The effects of enalapril and losartan on mechanical...
7
The effects of enalapril and losartan on mechanical ventilationeinduced sympathoadrenal activation and oxidative stress in rats Hale Zerrin Toklu, PhD, a,b,c, * Oh-Sung Kwon, PhD, d Yasemin Sakarya, a,b Scott K. Powers, PhD, d Katherine Llinas, a Nataliya Kirichenko, MSc, a,b Kurt J. Sollanek, MSc, d Michael P. Wiggs, PhD, d Ashley J. Smuder, PhD, d Erin E. Talbert, PhD, d Philip J. Scarpace, PhD, b and Nihal Tu ¨ mer, PhD a,b, ** a Malcom Randall Veterans Affairs Medical Center, Geriatric Research Education and Clinical Center, Gainesville, Florida b Department of Pharmacology and Therapeutics, College of Medicine, University of Florida, Gainesville, Florida c Department of Pharmacology, Marmara University School of Pharmacy, Istanbul, Turkey d Department of Applied Physiology and Kinesiology, College of Health & Human Performance, University of Florida, Gainesville, Florida article info Article history: Received 1 November 2013 Received in revised form 7 January 2014 Accepted 30 January 2014 Available online xxx Keywords: Mechanical ventilation Angiotensin Losartan Enalapril NPY Thyrosine hydroxylase Dopamine beta hydroxylase Sympathetic Noradrenergic Norepinephrine abstract Background: Mechanical ventilation (MV) is a method of maintaining appropriate gas ex- change in patients who are unable to sustain adequate alveolar ventilation. While life- saving in the short-term, prolonged MV leads to altered cardiovascular responses and enhanced lung injury, but the exact mechanism is unknown. Therefore, we investigated the involvement of the sympathoadrenergic and renineangiotensin system in MV-induced altered cardiovascular responses. Methods: SpragueeDawley rats were divided into six groups: (1) spontaneous breathing (SB); (2) SB þ enalapril (100 mg/kg intravenous infusion); (3) SB þ losartan (100 mg/kg infusion); (4) 12 h of MV; (5) MV þ enalapril; and (6) MV þ losartan. After the animals were sacrificed, blood and tissue samples were collected. Tyrosine hydroxylase, dopamine beta hydroxy- lase, and neuropeptide Y were measured in adrenal medulla and hypothalamus, whereas AT1 was measured in lung tissues by Western blot. Norepinephrine enzyme-linked immunosorbent assay and total antioxidant capacity were assayed in plasma. Results: Our findings indicated that MV increases the sympathetic activation markers in ad- renal medulla and hypothalamus. Moreover, oxidative stress was increased in lung and brain tissues. Treatment with enalapril or losartan reduced the lipid peroxidation in lung and brain tissues, while preserving the tissue glutathione content and plasma antioxidant capacity. Conclusions: These data demonstrate that the inhibition of the renineangiotensin system by enalapril or losartan may reduce the MV-induced increase in sympathetic activity markers and oxidative stress, and thus, may have a beneficial effect as adjuvant therapy. ª 2014 Elsevier Inc. All rights reserved. * Corresponding author. Department of Pharmacology and Therapeutics, College of Medicine, University of Florida, P.O. Box 100267, Gainesville, FL 32610. ** Corresponding author. Pharmacology & Therapeutics, College of Medicine, University of Florida, P.O. Box 100267, Gainesville, FL 32610. E-mail addresses: [email protected] (H.Z. Toklu), ntumer@ufl.edu (N. Tu ¨ mer). Available online at www.sciencedirect.com ScienceDirect journal homepage: www.JournalofSurgicalResearch.com journal of surgical research xxx (2014) 1 e7 0022-4804/$ e see front matter ª 2014 Elsevier Inc. All rights reserved. http://dx.doi.org/10.1016/j.jss.2014.01.054
Transcript of The effects of enalapril and losartan on mechanical...

ww.sciencedirect.com
j o u rn a l o f s u r g i c a l r e s e a r c h x x x ( 2 0 1 4 ) 1e7
Available online at w
ScienceDirect
journal homepage: www.JournalofSurgicalResearch.com
The effects of enalapril and losartan on mechanicalventilationeinduced sympathoadrenal activationand oxidative stress in rats
Hale Zerrin Toklu, PhD,a,b,c,* Oh-Sung Kwon, PhD,d Yasemin Sakarya,a,b
Scott K. Powers, PhD,d Katherine Llinas,a Nataliya Kirichenko, MSc,a,b
Kurt J. Sollanek, MSc,d Michael P. Wiggs, PhD,d Ashley J. Smuder, PhD,d
Erin E. Talbert, PhD,d Philip J. Scarpace, PhD,b and Nihal Tumer, PhDa,b,**aMalcom Randall Veterans Affairs Medical Center, Geriatric Research Education and Clinical Center, Gainesville,
FloridabDepartment of Pharmacology and Therapeutics, College of Medicine, University of Florida, Gainesville, FloridacDepartment of Pharmacology, Marmara University School of Pharmacy, Istanbul, TurkeydDepartment of Applied Physiology and Kinesiology, College of Health & Human Performance, University of Florida,
Gainesville, Florida
a r t i c l e i n f o
Article history:
Received 1 November 2013
Received in revised form
7 January 2014
Accepted 30 January 2014
Available online xxx
Keywords:
Mechanical ventilation
Angiotensin
Losartan
Enalapril
NPY
Thyrosine hydroxylase
Dopamine beta hydroxylase
Sympathetic
Noradrenergic
Norepinephrine
* Corresponding author. Department of PhaGainesville, FL 32610.** Corresponding author. Pharmacology & The
E-mail addresses: [email protected]/$ e see front matter ª 2014 Elsevhttp://dx.doi.org/10.1016/j.jss.2014.01.054
a b s t r a c t
Background: Mechanical ventilation (MV) is a method of maintaining appropriate gas ex-
change in patients who are unable to sustain adequate alveolar ventilation. While life-
saving in the short-term, prolonged MV leads to altered cardiovascular responses and
enhanced lung injury, but the exact mechanism is unknown. Therefore, we investigated
the involvement of the sympathoadrenergic and renineangiotensin system in MV-induced
altered cardiovascular responses.
Methods: SpragueeDawley rats were divided into six groups: (1) spontaneous breathing (SB);
(2) SB þ enalapril (100 mg/kg intravenous infusion); (3) SB þ losartan (100 mg/kg infusion); (4)
12 h of MV; (5) MV þ enalapril; and (6) MV þ losartan. After the animals were sacrificed,
blood and tissue samples were collected. Tyrosine hydroxylase, dopamine beta hydroxy-
lase, and neuropeptide Y were measured in adrenal medulla and hypothalamus, whereas
AT1 was measured in lung tissues by Western blot. Norepinephrine enzyme-linked
immunosorbent assay and total antioxidant capacity were assayed in plasma.
Results: Our findings indicated that MV increases the sympathetic activation markers in ad-
renal medulla and hypothalamus. Moreover, oxidative stress was increased in lung and brain
tissues. Treatment with enalapril or losartan reduced the lipid peroxidation in lung and brain
tissues, while preserving the tissue glutathione content and plasma antioxidant capacity.
Conclusions: These data demonstrate that the inhibition of the renineangiotensin system by
enalapril or losartan may reduce the MV-induced increase in sympathetic activity markers
and oxidative stress, and thus, may have a beneficial effect as adjuvant therapy.
ª 2014 Elsevier Inc. All rights reserved.
rmacology and Therapeutics, College of Medicine, University of Florida, P.O. Box 100267,
rapeutics, College of Medicine, University of Florida, P.O. Box 100267, Gainesville, FL 32610.(H.Z. Toklu), [email protected] (N. Tumer).ier Inc. All rights reserved.

j o u r n a l o f s u r g i c a l r e s e a r c h x x x ( 2 0 1 4 ) 1e72
1. Introduction treated with the AT1 antagonist losartan; (4) 12 h of MV; (5)
Mechanical ventilation (MV) is a method to mechanically
assist or replace spontaneous breathing (SB). Although it is
often a lifesaving intervention in critically ill patients, it
carries many potential complications including pneumo-
thorax, acute lung injury, and ventilator-associated pneu-
monia. Other complications include diaphragm atrophy,
decreased cardiac output, and oxygen toxicity [1]. The in-
flammatory response in the lungs due toMVmay lead to distal
organ dysfunction.
Recent research indicates a cross talk between lungs and
other organs, including brain [2].The hypothalamic sym-
pathoadrenal medullary axis leads tomarked activation of the
adrenal medulla and sympathetic ganglia characterized by
elevated activity of the catecholamine biosynthesizing en-
zymes such as tyrosine hydroxylase (TH) and dopamine beta
hydroxylase (DbH), resulting in a rise in circulating epineph-
rine and norepinephrine (NE). TH is the rate-limiting step
in catecholamine biosynthesis as it catalyzes the hydroxyl-
ation of tyrosine to dopamine, whereas DbH catalyzes the
conversion of dopamine to NE. In addition to catecholamines,
neuropeptide Y (NPY) is synthesized in the adrenal medulla
and is co-released with epinephrine and NE. The previously
mentioned factors, TH, DbH, and NPY are considered as bio-
markers of sympathetic nervous system activity [3].
Sympathoactivation contributes to systemic stress and
cardiovascular complications. The patients who have pro-
longed MV display blood pressure alterations and abnormal
autonomic responses [4], which may be because of MV-
associated activation of the hypothalamic-pituitary-adrenal
axis or hypothalamic sympathoadrenal medullary axis.
Whether MV activates these axis is unknown.
The present study was aimed to test the hypothesis that a
12 h exposure to MV results in increased activation of the
hypothalamic sympathoadrenal medullary axis besides
increasing oxidative stress in plasma and other organs. Thus,
we measured TH, DbH, and NPY protein expression in the
adrenalmedulla and hypothalamus, lung angiotensin II type 1
(AT1) receptor protein levels, oxidative stress in lung and
brain, and plasma NE. In addition, the effects of enalapril-
angiotensin converting enzyme inhibitor (ACE) and losartan-
AT1 receptor blocker on MV-induced changes were evaluated.
2. Materials and methods
2.1. Animals
Adult female SpragueeDawley rats were obtained from
Charles River Labs and were aged 4e6 mo and w300 g at the
time of sacrifice. All animals were housed at the University of
Florida Animal Care Services Center according to the guide-
lines set forth by the Institutional Animal Care and Use
Committee. Animals were maintained on a 12-h lightedark
cycle and provided food (AIN93 diet) and water ad libitum
throughout the experimental protocol. Animals were divided
into six groups (10 animals/group) as follows: (1) 12 h of SB; (2)
SB group treated with the ACE inhibitor enalapril; (3) SB group
12 h of MV with the ACE inhibitor enalapril; and (6) 12 h of MV
with the AT1 antagonist losartan.
Losartan group received an intraperitoneal priming dose
(30 mg/kg) followed by intravenous infusion (100 mg/kg/min,
infusion rate 0.30 mL/h), and enalapril group received
enalapril (40 mg/kg) followed by an intravenous infusion
(100 mg/kg/min, infusion rate 0.30 mL/h) while during the 12 h
experimental period.
2.2. Experimental protocol
Animals were anesthetized with sodium pentobarbital
(60mg/kg, intraperitoneally). After reaching a surgical plane of
anesthesia, tracheostomy was performed on the animals
using aseptic techniques and mechanically ventilated with a
controlled pressure-driven ventilator (Servoventilator 300;
Siemens; Bridgewater, NJ) for 12 h with the following settings:
upper airway pressure limit, 20 cm H2O; pressure control level
above positive end-expiratory pressure 4e6 cm H2O; respira-
tory rate, 80 beats/min; and positive end-expiratory pressure
1.0 cm H2O. In general, we estimate that these ventilator
settings result in a tidal volume of w1 mL/100 g of body
weight. All surgical procedures were performed as previously
described in detail [15]. Briefly, cannulas were inserted into
the carotid artery to permit continuousmeasurement of blood
pressure and the collection of periodic arterial blood samples
during MV. Blood samples were analyzed for pH, pO2, and
pCO2 using an electronic blood gas analyzer (GEM Premier
3000; Instrumentation Laboratory; Lexington, MA). If neces-
sary, adjustments were made to the ventilator to ensure that
the arterial blood gas and pH measures were within the
desired physiological ranges. PaO2 was maintained at 70 mm
Hg throughout the experiment by adjustments in FiO2 (22%e
25% oxygen). Cannulas were inserted into the jugular vein for
the constant infusion of sodium pentobarbital (w10 mg/kg/h).
Body temperature was maintained between 36�C and 37�C by
using a recirculating heating blanket. Continuous care during
the MV protocol included lubricating the eyes, expressing the
bladder, removing airway mucus, rotating the animal, and
passive limb movement. After 12 h of MV, the animals were
immediately killed, and blood and tissue samples were
collected.
2.3. Enzyme-linked immunosorbent assaymeasurements of plasma NE
Blood samples were taken via cardiac puncture at the time of
sacrifice and centrifuged at 5000 rpm for 10 min at 4�C. Thesamples were stored at �80�C until further analysis by an
enzyme-linked immunosorbent assay kit (Rocky Mountain
Diagnostics, Inc Colorado Springs, CO) following the in-
structions of the manufacturer.
2.4. Total antioxidant capacity in the plasma
Total antioxidant capacity in the plasma was evaluated by
Oxiselect kit (Biocell Laboratories, San Diego, CA) according to
the manufacturer’s instructions.
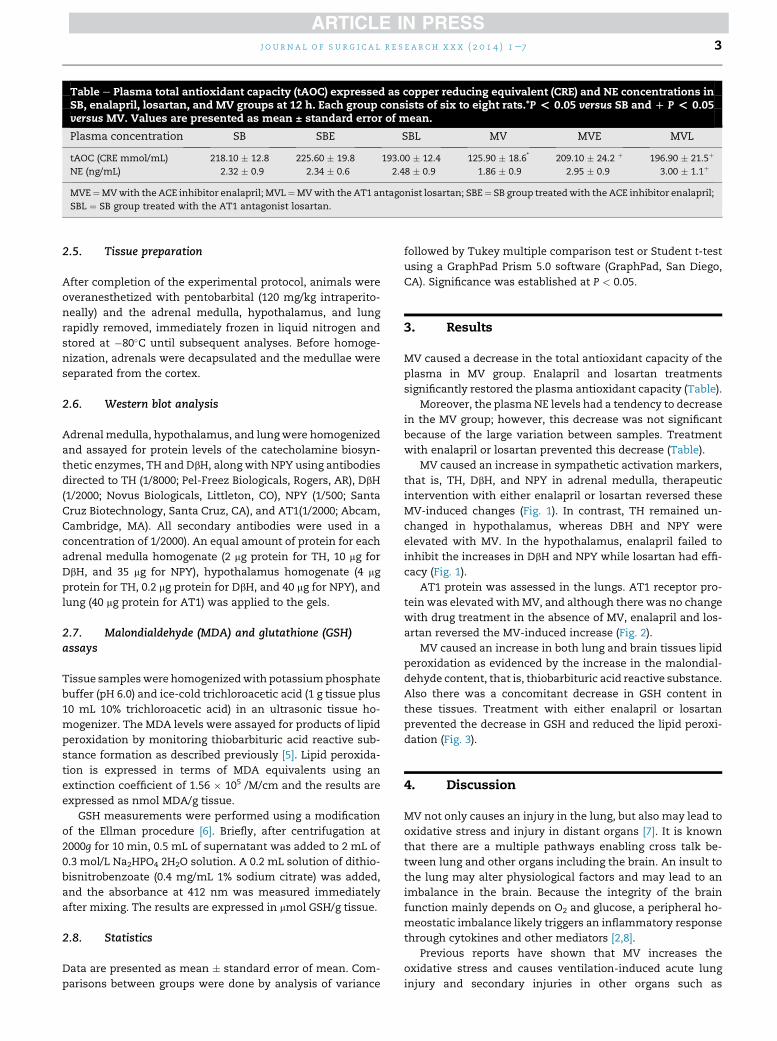
Table e Plasma total antioxidant capacity (tAOC) expressed as copper reducing equivalent (CRE) and NE concentrations inSB, enalapril, losartan, and MV groups at 12 h. Each group consists of six to eight rats.*P < 0.05 versus SB and D P < 0.05versus MV. Values are presented as mean ± standard error of mean.
Plasma concentration SB SBE SBL MV MVE MVL
tAOC (CRE mmol/mL) 218.10 � 12.8 225.60 � 19.8 193.00 � 12.4 125.90 � 18.6* 209.10 � 24.2 þ 196.90 � 21.5þ
NE (ng/mL) 2.32 � 0.9 2.34 � 0.6 2.48 � 0.9 1.86 � 0.9 2.95 � 0.9 3.00 � 1.1þ
MVE¼MVwith the ACE inhibitor enalapril; MVL¼MVwith the AT1 antagonist losartan; SBE¼ SB group treatedwith the ACE inhibitor enalapril;
SBL ¼ SB group treated with the AT1 antagonist losartan.
j o u rn a l o f s u r g i c a l r e s e a r c h x x x ( 2 0 1 4 ) 1e7 3
2.5. Tissue preparation
After completion of the experimental protocol, animals were
overanesthetized with pentobarbital (120 mg/kg intraperito-
neally) and the adrenal medulla, hypothalamus, and lung
rapidly removed, immediately frozen in liquid nitrogen and
stored at �80�C until subsequent analyses. Before homoge-
nization, adrenals were decapsulated and the medullae were
separated from the cortex.
2.6. Western blot analysis
Adrenal medulla, hypothalamus, and lung were homogenized
and assayed for protein levels of the catecholamine biosyn-
thetic enzymes, TH and DbH, along with NPY using antibodies
directed to TH (1/8000; Pel-Freez Biologicals, Rogers, AR), DbH
(1/2000; Novus Biologicals, Littleton, CO), NPY (1/500; Santa
Cruz Biotechnology, Santa Cruz, CA), and AT1(1/2000; Abcam,
Cambridge, MA). All secondary antibodies were used in a
concentration of 1/2000). An equal amount of protein for each
adrenal medulla homogenate (2 mg protein for TH, 10 mg for
DbH, and 35 mg for NPY), hypothalamus homogenate (4 mg
protein for TH, 0.2 mg protein for DbH, and 40 mg for NPY), and
lung (40 mg protein for AT1) was applied to the gels.
2.7. Malondialdehyde (MDA) and glutathione (GSH)assays
Tissue sampleswere homogenizedwith potassiumphosphate
buffer (pH 6.0) and ice-cold trichloroacetic acid (1 g tissue plus
10 mL 10% trichloroacetic acid) in an ultrasonic tissue ho-
mogenizer. The MDA levels were assayed for products of lipid
peroxidation by monitoring thiobarbituric acid reactive sub-
stance formation as described previously [5]. Lipid peroxida-
tion is expressed in terms of MDA equivalents using an
extinction coefficient of 1.56 � 105 /M/cm and the results are
expressed as nmol MDA/g tissue.
GSH measurements were performed using a modification
of the Ellman procedure [6]. Briefly, after centrifugation at
2000g for 10 min, 0.5 mL of supernatant was added to 2 mL of
0.3 mol/L Na2HPO4 2H2O solution. A 0.2 mL solution of dithio-
bisnitrobenzoate (0.4 mg/mL 1% sodium citrate) was added,
and the absorbance at 412 nm was measured immediately
after mixing. The results are expressed in mmol GSH/g tissue.
2.8. Statistics
Data are presented as mean � standard error of mean. Com-
parisons between groups were done by analysis of variance
followed by Tukey multiple comparison test or Student t-test
using a GraphPad Prism 5.0 software (GraphPad, San Diego,
CA). Significance was established at P < 0.05.
3. Results
MV caused a decrease in the total antioxidant capacity of the
plasma in MV group. Enalapril and losartan treatments
significantly restored the plasma antioxidant capacity (Table).
Moreover, the plasmaNE levels had a tendency to decrease
in the MV group; however, this decrease was not significant
because of the large variation between samples. Treatment
with enalapril or losartan prevented this decrease (Table).
MV caused an increase in sympathetic activation markers,
that is, TH, DbH, and NPY in adrenal medulla, therapeutic
intervention with either enalapril or losartan reversed these
MV-induced changes (Fig. 1). In contrast, TH remained un-
changed in hypothalamus, whereas DBH and NPY were
elevated with MV. In the hypothalamus, enalapril failed to
inhibit the increases in DbH and NPY while losartan had effi-
cacy (Fig. 1).
AT1 protein was assessed in the lungs. AT1 receptor pro-
tein was elevated with MV, and although there was no change
with drug treatment in the absence of MV, enalapril and los-
artan reversed the MV-induced increase (Fig. 2).
MV caused an increase in both lung and brain tissues lipid
peroxidation as evidenced by the increase in the malondial-
dehyde content, that is, thiobarbituric acid reactive substance.
Also there was a concomitant decrease in GSH content in
these tissues. Treatment with either enalapril or losartan
prevented the decrease in GSH and reduced the lipid peroxi-
dation (Fig. 3).
4. Discussion
MV not only causes an injury in the lung, but also may lead to
oxidative stress and injury in distant organs [7]. It is known
that there are a multiple pathways enabling cross talk be-
tween lung and other organs including the brain. An insult to
the lung may alter physiological factors and may lead to an
imbalance in the brain. Because the integrity of the brain
function mainly depends on O2 and glucose, a peripheral ho-
meostatic imbalance likely triggers an inflammatory response
through cytokines and other mediators [2,8].
Previous reports have shown that MV increases the
oxidative stress and causes ventilation-induced acute lung
injury and secondary injuries in other organs such as
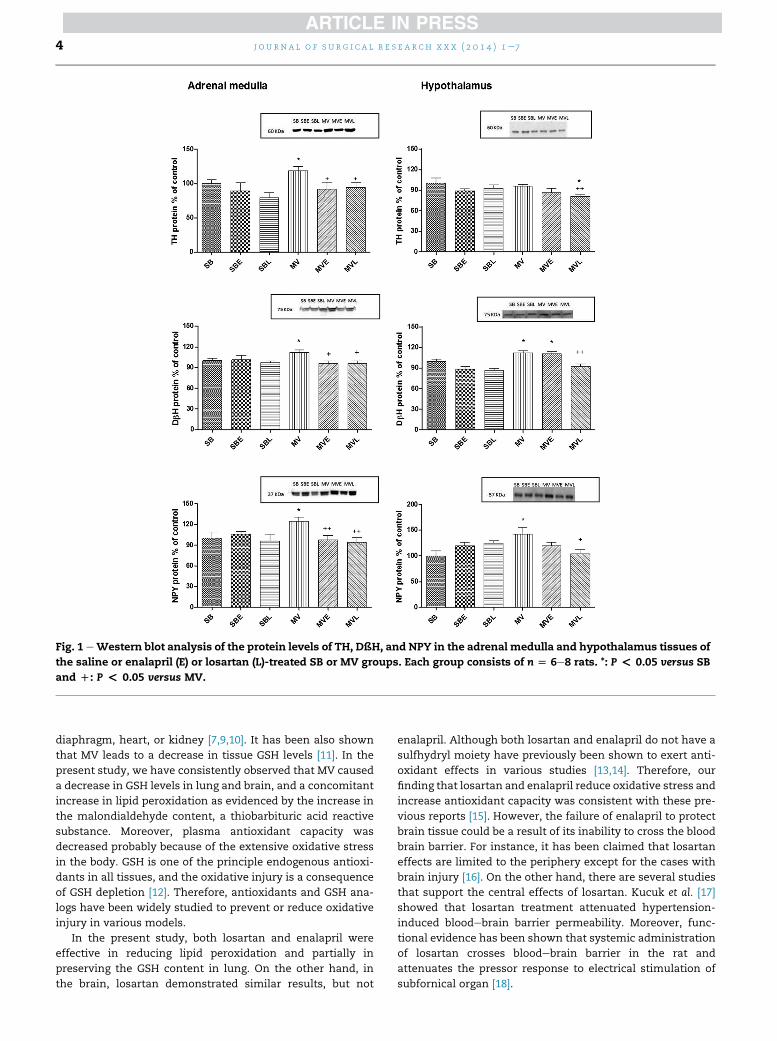
Fig. 1 eWestern blot analysis of the protein levels of TH, DßH, and NPY in the adrenal medulla and hypothalamus tissues of
the saline or enalapril (E) or losartan (L)-treated SB or MV groups. Each group consists of n [ 6e8 rats. *: P < 0.05 versus SB
and D: P < 0.05 versus MV.
j o u r n a l o f s u r g i c a l r e s e a r c h x x x ( 2 0 1 4 ) 1e74
diaphragm, heart, or kidney [7,9,10]. It has been also shown
that MV leads to a decrease in tissue GSH levels [11]. In the
present study, we have consistently observed that MV caused
a decrease in GSH levels in lung and brain, and a concomitant
increase in lipid peroxidation as evidenced by the increase in
the malondialdehyde content, a thiobarbituric acid reactive
substance. Moreover, plasma antioxidant capacity was
decreased probably because of the extensive oxidative stress
in the body. GSH is one of the principle endogenous antioxi-
dants in all tissues, and the oxidative injury is a consequence
of GSH depletion [12]. Therefore, antioxidants and GSH ana-
logs have been widely studied to prevent or reduce oxidative
injury in various models.
In the present study, both losartan and enalapril were
effective in reducing lipid peroxidation and partially in
preserving the GSH content in lung. On the other hand, in
the brain, losartan demonstrated similar results, but not
enalapril. Although both losartan and enalapril do not have a
sulfhydryl moiety have previously been shown to exert anti-
oxidant effects in various studies [13,14]. Therefore, our
finding that losartan and enalapril reduce oxidative stress and
increase antioxidant capacity was consistent with these pre-
vious reports [15]. However, the failure of enalapril to protect
brain tissue could be a result of its inability to cross the blood
brain barrier. For instance, it has been claimed that losartan
effects are limited to the periphery except for the cases with
brain injury [16]. On the other hand, there are several studies
that support the central effects of losartan. Kucuk et al. [17]
showed that losartan treatment attenuated hypertension-
induced bloodebrain barrier permeability. Moreover, func-
tional evidence has been shown that systemic administration
of losartan crosses bloodebrain barrier in the rat and
attenuates the pressor response to electrical stimulation of
subfornical organ [18].

Fig. 2 e Western blot analysis of the protein levels of AT1
receptor in the lung tissues of the saline or enalapril (E)-or
losartan (L)-treated SB or MV groups. Each group consists
of n [ 6e8 rats. **: P < 0.01 versus SB and D: P < 0.05
versus MV.
j o u rn a l o f s u r g i c a l r e s e a r c h x x x ( 2 0 1 4 ) 1e7 5
MV caused an increase in sympathetic activation markers,
that is, TH, DbH, and NPY in adrenal medulla. Although TH
remained unchanged in hypothalamus, DbH and NPY were
elevated. Both drugs (enalapril and losartan) reversed these
MV-induced changes in the adrenal medulla. However, ena-
lapril failed to inhibit the increase in DbH and NPY while
Fig. 3 eMalonedialdehyde and GSH levels in lung (A and C) and b
(L)-treated groups. Each group consists of n [ 6e8 rats. *: P < 0
losartan had some efficacy. This increase in the protein levels
of the biosynthetic enzymes (TH and DbH) was probably
because of a compensatory mechanism to restore NE plasma
levels; we observed that plasma NE levels tended to decrease
at 12 h after MV.
The alteration of plasma epinephrine and NE levels
because ofMVwas previously reported by several researchers.
Aneman et al. [19] showed NE was inconsistent or unstable in
patients. Monteverde [20] showed that the NE requirement
was increased in pediatric patients in prolonged MV and
Barbieri et al. [21] showed that the plasma epinephrine and NE
increased at the first hour of MV in patients, and this increase
was restored to baseline levels by the termination of MV.
Moreover, Wieske et al. [22] have proposed that the autonomic
dysfunction caused abnormal heart rates in intensive care
unit patients.
Activation of angiotensin system contributes to several
pathophysiological effects in the cardiovascular system via the
activation of sympathetic nervous system [23].Previous studies
have reported an increase in lung or bronchoalveolar fluid
angiotensin II levels at 2 or 4 h of MV [24e27]. However, lung
ACE levels were found to be unchanged [25] or increased in
bronchoalveolar fluid [26]. Moreover, captopril was effective in
reducing theMV-induced lung injury and elevatedACE activity,
and blockade of bradykinin receptors did not attenuate the
effect of captopril. Moreover, the serum ACE levels were un-
changed, although angiotensin II levels were increased in the
bronchoalveolar fluid. Thus, indicating the role of a non-ACE
pathway for the production of angiotensin II [26].
A recent study has also shown that angiotensin 1e7 ana-
logs protected the lung against acute lung injury, thereby
increasing the ratio of ACE2/ACE activity and reducing the
rain (B and D) tissues of the salineorenalapril (E) or losartan
.05 versus SB and D: P < 0.05 versus MV.

Fig. 4 e Mechanical ventilation increases the sympathetic nervous system (SNS) tonus as a result of increased
norepinephrine (NE) turnover. The levels of biosynthetic enzymes, tyrosine hydroxylase (TH) and dopamine beta
hydroxylase (DßH) are increased, along with an increase in NPY, which is co-released with NE. Sympathoactivation also
activates the renin-angiotensin system.
j o u r n a l o f s u r g i c a l r e s e a r c h x x x ( 2 0 1 4 ) 1e76
bioavailability of angiotensin II and AT1 receptor actions [28].
Increased angiotensin or AT1 levels have been correlated with
the severity of the injury. Both receptor types AT1 and AT2 in
the lungswere also shown to increase after MV [25,27]. Similar
to treatment with ACE inhibitors, treatment with an angio-
tensin receptor blocker, losartan, has been shown to reduce
the lung edema, inflammation, and injury score and AT1 re-
ceptor messenger RNA because of MV [25,27].
In the present study, we did not measure the ACE activity
but we found that lung AT1 receptor protein was increased
in the lung at 12 h of MV, and both enalapril and losartan
treatments were effective in preventing this increase. As we
previously discussed, both treatments also reduced the
oxidative stress in the lungs and sympathetic nervous sys-
tem activity markers in the adrenal medulla. On the other
hand, it would have been valuable to evaluate the AT1 re-
ceptor protein in the aorta and to evaluate the sympathetic
nervous system activity in different brain regions other than
hypothalamus.
5. Conclusions
In summary, these data, for the first time, demonstrate that
inhibition of renineangiotensin system by enalapril or los-
artan may reduce the MV-induced increase in sympathetic
activity markers and oxidative stress, and thus, may have a
beneficial effect as adjuvant therapy.
On the other hand, in humans and a number of species,
including the hamster, quantitatively important chymase-
independent Ang II formation from Ang I occurs in the
heart, arteries, and kidney. However, chymase differs in rats
and rabbits and is not active in the conversion of Ang I to Ang
II, but is involved in Ang II degradation. Consequently, one
would anticipate that blockade of the system at the ACE step
in rats would be equivalent to inhibition of the Ang II receptor
in humans. On the other hand, AT1 receptor blockers may be
more effective than ACE inhibitors in humans [29].
Although the preliminary data of this study are important
to in terms of showing the involvement of the interaction of

j o u rn a l o f s u r g i c a l r e s e a r c h x x x ( 2 0 1 4 ) 1e7 7
renineangiotensin system with the MV-induced sympathetic
activation (Fig. 4), further studies are needed to elucidate the
detailed mechanisms and implement it into the clinical
setting.
Acknowledgment
This work was supported by the Medical Research Service of
the Department of Veterans Affairs. The authors declare that
they have no conflict of interest.
Author contributions: H.Z.T. collected the data, performed
statistical analysis, and prepared the manuscript. O-S.K.
adapted the animal model, performed the surgery, and
collected the data. Y.S., K.L., and N.K. collected the data and
performed analysis. K.J.S., M.P.W., A.J.S., and E.E.T performed
the surgery, followup the animals, and collected the data. S.P.,
P.J.S., and N.T. were responsible for experimental design and
prepared the manuscript.
Disclosure
The authors reported no proprietary or commercial interest in
any product mentioned or concept discussed in this article.
r e f e r e n c e s
[1] Schmidt GA. Cardiopulmonary interactions in acute lunginjury. CurrOpinCrit Care 2013;19:51.
[2] Gonzalvo R, Martı-Sistac O, Blanch L, Lopez-Aguilar J. Bench-to-bedside review: brain-lung interaction in the criticallyillea pending issue revisited. Crit Care 2007;11:216.
[3] Goldstein DS, Eisenhofer G, Kopin IJ. Sources and significanceof plasma levels of catechols and their metabolites inhumans. J PharmacolExpTher 2003;305:800.
[4] Frazier SK, Moser DK, Schlanger R, Widener J, Pender L,Stone KS. Autonomic tone in medical intensive care patientsreceiving mechanical ventilation and during a CPAP weaningtrial. Biol Res Nurs 2008;9:301.
[5] Beuge JA, Aust SD. Microsomal lipid peroxidation. MethodsEnzymol 1978;53:302.
[6] Beutler E. Glutathione in red blood cell metabolism. Amanual of biochemical methods. New York: Grune&Stratton;1975. p. 112.
[7] de Prost N, Ricard JD, Saumon G, Dreyfuss D. Ventilator-induced lung injury: historical perspectives and clinicalimplications. Ann Intensive Care 2011;1:28.
[8] Pelosi P, Rocco PR. The lung and the brain: a dangerous cross-talk. Crit Care 2011;15:168.
[9] Kavazis AN, Talbert EE, Smuder AJ, Hudson MB, Nelson WB,Powers SK. Mechanical ventilation induces diaphragmaticmitochondrial dysfunction and increased oxidantproduction. Free RadicBiol Med 2009;46:842.
[10] Sweeney RM, Griffiths M, McAuley DF. Treatment of acutelung injury: current and emerging pharmacologicaltherapies. SeminRespirCrit Care Med 2013;34:487.
[11] Chiang CH, Chuang CH, Liu SL, Chian CF, Zhang H, Ryu JH. N-acetylcysteine attenuates ventilator-induced lung injury inan isolated and perfused rat lung model. Injury 2012;43:1257.
[12] Wu G, Fang YZ, Yang S, Lupton JR, Turner ND. Glutathionemetabolismand its implications for health. J Nutr 2004;134:489.
[13] Nishi EE, Bergamaschi CT, Oliveira-Sales EB, Simon KA,Campos RR. Losartan reduces oxidative stress within therostral ventrolateral medulla of rats with renovascularhypertension. Am J Hypertens 2013;26:858.
[14] Betto MR, Lazarotto LF, Watanabe TT, Driemeier D, Leite CE,Campos MM. Effects of treatment with enalapril onhepatotoxicity induced by acetaminophen in mice. NaunynSchmiedebergs Arch Pharmacol 2012;385:933.
[15] Yamazaki T, Tanimoto M, Gohda T, et al. Combinationeffects of enalapril and losartan on lipid peroxidation inthe kidneys of KK-Ay/Ta mice. Nephron Exp Nephrol 2009;113:e66.
[16] Ranadive SA, Chen AX, Serajuddin AT. Relative lipophilicitiesand structural-pharmacological considerations of variousangiotensin-converting enzyme (ACE) inhibitors. Pharm Res1992;9:1480.
[17] Kucuk M, Kaya M, Kalayci R, et al. Effects of losartan on theblood-brain barrier permeability in long-term nitric oxideblockade-induced hypertensive rats. Life Sci 2002;71:937.
[18] Li Z, Bains JS, Ferguson AV. Functional evidence that theangiotensin antagonist losartan crosses the blood-brainbarrier in the rat. Brain Res Bull 1993;30:33.
[19] Aneman A, Eisenhofer G, Fandriks L, et al. Splanchniccirculation and regional sympathetic outflow duringperoperative PEEP ventilation in humans. Br J Anaesth 1999;82:838.
[20] Monteverde E, Fernandez A, Poterala R, et al.Characterization of pediatric patients receivingprolonged mechanical ventilation. PediatrCrit Care Med2011;12:e287.
[21] Barbieri A, Siniscalchi A, De Pietri L, Pasetto A, Torsello A,Nolli M. Modifications of plasma concentrations of hormonaland tissue factors during mechanical ventilation withpositive end-expiratory pressure. IntAngiol 2004;23:177.
[22] Wieske L, Chan Pin Yin DR, Verhamme C, Schultz MJ, vanSchaik IN, Horn J. Autonomic dysfunction in ICU-acquiredweakness: a prospective observational pilot study. IntensiveCare Med 2013;39:1610.
[23] Mehta PK, Griendling KK. Angiotensin II cell signaling:physiological and pathological effects in the cardiovascularsystem. Am J Physiol Cell Physiol 2007;292:C82.
[24] Chen CM, Wang LF, Chou HC, Jiang JS, Lin CH, Chuang WC.Ventilation-induced lung injury increases lung angiotensin IIin rats. J PediatrPulmo 2007;5:122.
[25] Jerng JS, Hsu YC, Wu HD, et al. Role of the renin-angiotensinsystem in ventilator-induced lung injury: an in vivo study ina rat model. Thorax 2007;62:527.
[26] Wosten-van Asperen RM, Lutter R, Haitsma JJ, et al. ACEmediates ventilator-induced lung injury in rats viaangiotensin II but not bradykinin. EurRespir J 2008;31:363.
[27] Yao S, Feng D, Wu Q, Li K, Wang L. Losartan attenuatesventilator-induced lung injury. J Surg Res 2008;145:25.
[28] Klein N, Gembardt F, Supe S, et al. Angiotensin-(1e7) protectsfrom experimental acute lung injury. Crit Care Med 2013;41:e334.
[29] Hollenberg NK. Implications of species difference for clinicalinvestigation: studies on the renin-angiotensin system.Hypertension 2000;35:150.