The fetus with an abdominal wall defect: management and ...
7
Calisti et al, Fetus and abdominal wall defect 105 J. Perinat. Med. 15 (1987) 105 The fetus with an abdominal wall defect: management and outcome Alessandro Calisti, Carlo Manzoni, and Luigi Perrelli Division of Pediatric Surgery, Catholic University of "Sacro Cuore", Rome, Italy 1 Introduction The prenatal diagnosis of an abdominal wall defect has frequently been reported. With ultra- sonography, omphalocele and gastroschis may be discovered at an early gestational age, allow- ing prenatal transport of the affected fetus to a center which is specialized in high risk obstet- ric and pediatric surgical care. The ultrason- ographic characteristics of omphalocele (figure 1) include the presence of abdominal viscera in a sac at the base of the umbilical cord. This picture may be distinguished from that typical of gastroschisis, where free loops of bowel or solid organs appear floating in the amniotic sac (figure 2). A five years experience on treatment of prenatally diagnosed abdominal wall defects is here reported. Curriculum vitae ALESSANDRO CALISTI was born in Rome, Italy in 1946. He received his medi- cal degree at the Catholic University of Rome in 1971. His postgraduate training was in Italy, and at the Hospital for Sick Children, London. He is a specialist in Pediatric Sur- gery and Urology. He is currently teaching and working at the Catholic University of Rome, Division of Pediatric Surgery. His main fields of interest are neonatal surgery and prenatal diagnosis and the surgical treatment of congenital malformations. 2 Material and methods Fourteen cases with fetal abdominal wall defect (12 omphalocele and 2 gastroschisis) were col- lected by routine maternal ultrasonography be- tween the 16th and the 36th week of pregnancy in the Obstetrical Department of the Catholic University of Rome between January 1980 and April 1985. Antepartum planning for treatment following delivery was made in collaboration with the Pediatric Surgical Section of the same institution. Prenatal findings, obstetrical histo- ries, clinical presentation and outcome are de- scribed in table I. During the same period, 16 additional cases of abdominal wall defects (11 omphalocele and 5 gastroschisis) which had not been detected in utero (inborn or outside referrals) were ob- served and treated. A comparison was made between those antenatally detected (group B 2) and those which were not antenatally detected (group B1) in order to evaluate the influence of prenatal diagnosis on survival (tables II —III). The mode of treatment, associated anomalies and incidence of immaturity/low birth weight were recorded. Causes of death were analyzed. 1987 by Walter de Gruyter & Co. Berlin · New York
Transcript of The fetus with an abdominal wall defect: management and ...

Calisti et al, Fetus and abdominal wall defect 105
J. Perinat. Med.15 (1987) 105
The fetus with an abdominal wall defect: management and outcome
Alessandro Calisti, Carlo Manzoni, and Luigi Perrelli
Division of Pediatric Surgery, Catholic University of "Sacro Cuore", Rome,Italy
1 Introduction
The prenatal diagnosis of an abdominal walldefect has frequently been reported. With ultra-sonography, omphalocele and gastroschis maybe discovered at an early gestational age, allow-ing prenatal transport of the affected fetus toa center which is specialized in high risk obstet-ric and pediatric surgical care. The ultrason-ographic characteristics of omphalocele (figure1) include the presence of abdominal viscera ina sac at the base of the umbilical cord. Thispicture may be distinguished from that typicalof gastroschisis, where free loops of bowel orsolid organs appear floating in the amniotic sac(figure 2). A five years experience on treatmentof prenatally diagnosed abdominal wall defectsis here reported.
Curriculum vitae
ALESSANDRO CALISTI wasborn in Rome, Italy in1946. He received his medi-cal degree at the CatholicUniversity of Rome in1971. His postgraduatetraining was in Italy, andat the Hospital for SickChildren, London. He is aspecialist in Pediatric Sur-gery and Urology. He iscurrently teaching andworking at the Catholic University of Rome, Division ofPediatric Surgery. His main fields of interest are neonatalsurgery and prenatal diagnosis and the surgical treatmentof congenital malformations.
2 Material and methods
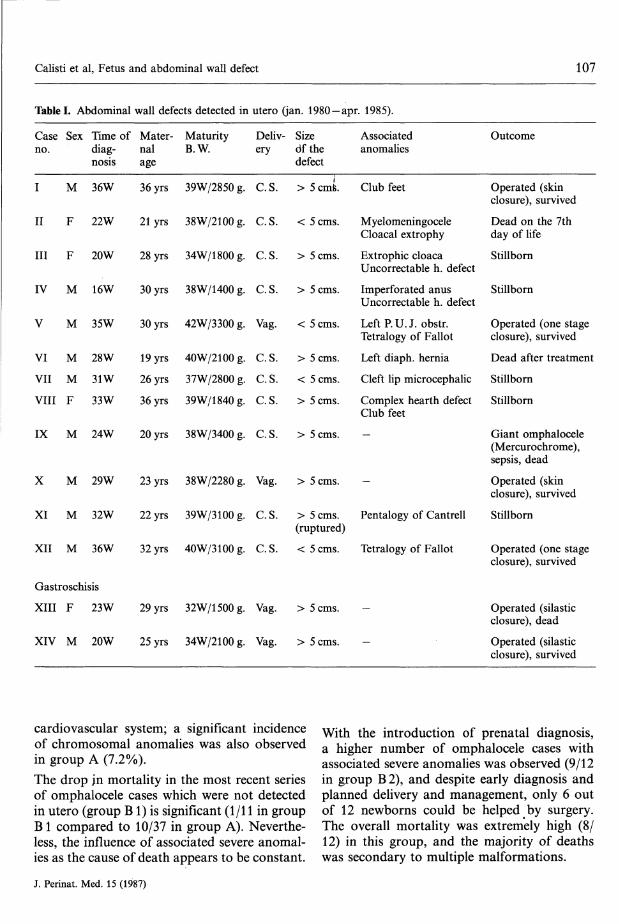
Fourteen cases with fetal abdominal wall defect(12 omphalocele and 2 gastroschisis) were col-lected by routine maternal ultrasonography be-tween the 16th and the 36th week of pregnancyin the Obstetrical Department of the CatholicUniversity of Rome between January 1980 andApril 1985. Antepartum planning for treatmentfollowing delivery was made in collaborationwith the Pediatric Surgical Section of the sameinstitution. Prenatal findings, obstetrical histo-ries, clinical presentation and outcome are de-scribed in table I.
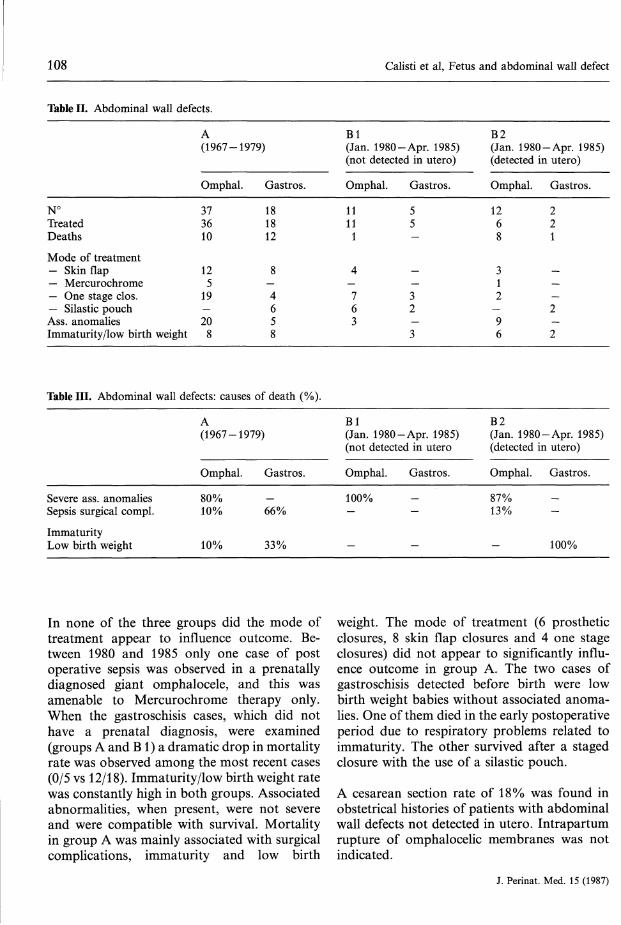
During the same period, 16 additional cases ofabdominal wall defects (11 omphalocele and 5gastroschisis) which had not been detected inutero (inborn or outside referrals) were ob-served and treated. A comparison was madebetween those antenatally detected (group B 2)and those which were not antenatally detected(group B1) in order to evaluate the influenceof prenatal diagnosis on survival (tablesII —III). The mode of treatment, associatedanomalies and incidence of immaturity/lowbirth weight were recorded. Causes of deathwere analyzed.
1987 by Walter de Gruyter & Co. Berlin · New York

106 Calisti et al, Fetus and abdominal wall defect
Figure 1. Transverse scan of a male fetus with omphalocele at 32 weeks. 1 = Spine; 2 = Fetal abdomen; 3Omphalocele; 4 = Stomach; 5 = Umbilical vessels; 6 = Liver.
Figure 2. Longitudinal scan of a female fetus at 29 weeks. F = Liver; A = Intestinal loops floating in the amnioticfluid.
The same type of review was carried out in 55cases of abdominal wall defects (tables II —III,group A) which were inborn or referred fromelsewhere and treated in our institution butwere from the October 1967 to December 1979interval. There were no prenatally diagnosedcases included in this group.
3 Results
For omphalocele the incidence of associatedanomalies and immaturity/low birth weight ratewas very similar in groups A and Bl. Com-bined abnormalities were severe in most of thecases, and more than one third affected the
J. Perinat. Med. 15 (1987)
Calisti et al, Fetus and abdominal wall defect 107
Table I. Abdominal wall defects detected in
Caseno.
I
II
III
IV
V
VI
VII
VIII
Sex
M
F
F
M
M
M
M
F
Time of Mater-diag- nalnosis age
36W
22W
20W
16W
35W
28W
31W
33W
36yrs
21yrs
28yrs
30yrs
30yrs
19yrs
26yrs
36yrs
MaturityB.W.
39W/2850 g.
38W/2100 g.
34W/1800g.
38W/1400 g.
42W/3300 g.
40W/2100 g.
37W/2800 g.
39W/1840g.
utero (jan. 1980 -apr. 1985).
Deliv-ery
C.
C.
C.
C.
s.
s.
s.
s.
Vag.
C.
C.
C.
s.s.s.
Sizedfthedefect
> 5 cms.
< 5 cms.
> 5 cms.
> 5 cms.
< 5 cms.
> 5 cms.
< 5 cms.
> 5 cms.
Associatedanomalies
Club feet
MyelomeningoceleCloacal extrophy
Extrophic cloacaUncorrectable h. defect
Imperforated anusUncorrectable h. defect
LeftP.U.J. obstr.Tetralogy of Fallot
Left diaph. hernia
Cleft lip microcephalic
Complex hearth defect
Outcome
Operatedclosure),
(skinsurvived
Dead on the 7thday of life
Stillborn
Stillborn
Operatedclosure),
(one stagesurvived
Dead after treatment
Stillborn
StillbornClub feet
IX M 24W 20 yrs 38W/3400 g. C. S. > 5 cms.
X M 29W 23 yrs 38W/2280 g. Vag. > 5 cms.
XI M 32W 22 yrs 39W/3100g. C.S. >5cms. Pentalogy of Cantrell(ruptured)
XII M 36W 32yrs 40W/3100g. C.S. <5cms. Tetralogy of Fallot
Gastroschisis
XIII F 23W 29 yrs 32W/1500g. Vag. >5cms.
XIV M 20W 25 yrs 34W/2100 g. Vag. > 5 cms.
Giant omphalocele(Mercurochr ome),sepsis, dead
Operated (skinclosure), survived
Stillborn
Operated (one stageclosure), survived
Operated (silasticclosure), dead
Operated (silasticclosure), survived
cardiovascular system; a significant incidenceof chromosomal anomalies was also observedin group A (7.2%).The drop in mortality in the most recent seriesof omphalocele cases which were not detectedin utero (group B1) is significant (1/11 in groupB l compared to 10/37 in group A). Neverthe-less, the influence of associated severe anomal-ies as the cause of death appears to be constant.
With the introduction of prenatal diagnosis,a higher number of omphalocele cases withassociated severe anomalies was observed (9/12in group B 2), and despite early diagnosis andplanned delivery and management, only 6 outof 12 newborns could be helped by surgery.The overall mortality was extremely high (8/12) in this group, and the majority of deathswas secondary to multiple malformations.
J. Perinat. Med. 15 (1987)
108 Calisti et al, Fetus and abdominal wall defect
Table II. Abdominal wall defects.
A(1967-1979)
Bl(Jan. 1980 -Apr. 1985)(not detected in utero)
N°TreatedDeaths
Mode of treatment- Skin flap— Mercurochrome— One stage clos.— Silastic pouchAss. anomaliesImmaturity/low birth
Table III. Abdominal
Omphal.
373610
125
19—20
weight 8
wall defects: causes
A
Castros.
181812
8—4658
of death (%).
(1967-1979)
Severe ass. anomaliesSepsis surgical compl.
ImmaturityLow birth weight
Omphal.
80%10%
10%
Gastros.
66%
33%
Omphal.
11111
4—763
Bl
Gastros.
55-
——32—3
(Jan. 1980-Apr. 1985)(not detected
Omphal.
100%-
—
in utero
Gastros.
—
—
B2(Jan. 1980-Apr. 1985)(detected
Omphal.
1268
312
—96
B2
in utero)
Gastros.
221
———2—2
(Jan. 1980-Apr. 1985)(detected
Omphal.
87%13%
—
in utero)
Gastros.
—
100%
In none of the three groups did the mode oftreatment appear to influence outcome. Be-tween 1980 and 1985 only one case of postoperative sepsis was observed in a prenatallydiagnosed giant omphalocele, and this wasamenable to Mercurochrome therapy only.When the gastroschisis cases, which did nothave a prenatal diagnosis, were examined(groups A and B1) a dramatic drop in mortalityrate was observed among the most recent cases(0/5 vs 12/18). Immaturity/low birth weight ratewas constantly high in both groups. Associatedabnormalities, when present, were not severeand were compatible with survival. Mortalityin group A was mainly associated with surgicalcomplications, immaturity and low birth
weight. The mode of treatment (6 prostheticclosures, 8 skin flap closures and 4 one stageclosures) did not appear to significantly influ-ence outcome in group A. The two cases ofgastroschisis detected before birth were lowbirth weight babies without associated anoma-lies. One of them died in the early postoperativeperiod due to respiratory problems related toimmaturity. The other survived after a stagedclosure with the use of a silastic pouch.
A cesarean section rate of 18% was found inobstetrical histories of patients with abdominalwall defects not detected in utero. Intrapartumrupture of omphalocelic membranes was notindicated.
J. Perinat. Med. 15 (1987)
Calisti et al, Fetus and abdominal wall defect 109
Among prenatally discovered cases of abdomi-nal wall defect an induced high rate of cesareansections was reported (70%). Only one rup-tured omphalocele was observed (case XI). Itwas detected in utero at 32 weeks and couldnot be followed up. The mother was admittedin advanced labor with ruptured membranesat 39 weeks, and a stillborn male infant withpentalogy of Cantrell was operatively delivered.
4 Discussion
With an omphalocele the most important fac-tors affecting survival are associated anomalies(mainly cardiovascular), chromosomal defectsand low birth weight. In gastroschisis mortalityis usually secondary to surgical complications[9]. While the omphalocele sac protects intesti-nal loops from amniotic fluid and postnatalinjuries, in gastroschisis the herniated visceraappear edematous and thickened. This aspectis usually worse in late referred cases. Postoper-ative sepsis and prolonged ileus are describedas the two main problems with treatment ofthis anomaly.The optimal method for operative managementof an abdominal wall defect remains controver-sial, and wide variations of opinions and en-thusiasm for different procedures have beenpresented in the literature in the past 30 years[2 — 4]. When a one stage closure is made impos-sible by the risk of ventilatory and caval circula-tion compromise, skin flap closure or, in thepast, escharification of the sac with Mercu-rochrome were the only alternatives. Theprosthetic sac closure, especially in largegastroschisis, was a milestone achievement andcontributed to reduce mortality of thesepatients [10]. Nevertheless, all these staged pro-cedures carry some risk and need multipleoperations.Recently, intraoperative abdominal wallstretching, gentle evacuation of gastrointestinalcontent and postoperative paralysis and mech-anical ventilation for some days have been pro-posed to achieve primary closure even in largedefects [1].
The improvement in treatment of abdominalwall defects also reflects the advances that havebeen made in general neonatal care, anesthetictechniques and availability of new supportivemeasures. This is reflected in a larger survivalrate for babies with gastroschisis [6] as wasconfirmed by our data.
Early treatment soon after delivery of thisanomaly, permitted by prenatal diagnosis, mayreduce exposure and handling of neonatal loopsand minimize risks of infection and long post-operative ileus.
Despite current methods of treatment, mortal-ity due to severe associated malformations [7]has not been significantly changed among in-fants with omphalocele. With prenatal diag-nosis a larger number of these newborns arenow seen in the early perinatal period. Amongthem there are many cases that, without antena-tal detection and maternal transport, wouldnever have been living long enough to be ob-served by the surgeon. This may explain theparadoxally high mortality rate (overall andsurgical) in prenatally diagnosed cases. Carefulantenatal search for associated anomalies ismandatory for a better prognostic evaluationof omphalocele cases. Concerns about potentialdystocia with large omphaloceles and aboutinjury and contamination of the abdominalcontent in gastroschisis have increased the useof cesarean section in our cases. There is noevidence of a real benefit from cesarean section.No intrapartum rupture of an omphalocele sachas been reported in all our cases abservedprior to the introduction of prenatal diagnosis.The presence of associated anomalies and un-avoidable poor outcome in many of these fe-tuses must be considered before increasing ma-ternal risk with an operative delivery.
5 Conclusion
Benefit of earlier treatment is not demonstrablefrom our small number of cases of gastroschisisdetected in utero and treated immediately fol-lowing birth.
J. Perinat. Med. 15 (1987)

110 Calisti et al, Fetus and abdominal wall defect
In the omphalocele cases, associated anomalieshave been an unavoidable limiting factor inimproving the overall and surgical mortalityrates. We must also consider that with prenataldiagnosis a large number of cases destined, inthe past, to be stillborn or to die before referralto a surgical center are now observed and some-times treated by pediatric surgeons.
Potentially better outcomes for fetuses with ab-dominal wall defects may be expected with theintroduction of prenatal diagnosis. Reduction
of risks related to perinatal transport and abetter quality of surgery and supportive mea-sures in a well equiped center may lead toa higher survival rate when multiple complexdeformities incompatible with life are not pre-sent. These cases must be identified beforebirth.The question of whether cesarean sectionshould be the preferred method of delivery isstill being debated [8]. In our opinion, extensiveindication for operative delivery does not ap-pear to be sufficently justified.
Summary
Despite prenatal diagnosis, maternal transport and earlyperinatal treatment in specialized hospitals, improve-ment in overall mortality has not been observed amongnewborns with abdominal wall defects (omphalocele andgastroschisis). A comparison has been made, for bothanomalies, between 55 cases treated in the periods1967-1979 and 30 treated in the periods 1980-1985.In this last group, 14 prenatally detected cases wereseparated from cases discovered at birth. Recent ad-vances in treatment have reduced mortality rates forboth of these anomalies. This was especially true forgastroschisis; in omphalocele cases, associated abnor-malities appeared to be an unavoidable limiting factorin survival. With prenatal diagnosis a surprising increasein mortality rate was observed among omphalocele casesdetected before birth. A possible reason for this is thetotal number of antenatally diagnosed cases that, withmaternal transport, are concentrated in centers wheresurgical facilities are available. Before introduction ofantenatal diagnosis, most of these cases would never
have been observed by the pediatric surgeon because ofdeath prior to referral or treatment.Gastroschisis cases may benefit more from antenatalrecognition and early treatment because multiple abnor-malities or immaturity are not so important limitingfactors in survival as in omphalocele cases. Reducedtrauma and contamination of exposed viscera, immedi-ate treatment and adequate supportive measures maysignificantly reduce mortality rate in gastroschisis cases.Operative delivery of fetuses with an abdominal walldefect is controversial. The risk of vaginal route deliveryhas been over emphasized. Intrapartum rupture of anomphalocelic sac was an extremely rare event beforeintroduction of antenatal diagnosis. It is the authors'opinion that extensive indication for cesarean section isnot justified'because it increases maternal risk and has anuncertain benefit for the fetus. In conclusion, antenataldiagnosis may potentially contribute to improve resultsin treatment of abdominal wall defects, provided thatmultiple, untreatable malformations are not present.
Keywords: Gastroschisis, omphalocele, prenatal diagnosis.
Zusammenfassung
Geburtsleitung und klinischer Zustand bei Neugeborenenmit BauchwanddefektenTrotz pränatal gestellter Diagnose, Einweisung der Müt-ter in Spezialkliniken und früher perinataler Behandlungdort konnte keine Senkung der Gesamtmortalität Neu-geborener mit Bauchwanddefekten (Omphalocele undGastroschisis) beobachtet werden. Es wurden für beideAnomalien 55 Fälle, die in den Jahren 1967-1979 be-handelt worden waren, mit 30 Fällen aus den Jahren1980 — 1985 verglichen. In der letzteren Gruppe wurden14 pränatal diagnostizierte Fälle von den restlichen, dieerst bei der Geburt festgestellt wurden, getrennt betrach-tet.Durch die jüngsten Fortschritte in der Behandlungkonnte die Mortalitätsrate für beide Anomalien erheb-lich gesenkt werden. Dies trifft insbesondere auf die
Gastroschisis zu; bei Fällen von Omphalocele scheinendamit assoziierte Anomalien ein limitierender Faktor fürdas Überleben zu sein, der nicht überwunden werdenkann. Mit zunehmender Verbreitung der Pränataldia-gnostik wurde ein überraschender Anstieg der Mortali-tät bei Fällen von pränatal festgestellter Omphalocelebeobachtet. Ein möglicher Grund hierfür ist die Gesamt-zahl pränatal diagnostizierter Fälle, die durch Einwei-sung der Mutter in Zentren konzentriert werden, dieüber die nötigen chirurgischen Einrichtungen verfügen.Vor Einführung der Pränataldiagnostik wurde der Groß-teil dieser Fälle niemals von einem Kinderchirurgen be-obachtet, da die Neugeborenen bereits vor der Einwei-sung zur Therapie verstarben.Neugeborene mit Gastroschisis mögen stärker von derpränatalen Diagnostik und früh einsetzenden Behand-
J. Perinat. Med. 15 (1987)

Calisti et al, Fetus and abdominal wall defect 111
lung profitieren, da multiple Anomalien oder Unreifeals limitierende Faktoren nicht so ins Gewicht fallen wiebei Fällen mit Omphalocele.Reduzierte Traumatisierung und Kontamination der ex-ponierten Organe, sofortige Therapie und angemesseneunterstützende Maßnahmen können die Mortalitätsratebei Gastroschisis signifikant herabsetzen. Die operativeEntbindung von Feten mit Bauchwanddefekt wird kon-trovers beurteilt. Das Risiko einer vaginalen Geburtwurde überbetont. Die Ruptur eines Omphalocelensacks
war auch vor Einführung der Pränataldiagnostik einextrem seltenes Ereignis. Nach Meinung des Autors istdie weit gestellte Indikation für einen Kaiserschnitt nichtgerechtfertigt, weil das mütterliche Risiko erhöht wirdzugunsten eines Ungewissen Vorteils für den Feten. Ab-schließend kann gesagt werden, daß pränatale Diagno-stik möglicherweise dazu beitragen kann, die Ergebnissebei der Behandlung von Bauchwanddefekten zu verbes-sern, vorausgesetzt, daß keine multiplen unbehandelba-ren Mißbildungen vorliegen.
Schlüsselwörter: Gastroschisis, Omphalocele, pränatale Diagnostik.
Resume
Anomalies de la paroi abdominale chez le foetus priseencharge et devenirMalgre le diagnostique prenatal, le transport maternelet le traitement precoce perinatal en hopitaux specialises,on n'a pas assiste a une diminution du taux de mortalitechez les nouveaux-nes presentant des defauts de la paroiabdominale (omphalocele et gastroschisis). Une compa-raison a etc faite, pour les deux anomalies, entre les 55cas traites pendant la periode de 1967 a 1979 et les 30cas traites pendant la periode de 1980 a 1985. Dans cedernier groupe, 14 cas ont ete decouverts a la naissance.Les recents progres dans le traitement ont reduit letaux de mortalite pour les deux anomalies. Cela estparticulierement vrai pour les gastroschisis, tandis queparmis les cas d'omphalocele, les anomalies associeessemblent etre un facteur inevitable limitant la survie.Une surprenante augmentation du taux de mortalite aete observee parmis les cas d'omphalocele decouvertsavant la naissance. Une possible explication de ce pheno-mene est fournie par le fait que la quasi totalite des casdiagnostiques avant la naissance, est concentree dans lescentres specialises, grace au transport maternel. Avantl'introduction du diagnostique prenatal la plus part de
ces cas etait rarement observes par le Chirurgien ä causede la mort du patient avant le transport ou le traitement.Les cas de gastroschisis ont beneficie d'avantage de ladecouverte prenatale et du traitement precoce car lesanomalies multiples ou Pimmaturite ne sont pas desfacteurs limitants la survie aussi importants que les mal-formations associees a omphalocele. La reduction dutraumatisme et de la contamination des visceres exposes,le traitement immediat et les soins intensifs peuventreduire considerablement le taux de mortalite pour lescas de gastrischisis.La cesarienne pour les foetus ayant un defaut de la paroiabdominale est discutee. Le risque de la voie vaginale aete surestime: en fait la rupture d'un sac omphaloceliquependant Paccouchement etait un evenement extreme-ment rare avant l'introduction du diagnostique prenatal.L'opinion des auteurs est qu'une indication extensive dela cesarienne n'est pas justifiee du fait qu'elle augmenteles risques maternels et ne donne que des avantagestres douteux au foetus. En conclusion, le diagnostiqueprenatal peut ameliorer les resultats du traitement desdefauts de la paroi abdominale pourvu que des malfor-mations multiples et intraitables ne soient pas presentes.
Mots-cles: Diagnostique prenatal, gastroschisis, omphalocele.
References
[1] BOWER RT, MJ BELL, JR TENBERG, ML COB: Venti-latory support and primary closure of gastroschisis.Surgery 91 (1982) 52
[2] CANTY TG, D COLLINS: Primary fascial closurein infants with gastroschisis and omphalocele: asuperior approach. J Pediatr Surg 18 (1983) 707
[3] DE VRIES P: The pathogenesis of gastroschisis andomphalocele. J Pediatr Surg 15 (1980) 245
[4] EIN SH, ZR RUBIN: Gastroschisis: primary closureo,r silon pouch. J Pediatr Surg 15 (1980) 549
[5] HARRISON MR, MS GOL#US, RA FILLY: The un-born patient. Prenatal diagnosis and treatment.Grune and Stratton, Orlando, FL-London 1984
[6] HOFMANN V, S KAP HERR, P EMMRICH: Causes ofpostoperative deaths in gastroschisis and omphalo-cele. Prog Pediatr Surg 13 (1979) 63
J. Perinat. Med. 15 (1987)
[7] HOLLABOUGHT RS: The management ofgastroschisis. J Pediatr Surg 8 (1973) 263
[8] KIRK P, R WAH: Obstetric management of the fetuswith omphalocele or gastroschisis: a rewiew andreport of one hundred twelwe cases. Am J ObstetGynecol 146 (1983) 512
[9] MAYER T, R BLACK, ME MATLAK, T MAYER, RBLACK, ME MATLAK, DG JOHNSON: Gastroschisisand omphalocele. Ann Surg 192 (1980) 783
[10] SCHWARTZ M, K TYSON, K MILLIORN, T LOBE:Staged reduction using a silastic sac in the treatmentof choice for large congenital abdominal wall de-fects. J Pediatr Surg 18 (1983) 713
Received November 9, 1985. Accepted March 21, 1986.Prof. Luigi PerrelliVia Bruxelles, 6700198 Rome, Italy


















