



The Effect of Statins on Skeletal Muscle Function -...
23
DOI: 10.1161/CIRCULATIONAHA.112.136101 1 The Effect of Statins on Skeletal Muscle Function Running title: Parker et al.; Statins and Skeletal Muscle Beth A. Parker, PhD 1 ; Jeffrey A. Capizzi, MS 1 ; Adam S. Grimaldi, BS 1 ; Priscilla M. Clarkson, PhD 2 ; Stephanie M. Cole, PhD 2 ; Justin Keadle, BS 2 ; Stuart Chipkin, MD 2 ; Linda S. Pescatello, PhD 3 ; Kathleen Simpson, MS 3 ; C. Michael White, PharmD 3 ; Paul D. Thompson, MD 1 1 Division of Cardiology, Henry Low Heart Center, Hartford Hospital, Hartford, CT; 2 University of Massachusetts, Amherst, MA; 3 University of Connecticut, Storrs, CT Address for Correspondence: Paul D. Thompson, MD Director of Cardiology, Henry Low Heart Center Hartford Hospital Hartford, CT06102 Tel: 860-545-1793 Fax: 860-545-2882 E-mail: [email protected] Journal Subject Codes: [112] Lipids; [118] Cardiovascular Pharmacology PhD 2 ; Stephanie M. Cole, PhD 2 ; Justin Keadle, BS 2 ; Stuart Chipkin, MD 2 ; Lind da a a S. S. S. P P Pes es esca ca cate te tell ll llo, PhD 3 ; Kathleen Simpson, MS 3 ; C. Michael White, PharmD 3 ; Paul D. Thompson, M MD 1 1 1 1 1 Di Di Div vision o of f Ca Ca Card rd rdio iolo lo logy gy gy, He He H nr nr nry y y Lo Lo Low w w He He Hear ar rt t t Ce Ce C nt n e er er, Ha a art rt rtfo fo ford rd rd H H Ho o ospi pi pita ta t l, l, l, H H Hartf tf or or ord, d, d C C CT; T; 2 2 Un Un Univ iv iver r ersi s s ty of o o M M Ma a assa ach ch huset et tts ts, , Am Amhe he h r rs st, , MA A; A; 3 Un n niv ver er rsi sit ty ty o o of Co onn nn necticu cu cut, t, S S Sto o orr rs, C C CT T T by guest on May 4, 2018 http://circ.ahajournals.org/ Downloaded from
Transcript of The Effect of Statins on Skeletal Muscle Function -...

DOI: 10.1161/CIRCULATIONAHA.112.136101
1
The Effect of Statins on Skeletal Muscle Function
Running title: Parker et al.; Statins and Skeletal Muscle
Beth A. Parker, PhD1; Jeffrey A. Capizzi, MS1; Adam S. Grimaldi, BS1; Priscilla M. Clarkson,
PhD2; Stephanie M. Cole, PhD2; Justin Keadle, BS2; Stuart Chipkin, MD2; Linda S. Pescatello,
PhD3; Kathleen Simpson, MS3; C. Michael White, PharmD3; Paul D. Thompson, MD1
1Division of Cardiology, Henry Low Heart Center, Hartford Hospital, Hartford, CT; 2University
of Massachusetts, Amherst, MA; 3University of Connecticut, Storrs, CT
Address for Correspondence:
Paul D. Thompson, MD
Director of Cardiology, Henry Low Heart Center
Hartford Hospital
Hartford, CT06102
Tel: 860-545-1793
Fax: 860-545-2882
E-mail: [email protected]
Journal Subject Codes: [112] Lipids; [118] Cardiovascular Pharmacology
PhD2; Stephanie M. Cole, PhD2; Justin Keadle, BS2; Stuart Chipkin, MD2; Lindda a a S.S.S. PPPesesescacacatetetellllllo,
PhD3; Kathleen Simpson, MS3; C. Michael White, PharmD3; Paul D. Thompson, MMD111
11DiDiDivvision ooff f CaCaCardrdrdioiololologygygy,, HeHeH nrnrnry y y LoLoLow w w HeHeHeararrt t t CeCeC ntn eerer, Haaartrtrtfofofordrdrd HHHooospipipitatat l,l,l, HHHartftffororord,d,d CCCT;T; 22UnUnUniviviverrersiss ty
ofoo MMMaaassaachchhusetetttsts,, AmAmheheh rrsst,, MAA;A; 3Unnnivvererrsisittyty ooof f Coonnnnnecticucucut,t, SSStooorrrs, CCCTTT by guest on May 4, 2018
http://circ.ahajournals.org/D
ownloaded from

DOI: 10.1161/CIRCULATIONAHA.112.136101
2
Abstract:
Background—Many clinicians believe that statins cause muscle pain, but this has not been
observed in clinical trials and the effect of statins on muscle performance has not been carefully
studied.
Methods and Results—The Effect of STatins On Skeletal Muscle Function and Performance
(STOMP) study assessed symptoms and measured creatine kinase (CK), exercise capacity, and
muscle strength before and after atorvastatin 80 mg or placebo were administered for 6 months
to 420 healthy, statin-naive subjects. No individual CK value exceeded 10 times normal, but
average CK increased 20.8 ± 141.1 U/L (p<0.0001) with atorvastatin. There were no significant
changes in several measures of muscle strength or exercise capacity with atorvastatin, but more
atorvastatin than placebo subjects developed myalgia (19 vs 10; p = 0.05). Myalgic subjects on
atorvastatin or placebo decreased muscle strength in 5 of 14 and 4 of 14 variables respectively (p
= 0.69).
Conclusions—These results indicate that high-dose atorvastatin for 6 months does not decrease
average muscle strength or exercise performance in healthy, previously untreated subjects.
Nevertheless, this blinded, controlled trial confirms the undocumented impression that statins
increase muscle complaints. Atorvastatin also increased average CK suggesting that statins
produce mild muscle injury even among asymptomatic subjects. This increase in CK should
prompt studies examining the effects of more prolonged, high-dose statin treatment on muscular
performance.
Clinical Trial Registration Information—www.clinicaltrials.gov; Identifier: NCT00609063.
Key words: atorvastatin; statins; muscle strength; aerobic capacity; myalgia
average CK increased 20.8 ± 141.1 U/L (p<0.0001) with atorvastatin. There weree nnnoo o sisigngng ifificicanant
changes in several measures of muscle strength or exercise capacity withr atorvasstataatititinnn, bbbuttut mmmorroreee
atorvastatin than plp acebo subjects developed myayalggia (19 vs 10; p = 0.05)5 . Myalgic subjects on
atattororvvvastatini ooor plplp acacacebeboo dededecrcrcreaeaseseeddd mumum scsclele sstrtrenengtgthhh iinn 5 ofoff 11144 4 anndd d 4 4 ofof 1144 4 vvaririababblelelesss rerespsppececectitivevevelylyl (p
== 0.696 ).
Concnclulu isionons—T—Theesese resulults iindndicicate thhatat hhigigh-h-dodose aattororvavaststatatini fforor 66 mmononthhs s dodoes nnoto ddececrereasse e
avavereragagee mumuscsclele sstrtrenengtgthh oror eexexercrcisisee peperfrforormamanncece iinn hehealalththyy pprereviviououslslyy ununtrtreaeatetedd susubjbjecectsts
by guest on May 4, 2018
http://circ.ahajournals.org/D
ownloaded from
DOI: 10.1161/CIRCULATIONAHA.112.136101
3
Introduction
Hydroxy-methyl-glutaryl (HMG) CoA reductase inhibitors or statins are the most effective
medications for reducing elevated concentrations of low-density lipoprotein cholesterol (LDL-C)
and produce remarkable reductions in cardiovascular events.1Statins can produce life-threatening
rhabdomyolysis, but this is rare.2 Statins are more frequently associated with mild muscle
complaints including myalgia, cramps and weakness which may compromise medication
compliance and quality of life. The reported incidence of myalgia during statin therapy ranges
from 1% in controlled studies 3 to 25% 4 in clinical reports. Muscle weakness has also been
reported with statin therapy, but muscle and exercise performance have not been carefully
studied. 5
The Effect of STatins On Muscle Performance study (STOMP; NHLBI 5R01HL081893,
NCT00609063) determined the incidence of statin-associated muscle complaints and examined
the effect of statins on muscle performance and exercise capacity by administering atorvastatin
80 mg daily or placebo to healthy subjects for 6 months or until subjects developed myalgia.
Methods
Study overview
STOMP was a double-blind, random-assignment clinical trial whose methods have been
described.6 Equal numbers of men and women across three age ranges (20-39, 40-54, and 55+
yrs) were recruited over 4 years. Baseline lipid, liver, kidney, thyroid, and CK measurements
were obtained. Subjects completed a baseline muscle symptom questionnaire and exercise testing
including a maximal exercise test with gas analysis; handgrip, elbow flexor, and knee extensor
strength testing; and a knee extensor endurance exercise test. Subjects were then randomly
tudied. 5
The Effect of STatins On Muscle Performance study (STOMP; NHLBI 5R01HL081893,
NCNCCT0T0T00606060909090606063) dddeeteteermined the incidence of staatititin-n-aassociated mususscle cccomomomplaints and examined
hhhe eeffect of sttatatinii ss ononn mmmusussclclcle e peperfrfrfoorormmamannnce anannd exxxeeerciisesese ccaapapaacacitityy byby aadmdmdmininisisistteteriringngng aaatotorvrvvaasastataatiiin n
8000 mmmggg dadailily y y ooror ppplalacecec bboo ttto o hehealaa thththyyy sususubjbjececectststs ffforor 666 momomontn hhshs ooorr r ununntititil l susuubjbjbjececctss ddevevvelellopopopededed mmyyayalglgl iaiaa..
by guest on May 4, 2018
http://circ.ahajournals.org/D
ownloaded from

DOI: 10.1161/CIRCULATIONAHA.112.136101
4
assigned in a double-blind fashion to identical placebo or atorvastatin 80mg daily (Lipitor;
Pfizer, Inc., New York, NY). Atorvastatin tablets were crushed for compounding, but this does
not influence relative bioavailability of the statin (Medical Information Letter 337882; Pfizer,
Inc.) Subjects were called twice monthly to ascertain symptoms. Subjects performed repeat
testing after 6 months or after they developed muscle symptoms meeting the study definition of
statin-induced myalgia. The study was approved by the Institutional Review Boards at Hartford
Hospital, University of Massachusetts, and University of Connecticut and monitored by a Data
Safety and Monitoring Board.
Subject Inclusion / Exclusion Criteria
1,415 possible subjects were evaluated. Subjects were not included if they had cancer within 5
years, a baseline alanine aminotransferase (ALT) value > 2 times upper normal limits (UNL), a
creatinine> 2 mg/L, an abnormal thyroid stimulating hormone level, a history of cardiovascular
disease or an ischemic appearing electrocardiographic response to exercise testing, diabetes
mellitus, subjective muscle complaints or weakness, or physical disabilities that would prohibit
exercise testing. LDL-C was not an inclusion/exclusion criterion because many patients with
cardiovascular disease or other cardiovascular risk factors presently receive statin therapy
regardless of their baseline LDL values. Women who were pregnant or planned to become
pregnant were not recruited and all women in the study of child-bearing age agreed to use an
established method of birth control for the duration of the trial. Subjects presently or previously
treated with lipid-lowering medications were excluded, as were individuals treated with
medications known to affect skeletal muscle or to alter statin metabolism 7. Subjects with
hypertension were recruited if their blood pressure was controlled and <140/90 at baseline. A
total of 468 subjects were randomized to atorvastatin or placebo of whom 203 in the atorvastatin
1,415 possible subjects were evaluated. Subjects were not included if they had cacaancecec r wiwiwithththininin 55
years, a baseline alanine aminotransferase (ALT) value > 2 times upper normal limits (UNL), a
crreaeaatititininininenee>>> 222 mggg/L/L/L,, an abnormal thyroid stimulatatatiningg hormone levevev l, aa hhhiisistory of cardiovascular
ddidiseeeasa e or an isischchcheememicicic aaappppppeaeaeaririringng eeeleleectctroroocardrddiooograaapphhic rreesesppoponnsnse e toto eexexerrrciiisee teteteststininggg, dddiaiiabebeettetes s
memeelllll itititususu ,, , susuubjbjbjececttiivevee mmmusussclclee cocoompmpmplalalainiintstss ooorr r wweweakakakneneessss,, ooor r phphphyyysiciccalala ddisisisababa iiilitttieies s thththatata wwwoououlddd ppprorohhihibibiit t
exercise testiingngng.. LDLDLDL-L-L C CC wawawass nononot t t anana iiincncclulul sisisiononon///exexexclclc usususioioi n n n crcrcritititerere ioioion n n beeecacacausususeee mamam nynyny pppatatatieieientn s with
by guest on May 4, 2018
http://circ.ahajournals.org/D
ownloaded from
DOI: 10.1161/CIRCULATIONAHA.112.136101
5
and 214 in the placbo group provided complete data for analysis. Subjects were removed from
the study if their CK exceeded 10 times UNL on any occasion or if their ALT exceeded 3 times
UNL on two measurements performed within one week of the first elevated value. No subject
was excluded for elevated CK values, but 9 atorvastatin and 1 placebo subjects were excluded
for elevated ALT levels (Figure 1).
Serologic markers
Total, LDL and HDL cholesterol, triglycerides, ALT, creatinine, 25-hydroxy Vitamin D
(25(OH)D (which measures both vitamin D2 andD3)), and CK levels were obtained at baseline
and 6 months. Participants, their physicians and investigators were unaware of subjects’ lipid
values during the study.
Study Measurements
Body anthropometrics, handgrip isometric strength of the dominant hand, elbow and knee
extension/flexion isometric and isokinetic strength as well as knee endurance fatigue index 8 of
the dominant limb, maximal oxygen uptake (VO2max), resting and peak respiratory gas exchange
ratio (RER) and ventilatory threshold, as well as habitual self-reported and directly-measured
physical activity were measured at baseline and after 6 months of drug treatment as described.6
Compliance with study medications was assessed by pill counts of unused medication at 3
months and again at 6 months.
Myalgia/Muscle Symptoms
Muscle complaints were assessed at the baseline, 3 and 6 month visits and by phone twice
monthly using the Short-Form Brief Pain Inventory as described.6Subjects met the study
definition for “myalgia” if all of the following occurred: 1) They reported new or increased
muscle pain, cramps, or aching, unassociated with exercise; 2) Symptoms persisted for at least 2
values during the study.
Study Measurements
BoBodydydy aaa tntnthrhrhropopopommmetetetrirics, handgrip isometric strengnggthth of the dominaaantnn hhananndd,d, elbow and knee
exxteeensn ion/flexxioionnn iiisomommetettriririccc anananddd isissokokokininetetiic stttreeengtthh aas wwweelell l asas kknneeee enendudud rraancnccee fafatitiigugugue ee ininindededex x 88 ooof
hhe e e dododomimim nanaantntnt llimimmb,b,, mmaaxaximimi all oooxyxyygegegennn upupptataakekeke (VOVOVO2ma2ma2maxxx),), resesestititingngng aaanndnd pppeaeae kkk rereespspiriri atatatorory y y ggagass exxxchchaanangegeg
atio (RER)) anannd d d veveventntn ilillatattorry y y thththreeeshshshololld,dd aaas s wewewelllll aaass hhhabababitituauaal ll seseselflfl -r-rrepepeporrrteteted d d aaandndnd ddiririrececectltlt y-y-y memm asured
by guest on May 4, 2018
http://circ.ahajournals.org/D
ownloaded from

DOI: 10.1161/CIRCULATIONAHA.112.136101
6
weeks; 3) Symptoms resolved within 2 weeks of stopping the study drug; and 4) Symptoms
reoccurred within 4 weeks of restarting the study medication. Subjects who tested positive for
myalgia using these criteria subsequently performed repeat serological, muscle and aerobic
testing immediately after reoccurrence of muscle symptoms.
Sample Size
The primary outcome was the incidence of statin-associated myalgia, and thus sample size
estimates were based on the projection that 10% of the statin group would develop myalgia. 9
Assuming a nonspecific muscle complaint rate of 2% with placebo, 162 subjects per group were
needed to detect a significant difference between groups ( =0.05, power = 0.80). In addition,
groups of 200 subjects each provided power to detect a 5-10% change with statin therapy in all
exercise outcomes.
Statistical Analyses
Outcomes were assessed for normality using normal probability plots, histograms, and
Kolmogorov test statistics. Transformations were used as necessary. All tests were two-sided
with statistical significance set at alpha=0.05. Analyses were performed using SAS9.1 (SAS
Institute Inc., Cary, NC).
Primary analyses were carried out on an intent-to-treat basis. We also compared
outcomes excluding 23 subjects who did not reduce LDL-C by 20% or more on atorvastatin (to
exclude noncompliant subjects as denoted in the original published analysis plan) but this did not
alter main study findings and thus the following data include all completed subjects. To
determine the incidence of statin muscle complaints, the proportion of subjects developing
complaints was compared between the statin and placebo groups using a Pearson chi-square. The
effect of atorvastatin on serologic markers, muscle strength, and aerobic performance was
groups of 200 subjects each provided power to detect a 5-10% change with statininn ttheheh rraapypypy iiin n n alall
exercise outcomes.
Sttatatatisisistititicacaalll AnAnAnallysysyseses
OOOuttctcomes werree asasa sesessssseddd fffooror nnnorormmamalilil tytyy uuusinggg nnnormamamal prprroobobababbilillitityy plplotots,s hiistotoogrgrgramamss,s, aaandndnd
KoKoolmlmlmogogogororovovov ttesesttt ssttatatiisstiicscs.. TTTraransnsnsfofoformrmmatattioioionsnsns wwwerere eee uuuseeded aaasss nnenecececessssararry.y.y AlAlAll l teteeststs sss weweererere twwowo-s-sididdeddd
with statisticcalalal sisis gngngnififi iciccanana ceee sssetee aaat t t alalphphp a=a=a=0.0.0.050505.. AnAnAnalallysysyseses wwwererere ee pepeperfrfr ororrmememed d d usususinini g g g SASASAS9S9S9.1.1. (SAS
by guest on May 4, 2018
http://circ.ahajournals.org/D
ownloaded from

DOI: 10.1161/CIRCULATIONAHA.112.136101
7
assessed with t-tests (or a Mann-Whitney U test for CK) comparing the change scores observed
in the statin and placebo treated subjects pre-to-post treatment. Models were also run controlling
for sex and age as categorical covariates and random site effects, which did not alter findings.
Further models examined two-way and three-way interactions with ANOVA by modeling
change scores in study outcomes with age, gender and drug treatment, again controlling for
random site effects with non-significant interactions dropped for parsimony. Change scores
according to myalgia status were also examined between treatment groups given the small
number of myalgic subjects.
Results
Baseline Characteristics and Lipid Changes
Subjects randomized to the atorvastatin and placebo groups were similar at baseline, although
more women on atorvastatin used oral contraceptives or hormone therapy and more placebo
subjects used prescription pain medication (Table 1). Compliance with treatment medication was
similiar in the atorvastatin and placebo groups (94.5 ± 7.0 vs. 93.9±8.2 %). Atorvastatin subjects
showed the expected reductions in LDL-cholesterol (Table 2).
Changes in Serological Markers
Atorvastatin produced a 20.8 ± 141.1 U/L (p<0.0001) increase in CK, although no subject
demonstrated a CK value > 10 X the upper normal limit (UNL) (Figure 2). In addition, forty
subjects on atorvastatin vs. 29 subjects on placebo demonstrated CK > UNL (X2 = 3.2; p = 0.08).
Atorvastatin also increased average ALT values 15.7 ± 27.4 U/L (p< 0.0001) (Figure 2). There
was no effect of 6 months atorvastatin treatment on Vitamin D (atorvastatin: 35.1 ± 12.4 to 34.2
± 12.5 vs. placebo: 36.8 ± 14.6 to 35.1 ± 14.3 ng/mL; p = 0.94).
Results
Baseline Characteristics and Lipid Changes
Suubjbjbjececctststs rrrananandodd mimimizzezed d to the atorvastatin and placccebebe oo groups were e siss mimilalalarr r at baseline, although
mmorrere women oonn atttorrvavvaststtatatatininin uuusesed dd orororalal ccoontrrracccepttiivvees ororor hhoormmomonnne ttheheraraappyy aaandndnd mmooore ee plpllacaccebebebo oo
uubjbjbjececectstst uusesesed dd prpreeesccrcripippttioonon paiaiain n mememedidid cacaatitiononon (((Taaablblb eee 111).) CComomompplpliaiaiancnccee wiwiw ththh ttrereatatatmemementntt mmmedediicaatatioionnn wwwa
imiliar in thhe e e atatatororrvavavaststtatattinn aaandndnd ppplalalaceceeboboo gggrororoupupupsss (9(9(94.4.4.5 5 ±± 7.7.7.0 0 0 vsvsvs. 939393.9. ±8±8±8.2.2.2 %%%).).). AtAtAtorororvavavaststtata in subjectts
by guest on May 4, 2018
http://circ.ahajournals.org/D
ownloaded from

DOI: 10.1161/CIRCULATIONAHA.112.136101
8
Muscle Complaints
Twenty three atorvastatin and 14 placebo subjects reported new, unexplained muscle pain.
Nineteen atorvastatin and 10 placebo subjects ultimately met the study definition for myalgia (X2
= 3.74; p = 0.05). Myalgic subjects on atorvastatin reported predominantly leg symptoms: hip
flexor, quadriceps, hamstring and/or calf aches (n=10), quadriceps or calf cramps (n=5), and/or
quadriceps, hamstring and/or calf fatigue (n=6). whereas myalgic subjects on placebo reported
more diverse symptoms such as whole-body fatigue (n=3), worsening of pain in previous injuries
(n=3), groin pain (n=3) and foot cramping (n=1), but were otherwise similar (Table 1). Time to
symptom onset was shorter in atorvastatin myalgic subjects than in myalgic subjects on placebo
(35 ± 31 vs: 61 ± 33 days; p = 0.045). Myalgic vs. nonmyalgic subjects on atorvastatin or
placebo did not exhibit differences in CK, ALT, lipid (Table 2) or Vitamin D changes with
treatment (p > 0.19).
Pain severity and pain interference with daily life in all subjects with myalgia averaged
0.7 ± 1.2 and 0.3 ± 0.6 at baseline out of a possible 10 and increased to 2.4 ± 1.8 and to 2.0 ± 2.3
with treatment (p = 0.001) and did not differ between the atorvastatin and placebo subjects
(p=0.37). Baseline pain severity and pain interference with daily life were similar in non-
myalgic subjects for the atorvastatin and placebo groups(0.4 ± 0.9 and 0.2 ± 0.7, respectively)
and did not change with treatment (p =0.14).
Effects of Atorvastatin on Muscle and Exercise Performance
There were no baseline differences in measured strength and aerobic outcomes (all p >
0.06).There were no differential effects of atorvastatin on skeletal muscle strength and
endurance, aerobic performance, or physical activity levels compared to placebo (all p values >
0.17)(Table 3). Physical activity decreased (p = 0.007) regardless of drug treatment,but the
35 ± 31 vs: 61 ± 33 days; p = 0.045). Myalgic vs. nonmyalgic subjects on atorvvaaastataatit nn n ororor
placebo did not exhibit differences in CK, ALT, lipid (Table 2) or Vitamin D changes with
rreaeaatmtmtmeenenttt (p(p(p >>> 00.1.1199)9).
Pain seeveveeriiityy aaandndd pppaiaiainn n iininteteerfrfrfeereenencce wwwittth daaaiilly liliifefefe iinnn aalall l ssubbjbjececttsts wwwitithh h mmymyalalalgigigia a aavaveereragaggeddd
0..7 7 7 ±± 1.1.1 22 anannd d d 0.0.333 ±±± 0.0.666 aatat bbassselelininineee ouoout t ofofof aaa pppossssisis blblle 10100 aandndnd iincnccrerer asasa ededed ttooo 22.2.4 4 ±±± 1.1.1 8 8 ananandd totoo 222.0.0 ±±± 222.3
with treatmeentntnt (((p pp == 0.00 0000001)1) aaandndn dddididid nnnoto dddififffefefer r r bebebetwtwweeeeeen n n thhhe ee atatatororo vavavaststs atattininin ananandd d plplp acaccebebebooo sususubjb ects
by guest on May 4, 2018
http://circ.ahajournals.org/D
ownloaded from

DOI: 10.1161/CIRCULATIONAHA.112.136101
9
decrease in the atorvastatin group was due to a decrease in activity among the oldest tertile of
study participants (p = 0.03; Figure 3).
Outcomes in Individuals with Myalgia
One atorvastatin subject with myalgia refused final testing and was not included in analyses.
Compared to the asymptomatic subjects on atorvastatin, myalgic subjects had lower muscle
strength in 5 of 14 measured variables (Table 4). Compared to the asymptomatic subjects on
placebo, placebo myalgic subjects had significantly lower muscle strength in 4 measured
variables (X2 = 0.16; p = 0.68).
Discussion
STOMP is, to our knowledge, the first randomized double-blind, clinical trial to confirm the
common clinical impression that statins increase the incidence of myalgia. The definition of
myalgia in STOMP was predefined and required resolution of muscle symptoms promptly after
stopping study medication and reappearance of symptoms on restarting the medication. STOMP
also documented that statin-associated mild muscle complaints do not appear to have measurable
physiologic consequences in that muscle strength was not reduced to a greater extent in myalgic
participants on atorvastatin compared to placebo subjects also satisfying the study definition of
myalgia. The observation that some placebo patients satisfied the myalgia definition documents
the importance of using a double-blind trial to examine the incidence and characteristics of
statin-associated myalgia and not relying solely on clinical characteristics. STOMP also
demonstrated, we believe again for the first time, that. high-dose statin treatment increases
average CK levels, suggesting that statins produce low level muscle injury in healthy subjects
that occurs independent of muscle symptoms.
Discussion
STOMP is, to our knowledge, the first randomized double-blind, clinical trial to confirm the
coommmmmmoonon ccclililininin caal ll imimimpression that statins increaseee ththee incidence off mmyaalglglgiiaia. The definition of
mmyaalalgia in STOTOOMPMMP wwwasas pprereredededeffifineneedd anannd d requuuirrred rrreessoluuuttitiononn ooof f mmumuscsclele ssyymmptptptoomoms s prprp omomo ptpttlylyly aaaftteer
ttopopoppipipingngng sstututudyddy mmmededdicicaaatioioon n annnd d rerereapapappepeaararananancecece ooof f f sysyymmpmpttotomsmsms oon nn rerer ssstararartititingngg ttthehe mmmedede iciccatattiionnn. STSTOMOMOMP
also documenennteteted d d thththatata ssstatatatin-n-n asasa sooocicic atattedede mmmililild d d mumumuscscclelee cccomommplplplaiaiaintntntss s dodod nnnototot aaappppppeaeaear r tototo hhhavavaveee measurableee
by guest on May 4, 2018
http://circ.ahajournals.org/D
ownloaded from
DOI: 10.1161/CIRCULATIONAHA.112.136101
10
The reported incidence of myalgia during statin therapy has varied from 1% to 25%. 3, 10,
11 Determining the true incidence of mild muscle complaints from prior studies is difficult
because these complaints are typically not solicited and because most large trials typically define
myopathy as either myositis or rhabdomyolysis and require CK levels > 10 ULN. We used a
standardized study protocol and definition and observed that high-dose atorvastatin doubled the
incidence of reproducible muscle complaints, from 4.6 to 9.4% of subjects. STOMP enrolled
equal numbers of young, middle-aged and older men and women, but the incidence of myalgia
was similar to the 10.5% rate reported among 7,924 French patients.9 Observational reports
suggest that statin-associated muscle complaints are more frequent in older adults and/or
women.12-14 Subjects with statin myalgia in STOMP did tend to be older and almost 60% were
women, but the STOMP sample size was too small to detect gender differences in incidence.
Interestingly, the French study cited above 9 observed that muscle symptoms generally appeared
within a month of drug initiation. This was also true in STOMP, and the time to symptom onset
was significantly shorter in myalgic subjects on atorvastatin than on placebo, 1 vs. 2 months.
Clinical trials define statin-associated myopathy as CK levels > 10 ULN.4, 14 No subject
in STOMP recorded a CK > 10 ULN, but 6 months of treatment with atorvastatin resulted in a
small (~20 U/L) but significant (p<0.01) increase in CK. This suggests that low level muscle
injury occurs with high-dose statins, although there are other possible explanations for the CK
increase. Inflammatory conditions including rheumatoid arthritis and systemic lupus are
associated with reduced CK levels.15Statins reduce systemic inflammation 1 and could increase
average CK by decreasing inflammation. We did not measure inflammatory markers in STOMP
so cannot evaluate this possible relationship. Alternatively, hepatic macrophages participate in
the clearance of CK.16 Decreasing hepatic macrophages in animal models increases CK
women.12-14 Subjects with statin myalgia in STOMP did tend to be older and almmmosostt t 60600% % % wewewerere
women, but the STOMP sample size was too small to detect gender differences in incidence.
nnteteerererestststiininglglgly,y,y theee FFFrer nch study cited above 9 obssserere vved that muscle e e sympmpmpttotoms generally appeared
wwithhhini a monthth ooof drruugg iiinininitititiaatatioioion.n. TThThiiss wwwas alllso ttruruue innn SSTTOOMPMPM , aanand d ththt eee titimememe tto o sysys mpmpm toommm onoonsses t
wawaass s sisisigngngnifificicicaanantltlyyy sshshororrteter r r inin mmmyayayalglglgicicic ssuububjejejectctctss s ononon aaatotorrvaaastatatatititinn thththanann ooonn n plpllacccebebo,o,o, 111 vvss.s. 222 mmmonnnththsss.
Clinicicalala ttririialalals s dededefinenene ssstatatititin-n-n asasassooocicic atatatededed mmmyoyoyopapapaththy y y asasas CCCK K K leleleveveelslsl >>> 1110 0 0 ULULULN.N.N.444, 141414 NoN subject
by guest on May 4, 2018
http://circ.ahajournals.org/D
ownloaded from

DOI: 10.1161/CIRCULATIONAHA.112.136101
11
concentrations suggesting that statins, if they decrease hepatic macrophage content, could reduce
CK clearance and increase CK levels. There was no correlation between changes in CK and
ALT in STOMP, but we cannot further evaluate this possibility. Both explanations seem less
likely than the hypothesis that statins produce low-level muscle injury given the plethora of data
linking statins with skeletal muscle damage, 17-19even in the absence of muscle symptoms. 20
The long-term clinical consequences of this mild CK elevation are unclear, since the CK
elevation was not accompanied by changes in muscle strength. Anecdotally, some patients with
weakness attributed to statin therapy develop such complaints only after years of treatment.12
Therefore, it is possible that low-level muscle injury, indicated by mild elevations in CK, will
produce subsequent weakness in some statin-treated subjects. Testing this hypothesis will be
difficult since it requires a long-term placebo-controlled trial, an ethically difficult proposition
given the documented therapeutic value of statins. Also, such a study would require
sophisticated strength testing since we detected decreased strength among our myalgic subjects
even though few complained of muscle weakness.
There were no significant changes in muscle strength and endurance as well as aerobic
performance in the total atorvastatin STOMP population. Previous investigations have been
equivocal, with some studies suggesting that statins reduce muscle strength in older individuals
and that statins may shift exercise substrate utilization from fat to carbohydrate. 21-24Most studies
were small, used crude measures of strength and exercise performance and were not blinded or
placebo-controlled. 5 STOMP provides reassurance that healthy adults who tolerate high-dose
atorvastatin without muscle complaints experience no deleterious effects on muscle strength or
performance over 6 months of treatment. We did observe that average physical activity,
measured by accelerometer, decreased significantly in the oldest STOMP age group with
produce subsequent weakness in some statin-treated subjects. Testing this hypotothehhesisis ss wiwiwillllll bbbe e
difficult since it requires a long-term placebo-controlled trial, an ethically difficult proposition
gigiveveenn n thththee dododocccumememenntnted therapeutic value of statinnns.ss Also, such a sstutut dyy wwwooould require
oophphhisticated ststrereennngththh tesesestititingngng sssinincecee wwwee ddetecccteeed decececrreaasaseeded ssstrrenengggthhh amamononong g oouourr r mymyyalallgigigicc suuubbjbjeececttts
evvenenen ttthohoh ugugughh h ffefewww ccoompmpmplaaainineddd oofff mumumuscsclelee wwweaeaeaknnnesese sss.
Theree wwwererreee nonon ssigigi nininififiicacac ntntnt cchhhanana gegegess s ininn mmmusususclclle e e sts rereengngngththth aaandndnd enenndududurararancncnceee asass wwwelelelll l asasa aerobic
by guest on May 4, 2018
http://circ.ahajournals.org/D
ownloaded from

DOI: 10.1161/CIRCULATIONAHA.112.136101
12
atorvastatin therapy, but this could simply represent measurement variability since physical
activity increased in the youngest atorvastatin-treated subjects.
In contrast to the total study sample, statin-treated subjects meeting the study definition
of myalgia did demonstrate reductions in muscle strength in 5 of 14 measured muscle strength
variables (Table 4). Several observational studies have suggested that patients with myalgia
experience a decrease in strength.4, 25However, placebo group subjects also meeting the study
definition of myalgia also demonstrated muscle strength declines in 4 measured variables,
suggesting that the majority of muscle strength changes with myalgia in STOMP may have been
non-specific. Caution should be warranted in interpreting these data though as the analyses were
secondary to major study outcomes in a very small sample of patients. Therefore, larger studies
of patients with true statin myalgia—rigorously tested with a double-blind, randomized cross-
over period to confirm myalgia in the initial study population—are needed to determine the
effects of statin on muscle outcomes in myopathic patients.
STOMP has significant advantages over prior observational studies, but also limitations.
STOMP only examined the effect of atorvastatin on muscle complaints and function so cannot
evaluate if other statins at comparable doses would produce similar results. STOMP only
enrolled healthy individuals so cannot address the frequency or severity of muscular complaints
in patients with concomitant diseases and medications. The inclusion of younger subjects and
both genders may have reduced the number of subjects with myalgia during atorvastatin
treatment since subjects with statin myalgia in STOMP tended to be older and more were
woman. STOMP only lasted 6 months so may underestimate the incidence of myopathic
complaints during longer term statin therapy, although onset of myalgia with atorvastatin
occurred an average of one month after initiation of therapy. Longer placebo-controlled trials to
econdary to major study outcomes in a very small sample of patients. Therefore,e,, llarara gegeger r stststudududieies
of patients with true statin myalgia—rigorously tested with a double-blind, randomized cross-
ovvererer pppeererioioiod d d tototo conononfifif rm myalgia in the initial studddyyy pppopulation—aarerer neeeeedededed to determine the
efffeeectc s of statiin n ononon mmuuusclclcleee ouououtctctcomommesess innn mmmyooopaaathiccc pppatiiienenntsts..
STSTOMOMOMP P hahaas s sisiigngnnififici ananant t adadadvavavantntagagageseses oooveveer r r pppriioor obobobseseserrvrvatatatioioonanaalll ststs uududiiieses, bububut t alallsosoo limimmiititatatiioionnsns.
STOMP onlylyy eeexaxax mimiminenened d d thhe e e efefeffeeectctct ooof f f atttororo vavavastststatata inini ooon n mumuuscscs lelele cccomomomplplaiaiaintntnts s snnn ananand d d fufuuncncnctititiononon sso cannot
by guest on May 4, 2018
http://circ.ahajournals.org/D
ownloaded from

DOI: 10.1161/CIRCULATIONAHA.112.136101
13
examine the frequency of myopathic complaints in sicker subjects will be difficult, however,
given the general reluctance to assign statin-eligible subjects to placebo treatment. On the other
hand, given that statins have been clinically available and widely used in the US since 1987 and
the paucity of documented decreases in muscle strength among statin-treated patients, STOMP
may overestimate the frequency and strength changes of statin-associated myalgia. This seems
unlikely, however, given the rigor of the STOMP design.
Summary
STOMP is, to our knowledge, the first randomly assigned, double-blind study designed to
examine the effects of statins on muscular complaints, muscle strength and exercise
performance. The results are reassuring since there was no effect of atorvastatin 80 mg daily on
muscle strength or exercise performance over 6 months of treatment in healthy subjects. On the
other hand, STOMP did document that atorvastatin significantly increased the frequency of
myalgia. STOMP also demonstrated an increase in average CK in the atorvastatin-treated cohort
suggesting that statins could produce low level muscle injury. These results should prompt
additional studies examining muscular performance with long term statin treatment in both
healthy patients as well as those with confirmed statin-associated myalgia.
Acknowledgments: The authors wish to acknowledge the following individuals for their
participation on the Data Safety Monitoring Board: JoAnne Foody, M.D., Pamela Hartigan,
Ph.D., and Ira Ockene, M.D. (chair). In addition, Gualberto Ruano, M.D., Ph.D. provided
statistical and scientific assistance with data interpretation.
Funding Sources: The STOMP study is funded by NHLBI/NIH grant RO1 HL081893 (P.
Thompson).
examine the effects of statins on muscular complaints, muscle strength and exercrcisiise ee
performance. The results are reassuring since there was no effect of atorvastatin 80 mg daily on
mumuscscsclelele sstrtrtrenene gggth ororor eexercise performance over 6 mmmoonnths of treatmemeent iin n n hhehealthy subjects. On the
otheeer r hand, STTOMOMOMP P didid d d dododocucuummementntnt ttthahatt aaatorvvavastatinin sigggnninifificccanntntlylyy inncncrereaaaseeded ttthehehe ffrereequququenencycyy oofff
mymyyalalalgigigia.a. SSTOTOTOMPMPP aaalslsooo ddedemomonnsn trtrtratatatededed aannn ininincrcrcreaaaseses iiinn aavveeraraagegege CCCK K K inini tttheheh aaatooorvrvaasastatatatitinn-n-ttrtreaaateted d d cocoohohoortr
uggesting thahaat t t ststatatatininins s s cococ ululld d d prpp odododucucuceee looow w w lelelevevevel l mumumuscscclele iiinjnjn ururury.y.y ThThThessse ee rereresususultltltsss shshhouououldldld pppror mpt
by guest on May 4, 2018
http://circ.ahajournals.org/D
ownloaded from

DOI: 10.1161/CIRCULATIONAHA.112.136101
14
Conflict of Interest Disclosures: Paul D. Thompson reports receiving research grants from the
National Institutes of Health, GlaxoSmithKline, Anthera, B. Braun, Genomas, Roche, Aventis,
Novartis, and Furiex; serving as a consultant for Astra Zenica, Furiex, Regeneron, Merck,
Roche, Genomas, Abbott, Lupin, Runners World, Genzyme, Sanolfi, Pfizer, and
GlaxoSmithKline; receiving speaker honoraria from Merck, Pfizer, Abbott, Astra Zenica,
GlaxoSmithKline, and Kowa: owing stock in General Electric, JA Wiley Publishing, J&J,
Sanolfi-Aventis and Abbott; and serving as a medical legal consultant on cardiac complications
of exercise, statin myopathy, tobacco, ezetimibe and non-steroidals.
References: 1. Ridker PM, Danielson E, Fonseca FA, Genest J, Gotto AM Jr, Kastelein JJ, Koenig W, Libby P, Lorenzatti AJ, MacFadyen JG, Nordestgaard BG, Shepherd J, Willerson JT, Glynn RJ.Rosuvastatin to prevent vascular events in men and women with elevated C-reactive protein. N Engl J Med. 2008;359:2195-2207. 2. Staffa JA, Chang J, Green L. Cerivastatin and reports of fatal rhabdomyolysis. N Engl J Med. 2002;346:539-540. 3. Physicians' Desk Reference. 2002. Montvale, NJ, Medical Economics. p56. 4. Phillips PS, Haas RH, Bannykh S, Hathaway S, Gray NL, Kimura BJ, Vladutiu GD, England JD. Statin-associated myopathy with normal creatine kinase levels. Ann Intern Med. 2002;137:581-585. 5. Krishnan GM, Thompson PD. The effects of statins on skeletal muscle strength and exercise performance. Curr Opin Lipidol. 2010;21:324-328.
6. Thompson PD, Parker BA, Clarkson PM, Pescatello LS, White CM, Grimaldi AS, Levine BD, Haller RG, Hoffman EP. A randomized clinical trial to assess the effect of statins on skeletal muscle function and performance: rationale and study design. Prev Cardiol. 2010;13:104-111. 7. Thompson PD, Clarkson P, Karas RH. Statin-associated myopathy. JAMA. 2003;289:1681-1690. 8. Katsiaras A, Newman AB, Kriska A, Brach J, Krishnaswami S, Feingold E, Kritchevsky SB, Li R, Harris TB, Schwartz A, Goodpaster BH.Skeletal muscle fatigue, strength, and quality in the elderly: the Health ABC Study. J Appl Physiol. 2005;99:210-216. 9. Bruckert E, Hayem G, Dejager S, Yau C, Begaud B. Mild to moderate muscular symptoms with high-dosage statin therapy in hyperlipidemic patients--the PRIMO study. Cardiovasc Drugs Ther. 2005;19:403-414.
RJ.Rosuvastatin to prevent vascular events in men and women with elevated C-reeacacctitit veve ppproroteteinin.N Engl J Med. 2008;359:2195-2207.
2. Staffa JA, Chang J, Green L. Cerivastatin and reports of fatal rhabdomyolysis. N Engl J Med. 2002;3;346:53939-540.
3.3. PPhhyhysicianns's's' DDesessk kk ReReefefef rererencncn e.e. 2220000002.2. MMonontvtvalale,e, NNNJJ, MMededdicicicalala EEcococonnonomimicscscs.. p556.6.
4.4.. PPhhillips PSPS, ,, HHaaaaas RRH,H, Baannnnynykhk SSS, , HaHaHathawwwaaay SS, GrGrayayay NNNL,LL Kimmmuuura BBBJ,,, VVllaaddutu iuu GGGD,D, EEEnglllannnd JDDD. StStStatata inin-a-aasssssocociiiatteted d mymymyopopatatthyhyhy wwwititithhh nnnororrmamamall crcrcreaeae tttinnene kkkininnasasasee leleleveveelsss.. AnAnAnnn IInInteteernrnrn MMMededed. 200202;1;13737:5:5818 -5-5855.
55 KKririshshnanann GMGM ThThomompspsonon PPDD TThehe eeffffecectsts ooff ststaatitinsns oonn skskeleletetalal mmususclclee ststrerengngthth aandnd eexexercrcisisee
by guest on May 4, 2018
http://circ.ahajournals.org/D
ownloaded from

DOI: 10.1161/CIRCULATIONAHA.112.136101
15
10. Phillips PS, Haas RH. Observations from a statin myopathy clinic. Arch Intern Med. 2006;166:1232-1233. 11. El-Salem K, Ababneh B, Rudnicki S, Malkawi A, AlrefaiA, Khader Y, Saadeh R, Saydam M. Prevalence and risk factors of muscle complications secondary to statins. Muscle Nerve. 2011;44:877-881. 12. Cham S, Evans MA, Denenberg JO, Golomb BA. Statin-associated muscle-related adverse effects: a case series of 354 patients. Pharmacotherapy. 2010;30:541-553.
13. Pasternak RC, Smith SC, Jr., Bairey-Merz CN, Grundy SM, Cleeman JI, Lenfant C. ACC/AHA/NHLBI clinical advisory on the use and safety of statins. J Am Coll Cardiol. 2002;40:567-572. 14. Maningat P, Breslow JL. Needed: pragmatic clinical trials for statin-intolerant patients. NEngl J Med. 2011;365:2250-2251.
15. Lee YH, Choi SJ, Ji JD, Song GG. Serum creatine kinase in patients with rheumatic diseases. Clin Rheumatol.2000;19:296-300. 16. Radi ZA, Koza-Taylor PH, Bell RR, Obert LA, Runnels HA, Beebe JS, Lawton MP, Sadis S. Increased serum enzyme levels associated with kupffer cell reduction with no signs of hepatic or skeletal muscle injury. Am J Pathol. 2011;179:240-247. 17. Hanai J, Cao P, Tanksale P, Imamura S, Koshimizu E, Zhao J, Kishi S, Yamashita M, Phillips PS, Sukhatme VP, Lecker SH. The muscle-specific ubiquitin ligase atrogin-1/MAFbx mediates statin-induced muscle toxicity. J Clin Invest. 2007;117:3940-3951. 18. Urso ML, Clarkson PM, Hittel D, Hoffman EP, Thompson PD. Changes in ubiquitin proteasome pathway gene expression in skeletal muscle with exercise and statins. ArteriosclerThromb Vasc Biol. 2005; 25:2560-2566. 19. Parker BA, Augeri AL, Capizzi JA, Ballard KD, Troyanos C, Baggish AL, D'Hemecourt PA, Thompson PD.Effect of statins on creatine kinase levels before and after a marathon run. Am J Cardiol. 2012;109:282-287. 20. Mohaupt MG, Karas RH, Babiychuk EB, Sanchez-Freire V, Monastyrskaya K, Iyer L,Hoppeler H, Breil F, Draeger A. Association between statin-associated myopathy and skeletal muscle damage. CMAJ.2009;18:E11-E18. 21. Paolisso G, Barbagallo M, Petrella G, Ragno E, Barbieri M, Giordano M, Varricchio M. Effects of simvastatin and atorvastatin administration on insulin resistance and respiratory quotient in aged dyslipidemic non-insulin dependent diabetic patients. Atherosclerosis. 2000;150:121-127. 22. Phillips PS, Phillips CT, Sullivan MJ, Naviaux RK, Haas RH. Statin myotoxicity is
15. Lee YH, Choi SJ, Ji JD, Song GG. Serum creatine kinase in patients with rheuumamamatiticc didiseseasasesClin Rheumatol.2000;19:296-300.
16. Radi ZA, Koza-Taylor PH, Bell RR, Obert LA, Runnels HA, Beebe JS, Lawton MP, Sadis Sncreased serum enzyme levels associated with kupfp fer cell reduction with no signs of hepatic orkkelelletetetalalal mmmususu cccle inininjjujury. Am J Pathol. 2011;179:22244040---247.
1177. HHanai J, CCaoao PPP, TaTaTanknkksasaalelele PPP,, ImImmaamamururaa S,, KKKoshhhimmmizuzuu EE,, ZhZhZhaoao J,, KiKiishshshii S,S, YYYamamasasashihihitata MMM,PhPhPhillllil ps PS, SSukhahahatmeee VVVP, LeLeLeckc ere SSSH.H. TTThe mmmuscllele-s-spepeecicicififificcc uuubiqqquuiitin llliggagasesee aaatrtrogiinin--1-1//MMAAFbxbxbx memeedididiatatateses sstatatatititin-n-iinndduduceceed d mumuscscclele tttoxoxoxiicicititty.y.y JJ J CCClininn IInnnveesestt.. 202020070707;11117171 :3:39494940-0--399951511..
18. Urso ML,L, CCClalarkrkrksososon n n PMPMM,,, HiHiH ttttttelele DDD, HoHoHofffff mamamannn EEEP,P,P, TTThohoompmpmpsososon n n PDPDP .. . ChChChananangegegess ininn uuubibibiquququiti in prprototeaeasosomeme ppatathwhwayay ggenenee exexprpresessisionon iinn skskeleletetalal mmususclclee wiwithth eexexercrcisisee anandd ststatatininss ArArteteririososclclerer
by guest on May 4, 2018
http://circ.ahajournals.org/D
ownloaded from

DOI: 10.1161/CIRCULATIONAHA.112.136101
16
associated with changes in the cardiopulmonary function. Atherosclerosis. 2004;177:183-188. 23. Mullen PJ, Zahno A, Lindinger P, Maseneni S, Felser A, Krähenbühl S, Brecht K. Susceptibility to simvastatin-induced toxicity is partly determined by mitochondrial respiration and phosphorylation state of Akt. Biochim Biophys Acta.2011;1813:2079-2087. 24. Wu JS, Buettner C, Smithline H, Ngo LH, Greenman RL. Evaluation of skeletal muscle during calf exercise by 31-phosphorus magnetic resonance spectroscopy in patients on statin medications. Muscle Nerve. 2011;43:76-81. 25. Dobkin BH. Underappreciated statin-induced myopathic weakness causes disability. Neurorehabil Neural Repair. 2005;19:259-263.
Table 1. Subject Baseline Characteristics And Medication Use By Drug Assignment For All Subjects and Those Who Developed Myalgia
Entire Sample Myalgic Sample ATOR (n=203) PL (n=217) ATOR (n=19) PL (n=10)
Women (n) 103 113 11 5 Caucasian (n) 92 201 18 10 Age (years) 43.6(41.4,45.8) 44.6(42.4,46.8) 52.5(47.1,50.9)* 56.9±8.0
(51.9,61.9)* BMI (kg/m2) 26.3(25.6,27.0) 26.5(25.8,27.2) 24.7(22.8,26.6) 25.0±3.0(23.1,26.9)VO2max (mL/kg/min)
34.6(33.3,35.9) 33.2(31.9,34.5) 31.0(26.7,35.3) 30.7(26.0,35.4)
Resting SBP (mmHg)
119.5(117.7,121.3) 118.3(116.5,120.1) 122.3(117.4,127.2) 119.0(112.7,125.3)
Resting DBP (mmHg)
75.5(74.2,76.8) 75.1(73.8,76.4) 76.4(73.2,79.6) 72.6(68.9,76.3)
Total-C (mg/dL) 198.7(193.3,204.1) 194.8(189.9,199.7) 215.3(195.9,234.7) 212.0(195.6,228.4)LDL-C (mg/dL) 119.0(114.1,123.9) 116.0(111.8,120.2) 128.9(110.8,147.0) 130.2(116.1,144.3)HDL-C (mg/dL) 57.6(55.2,60.0) 58.6(56.3,60.9) 68.7(61.5,75.9)* 61.0(53.2,68.8) TRIG (mg/dL) 110.5(102.9,118.1) 103.1(95.7,110.5) 88.1(72.4,103.8) 114.2(73.5,154.9) Medication OTC Pain (n) 21 21 3 2 Prescription Pain (n)
5 16* 2 2
Blood Pressure (n) 9 15 2 0 Thyroid (n) 12 13 4 2 Hormone Therapy (n)
31 18* 2 0
Data are presented as point estimates and 95% confidence intervals for atorvastatin (ATOR) vs. placebo (PL) subjects in the entire sample and only in subjects classified as myalgic. BMI = body mass index; VO2max = maximal oxygen uptake; SBP = systolic blood pressure; DBP = diastolic blood pressure; C = cholesterol; LDL = low density lipoprotein; HDL = high density lipoprotein; TRIG = triglycerides. OTC Pain = regular use of over-the-counter pain medications such as nonsteroidal anti-inflammatory drugs and acetaminophen; Prescription Pain = regular use of prescription pain medications; Blood Pressure = used a blood-pressure lowering drug; Thyroid = used a synthetic thyroid drug; hormone therapy = if female, used oral contraceptives or hormone replacement therapy. * indicates significant difference between myalgic and nonmyalgic subjects within a treatment group at p < 0.05.
Entire Sample Myalgic Saampmpmplele ATOR (n=203) PL (n=217) ATOR (n=19) PLPLL (((n=n=n=101010) )
Women (n) 103 113 11 555Caucasian (n) 92 201 18 10 Age (years) 43.6(41.4,45.8) 44.6(42.4,46.8) 52.5(47.1,50.9)* 56.9±8.0
(51.9,61.9)* BMBMMI I (k(kgg/mm22) ) 2626.33(2(25.6,6,2727.0. ) ) 262 .5.5(2(2555.88,27.22)) 24244.7.7(2( 2.2.8,8,2626.6) ) 2525.0.0±33.00(2(23.1,,2626.9VVOVO22m2maxmmmLL/L/kgk /min)
33434.6.6.6(3(3(33.3..3,3,3,353535.9.99)) ) 33333 .22.2(3311.99,344 5.5.5))) 313131.00(2(2(26.6.6 77,7,335.33)) ) 303030.7.77(2(2(26.6.0,0,0,353535.4.4.4)
ReReesttinini g g SBP mmmHmHmHg)g)g)
1119..5(5(11177.77,7,121...3)3)3 11888.333(1( 1666.55,11202020.1.1) ) 11222.3((117..4,4,1212777.2)2)2) 11999.0.00(111222.7,1,12555.3)
ReReststiningg g DBDBPP mmHg)
7575.5.5(7(7( 4.4.2,2,,7676.8.8)) ) 7575.1.1(7(7( 3.3.8,8,,7676.4.4))) 7676.4.4(7(7( 3.3.2,2,,7979.6.6)) ) 7272.6.6(6(6( 8.8.9,9,,7676.3.3)) )
TTottall CC ((m /g/dLdL)) 191988 7(7(191933 33 202044 1)1) 119494 88(1(18989 99 119999 77)) 212155 3(3(191955 99 232344 7)7) 221212 00(1(19595 66 222828 44)
by guest on May 4, 2018
http://circ.ahajournals.org/D
ownloaded from
DOI: 10.1161/CIRCULATIONAHA.112.136101
17
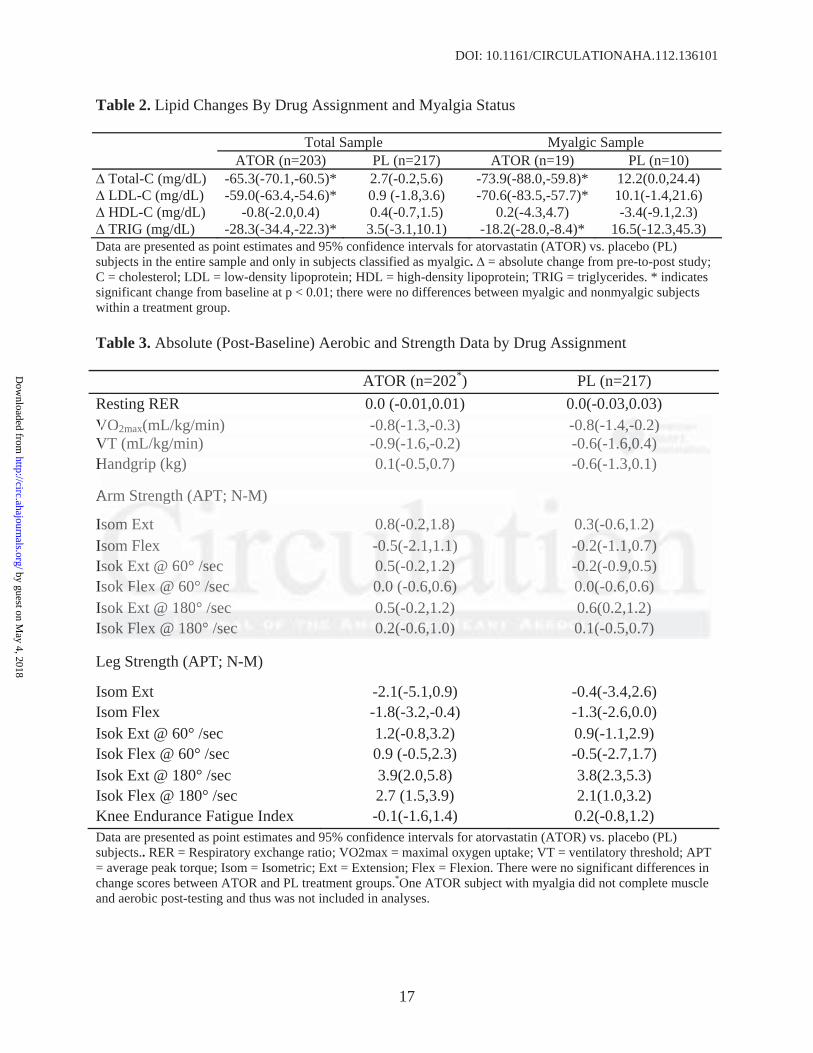
Table 2. Lipid Changes By Drug Assignment and Myalgia Status
Total Sample Myalgic Sample ATOR (n=203) PL (n=217) ATOR (n=19) PL (n=10)
Total-C (mg/dL) -65.3(-70.1,-60.5)* 2.7(-0.2,5.6) -73.9(-88.0,-59.8)* 12.2(0.0,24.4) LDL-C (mg/dL) -59.0(-63.4,-54.6)* 0.9 (-1.8,3.6) -70.6(-83.5,-57.7)* 10.1(-1.4,21.6) HDL-C (mg/dL) -0.8(-2.0,0.4) 0.4(-0.7,1.5) 0.2(-4.3,4.7) -3.4(-9.1,2.3) TRIG (mg/dL) -28.3(-34.4,-22.3)* 3.5(-3.1,10.1) -18.2(-28.0,-8.4)* 16.5(-12.3,45.3)
Data are presented as point estimates and 95% confidence intervals for atorvastatin (ATOR) vs. placebo (PL) subjects in the entire sample and only in subjects classified as myalgic. = absolute change from pre-to-post study; C = cholesterol; LDL = low-density lipoprotein; HDL = high-density lipoprotein; TRIG = triglycerides. * indicates significant change from baseline at p < 0.01; there were no differences between myalgic and nonmyalgic subjects within a treatment group.
Table 3. Absolute (Post-Baseline) Aerobic and Strength Data by Drug Assignment
ATOR (n=202*) PL (n=217) Resting RER 0.0 (-0.01,0.01) 0.0(-0.03,0.03) VO2max(mL/kg/min) -0.8(-1.3,-0.3) -0.8(-1.4,-0.2) VT (mL/kg/min) -0.9(-1.6,-0.2) -0.6(-1.6,0.4) Handgrip (kg) 0.1(-0.5,0.7) -0.6(-1.3,0.1)
Arm Strength (APT; N-M)
Isom Ext 0.8(-0.2,1.8) 0.3(-0.6,1.2) Isom Flex -0.5(-2.1,1.1) -0.2(-1.1,0.7) Isok Ext @ 60° /sec 0.5(-0.2,1.2) -0.2(-0.9,0.5) Isok Flex @ 60° /sec 0.0 (-0.6,0.6) 0.0(-0.6,0.6) Isok Ext @ 180° /sec 0.5(-0.2,1.2) 0.6(0.2,1.2) Isok Flex @ 180° /sec 0.2(-0.6,1.0) 0.1(-0.5,0.7)
Leg Strength (APT; N-M)
Isom Ext -2.1(-5.1,0.9) -0.4(-3.4,2.6) Isom Flex -1.8(-3.2,-0.4) -1.3(-2.6,0.0) Isok Ext @ 60° /sec 1.2(-0.8,3.2) 0.9(-1.1,2.9) Isok Flex @ 60° /sec 0.9 (-0.5,2.3) -0.5(-2.7,1.7) Isok Ext @ 180° /sec 3.9(2.0,5.8) 3.8(2.3,5.3) Isok Flex @ 180° /sec 2.7 (1.5,3.9) 2.1(1.0,3.2) Knee Endurance Fatigue Index -0.1(-1.6,1.4) 0.2(-0.8,1.2) Data are presented as point estimates and 95% confidence intervals for atorvastatin (ATOR) vs. placebo (PL) subjects.. RER = Respiratory exchange ratio; VO2max = maximal oxygen uptake; VT = ventilatory threshold; APT = average peak torque; Isom = Isometric; Ext = Extension; Flex = Flexion. There were no significant differences in change scores between ATOR and PL treatment groups.*One ATOR subject with myalgia did not complete muscle and aerobic post-testing and thus was not included in analyses.
VO2max(mL/kg/min) -0.8(-1.3,-0.3) -0.8(-1.1..44,4,-0-00.2.2.2)) ) VT (mL/kg/min) -0.9(-1.6,-0.2) -0.6(-11-1.6.6.6,0,0,0.4.4.4) ) )Handgrip (kg) 0.1(-0.5,0.7) -0.6(-1.3,0.1)
Arm m StStrerengngthth (APAPAPT;T N-M)
ssomomom EExt 00.8.8(-(-000.222,1.8)8)) 00.3.3(-(-( 0.0.6,6,1.1.2)2)) ssommm Flex ---0..5(-222.11,1...11)1) --0.0.0.22(2(-1-11.1.1.1,0,0,0.7.7.7) sssokokk Ext @ 660°00 ///seeec 0.0.55(-000.222,1,1.2.22))) --0-0.22. (-( 0.9,9,0.0.555) ssokokok FFFlelelexxx @ @ @ 60600°° /s/ssececec 000.0.00 ((-0-0-0.6.66,0,0,0.6.6.6) ) ) 0.0.0 0(0(0(-0-0-0.6.6.6,0,0.6.6.6) ))sssokokok EEExtxtxt @@@ 111808080° /s/s/sececec 000 55.5(-(-( 000.222,111.2)2)2) 000 66.6(0(0(0 22.2 11,1 22.2))) sok Flex @ @ 1818180°00° ///seseec cc 000.2(2(2(-00-0.666,11,1.00))) 000.1(1(1(-0-00 55.5 0,0,0.7) )
by guest on May 4, 2018
http://circ.ahajournals.org/D
ownloaded from

DOI: 10.1161/CIRCULATIONAHA.112.136101
18
Table 4. Absolute (Post-Baseline) Aerobic and Strength Data by Drug Assignment in Myalgic Patients. ATOR (n=18*) PL (n=10) Resting RER 0.0(-0.05,0.05) 0.1(-0.1,0.3) VO2max(mL/kg/min) -0.5(-1.3,0.3) -1.3(-2.8,0.2) VT (mL/kg/min) -2.1(-3.9,0.3) -2.3(-5.9,1.3) Handgrip (kg) -1.4(-3.4,0.6) -1.0(-3.7,1.7)
Arm Strength (APT; N-M)
Isom Ext -0.4(-4.2,3.4) 1.1(-2.4,4.6) Isom Flex -3.2(-7.5,1.1) 0.7(-3.6,5.0) Isok Ext @ 60° /sec -2.6 (-6.2,1.0) 0.3(-1.9,2.5) Isok Flex @ 60° /sec -3.8(-7.8,0.2)* 0.8(-1.2,2.8) Isok Ext @ 180° /sec -1.3(-4.4,1.8) -0.4(-2.2,1.4)* Isok Flex @ 180° /sec -0.5(-4.1,3.1) 0.2(-2.2,3.6)
Leg Strength (APT; N-M)
Isom Ext -17.3 ± (-25.1,-9.5)* -21.5(-30.6,-12.4)* Isom Flex -5.3(-10.4,-0.2) -4.3(-10.2,1.6) Isok Ext @ 60° /sec -10.4(-20.2,-0.6)* -6.6(-14.5,1.3) Isok Flex @ 60° /sec -3.6(-8.6,1.4)* -4.6(-8.7,-0.5) Isok Ext @ 180° /sec -3.0(-8.9,2.9)* -4.1(-10.1,1.9)* Isok Flex @ 180° /sec -1.0(-4.6,2.6) -3.9(-6.8,-1.0)* Knee Endurance Fatigue Index -2.1(-4.4,0.2) -3.6(-5.7,-1.5) Data are presented as point estimates and 95% confidence intervals for atorvastatin (ATOR) vs. placebo (PL) subjects in subjects classified as myalgic. RER = Respiratory exchange ratio; VO2max = maximal oxygen uptake; VT = ventilatory threshold; APT = average peak torque; Isom = Isometric; Ext = Extension; Flex = Flexion.* indicates significant difference in change scores between myalgic and nonmyalgicgroups (from Table 3) within a treatment group at p < 0.05. 1One ATOR subject with myalgia did not complete muscle and aerobic post-testing and thus was not included in analyses.
Figure Legends:
Figure 1.Study flow diagram detailing numbers (n) of participants who were screened,
randomized, completed and analyzed in the study.
@ ( , ) ( , ))
Leg Strength (APT; N-M)
som Ext -17.3 ± (-25.1,-9.5)* -21.5(-30.6,-12.4)* somm FFlelelex xx -5.3(-100.4.44,-, 0.2) -4.3(-10.2,1.6)ssokokok EEExxt @@@ 66600° //sesec c -10.4((-20.0.2,-0.6)*) -6.6(-( 14.5,1.3))sssokkk Flex @ @ 60600°°° s/s/seccc -333.6.6. (-(-( 8.8 666,11.4)))*** -444.6.6.6(-((-8.8.8 7,7,7,-0-00.5.5.5))sssokkk Ext @ 180°° /sssec -3..0(((-8.999,222.9))** -444.11(-10...1,,11.999)** ssokoko FFFlelex @ @ @ 1811800°° ///sesecc -1-11.00(-(-( 4.4.6,6,22.666) -3-33.9.9(-(-( 6.6.8,8,8,--1-1.000)***
Kneeee EEE dndndururanncece FFatatigiguee IIndndexex --2.2.1(1(-4-4 4.4 0,0 2.2)) -3-3.66(-((-555.7,-1-1 5.5))Data are presentntededed aass popopoininntt t esee timamam tetetes ananandd d 959595% % cococonfnfn idididenenencecec iiintntntererervav lslss fffororor aaatotoorvrvrvasasa taaatititin n n (A(A(ATOTOTOR)R)R vvvs.s. ppplalalacececebob (PL) uubjbjecectsts iinn susubjbjecectsts cclalassssififieiedd asas mmyayalglgicic. RERERR == ReRespspiriratatororyy exexchchanangege rratatioio;; VOVO2m2maxax == mmaxaximimalal ooxyxygegenn upuptatakeke;;
by guest on May 4, 2018
http://circ.ahajournals.org/D
ownloaded from

DOI: 10.1161/CIRCULATIONAHA.112.136101
19
Figure 2.Group mean ± SD of creatine kinase (CK; top) and alanine aminotransferase (ALT;
bottom) before (Pre) and after (Post) 6 months of atorvastatin (ATOR) or placebo (PL) treatment
with brackets indicating the p value for group-by-time interaction. *Significant difference
between groups within a timepoint at p <0.05.
Figure 3.Group mean ± SD of changes in physical activity (average counts/day) by age group
after 6 months of atorvastatin (ATOR) or placebo (PL) treatment with brackets indicating the p
value for treatment-by-age interaction.
by guest on May 4, 2018
http://circ.ahajournals.org/D
ownloaded from

ThompsonJustin Keadle, Stuart Chipkin, Linda S. Pescatello, Kathleen Simpson, C. Michael White and Paul D.
Beth A. Parker, Jeffrey A. Capizzi, Adam S. Grimaldi, Priscilla M. Clarkson, Stephanie M. Cole,The Effect of Statins on Skeletal Muscle Function
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 2012 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation published online November 26, 2012;Circulation.
http://circ.ahajournals.org/content/early/2012/11/26/CIRCULATIONAHA.112.136101World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer available in the
Permissions in the middle column of the Web page under Services. Further information about this process isOnce the online version of the published article for which permission is being requested is located, click Request
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Circulation Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on May 4, 2018
http://circ.ahajournals.org/D
ownloaded from


















