The Employment of Pilates to Improve Function And Reduce ... · PDF filejoint to form a very...
13
The Employment of Pilates to Improve Function And Reduce Injury Related to Congenital Pes Planus Julie Lopez Santiago November 22, 2009 Costa Mesa
Transcript of The Employment of Pilates to Improve Function And Reduce ... · PDF filejoint to form a very...

The Employment of Pilates to Improve Function And Reduce Injury Related to Congenital Pes Planus
Julie Lopez Santiago November 22, 2009
Costa Mesa

2
Abstract
The purpose of this paper is to discuss the following concepts: How congenital Pes Planus or flat
feet cause compensatory rotation in the tibia and other mechanical stressors in the legs, leading
to pain and predisposing to injury. Also investigated is the possibility of developing an exercise
routine that will minimize the negative effects of this condition and/or need for invasive
procedures. Despite the significant incidence of this condition, the pathophysiology is still
debated. This paper will attempt to show a possible exercise plan and rehabilitation for treatment
for less-severe malformations whether it be for the congenital condition or for acquired Pes
Planus in adults.

3
Table of Contents Abstract ………………………………………………………………………………… 2 Anatomical Description ……………………………………………………………….. 4-6 Case Study .…………………………………………………………………………….. 7 Conditioning Program .………………………………………………………………. 8-12 Conclusion ……………………………………………………………………………... 12 Bibliography …………………………………………………………………………… 13
4
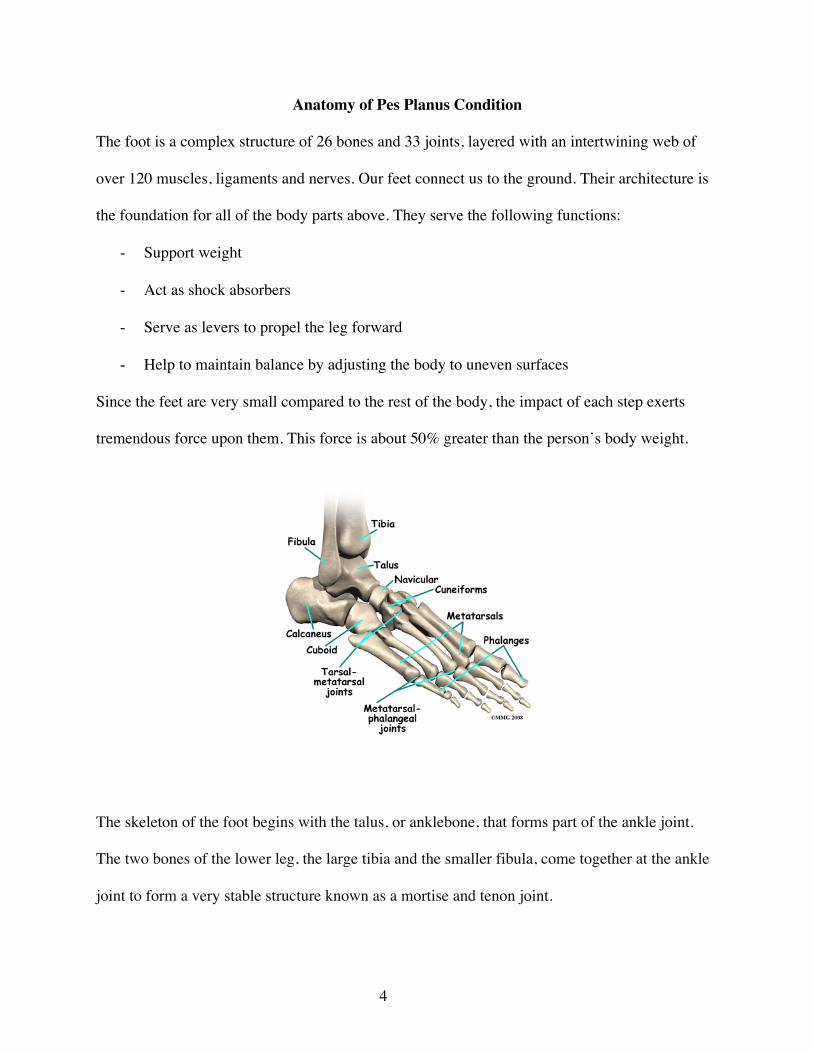
Anatomy of Pes Planus Condition The foot is a complex structure of 26 bones and 33 joints, layered with an intertwining web of
over 120 muscles, ligaments and nerves. Our feet connect us to the ground. Their architecture is
the foundation for all of the body parts above. They serve the following functions:
- Support weight
- Act as shock absorbers
- Serve as levers to propel the leg forward
- Help to maintain balance by adjusting the body to uneven surfaces
Since the feet are very small compared to the rest of the body, the impact of each step exerts
tremendous force upon them. This force is about 50% greater than the person’s body weight.
The skeleton of the foot begins with the talus, or anklebone, that forms part of the ankle joint.
The two bones of the lower leg, the large tibia and the smaller fibula, come together at the ankle
joint to form a very stable structure known as a mortise and tenon joint.

5
The two bones that make up the back part of the foot are the talus and the calcaneus, or heel
bone. The talus is connected to the calcaneus at the subtalar joint. The ankle joint allows the foot
to bend up and down.
The subtalar joint allows the foot to rock from side to side. People with flatfeet usually have
more motion at the subtalar joint than people who do not have flatfeet. The increased flexibility
of the subtalar joint results in many compensatory actions of the foot and ankle in order to keep
proper foot alignment during standing and walking.
Just down the foot from the ankle is a set of five bones called tarsal bones. The tarsal bones work
together as a group. They are unique in the way they fit together. There are multiple joints
between the tarsal bones. The tarsal bones are connected to the five long bones of the foot called
the metatarsals. The two groups of bones are fairly rigidly connected, without much movement at
the joints. Finally, there are the bones of the toes, the phalanges.
With a flatfoot deformity, bones, ligaments, and muscles are all affected. In the flexible flatfoot,
the bones are usually normal - but the supporting ligaments are lax or loose. The joints are
hypermobile. As the soft tissues and joints of the foot and ankle try to maintain a normal foot
position, increased stress is placed on them. This can lead to fatigue and loss of strength resulting
in a sagging of the arch. Other dysfunctions in the lower kinematic chain (i.e. knee, hip) are
commonly associated with excessive subtalar pronation.

6
In the uncommon severe cases, calluses may appear where pressure occurs as the bones make
contact with the floor or hard surface. The loss of joint stability may alter the foot's ability to
absorb the load and conform to uneven ground or surfaces.
Excess pressure on the surrounding soft tissues (ligaments, capsules, tendons, muscles) can lead
to other problems such as misalignment of the patella (kneecap), hallux valgus (bunions), and
rotation of the knee and hip.

7
Case Study
I have done the case study on myself, a moderately active 43-year old woman. The condition of
Pes Planus was not the source of injury or misalignment during childhood. The only injuries
suffered during that time were the occasional sprained ankle while participating in volleyball and
medial tibial stress syndrome (shin splints) as a participant in track.
In my 20s, I suffered from moderate to severe knee pain and chose to stop participating in
collegiate volleyball rather than undergo arthroscopic knee surgery to repair patellar tendonitis
and with physical therapy and time the pain subsided. Since that time I have been unable to jog
or run without experiencing pain and swelling in the knee joints. In addition I experience
occasional sharp knee pain while lifting weight with my legs or descending stairs.
Ten years ago, I underwent a bunionectomy combined with a procedure to repair the ligaments
and tendons around the big toe. The bunions had developed in my mid to late 20s but at that
point had reached a period in which severe foot pain was limiting my activities even when
wearing sensible shoes. The surgery was successful but I am still unable to wear shoes with a
heel for any length of time without discomfort in the foot. Additionally, I have severe callus
buildup due to excessive pressure under the second metatarsal head and on the outside of the big
toe. Ongoing maintenance on these callus points must be performed or the buildup is a cause of
additional foot pain.
Other problems which I have experienced and were likely caused by poor alignment is
Trochanteric bursitis in the hip joints and misalignment of the spine in the L3 and L4 vertebrae
both requiring chiropractic care and physical therapy to correct.

8
Conditioning Program
Despite its delicate architecture, the human foot is strong, dynamic and adaptable. For good
balance and stability, the foot should contact the ground like a tripod, with the weight evenly
spread between the calcaneus (the heel) and the heads of the first and fifth metatarsals. When we
stand, the distribution of weight should be the following: the heel should receive the majority of
the body’s weight, the first metatarsal head should be secondary in its capacity, and the fifth
metatarsal head should support the least amount of the body’s weight. In order to avoid the
excess pronation, which ultimately causes the femur to roll in and pull on the pelvis anteriorly,
this conditioning program will focus on restoring that tripod balance.
For thousands of years our feet have functioned fine and maybe even better without elaborately
padded shoes such as today’s athletic shoes and orthodics. However, this type of treatment seems
to be the primary focus in podiatry today. More recent studies including a book by Christopher
McDougall, Born to Run (Knopf 2009) are concluding that being barefoot or wearing flatter and
more flexible shoes (i.e. those with less support) are more beneficial in developing proper foot
functioning. Our feet have many muscles that originate in the leg. Wearing running shoes may
lessen or diminish the “firing” of some of these muscles. When the foot is not in shoes, it
adapts—rapidly—to uneven surfaces, and in theory, forcing us to “use” all the muscles in our
foot. Further, running or other elaborately padded athletic shoes may actually decrease an
athlete’s awareness of their foot and the foot’s position, increasing the risk of injury.
The teachings of Joseph Pilates confirmed that the body was a well-functioning machine if it was
taught to be in alignment and developed sufficient supportive strength. That is the theory I am
following in developing this therapeutic conditioning program. It will include progressive
9
stretching and strengthening exercises, including exercises that address impairments of the
pelvis, hip and knee which may be associated with excessive pronation, such as weak ankle
plantar flexors, week hip abduction and external rotation. Although the conditioning program
that follows includes a complete body workout, many of the exercises will include activities that
will challenge me to address the strength, flexibility, proprioception and endurance of the
muscles of my lower body in an attempt to restore proper functioning. Some highlights of the
workout that focus on the neuromuscular re-education for parts of my body that have long
functioned in a compensatory manner are as follows:
Footwork – I chose to do a majority of the footwork portion of the program on the Cadillac due
to my ability to watch my feet throughout the exercises. This would be to increase awareness of
any poor alignment issues in my feet and legs and focus on hip disassociation.
Two particular exercises to note are the Hip Opener and the Prehensile on the Reformer. These
two particularly focus on areas of interest. The Hip Opener I would use to address weak hip
abduction. The Prehensile exercise in wrapping the toes around the foot bar, places the forefoot
into a supportive transverse arch. Instead of rolling my legs inward to meet the bar evenly,
focusing on keeping the thighs in neutral alignment with the hip creates a pattern of strength
from the feet to the pelvis.
Abdominal – Focus on strengthening hip flexors and maintaining alignment in legs
Hip Work – Focus on building up mobility and support in the hip complex.
Spinal Articulation – Focus on watching alignment of feet and legs while stretching.
Stretches – Focus on lower body stretches to overcome compensatory tightness.
Full Body Integration 1 – Focus on ankle plantar flexor strength and knee extensors.

10
Arm Work – Done on knees to help maintain lower body stability.
Full Body Integration 2 – Maintaining strong plantar strength in feet during exercise.
Additional Leg Work – Focus on articulating the foot and focusing on building strength in the
plantar flexors, knee extensors and hip extensors.
Lateral Flexion/Rotation – Maintaining proper alignment to maximize oblique work.
Back Extension – Engaging legs throughout and activating adductor muscles in legs.
Warm Up Mat Work – Roll up, Spine Twist Supine,
Double Leg Stretch, Single Leg Stretch, Criss Cross
Foot Work Cadillac – Parallel Heels & Toes, V Position Toes, Open V Heels & Toes, Calf Raises, Prances, Hip Opener Reformer – Prehensile
Abdominal Work Reformer – Hundred, Double Leg and Double Leg with Rotation
Hip Work Reformer – Extended Frog Series – Down Circles, Up Circles, Extended Frog, Extended Frog Reverse
Spinal Articulation Cadillac – Monkey Original, Tower Prep
Stretches Ladder Barrel – Gluteals, Hamstrings, Adductors, Hip Flexors
Full Body Integration 1 Reformer – Stomach Massage: Round Back, Flat Back, Extended
Arm Work Reformer – Arms Kneeling Series: Chest Expansion, Up & Down Circles, Triceps, Biceps
Full Body Integration 2 Reformer – Balance Control Front
Additional Leg Work Reformer – Jump Board Series

11
Lateral Flexion/Rotation Wunda Chair – Side Pike
Back Extension Wunda Chair – Swan Basic, Back Extension Single Arm
In addition to the type of exercises noted in my conditioning program, I would recommend other
foot strengthening exercises to be done as well.
1) Doming the foot to improve the strength in the “tripod” contact points. Done either sitting
or standing.
2) Inch Worm is done by first doming the foot and then inching the heel point toward the
toe ball points, then moving the ball points away from the heel to relax the arch.
3) Toe Articulation exercises would include: Lifting toes up and separating them in the air;
Lifting the toes and lowering them one at a time; Keeping large toe down while lifting all
other toes also the reverse of this.
One final method of improving strength and alignment would be to include the Pilates Foot
Corrector exercises (see above) to my daily routine. This apparatus increases ankle stability,

12
flexibility, alignment and propulsion. It also helps strengthen and stretch the muscles of the foot
and lower leg, as well as shore up the alignment of the ankle, knee, and hip when in parallel and
externally rotated positions. If a Foot Corrector is not available, many of the same exercises can
be done with a tennis ball or other flexible ball.
Conclusion
The feet are one of the most overlooked parts of the body when it comes to people's workouts,
yet they are the foundation of the body. Like the rest of the body, to keep our feet healthy, they
need to be stimulated and exercised. Often injuries to the knee, hip and spine can be attributed to
weakness or muscle imbalance in the foot not just congenital issues such as the flat feet. This
conditioning program would be of benefit to anyone that experiences foot pain due to overuse,
poor shoe support, weakness due to overly supportive shoes or who have experienced alignment
issues of the lower extremities. Many issues will need to be treated surgically or may require
more extensive treatment from an orthopedist or physical therapist. But everyone could benefit
from increased emphasis on the feet and improve their affect on the overall functioning of the
body.

13
Bibliography
Christopher McDougall, Born to Run (New York, Knopf, May 2009)
R. Lorenzton, “Prevention and Management of Sports Injuries; Intrinsic Factors”, A. Dirix,
Howard G. Knuttgen, and Kurt Tittel, eds., The Olympic Book of Sports Medicine, (Wiley-
Blackwell (January 15, 1991), p. 376-384.
Rodney P. R. Dawber, Ivan Bristow, Warren Turner, Text atlas of podiatric dermatology
(London, Martin Dunitz Ltd, 2001)
Matthew Buchanan, MD, Gregory C Berlet, MD, FRCS(C), Abdi Raissi, MD, eMedicine
Orthopedic Surgery, February 27 2009.
Boerum DH, Sangeorzan, BJ. Biomechanics and pathophysiology of flat foot. Foot Ankle Clin N
Am. 2003(8):419-430.