
The Effect of the Addition of Adipose-Derived Mesenchymal...
10
The Effect of the Addition of Adipose-Derived Mesenchymal Stem Cells to a Meniscal Repair in the Avascular Zone: An Experimental Study in Rabbits Miguel Angel Ruiz-Iban, M.D., Ph.D., Jorge Diaz-Heredia, M.D., Ph.D., Ignacio Garcfa-Gomez, Ph.D., Fausto Gonzalez-Lizan, M.D., Elena Elias-Martm, M.D., and Victor Abraira, Ph.D. Purpose: To determine whether adipose-derived mesenchymal stem cells (ASCs) affect the healing rate of meniscal lesions sutured in the avascular zone in rabbits. Methods: Four groups were used. In group A (n = 12) a short, 5-mm-long longitudinal lesion in the avascular zone of the anterior horn of the medial meniscus was created and immediately sutured. In group B (n = 8) the same short lesion was created but suture was delayed 3 weeks. In group C (n = 12) a larger, 15-mm-long lesion that spanned the whole meniscus was created and sutured immediately. In group D (n = 8) the same large lesion was sutured 3 weeks later. Both knees in each rabbit were used: 1 served as the control, and in the other, 1 X 10 5 allogeneic ASCs marked with bromodeoxyuridine were placed in the lesion immediately before suturing. The animals were killed at 12 weeks. Results: In group A (short lesion, acute repair) 6 of 12 ASC-treated menisci and 0 of 12 controls had some healing (P = .014). In group B (short lesion, delayed repair) 2 of 8 ASC-treated menisci and 1 of 8 controls had some healing (P = .5). In group C (long lesion, acute repair) 6 of 12 ASC-treated menisci and 0 of 12 controls had some healing (P = .014). In group D (long lesion, delayed repair) 4 of 8 ASC-treated menisci and 0 of 8 controls had some healing (P = .07). The addition of ASCs increased the hearing rate (odds ratio, 32 [range, 3.69 to 277]; P = .002). The histologic analysis of the healed zones identified well-formed meniscal fibrocartilage with persistence of cells derived from the ASCs (immunolocated with anti-bromodeoxyuridine antibodies). Conclusions: Adding ASCs to a repair in the avascular zone of rabbit menisci increases the chances of healing. Healing is improved in small and larger lesions. When suture is delayed, the effect is not as evident. Clinical Relevance: In the future, ASCs might help in meniscal repair in the avascular zone. M enisci are essential parts of the knee that are tears is one of the most frequent orthopaedic surgical frequently injured. Meniscal tears are a com- procedures, and many times, a partial meniscectomy is mon cause of knee dysfunction, especially in active performed.2 Because there is ample evidence that me- and young patients.1 Surgical treatment of meniscal niscectomy has a deleterious effect on the knee in the From the Arthroscopic Surgery Unit, Department of Orthopedic Surgery (M.A.R-L, J.D-H., F.G-L.), Department of Anesthesiology (E.E-M.), and Clinical Biostatistics Unit (V.A.), Hospital Ramon y Cajal; and Laboratory of Cell Therapy, Hospital La Paz Health Research Institute (IdiPAZ) (I.G-G.), Madrid, Spain. Supported in pan by a grant awarded by the Asociacion Espanola de Artroscopia (Spanish Arthroscopy Association). The authors report no conflict of interest. Received September 20, 2010; accepted June 27, 2011. Address correspondence to Miguel Angel Ruiz-Ibdn, M.D., Ph.D., Unidad de Cirugia Artroscdpica, Departamento de COT, Hospital Ramon y Cajal, Cta Colmenar Km 9.100, Madrid 28034, Spain; E-mail: [email protected] © 2011 by the Arthroscopy Association of North America 0749-8063/1 OS53/$36.00 doi:10.1016/j.arthro.2011.06.041 1688 Arthroscopy: The Journal of Arthroscopic and Related Surgery, Vol 27, No 12 (December), 2011: pp 1688-1696
Transcript of The Effect of the Addition of Adipose-Derived Mesenchymal...

The Effect of the Addition of Adipose-Derived MesenchymalStem Cells to a Meniscal Repair in the Avascular Zone:
An Experimental Study in Rabbits
Miguel Angel Ruiz-Iban, M.D., Ph.D., Jorge Diaz-Heredia, M.D., Ph.D.,Ignacio Garcfa-Gomez, Ph.D., Fausto Gonzalez-Lizan, M.D.,
Elena Elias-Martm, M.D., and Victor Abraira, Ph.D.
Purpose: To determine whether adipose-derived mesenchymal stem cells (ASCs) affect the healingrate of meniscal lesions sutured in the avascular zone in rabbits. Methods: Four groups were used.In group A (n = 12) a short, 5-mm-long longitudinal lesion in the avascular zone of the anterior hornof the medial meniscus was created and immediately sutured. In group B (n = 8) the same shortlesion was created but suture was delayed 3 weeks. In group C (n = 12) a larger, 15-mm-long lesionthat spanned the whole meniscus was created and sutured immediately. In group D (n = 8) the samelarge lesion was sutured 3 weeks later. Both knees in each rabbit were used: 1 served as the control,and in the other, 1 X 105 allogeneic ASCs marked with bromodeoxyuridine were placed in the lesionimmediately before suturing. The animals were killed at 12 weeks. Results: In group A (short lesion,acute repair) 6 of 12 ASC-treated menisci and 0 of 12 controls had some healing (P = .014). In groupB (short lesion, delayed repair) 2 of 8 ASC-treated menisci and 1 of 8 controls had some healing(P = .5). In group C (long lesion, acute repair) 6 of 12 ASC-treated menisci and 0 of 12 controls hadsome healing (P = .014). In group D (long lesion, delayed repair) 4 of 8 ASC-treated menisci and0 of 8 controls had some healing (P = .07). The addition of ASCs increased the hearing rate (oddsratio, 32 [range, 3.69 to 277]; P = .002). The histologic analysis of the healed zones identifiedwell-formed meniscal fibrocartilage with persistence of cells derived from the ASCs (immunolocatedwith anti-bromodeoxyuridine antibodies). Conclusions: Adding ASCs to a repair in the avascularzone of rabbit menisci increases the chances of healing. Healing is improved in small and largerlesions. When suture is delayed, the effect is not as evident. Clinical Relevance: In the future, ASCsmight help in meniscal repair in the avascular zone.
Menisci are essential parts of the knee that are tears is one of the most frequent orthopaedic surgicalfrequently injured. Meniscal tears are a com- procedures, and many times, a partial meniscectomy is
mon cause of knee dysfunction, especially in active performed.2 Because there is ample evidence that me-and young patients.1 Surgical treatment of meniscal niscectomy has a deleterious effect on the knee in the
From the Arthroscopic Surgery Unit, Department of Orthopedic Surgery (M.A.R-L, J.D-H., F.G-L.), Department of Anesthesiology(E.E-M.), and Clinical Biostatistics Unit (V.A.), Hospital Ramon y Cajal; and Laboratory of Cell Therapy, Hospital La Paz Health ResearchInstitute (IdiPAZ) (I.G-G.), Madrid, Spain.
Supported in pan by a grant awarded by the Asociacion Espanola de Artroscopia (Spanish Arthroscopy Association).The authors report no conflict of interest.Received September 20, 2010; accepted June 27, 2011.Address correspondence to Miguel Angel Ruiz-Ibdn, M.D., Ph.D., Unidad de Cirugia Artroscdpica, Departamento de COT, Hospital
Ramon y Cajal, Cta Colmenar Km 9.100, Madrid 28034, Spain; E-mail: [email protected]© 2011 by the Arthroscopy Association of North America0749-8063/1 OS53/$36.00doi:10.1016/j.arthro.2011.06.041
1688 Arthroscopy: The Journal of Arthroscopic and Related Surgery, Vol 27, No 12 (December), 2011: pp 1688-1696

NONOPERATIVE TREATMENT FOR ACUTE PCL INJURIES 1687
3. Tewes DP, Fritts HM, Fields RD, Quick DC, Buss DD. Chron-ically injured posterior cruciate ligament: Magnetic resonanceimaging. Clin Orthop Relat Res 1997:224-232.
4. Jung YB, Tae SK, Lee YS, Jung HJ, Nam CH, Park SJ. Activenon-operative treatment of acute isolated posterior cruciateligament injury with cylinder cast immobilization. Knee SurgSports Traumatol Arthrosc 2008;16:729-733.
5. Patel DY, Allen AA, Warren RF, Wickiewicz TL, SimonianPT. The nonoperative treatment of acute, isolated (partial orcomplete) posterior cruciate ligament-deficient knees: An in-termediate-term follow-up study. HSS J 2007;3:137-146.
6. Shelbourne KD, Muthukaruppan Y. Subjective results of non-operatively treated, acute, isolated posterior cruciate ligamentinjuries, Arthroscopy 2005;21:457-461.
7. Boynton MD, Tietjens BR. Long-term followup of the un-treated isolated posterior cruciate ligament-deficient knee.Am J Sports Med 1996;24:306-310.
8. Oakes DA, Markolf KL, McWilliams J, Young CR, McAllisterDR. Biomechanical comparison of tibial inlay and tibial tunneltechniques for reconstruction of the posterior cruciate liga-ment. Analysis of graft forces. / Bone Joint Surg Am 2002;84:938-944.
9. Torg JS, Barton TM, Pavlov H, Sti'ne R. Natural history of theposterior cruciate ligament-deficient knee. Clin Orthop RelatRes 1989:208-216.
10. Cross MJ, Powell JF. Long-term followup of posterior cruciateligament rupture: A study of 116 cases. Am J Sports Med1984;12:292-297.
11. Schulte KR, Chu ET, Fu EH. Arthroscopic posterior cruciateligament reconstruction. Clin Sports Med 1997;16:145-156.
12. Hughston JC, Bowden JA, Andrews JR, Norwood LA. Acutetears of the posterior cruciate ligament. Results of operativetreatment. J Bone Joint Surg Am 1980;62:438-450.
13. Richter M, Kiefer H, Hehl G, Kinzl L. Primary repair forposterior cruciate ligament injuries. An eight-year followup offirry-three patients. Am J Sports Med 1996;24:298-305.
14. Bellelli A, Mancini P, Polito M, David V, Mariani PP. Mag-netic resonance imaging of posterior cruciate ligament inju-ries: A new classification of traumatic tears. Radial Med 2006;111:828-835.
15. Gross ML, Grover JS, Bassett LW, Seeger LL, Finerman GA.Magnetic resonance imaging of the posterior cruciate liga-ment. Clinical use to improve diagnostic accuracy. Am JSports Med 1992;20:732-737.
16. Jung YB, Jung HJ, Yang JJ, et al. Characterization of sponta-neous healing of chronic posterior cruciate ligament injury:Analysis of instability and magnetic resonance imaging. /Magn Reson Imaging 2008;27:1336-1340.
17. Mariani PP, Margheritini F, Camillieri G, Bellelli A. Serialmagnetic resonance imaging evaluation of the patellar tendonafter posterior cruciate ligament reconstruction. Arthroscopy2002;18:38-45.
18. Insall JN, Dorr LD, Scott RD, Scott WN. Rationale of theKnee Society clinical rating system. Clin Orthop Relat Res1989:13-14.
19. Hefti F, Mtiller W, Jakob RP, Staubli HU. Evaluation of kneeligament injuries with the IKDC form. Knee Surg SportsTraumatol Arthrosc 1993;l:226-234.
20. brgang JJ, Anderson AF, Boland AL, et al. Development andvalidation of the international knee documentation committeesubjective knee form. Am J Sports Med 2001;29:600-613.
21. Tegner Y, Lysholm J. Rating systems in the evaluation of kneeligament injuries. Clin Orthop Relat Res 1985:43-49.
22. Fowler PJ, Messieh SS. Isolated posterior cruciate ligamentinjuries in athletes. Am J Sports Med 1987;15:553-557.
23. Parolie JM, Bergfeld JA. Long-term results of nonoperativetreatment of isolated posterior cruciate ligament injuries in theathlete. Am J Sports Med 1986;14:35-38.
24. Clancy WG Jr, Shelbourne KD, Zoelmer GB, Keene JS,Reider B, Rosenberg TD. Treatment of knee joint instabilitysecondary to rupture of the posterior cruciate ligament. Reportof a new procedure. J Bone Joint Surg Am 1983;65:310-322.
25. Dejour H, Walch G, Peyrot J, Eberhard P. The natural historyof rupture of the posterior cruciate ligament. Rev Chir OrthopReparatrice Appar Mot 1988;74:35-43 (in French).
26. Shelbourne KD, Rubinstein RA Jr. Methodist Sports Med-icine Center's experience with acute and chronic isolatedposterior cruciate ligament injuries. Clin Sports Med 1994;13:531-543.
27. Gill TJ, Van de Velde SK, Wing DW, Oh LS, Hosseini A, LiG. Tibiofemoral and patellofemoral kinematics after recon-struction of an isolated posterior cruciate ligament injury: Invivo analysis during lunge. Am J Sports Med 2009;37:2377-2385.
28. Strobel MJ, Weiler A, Schulz MS, Russe K, Eichhorn HJ.Fixed posterior subluxation in posterior cruciate ligament-deficient knees: Diagnosis and treatment of a new clinical sign.Am J Spans Med 2002;30:32-38.
29. Grover JS, Bassett LW, Gross ML, Seeger LL, Finerman GA.Posterior cruciate ligament: MR imaging. Radiology 1990;174:527-530.
30. Heron CW, Calvert PT. Three-dimensional gradient-echo MRimaging of the knee: Comparison with arthroscopy in 100patients. Radiology 1992;183:839-844.
31. Akisue T, Kurosaka M, Yoshiya S, Kuroda R, Mizuno K.Evaluation of healing of the injured posterior cruciate liga-ment: Analysis of instability and magnetic resonance imaging.Arthroscopy 2001;17:264-269.
32. Servant CT, Ramos JP, Thomas NP. The accuracy of magneticresonance imaging in diagnosing chronic posterior cruciateligament injury. Knee 2004; 11:265-270.
33. Adachi N, Ochi M, Sumen Y, Deie M, Murakami Y, UchioY. Temporal changes in posterior laxity after isolated pos-terior cruciate ligament injury: 35 patients examined bystress radiography and MRI. Acta Orthop Scand 2003 ;74:683-688.

STEM CELLS IN MENISCAL REPAIR IN RABBITS 1689
long-term,1-3 meniscal repair is considered a betteroption when possible.
There have been many attempts to modify the bio-chemical environment of a meniscal suture to improvethe chances of healing. Different strategies have beentried such as perforations to the vascular zone,3-4 theuse of synovial grafts,5"7 osseous perforations,8 andthe addition of fibrin clots9'11 or various growth fac-tors.12-13 Some have shown limited success but aregenerally considered insufficient.
The success of a meniscal suture depends on manyfactors, but the local biologic properties of the menis-cal tissue have an important role. In particular, suturedlesions in the central avascular zone of the meniscushave a worse outcome14-16; this is because of not onlythe absence of vascularization but also the presence ofantiangiogenic factors.13-17
Stem cells have been proposed as an exciting alter-native in tissue and cellular regeneration.18 Althoughthe use of embryonic stem cells is controversial, adultmesenchymal stem cells (MSCs) are present in mosttissues and can be easily obtained in sufficient quan-tities from fat (adipose-derived mesenchymal stemcells [ASCs]) or bone marrow (bone marrow-derivedmesenchymal stem cells [BMSCs]) without ethicalconcerns. MSCs have been shown to be useful in theregeneration of skin and bone defects in humans19'22
and of many more different tissues in animals.23 Inparticular, recent evidence has shown that MSCs canhelp in the regeneration of meniscal defects.24-26
The purpose of this study was to determine whetherthe addition of ASCs to a sutured lesion in the avas-cular zone of the rabbit meniscus could help to im-prove meniscal healing and whether different lesionlengths and a delay in meniscal suture could affect theefficacy, if any, of this cell-assisted therapy. The hy-pothesis of this study was that ASCs would improvemeniscal healing and that different lesion lengths anda delay in meniscal suture would affect the efficacy ofthis therapy.
METHODS
The study was performed in 40 female New Zea-land white rabbits weighing 3.0 to 3.5 kg, with a meanweight of 3.2 kg. The rabbits had closed epiphyses.Approval from the animal care ethics committee ofour institution was obtained.
Isolation, Culture, and Characterization of ASCs
The ASCs were obtained from the adipose tissue ofthe inguinal fat pad of 3 rabbits not included in the
study that came from the same genetic pool as thoseused in the study and had been killed for otherpurposes. The adipose tissue was minced into smallpieces and digested with type I collagenase (GibcoBRL, Paisley, Scotland) for 30 minutes at 37°C.After centrifugation (300g, 5 minutes) of the di-gested tissue, mature adipocytes were discarded,and the pellet was centrifuged in a Ficoll-Paque(Amersham Biosciences, Uppsala, Sweden) densitygradient (670g, 30 minutes) to isolate low-densitymononuclear cells. Then, the cells were placed inplastic culture dishes and cultured in an incubator at37°C in a humid atmosphere with 5% carbon dioxide inDulbecco modified Eagle medium (DMEM) (GibcoBPvL) containing 10% fetal bovine serum (Gibco BRL)and 0.1% antibiotic-antimycotic solution (Gibco BRL).The culture medium was changed to eliminate nonad-herent cells 24 hours after seeding and every 4 daysthereafter. For subculture, cells were resuspended with0.05% (vol/vol) trypsin in Hanks Balanced Solution(Sigma-Aldrich, St. Louis, MO) when an 80% to 90%confluence was reached. All experiments were per-formed when cells were subcultured 3 to 5 times. Toidentify implanted ASCs, 50-ju,mol/L bromodeoxyuri-dine (BrdU) (Sigma-Aldrich) was added into the cul-ture medium 24 hours before cell implantation. BrdUis a thymidine analog that substitutes thymidine inDNA and has no known effect in cellular mitosis. It isa widely used method for immunostaining of newlysynthetized DNA.
Characterization studies were carried out analyzingthe expression of the surface markers CD90, CD49e,and HLA-DR to confirm the ASC phenotype of thecultured cells. Cells were analyzed by 4-color flowcytometry with a FACSCalibur flow cytometer (BDBiosciences, San Jose, CA) after staining with fluoro-chrome-conjugated monoclonal antibodies used at sat-urating quantities: allophycocyanin conjugated CD90(BD Biosciences), phycoerythrin conjugated CD49e(BD Biosciences), and phycoerythrin conjugatedHLA-DR (BD Biosciences). In brief, 2 X 105 nucle-ated cells were incubated for 20 minutes at roomtemperature, with the previously mentioned antibod-ies. Data acquisition and analysis were performedwith the CELLQuest PRO software program (BDBiosciences).
Study Groups
The animals were assigned consecutively to 4 dif-ferent groups. In group A (12 animals) the animalsunderwent creation of a short longitudinal lesion in the
1690 M. A. RUIZ-IBAN ET AL.
anterior horn of the medial meniscus that was imme-diately sutured. In group B (8 animals) an identicalshort lesion was created but suture was delayed for 3weeks. In group C (12 animals) a larger lesion thatspanned the meniscus from the anterior to posteriorhorn was created and sutured immediately. In group D(8 animals) the same large lesion was sutured in adelayed fashion 3 weeks later.
Surgical Technique
The animals were anesthetized with intravenous 1 %propofol (30 rag at induction and maintenance dosagebetween 1.5 and 3 mg/min). Preoperatively, both an-tibiotic prophylaxis and analgesics were administeredintramuscularly. Both knees were operated on at thesame time, and in each animal, 1 knee was assignedrandomly to the treatment group with ASCs and theother to the control group; this assignment was per-formed with a random number list.
The knee was accessed by a midline incision fromthe superior pole of the patella to the tibial tubercle. Amedial arthrotomy was performed longitudinally, andthe patella was dislocated laterally. The medial me-niscus was exposed and dislocated anteriorly, allow-ing for full exposure of the femoral side of the me-niscus.
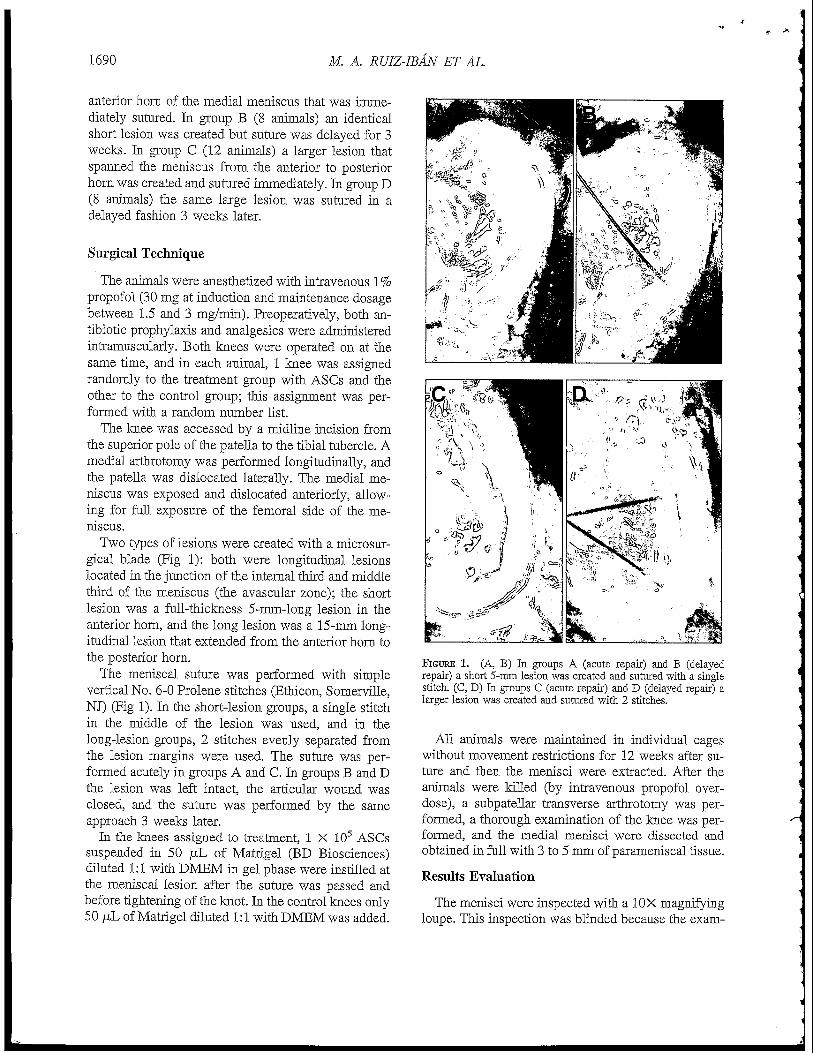
Two types of lesions were created with a microsur-gical blade (Fig 1): both were longitudinal lesionslocated in the junction of the internal third and middlethird of the meniscus (the avascular zone); the shortlesion was a full-thickness 5-mm-long lesion in theanterior horn, and the long lesion was a 15-mm long-itudinal lesion that extended from the anterior horn tothe posterior horn.
The meniscal suture was performed with simplevertical No. 6-0 Prolene stitches (Ethicon, Somerville,NJ) (Fig 1). In the short-lesion groups, a single stitchin the middle of the lesion was used, and in thelong-lesion groups, 2 stitches evenly separated fromthe lesion margins were used. The suture was per-formed acutely in groups A and C. In groups B and Dthe lesion was left intact, the articular wound wasclosed, and the suture was performed by the sameapproach 3 weeks later.
In the knees assigned to treatment, 1 X 105 ASCssuspended in 50 juJL of Matrigel (BD Biosciences)diluted 1:1 with DMEM in gel phase were instilled atthe meniscal lesion after the suture was passed andbefore tightening of the knot. In the control knees only50 juL of Matrigel diluted 1:1 with DMEM was added.
FIGURE 1. (A, B) In groups A (acute repair) and B (delayedrepair) a short 5-mm lesion was created and sutured with a singlestitch. (C, D) In groups C (acute repair) and D (delayed repair) alarger lesion was created and sutured with 2 stitches.
All animals were maintained in individual cageswithout movement restrictions for 12 weeks after su-ture and then the menisci were extracted. After theanimals were killed (by intravenous propofol over-dose), a subpatellar transverse arthrotomy was per-formed, a thorough examination of the knee was per-formed, and the medial menisci were dissected andobtained in full with 3 to 5 mm of parameniscal tissue.
Results Evaluation
The menisci were inspected with a 10X magnifyingloupe. This inspection was blinded because the exam-

STEM CELLS IN MENISCAL REPAIR IN RABBITS 1691
iner did not know which meniscus had received theASC treatment. The aspect and characteristics of themeniscal lesion and suture stitch were annotated, andthe suture was cut and extracted. The examination wascompleted by evaluation of the repair integrity withthe help of a microsurgical clamp and a graduatedprobe, and the lesions were assigned to 1 of thefollowing categories:
• Complete healing—the lesion is not apparent, or itis visible but completely healed with continuity ofthe meniscal tissue all along the lesion and throughall its depth.
• Partial healing-—in the short lesions the meniscushas healed all along the lesion but a defect is presenton either the tibial or femoral side that is deeperthan 20% of the meniscal depth; in the long lesionsthere is at least 1 zone (anterior horn or body orposterior horn) in which tissue continuity is presentbut there are areas of nonhealed tissue.
• No healing-—in the short lesions there is a full-thickness discontinuity at any level of the lesion; inthe long lesions there is a discontinuity of the me-niscal tissue that affects the entire length of thelesion.
After the macroscopic examination, the menisci werefixated in formaldehyde (solution A; DiaPath, Marti-nengo, Italy) for 15 days and were decalcified withhidrochloric acid and ethylenediaminetetraacetic acid(solution B; DiaPath) for 3 weeks and embedded inparaffin. Slides 5 to 10 /im thick were obtained in thecoronal plane of the meniscus perpendicular to thelesion. Slides were stained with H&E according tostandard laboratory protocols. The microscopic eval-uation consisted of examination of the healing zone ofthe meniscus and evaluation of meniscal cell morphol-ogy. Again, the examiner did not know which menis-cus had received the ASC treatment. Immunohisto-chemical staining for BrdU was performed by use of
anti-BrdU monoclonal antibody (Dako, Glostrup,Denmark) as primary antibody, biotin conjugatedgoat-x-mouse immunoglobulin G (Zymed, San Fran-cisco, CA) as secondary antibody, and 3,3-diamino-benzidine tetrahydrochloride (Dako) as chromogen.Negative controls were performed without primaryantibody incubation. The slides were analyzed withoptic microscopy at 20 X and 100X magnification.
Associations between treatment type and rate ofhealing were evaluated with a -£ test for each group.To estimate the effect on healing of the length of thelesion, timing of suture, and addition of ASCs (or not),a model of logistic regression was used. Because thedata were obtained from both knees of the same ani-mal, generalized estimating equations27 were used toadjust the model. The analysis was performed by astatistician who was independent from the rest of thestaff involved in the study and was unaware of thetreatment that was implemented in each group. Statis-tical analysis was performed with SPSS software (ver-sion 16.0; IBM, Armonk, NY) and Stata software(version 10.0; StataCorp, College Station, TX).
RESULTS
ASC Characterization
The ASC-cultured phenotypes were confirmed by theexpression of the surface markers CD90 (80%) andCD49e (98%) and the absence of HLA-DR (0.6%).
Surgical Technique
During the study, the animals did not have postoper-ative complications. The animals in groups B and D werereoperated on at 3 weeks to perform the suturing, and inall cases (32 knees [16 rabbits]) the meniscal lesionscreated previously were easily identified and no signs ofhealing were observed. Only visual and tactile analysiswas performed to confirm the absence of healing.
TABLE 1. Macroscopic Results: Healing Among Groups
Group
A: Short lesion, acute repair
B: Short lesion, chronic repair
C: Long lesion, acute repair
D: Long lesion, chronic repair
Treatment
ControlASCControlASCControlASCControlASC
No. ofMenisci
121288
121288
CompleteHealing
03010202
PartialHealing
03110402
NoHealing
12676
12684

1692 M. A. RUIZ-IBAN ET AL.
FIGURE 2. Macroscopic results. (A, B) Paired menisci of a rabbitin group A (short lesion, acute repair). In the ASC-treated meniscus(A), there is complete healing of the lesion that is barely visible; inthe control meniscus (B), the lesion has not healed. (C, D) Pairedmenisci of a rabbit in group D (long lesion, delayed repair). In theASC-treated meniscus (C), there is complete healing of the lesionthat is not visible and both stitches are included in meniscal tissue;in the control meniscus (D), the lesion has clearly not healed in theanterior horn and also did not heal in the posterior horn (confirmedwhen the stitches were taken out, not shown).
Macroscopic Findings
Loupe examination confirmed meniscal healing insome cases in both the ASC and control groups. Theresults are summarized in Table 1. Examples can be seenin Fig 2.
In group A (short lesion, sutured immediately, 12rabbits) 6 of the ASC-treated menisci and none ofthose in the control group had some kind of healing.These differences were significant (P = .014). Themenisci treated with ASCs presented partial healing in3 cases and complete healing in another 3.
In group B (short lesion, delayed suturing, 8 rabbits)2 of the ASC-treated menisci and 1 of those in thecontrol group had some kind of healing. These differ-ences were not significant (P = .5}. The meniscitreated with ASCs presented partial healing in 1 caseand complete healing in another; in the control me-nisci only partial healing was observed in 1 case.
In group C (long lesion, sutured immediately, 12rabbits) 6 of the ASC-treated menisci and none ofthose hi the control group had some kind of healing.These differences were significant (P = .014). Themenisci treated with ASCs presented partial healing in4 cases and complete healing in another 2.
In group D (long lesion, delayed suturing, 8 rabbits)4 of the ASC-treated menisci and none of those in thecontrol group had some kind of healing. These differ-ences were not significant (P = .07). The meniscitreated with ASCs presented partial healing in 2 casesand complete healing in another 2.
The multivariate analysis showed that the additionof MSCs to the repair increased the chances of me-niscal healing (odds ratio, 32 [range, 3.69 to 277]; P =.002). Delaying the suturing for 3 weeks did notsignificantly diminish the chances of healing (oddsratio, 1.14 [range, 0.35 to 3.66]; P = .2). Longerlesions did not have an increased chance of healing(odds ratio, 0.89 [range, 0.28 to 2.79]; P = .5~).
Microscopic Findings
The histologic characteristics of the parts of themenisci that had healed were different in the casestreated with ASCs compared with those in the controlgroup. In the ASC group the healed areas (Fig 3)presented a slight cellularity increase compared withthe normal tissue but the cellular morphology andfibrillar pattern were similar to those observed inadjacent areas of avascular meniscus. Meniscal fibro-chondrocytes were present and were the only apparentcell type at the lesion level. No vascular tissue wasobserved, strongly suggesting that the lesions hadbeen created in the avascular zone. In the controlgroup the single healed meniscus (1 case [2.5%])presented evident fibrous tissue at the healed areaclearly different from normal meniscal tissue.
Immunohistochemical Analysis
Antibody staining for BrdU showed that some ofthe fibrochondrocytes at the healed areas had positivenuclear staining and thus were direct descendantsfrom the original ASCs added at the time of suturing(Fig 3C).

STEM CELLS IN MENISCAL REPAIR IN RABBITS 1693
FIGURE 3. Histologic analysis. (A, B) H&B staining of a coronal section of the ASC-treated meniscus showing the injured zone filled withmeniscal-like cells and slightly hyperstained matrix (original magnification X10 hi A and X40 in B). (C) Imniunostaining of section showingcells with positive staining for BrdU (arrows) (original magnification X40). (D) Nonhealed control meniscus showing the defect (arrows)(original magnification XlO).
DISCUSSION
This study shows that the addition of ASCs to ameniscal repair improves the healing rates in the avas-cular zone. This effect is more evident when thesuturing is performed acutely.
Tears in the avascular zone of the meniscus do notheal spontaneously.28 Moreover, suturing does notfacilitate the healing process in rabbits29 or otheranimals.30 In humans, tears in the avascular zone havehealing rates below 20% to 30% after suturing. 15>31'32
Because the meniscal resection has well-known dele-terious effects in the long-term,33'36 it is necessary todevelop new strategies to improve meniscal hearing inthe avascular zone.
The rabbit was chosen as the experimental modelbecause there are no significant differences in thestructure and properties of the human and rabbit me-nisci.37 Indeed, it is a widely used model in meniscalhearing.38-40 The meniscal lesion created was specifi-cally designed to minimize the chances of spontane-ous healing: the medial meniscus has less healingpotential,27 and the lesion was created in the junctionof the internal third and middle third of the meniscus;this zone is avascular in rabbits.5-41-42 The meniscusavascular zone has an unusual environment that de-creases the chances of healing: there is little intrinsicresponse to cytokines, a small number of mitotic celldivisions, and a strong presence of antiangiogenic
factors.15-17 The difficulty of spontaneous healing ofthe meniscal lesions used in this study in the avascularzone was confirmed in the delayed repair groups inwhich the animals were reoperated on at 3 weeks toperform the suturing. The meniscal lesions createdpreviously were easily identified, and no signs ofhealing were observed in any cases (32 knees [16rabbits]). Furthermore, in the control groups (a total of40 knees) only 1 meniscus managed to heal (and onlypartially) even after suturing of the lesion.
MSCs can be obtained from many different tissues.Although bone marrow is often used (BMSCs), fattissue is more easily available and ASCs can be ob-tained in larger quantities with good viability.43 ASCshave been used extensively both in animal experimen-tal studies23-44 and in human clinical studies as treat-ment for Crohn fistulae45 and cranial bone defects.21
In our study we used allogeneic ASCs isolated fromdonor rabbits that were not syngeneic with the rabbitsused in the study. No signs of rejection were observedin the ASC-treated menisci. This result may be be-cause of the immunomodulatory properties ofASCs.46'47 Furthermore, the ASCs used in the exper-iments came from rabbits of a very homogeneouspopulation that have the same genetic pool.
The ASCs were placed in the repair in a gel carrier.This does not ensure maintenance of the ASCs at thelevel of the lesion, and some of these might have

1694 M. A. RUIZ-IB AN ET AL.
diffused to other parts of the joint. This did not haveany macroscopically relevant effects in the joint. Fur-thermore, MSCs have tropism to injured zones25 andmight have migrated to the injured meniscus.
Other authors have tried to increase the healingrates of meniscal lesions in the avascular zone withdifferent outcomes. Jitsuiki et al.6 used synovial tissuein a rabbit experimental model, obtaining only partialhealing in 90% of the animals without any completehealing. Sonoda et al.48 used hyaluronic acid associ-ated with suture in the same experimental setting andobtained partial healing in 25% of cases without anycomplete repair. The use of MSCs has been reportedby Port et al.49 in a study performed in goats. Theysupplemented the suture with BMSCs and fibrin clotsbut obtained only some degree of healing in 50% ofthe animals, concluding that there was no enhance-ment in meniscal healing. In other studies MSCs havebeen shown to help in the regeneration of meniscaldefects using artificial scaffolds50-51 or injected di-rectly into the joint.25-52 A recent report by Dutton etal.26 used BMSCs diluted in fibrin glue as adjuvantsfor suture. They showed complete macroscopic heal-ing in 75% of the BMSC-treated animals versus 0% ofthe animals in the control group in the treatment ofacute radial lesions in pig menisci. These studies arein agreement with our results that support the benefi-cial effect of MSCs (ASCs in our study) in the treat-ment of meniscal lesions in the avascular zone.
The mechanism of action of the ASCs cannot bedetermined from our study. The presence of cellsderived from the original implanted ASCs was con-firmed by the immunohistochemical analysis. Thisimplies that the ASCs proliferated and differentiatedto cellular lines compatible with the host tissue (his-tologically fibrochondrocytes in this case), whichmight have played a role in the healing process. Inaddition, a paracrine effect (secretion of growth fac-tors and other locally active substances) is a knownmechanism of action of MSC53 and cannot be ex-cluded.
Our results showed a clear improvement in menis-cal healing in acute lesions; there was less improve-ment in chronic lesions, but the multivariate analysisdid not appreciate a strong relation between time ofrepair and healing response. The biologic differencesbetween acute and chronic lesions have not been de-termined. In humans no clear advantage has beenobserved in healing rates of acute lesions.54-55 Thisstudy provides some supplementary evidence thatchronic lesions might have a decreased healing poten-
tial that may be related to the reported decrease incellularity at the lesion level.56
No significant differences were found between thehealing rates of longer lesions and shorter lesions inthe multivariate analysis. This may be attributed to thecontrary effect of 2 variables present: on the one hand,a longer lesion is more unstable and should heal withmore difficulty; on the other hand, the anterior hornseems to heal more poorly than the rest of the menis-cus,57 so extending the lesion posteriorly might in-crease the chances of healing.
This study suggests a new therapeutic approach forthe enhancement of meniscal repair in the avascularzone in humans. Nevertheless, it has some limitations.One potential weakness is that it may be possible thatsome of the lesions affected the vascular zone, al-though the lesions were created with special care so asnot to affect the vascular portion of the meniscus. Thispossibility is remote because the histologic analysisdid not show the presence of vascular structures at thelesion level in any case.
Another shortcoming of this study is that an initialpower analysis was not performed. This study wasintended to be an exploratory analysis of the potentialof ASCs in meniscal hearing, so a small number ofanimals was chosen. The difference in numbers in theacute and delayed repair groups was determined bybudget limitations over maintenance of animals forlong-term study.
Other studies with more animals, a different numberof ASCs implanted, and perhaps a larger animalmodel have to be considered before entering clinicaltrials. Furthermore, some fundamental aspects have tobe elucidated before clinical use; specifically, the al-logeneic nature of the cells and the type of cell carrierused initially preclude their use in humans and arelimitations of this study. Moreover, it is important toobtain better results in chronic lesions, which are themost common in the clinical setting.
CONCLUSIONS
Adding ASCs to a repair in the avascular zone ofrabbit menisci increases the chances of healing. Heal-ing is improved in small and larger lesions. Whensuture is delayed, the effect is not as evident.
Acknowledgment: The authors acknowledge the assis-tance of the Experimental Surgery Unit of Hospital Ramony Cajal, particularly veterinarians C. Correa, Ph.D., and A.Ortiz.

STEM CELLS IN MENISCAL REPAIR IN RABBITS 1695
REFERENCES
1. Starke C, Kopf S, Petersen W, Becker R. Meniscal repair.Arthroscopy 2009;25:1033-1044.
2. Praemer A, Burner S, Puce DP. Musculoskeletal conditions inthe United States. Rosemont, IL: American Academy of Or-thopaedic Surgeons, 1999.
3. Zhang ZN, Kaiyuan T, Yinkan X, Wenming Z, Zhentian L,Shihuan O. Treatment of longitudinal injuries in avascular areaof meniscus in dogs by trephination. Arthroscopy 1988;4:151-159.
4. Zhang ZN, Arnold JA, Williams T, McCann B. Repairs bytrephination and suturing of longitudinal injuries in the avas-cular area of the meniscus in goats. Am J Sports Med 1995;23:35-41.
5. Cisa J, Basora J, Madarnas P, Ghibely A, Navarro-Quilis A.Meniscal repair by synovial flap transfer. Healing of the avas-cular zone in rabbits. Acta Orthop Scand 1995;66:38-40.
6. Jitsuiki J, Ochi M, Ikuta Y. Meniscal repair enhanced by aninterpositional free synovial autograft: An experimental studyin rabbits. Arthroscopy 1994;10:659-666.
7. Shirakura K, Niijima M, Kobuna Y, Kizuki S. Free synoviumpromotes meniscal healing. Synovium, muscle and syntheticmesh compared in dogs. Acta Orthop Scand 1997;68:51-54.
8. Freedman KB, Nho SJ, Cole BJ. Marrow stimulating tech-nique to augment meniscus repair. Arthroscopy 2003;19:794-798.
9. Arnoczky SP, Warren RF, Spivak JM. Meniscal repair usingan exogenous fibrin clot. An experimental study in dogs.J Bone Joint Surg Am 1988;70:1209-1217.
10. Henning CE, Lynch MA, Yearout FT, Vequist SW, Stall-baumer RJ, Decker KA. Arthroscopic meniscal repair using anexogenous fibrin clot. Clin Orthop Relat Res 1990:64-72.
11. Ishimura M, Ohgushi H, Habata T, Tamai S, Fujisawa Y.Arthroscopic meniscal repair using fibrin glue. Part I: Exper-imental study. Arthroscopy 1997;13:551-557.
12. Hashimoto J, Kurosaka M, Yoshiya S, Hirohata K. Meniscalrepair using fibrin sealant and endothelial cell growth factor.An experimental study in dogs. Am J Sports Med 1992;20:537-541.
13. Petersen W, Pufe T, Starke C, et al. The effect of locallyapplied vascular endothelial growth factor on meniscus heal-ing: Gross and histological findings. Arch Orthop TraumaSurg 2007; 127:235-240.
14. Noyes FR, Barber-Westin SD. Arthroscopic repair of meniscaltears extending into the avascular zone in patients youngerthan twenty years of age. Am J Sports Med 2002;30:589-600.
15. Papachristou G, Efstathopoulus N, Plessas S, Levidiotis C,Chronopoulos E, Sourlas J. Isolated meniscal repair in theavascular area. Acta Orthop Belg 2003;69:341-345.
16. Kobayashi K, Fujimoto E, Deie M, Sumen Y, Ikuta Y, OchiM. Regional differences in the healing potential of the menis-cus—An organ culture model to eliminate the influence ofmicrovasculature and the synovium. Knee 2004;ll:271-278.
17. Becker R, Pufe T, Kulow S, et al. Expression of vascularendothelial growth factor during healing of the meniscus in arabbit model. J Bone Joint Surg Br 2004;86:1082-1087.
18. Garcia-Gomez I, Elvira G, Zapata AG, et al. Mesenchymalstem cells: Biological properties and clinical applications. Ex-pert Opin Biol Ther 2010;10:1453-1468.
19. Trebol Lopez J, Georgiev-Hristov T, Garcia-Arranz D, Garcia-Olmo D. Stem cell therapy for digestive tract diseases: Currentstate and future perspectives. Stem Cells Dev 2011;20:1113-1129.
20. Garcia-Olmo D, Garcia-Arranz D, Herreros D, Pascual I, PeiroC, Rodriguez-Montes JA. A phase I clinical trial of the treat-ment of Crohn's fistula by adipose mesenchymal stem celltransplantation. Dis Colon Rectum 2005;48:1416-1423.
21. Lendeckel SJ, Jodicke A, Christophis P, et al. Autologous stemcells (adipose) and fibrin glue used to treat widespread trau-matic calvarial defects: Case report. J Craniomaxillofac Surg2004;32:370-373.
22. Lee FH, Hui JHP. The potential of stem cells in orthopaedicsurgery. J Bone Joint Surg Br 2006;88:841-851.
23. Strem BM, Hicok KG, Zhu M, et al. Multipotential differen-tiation of adipose tissue-derived stem cells. Keio J Med 2005;54:132-141.
24. Izuta Y, Ochi M, Adachi N, Deie M, Yamasaki T, ShinomiyaR. Meniscal repair using bone marrow-derived mesenchymalstem cells: Experimental study using green fluorescent proteintransgenic rats. Knee 2005;12:217-223.
25. Horie M, Sekiya I, Muneta T, et al. Intra-articular injectedsynovial stem cells differentiate into meniscal cells directlyand promote meniscal regeneration without mobilization todistant organs in rat massive meniscal defect. Stem Cells2009;27:878-887.
26. Durton AQ, Choong PF, Goh JC, Lee FH, Hui HI Enhance-ment of meniscal repair in the avascular zone using mesen-chymal stem cells in a porcine model. J Bone Joint Surg Br2010;92:169-175.
27. Hardin JW, Hilbe JM. Generalized estimating equations. BocaRaton, FL: John Wiley & Sons, 2003.
28. King D. Mechanics of the healed meniscus in a canine model.J Bone Joint Surg 1936;18:333-342.
29. Veth RPH, Den Heeten GJ, Jansen HWB, Nielsen HKL.Repair of the meniscus. An experimental investigation in rab-bits. Clin Orthop Relat Res 1983;175:258-262.
30. Ghadially FN, Wedge JH, Lalonde JM. Experimental methodsof repairing injured menisci. / Bone Joint Surg Br 1986;68:106-110.
31. Rubman MH, Noyes FR, Barber-Westin SD. Arthroscopicrepair of meniscal tears that extend into the avascular zone. Areview of 198 single and complex tears. Am J Sports Med1998;26:87-95.
32. Okuda K, Ochi M, Shu N, Uchio Y. Meniscal rasping forrepair of meniscal tear in the avascular zone. Arthroscopy1999:15:281-286.
33. Fairbank T. Knee joint changes after meniscectomy. / BoneJoint Surg Br 1948;30:664-670.
34. Cox JS, Cordell LD. The degenerative effects of medial me-niscus tears in dogs' knees. Clin Orthop Relat Res 1977:236-242.
35. Baratz ME, Fu FH, Mengato R. Meniscal tears: The effect ofmeniscectomy and of repair on intraarticular contact areas andstress in the human knee. A preliminary report. Am J SportsMed 1986;14:270-275.
36. Hoser C, Fink C, Brown C, Reichkendler M, Hack! W, BartlettJ. Long-term results of arthroscopic partial lateral meniscec-tomy in knees without associated damage. / Bone Joint SurgBr 2001;83:513-516.
37. Sweigart MA, Zhu CF, Burt DM, et al. Intraspecies andinterspecies comparison of the compressive properties of themedial meniscus. Ann Biomed Eng 2004;32:1569-1579.
38. Huang TL, Lin GT, O'Connor S, Chen DY, Barmada R.Healing potential of experimental meniscal tears in the rabbit,freliminary results. Clin Orthop Relat Res 1991:299-305.
39. Roeddecker K, Nagelschmidt M, Koebke J, Guensche K. Me-niscal healing: A histological study in rabbits. Knee SurgSports Traumatol Arthrosc 1993;l:28-33.
40. Guisasola I, Vaquero J, Forriol F. Knee immobilization onmeniscal healing after suture: An experimental study in sheep.Clin Orthop Relat Res 2002:227-233.
41. King TV, Vallee BL. Neovascularisation of the meniscus withangiogenin. An experimental study in rabbits. J Bone JointSurg Br 1991;73:587-590.

1696 M. A. RUIZ-IB AN ET AL.
42. Burgos Flores J. The treatment of meniscal tears withoutmeniscal resection. Alcala de Henares: Universidad de Alcala,1986 (doctoral thesis in Spanish).
43. Zuk PA, Zhu M, Mizuno H, et al. Multilineage cells from humanadipose tissue: Implications for cell-based therapies. Tissue Eng2001:7:211-228.
44. Zuk PA, Zhu M, Ashjian P, et al. Human adipose tissue is asource of multipotent stem cells. Mol Biol Cell 2002;13:4279-4295.
45. Garcia-Olmo D, Herreros D, Pascual I, et al. Treatment ofenterocutaneous fistula in Crohn's disease with adipose-derived stem cells: A comparison of protocols with and with-out cell expansion. Int J Colorectal Dis 2009;24:27-30.
46. Plumas J, Chaperot L, Richard MJ, Molens JP, Bensa JC,Favrot MC. Mesenchymal stem cells induce apoptosis of ac-tivated T cells. Leukemia 2005;19:1604.
47. Puissant B, Barreau C, Bourin B, et al. Immunomodulatoryeffect of human adipose tissue-derived adult stem cells: Com-parison with bone marrow mesenchymal stem cells. Br JHaematol 2005;129:118-129.
48. Sonoda M, Harwood PL, Amiel ME, et al. The effects ofhyaluronan on tissue healing after meniscus injury and repairin a rabbit model. Am J Spans Med 2000;28:90-97.
49. Port J, Jackson DW, Lee TQ, Simon TM. Meniscal repairsupplemented with exogenous fibrin clot and autogenous cul-tured marrow cells in the goat model. Am J Spans Med1996:24:547-555.
50. Yamasaki T, Deie M, Shinomiya K, et al. Meniscal regen-eration using tissue engineering with a scaffold derivedfrom rat meniscus and mesenchymal stromal cells derivedfrom rat bone marrow. J Blamed Mater Res 2005:75:23-30.
51. Angele P, Johnstone B, Kujat R, et al. Stem cell based tissueengineering for meniscus repair. / Biomed Mater Res A 2008;85:445-455.
52. Agung M, Ochi M, Yanada S, et al. Mobilization of bonemarrow-derived mesenchymal stem cells into the injured tis-sues after intraatticular injection and their contribution totissue regeneration. Knee Surg Sports Traumatol Anhrosc2006:14:1307-1314.
53. Yagi H, Soto-Gutierrez A, Parekkadan B, et al. Mesenchymalstem cells: Mechanisms of immunomodulation and homing.Cell Transplant 2010:19:667-679.
54. Hamberg P, Gillquist J, Lysholm J. Suture of new and oldperipheral meniscus tears. J Bone Joint Surg Am 1983;65:193-197.
55. McCarty EC, Marx RG, DeHaven KB. Meniscus repair: Con-siderations in treatment and update of clinical results. ClinOnhop RelatRes 2002:122-134.
56. Nishida M, Higuchi H, Kobayashi K, Takagishi K. Histolog-ical and biochemical changes of experimental meniscus tear inthe dog knee. J Onhop Sci 2005;10:406-413.
57. Horibe S, Shino K, Nakata K, Maeda A, Nakamura N. Second-look arthroscopy after meniscal repair. J Bone Joint Surg Br1995:77:245-249.


















