extracted teeth (12.75 ± 8.39), and a high percentage of patients without replacements who needed prosthodontic treatment (81%) or those with inadequate prosthodontic replacements (67%).
Tooth loss is one general indicator of oral health status of a population. The presence of twenty teeth is an oral health goal of the WHO18. As the major physical characteristic of oral health, the number of teeth had an impact both on ability to chew food and oral health-related quality of life in prosthodontic patients19. Consistent with this, we found that total OHIP score was significantly higher in subjects who had more than eight teeth missing. Interestingly, oral health quality of life in patients with up to four missing teeth was worse than in patients with five to eight teeth missing, because oral symptoms in patients with a few missing teeth involved acute dental pain rather than reduced chewing ability. Brennan et al. 20 reported that the number of functional teeth was positively associated with chewing ability. The ability to chew food properly was positively associated with oral health-related quality of life and general health, which might be related to food choice and greater enjoyment of meals. Compromised chewing ability may not only negatively affect nutritional intake and oral health-related quality of life21, but an inappropriate diet may also be deleterious general health22, 23. In our study, 10.59% of the subjects reported that they frequently had

Balk J Dent Med, Vol 21, 2017 Quality of Life and Dental Status 99
using abbreviated Oral Health Impact Profile questionnaires. J Oral Rehabil, 2008;35:224-228.
20. Brennan DS, Spencer AJ, Roberts-Thomson KF. Tooth loss, chewing ability and quality of life. Qual Life Res, 2008;17:227-235.
21. Inukai M, John MT, Igarashi Y, Baba K. Association between perceived chewing ability and oral health-related quality of life in partially dentate patients. Health Qual Life Outcomes, 2010;8:118.
22. Nowjack-Raymer RE, Sheiham A: Association of edentulism and diet and nutrition in US adults. J Dent Res, 2002;82:123-126.
23. Moynihan P, Bradbury J: Compromised dental function and nutrition. Nutrition, 2001;17:177-178.
24. Gasparić LB, Catović A, Komar D, Bergman V, Catić A. Epidemiological study on prosthodontic appliance deliveries within elderly cohorts in the Republic of Croatia, 2002-2006. Coll Antropol, 2009;33:461-465.
25. Krunić N, Kostić M, Petrović M, Igić M. Oralno zdravlje i kvalitet života bezubih pacijenata nakon podlaganja totalnih zubnih proteza. Vojnosanit Pregl, 2015;72:307-311.
26. Rashid F, Awad MA, Thomason JM, Piovano A, Spielberg GP, Scilingo E et al. The effectiveness of 2-implant overdentures - a pragmatic international multicentre study. J Oral Rehabil, 2011;38:176-184.
27. John MT, Slade GD, Szentpétery A, Setz JM. Oral health-related quality of life in patients treated with fixed, removable, and complete dentures 1 month and 6 to 12 months after treatment. Int J Prosthodont, 2004;17:503-511.
28. Harris D, Höfer S, O’Boyle CA, Sheridan S, Marley J, Benington IC et al. A comparison of implant-retained mandibular overdentures and conventional dentures on quality of life in edentulous patients: a randomized, prospective, within-subject controlled clinical trial. Clin Oral Implants Res, 2013;24:96-103.
29. Petricević N, Celebić A, Papić M, Rener-Sitar K. The Croatian version of the Oral Health Impact Profile Questionnaire. Coll Antropol, 2009;33:841-847.
30. Rener-Sitar K, Celebić A, Petricević N, Papić M, Sapundzhiev D, Kansky A, et al. The Slovenian version of the Oral Health Impact Profile Questionnaire (OHIP-SVN): translation and psychometric properties. Coll Antropol, 2009;33:1177-1183.
Received on February 1, 2017.Revised on March 20, 2017.Accepted on March 29, 2017.
Correspondence:
Maja Lalić Faculty of Stomatology Pancevo Žarka Zrenjanina 179, Pancevo Tel: 063/8444-287 e-mail: [email protected]
2. John MT, LeResche L, Koepsell TD, Hujoel P, Miglioretti DL, Micheelis W. Oral health-related quality of life in Germany. Eur J Oral Sci, 2003; 111:483-491.
3. Shamrany MA. Oral health-related quality of life: a broader perspective. East Mediterr Health J, 2006;12:894-901.
4. Hebling E, Pereira AC. Oral health-related quality of life: a critical appraisal of assessment tools used in elderly people. Gerodontol, 2007;24:151-161.
5. Slade GD, Spencer AJ: Development and evaluation of the oral health impact profile. Community Dent Health, 1994;11:3-11.
6. Slade GD. Derivation and validation of a short-form oral health impact profile Community Dent Oral Epidemiol, 1997;25:284-290.
7. Stancic I, Sojic LT, Jelenkovic A. Adaptation of Oral Health Impact Profile (OHIP-14) index for measuring impact of oral health on quality of life in elderly to Serbian language. Vojnosanit Pregl, 2009;66:511-515.
8. Stančić I, Kulić J, Tihaček-Šojić L, Stojanović Z. Applicability of a Serbian version of the “Oral Impacts on Daily Performance (OIDP)” index – assessment of oral health-related quality of life. Vojnosanit Pregl, 2012;69:175-180.
9. Atchison KA, Dolan TA. Development of the Geriatric Oral Health Assessment Index. J Dent Educ, 1990;54:680-687.
10. Popović Ž, Gajić I, Obradović-Đuričić K, Milošević D. Uvod u verifikaciju instrumenta GOHAI za merenje oralnozdravstvenog kvaliteta života osoba sa zubnim nadoknadama primenom preliminarne srpske verzije – pilot studija. Vojnosanit Pregl, 2015;72:1055-1062.
11. Jović Lj, Doder R. Primena OHIP 14 i GOHAI upitnika u cilju procene uticaja oralnog zdravlja na kvalitet života kod starije populacije. Medicina Danas, 2012;11:186-191.
12. Lawrence HP, Thomson WM, Broadbent JM, Poulton R. Oral health-related quality of life in a birth cohort of 32-year olds. Community Dent Oral Epidemiol, 2008;36:305-316.
13. Sousa PC, Mendes FM, Imparato JC, Ardenghi TM. Differences in responses to the Oral Health Impact Profile (OHIP14) used as a questionnaire or in an interview. Braz Oral Res, 2009;23:358-364.
14. Papaioannou W, Oulis CJ, Latsou D, Yfantopoulos J. Oral health-related quality of life of Greek adults: a cross-sectional study. Int J Dent, 2011;2011:360292.
15. Adams C, Slack-Smith LM, Larson A, O’Grady MJ. Edentulism and associated factors in people 60 years and over from urban, rural and remote Western Australia. Aust Dent J, 2003;48:10-14.
16. Mc Grath C, Bedi R, Dhawan N. Factors influencung older people’s self reported use of dental services in the UK. Gerodontol, 1999;16:97-102.
17. Slade GD, Sanders AE. The paradox of better subjective oral health in older age. J Dent Res, 2011;90:1279-1285.
18. Petersen PE, Yamamoto T. Improving the oral health of older people: the approach of the WHO Global Oral Health Programme. Community Dent Oral Epidemiol, 2005;33:81-92.
19. Baba K, Inukai M, John MT: Feasibility of oral health-related quality of life assessment in prosthodontic patients
SUMMARYBackground/Aim: The use of CBCT in dentistry has been increasing
popularity nowadays. CBCT images provide valuable information from anatomic structures and pathologies. Images obtained with CBCT allow for more appropriate treatment planning. The purpose of this study was to assess the calcifications which were found incidentally on CBCT images and to reveal the frequency and characteristics. Material and Methods: A total of 691 CBCT images which obtained from the patients were assessed. Demographic data and calcifications which were found out of primarily interest area were noted. The incidental findings were categorized and analyzed using descriptive statistics. Results: 945 calcifications were discovered on 318(46.02%) of the 691 patients’ images. 373(53.98%) scans showed no calcificated findings. The age range of patients was from 5 to 84 years. The most common calcification was tonsillolith (86.03%), followed by stylohyoid calcifications (6.24%), antrolith and subdermal calcifications (2.33%). Conclusion: Calcified lesions in head and neck region were commonly seen in CBCT images. Although the most of the calcifications are asymptomatic and require no treatment but correct identification of these findings will reduce unnecessary further diagnostic assessments and will provide more appropriate treatment plans. It will also provide the ability comprehensively evaluation of underlying diseases and practitioners will have life-saving information by early diagnosis.Key words: CBCT, İncidental Findings, Calcifications, Radiology
Ali Altındağ1, Hakan Avsever2, Oguz Borahan3, Mesut Akyol4, Kaan Orhan1
1 Ankara Universitty, Faculty of Dentistry Department of Dentomaxillofacial Radiology Ankara, Turkey 2 Gulhane Training&Reserach Hospital Health Sciences University, Dentistry Center Department of Dentomaxillofacial Radiology Ankara, Turkey 3 Marmara University Department of Dentomaxillofacial Radiology Istanbul, Turkey 4 Yildirim Beyazit University Department of Biostatistics, Ankara, Turkey
ORIGINAL PAPER (OP)Balk J Dent Med, 2017; 100-107
BALKAN JOURNAL OF DENTAL MEDICINE ISSN 2335-0245
Incidental Findings in Cone-Beam Computed Tomographic Images: Calcifications in Head and Neck Region
STOMATOLOGICA
L S
OC
IET
Y
Introductıon
Soft tissue calcifications in the maxillofacial area are uncommon, and generally correspond to radiographic findings in routine examinations such as panoramic radiographs. Calcification of soft tissue structures in the head and neck can present as physiologic or pathologic mineralization. Pathologic mineralization is more likely to occur in the articular cartilage, ligaments, and glandular and vascular tissues and is usually associated with chronic inflammation or scarring1. There are 3 types of pathologic calcifications: 1) dystrophic
calcification, which occurs in degenerating and dead tissues; 2) metastatic calcification, in which calcium and other salts are deposited in previously undamaged tissue as a result of excess salts in the circulating blood; and 3) calcinosis, which is calcification in or under the skin. However many of the structures in the head and neck region are in close proximity to one another which makes these calcifications localization and identification difficult2. Such as panoramic radiographs, conventionally radiographic images are inherently planar and 2-dimensional (2D), making localization and diagnosis problematic. Conventional 2D imaging is likely to result
10.1515/bjdm-2017-0015

No ethical approval was obtained from the local ethical committee because only the retrospective data were used. All patients were informed about the procedure and taken their informed consent prior to clinical examinations and radiologic evaluation according to the principles of the Helsinki Declaration, including all amendments and revisions. Collected data were noted and only accessible to the researchers.
All the CBCT images were evaluated by a dentomaxillofacial radiologist who had 12 years of experience in the basis of calcifications which were detected outside of the regions of primary interest. All of the calcifications were detailed classified and reported.
For CBCT evaluations, proprietary manufacturer software (i-Dixel 2.0/One Data Viewer/One Volume Viewer; J Morita Mfg. Corp.) was used. Images were viewed in a dimly lit room on a 30 inch DellTM 3008WFP Flat Panel Monitor (Dell Inc., Round Rock, TX, USA) at a screen resolution of 1920x1200 pixels and 32-bit colour depth.
Data were analyzed by descriptive statistics. The occurence frequency of incidentally found calcifications in head and neck area was noted. Median and range were used to describe the age of the patients. Statistical analyses were performed using the SPSS software (version 15.0; SPSS Inc., Chicago, IL, USA) and MS Excel 2003.
Results
A total of 691 CBCT scans were assessed. Of 691 CBCT images, it was detected a great preponderance of males (n= 423 (61.2%)). The patients’ mean age was 43.5±17.3 years and within the age range of 5 to 84 years. The most commonly preferred reason for CBCT was dental implant planning with 69.5% (n= 480) of the patients in evaluated group. 11.4% (n= 79) were referred for the evaluation of third molars with anatomic structures and 6.7% (n= 46) were for cystic lesion evaluation. The age-gender distribution and frequency distribution of the sample referred for CBCT scans are shown in Table 1. Most frequently referred patient age groups were the 41-50 age group (20.98%) followed by 21-30 age group (19.39%). The least preferred age groups were 1-10 (0.43%) and over 70 group (4.92%). According to this table, the most common reason for CBCT scan was found in 41-50 age group as implant rehabilitation (90.3%, n= 131). It also found that orthodontic reasons were the most common reason for 1-10 and 21-30 age groups respectively (100%, n= 3; 37.3%, n= 22).
in relatively low diagnostic success, especially in cases in which relatively small calcifications are present or are superimposed on anatomic structures3. In such cases, a second radiologic 2D plane must be obtained. However, the combination of 2 conventional 2D imaging strategies could increase the radiation exposure to a level similar to that of low-dose cone beam computed tomography (CBCT) imaging4.
CBCT introduced in 1998, is increasingly used for 3-dimensional imaging in maxillofacial radiology5. Available CBCT scanners generate image volumes of a field of view from (height X width) 4 X 4 cm to 23 X 17 cm. Spatial resolution of isotropic voxel size of available scanners ranges from 0.08 to 0.4 mm1-4.
Larger scans provide a comprehensive radiologic view of the maxillofacial skeleton and partly of the soft tissue therein.
CBCT imaging has been applied in implantology, orthodontics, maxillofacial surgery and in the assessment of dentoalveolar pathology6,7. With the increasing use of CBCT imaging in dentistry, the incidental discovery of soft fissue calcifications is likely to increase. In addition, CBCT imaging provides images in the third dimension, which facilitates precise localization. The clinician should have a solid foundation in the radiographic presentation of the calcification condition as it relates to the various structures, particularly on CBCT images. CBCT imaging is an excellent diagnostic tool to determine the size, location, and shape of calcifications1-5. Dreiseidler et al.8 mentioned that diagnostic sensitivity and specificity levels with CBCT imaging are as high as or higher than those obtained using other diagnostic methods.
The aim of this study was to describe the patterns of referral and to reveal the type and prevalence of incidental findings such as anatomical variations, pathologies or calcifications in CBCT scans which were obtained for several diagnostic purposes.
Materıal and Methods
This prevalence study was made by using CBCT scans. CBCT images used in the study were acquired on a 3D Accuitomo 170 (3D Accuitomo; J Morita Mfg. Corp., Kyoto, Japan) which were obtained between 2011-2015. The study sample (n= 691) consisted of CBCT scans of patients who were referred for CBCT evaluation to the Department of Dentomaxillofacial Radiology, Gulhane Military Medical Academy, Ankara, Turkey. 202 of 893 images were excluded because of poor diagnostic quality or low FOV size. Images with low FOV size are obtained only for sectional imaging, so they can not provide sufficient information about out of interest regions of maxillofacial area. 691 CBCT images were included to the study.
Balk J Dent Med, Vol 21, 2017 Incidental findings in CBCT images 101

102 Ali Altındağ et al. Balk J Dent Med, Vol 21, 2017
common seen calcifications were tonsillolith (86.03%), followed by stylohyoid calcifications (6.24%), antrolith and subdermal calcifications (2.33%). The most prevalent age groups of calcifications were 41-50 age group and followed by 51-60 age group. The distribution of age groups and calcifications is shown in Table 3.
945 incidentally found calcified structures were discovered on 318 (46.02%) of the 691 patients’ CBCT scans. 373 (53.98%) scans showed no calcificated findings. Descriptive analysis and frequency of calcifications were shown in Table 2. Among all of the calcifications which were incidentally found in head and neck area, the most
Table 1. Age-gender distribution of subjects and distribution of referral reasons of CBCT (n, %)
Gender Age Groups
Female Male 1-10 11-20 21-30 31-40 41-50 51-60 61-70 70+ Total
Implant assessment 208 (77.6) 272 (64.3) N/A 3 (5.1) 38 (28.4) 63 (67.0) 131 (90.3) 120 (97.6) 92 (92.9) 33 (97.1) 480 (69.5)
Cyst 9 (3.4) 37 (8.7) N/A 5 (8.5) 20 (14.9) 8 (8.5) 7 (4.8) 2 (1.6) 4 (4.0) N/A 46 (6.7)
Embedded Teeth 6 (2.2) 17 (4.0) N/A 6 (10.2) 12 (9.0) 4 (4.3) N/A N/A N/A 1 (2.9) 23 (3.3)
Third molar evaluation 27 (10.1) 52 (12.3) N/A 18 (30.5) 41 (30.6) 13 (13.8) 4 (2.8) 1 (0.8) 2 (2.0) N/A 79 (11.4)
Trauma 6 (2.2) 9 (2.1) N/A 4 (6.8) 5 (3.7) 3 (3.2) 2 (1.4) N/A 1 (1.0) N/A 15 (2.2)
Orthodontics 9 (3.4) 28 (6.6) 3 (100.0) 22 (37.3) 10 (7.5) 2 (2.1) N/A N/A N/A N/A 37 (5.4)
Combination 2 (0.7) 5 (1.2) N/A 1 (1.7) 4 (3.0) 1 (1.1) 1 (0.7) N/A N/A N/A 7 (1.0)
Odontoma 1 (0.4) 3 (0.7) N/A N/A 4 83.0) N/A N/A N/A N/A N/A 4 (0.6)
Total 268 (100) 423 (100) 3 (100) 59 (100) 134 (100) 94 (100) 145 (100) 123 (100) 99 (100) 34 (100) 691 (100)
N/A : not available
Table 2. Descriptive analysis and frequency of the calcifications
Calcifications Number of Findings (%)Number of patients (%)
Female Male
Tonsillolith 813 (86.03) 75 (23.58) 141 (44.34)
Antrolith 22 (2.33) 12 (3.78) 9 (2.83)
Sialolith 9 (0.95) 3 (0.94) 4 (1.26)
Artery calcification 16 (1.7) 4 (1.26) 9 (2.83)
Stylohyoid calcification 59 (6.24) 14 (4.4) 21 (6.6)
Subdermal calcifications 22 (2.33) 8 (2.52) 14 (4.4)
Intracranial calcifications 4 (0.42) 0 (0) 4 (1.26)
TOTAL 945 (100) 116 (36.48) 202 (63.52)

Balk J Dent Med, Vol 21, 2017 Incidental findings in CBCT images 103
Table 3. Distribution of calcified lesions and age groups
Age Groups
1-10 11-20 21-30 31-40 41-50 51-60 61-70 70+
Tonsillolith 0 (0.0) 9 (4.2) 32 (14.8) 20 (9.3) 54 (25.0) 43 (19.9) 42 (19.4) 16 (7.4)
Antrolith 0 (0.0) 0 (0.0) 3 (15.0) 3 (15.0) 3 (15.0) 5 (25.0) 4 (20.0) 2 (10.0)
Sialolith 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 2 (40.0) 3 (60.0) 0 (0.0)
Artery calcification 0 (0.0) 0 (0.0) 1 (10.0) 0 (0.0) 1 (10.0) 2 (20.0) 2 (20.0) 4 (40.0)
Styloid calcification 0 (0.0) 0 (0.0) 1 (9.1) 2 (18.2) 4 (36.4) 2 (18.1) 1 (9.1) 1 (9.1)
Subdermal calcifications 0 (0.0) 0 (0.0) 2 (9.1) 2 (9.1) 7 (31.8) 7 (31.8) 3 (13.6) 1 (4.5)
Intracranial calcifications 0 (0.0) 2 (50.0) 1 (25.0) 1 (25.0) 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0)
A total of 809 palatinal tonsil calcifications were found in 212 patients (Figure 1). In addition it is also found 4 patients had calcifications in adenoidal region. 418 of tonsil calcifications were at the right side, 391 were at the left side. Distribution of total tonsil calcifications over their shape is shown in Table 4. Tonsil calcifications were classified according to its shape such as round, irregular and dot-like. Especially round-like shaped tonsilloliths with under 2 mm diameter were considered as dot-like. According to the table irregular shaped tonsil calcifications were the most frequently found, the second most common form was dot-like shaped. It was also found in one patient had totally 23 tonsil calcifications which 9 of them were
Table 4. Distribution of the shape and quantity of tonsilloliths
Tonsillolith Shape
0n (%)
1n (%)
2n (%)
3n (%)
4n (%)
5n (%)
6n (%)
7n (%)
8n (%)
9n (%)
10n (%)
RIG
HT
Dot-like shaped 608 (88.0) 36 (5.2) 22 (3.2) 13 (1.9) 7 (1.0) 4 (0.6) N/A 1 (0.1) N/A N/A N/A
Irregular shaped 592 (85.7) 48 (6.9) 21 (3.0) 17 (2.5) 7 (1.0) 2 (0.3) N/A 2 (0.3) N/A 1 (0.1) 1 (0.1)
Round shaped 664 (96.1) 25 (3.6) N/A 1 (0.1) 1 (0.1) N/A N/A N/A N/A N/A N/A
LEFT
Dot-like shaped 609 (88.1) 40 (5.8) 17 (2.5) 13 (1.9) 6 (0.9) 3 (0.4) 2 (0.3) 1 (0.1) N/A N/A N/A
Irregular shaped 586 (84.8) 63 (9.1) 22 (3.2) 10 (1.4) 6 (0.9) 4 (0.6) N/A N/A N/A N/A N/A
Round shaped 660 (95.5) 25 (3.6) 4 (0.6) 2 (0.3) N/A N/A N/A N/A N/A N/A N/A
N/A : not available
irregular. Distribution of number of tonsilloliths on CBCT is shown in Table 5.
A total of 22 antroliths were found in 21 patients (Figure 2). Of these 12 were females and 9 were males. Only one patient with bilateral antrolith was detected. Rest of cases were unilateral. Seven patients had nine sialoliths (Figure 3). Of these 3 were females and 4 were males. In two cases there were two sialoliths and in 5 cases there was one sialolith. 35 of the patients had 59 stylohyoid calcifications (Figure 4). 14 of them were females and 21 of them were males. Of these 24 were bilateral and 11 were unilateral. Subdermal calcifications were noted in 22 patients and only four male patients had intracranial calcifications (Figure 5).

104 Ali Altındağ et al. Balk J Dent Med, Vol 21, 2017
Table 5. Distribution of number of tonsilloliths.
Number of Tonsilloliths Number of patients (%)
0 479 (69.31)
1 57 (8.24)
2 41 (5.93)
3 27 (3.9)
4 20 (2.89)
5 18 (2.6)
6 11 (1.59)
7 13 (1.88)
8 8 (1.15)
9 8 (1.15)
≥10 9 (1.30)
Total 691(100)Figure 1. Female patient aged 81. Incidentally found, a very rare case
of the calcification of facial artery which is a branch of external carotid artery. Coronal, sagittal axial and 3D reconstructed views
Figure 2. Female patient aged 54. Coronal, sagittal and axial views of an opacification in maxillary sinus
Figure 3. 3D reconstructed view of bilateral multiple tonsilloliths of a female patient aged 83.
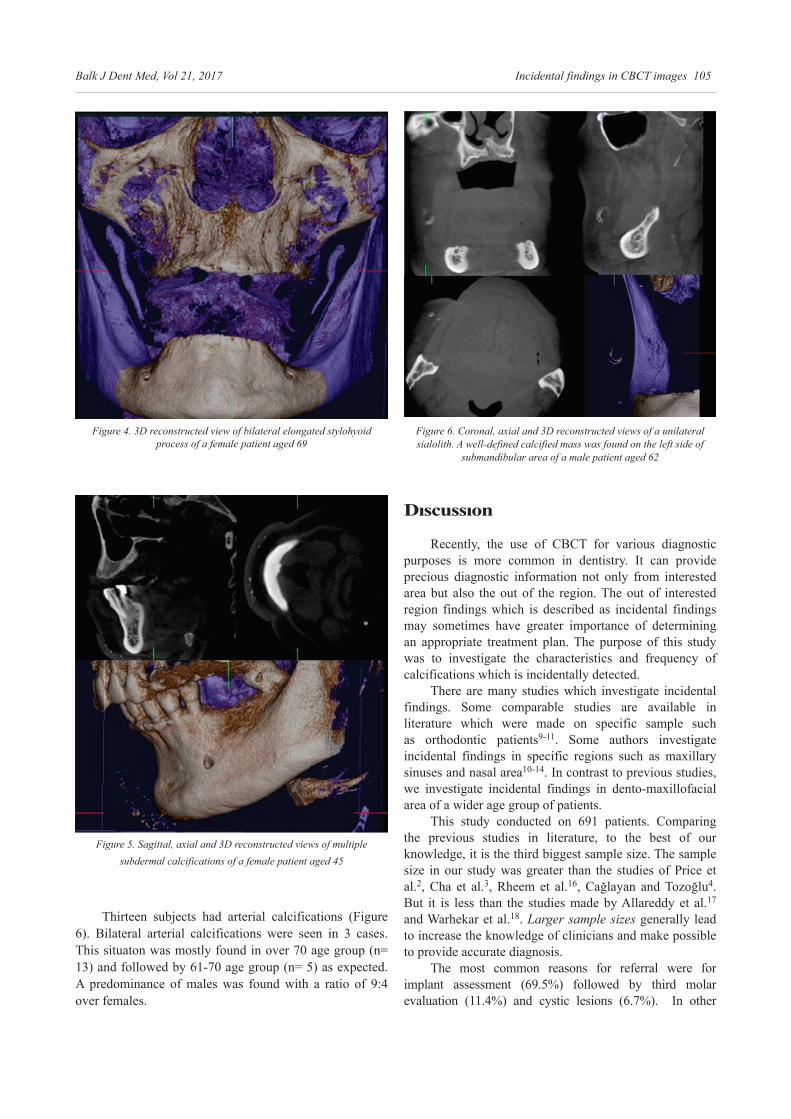
Balk J Dent Med, Vol 21, 2017 Incidental findings in CBCT images 105
Figure 6. Coronal, axial and 3D reconstructed views of a unilateral sialolith. A well-defined calcified mass was found on the left side of
submandibular area of a male patient aged 62
Dıscussıon
Recently, the use of CBCT for various diagnostic purposes is more common in dentistry. It can provide precious diagnostic information not only from interested area but also the out of the region. The out of interested region findings which is described as incidental findings may sometimes have greater importance of determining an appropriate treatment plan. The purpose of this study was to investigate the characteristics and frequency of calcifications which is incidentally detected.
There are many studies which investigate incidental findings. Some comparable studies are available in literature which were made on specific sample such as orthodontic patients9-11. Some authors investigate incidental findings in specific regions such as maxillary sinuses and nasal area10-14. In contrast to previous studies, we investigate incidental findings in dento-maxillofacial area of a wider age group of patients.
This study conducted on 691 patients. Comparing the previous studies in literature, to the best of our knowledge, it is the third biggest sample size. The sample size in our study was greater than the studies of Price et al.2, Cha et al.3, Rheem et al.16, Cağlayan and Tozoğlu4. But it is less than the studies made by Allareddy et al.17 and Warhekar et al.18. Larger sample sizes generally lead to increase the knowledge of clinicians and make possible to provide accurate diagnosis.
The most common reasons for referral were for implant assessment (69.5%) followed by third molar evaluation (11.4%) and cystic lesions (6.7%). In other
Figure 4. 3D reconstructed view of bilateral elongated stylohyoid process of a female patient aged 69
Figure 5. Sagittal, axial and 3D reconstructed views of multiple subdermal calcifications of a female patient aged 45
Thirteen subjects had arterial calcifications (Figure 6). Bilateral arterial calcifications were seen in 3 cases. This situaton was mostly found in over 70 age group (n= 13) and followed by 61-70 age group (n= 5) as expected. A predominance of males was found with a ratio of 9:4 over females.

106 Ali Altındağ et al. Balk J Dent Med, Vol 21, 2017
et al.20 found 46.1% of tonsilloliths and reported that the most common shape was dot shaped.
Antrolith is a calcified mass within the paranasal sinuses. Of the 22 discovered antroliths, only one case was bilateral, the others were unilateral. Total number of patients with antrolith were 21 (3.03%). Literature report that the incidences of antroliths are between 0.15%-4.54%2,14,19,21,22. Our study presents appropriate result with the above mentioned reports.
One another calcification detected in 7 patients was sialolith. Sialolith is mineral salt deposition in salivary glands or ducts. Seven patients had nine sialoliths. Of these two patients had two calcifications, rest of seven had one sialoliths. According to literature, incidences of sialoliths are low, between 0.3%-0.66%2,17,18. In our study we found relatively higher incidence rate (1.01%).
The other calcifications, arter calcification, stylohyoid calcification and subdermal calcifications were, respectively, found in 13 (1.88%), 35 (5.06%) and 22(3.18%) patients. According to literature, incidences of calcifications which mentioned above are between 2.04%-10.04%2,16,17,23, 6.12%-63.3%2,16,24 and 2.27%-28%17,25,26 respectively. In our study the incidences of carotis artery calcification and stylohyoid calcification were relatively lower than those in the above mentioned studies.
Literature reports that intracranial calcifications was common and occur at any age and of any ethnicity. And also Kwak et al.27 reported that intracranial calcifications are found more commonly in males than in females. In our study, we found only 4 patients who had intracranial calcifications and all of them were males. In addition, frequency of intracranial calcifications of this sample group was found relatively lower than in previous reports (4.76%-71%)16,17,27-30. Occurence of differences may be due to many reasons such as sample size, the size of the FOV, radiologic imaging devices and their different abilities in detecting pathologies. Hence, it may be making direct comparisons inappropriate.
Conclusion
In conclusion, clinicians should be aware of incidentally discovered calcified lesions. Correct identification of these findings will reduce unnecessary further diagnostic assessments and will provide more appropriate treatment plans. It will also provide the ability comprehensively evaluation of underlying diseases and practitioners will have life-saving information by early diagnosis.
Note: The results of this paper were awarded for the oral presentation at the 22nd BaSS Congress.
studies, CBCT referral rate for implant placement varied from 2.72% to 73%2-4,16-18. The referral rate of our study was nearly similar with the rates of studies made by Price et al.2 and Allareddy et al.17. Rheem et al.16 reported that the referral rate of implant patients was 2.72%. The greatest difference of rates is due to the study which previously mentioned was arranged by Orthodontic Division. In addition to referral reasons, it is also found that the most frequently referred patient age groups were 41-50 age group (20.98%) followed by 21-30 age group (19.39%) and 51-60 age group (17.8%). However, Warhekar et al.18 reported the most frequently referred patients’ age group was 21-30 (24%), Rheem et al.16 reported as 10-19 (44.21%), Price et al.2 reported as 60-69 (26.33%) and Allareddy et al.17 reported as 51-60 (22%). The less referred age group was found as 1-10 age group (0.43%). Similarly, Rheem et al.16 and Price et al.2 reported that the less referral age group was 1-10 age group.
Of the 691 CBCT scans reviewed, 318 scans (46.02%) showed at least 1 finding. A total of 945 calcifications were found. It is also found 2.97 of rate for per scan. 373 (53.98%) scans showed no calcified lesion. Actually, there are many studies in literature about incidental findings which also contain calcifications. But to the best of our knowledge, this report is the first comprehensive study on the basis of calcifications. It is also seen that the frequency of incidental findings in CBCT shows wide variety in literature. Some studies which conducted with incidental findings present higher frequency rates2,4,17,19, but some of them have lower frequency than this study3,16. It may be due to differences in age groups, target population, sample size or variety of catagorized findings. The authors whose studies previously mentioned did not categorized their findings as a different chapter titled calcifications. Hence, previous reports and our findings should be compared step by step.
Calcifications generally occur in vessels, ligaments, glandular tissues. Sometimes they occur as a result of chronic inflammation or scarring. Soft tissue calcifications in maxillofacial area can be pathological, age-related or idiopathic. Accurate definition of this calcifications is based on some characteristics such as location, morphology and distribution. Due to cross-sectional imaging advantage of CBCT, it become the first choice for accurate diagnosis2. In the light of the above information, a total of 945 calcification findings were found in study sample. In a total of 945 calcifications, 813 (86.03%) were tonsil calcifications in 216 patients (31.25%). Distribution of the other calcifications which were found in our study was shown in Table 2. In addition, tonsil calcifications were classified according to their shape. Irregular shaped tonsil calcifications were the most frequently found, the second most common form was dot-like shaped. To the best to our knowledge, there is only one report in literature in which tonsilloliths’ shape was classified. Oda

Balk J Dent Med, Vol 21, 2017 Incidental findings in CBCT images 107
17. Allareddy V, Vincent SD, Hellstein JW, Qian F, Smoker WR, Ruprecht A. Incidental findings on cone beam computed tomography images. Int J Dent, 2012;2012:871532.
18. Warhekar S, Nagarajappa S, Dasar PL, Warhekar AM, Parihar A, Phulambrikar T et al. Incidental findings on cone beam computed tomography and reasons for referral by dental practitioners in indore city (m.p). J Clin Diagn Res, 2015;9:ZC21-4.
19. Drage N, Rogers S, Greenall C, Playle R. Incidental findings on cone beam computed tomography in orthodontic patients. J Orthod, 2013;40:29-37.
20. Oda M, Kito S, Tanaka T, Nishida I, Awano S, Fujita Y et al. Prevalence and imaging characteristics of detectable tonsilloliths on 482 pairs of consecutive CT and panoramic radiographs. BMC Oral Health, 2013;13:54.
21. Nass Duce M, Talas DU, Ozer C, Yildiz A, Apaydin FD, Ozgür A. Antrolithiasis: a retrospective study. J Laryngol Otol, 2003;117:637-640.
22. Rege IC, Sousa TO, Leles CR, Mendonça EF. Occurrence of maxillary sinus abnormalities detected by cone beam CT in asymptomatic patients. BMC Oral Health, 2012 Aug 10;12:30.
23. Wells AB. Incidence of soft tissue calcifications of the head and neck region on maxillofacial cone beam computed tomography. Electronic Theses and Dissertations. Paper 1545, 2011.
24. Mahdian M, Moghaddam EJ, Alzahrani A, Rengasamy K, Tadinada A. Calcification of the stylohyoid ligament in panoramic radiography and cone beam computed tomography among patients referred for dental implant treatment planning. Implant Dent, 2014;23:508-513.
25. Shigehara H, Honda Y, Kishi K, Sugimoto T. Radiographic and morphologic studies of multiple miliary osteomas of cadaver skin. Oral Surg Oral Med Oral Pathol Oral Radiol Endod, 1998;86:121-125.
26. Safi Y, Valizadeh S, Vasegh Z, Aghdasi MM, Shamloo N, Azizi Z. Prevalence of osteoma cutis in the maxillofacial region and classification of its radiographic pattern in cone beam CT. Dermatol Online J, 2016;22(1):2.
27. Kwak R, Takeuchi F, Ito S, Kadoya S. Intracranial physiological calcification on computed tomography (Part 1): Calcification of the pineal region. No To Shinkei, 1988;40:56-74.
28. Daghighi MH, Rezaei V, Zarrintan S, Pourfathi H. Intracranial physiological calcifications in adults on computed tomography in Tabriz, Iran. Folia Morphol, 2007;66:115-119.
29. Kıroglu Y, Callı C, Karabulut N, Oncel C. Intracranial calcifications on CT. Diagn Interv Radiol, 2010;16:263-269.
30. Sedghizadeh PP, Nguyen M, Enciso R. Intracranial physiological calcifications evaluated with cone beam CT. Dentomaxillofac Radiol, 2012;41:675-678.
Received on May 10, 2017.Revised on Jun 1, 2017.Accepted on Jun 11, 2017.
Correspondence:
Ali Altındağ Department of Dentomaxillofacial Radiology Faculty of Dentistry, Ankara Universitty, Ankara, Turkey e-mail: [email protected]
References
1. Scarfe WC, Farman AG. Soft tissue calcifications in the neck: Maxillofacial CBCT presentation and significance. AADMRT Newsletter, 2010;2:3-15.
2. Price JB, Thaw KL, Tyndall DA, Ludlow JB, Padilla RJ. Incidental findings from cone beam computed tomography of the maxillofacial region: a descriptive retrospective study. Clin Oral Implants Res, 2012;23:1261-1268.
3. Cha JY, Mah J, Sinclair P. Incidental findings in the maxillofacial area with 3-dimensional cone-beam imaging. Am J Orthod Dentofacial Orthop, 2007;132:7-14.
4. Cağlayan F, Tozoğlu U. Incidental findings in the maxillofacial region detected by cone beam CT. Diagn Interv Radiol, 2012;18:159-163.
5. Mozzo P, Procacci C, Tacconi A, Martini PT, Andreis IA. A new volumetric CT machine for dental imaging based on the cone-beam technique: preliminary results. Eur Radiol, 1998;8:1558-1564.
6. Pohlenz P, Blessmann M, Blake F, Heinrich S, Schmelzle R, Heiland M. Clinical indications and perspectives for intraoperative cone-beam computed tomography in oral and maxillofacial surgery. Oral Surg Oral Med Oral Pathol Oral Radiol Endod, 2007;103:412-417.
7. De Vos W, Casselman J, Swennen GRJ. Cone-Beam Computerized Tomography (CBCT) Imaging of the Oral and Maxillofacial Region: A Systemic Review of the Literature. Int J Oral Maxillofac Surg, 2009;38:609-625.
8. Dreiseidler T, Mischkowski RA, Neugebauer J, Ritter L, Zöller JE. Comparison of cone-beam imaging with orthopantomography and computerized tomography for assessment in presurgical implant dentistry. Int J Oral Maxillofac Implants, 2009;24:216-225.
9. Rogers SA, Drage N, Durning P. Incidental findings arising with cone beam computed tomography imaging of the orthodontic patient. Angle Orthod, 2011;81:350-355.
10. Pazera P, Bornstein MM, Pazera A, Sendi P, Katsaros C. Incidental maxillary sinus findings in orthodontic patients: a radiographic analysis using cone-beam computed tomography (CBCT). Orthod Craniofac Res, 2011;14:17-24.
11. Gracco A, Parenti SI, Ioele C, Bonetti GA, Stellini E. Prevalence of incidental maxillary sinus findings in Italian orthodontic patients: A retrospective cone-beam computed tomography study. Korean J Orthod, 2012;42:329-234.
12. Raghav M, Karjodkar FR, Sontakke S, Sansare K. Prevalence of incidental maxillary sinus pathologies in dental patients on cone-beam computed tomographic images. Contemp Clin Dent, 2014;5:361-365.
13. Brüllmann DD, Schmidtmann I, Hornstein S, Schulze RK. Correlation of cone beam computed tomography (CBCT) findings in the maxillary sinus with dental diagnoses: a retrospective cross-sectional study. Clin Oral Investig, 2012;16:1023-1029.
14. Lana JP, Carneiro PM, Machado Vde C, de Souza PE, Manzi FR, Horta MC. Anatomic variations and lesions of the maxillary sinus detected in cone beam computed tomography for dental implants. Clin Oral Implants Res, 2012;23:1398-1403.
15. Göçmen G, Borahan MO, Aktop S, Dumlu A, Pekiner FN, Göker K. Effect of Septal Deviation, Concha Bullosa and Haller’s Cell on Maxillary Sinus’s Inferior Pneumatization; a Retrospective Study. Open Dent J, 2015;9:282-286.
16. Rheem S, Nielsen IL, Oberoi S. Incidental findings in the maxillofacial region identified on cone-beam computed tomography scans. J Orthod Res, 2013;1:33-39.

SUMMARYBackground/Aim: The aim of this in vitro study was to investigate
the influence of irradiation cycles and resting periods, on thermal effects on the external root surface during root canal irradiation of two diode laser systems (940 nm and 975 nm), at output powers of 1 W and 2 W in continuous mode. In previous studies the rising of temperature above 7°C has been reported as biologically accepted to avoid periodontal damage on the external root surface. Material and Methods: Twenty human inferior incisors were randomly distributed into four groups, the 940 nm, and the 975 nm diode laser irradiation, both with an output power of 1 W and 2 W, in continuous mode. The thermographic camera was used to detect temperature variations on the external root surface. Digital radiography of the samples was made. Results: After three cycles of irradiation, at apical third of the root, mean temperature variation by 940 nm diode laser irradiation was 2.88°C for output power of 1 W, and 6.52°C for output power of 2 W. The 975 nm laser caused a higher temperature increase in the apical region, with temperature variation of 13.56°C by an output power of 1 W, and 30.60°C at 2 W, with a statistical significance of p ≤ 0.0001 between two laser systems compared for the same power. The resting periods of 20 s between cycles were enough to lower temperature under 7°C in the case of 1 W and 2 W for 940 nm diode laser, while for 975 nm laser, after three irradiation cycles overheating occurred at both output power rates. Conclusion: Three cycles irradiation of 940 nm diode laser, with resting periods of 20 seconds, allowed safe usage of 1 W and 2 W in CW for endodontic treatment. For 975 nm at a power rate of 1 W, the last resting period drop the temperature near the safe limit and it came under 7°C in a period less than a minute, while at the power of 2 W the resting periods were not long enough for the safe temperature decrease. Key words: Diode Laser, Endodontics, Bactericidal, Temperature Variations, External Root Surface
Dijana Trišić1, Bojana Ćetenović1, Igor Jovanović2, Elizabeta Gjorgievska3, Branka Popović4, Dejan Marković1
1 Clinic for Paediatric and Preventive Dentistry Faculty of Dental Medicine University of Belgrade, Serbia 2 Department of Electronics Faculty of Electronic Engineering University of Niš, Serbia 3 Faculty of Dentistry University “Ss Cyril and Methodius” Skopje, FYRM 4 Institute of Human Genetics Faculty of Dental Medicine University of Belgrade
ORIGINAL PAPER (OP)Balk J Dent Med, 2017;108-111
BALKAN JOURNAL OF DENTAL MEDICINE ISSN 2335-0245
Diode Laser Irradiation in Endodontic Therapy through Cycles - in vitro Study
STOMATOLOGICA
L S
OC
IET
Y
Introduction
Reduction of intracanal bacteria prior to obturation is the main goal of endodontic therapy. Microorganisms in the root canal and infected tooth structure have to be minimized, to create optimal conditions for periapical healing1. Chemomechanical instrumentation, with various concentrations of sodium hypochlorite as the most common canal irrigant, was the standard approach in
elimination of bacteria biofilm, necrotic and vital tissue. Despite good instrumentation and intensive irrigation protocols, there was a lack of success in decontamination of root canal system2,3.
Diode lasers caught the attention of the researchers in the past years for their antimicrobial abilities through thermal effect. Studies reported bacterial decontamination of root canals by the application of diode laser with different success rates2,4. Diode lasers have a direct thermal effect on the microbiota.
10.1515/bjdm-2017-0016

from the root surface and the lens system transformed energy into electrical impulses. Digital images of the root temperature variations were analyzed by IRBIS Professional 2.2. graphic-oriented software package (InfraTec GmbH, Dresden, Germany).
All teeth were radiographed by digital radiographic system Trophy RadioVisioGraphy (Trophy Radiologie, Croissy-Beaubourg, France). Dentin thickness of the mesial walls of the roots was measured in all thirds.
Statistical analysis was performed by the Prism software version 6 (GraphPad Software, San Diego, CA). Two-way ANOVA was used to compare values of temperature variations, and One-way ANOVA for comparing dentine thickness between the groups. The statistical significance was tested at p < .05.
The effect depends on the irradiation mode and settings, and it is directly related to the amount of energy delivered. Heating in the root canal is a desirable effect, but it could also gain overheating of external root portions, causing injury of periodontal ligament and bone5. Temperature elevation on external root surface is dependent on dentine thickness, output power, and resting time between irradiation cycles6. In previous studies the rising of temperature above 7°C has been reported as biologically accepted to avoid periodontal damage on the external root surface during endodontic procedures7,8.
The aim of our in vitro study was to investigate the influence of three irradiation cycles and following resting periods, on thermal effects on the external root surface during root canal irradiation of 940 nm and 975 nm diode laser systems, at output powers of 1 W and 2 W, in continuous mode.
Materials and Methods
Twenty lower permanent incisors were collected at the Clinic for Oral Surgery, Faculty of Dental Medicine, Belgrade, Serbia, with written consent from patients. Freshly extracted teeth were cleaned by removing organic residue tissue and calculus from the external root portion, and cross-sectioned at a cementoenamel junction in the cervical portion, using a double-sided diamond disk (NTI-Kahla GmbH, Kahla, Thuringia, Germany), standardizing the roots at a 13 mm length. Further, chemomechanical instrumentation was applied, and all the root canals were enlarged to an apical size of #40 by hand, using K-files, 1% sodium hypochlorite and 40% acetic acid. Teeth were stored in PBS at +40C, prior to use.
The Epic 940 nm diode laser (Biolase® Technology, Inc., San Clemente, CA, USA) and the LaserHF 975 nm diode laser (Hager & Werken, Germany) were used in the study, with optical fiber of 200 µm for 940 nm, and 320 µm for 975 nm laser, provided by the manufacturers. The prepared samples were randomly divided into 2 main groups, and subdivided into two groups depending on the output power - 1W and 2W, in continuous mode (CW), as shown in Figure 1.
Laser fiber was inserted into the root canal to the apex, approximately 1 mm from the anatomic foramen, and activated in the moment it was pulled from the apical end in helicoidal movements (~ 2 mm/s), three consecutive times, with resting periods of 20 seconds after each laser dose. Prior to irradiation, teeth were dried, set on the plastic holders in a vertical position, with a mesial side of the root directed toward thermographic camera Varioscan® high-resolution model 3021 (Jenoptik, Dresden, Germany). All the experiments were measured in the controlled environment, at room temperature 21 - 23°C. Thermographic camera detected infrared irradiation
Figure 1. Teeth randomly assigned to the groups, depending on the treatment
Results
In Table 1. and Table 2. mean values of temperature variations (∆T), regarding experimental groups, are represented. After three cycles of irradiation, at apical third of the root, mean ∆T by 940 nm diode laser irradiation was 2.88°C for output power of 1 W, and 6.52°C for output power of 2 W, in continuous mode. The 975 nm caused a higher temperature increase in the apical region, with ∆T variation of 13.56°C by an output power of 1 W, and 30.60°C at 2 W, with a statistical significance of p ≤ 0.0001 between two laser systems compared for the same power. The trend continued in middle and cervical third of the root. There was not a statistical difference of ∆T between root thirds, for the same treatment, although temperature raised from cervical to apical third. Through irradiation cycles, and resting periods, ∆T values are represented in Figure 2. The resting periods of 20 s between cycles were enough to lower temperature under 7°C in the case of 1 W and 2 W for 940 nm diode laser, while for 975 nm laser, after three irradiation cycles overheating occurred at both output power rates.
Balk J Dent Med, Vol 21, 2017 Diode Laser in Endodontics 109

110 Dijana Trišić et al. Balk J Dent Med, Vol 21, 2017
Differences in ∆T values were significant at third cycle point between the laser systems in all thirds and between output powers (p < .0001), except between 1 W and 2 W in 940 nm group (p > .05). For 975 nm at a power rate of 1 W, the last resting period drop the temperature near the safe limit and temperature further lowered under 7 °C in a period less than a minute. Statistical analysis of dentine thickness showed no statistical differences between groups (p > .05), which suggested that the results from the groups were comparable.
Discussion
Healing of the tissue after endodontic treatment directly depends on successful disinfection of root canal system. Chemical disinfection can reach bacteria only at 0.1 mm in dentin canaliculi9, while microbiota is found at 1.1 mm deep into dentine10. It has been shown that the wavelengths of 940 nm and 980 nm diode lasers had high penetration into the dentine tissue with bactericidal effect11, which justify the usage of high-power diode lasers as adjutant in endodontic therapy. In in vitro study, Schoop et al.12 showed significant reduction of Enterococcus faecalis and Escherichia coli after diode laser irradiation. They concluded that diode laser could be successfully applied for disinfection in deep layers of dentin. On the other hand, it has been shown that during diode laser irradiation thermal stress on the external root surface could occur, if the safe temperature rising of 7°C last over one minute7,13.
Table 1. Mean and standard deviation (SD) values of the temperature variations ∆T (ºC) at external surface of the roots thirds, during irradiation cycles by 940 nm diode laser
940 nm 1 W apical
940 nm 1 W middle
940 nm 1 W cervical
940 nm 2 W apical
940 nm 2 W middle
940 nm 2 W cervical
1. cycle 1.96 (0.65) 1.48 (0.53) 0.98 (0.30) 5.02 (2.23) 3.24 (0.84) 1.68 (0.37)1. pause 1.18 (0.37) 1.08 (0.33) 0.88 (0.31) 1.72 (0.73) 1.64 (0.63) 1.22 (0.22)2. cycle 2.34 (0.82) 2.04 (0.54) 1.72 (0.40) 5.98 (1.73) 4.54 (0.82) 3.26 (1.08)2. pause 1.54 (0.38) 1.64 (0.40) 1.48 (0.36) 2.44 (0.79) 2.70 (0.53) 2.36 (0.25)3. cycle 2.88 (0.82) 2.68 (0.68) 2.50 (0.58) 6.52 (1.65) 5.88 (1.17) 4.36 (0.69)3. pause 1.98 (0.46) 2.18 (0.48) 2.06 (0.48) 3.52 (1.10) 3.82 (1.10) 3.24 (0.75)
Table 2. Mean and standard deviation (SD) values of the temperature variations ∆T (ºC) at external surface of the roots thirds, during irradiation cycles by 975 nm diode laser
975 nm 1 W apical
975 nm 1 W middle
975 nm 1 W cervical
975 nm 2 W apical
975 nm 2 W middle
975 nm 2 W cervical
1. cycle 7.18 (2.78) 8.94 (2.52) 8.36 (3.29) 16.60 (6.19) 17.92 (3.92) 19.60 (6.65)1. pause 3.82 (1.27) 4.18 (1.57) 3.32 (0.62) 7.62 (1.40) 8.06 (1.42) 7.28 (1.40)2. cycle 13.02 (2.27) 13.86 (3.00) 11.26 (2.31) 20.30 (4.94) 24.82 (5.36) 27.52 (6.69)2. pause 6.54 (1.08) 6.82 (1.44) 5.68 (0.40) 10.80 (2.17) 12.30 (1.86) 11.22 (1.51)3. cycle 13.56 (2.30) 15.66 (3.06) 14.34 (2.09) 30.60 (2.50) 32.42 (5.20) 31.22 (7.14)3. pause 8.02 (1.00) 8.80 (1.31) 7.56 (0.68) 14.80 (2.25) 14.00 (3.22) 14.98 (1.81)
Figure 2. Temperature variations ∆T (ºC) through cycles and resting periods, for 940 nm and 975 nm laser systems, at output powers of 1 W and 2 W. A - cervical third, B - middle third, C - apical third. The recommended safe temperature rising limit of 7 0C is represented by
horizontal bar.

Balk J Dent Med, Vol 21, 2017 Diode Laser in Endodontics 111
2. Neelakantan P, Cheng CQ, Mohanraj R, Sriraman P, Subbarao C, Sharma S. Antibiofilm activity of three irrigation protocols activated by ultrasonic, diode laser or Er:YAG laser in vitro. Int Endod J, 2015;48:602-610.
3. Fedorowicz Z, Nasser M, Sequeira-Byron P, de Souza RF, Carter B, Heft M. Irrigants for non-surgical root canal treatment in mature permanent teeth. Cochrane Database Syst Rev, 2012:Cd008948.
4. Bago I, Plecko V, Gabric Panduric D, Schauperl Z, Baraba A et al. Antimicrobial efficacy of a high-power diode laser, photo-activated disinfection, conventional and sonic activated irrigation during root canal treatment. Int Endod J, 2013;46:339-347.
5. Alfredo E, Marchesan MA, Sousa-Neto MD, Brugnera-Junior A, Silva-Sousa YT. Temperature variation at the external root surface during 980-nm diode laser irradiation in the root canal. J Dent, 2008;36:529-534.
6. da Costa Ribeiro A, Nogueira GE, Antoniazzi JH, Moritz A, Zezell DM. Effects of diode laser (810 nm) irradiation on root canal walls: thermographic and morphological studies. J Endod, 2007;33:252-255.
7. Machida T, Wilder-Smith P, Arrastia AM, Liaw LH, Berns MW. Root canal preparation using the second harmonic KTP:YAG laser: a thermographic and scanning electron microscopic study. J Endod, 1995;21:88-91.
8. Nammour S, Kowaly K, Powell GL, Van Reck J, Rocca JP. External temperature during KTP-Nd:YAG laser irradiation in root canals: an in vitro study. Lasers Med Sci, 2004;19:27-32.
9. Berutti E, Marini R, Angeretti A. Penetration ability of different irrigants into dentinal tubules. J Endod, 1997;23:725-727.
10. Kouchi Y, Ninomiya J, Yasuda H, Fukui K, Moriyama T, Okamoto H. Location of Streptococcus mutans in the dentinal tubules of open infected root canals. J Dent Res, 1980;59:2038-2046.
11. Schoop U, Kluger W, Dervisbegovic S, Goharkhay K, Wernisch J, Georgopoulos A et al. Innovative wavelengths in endodontic treatment. Lasers Surg Med, 2006;38:624-630.
12. Schoop U, Kluger W, Moritz A, Nedjelik N, Georgopoulos A, Sperr W. Bactericidal effect of different laser systems in the deep layers of dentin. Lasers Surg Med, 2004;35:111-116.
13. Eriksson AR, Albrektsson T. Temperature threshold levels for heat-induced bone tissue injury: a vital-microscopic study in the rabbit. J Prosthet Dent, 1983;50:101-107.
14. Hmud R, Kahler WA, Walsh LJ. Temperature changes accompanying near infrared diode laser endodontic treatment of wet canals. J Endod, 2010;36:908-911.
15. Hmud R, Kahler WA, George R, Walsh LJ. Cavitational effects in aqueous endodontic irrigants generated by near-infrared lasers. J Endod, 2010;36:275-278.
16. Beer F, Buchmair A, Wernisch J, Georgopoulos A, Moritz A. Comparison of two diode lasers on bactericidity in root canals--an in vitro study. Lasers Med Sci, 2012;27:361-364.
17. Kreisler M, Kohnen W, Beck M, Al Haj H, Christoffers AB, Götz H et al. Efficacy of NaOCl/H2O2 irrigation and GaAlAs laser in decontamination of root canals in vitro. Lasers Surg Med, 2003;32:189-196.
Received on May 10, 2017.Revised on Jun 1, 2017.Accepted on Jun 11, 2017.
Correspondence:
Dijana Trišić Clinic for Paediatric and Preventive Dentistry Faculty of Dental Medicine, University of Belgrade e-mail: [email protected]
In our study, 940 nm laser with output powers of 1 W and 2 W, in continuous mode, remained in the safe limit through three irradiation cycles. Contrary to these results, 975 nm laser came into the safe zone after two irradiation cycles at output power of 1 W, and only after first irradiation cycle for output power of 2 W. Hmud et al.14 found statistically significant higher increase of temperature on external root surface at apical third when 980 nm laser was used, in comparison to 940 nm laser, which is consistent with our results. These results could be explained by the stronger absorption of the 980 nm wavelength in water15. Also, in the study of Alfredo et al.5 with 980 nm diode laser in CW, they concluded that during one cycle of irradiation at higher power rate, rising of temperature over safe limit occurred.
The previous study, conducted in dry root canals, suggested 20 seconds of resting time between irradiation cycles, to provide time for the temperature to came into the safe limit6. Since irradiation of root canals for antimicrobial effect is recommended to be provided in cycles16,17, we investigated the variation of temperature during three irradiation cycles followed by 20 seconds of rest after each cycle. The resting periods allowed temperature decrease at the external root surface in all experimental groups. For 940 nm laser resting periods were long enough to provide safe roots irradiation through all irradiation cycles, with both power rates. For 975 nm laser, temperature decrease during resting periods was significant. Unfortunately, at a higher power rate of 975 nm diode laser, resting periods were not long enough to decrease temperature into the safe limit. A new protocol for irradiation with 975 nm laser should be provided, for safe endodontic usage, since the antimicrobial effect is more efficient at higher power rates17.
Conclusions
The results of this in vitro study showed that three cycles irradiation of 940 nm diode laser, with following resting periods of 20 seconds, allowed safe usage of 1 W and 2 W in CW for endodontic treatment. For 975 nm laser application at 1 W in CW, during the last resting period temperature drop near safe limit and came into the safe zone under the minute. At the power of 2 W of the 975 nm laser, resting periods were not long enough for ∆T to decrease into the safe limit.
Note: The results of this paper were awarded for the oral presentation at the 22nd BaSS Congress.
References
1. Nair PN. Pathogenesis of apical periodontitis and the causes of endodontic failures. Crit Rev Oral Biol Med, 2004;15:348-381.

SUMMARYBackground/Aim: In the pathogenesis of odontogenic tumors which
arise from the rests of the dental apparatus in the jaw, several molecular pathways have been shown to play critical roles such as genetic alterations in the hedgehog, BRAF/Ras/MAPK, epidermal growth factor receptor. Next generation genomic sequencing has identified gene mutations in many different tumors. Materials and Methods: Here we report four types of odontogenic tumor including six cases in which five had mutation according to next generation sequencing analysis from archival paraffin blocks that diagnosed previously as ameloblastoma (solid), amloblastoma (unicystic-mural), ameloblastic fibroma, squamous odontogenic tumor, and adenomatoid odontogenic tumor. Results: All ameloblastomatic tumors were shown BRAF mutation and adenomatoid odontogenic tumors were KRAS mutation. Conclusion: This evidence may highlight the poorly understood pathogenesis of odontogenic tumors. Further comparisons need to be made with other benign and malignant odontogenic tumors so that unique odontogenic features may be found.Key words: Odontogenic Tumors, Next Generation Sequencing, Mutation
Sibel Elif Gültekin1, Burcu Sengüven1, Reem Aziz2, Carina Heydt2, Reinhard Buettner2
1 Gazi University Faculty of Dentistry Department of Oral Pathology, Ankara-Turkey 2 University of Cologne, Faculty of Medicine, Department of Pathology, Cologne-Germany
ORIGINAL PAPER (OP)Balk J Dent Med, 112-115
BALKAN JOURNAL OF DENTAL MEDICINE ISSN 2335-0245
Molecular Profiling of Odontogenic Tumors - Pilot Study
STOMATOLOGICA
L S
OC
IET
Y
Introduction
Odontogenic tumors represent a spectrum of lesions ranging from malignant and benign neoplasms to dental hamartomas, all arising from epithelial or mesenchymal cells of the dental apparatus in the jaw or oral mucosa. Odontogenic tumors may pose both diagnostic and prognostic challenges due to overlapping histology and high propensity for local recurrence of some of them, even they are considered as benign1.
Current treatment options for odontogenic tumors include both conservative treatment (enucleation or curettage) and resection. The former is associated with high rates of recurrence, while the latter results in significant facial deformity and morbidity. Moreover, patients with some odontogenic tumors such as ameloblastoma, should be followed up for a lifetime due to unpredictable biological behavior of the tumor1,2.
Development of non-invasive therapies has been precluded by a lack of understanding of the molecular background of odontogenic tumors pathogenesis. A
number of molecular pathways have been shown to play critical roles in the pathogenesis of them. Its frequent association with a wide spectrum of mutations in genes encoding various signal transducers are often linked to therapy response leads developing of molecular profiling analysis2-5.
The term molecular profiling is used to collectively describe molecular approaches that concomitantly measure the expression of multiple genes on tissue or other biological samples. Next generation genomic sequencing (NGS) is the comprehensive molecular profiling method, which has identified gene mutations or single nucleotide polymorphisms associated with many of the tumors. The NGS based genetic alteration analyses remain open area of investigation for odontogenic tumors and may need to be identified for potential future tailored treatment approach5,6.
The main objectives of this study is to identify a comprehensive molecular profiling of benign odontogenic tumors and to analyze their association with clinical parameters.
10.1515/bjdm-2017-0017

17 melanoma relevant genes, and the GeneRead DNAseq Panel PCR Kit V2 (Qiagen) according to the GeneRead DNASeq Gene Panel Handbook (Qiagen). These two panels comprise a subset of cancer relevant genes including: ARAF, BRAF, CDK4, CDKN2A, CTNNB1, DDR2, EGFR, ERBB2, FGFR2, FGFR3, GNA11, GNAQ, HRAS, IDH1, KEAP1, KIT, KNSTRN, KRAS, MAP2K1, MET, NFE2L2, NRAS, OXA1L, PDGFRA, PIK3CA, PTEN, RAC1 and TP53.
Libraries were constructed using the Gene Read DNA Library I Core Kit and the Gene Read DNA I Amp Kit (Qiagen). After End-Repair and adenylation, NEXTflex DNA Barcodes were ligated (Bio Scientific, Austin, TX, USA). Library products were quantified with Qubit dsDNA HS Assay Kit (Thermo Fisher Scientific, Waltham, MA, USA) on the Qubit 2.0 Fluorometer (Thermo Fisher Scientific), diluted and pooled in equal amounts. Finally, 12 pM of the constructed libraries were sequenced on the MiSeq (Illumina, San Diego, CA, USA) with a MiSeq reagent kit V2 (300-cycles) (Illumina) following the manufacturer’s recommendations.
Data were exported as FASTQ files. Alignment and annotation was done using a modified version of a previously described method.7 BAM files were visualized in the Integrative Genomics Viewer (http://www.broadinstitute.org/igv/, Cambridge; USA). A 5% cutoff for variant calls was used and results were only interpreted if the coverage was >200x.
Results
Table 1 shows the demographic, histologic and genomic data of the cases. The distribution of the tumors are as follows: two adenomatoid odontogenic tumors (AOT), two ameloblastomas, one ameloblastic fibroma (AF) and one squamous odontogenic tumor (SOT) (Figure 1).
Materials and Methods
Sample selectionThe study was conducted on previously diagnosed
six odontogenic tumor specimens from the archives of paraffin-embedded diagnostic tissues of Department of Oral Pathology, Faculty of Dentistry, Gazi University, Ankara, Turkey.
The reevaluation and reclassification was done by an oral pathologist on hematoxylin-eosin (H&E) stained slides under light microscope according to World Health Organization (WHO) classifiaction1.
The data regarding age, gender and localization was recorded. The study protocol was approved by the institutional review board of the Faculty of Dentistry at the Gazi University, Ankara and Faculty of Medicine at Cologne University.
Molecular analysisA total of six tumor samples were sequenced at the
molecular pathology laboratory of Institute for Pathology University Cologne Cologne Germany, using the Ion Torrent PGM and the 30 gene AmpliSeq Library Kit from 10ng of extracted DNA.
Six sections of 10-μm thickness were cut from FFPE tissue blocks. Sections were deparaffinised and the tumor areas were macrodissected from unstained slides using a marked H&E stained slide as a reference. After proteinase K digestion, the DNA was isolated with the Maxwell® 16 FFPE Plus Tissue LEV DNA Purification Kit (Promega, Mannheim, Germany) on the Maxwell® 16 (Promega) following manufacturer’s instructions. The DNA content was measured using a real-time qPCR-based method.
For multiplex PCR-based target enrichment, the isolated DNA (10 ng each) was amplified with two customized GeneRead DNAseq Targeted Panel V2 (Qiagen, Hilden, Germany), targeting 17 lung cancer and
Case # Diagnosis Age Sex Site Mutation Size Teeth relation
1 AOT 33 M Right-both KRAS 6.5x4.5x0.5 cm Yes
2 AOT 23 F Anterior KRAS 1.5x1.2x1 cm No
3 SOT 56 M Right- posterior Unavailable 2x1x1 cm No
4 AF 15 F Left-posterior gingiva BRAF 4x3x2cm Yes
5 Ameloblastoma (Solid) 68 M Anterior BRAF 4.3x2.2x2 cm No
6 Ameloblastoma (Unicystic mural) 29 F Left-posterior BRAF 3.4x2.8x2.5 cm Yes
Balk J Dent Med, Vol 21, 2017 Odontogenic Tumors 113

114 Sibel Elif Gültekin et al. Balk J Dent Med, Vol 21, 2017
Figure 1. A) Hyperchromatic columnar cells with adenomatoid arrangements in adenomatoid odontogenic tumor (Hematoxylin and
eosin, x200). B) Follicular ameloblastoma with palisading basal cells and stellate reticulum like cells (Hematoxylin and eosin, x100). C)
Cellular loose connective tissue with islands of odontogenic epithelial in ameloblastic fibroma (Hematoxylin and eosin, x40). D) Squamous
odontogenic tumor exhibiting typical epithelial islands in fibrous stroma (Hematoxylin and eosin, x100).
The mean age of the patients was 37.3 and gender distribution was equal. All the tumors located in mandible. AOT cases were located in the anterior, other tumors mostly located at the posterior of the mandible. Half of the tumors (three out of six) had relation with the unerrupted teeth (Figure 2).
Figure 2. The unicystic ameloblastoma case had the relation with unerrupted third molar.
The total five out of six cases were performed comprehensive analysis by NGS. In one case sequence analysis failed due to massive degradation of DNA. Mutations were identified in all five odontogenic tumors. Two types of gene mutation were detected; BRAF V600E was seen in ameloblastoma and ameloblastic fibroma, both AOT cases showed KRAS mutations. The age of the patients with BRAF mutated tumors are higher (mean: 37.3) than KRAS mutated ones (mean:28).
Discussion
Odontogenic tumors are relatively rare tumors with challenging diagnosis and prognosis. The clinical course, imaging technique and both histological and immunohistochemical evaluations have defined the correct diagnosis of odontogenic tumors in the past. The practice of pathology is currently undergoing significant change, due to advances in the field of molecular pathology. In recent couple of years, an emerging technology- molecular genomic profiling by means of NGS- may provide clinicians with an additional tool to understand, better classify and develop new treatment modalities of the odontogenic tumors. In the present study NGS technologies has allowed us to generate a comprehensive molecular profiling of six benign odontogenic tumors, which adds additional new information to the field, limited with five studies since 20142-5,8.
The results of the study displayed BRAF (V600E) or KRAS mutations in all of the sequenced tumors. BRAF mutations were found in two ameloblastoma and one ameloblastic fibroma cases. BRAF is a potent activator of the mitogen activated protein kinase (MAPK) cascade, which is capable to induce proliferation and to promote proliferation. Our findings are in concordance with the studies, which showed the high frequency of driver mutation in BRAF in the ameloblastomas2-6. In our knowledge, the present study is the second research that showed the BRAF mutation in ameloblastic fibroma. Previously, Brown et al., who performed the molecular analysis in two ameloblastic fibromas, identified it3. Depending these findings, we may speculate that this tumor is pathogenetically associated to the amaloblastoma and moreover, it may represent the early phase of the ameloblastoma. Ameloblastic fibromas are generally found in younger age group and exhibit less aggressive behavior. On the other hand, these tumors are histologically very similar to conventional ameloblastoma1. Overall, these findings suggest that ameloblastic tumors may be a distinct group of odontogenic tumors with the common genetic alterations8,9. This may give rise to use BRAF mutations as a potential diagnostic marker for ameloblastic odontogenic tumors.
The other notable finding of our study is, both AOT cases displayed KRAS mutation. KRAS, is one of the oncogene belongs to the RAS protein family which activates the BRAF protein and is commonly mutated in cancers10. There has been limited studies that utilized deep sequencing analysis on odontogenic tumors which were mostly focused on amelobalstomas. Only one study reported KRAS mutation in the seven out of nine AOT cases11. These findings reveal that MAPK pathway plays critical role in the development of benign odontogenic tumors.

Balk J Dent Med, Vol 21, 2017 Odontogenic Tumors 115
5. Brown NA, Betz BL. Ameloblastoma: A Review of Recent Molecular Pathogenetic Discoveries. Biomark Cancer, 2015;7:19-24.
6. Heikinheimo K, Kurppa KJ, Elenius K. Novel Targets for the Treatment of Ameloblastoma. J Dent Res, 2015;94:237-240.
7. Peifer M, Fernández-Cuesta L, Sos ML, George J, Seidel D, Kasper LH et al. Integrative genome analyses identify key somatic driver mutations of small-cell lung cancer. Nat Genet, 2012;44:1104-1110.
8. Gomes CC, Diniz MG, Gomez RS. Progress towards personalized medicine for ameloblastoma. Comment on J Pathol, 2014;232:492-498.
9. Oikonomou E, Koustas E, Goulielmaki M, Pintzas A. BRAF vs RAS oncogenes: are mutations of the same pathway equal? differential signalling and therapeutic implications. Oncotarget, 2014;5:11752-1177.
10. Gomes CC, de Sousa SF, de Menezes GH, Duarte AP, Pereira Tdos S, Moreira RG et al. Recurrent KRAS G12V pathogenic mutation in adenomatoid odontogenic tumours. Oral Oncol, 2016;56:e3-5.
11. Bos JL. Ras oncogenes in human cancer: a review. Cancer Res, 1989;49:4682-4689.
Received on March 15, 2017.Revised on May 2, 2017.Accepted on May 29, 2017.
Correspondence:
Sibel Elif Gültekin Department of Oral Pathology Gazi University Faculty of Dentistry, Ankara-Turkey e-mail: [email protected]
Conclusion
In conclusion, we have performed a comprehensive molecular profiling of benign odontogenic tumors in order to identify novel genomic alterations that will led to recognition of molecular classification and influence the new therapeutic approaches. However, a similar study design should be applied to a larger and more varied group of odontogenic tumors to confirm the present results, and further comparisons need to be made with other malignant tumors so that unique odontogenic features may be found.
Note: The results of this paper were presented as a part of an invited lecture at the 22nd BaSS Congress.
References
1. Barnes L, Eveson JW, Reichart P, Sidransky D. World Health Organization Classification of Tumors. Pathology and Genetics. Head and Neck Tumours. Lyon: IARC Press; 2005.
2. Kurppa KJ, Caton J, Morgan RP, Ristimaki A, Ruhin B, Kelloski J et al. High Frequency of BRAF V600E mutations in aamelobastoma. J Pathol, 2014;232:492-498.
3. Brown NA, Rolland D, McHugh JB, Weigelin HC, Zhao L, Lim MS et al. Activating FGFR2-RAS-BRAF mutations in ameloblastoma. Clin Cancer Res, 2014;205517-5526.
4. Sweeney RT, McClary AC, Myers BR, Biscocho J, Neahring L, Kwei KA et al. Identification of recurrent SMO and BRAF mutations in ameloblastomas. Nat Genet, 2014;46:722-725.

SUMMARYBackground/Aim: The present analysis focuses on examining a case
series of eight patients diagnosed with a granular cell tumor located in the oral cavity. Case series: The patients’ clinical states were thoroughly studied, along with the histopathological and immunohistochemical examinations findings. Their surgical treatment and postoperative course are also within the scope of this analysis. Numerous histogenesis theories and the appropriate tumor treatment are mentioned within the article being always in accordance with the relative literature. Conclusions: Oral granular cell tumor is a benign oral disease of possible neural origin commonly located on the tongue. Surgical excision is the treatment of choice. In any case, histological and immunohistochemical examination confirm both the clinical diagnosis and the differential diagnosis between oral squamous cell carcinoma.Key words: Neurological Origin Oral Tumor, Oral Granular Cell Tumor, Tongue Soft Tumor
Panayiotis Karakostas, Apostolos Matiakis, Eleftherios Anagnostou, Alexandros Kolokotronis
Department of Oral Medicine and Pathology, School of Dentistry of Aristotle University of Thessaloniki, Greece
CASE REPORT (CR)Balk J Dent Med, 116-118
BALKAN JOURNAL OF DENTAL MEDICINE ISSN 2335-0245
Oral Granular Cell Tumor: Report of Case Series and a Brief Review of the Literature
STOMATOLOGICA
L S
OC
IET
Y
Introduction
The granular cell tumor (GCT) appears to be a benign neoplasm, probably of neural origin, which is usually located in the head and neck area (45% to 65% of the cases)1. Among the above, 70% of lesions are located intraorally and merely 2% of all GCTs turn out to be malignant2,3,4. A slight female prevalence is noted, especially between the third and the fourth decade of life5.
That lesion was first described by Arbikossoff in 1926, stating that the granular cells of the tumor derive from the skeletal muscles and consequently was termed myovlastoma3,5. Other theories of histogenesis claim that GCT derives from neurons, fibroblasts, mast cells and myoepithelial cells6. Furthermore, a number of authors have correlated regenerative changes and proliferation after injury with the morphogenesis of the GCT6. According to the prevailing theory, the oral GCT derives from cells of the neural tissue, and more specifically from the Schwann cells6,7,8. In support of the last theory, the GCT is positive to the S-100 protein during the immunohistochemical examination, just as in our case7,8.
In this paper, we report a case series of 8 patients, who were examined in our clinic from 2001 to 2016.
Cases series
Table 1. Main characteristics of our GCT cases.
Age (in years) Sex Location Clinical features
Case 1 7 Female Dorsum of the tongue
4 mm diameter, perceptible 4
months
Case 2 55 MaleMiddle third of the right side of
the tongue
1 cm diameter, perceptible 10
years
Case 3 68 FemaleIn the middle of
the dorsum of the tongue
Not reported
Case 4 21 FemaleIn the middle of the right edge of
the tongue0,5 cm diameter
Case 5 60 Female Top of the tongue 0,5 cm diameterCase 6 49 Female Left upper lip 0,5 cm diameter
Case 7 60 FemaleIn the middle of
the dorsum of the tongue
0,8 cm diameter, perceptible 6
months
Case 8 59 MaleIn the middle of
the dorsum of the tongue
0,6 cm diameter, perceptible 6
months, HIV+
10.1515/bjdm-2017- 0018

The following case reports are briefly described also in Table 1. Surgical excision was the treatment of choice in all cases, presenting no recurrence. Histological examination revealed GCT.
Case 1A 7-years-old girl was treated for a swelling located
at the dorsum of the tongue. The swelling had a diameter of 4 mm and was being noticed 4 months before the examination.
Case 2A 55-years-old male patient proceeded to our clinic
for a sessile overgrowth on the middle third of the right side of his tongue (Figure 1). The lesion had a diameter of 1cm and was being noticed 10 years before the examination.
Figure 1. Initial clinical appearance of case 2
Case 3A 68-years-old female patient was diagnosed with
a sessile overgrowth in the middle of the dorsum of the tongue. Further details concerning clinical characteristics of the lesion, as well as the time it appeared, were not recorded.
Case 4A 21-years-old female patient was examined in our
clinic and a 0,5 cm in diameter tumor-like lesion was detected in the middle of the right edge of her tongue.
Case 5A 60-years-old female patient was examined for a 0,5
cm swelling on the top of her tongue. Besides histological examination, the immunohistochemical examination revealed positivity for the S-100 protein.
Case 6A 49-years-old female patient was examined and a
swelling of 0,5 cm in diameter was detected, located at the left upper lip.
Case 7A 60-years-old female patient visited our clinic for
a 0,8 cm in diameter tumor-like lesion, located in the middle of the dorsum of the tongue (Figure 2). The patient had noticed the swelling 6 months before the examination.
Figure 2. Initial clinical appearance of case 7
Case 8A 59-years-old male patient was diagnosed with a
GCT, found in the middle of the dorsum of the tongue. The tumor had a diameter of 0,6 cm. He had noticed the tumor 6 months before the examination (Figure 3). The patient also reported that he was HIV- positive.
Figure 3. Initial clinical appearance of case 8
Discussion
Eight cases of oral GCT have been described. Seven of them were located on the tongue and one at the lip. The patients’ age ranged from 7 to 60 years old. A clear female prevalence is evident since six out of eight patients were women (75%).
The oral GCT occurs at any age, although it is mainly detected in patients aged between 30 and 40 years old3,4. The tumor might be located on any site of the oral mucosa, but the most frequent location is on the tongue, which is also confirmed by the description of our cases (87,5%)7,9.
In the case of oral GCT being reported in infants, especially in girls’ alveolar appendix, it is called congenital epulis10, 11.
The unique treatment of choice is the surgical excision of the lesion1. No recurrence is observed as long as the lesion has been surgically removed in toto6.
The clinical examination leads to the diagnosis of the oral GCT5. However, the latter should be confirmed by the histological examination (Figure 4 & 5). The epithelium cove ring the tumor might possibly present a pseudoepi-theliomatus hyperplasia, resulting in a misdiagnosis of an oral squamous cell carcinoma3,5. The close and substantial
Balk J Dent Med, Vol 21, 2017 Oral Granular Cell Tumor 117

118 Panayiotis Karakostas et al. Balk J Dent Med, Vol 21, 2017
misdiagnosing the oral GCT as an oral squamous cell carcinoma.
Note: The results of this paper were presented as a part of an invited lecture at the 22nd BaSS Congress.
References
1. Collins BM, Jones AC. Multiple granular cell tumors of the oral cavity: report of a case and review of the literature. J Oral Maxillofac Surg, 1995;53:707-711.
2. Gomes CC, Fonseca-Silva T, Gomez RS. Evidence for loss of heterozygosity (LOH) at chromosomes 9p and 17p in oral granular cell tumors: a pilot study. Orl Surg Oral Med Oral Pathol Oral Radiol, 2013;115:249-253.
3. Cole E, Rahman N, Webb R. Case series: two cases of an atypical presentation of oral granular cell tumour. Case Rep Med, 2012;2012.
4. Gayen T, Das A, Shome K, Bandyopadhyay D, Das D, Saha A. Granular cell tumor: An uncommon benign neoplasm. Indian J Dermatol, 2015;60:322.
5. Suchitra G, Tambekar KN, Gopal KP. Abrikossoff’s tumor of tongue: Report of an uncommon lesion. J Oral Maxillofac Pathol, 2014;18:134-136.
6. Suzuki S, Uchida K, Harada T, Nibe K, Yamashita M, Ono K et al: The origin and role of autophagy in the formation of cytoplasmic granules in canine lingual granular cell tumors. Vet Pathol, 2015;52:456-464.
7. Alotaibi O, Al Sheddi M. Neurogenic tumors and tumor-like lesions of the oral and maxillofacial region: A clinicopathological study. Saudi Dent J, 2016;28:76-79.
8. Kaiserling E, Ruck P,Xiao JC, Congenital epulis and granular cell tumor: a histologic and immunohistochemical study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod, 1995;80:687-697.
9. Al-Eryani K, Karasneh J, Sedghizadeh PP, Ram S, Sawair F. Lack of Utility of Cytokeratins in Differentiating Pseudocarcinomatous Hyperplasia of Granular Cell Tumors from Oral Squamous Cell Carcinoma. Asian Pac J Cancer Prev, 2015;17:1785-1787.
10. Kumar R, Jaiswal S, Singhal A, Garg R. Congenital granular cell lesion: A rare tumor of new born. J Oral Maxillofac Pathol, 2013;17:440-442.
11. Yıldırım C, Zerener T, Şençimen M, Akgün ÖM, Altuğ HA, Çiçek AF. Congenital Gingival Granular Cell Tumor: A Case Report. J Dent (Shiraz), 2017;18:70-72.
12. Ferreira JC, Oton-Leite AF, Guidi R, Mendonça EF. Granular cell tumor mimicking a squamous cell carcinoma of the tongue: a case report. BMC Res Notes, 2017;10:14.
Received on May 6, 2017.Revised on Jun 7, 2017.Accepted on Jun 12, 2017.
Correspondence:
Apostolos Matiakis Department of Oral Medicine and Pathology School of Dentistry, Aristotle University of Thessaloniki, Greece e-mail: [email protected]
cooperation between an expert pathologist and a clinician is of great importance, in order to avoid any misdiagnosis12. Besides the histological examination, the immunohistochem-ical examination declares the positivity of the tumor for the S-100 protein, validating its neural origin (Figure 6).
Figure 4. Granular Cell Tumor. The epithelium is overlying the tumor giving a severe pseudoepitheliomatus hyperplasia appearance which
could be mistaken for a squamus cell carcinoma (H-E x100)
Figure 5. Granular Cell Tumor. The cells are characterized by ovular nuclei without atypia and abundant granular eosinophilic cytoplasm
(H-E x400)
Figure 6. Immunohistochemistry positive for S-100 protein (magnification x400)
Conclusions
The GCT of the oral cavity is a rare benign tumor, mostly developing on the tongue. The surgical excision constitutes the treatment of choice. The histological as well the immunohistochemical examination confirms the diagnosis. As mentioned above the histological examination should be conducted carefully, especially in the presence of pseudoepitheliomatus hyperplasia, in order to avoid

SUMMARYBackground: Myeloid sarcoma (MS) is a solid malignant tumour
associated with infiltration of immature myeloid precursor cells in an extramedullary site. The term MS has replaced the term granulocytic sarcoma and chloroma, which were used in the past. MS in the oral cavity is very uncommon, with less of 40 cases reported until recently. Case Report: We report the first case, the features, and the diagnostic sequence, of intraoral MS with bilateral palatal involvement, which presented as an initial manifestation, and preceded the appearance of acute myeloid leukaemia (AML). Diagnostic confirmation of such oral mucosal lesions usually requires biopsy, histopathological examination with additional immunohistochemical investigation. MS can occur during the course of acute or chronic myelogenous leukaemia, and myelodysplastic syndromes. In the vast majority of the reported cases, only one site was involved with a single intraoral MS lesion, and the cases predominantly associated with AML. Conclusion: The majority of intraoral MS occurs in patients with known AML, but in some of them, presented as an initial manifestation, and preceded the appearance of the disease. Therefore, clinicians should carefully evaluate all unusual oral lesions of unknown origin.Key words: Myeloid sarcoma, Granulocytic sarcoma, Chloroma, Acute myeloid leukaemia, Oral tumours
Athanasios Poulopoulos1, Fotios Iordanidis2, Dimitrios Andreadis1, Konstantinos Antoniadis3
1 Department of Oral Medicine & Oral Pathology Dental School, Aristotle University of Thessaloniki Thessaloniki, Greece 2 Gloucestershire Cellular Pathology Laboratory Cheltenham General Hospital Cheltenham, United Kingdom 3 Department of Oral & Maxillofacial Surgery Dental School, Aristotle University of Thessaloniki Thessaloniki, Greece
CASE REPORT (CR)Balk J Dent Med, 119-122
BALKAN JOURNAL OF DENTAL MEDICINE ISSN 2335-0245
Intraoral Myeloid Sarcoma with Bilateral Involvement - Case Report
STOMATOLOGICA
L S
OC
IET
Y
Introduction
Myeloid sarcoma (MS) is a solid malignant tumour associated with infiltration of immature myeloid precursor cells in an extramedullary site1. The term MS has replaced the term granulocytic sarcoma and chloroma, which were used in the past2.
MS in the oral cavity is very uncommon with less of 40 cases reported between 1883 and 20141. MS can occur during the course of acute or chronic myeloid leukaemia, and myelodysplastic syndromes. In the vast majority of the reported cases, only one site was involved with a single intraoral MS lesion, and the cases predominantly associated with acute myeloid leukaemia (AML)3. Rarely, MS is possible to appear months before the AML manifests, during the course of the illness or represent a leukaemia relapse or remission4.
The involvement sites of MS are highly variable and has been reported to affect the skin, bones, upper respiratory tract, and gastrointestinal tract including the oral cavity3,5. Furthermore it has been reported that in 16% of MS cases were diagnosed in the head and neck region, although intraoral MS rarely occurs6.
We report the first case, the features, and the diagnostic sequence, of intraoral MS with bilateral palatal involvement, which presented as an initial manifestation, and preceded the appearance of the AML.
Patient Presentation
A 28 year old female was referred by her dentist to our clinic for investigation of a fast growing lesion with bilateral maxillary involvement and protrusion to the
10.1515/bjdm-2017-0020

120 Athanasios Poulopoulos et al. Balk J Dent Med
activity. Additional immunohistochemical staining was performed on paraffin sections (Fig. 3) and showed that the cells were positive for MPO (myeloperoxidase), LCA (leukocyte common antigen /CD 45), CD 68, CD 11c, and CD, 4 but negative for CD 7, CD 3, CD 20, CD 56, CD 34, CD 117, and Tdt (terminal deoxynucleotidyl transferase).
palate for both sides. She had been aware of the lesion for at least five weeks, and was experiencing increasing oral discomfort without pain. The medical history was non-contributory. Before the onset of the oral lesion, the patient did not experience any symptoms suggestive of any systemic abnormalities. There was no history of trauma or dental manipulation related to the site of the lesion.
The intraoral clinical examination revealed two painless sessile, soft in palpation, masses, 2cm in maximum dimension, with identical clinical appearance and location, with no colour changes. Furthermore, there was obvious palatal protrusion of both masses in the first and second molar area (Fig. 1). There were no odontogenic sources or other associated intraoral lesions. Plain radiographs and a computed tomography scan failed to show underlying bone erosion. In addition, the patient performed full blood investigations two months ago, which were ranged within the normal values.
Figure 1. Intraoral myeloid sarcoma with bilateral palatal involvement in the first and second upper molar area
An incisional biopsy was performed, and the microscopic findings of haematoxylin & eosin (H&E) staining demonstrated oral mucosa covered by stratified epithelium; in the underlying corium a cellular proliferation was observed with diffuse and dense infiltration of relatively big and medium size neoplastic blast-like cells, with scant cytoplasm and round-oval nuclei with finely-dispersed chromatin and small distinct nucleoli (Fig. 2 a-c). Furthermore, in the neoplastic cells was observed increased polymorphism, atypia and mitotic
Figure 2. Myeloid sarcoma involving lamina propria of the oral mucosa (a - H&E x 100; b - H&E x 200). The neoplastic cells are medium-
sized with scant cytoplasm and round-oval nuclei with finely-dispersed chromatin and small distinct nucleoli (c - H&E x 400)
a b c
Figure 3. Immunohistochemical stain for myeloperoxidase (MPO) was positive in the MS of the oral mucosa (H &MPO staining x 400)
The patient was immediately referred to haematologists/oncologists for evaluation and further examination. Full blood investigation, myelogram, immunophenotype of monocytes and flow cytometry of peripheral blood, established the diagnosis of AML (M5b) and the bilateral intraoral lesions were confirmed as MS. A computed tomography (CT) scan detected no other areas affected by the disease. Further investigations for molecular markers FMS-like tyrosine kinase 3 gene (FLT3) and nucleophosmin 1 gene (NPM1) were negative. The induction therapy consisted of cytarabine (Ara-C 175mg/m2 every 12 hours for 7 days) plus idarubicin (17,5 mg/m2 days 1, 3, 5), followed by high dose cytarabine (Ara-C 3 g/m2 every 12 hours for 3 days) and idarubicin (17,5 mg/m2 for 3days).
The patient after 1 year is currently in good condition with remission of the oral MS. An informed consent was obtained from the patient for the case presentation.

Balk J Dent Med Intraoral Myeloid Sarcoma 121
The prognosis of patients with MS is poor and strictly related to the clinical course of AML14. In patients with known AML at an older age, the appearance of MS is a significant adverse prognostic factor, moreover it has been reported that patients with multiple MS lesions have a shorter survival than those with only one tumor6. The treatment of MS depends on the patient’s medical history and clinical presentation, applying chemotherapy protocols similar to that used for AML10. Systemic chemotherapy and local radiotherapy remain the main treatment modalities, although a uniform treatment protocol for the intraoral MS doesn’t exist2. The use of imatinib mesylate has been proposed as the therapeutic agent of choice for MS in patients with a history of chronic myeloid leukaemia (CML), even if they are free of CML3.
Conclusion
Although the incidence of intraoral MS is rare, its occurrence should not be disregarded. The majority of intraoral MS occurs in patients with known AML, but in some of them, MS may be presented as an initial manifestation, and it may preced the appearance of the disease.
Furthermore, as the survival rates of patients with leukaemias increase, the incidence of rare intraoral tumours, such as MS, may become more common. Therefore, clinicians should carefully evaluate all unusual oral lesions of unknown origin. Diagnostic confirmation of such mucosal lesions usually requires biopsy, histopathological examination with additional immunohistochemical investigations.
References
1. Yap M, Hewson I, McLean C. Oral myeloid sarcoma: two case reports. Aust Dent J, 2014;59:511-515.
2. Papamanthos KM, Kolokotronis EA, Skulakis EH, Fericean AAM, Zorba TM, Matiakis TA. Acute Myeloid Leukaemia Diagnosed by Intra-Oral Myeloid Sarcoma. A Case Report. Head and Neck Pathol, 2010;4:132-135.
3. Xie Z, Zhang F, Song E, Ge W, Zhu F, Hu J. Intraoral granulocytic sarcoma presenting as multiple maxillary and mandibular masses: a case report and literature review. Oral Surg Oral Med Oral Pathol Oral Radiol Endod, 2007;103: e44-48.
4. Tong AC, Lam KY. Granulocytic sarcoma presenting as an ulcerative mucogingival lesion: Report of a case and review of the literature. J Oral Maxillofac Surg, 2000;58:1055-1058.
5. Carmona IT, Teijeiro JC, Dios PD, Feijoo JF, Posse JL. Intra-alveolar granulocytic sarcoma developing after tooth extraction. Oral Oncol, 2000;36:491-494.
Discussion
The majority of MS cases occur in association with AML or myelodysplastic/myeloproliferative diseases7. The occurrence of intraoral MS as multiple masses involving multiple sites is extremely rare, with only 2 reported cases in the literature3,8. Intraoral MS usually occurs concomitantly with or subsequent to the development of AML; it is most seen in patients with the subtype AML-M1 (myeloblastic leukaemia without maturation) or AML-M2 (myeloblastic leukaemia with maturation)5, whereas rarely, it precedes the appearance of AML as in our case. To our knowledge this is the first case of intraoral MS with bilateral maxillary involvement, which presented as an initial manifestation, and preceded the appearance of the AML.
Most articles reported MS presenting as symptomatic or asymptomatic mass and mucosa ulceration with colour varying among brown, red, black and pale grey9. The differential diagnosis would include benign tumours such as pyogenic granuloma, granulomatous epulis and peripheral giant granuloma, as well as malignant neoplasms such as sarcomas, lymphomas, epidermoid carcinomas and metastasis of other neoplasms10. Diagnosis of intraoral MS may be difficult, especially when it presents as an isolated finding and with no history of haematological disorders or peripheral blood or bone marrow involvement of myeloproliferative disorders. Consequently the diagnosis has clinical relevance because it can be the first sign of an AML. The lesion occurs more often in women; the age of affected patients ranges widely (3 to 89 years)11. The maxillary and mandibular gingivae were the most common sites involved, followed by the palate and very rarely the cheek3.
Histologically, MS usually is characterized by sheets of relatively monomorphic intermediate to large size polyhedral cells with irregular nuclear contours, vesicular chromatin, variably prominent nucleoli, and frequent mitotic figures12. The diagnosis of MS may be complicated by the diversity and inconsistency of its morphologic features and may be misdiagnosed as malignant lymphoma, Ewing’s sarcoma, acute lymphoblastic leukaemia, or other small blue cell tumors10. Therefore additional immunohistochemical studies may help in reaching to a definitive diagnosis because myeloid cells are reactive to antibodies against lysozyme, myeloperoxidase and chloroacetate esterase. Also MS myeloblasts usually express myeloid-associated antigens such as CD43, but are not reactive with lymphoid antigens3. In addition, immunophenotyping with flow cytometry and cytogenetics may contribute to a definitive diagnosis. Furthermore imaging studies with Magnetic Resonance Imaging (MRI) scans of MS exhibit low signal intensity on T2-weighted images, which helps to rule out inflammatory lesions13.

122 Athanasios Poulopoulos et al. Balk J Dent Med
12. Brunning RD, Matutes E, Head D, Flandrin G, Harris NL, Vardiman J. Acute myeloid leukemia not otherwise categorised. In: Tumors of hematopoietic and lymphoid tissues edited by Jaffe ES, Stein H, Vardiman JW. Lyon: IARC Press, 2001; pp. 104-105.
13. Lee SS, Kim HK, Choi SC, Lee JI. Granulocytic sarcoma occurring in the maxillary gingiva demonstrated by magnetic resonance imaging. Oral Surg Oral Med Oral Pathol Oral Radiol Endod, 2001;92:689-693.
14. Srinivasan B, Ethunandan M, Anand R, Hussein K, Ilankovan V. Granulocytic sarcoma of the lips: report of an unusual case. Oral Surg Oral Med Oral Pathol Oral Radiol Endod, 2008;105:e34-36.
Received on May 31, 2016.Revised on August 1, 2016.Accepted on October 2, 2016.
Correspondence:
Athanasios Poulopoulos Dental School, Aristotle University of Thessaloniki Thessaloniki, 54124 Greece E-mail: [email protected]
6. Colella G, Tirelli A, Capone R, Rubini C, Guastafierro S. Myeloid sarcoma occurring in the maxillary gingiva: a case without leukemic manifestations. Int J Hematol, 2005;81:138-141.
7. Breccia M, Mandelli F, Petti MC, D’Andrea M, Pescarmona E, Pileri SA, Carmosino I, Russo E, De Fabritiis P, Alimena G. Clinico-pathological characteristics of myeloid sarcoma at diagnosis and during follow-up: report of 12 cases from a single institution. Leuk Res, 2004;28:1165-1169.
8. Eisenberg E, Peters ES, Krutchkoff DJ. Granulocytic sarcoma (chloroma) of the gingiva: report of a case. J Oral Maxillofac Surg, 1991;49:1346-1350.
9. Koudstaal MJ, van der Wal KGH, Lam KH, Meeuwis CA, Speleman L, Levin MD. Granulocytic sarcoma (chloroma) of the oral cavity: report of a case and literature review. Oral Oncol EXTRA, 2006;42:70-77.
10. Jordan RC, Glenn L, Treseler PA, Regezi JA. Granulocytic sarcoma: case report with an unusual presentation and review of the literature. J Oral Maxillofac Surg, 2002;60:1206-1211.
11. Osterne RLV, Matos-Brito RG, Alves APNN, Nogueira TNAG, Rocha-Filho FD, Meneses FA, Sousa FB. Oral granulocytic sarcoma: a case report. Med Oral Patol Oral Cir Bucal, 2009;14:e232-235.

SUMMARYBackground: Crohn’s disease (CD) and ulcerative colitis (UC) are
the two major relapsing conditions of inflammatory bowel diseases. Case Report: A case of Crohn’s disease with orofacial manifestations in a 10 year old girl is described. She had suffered from fever, dysphagia, arthralgia, painful recurrent ulcers of the oral mucosa and swelling of the lower lip lasting over 6 weeks. Clinical examination and the punch biopsy from the buccal mucosa revealed major recurrent aphthous ulcerations. A partial regression and significant relief of lesions were achieved two weeks after the treatment, but the patient suffered from abdominal pain, irregular bowel movements, arthritis, multiple hyperplastic and swollen mucosal folds, after 3 months. The patient was referred to a pediatric gastroenterologist. Esophagogastroduodenoscopy showed pyloric ulcer formation. Abdominal ultrasound showed increased thickening of the ileal wall with multiple enlarged lympadenopathies in the periileal region. Colonoscopy images showed deep ulcers with surrounding erythema. The histopathological examination of biopsies from the terminal ileum and the colon showed basal plasmacytosis, minimal crypt distortions and aphthous ulcerations. The diagnosis of Orofacial Crohn’s disease was made. Exclusive enteral nutrition for 8 weeks, followed by azathiopurine treatment was started with an excellent clinical response on abdominal and oral symptoms. Conclusion: Diagnosis of the disease by dentists and other clinicians through the evaluation of oral clinical findings is very rare. Mucocutaneous and granulomatous lesions of the oral cavity should alert the clinician to pursue an underlying systemic cause. Early communication with a gastroenterologist can help early diagnosis of Crohn’s disease for better patient management and prognosis.Key words: Crohn’s Disease, Orofacial Granulomatosis, Inflammatory Bowel Disease, Recurrent Aphthous Ulcerations, Oral Lesions
Damla Tuncer Budanur1, Merve Şirin2, Elif Sepet1, Meral Ünür2, Mine Güllüoğlu3, Mustafa Serdar Cantez4, Özlem Durmaz Uğurcan4
Istanbul University 1Faculty of Dentistry, Department of Pediatric Dentistry, 2 Faculty of Dentistry, Department of Oral & Maxillofacial Surgery 3 Istanbul Faculty of Medicine, Department of Pathology 4 Istanbul Faculty of Medicine, Department of Pediatrics, Division of Gastroenterology Hepatology and Nutrition Istanbul, Turkey
CASE REPORT (CR)Balk J Dent Med, 123-126
BALKAN JOURNAL OF DENTAL MEDICINE ISSN 2335-0245
Orofacial Crohn’s disease: a Case Report
STOMATOLOGICA
L S
OC
IET
Y
Introduction
Crohn’s disease (CD) and ulcerative colitis (UC) are the two major relapsing conditions of inflammatory bowel diseases1. CD and UC are considered autoimmune disorders resulting from the interactions of various factors including genetics, environmental factors and immune response2-4.
CD is a chronic inflammation of the intestines and affects any site in the gastrointestinal tract from the
mouth to the anus, specifically localized to the ileocecal region2,5. The most presenting symptoms are abdominal pain, diarrhea, fever, anorexia and weight loss5-7. In addition to the aforementioned symptoms, anemia, skin rashes, arthritis, inflammation of the eye and growth retardation may occur6. Bowel obstruction also commonly occurs and CD patients are at risk of developing dysplasia or adenocarcinoma of the small intestine or colorectal mucosa6,8. Symptoms frequently begin in early adulthood7 and the first peak occurs before the age of 25.
10.1515/bjdm-2017- 0021

124 Damla Tuncer Budanur et al. Balk J Dent Med, Vol 21, 2017
the patient’s history and mucosal biopsy, a diagnosis of Major Recurrent Aphthous Ulcerations (RAU) of the oral mucosa was made. RAU was related with iron deficiency, emotional stress and local trauma. The patient was advised to use a pre-orthodontic trainer appliance. The treatment approach for major apthous ulcers included corticosteroid, analgesic, antibiotic drugs, epithelization agents and mouth rinses. A partial regression and significant relief of lesions were achieved two weeks after the treatment. A recurrence was observed after three months (Figure 2). The patient had history of intermittent abdominal pain, irregular bowel movements and arthritis. Multiple hyperplastic, swollen mucosal folds, forming the Cobblestone appearance of buccal mucosa were present in intraoral examination. The patient was referred to a pediatric gastroenterologist. Crohn’s disease, tuberculosis and sarcoidosis were included in the differential diagnosis. The colonoscopy, endoscopy of the gastrointestinal tract and blood tests were performed.
Oral manifestations of CD patients9 may be present in 8-29%. Orofacial Crohn’s disease (OCD) is a type of CD with specific oral lesions. CD patients may show orofacial signs with mucogingivitis, mucosal tags, oral ulcers, cobblestoning appereance of the cheeks and lip swelling (macrochelia)10. The differential diagnosis of oral manifestations in patients with CD must consider other granulomatous oral disorders. The presence of granulomatous inflammation in the oral mucosal biopsies is the differential marker for diagnosis of OCD11.
We present a 10-year-old girl with orofacial lesions as an initial manifestation of Crohn’s disease. Written informed consent was obtained from the parents of the patient for presenting of this case report and accompanying images.
Case Report
A 10-year-old girl presented with history of fever, dysphagia, arthralgia, painful recurrent oral ulcers, weight loss and swelling of the lower lip lasting over 6 weeks. Her familial history was unremarkable. The parents related the ulcer development with cheek-bite.
On physical examination her body weight was 23 kg (in the 3rd percentile), and height was 131 cm (between the 3rd-10th percentiles).
Clinical examination revealed the presence of painful, big and deep oral ulcers, cheek-bite and enlargement of lower lips (Figure 1). The lymph node examination was unremarkable. Abdominal examination showed no remarkable findings. Anorectal examination of the child showed no skin tags, fistula or fissures.
Figure 1. Clinical examination revealed the presence of painful, big and deep oral ulcers, cheek-bite and enlargement of lower lips
Initial laboratory investigations, including complete blood count, biochemistry profile and autoantibodies showed only mild iron deficiency anemia (hsCRP: 27.58 mg/L, WBC: 14.5 103/µl, HGB: 10.9 g/dL, MCV: 76.3 fL, HBsAg and Anti-HIV: negative).
A punch biopsy from the buccal mucosa was performed. Histopathological examination showed an erosive surface with a dense inflammatory infiltrate composed mainly of polymorphonuclear neutrophils extending into the mucosa and submucosa. Based on
Figure 2. A recurrence was observed after three months. On intraoral examination, multiple hyperplastic, swollen mucosal folds, forming
Cobblestone appearance of buccal mucosa were present
Faecal calprotectin was elevated to 773 µg/g. HsCRP was 27.58 mg/L and blood sedimentation rate was 65 mm/hr. Chest radiograph was normal, with no signs of sarcoidosis or tuberculosis, but the QuantiFERON TB® gold test was positive, showing tuberculosis exposure. Esophagogastroduodenoscopy showed pyloric ulcer formation. Abdominal ultrasound showed increased thickening of the ileal wall with multiple enlarged lympadenopathies in the periileal region. Colonoscopy images showed deep ulcers with surrounding erythema (Figure 3). The histopathological examination of biopsies from the terminal ileum and the colon showed basal plasmacytosis, minimal cyrpt distortions and aphthous ulcerations (Figure 4). The diagnosis of Orofacial Crohn’s disease was made. Exclusive enteral nutrition for 8 weeks followed by azathiopurine treatment was started with an excellent clinical response on abdominal and oral symptoms (Figure 5).
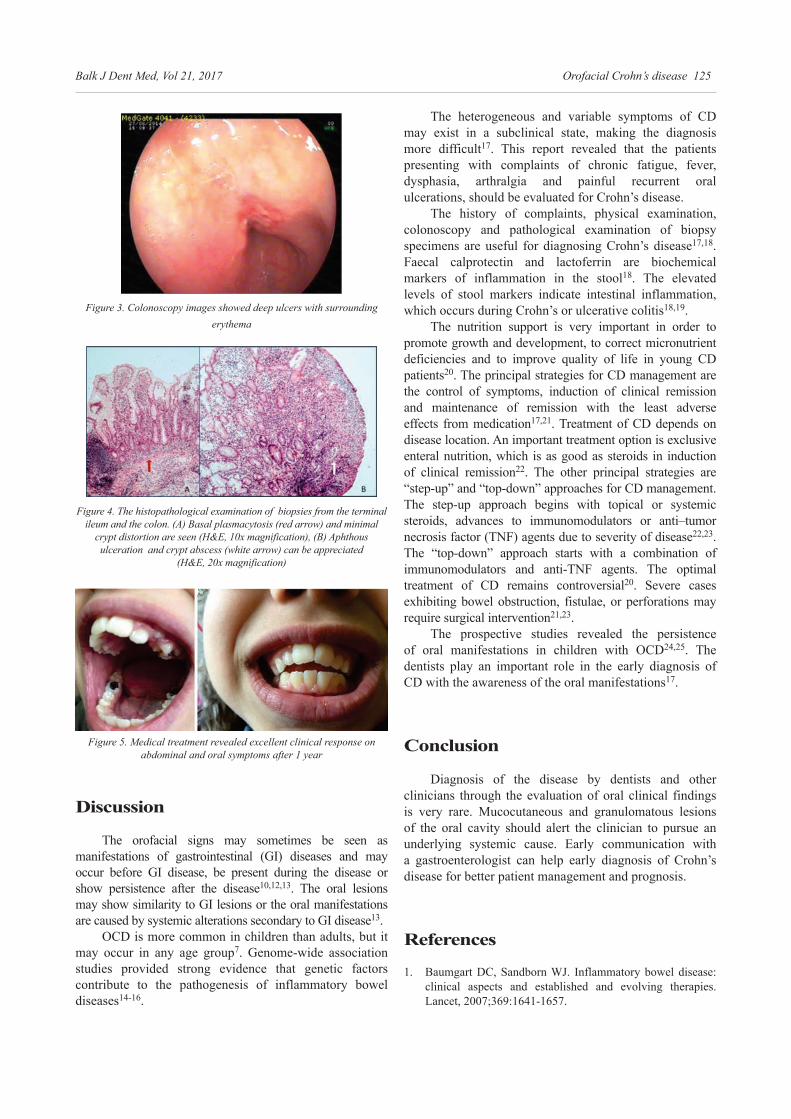
Balk J Dent Med, Vol 21, 2017 Orofacial Crohn’s disease 125
The heterogeneous and variable symptoms of CD may exist in a subclinical state, making the diagnosis more difficult17. This report revealed that the patients presenting with complaints of chronic fatigue, fever, dysphasia, arthralgia and painful recurrent oral ulcerations, should be evaluated for Crohn’s disease.
The history of complaints, physical examination, colonoscopy and pathological examination of biopsy specimens are useful for diagnosing Crohn’s disease17,18. Faecal calprotectin and lactoferrin are biochemical markers of inflammation in the stool18. The elevated levels of stool markers indicate intestinal inflammation, which occurs during Crohn’s or ulcerative colitis18,19.
The nutrition support is very important in order to promote growth and development, to correct micronutrient deficiencies and to improve quality of life in young CD patients20. The principal strategies for CD management are the control of symptoms, induction of clinical remission and maintenance of remission with the least adverse effects from medication17,21. Treatment of CD depends on disease location. An important treatment option is exclusive enteral nutrition, which is as good as steroids in induction of clinical remission22. The other principal strategies are “step-up” and “top-down” approaches for CD management. The step-up approach begins with topical or systemic steroids, advances to immunomodulators or anti–tumor necrosis factor (TNF) agents due to severity of disease22,23. The “top-down” approach starts with a combination of immunomodulators and anti-TNF agents. The optimal treatment of CD remains controversial20. Severe cases exhibiting bowel obstruction, fistulae, or perforations may require surgical intervention21,23.
The prospective studies revealed the persistence of oral manifestations in children with OCD24,25. The dentists play an important role in the early diagnosis of CD with the awareness of the oral manifestations17.
Conclusion
Diagnosis of the disease by dentists and other clinicians through the evaluation of oral clinical findings is very rare. Mucocutaneous and granulomatous lesions of the oral cavity should alert the clinician to pursue an underlying systemic cause. Early communication with a gastroenterologist can help early diagnosis of Crohn’s disease for better patient management and prognosis.
References
1. Baumgart DC, Sandborn WJ. Inflammatory bowel disease: clinical aspects and established and evolving therapies. Lancet, 2007;369:1641-1657.
Figure 3. Colonoscopy images showed deep ulcers with surrounding erythema
Figure 4. The histopathological examination of biopsies from the terminal ileum and the colon. (A) Basal plasmacytosis (red arrow) and minimal
crypt distortion are seen (H&E, 10x magnification), (B) Aphthous ulceration and crypt abscess (white arrow) can be appreciated
(H&E, 20x magnification)
Figure 5. Medical treatment revealed excellent clinical response on abdominal and oral symptoms after 1 year
Discussion
The orofacial signs may sometimes be seen as manifestations of gastrointestinal (GI) diseases and may occur before GI disease, be present during the disease or show persistence after the disease10,12,13. The oral lesions may show similarity to GI lesions or the oral manifestations are caused by systemic alterations secondary to GI disease13.
OCD is more common in children than adults, but it may occur in any age group7. Genome-wide association studies provided strong evidence that genetic factors contribute to the pathogenesis of inflammatory bowel diseases14-16.

126 Damla Tuncer Budanur et al. Balk J Dent Med, Vol 21, 2017
16. Liu JZ, Anderson CA. Genetic studies of Crohn’s disease: Past, present and future. Best Pract Res Clin Gastroenterol, 2014;28:373-386.
17. Stavropoulos F, Katz J, Guelmann M, Bimstein E. Oral Ulcerations as a Sign of Crohn’s Disease in a Pediatric Patient: A Case Report. Pediatr Dent, 2004;26:355-358.
18. Van Rheenen PF, Van de Vijver E, Fidler V. Faecal calprotectin for screening of patients with suspected inflammatory bowel disease: diagnostic meta-analysis. BMJ, 2010;341:c3369.
19. O’Sullivan S, Gilmer JF, Medina C. Matrix Metalloproteinases in Inflammatory Bowel Disease: An Update. Mediat Inflamm, 2015;2015:964131.
20. Gurram B, Joeckel R, Stephens M. Nutrition in pediatric inflammatory bowel disease. Nutr Clin Practice, 2010;25:335-339.
21. Wilkins T, Jarvis K, Patel J. Diagnosis and Management of Crohn’s Disease. Am Fam Physician, 2011;84:1365-1375.
22. Ruemmele F, Veres G, Kolho KL, Levine A, Escher JC. Consensus Guidelines of ECCO/ ESPGHAN on the medical management of pediatric Crohn’s disease. J Crohns Colitis, 2014;8:1179-1207.
23. Boirivant M, Cossu A. Inflammatory bowel disease. Oral Dis, 2012;18:1-15.
24. Harty S, Fleming P, Rowland M, Crushell E, McDermott M, Drumm B et al. A prospective study of the oral manifestations of Crohn’s disease. Clin Gastroenterol Hepatol, 2005;3:886-891.
25. Hussey S, Rowland M, Fleming P. Outcomes of oral Crohn’s disease in children. Can J Gastroenterol, 2007;21:5211.
Received on May 16, 2017.Revised on Jun 6, 2017.Accepted on Jun 12, 2017.
Correspondence:
Elif Sepet Istanbul University, Faculty of Dentistry Pediatric Dentistry DepartmentIstanbul-Turkey e-mail: [email protected]
2. Cho JH, Weaver CT. The genetics of inflammatory bowel disease. Gastroenterol, 2007;133:1327-1339.
3. Baumgart DC, Carding SR. Inflammatory bowel disease: cause and immunobiology. Lancet, 2007;369:1627-1640.
4. Abraham C, Cho JH. Inflammatory bowel disease. N Engl J Med, 2009;361:2066-2078.
5. Crohn’s Disease. National Digestive Diseases Information Clearinghouse (NDDIC) website. Available at: https://www.niddk.nih.gov/ Accessed: 12 June 2014.
6. Baumgart DC, Sandborn WJ. Crohn’s disease. Lancet, 2012;380:1590-1605.
7. Boraz RA. Oral manifestations of Crohn disease: Update of the literature and report of a case. J Dent Child, 1988;55:72-74.
8. Itzkowitz SH. Inflammatory bowel disease and cancer. Gastroenterol Clin North Am, 1997;26:129-139.
9. Lourenço SV, Hussein TP, Bologna SB, Sipahi AM, Nico MM. Oral manifestations of inflammatory bowel disease: a review based on the observation of six cases. J Eur Acad Dermatol Venereol, 2010;24:204-207.
10. Zbar AP, Ben-Horin S, Beer-Gabel M, Eliakim R. Oral Crohn’s disease: is it a separable disease from orofacial granulomatosis? A review. J Crohns Colitis, 2012;6:135-142.
11. Alawi F. Granulomatous diseases of the oral tissues: differential diagnosis and update Dent Clin North Am, 2005;49:203-221.
12. Cosnes J. Tobacco and IBD: Relevance in the understanding of disease mechanisms and clinical practice. Best Pract Res Clin Gastroenterol, 2004;18:481-496.
13. Daley DT, Armstrong JE. Oral manifestations of gastrointestinal diseases. Can J Gastroenterol, 2007;21:241-244.
14. Franke A, McGovern DP, Barrett JC, Wang K, Radford-Smith GL, Ahmad T et al. Genome-wide meta-analysis increases to 71 the number of confirmed Crohn’s disease susceptibility loci. Nat Genet, 2010;42:1118-1125.
15. Lu Z-K, Chen Z-R, Zhu J-Y, Xu Y, Hua X. Analysis of the association of single nucleotide polymorphisms of interleukin-23 receptor (IL-23R) and inflammatory bowel disease in a Chinese Han cohort. Oncotarget, 2016;7:67851-67856.
BALKAN JOURNAL OF DENTAL MEDICINE ISSN 2335-0245
Instructions to the authors
STOMATOLOGICA
L S
OC
IET
Y
Balkan Journal of Dental Medicine (BJDM) publishes only papers not published before, nor submitted to any other journals, in the order determined by the Editorial Board. From March 1, 2017 the BJDM turned to e-Ur: Electronic Journal Editing. All the users of the system: authors, editors and reviewers should be registered at: http://balkandentaljournal.com/ojs/index.php/bjdm
For any assistance, please use the contact: [email protected]. When submitting a paper a statement signed by corresponding author should be enclosed.The BJDM reserves all copyrights for the published papers. Accepted are only papers in English.
The BJDM publishes: reviews/meta-analyses original papers, case reports, short communications and perspective articles.Review papers will be accepted by the Editorial Board only if the authors prove themselves as the experts in the fields they write on by citing not less than 5 selfcitations.Papers should be written on IBM- compatible PC, using 12 pt font, and single spacing, with at least 4 cm left margin. Bold and italic letters should be avoided as reserved for subtitles. Original articles, reviews, meta-analyses and articles from medical history should not exceed 16 pages, case reports 6, short communications 5 and perspective articles 4.All measurements should be reported in the metric system of the International System of Units (SI), and the standard internationally accepted terms (except for mm Hg and °C).MS Word for Windows (97, 2000, XP, 2003) is recommended for word processing; other programs are to be used only exceptionally. Ilustrations should be made using standard Windows programs, Micro-soft Office (Excel, Word Graph). The use of colors and shading in graphs should be avoided.Papers are reviewed anonymously by at least two editors and/or invited reviewers. Remarks and suggestions are sent to the author for final composition. Galley proofs are sent to the corresponding author for final agreement.
Preparation of manuscript
Parts of the manuscript are: Title page (separate file), Summary with Key words, Text, Acknowledgements (to the authors’ desire), References.
Title page1) The title should be concise but informative, while
subheadings should be avoided,2) Full names of the authors, 3) Exact names and places of department(s) and
institution(s) of affiliation where the studies were performed, city and the state for any authors,
4) Data of the corresponding author.
Summary and key wordsThe second page should carry a structured abstract (250-300 words for original articles and meta-analyses) with the title of the article. In short, clear sentences the authors should write the Background/Aim, major procedures – Materials and Methods (choice of subjects or laboratory animals; methods for observation and analysis), the obtained findings – Results (concrete data and their statistical significance), and the Conclusion. It should emphasize new and important aspects of the study or observations. A structured abstract for case reports (up to 250 words) should contain subtitles Introduction, Case report, Conclusion. Below the abstract Key words should provide 3–10 key words or short phrases that indicate the topic of the article according to Index Medicus.
TextThe text of the articles includes: Introduction, Material and Methods, Results, and Discussion. Introduction. After the introductory notes, the aim of the article should be stated in brief (the reasons for the study or observation), only significant data from the literature, but not extensive, detailed consideratuion of the subject, nor data or conclusions from the work being reported.Material and Methods. The selection of study or experimental subjects (patients or experimental animals, including controls) should be clearly described. The methods, apparatus (manufacturer’s name and address in parentheses), and procedures should be identified in sufficient detail to allow other workers to reproduce the results. Also, give references to established methods, including statistical methods. State the approval of the Ethnics Committee for the tests in humans and animals.Results should be presented in logical sequence in the text, tables and illustrations. Emphasize or summarize only important observations.Discussion is to emphasize the new and significant aspects of the study and the conclusions that result from them. Relate the observations to other relevant studies. Link

Balk J Dent Med, Vol 21, 2017
Sternbach RA. Pain patients - traits and treatment. New York, London, Toronto, Sydney, San Francisko: Academic Press; 1974.Koulourides T, Feagin F, Pigman W. Experimental changes in enamel mineral density. In: Harris RS, editor. Art and Science of Dental Caries Research. New York: Academic Press; 1968. p. 355-378.
Journal title abbreviations should be those used by the U.S. National Library of Medicine. If you are uncertain about the correct abbreviation for a journal title, please search for the journal at http://www.ncbi.nlm.nih.gov/nlmcatalog.Authors may wish to make use of reference management software to ensure that reference lists are correctly formatted.
Tables
Each table should be typed single-spaced, numbered in the order of their first citation in the text and supplied with a brief title each. Explanatory notes are printed under a table. Each table should be placed within the text at the appropriate points, rather than at the end. If data from another source are used, acknowledge fully.
Illustrations
All illustrations, labelled as figures (such as photographs, line drawings, charts or tracings) should be submitted as high-contrast prints, suitable for publications. Illustrations should have a final resolution of 300 dpi, and line drawings of 800-1200 dpi. They must be numbered with Arabic numerals in the same order as they are cited in the text. Photomicrographs should have the magnifications and details of staining techniques shown. Short explanatory captions of all illustrations should be typed on a separate sheet.
Abbreviations and symbols
Use only standard abbreviations. Avoid abbreviations in the title and abstracts. The full term for which an abbreviation stands should precede its first use in the text.
the conclusions with the goals of the study, but avoid unqualified statements and conclusions not completely supported by your data.
References
References should be numbered consecutively in the order in which they appear in the text. All references are identified, whether they appear in the text, tables, or legends, by Arabic numbers in superscript. Two references are cited separated by a comma, with no space. Three or more consecutive references are given as a range. The use of abstracts, secondary publications, oral communications, official and classified documents as references is strongly discouraged. Manuscripts accepted for publication may be cited and should include the manuscript’s DOI, if known. Material submitted, but not yet accepted for publication, should not be included in the reference list, but may be included in the text and referred to as ”unpublished data“ giving the names of the involved researchers. Obtaining permission to quote unpublished data from the cited colleagues is the responsibility of the author.
The list of references should only include works that are cited in the text. The style and punctuation of references should strictly conform to The National Library of Medicine Style Guide for Authors, Editors, and Publishers (NLM Style).
Balkan Journal of Dental Medicine recommends that authors refer to NLM guidelines for formatting references at the Citing Medicine Web site (http://www.nlm.nih.gov/citingmedicine).
Several examples of references in NLM format are shown below.
For more samples of formatted references visit the NLM site (http://www.nlm.nih.gov/bsd/uniform_requirements.html).
Examples of references:Brown JS, Browne RM. Factors influencing the patterns of invasion of the mandible by squamous cell carcinoma. Int J Oral Maxillofac Surg. 1995; 24:417-426.
Balk J Dent Med, Vol 21, 2017


















