The Female Genital Tract. Infections Lower genital tract HSV- latent, recurrence, transmission to...
30
The Female Genital Tract
-
Upload
solomon-campbell -
Category
Documents
-
view
235 -
download
4
Transcript of The Female Genital Tract. Infections Lower genital tract HSV- latent, recurrence, transmission to...
The Female Genital Tract
Infections
Lower genital tract HSV- latent, recurrence, transmission to offspring, painful ulcers, multinucleated giant cells
Molluscum contagiosum –pox virus, umblicated papules
Fungal infections- Candida – DM, antibiotics, pregnancy, suppression of cell-mediated immunity
Trichomonas vaginalis- frothy, strawberry cervix
Gardnerella vaginalis – fishy odor, clue cells
Ureaplasma – Preterm laborChlamydia –usually cervicitis
LGV in tropicsSyphilis – painless chancre,
condyloma lata, fetal malformations
Toxic Shock – S. aureus, tampons,
PID
Ascending infectionGC- also pharyngitis, arthritis, proctitis, ophthalmia
neonatorum, Chlamydia – more mucosal involvement
Puerperal infections – polymicrobial, more reaction in the deeper layers
Acute salpingitisSalpingo-oophoritisTubo-ovarian abscessesAcute complications –peritonitis, bacteremiaChronic complications- infertility, tubal obstruction,
intestinal obstruction, ectopic pregnancy
Vulva
Skin diseases – similar to other areas of body – infection, inflammatory, cancers
Bartholin CystLichen sclerosus- thinning of epidermis, dermal fibrosisSquamous cell hyperplasia (Lichen simplex chronicus)Condyloma acuminatum-HPV 6 and 11, koilocytic (expanded
epithelial cells with perinuclear clearing) atypiaVIN and carcinoma – basloid and warty- HPV
keratinizing squamous cell- more common, not HPVPapillary hiradenoma – sweat glandsExtramammary Paget disease

Vagina
Vaginal adenosis and clear cell adencarinoma – DES
Vaginal intraepithelial neoplasia and squamous cell carcinoma
Embryonal rhadomyosarcoma- sarcoma botryoides – “bunch of grapes”
Cervix
Acute and Chronic Cervicitis
Intracellular gycogen
Lactobacillus – lower pH
May cause an abnormal PAP test
Endocervical polyps – may cause vaginal bleeding
Cervix
High oncogenic risk HPVs are considered to be the single most important factor in cervical oncogenesis – 16 and 18
Other risk factors-Multiple sexual partnersYoung age at first intercourseHigh parityImmunosuppressionCertain HLA typesUse of oral contraceptivesUse of smoking
Cervix
HPVMost infections are asymptomatic50% clear in 8 months90% clear in 2 yearsPersistent infection increases the risk of cervical dysplasia and carcinomaCan infect only the immature cells but replication occurs in the maturing cellsKoilocytic atypia – nuclear atypia and perinuclear haloActivate cell cycle by interference with Rb and p53
Cervix
Cervical Intraepithelial NeoplasiaCIN I – mild dysplasia (LSIL)CIN II – moderate dysplasia (HSIL)CIN III – severe dysplasia (HSIL)
Natural historyLSIL – 60% regress, 30% persist, 10% progress to HSILHSIL – 30% regress, 60% persist,10%
progress to carcinoma

Cervix
Cervical cancer80% squamous cell15% adenocarcinoma 5% adenosquamous and neuroendocrine
Stagingstage 0 - carcinoma in situ (CIN III, HSIL)stage I – confined to cervixstage II – beyond the cervix but not to pelvic wall or lower 1/3 of vaginastage III – extended to the pelvic wall, lower 1/3 of vaginastage IV – beyond the true pelvis, bladder or rectum or distant metastases
Screening and preventionPAP smearRemoval of precancerous lesions - colposcopysurgical removal of invasive cancersHPV vaccineHPV DNA testing
Endometrium
“Dating” the endometrium
Proliferative phase
Secretory phase
Exhaustion and disintegration
Hypothalmic-Pituitary-Ovarian Axis
Corpus luteum
Endometrium
Dysfunctional Uterine BleedingAnovulatory Cycle
Menopausal changesAtrophy
InflammationAcute endometritis
Retained products of conceptionChronic endometritis
Chronic PIDPostpartum or post-abortionIUDsTBNon-specific
Endometrium
EndometriosisPresence of endometrial tissue outside the uterus
InfertilityDysmenorrhea Pelvic pain
Metastatic theoryMetaplastic theory
Activation of inflammatory cascadeUpregulation of estrogen production
AdenomyosisPresence of endometrial tissue within the uterine wall (myometrium)
HyperplasiaProlonged estrogen stimulation of the endometrium
Relationship with endometrial carcinoma
Inactivation of the PTEN tumor suppressor gene
Simple hyperplasia + atypiaComplex hyperplasia +atypia
Endometrium
Endometrial carcinomaMost common invasive tumor of the female genital tract
Post-menopausal bleeding
Type IUnopposed estrogenObesity, hypertension, diabetesEndometroidHyperplasiaPTENIndolent
Type IIAtrophyThinSerous, clear cell, mixed mullerian tumorEndometrial intraepithelial carcinomaAggressivep53
-
Myometrium
Leiomyomas – fibroids
Leiomyosarcomas

Ovaries
Polycystic Ovarian diseasepersistent anovulationobesityhirsutismrarely virilism
Variety of enzymes involved in androgen synthesis are poorly regulated

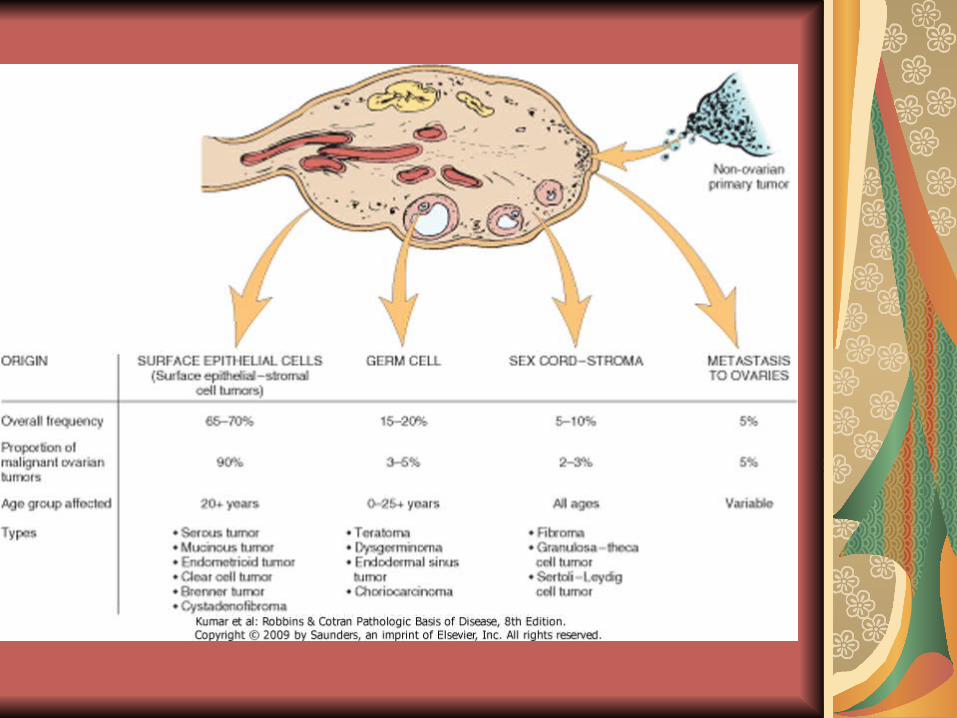
Ovarian Tumors
Surface Epithelial-stromalMost commonMost malignant
Most ovarian cancers are detected when they have spread beyond the ovary; account for a disportionate number of deaths
Germ cell
Sex cord-stromal
Metastasis to ovary-tumors of Mullerian origin, breast, GI, Krukenberg tumor

Surface Epithelial (Mullerian)
Most primary neoplasms of ovary
Transformation of coelmic epithelium
Lower abdominal pain, enlargement
GI compliants, urinary complaints,pelvic pressure
CA-125, osteopontin
TypesSerousMucinousEndometrioidClear cellBrenner – transitional cellCystadenofibroma
Serous Lined by tall, columnar ciliated and noniliated epithelial cells
Filled with clear serous fluid
BRCA1 and BRCA2
fimbriated end of fallopian tube
Higher frequency of malignancy in women of low parity
Mucinous
Endometrioid
KRAS
Pseudomyxoma peritonei
Less frequently bilateral
PTEN. KRAS, beta-catenin

Germ Cell Tumors
Types
Teratomas
Dysgerminoma
Endodermal sinus (yolk sac)
Choriocarcinoma
Most are benign cystic teratomas

Teratomas Mature (benign)- dermoid cyst
Immature (malignant)
Monodermal ( highly specialized) – strumi ovarii (thyroid) and carcinoid
Dysgerminoma
Yolk sac
Choriocarcinoma
Equivalent to seminoma
Gonadal dysgenesis
Alpha-fetoprotein and alpha1- antitrypsin
HCGAggressive
Sex Cord-Stromal
TypesFibroma – Meigs syndrome ( ovarian tumor, hydrothorax, ascites), basal cell nevus syndromeGranulosa-theca cell – estrogen, precocious puberty, endometrial hyperplasia or carcinoma, Call-Exner bodiesSertoli-Leydig cell - masculinizing
Gestational and Placental Disorders
Early Pregnancy
Late pregnancy
Spontaneous abortionEctopic pregnancy
Twin placentasPlacental Implantation
abnormalities – previa and accreta
Placental abruptionPlacental InfectionsPreeclampsiaEclampsia
Preeclampsia
Widespread endothelial dysfunction, vasoconstriction, increased vasopermeability
Hypertension, Edema, proteinuria3-5% womenLast trimesterPrimiparasHELLP syndrome ( hemolysis, elevated liver enzymes, low platelets)Abnormal placental vasculature- abnormal trophoblastic implantation is
the initial event – remodeling of vessels does not occurFollowed by endothelial dysfunction and imbalance of angiogenic and
anti-angiogenic factorsCoagulation abnormalitiesHeadache and visual changes – severe preeclampsiaSeizures - eclampsia
Gestational Trophoblastic Disease
Hydatidiform Mole
Complete
Partial
Invasive mole
Choriocarinoma
Placental-Site Trophoblastic Tumor