The Efficacy and Safety of Topical Retinoids for ...
33
The efficacy and safety of topical retinoids for preventing and reversing the effects of photoageing: a literature review. Dr. Sarah Tranter MBBS BSc Dermatology in Clinical Practice MSc. University of South Wales. Word count: 10095 Introduction Topical retinoids are widely recognised as the gold standard in the medical treatment of the cutaneous signs of photoageing. They have the largest evidence base regarding their ability to prevent and reverse the signs of photoageing 1 . Since their discovery, retinoids have been used as topical and systemic treatments for acne, disorders of keratinisation, neoplastic disease and photoageing 2 . They have gained more traction for their use as an anti-ageing product as consumer demand grows. Our population is living longer and accumulating sun damage. The desire to reverse the UV induced photodamage of years gone by is what is driving further research into newer formulations for this indication. Understanding the (photo)ageing process in the skin and the underlying mechanisms also gives insight into cutaneous malignancy, given how strongly associated UV irradiation is with both ageing and skin cancers 2 . Novel retinoids are the current focus of photoageing research, with the goal of improving retinoid tolerance, delivery and efficacy 3 . The topical retinoids with evidence for their use in photoageing are summarised in table 1. This review aims to discuss the role of the natural, synthetic and novel retinoids in the management of photoageing, with specific regards to their efficacy and safety, with the aim of generating a retinoid hierarchy. Methods A literature review was conducted using Google Scholar (no date limit) and PubMed (no date limit), to find relevant literature using MeSH keywords including ‘topical retinoid[s]’, tretinoin, Natural retinoids Synthetic retinoids • Retinol (vitamin A alcohol) • Tazarotene • Retinyl-palmitate (vitamin A ester) • Adapalene • Retinyl-acetate (vitamin A ester) • Seletinoid G • Retinaldehyde (vitamin A aldehyde) • Tretinoin (all-trans-retinoic acid) • Novel retinoids • Isotretinoin (13-cis-retinoic acid) • Alitretinoin (9-cis-retinoic acid) Table 1. Summary of the natural and synthetic retinoids with applications in photoageing.
Transcript of The Efficacy and Safety of Topical Retinoids for ...

The efficacy and safety of topical retinoids for preventing and reversing the effects of photoageing: a literature review.
Dr. Sarah Tranter MBBS BSc Dermatology in Clinical Practice MSc. University of South Wales.
Word count: 10095
Introduction
Topical retinoids are widely recognised as the gold standard in the medical treatment of the
cutaneous signs of photoageing. They have the largest evidence base regarding their ability to
prevent and reverse the signs of photoageing1. Since their discovery, retinoids have been used as
topical and systemic treatments for acne, disorders of keratinisation, neoplastic disease and
photoageing2. They have gained more traction for their use as an anti-ageing product as consumer
demand grows. Our population is living longer and accumulating sun damage. The desire to reverse
the UV induced photodamage of years gone
by is what is driving further research into
newer formulations for this indication.
Understanding the (photo)ageing process in
the skin and the underlying mechanisms also
gives insight into cutaneous malignancy, given
how strongly associated UV irradiation is with
both ageing and skin cancers2. Novel retinoids
are the current focus of photoageing research,
with the goal of improving retinoid tolerance,
delivery and efficacy3.
The topical retinoids with evidence for their use in photoageing are summarised in table 1. This
review aims to discuss the role of the natural, synthetic and novel retinoids in the management of
photoageing, with specific regards to their efficacy and safety, with the aim of generating a retinoid
hierarchy.
Methods A literature review was conducted using Google Scholar (no date limit) and PubMed (no date limit), to find relevant literature using MeSH keywords including ‘topical retinoid[s]’, tretinoin,
Natural retinoids Synthetic retinoids
• Retinol (vitamin A alcohol) • Tazarotene
• Retinyl-palmitate (vitamin A ester) • Adapalene
• Retinyl-acetate (vitamin A ester) • Seletinoid G
• Retinaldehyde (vitamin A aldehyde)
• Tretinoin (all-trans-retinoic acid) • Novel retinoids
• Isotretinoin (13-cis-retinoic acid)
• Alitretinoin (9-cis-retinoic acid)
Table 1. Summary of the natural and synthetic retinoids with applications in photoageing.

The efficacy and safety of topical retinoids for preventing and reversing the effects of photoageing: a literature review.
isotretinoin, retinol, retinal, retinaldehyde, adapalene, tazarotene, novel retinoids, receptor selective retinoids, photo-ageing, ultra violet radiation, extrinsic ageing, heliodermatosis.
Exclusion criteria Retinoids taken orally were excluded from the review, and concerning the retinoids that can be applied topically or taken orally, only the literature pertaining to their topical use has been considered. Articles not related to photoageing and topical retinoids were also excluded.
Literature review Our skin and the ageing process The skin - our largest organ - provides essential protection from various daily environmental
exposures. Divided into three layers: the epidermis, the dermis and the subcutaneous tissue, the skin
is a complex organ with many functions in addition to environmental protection. For the purpose of
this review, the protective function of the skin will take precedence. The epidermis is composed
predominantly of differentiating keratinocytes, with melanocytes and Langerhans cells also
featuring prominently. The stratum corneum forms the barrier function of the skin, and is made up
of corneocytes, which interact with proteins such as keratin and fillagrin. Alongside this cornified
involucre, lamellar lipids fill the intercellular spaces. The combination of hydrophilic cells and
proteins, with hydrophobic intercellular material, is what is responsible for the skin barrier. The
epidermis is separated from the dermis below by a basement membrane. The dermis comprises
extracellular matrix (ECM) proteins produced by fibroblasts below. Type I collagen is the most
abundant protein in the skin, and confers structural support, alongside other ECM proteins such as
collagens III, V and VII, elastin and proteoglycans4. The main environmental insult our skin
protects us from is ultraviolet radiation (UVR), along with cigarette smoke, pollution and
occupational exposures.
Skin ageing is a complex process influenced by a number of intrinsic and extrinsic factors. Natural
metabolic processes result in the generation of reactive oxygen species (ROS) which play a crucial
role in cell ageing, and as we age, our cells naturally decline in their ability to perform their normal
function and this is genetically determined. In addition, cumulative damage to our cells, genes and
resulting proteins also results in decreased functionality, and we are dependent on cellular repair
mechanisms to avoid premature ageing and cell death5,6.
Intrinsic ageing is characterised by a general trend towards skin atrophy and decline in normal
processes and cellular functions7. Intrinsically aged skin demonstrates thinning and decreased
growth rate of the epidermis, loss of corneocyte adhesion and flattening of the dermoepidermal
Dr. Sarah Tranter MBBS BSc Professional Project MSc Dermatology in Clinical Practice 2

The efficacy and safety of topical retinoids for preventing and reversing the effects of photoageing: a literature review.
interface. Melanocyte and Langerhans cell numbers are decreased and there are alterations in
dermal collagen, elastin and glycosaminoglycans. The normal immune and inflammatory responses
are impaired and there is reduced clearance of dermal fluid and foreign materials. The
microvasculature is altered and the physiological functions of thermoregulation, mechanical
protection, sensory perception, sweat and sebum production all decline with increasing age. These
structural, cellular and histological changes correlate clinically with intrinsically aged skin on non-
sun exposed sites that appears finely wrinkled, unblemished and xerotic (figure 1A). There is
impaired wound healing, increased susceptibility to infection and increased incidence of benign and
malignant neoplasms10.
Photoageing describes the constellation of clinical, histological and functional changes in older skin
that has been frequently exposed to ultraviolet radiation. It is these features that have been super-
imposed on intrinsically aged skin, giving rise to a prematurely aged appearance. Photoageing
accounts for 90% of visible skin ageing, particularly in those with less pigmented skin types11. In
contrast to intrinsically aged skin, photodamaged skin exhibits striking alterations in the dermis and
epidermis. Epidermal dysplasia is frequent, even if there are minimal clinical changes. The
photoaged phenotype appears as rough, pigmented, lax, wrinkled and furrowed skin, with solar
elastosis - the clinical and histological hallmark of photoageing (Figure 1B). This elastic
degenerative change results from a change in fibroblasts and collagenolytic activity in the
extracellular matrix (ECM)2. The accumulation of these degenerative changes and imperfect repair
mechanisms results in progressive wrinkling, skin structural changes, vascular and pigmentary
changes12.
Dr. Sarah Tranter MBBS BSc Professional Project MSc Dermatology in Clinical Practice 3
A B
Figure 1. A. The clinical appearance of chronologically aged skin on the abdomen of an Indian woman. The skin appears xerotic with loss of elasticity and fine wrinkles. B. The appearance of photo aged skin and solar elastosis. The skin is pigmented, deeply wrinkled, rough and leathery.
A. Reproduced from Durai et al 20128. B. © Professor Raimo Suhonen. Reproduced from ‘Solar elastosis’ via DermNet New Zealand with permission9.

The efficacy and safety of topical retinoids for preventing and reversing the effects of photoageing: a literature review.
Intrinsically aged skin and photoaged skin have been shown to have some shared mechanisms such
as impaired collagen synthesis, enhanced MMP expression, increased AP-1 expression, increased
oxidative stress13,14. It has been demonstrated that tretinoin is able to improve features of
intrinsically aged skin in a similar way as it does when applied to photoaged skin. The predominant
Dr. Sarah Tranter MBBS BSc Professional Project MSc Dermatology in Clinical Practice 4
Figure 2A. Changes seen with staining of elastin in sun-protected and sun-exposed skin from 1st and 8th decades. Facial (a) and abdominal (b) skin in the first decade. Facial skin demonstrating abnormal accumulation of elastin in the 8th decade (c), in comparison to the sun-protected skin in the same age group, which demonstrates a degree of elastin preservation (d).
Figure 2B. Type I collagen staining in facial and abdominal skin taken from 1st and 8th decades. There is loss of type I collagen in the facial skin in the 8th decade (c), collagen appears preserved in the abdominal skin from the 8th decade (d), this is a result of an alteration in the ratio of type I and type III collagen.Reproduced from El-Domyati et al 200217.

The efficacy and safety of topical retinoids for preventing and reversing the effects of photoageing: a literature review.
mechanism for these improvements is by reducing MMP expression and stimulating collagen
synthesis in the dermis14.
Photoageing in the epidermis and dermis Photoageing can be further considered in terms of the epidermal and dermal changes that occur as
result of exogenous insults. Epidermal photoageing is characterised by initial epidermal hyperplasia
and then epidermal atrophy, acanthosis, cellular atypia and decreased number and function of
Langerhans cells. Slow wound healing, depigmented pseudo scars, greater melanin production in
senescent melanocytes, freckles, lentigines and other pigmentary changes are also typically
seen15,16.
Dermal photoageing is what gives rise to the typical photoaged phenotype and it is the result of
underlying degradation of connective tissue within the dermal extracellular matrix, namely collagen
and elastin. Solar elastosis describes both the clinical appearance, and underlying histological
changes, associated with dermal photoageing. Elastoid material comprising abnormal elastin,
degenerated and homogenised collagen with lack of fibrillary structure is seen in the upper dermis
with a subepidermal grenzzone of sparing. This area represents a subepidermal layer of newly
synthesised collagen seen in photo damaged skin (figure 2A17). It is thought that solar elastosis
occurs as a combination of a process of degradation of ECM proteins whereby there is an initial
phase of collection of normal elastin in the papillary and reticular dermis, followed by a destructive
phase in which elastin becomes coarse and fragmented, leading to elastolysis17. Changes to the
structure and organisation of collagen were seen as early as the 4th decade on histological
assessment of facial skin, and the accumulation of abnormal elastin, occupying areas of lost
collagen, increased with age. There is also a change in the ratio of type I and type III collagen in
intrinsically aged skin (figure 2A and B)17.
In photoaged skin there is also the presence of a chronic perivascular inflammatory infiltrate which
contains high numbers of lymphocytes, macrophages and increased numbers of partially
degranulated mast cells. Their presence causes damage to the ECM proteins by nature of
inflammatory mediated processes - degranulating mast cells in close proximity to fibroblasts
causing collagen and elastin breakdown18. The result is a UV-induced inflammatory state, which is
in contrast to the trend toward senescence and atrophy seen in chronological ageing.
Dr. Sarah Tranter MBBS BSc Professional Project MSc Dermatology in Clinical Practice 5

The efficacy and safety of topical retinoids for preventing and reversing the effects of photoageing: a literature review.
Photoageing and ultraviolet radiationPhotoageing develops gradually after years of chronic UV light exposure, which is in contrast to the
more immediate effects of UVR seen as sunburn and suntan that develop over hours to days
respectively. The main wavelengths of light responsible for photoageing are UVB and UVA. Short-
wave UVB photons (290-315nm) carry higher energy than long-wave UVA photons (315-400nm).
The energy from short-wave UVB photons is mainly dispersed in the epidermis, with less than 10%
reaching the dermis below2. The ability of UVB irradiation to also cause deeper levels of damage
by inducing matrix metalloproteinase (MMP) mRNA, protein and activity within hours of exposure
in human skin was demonstrated to occur at lower doses than required to induce skin erythema.
MMPs are a group of enzymes responsible for the degradation of collagen and elevated levels of
MMPs degrade collagen and elastin within the dermis, which over time result in a ‘solar scar’.
These results highlight the fact that underlying damage to the dermis when exposed to UV
irradiation can occur with minimal external signs on the skin19.
In contrast to UVB, ~ 50% of the energy from long-wave UVA photons reaches the dermis, and so
UVA can be said to have a more damaging effect here2. UVA is also present more consistently
throughout the year, making up a larger percentage of daily UV light (~5% of terrestrial sunlight),
Identification characteristics
Type of ageing Epidermis Dermis Clinical appearance
Chronologically aged skin
(figure 1A)
Epidermal atrophy and reduced cell turnoverReduced corneocyte adhesionFlattening of dermo-epidermal junction, loss of rete pegs
Decreased dermal collagen, elastin and GAGs, irregular arrangement of elastinImpaired immune and inflammatory responsesDecreased melanocyte and Langerhans cellsAltered microvasculature
Laxity, fine wrinklesUnblemishedDevelopment of benign growths eg seborrhoeic keratoses and angiomas
Photoaged skin
(figure 1B)
Thickened stratum corneum Increased melanosomes in basal keratinocytesActinic lentigo - hyperkeratosis and increased basal melanocytes Cellular atypia
Solar elastosis - homogenised, irregular, bunched and degraded elastin, grenz zone Decreased collagen I, III, VII (anchoring fibrils) and fibrillin in papillary dermis
Dilated and tortuous microvasculature
Wrinkles, deep furrows, laxityMottled pigmentation (hypo- or hyperpigmentation, sallownessRough skin, loss of skin tone, dryness*Solar elastosisTelangectasias, actinic purpuraPrecancerous lesions, skin cancer and melanoma
Table 2. A comparison of the clinical features of extrinsic and intrinsic skin ageing. *Note solar elastosis is the hallmark of photoageing, and describes both clinical and histological changes. Chronologically aged skin does not exhibit pigmentary or vascular changes, as seen in photo aged skin.
Dr. Sarah Tranter MBBS BSc Professional Project MSc Dermatology in Clinical Practice 6

The efficacy and safety of topical retinoids for preventing and reversing the effects of photoageing: a literature review.
and it is able penetrate through glass - something UVB is unable to do. These features of UVA mean
that UVA irradiation plays a more significant role in photoageing than it does in the acute effects of
UV exposure (sunburn/tan) or photocarcinogenesis2.
Other exogenous factors in photoageing The role of IR radiation on skin ageing
In addition to UVR, studies have shown the effect of infra-red radiation (IR) on human skin ageing.
IR does not have the photon energy of UVR, but it comprises a much greater percentage of our
cumulative exposure (54% vs 5-7% respectively). IR-A (λ = 760-1440 nm) represents
approximately 30% of total solar energy and penetrates skin deeply compared to UVR, with
approximately 50% reaching the dermis. The mechanisms for IR induced skin damage are similar to
that of UVR, and are a result of induction of MMP-1 and reactive oxygen species (ROS)20.
The role of smoking in skin ageing
Extrinsic ageing can almost be completely attributed to UV irradiation11. However, cigarette
smoking is strongly associated with elastosis in men and women, and telangectasias in men.
Smoking damages the skins microvasculature and reduces capillary blood flow, causing an oxygen
deprived state in the skin. It also induces free radial formation, damages collagen and increases
keratinocyte dysplasia. Studies have shown that smoking can be even more detrimental to the
formation of wrinkles than even UV exposure and found that smoking is an independent risk factor
for premature wrinkle formation even when controlled for age, pigmentation and sun exposure21.
The molecular mechanisms of UV induced photodamage UV radiation (UVR) is a complete carcinogen and can affect the skin in various ways, causing
direct and indirect image to DNA. UVB causes direct damage to DNA through the generation of
photoproducts such as thymidine dimers. UVA primarily causes damage through indirect oxidative
damage of guanine bases and interacts with chromophores to generate ROS. This direct and indirect
damage ultimately leads to mutation of key regulatory genes2. UVA also inhibits DNA repair by
damaging nucleotide excision repair (NER), the mechanism by which this occurs22.
The generation of ROS causes the oxidation and inhibition of protein tyrosine phosphatases, which
have an inhibitory and regulatory function for the pro-inflammatory cytokines; epidermal growth
factor (EGF), tumour necrosis factor (TNF)-α and interleukin-1 (IL-1). Therefore, in UV exposed
skin, there is up regulation of EGF, TNF-α and IL-1 in keratinocytes and fibroblasts23. This is
further compounded by the increase in nuclear factor-κB (NF-κB), releasing further pro-
inflammatory cytokines and increasing ROS24. This switches on mitogen-activated protein (MAP) Dr. Sarah Tranter MBBS BSc Professional Project MSc Dermatology in Clinical Practice 7

The efficacy and safety of topical retinoids for preventing and reversing the effects of photoageing: a literature review.
kinase pathways that lead to the degradation of extracellular matrix by the induction of transcription
factor AP-1 and subsequent matrix metalloproteinase (MMP) production25. AP-1 is constitutively
composed of c-Fos and JunD proteins (e.g c-Jun). In UV irradiated skin, increased expression of c-
Jun protein occurs within 30 minutes of UV exposure, and continues to be expressed for 24 hours26.
The heterodimer of c-Fos:c-Jun AP-1 complex up-regulates several MMPs that are the mediators of
collagen breakdown - MMP-1 (collagenase 1) degrades type I and III fibrillar collagen, MMP-9
(gelatinase B) further degrades collagen fragments, and MMP-3 (stromelysin 1) which degrades
type IV collagen in the basement membrane and activates proMMP-1. Together, these MMPs have
the capacity to completely degrade mature fibrillar collagen in the skin. Increased collagen
breakdown has been demonstrated to occur within 24 hours of UV exposure in human skin in
vivo4,25. Not only does UV irradiation cause collagen and ECM breakdown, it also impairs new type
I collagen synthesis. It decreases collagen formation19,25 and also impairs the formation of collagen
fibrils27. Type I procollagen gene transcription is negatively regulated by AP-1. Fisher et al 2000
demonstrated the reduction in type I procollagen mRNA within 8 hours of UV exposure in human
skin, and subsequent absence of procollagen mRNA and protein in the upper dermis after 24
hours28. UV irradiation also has the negative effect of impairing TGF-β signalling. This major
profibrotic cytokine regulates multiple cellular functions involving differentiation, proliferation, and
induction of synthesis of ECM proteins, and in human skin, TGF-β inhibits the proliferation of
keratinocytes, stimulates dermal fibroblast growth, and induces the synthesis and secretion of
collagen and elastin within the ECM29,30. It also inhibits MMP-1 and MMP-3. UV irradiation
impairs the TGF-β signalling pathway by reducing expression of it’s receptor protein TβRII and by
increasing the inhibitory signalling protein Smad731. Additionally, TGF-β interacts with CTGF
(connective tissue growth factor; stimulatory effect) and Cyr61 (inhibitory effect) to modulate
procollagen I production. UV irradiation inhibits CTGF gene expression via an unknown
mechanism. This can explain why UV exposure causes reduction of type I collagen production4.
Additionally, UVR alters endogenous antioxidants in the skin, and promotes angiogenesis by
increasing expression of vascular-endothelial growth factor (VEGF)23. UVB also acts via a
paracrine pathway between keratinocytes and fibroblasts to increase elastase that degrade elastic
fibres in the dermis32.
UVR also degrades proteoglycans (PG) within the extracellular matrix In photoaged skin, in addition to loss of collagen and elastin, there are changes to the structure and
distribution of glycosaminoglycans (GAGs) and proteoglycans (PGs) within the extracellular
matrix. These molecules have important roles in the assembly and structure of the ECM, and
associate closely with collagen and elastin fibres. In the skin, the most abundant GAG - hyaluronic
Dr. Sarah Tranter MBBS BSc Professional Project MSc Dermatology in Clinical Practice 8

The efficacy and safety of topical retinoids for preventing and reversing the effects of photoageing: a literature review.
acid (HA), forms aggregates of HA and HA-binding PGs which confer structure and stability to the
ECM33. Following exposure of UVR, there is abnormal accumulation of hyaluronic acid (HA), in
addition to the sulphated GAG/PGs versican and chondroitin sulphate (CS), with elastotic material
and reduced decorin within regions of solar elastosis, which is related to chronic sun exposure and
UV induced damage33. In addition, UVB irradiation decreases HA-1 synthase (along with HA-2 and
HA-3) which contributes to the loss of HA from the dermis34. The combined effect of abnormal
accumulation and decreased synthesis of, predominantly, HA compounds the loss of structural
integrity of the dermis, and contributes to the formation of wrinkles. The family of GAGs and PGs
within the ECM are a diverse group of molecules, and Lee et al (2016)33 concluded that further
research into how these changes manifest in ageing phenotypes may give rise to novel therapeutic
targets.
Summary of UVR induced mechanisms of photodamage
UVR causes photo damaged by 1) direct damage to DNA (both mitochondrial and nuclear) - e.g.
UVB causing formation of pyrimidine dimers, 2) indirect damage to DNA by the generation of
ROS - e.g. interaction of UVA with photosensitisers within the skin leading to the formation of
DNA photoproducts (e.g. abnormalities such as base dimers, DNA strand breaks and crosslinks), 3)
by damaging the ability of DNA to repair itself (NER and BER mechanisms impaired) and 4) by
interacting with cell surface receptors on keratinocytes and fibroblasts, triggering signalling
cascades involving AP-1 and NFκB, leading to the breakdown of proteins within the extracellular
matrix of the dermis. This results in a cycle of imperfect repair and ongoing damage, leading to
solar scar formation and ultimately deep wrinkling and furrows in the skin over an extended period
of time as the structural integrity of the skin is gradually broken down. The accumulation of these
repeated exposures and resulting ‘solar scars’ over years is what results in the photoaged phenotype
of prematurely aged rough, lax, skin with mottled pigmentation and leathery appearance19 (figure
1A).
Retinoids in the management of photoageing
Since being shown to improve the signs of mild to moderate photoageing by Kligman and
colleagues in 198463, there have been various large-scale, double-blind, placebo-controlled 6 month
trials that show the beneficial effects of tretinoin (and other topical retinoids) on reducing fine lines
and wrinkles and improving skin roughness. Photoageing leads to the loss of structure support
within the dermal extracellular matrix due to collagenolytic activity and reduced collagen
synthesis25. Tretinoin has been shown to restore extracellular matrix and prevent the loss of
Dr. Sarah Tranter MBBS BSc Professional Project MSc Dermatology in Clinical Practice 9

The efficacy and safety of topical retinoids for preventing and reversing the effects of photoageing: a literature review.
extracellular matrix in chronically photo-damaged skin. Pre-treating the skin with tretinoin also has
the effect of inhibiting UVR induced ECM degradation and it can restore procollagen I levels in
sun-exposed skin to the levels seen in sun-protected skin of the same subject25,35. Retinoids regulate
cell apoptosis, differentiation and proliferation. Anti-wrinkle properties of retinoids promote
keratinocyte proliferation, strengthen the protective function of the epidermis, restrain
transepidermal water loss, protect collagen against degradation and inhibit metalloproteinases
activity36. Retinoids also work by increasing epidermal thickness, increasing granular layer
thickness, compaction of the stratum corneum and decreased melanin content. These changes are
seen after 6 months of regular tretinoin use. These improvements are continued after another 6
months, however at this time point there was also regression of the epidermis. After 12 months of
use new collagen formation was demonstrated in the papillary dermis, along with dermal
reconstruction, improved DEJ adhesion and improved keratinocyte function37. These benefits have
also been observed with lower concentrations of tretinoin, for example 0.02% tretinoin used
regularly demonstrated similar histological changes after 12 months38.
Retinoids and photoageing The retinoid family comprises vitamin A (all-trans-retinol) and its natural derivatives, including
retinaldehyde, retinyl esters and retinoic acid (and its isomers), along with a number of synthetic
and novel compounds (table 1). A ‘retinoid’ can be any molecule that has the capacity to bind and/
or activate retinoid receptors, resulting in the activation of retinoid-sensitive gene transcription
elements within DNA. The stratified structure of the epidermis is organised by retinoid-influenced
cellular processes, and retinoids significantly affect dermal ageing, immune response and wound
healing39. For the purpose of this review, first generation (naturally occurring) retinoids and 3rd/4th
generation (synthetic and novel) retinoids will be considered. The second generation synthetic
retinoids acitretin and etretinate will not be considered in this review as they are approved for the
treatment of psoriasis, and have no role in the management of photoageing40. Third generation
retinoids (synthetic, receptor-specific) include tazarotene and adapalene, which have been employed
against psoriasis and acne respectively, however both show promise and benefit in photoageing40.
Fourth generation novel retinoids, such as seletinoid G, have been developed to help improve the
effects and reduce unwanted side effects, and improve patient compliance41. A prescription is
required to obtain tretinoin, isotretinoin, alitretinoin, tazarotene and adapalene, and they are classed
as drugs. The remaining retinoids, and adapalene sold as Differin, can be purchased and are
cosmeceuticals (medically active cosmetics)42. The most extensively studied, and widely used,
topical retinoid in managing photoageing is tretinoin. Topical retinoids are not the only agents that
Dr. Sarah Tranter MBBS BSc Professional Project MSc Dermatology in Clinical Practice 10

The efficacy and safety of topical retinoids for preventing and reversing the effects of photoageing: a literature review.
can be employed in the management of photodamage, and they can work synergistically with SPF,
alpha hydroxy acids (AHAs) and antioxidants. However, they are the only agents with a significant
evidence base for their use1.
Tretinoin used with SPF has been proven to be one of the most effective regimens for photoageing,
both in prevention and repair of the damage caused. SPF and tretinoin was shown to enhance the
reparative ability of the skin post UV irradiation43. AHAs (especially glycolic and lactic acid)
enhance skin exfoliation and moisturisation. Lactic acid interacts with fibroblasts to induce water
retention in the epidermis and dermis, and glycolic acid has anti-inflammatory and antioxidant
effects, it also penetrates the skin more readily than other AHAs, due to its smaller molecular size44.
AHAs in concentrations of up to 20% can be used comfortably, and AHAs can also be used in
conjunction with retinoids in a synergistic way. Tran et al (20050 demonstrated the efficacy of a
retinaldehye and glycolic acid regime in terms of enhanced bioavailability and delivery of the
retinoid while mitigating the irritant effects45. The use of antioxidants such as vitamin C and
vitamin E have also proven to be effective and complimentary in photoageing20.
Other treatments for photoageing include medium depth chemical peels, dermabrasion and light
chemical peels - but needs repetition, CO2 laser and fractionated laser. There has been some
evidence for the use of fluorouracil (Efudex) and imiquimod (Aldara) in photoageing, however
these treatments remain largely used for preskin cancers, actinic keratoses and non melanoma skin
cancer23,46.
Safety concerns and teratogenicity of topically applied retinoids Tretinoin has long been established as a safe and effective treatment for photoageing. The use of
any of the topically prescribed retinoids, at any strength, does not alter the circulating endogenous
retinoic acid level, or the levels of its metabolites and there is minimal percutaneous absorption of
topically applied tretinoin - the daily dose is approximately 30-fold lower than the lowest
teratogenic dose of isotretinoin. There have been three prospective cohort studies clearly
demonstrating the safety of tretinoin and lack of embryo toxic effects47,48,49. The long term efficacy
and safety of tretinoin has been proven by various studies. They demonstrated no cellular atypia,
with the only adverse effect being a skin irritant dermatitis, characterised by erythema, peeling and
itching. This reaction was self limiting and improved after 3 months of regular tretinoin use37.
The irritant skin reaction occurs in a predictable dose-related manner, with the retinoids most likely
to cause skin irritation being tretinoin and tazarotene, with adapalene, retinaldehyde, retinol (and
derivatives), and retinyl esters being less likely to cause significant irritation. The closer a form of
Dr. Sarah Tranter MBBS BSc Professional Project MSc Dermatology in Clinical Practice 11

The efficacy and safety of topical retinoids for preventing and reversing the effects of photoageing: a literature review.
retinoid is to retinoic acid the better and faster it works, however there is more potential for skin
irritation.
Retinoid nomenclature Vitamin A (all-trans-retinol) is an essential fat-soluble vitamin, present naturally as retinyl esters
(the main storage form of vitamin A) and beta-carotene. It is vital for many biological processes
involved in embryogenesis, reproduction, growth, vision, inflammation, cell growth and
proliferation, and cell death. The most abundant retinoid forms in the body are retinyl esters and
retinol50. Retinyl esters consumed in the diet are converted to retinaldehyde in the intestine and then
converted back to retinyl esters for storage via the liver. In the circulation retinol is bound to retinol
binding protein (RBP; figure 6), and once in the cell it is strongly associated with cytosolic retinol
binding protein (CRBP; figure 6). These specialised transport proteins allow retinoids to be utilised
in target tissues, given their hydrophobic nature51.
All-trans-retinol is a 20 carbon molecule with a cyclohexenyl ring with a 4 double bond side chain
and an alcohol end group (figure 4A). Retinol is a precursor of the active metabolite all-trans-
retinoic acid (RA), which undergoes a two-step enzymatic activation involving an initial reversible,
and rate limiting step, whereby all-trans-retinol is converted to all-trans-retinaldehyde via oxidation
of the alcohol end group; catalysed by
retinol dehydrogenase (retinol DH, figure
6). The second step is further oxidation by
retinal dehydrogenase (retinal DH) to
irreversibly convert all-trans-retinaldehyde
to all-trans-retinoic acid, or tretinoin (RA),
the active metabolite (figure 4A; figure 6).
Tretinoin has two stereoisomers; 9-cis-
retinoic acid (alitretinoin) and 13-cis-
retinoic acid (isotretinoin) which are formed
via a non-enzymatic process (figure 4B). 13-
cis-retinoic acid is less transcriptionally
active than the all-trans and 9-cis isomers.
The numbering of carbon atoms in all-
trans-retinoic acid, and stereoisomer forms
9-cis-retinoic acid and 13-cis-retinoic acid,
Dr. Sarah Tranter MBBS BSc Professional Project MSc Dermatology in Clinical Practice 12
Figure 4. Nomenclature of the natural retinoids.
Reproduced from Fitzpatrick’s Dermatology in General Practice (2003). McGraw-Hill

The efficacy and safety of topical retinoids for preventing and reversing the effects of photoageing: a literature review.
can be seen in figure 4B. In addition to retinaldehyde and retinyl esters, all-trans-retinol is
metabolised to 4-hydroxy-all-trans-retinoic acid and 4-oxo-retinoic acid (figure 4C) by a
hydroxylation reaction and subsequent oxidation reaction. These hydroxy- and oxo- forms are less
active forms of retinoic acid and are 10-fold less potent at inducing retinoic acid-dependent
responses within the cell, and these forms are likely destined for elimination50,52.
The esterification of retinol with a fatty acyl group generates the storage form of retinol; retinyl
esters (figure 4D). The most abundant esters are those of palmitic, oleic, stearic and linoleic acids50.
The predominant catalyst for this esterification reaction in the skin is Lethicin:retinol
acyltransferase (LRAT; figure 6). Retinyl esters have no known biological activity except to serve as
the storage form of retinol and the substrate for the visual chromophore 11-cis-retinal50. Hydrolysis
of a retinyl ester generates retinol, which then undergoes 2-step oxidation to form RA.
Retinoid metabolism in the skin and mechanism of action When tretinoin is applied topically to human skin, ~50% remains in the active form, the remaining
50% is either isomerised or hydroxylated to 4-hydroxy-all-trans-retinoic acid [DUELL et al 1992].
Topically applied retinoids act via two pathways - the transepidermal pathway and the
transfollicular pathway. The transepidermal pathway gives rise to an epidermal/dermal gradient of
retinoid penetration, which is highly important for disorders of keratinisation. The transfollicular
pathway sees higher association of retinoid to the follicle, linking to its MOA in acne. Spill over to
the systemic compartment from either route is so minimal that circulating levels remain unaltered47.
Once retinoic acid (RA) is generated in the cell, it associates strongly with cytosolic retinoic acid
binding protein (CRABP), of which there are 2 forms, CRABP I and CRABP II, the predominant
form in skin is CRABP II. The expression of CRABP II genes can be used as a marker of retinoid
biological activity53. The RA-CRABP II complex is transported to the nucleus where it binds with
nuclear RA receptors (RARs) and retinoid X receptors (RXRs; figure 6)36,51. The discovery that
these retinoid-specific receptors shared similar features in the DNA binding regions as the thyroid
and vitamin D receptors was first demonstrated in 1987, forming our understanding today that the
RARs function as hormone receptors to activate gene transcription54,55. RA binds RAR and the
isomerisation to 9-cis-retinoic acid allows for binding to the RXR. RAR and RXR form
heterodimers (they are also are capable of forming heterodimers with thyroid and vitamin D
receptors) and they form homodimers that bind RA response elements (RARE) in DNA to change
gene expression through activation and repression of target genes50.
Dr. Sarah Tranter MBBS BSc Professional Project MSc Dermatology in Clinical Practice 13

The efficacy and safety of topical retinoids for preventing and reversing the effects of photoageing: a literature review.
RAR and RXR subtypes are as
follows; RAR-α, RAR-β, RAR-γ,
and RXR-α, RXR-β, RXR-γ. Elder
et al (1992)56 found that human
epidermis expresses RAR-α and 𝛾,
and RXR-α, while RXR-β is
expressed by dermal fibroblasts50.
Roughly 90% of the RAR present in
skin is the RAR-𝛾 subtype and 90%
of the RXR present is RXR-α
subtype58. It has been demonstrated
that normal human epidermis is
regulated by a heterodimer of
RXR-γ and RAR-α , with the RAR-
α portion of the heterodimerbeing
responsible for binding to RARE,
however this would not occur
without the presence of the RXR-𝛾 element56,57. Wang et al (1999) demonstrated that UVR causes a
decrease in the expression of RAR/RXR, and that pre-treatment of the skin prior to UV irradiation
was able to improve this59. In addition to the RAR/RXR subtype, there are also RAR/RXR isomers
and together they form a highly diverse group of retinoid-responsive receptors12,58.
Receptor-selective retinoidsThe discovery of the various retinoid receptor subtypes has lead to the development of synthetic
retinoids that are receptor specific. Adapalene is a third generation, receptor-selective retinoid, with
a napthoic acid base (figure 5). It shows affinity for the RAR β/𝛾 receptors, and does not directly
bind CRABP II but has been shown to have the capacity to induce CRABP II mRNA60.
Tazarotene is the precursor to tazarotenic acid and an analogue of tretinoin (figure 5). It cannot itself
bind directly to RAR/RXR. Tazarotenic acid is the active form and has affinity for the RARs
(RARβ > RARγ > RARα)61.
There is naturally a great variability between the retinoids, in part due to their differing chemical
structure conferring varying degrees of binding and receptor selectivity between them. The retinoids Dr. Sarah Tranter MBBS BSc Professional Project MSc Dermatology in Clinical Practice 14
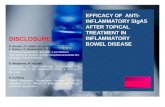
Fig. 6 Overview of retinoid metabolism (Note: Retinol is oxidised to retinoic acid in two steps: retinol is reversibly oxidised by retinol dehydrogenase to give retinal, then retinal is irreversibly oxidised by retinal dehydrogenase to give retinoic acid). CRABP cytosolic retinoic acid binding protein, CRBP cytosolic retinol binding protein, LRAT lecithin retinol acyltransferase, RA retinoic acid, RAR retinoic acid receptor, RARE retinoic acid response element, RBP retinol-binding protein, Retinal DH retinal dehydrogenase, RXR retinoid X receptor, TTR transthyretin
Reproduced from Riahi 201650

The efficacy and safety of topical retinoids for preventing and reversing the effects of photoageing: a literature review.
are a diverse group of molecules that modulate the expression of
genes involved in cellular differentiation and proliferation,
resulting in normalising cell keratinisation42.
The topical retinoid family
1. Tretinoin (table 3-1)
Tretinoin was found incidentally to improve the appearance of
fine lines in patients using topical tretinoin for acne62. This
finding generated interest in the potential for tretinoin to be used
in photoageing, and this was further investigated using the
hairless albino mouse model as a surrogate for human skin.
These mice were irradiated with UVB for a period of 10 weeks, during which time they developed
fine wrinkles and the histological features of solar elastosis63. Tretinoin was then applied for a
further 10 weeks, during which time the authors found there was the generation of a subepidermal
collagen repair zone that correlated clinically with wrinkle effacement63. The same authors were the
first to conduct an in vivo trial of the effect of 0.05% tretinoin in photo aged skin of the face and
forearms of volunteers over 3-10 month period. They found significant improvements in wrinkling
that correlated with the animal model in 1984. The first vehicle-controlled trial looking at the
efficacy of tretinoin in photoageing was in 1988. 0.1% tretinoin emollient cream was applied daily
to the face and forearms for a period of 4 months64. After 4 months there was significant
improvement in the tretinoin treated skin vs. the vehicle treated skin in terms of fine wrinkling,
coarse wrinkles, sallowness, tactile roughness, and actinic lentigines. The authors noted the main
side effect of treatment was the development of a skin irritant reaction, characterised by erythema,
scaling and pruritus, which occurred in approximately 90% of participants64. Within the following
years, the results of 2 large, multi centre trials confirmed that tretinoin was an effective treatment
for photoaged65,66. They enrolled a total of 547 subjects, 393 of which used topical tretinoin in
varying concentrations (0.001% - 0.05%), and their conclusion was that 0.05% tretinoin applied
daily for 6 months was effective at improving fine wrinkling, mottled hyperpigmentation and skin
roughness that result from chronic UV exposure. These clinical improvements correlate with
histological findings of increased stratum corneum compaction, spongiosis, thickened granular
cellular layer, increased basal keratinocyte turnover and increased mucin deposition65,66.
In an attempt to answer the hotly debated question at the time of whether the improvement seen
with topical tretinoin application was a result of the irritant skin reaction that was observed, a study
comparing two different concentrations of retinoic acid 0.025% and 0.1%, was conducted over a
Dr. Sarah Tranter MBBS BSc Professional Project MSc Dermatology in Clinical Practice 15
Figure 5. Nomenclature of the receptor-selective retinoids adapalene and tazarotene.Reproduced from Fitzpatrick’s Dermatology in General Practice (2003). McGraw-Hill

The efficacy and safety of topical retinoids for preventing and reversing the effects of photoageing: a literature review.
period of 48 weeks, and found no significant difference in clinical efficacy between the two
concentrations67. This would imply that the results seen from tretinoin in the skin are independent
of the irritant effect it can cause.
Long term use of tretinoin in photoageing Since the 1980’s there have been many studies that have confirmed the efficacy of tretinoin in
treating the clinical and ultrastructural changes associated with photoageing both in the short and
long term. Kang et al (2005) reported the results of a 2 year vehicle controlled trial of once daily
0.05% tretinoin cream vs vehicle in 204 subjects. Significant improvements in photoageing,
specifically fine wrinkles were demonstrated after 4 months, and continued throughout the 2 year
time frame for the study68. Sustained improvement with topical tretinoin use has been shown after 4
years without detrimental effects on keratinocytes and melanocytes, and with improvements in
epidermal mucin seen at biopsy. In addition to the benefits seen over the short term, long term
therapy decreased dermal elastin content and perivascular inflammation. These changes could
possibly account for the observed continued clinical improvement69,70.
Furthermore, Kligman and Graham (1993) reported that there was markedly reduced density of
melanosomes in the basal layer and they demonstrated the formation of a band of new subepidermal
collagen, evidence of resorption of abnormal and amorphous elastic material, formation of new
reticulin and reduction in GAGs71. This would imply that the long term benefits of tretinoin therapy
can reverse the damage seen with photoageing and encourage normalisation of the epidermis and
dermis.
In addition to the improvements observed with wrinkling, tretinoin also has beneficial effects on
hyperpigmentation that is associated with photoageing. There have been a number of 10 month
studies looking at the efficacy of 0.1% tretinoin in photoageing, that have found significant
improvements in pigmentation. These studies have then been extended, and found that tretinoin
0.1% improved epidermal turnover and thickness and also reduced the number and activity of
melanocytes72,73,74. Another double-blind, vehicle-controlled study examining the effect of 0.1%
tretinoin vs vehicle over 4, 10 and then 22 months found a 71% reduction in discrete lentigines
compared to the number present prior to treatment. An improvement in hyperpigmentation is a
result of dispersion of melanin granules thereby improving the appearance of pigmentation. The
lightening of actinic lentigines and mottled hyperpigmentation correlates with a reduction in
epidermal melanin content maybe resulting from inhibition of tyrosinase activity75,76.
Sorg et al (2005) proposed that retinoids can also improve photoaging due to their chemical
structure and their conjugated double bonds. These structural features allow them to absorb free
Dr. Sarah Tranter MBBS BSc Professional Project MSc Dermatology in Clinical Practice 16

The efficacy and safety of topical retinoids for preventing and reversing the effects of photoageing: a literature review.
radials and oxidative damage, thereby being able to protect DNA, lipid membranes and proteins by
directly preventing photochemical damage or UV-induced oxidative stress77.
The overwhelming evidence for efficacy for tretinoin in photoageing is such that patients should be
advised it is not a cosmetic preparation and there should be appropriate counselling on the
appropriate frequency and method of application for maximal benefits to be obtained. Daily
application of tretinoin for at least 3 months is required to see improvements78.
The beneficial effects of continuing with tretinoin therapy in the long term, but with reduced
frequency of application has also been proven74,79. 126 participants who completed 48 weeks of
daily 0.05% tretinoin use were continued on a three weekly, once weekly or no treatment dosing for
a further 24 weeks. Those who continued on a three weekly and, to a lesser extent, those on a once
weekly dosing schedule maintained and in some cases contained to see improvements. In those
subjects who were assigned to no therapy, the authors found regression in the areas of improvement
obtained from prior treatment79.
1a. Comparison of tretinoin with other retinoids
A randomised trial comparing 0.25%/0.5%/1.0% cosmetic formulations of retinol (with added
agents for optimal irritation control) vs 0.025%, 0.05%, 0.1% tretinoin. Participants were
randomised to receive either 0.025% tretinoin and 0.25% retinol, 0.05% tretinoin and 0.05% retinol,
or 0.1% tretinoin and 1.0% retinol in a split face trial over 12 weeks, with clinical photos at 0, 4, 8,
12 weeks. 65 subjects took part in the trial. After 12 weeks both retinol and tretinoin groups had
statistically significant improvements in the measured parameters of photoageing (fine and coarse
lines/wrinkles, pigmentation, skin tone, brightness, tactile roughness). There were no significant
differences in efficacy between tretinoin and retinol, and retinol produced comparable results to
tretinoin80. Draelos and Peterson (2020) reported results of a step up protocol for increasing dose of
retinol serum vs tretinoin cream in combination with a test moisturiser over 12 weeks. Their aim
was to achieve the rapid benefits of retinisation, but with minimal irritation. At 12 weeks there was
no statistically significant difference between the retinol serum vs tretinoin cream in patient
assessment of improvement in clinical signs of photoageing. Difference in TEWL with the two
products was also not statistically different. However, the retinol serum group showed marked
improvement in skin smoothness at week 4 and highly significant improvement skin dryness with
this group (not seen in tretinoin group). Punch biopsies taken at 12 weeks also demonstrated newly
formed collagen and epidermal thickening in the retinol serum group, compared to tretinoin
group81. Bouloc et al (2015) compared 0.025% tretinoin with a combination product containing
retinal and tetrahydrojasmonic acid (LR2412). LR2412 is a plant-derived hormone from linoleic
Dr. Sarah Tranter MBBS BSc Professional Project MSc Dermatology in Clinical Practice 17

The efficacy and safety of topical retinoids for preventing and reversing the effects of photoageing: a literature review.
acid and is part of a family of compounds that were originally isolated from the jasmine plant.
These compounds have been shown to have beneficial effects in epidermal hyaluronic acid in
human skin83. In this study retinol 0.2% combined with 2% LR2412 was compared to tretinoin
0.025%. Participants used SPF 50 in the morning and either retinol or tretinoin at night. The results
showed no difference between groups in clinical outcome, but retinol/LR2412 was better perceived
and tolerated by participants82. Fu et al (2010) evaluated another cosmetic based preparation with
0.02% tretinoin. A niacinamide⁄peptide⁄retinylpropionate product regimen vs. a prescription 0.02%
tretinoin product regimen was tested over 24 weeks. After 8 weeks those using the cosmetic
preparation reported better improvement wrinkle appearance. This had equalised between the
groups after the full 24 weeks. The cosmetic preparation was better tolerated than the 0.02%
tretinoin throughout all parameters after 8 weeks (erythema, perceived dryness from participants,
TEWL and thinner stratum corneum)84.
2. Retinol (table 3-2)
In photoageing, retinol is used in a cream formulation in concentrations ranging between 0.075% to
1%. It is often considered the “lighter alternative” to tretinoin in patients with sensitive skin42.
However it is regarded as approximately 20-fold less efficacious than tretinoin and a much higher
concentration of retinol required to match the outcomes seen with tretinoin. However, retinol
applied to normal human skin does induce the expression of CRABP-II and CRBP mRNAs and
proteins, similarly to retinoic acid, but without the irritation and erythema85. Retinol is extremely
unstable and easily degraded to biologically inactive forms on exposure to UV light, and there are
few formulations available that offer a stable and appropriate concentration of retinol to be
effective86.
3. Retinol derivatives e.g. retinyl esters, combinations (table 3-3a)
Developed to combat the inherent instability of retinol, retinol derivatives are now widely used in
cosmetic and OTC products instead of retinol. There has been some evidence of their efficacy in
treating photoageing, with Han and colleagues (2003) developing various retinol derivatives for use
in anti-aging products. An in-vitro study found that N-formyl aspartame derivative has potential due
to good photo stability and its ability to interact well with fibroblasts and suppress collagen
breakdown87. However, not all retinol derivatives are equal, and despite initial promise in in-vitro
studies using animal models (induction of epidermal thickening and collagen formation in UV
irradiated mouse tails), retinyl propionate 0.15% did not translate to a signifiant effect in vivo when
Dr. Sarah Tranter MBBS BSc Professional Project MSc Dermatology in Clinical Practice 18

The efficacy and safety of topical retinoids for preventing and reversing the effects of photoageing: a literature review.
compared to placebo88. Results of a current clinical trial comparing the clinical efficacy and side
effect profile of bakuchiol and retinol in cuteaneous facial photoageing was published in 2019.
Randomised, double-blind trial over 12 weeks in 44 participants. Both agents significantly
decreased surface wrinkles and pigmentation with no statistically significant difference between
them. Retinol was more irritating, with users reporting stinging, erythema and scaling. This trial is
ongoing and is the only currently active clinical trial listed on clinicaltrials.gov looking at retinoids
in the management of photoageing89.
3a. Retinol combinations (table 3-3a)
Retinol combinations can offer significant benefits when combined with the right agent e.g. hydroxy
acids, hydroquinone or ascorbic acid. Evaluation of the efficacy of retinol 0.1% and glycolic acid
8% combination compared with each agent individually on photo damaged forearms, results
showed the combination offered significant improvement than either agent alone90. Retinol 0.3%
plus hydroquinone 4% compared to 0.05% tretinoin in treatment of photoageing - combination
product significantly improved the collective signs of photodamage, including dyspigmentation,
fine wrinkles, tactile roughness within 16 weeks of treatment91.
2 double blind vehicle controlled trials have been conducted to investigate the effect of retinol and
vitamin C combination in 2 different formulations. Study 1 looked at 0.07% retinol and 3.5%
vitamin C applied twice daily over 3 months. Study 2 compared 0.04% retinol and 3% vitamin C
applied twice daily over 6 months. After 3 months results showed thinning of stratum corneum,
increased epidermal thickness and increased interdigitation at the dermo-epidermal junction, and
after 6 months dermal changes were evident including improvement in type III-to-type I
procollagen ratio and an increase in size and frequency of the grenz zone in vitamin C and retinol
treated groups compared to vehicle controls, with the authors concluding that topical application of
preparations containing retinol and vitamin C can reverse, in part, the changes induced by
photoageing92.
A formulation containing an AHA (lactic acid) double conjugated with retinoid cream was
compared to 1.0% retinol and 0.025% tretinoin in a randomised split face trial over 12 weeks.
Retinoid conjugated with lactic acid, formed via double hydrolysis, allows the controlled release of
both agents via the breakdown of the ester bonds that hold the two molecules together. This process
is catalysed by enzymes naturally occurring in the skin. Less irritation was reported compared to
retinol or tretinoin, and significantly improved fine lines/wrinkles, erythema, dyschromia, skin tone
and pore size, with the AHA-retinoid formulation. Improved skin hydration was seen with AHA-
Dr. Sarah Tranter MBBS BSc Professional Project MSc Dermatology in Clinical Practice 19

The efficacy and safety of topical retinoids for preventing and reversing the effects of photoageing: a literature review.
retnoid cream and not with tretinoin or retinol. AHA-retinoid cream offers increased molecular
stability, reduced irritation, and improved passage through the skin44.
4. Retinaldehyde (table 3-4)
Retinaldehyde, or retinal, is the oxidised form of retinol and the immediate precursor to retinoic
acid. Formulated as a cream or gel in concentrations between 0.015% to 0.1% it has shown promise
in the treatment of photoageing. A pilot clinical tolerance study by Saurat et al (1994) followed 129
patients who applied varying concentrations of retinaldehyde cream (0.05%, 0.1% and 0.5%) over a
1-3 month period. They found that topical application of retinaldehyde induces CRABP II mRNA
and protein, and significantly increases the epidermal thickness in a dose-dependent manner93. The
efficacy of 0.05% retinaldehyde has been compared to 0.05% tretinoin, and retinaldehyde vehicle,
when applied to the face of 125 patients followed over a 44 week period, with follow up at 18
weeks and 44 weeks. Both tretinoin and retinaldehyde reduced roughness and wrinkles after 18
weeks, and these effects were maintained but had plateaued by week 44. Retinaldehyde 0.05% had
efficacy similar to 0.05% tretinoin but was found to be significantly less irritating94,95. Kwon and
colleagues assessed the efficacy of 0.1% and 0.05% retinaldehyde in 40 Korean volunteers who
applied the cream twice daily for 3 months. They found that there was improvement in overall
photoageing with both 0.1% and 0.05%, and both preparations improved skin texture, reduced
TEWL and increased skin hydration, without any statistical significance between groups.
Retinaldehyde 0.1% improved the melanin index by 6.5% (the 0.5% concentration did not affect
this parameter significantly)96.
5. Isotretinoin (table 3-5)
Isotretinoin (13-cis retinoic acid) in topical preparations is available as a 0.05% cream or gel. More
commonly administered as the oral agent Accutane for cystic and severe acne, topical isotretinoin
can also have beneficial effects in treating the signs of photoageing. A double-blind randomised-
control trial involving 776 patients compared the efficacy of the application of vehicle or 0.05%
isotretinoin cream nightly for 12 weeks, followed by application of 0.1% isotretinoin cream for the
next 24 weeks. When compared with vehicle, treatment with 0.05% and then 0.1% isotretinoin
resulted in statistically significant improvement in overall appearance, fine wrinkling, discrete
pigmentation, sallowness, and texture. Isotretinoin cream was well tolerated over the 36 week
period97. There have been no studies directly comparing isotretinoin to tretinoin in terms of efficacy.
6. Alitretinoin (table 3-6)
Dr. Sarah Tranter MBBS BSc Professional Project MSc Dermatology in Clinical Practice 20

The efficacy and safety of topical retinoids for preventing and reversing the effects of photoageing: a literature review.
Alitretinoin (9-cis-retinoic acid) is an approved topical treatment of Kaposi sarcoma. The
theoretical benefit of alitretinoin 0.1% gel for photoageing stems from its ability to bind all subtypes
of RAR and RXR receptors, thus promoting the repair mechanisms within photo damaged skin. An
open label study including 20 participants looked at the use of 0.1% alitretinoin gel in photoageing.
It was well tolerated and participants showed improvements in benign skin lesions (eg seborrhoeic
keratoses) and precancerous lesions such as actinic keratoses. However, larger clinical trials are
needed to further investigate the use of alitretinoin for this indication98. There have been no studies
directly comparing alitretinoin to tretinoin in terms of efficacy, and alitretinoin is not a topical
retinoid that is currently routinely used in the treatment of photoageing.
7. Tazarotene (table 3-7)
Tazarotene is the precursor to tazarotenic acid and an analogue of tretinoin, and is usually available
in 0.05% and 0.1% gel and cream. It binds to RAR-β and RAR-γ subtypes only. Used in acne,
psoriasis and photoageing, it enhances keratinocyte turnover, normalises keratinocyte differentiation
and is anti-inflammatory99. In acne and psoriasis it is usually combined with topical antibiotics and
topical corticosteroids respectively100. There have been a number of large, multi-centre trials
comparing tazarotene in varying concentrations, and tazarotene with tretinoin 0.05% and vehicle. In
2001, Kang et al., conducted a 24 week, multi-centre, randomised control trial with 349 patients
enrolled, comparing the efficacy of tazarotene 0.01%, 0.025%, 0.05%, and 0.1%, with tretinoin
0.05% and vehicle101. All concentrations of tazarotene and 0.05% tretinoin improved the appearance
of wrinkles and pigmentation. 0.1% tazarotene had the biggest improvement at 67%, followed by
0.05% tretinoin (55%), 0.05% tazarotene (52%), 0.025% tazarotene (36%) and 0.01% tazarotene
(41%). There was also increasing chance of skin irritation with increasing strengths of tazarotene
and with tretinoin. However, the reaction was limited to a mild-moderate irritant reaction that was
self limiting101. A further 24 week, vehicle-controlled trial by the same authors concluded that 0.1%
tazarotene was particularly efficacious in relation to the speed in which participants saw
improvements in wrinkles, hyperpigmentation, lentigines, pore size, elastosis, tactile roughness and
overall integrated assessment of photodamage, with some seeing improvement after 2 weeks, and
the majority having reported improvement after week 4. Improvements continued and did not
plateau by week 24102. Lowe et al (2004) further backed up these findings in a study comparing
0.05% tretinoin with 0.1% tazarotene over 24 weeks. The results indicated that tazarotene can offer
a faster improvement in the clinical signs of photoageing103. These impressive clinical results were
supported by Machtinger et al (2004), who reported the histological findings after 24 weeks of 0.1%
Dr. Sarah Tranter MBBS BSc Professional Project MSc Dermatology in Clinical Practice 21

The efficacy and safety of topical retinoids for preventing and reversing the effects of photoageing: a literature review.
tazarotene application to photo damaged skin. There was amelioration in keratinocyte and
melanocyte atypia, increased epidermal thickness and improved epidermal polarity104.
There have been further, interesting studies that seem to indicate that tazarotene may offer another
advantage over tretinoin in terms of treating the photoaged phenotypes in which pigmentation may
feature more prominently. An RCT comparing 0.1% tazarotene vs adapalene 0.3% gel in patients
with post inflammatory hyperpigmentation (PIH) and acne found that tazarotene was more effective
than adapalene at improving the appearance of pigmentation associated with PIH105. Further
evidence for early improvements in mottled hyperpigmentation, as early as 2 weeks, were
demonstrated by Phillips (2004) who looked at 0.1% tazarotene vs vehicle over a 24 week period,
and then continued with an open label extension with 0.1% tazarotene for a further 28 weeks.
Within 4 weeks there were improvements in lentigines and irregular pigmentation, fine wrinkling
improved within 8 weeks, elastosis, roughness and coarse wrinkling had improved by 12 weeks.
These improvements were continued in the 28 week extension period105,106.
8. Adapalene (table 3-8)
A third generation, receptor specific retinoid, with napthoic acid base. Adapalene behaves similarly
to tretinoin but is photochemically and chemically stable. Adapalene is already approved for the
treatment of acne and is highly beneficial in regulating abnormal desquamation of the skin, cellular
differentiation and inflammation107. Adapalene binds more readily to RAR-β, with low affinity for
RAR-α and no cross-reactivity with RXR subtypes. This indicates that adapalene affects the
terminal differentiation pathway of epidermal cells rather than their proliferation107,108. Adapalene
has also been indicated in photoageing. Once daily application of adapalene 0.1% gel for 4 weeks,
followed by twice-daily application for up to 9 months significantly reduced AK and lentigines109.
Adapalene 0.1% gel applied under occlusion for 4 days demonstrated the ability to induce
expression of CRABP-II at 70% of the potency of tretinoin 0.1% under the same circumstances.
Tretinoin induced erythema, epidermal hyperplasia and spongiosis, whereas both vehicles and 0.1%
adapalene did not. CRABP-II gene expression is more useful marker of retinoid biologic activity
than skin erythema or changes in epidermal morphology or differentiation110.
Adapalene comparison studies Adapalene 0.3% gel was shown to be non-inferior to 0.05% tretinoin cream, with a similar safety
profile and effective in global cutaneous photoageing, periorbital wrinkles, ephelides/melanosis,
forehead wrinkles and AK. Can be considered safe and effective treatment for mild or moderate
photoageing111. The cumulative irritation potential of adapalene 0.1% gel and 0.1% cream was
Dr. Sarah Tranter MBBS BSc Professional Project MSc Dermatology in Clinical Practice 22

The efficacy and safety of topical retinoids for preventing and reversing the effects of photoageing: a literature review.
compared with erythromycin (4%)/tretinoin (0.025%) gel, erythromycin (4%)/tretinoin (0.025%)
solution, erythromycin (2%)/isotretinoin (0.05%) gel, and white petroleum as a control. Adapalene
showed itself to be only slightly more irritating than the control (mean cumulative irritation index of
0.25-1), and was significantly less irritating than any of the tretinoin/erythromycin products (P <
0.01). Despite this study looking at the indication of acne, parallels can be drawn when decisions
need to be made on an appropriate retinoid to use in those with acne and photoageing - adapalene
would be beneficial in these cases given its low irritation112. Clinical trials have found that 0.1%
adapalene works faster than 0.025% tretinoin, the most commonly used retinoid, and with less
irritation113.
9. Novel retinoids Various receptor-selective and function-specific retinoids are in experimental stages. Focusing on
selective targets can offer a more narrow therapeutic indication and reduce unwanted side effects.
Current research is focused on “function-specific” retinoids, for example retinoid receptor
antagonists which have implications in the management of mucocutaneous toxicity associated with
retinoids114. With regard to the current research into topical novel retinoids for photoageing, 2 such
agents are discussed below, neither of which are in current clinical use.
9a. Seletinoid G (table 3-9a)
Kim et al (2005) developed a novel synthetic retinoid seletinoid G, using computer-aided molecular
modelling. They applied seletinoid G and tretinoin, under 4-day occlusive dressing, to the buttocks
of 23 subjects and measured skin erythema and cutaneous blood flow (markers of skin irritation),
and also measured the expression of MMP-1 in biopsied taken from the treated areas. The results of
this study showed that seletinoid G did not induce any skin erythema, in contrast to tretinoin which
induces severe erythema. Seletinoid G also induced the expression of procollagen I, tropoelastin
and fibrillin-1, and a reduction in MMP-1115.
Lee et al 2020 demonstrated that seletinoid G promotes the proliferation and migration of
keratinocytes in vitro. They also found that seletinoid G improved wound healing and closure, and
increased dermal collagen in human skin equivalents exposed to UVB irradiation116.
9b. N-retinoyl-D-glucosamine (GRA) (table 3-9b)
A retinoic acid agonist, compared with retinoic acid in photoaged mice. To determine RAR/RXR
activity. Hairless mice irradiated for 10 weeks UVB - then treated with 8 weeks of either RA 0.05%
vs GRA 0.05%, expression of RAR-α and RXR-α. Clinically both agents improved wrinkles caused
Dr. Sarah Tranter MBBS BSc Professional Project MSc Dermatology in Clinical Practice 23

The efficacy and safety of topical retinoids for preventing and reversing the effects of photoageing: a literature review.
by UVB irradiation - promoting wide repair zone and expression of type I collagen. GRA did not
produce erythema or roughness, or TEWL as compared to RA. GRA resulted in a significant, dose-
dependent transcription of RAR 100 time potency of RA, GRA did not induce RXR at all117.
Factors affecting the efficacy of topical retinoid application There are a variety of factors that will affect the efficacy of topical retinoids, including the
formulation and concentration of retinoid, the vehicle used, the frequency and consistency of
application, the degree of baseline photodamage and degree of pigmentation, the patients skin type.
Previous studies with participants lost from the study have indicated that the irritant reaction caused
by the use of topical retinoids has caused issues with patient compliance, and in a significant
number of cases cessation of use. It would follow then that minimising the irritation associated with
topical retinoid use would improve compliance of retinoid use. The factors influencing cutaneous
irritation involve an interplay between patients individual differences in skin sensitivity, the
concentration of the applied retinoid, and vehicle formation. To optimise tolerance both the
concentration and delivery vehicle can be adapted118.
The role of retinoid formulation on efficacy and tolerance Retinoic acid has limitations due to its inherent photo-instability, low aqueous solubility, and
cutaneous irritant effects3. These factors must be mitigated to deliver RA to the skin where it can
exert its effects and increase patient compliance. In order to achieve this, various formulations for
delivery of typical retinoids have been developed; traditional vehicles such as emulsions, gels,
liposomes and polymeric nanoparticles, which in some cases have been modified to target specific
tissues and cells of interest119; compared tretinoin 0.025% was conjugated with polyolprepolymer-2
(PP-2) and compared to standard gel formulation of tretinoin 0.025%. The conjugated formulation
decreased the penetration of tretinoin and enhanced epidermal deposition. It is able to do this by
forming a liquid polymer containing solubilised tretinoin on the epidermis that was shown to
become established in the epidermis 15 minutes after application119.
Further advances and research into topical drug delivery systems; They can roughly be categorised
into 1) phospholipid-based particles, 2) polymeric nanoparticles, and 3) retinoid-conjugated
polymers, in varying sizes (100-400nm) with either neutral (liposomes) or negative charge (SLN,
NLC, polymeric nanoparticles)3. These formulations have demonstrated high retinoid entrapment
efficiency (~65%), a 2-3 fold higher photostability than tretinoin in ethanol, and higher stability
under normal storage conditions3.
Dr. Sarah Tranter MBBS BSc Professional Project MSc Dermatology in Clinical Practice 24

The efficacy and safety of topical retinoids for preventing and reversing the effects of photoageing: a literature review.
Newer nanostructured formulations, such as solid lipid nanoparticles (SLNs) and nanostructure
lipid carriers (NLCs), have been found to further enhance retinoid delivery and have become the
target of the cosmeceutical industry in the quest for formulations that are efficacious and well
tolerated by consumers. The nanoencapsulation of tretinoin in a lipid core polymeric nanocapsule
improved the photo stability and reduced the skin permeation of tretinoin. It does this by retaining
the drug on the surface of the skin for longer, prolonging the half life of tretinoin by 7 times and
reducing the degradation of tretinoin by UVA120. Further support of the nanoparticle method of
delivery has been demonstrated by Puglia and Bonina (2012)121. They demonstrated that solid lipid
nanoparticles (SLNs) and nanostructure lipid carriers (NLCs) increased the efficacy and delivery of
cosmeceutical and dermal pharmaceutical drugs to the epidermis. Furthermore, they were
completely biodegraded and were felt to offer greater efficacy when compared to emulsions,
liposomes and polymeric nanoparticles delivery systems121.
Most recently, Raminelli et al 2018 have found that tretinoin in small unilamellar vesicles promoted
greater cutaneous delivery and retention in the skin of RA, even more so when the lipid carried a
negative charge122. Rahimpour and Hamishehkar (2012) found that liposomes enhance the topical
delivery of tretinoin and improve skin moisturisation when used. They allow for better penetration
into the dermis due to their structure being similar to biological cell123. In a pilot trial involving
acne patients, retinoic acid in liposomal delivery system enhanced the penetration of RA into the
stratum corneum124. Tretinoin complexed with cyclodextrin (Cyd; an oligosaccharide) was found to
be less irritating and less inflammation-inducing than tretinoin in a double-blind trial involving 12
participants. They found that the RA-Cyd complex had an equal effect to RA in improving wrinkle
scores, skin elasticity and wrinkle area, and both agents induced epidermal hyperplasia125.
Formulations enhancing target area of action of retinoid Sardana et al 2003 reported the ability of a tretinoin gel microsphere formulation (10-20μm) to
target the follicle in acne patients. The gel microsphere formulation was found to accumulate
preferentially at the follicle and so can be targeted towards this site, particularly useful in acne, a
disorder of the follicular unit126.
Discussion
Can we make conclusions about a hierarchy of retinoids?
The overwhelming evidence for the efficacy of topical retinoids in preventing and reversing the
clinical and histological features of photoageing has been demonstrated by various groups and in
various patient populations. Tretinoin is the oldest, and most commonly used retinoid for this Dr. Sarah Tranter MBBS BSc Professional Project MSc Dermatology in Clinical Practice 25

The efficacy and safety of topical retinoids for preventing and reversing the effects of photoageing: a literature review.
indication, and it is effective when used appropriately. However, the irritant reaction it can cause
may not be tolerated in those with sensitive skin or other concurrent skin disease. It is not often you
come across a patient who simply needs an agent that will address one problem; the skin and the
patient is unique, and so treatment must be tailored to that. Younger patients with skin types I and
II, who have mild early signs of photoageing may also suffer with acne. In contrast, a more mature
patient with pigmentation and melasma, may have more significant photodamage. Treatment choice
in terms of type of retinoid, formulation, delivery system and method of application (i.e. patient
compliance, frequency of use, baseline skin sensitivity and type) will all contribute to treatment
success. The variety of preparations and formulations mean that a tailored treatment regime can be
determined for almost all patients.
The evidence presented in this review supports a recommendation for the use of tazarotene in those
for whom a more rapid response may be required, and whose skin can tolerate the potential for
irritation. In addition, the use of adapalene in those patient wishing to treat both acne and
photoageing can be recommended. In those patients with sensitive skin, a retinol combination
product, with a focus on skin barrier repair and hydration, may be the most appropriate choice, and
the evidence suggests that a similar improvement in comparison to that seen with tretinoin can be
gained with these products.
Ultimately, the evidence supports the use of tretinoin, tazarotene, adapalene, retinaldehyde and
retinol in combination with complimentary agents such as AHAs, hydroxyquinone and anti-
oxidants for the management of photoageing. However patient assessment and education on the
appropriate way to use topical retinoids is key to ensuring the most successful outcome.
Conclusion Topical retinoids are an efficacious and well tolerated medical treatment for the clinical and
histological signs of cutaneous photoageing. The variety of preparations mean that treatment can be
tailored to specific patient characteristics and requirements, and almost all patients can benefit from
the addition of a topical retinoid to their skin care regime.
Dr. Sarah Tranter MBBS BSc Professional Project MSc Dermatology in Clinical Practice 26

The efficacy and safety of topical retinoids for preventing and reversing the effects of photoageing: a literature review.
Word count: 10095
Dr. Sarah Tranter MBBS BSc Professional Project MSc Dermatology in Clinical Practice 27

Table 3. The topical retinoids and their applications in preventing and reversing photoageing - a summary of their key characteristics, actions and evidence
Observations with treatment
RetinoidRAR affinity Prep
Histological and ultrastructural changes Clinical
Adverse effects Ref.
1. Tretinoin All-trans-retinoic acid
Natural1st generation
Directly activates all RARs, indirectly RXR
0.1%
0.05%
0.02%0.025%
Compaction of stratum corneum, increased GAGsStimulates epidermal proliferation
Compaction of stratum corneum, disappearance of atypia and dysplasia
Similar to effects seen with 0.05 and 0.1% however to lesser degree
Additional effects:Accelerates elimination of sebum and reduces inflammation of sebaceous glands, inhibits keratosis
Improvement in fine and coarse wrinkles, tactile roughness and sallownessHyperpigmentation/mottled hyperpigmentation (>6 months)
Improvement in fine wrinkles (after 3 months)
Similar to effects seen with 0.05 and 0.1% however to lesser degree
Improvement in inflammatory conditions, acne, psoriasis, keratosis pilaris
Mild-moderate irritant reaction, characterised by erythema, skin peeling, irritation.
Self limiting with continued use.
Dose dependent and improves on cessation of product.
[64], [65], [66], [68], [69], [70], [71], [75], [76]
2. Retinol All-trans-retinolRetinoic acid precursor
Natural1st generation
Directly activates all RARs, indirectly RXR
0.1%
0.5%
0.25%
Inhibits collagenase and MMP expression; stimulates collagen type 1 and GAGs synthesis
Less efficacious in improving fine lines and wrinkle, pigmentation. Approx 20-fold less effective than tretinoin.
Well tolerated
[42], [85], [86]
3. Retinol derivatives
Esters/ Combination products
Natural1st generation
RARs Varied Stimulates epidermal proliferationRegulates sebum
Improvement in fine lines and wrinkles
Well tolerated
[44], [87], [88], [91], [92]
4. Retinaldehyde
Retinoic acid and retinol precursor
Natural1st generation
Directly activates all RARs, indirectly RXR
0.05% Stimulates epidermal proliferationReduced TEWL
Reduction in skin roughness and wrinkles (after 44 weeks).Improved skin hydration
Well tolerated
[93], [94], [95]
5. Isotretinoin
13-cis-retinoic acid
Natural1st generation
Low affinity for RAR and RXR. May be converted intracellularly to active metabolites.
0.1% cream
Not reported Improvement in fine wrinkles, roughness, discrete pigmentation and sallowness over 36 weeks
Well tolerated
[97]
6. Alitretinoin
9-cis-retinoic acid
Natural1st generation
RXRs 0.1% Not reported Improvement in actinic and seborrhoeic keratoses
Well tolerated
[98]
Retinoid

The efficacy and safety of topical retinoids for preventing and reversing the effects of photoageing: a literature review.
7. Tazarotene
Precursor of tazarotenic acid
Synthetic3rd generation
RAR β/γ 0.1%
0.05%
0.025%
Regulates keratinocyte proliferation, differentiation and inflammationIncreases epidermal thickness, improved epidermal polarity
Improvement in wrinkles, pigmentation*, pore size, elastosis, tactile roughness
*possibly more efficacious than retinoic acid for this indication
Increasing irritant reaction with increasing concentration
[99], [100], [101], [102], [103], [104], [105], [106]
8. Adapalene
Napthoic acid base
Synthetic3rd generation
RAR β/γ 0.3% and 0.1% gel
Improved cellular atypia
Reduced epidermal melanin content
Potent modulator of follicular keratinisation, increases keratinocyte proliferation, keratolytic
Lightening of solar lentigines
Improvement in wrinkles, pigmentation
Improvement in acne, inflammation, excessive keratosis
Well tolerated
[108], [109], [110], [111]
9. Novel retinoids
9a. Seletinoid G
9b. N-retinoyl-D-glucosamine
Varied
Pyranone based
Synthetic4th generation
Retinoic acid agonist
Synthetic4th generation
RAR
RAR 0.05%
Induces procollagen I, tropoelastin and fibrillin-1Reduces expression of MMP-1Promotes proliferation /migration of keratinocytes (in vitro)Increases dermal collagen in human skin equivalents
Promotes wide repair zone and expression of collagen IInduces RAR transcription 100 times the potency of RA
Improved wound healing and closure
Improvement of wrinkles (in in UVB irradiated animal model)
Does not induce erythema
Does not induce erythema, roughness. Reduced TEWL
[115], [116]
[117]
Observations with treatment
RetinoidRAR affinity Prep
Histological and ultrastructural changes Clinical
Adverse effects Ref.Retinoid
Dr. Sarah Tranter MBBS BSc Professional Project MSc Dermatology in Clinical Practice 29

References:
[1] Samuel M, Brooke RC, Hollis S, Griffiths CEM. Interventions for photodamaged skin. Cochrane Database Syst Rev 2005: 25: CD001782. [2] Gilchrest BA. Photoaging. J Invest Dermatol. 2013 Jul 1;133(E1):E2-6. doi: 10.1038/skinbio.2013.176. PMID: 23820721.[3] Ferreira, R., Napoli, J., Enver, T. et al. Advances and challenges in retinoid delivery systems in regenerative and therapeutic medicine. Nat Commun 11, 4265 (2020). https://doi.org/10.1038/s41467-020-18042-2 [4] Rittié L, Fisher GJ. UV-light-induced signal cascades and skin aging. Ageing Res Rev. 2002 Sep;1(4):705-20. doi: 10.1016/s1568-1637(02)00024-7. PMID: 12208239.[5] Yaar M, Lee MS, Rünger TM, Eller MS, Gilchrest B. Telomere mimetic oligonucleotides protect skin cells from oxidative damage. Annales de Dermatologie et de Vénéréologie. 2002;129:1–18.[6] Kosmadaki MG, Gilchrest BA. The role of telomeres in skin aging/photoaging. Micron 2004; 35:155–159[7] McCallion, R. and Li Wan Po, A. Dry and photo-aged skin: manifestations and management. J. Clin. Pharm. Ther. 18, 15–32 (1993)[8] Durai PC, Thappa DM, Kumari R, Malathi M. Aging in elderly: chronological versus photoaging. Indian J Dermatol. 2012;57(5):343-352. doi:10.4103/0019-5154.100473[9] Suhonen R. (2012) Solar elastosis. [image]. Available at: https://dermnetnz.org/topics/solar-elastosis/ (Accessed: 30th June 2021). https://creativecommons.org/licenses/by-nc-nd/3.0/nz/legalcode[10] Fenske NA, Lober CW. Structural and functional changes of normal aging skin. J Am Acad Dermatol. 1986 Oct;15(4 Pt 1):571-85. doi: 10.1016/s0190-9622(86)70208-9. PMID: 3534008.[11] Farage, M.A., Miller, K.W., Elsner, P. and Maibach, H.I. (2008), Intrinsic and extrinsic factors in skin ageing: a review. International Journal of Cosmetic Science, 30: 87-95. https://doi.org/10.1111/j.1468-2494.2007.00415.x[12] Mukherjee S, Date A, Patravale V, Korting HC, Roeder A, Weindl G. Retinoids in the treatment of skin aging: an overview of clinical efficacy and safety. Clin Interv Aging. 2006;1(4):327-348. doi:10.2147/ciia.2006.1.4.327[13] Griffiths CE. The role of retinoids in the prevention and repair of aged and photoaged skin. Clin Exp Dermatol. 2001 Oct;26(7):613-8. [14] Varani J, Warner RL, Gharaee-Kermani M, Phan SH, Kang S, Chung JH, Wang ZQ, Datta SC, Fisher GJ, Voorhees JJ. Vitamin A antagonizes decreased cell growth and elevated collagen-degrading matrix metalloproteinases and stimulates collagen accumulation in naturally aged human skin. J Invest Dermatol. 2000 Mar;114(3):480-6. doi: 10.1046/j.1523-1747.2000.00902.x. PMID: 10692106.[15] Gilchrest, B.A. A review of skin aging and its medical therapy. Br. J. Dermatol. 135, 867– 875 (1996).[16] Gilchrest BA. Photoaging. PHOTOBIOLOGY/PHOTOMEDICINE| VOLUME 133, SUPPLEMENT 2, E2-E6, JULY 01, 2013[17] El-Domyati M, Attia S, Saleh F, et al. Intrinsic aging vs. photoaging: a comparative histopathological, immunohistochemical, and ultrastructural study of skin. Exp Dermatol. 2002;11(5):398-405. doi:10.1034/j.1600-0625.2002.110502.x[18] Fisher GJ, Voorhees JJ. Molecular mechanisms of photoaging and its prevention by retinoic acid: ultraviolet irradiation induces MAP kinase signal transduction cascades that induce Ap-1-regulated matrix metalloproteinases that degrade human skin in vivo. J Investig Dermatol Symp Proc. 1998 Aug;3(1):61-8. PMID: 9732061.[19] Fisher, G., Datta, S., Talwar, H. et al. Molecular basis of sun-induced premature skin ageing and retinoid antagonism. Nature 379, 335–339 (1996). https://doi.org/10.1038/379335a0[20] Pandel R, Poljšak B, Godic A, Dahmane R. Skin photoaging and the role of antioxidants in its prevention. ISRN Dermatol. 2013;2013:930164. Published 2013 Sep 12. doi:10.1155/2013/930164[21] Leow, Y.H. and Maibach, H.I. Cigarette smoking, cutaneous vasculature, and tissue oxygen. Clin. Dermatol. 16, 579–584 (1998).[22] Brem R, Macpherson P, Guven M, Karran P. Oxidative stress induced by UVA photoactivation of the tryptophan UVB photoproduct
6-formylindolo[3,2-b]carbazole (FICZ) inhibits nucleotide excision repair in human cells. Sci Rep. 2017 Jun 27;7(1):4310. doi: 10.1038/s41598-017-04614-8. PMID: 28655934; PMCID: PMC5487344.[23] Helfrich, Yolanda & Sachs, Dana & Voorhees, John. (2008). Overview of skin aging and photoaging. Dermatology nursing / Dermatology Nurses' Association. 20. 177-83; quiz 184.[24] Reelfs O, Tyrrell RM, Pourzand C. Ultraviolet A radiation induced immediate iron release is a key modulator of the activation of NF-kB in human skin fibroblasts. J Invest Dermatol. 2004; 122:1440-7[25] Fisher GJ, Wang ZQ, Datt SC, et al. Pathophysiology of premature skin aging induced by ultraviolet light. N Engl J Med 1997: 337: 1419–1428.[26] Fisher GJ, Voorhees JJ. Molecular mechanisms of photoaging and its prevention by retinoic acid: ultraviolet irradiation induces MAP kinase signal transduction cascades that induce Ap-1-regulated matrix metalloproteinases that degrade human skin in vivo. J Investig Dermatol Symp Proc. 1998 Aug;3(1):61-8. PMID: 9732061.[27] Nishimori, Y., Edwards, C., Pearse, A., Matsumoto, K., Kawai, M., Marks, R., 2001. Degenerative alternations of dermal collagen fiber bundles in photodamaged human skin and UV-irradiated hairless mouse skin: possible effect on decreasing skin mechanical properties and appearance of wrinkles. J. Invest. Dermatol. 117, 1458– 1463.[28] Fisher GJ, Datta S, Wang Z, Li XY, Quan T, Chung JH, Kang S, Voorhees JJ. c-Jun-dependent inhibition of cutaneous procollagen transcription following ultraviolet irradiation is reversed by all-trans retinoic acid. J Clin Invest. 2000 Sep;106(5):663-70. doi: 10.1172/JCI9362. PMID: 10974019; PMCID: PMC381286. [29] Massagué, J., 1998. TGF-︎ signal transduction. Annu. Rev. Biochem. 67, 753–791.[30] Massagué, J., 2000. How cells read TGF- ︎ signals. Nat. Rev. 1, 169–178.[31] Quan, T., He, T.Y., Voorhees, J.J., Fisher, G.J., 2001. Ultraviolet irradiation blocks cellular responses to transforming growth factor- ︎ by down regulating its type-II receptor and inducing Smad7. J. Biol. Chem. 276, 26349–26356. [32] Imokawa G. Recent advances in characterizing biological mechanisms underlying UV-induced wrinkles: a pivotal role of fibrobrast-derived elastase. Arch Dermatol Res. 2008; 300 Suppl 1:S7-20[33] Lee DH, Oh JH, Chung JH. Glycosaminoglycan and proteoglycan in skin aging. J Dermatol Sci. 2016 Sep;83(3):174-81. doi: 10.1016/j.jdermsci.2016.05.016. Epub 2016 May 27. PMID: 27378089.[34] Dai G, Freudenberger T, Zipper P, et al. Chronic ultraviolet B irradiation causes loss of hyaluronic acid from mouse dermis because of down-regulation of hyaluronic acid synthases. Am J Pathol. 2007; 171:1451-61[35] Griffiths CEM, Russman A, Majmudar G, et al. Restoration of collagen formation in photodamaged human skin by tretinoin (retinoic acid). N Eng J Med 1993: 329: 530 – 535.[36] Zasada M, Budzisz E. Retinoids: active molecules influencing skin structure formation in cosmetic and dermatological treatments. Postepy Dermatol Alergol. 2019;36(4):392-397. doi:10.5114/ada.2019.87443[37] Gilchrest BA. Treatment of photodamage with topical tretinoin: an overview. Journal of the American Academy of Dermatology. 1997;36(3, part 2):S27–S36[38] Kircik LH. Histologic improvement in photodamage after 12 months of treatment with tretinoin emollient cream (0.02%). J Drugs Dermatol. 2012 Sep;11(9):1036-40. PMID: 23135644.[39] Peter P Fu, Qingsu Xia, Mary D Boudreau, Paul C Howard, William H Tolleson, Wayne G Wamer Physiological role of retinyl palmitate in the skin. Vitam Horm. 2007;75:223-56. doi: 10.1016/S0083-6729(06)75009-9[40] Thacher SM, Vasudevan J, Chandraratna RA. Therapeutic applications for ligands of retinoid receptors. Curr Pharm Des. 2000 Jan;6(1):25-58. doi: 10.2174/1381612003401415. PMID: 10637371.[41] Kim MS, Lee S, Rho HS, Kim DH, Chang IS, Chung JH. The effects of a novel synthetic retinoid, seletinoid G, on the expression of extracellular matrix proteins in aged human skin in vivo. Clin Chim Acta. 2005 Dec;362(1-2):161-9. doi: 10.1016/j.cccn.2005.06.016. Epub 2005 Aug 1. PMID: 16055107.

The efficacy and safety of topical retinoids for preventing and reversing the effects of photoageing: a literature review.
[42] Serri R, Iorizzo M. Cosmeceuticals: focus on topical retinoids in photoaging. Clin Dermatol. 2008 Nov-Dec;26(6):633-5. doi: 10.1016/j.clindermatol.2007.09.016. PMID: 18940544.[43] Kligman LH, Akin FJ, Kligman AM. Prevention of ultraviolet damage to the dermis of hairless mice by sunscreens. J Invest Dermatol. 1982 Feb;78(2):181-9. doi: 10.1111/1523-1747.ep12506359. PMID: 6173447.[44] McDaniel, D Mazur, C, Wortzman, M, Nelson, D. Efficacy and tolerability of a double-conjugated retinoid cream vs 1.0% retinol cream or 0.025% tretinoin cream in subjects with mild to severe photoaging. J Cosmet Dermatol 2017 Dec;16(4):542-548.[45] Tran C, Kasraee B, Grand D, et al. Pharmacology or RALGA, a mixture of retinaldehyde and glycolic acid. Dermatology. 2005;210(Suppl 1):6-13.[46] Ditre CM., Whitney K. 2013. Actinic (solar) elastosis (Other chronic dermatitis due to solar radiation). Dermatology Advisor. https://www.dermatologyadvisor.com/home/decision-support-in-medicine/dermatology/actinic-solar-elastosis-other-chronic-dermatitis-due-to-solar-radiation/[47] Schaefer, H., 1993. Penetration and percutaneous absorption of topical retinoids. Skin Pharmacology and Physiology, 6(Suppl. 1), pp.17-23.[48] Nau, H., 1993. Embryotoxicity and teratogenicity of topical retinoic acid. Skin Pharmacology and Physiology, 6(Suppl. 1), pp.35-44.[49] Veraldi S, Rossi LC, Barbareschi M. Are topical retinoids teratogenic? G Ital Dermatol Venereol. 2016 Dec;151(6):700-705. Epub 2016 Sep 6. PMID: 27598619.[50] O'Byrne SM, Blaner WS. Retinol and retinyl esters: biochemistry and physiology. J Lipid Res. 2013;54(7):1731-1743. doi:10.1194/jlr.R037648[51] Riahi, R, Bush AE, Cohen PR. Topical Retinoids: Therapeutic Mechanisms in the Treatment of Photodamaged Skin. Am J Clin Dermatol. 2016 Jun;17(3):265-76. doi: 10.1007/s40257-016-0185-5.[52] Fitzpatrick, TB., & Freedberg, IM. (2003). ‘Topical Retinoids’, in Fitzpatrick's Dermatology in General Medicine. New York, McGraw-Hill, Medical Pub, pp. 2589-2595[53] C E Griffiths, J T Elder, B A Bernard, P Rossio, M A Cromie, L J Finkel, B Shroot, J J Voorhees. Comparison of CD271 (adapalene) and all-trans retinoic acid in human skin: dissociation of epidermal effects and CRABP-II mRNA expression. J Invest Dermatol.1993 Sep;101(3):325-8.[54] Petkovich M et al: A human retinoic acid receptor which belongs to the family of nuclear receptors. Nature 330:444, 1987 [55] Giguére V et al: Identification of a receptor for the morphogen retinoic acid. Nature 330:624, 1987[56] Elder JT et al: Differential regulation of retinoic acid receptors and binding proteins in human skin. J Invest Dermatol 98:673, 1992[57] Elder JT, Åström A, Pettersson U, Tavakkol A, Krust A, Kastner P, Chambon P, Vorhees JJ. Retinoic Acid Receptors and Binding Proteins in Human Skin. J Invest Dermatol. 1992; 98:6; S36-S41. ISSN 0022-202X. https://doi.org/10.1111/1523-1747.ep12462180.[58] Fisher GJ et al: Immunological identification and functional quantitation of retinoic acid and retinoid X receptor proteins in human skin. J Biol Chem 269:20629, 1994[59] Wang, Z et al: Ultraviolent irradiation of human skin causes functional vitamin A deficiency, preventable by all- trans retinoic-acid pretreatment. Nat Med 5:418, 1999[60] Leyden J . Adapalene in clinical practice. Cutis. 2001 Oct; 68(4 Suppl):7-9.[61] Wolff, K, Goldsmith, L, Katz, S, Gilchrest, B, Paller, AS & Leffell, D 2011, Fitzpatrick's Dermatology in General Medicine, 8th Edition. McGraw-Hill, New York.[62] Kligman LH, Kligman AM. The nature of photoaging: its prevention and repair. Photodermatol. 1986 Aug; 3(4):215-27.[63] Kligman LH, Duo CH, Kligman AM. Topical retinoic acid enhances the repair of ultraviolet damaged dermal connective tissue. Connect Tissue Res. 1984;12(2):139-50. doi: 10.3109/03008208408992779. PMID: 6723309.[64] Weiss JS, Ellis CN, Headington JT, Tincoff T, Hamilton TA, Voorhees JJ: Topical tretinoin improves photoaged skin: A double-blind vehicle-controlled study. JAMA 1988;259:527– 532.
[65] G D Weinstein 1, T P Nigra, P E Pochi, R C Savin, A Allan, K Benik, E Jeffes, L Lufrano, E G Thorne. Topical tretinoin for treatment of photodamaged skin. A multicenter study. Arch Dermatol. 1991 May;127(5):659-65.[66] E A Olsen 1, H I Katz, N Levine, J Shupack, M M Billys, S Prawer, J Gold, M Stiller, L Lufrano, E G Thorne.Tretinoin emollient cream: a new therapy for photodamaged skin. J Am Acad Dermatol 1992 Feb;26(2 Pt 1):215-24.[67] Griffiths CEM, Kang S, Ellis CN et al. Two concentrations of topical tretinoin (retinoic acid) cause similar improvement of photoaging but different degrees of irritation. Arch Dermatol 1995; 131: 1037– 44.[68] Kang S, Bergfield W, Gottlieb A et al. Long-term efficacy and safety of tretinoin emollient cream 0.05% in the treatment of photodamaged facial skin: a two-year, randomized, placebo-controlled trial. Am J Clin Dermatol. 2005;6(4):245-53.[69] Bhawan J, Olsen E, Lufrano L, Thorne EG, Schwab B, Gilchrest BA. Histologic evaluation of the long term effects of tretinoin on photodamaged skin. J Dermatol Sci. 1996 Mar;11(3):177-82. doi: 10.1016/0923-1811(95)00432-7. PMID: 8785167.[70] Bhawan J. Short- and long-term histologic effects of topical tretinoin on photodamaged skin. Int J Dermatol. 1998 Apr;37(4):286-92. doi: 10.1046/j.1365-4362.1998.00433.x. PMID: 9585903.[71] AM Kligman & GF Graham (1993) Histological changes in facial skin after daily application of tretinoin for 5 to 6 years, Journal of Dermatological Treatment, 4:3, 113-117, DOI: 10.3109/09546639309080547[72] Voorhees JJ. Clinical effects of long-term therapy with topical tretinoin and cellular mode of action. J Int Med Res.1990;18 Suppl 3:26C-28C.[73] Rafal ES, Griffiths CEM, Ditre CM, et al. Topical tretinoin (retinoic acid) treatment for liver spots associated with photodamage. N Engl J Med 1992: 326: 368–374.[74] Ellis CN, Weiss JS, Hamilton TA, Headington JT, Zelikson AS, Voorhees JJ. Sustained improvement with prolonged topical tretinoin (retinoic acid) for photoaged skin. Journal of the American Academy of Dermatology, Volume 23, Issue 4, Part 1, 1990, Pages 629-637, ISSN 0190-9622, https://doi.org/10.1016/0190-9622(90)70265-J.[75] Griffiths CEM, Voorhees JJ. Topical Retinoic Acid for Photoaging: Clinical Response and Underlying Mechanisms. Skin Pharmacol 1993;6:70–77[76] Kligman LH. Prevention and repair of photoaging: sunscreens and retinoids. Cutis. 1989 May;43(5):458-65. PMID: 2656109.[77] Sorg O, Kuenzli, Kaya G, Saurat J. Proposed mechanisms of action for retinoid derivatives in the treatment of skin aging. J Cosmet Dermatol. 2005 Dec;4(4):237-44. doi: 10.1111/j.1473-2165.2005.00198.x.[78] Kligman AM. Guidelines for the use of topical tretinoin (Retin-A) for photoaged skin. J Am Acad Dermatol 1989;21:650-4. [79] Olsen EA, Katz HI, Levine N, Nigra TP, Pochi PE, Savin RC, Shupack J, Weinstein GD, Lufrano L, Jou HC. Sustained improvement in photodamaged skin with reduced tretinoin emollient cream treatment regimen: effect of once-weekly and three-times-weekly applications. J Am Acad Dermatol. 1997 Aug;37(2 Pt 1):227-30. doi: 10.1016/s0190-9622(97)80129-6. PMID: 9270508.[80] Michael Babcock, Rahul C. Mehta, Elizabeth T. Makino. A Randomized, Double-blind, Split-face Study Comparing the Efficacy and Tolerability of Three Retinol-based Products vs. Three Tretinoin-based Products in Subjects With Moderate to Severe Facial Photodamage. J Drugs Dermatol. 2015;14(1):24-30.[81] Draelos ZD, Peterson RS. A Double-Blind, Comparative Clinical Study of Newly Formulated Retinol Serums vs Tretinoin Cream in Escalating Doses: A Method for Rapid Retinization With Minimized Irritation. J Drugs Dermatol. 2020;19(6): doi:10.36849/JDD.2020.5085.[82] Bouloc A, Vergnanini AL, Issa MC. A double-blind randomized study comparing the association of Retinol and LR2412 with tretinoin 0.025% in photoaged skin. J Cosmet Dermatol. 2015 Mar;14(1):40-6.[83] Alexiades M. Jasmonates and Tetrahydrojasmonic Acid: A Novel Class of Anti-Aging Molecules. J Drugs Dermatol. 2016 Feb;15(2):206-7. PMID: 26885789.
Dr. Sarah Tranter MBBS BSc Professional Project MSc Dermatology in Clinical Practice 31

The efficacy and safety of topical retinoids for preventing and reversing the effects of photoageing: a literature review.
[84] Fu JJ, Hillebrand GG, Raleigh P, et al. A randomized, controlled comparative study of the wrinkle reduction benefits of a cosmetic niacinamide/peptide/retinyl propionate product regimen vs. a prescription 0.02% tretinoin product regimen. Br J Dermatol. 2010;162(3):647-654. doi:10.1111/j.1365-2133.2009.09436.x[85] Kang S, Duell EA, Fisher GJ, et al. Application of retinol to human skin in vivo induces epidermal hyperplasia and cellular retinoid binding proteins characteristic of retinoic acid but without measurable retinoic acid levels or irritation. J Invest Dermatol. 1995;105(4):549-556. doi:10.1111/1523-1747.ep12323445[86] Kligman AM. Cosmetics: a dermatologist looks to the future: promises and problems. Derm Clin 2000; 18: 699–709. [87] Han HS, YJ, Park MS, et al. Efficacy validation of synthesized retinol derivatives in vitro: stability, toxicity, and activity. Bioorg Med Chem. 2003;11:3839–45.[88] Green C, Orchard G, Cerio R, Hawk JL. A clinicopathological study of the effects of topical retinyl propionate cream in skin photoageing. Clin Exp Dermatol. 1998 Jul;23(4):162-7. doi: 10.1046/j.1365-2230.1998.00331.x. PMID: 9894360.[89] Dhaliwal S, Rybak I, Ellis SR, Notay M, Trivedi M, Burney W, Vaughn AR, Nguyen M, Reiter P, Bosanac S, Yan H, Foolad N, Sivamani RK. Prospective, randomized, double-blind assessment of topical bakuchiol and retinol for facial photoageing. Br J Dermatol. 2019 Feb;180(2):289-296. doi: 10.1111/bjd.16918. Epub 2018 Sep 21. PMID: 29947134.[90] Feinberg C, Hawkins S, Battaglia A, et al. Comparison of anti-aging efficacy from cosmetic ingredients on photoaged skin. J Am Acad Dermatol. 2004;50(3:S1):P27.[91] Draelos ZD. Novel approach to the treatment of hyperpigmented photodamaged skin: 4% hydroquinone/0.3% retinol versus tretinoin 0.05% emollient cream. Dermatol Surg. 2005 Jul; 31(7 Pt 2):799-804.[92] Seité S, Bredoux C, Compan D, Zucchi H, Lombard D, Medaisko C, Fourtanier A. Histological evaluation of a topically applied retinol-vitamin C combination. Skin Pharmacol Physiol. 2005 Mar-Apr; 18(2):81-7.[93] Saurat JH, Didierjean L, Masgrau E, Piletta PA, Jaconi S, Chatellard-Gruaz D, Gumowski D, Masouyé I, Salomon D, Siegenthaler G. Topical retinaldehyde on human skin: biologic effects and tolerance. J Invest Dermatol. 1994 Dec;103(6):770-4. doi: 10.1111/1523-1747.ep12412861.[94] Creidi P, Vienne MP, Ochonisky S, Lauze C, et al. Profilometric evaluation of photodamage after topical retinaldehyde and retinoic acid treatment. J Am Acad Dermatol. 1998;39:960-965.[95] Creidi P, Humbert P. Clinical use of topical retinaldehyde on photoaged skin. Dermatology. 1999;199 Suppl 1:49-52. doi: 10.1159/000051379. PMID: 10473961.[96] Kwon HS, Lee JH, Kim GM, Bae JM. Efficacy and safety of retinaldehyde 0.1% and 0.05% creams used to treat photoaged skin: A randomized double-blind controlled trial. J Cosmet Dermatol. 2018 Jun;17(3):471-476. doi: 10.1111/jocd.12551. Epub 2018 Apr 16. PMID: 29663701.[97] Sendagorta E, Lesiewicz J, Armstrong RB. Topical isotretinoin for photodamaged skin. J Am Acad Dermatol.1992 Dec;27(6 Pt 2):S15-8.[98] Baumann L, Vujevich J, Halem M, Martin LK, Kerdel F, Lazarus M, Pacheco H, Black L, Bryde J. Open-label pilot study of alitretinoin gel 0.1% in the treatment of photoaging. Cutis 2005 Jul;76(1):69-73.[99] Guenther LC. Topical tazarotene therapy for psoriasis, acne vulgaris, and photoaging. Skin Therapy Lett. 2002 Mar;7(3):1-4.[100] Guenther, LC. Optimizing treatment with topical tazarotene. Am J Clin Dermatol. 2003;4(3):197-202.[101] Kang S, Leyden JJ, Lowe NJ et al. Tazarotene Cream for the Treatment of Facial PhotodamageA Multicenter, Investigator-Masked, Randomized, Vehicle-Controlled, Parallel Comparison of 0.01%, 0.025%, 0.05%, and 0.1% Tazarotene Creams With 0.05% Tretinoin Emollient Cream Applied Once Daily for 24 Weeks. Arch Dermatol. 2001;137(12):1597-1604. doi:10.1001/archderm.137.12.1597[102] Kang S, Krueger GG, Tanghetti EA, Lew-Kaya D, Sefton J, Walker PS, Gibson JR, Tazarotene Cream in Photodamage Study Group. A multicenter, randomized, double-blind trial of tazarotene 0.1% cream in the treatment of photodamage. J Am Acad Dermatol. 2005 Feb;52(2):268-74. doi: 10.1016/j.jaad.2004.06.021.
[103] Lowe N, Gifford M, Tanghetti E, Poulin Y, Goldman M, Tse Y, Yamauchi P, Rosenweig H, Kang S. Tazarotene 0.1% cream versus tretinoin 0.05% emollient cream in the treatment of photodamaged facial skin: a multicenter, double-blind, randomized, parallel-group study. J Cosmet Laser Ther. 2004 Jun;6(2):79-85.[104] Machtinger LA, Kaidbey K, Lim J, Loven KH, Rist TE, Wilson DC, Parizadeh DD, Sefton J, Holland JM, Walker PS. Histological effects of tazarotene 0.1% cream vs. vehicle on photodamaged skin: a 6-month, multicentre, double-blind, randomized, vehicle-controlled study in patients with photodamaged facial skin. Br J Dermatol. 2004 Dec;151(6):1245-52.[105] Tanghetti E, Dhawan S, Green L, Del Rosso J, Draelos Z, Leyden J, Shalita A, Glaser DA, Grimes P, Webster G, Barnett P, Le Gall N. Randomized comparison of the safety and efficacy of tazarotene 0.1% cream and adapalene 0.3% gel in the treatment of patients with at least moderate facial acne vulgaris. J Drugs Dermatol. 2010 May;9(5):549-58.[106] Phillips TJ. Tazarotene 0.1% cream for the treatment of photodamage. Skin Therapy Lett. 2004 Apr;9(4):1-2.[107] Leyden J. Adapalene in clinical practice. Cutis. 2001 Oct;68(4 Suppl):7-9. PMID: 11845950.[108] Bernard BA. Adapalene, a new chemical entity with retinoid activity. Skin Pharmacol. 1993;6 Suppl 1:61-9. doi: 10.1159/000211165.[109] Kang S, Goldfarb MT, Weiss JS, et al. Assessment of adapalene gel for the treatment of actinic keratoses and lentigines: a randomized trial. J Am Acad Dermatol 2003;49:83-90. [110] Griffiths CE, Elder JT, Bernard BA, Rossio P, Cromie MA, Finkel LJ, Shroot B, Voorhees JJ. Comparison of CD271 (adapalene) and all-trans retinoic acid in human skin: dissociation of epidermal effects and CRABP-II mRNA expression. J Invest Dermatol.1993 Sep;101(3):325-8[111] Bagatin E et al., Comparable efficacy of adapalene 0.3% gel and tretinoin 0.05% cream as treatment for cutaneous photoaging. Eur J Dermatol. 2018 Jun 1;28(3):343-350.[112] Queille-Roussel C, Poncet M, Mesaros S, Clucas A, Baker M, Soloff AM. Comparison of the cumulative irritation potential of adapalene gel and cream with that of erythromycin/tretinoin solution and gel and erythromycin/isotretinoin gelClin Ther. 2001 Feb;23(2):205-12. doi: 10.1016/s0149-2918(01)80003-5.[113] WJ Cunliffe, M Poncet, C Loesche & M Verschoore, A comparison of the efficacy and tolerability of adapalene 0.1% gel versus tretinoin 0.025% gel in patients with acne vulgaris: a meta-analysis of five randomized trials, Br J Dermatol 1998, 139 Suppl 52, 48-56.[114] Thacher SM, Vasudevan J, Chandraratna RA. Therapeutic applications for ligands of retinoid receptors. Curr Pharm Des. 2000 Jan;6(1):25-58. doi: 10.2174/1381612003401415. PMID: 10637371.[115] Kim MS, Lee S, Rho HS, Kim DH, Chang IS, Chung JH. The effects of a novel synthetic retinoid, seletinoid G, on the expression of extracellular matrix proteins in aged human skin in vivo. Clin Chim Acta. 2005 Dec;362(1-2):161-9. doi: 10.1016/j.cccn.2005.06.016. Epub 2005 Aug 1. PMID: 16055107.[116] Lee ES, Ahn Y, Bae IH, Min D, Park NH, Jung W, Kim SH, Hong YD, Park WS, Lee CS. Synthetic Retinoid Seletinoid G Improves Skin Barrier Function through Wound Healing and Collagen Realignment in Human Skin Equivalents. Int J Mol Sci. 2020 Apr 30;21(9):3198. doi: 10.3390/ijms21093198. PMID: 32366052; PMCID: PMC7247558.[117] Kambayashi H, Odake Y, Takada K, Funasaka Y, Ichihashi M, Kato S. N-retinoyl-D-glucosamine, a new retinoic acid agonist, mediates topical retinoid efficacy with no irritation on photoaged skinBr J Dermatol. 2005 Dec;153 Suppl 2:30-6. doi: 10.1111/j.1365-2133.2005.06967.x.[118] Kircik LH. Evaluating tretinoin formulations in the treatment of acne. J Drugs Dermatol. 2014 Apr;13(4):466-70. PMID: 24719067.[119] Skov MJ, Quigley JW, Bucks DA. Topical delivery system for tretinoin: research and clinical implications. J Pharm Sci. 1997 Oct;86(10):1138-43. doi: 10.1021/js9604568. PMID: 9344171.[120] Ourique, A. F. et al. Improved photostability and reduced skin permeation of tretinoin: development of a semisolid nanomedicine. Eur. J. Pharm. Biopharm. 79, 95–101 (2011).
Dr. Sarah Tranter MBBS BSc Professional Project MSc Dermatology in Clinical Practice 32

The efficacy and safety of topical retinoids for preventing and reversing the effects of photoageing: a literature review.
[121] Puglia C, Bonina F. Lipid nanoparticles as novel delivery systems for cosmetics and dermal pharmaceuticals. Expert Opin Drug Deliv. 2012 Apr;9(4):429-41. doi: 10.1517/17425247.2012.666967. Epub 2012 Mar 6. PMID: 22394125.[122] Raminelli ACP, Romero V, Semreen MH, Leonardi GR. Nanotechnological Advances for Cutaneous Release of Tretinoin: An Approach to Minimize Side Effects and Improve Therapeutic Efficacy. Curr Med Chem. 2018;25(31):3703-3718. doi: 10.2174/0929867325666180313110917. PMID: 29532749.[123] Rahimpour Y, Hamishehkar H. Liposomes in cosmeceutics. Expert Opin Drug Deliv. 2012 Apr;9(4):443-55. doi: 10.1517/17425247.2012.666968. Epub 2012 Mar 13. PMID: 22413847.[124] Rahman, S. A. et al. Tretinoin-loaded liposomal formulations: from lab to comparative clinical study in acne patients. Drug Deliv. 23, 1184–1193 (2016).[125] Miura T, Takada A, Ooe M. Tretinoin cyclodextrin complex (RA/CyD) causes less irritation with an equal antiwrinkle effect compared with conventional tretinoin: clinical and histologic studies of photoaged skinAesthetic Plast Surg. 2012 Aug;36(4):971-81. doi: 10.1007/s00266-012-9903-4. Epub 2012 Apr 27.[126] Sardana, K. & Sehgal, V. N. Retinoids: fascinating up-and-coming scenario. J. Dermatol. 30, 355–380 (2003).[127] Fisher GJ, Kang S, Varani J, Bata-Csorgo Z, Wan Y, Datta S, Voorhees JJ. Mechanisms of photoaging and chronological skin aging. Arch Dermatol. 2002 Nov; 138(11):1462-70.[128] Lewis, KG, Bercovitch, L, Dill, SW, Robinson-Bostom, L. “Acquired disorders of elastic tissue: Part I. Increased elastic tissue and solar elastotic syndrome”. J Am Acad Dermatol. vol. 51. 2004. pp. 1-21.[129] Calderone, DC , Fenske, NA. ” The clinical spectrum of actinic elastosis”. J Am Acad Dermatol. vol. 32. 1995. pp. 1016-24.[130] Fisher GJ, Talwar HS, Xiao JH et al. Immunological identification and functional quantification of retinoic acid and retinoid X receptor proteins in human skin. J Biol Chem 1994; 269: 20629–35. [131] Duell EA, Astrom A, Griffiths CEM et al. Human skin levels of retinoic acid and cytochrome p -450 derived hydro yretinoic acid after topical application of retinoic acid receptor-mediated transcription in vitro. J Clin Invest 1992; 90: 1269–74. [132] Chambon PA. A decade of molecular biology of retinoic acid receptors. FASEB J 1996; 10: 940 – 54. [133] Kligman AM, Dogadkinn D, Lavker RM. Effects of tretinoin on non-sun exposed protected skin of the elderly. J Am Acad Dermatol 1993: 29: 25 – 33. [134] Singh M, Griffiths CE. The use of retinoids in the treatment of photoaging. Dermatol Ther. 2006 Sep-Oct;19(5):297-305. doi: 10.1111/j.1529-8019.2006.00087.x. PMID: 17014485.[135] Berneburg M, Plettenberg H, Krutmann J. Photoaging of human skin. Photodermatol Photoimmunol Photomed. 2000; 16:239-44
Dr. Sarah Tranter MBBS BSc Professional Project MSc Dermatology in Clinical Practice 33